Embed Size (px)
Citation preview

Mobitz I versus Mobitz II: through storytelling
Learning
Author: Andrea Novak, RN, MS, CEN, Fayetteville, North Carolina
M ' n emon ic dev ices a re wonder fu l tools to he lp us , r e m e m b e r those drugs , a lgor i thms, a n d such,
b u t I stil l ge t confused. Which O in the m n e m o n i c for t he 12 crania l ne rves is optic, olfactory, or oculomotor? I found the b e s t w a y to r e m e m b e r is to tel l myse l f a story. As a nurse educator , I a lso use th is t e chn ique w i th the nurses a t m y hosp i t a l to he lp t h e m in te rpre t b lood gas read ings , a n d to d i f ferent ia te b e t w e e n Mo- bi tz I a n d Mobi tz II h e a r t blocks.
It u s e d to b e a g i a n t c ram sess ion every 2 yea r s w h e n it w a s t ime for ACLS "recert ." H o w to r e m e m - ber t he di f ference b e t w e e n the s e c o n d - d e g r e e b locks? The only w a y I could g e t p a s t th i s men ta l "b lock" w a s to tel l myse l f a s tory t ha t w o u l d m a k e i t e a sy for m e to unde r s t and , a s tory t ha t has no th ing to do w i th u n d e r s t a n d i n g a c o m p l i c a t e d pa thophys io logy .
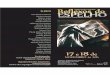
Mobi tz I is also k n o w n as "Wenckebach . " This a lone can b e confusing, a n d so m y story beg ins . Mo- bi tz I (or "one") s o u n d s jus t l ike t he word won. There ' s a W in "Won" a n d in "Wenckebach , " so a Mobi tz I is also k n o w n as Wenckebach . To d i s t i n g u i s h the blocks, look a t t he fol lowing strips. Not ice in F igure i t h a t the QRS c o m p l e x e s b e g i n to pul l a w a y from the P waves . I t ' s a l m o s t l ike t h e y are runner s rac ing across t h e s t r ip w i th each QRS pu l l i ng further a h e a d of i ts pa r tne r P w a v e unt i l one QRS "falls down ," w h i c h is, of course, t he b locked beat . This r h y t h m m u s t b e W e n c k e b a c h b e c a u s e t he re is a " Winner" in m y i m a g i n a r y race (aka Mobi tz I [ Won]).
F i g u r e 2 is an e x a m p l e of t y p e II s e c o n d - d e g r e e b lock or Mob i t z II. In t h i s d y s r h y t h m i a , look for a c o n s t a n t PR i n t e r v a l w i t h t h e b l o c k e d bea t s . Both
d y s r h y t h m i a s h a v e a r e c o g n i z a b l e pa t t e rn , h o w e v e r b iza r re i t m a y seem,
On to b l o o d gases . The only v a l u e s w e n e e d to r e m e m b e r to i n t e r p r e t a r t e r i a l b l o o d g a s r e a d i n g s a re c a r b o n d i o x i d e (CO2), b i c a r b o n a t e (HCO3), a n d pH. Usua l ly , t h e n o r m a l l eve l s a re l i s t e d on t h e ABG repo r t form, b u t jus t in case, m e m o r i z e t h e s e n u m - bers : pH, 7.35 to 7.45; p a r t i a l a r t e r i a l p r e s s u r e of c a r b o n d i o x i d e (Paco2) u s e s t he s a m e n u m b e r s : 35 to 45 m m Hg a n d HCO3, 22 to 26 m m o l / L . To in te r - p r e t a b l o o d g a s r e a d i n g , s t a r t w i t h t h e pH. If t he pH is l e ss t h a n 7.35, i t ' s an acid; if the p H is more t h a n
Ms. Novak was Emergency Nurse Educator, South Shore Hospi- tal, S. Weymouth, Massachusetts.
