Embed Size (px)
Citation preview

Am. J. Hum. Genet. 51:1089-1102, 1992
X-linked Nephrogenic Diabetes Insipidus:From the Ship Hopewell to RFLP StudiesDaniel G. Bichet,* Geoffrey N. Hendy,t Michele Lonergan,* Marie-Fransoise Arthus,*Sophie Ligier, * Zdenka Pausova, t Rudiger Kluge, * Hans Zingg, t Paul Saenger, * *Ellen Oppenheimer, * * David J. Hirsch, t t Simone Gilgenkrantz, t$ Jean-Pierre Salles,§§Isabelle Oberle,##"' Jean-Louis Mandel,## Martin C. Gregory,liii T. Mary Fujiwara,Kenneth Morgan,§ and Charles R. Scriverill#
Unite de Recherche Clinique, Centre de Recherche et Service de Nephrologie, D6partement de Medecine, H6pital du Sacr6-Coeur, Universit6de Montreal; tCalcium Research Laboratory and tLaboratory of Molecular Endocrinology, Royal Victoria Hospital and McGill University;§Department of Epidemiology and Biostatistics and Department of Medicine, IlDepartment of Pediatrics, and #Department of Biology, McGillUniversity, Montreal; * * Department of Pediatrics, Albert Einstein College of Medicine, New York; ttDepartment of Medicine, DalhousieUniversity, Halifax; ttService de Genetique, Universit6 de Nancy, Nancy; §§Service de Medecine Infantile, Centre Hospitalier Purpan, Toulouse;1I1IDivision of Nephrology, Department of Medicine, The University of Utah, Salt Lake City; and ##Unite de Biologie Moleculaire et de GenieG&n6tique, Strasbourg
Summary
Nephrogenic diabetes insipidus (NDI; designated 304800 in Mendelian Inheritance in Man) is an X-linkeddisorder with abnormal renal and extrarenal V2 vasopressin receptor responses. The mutant gene has beenmapped to Xq28 by analysis of RFLPs, and tight linkage between DXS52 and NDI has been reported. In1969, Bode and Crawford proposed, under the term "the Hopewell hypothesis," that most cases in NorthAmerica could be traced to descendants of Ulster Scots who arrived in Nova Scotia in 1761 on the shipHopewell. They also suggested a link between this family and a large Mormon pedigree. DNA samplesobtained from 13 independent affected families, including 42 members of the Hopewell and Mormon pedi-grees, were analyzed with probes in the Xq28 region. Genealogical reconstructions were performed. Linkagebetween NDI and DXS304 (probe U6:2.spl), DXS305 (St35-691), DXS52 (St14-1), DXS15 (DX13), andF8C (F814) showed no recombination in 12 families, with a maximum lod score of 13.5 for DXS52. Arecombinant between NDI and DXS304, DXS305, was identified in one family. The haplotype segregatingwith the disease in the Hopewell pedigree was not shared by other North American families. PCR analysisof the St14 VNTR allowed the distinction of two alleles that were not distinguishable by Southern analysis.Carrier status was predicted in 24 of 26 at-risk females. The Hopewell hypothesis cannot explain the originof NDI in many of the North American families, since they have no apparent relationship with the Hopewellearly settlers, either by haplotype or by genealogical analysis. We confirm the locus homogeneity of thedisease by linkage analysis in ethnically diverse families. PCR analysis of the DXS52 VNTR in NDI familiesis very useful for carrier testing and presymptomatic diagnosis, which can prevent the first manifestationsof dehydration.
Introduction1990]) is an X-linked disorder in which the affected
Nephrogenic diabetes insipidus (NDI; designated patients do not concentrate their urine after the admin-304800 in Mendelian Inheritance in Man [McKusick istration of the antidiuretic hormone arginine-vaso-
Received April 2, 1992; revision received July 6, 1992. pressin (AVP) (Reeves and Andreoli 1989). In thisAddress for correspondence and reprints: Daniel G. Bichet, disease, the vasopressin signal is not recognized- or
M.D., Research Centre, Hopital du Sacre-Coeur de Montreal, its transmission is altered- by the principal cells of the5400, boulevard Gouin ouest, Montreal, Quebec, Canada H4J renal collecting ducts. The defect is not confined to thelCS. kidneys, since affected male patients have no vasode-
1. Deceased, November 17, 1991.C 1992 by The American Society of Human Genetics. All rights reserved. pressor or factor VIII stimulation response to the ad-0002-9297/92/5105-0019$02.00 ministration of the antidiuretic vasopressin agonist
1089
Bichet et al.
