Embed Size (px)
Citation preview

CASE REPORT
Multiple hematogenous metastasis after curative surgeryin a patient with pT1a-LPM pN0 primary malignant melanomaof the esophagus
Tomoyuki Okumura • Yutaka Shimada • Shin Ishizawa •
Isaya Hashimoto • Tomoko Watanabe • Koshi Matsui •
Isaku Yoshioka • Takuya Nagata • Kazuhiro Tsukada
Received: 10 January 2013 / Accepted: 11 March 2013 / Published online: 3 April 2013
� The Japan Esophageal Society and Springer Japan 2013
Abstract Primary malignant melanoma of the esopha-
gus (PMME) is a rare disease. Here, we describe a case of
PMME that was identified at a very early stage. A
65-year-old man underwent upper gastrointestinal endos-
copy and was found to have a pigmented small nodule in
the lower esophagus. A biopsy was taken and diagnosed
as malignant melanoma, so the patient then received
radical esophagectomy. Histopathological examination
showed atypical cell infiltrate in the lamina propria
mucosae without lymph-node metastasis. The patient was
followed up without adjuvant chemotherapy. Multiple
liver and lung metastases were found at 19 months after
surgery, and the patient received DAV-feron (DTIC/
ACNU/VCR/IFN-b) therapy. However, the tumors pro-
gressed and the patient died of the disease at 27 months
after surgery. More detailed surveys after surgery with
diagnostic imaging and tumor markers are recommended.
Adjuvant chemotherapy is worth considering, even in
patients with early-stage PMME.
Keywords Early-stage primary malignant melanoma of
the esophagus � Melanocytosis � Hematogenous
metastasis
Introduction
Primary malignant melanoma of the esophagus (PMME) is
a rare disease representing 0.1–0.5 % of all primary
esophageal neoplasms [1]. It is a very aggressive disease
with high metastatic potential, and the prognosis is very
poor. Because most of patients with PMME are diagnosed
at an advanced stage, little is known about the malignant
features of PMME in its early stages. In this report, we
describe a case of PMME in which the depth of the tumor
in the lamina propria mucosae was limited. The patient
underwent radical esophagectomy and no lymph-node
metastasis was seen, but multiple hematogenous metastases
were detected after surgery.
Case report
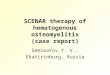
In December 2009, a 65-year-old Japanese man without
any symptoms underwent upper gastrointestinal (GI)
endoscopy during a periodic medical checkup and was
found to have a pigmented small nodule in the lower tho-
racic esophagus. Histological examination of biopsy sam-
ples confirmed the diagnosis of malignant melanoma, and
the patient was subsequently referred to our hospital in
January 2010. The patient had a medical history of distal
gastrectomy with Billroth 1 reconstruction due to gastric
cancer at the age of 41. He received upper GI endoscopy
annually and no lesion was detected at the previous
checkup, which was performed in November 2008
S. Ishizawa previously worked for the Department of Pathology,
Graduate School of Medicine and Pharmaceutical Sciences,
University of Toyama.
T. Okumura (&) � Y. Shimada � I. Hashimoto � T. Watanabe �K. Matsui � I. Yoshioka � T. Nagata � K. Tsukada
Department of Surgery and Science, Graduate School
of Medicine and Pharmaceutical Sciences, University
of Toyama, Sugitani 2630, Toyama City 930-0194, Japan
e-mail: [email protected]
S. Ishizawa
Department of Pathology,
Toyama Prefectural Central Hospital, Toyama City, Japan
123
Esophagus (2013) 10:184–191
DOI 10.1007/s10388-013-0373-9

(Fig. 1a, b). The patient had a smoking history of 24 packs
per year until he received the gastrectomy. Both of his
parents died of gastric cancer, and his elder brother died of
colon cancer. Physical examination was normal without
any suspicious pigmented skin lesions. The results of lab-
oratory tests, including tumor markers such as carcino-
embryonic antigen (CEA), squamous cell carcinoma-
related antigen (SCC), and neuron-specific enolase (NSE),
were all within the normal ranges.
