Embed Size (px)
Citation preview

Journal of Substance Abuse Treatment 39 (2010) 399–407
Brief article
Motivation for reducing substance use among minority adolescents:Targets for intervention
Ashley Austin, (Ph.D.)a,⁎, Michelle Hospital, (Ph.D.)b,Eric F. Wagner, (Ph.D.)b, Staci Leon Morris, (Psy.D.)b
aSchool of Social Work, Barry University, Miami, FL 33161, USAbCommunity-Based Intervention Research Group, Florida International University, Miami, FL 33199, USA
Received 17 September 2009; received in revised form 19 July 2010; accepted 22 July 2010
Abstract
Motivation to change substance use is considered to be one of the most important predictors of client readiness for alcohol and other drugtreatment and ability to benefit from treatment. Enhancing motivation to change substance use is an important emphasis of many substanceuse intervention programs. The specific factors predicting motivation to change substance use remain largely unidentified and poorlyunderstood, particularly among racial/ethnic minority youth. This study examines the influence of adolescent and parental factors onmotivation to change substance use among 310 alcohol-using and/or drug-using racial/ethnic minority adolescent males. The analytic planinvolved the use of structural equation modeling. Adolescents' motivation to change substance use was influenced directly and indirectly byparental factors, as well as by adolescent substance use severity and externalizing disorders. Findings have implications for treatment withracial/ethnic minority youth, as parental factors may be exceptionally useful targets for interventions aimed at enhancing motivation to reducesubstance use among these at-risk youth. © 2010 Elsevier Inc. All rights reserved.
Keywords: Substance use; Motivation; Adolescents; Ethnic minority; Intervention
1. Introduction
The role of client motivation has emerged as anincreasingly important topic for substance abuse treatmentproviders and researchers. Research with adults hasestablished that higher motivation for change predicts greatertreatment engagement and retention (De Leon & Jainchill,1986; De Leon, Melnick, & Hawke, 2000; Hiller, Knight,Leukefeld, & Simspson, 2002) and better treatment out-comes (De Leon, Melnick, & Kressel, 1997; De Leon,Melnick, Kressel, & Jainchill, 1994). The importance ofmotivation for treatment in predicting treatment response hasbeen demonstrated consistently across modalities, includingoutpatient methadone, outpatient drug free, and residential(Joe, Simpson, & Broome, 1998, 1999), as well as among
⁎ Corresponding author. Barry University, School of Social Work,11300 NE Second Avenue, Miami Shores, FL 33161-6695, USA. Tel.: +1305 899 3936; fax: +1 305 899 3934.
E-mail address: [email protected] (A. Austin).
0740-5472/10/$ – see front matter © 2010 Elsevier Inc. All rights reserved.doi:10.1016/j.jsat.2010.07.008
adults in both community-based (Simpson & Joe, 1993) andcriminal justice settings (Hiller et al., 2002).
Substance abuse treatment research has explored bothmotivation to change substance use and motivation to seekhelp with making substance use changes, which have beenshown to be distinct, although positively correlated,constructs (Freyer et al., 2004; Lau et al., 2010). Despitegeneral recognition that motivation to change substance useand motivation to seek treatment are discernable, substanceabuse treatment research has been plagued by definitionaland operational inconsistencies in the conceptualization ofmotivation. For example, Severtson, von Thomsen, Hedden,and Latimer (2010) examined motivation for treatmentamong substance-abusing adults at risk for HIV; however,these investigators' measure of “motivation to entertreatment” involved a six-item questionnaire composedexclusively of items measuring problem recognition (e.g.,“my drug use is more trouble than it's worth”) andmotivation to change substance use (e.g., “I am ready toquit using now”). Hogue, Dauber, and Morgenstern (2010)

400 A. Austin et al. / Journal of Substance Abuse Treatment 39 (2010) 399–407
assessed both motivation to change substance use andmotivation to seek help (i.e., “How important to you now istreatment for alcohol/drug problems?”) among substance-abusing adults and found that motivation to change itemswere significantly associated with substance use outcomes,whereas the motivation to enter treatment item was not. Insum, among adults with substance use problems, it appearsthat motivation to change and motivation to enter treatmentare different constructs, with different associations toindicators of treatment response.
Among adolescents with substance use problems, denialof addiction problems and ambivalence (if not outrightrejection) toward treatment participation are characteristic.Given their relatively brief history of substance use andnormative developmental predisposition toward challengingauthority (Wagner, 2008), it is no wonder that mostteenagers with drinking or drugging problems are notenthusiastic about entering treatment. As a result, the fewstudies that have examined motivational factors influencingadolescents' substance use outcomes have focused exclu-sively on motivation to change substance use. For example,King, Chung, and Maisto (2009) examined motivation toabstain and perceived difficulty of abstaining amongadolescents receiving treatment for marijuana problemsand found that these motivation to change constructspredicted changes in marijuana use. Additional studieswith adolescents have found that motivation for substanceuse change is associated with greater rates of treatmentretention (Fickenscher, Novins, & Beals, 2006; Melnick,De Leon, Hawke, Jainchill, & Kressel, 1997), greatertherapeutic engagement (Broome, Joe, & Simpson, 2001),and better treatment outcomes (Breda & Heflinger, 2007;Cady, Winters, Jordan, Solberg, & Stinchfield, 1996;Friedman, Granick, & Kreisher, 1994). Thus, a growingbody of evidence supports the important relation betweenadolescents' motivation to change substance use andtreatment engagement and retention. Consistent with theexisting literature, this study explored issues associatedwith motivation to change substance use (Garner, Godley,& Funk, 2008).
2. Factors influencing motivation for change
Because it is widely recognized that motivation forchange plays a critical role in treatment engagement,retention, and outcome, it is increasingly expected thatsubstance abuse treatment providers take an active role inenhancing client motivation for change (DiClemente, Garay,& Gemmell, 2008). According to DiClemente et al. (2008),motivational considerations are often viewed as critical forinitial engagement in treatment, and subsequent substanceuse changes and motivational enhancement strategies arebecoming an integral part of most outreach, detoxification,and treatment programs. Nevertheless, to date, there isrelatively little known about the factors influencing substance-
using adolescents' motivation to reduce or end their substanceuse. There is speculation that a variety of psychosocial andcontextual factors may influence adolescents' motivation forchange. For example, externalizing behavior disorders, such asconduct disorder, negatively impact treatment response andretention (Galaif, Hser, Grella, & Joshi, 2001; Kaminer, Tarter,Bukstein, & Kabene, 1992), but it is unclear whetherexternalizing disorders also influence a teen's motivation toreduce substance use behavior. Battjes, Gordon, O'Grady,Kinlock, and Carswell (2003) explored the relationshipbetween motivation (“internal recognition of the need tochange”) andmeasures of deviant behavior, including a varietyof conduct disorder symptoms, aggressive behavior, and daysof illegal activities in the prior 90 days. Only one measure,number of days engaged in illegal activities, was predictive ofmotivation to change. However, in this study, there was nomeasure of conduct disorder diagnosis available for inclusion;as such, the authors encourage research that further exploresthe potential role of conduct disorder in predicting adolescents'motivation to change (Flynn, Joe, Broome, Simpson, &Brown, 2003).
