Embed Size (px)
Citation preview

Neglect assessment as an application ofvirtual reality
Introduction
Visuospatial neglect is a common syndrome fol-lowing right hemisphere lesions. Almost half of allpatients with a stroke in the right side of the brainmay show visuospatial neglect in the acute phase(1, 2). A variety of methods is used to assessvisuospatial neglect, such as figure copying andfreehand drawing, line bisection, reading andwriting and target cancellation tasks (3). Themost common method is probably cancellationtasks (4). These tasks require visual search andcoordinated explorative hand and eye movementsin space. In this type of tasks, a high number ofomissions of the target stimuli and a bias to thecontralesional side in the location of the omissionsare typically considered as basic components ofneglect (3). In visual search tasks, patients withneglect do not only exhibit omissions of visualtargets but also demonstrate more general deficitsin their search performance such as an unsystem-atic search pattern and irregular eye movementpatterns (5, 6). Further, the pattern of visuo-motor
search in patients with neglect is affected by spacere-exploration and re-marking of targets (7).Although oculomotor behaviour in visual searchhas been extensively studied, relatively less isknown about the kinematics of the hand move-ments during the performance in visual searchtests. Recently, virtual reality (VR) technologieshave begun to be used as an assessment tool inneuropsychological practice (8, 9). There are sev-eral strengths underlying the use of VR technology.VR is designed to simulate naturalistic environ-ments in which performance can be tested andtrained in a systematic way. VR has the possibil-ities for real-time performance feedback, and fordetailed recordings of the kinematics of the handmovement, allowing the monitoring of the patient’sprogress (10, 11).The purpose of this pilot study was to: (1) test a
novel VR application in neglect assessment bycomparing a cancellation task in a virtual environ-ment with conventional tests of neglect; (2) des-cribe the pattern of manual search performance;and (3) obtain kinematic data of hand movement.
Acta Neurol Scand 2007: 116: 157–163 DOI: 10.1111/j.1600-0404.2007.00821.x Copyright � 2007 The AuthorsJournal compilation � 2007 Blackwell Munksgaard
ACTA NEUROLOGICASCANDINAVICA
Broeren J, Samuelsson H, Stibrant-Sunnerhagen K, Blomstrand C,Rydmark M. Neglect assessment as an application of virtual reality.Acta Neurol Scand 2007: 116: 157–163.� 2007 The Authors Journal compilation � 2007 Blackwell Munksgaard.
Objective – In this study a cancellation task in a virtual environmentwas applied to describe the pattern of search and the kinematics ofhand movements in eight patients with right hemispherestroke. Methods – Four of these patients had visual neglect and fourhad recovered clinically from initial symptoms of neglect. Theperformance of the patients was compared with that of a control groupconsisting of eight subjects with no history of neurologicaldeficits. Results – Patients with neglect as well as patients clinicallyrecovered from neglect showed aberrant search performance in thevirtual reality (VR) task, such as mixed search pattern, repeated targetpressures and deviating hand movements. The results indicate that inpatients with a right hemispheric stroke, this VR application canprovide an additional tool for assessment that can identify smallvariations otherwise not detectable with standard paper-and-penciltests. Conclusion – VR technology seems to be well suited for theassessment of visually guided manual exploration in space.
