Embed Size (px)
DESCRIPTION
cancer
Citation preview

R
M
D
a
b
c
a
KIAMLIEMM
1
tmact
pmoTvbcht
4
1h
Seminars in Cancer Biology 22 (2012) 234– 249
Contents lists available at SciVerse ScienceDirect
Seminars in Cancer Biology
j ourna l ho me p ag e: www.elsev ier .com/ locate /semcancer
eview
olecular networks that regulate cancer metastasis
aniela Spanoa,b,1, Chantal Heckc,1, Pasqualino De Antonellisa,b, Gerhard Christofori c, Massimo Zolloa,b,∗
CEINGE, Biotecnologie Avanzate, Naples, ItalyDepartment of Biochemistry and Medical Biotechnology (DBBM), ‘Federico II’ University of Naples, Naples, ItalyInstitute of Biochemistry and Genetics, Department of Biomedicine, University of Basel, Basel, Switzerland
r t i c l e i n f o
eywords:nvasionmoeboidesenchymal
ymphogenicntravasationxtravasationicroenvironmentetastatic outgrowth
a b s t r a c t
Tumor metastases are responsible for approximately 90% of all cancer-related deaths. Although manypatients can be cured, in the US and UK, cancer still causes 730,000 deaths every year, and it is secondonly to cardiovascular disease as a cause of death. The functional roles of many critical players involved inmetastasis have been delineated in great detail in recent years, due to the draft of the human genome andto many associated discoveries. Here, we address several genetic events and critical factors that definethe metastatic phenotype acquired during tumorigenesis. This involves molecular networks that promotelocal cancer-cell invasion, single-cell invasion, formation of the metastatic microenvironment of primarytumors, intravasation, lymphogenic metastasis, extravasation, and metastatic outgrowth. Altogether,
these functional networks of molecules contribute to the development of a selective environment thatpromotes the seeding and malignant progression of tumorigenic cells in distant organs. We include herecandidate target proteins and signaling pathways that are now under clinical investigation. Althoughmany of these trials are still ongoing, they provide the basis for the development of new aspects inthe treatment of metastatic cancers, which involves inhibition of these proteins and their molecularnetworks.. Introduction
Cancer is still a major health problem around the world, despitehe progress that has been made toward reducing its incidence and
ortality rates, and toward improving the survival of the patientsffected. Metastasis formation, which defines the ability of cancerells to spread to distant organs in the body, is responsible for morehan 90% of cancer-associated deaths [1–3].
To date, the observations made by the English surgeon Pagetrovide perhaps the most appropriate definition of cancer andetastasis: “Organ-specific metastases are due to the dependence
f the seed (the cancer cell) on the soil (the secondary organ)” [4].hen, the American pathologist James Ewing provided one of theariety of further descriptions, noting that, “circulatory patternsetween a primary tumor and specific secondary organs are suffi-
ient to account for organ-specific ‘metastasis”’ [5]. In other terms,e said “both mechanical factors and seed-soil compatibility fac-ors, contribute to the ability of specific types of cancer to spread∗ Corresponding author at: CEINGE Biotecnologie Avanzate, Via Gaetano Salvatore86, 80145 Naples, Italy. Tel.: +39 081 3737875.
E-mail addresses: [email protected], [email protected] (M. Zollo).1 The first two authors contributed equally to the study.
044-579X/$ – see front matter © 2012 Elsevier Ltd. All rights reserved.ttp://dx.doi.org/10.1016/j.semcancer.2012.03.006
© 2012 Elsevier Ltd. All rights reserved.
to various target organs, and the initial delivery and arrest of can-cer cells to specific organs seems to be primarily ‘mechanical”’ [5].Thus, once cells have been ‘seeded’ to an organ, their subsequentgrowth will depend on the compatibility of the ‘seed’ and the ‘soil’that they encounter in the target organ.
It is now known that the formation of a metastasis is anextremely complex, multistep and multifunctional biological event.This results from a complex molecular cascade through which can-cer cells leave the site of the primary tumor and disseminate todistant anatomical sites, where they can proliferate and form sec-ondary tumor foci. A metastasis arises through a cascade of events,all of which are interconnected through a series of adhesive inter-actions and invasive processes, as well as responses to chemotacticstimuli. This cascade of events includes: the development of newblood vessels; the ‘escape’ of tumor cells from the primary tumor;the invasion of and the migration through the basement membrane(BM) and extracellular matrix (ECM) surrounding the tumor epithe-lium; the invasion of the BM supporting the endothelium of localblood and/or lymphatic vessels; the intravasation of the tumor cellsinto the blood and/or lymphatic vessels; the adhesion of the circu-
lating tumor cells to the endothelium of capillaries of the targetorgan site; the invasion of the tumor cells through the endothelialcell layer and the surrounding BM (extravasation); the growth ofsecondary tumors at the target organ site.
Cancer
mcnnuatn
am
1
ccmntscdiftcTFmm[
dsmttsmGtitrr[
1
leso
1
pepTrdl
D. Spano et al. / Seminars in
It is now known that to establish a secondary tumor focus aetastatic tumor cell needs to successfully complete this entire
ascade of events. Many aspects of the molecular interactionetworks underlining these cascades have been defined throughumerous studies, although a full understanding of these molec-lar mechanisms and of the hierarchical networks of connectionswaits further studies. There is no doubt that the full unraveling ofhese events represents an important issue for the development ofew therapeutic agents that can fight cancer metastasis.
This review focuses on the key molecules and molecular inter-ctions involved in the cascade of events that culminate in canceretastasis.
.1. Local cancer-cell invasion
The migratory and invasive abilities of cancer cells are theritical parameters of the metastatic cascade. The majority ofancers originate from epithelial tissues, and to leave the pri-ary tumor and invade the surrounding tissue, these tumor cells
eed to remodel their tight cell–cell and cell–matrix adhesiono gain migratory capabilities, and thus to invade adjacent tis-ues [6,7]. These initial steps involve various cell strategies thatan be classified according to histological criteria, into two fun-amentally different patterns of cancer-cell invasion: single-cell
nvasion, and collective cell invasion [8,9]. These strategies haveundamental differences in their extracellular protease activi-ies, integrin-mediated cell–matrix adhesion, cadherin-mediatedell–cell adhesion, cell polarity, and cytoskeletal arrangements.hese factors thus define the type of cell migration and invasion.inally, stromal cells can contribute to the different types of celligration, such as stromal fibroblast leader cells in collective celligration, and macrophage pioneer cells in single-cell migration
10].In cancers, the various types of cell migration can be found to
ifferent degrees and in different mixes. For example, at the inva-ive front, colorectal cancer cells disseminate as solitary, activelyigrating cells, and once they have reached their target organ,
hey re-differentiate to form secondary tumors with a phenotypehat is comparable to that of the primary tumor [11]. In contrast,quamous cell carcinomas invade predominantly by collective celligration, with cone-shaped or sheet-like invasion fronts [12].enerally, cancer cells use morphogenic developmental programs
o control their migratory and invasive abilities. These processesnvolve the dramatic reorganization of the actin cytoskeleton, andhe concomitant formation of the membrane protrusions that areequired for cell motility in a complex three-dimensional envi-onment: the lamellipodia, filopodia, podosomes, and invadopodia13].
.2. Single-cell invasion
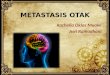
Single-cell migration and invasion can be identified in histo-ogical sections by isolated and scattered tumor cells that haventered the surrounding tissue. Cancer cells can follow two distincttrategies to migrate as single cells: fibroblastoid (mesenchymal)r amoeboid patterns (Fig. 1).
.2.1. Mesenchymal migrationIn most cases, single cells that leave a primary tumor at its
eriphery migrate through a mechanism that involves the loss ofpithelial polarity and the achievement of a mesenchymal mor-hology through the epithelial to mesenchymal transition (EMT).
his is a process that is currently a major focus in metastasisesearch [14–16]. The essential characteristics of EMT are theisruption of tight cell–cell contacts, and the acquisition of a fibrob-astoid spindle-shape morphology, with increased invasiveness
Biology 22 (2012) 234– 249 235
and cell–stroma interactions, as well as slower rates of cell divi-sion; altogether, these can result in the release of single cells froma solid epithelial tumor.
Mesenchymal cell migration is not only used by cancer cells,as it is also seen with normal untransformed cells, such as fibrob-lasts, and endothelial and smooth muscle cells. This is based oncellular movement that is driven by the leading edge, where thereare Rac-induced cell protrusions and there is the formation of afocalized actin cytoskeleton and stress fibers. These spindle-shapedcells can remodel their ECM by proteolytic reorganization andslow turnover of integrin-mediated focal adhesions, which resultsin relatively slow cell migration velocities of 0.1–1.0 �m/min[17,18].
The actual occurrence of EMT in patients is still debated,although with more detailed molecular and histopathological anal-yses and the discovery of novel markers, there is increasingevidence for EMT in various human cancers [19–21]. As theseinvading cells acquire more mesenchymal traits, it becomes moredifficult for the pathologist to distinguish them from the mes-enchymal cells surrounding a tumor. Nevertheless, there is moreand more evidence that at least to some extent, EMT has a rolein cancer-cell metastases. Indeed, the expression of vimentin, amesenchymal marker, in epithelial cells of breast tumors cor-relates with a shorter post-operative survival of patients [22].Furthermore, nuclear �-catenin, which is another characteris-tic of EMT, is seen to be distributed along the invasive frontin colorectal cancer cells, but not in the center of the tumor[23].
The highly invasive metaplastic and claudin-low subtypes ofbreast cancer have both been reported to have EMT attributes,such as attenuated E-cadherin expression, as well as elevated lev-els of the EMT-inducing transcription factors Twist and Slug [24].These data suggest that EMT is an important process that needs tobe dissected apart so that we can decode the mechanisms under-lying single-cell migration and invasion in cancers. The currentknowledge of the molecular regulation of EMT and of its func-tional contributions to metastasis are summarized by Tiwari andcollaborators in this issue (Tiwari et al., 2012).
1.2.2. Amoeboid migrationSome cell types, such as circulating stem cells, leukocytes and
tumor cells of hematopoietic origin, have a more diffuse structure oftheir actin cytoskeleton, and use more short-lived and less adhesivecell–matrix interactions [8]. This fast-gliding manner of migrationis not highly dependent on integrins and focal contact formation,and also not on proteolytic activities. This movement is mainlydriven by RhoA/ROCK-mediated bleb-like protrusions with activemyosin–actin contractions, and the cells ‘squeeze’ through gaps inthe ECM. The low adhesion attachment to the ECM allows thesecells to move with high speed in a three-dimensional environment[25].
Of note, the amoeboid and mesenchymal types of migration aremutually interchangeable. Suppression or increase of the activityof the molecular pathways underlying either of these modes cancause a switch to the other type of migration. This change is knownas amoeboid–mesenchymal transition or mesenchymal–amoeboidtransition. These transitions are triggered by rapid alterations inthe migratory mode that arise in response to the local microen-vironment, and they might have roles in different stages of themetastatic process, when a specific environment requires suchan adaptation of the tumor cells [25,26]. The molecular networksdefining the differences between mesenchymal and amoeboid cell
migration are currently being delineated. Specifics in the activa-tion of RhoA and Rac that directly impact on mesenchymal andamoeboid migration have been recently identified by functionalsiRNA screening against RhoGEFs and RhoGAPs [27]. The RhoGEF
236 D. Spano et al. / Seminars in Cancer Biology 22 (2012) 234– 249
Fig. 1. Cancer cell migration. Single amoeboid migration does not involve significant cell–matrix adhesion and proteolytic activity, and no cell–cell adhesion at all. Migrationis achieved by cortical-actin-dependent blebbing of the membrane and by cytoplasmic streaming and squeezing through the matrix. Single-cell mesenchymal migration, assolitary cells or in Indian files, relies on integrin-mediated cell–matrix adhesion and cortical actin and stress fibers, but not on cadherin-mediated cell–cell adhesions. Duringmesenchymal migration, a track is generated for the following cells by proteolytic digestion of the matrix. Collective cell invasion shows various multi-cellular organizationand structures. Migrating clusters or cohorts of cells separate from their originating tissue. The cells are connected to each other by E-cadherin-mediated cell–cell junctions,and the leader cells provide the migratory traction and proteolytic digestion of the matrix, to digest a path for the following cells. Strand or sheet-like invasion usually occurswhen cells of the invading tumor front do not separate from the primary tumor. These invasive fronts are characterized by migratory leader cells that are connected totheir neighbors by E-cadherin-mediated adhesion and that provide the migratory traction and the proteolytic activity to collectively move through the matrix. In branchingmorphogenesis of the mammary epithelial duct, the leading cells migrate and dissolve the matrix by proteolysis. The following cells are connected by E-cadherin-mediatedadhesions and form a tube-like structure with a basal lamina and a lumen. Vascular sprouts occur during angiogenesis, when new blood vessels form by sprouting andb herin
m
A
DarthRatRdttldRpnccRrm
mTi
ranching. Endothelial cells are connected to each other by vascular endothelial cadatrix.
dapted from [9].
ock3 and the adaptor protein NEDD9 are required for Rac GTPasectivity, and thus for mesenchymal cell movement. Activated Racepresses the phosphorylation of myosin light chain 2 via WAVE2,hereby blocking amoeboid (Rho-mediated) motility. On the otherand, RhoA signaling activates its effector kinase ROCK and theacGAP ARHGAP22, which leads to repression of Rac activitynd thus to mesenchymal motility. Also, the amoeboid migra-ion of A375 melanoma cells in three-dimensional culture requiresOCK-mediated actin–myosin contraction [28]. Phosphoinositide-ependent protein kinase 1 (PDK1), as a protein rather thanhrough its kinase activity, together with RhoA-GTP is requiredo localize ROCK to the plasma membrane, where it phosphory-ates myosin light chain and induces cell motility. PDK1 therebyirectly outcompetes RhoE for binding to ROCK and abolishes thehoE negative regulation of ROCK. Of note, these data link phos-hoinositide 3-kinase (PI3K) signaling and RhoA activity via thison-catalytic function of PDK1. Finally, ablation of cofilin functiononverts amoeboid migrating cancer cells into mesenchymal-typeells [29]. Thus, there are a number of mechanisms through whichhoA and Rac appear to be antagonistically regulated, which canesult in stimulation of either amoeboid or mesenchymal celligration.
