Embed Size (px)
Citation preview

Biodrugs 2004; 18 (4): 211-223NOVEL THERAPEUTIC STRATEGIES 1173-8804/04/0004-0211/$31.00/0
© 2004 Adis Data Information BV. All rights reserved.
New Advances and Potential Therapies for theTreatment of AsthmaMaria G. Belvisi, David J. Hele and Mark A. Birrell
Respiratory Pharmacology Group, Cardiothoracic Surgery, National Heart & Lung Institute, Faculty of Medicine, ImperialCollege, London, UK
ContentsAbstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2111. Therapeutic Approaches Targeting Specific Components or Steps in the Allergic Response in Asthma . . . . . . . . . . . . . . . . . . . . . . . 212
1.1 T Cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2121.1.1 Immunotherapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2121.1.2 Antigen Processing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2131.1.3 T-Cell Activation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2141.1.4 T-Cell Phenotype . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2141.1.5 T-Cell Chemotaxis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 215
1.2 Eosinophils . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2151.3 Mast Cells/Basophils . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 216
1.3.1 IgE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2161.3.2 Histamine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2171.3.3 Leukotrienes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2181.3.4 Tryptase/Chymase . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 218
1.4 Other Mediators . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2181.4.1 Adenosine Receptor Ligands . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2181.4.2 Prostanoids . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2181.4.3 TNFα . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 219
2. General Anti-Inflammatory Therapies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2192.1 Corticosteroids . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2192.2 Phosphodiesterase 4 Inhibitors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2192.3 p38 Mitogen-Activated Protein Kinase Inhibitors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2192.4 Peroxisome Proliferator-Activated Receptor Agonists . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2202.5 Lipoxins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 220
3. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 220
Asthma is a disease of the airways with an underlying inflammatory component. The prevalence andAbstracthealthcare burden of asthma is still rising and is predicted to continue to rise in the current century. Inhaledβ2-adrenoceptor agonists and corticosteroids form the basis of the treatments available to alleviate the symptomsof asthma. There is a need for novel, safe treatments to tackle the underlying inflammation that characterizesasthma pathology. Furthermore, there is a requirement for new treatments to be developed as oral therapy inorder to alleviate patient compliance issues, especially in children. A multitude of new approaches and newtargets are being investigated, which may provide opportunities for novel therapeutic interventions in thisdebilitating disease. For simplicity, these approaches can be divided into two categories. The first comprisestherapies directed against specific components or steps seen in allergic asthma. By ‘components’ we mean thekey inflammatory cells (T cells [in particular Th2], B cells, eosinophils, mast cells, basophils and antigenpresenting cells [APC]) and mediators (immunoglobulin E [IgE], cytokines, histamines, leukotrienes and

212 Belvisi et al.
prostanoids) believed to be involved in the chronic inflammation seen in asthma. By ‘steps’ we mean the allergicresponse, such as antigen processing and presentation, Th2-cell activation, B-cell isotype switching, mast cellinvolvement and airway remodeling. The other category of novel approaches to disease modification in asthmaencompasses general anti-inflammatory therapies including phosphodiesterase 4 (PDE4) inhibitors, p38mitogen-activated protein kinase (MAPK) inhibitors, peroxisome proliferator-activated receptor-γ (PPARγ)agonists, and lipoxins.
Inhaled β2-adrenoceptor agonists and corticosteroids form the The recognition of asthma as an inflammatory disorder hasshifted the focus of treatment from bronchodilator therapy tobasis of the treatments available to alleviate the symptoms ofanti-inflammatory drugs.[4] The aim of new therapies to treat theasthma. However, although in most cases effective treatments aredisease should therefore be directed at inhibiting airway inflam-available to control this disease, many patients are reluctant to usemation and modifying the progression of the disease, an approachinhaled corticosteroids because of the risk of adverse effects.that may improve the long-term morbidity associated with asthma.Therefore, despite their use, the prevalence and burden of asthmaAn excellent review by Holtzman (2003)[5] has recently beenis still increasing[1] and in industrialized countries asthma accountspublished that describes the recent drug discovery efforts beingfor 1% of all healthcare costs.[2] In the last 10 years, a largeadopted for the development of new asthma therapeutics.proportion of effort from within the pharmaceutical industry has
focused on optimizing existing therapies by improving the thera-1. Therapeutic Approaches Targeting Specificpeutic ratio and extending the duration of action of inhaled cortico-Components or Steps in the Allergic Responsesteroids to achieve once-a-day asthma control. New β2-adre-in Asthmanoceptor agonists have also been developed with a longer duration
of action. Taking this philosophy further and incorporating a newstrategy for improving patient compliance has led to the develop- 1.1 T Cellsment of therapies combining corticosteroids with long acting
There is considerable evidence to support a critical role for Tβ2-adrenoceptor agonist bronchodilators. However, there are somecells (particularly the involvement of T helper type 2 [Th2] cells)asthmatic patients at the more severe end of the scale that do notin asthma. Interestingly, there appears to be immune deviationderive enough benefit from the drugs currently in clinical use.from Th1 to Th2 cells in this disease, which may be caused by theThus, there is a need for more effective therapies to treat thisinability to inhibit the normal rise in the number of Th2 cellsdisease. To this end, research into the inflammatory mechanismsrelative to Th1 seen at birth. One theory (the ‘hygiene hypothesis’)that underlie asthma pathology is ongoing, in the hope of provid-suggests that this may be caused by the absence of bacterialing novel and more effective treatments for these diseases.[1]
infections and endotoxins which would normally stimulate the Th1Asthma is defined as a chronic inflammatory disorder of the
response.[6] Activated Th2 cells are believed to be directly orairways, and inflammation is believed to be the underlying cause
indirectly involved in most of the aspects of the inflammatoryof the symptoms of asthma: wheezing, breathlessness, chest tight-
response seen in asthma. For this reason, a great deal of research isness, and cough. Often these acute episodes may be triggered by a
focused on impacting on Th2 cell phenotype and function.specific allergen, exercise, stress, cold air, or upper respiratory
1.1.1 Immunotherapytract infections. These symptoms are associated with airflow limi-tation that is partly reversible, and with airway hyperreactivity to The aim of immunotherapy is to dampen the immune responsevarious stimuli that is thought to be as a result of the chronic to allergens and desensitize the asthmatic patient.[7] This has beeninflammatory process.[3] The inflammatory lesion seen in the achieved in the treatment of allergy (e.g. hay fever) by the subcuta-asthmatic airway is characterized by an infiltration of T cells, neous injection of small amounts of purified allergen[8] but haseosinophils, mast cells, macrophages and, in severe asthma or been less successful for the treatment of asthma. The obviousduring exacerbations, neutrophils. In addition to the influx of advantage of this sort of approach over the traditional smallinflammatory cells, changes in resident cells are also apparent in molecule anti-asthma drug is that specific allergen immunotherapythe asthmatic airway, and these phenomena contribute to the may suppress symptoms for several years after treatment is dis-airway remodeling seen in this disease (e.g. increase in the thick- continued. However, there are certain limitations to this form ofness of the airway smooth muscle layer, increase in goblet cell therapy, including the following: (i) the tolerance to one particularnumbers in the airway epithelium). allergen may not extend to other allergens; (ii) this approach
© 2004 Adis Data Information BV. All rights reserved. Biodrugs 2004; 18 (4)

Novel Therapies for Asthma 213
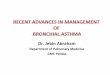
IL-5, IL-4, IL-13
Th2 cell
Therapeutic interventions
TCR
MHC II
CD28
B7 family
Cytokine modulators
Specific allergen immunotherapy,e.g. peptide sequences of Fel d 1
Inhibition of antigen presentation,e.g. cathespin S and F inhibitors
Inhibition of co-stimulation, e.g. ICOS, CD80/CD86 inhibitors,CTLA4-Ig
Inhibition of Th2 cell phenotype,e.g. IFNγ, IL-12, IL-18,CpG DNA immunotherapy,Mycobacterium vaccae,Notch ligands, CrTH2 receptor antagonist
Antigen presenting cell (e.g. dendritic cell)
Fig. 1. Different strategies can be employed to inhibit antigen presentation and T-cell activation including: (i) allergen immunotherapy; (ii) inhibition ofantigen presentation; (iii) inhibition of costimulatory pathways; (iv) inhibition of T helper 2 (Th2) cell phenotype; and (v) blockade of specific Th2 cytokines.All interventions are shown in boxes. ICOS = inducible costimulator; IFN = interferon; IL = interleukin; MHC II = major histocompatibility complex class II;TCR = T-cell receptor.
would not be possible in nonatopic (intrinsic) and occupational on cell surfaces for recognition by CD4(+) T cells. Proteolysis isasthma even though Th2 cells are believed to be involved; and required in this process both for degradation of the invariant chain(iii) the potential exists for adverse effects and in particular ana- protein (Ii) [CD74] to a ~3-kD peptide termed CLIP (class II–as-phylaxis, however, the use of purified extracts and hypoallergenic sociated invariant chain peptide) from class II-CD74 complexes toisoforms of these allergens has reduced the risk of anaphylactic allow subsequent binding of peptides, and for generation of theshock. In fact, many allergens are available as recombinant DNA- antigenic peptides. Enzymes such as aspartate proteases (e.g.derived peptides and can be presented directly to T cells, causing cathepsin D) and cysteine proteases (e.g. cathepsins B, S and L)an alteration in the T-cell response.[9] One recent improvement to are thought to be involved in this process. The cysteine en-this approach has been the use of peptide sequences corresponding doprotease, cathepsin S, mediates CD74 degradation in human andto T-cell epitopes of the allergen. These short, synthetic, allergen- mouse antigen-presenting cells and therefore it has been suggestedderived peptides induce T-cell anergy/tolerance, but because of that selective inhibition of cathepsin S may have an importanttheir length are unable to cross-link IgE, making them safer to therapeutic target in modulating class II-restricted immuneadminister as they are not able to cause anaphylaxis. Using pep- processes such as asthma. Indeed, in a murine model of allergictides from the sequence of the cat allergen, Fel d 1, investigators inflammation, a selective cathepsin S inhibitor has been shown tohave demonstrated the ability to induce transient T-cell activation, block increases in IgE titers and eosinophil infiltration into theresulting in isolated late asthmatic reactions, which are followed lungs.[12] There are currently efforts underway by several biotech-by prolonged periods of allergen-specific hyporesponsiveness, nology companies to develop small molecule inhibitors of theboth to peptide re-challenge and to cutaneous challenge with cathepsin family (and in particular, cathepsin S) for the treatmentwhole allergen. Thus, peptide therapy may prove safe and effica- of a wide range of inflammatory and autoimmune disorders, but ascious in the treatment of allergic diseases[10,11] (see figure 1). yet no clinical data exist.