Endoscopically, flat, pigmented mucosal lesions were
seen in the middle and lower thoracic esophagus (Fig. 2a,
b), and a small pigmented nodule surrounded by flat pig-
mentation was found in the lower thoracic esophagus
(Fig. 2b, c). Histological examination of a biopsy specimen
revealed atypical melanocytic infiltration with junctional
activity, confirming the diagnosis of malignant melanoma.
Esophagography demonstrated a small, elevated, nodular
lesion in the lower esophagus (Fig. 2d).
A computed tomograpy (CT) scan detected no tumor in
the esophagus, no lymph node swelling in the mediastinum
and abdomen, and no distant metastasis to the liver and
lungs. Positron emission tomography (PET) using F-18-
fluorodeoxyglucose (FDG) showed no abnormal accumu-
lation, even in the primary lesion.
Because the nodular lesion diagnosed as PMME was
accompanied by widely spreading flat lesions with pig-
mentation and it was difficult to differentially diagnose
melanocytosis and melanoma, endoscopic mucosal resec-
tion (EMR) was not carried out.
The patient received video-assisted thoracoscopic
esophagectomy with extensive lymph-node dissection
reconstructed with colonic interposition in February 2010.
The resected specimen showed weak, spotted pigmentation
throughout the esophagus. There were 2 flat lesions
(30 mm in diameter at the middle thoracic esophagus and
10 mm at the abdominal esophagus, respectively) with
strong pigmentation and an elevated lesion (8 mm in
diameter) with strong pigmentation (Fig. 3a). Histopa-
thological examination with whole tissue sections (Fig. 3b)
showed melanocytosis at the spotted pigmentation (lesion 1
in Fig. 3b), melanoma in situ at the 2 flat lesions (lesions 2
and 3 in Fig. 3b), and invasive melanoma at the elevated
lesion (lesion 4 in Fig. 2b).
No atypical change was seen in HE-stained sections
(Fig. 4a) of the weak, spotted pigmentation (Lesion 1 in
Fig. 2b), while Melan-A was strongly expressed in the
whole basal layer of the esophageal epithelium (Fig. 4b),
leading to a diagnosis of melanocytosis. In the flat lesions
with strong pigmentation (lesions 2 and 3 in Fig. 2b),
atypical cells infiltrated from the basal layer towards the
epithelial surface in HE-stained sections (Fig. 4c), and
immunohistochemistry revealed that the cells were positive
for Melan-A (Fig. 4d). Melan-A is recognized as an anti-
gen on melanoma cells by cytotoxic T-lymphocytes. The
antibody against Melan-A is reactive with cells and tumors
of the melanocytic lineage, and has been commonly used
as a melanocyte differentiation marker [2]. No invasion
across the basement membrane was seen, leading to a
diagnosis of melanoma in situ. According to the classifi-
cation of the Japan Esophageal Society [3, 4], the 2 lesions
of the disease were diagnosed as Mt, 30 9 3 mm, p0-IIb,
pT1a-EP, INFb, ly0, v0, pStage0, and Ae, 10 9 4 mm, p0-
IIb, pT1a-EP, INFb, ly0, v0, pStage0. In the nodular lesion
in the lower thoracic portion (lesion 4 in Fig. 2b), undif-
ferentiated round cells infiltrated into the lamina propria
mucosae with junctional activity (Fig. 3e). The depth of the
Fig. 1 Upper GI endoscopy at the previous medical checkup
performed in November 2008 showed a normal appearance without
any pigmentation or lesion in the upper-middle esophagus (a) and
lower esophagus (b)
Esophagus (2013) 10:184–191 185
123

invasion from the surface of the epithelium was 1–1.5 mm.