J. Broeren1,4, H. Samuelsson2,3,K. Stibrant-Sunnerhagen1,C. Blomstrand3, M. Rydmark4
1Rehabilitation Medicine, Institute of Neuroscience andPhysiology, Gçteborg, Sweden; 2Department ofPsychology, Faculty of Social Sciences, Gçteborg,Sweden; 3Stroke Research Group, Institute ofNeuroscience and Physiology, Gçteborg, Sweden;4Mednet, Institute of Biomedicine, Gçteborg, Sweden
Key words: kinematics; neglect; neuropsychologicalassessment; stroke; virtual environments; virtualreality
Jurgen Broeren, Rehabilitation Medicine, Institute ofNeuroscience and Physiology, Guldhedsgatan 19,Gçteborg SE 413 45, SwedenTel.: +46 704380836Fax: +46 31415433e-mail: [email protected]
Accepted for publication January 12, 2007
157

Methods
Subjects
Eight patients with stroke (P1–P8) and right braindamage were included, mean age 54 years (range44–63) (Table 1). All subjects underwent in- or outpatient rehabilitation at the Department of Reha-bilitation Medicine at Sahlgrenska University Hos-pital, Goteborg, Sweden. The criteria for inclusionwere: (1) right-sided brain damage confirmed byCT or MRI scans; (2) visual neglect identified bythe star cancellation test and the baking tray task,2–5 weeks post-stroke; (3) ability to understandinformation; (4) right-handed with no signs ofmotor impairment on the right side; and (5) noprestroke history of visual deficits. Eight controlsubjects were recruited; four men and four women,mean age 53 years (range 33–63). The criteria forinclusion for the controls were: (1) right-handed;and (2) no history of visual or neurological deficits.All subjects gave informed consent to participate inthe study which has been performed in accordancewith the local Ethics Committee at GoteborgUniversity.
Lesion analysis
Stroke classification was based on review of themedical records. The localization and extent of thelesions was determined from magnetic resonanceimaging and/or computed tomography scans by anexperienced neuro-radiologist and re-evaluated byan experienced stroke neurologist.
Computer equipment
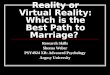
The VR environment consisted of a PC-basedsemi-immersive workbench (Fig. 1). The computer
hardware was composed of an Intergraph Zx10ViZual Workstation (2 · 750 MHz Pentium IIIwith 512 MB RAM and a WildCat 4110 graphiccard, Windows 2000). Stereoscopic glasses usedhere were liquid crystal shutter eyewear for Ste-reo3D imaging.The user looked into a virtual world generated in
the computer. Using stereoscopic shuttered glasses,the user observed a 3D image displayed on thetabletop. He/she was now able to reach into avirtual space and interact with 3D objects througha hand-held stylus (haptic device) positioned in theline of sight. A haptic device gave the sense oftouch feedback to users when they contactedvirtual objects. Haptic force feedback was provi-ded by using a desk-mounted robot samplingat 1000 Hz (PHANTOM� DesktopTM) fromSensAble Technologies.
Conventional tests of visual neglect
Star cancellation test – It is a subtest in theBehavioural Inattention Test battery (12). It con-sists of a total of 52 large stars, 56 smaller stars, 13letters and 10 short words, which are pseudo-randomly positioned over a landscape A4 sheet.The patients where asked to cross out all the smallstars on the sheet with a pen. The maximum scorewas 54; 27 on each side of the midline (two smallstars in the centre were not counted). The cut-offcriterion for visual inattention is based on thenormative range obtained from a Swedish controlgroup (13) and the cut-off for visual neglect was setto a score below 51 targets.
Stereoscopic glasses
Haptic device
Figure 1. Semi-immersive work bench (http://www.reachin.se)with haptic device and stereoscopic glasses.
Table 1 Clinical data and demographics for the patient group
Subjects SexAge
(years) AetiologyLesion
localization
Weekssincestroke
Lengthof stay(days)
P1 M 55 Infarction F/P/T 36 126P2 M 51 Infarction F/P/T/Th/C/L/I 13 75P3 F 44 Infarction Th/C/L 7 91P4 F 60 Infarction P/T/Th/ 39 65P5 M 58 Haemorrhage F/P/T//Th/C/L/I 5 64P6 F 63 Aneurysm F/T/C/L/I 10 88P7 F 50 Infarction F/T/I 34 57P8 M 54 Haemorrhage F/P/T 14 93
Involvement of frontal (F), parietal (P), temporal (T), thalamus (Th), Caudate Nucleus(C), Lenticular Nucleus (L), Insula (I). Length of stay: as in-patient after the acutestroke.
Broeren et al.
158

The baking tray task – The subjects have to place 16identical items (3.5 cm wooden cubes) on a blanktest board, the baking tray (75 · 100 cm). They areasked to place the wooden blocks as symmetricalas possible as if they were �buns� on a baking tray.The number of cubes in each half of the field wascounted. When a cube straddled on the midline, ascore of 1/2 was counted. A normal distribution iseight cubes in each field. Cut-off is a distributionmore skewed than seven items on the left half andnine items (7/9) on the right (14).