An additional level of control of these migration processesight occur within cells that have acquired a migratory phenotype.hese cells are mainly influenced by protein–protein interact-ng networks of actions, which together influence migratory cells
(VE-cadherin) and maintain a lumen, while one tip cell guides the way through the
and might explain these acquired properties. Some explanationsmight involve the actions of metastasis-suppressor genes and theirinteracting proteins (e.g. the role of nm23-H1; h-prune; glyco-gen synthase kinase 3-� [GSK-3�] and ASAP-1 [30–33]). The rolesof these binding partners have been proposed as influencing thepro-motility phenotype as part of a major larger complex, thusinfluencing the migratory properties of breast, pancreas and coloncancer cells. H-prune was originally described as an inhibitor of thenm23-H1 metastasis-suppressor protein, which is present in thismajor complex upon phosphorylation by casein kinase I [30] (forreview on nm23-H1, see [33]). H-prune influences the cAMP poolsin the cell by changing the physiology into a pro-motility acquiredphenotype, which counteracts the nm23-H1 anti-motility function.Then H-prune brings an additional protein partner into the com-plex: GSK-3�. This event makes the cell prone to the acquisitionof new cellular properties, which further delays the disassem-bly of paxillin and regulates the disassembly of focal adhesionsin a cooperative action with GSK-3� [31]. Other protein partnersof the major protein complex including h-prune are now underinvestigation, including ASAP-1 and a multi-domain adaptor pro-tein, ADP-ribosylation factor (Arf); the latter two are myristoylatedsmall GTPases that regulate membrane trafficking and cytoskele-
tal organization [32]. Taken together, these intrinsic and extrinsiccellular properties are all linked to the remodeling of the actincytoskeleton, which has a central role in defining the mode of cellmotility.
Cancer
1
cootcsvmdccEmtoThscflt[
otPalskdapgcpp[ol[bapo
hptdtcrisi[odp
c
D. Spano et al. / Seminars in
.3. Collective cell migration
In contrast to individual cell migration, collectively migratingells retain their cell–cell junctions through continuous expressionf adhesion molecules, and they migrate as sheets, strands, tubesr clusters. They can also remain either connected to the primaryumor (coordinated invasion) or move as detached cell groups orlusters (cohort migration) (Fig. 1). This type of migration is mainlyeen for basal cell carcinomas and squamous cell carcinomas ofarious origins [34,35]. As with single invasive cells, collectivelyigrating cells form membrane protrusions like ruffles and pseu-
opodia, and they form integrin-mediated focal adhesions that areonnected to the actin cytoskeleton. These collectively migratingells apply pericellular proteolysis to generate a path through theCM scaffold, and they use actin–myosin contraction for cell move-ent [36]. Collectively migrating cells do not retract their cellular
ails, but instead exert mechanical forces, such as moving by pullingn adjacent cells that are connected by adhesion junctions [18].his clustered cohort-like cancer cell dissemination appears to beighly efficient in embolizing lymphatic or blood vessels and in cellurvival in the circulation [37]. To penetrate the ECM, the leadingells generate an invasion path by the use of �1-integrin-mediatedocal adhesions and local expression of MT1-MMP (MMP14) at theireading edges, to cleave the collagen fibers and to orient them inube-like structures in which the following cell mass can migrate38,39].
Studies in several laboratories have detected the expressionf podoplanin (T1�-2, aggrus, gp36) in the outer cell layer ofhe invading front of collectively migrating cancer cells [40,41].odoplanin is a small transmembrane glycoprotein, which is usu-lly expressed on kidney podocytes, alveolar type I cells, andymphatic endothelial cells, among others [12]. Forced expres-ion of podoplanin in epithelial breast cancer cells and in humaneratinocytes induces cell migration and invasion, with filopo-ia formation in the absence of a loss of E-cadherin expressionnd with the gain of mesenchymal markers [41,42]. Moreover,odoplanin-expressing A431 squamous cell carcinoma cells havereater tumorigenicity when they are transplanted into immuno-ompromised mice, as compared to A431 cells not expressingodoplanin, and the resulting tumors show collective invasion withodoplanin expression in the outer cell layer of the invading front43]. Similarly, transgenic expression of podoplanin in tumor cellsf the Rip1Tag2 mouse model of pancreatic �-cell carcinogenesiseads to the formation of invasive carcinomas in the absence of EMT41]. These data indicate that cell adhesion and spreading inducedy podoplanin expression depend on the activity of �1-integrinnd on the assembly of functional focal adhesion plaques. Thus,odoplanin can induce collective cell invasion, even in the absencef EMT.
In contrast, the forced expression of podoplanin in MDCK cellsas been reported to induce cell motility and invasion in theresence of full EMT, with the loss of E-cadherin expression andhe gain of N-cadherin expression [44]. This activity appears toepend on the juxtamembrane RK dipeptide that is present inhe short C-terminal domain through which podoplanin asso-iates with ezrin and moesin. Both ezrin and RhoA function areequired for podoplanin-induced EMT, and their interactions resultn elevation of RhoA GTPase activity. In addition, the forced expres-ion of podoplanin in MDCK and MCF7 cells leads to a markedncrease in phosphorylation of ezrin in a RhoA-dependent manner41,44]. Thus, ERM proteins can link podoplanin expression to thesebserved rearrangements of the actin cytoskeleton, although the
etailed mechanisms and signaling pathways by which podoplaninromotes collective tumor cell invasion remain to be elucidated.Collective cancer cell migration might depend on guiding theancer cells or stromal cells to find a way through the ECM. Indeed,
Biology 22 (2012) 234– 249 237
leader cells have been identified in cell cultures as cells that havea distinct morphology and a highly polarized cell shape, and theyshow the formation of lamellipodia [45]. These leader cells appearto connect with their neighboring cells by E-cadherin-mediatedjunctions, and when they invade the surrounding tissues, theyappear to ‘drag’ their neighbor cells with them. Moreover, in co-culture experiments with carcinoma cells and stromal fibroblasts,the fibroblasts appear to take the lead and prepare the migratorytracks for the migrating carcinoma cells, through proteolytic diges-tion and migration-force-mediated remodeling of the ECM [46].Such stromal support appears to be mainly required for cancer cellsthat retain their epithelial organization during collective invasion,while mesenchymal invasive cells either lead themselves or relyon tumor-associated macrophages (TAMs) or other inflammatorycells to guide their way through the tumor microenvironment, andto support their entry into the vasculature.
1.4. The metastatic microenvironment in primary tumors
The metastatic capabilities of cancer cells not only depend oncell-autonomous genetic and epigenetic alterations, but also onchanges and adaptation in the tumor microenvironment. A tumoris composed not only of cancer cells, but also of a large varietyof other cell types, including fibroblasts, resident epithelial cells,pericytes, myofibroblasts, vascular and lymphovascular endothe-lial cells, and infiltrating cells of the immune system. Together withthe ECM, these non-malignant cell types constitute the stromal tis-sue of a tumor. The tumor composition is highly dynamic, bothspatially and temporally [47,48]. An overview of the cell types inthe tumor microenvironment and their functions in the promotionof tumor progression and metastatic dissemination was given bySpano and Zollo [49]. However, it is reasonable that during earlytumorigenesis, the first cells that are recruited by an incipient neo-plasia are fibroblasts, as these represent the main constituent ofstromal tissue. These cancer-associated fibroblasts (CAFs) have afundamental role in the secretion of factors that act on tumor cellsin both paracrine and autocrine fashions, which can result in a moreaggressive cancer phenotype. Across most cancers, activated CAFssecrete a wide variety of growth factors, chemokines, collagens, andmatrix-modifying enzymes, which collectively supply a communi-cation network and an altered three-dimensional ECM scaffold thattogether govern proliferation of cancer cells, and tumor invasionand metastasis across tissue types [49,50]. For example, in breastcancer, CAFs have been shown to initiate and mediate tumorige-nesis through a macrophage-recruitment inflammatory signaturethat is highly dependent on breast CAF nuclear factor-�B signal-ing [51]. As a comprehensive signaling axis, the IL-1�/IL-1 receptor1 (IL-1R1) activates a defined set of downstream signaling effec-tors and binding partners [52]. The IL-1R1 axis effectors includeseveral isoforms of the IL-1 receptor-associated kinases (IRAKs), aswell as protein–protein interaction effector tumor necrosis factor-� receptor-associated factor 6 [53–55]. Nuclear localization ofIRAK-1 has been correlated with enhanced malignancy in lungcancer [56] and prostate cancer, and it has been shown to binddirectly to the I�B� promoter and enhance the binding of NF-�Bp65.
Over the past few years, transgenic mouse models of cancerhave been instrumental in the unraveling of the complex inter-play between tumor cells, infiltrating leukocytes, CAFs, and thetumor blood and lymphatic vasculature. Bone-marrow transplanta-tion in combination with genetic or pharmacological manipulationsof gene functions in mice has revealed that most immune cell
lineages can have both anti-tumorigenic and pro-tumorigenicfunctions, and that established tumors push immune cells intoa pro-angiogenic, immuno-suppressive and pro-malignant state[47].
2 ancer
socsMacapaodaia
cinaiealpCapaLkCtiboaiptiat[
slRpf[itttwfcIpares(
38 D. Spano et al. / Seminars in C
Within the tumor microenvironment, the tumor cells secreteeveral cytokines, which modulate the recruitment and functionf the stromal cells. In particular, the tumor-derived RANTES/CCL5ytokine stimulates CAFs to externalize the S100A4 protein, whichtimulates tumor-cell survival and migration, up-regulation of theMPs, down-regulation of tissue inhibitors of the MMPs (TIMPs),
ctivation of the NF-kB and MAP kinase pathways, infiltration of Tells, and finally, up-regulation of RANTES [57–60]. This thus gener-tes a signal amplification loop. CAFs secrete monocyte chemotacticrotein 1 (MCP1/CCL2) and stromal-cell-derived factor 1 (SDF1),lso known as CXCL12, which are involved in the recruitmentf myeloid-derived suppressor cells (MDSCs) and TAMs. Tumor-erived stem cell factor (SCF) promotes the recruitment andctivation of mast cells, which induce proliferation, migration andnvasion of cancer cells, promote degradation of the ECM, inducengiogenesis, and recruit and modulate MDSC function.
At the tumor site, all of these immune cells secrete severalhemokines and cytokines which generate an inflammatory andmmuno-suppressive state which critically contributes to malig-ant tumor progression. Between the secreted chemokines, thebove-mentioned CCL2 strongly contributes to the recruitment ofmmune inflammatory cells. CCL2 has been shown to be over-xpressed in a wide variety of cancer types. As also indicatedbove, it is a potent chemoattractant for monocytes, memory Tymphocytes, and natural killer cells, and it stimulates tumor cellroliferation, migration and invasion [61]. The important role ofCL2 in cancer biology suggests that this chemokine is a useful ther-peutic target in cancer treatment. Recent studies have describedroof-of-concept animal models with the use of human or mousenti-CCL2 antibodies, or combinations of both, to block PC-3M-uc2 prostate cancer and 4T1-Luc breast cancer cells, which arenown to develop metastases [62–65]. MCP-1 and its receptorCR2 have been previously and successfully targeted using generansfer, an MCP-1-neutralizing antibody, and a CCR2 antagonistn rodent models [64,66]. Recently, a small molecule, known asindarit that can inhibit CCL2 synthesis and/or secretion was devel-ped. This molecules is an anti-inflammatory indazolic derivative,nd it has been shown to inhibit the synthesis of a subfamily ofnflammatory chemokines, including MCP-1/CCL2. Through theseroperties, bindarit might have a potential inhibitory function inumor progression and metastasis formation [67]. In vitro andn vivo studies performed on both breast and prostate cell linesnd on xenograft animal models were carried out in our labora-ory, to address the clinical potential of bindarit in cancer therapy68].
Among the other chemokines and cytokines secreted at tumorites by immune cells, SDF1, a potent chemoattractant for endothe-ial cells, and the chemokines CCL2, CXCL8, CXCL1, CXCL13 andANTES contribute to neoangiogenesis [69]. CCL17 and CCL22referentially attract T-cell subsets that are devoid of cytotoxicunctions, such as regulatory T (Treg) cells and Th2 lymphocytes69]. CCL18 recruits naïve T cells which induce T-cell anergy, whichs the mechanism responsible for the inability of an immune T cello mount a complete response against its target [70]. Within theumor microenvironment, the immuno-suppressive milieu is fur-her enhanced by production of interleukin (IL)-10, which togetherith the IL-4, IL-6 and IL-13 cytokines induces monocyte dif-
erentiation toward a mature M2-polarized phenotype that isharacteristic of TAMs. Moreover at the tumor site, the IL-1� andL-6 cytokines [71], the S100A8 and S100A9 pro-inflammatoryroteins [72,73], the chemoattractant molecules CCL2 [74], SDF1nd CXCL5 [75] are the main factors that are responsible for the
ecruitment and the induction of MDSCs. The angiogenic vascularndothelial growth factor (VEGF) is one of the main factors respon-ible for the expansion of MDSCs [76], while IL-4, IL-13, interferonIFN)-�, IL-1� and transforming growth factor-� (TGF-�) turnBiology 22 (2012) 234– 249
on their suppressive functions. In the tumor microenvironment,MDSCs produce high levels of IL-17, which further exacerbatesthe inflammatory tumor microenvironment. IL-17 leads to the up-regulation of IL-9, IL-10, IL-13, CCL17, CCL22, CD39 and CD73.This results in various actions: CCL17 and CCL22, in turn, arechemoattractants that bring more Treg cells to the tumor sites;CD39 and CD73 enhance the suppressor function of Treg cells; IL-9 produced by Treg cells helps to maintain the survival of mastcells, which further contribute to the establishment of inflamma-tory and immuno-suppressive conditions at the tumor site, bysecretion of pro-inflammatory and immuno-suppressive cytokinesand chemokines [77–79]. Finally IL-10 and IL-13 induce MDSCsimmuno-suppressive function.
In this tumor microenvironment, the high levels of pro-inflammatory cytokines can induce actomyosin contractility instromal fibroblasts, for example through signaling via the recep-tor subunit GP130-IL6ST, the tyrosine kinase JAK1, and Rho-kinase[27]. Stromal fibroblasts, in turn, remodel the ECM by secretinglarge amounts of collagen types I and III, tenescin C (TNC) andMMPs, and they create tracks for collective migration of squa-mous carcinoma cells. On the other hand, cytokine signaling caninduce actomyosin contractility in individual melanoma cells, sothey migrate in a rounded, ‘amoeboid’ mode. Hence, cytokine sig-naling pathways can induce actomyosin contractility, and thus cellmigration in both stroma and tumor cells [27].