Immunohistochemistry revealed that the lesion was posi-
tive for Melan-A (Fig. 3f) and S100, leading to a diagnosis
of invasive melanoma. According to the classification of
the Japan Esophageal Society, the disease was diagnosed as
Lt, 8 9 3 mm, p0-Is ? IIb, pT1a-LPM, INFb, ly0, v0,
pIM0, pPM0, pDM0, pStage0.
Detailed observation revealed that the margin of the
melanoma in situ adjoined the melanocytosis (Fig. 3g) and
the margin of the invasive melanoma adjoined the mela-
noma in situ (Fig. 3h).
The patient was discharged at 26 days after surgery and
closely observed at an outpatient service without adjuvant
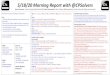
chemotherapy. A CT scan was taken at 6 months after
surgery and showed no metastatic lesions, but multiple
hematogenous metastases were found in CT scans of lung
(Fig. 5a) and liver (Fig. 5b) taken at 19 months after sur-
gery. Laboratory examination revealed high levels of NSE
(14.4 ng/ml) and 5-S-cysteinyldopa (41.8 nmol/L).
The patient received combined chemotherapy with
dacarbazine (DTIC), nimustine (ACNU), vincristine
(VCR), and interferon-b (IFN-b), i.e., DAV-feron therapy
[5, 6]. However, the tumors progressed very rapidly and the
patient died of the disease at 27 months after surgery.
Discussion
PMME is a very aggressive disease with high metastatic
potential, and the prognosis is very poor. In earlier reports,
the average overall survival in cases of PMME was
10–13 months and the 5-year survival rate was\5 % [1, 7,
Fig. 2 Upper GI endoscopy showed flat, pigmented mucosal lesions
in the middle (a) and lower (b) thoracic esophagus. A small
pigmented nodule surrounded by flat pigmentation was found in the
lower thoracic esophagus (b, c). Esophagography demonstrated a
small, elevated, nodular lesion in the lower esophagus (d)
186 Esophagus (2013) 10:184–191
123

8], largely because the disease tends to be identified at an
advanced stage. It has been reported that about 50 % of
patients present distant metastases to the liver (31 %), the
mediastinum (29 %), the lungs (18 %), and the brain
(13 %) at initial diagnosis [7]. On the other hand, a recent
report showed an improved 5-year survival rate of 37 %
[9], reflecting improvements in early endoscopic detection
[10]. This is compatible with previous reports which indi-
cated that the depth of the primary tumor, lymph node
metastasis, distant metastasis, and disease stage were pre-
dictive factors for the prognosis in cases of PMME [11,
12]. However, PMME still shows high metastatic potential,
even during its early stages, as it is reported that lymph
node metastasis is usually seen even when the depth of the
tumor is limited to the submucosal layer [13, 14].
The incidence of metastasis has not yet been established
for early-stage PMME limited to the mucosal layer
(pT1aPMME). There have been 10 previously reported
cases with pT1a PMME, as summarized in Table 1 [13,
15–22]. No lymph-node metastasis was seen in any of the
cases, and liver metastasis was seen in 1 case with a pT1a-
LPM primary tumor during repeated endoscopic mucosal
resection and ablation. In our case, the tumor was patho-
logically diagnosed as pT1a-LPM pN0M0, but liver and
lung metastases developed after curative surgery, present-
ing very high metastatic potential. Considering the rela-
tively short observiation periods in the cases summarized
in Table 1, at least 2 (18.2 %) of the 11 pT1aPMME cases
developed hematogenous metastasis.
In our case, multiple hematogenous metastases devel-
oped during the 13-month interval between the first (at
6 months) and second (at 19 months) CT scans performed
after surgery, suggesting that more detailed imaging sur-
veys should be done at shorter intervals (i.e., every
6 months), even in cases with early-stage PMME.
Surgical resection with radical lymph-node dissection is
the most common treatment for PMME [1, 7, 14, 23] and
long-term survival has occasionally been reported after
surgery [8, 24]. In the present case, the patient underwent
subtotal esophagectomy with lymph-node dissection.