Recent experiments show that cathepsin F, in a subset of APCs,1.1.2 Antigen Processing can also efficiently degrade CD74. Therefore, it would seem thatCD4+ T helper cells can only recognize, and hence be activated, different APCs can use distinct proteases to mediate MHC class II
by exogenous antigens that are presented by major histocompa- maturation and peptide loading, suggesting that other cathepsinstibility complex (MHC) class II molecules on antigen presenting may also be attractive targets for small molecule intervention forcells (APCs). MHC class II molecules display antigenic peptides the treatment of asthma[13] (see figure 1).
© 2004 Adis Data Information BV. All rights reserved. Biodrugs 2004; 18 (4)

214 Belvisi et al.
1.1.3 T-Cell Activation might actually exacerbate, lung inflammatory responses to inhaledActivation of naive T cells occurs through the delivery of two antigen.
signals. The first signal is triggered by the cognate interaction Another approach to suppress Th2 responses by stimulation ofbetween the CD4+ T-cell receptor and the APC-bound antigen to
Th1 responses is the use of CpG oligodeoxynucleotides (ODN).the MHC-II; the second occurs via co-stimulatory molecule inter-
These are synthetic oligodeoxynucleotides with immunostimu-actions, such as CD28 interacting with B7 molecules (CD80)/
latory sequences which, when used either alone or in combination(CD86). Without this co-stimulation, not only does the T cell not
with allergen, suppress Th2 responses. Strong immunostimulatorybecome activated but it can adopt a non-responsive state whereby
events are often driven by sequences containing unmethylatedeven with further correct stimulation present the T cell does not
CpG motifs that are more evident in microbial rather than verte-become activated. However, CD80/86-mediated co-stimulatory
brate DNA and so can be recognized by the innate immune system.pathways may be redundant and it may be necessary to block more
These motifs are thought to promote a switch from the usual Th2than one co-stimulatory molecule to achieve therapeutic efficacy.phenotype to Th1 responses through a signaling pathway involvingIt is for this reason that attention has recently focused on other co-Toll-like receptor 9.[21,22] In a recent study, CpG DNA-basedstimulatory pathways including inducible costimulator (ICOS)/immunotherapy inhibited acute and chronic markers of inflamma-B7-related protein (RP)-1 and PD-1/B7H-1.[14] The ICOS/tion and enhanced the release of IL-10 in an allergic mouseB7-RP-1 interaction has been characterized primarily as a co-model,[23] suggesting the involvement of Treg cells. In fact, it isstimulatory pathway that orchestrates events downstream of T-cellbelieved that the effects seen with CpG DNA treatment are notactivation, and ICOS has been singled out by its association withsolely due to promoting a Th1 response but also due to increasingTh2 effector activity. In fact, inhibition of ICOS during allergenthe number of Treg cells. The ability to increase Treg cells haschallenge has been shown to attenuate eosinophil accumulation inreceived a great deal of interest recently not only for the treatmentthe airway, IgE production, and cytokine release in theof asthma but also for autoimmune diseases. Clinical studies havebronchoalveolar lavage (BAL) fluid in models of antigen-inducednot been reported but clinical trials utilizing CpG ODNs areallergic airway inflammation.[15,16]
ongoing.[24] However, there are several phase I and phase II trialsAnother approach along the same theme has been to explore theunderway in a number of different therapeutic areas, includingeffects of CTLA4, which is a molecule expressed on activated Tasthma, and early indications are that CpG ODNs are well tolerat-cells and appears to act as an endogenous inhibitor of T-celled.[25] Recently work has been published suggesting stimulation ofactivation. Interestingly, a soluble fusion protein constructthe Notch pathway or exposure to heat-killed mycobacterium(CTLA4-Ig) is effective at blocking airway hyperreactivity, eosi-vaccae may also be a way of increasing Treg cells[26,27] and therebynophilia and IgE levels in a murine model of allergic asthma[17,18]
suppressing the Th2 phenotype.(see figure 1).
An alternative strategy to suppress the Th2 phenotype seen in1.1.4 T-Cell Phenotypethe asthmatic airway is to reduce the amount of key cytokinesDuring an immune response, naive CD4+ T helper cells canreleased by these cells (eg. IL-4, IL-5, IL-13) or to inhibit thedifferentiate into three main types, Th1, Th2 and Treg. There arepathway stimulated by these cytokines. IL-4 and IL-13 have beenmany factors that contribute to the decision as to which sub-type oflinked with not only Th2 phenotype switching but also many otherT helper cell is produced, including the dose of antigen, thefacets of the disease process including B-cell isotype switching,strength of T-cell receptor ligation, and the tissue the antigen isairway eosinophilia, airway hyperreactivity and airway remodel-exposed to, but the most important factor is reported to be theing. Beneficial effects were achieved in asthmatics using an in-cytokine profile present. For example, interleukin (IL)-12 andhaled soluble IL-4 receptor, altrakincept, an agent that sequestersinterferon (IFN)γ promote differentiation into Th1 cells, whereasIL-4 without mediating cellular activation.[28] IL-4 shares manyIL-4 promotes differentiation into Th2 cells. Additional mecha-biological functions with IL-13 as the IL-4 receptor α chain formsnisms that favor a Th1 cell phenotype include the expression ofan important component of both the IL-4 and IL-13 receptors.IL-12β2 receptor and production of IL-12 and IL-18 versus IL-10.Another study showed that a murine IL-4 receptor antagonist thatAlso, the cytokine profile that each T cell sub-type releases caninhibits IL-4 and IL-13-induced responses also inhibited antigen-inhibit the other, i.e. IFNγ tends to inhibit Th2 cell production andinduced airway eosinophilia and airway hyperreactivity in a mu-IL-4 inhibits Th1 cell production. In patients with asthma, not onlyrine model of asthma.[29] However, other groups have shown thatdid the administration of IFNγ not impact on symptoms, but it alsobecause IL-13 shares many of the biological functions of IL-4 andresulted in increased numbers of lymphocytes in the airways.[19,20]
is independently involved in other disease manifestations, thisThus, Th1 effector T cells do not appear to be able to prevent, and
© 2004 Adis Data Information BV. All rights reserved. Biodrugs 2004; 18 (4)

Novel Therapies for Asthma 215
cytokine, rather than IL-4, should be targeted for disease modifica- ing clinical trials for asthma although results have not yet beention.[30] reported. The hunt is also on for small molecule antagonists of
other chemokine receptors. As a cautionary note, because of theAnother way of impacting on IL-4 and IL-13 triggered eventsredundancy seen with chemokines and chemokine receptors, it iswould be to inhibit the IL-4/IL-13 receptor signaling pathway.yet to be determined whether the actions of specific antagonistsRecent research has involved exploring the possibility of targetingwill be enough to impact on the inflammation or disease state seenthe transcription factors activated by IL-4/IL-13, such as signalin patients with asthma.transducer and activator of transcription 6 (STAT6), GATA-bind-
ing protein 3 (GATA3) and friend of GATA1 (FOG1). In a murinemodel of allergic inflammation, Tomkinson et al. (2002)[31] have 1.2 Eosinophilsshown that the development of airway hyperreactivity was depen-dent on STAT6 (figure 1). Eosinophilic inflammation is a characteristic of the airway
inflammation seen in asthma and is believed to play a possible role1.1.5 T-Cell Chemotaxis in the disease pathogenesis.[41] A great deal of research has beenThe trafficking of Th2 cells to the lung and to and from the geared to inhibit eosinophil recruitment into the airways. The
lymph nodes are thought to be a key early step in the pathogenesis research includes impacting on cells believed to be involved inof asthma.[32] Th2 cells have been shown to preferentially express eosinophil recruitment such as Th2 cells (outlined above) and mastthe chemokine receptors CCR3, CCR4, CCR8, CXCR4 and the cells (outlined below). Other strategies have involved the use ofprostaglandin D2 receptor CRTH2, while Th1 cells preferentially general anti-inflammatory therapies, which will be discussed later.express CCR5, CXCR3, CXCR6 and CX3CR1.[33] It has been More direct approaches for reducing eosinophilic recruitment intosuggested that inhibiting the expression of the relevant the airway have involved impacting on the cytokines implicated inchemokines or blockade of the chemokine receptor may represent eosinophil differentiation and chemotaxis, such as IL-5. A human-attractive targets for asthma therapy. One example of the effective- ized antibody against IL-5, mepolizumab, has been developed andness of blocking the expression of chemokines comes from work tested in the clinic. Interestingly, it markedly reduced circulatingreported by Mathew et al.[34] in which they showed, in a murine and sputum eosinophils in patients with asthma but was withoutallergen model, that STAT6 controls chemokine production and effect on early and late responses to allergen challenge, and did notTh2 cell trafficking in allergic pulmonary inflammation. reduce airway reactivity to methacholine challenge.[42] A study to