1-desamino[8-D-arginine]vasopressin (dDAVP) (Ko-brinsky et al. 1985; Bichet et al. 1988, 1989, 1991).By linkage analysis, the NDI gene has been assigned
to the Xq28 region (Kambouris et al. 1988; Knoers etal. 1988a, 1988b, 1989). Genetic linkage studies havebeen carried out in one North American family and inseveral European families. The odds of linkage be-tween Xq28 marker DXSS2 and the NDI locus aregreater than 1013:1 (Kambouris 1988; Knoers et al.1988b).The availability of Xq28 markers provided us with
the opportunity to test a hypothesis put forward byBode and Crawford (1969). They proposed that NDIpatients in eastern North America shared a commonancestor who was an Ulster Scot and who had arrivedin Halifax in 1761 on the ship Hopewell. A link be-tween this family and a large Mormon pedigree (Can-non 1955) was also suggested.Our first objective was to test the assumption that
the chromosomal location ofthe altered gene responsi-ble for the disorder was identical in all affected fami-lies-i.e., locus homogeneity. A total of 13 familieswere studied: representatives ofthe Hopewell pedigree(Bode and Crawford 1969), the Mormon pedigree(Cannon 1955), and 11 unrelated families from di-verse ethnic backgrounds (5 French-Canadian, 1 Afri-can-American, 1 Puerto Rican, 1 Iranian, 2 French,and 1 English). The phenotypic characteristics ofaffected persons were similar in all families. Our sec-ond objective was to test the Hopewell hypothesis byusing DNA probes: if recombination in the Xq28 re-gion is rare and if the mutant NDI alleles in the Hope-well pedigree and other North American families areidentical by descent from an Ulster Scot ancestor, thenthe haplotypes of the Xq28 loci segregating with thedisease should be identical in these families. Our thirdobjective was to determine whether the heterozygotesin our pedigrees could be identified by DNA analysis,since carrier detection by other means has been diffi-cult up to now (Bode and Crawford 1969; Bichet etal. 1988, 1989).
Subjects and Methods
Study SubjectsThirteen families with well-documented X-linked
NDI who were distributed in distinctive geographical,historical, and ethnic groups were studied. All affectedmale patients had a documented lifelong history ofpolyuria and polydipsia, normal or elevated plasma
concentrations of arginine-vasopressin, and uncon-centrated urine despite administration of arginine-vasopressin or dDAVP. Phenotypic characteristicswere similar within and between families (Bichet etal. 1988, 1989, 1991). Mental retardation correlatedpositively with delay in diagnosis and with the severityof clinical course. The phenotypic characteristics of14 male patients and 12 obligate carriers have beendescribed elsewhere (Bichet et al. 1988, 1989, 1991).We studied 38 affected males, 18 nonaffected malerelatives, 30 obligate carriers, and 26 females at riskfor heterozygosity.The families studied are shown in figures 1-4. The
Hopewell pedigree (fig. 1) was reconstructed to adepth of six generations, from detailed bibliographicalrecords (Eaton 1912; Miller 1972), from informationgiven by family members, and from the Nova ScotianArchives (Halifax). DNA was obtained from three re-lated families (A-C) of the Hopewell pedigree (fig. 1).Families A, B. and C were depicted, respectively, inthe central, paracentral right, and right parts of thegenealogy originally presented by Bode and Crawford(1969). Historical records were reviewed, and bloodsamples obtained from the Mormon family (Cannon1955) (fig. 2). The five French-Canadian families(Quebec [Ql-Qs]; fig. 3) had been established in Que-bec since the 18th century; their genealogies were re-constructed from Quebec archives. The other families(other [01-06]; fig. 4) reside in Quebec, Ontario, NewYork, and France. Family 01 is Iranian in origin, 02is Puerto Rican, 03 and Os are French, 04 is British,and 06 is African-American.
DNA, PCR, and Linkage Analyses