Metastasis was not seen in any of the 25 dissected nodes,
and lymphovascular invasion was not observed, but the
patient died of multiple hematogenous metastasis. Because
the incidence of lymph-node metastasis in pT1a PMME is
still unclear, one proposed treatment is adjuvant chemo-
therapy with extended radical surgery [16]. The combina-
tion of radical surgery and DAV or DAV-feron therapy was
reported to be effective for PMME [6, 25–28].
In some cases, EMR has reported to be a curative
treatment [18, 19] in early-stage PMME. On the other
hand, local recurrence after EMR was also reported [20].
The combination of EMR and adjuvant chemotherapy is a
possible alternative strategy in T1a PMME without lymph-
node metastasis. However, the development of accurate
preoperative diagnostic strategies, such as endoscopic
ultrasound, is necessary.
Endoscopic biopsy was carried out in the present case to
achieve a definitive diagnosis. In malignant melanoma of
Fig. 3 Resected specimen (a) showed weak, spotted pigmentation
throughout the esophagus. There were several flat lesions with strong
pigmentation and an elevated nodular lesion with strong pigmentation
in the lower esophagus. Histopathological examination with whole
tissue sections (b) showed melanocytosis at the spotted pigmentation
(lesion 1), melanoma in situ at the 2 flat lesions (lesions 2 and 3), and
invasive melanoma at the elevated lesion (lesion 4)
Fig. 4 No atypical change was seen in HE-stained sections of lesion
1 (a), while Melan-A was strongly expressed in the whole basal layer
of the epithelium (b). In lesions 2 and 3, atypical cells infiltrated from
the basal layer towards the epithelial surface in HE-stained sections
(c). Immunohistochemistry revealed that the cells were positive for
Melan-A (d), leading to a diagnosis of melanoma in situ. In lesion 4,
undifferentiated round cells infiltrated into the lamina propria
mucosae with junctional activity in HE-stained sections (e). The
depth of the invasion from the surface of the epithelium was
1–1.5 mm. Immunohistochemistry revealed that the lesion was
positive for Melan-A (f), leading to a diagnosis of invasive
melanoma. The margin of the melanoma in situ adjoined the
melanocytosis (g) and the margin of the invasive melanoma adjoined
the melanoma in situ (h)
c
Esophagus (2013) 10:184–191 187
123

188 Esophagus (2013) 10:184–191
123

the skin, biopsy is generally considered to be contraindi-
cated in order to avoid triggering hematogenous metastasis
[29]. However, it is difficult to perform radical esopha-
gectomy without a definitive diagnosis. Especially in early-
stage cases, a pathological diagnosis is necessary because
performing a differential diagnosis between melanocytosis
and melanoma in situ by endoscopy is difficult [12]. In the
pT1aPMME cases summarized in Table 1, hematogenous
metastasis was not established in 9 of the 11 cases, even
though all 11 patients underwent biopsy prior to curative
treatment.
In the present case, a malignant melanoma and 2 mel-
anoma in situ lesions were accompanied by widely
spreading melanocytosis. This is compatible with a previ-
ous report that 25–30 % of PMMEs are accompanied by
melanocytosis [30]. More detailed observations revealed
that the margin of the melanoma in situ adjoined the
melanocytosis, and the margin of the invasive melanoma
adjoined the melanoma in situ, suggesting a possible
melanocytosis–melanoma sequence in this case. A case has
been reported in which a melanoma arose from a previ-
ously detected melanotic lesion [31]. In addition, in the
present case, all of the mixed lesions developed within
1 year, indicating very rapid progression after initiation.
Although the patient did not suffer from reflux esophagitis,
it is possible that long-term stimulation by reflux after
gastrectomy influenced the development of melanocytosis
and melanoma.
