Embed Size (px)
Citation preview

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
1
National Continence Management Strategy
Innovative Grants
Final Report
Innovative Grant Round 2 No. 29
Project Title: Randomised control trial bladder pressure management vs. management based on symptoms and residual volumes in patients with established Multiple Sclerosis. Full Business Name of Administrating Organisation: The University of Melbourne ABN number: 84 002 705 224 Full Street Address: Parkville, Victoria 3052 Australia Post Office Box Address: Ethical approval: The Royal Melbourne Hospital Ethics Committee Contact Person: Dr Helen E O’Connell Position Title: Urologist and Senior Lecturer Address: Suite 12 Private Medical Centre Royal Pde Parkville Vic 3050 Phone: 03 9347 9911 Fax: 03 9347 5960 E-mail: [email protected]

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
2
Research Team at RMH:
Dr Helen E. O’Connell, MBBS, MMed, FRACS, Urologist, Principal Investigator Professor Anthony J. Costello, MBBS, FRACS, MD Urologist, Co-investigator Dr. John King, MBBS, MD, FRACP Neurologist, Co-investigator A/Professor Trevor Kilpatrick, MBBS, FRACP, PhD Neurologist, Co-investigator Dr Mike Whishaw, MBBS, FRACP Geriatrician, Melbourne Health,
Melbourne Extended Care and Rehabilitation Service
Dr Ramin Samali, BSc (Med), MBBS (Hon) Urology Fellow Mrs. Louise Kurczycki, RN, BAppScN, GradDipN, Continence Nurse Advisor Unit Manager Mrs Kathy Myles, DipAppSci, BSc (Hons) Research Assistant Dr Lachlan MacGregor, MBBS,MMedSc,DRANZCOG Statistician
Acknowledgements:
Professor Steven Davis Neurologist, Director of Neurology Dr Samantha Pillay Urologist Dr Catherine Temelcos Urologist Dr Helmut Butzkueven Neurologist Dr Niall Tubridy Neurologist Dr Mark Marriott Neurologist Mr John Carey MS Research Nurse Neurology
Ms Josephine Baker Clinical Research Nurse Urology Dr Elizabeth McDonald, Medical Director MS Society (Victoria) Ms Janet Francis and staff MS Nerve Centre Blackburn Mrs Lynda Erskine Secretary

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
3
PROJECT SUMMARY
The initial National Continence Management Strategy grant has enabled the NeuroUrology
and Continence Unit, Royal Melbourne Hospital (RMH) to set up as a clinical research Unit
that offers a state wide clinical service. A working infrastructure is in place and promotional
and collaborative research networks have been made. A close working partnership has been
forged with the Neurology department who collaborate in the study.
The Randomised Control Trial (RCT) of bladder pressure management in people with
Multiple Sclerosis (MS) and bladder dysfunction is in progress. The preliminary data
presented in this report are the result of the pilot study and the initial study recruits.
Objectives
Evaluate by RCT design, two different management strategies and to assess their relative
effect on quality of life as well as their short and long term efficacy. To carry this out:
• Develop the necessary staff, infrastructure, systems and networks to carry out the
study including the fluoroscopic and other urodynamic studies, questionnaires,
Urological and Neurological clinical care, community links for ongoing care,
administration of the clinic, investigations, database, reporting and fund raising
• Perform a pilot study to systematically evaluate management of significant urinary
disorder people with multiple sclerosis (MS) to determine the impact of management
on urinary specific quality of life.
• Determine whether questionnaires used in other patient populations are suited to use
for studies of people with MS related urinary dysfunction and which of these is
suitable as the primary outcome measure for the RCT
• Perform a power study to determine sample size for the RCT
Develop a service in the public environment to provide a prospectively evaluated service to
people with significant urinary distress due to MS and other neurological disorders.
Methodology
Preliminary Studies
The staff, equipment and clinical facilities of the NeuroUrology and Continence Unit
(NUCU) were developed at Royal Melbourne Hospital from November 2001 to the present.
The service is comparable to that which has been carried out in private practice but with a

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
4
greater focus on systematic prospective evaluation of management strategies. Established
urinary quality of life tools; Urogenital Distress Inventory (UGDI), Incontinence Impact
Questionnaire (IIQ), American Urological Association Symptom Score (AUA symptom
score) and Global Quality of life question were used to determine their responsiveness to
treatment in people with MS and suitability for use in long-term studies of urinary treatments.
These measures were then used to obtain preliminary outcome data on the effectiveness of
one of the Algorithms being evaluated i.e. management of significant urinary problems in
people with MS using a bladder pressure management (or Urodynamic diagnosis directed)
strategy. This data then served as the basis for the power study for the RCT to determine
appropriate sample size. Appropriate tools for evaluation of MS status were determined and
arrangements were made with the Neurologists to co-evaluate the patients. Links between
our Unit and a number of relevant organisations have been developed to provide ongoing
assistance to people with MS and facilitate recruitment. With the rate of referral from GPs
and Neurologists it became apparent that formal recruitment activities would be necessary to
ensure an adequate number of recruits for the RCT.
RCT bladder pressure management vs. management based on symptoms and residual
volumes in patients with established Multiple Sclerosis.
• Patients with Multiple Sclerosis and urinary symptoms from various sources were invited
to participate.
• Following consent procedures, patients are randomly allocated to 2 groups.
- The Control group: Management based on history and urodynamics evaluation.
- The Trial group: Management based on history and presenting problems
• At enrolment, and regular intervals (1 month, 3 month, 6 month and annually), patients
complete the Urogenital Distress Inventory (UGDI-6), the Incontinence Impact
Questionnaire (IIQ-7) and the AUA-Symptom Score including the global quality of life
question. Multiple Sclerosis severity is graded by the Neurologist using the Kurtze
Expanded Disability Status Scale (EDSS) and the UK Neurological Disability Scale
(UKNDS). Other outcome measures include urine cultures, residual volume
measurement, voiding chart parameters and a log of adverse events
• The Control group undergoes a fluoroscopic urodynamic study (FUDS) involving
assessment of flow rate, cystometrogram, residual urine volume, external sphincter
assessment behaviour and bladder leak point pressure. This study forms the basis for
initiating treatment in the Control Group