A plethora of recent reports have painted a consistent pictureof how the stromal cells (CAFs and inflammatory cells, such asTAMs, MDSCs and mast cells) can promote tumor malignant pro-gression. Indeed, within the primary tumor microenvironment, thestromal cells provide potent oncogenic signals, such as TGF-�, hep-atocyte growth factor (HGF) [80], epidermal growth factor (EGF)[81,82], Wnt [83,84], and bFGF [85], which stimulate cancer-cellproliferation, survival and invasion, thus facilitating metastasis.Moreover these cells produce several angiogenesis-modulatingenzymes, such as VEGF, thymidine phosphorylase, MMP2, MMP7,MMP9, MMP12, cyclooxygenase-2 (COX-2), urokinase plasmino-gen activator (uPA), and cathepsins B and D [86,87], which togetherdegrade the ECM, thus again promoting metastasis.
However, these effects are highly pleiotropic, in that they donot exclusively affect a single step of the metastatic cascade.For example, the EGF and Wnt signaling pathways induce bothcancer-cell proliferation and motility [81,83,84]. Again changes inthe extent and quality of tumor angiogenesis will have an effecton primary tumor growth, tumor-cell survival, and intravasation;alterations in cancer-cell migration will affect intravasation, andthe blockade of an anti-tumor immune response will promoteall of the stages of tumor metastasis. Another example of suchpleiotropic activities is histidine-rich glycoprotein (HRG), whichrepresses tumor growth and metastasis by pushing macrophagesfrom an M2-tumor-promoting to an M1-tumor-inhibiting pheno-type. With the reduction in the pro-angiogenic factors suppliedby M2 macrophages, tumor vessels are less leaky and permeable(they are ‘normalized’), and cancer cell intravasation and metastaticdissemination is reduced [88]. On the other hand, the loss of E-cadherin-mediated cell–cell adhesion, and with it, the inductionof cancer-cell EMT, goes along with increased tumor angiogenesis,cancer-cell invasion, intravasation and metastasis [89]. More-over, intracellular oncosuppressor miRNAs that regulate EMT haveimportant roles in the definition of the capabilities of tumor cells.For example, by targeting the novel pro-angiogenic genes IGFBP2,PITPNC1 and MERTK, miR-126 represses the specific recruitmentof endothelial cells to cancer cells, and thus inhibits angiogenesis
and metastasis [90]. As another example of the pleiotropic activ-ities that underlie the metastatic process, miR-30b/30d repressesthe expression of the GalNAc transferase GALNT7, which leads toincreased expression of the immune-suppressor IL-10, and hence
Cancer
t[Nn
1
tppmpp
uoapoiarr“ir
aatistotd
tiiawftaCoa
aMIaPawosrdp[sHa
D. Spano et al. / Seminars in
o reduced immune-cell activation and increased tumor metastasis91]. This example is overridden by others that show that miR-As expression and target regulation can control the molecularetworks of cancer metastasis [92].
.5. Tumor immune escape
Once recruited into the tumor microenvironment, inflamma-ory cells of the immune system can contribute to the malignantrogression of cancer cells. This thus leads them to establish a com-lex network of interplay that contributes to the promotion andaintenance of an immuno-suppressive environment, which itself
romotes immune escape, and as a consequence, enhances tumorrogression.
One hypothesis to explain immune escape is the “law of nat-ral selection”. This hypothesis suggests that under the pressuref the immune system, only the cancer cells that have geneticnd epigenetic traits that are beneficial to their survival and/orroliferation will have a growth advantage over other cells. Theutcome of this passive process is determined by multiple factorsn the tumor environment, such as growth factors, nutrient supplynd immune pressure. Genomic instability simply creates a vastepertoire of tumor cells that will be selected according to envi-onmental factors. Therefore, terms such as “tumor evasion” ortumor escape” become misnomers, because evasion and escapemply active acquisition of certain characteristics or phenotypes,ather than the differential propagation of tumor subclones.
At present, we can categorize the tumor immune escape mech-nisms into two major types. One category of escape mechanism isctive at the level of tumor cells and can be ascribed to defects inhe expression of major histocompatibility complex (MHC) class I,n the processing of MHC class I restricted antigens, or in the pre-entation machinery of the antigens. These abnormalities might behe result of the activation of oncogenes within tumor cells, withne example seen in Her2/Neu-transformed cells, which enablesumors to take on a ‘stealth’ phenotype and thus to hide frometection by cytotoxic T lymphocytes [93].
The second category of immune escape mechanism arises fromhe ability of the progressing tumor to interfere with the hostmmune system. To this end, and as mentioned above, the tumornduces and/or recruits immuno-suppressive cells, such as TAMsnd MDSCs, which normally serve as safeguards against over-helming inflammation or autoimmunity. Immune activation and
unction can be hampered by a lack of appropriate co-stimulation,he presence of immuno-suppressive cytokines (e.g. VEGF, IL-10nd TGF-�), and the impact of immunoregulatory cells such asD4+CD25+ T cells and natural-killer (NK) cells. Therefore the fatef tumors might be dictated by the net effect of immune activationnd immune inhibition.
The dual functions of IL-10 and IFN-� in antitumor immunitynd immunoregulation have been recognized for some time [94].umm et al. [95] showed that host IL-10 and exogenous pegylated
L-10 (PEG-IL-10) can promote CD8+ T-cell control of developingnd established tumors, respectively. These findings show thatEG-IL-10 increases CD8+ T-cell numbers in large transplantednd spontaneous tumors and reduces the tumor size. It is unclearhether PEG-IL-10 increases T-cell infiltration or increases survival
r proliferation of T cells in the tumor. Data that show suppres-ion of large HER2-driven mammary cancers by PEG-IL-10 are quiteemarkable for a single therapy. In correlation with this, PEG-IL-10irectly induces granzymes and IFN-� in CD8+ T cells and antigenresentation indirectly via CD8+ T-cell-derived IFN-�. Mumm et al.
95] also showed that IL-10 expression correlates with the expres-ion of granzymes, IFN-�, and MHC molecules in human tumors.owever PEG-IL-10 might not use an immune escape mechanisms therapy for tumors that lack responsiveness to IFN-�.Biology 22 (2012) 234– 249 239
Another immune escape mechanism of interest was describedby Watkins et al. [96], who identified Foxo3 as a master regula-tor of the tolerogenic program in tumor-associated, plasmacytoiddendritic cells (TApDCs or TADCs). Foxo3 enables TADCs to inducetolerance in tumor antigen-specific CD8+ T cells, turning theminto regulatory lymphocytes that can inhibit nearby CD8+ T lym-phocytes. They showed that siRNAs against Foxo3 abrogate theability of human and mouse TADCs to induce suppressive activ-ity by T cells, diminish the expression of tolerogenic mediators,such as indoleamine-2,3-dioxygenase, arginase, and TGF-�, andup-regulate the expression of co-stimulatory molecules and proin-flammatory cytokines.
By turning the host immune system against itself, tumors cangain an impressive arsenal of weapons to hamper the induction andprogression of this anti-tumor immune activity.
1.6. Intravasation
The process of intravasation of cancer cells into the blood streamor the lymphatic system is a logical requirement for metastatic dis-semination of cancer cells in the body. Tumor cells must traverseany BM surrounding the vessel. This is achieved through adhesiveinteractions between the tumor cells and the BM endothelial cells,and through integrin-mediated interactions and dissolution of theBM by proteolytic enzymes. Most studies indicate that cancer cellsactively migrate and invade, to disseminate throughout the bodyand seed metastasis. However, in this context, we should not ignorethe possibility that cancer cells might be able to leave the primarytumor and disseminate by a passive mechanism, such as the dis-placement of single tumor cells or clusters of tumor cells into theblood or lymphatic circulation, and their subsequent disseminationand outgrowth at distant sites [97].
What is the evidence for such passive dissemination? First,as most of the many cancer cells that enter the blood stream(3–4 × 106 cells/g tumor) do not survive [97,98], it is likely thatthese cells have not been programmed to be fully metastatic, andmight have been passively shed into the blood stream. Althoughthe rate of disseminating tumor cells increases with primary tumorsize, the shedding of malignant cells can already occur in the earlystages of a tumor [3,99]. Indeed, metastatic outgrowth can beuncoupled from cancer-cell dissemination: non-transformed cellshave been found to disseminate to the lungs via the blood streamand survive there for unexpectedly long periods of time. Only whentransformed by inducible expression of oncogenes will these cellsgrow macroscopic metastases [100]. In a similar manner, tumorcells have been shown to disseminate systemically from the earli-est epithelial alterations in transgenic breast cancer mice and fromductal carcinomas in situ in women [101].
Secondly, based on molecular and genetic marker analysis, pas-sive displacement of cancer cells into the blood stream has beenproposed [52,97]. In particular, detailed analysis of lymph nodesand bone marrow of esophageal cancer patients have revealed thatprimary tumors and cancer cells in the circulation diverge for mostgenetic aberrations, which indicates the high heterogeneity in dis-seminating cancer cells [102].
Thirdly, tumor blood vessels are highly abnormal and havehigh permeability and leakiness [103]. Tumor growth requiresongoing remodeling of the environment, including blood vessels,and together with pushing forces the confined space can collapseblood vessels and allow cells to enter the blood vessels or lym-phatic vessels. Conversely, forced tumor vessel normalization hasbeen shown to repress tumor metastasis [88]. Moreover, ongoing
angiogenesis and the subsequent increase in microvessel density,together with the presence of inflammatory sites, facilitate invasivetumor cells for intravasation and disseminate through the bloodstream.
2 ancer
ceac[ot(EostttimabthipmbsciCcernosmtmiMOsmmstrp
UdievTs
ttnspit
s
40 D. Spano et al. / Seminars in C
In contrast to a mechanism of passive displacement of can-er cells into the bloodstream, the tumor microenvironment canncourage cancer-cell migration and intravasation by the gener-tion of gradients of cytokines and/or by pioneer cells guidingancer cells toward blood vessels and aiding in their intravasation104]. In this scenario, the microenvironment-controlled migrationf breast carcinoma cells toward blood vessels has been reportedo depend on the secretion of EGF by colony stimulating factorCSF) receptor-expressing macrophages and the CSF1 release ofGFR-expressing mammary tumor cells [47,82,105]. The secretionf CXCL12/SDF1 at a tumor site can enhance the invasion, intrava-ation, metastasis formation and recruitment of macrophages tohe primary tumor. This enhancement of invasion and intravasa-ion depends upon CXCR4 signaling, and it is most likely to occurhrough activation of CXCR4 on macrophages, which results inncreased paracrine interactions with tumor cells in the tumor
icroenvironment. Increased CXCL12 secretion also gives rise ton increased microvessel density, which might also be mediatedy TAMs and might contribute to an altered tumor architecture,hus resulting in increased intravasation through the presence of aigher density of entrance sites into the blood, with a correspond-
ng increase in the formation of metastases [106]. Moreover thearacrine loop that involves CXCR4/CXCL12 signaling in the tumoricroenvironment is needed for EGF-induced in vivo invasion in
reast cancer tumors [106]. The significance of CXCL12/CXCR4ignaling in breast cancer invasion and metastasis is widely appre-iated. CXCR4 expression in breast cancer cells has been shown toncrease metastasis by homing of tumor cells to sites of increasedXCL12 expression, such as the lymph nodes [107]. Recently, theontribution of the CXCL12 orphan receptor CXCR7 to the tumornvironment introduced a new level of complexity within theealm of chemokine/chemokine-receptor signaling. Indeed, Her-andez et al. attempted to dissect out the individual contributionsf CXCR4 and CXCR7 in tumor invasion and metastasis [108]. Theyhowed that the interaction of CXCL12 and CXCR4 expressed onammary adenocarcinoma MTLn3 cells increases the chemotac-
ic and invasive behavior of these cells to CXCL12, as well as theirotile behavior within the primary tumor and their ability to
ntravasate. These effects are the result of increased expression ofMP12 induced by the activation of the CXCR4 signaling pathway.n the other hand, the CXCL12-induced activation of the CXCR7
ignaling pathway inhibits MMP12 expression, and consequentlyatrix degradation, invasion, intravasation and spontaneous lungetastasis formation. However, CXCR7 expression was found to
timulate VEGF-A expression, microvessel density, and primaryumor growth. These findings provide evidence of the importantole of CXCL12-activated signaling pathways in the intravasationrocess.
A role of ATP in the intravasation process has also been provided.nder hypoxic conditions, breast cancer cells secrete nucleosideiphosphate kinase (sNDPK-B) adjacent to and within the cap-
llaries, which generates ATP from ADP locally. ATP acts on thendothelial nucleotide receptor (P2Y receptor), thus stimulatingasodilatation, platelet aggregation and endothelial cell migration.hese actions in turn promote entry of tumor cells into the bloodtream [109].
The tumor cells show high plasticity in the adaptation of theirype of migration and invasion for entry into blood vessels ando disseminate into the circulation. Collectively, migrating cellseed to break away from their neighbors to enter the blood-tream. Migratory cancer cells that undergo EMT acquire specificroperties, like expression of VE-cadherin, which allows them to
nteract with endothelial cells and to enhance their capacity for
ransendothelial migration [110,111].Furthermore, the widely observed increases in microvessel den-ity, as well as the leakiness of the tumor vasculature, facilitate
Biology 22 (2012) 234– 249
the entry of cancer cells into the circulation [103]. Survival in thebloodstream necessitates the acquisition of novel cell features, suchas overcoming detachment-triggered cell death (anoikis), as wellas surviving the shear forces of the circulating blood stream andattacks by the immune system [112]. Once in the blood stream,only a few cancer cells can outlive the many challenges from theimmune defense. For example, to be protected from immunologi-cal assault, tumor cells induce platelet aggregation, which shieldstheir cell surfaces from immunological recognition and facilitatestumor-cell thrombus formation in the microvasculature [37,113].One of the factors identified in the induction of platelet aggregationin human cancers is the transmembrane protein podoplanin [114]which has already been described as having an important role incollective cell migration (see above).
The Massague laboratory recently reported on MDA-MB-231breast cancer cell line variants that show organ-specific metastasis,to either bone or lung [115,116]. Subsequent gene expression pro-filing analysis identified bone-specific and lung-specific metastasisgene expression signatures. Functional analysis of some of thesegenes confirmed their critical roles in this organ-specific metasta-sis. Of note, some of the lung-metastasis-specific genes appeared tobe part of a ‘multifunctional vascular remodeling program’ [117].These included well-known cancer-relevant genes: epiregulin, aligand for the epidermal growth factor receptor (EGFR), MMP-1and 2, and COX-2. Together, epiregulin, COX-2 and MMP-1/2 gen-erate the tortuous and highly permeable tumor blood vasculaturethat is frequently seen in aggressive tumors, and which facilitatescancer-cell intravasation.