determine the effect of mepolizumab on airway tissue eosinophilsTargeting a specific chemokine is problematic because of thehas shown that it reduces but does not deplete eosinophils from theamount of redundancy in the ligand/receptor interactions. CCR3airway or bone marrow, suggesting that the role of the eosinophilreceptors can be activated by a number of chemokines includingin asthma is at present unclear.[43] A preliminary study with aeotaxin, CCL5 and monocyte chemotactic protein 4 (MCP-4,different humanized antibody against IL-5, reslizumab, has report-CCL13); these chemokines in turn can activate other chemokineed similar results.[44] A recent safety study by the same groupreceptors. Because of this, many pharmaceutical companies haveshowed that the antibody was without adverse effects and that itattempted to find chemokine receptor antagonists rather thandemonstrated an improvement in baseline forced expiratory vol-target specific chemokines. Specific chemokine receptor antago-ume in 1 second (FEV1) in patients with severe persistent asth-nists would inhibit the actions of a number of chemokines on thatma.[45] Further, more powerful clinical studies are needed to con-receptor. An additional advantage with receptor blockade is thefirm this observation.inhibition of chemotaxis of other inflammatory cells. For example,
CCR3 receptors, as well as being present on Th2 cells, are also It would seem from the information available that inhibitingpresent on eosinophils and mast cells, both of which are thought to IL-5 alone is not sufficient to deplete lung tissue eosinophils. Evenbe involved in the inflammation seen in asthma. Many pharmaceu- in animal models of asthma there was residual eosinophilia in thetical companies have small-molecule CCR3 receptor antagonists airways after anti-IL-5 therapy.[46] It has been suggested thatin development including SB297006, SB238437,[35] and combination therapy of anti-IL-5 (to block bone marrow matura-UCB35625,[36] and others that are in the pipeline from Bristol tion of eosinophils) and a CCR3 receptor antagonist (to blockMyers Squibb,[37] Abbott[38] Novartis, Roche, Merck, Banyu and eosinophil lung tissue accumulation) may lead to a more promis-AstraZeneca.[39] Studies described recently in both rodents and ing therapy in the clinic than the use of an anti-IL-5 therapyprimates using two different CCR3 antagonists, RO1164875 and alone.[47] Another possibility is that the apparent lack of efficacyRO3202947, showed reductions in eosinophil influx and airway seen in some of these studies may be due to redundancy, in that thehyper-responsiveness.[40] Some of these compounds are undergo- role of IL-5 could be performed by granulocyte-macrophage colo-
© 2004 Adis Data Information BV. All rights reserved. Biodrugs 2004; 18 (4)

216 Belvisi et al.
Th2 cell
B cellMast cell Eosinophil
IgE Mediator releaseMajor basic protein
IL-4,5,13IL-4,5,13
IL-4 IL-5
Asthma phenotype
Anti-IL-4, 13, 5
Anti-IgE
Mast cell inhibitors,e.g. anti-histamines,LT receptor antagonists,tryptase/chymase inhibitors,PAR-2 antagonist
Mediator release,e.g. histamine, lipidscytokines
Eosinophilchemotaxis inhibitors,e.g. CCR3antagonist
Adhesion inhibitors,e.g.VLA4 inhibitor
Fig. 2. Inhibition of specific inflammatory processes and in particular eosinophil, mast cell and B-cell functions. Several therapeutic strategies may bepossible to inhibit eosinophil chemotaxis and function (e.g. blockade of adhesion molecules and chemokine receptors). IgE, from B cells, can be blockedusing an IgE monoclonal antibody and mast cell mediators inhibited by selective blockers (e.g. antihistamines, leukotriene [LT] receptor antagonists,tryptase/chymase inhibitors, protease-activated receptor-2 [PAR-2] receptor antagonists). Cytokines (IL-4, 5, 13), from Th2 cells, can be blocked bymonoclonal antibodies or soluble receptors. All interventions are shown in boxes. CCR3 = chemokine, cc motif, receptor 3; IL = interleukin; Th2 = T helper2; VLA4 = very late antigen-4.
ny stimulating factor (GM-CSF) or IL-3 after IL-5 has been 1.3 Mast Cells/Basophils
eliminated. Therefore, an approach that may have more impactMast cells and basophils have been reported to be present inwould be to interfere with the common pathway that these
BAL fluid and bronchial biopsies from asthmatic lungs, and,cytokines signal through. A monoclonal antibody (BION-1) di-although not necessarily increased in number, they are in a height-rected against the common βc (signaling) subunit of the cytokineened activity state.[54,55] These cells are linked to the allergicreceptor has been developed which allows the simultaneous inhi-response, in that allergen can trigger degranulation by cross-bition of all three cytokines.[48] Ramshaw et al.[49] have solved thelinking specific IgE bound to the FcεRI receptor on cells.structure of BION-1 bound to the βc subunit and revealed an areaMediators released upon degranulation have been implicated inwhich should prove an attractive target for the rational design ofthe early and late response in atopic asthma (eg. histamine, leuko-small-molecule inhibitors of βc function.trienes, tryptase, chymase) [see figure 2].
Another area of interest for inhibiting airway eosinophilia isinhibition of very late antigen-4 (VLA-4). VLA-4 is a heter- 1.3.1 IgEodimeric cell surface molecule found on mononuclear cells and its Several therapies have been proposed to reduce the amount ornatural ligand is vascular cell adhesion molecule (VCAM-1). The effect of IgE, thereby reducing the degranulation of mast cell andVLA-4 receptor is believed to be responsible for mononuclear cell basophils. Some of these involve inhibiting the B-cell isotypetrafficking and anti-VLA-4 and VLA-4 antagonists have been switching, proliferation and activation by either impacting on IL-4shown to impact on animal models of asthma.[50-52] Initial commu- (and IL-13) whether it be directly or by interrupting downstreamnications, however, have indicated little efficacy of anti-VLA-4 signaling (discussed above). Similarly, interruption of FcεRI sig-mAb in asthma despite success in other inflammatory condi- naling by blocking its interaction with ligand or downstreamtions.[53] It has been suggested that if this agent was retested in a signaling molecules such as spleen tyrosine kinase (SYK) are alsopatient population that was purely atopic, and the delivery was strategies under investigation. However, the therapy that has re-improved, this type of therapy may still show beneficial effects ceived most interest recently is the one designed to deplete IgE.(see figure 2). Depleting IgE in animal models by the use of an anti-IgE mAb has
© 2004 Adis Data Information BV. All rights reserved. Biodrugs 2004; 18 (4)

Novel Therapies for Asthma 217
been shown to reduce eosinophilic inflammation.[56] Phase III cyclase and activation leads to increasing levels of cAMP. Instudies have been conducted with the recombinant human anti- contrast, the HR3 receptor is negatively coupled to adenylylIgE, omalizumab, resulting in a reduction in early and late phase cyclase, and signaling involves G(i/o), leading to inhibition ofresponses and reduced eosinophil counts in sputum, and the treat- cAMP. HR3 receptors have been found as pre-junctional receptorsment has been shown to be safe and well tolerated.[57,58] A reduc- both in the peripheral and central nervous system. HR4 receptorstion in inhaled corticosteroid requirement has also been demon- are coupled to G(i/o), inhibiting forskolin-induced cAMP forma-strated in patients receiving omalizumab.[59] The importance of tion (similar to the HR3). HR4 receptors demonstrate high levelsomalizumab as an add-on therapy when treating patients with of expression on neutrophils, eosinophils and T cells.severe asthma has been demonstrated in three large placebo con-
Recent data suggests that histamine affects the maturation oftrolled trials. Omalizumab treatment halved the rate of significant
the immune cells and alters their activation, polarization, chemo-asthma exacerbations, reduced the number of re-hospitalizations,
taxis and effector functions. Histamine also regulates antigen-improved quality of life and asthma symptom scores, and im-
specific T cells. Furthermore, it has been suggested that differen-proved baseline peak expiratory flow rate.[60-62] The greatest bene-tial patterns of expression on Th1 and Th2 cells determine T-cellfit with this treatment was seen in patients with the most severeresponses following histamine stimulation. Th1 cells expressasthma. These results suggest that specific inhibition of IgE maypredominantly, but not exclusively, the HR1 receptor, whereasprovide an important novel therapeutic option for the treatment ofTh2 cells express increased levels of the HR2 receptor.[70] It hassevere asthma.been suggested that histamine enhances Th1 type responsesthrough the activation of the HR1 receptor, whereas both Th1 and
1.3.2 HistamineTh2 type responses are negatively regulated by activation of the
Histamine was one of the first mediators implicated in the HR2 receptor. In fact, in mice the deletion of the HR1 receptorpathophysiology of asthma. Histamine binds and activates four results in a dominant Th2 type phenotype with the secretion ofdifferent G protein coupled receptors (HR1–4). Elevated levels of IL-4 and IL-13, whereas deletion of the HR2 receptor results inhistamine have been measured in BAL fluid from asthmatic pa- upregulation of Th1 and Th2 responses.tients compared with non-asthmatic individuals.[63] Histamine is
Interestingly, the effect of histamine on eosinophil migrationreleased from mast cells and basophils and can cause bronchocon-