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
5
• Treatment for the Control Group is based on urodynamic findings. The medical treatment
includes anticholinergic and other medications +/- intermittent catheterisation. Possible
surgical treatment may include augmentation cystoplasty or detrusor mymectomy, urinary
diversion as indicated. Fluoroscopic urodynamic evaluation is repeated at 12 months
• The Trial Group undergoes a plain urodynamic study (UDS). Evaluation and treatment
are initiated by a Continence Nurse Advisor (CNA) who is blinded to the result of the
UDS. A comprehensive assessment is taken by the CNA. Treatment is based on the
presenting symptoms and problems rather than urodynamic findings. The treatment may
include anticholinergic and other medications +/- intermittent catheterisation.
Results Pilot studies
Urogenital distress in people with MS is severe. In the pilot study, treatment was associated
with a reduction of 48% and 77% at 3 and 6 months respectively in UGDI-6 scores
representing a significant improvement in urinary specific quality of life and reduction in
urogenital distress. All measures reflected this improvement including a drop of 30% and
74% for IIQ-7; 53% and 61% for AUA-SS as well as 20% and 20% for Urological Quality of
Life respectively at 3 and 6 months post treatment. In people with MS all of the outcome
measures tested (UGDI, IIQ, AUA-SS) appear to be responsive to treatment. The UGDI
appears to be highly responsive, simple to administer and appropriate as a primary outcome
measure for this research.
RCT to develop ongoing outcome data about urinary management in people with MS and
investigate the effect of urodynamics studies.
The RCT comparing the two treatment strategies is well underway. To date, 19 patients have
been randomised and over 100 patients have been treated by the Unit. Having established the
staff, clinic, urodynamics and other facilities as well as the links with people who support
people with MS, the recruitment rate has accelerated.
Conclusions: Urinary problems in people with MS are associated with severe urogenital distress. Urinary
treatment is associated with a significant reduction in that distress as measured by all urinary
outcome measures tested. The UGDI appears to be the most responsive of the questionnaires.

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
6
None of the existing urinary questionnaires specifically evaluate the effect of intermittent self
catheterisation on urinary distress.
Determination of the effect of Urodynamic testing on urinary and neurological outcomes in
people with MS requires an RCT design. This study is well underway. Collaborative
research between Continence Nurse Advisors, Urologists, Neurologists and other health
professionals is needed to determine the effectiveness of urinary management in people with
MS. Medical treatment needs to be supplemented with education and considerable support
for people with MS and their carers. The systematic evaluation process developed for this
study will deliver long term data regarding the effectiveness of standard strategies currently
used for significant urinary problems in people with MS. RCT studies of the effect of
Urodynamic studies on MS outcome are long overdue and are expected to have a major
impact on resource management. Future studies of the Unit stemming from the studies to
date will include: studies to determine the relative financial cost of these two major
management strategies, outcome studies of new treatments and the development of an
outcome tools for measuring the impact of intermittent self catheterisation.

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
7
BACKGROUND
Prevalence studies conservatively estimate that 12,000-15,000 Australians have Multiple
Sclerosis and up to 4,000 people are registered with the MS Society in Victoria. The
literature indicates that up to 90% of people with Multiple Sclerosis have bladder
dysfunction; the prevalence increasing as MS itself deteriorates1. Many people even with
severe bladder dysfunction have not sought help. It is understood that onset of MS symptoms
occurs most often between the ages of 20 to 40 years, and that almost all people with
Multiple Sclerosis develop dysfunction of the lower urinary tract at some point. Though the
impact on quality of life of MS-induced bladder dysfunction has not been well quantified it is
clear from existing studies that the impact in some people is devastating.
There is a dearth of prospective controlled studies to support clinical strategies for patients
who have MS and significant urinary problems. The only randomised control trials for
people with MS who have urinary problems are relatively recent and involve the
administration of new medications. There are very few of these. Clinical decision making
for people with MS who have urinary problems appears to be rather ad hoc, based on
available facilities rather than on the basis of established need and effectiveness data. There
are no prospective studies which evaluate the merit of performing sophisticated urodynamics
in this patient group, though most repeated studies have involved such a test.2,3 Some
prospective studies have been performed in the spinal cord injury (SCI) patients who have
many similar problems to people with MS.4 In the SCI population there appears to be a
significant benefit from providing urinary treatment guided by a Urodynamic (or bladder
pressure) diagnosis. Even in the SCI group of patients there are few randomised control
trials.
In recent years there has been some progress in the development of urinary quality of life
tools for patients with urinary distress. To date these relatively new tools have not been used
in patients with MS. This lack of data is an obstacle to performing prospective studies in MS
populations. There are well-developed tools for the evaluation and stratification of the
neurological status of patients. However, the urinary quality of life tools have lagged behind.
The UK Neurological Disability Scale (UKNDS) is a useful tool for monitoring quality of
life in a general sense in people with an underlying neurological condition. It includes a
bladder disability score which grades severity of urinary symptoms but which lacks