Recently, it has been reported that Notch signaling can directlycontribute to transendothelial migration and intravasation of can-cer cells [118]. Notch receptors are expressed on cancer cells,whereas their ligands are on stromal cells, such as Jagged1 inendothelial cells of tumor-associated blood vessels, and Dll4on endothelial cells, smooth muscle cells, and macrophages.Hence, the activation of Notch signaling mainly occurs in can-cer cells that are in the vicinity of blood vessels in primarytumors. The interaction between cancer and host cells acti-vates Notch signaling and promotes transendothelial migration,thus inducing cancer-cell intravasation. The transcriptional reg-ulator amino-terminal-enhancer of Split (Aes), and its mousehomolog, Groucho gene-related protein 5 (Grg5), suppress can-cer metastasis by inhibiting the Notch signaling pathway [118].The molecular mechanisms by which Aes/Grg5 inhibits the Notchsignaling pathway are through the sequestering of the Notchsignaling effector proteins Rbpj�, NICD and Maml1 in nuclearfoci that are transcriptionally inactive [118]. Hence, Aes/Grg5 isa metastasis suppressor gene, which acts mainly by preventingNotch signaling, Notch-mediated local invasion and intravasa-tion. Interestingly, the highest TGF-� activation was seen inblood vessels and at tumor margins that included 30–50% can-cer cells. TGF-� type II receptor/Smad4 activation has been shownto cause hematogenous dissemination of breast carcinoma [119],although prolonged TGF-� activation hampered lung metastasisformation, suggesting transient TGF-� activation for successfulmetastasis.
Angiopoietin-like 4 (ANGPTL4) has also been shown to disruptendothelial cell–cell junctions and to increase vessel permeabil-ity, which thus not only allows the easier passage of cancer cellsinto the vessels of primary tumors, but easier exit from the ves-sels in the secondary organ [120]. Interestingly, the expressionof ANGPTL4 is induced in cancer cells by the TGF-� present inthe primary breast cancer microenvironment, and the cancer cellsare thus primed at the primary tumor site for their colonizing ofthe distant organ. TGF-� also enhances breast-cancer intravasa-
tion by increasing cancer-cell penetration and general invasion andtransendothelial migration [119].
Cancer
1
altlolgoaptonLt[
VmsmpCtibnfsirA-gmC[
foIipVtie
cv[v[aransoctts
D. Spano et al. / Seminars in
.7. Lymphogenic metastasis
A large number of recent correlation studies in cancer patientsnd functional studies in mouse models have indicated that tumorymphangiogenesis, as the formation of new lymphatic vessels inhe tumor environment, can directly promote the formation ofymph-node metastases [121,122]. With the recent identificationf lymphangiogenic factors and their receptors, the causal role ofymphangiogenesis in the metastatic process has also been investi-ated. Most importantly, VEGF-C and VEGF-D, which are membersf the VEGF family of angiogenic factors, have been characterizeds critical players in the induction of lymphangiogenesis in normalhysiology and in disease. VEGF-C and VEGF-D bind preferentiallyo VEGFR-3 (Flt-4), which in the adult is predominantly expressedn lymphatic endothelial cells. Moreover, the recent discovery of aumber of additional markers for lymphatic endothelium, such asYVE-1, podoplanin and the transcription factor Prox-1, has facili-ated studies on the molecular mechanisms of lymphangiogenesis123].
Up-regulated expression of VEGF-C, and to a lesser extent ofEGF-D, highly correlates with lymphangiogenesis and lymph nodeetastasis in cancer patients [121–123]. Moreover, forced expres-
ion of VEGF-C and VEGF-D in tumor cell lines and in transgenicouse models of tumorigenesis results in the up-regulation of lym-
hangiogenesis and in the formation of lymph-node metastasis.onversely, a soluble form of VEGFR-3 and neutralizing antibodieso VEGFR-3 block lymphangiogenesis by binding to and sequester-ng VEGF-C and VEGF-D [124–128]. In contrast, VEGF-C depletiony siRNA technology reduces lymphangiogenesis, although this haso impact on metastasis [129]. Endostatin, which is a proteolytic
ragment of collagen XVIII and a potent endogenous angiogene-is inhibitor, and a neutralizing antibody to neuropilin-2, whichs a co-receptor of VEGFR-3, have also recently been shown toepress lymphangiogenesis and lymph node metastasis [130,131].lso, PTK787/ZK222584, a pharmacological inhibitor of VEGFR-1,2 and -3, has also been reported to inhibit tumor lymphangio-enesis and lymph node metastasis in a syngeneic transplantationodel of melanoma [132]. Additionally tumor expression of VEGF-
and VEGF-D actively induces vessel sprouting toward a tumor133,134].
While active lymphangiogenesis appears to contribute to theormation of lymph-node metastasis, the mode of regulationf lymphangiogenesis during tumor progression is not known.nvestigations with cultured cells in vitro have suggested thatnflammatory responses that activate the NF�B transcriptionalathway might be involved in the transcriptional regulation ofEGF-C expression [135,136] and that VEGF-D is induced by Fos
ranscriptional activity [137] although their regulation pathwaysn vivo, and in particular during tumor progression, have remainedlusive.
As well as passive intravasation into tumor lymphatics,hemokine-mediated migration of cancer cells toward lymphaticessels might also have a critical role in lymphogenic metastasis138]. Indeed, tumor cells might be even attracted to lymphaticessels through secretion of chemokines such as CCL21 and CCL19139]. These chemokines are secreted by the lymphatic vessel,nd they are ligands for CCR7, the expression of which is up-egulated in several human cancers, including breast cancer [140]nd melanoma [94,141], as well as colorectal [142], head andeck [143], prostate [144], non-small-cell lung [145], esophagealquamous cell [146], and gastric [147] cancers. Shields and collab-rators [95] suggested a mechanism for CCR7-mediated tumor cell
hemotaxis into the lymphatics. In addition to sensing chemotac-ic gradients of CCL21/19 from the lymphatics, they showed thatumor cells also generate autologous gradients of CCR7 ligands byecreting them into the ECM under the influence of slow interstitialBiology 22 (2012) 234– 249 241
flow. This mechanism uses the drainage function of the lymphaticsto direct tumor cells in a chemotactic manner toward lymphaticvessels serving the tumor, thus promoting tumor-cell migrationtoward functional, rather than nonfunctional, lymphatics. A partic-ularly recent study demonstrated that aggregates of breast cancercells can directly penetrate lymphatic vessels through ruptures inthe vascular wall [148]. This process is mediated by the inductionof the hypoxia-inducible enzyme ALOX12 or ALOX15 in mammarycarcinoma cells [148].
Thus, both angiogenesis and lymphangiogenesis contribute notonly to primary tumor growth, but also to the metastatic dissemina-tion of tumor cells. Together, these offer attractive targets for thedevelopment of anti-metastatic therapies. While the first angio-genesis inhibitors are in routine clinical use now, we need to awaitresults on the combinatorial inhibition of angiogenesis and lym-phangiogenesis and its effects on tumor metastasis.
1.8. Extravasation
The term extravasation has long been used to describe thepassage of immune cells and serum, together with tumorigeniccells, from vessels to tissues, to initiate secondary metastatic out-growth.
As described above, in primary carcinomas, secreted growthfactors and cytokines contributed by stromal cells are key for theinduction of EMT, a transient and reversible process that promotescell motility, invasion, and dissemination of cancer cells out ofthe tumor microenvironment [16,149]. Subsequently, tumor cellstravel through the bloodstream before arresting and extravasatinginto a new microenvironment.
Migratory and adhesive properties of tumor cells are criticalparameters for the development of metastasis [150]. Moreoverthe site of a tumor metastasis is influenced by both the pri-mary tumor cell and the distant microenvironment into which itspreads. Recently, through the use of real-time intravital imaging ofhuman tumor cells transplanted into transparent zebrafish, it wasestablished that extravasation of cancer cells is a highly dynamicprocess that involves the modulation of tumor-cell adhesion to theendothelium and intravascular cell migration along the luminalsurface of the vascular wall [151]. The earliest event in metasta-sis is the extravasation of tumor cells from the vasculature intothe surrounding stroma of the metastatic site. Circulating tumorcells, as with leukocytes, can use endothelial-cell-specific adhesionmolecules, such as selectins or intercellular adhesion molecules(ICAMs), to interact with these cells before they touch the under-lying BM in the further course of their extravasation.
What happens when the tumor cells are in the blood vessel?Huh et al. [152] showed that neutrophils regulate lung metasta-sis development through physical interactions and anchoring ofthe circulating tumor cells to endothelium. In this study, they indi-cated the neutrophils as carriers for cancer-cell extravasation. Theyshowed that by producing and secreting high levels of IL-8, a neu-trophil chemotactic factor, cancer cells initially attract neutrophilsand then increase the expression of adhesion molecules on neu-trophils, such as the tethering �2, to promote anchorage to thevascular endothelium.
Another corpuscular component within the blood thatis involved in cancer-cell extravasion is the platelets. Theprometastatic effects of platelets have so far been attributed totheir ability to promote adhesion to the endothelium or to theircapacity to prevent cell death in the circulation by forming fibrino-gen, a physical shield around tumor cells, and also by protecting
cancer cells from the immune system. This shield protects tumorcells from NK-cell-mediated lysis [153,154], limits their exposureto shear stress, and promotes their adhesion to the endothelium[113,155–157]. Moreover, platelets are a natural source of several
2 ancer
gcItscpTcmmiTcm�hpidpemapcimtbenftesitaFierVb
s�tmdheaocte
prkbibd
42 D. Spano et al. / Seminars in C
rowth factors that can enhance the abilities of a circulating can-er cell to extravasate by activating several molecular pathways.n a recent study by Labelle et al. [158], they demonstrated howhe metastatic potential of tumor cells continues to evolve out-ide of the primary tumor site in response to platelet-to-tumorell signaling. They identified specific platelet factors and signalingathways evoked in tumor cells that critically support metastasis.hey demonstrated that a transient interaction between colon can-er cells and platelets in vitro was sufficient to increase tumor celletastatic seeding in the lung. Then they defined the molecularechanisms induced by platelet–tumor cell interactions, show-
ng that cancer cells acquire EMT-like features, and revealing thatGF-�1 secreted by the platelets activates TGF-�/Smad in the can-er cells, which synergizes with NF-kB to mediate the increasedetastatic capacity of the tumor cells. Finally, by generating a TGF-1 knock-out mouse model specifically in megakaryocytes, andence in platelets, they elegantly demonstrated how the potentiallatelet-induced metastatic behavior of cancer cells was dramat-
cally diminished. This suggests that a lack of TGF-�1 in plateletselays tumor-cell extravasation in the lung, which indicates thatlatelets can expedite tumor-cell exit from the vasculature and thusnhance lung metastasis. Based on the contribution of platelets inetastasis formation, it is not surprising that indeed anti-platelet
ggregation therapy can provide a benefit in the treatment of canceratients [112,159]. The interactions between endothelial cells andancer cells, assisted by a release of cytokines, are the major eventn extravasation. How cell–cell adhesive junctional structures that
aintain vascular integrity can dynamically change their proper-ies to generate a permissive microenvironment is an issue that haseen covered by several studies. To date, it is well documented thatndothelial vessels are dynamically regulated by VEGF receptor sig-aling. Cheng et al. [72] characterized a role for integrin-associated
ocal adhesion tyrosine kinase (FAK) signaling in vascular func-ion, showing that genetic or pharmacological FAK inhibition inndothelial cells prevents VEGF-stimulated permeability down-tream of the VEGF receptor, and Src tyrosine kinase activationn vivo. In their studies, they established a role for FAK as an essen-ial signaling switch within endothelial cells for the regulation ofdherens junction dynamics. VEGF promotes tension-independentAK activation, rapid FAK localization to cell–cell junctions, bind-ng of the FAK FERM domain to the cytoplasmic tail of vascularndothelial cadherin (VE-cadherin), and direct FAK phospho-ylation of �-catenin at tyrosine-142 (Y142), which facilitatesE-cadherin-�-catenin dissociation and endothelial cell junctionalreakdown.
Another important molecule that appears to promote extrava-ation is the ECM protein TGF-�-induced (TGFBI; referred to asig-h3), a structural homolog of periostin, the physiological func-
ion of which has been postulated as an involvement in cellatrix interactions and cell migration [160,161]. Ma et al. [162]
emonstrated that when cancer cells express high levels of �ig-3, they can induce dissociation of VE-cadherin junctions betweenndothelial cells via the integrin �v�5-Src signaling pathway. Srcctivation results in phosphorylation of VE-cadherin and �-cateninn specific tyrosine residues, leading to the dissociation of the VE-adherin/�-catenin complex and consequently the breakdown ofhe endothelial barrier [163], which results in enhanced cancer-cellxtravasation.
The coagulation protease thrombin, which activates therotease-activated receptor (PAR) family of G-protein-coupledeceptors [164] by proteolytic cleavage, should represent anotherey regulator of endothelial barrier function. In a model presented
y Gavard and Gutkind [165], exposure to thrombin stimulationnduced rapid morphological and cytoskeletal changes, followedy the loss of the endothelial barrier integrity, as a mechanismistinct from that initiated by VEGF. They showed that thrombin
Biology 22 (2012) 234– 249
induces activation of its cognate receptor, PAR-1, which is cou-pled to both G11/q, which is required for calcium entry and RhoAactivation, and G12/13, the signaling of which cooperates in RhoAactivation. This dual coupling might regulate the activity, localiza-tion and cycling of multiple RhoGEFs. The role of RhoA is centralin the thrombin-induced increase in permeability in endothelialcells, as both an activator of two essential downstream effectors,ROCK and PRK, and in the control of formin activity on actin andmicrotubule organization. ROCK activity is required for actomyosincontractility, through the regulation of MLC and cofilin, and theactin stress fiber architecture. Conversely, PRK expression con-tributes to FAK and paxillin phosphorylation and a correct focaladhesion morphology. Finally, both signaling routes converge onthe increase in actomyosin contractility and on cell–cell junctionremodeling, which leads to endothelial barrier destabilization anda permeability increase.
Thus, when cancer cells get into the bloodstream, they canspread through the whole body, and are later arrested in the cap-illary bed of several distant organs, so as to extravasate and try togrow. Here, the potential metastatic target organs provide a vari-ety of pro-metastatic and anti-metastatic stimuli that regulate theonset of organ colonization by the metastatic tumor cells. However,cancer metastasis results from a non-random process, in which theorgan selectivity by the tumor cells is largely determined by fac-tors that are expressed at the remote organs that eventually turninto the preferred sites for metastasis formation. This issue will beaddressed later in terms of metastatic outgrowth, while it appearsto be a little different to what happens in the brain environmentduring the extravasation process.