Substance use severity is another issue suspected toinfluence youths' response to treatment. Some researchsuggests that higher levels of pretreatment substance use arepredictive of poor treatment retention (Galaif et al., 2001)and outcome (Hsieh, Hoffman, & Hollister, 1998), whereasother research indicates that more severe pretreatmentsubstance use actually predicts better treatment retention(Harrison & Asche, 2001) and outcome (Jainchill, Hawke,De Leon, & Yagelka, 2000) among teens. The relationbetween substance use severity and motivation to changesubstance use is no less ambiguous. For instance, in a studyexamining motivation to change among adolescents beingtreated for an alcohol-related injury in the emergencydepartment, higher levels of drinking and drinking problemsat baseline were related to lower levels of motivation tochange substance use (Barnett, Lebeau-Craven, Wollard, etal., 2002). In contrast, studies with college students foundthat young people indicating the greatest motivation tochange substance use had higher levels of drinking (e.g., seeVik, Culbertson, & Sellers, 2000). Moreover, in a study of196 adolescents admitted to outpatient substance abusetreatment, Battjes et al. (2003) found that substance useseverity was unrelated to motivation to change. Although theinfluence of substance use severity on motivation to changesubstance use has received some research attention, therelation requires further elucidation. It is important thatpractitioners understand how pretreatment substance useexperiences may influence response to treatment and howintervention approaches, including motivational enhance-ment strategies, may be tailored to best address the specificneeds of adolescents with divergent substance use histories.
In addition to personal factors such as substance useseverity and externalizing behaviors, there is a growinginterest in the potential relation between parental factors(e.g., parental support, parental substance use involvement)

401A. Austin et al. / Journal of Substance Abuse Treatment 39 (2010) 399–407
and adolescents' motivation to change substance use.Parental substance use and a lack of parental support havelong been recognized as risk factors for the development ofsubstance use problems among teens (Baumrind, 1991;Cohen & Rice, 1997; Chassin, Curran, Hussong, & Colder,1996; Hawkins, Catalano, & Miller, 1992; Weiss &Schwarz, 1996) and have typically been measured by askingadolescents about their perceptions of parental behaviors,which are thought to be less subject to social desirabilityreporting biases than parents' reports of parent behavior. Tothis end, we conducted a comprehensive literature of recentstudies examining relations between parenting factors andadolescent substance use and found that every single studypublished since 2007 measured adolescents' perceptions ofparenting behavior (e.g., Marti, Stice, & Springer, 2010;Miller, Gorman-Smith, Sullivan, Orpinas, & Simon, 2009;Mistry, McCarthy, Yancey, Lu, & Patel, 2009; Pedersen &Skardhamar, 2010; Rueger, Malecki, & Demaray, 2010;Ryan, Miller-Loessi, & Nieri, 2007). Consistent withexisting literature, this study assessed adolescents' percep-tions of parenting behavior.
Only recently have researchers begun to explore thepotential relation between familial factors and teen motiva-tion to change substance use (Broome et al., 2001). In theBroome et al. (2001) study, higher levels of social supportfrom family and friends were associated with greatertreatment motivation (readiness) to change substance use,whereas family substance use demonstrated no relation tomotivation to change. Interestingly, Barnett et al. (2002)found teen perceptions that parents will impose conse-quences for drinking were associated with greater motivationto change drinking behavior. In sum, although it seemslogical that parental factors contribute to youth motivation toreduce substance use, there is scant research addressing thenature and extent of these relationships.
Thus, motivation to change substance use has been linkedto (a) greater treatment engagement and retention and bettertreatment outcomes among both adolescent and adultsubstance users and (b) enhancing motivation to changehas become an increasingly important component of manyefficacious substance use intervention programs for bothadults and adolescents (DiClemente et al., 2008). However,the specific factors influencing adolescents' motivation tochange remain largely unidentified and poorly understood.This is particularly true for racial/ethnic minority youthbecause most studies examining adolescents' motivation tochange substance use have been conducted with primarilynon-Hispanic White samples. Hispanic/Latinos and AfricanAmericans with substance use problems consistently expe-rience greater rates of unmet treatment need (Wu, Hoven,Tiet, Kovalenko, & Wicks, 2002), an increased likelihood oftreatment dropout (Office of Applied Studies, 2000), andmore severe psychosocial, health, and legal consequencesassociated with substance use behaviors (Herd, 1994; Mulia,Ye, Greenfield, & Zemore, 2009). As such, identifying thefactors relevant to adolescents' motivation to change
substance use, particularly for racial/ethnic minority teens,represents an increasingly important research focus becausethese factors may prove to be exceptionally useful targets forinterventions aimed at improving treatment engagement,retention, and outcome for these at-risk youth.
The primary aim of this study is to address this gap in theliterature through a hypothesis-based exploration of theinfluences of adolescent substance use severity andexternalizing behaviors, parental support, and parentalsubstance use problems on motivation to change substanceuse among Hispanic/Latino and African American adoles-cents. The initial model to be tested will examinehypothesized links between parental substance use, parent-ing behavior (control and support), adolescent substanceuse and externalizing psychiatric disorders, and adoles-cents' motivation to change substance use. It was expectedthat parental substance use and parenting behavior woulddirectly influence adolescents' motivation to changesubstance use. In addition, it was expected that parentalsubstance use and parenting behavior would indirectlyinfluence adolescents' motivation to reduce substance usethrough their influence on adolescent substance use andadolescent externalizing disorders. Better understanding therole of parental factors in influencing adolescents' motiva-tion to reduce substance use can lead to interventionapproaches that more effectively and comprehensivelytarget factors associated with increasing motivation forchange and engagement in treatment.
