Embed Size (px)
DESCRIPTION
Mood Disorders. An Overview of Mood Disorders. Gross Deviations in Mood Depression: “The Low” The “Common Cold” of Mental Illness Major Depressive Episode is Most Common Mania: “The High” Abnormally Exaggerated Elation, Joy, or Euphoria. An Overview of - PowerPoint PPT Presentation
Citation preview

Gross Deviations in Mood Depression: “The Low”
– The “Common Cold” of Mental Illness– Major Depressive Episode is Most
Common Mania: “The High”
– Abnormally Exaggerated Elation, Joy, or Euphoria
Gross Deviations in Mood Depression: “The Low”
– The “Common Cold” of Mental Illness– Major Depressive Episode is Most
Common Mania: “The High”
– Abnormally Exaggerated Elation, Joy, or Euphoria
ManiaMania
DepressionDepression
Unipolar Mood Disorder– Either Depression or Mania
Bipolar Mood Disorder– Alternates Between Depression and Mania
Important to Determine the Course– Temporal Patterning of the Episodes
Unipolar Mood Disorder– Either Depression or Mania
Bipolar Mood Disorder– Alternates Between Depression and Mania
Important to Determine the Course– Temporal Patterning of the Episodes
Depressive Disorders– Major Depression– PDD, formerly Dysthymic Disorder– “Double Depression” - - dysthymia
punctuated by period of major depression
Bipolar I and Bipolar II Disorders– Cyclothymic Disorder
Depressive Disorders– Major Depression– PDD, formerly Dysthymic Disorder– “Double Depression” - - dysthymia
punctuated by period of major depression
Bipolar I and Bipolar II Disorders– Cyclothymic Disorder
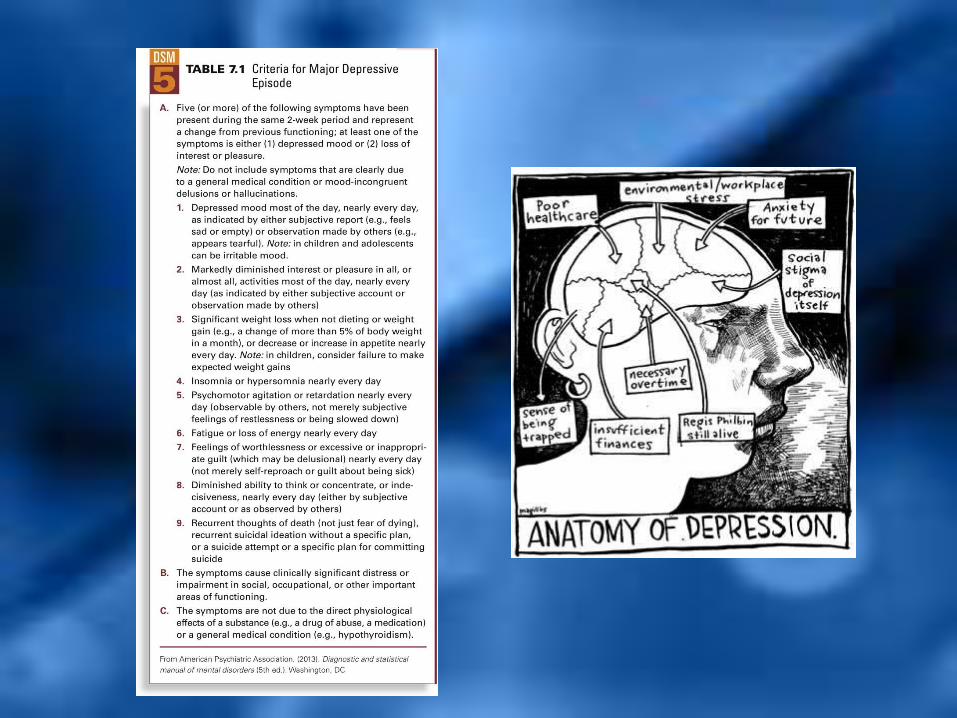