Computerized task – VR and haptics
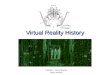
A cancellation test was developed in the VRenvironment, with 20 targets and 60 distracters(2.7 cm diameter). The physical search area wascomprised of a rectangular tilted plane (width ·height: 24 · 18 cm) with a visual angle approxi-mately between 35� and 40� (Fig. 2).The target was the digit �1� and the distracters
were other numbers. The targets marked with thenumber 1 were distributed pseudo-randomly on thecomputer screen with 10 targets to the left and 10targets to the right of the centre of the computerscreen. When the response pattern was analysed,the screen was divided into four columns and threerows (see Fig. 2). The maximum score was 18; nineon each side of the midline (two targets in thecentre were not scored). The cut-off criterion forvisual neglect was based on the normative rangeobtained from the control group and the cut-offwas set to 18 targets.The following registrations were obtained.
Omissions of targets – The number of targetsmarked in the test was counted. The ideal score is9/9.
Search pattern – The pattern of hand movementsduring the search was classified as search by row,column or as a mix of search patterns. It wasclassified as row if the pattern proceeded insuccessive horizontal sweeps across the VR task,column if the pattern proceeded in successivevertical sweeps, otherwise it was classified as amix of search pattern. Additional information onthese patterns was provided by a method des-cribed by Mark et al. (15). The x coordinate andy coordinate values of all marked locations weremeasured. Pearson correlation coefficients (r)were calculated from the linear regression of thex values of the marked locations relatively to theorder in which they were marked. The sameprocedure was undertaken for the y values. Fromthese two measures, the higher r value (the �best�correlation) was chosen to characterize the extentto which cancellations were completed orthogo-nally. The strength of the correlation providesinformation about the degree to which themovements are pursued in successive horizontalor vertical sweeps across the VR task. A mix ofhorizontal and vertical movement will yield aweaker correlation.
Start column – The location of the start of searchwas registered. The columns were defined ascolumns 1–4 from left to right (Fig. 2).
Repeated target press – The proportions of targetpushes that were repetitions of previously pressedtargets. All targets and distracters on the screenhad a green colour, but when a target was pushed,it shifted colour from green to yellow and then itstayed yellow throughout the test session, i.e. avisual cue was given that the target had beenpressed.
Kinematics – The x, y and z coordinates (resam-pled at 50 Hz) of the haptic device were recordedand time stamped, giving the basic pattern ofhand movement. Time and trajectory (length)were recorded. From these records, velocity andhand path ratio (HPR) was computed. The HPRwas the distance traversed by the haptic stylus,divided by the straight line distance between thetargets. Thus, a hand trajectory that followed astraight line pathway to the target would have anHPR equal to 1, whereas a hand trajectory thattravelled twice as far would have an HPR of 2.One-tailed upper 97.5% reference limits werecalculated for the time and the HPR variables:mean + 2.5 · SD (2.5 being the tolerance factorfor n ¼ 8).
1 2 3 4
Figure 2. The virtual reality task (screenshot) divided intorows and columns. Zero (0) is end target.
Neglect assessment as an application of virtual reality
159

Procedure
Conventional tests of visual neglect – The subjectswere comfortably seated on a table. The sheet orthe test board for the cancellation test and bakingtray task was placed in front of the subject centredto the body midline. It was not permitted to movethe test board or test sheet during the session.
Computerized test – The subjects were placed infront of the computer screen centred to the bodymidline and were then instructed to grasp andmove the stylus and press all targets marked withthe digit 1 on the computer screen. Once a targetwas pressed, it turned from green to yellow. Thehaptic device (resistive force feedback) added thesense of real touch to the visual cue when pressingthe targets. The subjects were asked to indicatewhen they have finished their search by pressing ared button marked with 0 (zero), located in thelower right end of the screen (see Fig. 2).
