Embed Size (px)
Citation preview

MORPHEA AFFECTING A FATHER AND SON
Abstract: Morphea, also known as localizedscleroderma, is characterized by firm plaques that canoccur anywhere on the body. Reports of familial morp-hea are rare, and we report an unusual case of morpheaaffecting both a father and a son.
Morphea, also known as localized scleroderma, is char-acterized by thickening or hardening of the skin andsubcutaneous tissue as a result of excess collagen depo-sition. Morphea is not related to systemic sclerosis; itaffects the skin alone, with no internal organ involve-ment. We report a unique case of a father and sonaffected by plaque-type morphea.
CASE REPORT
A 9-year-old Puerto Rican boy presented to the derma-tology clinic with complaints of thickened skin over theleft anterior leg for2 years. It startedafter beingkicked inthe left shinand initially appearedas abruise that became‘‘thick’’ and never resolved. It had been stable until re-cently when similar lesions appeared on the left calf andleft foot. Itwasotherwise asymptomatic anddidnot limitany daily activities.
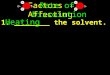
Physical exam was notable for a 5 · 5 cm hyper-pigmented plaque with a bound-down texture on theleft anterior leg (Fig. 1) with smaller, similar plaqueson the left dorsal foot and left thigh. A clinical diag-nosis of plaque-type morphea was suspected. This wasconfirmed histologically by a thickened dermis withentrapment of eccrine glands, and sparse perivascularlymphocytes. The family was particularly concernedregarding this diagnosis because the child’s father haddeveloped morphea at age 30 on his chest followingsunburn several years before (Fig. 2). Of note, thefather’s case of morphea was diagnosed by skinbiopsy; he is otherwise healthy. There is no familyhistory of autoimmune disease.
DISCUSSION
Familial morphea is uncommon and has rarely beenreported in the medical literature. In 1953 Rees andBennett documented the first familial case, which in-volved a father and daughter (1). Since then, more caseshave documented morphea of varying subtypes, occur-ring in parent, child, and siblings. To our knowledge,there have been only 19 reported cases of familial
morphea (2–8). This report adds one more to the litera-ture.
Although the cause of morphea remains unknown,autoimmune, environmental, and infectious factors havebeen proposed. Nonhereditary factors are thought toplay a major factor in the pathogenesis of disease (9).However, the rising numbers of familial cases reportedsuggests a genetic component may be present thatpredisposes individuals todevelopmorphea.The familialcases exhibit a nonMendelian pattern; this is suggestiveof a multifactorial, polygenic inheritance (8).
Figure 1. Older atrophic plaque at site of trauma on anteriorleg; newer erythematous plaque.
Figure 2. Hyperpigmented, burned-out plaque on chest.
536 Pediatric Dermatology Vol. 27 No. 5 September ⁄October 2010

The onset of morphea has been associated withenvironmental triggers. Two different case series bothreported a possible trigger of morphea in over 13% ofpatients (9,10). Trauma, as in the case of our 9-year-oldpatient, is the most common trigger, reported in 7.3–11.8% of patients (9,10). The father in our case reportedsunburn in the area where morphea subsequentlydeveloped. To our knowledge, only one other case hasbeen documented of sunburn as a trigger for morphea(10).
Our case features morphea in a father and son whoindependently developed morphea after exposure to atrigger factor. Our findings along with previous reportssuggest a genetic or environmental component, or both,to morphea is likely.
REFERENCES
1. Rees RB, Bennett J. Localized scleroderma in father anddaughter. Arch Dermatol 1953;68:360.
2. Taj M, Ahmad A. Familial localized scleroderma (mor-phoea). Arch Dermatol 1977;113:1132–1133.
3. Wadud MA, Bose BK, Al Nasir T. Familial localizedscleroderma from Bangladesh: two case reports. Bangla-desh Med Res Counc Bull 1989;15:15–19.