Extremely Depressed Mood– Lasting at Least 2 Weeks
Cognitive Symptoms Anhedonia Vegetative Symptoms Single or Recurrent Episode
– No Manic or Hypomanic Episodes
Extremely Depressed Mood– Lasting at Least 2 Weeks
Cognitive Symptoms Anhedonia Vegetative Symptoms Single or Recurrent Episode
– No Manic or Hypomanic Episodes
Clinical Description Clinical Description
Similar to Major Depression BUT With a Different Course – Symptoms are Milder
– Symptoms can Last 20-30+ Years
Persistently Depressed Mood for 2+ Years– Cannot be Symptom Free > 2 Months
Similar to Major Depression BUT With a Different Course – Symptoms are Milder
– Symptoms can Last 20-30+ Years
Persistently Depressed Mood for 2+ Years– Cannot be Symptom Free > 2 Months
Clinical Description Clinical Description
Facts and Statistics Facts and Statistics Mean Age of Onset Early 20s Onset Prior to Age 20
– Greater Chronicity
– Poor Prognosis
Major Depressive Episodes are Common
Mean Age of Onset Early 20s Onset Prior to Age 20
– Greater Chronicity
– Poor Prognosis
Major Depressive Episodes are Common
Suffer From Both – Major Depression Episodes
– PDD - Dysthymic Disorder
Dysthymia Usually Begins First Associated With Severe Pathology A Problematic Future Course
Suffer From Both – Major Depression Episodes
– PDD - Dysthymic Disorder
Dysthymia Usually Begins First Associated With Severe Pathology A Problematic Future Course
Clinical Description Clinical Description
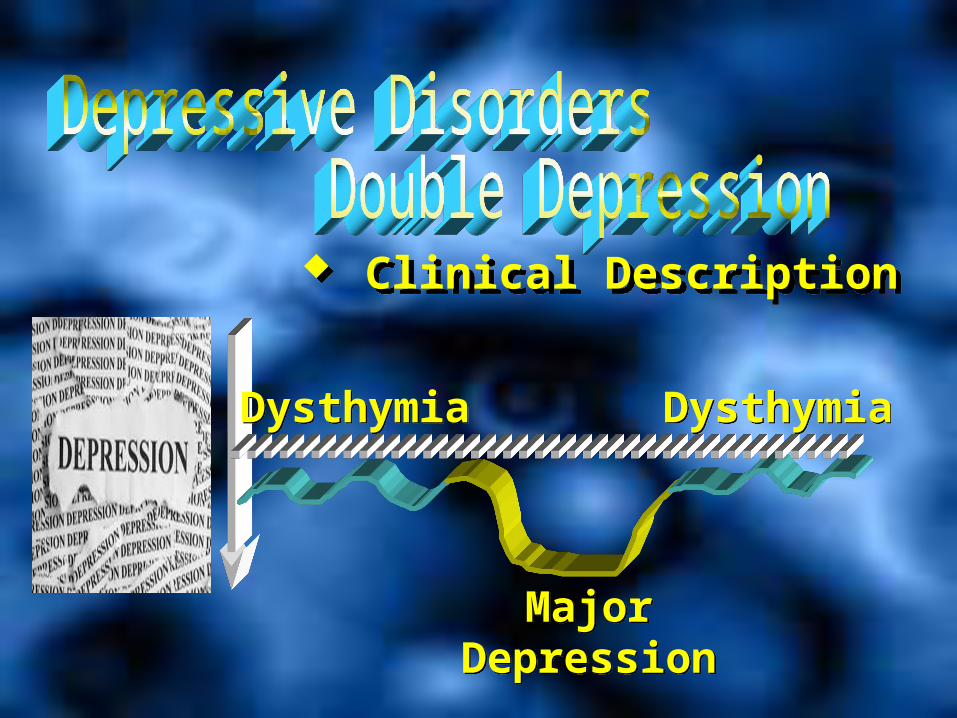
DysthymiaDysthymia
MajorDepression
MajorDepression
DysthymiaDysthymia
Clinical Description Clinical Description