DNA was extracted and purified from blood sam-ples by a conventional phenol-chloroform technique(Sambrook et al. 1989) and was cut with differentrestriction enzymes (New England Biolabs, Beverly,MA) in the presence of 2 mM spermidine. After elec-trophoresis (0.9% agarose, TAE buffer) (Sigma, St.Louis) Southern blots were performed (0.45 gm; Ny-tran, Schleicher and Schuell, Keene, NH) with 10 xsodium chloride-sodium citrate (pH 7.0).The DNA probes were labeled with [a-32P]dCTP
(ICN Radiochemicals, Irvine, CA) by using the ran-dom primer method (Multiprime DNA labeling sys-tems; Amersham, Oakville, Ontario). The filters wereautoradiographed (X-Omat AR5, Kodak) at - 80°Cwith 2 intensifying screens (Lightning Plus; DuPont)for 4-7 d.The DNA probes (Harper et al. 1984; Oberle et al.
1090

Insert A
Insert BVII 0,
IX 2 52
53 5 5 54 52 l 1 12 1
22 2 2 21 2
23 45 6 718 9see PCR analysis fig 7
ixViIIViIVI V IV 1II IV v VIVIIVIIIIx PROBES LOCI
St35- 691Stl4- 1DX13F814
Insert C
11 11
45 55 _22 1211 21 -
5
2
11 155 512 121 2
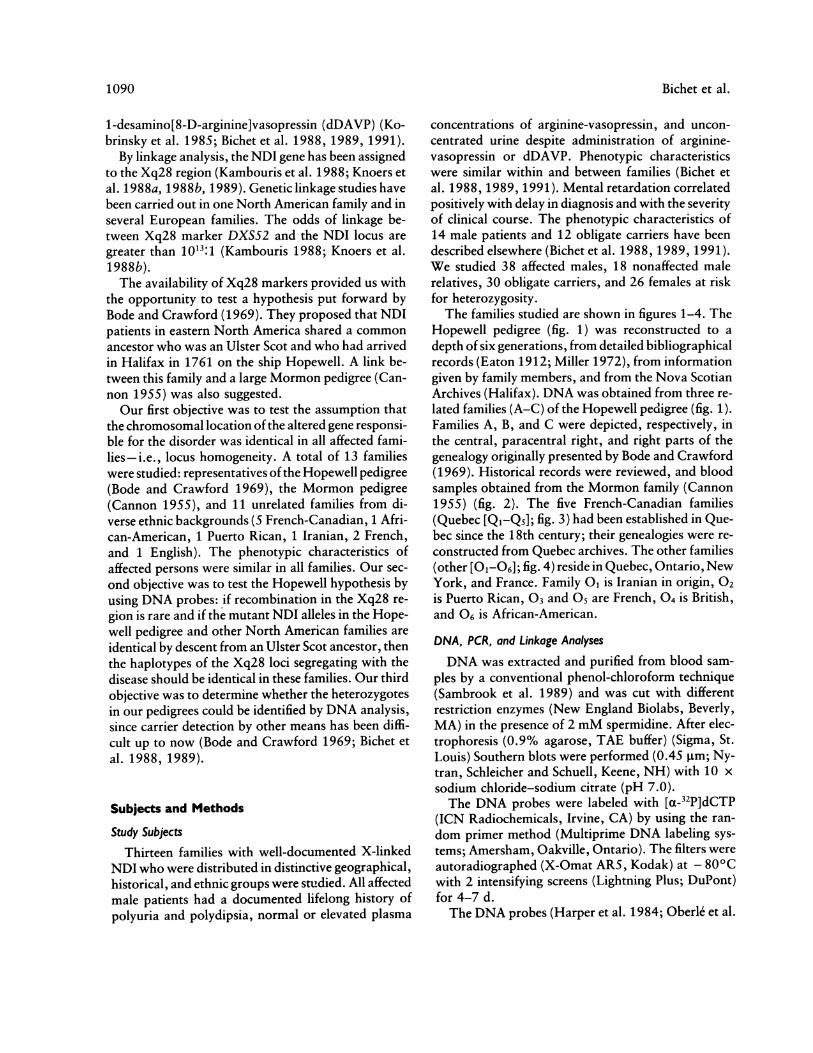
Figure I Pedigree of the Hopewell family, segregating for X-linked NDI and Xq28 RFLP markers. Generations are numberedaccording to the protocol of Bode and Crawford (1969). The couple at the origin of the inserts is 111-9 and III-10 (also see fig. 5). Probesand loci are listed from centromere to telomere. In females in whom the inheritance of paternal and maternal alleles can be ascertained,the paternal X chromosome is shown on the right. In this family, the disease is segregating with the 1-5-1-2 haplotype. Allele 5, markedwith an asterisk (*) was subsequently identified as allele 6, by PCR. C = Unaffected male; * = affected male; ( = obligate carrier female;and = predicted carrier female. Double lines denote consanguineous marriage.
VA'S305/2XS52/2XS15FIIC

Bichet et al.
1 21 24 32 12 1
1 23 31 1
l-1 1 l i 2 2 --or--1 11 1 1 1 2 2 1 12 2142 42 4 3 3 3 3 3 34 342 1 2 1 2 1 1 1 1 1 12 1221 21 2 1 1 1 1 1 11 11
PROBES LOC/
U6:2.splSt35-691Stl4- 1DX13F814
121S304JA'S3605DXS52VlSi 5F8C
Figure 2 Historical reconstitution of Cannon's Mormon pedigree. The disease allele could not originate from Fullmer (born in 1803).The disease is segregating with the 2-3-1-1 haplotype, and a recombination was observed in the male twins, between the DXS30S and theNDI loci.0) = Carrier status unknown. All other symbols are as in fig. 1.
1985; Mandel et al. 1986; Heilig et al. 1988; Vincentet al. 1989; Rousseau et al. 1990) used here are de-scribed in table 1 and are located, from centromere totelomere, according to the results of Rousseau et al.1990. Alleles were numbered according to the proto-col of the 10th International Workshop on HumanGene Mapping (Kidd et al. 1989) and, for U6:2.spl,according to the protocol of Rousseau et al. (1990).A PCR analysis of the Stl4 (DXSS2) VNTR was
done by a modification of the technique described byRichards et al. (1991). We used a thermocycler andreagents from Perkin Elmer Cetus (Montreal). Taqpolymerase (2.5 U/sample; BRL, Gaithersburg, MD)
was added to a protease-inactivated mixture (DNA,nucleotide, buffer, and primers). We programmed 25cycles (1 min at 94°C and 4 min at 60°C). Amplifiedproducts were examined on agarose gel electrophore-sis: they include VNTRs of 60 bp each and a 650-bpflanking sequence (Richards et al. 1991). PCR analysiswas found to be the method of choice for analyzingthe Stl4 VNTR, because this method enabled thedifferentiation of alleles previously not distinguishableby Southern analysis (table 1). Alleles 5 (1,630 bp)and 6 (1,570 bp) are difficult to distinguish on theSouthern blots and are arbitrarily noted on figures1-4 as allele 5, except for family O3 (allele 6 verified).
1092

2 2 1 224 4 5 4 22 2 2 221 12 11
1 23 21 11 1
91 9 2 2 1 2 1 1
Fi1512LiI 1 11
Q) 2 25 d±124 2 2 5 2 5 3 3 3 3d 85 12 n r~ ~~~1 2 11 12 1 1 1 12 _ ( 1
2 2 11 1124 5 3 581 2 2 1 2 1
0~~~~~~~~~~~~~~~~~~~~~~~12I I 1
2 2 1 2 1 2 1 2 28 8 5' 8 5,
Q3 i22 1 2 L 2 2 12 1 2 1 1 1 1 228 4 8 5*4 5*4 4 81 2 1 1 2 1 2 1 12 1 2 1 1 1 1 22
Q4
I~~ 2 12 *
1 1 12 1 1
2 5 2 2 5 4 5
Q4 ,~~~~~~2 2 2 2 2 PROBES Goc/
S -35 691 1XS305St14 - 1 12AS52DX I'3 PIJSISF814 F8C
Figure 3 Five Quebec families with X-linked NDI. In family Q4, crosses indicate that the two affected males died early in infancy.All other symbols are as in fig. 1.