3. Materials and methods
3.1. Procedures
This study was conducted with data culled from AlcoholTreatment Targeting Adolescents in Need (ATTAIN; PI:Wagner), a National Institute on Alcohol Abuse andAlcoholism (NIAAA)-funded randomized clinical trialexamining the efficacy of a brief motivational substanceabuse intervention for racially/ethnically diverse adolescentswith substance use problems in Miami, FL. Youth inATTAIN participated in an adolescent-specific version ofGuided Self Change (Sobell & Sobell, 1998), an evidence-based, brief (five-session) behavioral and motivationalintervention designed for use with individuals withsubstance use problems. The mean age of the sample inour study was 16.69 years (SD = 1.14). Youth werereferred to ATTAIN through the Miami-Dade County, FL,juvenile justice system; most of the youth in the sample(68%) were not court mandated and voluntarily participatedin treatment. Assessment measures for ATTAIN wereadministered to all participants in a structured interviewformat by a trained interviewer at five periods: intake,posttreatment, and 3-, 6-, and 9-month follow-ups.Analyses for this study were conducted with data collectedduring the intake assessment.

402 A. Austin et al. / Journal of Substance Abuse Treatment 39 (2010) 399–407
3.2. Measures
3.2.1. Background measuresA number of sociodemographic variables (e.g., age,
grade, race/ethnicity, nativity) were used to describe theparticipants. These data were collected utilizing a standar-dized measure that is used across all studies conductedthrough the Community Based Intervention Research Group(C-BIRG) at Florida International University.
3.2.2. Externalizing disordersThe primary diagnostic instrument used was the Brief
Michigan Composite International Diagnostic Interview(CIDI; Robins, Wing, Wittchen, & Helzer, 1988). TheCIDI is a structured interview originally developed by theWorld Health Organization for administration by layinterviewers, and it has been updated to yield Diagnosticand Statistical Manual of Mental Disorders, Fourth Edition(DSM-IV) diagnoses (for an overview, see Andrews &Peters, 1998). The CIDI has been shown to reliably andvalidly assess DSM-IV substance use disorders (Cottler et al.,1997; Hasin, van Rossem, McCloud, & Endicott, 1997),both across different cultural groups (Caetano, Mora,Schafer, & Marino 1999; Cottler et al., 1997; Horton,Compton, & Cottler, 2000) and with adolescents (Perkonigget al., 1999; Wagner, Lloyd, & Gil, 2002). The CIDI wasused to assess the past year presence of the followingdisorders: conduct disorder, oppositional defiant disorder,and attention deficit hyperactivity disorder (inattentive type,hyperactive type, and combined inattentive and hyperactivetype). From this assessment tool, a summary variable,“adolescent externalizing disorders,” which reflects the sumof the number of externalizing behavior diagnoses—conductdisorder, oppositional defiant disorder, or attention deficithyperactive disorder diagnoses, was created.
3.2.3. Substance use disordersThe CIDI, described previously, was also used to
determine whether participants met criteria for one or moreof four DSM-IV substance use disorders: (a) alcohol abuse,(b) alcohol dependence, (c) drug abuse, and (d) drugdependence. A variable was created, “adolescent substanceuse,” which categorized the four substance use disordersdiagnoses as measured by the CIDI in such a way as toreflect increasing levels of substance use (0 = no use, 1 =monosubstance use diagnosis [e.g., abuse or dependencediagnoses for only one substance], 2 = polysubstance usediagnoses [e.g., abuse or dependence diagnoses for more thanone substance]).
3.2.4. Motivation to changeThe Problem Recognition Questionnaire (PRQ) measures
drug use problem recognition and readiness to changesubstance use (i.e., action orientation) among adolescentsubstance users. The scale was developed with a combina-tion of rational and empirical procedures and demonstrated a
high degree of internal consistency (α = .91) when tested onan adolescent substance abuse treatment sample (Cady et al.,1996). Cady et al. also found that high scores on the PRQ(representing a higher level of motivation/readiness) werepredictive of decreased drug use and increased abstinence atposttreatment. To date, the PRQ is the only published stand-alone questionnaire concerning problem recognition andreadiness to change expressly developed for use withadolescent substance users. As such, it is included amongthe questionnaires recommended by NIAAA for assessingalcohol behaviors among teenagers (Allen & Wilson, 2003).
3.2.5. Family substance involvementFamily substance involvement was measured through a
series of yes or no questions about the adolescents'knowledge of parental/guardian substance use developedfor the ATTAIN study (e.g., “Do your parents/guardiansdrink alcohol/use marijuana/cocaine/other illicit drugs(asked separately)?” and “Do your parents drink or usedrugs so often it causes problems for the family?”). Asummary variable was categorized so that higher numbersreflect more problematic levels of parental use as reported bythe adolescent (0 = no use, 1 = monosubstance use [i.e.,reported parental use of only one substance—alcohol ormarijuana] nonproblematic, 2 = polysubstance use [i.e.,reported parental use of multiple substances] nonproble-matic, 3 = any substance use and problematic).
3.2.6. Parenting behaviorChildren's Report of Parent Behavior Inventory Short-
Form (CRPBI; Schaefer, 1965; Schluderman & Schluder-man, 1970) is a brief inventory of children's perceptions ofparent's behavior. Adolescents were asked to respond toitems regarding parents' behavior over the past year (e.g.,“My primary caregiver tried to control whatever I did”).CRPBI items were scored on a 5-point scale (almost never,once in a while, sometimes, a lot of the time, almost always).The version of this measure used in this study contained 39items and assessed two major dimensions (parental accep-tance/support and parental control). The subscales of theCRPBI have shown good discriminant and convergentvalidity in previous studies (e.g., Schwarz, Barton-Henry,& Pruzinsky, 1985). In this study, each of the subscales wasderived by summing and averaging the items. Cronbach'salpha indicate high levels of internal consistency for both thesupport subscale and the control subscale (α = .91 and α =.81, respectively).
