Embed Size (px)
Citation preview

Personalized Medicine and Imaging
MMP-1 and Pro-MMP-10 as Potential UrinaryPharmacodynamic Biomarkers of FGFR3-Targeted Therapyin Patients with Bladder Cancer
Xiangnan Du1, Benjamin C. Lin2, Qian-Rena Wang1, Hao Li1, Ellen Ingalla1, Janet Tien1, Isabelle Rooney3,Avi Ashkenazi4, Elicia Penuel2, and Jing Qing1
AbstractPurpose: The aim of this study was to identify noninvasive pharmacodynamic biomarkers of FGFR3-
targeted therapies in bladder cancer to facilitate the clinical development of experimental agent targeting
FGFR3.
ExperimentalDesign:Potential soluble pharmacodynamic biomarkers of FGFR3were identified using a
combination of transcriptional profiling and biochemical analyses in preclinical models. Two matrix
metalloproteinases (MMP),MMP-1 andMMP-10, were selected for further studies in humanbladder cancer
xenograftmodels treatedwith a specific anti-FGFR3monoclonal antibody, R3Mab. Serumandurinary levels
of MMP-1 and MMP-10 were determined in healthy donors and patients with bladder cancer. The
modulation of MMP-1 and MMP-10 by R3Mab in patients with bladder cancer was further evaluated in
a phase I dose-escalation study.
Results:MMP-1 andMMP-10mRNA and proteinwere downmodulated by FGFR3 shRNA andR3Mab in
bladder cancer cell lines. FGFR3 signaling promoted the expression and secretion of MMP-1 and pro-MMP-
10 in a MEK-dependent fashion. In bladder cancer xenograft models, R3Mab substantially blocked tumor
progression and reduced the protein levels of humanMMP-1 and pro-MMP-10 in tumor tissues as well as in
mouse serum. Furthermore, both MMP-1 and pro-MMP-10 were elevated in the urine of patients with
advanced bladder cancer. In a phase I dose-escalation trial, R3Mab administration resulted in an acute
reduction of urinary MMP-1 and pro-MMP-10 levels in patients with bladder cancer.
Conclusion: These findings reveal a critical role of FGFR3 in regulating MMP-1 and pro-MMP-10
expression and secretion, and identify urinary MMP-1 and pro-MMP-10 as potential pharmacodynamic
biomarkers for R3Mab in patients with bladder cancer. Clin Cancer Res; 20(24); 6324–35. �2014 AACR.
IntroductionBladder cancer is the fifth most common cancer world-
wide, with an estimated 386,330 new cases and 150,200deaths in2008 (1).Despite radical cystectomyand intensivechemotherapy, the 5-year survival rate for patients with
localized and distant metastatic bladder cancer is approx-imately 35% and 5% to 6%, respectively (2). Thus, noveltherapeutic agents are urgently needed to improve patientoutcome.
FGFR3 belongs to a family of four structurally andfunctionally related single-transmembrane receptor tyro-sine kinases, which transduce signals frommany of the 22identified FGF polypeptides in humans (3–5). Uponcanonical FGF binding in a ternary complex with heparinsulfate proteoglycans, FGFR3 undergoes dimerization,autophosphorylation, and activation. This triggers therecruitment of adaptor proteins, such as FGFR substrate2a (FRS2a), leading to activation of several downstreamsignaling cascades, including the Ras–Raf–MAPK,PI3K–Akt–mTOR, and phospholipase C g (PLCg) path-ways. Dysregulation and activation of FGFR3 through avariety of mechanisms has been identified in a widespectrum of human cancers, including multiple myeloma(6–8), squamous cell carcinoma of the lung (9, 10),breast cancer (11, 12), glioblastoma (13, 14), testicularcancer (15), and bladder cancer (16).
1Translational Oncology, Genentech, Inc., South San Francisco, California.2Oncology Biomarker Development, Genentech, Inc., South San Fran-cisco, California. 3Oncology Clinical Science ECD, Genentech, Inc., SouthSan Francisco, California. 4Research Oncology, Genentech, Inc., SouthSan Francisco, California.