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
8
specificity and detail about the nature of the urinary disorder. A well-validated urinary
specific quality of life tool is required to monitor the progress of a urinary treatment strategy.
No single quality of life measure has been validated or widely used in people with MS.
The urinary quality of life questionnaire that has been increasingly used in recent years is the
Urogenital Distress Inventory (UGDI). The UGDI-6, a validated short form of the UGDI is
included as Appendix 1A. The American Urological Association Symptom Score (AUA-SS
Appendix 1C), has been widely used as a measure of non-specific urinary distress,
particularly in male populations. Its primary use has been in men suspected of having
prostate obstructions although data does suggest it has broad applicability including to female
populations though there are no studies of its use in people with MS.
The UGDI has been validated in both its long and short forms5,6 and has been found to have
high test-retest reliability and responsiveness in 3 different sub-populations of women with
urinary incontinence.
The optimal treatment or treatment algorithm for people with significant bladder problems
due to MS is not known. Two well established treatment algorithms are provided in
Appendices 2A and 2B. Although no precise data exist detailing who uses which strategies, a
variant of Algorithm 1 appears to be used by many highly skilled Continence Nurses in the
community. This Algorithm is promoted on the US MS Society Website. Algorithm 2
(Appendix 2B) is more likely to be used if someone is referred to a specialist Urologist.
There are no comparative data regarding which strategy is more effective or more cost
effective. Systematic comparison using validated outcome measures will have major
implications for resource allocation.

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
9
OBJECTIVES
The Innovative Grant Round 2, Project 29 project objectives were to:
1.1 Demonstrate an improvement in quality of life of urinary management in people with
multiple sclerosis (MS) who have distressing urinary symptoms, urinary tract
infections and the consequences of urinary infection when provided with treatment.
1.2 Establish the necessary staff, infrastructure, systems and networks required to carry
out the study including the fluoroscopic urodynamic studies, questionnaires,
Urological and Neurological clinical care, community links for ongoing care,
administration of the clinic, investigations, database, reporting and fund raising to
effect Objective 1.1, and pursue the following further objectives:
1.3 Develop a management model for neurology and urology outpatients to improve
detection and case finding for such patients to enable patients to be encouraged to
volunteer urinary symptoms to the Neurologist or Urologist
1.4 Inform on current treatment patterns of MS patients with urinary symptoms and
whether their symptoms are being addressed and treated effectively
1.5 Commence the study to clarify whether early urodynamic evaluation influences
treatment outcome
1.6 Commence building a database evaluation of patients with MS and urinary symptoms
to facilitate future studies including novel treatments
It became apparent that there was no urinary specific quality of life tool was sufficiently
established in a population of people with MS for its use. To address this deficiency the first
phase of the study required:
1.7 Consultation with Australasian NeuroUrology experts about the choice of urinary
quality of life measures
1.8 A pilot study to assess the responsiveness and validity of the most likely contender
for primary outcome measure of urinary quality of life – the Urogenital Distress
Inventory. This in turn would provide the basis for the power study to determine
sample size required to carry out the long term RCT comparing the two management
methods.

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
10
AIMS
To test the following hypotheses:
1. UGDI is a responsive and useful questionnaire for determining urinary quality of life in
people who have MS and significant urinary difficulty
2. A significant improvement in urinary-specific quality of life is associated with Urological
treatment of MS urinary problems
3. That urinary-specific quality of life and other secondary outcome measures are improved
with interventions that are independent of sophisticated urodynamic testing
4. That effective treatment of significant urinary distress in people with MS is associated
with a reduction in urinary tract infection and the consequences of that complication

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
11
METHODOLOGY
Demonstration of Improvement in Quality of Life in People with MS and Significant
Urinary Problems –
Pilot Study and Randomised Control Trial (RCT)
Pilot Study
A pilot study was developed to
a) provide data about sample size for a definitive Randomised Control Trial (RCT)
b) provide preliminary data about the responsiveness of proposed outcome measures in
people with MS and significant urinary problems to ensure the appropriateness of
those outcome measures to broader application
c) help refine the inclusion / exclusion criteria, research forms and protocol, urodynamic
tools.
d) determine whether additional recruitment beyond standard patterns of referral would
be required to permit the definitive RCT.
In the pilot study patients were all referred to the Urologist either privately or to our Unit.
They were then offered standard Urological care, corresponding to Algorithm 2A.
The outcome measures used to evaluate this group included standardised questionnaires:
UKNDS, UGDI, IIQ, AUA symptom score. The patients were evaluated by the Neurologist
for their MS status using the Expanded Disability Status Scale (EDSS). Further evaluation of
their urinary condition involved: Baseline MSU, Voiding Chart including times and volumes
voided over three days, Residual volume estimate and Fluoroscopic Urodynamic testing
including assessment of: bladder sensation, detrusor reflex function, detrusor compliance,
presence of obstruction and its location, activity of the external urethral sphincter by direct
measurement, and indirect measurement using bladder leak point pressures. The morphology
of the bladder, vesico-ureteric junction, and urethra were determined fluoroscopically.
Where indicated, patients also underwent digital rectal examination, prostatic specific antigen
testing, renal ultrasound, abdominal leak point pressure testing, cystoscopy, and pregnancy
testing. During the pilot study we developed the repeated measures design (Table 1) to
evaluate the patients as they are offered treatment.