Several genes, such as MC1R and CDKN2A, are repor-
ted to be involved in the development of malignant mela-
noma of the skin, but their role in PMME is unknown.
Exposure to ultraviolet (UV) radiation is widely recognized
as a carcinogen for malignant melanoma of the skin. UVB
has been shown to enhance cyclooxygenase 2 (COX-2)
protein levels in skin, indicating its role in the development
of UVB-related malignant melanoma [32, 33]. On the other
hand, COX-2 has been reported to play a role in the
development of reflux esophagitis as well as esophageal
carcinoma. Reports have also shown a relationship between
bile reflux and induced COX-2 expression [34]. Taken
together, it is possible that long-term stimulation by reflux
after gastrectomy affected the development of melanocy-
tosis through COX-2 induction, and then additional
molecular events accelerated the transformation to malig-
nant melanoma. Further investigations of the biological
process involved in the development of melanocytosis and
melanoma in esophagus may provide us with a better
understanding of and treatment for the disease.
In conclusion, the present case demonstrated very rapid
development and progression of PMME from normal
mucosa to melanocytosis, to malignant melanoma, and
then to multiple hematogenous micrometastases, all within
1 year. Based on the extremely malignant characteristics of
PMME, we suggest that melanocytosis of the esophagus
should be considered a high-risk precancerous lesion.
Although the overall outcomes of therapies for this extre-
mely rare disease are unclear, radical esophagectomy with
adjuvant chemotherapy is worth considering, even for
patients with early-stage PMME. In addition, more detailed
surveys after surgery, utilizing diagnostic imaging and
tumor markers such as NSE and 5-S-cysteinyldopa, are
strongly recommended.
Fig. 5 Multiple hematogenous metastases were found in CT scans of
lung (a) and liver (b) at 19 months after surgery
Esophagus (2013) 10:184–191 189
123

Conflict of interest The authors declare that they have no conflict
of interest.
References
1. Sabanthan S, Eng J, Pradhan GN. Primary malignant melanoma
of the esophagus. Am J Gastroenterol. 1989;12:1475–81.
2. Jungbluth AA. Serological reagents for the immunohistochemical
analysis of melanoma metastases in sentinel lymph nodes. Semin
Diagn Pathol. 2008;25(2):120–5.
3. Japan Esophageal Society. Japanese classification of esophageal
cancer, 10th edn: part I. Esophagus. 2009;6:1–25.
4. Japan Esophageal Society. Japanese classification of esophageal
cancer, tenth edition: parts II and III. Esophagus. 2009;6:71–94.
5. Yamashita Y, Hirai T, Mukaida H, Kawano K, Toge T, Niimoto
M, et al. Primary malignant melanoma of the esophagus—a case
report. Jpn J Surg. 1989;19:498–501.
6. Kawada K, Kawano T, Nagai K, Nishikage T, Nakajima Y,
Tokairin Y, et al. Local injection of interferon beta in malignant
melanoma of the esophagus as adjuvant of systemic pre- and
postoperative DAV chemotherapy: case report with 7 years of
long-term survival. Gastrointest Endosc. 2007;66:408–10.
7. Calhkiadakis G, Wihlm JM, Morand G, Weill-Bousson M, Witz
JP. Primary malignant melanoma of the esophagus. Ann Thorac
Surg. 1985;39:472–5.
8. Joob AW, Haines GK, Kies MS, Shields TW. Primary malignant
melanoma of the esophagus. Ann Thorac Surg. 1995;60(1):
217–22.
9. Volpin F, Sauvanet A, Couvelard A, Belghiti J. Primary malig-
nant melanoma of the esophagus: a case report and review of the
literature. Dis Esophagus. 2002;15:244–9.
10. Miyatani H, Yoshida Y, Ushimaru S, Sagihara N, Yamada S.
Slow growing flat-type primary malignant melanoma of the
esophagus treated with cap-assisted EMR. Dig Endosc.
2009;21(4):255–7.