Results
Visuospatial attention
Data from the two conventional tests of neglectand from the VR task are shown in Table 2. Thedata demonstrate the level of impairments in visualattention in terms of omissions and spatial bias inthe performance. In four patients (P1–P4), visualneglect was identified by the conventional tests. Inone of these patients (P4), neglect was onlyidentified by the baking tray test while for P1 andP3 neglect was only observed in the star cancella-tion test. In the VR task, omissions of targets wereobserved in all these four patients. Another fourpatients who exhibited neglect at the admission tothe rehabilitation unit had recovered from these
symptoms at the time of this assessment and theyshowed no omissions and no contralesional bias.However, one patient (P5) had a slight sign of anipsilesional bias in the baking tray task.
Hand movement pattern during visual search
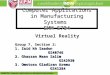
The search performance in the VR task is given inTable 3. The data for the two patient groups aresimilar while the patients differ in their perform-ance compared with the control subjects. Six out ofeight patients used a mixture of row and columnsearch while the search performance in the controlgroup was dominated by search by row only or bycolumn only. A relatively low correlation (i.e. Best rin Table 3) was observed in four of the patients(P1, P2, P5 and P6) and in one of the controls (C5).None of the controls showed repeated targetpressures but this observation was made in fiveout of eight patients. These patients exhibitedrepetitive pressures of the same target during theexploration, but no left/right predominance couldbe discerned. In Fig. 3, data from two �typical�subjects (P3 and C3) are presented. The patientstarts in the right most column and displays atypical mixed pattern, while the control starts inthe upper left part of the search area and has arow-by-row search strategy. Noteworthy are theweb-like clusters found frequently in the patient’spattern, but only initially in the control’s pattern.
Hand path ratio – The data in Table 3 describe thedeviation of the movements of the hand whenmoving from one target to the next during thesearch. Most of the patients (6/8) had greaterdivergence than the control group (controls:mean ¼ 2.4, SD ¼ 0.480, upper 97.5% referencelimit 3.6.).
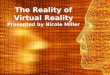
Time (s) and velocity (m/s) – The individual timevalues (controls: mean ¼ 36.5 s, SD ¼ 18.5, upper97.5% reference limit 82.7) to conclude the test aregiven in Table 3. The velocity profiles (Fig. 4)reflect the median speed it takes to press eachtarget during the test. The median velocity was0.78 m/s for the controls, 0.75 m/s for the clinicallyrecovered patients, and 0.65 m/s for the patientsnot recovered from neglect. The controls show asomewhat larger dispersion when compared withthe patient group.
Discussion
In this study, we evaluated novel VR technique bycomparing a cancellation task in a virtual environ-ment with conventional tests of neglect. It was
Table 2 Clinical data for the patient group on visuospatial neglect
Patients
Star cancella-tion (27/27)*
Baking traytask (8/8)* VR task (9/9)*
Left Right Left Right Left Right
Not recoveredP1 19 25 7 9 6 9P2 11 13 2 14 2 7P3 19 25 8 8 4 9P4 25 27 6,5 9,5 5 5
Clinically recoveredP5 27 27 9 7 9 9P6 26 27 8 8 9 9P7 27 27 8 8 9 9P8 27 27 8 8 9 9
*Maximum score for each test
Broeren et al.
160

found that the presence or absence of visualinattention was identified for the same patientseither by using VR or the conventional neglecttests. A further aim was to use the VR task toanalyse the manual search performance in a virtualcancellation task. Patients with neglect as well aspatients recovered from neglect showed aberrantsearch performance in the VR task, i.e. mixedsearch pattern, repeated target pressures, ipsile-sional start of search and deviating hand move-ments. The data indicate that this VR task is moreinformative for deviating search performance com-pared with examination of search by more con-ventional paper and pencil tests. For example, in asearch test administered in a study by Samuelsson
(5) the patients had to search and report allnumbers and letters that they could find on a testsheet. In this study, aberrant search performancewas significantly associated with the presence ofvisuospatial neglect. Furthermore, recovery fromthe neglect symptoms at a 6-month follow-up wasfollowed by a return to normal search perform-ance. However, in the present study patients whohad recovered from neglect still exhibited persistingaberrant search. This finding is in accordance witha study by Pflugshaupt et al. (16), showing thatpatients who had recovered from neglect inconventional paper and pencil tests still exhibitedoculomotor and exploratory deficits in novel orcomplex search tasks.