I

Bichet et al.
01
73 lIl 5
1 2 _1
1 2
3 72 1
2 1
02
38 52 1
1 1 1 13 8 3 32 1 2 21 1 1 1
68 6
2 1 ov-"|--EEl-o C8 6 8 6 8 66 86 4
2-l 2-,/l\ 2- 1l1 2:lO O21 1
6 6 8 8
1 2 2
23l l
2 2
2 2
05
7 5* L l
1 2 * -2 25* 5*
2 2
06
PROBES LOCI
St35-Stl4-DX13F814
691 12AS30512XS5212XS15
TI/C
Figure 4 Other families. In family 03, chorionic villus sampling established that the unborn child indicated by a triangle (A) was
not at risk of inheriting the disease. This prediction was confirmed by the birth of a normal infant. In 06, allele 5, marked with an asterisk
(*), was identified as allele 6, by PCR. All other symbols are as in figs. 1 and 2.
PCR analysis was used, a posteriori, to reclassify al-leles 5 and 6 (denoted by "5k," in the figures).
Linkage analysis was carried out by the likelihoodmethod (Ott 1991) using the LINKAGE programs(Lathrop et al. 1984, 1985). Dr. Mark Lathrop pro-
vided the LINKAGE programs (version 5.1a). Pub-
lished allele frequencies for the RFLPs were used (seetable 1). Linkage equilibrium was assumed. The mu-
tant allele frequency for X-linked NDI was set at .03for the Hopewell pedigree and at 7.4 x 10-6 for theother families (see below), and a mutation rate of 10-6was assumed.
04242
4 42 21 1
242l
2 24 42 21 1
03
1094

1095X-linked Nephrogenic Diabetes Insipidus
Table I
RFLPs Used in the Linkage Study
SOUTHERN ANALYSIS PCR ANALYSISa
Size Frequency Size FrequencyLocus PROBE ENZYME ALLELE (kb) (%) References (bp) (%)
DXS304 ... U6:2.spl BanI 1 4.1 76 152 2.1 24
DXS30S ... St35-691 TaqI 1 4.4 65 162 4.0 35
DXS52 .... Stl4-1 TaqI 1 6.6 <1 17, 18 >3,000 22 5.4-5.2 4 2,900 83 4.8 12 2,400 124 4.5 36 1,690 365 4.1 20 1,630 26(5*) 4.0 1,570 147 3.9-3.6 10 1,390 10
1,300 21,220 2
8 3.4 15 700 129 1.9 <1
10 1.4 <1DXS1S .... DX13 BglII B 2.8 62 19
A 5.8 38F8C..F814 BclI B .9 71 20
A 1.2 29
a Richards et al. (1991).
Results
Prevalence and Gene FrequencyThe prevalence of X-linked NDI is much higher in
the Nova Scotian descendants of Ulster Scots thanelsewhere. The survival ofNDI infants in the past wasconsiderably less than 50%, while today it may be80% or greater. Furthermore, the knowledge gainedby the family in providing for the needs of earlier-bornsons affected with the disease contributes to improvedsurvival of later-born affected infants. We estimatedthe prevalence of NDI in males in Quebec to be 3.7/1,000,000 males, on the basis of our knowledge of 12patients who were 10-40 years of age. If an averagesurvival of50% is assumed for NDI infants in Quebec,then the estimated NDI allele frequency would be 7.4x 1 6. By contrast, we know of 30 Nova Scotia malepatients 10-70 years of age whose families reside pre-dominantly in two villages with a total population sizeof about 2,500. We estimate the allele frequency tobe .03, assuming 80% survival of Nova Scotian NDIinfants. Thus, in certain well-defined communities of
Nova Scotia the expected carrier frequency is about6%.
Locus HomogeneityIn all the families tested, NDI cosegregated with the
Xq28 marker alleles, confirming locus homogeneityof NDI in these families (figs. 1-4). The RFLP/PCRalleles are described in table 2. Pairwise lod scores oflinkage of NDI to each of the Xq28 loci are shown intable 3. A recombinant was observed in the Mormonpedigree (fig. 2), between the pair of loci DXS304,DXS30S and the other loci. No recombination wasobserved between NDI and the loci DXSS2, DXS1S,and F8C. For 12 informative pedigrees, a maximumlod score of 13.5 for linkage of NDI and DXSS2 wasobtained at zero recombination; the 1-lod-unit sup-port interval (Conneally et al. 1985) for the estimateof the recombination fraction was 0-.05. For linkage,a combined lod score of 26.6 at zero recombinationwas obtained when our data were added to those re-ported elsewhere (Kambouris et al. 1988; Knoers etal. 1988b).

Bichet et al.
Table 2
Haplotypes Associated with MDI Phenotypes in 13 Families
HAPLOTYPE, BY SOUTHERN ANALYSIS ALLELE SIZE,DXS305 DXSS2 DXS1S F8C WITH DXSS2 (5t14)a(St35-691) (St14-1) (DX13) (F814) (bp)
Hopewell ... 1 5 1 2 1,630Cannon 2 3 1 1 2,400Ql ............ 2 4 2 1 1,690Q2 ............ 1 3 1 1 2,400Q3 ............ 2 8 1 2 700Q4 ............ . 1 2 2 1 2,900QS ............ . 1 4 1 2 1,6900, ............ 1 3 2 2 2,400
02 ............ 1 3 2 1 2,40003 ....... ... 8 ... 2 ...