depends on dose. High doses of histamine inhibit chemotaxis viastriction,[64] plasma extravasation,[65] mucus secretion,[66] induceactivation of HR2 and low doses enhance eosinophil chemotaxisairway smooth muscle proliferation[67] and augment cholinergicthrough activation of the HR1. A role for the HR4 receptor inbronchoconstriction[68] through its actions on HR1 receptors. Ineosinophil chemotaxis has also been suggested. A similar profile isisolated airway smooth muscle preparations from asthmatic pa-observed on dendritic cells with HR2 acting as a suppressivetients and non-asthmatic individuals, it has been shown that themolecule for antigen presenting capacity, while HR1 and HR3 actcontraction responses to histamine are the same, which suggestsas positive stimulators. In immature dendritic cells, histaminethat airway hyper-responsiveness to histamine in the asthmaticinduces intracellular Ca++ flux, actin polymerization, and chemo-lung is not due to alteration in HR1 receptors in the airways.[69]
taxis as a result of stimulation of the HR1 and HR3 receptorOther histamine receptors, HR2 and HR3, have also been identi-subtypes. Mature dendritic cells lose these responses and hista-fied in human airways. Although their relevance in asthmaticmine, via the HR2 receptor, dose-dependently enhances intracellu-airway inflammation is not known, activation of HR2 on airwaylar cAMP levels and stimulates IL-10 secretion, while inhibitingepithelial cells can cause release of prostaglandin E2 (PGE2),the production of IL-12.[70] Therefore, it would appear that onwhich despite being a tussive agent, is thought to have beneficialbalance HR1 receptors are involved in activating immune cellsbronchodilatory activity in the airways.[64]
whereas HR2 receptors are involved in suppressing inflammatoryThe G-protein G(q/11)-coupled HR1 receptor is responsible for
responses.many of the symptoms observed in allergic diseases. Activation of
Thus far antihistamine therapy has been shown to provide onlyG(q/11) stimulates inositol phosphate signaling pathways result-limited clinical benefit for patients with asthma.[71] However,ing in formation of inositol -1,4,5-triphosphate and diacylglycerolrecently there have been suggestions[72] that there may be a role forand a consequent increase in intracellular calcium concentrations.second-generation antihistamines in treating asthma, with patientIn addition, HR1 has been shown to activate phospholipase D, A2
selection as well as dosing regimens being important therapeuticand NF-kβ, however the functional consequences of this are notknown. The HR2 receptor is positively coupled to adenylyl considerations.
© 2004 Adis Data Information BV. All rights reserved. Biodrugs 2004; 18 (4)

218 Belvisi et al.
1.3.3 Leukotrienes flux when compared with wild type mice.[85] Airway hyperreactiv-Cysteinyl leukotrienes are important pro-inflammatory ity was similarly affected. APC-366 has been tested in a short-term
mediators in the pathogenesis of asthma. They are formed when study in patients with atopic asthma, where it reduced the latearachidonic acid is metabolized via 5-lipoxygenase to give rise to asthmatic response and the fall in FEV1 caused by antigen chal-leukotrienes C4, D4 and E4. The only development of a novel drug lenge.[86] An inhibitor at the PAR2 receptor may also be worthy ofclass for the treatment of asthma in recent years has been the investigation.introduction of cysteinyl leukotriene antagonists such as
1.4 Other Mediatorsmontelukast, zafirlukast, and pranlukast, and the 5-lipoxygenaseinhibitor, zileuton.[73] The cysteinyl leukotrienes are potent
1.4.1 Adenosine Receptor Ligandsbronchoconstricting agents that have been shown to play a role inAdenosine has long been implicated in the pathophysiology ofboth the increase in airway hyperreactivity seen in asthma and in
asthma and there is much evidence in the literature to support thisairway remodeling. Recent evidence from a murine model ofconcept.[87-90] A recent review highlights the A1, A2A and A2Basthma has shown that a leukotriene receptor antagonist can inhib-receptor-selective molecules currently in development.[91]it the remodeling process, including eosinophil trafficking andEPI-2010, an antisense oligonucleotide that targets the human A1degranulation, cytokine release, mucus gland hyperplasia andreceptor,[92] entered phase II clinical trials in 2001 as an inhaledhypersecretion, smooth muscle cell hyperplasia, collagen deposi-formulation for asthma, but development has since been discontin-tion, and lung fibrosis.[74] A review of the benefits achieved byued. Activation of the A2A receptor is known to suppress inflam-using anti-leukotrienes as an add-on therapy to inhaled corticoste-mation and is therefore another potential target. To this end, aroids showed a modest improvement in asthma control but did notselective A2A receptor agonist, CGS-21680, was developed thatallow a lowering of the steroid dose.[75] Another review proposesshowed anti-inflammatory activity similar to that of the steroidthat these compounds provide an effective anti-inflammatorybudesonide in an animal model of allergic asthma.[93] This com-treatment for asthma.[76] While there is evidence that the leuko-pound did not advance to the clinic. GW-328267, an inhaled A2Atriene antagonists are effective anti-asthma agents in young peo-receptor agonist, is in phase I clinical development for asthma andple, there are suggestions that they are less effective in those agedCOPD.[94] There is evidence to support the involvement of the A2Bover 50 years,[77] that the long acting β-agonists are more effec-receptor in mast cell activation, and selective antagonists for thistive,[78] and that some patients respond better than others.[9] Therereceptor could be beneficial in asthma.[90] There are no selectiveis evidence to suggest that leukotriene antagonists may provideA3 receptor antagonists in clinical development, although there iseffective therapy for aspirin-sensitive asthma and exercise-in-a report in the literature suggesting that adenosine acting at the A3duced asthma.[79] This suggests that it may be possible to predictreceptor may contribute to the anti-inflammatory activity of theo-which patients will respond well to these drugs, and thereforephylline in vivo.[95] It has also been suggested that both agonistscareful patient selection in the future may reveal the benefits ofand antagonists at the A3 receptor may have potential in thethese compounds.treatment of asthma, as adenosine exhibits both pro- and anti-
1.3.4 Tryptase/Chymaseinflammatory actions via this receptor.[96]
The degranulation of mast cells is an important event in allergic1.4.2 Prostanoidsasthma, and results in the release of many different mediators such
as histamine and the serine protease, tryptase. Tryptase is thought Prostanoids consist of several groups of lipid mediators, pros-to play a role in airway remodeling, increased mucus secretion,[80] taglandins, prostacyclin, and thromboxanes, which are generatedand fibroblast proliferation via protease-activated receptor-2 from arachidonic acid, mainly through the cyclo-oxygenase path-(PAR2)[81] in asthma. Tryptase inhibitors including APC-366,[82] way. One of the prostaglandins produced, PGE2, is thought to haveAMG-126737[83] and MOL-6131[84] have been developed and beneficial effects in the airways. It has been shown, at low concen-tested in animal models and the results from these studies support trations, to relax human airway smooth muscle in vitro[97] andthe notion that selective inhibition of tryptase is a reasonable exhibit bronchodilation in vivo in healthy subjects, but may inducetherapeutic target for asthma. Further recent evidence has demon- airway constriction in asthmatic patients through activation ofstrated a role for PAR2 in the development of allergic inflamma- reflex cholinergic bronchoconstriction.[98] PGE2 also inhibits thetion in the airway. Wild type mice and mice lacking or overexpres- proliferation of airway smooth muscle[99] and the release ofsing PAR2 were subjected to antigen challenge; those lacking mediators from mast cells, monocytes, neutrophils and eosino-PAR2 showed a greatly reduced eosinophil influx into the airways phils. Inhalation of PGE2 has been suggested to reduce early andwhile those over expressing PAR2 showed greatly enhanced in- late responses to allergen challenge.[100] However, PGE2 also
© 2004 Adis Data Information BV. All rights reserved. Biodrugs 2004; 18 (4)

Novel Therapies for Asthma 219
exhibits tussive effects.[101] Other prostanoids such as PGD2, portions of these inhaled glucocorticoids reaching the systemicPGF2α, the isoprostane 8-epi-PGF2α, and thromboxanes have circulation. These adverse effects have led to the search not onlybeen shown to constrict human airways in vitro.[102,103] In the for novel anti-inflammatory approaches but also for improvedclinic, non-selective prostanoid receptor antagonists and corticosteroids.[112] Several new corticosteroids are in develop-thromboxane synthase inhibitors have not shown any beneficial ment, including mometasone furoate,[113,114] and some of these areeffects in patients with asthma. The anti-inflammatory actions of predicted to have a reduced adverse-effect profile, including thePGE2 have led to the suggestion that prostanoid receptor agonists soft steroid loteprednol etabonate,[115] and ciclesonide.[116,117] Re-may be useful for the treatment of airway inflammatory diseases. cent studies with ciclesonide have demonstrated both efficacy inIn particular, the focus has been on the development of agonists at the treatment of asthma[118,119] and an improved adverse-effectthe prostaglandin E receptor 2 (EP2), as this receptor is positively profile.[120,121]
coupled to adenylyl cyclase. The provision of longer acting β-agonists such as formoteroland salmeterol has also been a goal for the pharmaceutical indus-
1.4.3 TNFαtry, as have combinations of steroids and β-agonists such as
TNFα is also implicated in the inflammatory response in asth-fluticasone with salmeterol, or budesonide with formoterol. This
ma, and has already proved to be an attractive target with theapproach may confer advantages in both treatment and compli-
development of etanercept, a soluble TNF receptor hybrid mole-ance.