Table 3 Kinematic data for the patient group and healthy subjects
PatientsSearchpattern Best r
Repeated targetpressure
No. of repeatedtarget pressures
Startingcolumn
Handpath ratio
Time to completethe exercise (s)
Medianvelocity (m/s)
Not recoveredP1 Mixture )0.42 Yes 3 (3) 3.7 34 0.058P2 Mixture )0.58 Yes 1 (3) 7.5 59 0.045P3 Mixture )0.81 Yes 2 (3) 4.2 68 0.058P4 Mixture )0.76 No 0 (3) 2.6 37 0.044
Clinical RecoveredP5 Mixture 0.40 Yes 2 (2) 6.6 156 0.062P6 Mixture )0.57 Yes 4 (4) 3.7 43 0.071P7 Column )0.91 No 0 (4) 4.4 46 0.103P8 Row )0.79 No 0 (3) 3.4 66 0.044
Healthy subjectsC1 Row )0.80 No 0 (4) 2.8 24 0.072C2 Row 0.81 No 0 (4) 2.3 30 0.063C3 Row )0.96 No 0 (1) 2.1 33 0.056C4 Row )0.93 No 0 (1) 2.7 48 0.045C5 Mixture 0.47 No 0 (3) 2.0 32 0.046C6 Column 0.96 No 0 (1) 2.4 77 0.029C7 Row )0.86 No 0 (1) 3.2 30 0.086C8 Column 0.87 No 0 (1) 1.7 18 0.096
Patients with values in italics are outside the 95% reference interval.
–0.08
0
0.08
X
P3
Y
Endpoint
Y
–0.1 0 0.1–0.1 0 0.1
–0.08
0
0.08
X
C3
Startpoint
Endpoint
Startpoint
Figure 3. The trajectory way of the right arm for a patient (P3) and a healthy control (C3). The selection of these �typical� subjectswas based on the data in Tables 2 and 3. Accordingly for each group, a subject was chosen who exhibited data that represented acombination of: (1) the most frequent outcome of each nominal variable in the group; and (2) a value as close as possible to themedian for each continuous variable in the group.
Neglect assessment as an application of virtual reality
161

Repeated target pressures were observed in amajority of the patients in the present study.Repeated responses toward the same target intasks of visual search have been described inseveral studies of stroke patients and differentpossible mechanisms behind this phenomenonhave been investigated and discussed (4, 17–20)One mechanism that has been suggested in severalstudies is impaired spatial working memory (WM)(21, 22). Spatial WM is described as importantduring visual search to hold in mind which part ofa visual array that just have been examined (21,22). In the present study, repeated target pressureswere made in spite of the fact that a distinct visualcue was given for each target that had beenpressed. The distinct visual �stop signal� given inthis trial was not based on spatial information andyet the patient was not able to make use of thisinformation to prevent a repeated target pressure.These observations seem to indicate that spatialWM cannot be the only component behind repea-ted pressures in our study. Another possiblemechanism (among others) is a motor persevera-tion due to an inability to inhibit motor responses.This mechanism has for example been described asimportant to prevent preservative responses instandard cancellation tasks (19, 20, 23).Thus, both impaired spatial WM and motor
perseveration may have affected the incidence ofrepeated target pressures in our study. In previousstudies of re-explorations and repeated responsesin patients with neglect, it is suggested that
symptoms of impaired spatial WM is associatedwith brain damage involving the parietal lobe (21,23), while motor perseveration has been associatedwith anterior/frontal involvement (20, 24) ordamage to the underlying basal ganglia (19). Apost hoc examination of the involvement of thefrontal lobe, parietal lobe and basal ganglia wasundertaken in our sample. No systematic relation-ships were observed between the presence ofrepeated responses and damage to either of thesebrain areas. However, the power of these analyseswas week due to the small number of patients.Two of the patients with repeated target pres-
sures in our sample had no symptoms of neglect atthe time of the examination. It is noteworthy thatNys et al. (19) have observed that in stroke patientswithout neglect, repeated responses during visualsearch are associated with the level of executivefunctioning.We found that six of eight patients had more
