-
8/11/2019 Neuromediatorii in Ochiul Uscat
1/6
CLINICAL SCIENCES
Alterations of Tear Neuromediatorsin Dry Eye Disease
Alessandro Lambiase, MD, PhD; Alessandra Micera, PhD; Marta
Sacchetti, MD, PhD;Magdalena Cortes, MD; Flavio Mantelli, MD;
Stefano Bonini, MD
Objectives:To evaluate tear levels of neuromediatorsin patients
with dry eye disease and to identify statisti-cal correlations with
the clinical findings.
Methods: Nineteen patientswith dry eyedisease(Sjogrensyndrome,
n=5 patients; nonSjogren syndrome, n=10;and ocular cicatricial
pemphigoid, n=4) and 12 healthyvolunteers were enrolled.The eyes of
all participantswere
evaluatedby slitlamp examination, Schirmer testing, fluo-rescein
staining, and tear film break-up time. Grading ofdry eye severity
was recorded. Tear samples were col-lected, and substance P,
calcitonin generelated peptide(CGRP), neuropeptide Y (NPY),
vasoactive intestinal pep-tide, and nerve growth factor (NGF)
concentrations wereevaluated by enzyme-linked immunoassay and
corre-lated with the clinical findings.
Results: Nerve growth factor tear levels were signifi-cantly
increased in participants with dry eyedisease; CGRPand NPY
concentrations weresignificantly decreased when
compared with those in healthy participants. Dry eye se-verity
showed a direct correlation with NGF and an in-verse correlation
with CGRP and NPY tear levels. Nervegrowth factor tear levels
showed a direct correlation withconjunctival hyperemia and
fluorescein staining results,CGRP directlycorrelated with Schirmer
testvalues, andNPYinversely correlated with tear film break-up
time. Sub-group analysis showed that CGRP and NPY but not NGF
were changed in autoimmune (ie, Sjogren syndrome andocular
cicatricial pemphigoid) dry eye disease.
Conclusions: Thedecreased tear levels of NPYand CGRPin dry eye
disease are related to impaired lacrimal func-tion, and tear levels
of NGF are more closely related tocorneal epithelial damage. Our
findings suggest that NPY,CGRP, and NGF could become useful markers
of dry eyeseverity.
Arch Ophthalmol. 2011;129(8):981-986
THE OCULAR SURFACE IS EX-tensively supplied by sen-sory and
autonomic nervefibers that play a crucial rolein maintaining
healthy epi-
thelia and represent the main sources ofneurogenic
inflammation.1- 3 Cross-communication between the nervous andimmune
systems is shown by the releaseand binding of common
neuromediatorsand cytokines.4-6 Specifically, substance P(SP),
calcitonin generelated peptide(CGRP), vasoactive intestinal
peptide(VIP), and neuropeptide Y (NPY) are re-
leased from ocular surface epithelial cells,lacrimal gland
tissues, and nerve endingsat inflammatory sites, modulating the
in-filtration and activation of the immunecells andtriggering
thereflex of tearing andocular discomfort.7,8
Evidence suggests that neuromedia-tors are involved in chronic
ocular sur-face diseases such as dry eye. Dry eye is acomplex
disease characterized by changesin the ocular surface related to
reduced
quality and/or quantity of tears, inflam-matory reaction, and
impairment of ocu-lar surface sensitivity.9,10 Lacrimal
glandfunction is regulated by the nervous sys-tem, with autonomic
and sensory nervesbeing capable of influencing acinar
glandsecretion and inflammatory reactionsthrough the release of
neuromedia-tors.8,11,12 Substance P and CGRP pro-mote local
inflammationby inducing bloodvessel dilatation, leukocyte
extravasa-tion, immune cell activation, and synthe-sis and release
of several cytokines.8,13-15
Vasoactive intestinal peptide and NPY ex-
ert anti-inflammatory actions by inhibit-ing T-cell
proliferation and helper T-celltype 1 response and modulating the
re-lease of cytokines, chemokines, and ni-tric oxide.16-20 This
neuroimmune cross-communication is capable of modulatinglocal
inflammation by enhancing sensorynerve excitability and triggering
the acti-vation of different immune cell types.