3.3. Analytic plan
This study involved the investigation of complex andmultivariate relationships; therefore, the analytic planinvolved the use of structural equation modeling (SEM).The initial model tested is depicted in Fig. 1, whichrepresents hypothesized sequential causal links betweenparental substance use, parenting behavior (control and
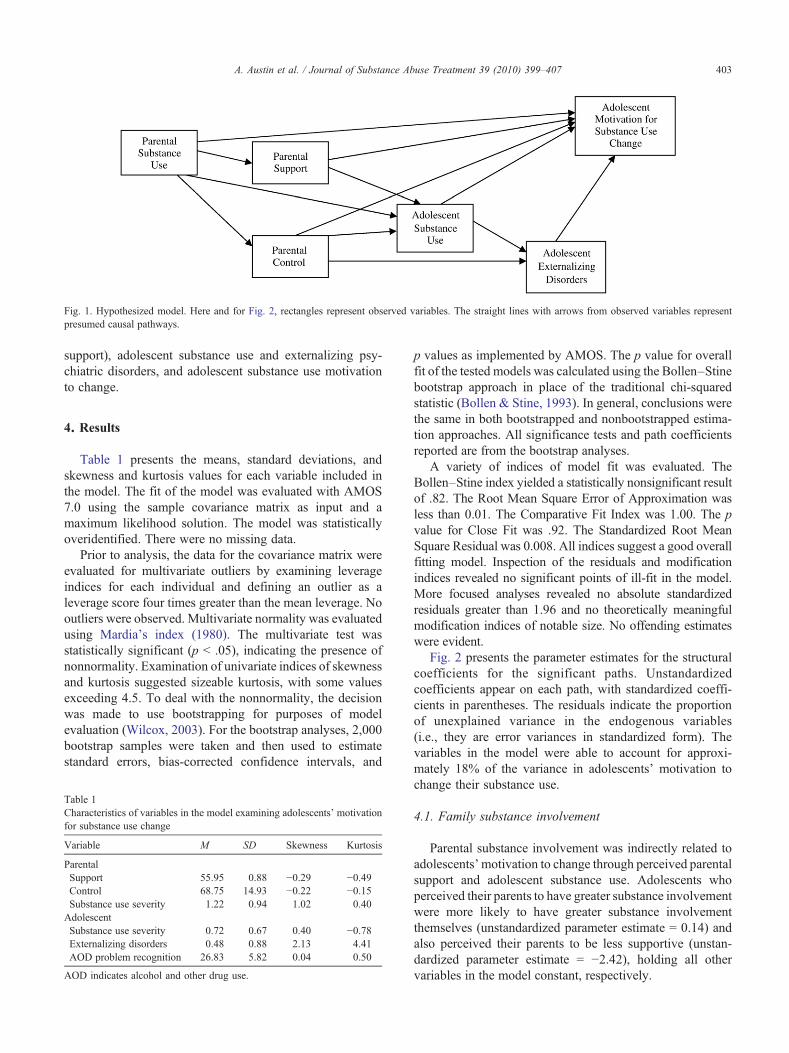
Fig. 1. Hypothesized model. Here and for Fig. 2, rectangles represent observed variables. The straight lines with arrows from observed variables representpresumed causal pathways.
403A. Austin et al. / Journal of Substance Abuse Treatment 39 (2010) 399–407
support), adolescent substance use and externalizing psy-chiatric disorders, and adolescent substance use motivationto change.
4. Results
Table 1 presents the means, standard deviations, andskewness and kurtosis values for each variable included inthe model. The fit of the model was evaluated with AMOS7.0 using the sample covariance matrix as input and amaximum likelihood solution. The model was statisticallyoveridentified. There were no missing data.
Prior to analysis, the data for the covariance matrix wereevaluated for multivariate outliers by examining leverageindices for each individual and defining an outlier as aleverage score four times greater than the mean leverage. Nooutliers were observed. Multivariate normality was evaluatedusing Mardia's index (1980). The multivariate test wasstatistically significant (p b .05), indicating the presence ofnonnormality. Examination of univariate indices of skewnessand kurtosis suggested sizeable kurtosis, with some valuesexceeding 4.5. To deal with the nonnormality, the decisionwas made to use bootstrapping for purposes of modelevaluation (Wilcox, 2003). For the bootstrap analyses, 2,000bootstrap samples were taken and then used to estimatestandard errors, bias-corrected confidence intervals, and
Table 1Characteristics of variables in the model examining adolescents' motivationfor substance use change
Variable M SD Skewness Kurtosis
ParentalSupport 55.95 0.88 −0.29 −0.49Control 68.75 14.93 −0.22 −0.15Substance use severity 1.22 0.94 1.02 0.40AdolescentSubstance use severity 0.72 0.67 0.40 −0.78Externalizing disorders 0.48 0.88 2.13 4.41AOD problem recognition 26.83 5.82 0.04 0.50
AOD indicates alcohol and other drug use.
p values as implemented by AMOS. The p value for overallfit of the tested models was calculated using the Bollen–Stinebootstrap approach in place of the traditional chi-squaredstatistic (Bollen & Stine, 1993). In general, conclusions werethe same in both bootstrapped and nonbootstrapped estima-tion approaches. All significance tests and path coefficientsreported are from the bootstrap analyses.
A variety of indices of model fit was evaluated. TheBollen–Stine index yielded a statistically nonsignificant resultof .82. The Root Mean Square Error of Approximation wasless than 0.01. The Comparative Fit Index was 1.00. The pvalue for Close Fit was .92. The Standardized Root MeanSquare Residual was 0.008. All indices suggest a good overallfitting model. Inspection of the residuals and modificationindices revealed no significant points of ill-fit in the model.More focused analyses revealed no absolute standardizedresiduals greater than 1.96 and no theoretically meaningfulmodification indices of notable size. No offending estimateswere evident.
Fig. 2 presents the parameter estimates for the structuralcoefficients for the significant paths. Unstandardizedcoefficients appear on each path, with standardized coeffi-cients in parentheses. The residuals indicate the proportionof unexplained variance in the endogenous variables(i.e., they are error variances in standardized form). Thevariables in the model were able to account for approxi-mately 18% of the variance in adolescents' motivation tochange their substance use.
4.1. Family substance involvement
Parental substance involvement was indirectly related toadolescents' motivation to change through perceived parentalsupport and adolescent substance use. Adolescents whoperceived their parents to have greater substance involvementwere more likely to have greater substance involvementthemselves (unstandardized parameter estimate = 0.14) andalso perceived their parents to be less supportive (unstan-dardized parameter estimate = −2.42), holding all othervariables in the model constant, respectively.