11. Cheung MC, Perez EA, Molina MA, Jin X, Gutierrez JC,
Franceschi D, et al. Defining the role of surgery for primary
gastrointestinal tract melanoma. J Gastrointest Surg. 2008;12(4):
731–8.
12. Iwanuma Y, Tomita N, Amano T, Isayama F, Tsurumaru M,
Hayashi T, et al. Current status of primary malignant melanoma
of the esophagus: clinical features, pathology, management and
prognosis. J Gastroenterol. 2012;47(1):21–8.
13. Suzuki H, Nakanishi Y, Taniguchi H, Shimoda T, Yamaguchi H,
Igaki H, et al. Two cases of early-stage esophageal malignant
melanoma with long-term survival. Pathol Int. 2008;58(7):432–5.
14. Ludwig ME, Shaw R, de Suto-Nagy G. Primary malignant mel-
anoma of the esophagus. Cancer. 1981;48(11):2528–34.
15. Kido T, Morishima H, Nakahara M, Nakao K, Tanimura H, Ni-
shimura R, Tsujimoto M. Early stage primary malignant mela-
noma of the esophagus. Gastrointest Endosc. 2000;51(1):90–1.
Table 1 A summary of the reported cases of early-stage primary malignant melanoma of the esophagus
No Author Age
(years)
Sex TNM
stage
Japanese
classification
Biopsy Treatment Survival
(months)
Outcome
1 Kido [15] 60 M T1N0M0 pT1a-MM N0M0
Stage0
? Surgery 1 Disease-free
Stage1
2 Mikami
[16]
41 F T1N0M0 pT1a N0M0
Stage0
? Surgery ? chemotherapy 31 Disease-free
Stage1
3 Hara [17] 52 M TisN0M0 pT1a-EP N0M0
Stage0
? Surgery 1 Disease-free
Stage0
4 Kimura
[18]
73 M T1N0M0 pT1a-LPM
N0M0 Stage0
? EMR 15 Disease-free
Stage1
5 Suzuki
[13]
62 M TisN0M0 pT1a-EP N0M0
Stage0
? Surgery 33 Disease-free
Stage0
6 Suzuki
[13]
67 M T1N0M0 pT1a-LPM
N0M0 Stage0
? Surgery 53 Disease-free
Stage1
7 Miyatani
[19]
64 M T1N0M0 pT1a-LPM
N0M0 Stage0
? EMR 20 Disease-free
Stage1
8 Morita
[20]
75 M T1N0M0 pT1a-LPM
N0M0 Stage0
? EMR 9 6,
tumor ablation 9 7,
chemotherapy,
TACE
84 Survive with liver
metastasisStage1
9 Minami
[21]
72 M TisN0M0 pT1a-EP N0M0
Stage0
? Surgery 25 Disease-free
Stage0
10 Hikage
[22]
61 M T1N0M0 pT1a-MM N0
M0 pStage0
? Surgery 17 Disease-free
Stage1
11 Our case 65 M T1N0M0 pT1a-LPM
N0M0 Stage0
? Surgery ? chemotherapy 27 Death due to liver and
lung metastasesStage1
190 Esophagus (2013) 10:184–191
123

16. Mikami T, Fukuda S, Shimoyama T, Yamagata R, Nishiya D,
Sasaki Y, et al. A case of early-stage primary malignant mela-
noma of the esophagus. Gastrointest Endosc. 2001;53(3):365–7.
17. Hara S, Noguchi M, Sugiyama K, Yamaguch M, Unakami M,
Imatani A, et al. A case of primary malignant melanoma of the
esophagus in situ. Gastroenterol Endosc. 2003;45:935–9.
18. Kimura H, Kato H, Sohda M, Nakajima M, Fukai Y, Miyazaki T,
et al. Flat-type primary malignant melanoma of the esophagus
treated by EMR: case report. Gastrointest Endosc.