Changes in circulating levels of neuro-peptides and
neurotrophins, as well as the
Author Affiliations:Department of Ophthalmology,Campus
Bio-Medico, Universityof Rome (Drs Lambiase, Micera,Sacchetti,
Cortes, Mantelli, andBonini), and Istituto diRecovero e Cura a
CarattereScientifico G. B. Bietti EyeFoundation (Dr Micera),Rome,
Italy.
ARCH OPHTHALMOL/ VOL 129 (NO. 8), AUG 2011
WWW.ARCHOPHTHALMOL.COM981
2011 American Medical Association. All rights reserved.
wnloaded From: http://archopht.jamanetwork.com/ on
12/04/2013
-
8/11/2019 Neuromediatorii in Ochiul Uscat
2/6
impairment of salivary gland innervation in patients withSjogren
syndrome, have been demonstrated.21-24 Thesechanges
arehypothesizedto be a cause of salivary fluid flowdecrease during
Sjogren syndrome. In fact, a remarkablediscrepancy can be observed
between the inflammatory in-volvementof theglands andthe decrease
in fluid flow. Onepossibleexplanation is that thisautoimmune
diseaseand/orlocal inflammation may cause vasoneural dysregulation
ofand injury to the peripheral nerves, leading to decreasedfluid
flow andatrophy of the acinar cells.25,26 Patients with
autoimmune diseases are known to have a decrease in cir-culating
levels of NPY, and the salivary glands of patientswith Sjogren
syndromehave reducedNPY-containing nerveterminals.25 Of interest,
an increase in nerve growth factor(NGF) tear levels also has been
reported in patients withdry eye disease.27 Nerve growth factor is
a neurotrophinexerting a pleiotropic action on the ocular surface,
modu-lating immune reaction, sensitivity, corneal and conjunc-tival
epithelia proliferation, and differentiation and stimu-lation of
mucin production by goblet cells.28
The aim of this study was to measure the tear con-tent of VIP,
NPY, CGRP, SP, and NGF in patients af-fected by Sjogren syndrome
and nonSjogren syndromedry eye disease compared with that of
healthy volun-
teers. Potential correlations with the clinical character-istics
of the patients also were evaluated.
METHODS
PARTICIPANTS ANDTEAR SAMPLE COLLECTION
The study was performed in accordance with the Declarationof
Helsinki for research involving humans, and the Intramural
Ethics Committee approved the project.Informed consentwaiv-ers
were signed by each participant.
Participants included 12 healthy individuals (8 men and 4women;
mean [SD] age, 41 [21] years) and 19 patients (4 menand 15 women;
68 [13] years) with dry eye disease due toSjogren syndrome (n = 5),
nonSjogren syndrome (n = 10), orocular cicatricial pemphigoid (n=
4), with no history of otherocular diseases.
The diagnosis of dry eye disease was based on clinical his-tory
and the results of slitlamp examination, Schirmer testing,ocular
surface fluorescein staining, and tear film break-up
time.Conjunctivalhyperemia wasgraded as follows: 0, absent; 1,
mild;2, moderate; and 3, severe. Corneal staining was recorded
andgraded according to the Oxford scheme. Dry eye severity grad-ing
from 1 to 4 was recorded according to the Dry Eye Work-Shop
classification.29,30 Evaluation by an immunologist and bio-chemical
investigations were performed to identify systemicautoimmune
diseases.
Tear samples were collected without anesthetic from
allparticipants using dry microsponges (Sharp-tip Micro-sponges;
Alcon Laboratory Inc, Fort Worth, Texas) insertedsimultaneously in
the inferior conjunctival fornix of botheyes, removed after 60
seconds, and then immediately im-
mersed in a 1.5-mL Eppendorf vial containing 50 L of
tissueprotein extractor solution (T-PER; Thermo Scientific
PierceProtein Research Products, Rockford, Illinois) with 10 g/mLof
aprotinin and 1 mM of phenyl methyl sulfonyl fluoride.