superfluous movements of the hand during thevisual search compared with the control group.Noteworthy are also the frequent web-like move-ment clusters which are found initially, once, inhealthy persons, but occur frequently during thesearch course of patients with neglect.These phenomena might reflect �planning hesi-
tations� during the navigation that add to thedeviation of the hand movement. These web-likeclusters are minor irregular non-directional move-ments. The clusters are round or oval in outliningand with a diameter of about 10 mm. We consid-ered them to reflect tremor around a waitingposition when planning for a new movement,hence we call them hesitation or planning clusters.The velocity profile in the present study did notdiffer between clinically recovered patients andcontrols. The patients who were not recoveredfrom neglect showed a somewhat lower medianvelocity. This might indicate that the ability to startand continue movements is affected due to plan-ning uncertainty.Tentatively, several components may have led to
the aberrant explorative behaviour observed in thepatient group in the present study. Such compo-nents are: (1) an ipsilesional bias in egocentricrepresentations of space (25); (2) impaired visuo-spatial WM with inability to keep track oflocations already explored (21); and (3) a biastoward local attention during the exploration witha failure to maintain a global (panoramic) patternof the stimuli array (26). These components haveall been suggested as important mechanisms in theneglect phenomenon and they may as well result inineffective guidance of manual performance duringspatial search. However, it is noteworthy that
Patient and control group
0.15
0.10
0.05
0.00
0.20
Clinicallyrecovered(P5–P8)
Not recovered (P1–P4)
Vel
ocity
(m/s
)
Controls (C1–C8)
Figure 4. The average interval velocity (m/s) to detect thetargets for the patient groups and control group is shown asbox plots (25th and 75th percentiles). The median values (thickblack line) with 10th and 90th percentiles are shown at the endof the lines. (—) controls median velocity (m/s).
Broeren et al.
162

Mark et al. (15) in a recent study failed todemonstrate a relation between spatial neglectand disorganized target marking on cancellation.In conclusion, this VR application can provide a
quantitative analysis of detecting small variationsin the manual search performance otherwise notdetected in standard paper-and-pencil tests. TheVR cancellation test takes less than a minute tocomplete and produces kinematic data (27, 28). VRseems suited for attempting the assessment out-lined in this paper. It provides for modification ofthe sensory environment facilitating straightfor-ward and precise assay of phenomena related tocomplex motor behaviour in the real world.Although the results imply that this VR taskrepresents a sensitive measure of more subtleimpairments of the explorative performance instroke patients, future studies using a large groupof patients are needed to further verify the results.
Acknowledgements
We wish to thank all subjects for their collaboration andRagnar Pascher for programming the software. This study wasin part supported by grants from the Swedish Stroke VictimsAssociation, the Hjalmar Svensson Research Foundation,Goteborg Foundation for Neurological Research, Federationof Swedish County Councils (VG-region), Trygg-Hansa insur-ance company, The Swedish Research Council (VR K2002-27-VX-14318-01A) and VINNOVA (2004-02260).
References
1. Fullerton KJ, McSherry D, Stout RW. Albert’s test: aneglected test of perceptual neglect. Lancet 1986;1:430–2.
2. Pedersen PM, Jorgensen HS, Nakayama H, Raaschou HO,
Olsen TS. Hemineglect in acute stroke – incidence andprognostic implications. The Copenhagen Stroke Study.Am J Phys Med Rehabil 1997;76:122–7.
3. Halligan PW, Cockburn J, Wilson BA. The behaviouralassessment of unilateral visual neglect. NeuropsycholRehabil 1991;1:5–32.
4. Parton A, Malhotra P, Husain M. Hemispatial neglect.J Neurol Neurosurg Psychiatry 2004;75:13–21.
5. Samuelsson H, Hjelmquist EK, Jensen C, Blomstrand C.Search pattern in a verbally reported visual scanning test inpatients showing spatial neglect. J Int Neuropsychol Soc2002;8:382–94.