7.45, i t ' s a b a s e or a lka lo t ic . N e x t look a t t h e Paco2 va lue , w h i c h ref lec ts t he r e s p i r a t o r y c o m p o n e n t of t he ABG s ince CO2 goes in a n d out of t he lungs . If more CO2 goes out t h a n is c o m i n g in (as w i t h t he h y p e r v e n t i l a t i n g p a t i e n t w h o is blowing off CO2), i t wi l l b e r e f l ec t ed as a low Paco2 v a l u e on the ABG report . A Paco2 v a l u e of 20 can b e i d e n t i f i e d as res- p i r a to ry a lka los i s . R e s p i r a t o r y a lka los i s = " low- b l o w CO2." By u s i n g p r o c e s s of e l imina t ion , a h i g h Paco2 level i n d i c a t e s r e s p i r a t o r y ac idos is .
N e x t c h e c k the HCO3 va lue . Th i s n u m b e r , if ou t of l ine, i n d i c a t e s t h a t t h e k i d n e y s h a v e " k i c k e d in" to h e l p buf fe r t h e sy s t e m. If t h e k i d n e y s a re in- vo lved , w e k n o w t h e r e is a m e t a b o l i c c o m p o n e n t to e i t he r a ch ron ic c o n d i t i o n or one t h a t is a c u t e l y t r a u m a t i c (i.e., c a r d i a c ar res t ) . Ask yourse l f t h i s ques t ion : is t he HCO3 v a l u e a b o v e or b e l o w the nor- m a l r a n g e ? Keep t h a t n u m b e r in m i n d a n d refer a g a i n to t h e pH. Was t h a t n u m b e r ~ or ~? The p a t i e n t wi l l b e in m e t a b o l i c d e p e n d i n g on w h i c h w a y t h e a r rows point . If your p a t i e n t has a pH of 7.50 a n d t h e HCO3 is 30 (bo th v a l u e s t), t h e n the p a t i e n t is in a s t a t e of m e t a b o l i c a lka los i s . If your p a t i e n t h a s a pH of 7.23 a n d a n HCO3 of 20, t h e pa - t i en t is in a s t a t e of m e t a b o l i c ac idos i s (bo th ~).
" A h a ! " you say; w h a t if t h e a r rows d o n ' t m a t c h ? T h e n you n e e d to d e t e r m i n e w h e t h e r the p a t i e n t is in a s t a t e of c o m p e n s a t i o n or an u n c o m p e n s a t e d s ta te , a n d w h i c h c o m p o n e n t is t he p r i m a r y cause . Go b a c k a n d s t u d y the ABG va lues . Are all t h r e e c o m p l e t e l y " a b b y " - n o r m a l ? If so, i t m e a n s t he b o d y is t r y i n g to a c h i e v e a n o r m a l level , a n d the p a t i e n t is uncompensated (pH, 7.29; Paco2, 47; HCO3, 19). If t he pH is normal , b u t b o t h t h e Paco2 a n d HCO3 va lues are abnormal , t he b o d y has successful ly com- pensated b e c a u s e i t ha s a t t a i n e d a r ange tha t is com- pa t ib l e for life (pH, 7.38; Paco2; 29; HCO3, 15). Finally, w h a t is the p r imary cause of the condi t ion? Answer : w h i c h e v e r va lue follows in t he s a m e direct ion as the pH. For example , if the pH is 7.25, Paco2 is 28, and HCO3 is 17, t he p a t i e n t ' s p r ima ry condi t ion is me ta -
For reprints, write Ms. Andrea Novak, RN, MS, CEN, 331 Jura Dr., Fayetteville, NC 28303. J EMERG NURS 1995;21:80-1 Copyright �9 1995 by the Emergency Nurses Association. 0099-t767/95 $3.00 + 0 18 /9 /61430
80 Volume 21, Number 1

Novak/JOURNAL OF ICME]RGICNC~ NURSING