Mi-crosponges were then centrifuged to dryness at 13 000 rpmfor 3
minutes to recover tears. The amount of fluid recoveredwas
determined, as previously described.31 Briefly, it was ob-tained by
weighing the sponge and the tube after the absorp-tion and
centrifugation steps. The protein profile of the tearswas then
recorded (A280 program of a NanoDrop ND-1000UV-Vis
Spectrophotometer; NanoDrop Technologies Inc,
Wilmington, Delaware).
Table 1. Characteristics of ParticipantsWith Dry Eye Disease
Characteristic Value
Patients, No. 19
Sex, No.
Male 4Female 15
Age, y
Range 45-82Mean (SD) 68 (13)
Dry eye type, No.
NonSjogren syndrome 10
Sjogren syndrome 5Ocular ci catri cial pemphigoi d 4
Conjunctival hyperemia score
Median (range) 1 (0-2)
Mean (SD) 0.9 (0.7)
Schirmer test, mm/5 min
Median (range) 4 (1-10)
Mean (SD) 4.4 (3.1)Tear film break-up time, s
Median (range) 4.0 (3.0-5.0)
Mean (SD) 3.7 (1.3)
Oxford score
Median (range) 3 (0-5)
Mean (SD) 1.8 (1.6)
9.0
7.0
8.0
6.0
3.0
2.0
1.0
5.0
4.0
0SP
NP
YTearLevel,ng/mL
A HealthyDry eye
HealthyDry eye
CGRP NPY VIP
250.0
150.0
100.0
200.0
50.0
0
TearLevel,pg/mL
B
NGF
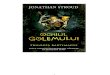
Figure 1.Changes in tear levels in patients with dry eye disease
comparedwith healthy participants. A, Significant decrease in tear
levels of calcitoningenerelated peptide (CGRP) (P=.001) and
neuropeptide Y (NPY) (P=.01),but not of substance P (SP) and
vasoactive intestinal peptide (VIP) inpatients with dry eye. B,
Nerve growth factor (NGF) tear concentrationsignificantly increased
in patients with dry eye (P=.02).
ARCH OPHTHALMOL/ VOL 129 (NO. 8), AUG 2011
WWW.ARCHOPHTHALMOL.COM982
2011 American Medical Association. All rights reserved.
wnloaded From: http://archopht.jamanetwork.com/ on
12/04/2013
-
8/11/2019 Neuromediatorii in Ochiul Uscat
3/6
-
8/11/2019 Neuromediatorii in Ochiul Uscat
4/6
Schirmer test and break-up time values) were not sig-nificantly
different between subgroups (Table 4).
COMMENT
Dry eye is a multifactorial disease characterized by de-creased
tear flow, conjunctival inflammation, impairmentof corneal
sensitivity, decrease in goblet cell density, epi-thelial
metaplasia, and corneal damage, frequently lead-ing to visual
impairment.9 It is well known33 that normaltear flow is regulated
by a fine balance between the para-sympathetic, sympathetic, and
sensory nerves. In fact, theautonomic and sensory nerves locally
release several me-
diators that are able to influence acinar gland secretion aswell
as theinflammatory reaction at thelacrimal glandandthe
conjunctiva.1 The main causes of this neurogenic in-flammation are
considered to be SP and CGRP, both re-leased by the sensory nerves.
In this study, we demon-strated a significantdecreaseinCGRP
inthetears ofpatientsaffected by dry eye; although not significant,
a trend of de-
creasein SPalso was observedin patientswith dryeye. Also,in
those patients,we observed a significant decrease in NPYand a
significant increase in NGF; changes in VIP levelswere not
significant. These results suggest that at leastCGRP,NPY, andNGF
areinvolvedin dryeye disease. How-ever, because the source of these
factors was not estab-lished in this study, it is unclear whether
these alterationsin the tears of patients with dry eye represent a
patho-genic mechanism of the disease or whether they may
re-sultfromchanges inthe ocular surface ofdry eyes. Wehopethat
these aspects will be investigated in studies aimed at
6.0
4.0
3.0
5.0
1.0
2.0
0
TearLevel,ng/mL
A
=
5 mm/5 min
Schirmer Test Values
BUT Values
NPY
CGRP
-
8/11/2019 Neuromediatorii in Ochiul Uscat
5/6
-
8/11/2019 Neuromediatorii in Ochiul Uscat
6/6
Medico, Via Alvaro del Portillo 200, 00128 Rome,
Italy([email protected]).Financial Disclosure:None
reported.