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
X. Du and B.C. Lin contributed equally to this article.
Corresponding Authors: Elicia Penuel, ES Oncology Biomarker Devel-opment, Genentech, Inc., 1 DNA Way, South San Francisco, CA 94080.Phone: 650-467-7214; Fax: 650-467-5470; E-mail: [email protected];and Jing Qing, Department of Translational Oncology, Genentech, Inc.,1 DNA Way, South San Francisco, CA 94080. Phone: 650-467-8266;E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-13-3336
�2014 American Association for Cancer Research.
ClinicalCancer
Research
Clin Cancer Res; 20(24) December 15, 20146324
on November 11, 2020. © 2014 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 17, 2014; DOI: 10.1158/1078-0432.CCR-13-3336

Specifically, accumulating genetic and functional evi-dence has established FGFR3 as a potential oncogenic driverand therapeutic target in bladder cancer. About 60% to 70%of non–muscle-invasive low-grade papillary and 11% to16% of muscle-invasive bladder tumors contain somaticactivating mutations in FGFR3 (17–20), the majority ofwhich are missense substitutions in the extracellular orjuxtamembrane domains of FGFR3 that lead to ligand-independent receptor dimerization and activation. Besidesactivating mutations, gene fusion between FGFR3 andTACC3 or BAIAP2L1 has been recently identified in bladdercancer cell lines as well as primary tumors, resulting inaberrant regulation and activation of FGFR3 (21, 22). Inaddition, high levels of wild-type FGFR3 is found in morethan 40% to 50%ofmuscle-invasive andmetastatic bladdercancers (19, 23). Moreover, expression of activated FGFR3transformsNIH-3T3 cells andhematopoietic cells in cultureand confers tumorigenicity in vivo (24–26). Importantly,several preclinical studies using genetic and/or pharmaco-logic approaches have demonstrated that inhibition ofFGFR3 in bladder cancer suppresses cell proliferation inculture and tumor growth in xenograft and orthotopicmodels (23, 27–31). Collectively, these data suggest thatFGFR3 could be an oncogenic driver in a subset of bladdercancers and hence that targeting this receptor may betherapeutically beneficial. Indeed, several small-moleculeinhibitors of FGFR have entered into clinical investigationsfor cancer therapy (32–34). A specific human monoclonalanti-FGFR3 antibody we developed (designated R3Mabor MFGR1877S) has been evaluated in a phase I clinicaltrial (35).
While the advances in developing FGFR3-targeted ther-apeutic agents are encouraging, identification and valida-tion of accessible, mechanism-based biomarkers to gaugetargeted pharmacodynamic modulation is urgently need-ed to facilitate clinical investigation. In the current study,combining transcriptional profiling and biochemicalapproaches, we identified MMP-1 and pro-MMP-10 asbona fide FGFR3 downstream targets and the urinary levelof these metalloproteinases could serve as potential easilyaccessible pharmacodynamic biomarkers for FGFR3-tar-geted therapy in bladder cancer.
Materials and MethodsCell culture, siRNA transfection, and reagents
Bladder cancer cell lines RT112 which contain FGFR3-TACC3 fusion endogenously (21) was purchased from theGerman Collection of Microorganisms and Cell Cultures(DSMZ, Germany). RT112 cells stably expressing doxycy-cline-inducible shRNAs targeting FGFR3 or enhanced GFP(EGFP) were described in our previous study (29). Bladdercancer cell line UMUC-14 which contains FGFR3S249C wasobtained as described (29). Bladder cancer cell line SW780which contains FGFR3-BAIAP2L1 fusion (21) was pur-chased from ATCC. All cells are stored at early passages ina central cell bank at Genentech. Cell lines were authenti-cated by short tandem repeat and genotyped upon reexpan-sions, and experiments were carried out with low-passagecultures of these stocks. The cells were maintained withDMEM supplemented with 10% FBS (Sigma), 100 U/mLpenicillin, 0.1mg/mL streptomycin, and L-glutamine underconditions of 5% CO2 at 37
�C.Rapamycin and PI3K inhibitor LY294002 were obtained
from Cell Signaling Technology. A potent and selectiveMEK1/2 inhibitor PD0325901 (Pfizer) was purchased fromSynthesis Med Chem.