04 2 4 2 1 1,69005 2 2 ... 1 2,90006 2 6 ... 2 1,570
a St14 VNTR analyzed by PCR.
Haplotype Segregating with the Disease in the HopewellPedigree: Correlations with Historical andGenealogical Information
All the 11 affected male patients from the Hope-well pedigree shared the 1-5-1-2 haplotype (DX305-DXS52-DXS1 5-F8C), and no recombination was ob-served. The couple (III-9 and 111-10) at the origin ofinserts A-C (fig. 1) is indicated by a horizontal arrowin the third generation of the Hopewell pedigree (fig.5). With historical documents, we were able to recon-struct the first three generations and the relationshipsbetween the "Barnhills" (I-1 and 1-2) and the "Wil-sons" (II-1 and 11-2) (fig. 6). The Wilsons were mer-chants already established in Nova Scotia when the
Table 3
Maximum-Likelihood Estimates of theRecombination Fraction (0) and Lod Scores(Z(O)) and I-Lod-Unit Support Interval betweenNDI and Xq28 Loci
Locus (no. of families 1-Lod-Unit Supportinformative for linkage) Z(0) 6 Interval for 0
DXS305 (7) ................. 4.0 .04 .001-.18DXSS2' (12) ................. 13.5 00-.05DXS1S (8) ................. 7.8 0 0-.07F8C (9) ................. 8.2 0 0-.07
a St14 VNTR analyzed by PCR.
Hopewell landed in Halifax in 1761; II-3 and her hus-band immigrated later, in 1767 (Miller 1972). CoupleII-7 and 11-8 was on the Hopewell with the Barnhills(I-1 and 1-2) and lost three children (III-12-111-14) onthe ship, which suggested to Bode and Crawford thatthese children had had NDI. However, this branch ofthe Hopewell pedigree is not the origin of the NDImutation of the patients tested by Bode and Crawford(1969) or of the patients tested later by us (figs. 1, 5,and 6). The likely paths of descent of the NDI mutantallele to families A-C require some discussion (fig. 6).If we consider that, in the past, affected males died ininfancy, with a mortality rate greater than 50%, thenit is more likely that transmission occurred throughcarrier women, i.e., through female descendants inthe past. Thus, if we assume, because of the sharedhaplotype associated with NDI, that the NDI mutantallele was introduced only once into the Hopewell ped-igree, then individual III-9 is the most likely recentcommon ancestor, IV-27 was a carrier, and individualIV-20 would have been affected but survived to havechildren. However, there is no reliable evidence thatIII-10, IV-20, or IV-26 were affected. But, if IV-21and IV-27 were the nearest ancestral carriers of NDIin families A-C, then the original carrier, who is theircommon ancestor, has not been identified. Therefore,we propose that the NDI mutant allele was widelydispersed among the descendants of the Ulster Scotsin eastern North America and that all affected individ-
1096

cv
cv~~~~~~~~~~~~~~~c
C~i0
_-§ -
cli~~~~~c
0~~~~~~~~~~~~~~~~~~~.
*0~~~~~~~~~~~~~~
C~~~~~~~~~~~~~~~~~~6a
V I
coz~~~~~~~~~~I

Bichet et al.
Barnhill
III-20 111-17.19
Insert B Insert A Insert C
Figure 6 Historical reconstruction of generations I-III of the Hopewell pedigree, including extensions to the genealogy presentedby Bode and Crawford (1969); see fig. S. The Wilson lineage is represented by dashed lines. Generations and individuals are numberedaccording to the protocol of Bode and Crawford (1969) and bear the same numbers as in figs. 1, 5, and 6. The couple III-9 and III-10is also represented in figs. 1 and 5. m 1849 = marriage in 1849. All other symbols are as in fig. 5.
uals with haplotype 1-5-1-2 are likely identical by de-scent for the same mutation.
Haplotypes Segregating in the Other Families
In Cannon's Mormon pedigree, male patients hadhaplotype 1-3-1-1 or 2-3-1-1, which was differentfrom the haplotype in the Hopewell pedigree. 1-3-1-1is likely a recombinant haplotype which occurs in themonozygous twins. Genealogical details obtainedfrom the Mormon pedigree linked the "Fulmer"founder cited by Bode and Crawford (1969) to Ger-man immigrants and not to Ulster Scots (fig. 2).Fulmer (or Fulmore), born in 1837, was probablyaffected and probably inherited the disease from hismother (fig. 2), who was not known to be related to
Nova Scotian settlers.
All the other families studied (figs. 3 and 4 and table2) had different haplotypes, except for families Qi and04, who shared haplotype 2-4-2-1. There was noknown historical link between the Hopewell pedigreeand five French-Canadian families for which historicalinformation was obtained up to the beginning of the18th century.
Carrier Testing and Prenatal Diagnosis
Twenty-six females at risk for inheriting the diseaseallele had their status determined: 13 females are carri-ers, 11 are noncarriers, and carrier status could not bedetermined for 2 (figs. 2 and 4). In family 03, fetalchorionic samples were obtained during a first-tri-mester pregnancy, and RFLP analysis demonstratedthat the male offspring had a very low probability of
1098

X-linked Nephrogenic Diabetes Insipidus
M 1 2 3 4 5 6 7 8 9
Figure 7 PCR analysis of the Stl4 VNTR in,,the Hopewell family (fig. 1, insert B). All the availabof insert B are represented, from left to right, after(which represents molecular markers). Clear separatifor alleles of 1690, 1630, and 1570 bp.
inheriting the disease (fig. 4). PCR analysisVNTR was particularly useful in the Hopei(fig. 1, insert B), where the status of the tpatients (IX-1 and IX-4) could not be deteSouthern analysis of the Stl4-1 RFLP,mothers (VIII-2 and VIII-4) were homozyglele 5. However, by PCR analysis, two all1bp and 1,570 bp) were clearly observed (fthe two women (IX-1 and IX-4) were inf(carriers, since they inherited the 1 ,630-bp;carrier status was supported by the typingDX13. In family 04, the mother is homothe four loci and is not informative for linkright-hand part of Cannon's pedigree (fig.status could not be determined, because thenot typed.