REFERENCES
1. Beuerman RW, Stern ME. Neurogenic inflammation: a first line
of defense forthe ocular surface.Ocul Surf.
2005;3(4)(suppl):S203-S206.
2. Goetzl EJ, Sreedharan SP. Mediators of communication and
adaptation in the
neuroendocrine and immune systems.FASEB J.
1992;6(9):2646-2652.
3. Lambrecht BN. Immunologists getting nervous: neuropeptides,
dendritic cellsand T cell activation.Respir Res.
2001;2(3):133-138.
4. De Swert KO, Joos GF. Extending the understanding of sensory
neuropeptides.Eur J Pharmacol. 2006;533(1-3):171-181.
5. Melik-Parsadaniantz S, Rostne W. Chemokines and
neuromodulation.J Neuroimmunol. 2008;198(1):62-68.
6. EskandariF, Webster JI,Sternberg EM.Neuralimmune pathways
andtheir con-nection to inflammatory diseases.Arthritis Res Ther.
2003;5(6):251-265.
7. Dartt DA, Kessler TL, Chung E-H, Zieske JD. Vasoactive
intestinal peptide-stimulated glycoconjugatesecretion
fromconjunctival goblet cells. ExpEyeRes.
1996;63(1):27-34.8. Kovacs I, Ludany A, Koszegi T, et al.
Substance P released from sensory nerve
endings influencestearsecretion andgoblet cell functionin
therat. Neuropeptides.2005;39(4):395-402.
9. The definition and classification of dry eye disease: report
of the Definition andClassification Subcommittee of
theInternational DryEye WorkShop(2007).OculSurf.
2007;5(2):75-92.
10. Lemp MA.Report ofthe National
EyeInstitute/Industryworkshopon Clinical Trialsin Dry Eyes.CLAO J.
1995;21(4):221-232.
11. Dartt DA. Regulation of lacrimal gland secretion by
neurotransmitters and theEGF family of growth factors. Exp Eye Res.
2001;73(6):741-752.
12. Chung CW, Tigges M, Stone RA. Peptidergic innervation of the
primate meibo-
mian gland.Invest Ophthalmol Vis Sci. 1996;37(1):238-245.13.
Springer J, Geppetti P, Fischer A, Groneberg DA. Calcitonin
gene-related pep-
tide as inflammatory mediator.Pulm Pharmacol Ther.
2003;16(3):121-130.14. OConnor TM,OConnellJ, OBrien DI,Goode
T,Bredin CP,Shanahan F.The role
of substance P in inflammatory disease.J Cell Physiol.
2004;201(2):167-180.
15. Hosoi J, Murphy GF, Egan CL, et al. Regulation of Langerhans
cell function bynerves containing calcitonin gene-related peptide.
Nature. 1993;363(6425):159-163.
16. Pozo D, Gonzalez-Rey E, Chorny A, Anderson P, Varela N,
Delgado M. Tuningimmune tolerance with vasoactive intestinal
peptide: a new therapeutic ap-proach for immune disorders.
Peptides. 2007;28(9):1833-1846.
17. Wheway J, Mackay CR, Newton RA, et al. A fundamental bimodal
role for neu-
ropeptide Y1 receptor in the immune system. J Exp Med.
2005;202(11):1527-1538.
18. GronebergDA, FolkertsG, PeiserC, ChungKF, Fischer
A.NeuropeptideY (NPY).Pulm Pharmacol Ther. 2004;17(4):173-180.
19. BedouiS, MiyakeS, LinY, etal. NeuropeptideY (NPY) suppresses
experimental
autoimmune encephalomyelitis: NPY1receptor-specific inhibition
of autoreac-tive Th1 responses in vivo.J Immunol.
2003;171(7):3451-3458.
20. Kodali S, Ding W, Huang J, Seiffert K, Wagner JA, Granstein
RD. Vasoactive in-
testinal peptide modulates Langerhans cell immune function.J
Immunol. 2004;
173(10):6082-6088.