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
12
Table 1
Time line of patient visits and data acquisition.
Base Line
pre visit Urodynamics R/V 1/12 R/V 3/12 R/V 6/12 R/V 12/12 R/V 24/12
Plain Language
Informed consent
Patient Info
MS Status Info
Initial History
MSU
Q-Inclusion/Exclusion
Q-IPSS
Q-UKNDS Q8
Q-UGDI-6
Q-IIQ-7
Q-EDSS
Q-UKNDS
Q-PGI-I
Bladder Chart
FUDS/UDS
PVR
Adverse Reactions
Hospital Visits
LMO Visits
Incidence of UTI's
Active Non Active
This table represents the process that patients follow when in the Study. Included are
questionnaires and key clinical issues that are addressed at each visit.
Standard Urological treatment involved anticholinergic medication, intermittent self-
catheterisation, antibiotics, intra-vesical treatments and rarely urinary diversion. Treatments
typically require the expert assistance of a well-informed and skilled Registered Nurse. The
employment of a Continence Nurse Advisor enabled the development of this role which had
to that point been developed in the private system but was lacking for public patients.

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
13
Time Frame
1. Development of staff, clinical facilities for effecting studies, preliminary collaborations,
determination of research tools, development of protocol (Nov 2001-December 2002)
2. Pilot study and recruitment of patients (non-randomized) (Aug 2002-December 2002).
3. Recruitment of patients (randomized) over 2 years (2003-2004).
4. Preliminary Evaluation at 6 months
5. Long term evaluation to 36 months
6. Anticipated completion of RCT study - 2006.
Inclusion and Exclusion Criteria
After pilot testing the provisional protocol and questionnaires, the inclusion and exclusion
criteria were decided upon.
The inclusion criteria include:
• Confirmed diagnosis of MS. • The ability to comprehend the Plain Language Statement and give informed
consent • Be willing to be contacted regarding study participation • A ‘yes’ answer to any of the following 3 questions:
Do you have problems with your bladder? Do you need to rush to the toilet, go frequently, or have difficulty starting to
pass urine? Have you been incontinent in the last month?
• Have a score of 15 or more on the AUA-Symptom Score, or a score of 2 or more
on the UKNDS-Q8 Bladder Disability.
Exclusion criteria include:
• Asymptomatic on current treatment (medical or intermittent self catheterisation) • Recent urodynamic investigation
• Uncertain neurological diagnosis • Unable to understand English or comprehend questionnaires and Plain language
statement • Unable to attend clinic visits at the designated times. • Unwilling to undergo testing that requires catheterisation

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
14
• Abnormal Digital Rectal Examination (prostate cancer or BPH) • Raised PSA • Pregnancy • Any other organic bladder pathology • Urinary diversion
Setting
Patients are seen predominantly at the Royal Melbourne Hospital. Urodynamic investigation
is done either in the Radiology Department or the Unit, which has been purpose-built.
Follow-up visits are carried out in the Outpatient Department at the Royal Melbourne
Hospital where a dedicated NeuroUrology and Continence Outpatient Clinic has been
established concurrent with the General Urology Clinic. In addition Continence Nurse
Advisor provides patient education e.g. for the initiation and ongoing support for intermittent
self catheterisation. In some cases the CNA has visited the patients at home where
practicable, or has liaise with and referred to another agency such as the Royal District
Nursing Service.
The Unit has also sought to establish stronger ties with the MS Nerve Centre (formerly MS
Society) with a view to providing relevant clinical expertise to screen and assess bladder
dysfunction. This has been well received by the Centre. It is intended that the CNA
participate in the multidisciplinary assessment clinic based at Blackburn, or establish a stand-
alone clinic on site. It is the general view that the CNA would also help to streamline the
referral process, so that more complex care issues are referred to NeuroUrology and
Continence Unit, and others referred to other relevant and pre-existing services.
Recruitment and Promotion of Continence Activities for People with MS.
Initially the Research Assistant attended the MS Neurology Outpatients to improve case
detection and case finding by specifically asking patients if they had a urinary problem. Her
attendance at the clinic was augmented by the attendance of the Continence Nurse Advisor.
The number of patients recruited from this Outpatients Department and via Private referral
was not sufficient to provide sufficient power to answer the research question. Some patients
referred had already had a urodynamic diagnosis thereby excluding them from the RCT
although they were offered treatment and their outcome data were collected. Active

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
15
recruitment outside of the natural flow of consultations from the Neurologists and General
practitioners has occurred since February 2003.
Recruitment so far has been achieved by:
• Access to the large MS Research Unit database
• Direct referral to the Service/Unit from Neurologists, MS Nerve Centre, Melbourne
Metropolitan Continence Services, Urologists and Local Medical Officers (LMO’S)
• MS Clinic
• A significant effort has been made in relation to raising nurse awareness and education,
which has directly increased patient referrals to the Unit.
• An initial mailout drive to the:
M.S Nerve Centre membership
Continence Foundation of Australia (Victoria Branch) membership
M.S Nurses
Continence Clinics
Neurologists
Royal District Nursing Service
LMO’s in the Western district
Ongoing mailout to other relevant stakeholders is planned.
• Attendance at a MS consumer conference which attracts 500 people with MS and carers
Design of Randomised Control to Evaluate Two Management Models
This study uses a randomised, controlled, repeated-measures design. The two strategies
being compared by RCT are summarised in Appendices 2A and 2B.
Randomisation
Patients are randomly assigned to the two treatment groups using a balanced randomisation
schedule based upon permuted blocks was devised. The trial is blinded with respect that
patients in both groups do not know what the treatments are ahead of time, and to which
group they are allocated. All patients have a urodynamic study but the Continence Nurse
Adviser, who manages the treatment strategy of the Symptom Group, is also blinded to the
urodynamic results of those patients randomised to this group following Algorithm 1. A

