Embed Size (px)
Citation preview

P5911Keratitis, congenital ichthyosis, and neurosensory deafness syndromewith tinea capitis and severe kerion formation
Brooke Walls, DO, Nova Southeastern University, Largo, FL, United States
Keratitis, congenital ichthyosis, and neurosensory deafness (KID) syndrome is arare autosomal dominant disorder with a mutation in GJB2, which encodes forconnexin 26, a gap junction protein responsible for intercellular communicationsin the epidermis and cochlea. We report a case of KID syndrome in a 6-year-oldAfrican American girl. She presented to our clinic with erythematous, keratoticplaques on the cheeks and a stippled palmoplantar keratoderma. Examination ofher scalp revealed large, fungating, malodorous, yellowish-brown hyperkeratoticnodules that were tender and cervical lymphadenopathy. Both the mother andyounger brother of our patient presented with similar classic cutaneous findingsof KID syndrome, without evidence of severe fungal infection. Recurrentbacterial and fungal infections are a known complication due to the underlyingcutaneous abnormality. There have been several reports of squamous cellcarcinomas in patients with KID, therefore a low threshold for repeated use ofantifungals and biopsy of unusual looking keratotic papules is warranted. Ourpatient was admitted to the hospital for surgical debridment and IV treatment.
APRIL 20
cial support: None identified.
CommerP6072Loss of genomic DNA copy numbers in the p18, p16, p27, and RB loci inblastic plasmacytoid dendritic cell neoplasm
Reiko Morita, PhD, Department of Dermatology, Kinki University Faculty ofMedicine, Osakasayama city, Japan; Akira Kawada, PhD, Department ofDermatology, Kinki University Faculty of Medicine, Osakasayama, Japan; AyakaHirao, PhD, Department of Dermatology, Kinki University Faculty of Medicine,Osakasayama, Japan; Naoki Oiso, PhD, Department of Dermatology, KinkiUniversity Faculty of Medicine, Osakasayama, Japan; Tomohiko Narita, PhD,Department of Dermatology, Kinki University Faculty of Medicine, Osakasayama,Japan
Blastic plasmacytoid dendritic cell neoplasm (BPDCN) is a rare plasmacytoiddendritic cell precursor-derived aggressive neoplasm with poor prognosis.Recently, some studies have indicated that patients with BPDCN have an unusualtumor cell karyotype with an average of 6 to 8 abnormalities. We here report a 74-year-old man with BPDCN. The patient’s genomic DNA copy numbers wereanalyzed using array-comparative genomic hybridization (CGH) to identify thechromosomal and genetic features of the malignant cells. The array-CGH analysisrevealed the loss of the chromosomes1p31.3-33, 9p/q, 12p13.1-13.2 and 13p/q, andthe gain of chromosome 16p/q. These lost regions included the loci of the tumorsuppressor genes of CDKN2C/p18, CDKN2A/p16, CDKN1B/p27 and RB1, whichare known as cell-cycle inhibitors. We identified a novel loss of a chromosome1p31.3-33 region including CDKN2C/p18, which may be involved in the pathogen-esis of BPDCN.
cial support: None identified.
Commer13
P7103Multiple facial angiofibromas revealing Birt-Hogg-Dub�e syndrome
Fr�ed�eric Caux, MD, PhD, Reference Center for Genetic Skin Diseases, Bobigny,France; Alexis Guyot, MD, Reference Center for Genetic Skin Diseases, Bobigny,France; Annie L�evy, MD, Department of Pathology, Bobigny, France; Jean-BenoitMonfort, MD, Reference Center for Genetic Skin Diseases, Bobigny, France;Liliane Laroche, MD, Reference Center for Genetic Skin Diseases, Bobigny,France; Nadem Soufir, MD, Laboratory of Genetics, Paris, France
Angiofibromas are benign cutaneous tumors. Multiple angiofibromas are ahallmark of tuberous sclerosis (Bourneville disease). We reported a patient withnumerous facial angiofibromas leading to the diagnosis of Birt-Hogg-Dub�esyndrome (BHD). A 37-year-old man was referred with facial skin lesions of 6years’ duration. His medical history included psoriasis, epilepsy since the age of27 years and depression treated with valproic acid and escitalopram. Familyhistory indicated that the patient’s father had lung cancer and facial lesions.Clinical examination revealed numerous whitish papules on the nose and thecheeks but no shagreen patch nor hypopigmented macules. Histologic analysis offour facial papules showed three angiofibromas and one fibrous papule. BrainMRI and cardiac and abdominal ultrasound examinations were normal except fora 19-mm renal cyst. Tuberous sclerosis was suspected; genetic analysis of TSC1and TSC2 genes was performed but no abnormality was found. Association of arenal cyst and multiple facial angiofibromas in this patient led to analyse theFLCN gene and a complete deletion of exon 4 was demonstrated. A diagnosis ofBirt-Hogg-Dub�e syndrome was finally reached. Additional work-up showed three5-, 8-, and 9-mm lung cysts on CT scan. Numerous facial angiofibromas arecharacteristic of tuberous sclerosis. They also have been described in multipleendocrine neoplasia type 1. Only one case of multiple angiofibromas associatedwith BHD has been reported in the literature. Indeed, cutaneous lesionsencountered in BHD are usually whitish or flesh-colored facial papules withhistology showing fibrofolliculomas. Other skin lesions of this rare autosomaldominant disease are trichodiscomas and acrochordons. The extra-cutaneousmanifestations of BHD include spontaneous pneumothorax and lung cysts andbenign or malignant kidney tumors such as oncocytomas and chromophobe renalcell carcinomas. Our patient had molecularly confirmed BHD with typicalpulmonary and renal manifestations but the fact this disease was revealed byangiofibromas is exceptional. In summary we reported a case demonstrating thata FLCN gene mutation may be associated with multiple angiofibromas.Consequently, the dermatologist confronted to a patient with numerous angio-fibromas must evoke BHD as well as tuberous sclerosis.
cial support: None identified.
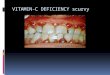
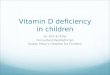
CommerP6186Netherton syndrome in association with vitamin D deficiency
Ashley Delacerda, MD, Scott and White Dermatology, Temple, TX, United States;Karina Parr, MD, Scott and White Dermatology, Temple, TX, United States;Lenore Chiles, MD, Scott and White Dermatalogy, Temple, TX, United States;Matthew Stephen, MD, Scott and White Pediatric Endocrinology Clinic, Temple,TX, United States
Netherton syndrome is an autosomal recessive disorder that usually presents witha triad of ichthyosis linearis circumflexa, atopy, and trichorrhexis invaginata.Several other clinical features including delayed growth and bone developmentand short stature can develop during its clinical course. The disorder is caused bya mutation in the SPINK5 gene important in skin barrier formation and immunity.We report a case of a 10-year-old girl with classic symptoms of congenitalNetherton syndrome who developed severe growth retardation and severevitamin D deficiency. Our patient did not respond well to growth hormonereplacement trial by pediatric endocrinology, perhaps due to concomitantvitamin D deficiency. Since patients with Netherton syndrome have severalfactors predisposing them to the development of vitamin D deficiency withsuggest screening these patients with serum vitamin D levels. We compare thecurrent treatment options, which are targeted at minimizing the classic manifes-tations of Netherton syndrome, and consider how Vitamin D supplementationcan play a role in the treatment regimen.
cial support: None identified.
CommerJ AM ACAD DERMATOL AB99