These few above-described events show how several complexmolecular interactions occur during extravasation. They have high-lighted cell–cell interactions, cell signals, and finally the exposureof the tumor cells within the bloodstream. These factors act eitheron the tumor cells or on non-neoplastic cells that are needed togenerate the early events in the metastatic process.
1.9. Passing through the blood–brain barrier: an example ofextravasation
The essential role of the tumor microenvironment in cancer pro-gression has been well documented for extracranial malignancies.However, precisely how tumor cells penetrate the ‘blood–brainbarrier’ and gain access to the brain parenchyma is not completelydefined and understood. Brain metastases most commonly arisefrom cancers of the lung, breast and skin (melanoma), but canalso occur at a reduced frequency in patients with diverse cancertypes [166]. The brain is one of the few organs that are separatedfrom circulating immune cells, partially due to the presence ofthe blood–brain barrier. Although long regarded as an immune-privileged organ, the brain is not immune deficient. Microgliaare a specialized population of glial cells that are regarded asthe resident macrophages in the brain. Like macrophages, underthe correct conditions microglia are phagocytic and can presentantigens. Astroglial cells, which are also commonly known as astro-cytes, are another major population of glial cells in the brain.They carry out housekeeping functions in the brain to main-tain homeostasis and deliver nutrients and energy. Activationof microglial and astroglial cells is found in a wide range ofbrain-related diseases, such as neurodegenerative diseases, trau-matic injuries and brain tumors, and including brain metastases[167].
It is well established that the host microenvironment affects
tumor growth and metastatic progression and impacts on the suc-cess of tumor cells to survive and grow within the brain. Theinvasion of brain tissue by individual cancer cells can induce avariety of glial responses that add to the uniqueness of each
Cancer
lesapdmotstlepsewn
sIlwodteetcbd
hoItpfictm
voypsttccioiitmoc
tsms
D. Spano et al. / Seminars in
ocal microenvironment. However, the contributions of differ-nt astrocytic and microglial cell populations to the very earlytages of metastatic invasion remain to be determined. An excitingpproach to visualize the early stages of extravasation into the brainarenchyma was reported by Kienast et al. [168], although theyescribed few molecular events. Using multiphoton laser scanningicroscopy, they showed for the first time that the initial arrest
f blood-borne cancer cells in the brain results from size restric-ions and not from vascular wall adhesion. They also identified theteps that would never lead to successful metastasis growth in theumor cells types they analyzed: perpetuation of an intravascu-ar position, lack of close association with cerebral microvessels,ither directly after extravasation or after cessation in a primaryerivascular position, and lack of vascular changes during metasta-is growth. Instead, an essential step to metastatic growth followingxtravasation was the perpetuation of a strict perivascular position,hich probably provides an optimal oxygen supply and access toutrients.
Recently, Bos et al. [169] used gene expression profiling analy-is to identify genes that promote breast cancer brain metastasis.n their study, tumor cell lines were injected into the general circu-ation (intracardiac injection), and the resulting brain metastases
ere then harvested, expanded in culture, and subjected to a sec-nd round of re-injection and harvesting. Using this approach, theirata indicated that the expression of COX2 and HBEGF in primaryumors enhances cancer cells for extravasation through the nonfen-strated capillaries of the brain and lungs, whereas ST6GALNAC5xpression acts as a specific mediator of cancer-cell infiltrationhrough the blood–brain barrier, drawing attention to the role ofell surface sialylation as a previously unrecognized participant inrain metastasis formation, and to the possibility of therapeuticallyisrupting these interactions.
In another recent report by Lee et al. [170] it was shown thatuman brain endothelial cells (HBECs), which are a major elementf the blood–brain barrier, take part in the extravasation process.n their in vitro model of the blood–brain barrier, they showed thatransmigration of breast cancer cells was markedly enhanced in theresence of HBECs than in their absence. This suggests that HBECsacilitate the transmigration of breast cancer cells rather than act-ng as a barrier against them. Moreover, they showed that bothyclooxygenase (COX-2) and MMP-2, produced by HBECs, ratherhan that generated by breast cancer cells, have key roles in trans-
igration.Lorger et al. [171] demonstrated that cancer cell survival in the
asculature is probably the critical step that limits the success ratef brain metastasis formation. They provided detailed in vivo anal-ses of breast cancer cell arrest and extravasation into the brainarenchyma, and they showed that breast cancer cells arrest exclu-ively in the brain capillaries and/or postcapillary venules. Whenhey compared five different breast cancer cell models, they iden-ified three as suitable models for detailed studies of the earliestritical events of breast cancer cell extravasation and initial brainolonization. They also observed cancer-cell protrusions stretch-ng through the vessel walls, which indicated that the crossingf the blood–brain barrier is an active, specific process that isnitiated by the tumor cells. Moreover, exit of cancer cells from cap-llaries or post-capillary venules might involve mechanical forceshat are generated by the rounding of the cancer cells, the for-
ation of cytoplasmic protrusions, and most likely, the secretionf disruptive enzymes, such as MMP-9 and heparanase, or theirombinations.
Another important concept reported by Lorger et al. [171] was
hat invasion of the brain parenchyma was always followed bytrong local activation of astrocytes and to varying degrees, oficroglia. Astrocytic responses were heterogeneous in their inten-ity and cellular composition, and involved cells with up-regulated
Biology 22 (2012) 234– 249 243
expression of GFAP, nestin, or both. Reactive astrocytes occasionallyshowed strong up-regulation of the expression of MMP-9, whichis known to promote growth of primary brain tumors based onits pro-angiogenic activity of releasing VEGF from the surroundingmatrix. In addition, VEGF can also directly stimulate the prolifer-ation of cancer cells [172]. Furthermore, astrocytes were shownto support brain metastasis growth by secretion of heparanase andneurotrophins [173]. Thus, reactive astrocytes might provide initialcues for extravasating tumor cells to survive and proliferate withinthe brain parenchyma.
Although the exact roles of invading cancer cells, brain endothe-lial cells, and glial cells in metastatic events remain elusive, furtherstudies will no doubt delineate the functional contributions of theseand other actors that are essential for brain metastatic invasion.
1.10. Metastatic outgrowth
During the metastatic process, tumor cells detach from the pri-mary tumor, invade and intravasate the vasculature, and come torest in local capillaries in secondary organs. Here they need toextravasate, invade, survive and proliferate. Several studies havesuggested that the intrinsic properties of both the metastatic cells(genetic and epigenetic changes) and the host microenvironmentare important determinants in metastatic dissemination. Thesefindings lead to a metastatic-niche model, in which a suitably con-ducive microenvironment (the pre-metastatic niche) must evolvefor tumor cells to engraft (metastatic niche) and proliferate atsecondary sites (micrometastatic to macrometastatic transition)[174]. Primary tumors can secrete several factors that mediatethe establishment of specific cell populations, such as hematopoi-etic progenitor cells and macrophages, in the sites of futuremetastasis (pre-metastatic niche). These cells cluster in the pre-metastatic niches, thus creating an environment that is conduciveto tumor-cell adhesion and invasion [175,176]. In the lung pre-metastatic niche, the primary tumor-derived molecules involvedin this recruitment are VEGF-A, TNF�, and TGF�. These moleculesstimulate the expression of the S100A8 and S100A9 inflammatoryproteins, which in turn induce the expression of the chemoattrac-tant serum amyloid A3 (SAA3) protein, which is responsible forthe recruitment of both tumor cells and hematopoietic progenitorcells to the pre-metastatic niche [177]. At the location of secondarytumor development, and in combination with other factors (such ascytokines), the tumor-derived factor RANTES promotes the releaseof S100A4, which stimulates T-cell attraction and T-cell produc-tion of proinflammatory cytokines (e.g. G-CSF); these, in turn, willattract myeloid cells to the pre-metastatic niche [59,178]. Also, thecomponents of the ECM have important roles in the formation of thepre-metastatic niche. In particular, lysyl oxidase (LOX) co-localizeswith fibronectin at this site. LOX serves to cross-link collagen IV inthe BM of the lung, thus increasing the adherence of hematopoieticprogenitor cells. These cells produce MMP2, to cleave collagen IV,which leads to their invasion of the lung and further recruitmentof hematopoietic progenitor cells and, finally, of metastasizingtumor cells [179]. Tenascin C (TNC) is another component of theECM that engages the Notch and Wnt signaling pathways to sup-port the fitness of breast cancer cells during the establishment oflung metastases [180]. The fibroblast-derived Fibulin-5 (FBLN5), amatricellular protein that modulates cell–ECM interactions, sup-presses metastasis formation by inhibiting the production of MMP9and by repressing the invasive behavior of fibroblasts. Conversely,the production of FBLN5 in stromal fibroblasts is repressed bytumor-derived factors, resulting in the up-regulation of MMP9,
ECM remodeling, stimulation of angiogenesis, and invasion offibroblasts. All these events will further create a fertile milieuwithin which tumor cells can develop metastases [181]. Moreover,hematopoietic progenitor cells established at pre-metastatic niche
244 D. Spano et al. / Seminars in Cancer Biology 22 (2012) 234– 249
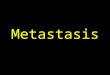
F g the
m withina
statrit
mao
ig. 2. Molecular networks. String analyses through a literature search, includinetastasis. Individual colors group proteins and their specific interaction networks
t http://david.abcc.ncifcrf.gov) are indicated here.
ites express osteopontin, a protein that has been implicated inumor-cell adhesion and survival, and in the regulation of MMPctivity and host immune defense [182,183]. These findings suggesthat in the pre-metastatic niche, as in the primary tumor microenvi-onment, hematopoietic progenitor cells and myeloid cells have anmmune-regulatory function, which creates immune sites in whichhe malignant cells can survive and proliferate without detection.
Altogether, these findings support a concept that the develop-ent of new therapeutic approaches targeting the specific cellular
nd molecular networks driving tumor metastasis is feasible andf utmost urgency to combat metastatic disease.
gene symbols involved in each individual action within networks that regulate their gene functional classification (DAVID functional annotation system available
2. Concluding remarks and the future
It is now recognized that metastasis is an extremely complexand multistep biological event that results from a complex molec-ular cascade through which cancer cells leave the primary tumorand disseminate to distant anatomical sites, where they prolif-erate and form secondary tumors. Several studies have provided
insights into the definition of which molecular components facili-tate this process. The full understanding of the molecular networksunderlying this process will allow the development of new thera-peutic approaches. The present findings support the rationale for
D. Spano et al. / Seminars in Cancer Biology 22 (2012) 234– 249 245
Table 1A summary of the signaling pathways and their specific targets, and the drugs used in current clinical trials to impair the molecular network regulating cancer metastasis.The colored functional categories are linked to Fig. 2, and they indicate potential targeted molecules and networks. This is an example of the expanded list in SupplementalTable 1.
Biological process Signaling pathways and targets Targeting agent
Mesenchymal migration Wnt signaling pathway; Rac; Twist; Slug Resveratrol
Amoeboid migration PI3K signaling pathway; RhoA/ROCK;Rac; RhoGEFs; RhoGAPs; RhoGEF Dock3;NEDD9; WAVE2; Rho; RacGAPARHGAP22; PDK1
MK-2206; PX-866; BGT226; Sirolimus;Anastrozole; Imatinib Mesylate; RAD001;Docetaxel; Everolimus; Ridaforolimus;Allogeneic GM-CSF-secreting breast cancervaccine; Trastuzumab; Cyclophosphamide
Metastatic microenvironment in primary tumors WNT signaling pathway; Notch signalingpathway; Sonic hedgehog signalingpathway; receptor subunit GP130-IL6ST;the tyrosine kinase JAK1; Rho-kinase,histidine-rich glycoprotein; IGFBP2;PITPNC1; MERTK; GalNAc transferaseGALNT7
Resveratrol; MK0752; RO4929097;Bevacizumab; FOLFOX regimen; Fluorouracil;Leucovorin calcium; Oxaliplatin; Dexamethasone
Intravasation TGF-� signaling pathway; Notchsignaling pathway; podoplanin;epiregulin; MMP-1; MMP 2;cyclooxygenase-2
Anti-transforming growth factor-beta (GC 1008);Lucanix; AP 12009; Fenretinide; Ammoniumtetrathiomolybdate; MK 0752; RO4929097;Bevacizumab, FOLFOX regimen; Fluorouracil;Leucovorin calcium; Oxaliplatin; Dexamethasone
Lymphogenic metastasis NFkB signaling pathway; Fos; VEGF-C;VEGF-D; VEGFR-3; endostatin;neuropilin-2
Bortezomib (Velcade, PS-341); Cetuximab;Cisplatin; Temozolomide; Tanespimycin;Topotecan hydrochloride; Rituximab;Cyclophosphamide; Doxorubicin; Vincristine;Prednisone; Idarubicin; Pemetrexed disodium;Diindolylmethane; Vorinostat (SAHA); Nitricoxide-releasing acetylsalicylic acid derivative;Gemcitabine hydrochloride; Arsenic trioxide;Dexamethasone; Thalidomide; Pioglitazonehydrochloride; Erlotinib hydrochloride
Metastatic outgrowth Wnt signaling pathway; Notch signalingpathway; TGF-� signaling pathway;VEGF-A; TNF�; S100A8; S100A9; SAA3;S100A4; lysyl oxidase; fibronectin;tenescin C; osteopontin, Fibulin-5
Resveratrol; anti-transforming growthfactor-beta (GC 1008); Lucanix; AP 12009;Fenretinide; Ammonium tetrathiomolybdate;MK 0752; RO4929097; Bevacizumab, FOLFOXregimen; Fluorouracil; Leucovorin calcium;
ticptetaiiasspmtccrtt
argeting the multiple biological processes and the moleculesnvolved in these processes in conjunction with targeting the tumorells directly, to improve the treatment of metastatic disease. Aattern depicted through our literature search (Fig. 2) shows howhese molecular networks of genes interact within a metastaticnvironment. A list of genes, with the grouping of their func-ional categories, is indicated here, while the spatial and temporalctions of those genes within this scenario need further futurenvestigations. Therapeutic strategies can be used to inhibit thenvasion, migration, intravasation, extravasation, establishmentnd growth of tumor cells, and the recruitment and function ofpecific cell populations that contribute to these processes. Con-equently molecules and signaling pathways that regulate theserocesses can serve as novel therapeutic targets in cancer treat-ents (Fig. 2). Moreover, some potential drugs (see Table 1) that
arget these pathways are in use in ongoing studies. Indeed, ongoinglinical trials are already testing drugs that can impair some of the
ellular and molecular processes described above. Table 1 summa-izes further the “state of the art” of these clinical trials, underlininghat few of the drugs in use have shown multiple actions againsthose molecular processes.Oxaliplatin; Dexamethasone
Several studies have provided evidence of the role of inflamma-tion in cancer progression. Our understanding of the relationshipbetween inflammation and cancer is growing. This improvedknowledge will undoubtedly allow for the development ofapproaches to fight these molecular networks and pathways linkedto inflammation in cancer, at this time of relevance for new clini-cal evaluations. The results of these ongoing trials (SupplementalTable 1) will define new avenues for future therapeutic strategies,bringing together studies on systems biology and new drug discov-eries, awaiting the development of the best clinical protocol for thetreatment of metastatic cancer.