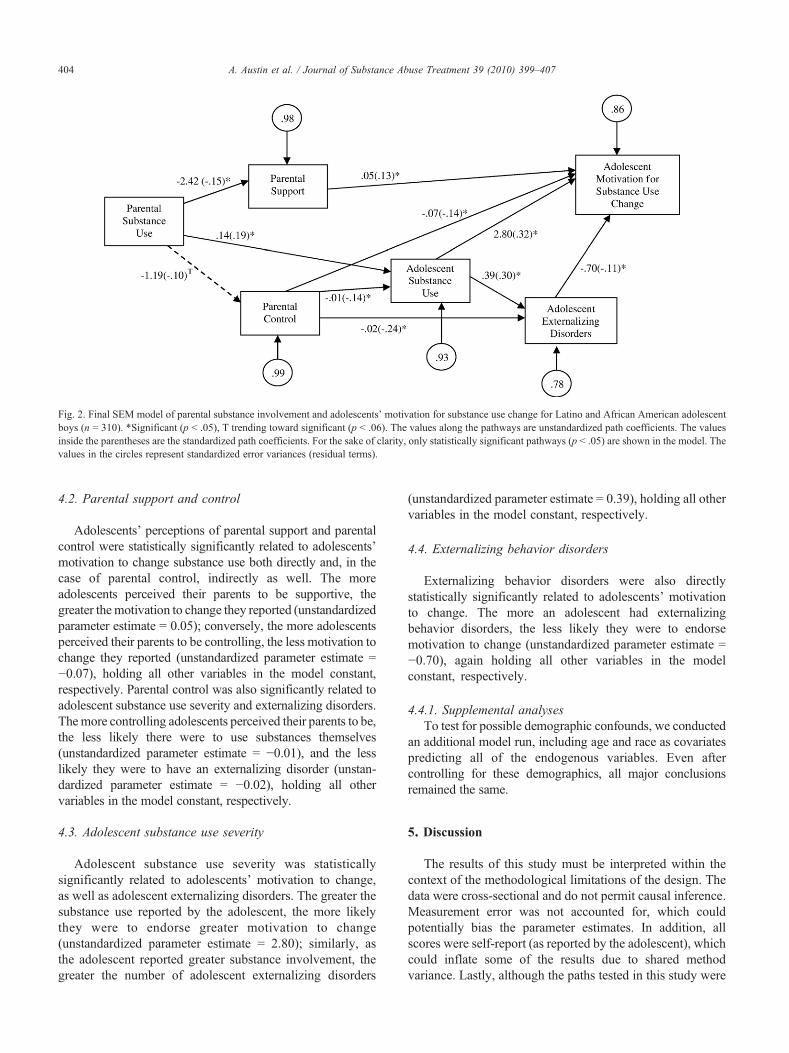
Fig. 2. Final SEM model of parental substance involvement and adolescents' motivation for substance use change for Latino and African American adolescentboys (n = 310). *Significant (p b .05), T trending toward significant (p b .06). The values along the pathways are unstandardized path coefficients. The valuesinside the parentheses are the standardized path coefficients. For the sake of clarity, only statistically significant pathways (p b .05) are shown in the model. Thevalues in the circles represent standardized error variances (residual terms).
404 A. Austin et al. / Journal of Substance Abuse Treatment 39 (2010) 399–407
4.2. Parental support and control
Adolescents' perceptions of parental support and parentalcontrol were statistically significantly related to adolescents'motivation to change substance use both directly and, in thecase of parental control, indirectly as well. The moreadolescents perceived their parents to be supportive, thegreater themotivation to change they reported (unstandardizedparameter estimate = 0.05); conversely, the more adolescentsperceived their parents to be controlling, the less motivation tochange they reported (unstandardized parameter estimate =−0.07), holding all other variables in the model constant,respectively. Parental control was also significantly related toadolescent substance use severity and externalizing disorders.Themore controlling adolescents perceived their parents to be,the less likely there were to use substances themselves(unstandardized parameter estimate = −0.01), and the lesslikely they were to have an externalizing disorder (unstan-dardized parameter estimate = −0.02), holding all othervariables in the model constant, respectively.
4.3. Adolescent substance use severity
Adolescent substance use severity was statisticallysignificantly related to adolescents' motivation to change,as well as adolescent externalizing disorders. The greater thesubstance use reported by the adolescent, the more likelythey were to endorse greater motivation to change(unstandardized parameter estimate = 2.80); similarly, asthe adolescent reported greater substance involvement, thegreater the number of adolescent externalizing disorders
(unstandardized parameter estimate = 0.39), holding all othervariables in the model constant, respectively.
4.4. Externalizing behavior disorders
Externalizing behavior disorders were also directlystatistically significantly related to adolescents' motivationto change. The more an adolescent had externalizingbehavior disorders, the less likely they were to endorsemotivation to change (unstandardized parameter estimate =−0.70), again holding all other variables in the modelconstant, respectively.
4.4.1. Supplemental analysesTo test for possible demographic confounds, we conducted
an additional model run, including age and race as covariatespredicting all of the endogenous variables. Even aftercontrolling for these demographics, all major conclusionsremained the same.
5. Discussion
The results of this study must be interpreted within thecontext of the methodological limitations of the design. Thedata were cross-sectional and do not permit causal inference.Measurement error was not accounted for, which couldpotentially bias the parameter estimates. In addition, allscores were self-report (as reported by the adolescent), whichcould inflate some of the results due to shared methodvariance. Lastly, although the paths tested in this study were

405A. Austin et al. / Journal of Substance Abuse Treatment 39 (2010) 399–407
considered primary and predominant, we also recognize thatexisting literature in this area suggests the possibility of somereciprocal dynamics, and as such, some specification errormay exist. However, despite these limitations, the results areintriguing and informative.
Findings were consistent with expectations that adoles-cents' motivation to change substance use is the result ofcomplex multidimensional relationships. Specifically, studyfindings identify meaningful adolescent (externalizing dis-orders, substance use severity) and parental (support,control, and substance use) targets of intervention forprograms attempting to enhance youth motivation to reducesubstance use. This study's findings indicate that moresubstance-involved parents are perceived as less supportiveby their children, which in turn is associated with lowermotivation for substance use reductions. Stated another way,increases in adolescents' perceptions of parental support leaddirectly to increases in substance-using adolescents' moti-vation for substance use change. In addition, parental controlappears to negatively influence youth motivation for change,whereby greater levels of parental control influence reduc-tions in adolescent's motivation to reduce substance use.Although there is a host of research indicating that parentingbehaviors influence substance use initiation and the laterdevelopment of substance use problems (Baumrind, 1991;Chassin et al., 1996; Hawkins et al., 1992), there is relativelylittle understood about the importance of parental support onother aspects of adolescent substance use, includingmotivation for substance use change. As such, these findingsregarding the direct influence of adolescents' perceptions ofparental support and control on adolescents' motivation tochange substance use represent an important contribution tothe literature. In addition, these results suggest theimportance of involving parents in treatment for adolescentsubstance use problems. Specifically, tailoring interventionapproaches to include components that focus on effectiveparenting strategies (e.g., increasing parent support anddecreasing authoritarian parental control) may prove impor-tant in enhancing youth motivation for making substanceuse changes.