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
16
strategy for ensuring both groups are randomly allocated in a random, equivalent way with
respect to neurological status and urodynamic diagnoses to severity is shown in Table 1.
Table 2 Stratification
Status MS HM High EDSS 5-9.5
LM Low EDSS 0-4.5
Urological HU High AUA-SS 20-35 LU Low AUA-SS 15-19 HM=High MS Status, LM=Low MS Status, HU=High Urology Status, LU=Low Urology Status. There are four levels of stratification: HMHU, HMLU, LMHU and LMLU. The patients in each level are randomly allocated within that level to each group. Treatment allocations are arranged such that within each stratum, equal numbers of patients are randomized to each group after every sixth allocation. Power and sample size
For the purpose of sample size calculation, the primary endpoint of this study will be the
difference between the mean within-patient change in UGDI, comparing each group (the
symptom-based treatment group and the urodynamic study-based treatment group). In other
words, it is anticipated that both groups are likely to improve with treatment, but that the
greatest improvement might be seen in those patients treated according to the results of
urodynamic study results.
UGDI scores take values ranging from 18 (most severe symptoms), to 0 (no symptoms).
UGDI scores can be expressed as a percentage of the maximum possible score. In a pilot
sample of patients with MS-related urological symptoms attending the neurourology unit at
RMH during 2003, the mean UGDI percent score was 54, and standard deviation 19. At
present there is insufficient data on within-patient variability, and we have used the sample
standard deviation as a conservative (inflated) estimate of the likely variability of within-
patient change in UGDI over time.
A within-patient change of –30% (equivalent to a mean reduction of just over 5 UGDI points,
or –1 point change on 5/6 items in the UGDI questionnaire) is likely to represent a clinically

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
17
meaningful change in symptoms for any individual patient. Less than this probably is not
clinically meaningful. For the purpose of power and sample size calculation, we have defined
a change of –30% to be the effect size.
Although the distribution of the variable UGDI is probably non-normal, for the purpose of
sample size calculation we have assumed normality.
A sample of ≥17 patients in each group will have 90% power to detect a significant effect of
the intervention, if the true difference between the mean within-patient change in UGDI,
comparing each group, is at least 30%. This assumes α = 0.05.
A comparison of groups using non-parametric tests is likely to be less powerful, and so
require a larger sample. Furthermore, some additional patients will be enrolled to allow for
patients who withdraw, or who `drop-in’ (control group patients who obtain their results).
Based upon these factors, we believe that a sample of around 25 patients in each group
should provide sufficient power for the study.
Statistical analysis
Eligible patients who have given their consent will be stratified according to their UGDI and
EDSS scores, and assigned to one of the treatment groups by stratified randomization using
permuted blocks. This will ensure that there is no substantial imbalance in terms of baseline
symptom severity within each treatment group.
Drop-ins will be analysed on an intention-to treat basis.
The primary outcome will be the change in UGDI from baseline to follow-up. The
differences in UGDI between groups will be compared using an analysis-of-covariance
model to assess the within-patient change whilst allowing for the effect of baseline score and
potential confounders such as, age, sex, and duration of illness. If the distribution of the data
is clearly non-normal, we will use non-parametric tests as appropriate, or else categorize
patients according to a threshold UGDI score.
Secondary outcome measures include: scores on other questionnaires – AUA symptom score,
IIQ, UKNDS, number of hospital admissions, and the number of episodes of febrile urinary

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
18
infection. AUA symptom score, IIQ and UKNDS will be compared using an analysis-of-
covariance model, as for the UGDI score. If clearly non-normal, the measures may be
categorized or assessed using non-parametric tests as appropriate. Numbers of hospital
admissions and urinary infections will be compared between groups using Poisson or
negative binomial regression, and expressed in terms of incidence rate ratios.

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
19
RESULTS
Pilot studies
All urinary quality of life tools (UGDI, IIQ, AUA symptom score) were found to be very
responsive to treatment in people with MS. The UGDI appears to be a highly responsive and
simple tool and appropriate as a primary outcome measure. Its short form contains domains
which evaluate voiding dysfunction, incontinence, and recurrent infections thereby broadly
serving to evaluate the spectrum of urinary problems in people with MS. We are continuing
to monitor the responsiveness of the UGDI and other urinary and MS outcome measures
throughout the study and will publish its suitability as an outcome measure for MS urinary
studies when the data are sufficiently mature. None of the outcome measures adequately
evaluate the effect of intermittent self-catheterisation on urinary quality of life. This appears
to be a significant short-coming which will be addressed by further studies. The pilot studies
were used to determine the power calculation provided above in Methodology.
The pilot studies of urinary management based on Urodynamic studies served as the template
for the Control Group. The following results are the short term data from the pilot study and
preliminary data from the RCT. Since August 2002 over 100 patients have been seen by our
service, 80% have been female. Formal recruitment activities with a number of sources have
increased the rate of recruitment.
Table 3
NUCU Patient Referral Sources May 2003
Source Total Male Female
MS Clinic RMH 32 7 25 Urology Clinic RMH 13 6 7 MS Genetic Database 11 3 8 Private Referrals 47 6 41 MS Society 10 3 7 Total 113 25 88