All RNA interference experiments were carried out withON-TARGETplus siRNAs (25 nmol/L, Dharmacon). Cellswere transfected with Lipofectamine RNAiMax (Invitro-gen), and RNA or conditioned medium was collected at48 or 72 hours after transfection.
Gene expression array and quantitative reversetranscriptase-PCR analyses of mRNA expression level
Themicroarray studies with RT112 cells expressing doxy-cycline-inducible shRNAs targeting FGFR3 or EGFP wereconducted as described (36), and can be accessed at theGene Expression Omnibus database under the accessionnumber GSE41035. To detect transcripts of MMP-1 andMMP-10, quantitative reverse transcriptase (qRT)-PCR wasperformed with predesigned TaqMan gene expressionassays (Applied Biosystems). All reactions were performedat least in triplicates. The relative amount of all mRNAs wascalculated using the comparative Ct method after normal-ization to human RPL19.
Protein analysesCells were treated as described in the figure legends. For
total cell lysates, cells were washed twice with ice-cold PBS
Translational RelevanceDysregulation of FGFR3 has been implicated in the
pathogenesis of bladder cancer, and several investiga-tional agents targeting FGFR3 have been evaluated inearly-phase clinical studies. To facilitate the clinicaldevelopment of FGFR3-targeted therapy, we sought toidentify potential noninvasive pharmacodynamic bio-markers to gauge drug activities. Combining transcrip-tional profiling and biochemical analyses, we identifiedand confirmed two matrix metalloproteinases, MMP-1and MMP-10, as downstream targets of FGFR3. Inhibit-ing FGFR3 function with a humanized monoclonalantibody, R3Mab, led to a significant reduction ofMMP-1 and MMP-10 in xenograft models in conjunc-tion with attenuated tumor growth. Importantly, in aphase I dose-escalation trial, R3Mab caused an acutereduction of urinary MMP-1 and pro-MMP-10 levels inpatients with advanced bladder cancer. These data war-rant further investigation in larger clinical studies usingthese potentially actionable noninvasive pharmacody-namic biomarkers to stratify patients with elevatedMMP-1 and pro-MMP-10 and potentially to monitortherapeutic response.
Urinary Pharmacodynamic Markers for R3Mab in Bladder Cancer
www.aacrjournals.org Clin Cancer Res; 20(24) December 15, 2014 6325
on November 11, 2020. © 2014 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 17, 2014; DOI: 10.1158/1078-0432.CCR-13-3336

and extracted inRIPAbuffer (Millipore) supplementedwithphosphatase inhibitor cocktail PhosSTOP and Completeprotease inhibitor cocktail (Roche Applied Science). Foranalysis of protein expression in tumor xenografts, lysatefrom tumor tissues was extracted with lysis buffer[consisting of 150 mmol/L sodium chloride, 20 mmol/LTris (pH 7.5), 2 mmol/L EDTA, 1% Triton X-100, 10mmol/L sodiumfluoride, supplementedwithprotease inhi-bitors and phosphatase inhibitors] by pulverizing the fro-zen tissues using the FastPrep-24 homogenizer as describedby the manufacturer (MP Biomedicals).
Protein lysates were analyzed by SDS-PAGE and Westernblot analysis. The primary blotting antibody for total FRS2(sc-8318) was purchased from Santa Cruz Biotechnology.The following primary antibodies were purchased fromCell Signaling Technology: pFRS2 Y196 (#3864), pMAPK(#9101), total MAPK (#4695), pAKT (#9271), and totalAKT (#9272). Anti-MMP-1 (MAB901) and anti-MMP-10(MAB910) were purchased from R&D Systems. The blotswere visualized using a chemiluminescent substrate (ECLPlus, Amersham Pharmacia Biotech).
Analyses of secretedMMP-1, pro-MMP-10, andMMP-10in conditioned medium
Secreted MMPs were measured with the following ELISAKits according to the manufacturers’ instructions: Totalhuman MMP-1 protein (ELH-MMP1) and total humanMMP-10 (ELH-MMP10-001) ELISA kits were purchasedfrom RayBiotech, and human pro-MMP-10 ELISA kit(DM100) was purchased from R&D Systems.