Discussion
Phenotypic homogeneity is now well derin male patients with X-linked NDI: male lnot demonstrate any antidiuretic, vasodilcoagulation factor responses to dDAVP (B1988, 1989; Brommer et al. 1990; Knoers eBichet et al. 1991). These defective resp(
been observed in the Hopewell (Bichet etand other North American (Bichet et al.
European (Brommer et al. 1990; Knoers et al. 1990)families. Our study of this rare disease suggests thatthis phenotypic homogeneity is paralleled by locus ho-mogeneity. Knoers et al. (1988a, 1988b, 1989) stud-ied 11 pedigrees with 20 affected males and also dem-
2400 onstrated tight linkage of the affected gene to DXSS2.1690 We studied 13 families with 34 affected males and1630 obtained similar results.1570 "It is likely that the Hopewell hypothesis can never
be proved" concluded Bode and Crawford (1969) afterthey proposed a common origin of all eastern NorthAmerican families affected by NDI. We demonstrate
700 here with RFLP analysis that affected males from Can-non's Mormon pedigree and from five French-Canadian families have different Xq28 region haplo-types as compared with affected males from theHopewell pedigree. It is therefore unlikely that these
samples from six North American families affected with congenitalole individuals NDI are related to the Nova Scotian settlers of thethe first lane Ulster Scots. Our DNA analysis was complementedon is obtained by extensive new historical information tending to link
the disease not to the Hopewell immigrants but toother Ulster Scots. Further demonstration of separateorigins of the NDI alleles would be provided by the
of the Stl4 discovery of different mutations possibly in the vaso-well family pressin V2 receptor gene (Sharif and Hanley 1992).two female Our analysis of 13 independent families with con-'rmined by genital NDI demonstrates that the recombination fre-since their quency between DXS52 (Stl4 VNTR) and NDI is less;OUs for al- than 5% with respect to the 1-lod-unit support inter-eles (1,630 val (Conneally et al. 1985). In addition, we were ableig. 7), and to infer the carrier status for 24 of 26 females at riskerred to be in these families. This is in sharp contrast with theallele. This unreliability of phenotypic information of females atwith probe risk: these patients could be polyuro-polydipsic, butlzygous for most of them have normal concentrating ability. Inage. In the our experience, DXSS2 genotyping was easily and2), carrier rapidly achieved by PCR analysis of the Stl4 VNTRfather was (Richards et al. 1991). We propose that all pedigrees
with X-linked NDI should be evaluated by thismethod. For informative families, male fetuses couldhave their status determined byDNA analysis ofchori-onic villus biopsy samples. Alternatively, PCR analy-
nonstrated sis of a DNA sample from a newborn son could bepatients do done within 48 h of birth, and appropriate water ad-lating, and ministration and clinical and plasma electrolyte sur-'ichet et al. veillance could be carried out.t al. 1990; No recombination was observed between fouronses have Xq28 markers and NDI in 10 families from the Neth-al. 1989) erlands (Knoers et al. 1988b). We observed in the1988) and Mormon pedigree a recombination between DXS304
1099

1100 Bichet et al.
(probe U6:2.spl), DXS30S (St3S-691), and NDI.DXS304 is centromeric to the four other Xq28 loci(Rousseau et al. 1990). Thus NDI maps telomeric toDXS304,DXS30S but close to the more distal lociDXSS2, DXS15, and F8C (see table 3). On the basisof meiotic (Mulligan et al. 1987; Vincent et al. 1989;Rousseau et al. 1990; Suthers et al. 1991) and physicalmapping (Feil et al. 1990; Poustka et al. 1991; Schles-singer et al. 1991), the most likely order with recombi-nation fractions is q27-DXS304-.109-DXS305-.014-DXSS2-.006-DXS1S-.024-F8C.Our recent work supports a precyclic AMP-defec-
tive mechanism as the explanation for the lack of uri-nary concentration in response to vasopressin (Bichetet al. 1988). This suggests that the vasopressin recep-tor itself could be altered. Jans et al. (1990) tested thehypothesis that the V2 receptor gene can be localizedto the same chromosomal region as the NDI locus.They examined series of hamster lung fibroblast andmouse lymphocyte cell lines carrying fragments of hu-man X chromosome. V2 receptor binding activity andinduction of cyclic-AMP production in response tovasopressin were exhibited by all somatic cell hybridlines carrying human X-chromosome portions whichcontain Xq28. These data are compatible with a re-gional colocalization of the V2 receptor and the NDIlocus. When we initiated our study, the cyclic-AMP-dependent renal vasopressin receptor (the V2 receptor)had not been characterized. However, very recentlyBirnbaumer et al. (1992) reported cloning of the hu-man V2 receptor, and Lolait et al. (1992) reported thecloning of the rat counterpart. Mutational analyses ofthe V2 receptor gene in congenital NDI can now becarried out. These studies will be facilitated by havinga well-characterized cohort of affected kindreds suchas those reported here. Even if it is demonstrated thata mutation in the V2 receptor gene is responsible forNDI, it may be that there are different mutations indifferent families, so that direct detection of all muta-tions might be impractical and testing for carrier statusmight still rely on RFLP analysis in informative fami-lies.