In addition to the importance of targeting parental factors,this study's findings suggest that externalizing disordershave a direct negative influence on adolescents' motivationto change substance use. Research consistently demonstratesthat substance-using adolescents with externalizing behaviordisorders, such as conduct disorder, have an increasedlikelihood for treatment dropout (Austin & Wagner, 2006;Galaif et al., 2001; Kaminer et al., 1992) and poor treatmentoutcome (Crowley, Mikulich, MacDonald, Young, & Zerbe,1998; Rowe, Liddle, Greenbaum, & Henderson, 2004).However, this study is the first to identify the importantinfluence that externalizing disorders have on motivation tochange among African American and Hispanic adolescentswith substance use problems. Because African American andHispanics experience disproportionate negative outcomesassociated with high-risk behaviors, including substance use
(Herd, 1994; Mulia et al., 2009) and criminal involvement(Children's Defense Fund, 2009), enhancing motivation tochange substance use among minority youth with externa-lizing disorders may be critical to decreasing disparatepsychosocial and health outcomes.
Further inquiry into the specific strategies most effectivein enhancing motivation to change among this uniquelyhigh-risk subgroup of substance users is recommended. Inthe meantime, however, this study's results highlight theimportance of including current motivational enhancementtechniques (e.g., see DiClemente et al., 2008) as a necessarycomponent of substance abuse interventions targetingminority youth with externalizing behaviors.
Interestingly, findings indicate that higher levels ofadolescent substance use were related to greater levels ofmotivation to change. This is consistent with research amongcollege-aged drinkers (Minugh et al., 1997; Vik et al., 2000).Although Battjes et al. (2003) found no relation betweensubstance use severity and motivation for change, theirresearch indicated that external consequences of substanceuse were predictive of motivation for change. Because oursubstance use variable was based on meeting criteria forsubstance use disorders (e.g.,DSM-IV substance use disorderdiagnoses yielded through the CIDI) and not simply thefrequency and amount of substances used, this may makeinterpretation of findings more complicated.
Specifically, some criteria associated with substance usedisorder diagnoses are also consistent with the experience ofnegative external consequences for use, for example, (a)recurrent substance use resulting in a failure to fulfill majorrole obligations at work, school, or home; (b) recurrentsubstance use in situations in which it is physicallyhazardous; (c) recurrent substance-related legal problems;and (d) continued substance use despite having persistent orrecurrent social or interpersonal problems caused orexacerbated by the effects of the substance (DSM-IV;American Psychiatric Association, 1994). As such, consis-tent with Battjes et al. (2003), the external consequencesassociated with substance use may be better predictors ofmotivation for change than level of substance use severity interms of frequency and amount used. Because of thelimitations of our data set, we were unable to conduct posthoc analyses including the individual DSM-IV-R criterionassociated with the substance use disorder diagnoses;however, we feel this is an area of inquiry that requiresfurther examination in future research with adolescentsubstance users. Nevertheless, it is important that substanceabuse treatment providers be aware that minority youthmeeting criteria for substance use disorders may be uniquelymotivated to makes changes in their substance use.
Given that Hispanic and African Americans withsubstance use problems experience numerous treatmentdisparities including greater rates of unmet treatment need(Wu et al., 2002), disproportionate rates of treatment dropout(Office of Applied Studies, 2000), and more severeconsequences associated with substance use behaviors

406 A. Austin et al. / Journal of Substance Abuse Treatment 39 (2010) 399–407
(Herd, 1994; Mulia et al., 2009), there is a compelling needfor research focused on identifying strategies to improvetreatment for racial/ethnic minority youth. As such, thisstudy makes an important contribution to research andpractice aimed at understanding the factors relevant tomotivation to change among a high-risk and inadequatelyserved population of youth. Because motivation is crucial totreatment engagement, retention, and outcome, successfullyidentifying and targeting predictors of motivation to changesubstance use among adolescents presenting for treatmentrepresents a significant step toward reducing substance abusetreatment disparities.
Acknowledgments
This study was supported in part by a grant from theNational Institute Alcohol Abuse and Alcoholism to Dr. EricF. Wagner (R01 AA12180). The authors wish to expresstheir appreciation to the staff and clients associated with theC-BIRG at Florida International University, whose partici-pation made this study possible.
References
Allen, J. P., & Wilson, V. B. (2003). Assessing alcohol problems: A guidefor clinicians and researchers, 2nd. ed. Bethesda, MD [NIAAATreatment Handbook Series 4] [HE 20.8308/2:4 2003].
American Psychiatric Association. (1994). Diagnostic and statisticalmanual of mental disorders, 4th ed. Washington, DC: Author.
Andrews, G., & Peters, L. (1998). The psychometric properties of theComposite International Diagnostic Interview. Social Psychiatry andPsychiatric Epidemiology, 33, 80−88.
Austin, A. M., & Wagner, E. F. (2006). Correlates of treatment retentionamong multiethnic youth with substance use problems: Ethnic groupdifferences. Journal of Child and Adolescent Substance Abuse, 15,105−128.
Barnett, N. P., Lebeau-Craven, R., Wollard, R., Rohsenow, D. J., Spirito, A.,& Monti, P. M. (2002). Predictors of motivation to change after medicaltreatment for drinking-related events in adolescents. Psychology ofAddictive Behaviors, 16, 106−112.
Battjes, R. J., Gordon, M. S., O'Grady, K. E., Kinlock, T. W., &Carswell, M. A. (2003). Factors that predict adolescent motivation forsubstance abuse treatment. Journal of Substance Abuse Treatment,24, 221−232.
Baumrind, D. (1991). The influence of parenting style on adolescentcompetence and substance use. Journal of Early Adolescence, 11, 56−95.
Bollen, K. A., & Stine, R. (1993). Bootstrapping goodness of fit measures instructural equation models. In K. A. Bollen, & J. S. Long (Eds.), Testingstructural equation models (pp. 111−135). Newbury Park, CA: Sage.
Breda, C. S., & Heflinger, C. A. (2007). The impact of motivation to changeon substance use among adolescents in treatment. Journal of Child andAdolescent Substance Abuse, 16, 109−124.
Broome, K. M., Joe, G. W., & Simpson, D. D. (2001). Engagement modelsfor adolescents in DATOS-A. Journal of Adolescent Research, 16,608−623.
Cady, M. E., Winters, K. C., Jordan, D. A., Solberg, K. B., & Stinchfield, R.D. (1996). Motivation to change as a predictor of treatment outcome foradolescent substance abusers. Journal of Child and AdolescentSubstance Abuse, 5, 73−91.