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
20
Referral source - MS Clinic RMH
Patients, who are assessed as having no bladder dysfunction or whose score falls below
recommended eligibility for the study, are reassessed every six months. Those patients that
have problems but do not fit the criteria of the study are offered the facilities of our service.
Table 4
Recruitment Status MS Clinic RMH May 2003
Recruitment Status Total Male Female
Interviewed 32 7 25 Eligible 10 2 8 Package Sent 10 2 7 Ineligible 22 5 7 Service 8 1 7 Pilot Study 6 2 4 RCT 0 0 0
Referral source - Urology Clinic, RMH
Table 5
Recruitment Status Urology Clinic, RMH, May 2003
Recruitment Status Total Male Female
Referrals 13 6 7 Service 12 6 6 Information Sent 0 0 0 Pilot Study 0 0 0 Study RCT 1 0 2

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
21
Referral source - MS Genetic Data Base The MS Clinical and Research Unit, Neurology Department, at the RMH, hold this database
Table 6
Recruitment Status MS Genetic Data Base May 2003
Recruitment Status Total Male Female February Selection
Initial Selection 38 13 25 Information Sent 14 6 8 Replied 11 3 8 Study RCT 11 3 8
Selection May
Initial Selection 16 3 13
Referral source - Private Referrals
Table 7
Recruitment Status Private Referrals May 2003
Recruitment Status Total Male Female
Referrals 47 6 41 Service 39 6 33 Information Sent 8 0 8 Pilot Study 3 0 3 Not Interested 1 0 1 Study RCT 4 0 4
Referral source - MS Nerve Centre
Table 8
Recruitment Status MS Society May 2003
Recruitment Status Total Male Female
Referrals 10 3 7 Service 3 1 2 Information Sent 6 2 4 Pilot Study 1 0 1 Study RCT 0 0 0

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
22
RANDOMISATION
Table 9
Stratification Patients May 2003
Strata Total Male Female
1 HMHU 4 1 3 2 HMLU 1 0 1 3 LMHU 7 1 6 4 LMLU 7 2 5
HM=High MS Status, LM=Low MS Status, HU=High Urology Status, LU=Low Urology Status. There are four levels of stratification: HMHU, HMLU, LMHU and LMLU. The patients in each level are randomly allocated within that level to each group. Treatment allocations are arranged such that within each stratum, equal numbers of patients are randomized to each group after every sixth allocation.
Table 10
Stratification and Randomisation of Patients May 2003
Recruitment Status Total Male Female
Patients Randomized 19 4 15 Control Group 9 1 8 Trial Group 10 3 7
DATA EVALUATION FOR RANDOMISED CONTROL TRIAL
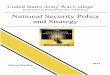
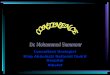
Demonstrate an improvement in quality of life of urinary management in people with MS who have distressing urinary symptoms, urinary tract infections and the consequences of urinary infection This preliminary data in Table 11 and the following graphs indicate a trend toward a decrease
in urinary symptoms and improved quality of life in patients seen by the Unit, particularly
those patients with MS. The UGDI-6, IIQ-7, AUA-SS and the urological quality of life
question have been represented.

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
23
Table 11
Percentage Change From Baseline Measurements in MS Patients May 2003
Measure 3 Months 6 Months
UGDI-6 -48 -77 IIQ-7 -30 -74 AUA-SS -53 -61 Urol. QoL -20 -20
Fig. 1 Fig. 2
01234567
Patient Visit
MS PatientsGeneral Patients
Uro
logi
cal
Qua
lity
of L
ife
Pre Treat 1 Mon 6 Mon3 Mon
0
10
20
30
Patient Visit
MS PatientsGeneral Patients
AU
A-S
S
Pre Treat 1 Mon 6 Mon3 Mon

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
24
Fig. 3
Fig. 4
1.1 Establish the necessary infrastructure, systems and networks required to provide a service
During the past year the renovation of the Unit has been completed and has resulted in a
certificated radiation-protected large room fitted to enable fluoroscopic urodynamic
studies and office space. The design has been in keeping with standards for the
disabled, including a suitably enlarged door and sufficient space within the room for
wheelchair access. An application for hoist facilities to be placed in the room has also
been processed. Recently, an adjacent office has also been renovated to accommodate
0
20
40
60
80
100
Patient Visit
MS PatientsGeneral Patients
IIQ-7
%
Pre Treat 1 Mon 6 Mon3 Mon
0
20
40
60
80
100
Patient Visit
MS PatientsGeneral Patients
UG
DI %
Pre Treat 1 Mon 6 Mon3 Mon