In summary, we obtained DNA from a number offamilies with phenotypically similar X-linked NDI pa-tients. We analyzed polymorphic markers in the Xq28region by using Southern and PCR analyses. No re-combination was observed between NDI and theX-telomeric loci DXSS2, DXS15, and F8C, anddifferent haplotypes segregating with the disease wereobserved among independent families, suggesting in-dependent origins of NDI mutations. These results
were supported by extensive historical informationobtained on the Hopewell, Mormon, and French-Canadian pedigrees. The Hopewell hypothesis cannotexplain the origin ofNDI in many of the North Ameri-can families, since they have no apparent relationshipwith the Hopewell early settlers, either by haplotypeor genealogical analysis. Our results provide addi-tional support for the mapping of X-linked NDI anddemonstrate the usefulness ofPCR analysis of the Stl4VNTR for carrier detection in NDI families.
Note added in proof. -van den Ouweland et al.(1992) report two recombinants between NDI andDXS30S.
AcknowledgmentsWe thank the patients and their families for their partici-
pation; Nicole Ruel, Isabel Bolivar, Johanne Bourdon, andCeline Champigny for technical assistance; Don Awalt forhistorical and pedigree analysis; and Diane Dugas and Do-minique Castonguay for secretarial expertise. This researchwas supported by grants from the Medical Research Councilof Canada (MT-8126 and MA-9315), the Canadian KidneyFoundation, and the Canadian Networks of Centres of Ex-cellence program (Canadian Genetic Diseases Network).D.G.B. and G.N.H. are senior scholars of Le Fonds de laRecherche en Sante du Quebec.
ReferencesBichet DG, Arthus MF, Lonergan M (1991) Platelet vaso-
pressin receptors in patients with congenital nephrogenicdiabetes insipidus. Kidney Int 39:693-699
Bichet DG, Razi M, Arthus MF, Lonergan M, Tittley P,Smiley RD, Rock G, et al (1989) Epinephrine and dDAVPadministration in patients with congenital nephrogenicdiabetes insipidus: evidence for a pre-cyclic AMP V2 re-ceptor defective mechanism. Kidney Int 36:859-866
Bichet DG, Razi M, Lonergan M, Arthus MF, Papukna V,Kortas C, Barjon JN (1988) Hemodynamic and coagula-tion responses to 1 -desamino[8-D-arginine]vasopressin inpatients with congenital nephrogenic diabetes insipidus.N Engl J Med 318:881-887
Birnbaumer M, Seibold A, Gilbert S, Ishido M, Barberis C,Antaramian A, Brabet P, et al (1992) Molecular cloningof the receptor for human antidiuretic hormone. Nature357: 333-335
Bode HH, CrawfordJD (1969) Nephrogenic diabetes insip-idus in North America: the Hopewell hypothesis. N EnglJ Med 280:750-754
Brommer EJP, Brink H, Derkx FHM, Schalekamp MAH,Stibbe J (1990) Normal homeostasis of fibrinolysis innephrogenic diabetes insipidus in spite of defective V2-

X-linked Nephrogenic Diabetes Insipidus 1101
receptor-mediated responses of tissue plasminogen activa-tor release. Eur J Clin Invest 20:72-78
Cannon JF (1955) Diabetes insipidus: clinical and experi-mental studies with consideration of genetic relationships.Arch Intern Med 98:215-272
Conneally PM, Edwards JH, Kidd KK, LalouelJM, MortonNE, Ott J, White R (1985) Report of the Committee onMethods of Linkage Analysis and Reporting. CytogenetCell Genet 40:356-359
Eaton AWH (1912) The settling of Colchester County,Nova Scotia, by New England Puritans and Ulster Scots-men. Proc Trans R Soc Can 6 (ser 3, Trans sec 2): 221-265
Feil R. Palmieri G, d'Urso M, Heilig R, Oberle I, MandelJL (1990) Physical and genetic mapping of polymorphicloci in Xq28 (DXS15, DXSS2, and DXS124): analysis ofa cosmid clone and a yeast artificial chromosome. Am JHum Genet 46:720-728
Harper K, Winter RM, Pembrey ME, Hartley D, DaviesKE, Tuddenham EGD (1984) A clinically useful DNAprobe closely linked to Haemophilia A. Lancet 2:6-8
Heilig R, Oberle I, Arveiler B, Hanauer A, Vidaud M, Man-delJL (1988) Improved DNA markers for efficient analysisof fragile X families. Am J Med Genet 30:543-550
Jans DA, van Oost BA, Ropers HH, Fahrenholz F (1990)Derivatives of somatic cell hybrids which carry the humangene locus for nephrogenic diabetes insipidus (NDI) ex-press functional vasopressin renal V2-type receptors. JBiol Chem 265:15379-15382
Kambouris M, Dlouhy SR, Trofatter JA, Conneally PM,Hodes ME (1988) Localization of the gene for X-linkednephrogenic diabetes insipidus to Xq28. Am J Med Genet29:239-246