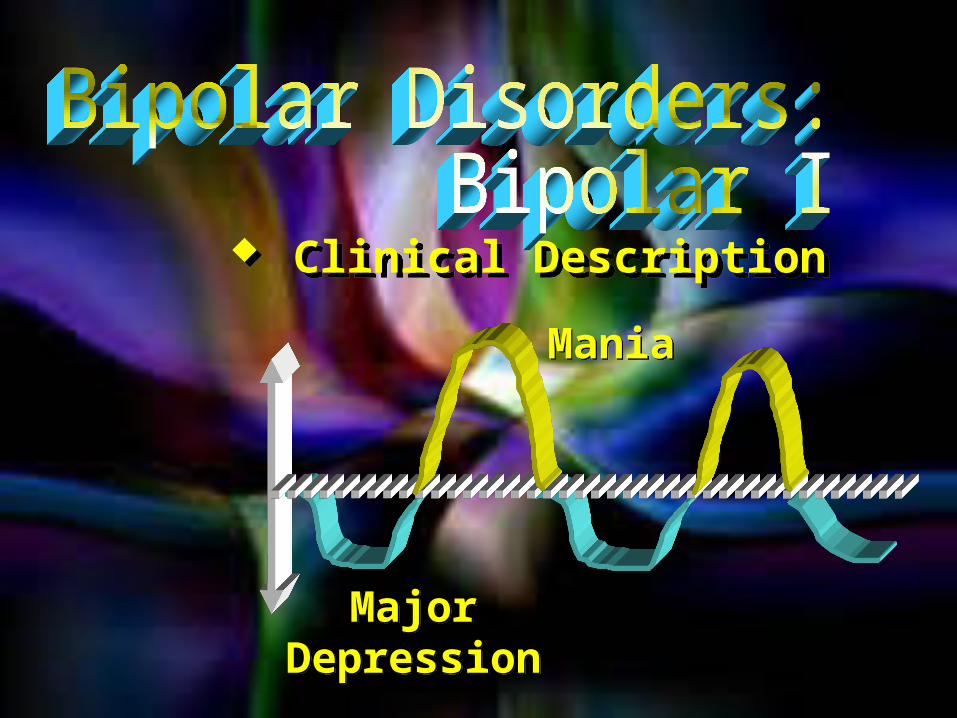
Major Features Major Features Experience Both
– Manic Episodes
– Major Depressive Episodes
Roller Coaster of Mood
Experience Both– Manic Episodes
– Major Depressive Episodes
Roller Coaster of Mood
What are Manic Episodes?What are Manic Episodes?
Mania and Hypomania Mania and Hypomania
Elevated Mood Elevated Mood
Grandiosity Grandiosity
Increased Activity Increased Activity
Varied Impairment Varied Impairment
MajorDepression
MajorDepression
ManiaMania
Clinical Description Clinical Description
Major Depressive Episodes
Alternate With Hypomanic Episodes
Major Depressive Episodes
Alternate With Hypomanic Episodes
Clinical Description Clinical Description
Milder Depressive Episodes
Alternate With Hypomanic Episodes
Milder Depressive Episodes
Alternate With Hypomanic Episodes
Clinical Description Clinical Description
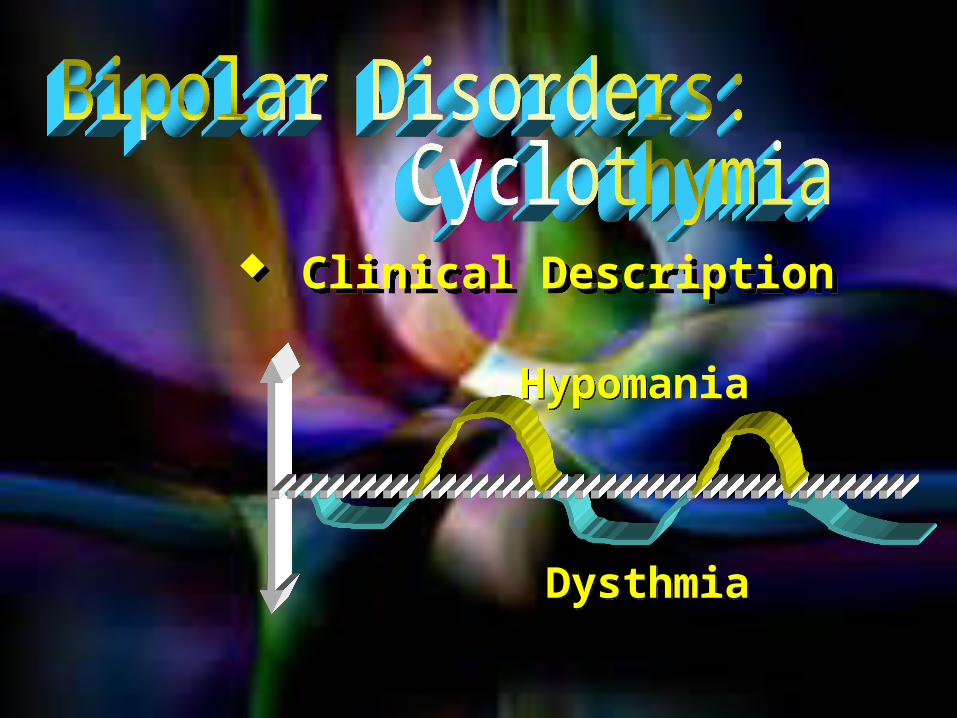
Clinical Description Clinical Description
DysthmiaDysthmia
HypomaniaHypomania
General Facts and Statistics General Facts and Statistics Bipolar I
– Onset Around 18 Years
Bipolar II – Onset Around 22 Years
16% Commit Suicide Cyclothymia
– Typically Chronic
Bipolar I– Onset Around 18 Years
Bipolar II – Onset Around 22 Years
16% Commit Suicide Cyclothymia
– Typically Chronic
Descriptions of Recent Episode and Pattern Varies Descriptions of Recent Episode and Pattern Varies
1. Atypical– Pertains to Depressive Episodes and Dysthymia,
not Manic Episodes– Typically Overeat and Oversleep
1. Atypical– Pertains to Depressive Episodes and Dysthymia,
not Manic Episodes– Typically Overeat and Oversleep