To collect conditioned medium: RT112 and UMUC-14cells were grown to 90% confluence in DMEM containing10% FBS, 2 mmol/L glutamine, 100 U/mL penicillin, and100 mg/mL streptomycin. To evaluate the effects of FGFR3knockdown on MMP-1 and MMP-10 protein expression,cells were cultured in the presence or absence of doxycycline(1 mg/mL) for the indicated time, and conditionedmediumwas collected. To study the effect of R3Mab on MMP-1 andMMP-10 expression, 106 cells per dish were seeded onto 10cm dishes in complete growth medium and allowed toattach overnight. Then, serum-free DMEM containingR3Mab (15 mg/mL) or a control antibody was applied, andsupernatants were collected at the indicated time points.The conditioned medium was concentrated 10-fold usingAmicon Ultra Centrifugal filters (Millipore) for ELISA anal-ysis, and the corresponding cells were lysed in the RIPAbuffer (50mmol/L pH7.4 Tris-Cl, 1%NP40, 0.25%sodiumdeoxycholate) with complete protease inhibitor cocktail(Roche Applied Science). MMP-1 and MMP-10 amountswere normalized to total cellular proteins.
Xenograft studies and collection of serum for ELISAanalyses
All animal studies were conducted in accordance with theGuide for the Care and Use of Laboratory Animals, pub-lished by the NIH (NIH publication 8523, revised 1985).The Institutional Animal Care and Use Committee at Gen-entech reviewed and approved all animal protocols. Female
C.B-17 SCID mice, 6 to 10 weeks of age, were purchasedfrom Charles River Laboratory. Female athymic nude micewere obtained from Harlan Sprague Dawley. Mice weremaintained under specific pathogen-free conditions.Female C.B-17 SCID or athymic nudemice were inoculatedsubcutaneously with 7� 106 RT112 cells in Hank balancedsalt solution (HBSS)/Matrigel (1:1 v/v, BD Biosciences) or5 � 106 UMUC-14 cells in HBSS (0.1 to 0.2 mL/mouse),respectively. Mice with tumors reaching a mean volume of150 to 200mm3were randomly grouped into groups of 12,andwere treatedwith vehicle (PBS)orR3Mab (0.3–100mg/kg) via weekly intraperitoneal injections. Body weights andcaliper measurements were taken twice weekly. The tumorvolume (mm3) was calculated using the following formula:length � width2 � 0.5. Log2 (tumor volume) growth traceswere fitted to each treatment group with restricted cubicsplines for the fixed time effect in each group. Fitting wasdone as previously described (37) via a linear mixed effectsmodel, using the R package "nlme," version 3.1–108 in Rversion 2.15.2 (R Development Core Team 2012; R Foun-dation for Statistical Computing). Plotting was performedusing Excel 14.3.2 (Microsoft Corporation).
To analyze MMP-1 and MMP-10 levels in tumor tissuesand serum, mice with tumors reaching a mean volume of150 to 200mm3were randomly grouped into cohorts of 10,and were treated with a control human IgG1 or R3Mab(30 mg/kg) on days 1, 4, and 7. Tumors and mouse serumwere collected at indicated time points and kept frozen.Human MMP-1 and pro-MMP-10 level in mouse serumwere determined using the ELISA assays as described above.
Clinical study designThe phase IMFG4991g trial (35) was an open-label dose-
escalation study to evaluate the safety, tolerability, andpharmacokinetics of R3Mab (designated MFGR1877S) inpatients with solid tumors. The trial consisted of a doseescalation of single-agent R3Mab administered intrave-nously at 2, 4, 8, 15, and 30 mg/kg once every 28 days.Serum and urine samples were collected at designated timepoints, frozen in liquid nitrogen, and shipped to Genen-tech, Inc. for measurement of pharmacodynamic biomar-kers of R3Mab activity.