Caetano, R., Mora, M. E. M., Schafer, J., & Marino, M. (1999). Thestructure of DSM-IV alcohol dependence in a treatment sample ofMexican and Mexican American men. Addiction, 94, 533−541.
Chassin, L., Curran, P. J., Hussong, A. M., & Colder, C. R. (1996). Therelation of parent alcoholism to adolescent substance use: A longitudinalstudy. Journal of Abnormal Psychology, 105, 70−80.
Children's Defense Fund. (2009). Cradle to Prison Pipeline SummaryReport. Retrieved August 19, 2009 from http://www.childrensdefense.org/child-research-data-publications/data/cradle-prison-pipeline-summary-report.pdf.
Cohen, D. A., & Rice, J. (1997). Parenting styles, adolescent substance use,and academic achievement. Journal of Drug Education, 27, 199−211.
Cottler, L. B., Grant, B. F., Blaine, J., Mavreas, V., Pull, C., Hasin, D., et al.(1997). Concordance of the DSM-IV alcohol and drug use disordercriteria and diagnoses as measured by AUDADIS-ADR, CIDI andSCAN. Drug and Alcohol Dependence, 47, 195−205.
Crowley, T. J., Mikulich, S. K., MacDonald, M., Young, S. E., & Zerbe,G. O. (1998). Substance-dependent, conduct-disordered adolescentmales: Severity of diagnosis predicts 2-year outcome. Drug andAlcohol Dependence, 49, 225−237.
De Leon, G., & Jainchill, N. (1986). Circumstance, motivation, readiness,and suitability as correlates of treatment tenure. Journal of PsychoactiveDrugs, 18, 203−208.
De Leon, G., Melnick, G., & Hawke, J. (2000). The motivation–readinessfactor in drug treatment: Implications for research and policy. Ad-680vances in medical sociology (vol. 7, pp. 103–129). Greenwich, CT:JAI Press, Inc.
De Leon, G., Melnick, G., & Kressel, D. (1997). Motivation and readinessfor therapeutic community treatment among cocaine and other drugabusers. American Journal of Drug and Alcohol Abuse, 23, 169−189.
De Leon, G., Melnick, G., Kressel, D., & Jainchill, N. (1994).Circumstances, motivation, readiness, and suitability (the CMRS scales):predicting retention in therapeutic community treatment. AmericanJournal of Drug and Alcohol Abuse, 20(4), 495−515.
DiClemente, C., Garay, M., & Gemmell, L. (2008). Motivationalenhancement. In M. Galanter, & H. D. Kleber (Eds.), The AmericanPsychiatric Publishing Textbook of Substance Abuse Treatment (4th ed.,pp. 361−372). Washington, DC: American Psychiatric Publishing 366.
Fickenscher, A., Novins, D. K., & Beals, J. (2006). A pilot study ofmotivation and treatment completion among American Indian adoles-cents in substance abuse treatment. Addictive Behaviors, 31, 1402−1414.
Flynn, P. M., Joe, G. W., Broome, K. M., Simpson, D. D., & Brown, B. S.(2003). Recovery from opioid addiction in DATOS. Journal ofSubstance Abuse Treatment, 25, 177−186.
Friedman, A. S., Granick, S., & Kreisher, C. (1994). Motivation ofadolescent drug abusers for help and treatment. Journal of Child &Adolescent Substance Abuse, 3(1), 69−88.
Freyer, J., Tonigan, J. S., Keller, S., John, U., Rumpf, H. J., & Hapke, U.(2004). Readiness to change versus readiness to seek help for alcoholproblems: The development of the Treatment Readiness Tool (TReaT).Journal of Studies on Alcohol, 65, 801−809.
Galaif, E. R., Hser, Y. I., Grella, C. E., & Joshi, V. (2001). Prospective riskfactors and treatment outcomes among adolescents in DATOS-A.Journal of Adolescent Research, 16, 661−678.
Garner, B. R., Godley, S. H., & Funk, R. R. (2008). Predictors of earlytherapeutic alliance among adolescents in substance abuse treatment.Journal of Psychoactive Drugs, 40, 55−65.
Harrison, P. A., & Asche, S. E. (2001). Adolescent treatment for substanceuse disorders: Outcomes and outcome predictors. Journal of Child &Adolescent Substance Abuse, 1(2), 1−17.
Hasin, D., van Rossem, R., McCloud, S., & Endicott, J. (1997).Differentiating DSM-IV alcohol dependence and abuse by course:Community heavy drinkers. Journal of Substance Abuse, 9, 127−135.
Hawkins, J. D., Catalano, R. F., & Miller, J. Y. (1992). Risk and protectivefactors for alcohol and other drug problems in adolescence and earlyadulthood: Implications for substance abuse prevention. PsychologicalBulletin, 112, 64−105.
Herd, D. (1994). Predicting drinking problems among Black andWhite men:Results from a national survey. Journal of Studies on Alcohol, 55,61−71.
407A. Austin et al. / Journal of Substance Abuse Treatment 39 (2010) 399–407
Hogue, A., Dauber, S., & Morgenstern, J. (2010). Validation of acontemplation ladder in an adult substance use disorder sample.Psychology of Addictive Behaviors, 24, 137−144.
Horton, J., Compton, W., & Cottler, L. B. (2000). Reliability of substanceuse disorder diagnoses among African-Americans and Caucasians.Drugand Alcohol Dependence, 57, 203−209.
Hiller, M. L., Knight, K., Leukefeld, C., & Simspon, D. D. (2002).Motivation as a predictor of therapeutic engagement in mandatedresidential substance abuse treatment. Criminal Justice and Behavior,29, 56−75.
Hsieh, S., Hoffman, N. G., & Hollister, D. C. (1998). The relationshipbetween pre-, during-, post-treatment factors, and adolescent substanceabuse behaviors. Addictive Behaviors, 23, 477−488.
Jainchill, N., Hawke, J., De Leon, G., & Yagelka, J. (2000). Adolescents intherapeutic communities: One-year posttreatment outcomes. Journal ofPsychoactive drugs, 32, 81−94.
Joe, G. W., Simpson, D. D., & Broome, K. M. (1998). Effects of readinessfor drug abuse treatment on client retention and assessment of process.Addiction, 93, 1177−1190.
Joe, G. W., Simpson, D. D., & Broome, K. M. (1999). Retention and patientengagement models for different treatment modalities in DATOS. Drugand Alcohol Dependence, 57, 113−125.