Recent Episode and Pattern Recent Episode and Pattern
2. Melancholic– Pertains to Major Depressive Episode
Only– More Severe Symptoms– Strong Biological Component
2. Melancholic– Pertains to Major Depressive Episode
Only– More Severe Symptoms– Strong Biological Component
Atypical (overeat, oversleep, wght gain – keep interested, can experience pleasure)
Atypical (overeat, oversleep, wght gain – keep interested, can experience pleasure)

Recent Episode and Pattern Recent Episode and Pattern
3. Mixed Features– With some mania symptoms
3. Mixed Features– With some mania symptoms
Atypical Atypical Melancholic Melancholic

Recent Episode and Pattern Recent Episode and Pattern
4. Catatonic– Can be part of Major Depression and
Mania– Very Serious Condition– Catalepsy (“Muscle Rigidity”)
4. Catatonic– Can be part of Major Depression and
Mania– Very Serious Condition– Catalepsy (“Muscle Rigidity”)
Atypical Atypical Melancholic Melancholic Mixed Mixed
Recent Episode and Pattern Recent Episode and Pattern
Catatonic Catatonic
Atypical Atypical Melancholic Melancholic Mixed Mixed
5. Psychotic– Hallucinations and Delusions– Very Rare but Serious Condition– Poor Treatment Response
5. Psychotic– Hallucinations and Delusions– Very Rare but Serious Condition– Poor Treatment Response