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
25
the Research Assistant and Urology Research fellow, thereby separating administrative
functions from clinical and client educational activities. Education of people with MS
appears to play a major role in the satisfaction that is apparent with the service and
research program.
The Unit has now established itself as a service within the hospital, and
communications with relevant departments are streamlined. Protocols and processes
for the Service and for the Study have been established. All forms used in the research
protocol have been developed and their format standardised. A policy and procedure
manual is also being developed.
Six weekly Unit Business meetings enable clinical, administrative and process issues
for the Service and Study to be identified and worked through. Six monthly Planning
meetings facilitate individual goal-directed projects to be identified and achieved.
Quarterly Collaborative Research meetings have also been set in place and involve all
interested Study partners to work through research-related issues.
The CNA/Manager of the Unit has developed a brochure to alert GPs, the Neurologists
and people with MS and their cares of the service and the research program. We have
focussed on relevant community organisations and health professionals, and cemented
ongoing relations with significant groups such as the MS Nurses, Continence Nurse
Advisors and Continence Clinics, and MS Nerve Centre. Educational Sessions related
to the service and study have been given to the MS Nurses Special Interest Group, the
Nurses for Continence Special Interest Group, the Urological Nurses Special Interest
Group, a number of rural groups of Continence Nurse Advisors.
1.2 Develop a management model for neurology and urology outpatients to improve detection and case finding for such patients to enable patients to be encouraged to volunteer urinary symptoms to the Neurologist or Neurologist To improve case finding and detection of people at RMH with MS and significant
urinary problems, we discussed strategies with the MS specialist Neurologists at the
RMH, Dr John King, Assoc. Professor Trevor Kilpatrick, Dr Helmut Butzkueven and
their research Fellows, Drs Tubridy and Marriott. It was decided that recruitment
would best be done from the rooms and through their dedicated MS outpatients.
Initially Mrs. Kathy Myles, Research Assistant or Mrs. Louise Kurczycki Continence

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
26
Nurse Advisor and Unit Manager attended the MS outpatients to interview any patients
identified by the Neurologists to have urinary problem. The accrual rate from this
source and private referral was relatively low. Once the original patient list is covered,
the intake of new patients is small and irregular. Currently Josephine Baker and John
Carey, MS Research Nurses, are involved in the recruitment process from the MS
clinics. They screen patients with MS to see if they have significant urinary problems.
This has resulted in a more effective and time-efficient process.
In addition, there is a monthly multidisciplinary clinic held at RMH for MS patients.
This involves the assessment of MS patients by a Neurologist, Community Nurse and
Physiotherapist both from MS Nerve Centre, and Louise Kurczycki the Unit Continence
Nurse Advisor. A case discussion follows where information is shared and the team
recommends management directives. This has been instrumental in strengthening
relationships between the Neurologists, MS Nerve Centre and the Unit.
1.3 Inform on current treatment patterns of MS patients with urinary symptoms and
whether their symptoms are being addressed and treated effectively
Both medical and nursing staff in the Unit have already begun to formally inform
colleagues about treatment protocols. Lectures and Seminars given by the Unit’s staff
to professional groups include:
Dr Helen O’Connell:
Regular NeuroUrology and Continence tutorials to final year medical students
at Royal Melbourne Hospital Lecture to Melbourne Geriatricians updating on NeuroUrology and Continence
treatments Urodynamic workshops in Melbourne and Sydney Pelvic Floor Dysfunction workshop in Melbourne GP lectures on NeuroUrology and Continence
Dr Ramin Samali:
Lecture on Voiding Dysfunction to Physiotherapy students at Melbourne
University Regular Urological tutorials to final year medical students at Royal Melbourne
Hospital

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
27
Ms. Louise Kurczycki provided lectures on our Unit and general continence sessions to:
Council Nursing Practice at RMH
MS Nurses at MS Nerve Centre
6 Continence Education Sessions in a Comprehensive Package at Melbourne
Extended Care and Rehabilitation Service (MECRS),
Nursing For Continence (rural) at Drouin
Victorian Urological Nurses Society and Nurses For Continence Meeting at
RMH
Lecture at the Professional Nursing Forum at the RMH
1.4 Initiate the initial phase of the study
The initial phase of the study to clarify whether early urodynamic evaluation influences
a treatment outcome began in February 2003 with the randomisation of the first batch
of eligible patients. Recruitment strategies have been set in place so that the maximum
number of eligible patients will use the Unit’s facilities.
1.5 Establish a database of people with multiple sclerosis and urinary symptoms
Close association with the Study’s biostatistician, Dr Lachlan Macgregor, has helped to
establish a database with the details of all patients who have used our service so far.
This incorporates information with respect to procedures, questionnaires and other
qualitative data for retrospective analysis and to facilitate future studies including novel
treatment.
There is a dearth of research on quality of life and intermittent catheterisation. The majority
of patients seen in our Unit require intermittent catheterisation in conjunction with anti-
cholinergic medications. Review of the literature has not identified any research tool which
addresses this important aspect of urinary management in people with neurological disease or
dysfunction. It is important to develop a suitable tool as our early research findings indicate
this management strategy has an important impact but also is associated with a number of
difficulties. Many of these difficulties appear to be surmountable with education and ongoing
support from nursing, medical staff and particularly carers. At this point in time it appears
impossible to predict who will be able to overcome the obstacles encountered in learning
intermittent self-catheterisation. Our experience indicates that limited dexterity, recurrent
infection, age do not appear to be obstacles to success. Cognitive function and limited

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
28
mobility appear to be the most important predictors of failure. The other shortcoming of
existing outcome measures is omission of questions relating to urinary diversion be that by
catheter drainage or stoma.
We have refined the protocols for urinary management based on urodynamic studies and
management based on the treatment of presenting problems. The early findings of this study
show an improvement with a treatment strategy based on Urodynamic findings. The
treatments have included anticholinergic medication supplemented by alpha-blockade and
low dose tri-cyclic anti-depressant medication. Intermittent self-catheterisation has been
associated with a reduction in febrile urinary infection in several patients including those
previously on constant antibiotics prior to the strategy being introduced. Some patients have
required urinary diversion. This appears to be of greatest importance when transferring from
bed to commode requires assistance. To date, patients requiring urinary diversion have been
excluded from the RCT.
The management of urinary problems in people with MS appears to respond to oral or intra-
vesical medication, intermittent catheterisation supplemented sometime with prophylactic
antibiotics. The extent to which education and support of these patients is required cannot be
under-estimated. Thus it appears that medical input alone is insufficient to implement
management. Specialist nursing is necessary and provides the education and ongoing support
for carers to enable some patients to live independently at home who would otherwise require
nursing home support. We will be researching further the impact on independence of
adequate education and support. This support will be effected by the team at RMH in
association with community based resources, RDNS, MS Society and other links that become
established.