4. Kaur V, SinghG. Linear scleroderma in a family. Indian JDermatol Venereol Leprol 1993;59:15–16.
5. Patrizi A, Marzaduri S, Marini R. A familial case ofscleroderma en coup de sabre. Acta Derm Venereol2000;80:237.
6. Iranzo P, Lopez I, Palou J et al. Morphoea in three sib-lings. J Eur Acad Dermatol Venereol 2001;15:46–47.
7. Brownell I, Soter NA, Franks AG et al. Familial linearscleroderma (en coup de sabre) responsive to antimalarialsand narrowband ultraviolet B therapy. Dermatol Online J2007;13:11.
8. Leitenberger JJ, Cayce RL, Haley RW et al.Distinct autoimmune syndromes in morphea. A review of245 adult and pediatric cases. Arch Dermatol 2009;145:545–550.
9. Zulian F, Athreya BH, Laxer R et al. Juvenile localizedscleroderma: clinical and epidemiological features in 750children. An international study. Rheumatology (Oxf)2005;45:614–620.
10. Christen-ZaechS,HakimMD,SuleAfsarFet al. Pediatricmorphea (localized scleroderma): review of 136 patients.J Am Acad Dermatol 2008;59:385–396.
CATHERINEM. PHAM, B.S.*JOHN C. BROWNING, M.D.*,�*Division of Dermatology and Cutaneous Surgery,�Department of Pediatrics, Pediatric DermatologySection, SanAntonio, University of Texas Health ScienceCenter at San Antonio, Texas
BULLOUS PEMPHIGOID IN LATE
CHILDHOOD SUCCESSFULLY TREATED
WITH MYCOPHENOLATE MOFETIL AS AN
ADJUVANT THERAPY
Abstract: Bullous pemphigoid is an acquired sub-epidermal vesiculobullous disease most commonlyseen in the elderly. We report a 16-year-old girl withbullous pemphigoid who achieved disease remissionwith mycophenolate mofetil as an adjuvant therapy.
CASE REPORT
A 16-year-old African American girl with a history ofatopy presented with a 10-day history of a progressive,blistering skin eruption. Physical examination revealednumerous erythematous targetoid plaques with duskycenters, and pink urticarial plaques with overlying vesi-cles and bullae involving greater than 70% of her totalbody surface area (Fig. 1).
Histopathologic evaluation of a punch biopsy frominvolved skin revealed a subepidermal blister withprominent eosinophils (Fig. 2A,B). Direct and indirectimmunofluorescence studieswere consistentwithbullouspemphigoid (BP). Leukocytosis of 17.5 K ⁄lL (refs. 3.5–11) and eosinophilia of 21% were also present. Liverfunction and serum chemistry panels werewithin normallimits. Rapid plasma regain (RPR) was nonreactive.
The patient was admitted to the burn intensive careunit and treated with high-dose oral prednisone(1 mg ⁄kg body weight), mycophenolate mofetil (MM)(500 mg p.o. three times daily for 7 days, then 1000 mgp.o. two times daily), tacrolimus ointment, and fluocin-onide ointment until stabilization was obtained. Thepatient was discharged after a 21-day admission onMM1000 mg p.o. two times daily, prednisone 60 mg p.o.daily, esomeprazole magnesium 40 mg p.o. daily, andtriamcinolone ointment 0.1% twice daily. Bullae subse-quently healed without scarring or recurrence, but withsignificant hyperpigmentation. Oral and topical steroidswere slowly tapered and discontinued over the nextseveral months, and MM was eventually tapered anddiscontinued after 18 months without recurrence ofsymptoms. Indirect immunofluorescence continues todemonstrate antibodies at titers of 1:160.
DISCUSSION
Bullous pemphigoid most commonly affects the elderly,and childhood disease is rare. Childhood and adult
Address correspondence to John C. Browning, M.D., PediatricDermatology Section, University of Texas Health Science Cen-ter—San Antonio, 7703 Floyd Curl Drive, MSC 7808, San Anto-nio, TX 78229-3900, or e-mail: [email protected].
Brief Reports 537