cule, and infliximab, an antibody against TNFα.[104] Adalimumabis a humanized monoclonal antibody against TNFα that was
2.2 Phosphodiesterase 4 Inhibitorsapproved by the US FDA in December 2002. These products weredeveloped to treat rheumatoid arthritis and inflammatory bowel Phosphodiesterase 4 (PDE4) inhibitors, although in develop-disease, however, clinical trials are now underway to determine ment as potential therapies for COPD, are now, because of theirtheir effect in patients with severe asthma.[105] Small molecule anti-inflammatory properties combined with bronchodilator activ-inhibitors of TNFα are now being sought in order to avoid some of ity, being considered as potential therapies for asthma. The secondthe problems involved with antibody therapy, and specifically generation PDE4 inhibitors, roflumilast[122] and cilomilast,[123]
with TNFα neutralizing agents, such as the development of tuber- lead the field, although it is probable that the development ofculosis and other such opportunistic infections and an adverse cilomilast for asthma has been discontinued.[124] Roflumilast haseffect on congestive heart failure.[106] A novel approach to reduc- been shown to significantly improve lung function in patients withing TNFα levels could be provided by inhibitors of TNFα-con- exercise-induced asthma,[125] and in a 12-week study in asthma,verting enzyme (TACE).[107] A study with two dual TACE/MMP roflumilast produced a dose-dependent improvement in asthmainhibitors, PKF 242-484 and PKF 241-466, demonstrated com- control and was well tolerated.[126] The latest clinical findings inplete inhibition of TNFα and a reduction in inflammatory cell asthma show that roflumilast improves asthma control to a levelinflux in an animal model of acute lung inflammation,[108] sug- equivalent to beclamethasone dipropionate. Furthermore, roflumi-gesting that these compounds may have therapeutic potential for last significantly and dose-dependently attenuates the late asthmat-the treatment of asthma. ic reaction, indicating that its clinical efficacy in asthma is based
on its anti-inflammatory activity. One other compound worthy of2. General Anti-Inflammatory Therapies mention in this class is AWD12-281, which recently demonstrated
efficacy in animal models of asthma when given by the inhaledroute.[127] It is also claimed that when given orally, intravenously,2.1 Corticosteroidsor intratracheally, AWD12-281 has a lower emetic potential than
Inhaled corticosteroids provide the current maintenance ther- cilomilast or roflumilast, which may confer an advantage on thisapy of choice for asthma and, with the bronchodilator β-agonists compound when it reaches the clinic. Interestingly, recent datafor acute symptom relief, they form the mainstay of current suggests that roflumilast may also inhibit the remodeling processtherapy for the disease. However, steroid treatment, especially if in a chronic asthma model in the mouse.[128]
high or frequent doses are required, is associated with a range ofadverse effects including adrenal suppression and an adverse 2.3 p38 Mitogen-Activated Protein Kinase Inhibitorseffect on growth and bone formation[109,110] including the develop-ment of corticosteroid-induced osteoporosis.[111] These adverse The p38 mitogen-activated protein kinase (MAPK) signalingeffects and many others, such as skin thinning, easy bruising, pathway is common to many pro-inflammatory cytokines andcataracts, oral candidiasis and dysphonia, result from significant chemokines,[129] and thus presents an attractive target for the
© 2004 Adis Data Information BV. All rights reserved. Biodrugs 2004; 18 (4)

220 Belvisi et al.
development of nonpeptide inhibitors.[130] Several p38 MAPK also demonstrated that transgenic expression of human LXA4
inhibitors are being examined for their potential to provide novel receptors in murine leukocytes led to significant inhibition oftherapies for asthma.[131] Two p38 MAPK inhibitors, SB-203580 pulmonary inflammation and eicosanoid-initiated eosinophil tis-and SB-239063, have shown anti-inflammatory activity in animal sue infiltration. These findings suggest that the lipoxin pathwaymodels of airway inflammation.[132,133] It remains to be seen if this may offer a novel multi-pronged therapeutic approach to theactivity will transfer to efficacy in the clinic. An interesting recent treatment of asthma.observation has shown that SB-203580 may have potential in
3. Conclusionreversing glucocorticoid insensitivity and re-establishing the bene-ficial effects of glucocorticoids in patients with severe asthma,[134]
Asthma is a disease of the airways with an inflammatorythus suggesting that a p38 MAPK inhibitor may have potential ascomponent. Asthma has been studied for many years and thean add-on therapy to corticosteroid treatment in asthma. A numberunderstanding of the pathophysiology resulting from this researchof these compounds are about to have their anti-inflammatoryhas led to the development of several effective therapies to treatpotential examined in the clinic: SB-281832 (phase I), SCIO-469the symptoms of the disease. However, the incidence of asthma is(phase II), and the newer compounds VX-702 and VX-850still on the increase and further understanding of the basic mecha-(phase I); and the development of inhaled formulations for thenisms central to the development of the disease has resulted in thetreatment of asthma is also underway.[131]
development of novel therapeutic strategies to improve the treat-ment options for the disease. Improvements to the current therapy2.4 Peroxisome Proliferator-Activated Receptor Agonistsavailable to treat asthma in the form of longer acting β-agonists,safer corticosteroids, and combination therapies, are ongoing butPeroxisome proliferator-activated receptor γ (PPARγ) is aas yet no treatment has been shown to impact significantly on themember of the nuclear hormone family and the development ofdevelopment of asthma. The identification of some of the process-PPARγ agonists has been suggested as a novel anti-inflammatoryes and pathways involved in the inflammatory responses in asthmatarget for asthma.[135] An immunoregulatory role for PPARγ hashas led to the identification of novel targets, and this has allowedbeen proposed in airway epithelial cells, where it has been shownpharmaceutical companies to develop novel therapies, some ofto antagonize pro-inflammatory pathways in the airways.[136] Awhich have progressed to the clinic. It will be interesting torole for PPARγ has also been demonstrated in human asthmaticobserve which of the many and diverse approaches will result inairways, where increased expression has been thought to representsafe, novel treatments, and whether these treatments can effective-a regulatory mechanism aimed at limiting airway inflamma-ly suppress inflammation in the airways and thereby start to impacttion.[137] A recent study employing a murine model of asthmaon the prevalence of asthma worldwide.demonstrated that selective PPARγ but not PPARδ agonists limit-
ed the development of ovalbumin-induced airway inflamma-Acknowledgmentstion.[138] Several pharmaceutical companies are developing newer
and more potent PPARγ agonists for various inflammatory indica-Drs Birrell and Hele were funded by a grant from GlaxoSmithKline.
tions,[139] but whether this approach proves to be beneficial intreating inflammatory disease remains to be seen.