Acknowledgments
For funding support: the European GRANT-FP7-Tu-micHEALTH-F2-2008-201662 (MZ), Associazione Italiana per laRicerca sul Cancro, AIRC (MZ), PRIN Ministero Dell’ Istruzione, dell’
Università e della Ricerca E5AZ5F (2008), Associazione Italianaper la Lotta al Neuroblastoma 2008–2010 (MZ). DS and PD aresupported by the Department of Biochemistry and Biotechnolog-ical Medicine, ‘Federico II’ University of Naples, Naples, Italy, and
2 ancer
CN
A
t
R
46 D. Spano et al. / Seminars in C
EINGE, Centro di Ingegneria Genetica e Biotecnologie Avanzate,aples, Italy.
ppendix A. Supplementary data
Supplementary data associated with this article can be found, inhe online version, at doi:10.1016/j.semcancer.2012.03.006.
eferences
[1] Mehlen P, Puisieux A. Metastasis: a question of life or death. Nature ReviewsCancer 2006;6:449–58.
[2] Monteiro J, Fodde R. Cancer stemness and metastasis: therapeutic conse-quences and perspectives. European Journal of Cancer 2010;46:1198–203.
[3] Nguyen DX, Bos PD, Massague J. Metastasis: from dissemination to organ-specific colonization. Nature Reviews Cancer 2009;9:274–84.
[4] Paget S. The distribution of secondary growths in cancer of the breast. 1889.Cancer Metastasis Reviews 1989;8:98–101.
[5] Ewing J. The general pathological conception of cancer. Canadian MedicalAssociation journal 1935;33:125–35.
[6] Christofori G. New signals from the invasive front. Nature 2006;441: 444–50.[7] Valastyan S, Weinberg RA. Tumor metastasis: molecular insights and evolving
paradigms. Cell 2011;147:275–92.[8] Friedl P, Alexander S. Cancer invasion and the microenvironment: plasticity
and reciprocity. Cell 2011;147:992–1009.[9] Friedl P, Wolf K. Tumour-cell invasion and migration: diversity and escape
mechanisms. Nature Reviews Cancer 2003;3:362–74.[10] Condeelis J, Pollard JW. Macrophages: obligate partners for tumor cell migra-
tion, invasion, and metastasis. Cell 2006;124:263–6.[11] Brabletz T, Jung A, Spaderna S, Hlubek F, Kirchner T. Opinion: migrating cancer
stem cells—an integrated concept of malignant tumour progression. NatureReviews Cancer 2005;5:744–9.
[12] Wicki A, Christofori G. The potential role of podoplanin in tumour invasion.British Journal of Cancer 2007;96:1–5.
[13] Yilmaz M, Christofori G. EMT, the cytoskeleton, and cancer cell invasion. Can-cer Metastasis Reviews 2009;28:15–33.
[14] Kalluri R, Weinberg RA. The basics of epithelial–mesenchymal transition. TheJournal of Clinical Investigation 2009;119:1420–8.
[15] Polyak K, Weinberg RA. Transitions between epithelial and mesenchymalstates: acquisition of malignant and stem cell traits. Nature Reviews Cancer2009;9:265–73.
[16] Thiery JP, Acloque H, Huang RY, Nieto MA. Epithelial–mesenchymal transi-tions in development and disease. Cell 2009;139:871–90.
[17] Friedl P, Wolf K. Plasticity of cell migration: a multiscale tuning model. TheJournal of Cell Biology 2010;188:11–9.
[18] Yilmaz M, Christofori G. Mechanisms of motility in metastasizing cells. Molec-ular Cancer Research 2010;8:629–42.
[19] Brabletz T, Hlubek F, Spaderna S, Schmalhofer O, Hiendlmeyer E, Jung A, et al.Invasion and metastasis in colorectal cancer: epithelial–mesenchymal tran-sition, mesenchymal–epithelial transition, stem cells and beta-catenin. CellsTissues Organs 2005;179:56–65.
[20] Sarrio D, Rodriguez-Pinilla SM, Hardisson D, Cano A, Moreno-Bueno G, Pala-cios J. Epithelial–mesenchymal transition in breast cancer relates to thebasal-like phenotype. Cancer Research 2008;68:989–97.
[21] Tarin D, Thompson EW, Newgreen DF. The fallacy of epithelial mesenchymaltransition in neoplasia. Cancer Research 2005;65:5996–6000 [discussion -1].
[22] Thomas PA, Kirschmann DA, Cerhan JR, Folberg R, Seftor EA, Sellers TA, et al.Association between keratin and vimentin expression, malignant pheno-type, and survival in postmenopausal breast cancer patients. Clinical CancerResearch: An Official Journal of the American Association for Cancer Research1999;5:2698–703.
[23] Hlubek F, Brabletz T, Budczies J, Pfeiffer S, Jung A, Kirchner T. Heterogeneousexpression of Wnt/beta-catenin target genes within colorectal cancer. Inter-national Journal of Cancer 2007;121:1941–8.
[24] Hennessy BT, Gonzalez-Angulo AM, Stemke-Hale K, Gilcrease MZ, Krishna-murthy S, Lee JS, et al. Characterization of a naturally occurring breast cancersubset enriched in epithelial-to-mesenchymal transition and stem cell char-acteristics. Cancer Research 2009;69:4116–24.
[25] Pankova K, Rosel D, Novotny M, Brabek J. The molecular mechanisms oftransition between mesenchymal and amoeboid invasiveness in tumor cells.Cellular and Molecular Life Sciences 2010;67:63–71.
[26] Sanz-Moreno V, Gadea G, Ahn J, Paterson H, Marra P, Pinner S, et al. Racactivation and inactivation control plasticity of tumor cell movement. Cell2008;135:510–23.
[27] Sanz-Moreno V, Gaggioli C, Yeo M, Albrengues J, Wallberg F, Viros A, et al.ROCK and JAK1 signaling cooperate to control actomyosin contractility intumor cells and stroma. Cancer Cell 2011;20:229–45.
[28] Pinner S, Sahai E. PDK1 regulates cancer cell motility by antagonising inhibi-
tion of ROCK1 by RhoE. Nature Cell Biology 2008;10:127–37.[29] Sidani M, Wessels D, Mouneimne G, Ghosh M, Goswami S, SarmientoC, et al. Cofilin determines the migration behavior and turning fre-quency of metastatic cancer cells. The Journal of Cell Biology 2007;179:777–91.
Biology 22 (2012) 234– 249
[30] Garzia L, D’Angelo A, Amoresano A, Knauer SK, Cirulli C, Campanella C, et al.Phosphorylation of nm23-H1 by CKI induces its complex formation with h-prune and promotes cell motility. Oncogene 2008;27:1853–64.
[31] Kobayashi T, Hino S, Oue N, Asahara T, Zollo M, Yasui W, et al. Glycogensynthase kinase 3 and h-prune regulate cell migration by modulating focaladhesions. Molecular and Cellular Biology 2006;26:898–911.
[32] Muller T, Stein U, Poletti A, Garzia L, Rothley M, Plaumann D, et al. ASAP1promotes tumor cell motility and invasiveness, stimulates metastasis forma-tion in vivo, and correlates with poor survival in colorectal cancer patients.Oncogene 2010;29:2393–403.
[33] Steeg PS, Zollo M, Wieland T. A critical evaluation of biochemical activitiesreported for the nucleoside diphosphate kinase/Nm23/Awd family pro-teins: opportunities and missteps in understanding their biological functions.Naunyn-Schmiedebergs Archives of Pharmacology 2011;384:331–9.
[34] Friedl P, Gilmour D. Collective cell migration in morphogenesis, regenerationand cancer. Nature Reviews Molecular Cell Biology 2009;10:445–57.
[35] Kerkela E, Saarialho-Kere U. Matrix metalloproteinases in tumor progression:focus on basal and squamous cell skin cancer. Experimental Dermatology2003;12:109–25.
[36] Hegerfeldt Y, Tusch M, Brocker EB, Friedl P. Collective cell movement in pri-mary melanoma explants: plasticity of cell–cell interaction, beta1-integrinfunction, and migration strategies. Cancer Research 2002;62:2125–30.
[37] Fidler IJ. The relationship of embolic homogeneity, number, size and viabil-ity to the incidence of experimental metastasis. European Journal of Cancer1973;9:223–7.
[38] Friedl P, Wolf K. Tube travel: the role of proteases in individual and collectivecancer cell invasion. Cancer Research 2008;68:7247–9.
[39] Wolf K, Friedl P. Mapping proteolytic cancer cell–extracellular matrix inter-faces. Clinical & Experimental Metastasis 2009;26:289–98.
[40] Schacht V, Dadras SS, Johnson LA, Jackson DG, Hong YK, Detmar M.Up-regulation of the lymphatic marker podoplanin, a mucin-type trans-membrane glycoprotein, in human squamous cell carcinomas and germ celltumors. The American Journal of Pathology 2005;166:913–21.
[41] Wicki A, Lehembre F, Wick N, Hantusch B, Kerjaschki D, Christofori G. Tumorinvasion in the absence of epithelial–mesenchymal transition: podoplanin-mediated remodeling of the actin cytoskeleton. Cancer Cell 2006;9: 261–72.
[42] Scholl FG, Gamallo C, Vilaro S, Quintanilla M. Identification of PA2.26 anti-gen as a novel cell-surface mucin-type glycoprotein that induces plasmamembrane extensions and increased motility in keratinocytes. Journal of CellScience 1999;112(Pt 24):4601–13.
[43] Atsumi N, Ishii G, Kojima M, Sanada M, Fujii S, Ochiai A. Podoplanin anovel marker of tumor-initiating cells in human squamous cell carcinomaA431. Biochemical and Biophysical Research Communications 2008;373:36–41.
[44] Martin-Villar E, Megias D, Castel S, Yurrita MM, Vilaro S, Quin-tanilla M. Podoplanin binds ERM proteins to activate RhoA andpromote epithelial–mesenchymal transition. Journal of Cell Science2006;119:4541–53.
[45] Poujade M, Grasland-Mongrain E, Hertzog A, Jouanneau J, Chavrier P, LadouxB, et al. Collective migration of an epithelial monolayer in response to a modelwound. Proceedings of the National Academy of Sciences of the United Statesof America 2007;104:15988–93.
[46] Gaggioli C, Hooper S, Hidalgo-Carcedo C, Grosse R, Marshall JF, HarringtonK, et al. Fibroblast-led collective invasion of carcinoma cells with differ-ing roles for RhoGTPases in leading and following cells. Nature Cell Biology2007;9:1392–400.
[47] Joyce JA, Pollard JW. Microenvironmental regulation of metastasis. NatureReviews Cancer 2009;9:239–52.
[48] Zumsteg A, Christofori G. Corrupt policemen: inflammatory cells promotetumor angiogenesis. Current Opinion in Oncology 2009;21:60–70.
[49] Spano D, Zollo M. Tumor microenvironment: a main actor in the metastasisprocess. Clinica Experimental Metastasis 2012;29(4):381–95.
[50] Zhang Y, Tang H, Cai J, Zhang T, Guo J, Feng D, et al. Ovarian cancer-associatedfibroblasts contribute to epithelial ovarian carcinoma metastasis by promot-ing angiogenesis, lymphangiogenesis and tumor cell invasion. Cancer Letters2011;303:47–55.
[51] Kobayashi Y. The role of chemokines in neutrophil biology. Frontiers in Bio-science: A Journal and Virtual Library 2008;13:2400–7.
[52] Bockhorn M, Roberge S, Sousa C, Jain RK, Munn LL. Differential gene expres-sion in metastasizing cells shed from kidney tumors. Cancer Research2004;64:2469–73.
[53] Cao Z, Henzel WJ, Gao X. IRAK: a kinase associated with the interleukin-1receptor. Science 1996;271:1128–31.
[54] Li S, Strelow A, Fontana EJ, Wesche H. IRAK-4: a novel member of the IRAKfamily with the properties of an IRAK-kinase. Proceedings of the NationalAcademy of Sciences of the United States of America 2002;99:5567–72.
[55] Muzio M, Ni J, Feng P, Dixit VM. IRAK (Pelle) family member IRAK-2 andMyD88 as proximal mediators of IL-1 signaling. Science 1997;278:1612–5.
[56] Behrens C, Feng L, Kadara H, Kim HJ, Lee JJ, Mehran R, et al. Expression ofinterleukin-1 receptor-associated kinase-1 in non-small cell lung carcinomaand preneoplastic lesions. Clinical Cancer Research: An Official Journal of the
American Association for Cancer Research 2010;16:34–44.[57] Boye K, Grotterod I, Aasheim HC, Hovig E, Maelandsmo GM. Activation ofNF-kappaB by extracellular S100A4: analysis of signal transduction mech-anisms and identification of target genes. International Journal of Cancer2008;123:1301–10.

Cancer
D. Spano et al. / Seminars in[58] Forst B, Hansen MT, Klingelhofer J, Moller HD, Nielsen GH, Grum-SchwensenB, et al. Metastasis-inducing S100A4 and RANTES cooperate in promotingtumor progression in mice. PLoS One 2010;5:e10374.
[59] Grum-Schwensen B, Klingelhofer J, Grigorian M, Almholt K, Nielsen BS,Lukanidin E, et al. Lung metastasis fails in MMTV-PyMT oncomice lack-ing S100A4 due to a T-cell deficiency in primary tumors. Cancer Research2010;70:936–47.
[60] Klingelhofer J, Moller HD, Sumer EU, Berg CH, Poulsen M, Kiryushko D,et al. Epidermal growth factor receptor ligands as new extracellular targetsfor the metastasis-promoting S100A4 protein. The FEBS Journal 2009;276:5936–48.