, l i l l i i l l l l , , , , , , i , , i [ i i i i i i i i I i l i l J i l l , [ I I I ' m I I I t I [ 111 I I I I f l a i l ] I 1 i l l l i t J J i l l i
d ~ . . . . . . . . . . . . . . . . . . . , . . . . . . . . . . . . . . . . . . . . ', ', *, : ', ', ' , , , , ', ~ ', ', ', ', ', ', ', ', ', ', ', ', ', I ', ', ', I ', . . . . . . . . ,
.: i l,[,:iiiU.,.,iii ~ i [i[ i~] ![[[! !![][ !!ill!!!!!'!]! !!:!!![!!!!! ! !!!! !:~! ~[ ~ ,.~,1 ~ ! 5 7 F ~ ~,'fJlii:[iii:iiiiiiiiiiiii[iiiiiiiiiiiiiiiiiiiil],iiii,~iiiilH 1111111111~~
F i g u r e 1
EKO t r ac ing s h o w s Mobi tz I ( W e n c k e b a c h ) s e c o n d - d e g r e e a t r i oven t r i cu l a r h e a r t block. Note b locked b e a t i n d i c a t e d by s e c o n d arrow, w h e r e QRS "fell d o w n . "
I I I'II I I I I ', ', ; ', ', I I ', ", ', ', ', : ', ', ', I I ', ', ', ', : I ', ', (': ', ', ', ', : ', ', I ', I ', I I ', I ', I : I I [ [
i]iii:~i111!ii!!!!!I~!!!i[iiii[i] L"iiii!,,:!!!!!!!iiii,'.ill][
I ~ I I I ` ~ : ~ - ~ : ~ ` ~ I ~ : I ~ ` ~ I ~ ` ` I ~ I ~ I ~ : I ~ ` ~ I ` ~ I I ~ ? - ~ I I ~ I ~ ~ I I I I I I ~ I ~ ` I ~ I ` ` ~ ` ~ I ~ ` I ` ` ~ I ~ I ~ I ~ I I I ~ ` ~ I ~ I ~ ` . ~ . ~ I ` ~ ` ~ ` ` ',
v~
F i g u r e 2
S e c o n d - d e g r e e a t r ioven t r i cu la r h e a r t b lock (Mobi tz II). There is a c o n s t a n t PR in te rva l w i t h the b locked bea t s .
b o l i c a c i d o s i s b e c a u s e b o t h t h e p H a n d HCO3 n u m b e r s
a r e low. A r e s p i r a t o r y a l k a l o s i s a l so ex i s t s , a s i n d i c a t e d
b y t h e l o w Paco2 v a l u e ; t h i s is t h e b o d y ' s a t t e m p t to
c o m p e n s a t e for t h e m e t a b o l i c a c i d o s i s .
T r y u s i n g t h i s s t o r y to f i g u r e o u t y o u r A B G s ; i t
w o r k s .
Oh , yes , b a c k to t h e c r a n i a l n e r v e s . You r e m e m -
b e r f r o m n u r s i n g s c h o o l t h a t m n e m o n i c " O n O l d
O l y m p u s T o w e r i n g T o p s . . . . ," b u t w h i c h O is
w h i c h ? Te l l y o u r s e l f a s to ry , w h e n y o u w i n b y a
nose , y o u c o m e i n first, so c r a n i a l n e r v e I is O l f ac to ry .
M o s t of u s h a v e t w o eyes , so c r a n i a l n e r v e II is Op-
t ic . T h a t l e a v e s t h e l a s t O of t h e m n e m o n i c to b e
O c u l o m o t o r ( c r a n i a l n e r v e III).
Dr. Kirksey is Assistant Professor of Nursing, The University of Texas Health Science Center at San Antonio School of Nursing, San Antonio, Texas. Dr. Ashley is Director of Medical Nursing, Ben Taub General Hospital, Houston, Texas. Ms. Williamson is a recent graduate of The University of Texas Health Science Cen- ter at San Antonio School of Nursing. Mr. Garza is a staff nurse, Emergency Department, University Hospital, San Antonio, Texas.
For reprints, write Kenn M. Kirksey, RN, PhD, CS, CEN, CNS, 11226 Candle Park, San Antonio, TX 78249. J EMERG NURS 1995;21:81-3. Copyright �9 1995 by the Emergency Nurses Association. 0099-1767/95 $3.00 + 0 18/9 /61504
February 1995 81
























![Visual storytelling [storytelling matters]](https://img.dokumen.tips/doc/110x75/54b865614a795970478b4802/visual-storytelling-storytelling-matters.jpg)