References1. Pahl A, Szelenyi I. Asthma therapy in the new millennium. Inflamm Res 2002; 51:
2.5 Lipoxins 273-822. Rutten Van Molken MP, Feenstra TL. The burden of asthma and chronic obstruc-
tive pulmonary disease: data from The Netherlands. Pharmacoeconomics 2001;The endogenous lipoxins (LX) have been suggested as anti-19: 1-6inflammatory mediators with potential in the treatment of inflam-
3. Global Initiative for Asthma. Global strategy for asthma management and preven-matory diseases of the airways such as asthma.[140] LXA4 has been tion. NHLBI/WHO Workshop Report. National Institutes of Health. National
Heart Lung and Blood Institute. Publication number 02-3659 2002: 16shown to be upregulated in the sputum of severe asthmatics, and4. Bjermer L. History and future perspectives of treating asthma as a systemic and
LXA4 and LXB4 have been shown to inhibit IL-8 release in small airway disease. Respir Med 2001; 95: 703-195. Holtzman MJ. Drug development for asthma. Am J Respir Cell Mol Biol 2003; 29:vitro.[141] Allergen challenge has also been shown to initiate air-
163-71way biosynthesis of LXA4 and increase expression of its receptor.6. Holt PG, Yabuhara A, Prescott S, et al. Allergen recognition in the origin of
Administration of a stable analog of LXA4 blocked both airway asthma. Ciba Found Symp 1997; 206: 35-497. Norman PS. Immunotherapy: past and present. J Allergy Clin Immunol 1998; 102:hyperreactivity and pulmonary inflammation, as shown by de-
1-10creased leukocytes and mediators, including IL-5, IL-13, eotaxin, 8. Durham SR, Walker SM, Varga EM, et al. Long-term clinical efficacy of grass-prostanoids and cysteinyl leukotrienes.[142] The same investigators pollen immunotherapy. N Engl J Med 1999; 341: 468-75
© 2004 Adis Data Information BV. All rights reserved. Biodrugs 2004; 18 (4)

Novel Therapies for Asthma 221
9. Hansel TT, Barnes PJ. Novel drugs for treating asthma. Curr Allergy Asthma Rep 34. Mathew A, MacLean JA, DeHaan E, et al. Signal transducer and activator of2001; 1: 164-73 transcription 6 controls chemokine production and T helper cell type 2 cell
trafficking in allergic pulmonary inflammation. J Exp Med 2001 May 7; 19310. Larche M. Anti-T-cell strategies in the treatment of allergic disease. Allergy 2002;(9): 1087-9657: 20-3
35. White JR, Lee JM, Dede K, et al. Identification of potent, selective non-peptide CC11. Oldfield WL, Larche M, Kay AB. Effect of T-cell peptides derived from Fel d 1 onchemokine receptor-3 antagonist that inhibits eotaxin-, eotaxin-2-, and mono-allergic reactions and cytokine production in patients sensitive to cats: acyte chemotactic protein-4-induced eosinophil migration. J Biol Chem 2000;randomised controlled trial. Lancet 2002 Jul 6; 360: 47-53275: 626-3112. Riese RJ, Mitchell RN, Villadangos JA, et al. Cathepsin S activity regulates antigen
presentation and immunity. J Clin Invest 1998 Jun 1; 101 (11): 2351-63 36. Sabroe I, Peck MJ, Van Keulen BJ, et al. A small molecule antagonist ofchemokine receptors CCR1 and CCR3. Potent inhibition of eosinophil function13. Shi GP, Bryant RA, Riese R, et al. Role for cathepsin F in invariant chainand CCR3-mediated HIV-1 entry. J Biol Chem 2000; 275: 985-92processing and major histocompatibility complex class II peptide loading by
macrophages. J Exp Med 2000 Apr 3; 191 (7): 1177-86 37. Wacker DA, Santella III JB, Gardner DS, et al. CCR3 antagonists: a potential newtherapy for the treatment of asthma: discovery and structure-activity relation-14. Dong H, Zhu G, Tamada K, et al. B7-H1, a third member of the B7 family, co-ship. Bioorg Med Chem Lett 2002; 12: 1785-9stimulates T cell proliferation and interleukin 10 secretion. Nat Med 2001; 5:
1365-9 38. Warrior U, McKeegan EM, Rottinghaus SM, et al. Identification and characterisa-15. Gonzalo JA, Tian J, Delaney T, et al. ICOS is critical for T helper cell-mediated tion of novel antagonists of the CCR3 receptor. J Biomol Screen 2003 Jun; 8
lung mucosal inflammatory responses. Nat Immunol 2001; 2: 597-604 (3): 324-3116. Tesciuba AG, Subudhi S, Rother RP, et al. Inducible costimulator regulates 39. D’ambrosio D, Mariani M, Panina-Bordignon P, et al. Chemokines and their
Th2-mediated inflammation, but not Th2 differentiation, in a model of allergic receptors guiding T lymphocyte recruitment in lung inflammation. Am J Respirairway disease. J Immunol 2001; 167: 1996-2003 Crit Care Med 2001; 164: 1266-75
17. Van Oosterhout AJ, Hofstra CL, Shields R. Murine CTLA4-IgG treatment inhibits 40. Gater P, Satjawatcharaphong C, Staley C, et al. Effect of orally active CCR3airway eosinophilia and hyperresponsiveness and attenuates IgE upregulation antagonists in animal models of allergic airway inflammation [abstract]. Am Jin murine model of allergic asthma. Am J Respir Cell Mol Biol 1997; 17: Respir Crit Care Med 2002; 165: A313386-92 41. Bousquet J, Chanez P, Lacoste JY, et al. Eosinophilic inflammation in asthma. N
18. Deurloo DT, Van Esch BC, Hofstra CL, et al. CTLA4-IgG reverses asthma Engl J Med 1990 Oct 11; 323 (15): 1033-9manifestations in a mild but not in a more “severe” ongoing murine model. Am 42. Leckie MJ, Ten Brinke A, Khan J, et al. Effects of an interleukin-5 blockingJ Respir Cell Mol Biol 2001; 25: 751-60 monoclonal antibody on eosinophils, airway hyper-responsiveness, and the late
19. Boguniewicz M, Martin RJ, Martin D, et al. The effects of nebulized recombinant asthmatic response. Lancet 2001; 356: 2144-8interferon-gamma in asthmatic airways. J Allergy Clin Immunol 1995 Jan; 95
43. Flood-Page PT, Menzies-Gow AN, Kay AB, et al. Eosinophil’s role remains(1 Pt 1): 133-5
uncertain as anti-interleukin-5 only partially depletes numbers in asthmatic20. Martin RJ, Boguniewicz M, Henson JE, et al. The effects of inhaled interferon airway. Am J Respir Crit Care Med 2003; 167: 199-204
gamma in normal human airways. Am Rev Respir Dis 1993 Dec; 148 (6 Pt 1):44. Kips JC, Tournoy KG, Pauwels RA. New asthma therapies: suppression of the
1677-82effect of interleukin (IL)-4 and IL-5. Eur Respir J 2001; 17: 499-506
21. Hemmi H, Takeuchi O, Kawai T, et al. A toll-like receptor recognizes bacterial45. Kips JC, O’Connor BJ, Langley SJ, et al. Effect of SCH55700, a humanized anti-DNA. Nature 2000; 408: 740-5
human interleukin-5 antibody, in severe persistent asthma: a pilot study. Am J22. Silverman ES, Drazen JM. Immunostimulatory DNA for asthma: better than eating
Respir Crit Care Med 2003; 167: 1655-9dirt. Am J Respir Cell Mol Biol 2003 Jun; 28 (6): 645-7
46. Foster PS, Martinez-Moczygemba M, Huston DP, et al. Interleukins-4, -5, and –13:23. Jain VV, Businga TR, Kitagaki K, et al. Mucosal immunotherapy with CpG
emerging therapeutic targets in allergic disease. Pharmacol Ther 2002; 94:oligodeoxynucleotides reverses a murine model of chronic asthma induced by
253-64repeated antigen exposure. Am J Physiol Lung Cell Mol Physiol 2003 Nov; 285
47. Kay AB, Menzies-Gow A. Eosinophils and interleukin-5: the debate continues.(5): 4137-46Am J Respir Crit Care Med 2003 Jun 15; 167 (12): 1586-724. Kline JN. DNA therapy for asthma. Curr Opin Allergy Clin Immunol 2002; 2:
48. Sun Q, Jones K, McClure B, et al. Simultaneous antagonism of IL-5, granulocyte-69-73macrophage colony stimulating factor, and IL-3 stimulation of human eosino-25. Uhlmann E, Vollmer J. Recent advances in the development of immunostimulatoryphils by targeting the common cytokine binding site of their receptors. Bloodoligonucleotides. Curr Opin Drug Discov Devel 2003 Mar; 6 (2): 204-171999; 94: 1943-5126. Ng WF, Duggan PJ, Ponchel F, et al. Human CD4(+)CD25(+) cells: a naturally
49. Ramshaw HS, Woodcock JM, Bagley CJ, et al. New approaches in the treatment ofoccurring population of regulatory T cells. Blood 2001 Nov 1; 98 (9): 2736-44asthma. Immunol Cell Biol 2001; 79: 154-927. Zuany-Amorim C, Manlius C, Trifilieff A, et al. Long-term protective and antigen-
50. Abraham WM, Gill A, Ahmed A, et al. A small-molecule, tight-binding inhibitorspecific effect of heat-killed Mycobacterium vaccae in a murine model ofof the integrin alpha(4)beta(1) blocks antigen-induced airway responses andallergic pulmonary inflammation. J Immunol 2002 Aug 1; 169 (3): 1492-9inflammation in experimental asthma in sheep. Am J Respir Crit Care Med28. Borish LC, Nelson HS, Corren J, et al. Efficacy of soluble IL-4 receptor for the2000 Aug; 162 (2 Pt 1): 603-11treatment of adults with asthma. J Allergy Clin Immunol 2001; 107: 963-70
51. Kudlacz E, Whitney C, Andresen C, et al. Pulmonary eosinophilia in a murine29. Tomkinson A, Duez C, Cieslewicz G, et al. A murine IL-4 receptor antagonist thatmodel of allergic inflammation is attenuated by small molecule alpha4beta1inhibits IL-4 and IL-13-induced responses prevents antigen-induced airwayantagonists. J Pharmacol Exp Ther 2002 May; 301 (2): 747-52eosinophilia and airway hyperresponsiveness. J Immunol 2001; 166: 5792-800
52. Koo GC, Shah K, Ding GJ, et al. A small molecule very late antigen-4 antagonist30. Wills-Karp M, Luyimbazi J, Xu X, et al. Interleukin-13: central mediator ofcan inhibit ovalbumin-induced lung inflammation. Am J Respir Crit Care Medallergic asthma. Science 1998 Dec 18; 282 (5397): 2258-612003 May 15; 167 (10): 1400-931. Tomkinson A, Duez C, Lahn M, et al. Adoptive transfer of T cells induces airway
53. Miller DH, Khan OA, Sheremata WA, et al. International Natalizumab Multiplehyperresponsiveness independently of airway eosinophilia but in a signalSclerosis Trial Group. A controlled trial of natalizumab for relapsing multipletransduction and activator of transcription 6-dependent manner. J Allergy Clinsclerosis. N Engl J Med 2003 Jan 2; 348 (1): 15-23Immunol 2002 May; 109 (5): 810-6
54. Tomioka M, Ida S, Shindoh Y, et al. Mast cells in bronchoalveolar lumen of32. Mathew A, Medoff BD, Carafone AD, et al. Cutting edge: Th2 cell trafficking intopatients with bronchial asthma. Am Rev Respir Dis 1984 Jun; 129 (6): 1000-5the allergic lung is dependent on chemoattractant receptorsignaling. J Immunol
2002 Jul 15; 169 (2): 651-5 55. Brewster CE, Howarth PH, Djukanovic R, et al. Myofibroblasts and subepithelial33. Moser M. Regulation of Th1/Th2 development by antigen-presenting cells in vivo. fibrosis in bronchial asthma. Am J Respir Cell Mol Biol 1990 Nov; 3 (5):
Immunobiology 2001 Dec; 204 (5): 551-7 507-11
© 2004 Adis Data Information BV. All rights reserved. Biodrugs 2004; 18 (4)