Kaminer, Y., Tarter, R. E., Bukstein, O. G., & Kabene, M. (1992).Comparison between treatment completers and noncompleters amongdually diagnosed substance-abusing adolescents. Journal of theAmerican Academy of Child and Adolescent Psychiatry, 31,1046−1049.
King, K. M., Chung, T., & Maisto, S. A. (2009). Adolescents' thoughtsabout abstinence curb the return of marijuana use during and aftertreatment. Journal of Consulting and Clinical Psychology, 77,554−565.
Lau, K., Freyer-Adam, J., Gaertner, B., Rumpf, H. J., John, U., & Hapke, U.(2010). Motivation to change risky drinking and motivation to seek helpfor alcohol risk drinking among general hospital inpatients with problemdrinking and alcohol-related diseases. General Hospital Psychiatry, 32,86−93.
Mardia, K. V. (1980). Tests of univariate and multivariate normality.Handbook of statistics (vol. 1, pp. 279–320). New York, NY: JohnWiley & Sons, Inc.
Marti, C. N., Stice, E., & Springer, D. W. (2010). Substance use and abusetrajectories across adolescence: A latent trajectory analysis of acommunity-recruited sample of girls. Journal of Adolescence, 33,449−461.
Melnick, G., De Leon, G., Hawke, J., Jainchill, N., & Kressel, D. (1997).Motivation and readiness for therapeutic community treatment amongadolescents and adult substance abusers. American Journal of Drug andAlcohol Abuse, 23, 485−506.
Miller, S., Gorman-Smith, D., Sullivan, T., Orpinas, P., & Simon, T. R.(2009). Parent and peer predictors of physical dating violenceperpetration in early adolescence: Tests of moderation and genderdifferences. Journal of Clinical Child & Adolescent Psychology, 38,538−550.
Minugh, P. A., Nirenberg, T. D., Clifford, P. R., Longabaugh, R., Becker,B. M., & Woolard, R. (1997). Analysis of alcohol use clusters amongsubcritically injured emergency department patients. AcademicEmergency Medicine, 4, 1059−1067.
Mistry, R., McCarthy, W. J., Yancey, A., Lu, Y., & Patel, M. (2009).Resilience and patterns of health risk behaviors in Californiaadolescents. Preventive Medicine, 48, 291−297.
Mulia, N., Ye, Y., Greenfield, T. K., & Zemore, S. E. (2009). Disparities inalcohol-related problems among White, Black, & Hispanic Americans.Alcoholism: Clinical and Experimental Research, 33, 654−662.
Office of Applied Studies. (2000). National survey of substance abusetreatment services (N-SSATS). Retrieved on February 17, 2003 fromhttp://www.samsha.org.
Pedersen, W., & Skardhamar, T. (2010). Cannabis and crime: Findings froma longitudinal study. Addiction, 105, 109−118.
Perkonigg, A., Lieb, R., Hoefler, M., Schuster, P., Sonntag, H., & Wittchen,H. -U. (1999). Patterns of cannabis use, abuse and dependence over time:Incidence, progression and stability in a sample of 1228 adolescents.Addiction, 94, 1663−1678.
Robins, L. N., Wing, J., Wittchen, H. U., & Helzer, J. E. (1988). TheComposite International Diagnostic Interview: An epidemiologicinstrument suitable for use in conjunction with different systems andin different cultures. Archives of General Psychiatry, 45, 1069−1077.
Rowe, C. L., Liddle, H. A., Greenbaum, P. E., & Henderson, C. E. (2004).Impact of psychiatric comorbidity on treatment of adolescent substanceabusers. Journal of Substance Abuse Treatment, 26, 129−140.
Rueger, S. Y., Malecki, C. K., & Demaray, M. K. (2010). Relationshipbetween multiple sources of perceived social support and psychologicaland academic adjustment in early adolescence: Comparisons acrossgender. Journal of Youth and Adolescence, 39, 47−61.
Ryan, L. G., Miller-Loessi, K., & Nieri, T. (2007). Relationships with adultsas predictors of substance use, gang involvement, and threats to safetyamong disadvantaged urban high-school adolescents. Journal ofCommunity Psychology, 35, 1053−1071.
Schaefer, E. S. (1965). A configurational analysis of childrens’ reports ofparent behavior. Journal of Consulting Psychology, 29(6), 552−557.
Schluderman, E., & Schluderman, S. (1970). Replicability of factors inchildren's perceptions of parent behavior (CRPBI). Journal ofPsychology, 76, 239−249.
Schwarz, J. C., Barton-Henry, M. L., & Pruzinsky, T. (1985). Assessingchild-rearing behaviors: A comparison of ratings made by mother,father, child and sibling on the CRPBI. Child Development, 56,462−479.
Severtson, S. G., von Thomsen, S., Hedden, S. L., & Latimer, W. (2010).The association between executive functioning and motivation to entertreatment among regular users of heroin and/or cocaine in Baltimore,MD. Addictive Behaviors, 35, 717−720.
Simpson, D. D., & Joe, G. W. (1993). Motivation as a predictor of earlydropout from drug abuse treatment. Psychotherapy, 30, 357−368.
Sobell, L. C., & Sobell, M. B. (1998). Identification and assessment ofalcohol problems. In G. P. Koocher, J. A. Norcross, & S. S. Hill III(Eds.), Psychologist's desk reference (pp. 62−67). New York: OxfordUniversity Press.
Vik, P. W., Culbertson, K. A., & Sellers, K. (2000). Readiness to changedrinking among heavy-drinking college students. Journal of Studies onAlcohol, 61, 674−680.
Wagner, E. F. (2008). Developmentally informed research on theeffectiveness of clinical trials: A primer for assessing how developmen-tal issues may influence treatment responses among adolescents withalcohol use problems. Pediatrics, 121, S337−S347.
Wagner, E. F., Lloyd, D. A., & Gil, A. G. (2002). Racial/Ethnic and genderdifferences in the incidence and onset age of DSM-IV alcohol usedisorder symptoms among adolescents. Journal of Studies on Alcohol,63, 609−619.
Weiss, L. H., & Schwarz, J. C. (1996). The relationship between parentingtypes and older adolescents' personality, academic achievement,adjustment, and substance use. Child Development, 67, 2101−2114.
Wilcox, R. (2003). Applying contemporary statistical techniques. SanDiego: Academic Press.
Wu, P., Hoven, C. W., Tiet, Q., Kovalenko, P., & Wicks, J. (2002). Factorsassociated with adolescent utilization of alcohol treatment services.American Journal of Drug and Alcohol Abuse, 28, 353−369.





