[61] Mishra P, Banerjee D, Ben-Baruch A. Chemokines at the crossroads of tumor-fibroblast interactions that promote malignancy. Journal of Leukocyte Biology2011;89:31–9.
[62] Hembruff SL, Jokar I, Yang L, Cheng N. Loss of transforming growth factor-betasignaling in mammary fibroblasts enhances CCL2 secretion to promote mam-mary tumor progression through macrophage-dependent and -independentmechanisms. Neoplasia 2010;12:425–33.
[63] Loberg RD, Ying C, Craig M, Day LL, Sargent E, Neeley C, et al. Targeting CCL2with systemic delivery of neutralizing antibodies induces prostate cancertumor regression in vivo. Cancer Research 2007;67:9417–24.
[64] Loberg RD, Ying C, Craig M, Yan L, Snyder LA, Pienta KJ. CCL2 as an impor-tant mediator of prostate cancer growth in vivo through the regulation ofmacrophage infiltration. Neoplasia 2007;9:556–62.
[65] Lu X, Kang Y. Chemokine (C–C motif) ligand 2 engages CCR2+ stromal cells ofmonocytic origin to promote breast cancer metastasis to lung and bone. TheJournal of Biological Chemistry 2009;284:29087–96.
[66] Salcedo R, Ponce ML, Young HA, Wasserman K, Ward JM, Kleinman HK, et al.Human endothelial cells express CCR2 and respond to MCP-1: direct role ofMCP-1 in angiogenesis and tumor progression. Blood 2000;96:34–40.
[67] Mirolo M, Fabbri M, Sironi M, Vecchi A, Guglielmotti A, Mangano G, et al.Impact of the anti-inflammatory agent bindarit on the chemokinome: selec-tive inhibition of the monocyte chemotactic proteins. European CytokineNetwork 2008;19:119–22.
[68] Zollo M, Di Dato V, Spano D, De Martino D, Liguori D, Marino N, et al. Target-ing monocyte chemotactic protein-1 synthesis with bindarit induces tumorregression in prostate and breast cancer animal models. Clin Exp Metastasis2012, http://dx.doi.org/10.1007/s10585-012-9473-5.
[69] Balkwill F. Cancer and the chemokine network. Nature Reviews Cancer2004;4:540–50.
[70] Solinas G, Germano G, Mantovani A, Allavena P. Tumor-associatedmacrophages (TAM) as major players of the cancer-related inflammation.Journal of Leukocyte Biology 2009;86:1065–73.
[71] Bunt SK, Yang L, Sinha P, Clements VK, Leips J, Ostrand-Rosenberg S. Reducedinflammation in the tumor microenvironment delays the accumulationof myeloid-derived suppressor cells and limits tumor progression. CancerResearch 2007;67:10019–26.
[72] Cheng P, Corzo CA, Luetteke N, Yu B, Nagaraj S, Bui MM, et al. Inhibition ofdendritic cell differentiation and accumulation of myeloid-derived suppres-sor cells in cancer is regulated by S100A9 protein. The Journal of ExperimentalMedicine 2008;205:2235–49.
[73] Sinha P, Okoro C, Foell D, Freeze HH, Ostrand-Rosenberg S, Srikrishna G. Proin-flammatory S100 proteins regulate the accumulation of myeloid-derivedsuppressor cells. Journal of Immunology 2008;181:4666–75.
[74] Sawanobori Y, Ueha S, Kurachi M, Shimaoka T, Talmadge JE, Abe J, et al.Chemokine-mediated rapid turnover of myeloid-derived suppressor cells intumor-bearing mice. Blood 2008;111:5457–66.
[75] Yang L, Huang J, Ren X, Gorska AE, Chytil A, Aakre M, et al. Abrogation of TGFbeta signaling in mammary carcinomas recruits Gr-1+CD11b+ myeloid cellsthat promote metastasis. Cancer Cell 2008;13:23–35.
[76] Melani C, Chiodoni C, Forni G, Colombo MP. Myeloid cell expansion elicited bythe progression of spontaneous mammary carcinomas in c-erbB-2 transgenicBALB/c mice suppresses immune reactivity. Blood 2003;102:2138–45.
[77] Abraham SN, St John AL. Mast cell-orchestrated immunity to pathogens.Nature Reviews Immunology 2010;10:440–52.
[78] Kim BG, Li C, Qiao W, Mamura M, Kasprzak B, Anver M, et al. Smad4 sig-nalling in T cells is required for suppression of gastrointestinal cancer. Nature2006;441:1015–9.
[79] Mekori YA, Metcalfe DD. Mast cell–T cell interactions. Journal of Allergy andClinical Immunology 1999;104:517–23.
[80] Kalluri R, Zeisberg M. Fibroblasts in cancer. Nature Reviews Cancer2006;6:392–401.
[81] Goswami S, Sahai E, Wyckoff JB, Cammer M, Cox D, Pixley FJ, et al.Macrophages promote the invasion of breast carcinoma cells via acolony-stimulating factor-1/epidermal growth factor paracrine loop. CancerResearch 2005;65:5278–83.
[82] Pollard JW. Macrophages define the invasive microenvironment in breastcancer. Journal of Leukocyte Biology 2008;84:623–30.
[83] Ojalvo LS, Whittaker CA, Condeelis JS, Pollard JW. Gene expression analysis ofmacrophages that facilitate tumor invasion supports a role for Wnt-signalingin mediating their activity in primary mammary tumors. Journal of Immunol-
ogy 2010;184:702–12.[84] Pukrop T, Klemm F, Hagemann T, Gradl D, Schulz M, Siemes S, et al. Wnt5a signaling is critical for macrophage-induced invasion of breast cancer celllines. Proceedings of the National Academy of Sciences of the United Statesof America 2006;103:5454–9.
Biology 22 (2012) 234– 249 247
[85] Conti P, Castellani ML, Kempuraj D, Salini V, Vecchiet J, Tete S, et al. Roleof mast cells in tumor growth. Annals of Clinical and Laboratory Science2007;37:315–22.
[86] Hagemann T, Robinson SC, Schulz M, Trumper L, Balkwill FR, Binder C.Enhanced invasiveness of breast cancer cell lines upon co-cultivation withmacrophages is due to TNF-alpha dependent up-regulation of matrix metal-loproteases. Carcinogenesis 2004;25:1543–9.
[87] Vasiljeva O, Papazoglou A, Kruger A, Brodoefel H, Korovin M, Deussing J,et al. Tumor cell-derived and macrophage-derived cathepsin B promotesprogression and lung metastasis of mammary cancer. Cancer Research2006;66:5242–50.
[88] Rolny C, Mazzone M, Tugues S, Laoui D, Johansson I, Coulon C, et al. HRGinhibits tumor growth and metastasis by inducing macrophage polariza-tion and vessel normalization through downregulation of PlGF. Cancer Cell2011;19:31–44.
[89] Ceteci F, Ceteci S, Karreman C, Kramer BW, Asan E, Gotz R, et al.Disruption of tumor cell adhesion promotes angiogenic switch and pro-gression to micrometastasis in RAF-driven murine lung cancer. Cancer Cell2007;12:145–59.
[90] Png KJ, Halberg N, Yoshida M, Tavazoie SF. A microRNA regulon thatmediates endothelial recruitment and metastasis by cancer cells. Nature2011;481:190–4.
[91] Gaziel-Sovran A, Segura MF, Di Micco R, Collins MK, Hanniford D, Vega-Saenz de Miera E, et al. miR-30b/30d regulation of GalNAc transferasesenhances invasion and immunosuppression during metastasis. Cancer Cell2011;20:104–18.
[92] Le XF, Merchant O, Bast RC, Calin GA. The roles of microRNAs in the cancerinvasion-metastasis cascade. Cancer Microenvironment 2010;3:137–47.
[93] Poschke I, Mougiakakos D, Kiessling R. Camouflage and sabotage: tumorescape from the immune system. Cancer Immunology, Immunotherapy: CII2011;60:1161–71.
[94] Wilke CM, Wei S, Wang L, Kryczek I, Kao J, Zou W. Dual biological effectsof the cytokines interleukin-10 and interferon-gamma. Cancer Immunology2011;60:1529–41.
[95] Mumm JB, Emmerich J, Zhang X, Chan I, Wu L, Mauze S, et al. IL-10 elicits IFNgamma-dependent tumor immune surveillance. Cancer Cell2011;20:781–96.
[96] Watkins SK, Zhu Z, Riboldi E, Shafer-Weaver KA, Stagliano KE, SklavosMM, et al. FOXO3 programs tumor-associated DCs to become tolerogenicin human and murine prostate cancer. The Journal of Clinical Investigation2011;121:1361–72.
[97] Bockhorn M, Jain RK, Munn LL. Active versus passive mechanisms in metas-tasis: do cancer cells crawl into vessels, or are they pushed. Lancet Oncology2007;8:444–8.
[98] Butler TP, Gullino PM. Quantitation of cell shedding into efferent blood ofmammary adenocarcinoma. Cancer Research 1975;35:512–6.
[99] Klein CA. Parallel progression of primary tumours and metastases. NatureReviews Cancer 2009;9:302–12.
[100] Podsypanina K, Du YC, Jechlinger M, Beverly LJ, Hambardzumyan D, VarmusH. Seeding and propagation of untransformed mouse mammary cells in thelung. Science 2008;321:1841–4.
[101] Husemann Y, Geigl JB, Schubert F, Musiani P, Meyer M, Burghart E, et al.Systemic spread is an early step in breast cancer. Cancer Cell 2008;13:58–68.
[102] Stoecklein NH, Hosch SB, Bezler M, Stern F, Hartmann CH, Vay C, et al.Direct genetic analysis of single disseminated cancer cells for prediction ofoutcome and therapy selection in esophageal cancer. Cancer Cell 2008;13:441–53.
[103] Carmeliet P, Jain RK. Principles and mechanisms of vessel normalizationfor cancer and other angiogenic diseases. Nature Reviews Drug Discovery2011;10:417–27.
[104] van Zijl F, Krupitza G, Mikulits W. Initial steps of metastasis: cell invasion andendothelial transmigration. Mutation Research 2011;728:23–34.
[105] Wyckoff JB, Wang Y, Lin EY, Li JF, Goswami S, Stanley ER, et al. Direct visual-ization of macrophage-assisted tumor cell intravasation in mammary tumors.Cancer Research 2007;67:2649–56.
[106] Boimel PJ, Smirnova T, Zhou ZN, Wyckoff J, Park HI, Coniglio SJ, et al. Contri-bution of CXCL12 secretion to invasion of breast cancer cells. Breast CancerResearch 2012;14:R23.
[107] Muller A, Homey B, Soto H, Ge N, Catron D, Buchanan ME, et al. Involvementof chemokine receptors in breast cancer metastasis. Nature 2001;410:50–6.
[108] Hernandez L, Magalhaes MA, Coniglio SJ, Condeelis JS, Segall JE. Opposingroles of CXCR4 and CXCR7 in breast cancer metastasis. Breast Cancer Research2011;13:R128.
[109] Buxton IL, Yokdang N, Matz RM. Purinergic mechanisms in breast can-cer support intravasation, extravasation and angiogenesis. Cancer Letters2010;291:131–41.
[110] Bonnomet A, Brysse A, Tachsidis A, Waltham M, Thompson EW, Polette M,et al. Epithelial-to-mesenchymal transitions and circulating tumor cells. Jour-nal of Mammary Gland Biology and Neoplasia 2010;15:261–73.
[111] Labelle M, Schnittler HJ, Aust DE, Friedrich K, Baretton G, Vestweber D, et al.Vascular endothelial cadherin promotes breast cancer progression via trans-
forming growth factor beta signaling. Cancer Research 2008;68:1388–97.[112] Nierodzik ML, Karpatkin S. Thrombin induces tumor growth, metastasis, andangiogenesis: evidence for a thrombin-regulated dormant tumor phenotype.Cancer Cell 2006;10:355–62.

2 ancer
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
48 D. Spano et al. / Seminars in C
113] Im JH, Fu W, Wang H, Bhatia SK, Hammer DA, Kowalska MA, et al. Coagulationfacilitates tumor cell spreading in the pulmonary vasculature during earlymetastatic colony formation. Cancer Research 2004;64:8613–9.
114] Kunita A, Kashima TG, Morishita Y, Fukayama M, Kato Y, Tsuruo T,et al. The platelet aggregation-inducing factor aggrus/podoplanin pro-motes pulmonary metastasis. The American Journal of Pathology 2007;170:1337–47.
115] Kang Y, Siegel PM, Shu W, Drobnjak M, Kakonen SM, Cordon-Cardo C, et al. Amultigenic program mediating breast cancer metastasis to bone. Cancer Cell2003;3:537–49.
116] Minn AJ, Gupta GP, Siegel PM, Bos PD, Shu W, Giri DD, et al. Genes that mediatebreast cancer metastasis to lung. Nature 2005;436:518–24.
117] Gupta GP, Nguyen DX, Chiang AC, Bos PD, Kim JY, Nadal C, et al. Mediators ofvascular remodelling co-opted for sequential steps in lung metastasis. Nature2007;446:765–70.
118] Sonoshita M, Aoki M, Fuwa H, Aoki K, Hosogi H, Sakai Y, et al. Suppression ofcolon cancer metastasis by Aes through inhibition of Notch signaling. CancerCell 2011;19:125–37.
119] Giampieri S, Manning C, Hooper S, Jones L, Hill CS, Sahai E. Localized andreversible TGFbeta signalling switches breast cancer cells from cohesive tosingle cell motility. Nature Cell Biology 2009;11:1287–96.
120] Padua D, Zhang XH, Wang Q, Nadal C, Gerald WL, Gomis RR, et al. TGFbetaprimes breast tumors for lung metastasis seeding through angiopoietin-like4. Cell 2008;133:66–77.
121] Albrecht I, Christofori G. Molecular mechanisms of lymphangiogenesis indevelopment and cancer. International Journal of Developmental Biology2011;55:483–94.
122] Alitalo K, Carmeliet P. Molecular mechanisms of lymphangiogenesis in healthand disease. Cancer Cell 2002;1:219–27.
123] Saharinen P, Petrova TV. Molecular regulation of lymphangiogenesis. Annalsof the New York Academy of Sciences 2004;1014:76–87.
124] Burton JB, Priceman SJ, Sung JL, Brakenhielm E, An DS, Pytowski B, et al. Sup-pression of prostate cancer nodal and systemic metastasis by blockade of thelymphangiogenic axis. Cancer Research 2008;68:7828–37.