222 Belvisi et al.
56. Tumas DB, Chan B, Werther W, et al. Anti-IgE efficacy in murine asthma models 81. Akers IA, Parsons M, Hill MR, et al. Mast cell tryptase stimulates human lungis dependent on the method of allergen sensitisation. Allergy Clin Immunol fibroblast proliferation via protease-activated receptor-2. Am J Physiol Lung2001; 107: 1025-33 Cell Mol Physiol 2000; 278: L193-201
82. Sylvin H, Dahlback M, Van Der Ploeg I, et al. The tryptase inhibitor APC-36657. Berger WE. Monoclonal anti-IgE antibody: a novel therapy for allergic airwaysreduces the acute airway response to allergen in pigs sensitised to Ascaris suum.disease. Ann Allergy Asthma Immunol 2002; 8: 152-60Clin Exp Allergy 2002; 32: 967-7158. D’Amato G. Therapy of allergic bronchial asthma with omalizumab: an anti-IgE
83. Wright CD, Havill AM, Middleton SC, et al. Inhibition of allergen-inducedmonoclonal antibody. Expert Opin Biol Ther 2003; 3 (2): 371-6pulmonary responses by the selective tryptase inhibitor 1,5-bis-59. Soler M, Matz J, Townley R, et al. The anti-IgE antibody omalizumab reduces[4-[3-cabamimidoyl-benzenesulfonylamino)-methyl]-phenoxy-pentaneexacerbations and steroid requirement in allergic asthmatics. Eur Respir J 2001;(AMG-126737). Biochem Pharmacol 1999; 58: 1989-9618: 254-61
84. Oh SW, Pae CI, Lee DK, et al. Tryptase inhibition blocks airway inflammation in a60. Holgate S, Bousquet J, Wenzel S, et al. Omalizumab improves disease control inmouse asthma model. J Immunol 2002; 168: 1992-2000patients at high risk of serious asthma-related morbidity and mortality [ab-
85. Schmidlin F, Amadesi S, Dabbagh K, et al. Protease-Activated Receptor 2 medi-stract]. Am J Respir Crit Care Med 2002; 165: A187ates eosinophil infiltration and hyperreactivity in allergic inflammation of the61. Bousquet J, Holgate S, Wenzel S, et al. Omalizumab reduces the incidence andairway. J Immunol 2002 Nov 1; 169 (9): 5315-21frequency of exacerbations in patients at high risk of serious asthma-related
86. Krishna MT, Chauhan A, Little L, et al. Inhibition of mast cell tryptase by inhaledmorbidity and mortality [abstract]. Am J Respir Crit Care Med 2002; 165: A187APC 366 attenuates allergen-induced late-phase airway obstruction in asthma. J62. Wenzel S, Bousquet J, Holgate S, et al. Patients with more severe allergic asthmaAllergy Clin Immunol 2001; 107: 1039-45gain greatest relative benefit from omalizumab therapy [abstract]. Am J Respir
87. Fozard JR, Hannon JP. Adenosine receptor ligands: potential as therapeutic agentsCrit Care Med 2002; 165: A215in asthma and COPD. Pulm Pharmacol Ther 1999; 12: 111-463. Liu MC, Hubbard WC, Proud D, et al. Immediate and late inflammatory responses
88. Fozard JR. The case for a role of adenosine in asthma: almost convincing? Currto ragweed antigen challenge of the peripheral airways in allergic asthmatics.Opin Pharmacol 2003; 3: 264-9Cellular, mediator, and permeability changes. Am Rev Respir Dis 1991 Jul; 144
89. Holgate ST. Adenosine: a key effector molecule of asthma or just another media-(1): 51-8tor? Am J Physiol Lung Cell Mol Physiol 2002; 282: L167-864. Knight DA, Stewart GA, Thompson PJ. Histamine tachyphylaxis in human airway
90. Ohta A, Sitkowsky M. Role of G-protein-coupled adenosine receptors in downsmooth muscle: the role of H2-receptors and the bronchial epithelium. Am Revregulation of inflammation and protection from tissue damage. Nature 2001;Respir Dis 1992 Jul; 146 (1): 137-40414: 916-2065. Hele DJ, Birrell MA, Webber SE, et al. Mediator involvement in antigen-induced
91. Fozard JR, McCarthy C. Adenosine receptor ligands as potential therapeutics inbronchospasm and microvascular leakage in the airways of ovalbumin sensi-asthma. Curr Opin Investig Drugs 2002; 3: 69-77tized Brown Norway rats. Br J Pharmacol 2001 Jan; 132 (2): 481-8
92. Sandrasagra A, Leonard SA, Tang L, et al. Discovery and development of respira-66. Shelhamer JH, Marom Z, Kaliner M. Immunologic and neuropharmacologicble antisense therapeutics for asthma. Antisense Nucleic Acid Drug Dev 2002;stimulation of mucous glycoprotein release from human airways in vitro. J Clin12: 177-81Invest 1980 Dec; 66 (6): 1400-8
93. Fozard JR, Ellis KM, Villela Ddantas MF, et al. Effects of CGS 21680, a selective67. Panettieri RA, Yadvish PA, Kelly AM, et al. Histamine stimulates proliferation ofadenosine A2A receptor agonist, on allergic airways inflammation in the rat.airway smooth muscle and induces c-fos expression. Am J Physiol 1990 Dec;Eur J Pharmacol 2002; 438: 183-8259 (6 Pt 1): L365-71
94. GlaxoSmithKline PLC. Product development pipeline February 2001. Company68. Loring SH, Drazen JM, Snapper JR, et al. Vagal and aerosol histamine interactions
brochure. Stewerage, UK: GlaxoSmithKline PLC, 2001 Feb 22on airway responses in dogs. J Appl Physiol 1978 Jul; 45 (1): 40-4
95. Ezeamuzie CI. Involvement of A(3) receptors in the potentiation by adenosine of69. Whicker SD, Armour CL, Black JL. Responsiveness of bronchial smooth muscle
the inhibitory effect of theophylline on human eosinophil degranulation: possi-from asthmatic patients to relaxant and contractile agonists. Pulm Pharmacol
ble novel mechanism of the anti-inflammatory action of theophylline. Biochem1988; 1 (1): 25-31
Pharmacol 2001; 61: 1551-970. Akdis CA, Blaser K. Histamine in the immune regulation of allergic inflammation. 96. Muller CE. Medicinal chemistry of adenosine A3 receptor ligands. Curr Top Med
J Allergy Clin Immunol 2003 Jul; 112 (1): 15-22 Chem 2003; 3 (4): 445-6271. Van Ganse E, Kaufman L, Derde MP, et al. Effects of antihistamines in adult 97. Armour CL, Johnson PR, Alfredson ML, et al. Characterization of contractile
asthma: a meta-analysis of clinical trials. Eur Respir J 1997 Oct; 10 (10): prostanoid receptors on human airway smooth muscle. Eur J Pharmacol 19892216-24 Jun 20; 165 (2-3): 215-22
72. Gelfand EW. Role of histamine in the pathophysiology of asthma: immunomodu- 98. Walters EH, Davies BH. Dual effect of prostaglandin E2 on normal airwayslatory and anti-inflammatory activities of H1-receptor antagonists. Am J Med smooth muscle in vivo. Thorax 1982 Dec; 37 (12): 918-222002 Dec 16; 113 Suppl. 9A: 2S-7S 99. Belvisi MG, Saunders M, Yacoub M, et al. Expression of cyclo-oxygenase-2 in
73. McMillan RM. Leukotrienes in respiratory disease. Paediatr Respir Rev 2001 Sep; human airway smooth muscle is associated with profound reductions in cell2 (3): 238-44 growth. Br J Pharmacol 1998 Nov; 125 (5): 1102-8
74. Holgate ST, Peters-Golden M, Panettieri RA, et al. Roles of cysteinyl leukotrienes 100. Pavord ID, Wong CS, Williams J, et al. Effect of inhaled prostaglandin E2 onin airway inflammation, smooth muscle function and remodeling. J Allergy allergen-induced asthma. Am Rev Respir Dis 1993 Jul; 148 (1): 87-90Clin Immunol 2003; 111: S18-36 101. Costello JF, Dunlop LS, Gardiner PJ. Characteristics of prostaglandin induced
75. Ducharme FM. Anti-leukotrienes as add-on therapy to inhaled glucocorticoids in cough in man. Br J Clin Pharmacol 1985 Oct; 20 (4): 355-9patients with asthma: systematic review of current evidence. BMJ 2002; 324: 102. Coleman RA, Sheldrick RL. Prostanoid-induced contraction of human bronchial1545-52 smooth muscle is mediated by TP-receptors. Br J Pharmacol 1989 Mar; 96 (3):
76. Borish L. The role of leukotrienes in upper and lower airway inflammation and the 688-92implications for treatment. Ann Allergy Asthma Immunol 2002; 88: 16-22 103. Kawikova I, Barnes PJ, Takahashi T, et al. 8-Epi-PGF2 alpha, a novel noncycloox-