Kidd KK, Bowcock AM, Schmidtke J, Track RK, RicciutiF, Hutchings G, Bale A, et al (1989) Report of the DNAcommittee and catalogs of cloned and mapped genes andDNA polymorphisms. Human gene mapping 10. Cyto-genet Cell Genet 51:622-947
Knoers N, Brommer EJP, Willems H, van Oost BA, Mon-nens LAH (1990) Fibrinolytic responses to 1 -desamino-8-D-arginine-vasopressin in patients with congenital neph-rogenic diabetes insipidus. Nephron 54:322-326
Knoers N, van der Heyden H, van Oost BA, Monnens L,WillemsJ, RopersHH (1988a) Linkage of X-linked neph-rogenic diabetes insipidus with DXS52, a polymorphicDNA marker. Nephron 50:187-198
(1989) Three-point linkage analysis using multipleDNA polymorphic markers in families with X-linkednephrogenic diabetes insipidus. Genomics 4:434-437
Knoers N, van der Heyden H, van Oost BA, Ropers HH,Monnens L, Willems J (198 8b) Nephrogenic diabetes in-sipidus: close linkage with markers from the distal longarm of the human X chromosome. Hum Genet 80:31-38
Kobrinsky NL, Doyle JJ, Israels ED, Winter JSD, CheangMS, Walker KD, Bishop AJ (1985) Absent factor VIII
response to synthetic vasopressin analogue (DDAVP) innephrogenic diabetes insipidus. Lancet 1:1293-1294
Lathrop GM, Lalouel JM, Julier C, Ott J (1984) Strategiesfor multilocus linkage analysis in humans. Proc Natl AcadSci USA 81:3443-3446
(1985) Multilocus linkage analysis in humans: detec-tion of linkage and estimation of recombination. Am JHum Genet 37:482-498
Lolait SJ, O'Carroll AM, McBride OW, Konig M, Morel A,Brownstein MJ (1992) Cloning and characterization of avasopressin V2 receptor and possible link to nephrogenicdiabetes insipidus. Nature 357: 336-339
McKusick VA (1990) Diabetes insipidus renal type I. In:Mendelian inheritance in man, 9th ed. Johns HopkinsUniversity Press, Baltimore, p 1585
Mandel JL, Arveiler B, Camerino G, Hanauer A, Heilig R,Koenig M, Oberle I (1986) Genetic mapping of the humanX chromosome: linkage analysis of the q26-q28 regionthat includes the fragile X locus and isolation of expressedsequences. Cold Spring Harbor Symp Quant Biol 51: 195-203
Miller T (1972) Historical and genealogical record of thefirst settlers of Colchester County. Mika Publishing,Belleville, Ontario (First published in 1873 by A & WMacKinlay, Halifax)
Mulligan LM, Grover HJ, Blanchette VS, Giles AR, LillicrapDP, Phillips A, Holden JJ, et al (1987) Recombinationbetween the factor VIII gene and the DXSS2 locus givesthe most probable genetic order as centromere-FRA(X)-DXS15-DXSS2-F8C-telomere. Am J Med Genet 26:751-760
Oberle I, Camerino G, Heilig R, Grunebaum L, CazenaveJP, Crapanzano C, Mannucci PM, et al (1985) Geneticscreening for hemophilia A (classic hemophilia) with apolymorphic DNA probe. N Engl J Med 312:682-686
OttJ (1991) Analysis ofhuman genetic linkage, rev ed. JohnsHopkins University Press, Baltimore and London
Poustka A, Dietrich A, Langenstein G, Toniolo D, WarrenST, Lehrach H (1991) Physical map of human Xq27-qter:localizing the region of the fragile X mutation. Proc NatlAcad Sci USA 88:8302-8306
Reeves WB, Andreoli TE (1989) Nephrogenic diabetes in-sipidus. In: Scriver CR, Beaudet AL, Sly WS, Valle D(eds) The metabolic basis of inherited disease, 6th ed.McGraw-Hill, New York, pp 1985-2011
Richards B, Heilig R, Oberle I, Storjohann L, Horn GT(1991) Rapid PCR analysis of the St14 (DXSS2) VNTR.Nucleic Acids Res 19:1944
Rousseau F. Vincent A, Oberle I, Mandel JL (1990) Newinformative polymorphism at the DXS304 locus, a closedistal marker for the fragile X locus. Hum Genet 84:263-266
SambrookJ, Fritsch EF, Maniatis T (eds) (1989) Molecularcloning: a laboratory manual. Cold Spring Harbor Labo-ratory, Cold Spring Harbor, NY

1102 Bichet et al.
Schlessinger D, Little RD, Freije D, Abidi F, Zucchi I, PortaG, Pilia G, et al (1991) Yeast artificial chromosome-basedgenome mapping: some lessons from Xq24-q28. Geno-mics 11:783-793
SharifM, HanleyMR (1992) Peptide receptors: stepping upthe pressure. Nature 357:279-280
Suthers GK, Oberle I, Nancarrow J, MulleyJC, Hyland VJ,Wilson PJ, McCureJ, et al (1991) Genetic mapping of thenew RFLPs at Xq27-q28. Genomics 9:37-43
van den OuwelandAMW, KnoopMT, KnoersWAM, Marks-lag PWB, Rocchi M, Warren ST, Ropers HH, et al (1992)Colocalization of the gene for nephrogenic diabetes insip-idus (DIR) and the vasopressin type 2 receptor gene(AVPR2) in the Xq28 region. Genomics 13:1350-1352
Vincent A, Kretz C, Oberle I, Mandel JL (1989) A newpolymorphic marker very closely linked to DXS52 in theq28 region of the human X chromosome. Hum Genet 82:85-86





