Recent Episode and Pattern Recent Episode and Pattern
Catatonic Catatonic
Atypical Atypical Melancholic Melancholic Mixed Mixed
6. Peripartum– Major Depression and Mania– Prior to…Four Weeks Following
Birth…and up to a year: high % – Mood Episodes of a Psychotic Nature
Relatively Rare
6. Peripartum– Major Depression and Mania– Prior to…Four Weeks Following
Birth…and up to a year: high % – Mood Episodes of a Psychotic Nature
Relatively Rare
Psychotic Psychotic

Recent Episode and Pattern Recent Episode and Pattern
Catatonic Catatonic
Atypical Atypical Melancholic Melancholic Mixed Mixed
Peripartum Anxious Distress
Peripartum Anxious Distress
Psychotic Psychotic

Course and Pattern Course and Pattern Rapid-Cycling Rapid-Cycling Seasonal Pattern
– Bipolar and Recurrent Major Depression– Episodes During Certain Seasons
Seasonal Pattern– Bipolar and Recurrent Major Depression– Episodes During Certain Seasons
• Premenstrual Dysphoric Disorder (PMDD)– 2- 5% of women meet criteria
• Disruptive Mood Dysregulation Disorder
– Children: increased diagnosis for bipolar, up 40% between 1995 and 2005
• Bipolar (NOS)
Other Depressive Disorders - new to DSM-5
About 16% Lifetime Global Prevalence MDD Past Year:
Bipolar-.8% Maj Depression-6%
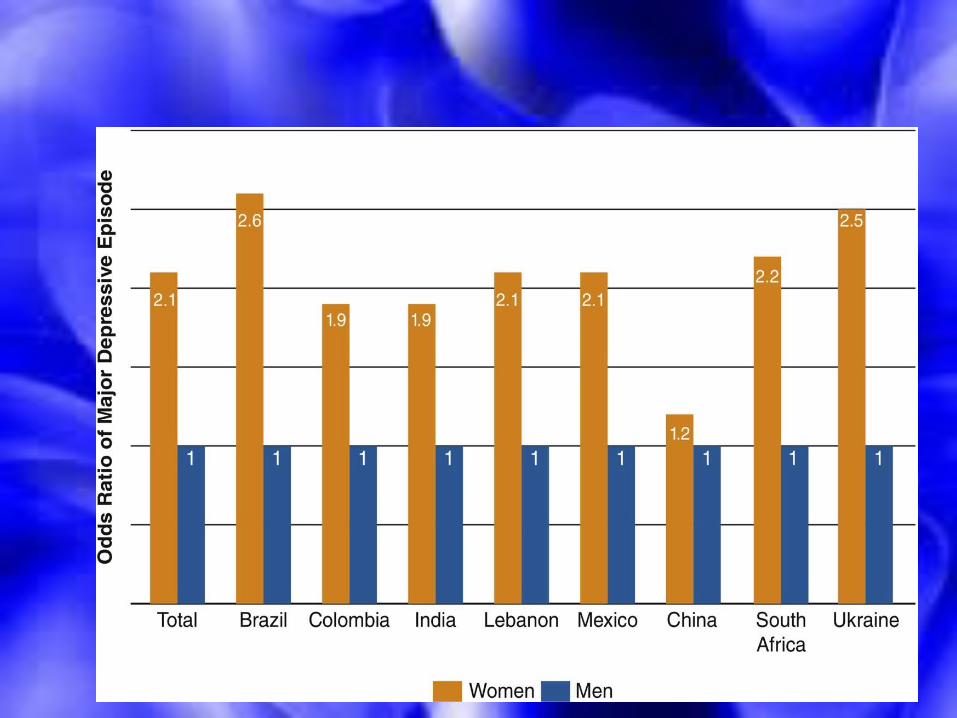
Females > Males– Major Depression and Dysthymia
Females = Males– Bipolar Disorders
About 16% Lifetime Global Prevalence MDD Past Year:
Bipolar-.8% Maj Depression-6%
Females > Males– Major Depression and Dysthymia
Females = Males– Bipolar Disorders
Biological Dimensions Biological Dimensions Family Studies Twin Studies
– As Severity Increases, so Does the Genetic Connection
No Single Genetic Link
Family Studies Twin Studies
– As Severity Increases, so Does the Genetic Connection
No Single Genetic Link
Neurotransmitters Neurotransmitters The Serotonin Connection The Serotonin Connection
Endocrine Function Endocrine Function Elevated Cortisol Dexamethasone Suppression Test:
cortisol suppressed in non-depressed people, not in severely depressed….but….
Elevated Cortisol Dexamethasone Suppression Test:
cortisol suppressed in non-depressed people, not in severely depressed….but….
Sleep and Circadian Rhythms Sleep and Circadian Rhythms Sleep Disturbances are Common More intense and earlier start to REM Sleep among the Depressed Diminished Deep Sleep Disruption of Circadian Rhythms
Sleep Disturbances are Common More intense and earlier start to REM Sleep among the Depressed Diminished Deep Sleep Disruption of Circadian Rhythms
Stressful Life Events; Loss Learned Helplessness Attributional Style
Stressful Life Events; Loss Learned Helplessness Attributional Style