77. Creticos P, Knobil K, Edwards LD, et al. Loss of response to treatment with ygenase-derived prostaglandin, constricts airways in vitro. Am J Respir Critleukotriene receptor antagonists but not inhaled corticosteroids in patients over Care Med 1996 Feb; 153 (2): 590-650 years of age. Ann Allergy Asthma Immunol 2002; 88: 401-9 104. Taylor PC. Anti-tumour necrosis factor therapies. Curr Opin Rheumatol 2001; 13:
78. Busse W, Nelson H, Wolfe J, et al. Comparison of inhaled salmeterol and oral 164-9zafirlukast in patients with asthma. J Allergy Clin Immunol 1999; 103: 1075-80 105. Fernandez-Botran R, Crespo FA, Sun X. Soluble cytokine receptors in biological
79. Barnes PJ. Anti-leukotrienes: here to stay? Curr Opin Pharmacol 2003; 3: 257-63 therapy. Expert Opin Biol Ther 2002; 2: 585-60580. Hart PH. Regulation of the inflammatory response in asthma by mast cell products. 106. Weismann MH. What are the risks of biologic therapy in rheumatoid arthritis? an
Immunol Cell Biol 2001; 79: 149-53 update on safety. J Rheumatol Suppl 2002; 65: 33-8
© 2004 Adis Data Information BV. All rights reserved. Biodrugs 2004; 18 (4)

Novel Therapies for Asthma 223
107. Black RA. Tumour necrosis factor-alpha converting enzyme. Int J Biochem Cell 128. Kumar RK, Herbert C, Thomas PS, et al. Inhibition of inflammation and remodel-Biol 2002; 34: 1-5 ing by roflumilast and dexamethasone in murine chronic asthma. J Pharmacol
Exp Ther 2003 Oct; 307 (1): 349-55108. Trifilieff A, Walker C, Keller T, et al. Pharmacological profile of PKF242-484 andPKF241-466, novel dual inhibitors of TNF-alpha converting enzyme and 129. Carter AB, Monick MM, Hunninghake GW. Both erk and p38 kinases arematrix metalloproteinases, in models of airway inflammation. Br J Pharmacol necessary for cytokine gene transcription. Am J Respir Cell Mol Biol 1999; 20:2002; 135: 1655-64 751-8
109. Todd G, Dunlop K, McNaboe J, et al. Growth and adrenal suppression in asthmatic130. Lee JC, Kumar S, Griswold DE, et al. Inhibition of p38 MAP kinase as achildren treated with high-dose fluticasone propionate. Lancet 1996; 348: 27-9
therapeutic strategy. Immunopharmacology 2000; 47: 185-201110. Whol E, Majzoob J. Asthma, steroids and growth. N Engl J Med 2000; 343: 1113-4
131. Newton R, Holden N. Inhibitors of p38 mitogen-activated protein kinase: potential111. Shacke H, Docke W-D, Asadullah K. Mechanisms involved in the side effects of as anti-inflammatory agents in asthma. Biodrugs 2003; 17 (2): 113-29
glucocorticoids. Pharmacol Ther 2002; 96: 23-43132. Birrell M, Hele D, McCluskie K, et al. Effect of p38 kinase inhibitor, SB 203580,112. Belvisi MG, Hele DJ. Soft steroids: a new approach to the treatment of inflammato-
on sephadex induced airway inflammation in the rat. Eur Respir J 2000; 16:ry airways diseases. Pulm Pharmacol Ther 2003; 16 (6): 321-5947-50
113. O’Connor B, Bonnaud G, Haahtela T, et al. Dose-ranging study of mometasone133. Underwood DC, Osborn RR, Kotzer CJ, et al. SB 239063, a potent p38 MAPfuronate dry powder inhaler in the treatment of moderate persistent asthma
kinase inhibitor, reduces inflammatory cytokine production, airways eosinophilusing fluticasone propionate as an active comparator. Ann Allergy AsthmaImmunol 2001 Apr; 86 (4): 397-404 infiltration, and persistence. J Pharmacol Exp Ther 2000; 293: 281-8
114. Schmier J, Leidy NK, Gower R. Reduction in oral corticosteroid use with 134. Irusen E, Matthews JG, Takahashi A, et al. p38 mitogen-activated protein kinase-mometasone furonate powder inhaler improves health-related quality of life in induced glucocorticoid receptor phosphorylation reduces its activity: role inpatients with severe persistent asthma. J Asthma 2003 Jun; 40 (4): 383-93 steroid-insensitive asthma. J Allergy Clin Immunol 2002; 109: 649-57
115. Bodor N, Buchwald P. Soft drug design: general principles and recent applications. 135. Serhan CN, Devchand PR. Novel anti-inflammatory targets for asthma: a role forMed Res Rev 2000; 1: 58-101
PPARγ? Am J Respir Cell Mol Biol 2001; 24: 658-61116. Taylor DA, Jensen MW, Kanabar V, et al. A dose-dependent effect of the novel
136. Wang AC, Dai X, Luu B, et al. Peroxisome proliferator-activated receptor-gammainhaled corticosteroid ciclesonide on airway responsiveness to ade-regulates airway epithelial cell activation. Am J Respir Cell Mol Biol 2001; 24:nosine-5-monophosphate in asthmatic patients. Am J Respir Crit Care Med688-931999; 160: 237-43
137. Benayoun L, Letuve S, Druilhe A, et al. Regulation of peroxisome proliferator-117. Dent G. Ciclesonide (Byk Gulden). Curr Opin Investig Drugs 2002; 3: 78-83activated receptor gamma expression in human asthmatic airways: relationship118. Postma DS, Sevette C, Martinat Y, et al. Treatment of asthma by the inhaledwith proliferation, apoptosis, and airway remodeling. Am J Respir Crit Carecorticosteroid ciclesonide given either in the morning or evening. Eur Respir JMed 2001; 164: 1487-942001; 17: 1083-8
138. Trifillieff A, Bench A, Hanley M, et al. PPAR-α and –γ but not -δ agonists inhibit119. Drollmann A, Langdon C, Engelstatter R, et al. Ciclesonide is effective in theairway inflammation in a murine model of asthma: in vitro evidence for an NF-treatment of bronchial asthma [abstract]. Eur Respir J 2001; 18: P681κB-independent model. Br J Pharmacol 2003 May; 139 (1): 163-71120. Weinbrenner A, Huneke D, Zschiesche M, et al. Circadian rhythm of serum
cortisol after repeated inhalation of the new topical steroid ciclesonide. J Clin 139. Oates JC, Reilly CM, Crosby MB, et al. Peroxisome proliferator-activated receptorEndocrinol Metab 2002; 87: 2160-3 γ agonists: potential use for treating chronic inflammatory diseases. Arthritis
Rheum 2002; 46: 598-605121. Pauwels RA, Derom E, Van de Velde V, et al. Effects of inhaled ciclesonide andfluticasone propionate on cortisol secretion and PC20 for adenosine in asthma
140. Levy BD, Serhan CN. Exploring new approaches to the treatment of asthma:patients [abstract]. Am J Respir Crit Care Med 2002; 165: A768
potential roles for lipoxins and aspirin-triggered mediators. Drugs Today (Barc)122. Reid P. Roflumilast Altana Pharma. Curr Opin Investig Drugs 2002; 3: 1165-70 2003 May; 39 (5): 373-84
123. Giembycz MA. Cilomilast: a second generation phosphodiesterase 4 inhibitor for 141. Bonnans C, Vachier I, Chavis C, et al. Lipoxins are potential endogenous anti-asthma and chronic obstructive pulmonary disease. Expert Opin Investig Drugs inflammatory mediators in asthma. Am J Respir Crit Care Med 2002; 165:2001; 10: 1361-79
1531-5124. Giembycz MA. Development status of second generation PDE4 inhibitors for
142. Levy BD, De Sanctis GT, Devchand PR, et al. Multi-pronged inhibition of airwayasthma and COPD: the story so far. Monaldi Arch Chest Dis 2002; 57: 48-64hyper-responsiveness and inflammation by lipoxin A4. Nat Med 2002; 8:
125. Timmer W, Leclerc V, Birraux G, et al. The new phosphodiesterase 4 inhibitor 1018-23roflumilast is efficacious in exercise-induced asthma and leads to suppressionof LPS-stimulated TNFα ex vivo. J Clin Pharmacol 2002; 42: 297-303
126. Leichtl S, Schmid-Wirlitsch C. Dose-related efficacy of once-daily Roflumilast, a Correspondence and offprints: Prof. Maria G. Belvisi, Respiratory Pharma-new orally active, selective phosphodiesterase 4 inhibitor, in asthma [abstract].
cology Group, Cardiothoracic Surgery, National Heart & Lung Insti-Am J Respir Crit Care Med 2002; 165: A185tute, Faculty of Medicine, Imperial College, Dovehouse Street, London,
127. Kuss H, Hoefgen N, Johanssen S, et al. In vivo efficacy in airway disease models ofSW3 6LY, UK.AWD12-281, a selective PDE4 inhibitor for inhaled administration. J
Pharmacol Exp Ther 2003 Oct; 307 (1): 373-85 E-mail: [email protected]
© 2004 Adis Data Information BV. All rights reserved. Biodrugs 2004; 18 (4)