2005;61(6):787–9.
19. Miyatani H, Yoshida Y, Ushimaru S, Sagihara N, Yamada S.
Slow growing flat-type primary malignant melanoma of the
esophagus treated with cap-assisted EMR. Dig Endosc.
2009;21(4):255–7.
20. Morita S, Miyamoto S, Matsumoto S, Muto M, Chiba T. Multiple
early stage malignant melanoma of the esophagus with long
follow-up period after endoscopic treatment: report of a case.
Esophagus. 2009;6:249–52.
21. Minami H, Inoue H, Satodate H, Hamatani S, Shin-Ei K. A case
of primary malignant melanoma in situ in the esophagus. Gas-
trointest Endosc. 2011;73(4):814–5.
22. Hikage M, Kamei T, Fujishima F, Miyata G, Onodera K, Ichi-
kawa H, et al. Early stage primary malignant melanoma of the
esophagus detected simultaneously with esophageal squamous
cell carcinoma. Esophagus. 2012;9:33–8.
23. Adili F, Monig SP. Surgical therapy of primary malignant mel-
anoma of the esophagus. Ann Thorac Surg. 1997;63(5):1461–3.
24. Itami A, Makino T, Shimada Y, Imamura M. A case of primary
malignant melanoma of the esophagus with long term survival.
Esophagus. 2004;1:135–7.
25. Naomoto Y, Perdomo JA, Kamikawa Y, Haisa M, Yamatsuji T,
Kenzo A, et al. Primary malignant melanoma of the esophagus:
report of a case successfully treated with pre- and post-operative
adjuvant hormone chemotherapy. Jpn J Clin Oncol.
1998;28:758–91.
26. Matsutani T, Onda M, Miyashita M, Hagiwara N, Akiya Y,
Takubo K, et al. Primary malignant melanoma of the esophagus
treated by esophagectomy and systemic chemotherapy. Dis
Esophagus. 2001;14:241–4.
27. Sunagawa H, Nishimaki T, Shimoji H, Kuninaka K, Nakachi N,
Kinjyou F. Primary malignant melanoma of the esophagus suc-
cessfully treated by an esophagectomy followed by systemic
chemotherapy. Esophagus. 2005;2:33–7.
28. Larkin J, Gore M. Malignant melanoma (metastatic). Clin Evid
(Online). 2008;Aug 22;pii:1718.
29. Shapiro RL. Surgical approaches to malignant melanoma. Prac-
tical guidelines. Dermatol Clin. 2002;20(4):681–99.
30. Lohmann CM, Hwu WJ, Iversen K, Jungbluth AA, Busam KJ.
Primary malignant melanoma of the oesophagus: a clinical and
pathological study with emphasis on the immunophenotype of the
tumours for melanocyte differentiation markers and cancer/testis
antigens. Melanoma Res. 2003;13(6):595–601.
31. Oshiro T, Shimoji H, Matsuura F, Uchima N, Kinjo F, Nakayama
T, Nishimaki T. Primary malignant melanoma of the esophagus
arising from a melanotic lesion: report of a case. Surg Today.
2007;37(8):671–5.
32. Denkert C, Kobel M, Berger S, Siegert A, Leclere A, Trefzer U,
Hauptmann S. Expression of cyclooxygenase 2 in human
malignant melanoma. Cancer Res. 2001;61(1):303–8.
33. Kim JY, Shin JY, Kim MR, Hann SK, Oh SH. siRNA-mediated
knock-down of COX-2 in melanocytes suppresses melanogene-
sis. Exp Dermatol. 2012;21(6):420–5.
34. Song S, Guha S, Liu K, Buttar NS, Bresalier RS. COX-2
induction by unconjugated bile acids involves reactive oxygen
species-mediated signalling pathways in Barrett’s oesophagus
and oesophageal adenocarcinoma. Gut. 2007;56(11):1512–21.
Esophagus (2013) 10:184–191 191
123