21. Batbayar B, Nagy G, Kovesi G, Zelles T, Feher E.
Morphological basi s of sensory
neuropathy and neuroimmunomodulation in minor salivary glands of
patients
with Sjogrens syndrome. Arch Oral Biol. 2004;49(7):529-538.
22. Ekstrom J, EkmanR, Hakanson R, Sjogren S, Sundler F.
Calcitoningene-related
peptide in rat salivary glands: neuronal localization,
depletionupon nervestimu-
lation, and effects on salivation in relation to substance
P.Neuroscience. 1988;
26(3):933-949.
23. Lodde BM,Mineshiba F, WangJ, et al. Effect of human
vasoactive intestinal pep-
tide gene transfer in a murine model of Sjogrens syndrome.Ann
Rheum Dis.2006;65(2):195-200.
24. Konttinen YT, Hukkanen M, Kemppinen P, et al.
Peptide-containing nerves in la-
bial salivary glands in Sjogrens syndrome.Arthritis Rheum.
1992;35(7):815-
820.
25. Santavirta N, Konttinen YT, Tornwall J, et al. Neuropeptides
of the autonomic
nervous system in Sjogr ens syndr ome. Ann Rheum Dis.
1997;56(12):737-
740.
26. Feher E, Zelles T, Nagy G. Immunocytochemical localisation
of neuropep-
tide-containing nerve fibres in human labial glands. Arch Oral
Biol. 1999;44
(suppl 1):S33-S37.
27. Lee HK, Lee KS, Kim HC, Lee SH, Kim EK. Nerve growth factor
concentration
and implications in photorefractive keratectomy vs laser in situ
keratomileusis.
Am J Ophthalmol. 2005;139(6):965-971.
28. Lambiase A, Micera A, Pellegrini G, et al. In vitro evidence
of nerve growth fac-
tor effects on human conjunctival epithelial cell
differentiation and mucin gene
expression.Invest Ophthalmol Vis Sci. 2009;50(10):4622-4630.
29. Methodologies to diagnose and monitor dry eye disease:
report of the Diagnos-tic Methodology Subcommittee of the
International Dry Eye WorkShop (2007).
Ocul Surf. 2007;5(2):108-152.
30. Managementand therapy of dryeye disease:report ofthe
Management andTherapy
Subcommittee of the International Dry Eye WorkShop (2007).Ocul
Surf. 2007;
5(2):163-178.
31. Mantelli F, Tiberi E, Micera A, Lambiase A, Visintini F,
Bonini S. MUC5AC over-
expression in tear film of neonates. Graefes Arch Clin Exp
Ophthalmol. 2007;
245(9):1377-1381.
32. Lambiase A, Manni L, Bonini S, Rama P, Micera A, Aloe L.
Nerve growth factor
promotescornealhealing:structural,biochemical,and molecular
analyses of rat
and human corneas.Invest Ophthalmol Vis Sci.
2000;41(5):1063-1069.
33. Stern ME, Gao J, Siemasko KF, Beuerman RW, Pflugfelder SC.
The role of the
lacrimal functional unit in the pathophysiology of dry eye. Exp
Eye Res. 2004;
78(3):409-416.
34. Bentez-del-Castillo JM, Acosta MC, Wassfi MA, et al.
Relation between corneal
innervationwith confocalmicroscopyand
cornealsensitivitywithnoncontactes-thesiometry in patients with dry
eye. Invest Ophthalmol Vis Sci. 2007;48(1):
173-181.
35. MantelliF, Argueso P. Functionsof ocular surface mucins in
health and disease.
Curr Opin Allergy Clin Immunol. 2008;8(5):477-483.
36. Nguyen DH,Beuerman RW,Thompson HW,DiLoreto
DA.Growthfactorand neu-
rotrophic factor mRNA in human lacrimal gland. Cornea.
1997;16(2):192-199.
ARCH OPHTHALMOL/ VOL 129 (NO. 8), AUG 2011
WWW.ARCHOPHTHALMOL.COM986
2011 American Medical Association. All rights reserved.