Internal Stable Global
Internal Stable Global
Negative Cognitive Biases Beck’s Cognitive Triad
Negative Cognitive Biases Beck’s Cognitive Triad
Negative Schema About
Self,
World,
& Future
Negative Schema About
Self,
World,
& Future
In the United States: In the United States: About 30,000 Kill Themselves Annually More Die from Suicide Each Year Than Homicide
(about 20,000) More Common Among Whites, Native Americans Increasing in Adolescents (3rd leading cause of
death) & Elderly (globally, the elderly have highest suicide rate, esp. males)
Males > Females in Killing Themselves Females > Males in Attempts
About 30,000 Kill Themselves Annually More Die from Suicide Each Year Than Homicide
(about 20,000) More Common Among Whites, Native Americans Increasing in Adolescents (3rd leading cause of
death) & Elderly (globally, the elderly have highest suicide rate, esp. males)
Males > Females in Killing Themselves Females > Males in Attempts
Approximately 500,000 people each year require ER
treatment as a result of attempted suicide Suicidal behavior typically occurs in the presence of
mental illness or substance use disorders Firearms account for 59% of all suicide deaths
Website of Extreme and Urgent Interest suicidology.org
Approximately 500,000 people each year require ER treatment as a result of attempted suicide
Suicidal behavior typically occurs in the presence of mental illness or substance use disorders
Firearms account for 59% of all suicide deaths
Website of Extreme and Urgent Interest suicidology.org

Medications Medications Tricyclic Antidepressants
Imipramine (Tofranil)
Amitriptyline (Elavil) Block Neurotransmitter Reuptake Side Effects
Tricyclic Antidepressants
Imipramine (Tofranil)
Amitriptyline (Elavil) Block Neurotransmitter Reuptake Side Effects

Medications Medications MAO Inhibitors Block Enzyme MonoAmine Oxidase The Result?
More Neurotransmitter is Available Side Effects and Complications
MAO Inhibitors Block Enzyme MonoAmine Oxidase The Result?
More Neurotransmitter is Available Side Effects and Complications

Medications Medications SSRIs Block Reuptake of Serotonin- Prozac SSNRIs
SSRIs Block Reuptake of Serotonin- Prozac SSNRIs

Medications - Bipolar Medications - Bipolar Lithium, Depakote, Lamictal…Effective
for Manic Episodes Lithium Must be Carefully Regulated
Lithium, Depakote, Lamictal…Effective for Manic Episodes
Lithium Must be Carefully Regulated
Other Medical Treatments Other Medical Treatments Electroconvulsive Therapy (ECT) TMS
Electroconvulsive Therapy (ECT) TMS

Psychological Interventions Psychological Interventions
Combined Treatments? Combined Treatments?