6. Behrmann M, Ebert P, Black SE. Hemispatial neglect andvisual search: a large scale analysis. Cortex 2004;40:247–63.
7. Parton A, Malhotra P, Nachev P et al. Space re-explora-tion in hemispatial neglect. Neuroreport 2006;17:833–6.
8. Parsons TD, Larson P, Kratz K et al. Sex differences inmental rotation and spatial rotation in a virtual environ-ment. Neuropsychologia 2004;42:555–62.
9. Rose FD, Brooks BM, Rizzo AA. Virtual reality in braindamage rehabilitation: review. Cyberpsychol Behav2005;8:241–62.
10. Rizzo AA, Kim GJ. A SWOT analysis of the field of virtualrehabilitation and therapy. In Presence: TeleoperatorsVirtual Environ 2005;14:119–46.
11. Weiss P, Rand D, Katz N, Kizony R. Video capture virtualreality as a flexible and effective rehabilitation tool.J NeuroEng Rehabil 2004;1:12.
12. Halligan PW, Marshall JC, Wade DT. Visuospatial neglect:underlying factors and test sensitivity. Lancet 1989;2:908–11.
13. Samuelsson H, Hjelmqvist E, Naver H, Blomstrand C. Vis-uospatial neglect and an ipsilesional bias during the start ofperformance in conventional tests of neglect. Clin Neuro-psychol 1996;10:15–24.
14. Tham K, Tegner R. The baking tray task: a test of spatialneglect. Neuropsychol Rehabil 1996;6:19–25.
15. Mark VW, Woods AJ, Ball KK, Roth DL, Mennemeier M.Disorganized search on cancellation is not a consequenceof neglect. Neurology 2004;63:78–84.
16. Pflugshaupt T, Bopp SA, Heinemann D et al. Residualoculomotor and exploratory deficits in patients withrecovered hemineglect. Neuropsychologia 2004;42:1203–11.
17. Husain M, Rorden C. Non-spatially lateralized mecha-nisms in hemispatial neglect. Nat Rev Neurosci 2003;4:26–36.
18. Manly T, Woldt K, Watson P, Warburton E. Is motorperseveration in unilateral neglect �driven� by the presenceof neglected left-sided stimuli? Neuropsychologia2002;40:1794–803.
19. Nys GM, van Zandvoort MJ, van der Worp HB, Kappelle LJ,
de Haan EH. Neuropsychological and neuroanatomicalcorrelates of perseverative responses in subacute stroke.Brain 2006;129(Pt 8):2148–57.
20. Rusconi ML, Maravita A, Bottini G, Vallar G. Is the intactside really intact? Perseverative responses in patients withunilateral neglect: a productive manifestation. Neuro-psychologia 2002;40:594–604.
21. Husain M, Mannan S, Hodgson T, Wojciulik E, Driver J,
Kennard C. Impaired spatial working memory across sac-cades contributes to abnormal search in parietal neglect.Brain 2001;124(Pt 5):941–52.
22. Wojciulik E, Husain M, Clarke K, Driver J. Spatial workingmemory deficit in unilateral neglect. Neuropsychologia2001;39:390–6.
23. Mannan SK, Mort DJ, Hodgson TL, Driver J, Kennard C,
Husain M. Revisiting previously searched locations in vis-ual neglect: role of right parietal and frontal lesions inmisjudging old locations as new. J Cogn Neurosci2005;17:340–54.
24. Na DL, Adair JC, Kang Y, Chung CS, Lee KH, Heilman KM.Motor perseverative behavior on a line cancellation task.Neurology 1999;52:1569–76.
25. Karnath HO, Niemeier M, Dichgans J. Space exploration inneglect. Brain 1998;121(Pt 12):2357–67.
26. Halligan PW, Marshall JC. Toward a principled explan-ation of unilateral neglect. Cogn Neuropsychol1994;11:167–206.
27. Baheux K, Yoshizawa M, Seki K, Handa Y. Virtual realitypencil and paper tests for neglect: a protocol. Cyber-psychol Behav 2006;9:192–5.
28. Bardorfer A, Munih M, Zupan A, Primozic A. Upper limbmotion analysis using haptic interface. IEE Trans Mech-atron 2001;6:253–60.
Neglect assessment as an application of virtual reality
163