125] Crnic I, Strittmatter K, Cavallaro U, Kopfstein L, Jussila L, Alitalo K, et al. Lossof neural cell adhesion molecule induces tumor metastasis by up-regulatinglymphangiogenesis. Cancer Research 2004;64:8630–8.
126] He Y, Kozaki K, Karpanen T, Koshikawa K, Yla-Herttuala S, Takahashi T, et al.Suppression of tumor lymphangiogenesis and lymph node metastasis byblocking vascular endothelial growth factor receptor 3 signaling. Journal ofthe National Cancer Institute 2002;94:819–25.
127] Krishnan J, Kirkin V, Steffen A, Hegen M, Weih D, Tomarev S, et al. Differ-ential in vivo and in vitro expression of vascular endothelial growth factor(VEGF)-C and VEGF-D in tumors and its relationship to lymphatic metastasisin immunocompetent rats. Cancer Research 2003;63:713–22.
128] Lin J, Lalani AS, Harding TC, Gonzalez M, Wu WW, Luan B, et al. Inhibi-tion of lymphogenous metastasis using adeno-associated virus-mediatedgene transfer of a soluble VEGFR-3 decoy receptor. Cancer Research2005;65:6901–9.
129] Wong SY, Haack H, Crowley D, Barry M, Bronson RT, Hynes RO. Tumor-secreted vascular endothelial growth factor-C is necessary for prostate cancerlymphangiogenesis, but lymphangiogenesis is unnecessary for lymph nodemetastasis. Cancer Research 2005;65:9789–98.
130] Brideau G, Makinen MJ, Elamaa H, Tu H, Nilsson G, Alitalo K, et al. Endostatinoverexpression inhibits lymphangiogenesis and lymph node metastasis inmice. Cancer Research 2007;67:11528–35.
131] Caunt M, Mak J, Liang WC, Stawicki S, Pan Q, Tong RK, et al. Block-ing neuropilin-2 function inhibits tumor cell metastasis. Cancer Cell2008;13:331–42.
132] Sini P, Samarzija I, Baffert F, Littlewood-Evans A, Schnell C, Theuer A, et al.Inhibition of multiple vascular endothelial growth factor receptors (VEGFR)blocks lymph node metastases but inhibition of VEGFR-2 is sufficient to sen-sitize tumor cells to platinum-based chemotherapeutics. Cancer Research2008;68:1581–92.
133] He Y, Rajantie I, Pajusola K, Jeltsch M, Holopainen T, Yla-Herttuala S, et al.Vascular endothelial cell growth factor receptor 3-mediated activation oflymphatic endothelium is crucial for tumor cell entry and spread via lym-phatic vessels. Cancer Research 2005;65:4739–46.
134] Padera TP, Kadambi A, di Tomaso E, Carreira CM, Brown EB, Boucher Y, et al.Lymphatic metastasis in the absence of functional intratumor lymphatics.Science 2002;296:1883–6.
135] Ristimaki A, Narko K, Enholm B, Joukov V, Alitalo K. Proinflammatorycytokines regulate expression of the lymphatic endothelial mitogen vas-cular endothelial growth factor-C. The Journal of Biological Chemistry1998;273:8413–8.
136] Tsai PW, Shiah SG, Lin MT, Wu CW, Kuo ML. Up-regulation of vascularendothelial growth factor C in breast cancer cells by heregulin-beta 1. Acritical role of p38/nuclear factor-kappa B signaling pathway. The Journal ofBiological Chemistry 2003;278:5750–9.
137] Orlandini M, Marconcini L, Ferruzzi R, Oliviero S. Identification of a c-fos-induced gene that is related to the platelet-derived growth factor/vascular
endothelial growth factor family. Proceedings of the National Academy ofSciences of the United States of America 1996;93:11675–80.138] Shields JD, Fleury ME, Yong C, Tomei AA, Randolph GJ, Swartz MA. Autologouschemotaxis as a mechanism of tumor cell homing to lymphatics via interstitialflow and autocrine CCR7 signaling. Cancer Cell 2007;11:526–38.
Biology 22 (2012) 234– 249
[139] Alitalo K, Tammela T, Petrova TV. Lymphangiogenesis in development andhuman disease. Nature 2005;438:946–53.
[140] Cabioglu N, Yazici MS, Arun B, Broglio KR, Hortobagyi GN, Price JE, et al. CCR7and CXCR4 as novel biomarkers predicting axillary lymph node metastasis inT1 breast cancer. Clinical Cancer Research: An Official Journal of the AmericanAssociation for Cancer Research 2005;11:5686–93.
[141] Takeuchi H, Fujimoto A, Tanaka M, Yamano T, Hsueh E, Hoon DS. CCL21chemokine regulates chemokine receptor CCR7 bearing malignant melanomacells. Clinical Cancer Research 2004;10:2351–8.
[142] Gunther K, Leier J, Henning G, Dimmler A, Weissbach R, Hohenberger W,et al. Prediction of lymph node metastasis in colorectal carcinoma by expres-sion of chemokine receptor CCR7. International Journal of Cancer 2005;116:726–33.
[143] Wang J, Xi L, Gooding W, Godfrey TE, Ferris RL. Chemokine receptors 6 and7 identify a metastatic expression pattern in squamous cell carcinoma of thehead and neck. Advances in Otorhinolaryngology 2005;62:121–33.
[144] Heresi GA, Wang J, Taichman R, Chirinos JA, Regalado JJ, Lichtstein DM, et al.Expression of the chemokine receptor CCR7 in prostate cancer presentingwith generalized lymphadenopathy: report of a case, review of the liter-ature, and analysis of chemokine receptor expression. Urologic Oncology2005;23:261–7.
[145] Takanami I. Overexpression of CCR7 mRNA in nonsmall cell lung cancer:correlation with lymph node metastasis. International Journal of Cancer2003;105:186–9.
[146] Ding Y, Shimada Y, Maeda M, Kawabe A, Kaganoi J, Komoto I, et al. Associa-tion of CC chemokine receptor 7 with lymph node metastasis of esophagealsquamous cell carcinoma. Clinical Cancer Research: An Official Journal of theAmerican Association for Cancer Research 2003;9:3406–12.
[147] Mashino K, Sadanaga N, Yamaguchi H, Tanaka F, Ohta M, Shibuta K, et al.Expression of chemokine receptor CCR7 is associated with lymph node metas-tasis of gastric carcinoma. Cancer Research 2002;62:2937–41.
[148] Madlener S, Saiko P, Vonach C, Viola K, Huttary N, Stark N, et al. Multifacto-rial anticancer effects of digalloyl-resveratrol encompass apoptosis, cell-cyclearrest, and inhibition of lymphendothelial gap formation in vitro. British Jour-nal of Cancer 2010;102:1361–70.
[149] Scheel C, Onder T, Karnoub A, Weinberg RA. Adaptation versus selection: theorigins of metastatic behavior. Cancer Research 2007;67:11476–9 [discussion9–80].
[150] Price JT, Thompson EW. Mechanisms of tumour invasion and metasta-sis: emerging targets for therapy. Expert Opinion on Therapeutic Targets2002;6:217–33.
[151] Stoletov K, Kato H, Zardouzian E, Kelber J, Yang J, Shattil S, et al. Visualiz-ing extravasation dynamics of metastatic tumor cells. Journal of Cell Science2010;123:2332–41.
[152] Huh SJ, Liang S, Sharma A, Dong C, Robertson GP. Transiently entrapped cir-culating tumor cells interact with neutrophils to facilitate lung metastasisdevelopment. Cancer Research 2010;70:6071–82.
[153] Nieswandt B, Hafner M, Echtenacher B, Mannel DN. Lysis of tumor cellsby natural killer cells in mice is impeded by platelets. Cancer Research1999;59:1295–300.
[154] Palumbo JS. Mechanisms linking tumor cell-associated procoagulant func-tion to tumor dissemination. Seminars in Thrombosis and Hemostasis2008;34:154–60.
[155] Erpenbeck L, Schon MP. Deadly allies: the fatal interplay between plateletsand metastasizing cancer cells. Blood 2010;115:3427–36.
[156] Gay LJ, Felding-Habermann B. Contribution of platelets to tumour metastasis.Nature Reviews Cancer 2011;11:123–34.
[157] Sierko E, Wojtukiewicz MZ. Inhibition of platelet function: does it offer achance of better cancer progression control. Seminars in Thrombosis andHemostasis 2007;33:712–21.
[158] Labelle M, Begum S, Hynes RO. Direct signaling between platelets and can-cer cells induces an epithelial–mesenchymal-like transition and promotesmetastasis. Cancer Cell 2011;20:576–90.
[159] Hejna M, Raderer M, Zielinski CC. Inhibition of metastases by anticoagulants.Journal of the National Cancer Institute 1999;91:22–36.
[160] Bae JS, Lee SH, Kim JE, Choi JY, Park RW, Yong Park J, et al. Betaig-h3 supports keratinocyte adhesion, migration, and proliferation throughalpha3beta1 integrin. Biochemical and Biophysical Research Communica-tions 2002;294:940–8.
[161] Kim JE, Kim SJ, Jeong HW, Lee BH, Choi JY, Park RW, et al. RGD peptides releasedfrom beta ig-h3, a TGF-beta-induced cell-adhesive molecule, mediate apopto-sis. Oncogene 2003;22:2045–53.
[162] Ma C, Rong Y, Radiloff DR, Datto MB, Centeno B, Bao S, et al. Extracellu-lar matrix protein betaig-h3/TGFBI promotes metastasis of colon cancer byenhancing cell extravasation. Genes & Development 2008;22:308–21.
[163] Weis S, Cui J, Barnes L, Cheresh D. Endothelial barrier disruption by VEGF-mediated Src activity potentiates tumor cell extravasation and metastasis.The Journal of Cell Biology 2004;167:223–9.
[164] Coughlin SR. Protease-activated receptors in hemostasis, thrombosis and vas-cular biology. Journal of Thrombosis and Haemostasis 2005;3:1800–14.
[165] Gavard J, Gutkind JS. Protein kinase C-related kinase and ROCK are
required for thrombin-induced endothelial cell permeability downstreamfrom Galpha12/13 and Galpha11/q. The Journal of Biological Chemistry2008;283:29888–96.[166] Steeg PS, Camphausen KA, Smith QR. Brain metastases as preventive andtherapeutic targets. Nature Reviews Cancer 2011;11:352–63.

Cancer
D. Spano et al. / Seminars in[167] Zhang C, Yu D. Microenvironment determinants of brain metastasis. Cell Bio-science 2011;1:8.
[168] Kienast Y, von Baumgarten L, Fuhrmann M, Klinkert WE, Goldbrunner R,Herms J, et al. Real-time imaging reveals the single steps of brain metastasisformation. Nature Medicine 2010;16:116–22.
[169] Bos PD, Zhang XH, Nadal C, Shu W, Gomis RR, Nguyen DX, et al. Genes thatmediate breast cancer metastasis to the brain. Nature 2009;459:1005–9.
[170] Lee KY, Kim YJ, Yoo H, Lee SH, Park JB, Kim HJ. Human brain endothelialcell-derived COX-2 facilitates extravasation of breast cancer cells across theblood–brain barrier. Anticancer Research 2011;31:4307–13.
[171] Lorger M, Felding-Habermann B. Capturing changes in the brain microenvi-ronment during initial steps of breast cancer brain metastasis. The AmericanJournal of Pathology 2010;176:2958–71.
[172] Marchetti D, Li J, Shen R. Astrocytes contribute to the brain-metastaticspecificity of melanoma cells by producing heparanase. Cancer Research2000;60:4767–70.
[173] Marchetti D, Aucoin R, Blust J, Murry B, Greiter-Wilke A. p75 neurotrophinreceptor functions as a survival receptor in brain-metastatic melanoma cells.Journal of Cellular Biochemistry 2004;91:206–15.
[174] Langley RR, Fidler IJ. The seed and soil hypothesis revisited—the role of
tumor–stroma interactions in metastasis to different organs. InternationalJournal of Cancer 2011;128:2527–35.[175] Hiratsuka S, Watanabe A, Aburatani H, Maru Y. Tumour-mediated upregu-lation of chemoattractants and recruitment of myeloid cells predetermineslung metastasis. Nature Cell Biology 2006;8:1369–75.
Biology 22 (2012) 234– 249 249
[176] Kaplan RN, Riba RD, Zacharoulis S, Bramley AH, Vincent L, Costa C, et al.VEGFR1-positive haematopoietic bone marrow progenitors initiate the pre-metastatic niche. Nature 2005;438:820–7.
[177] Hiratsuka S, Watanabe A, Sakurai Y, Akashi-Takamura S, Ishibashi S,Miyake K, et al. The S100A8-serum amyloid A3-TLR4 paracrine cas-cade establishes a pre-metastatic phase. Nature Cell Biology 2008;10:1349–55.
[178] Lin EY, Jones JG, Li P, Zhu L, Whitney KD, Muller WJ, et al. Progression tomalignancy in the polyoma middle T oncoprotein mouse breast cancer modelprovides a reliable model for human diseases. The American Journal of Pathol-ogy 2003;163:2113–26.
[179] Erler JT, Bennewith KL, Cox TR, Lang G, Bird D, Koong A, et al. Hypoxia-inducedlysyl oxidase is a critical mediator of bone marrow cell recruitment to formthe premetastatic niche. Cancer Cell 2009;15:35–44.
[180] Oskarsson T, Acharyya S, Zhang XH, Vanharanta S, Tavazoie SF, Morris PG,et al. Breast cancer cells produce tenascin C as a metastatic niche componentto colonize the lungs. Nature Medicine 2011;17:867–74.
[181] Moller HD, Ralfkjaer U, Cremers N, Frankel M, Pedersen RT, Klingelhofer J, et al.Role of fibulin-5 in metastatic organ colonization. Molecular Cancer Research2011;9:553–63.
[182] Bellahcene A, Castronovo V, Ogbureke KU, Fisher LW, Fedarko NS. Smallintegrin-binding ligand N-linked glycoproteins (SIBLINGs): multifunctionalproteins in cancer. Nature Reviews Cancer 2008;8:212–26.
[183] Wai PY, Kuo PC. Osteopontin: regulation in tumor metastasis. Cancer Metas-tasis Reviews 2008;27:103–18.






![arXiv:1503.00777v1 [cond-mat.mtrl-sci] 2 Mar 2015 · to regulate the interaction between di erent molecular electronic states by modulating inter- and intra-molecular couplings, by](https://img.dokumen.tips/doc/110x75/5f5b2b5c5d7b7621830aaea0/arxiv150300777v1-cond-matmtrl-sci-2-mar-2015-to-regulate-the-interaction-between.jpg)