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
29
CONCLUSION
Under this Innovative Grant from the National Continence Management Strategy, the
NeuroUrology and Continence Unit was established in March 2002 at the Royal Melbourne
Hospital (RMH). The Grant has enabled the Unit to develop a model of service to meet the
needs of patients whose urological problems have a neurological basis, and to embark on a
study which investigates two accepted and different treatment regimens for significant
bladder problems in patients with MS. Much of the effort thus far has centered on
establishing the necessary infrastructure, systems and networks required to provide a service
and initiate the research project. The Unit has created a comprehensive database and is now
fully operational.
The Unit has strengthened many collegial networks. The Unit currently interfaces with the
service at Melbourne Extended Care and Rehabilitation Service (MECRS), and this
collaboration is increasing between medical and nursing personnel. Other collaborations
within the RMH and key external organisations and a diverse range of health professionals
such as the MS Nerve Centre (formerly MS Society), rural and metropolitan Continence
Services, Neurologists, General Practitioners and the broader community, coupled with a
robust promotional drive which began in January 2003, have enabled the Unit to provide a
valuable multidisciplinary and holistic service to many patients and also commence the initial
phase of the research study after carrying out a pilot study. The collaborative input of
Neurologists and other professionals involved in the care of people with MS has been critical
to the development of this Unit and its service.
The pilot study revealed a significant decrease in Urogenital Distress associated with the
treatment of MS related urinary problems. This was associated with reduced impact of
incontinence (improved continence) and an improvement in global urinary quality of life. To
date the UGDI appears to be a highly responsive measure of urinary distress in people with
MS. We are currently preparing these findings for publication.
Randomisation of eligible patients began in February 2003. Early evaluation of data so far,
demonstrates promising trends in relation to improved symptom management and improved
quality of life for the general and the MS patients. However, the true impact of data in
patients with multiple sclerosis and urinary symptoms, who are participating in our study, is
dependent on the full time frame allowed in the study. The recruitment of patients for the

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
30
study will continue for at least 2 years (2003-2004) and each patient will be followed under
the study protocol for at least two years.
The model of service developed through this Grant is unique to Australia and endeavours to
provide a state-of-the-art service which benchmarks clinical care for people who have
complex neurological, urological and continence needs. Nursing and medical staff of the Unit
have been invited by many relevant interest groups to provide education in the field of
NeuroUrology and reducing severe urinary distress. Other metropolitan and rural continence
clinics have also expressed interest in replicating the algorithms used in this research.
Further education of health workers especially interested Registered Nurses is anticipated.
The Unit provides an excellent training opportunity for Urologists and Neurologist and a
Fellowship program for advanced trainees in Urology has been established. Further links
with Urogynaecology, Colorectal surgery as well as fostering the existing link with
Gerontology Continence is expected.
Urological management does improve urinary quality of life in people with MS. The extent
to which this depends upon a Urodynamic diagnosis as distinct from careful clinical
management supported by high quality education will be determined over the course of the
study. The people with MS most likely to benefit from sophisticated Urodynamic studies
will become apparent. Further studies are proposed to determine the costs of the treatment
options available for people with significant urinary distress who have MS.

National Continence Management Strategy
Department of Health and Aged Care - Innovative Grant Second Round No. 29
31
REFERENCES
1. Ozyurt, C., et al (2000) Voiding dysfunction in multiple sclerosis. Braz J Neurol, 26 (3), pp.315-320.
2. McGuire, E. J. & Savastano, J. A. (1984) Urodynamic findings and long-term
outcome management of patients with multiple sclerosis-induced lower urinary tract dysfunction. J Urol, 132 (Oct), pp.713-715.
3. Sirls, L. T., et al (1994) Role of limited evaluation and aggressive medical
management in multiple sclerosis: A review of 113 patients. J Urol, 151 (April), pp.946-950.
4. McGuire, E. J., et al (1991) A pressure management system for the neurogenic
bladder after spinal cord injury. Neurourol Urodynamics, 10, pp.223-230.
5. Hagen, S., et al (2002) Test-retest reliability, validity, and sensitivity to change of the
Urogenital Distress Inventory and the Incontinence Impact Questionnaire. Neurourol
Urodynamics, 21, pp.534-539.
6. Uebersax, J. S., et al (1995) Short forms to assess life quality and symptom distress
for urinary incontinence in women: The Incontinence Impact Questionnaire and the
Urogenital Distress Inventory. Neurourol Urodynamics, 14, pp.131-139.
7. Kelleher, C. J., et al (1997) A new questionnaire to assess the quality of life of urinary
incontinent women. Br J Obstet Gynaecol, 104 (12) Dec, pp.1374-1379.