ELISA analyses of MMPs in human serum and urineThe levels of a panel of MMPs weremeasured by ELISA in
serum and urine samples from normal healthy volunteers,procured bladder cancer patients, and patients enrolled inthe phase I MFG4991g clinical trial. To this end, the humanMMP 3-Plex (i.e., MMP-1, MMP-3, and MMP-9; MesoscaleDiscovery) and human pro-MMP-10 immunoassay (R&DSystems) kits were utilized according to the manufacturer’sinstructions. For the human pro-MMP-10 immunoassaykit, serum samples were diluted 2-fold in the appropriateassay diluent. For the human MMP 3-Plex kit, serum sam-ples were diluted 10-fold. For all MMP kits, urine was usedundiluted. As a reference for quantification, a standardcurve was used for each kit according to the manufacturer’sdirections. Mann–Whitney tests were used for comparison
Du et al.
Clin Cancer Res; 20(24) December 15, 2014 Clinical Cancer Research6326
on November 11, 2020. © 2014 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 17, 2014; DOI: 10.1158/1078-0432.CCR-13-3336

between two groups. A value of P < 0.05 was consideredstatistically significant.
ResultsFGFR3 knockdown inhibits MMP-1 and MMP-10expression and secretionUsing doxycycline-inducible shRNA targeting FGFR3, we
previously determined the transcriptional profile of RT112-derived cell lines that express endogenous or depleted levelsof FGFR3, using microarray analysis (36). To facilitateidentification of serumor urine pharmacodynamicmarkersof FGFR3-targeted therapeutics, we focused on secretedmolecules thatwere specificallymodulatedby FGFR3deple-tion. Comparing independently established stable cell linestransduced with a doxycycline-inducible control shRNAversus three independent FGFR3 shRNAs, we found thattwo matrix metalloproteinases, MMP-1 and MMP-10, wereamong the genes showing the greatest decline upon FGFR3knockdown (Supplementary Table S1). The transcriptsweredownregulated by about 16-fold and 4-fold for MMP-1 andMMP-10, respectively (Supplementary Fig. S1). Thesemicroarray results were further confirmed using qRT-PCRanalysis of the mRNA abundance of these two genes(Fig. 1A). In addition, the FGFR3-dependent regulation of
these genes was also verified in UMUC-14 bladder cancercells subjected to siRNA-mediated FGFR3knockdown (Sup-plementary Fig. S2A), or treated with a specific anti-FGFR3humanmonoclonal antibody, R3Mab (Supplementary Fig.S2B). Together, these data suggest that FGFR3 signalingpromotes transcription of MMP-1 and MMP-10 in bladdercancer cells.
Next,we examined the effect of FGFR3knockdownon theexpression and secretion of MMP-1 and MMP-10 proteins.RT112 cells were treated with or without doxycycline for 72hours to deplete FGFR3protein, and the conditionedmediawere collected at specific time points thereafter. FGFR3shRNAs substantially diminished the secretion of MMP-1and pro-MMP-10 as early as 24 hours after induction andthe decrease was sustained at 48 and 72 hours, whereas thecontrol shRNA had no effect (Fig. 1B). MMP-10 was down-regulated in a similar manner by FGFR3 shRNAs (Supple-mentary Fig. S3). Consistently, pretreatment with R3Mabalso blocked the production and secretion of MMP-1, pro-MMP-10, andMMP-10 proteins into conditionedmedia byboth RT112 and UMUC-14 cells (Fig. 1C and Supplemen-tary Fig. S4). Together, these results suggest that FGFR3signaling promotes the expression and secretion of MMP-1and MMP-10 proteins by these bladder cancer cell lines. As
0
0.2
0.4
0.6
0.8
1
CtrlshRNA
R3shRNA2
R3shRNA4
R3shRNA6
Rel
ativ
e M
MP
-1 m
RN
A(+
Dox
/−D
ox)
0
0.2
0.4
0.6
0.8
1
1.2
1.4
CtrlshRNA
R3shRNA2
R3shRNA4
R3shRNA6
Rel
ativ
e M
MP
-10
mR
NA
(+
Dox
/−D
ox)
A
CR3 shRNA4R3 shRNA2Ctrl shRNA
72 h48 h24 h72 h48 h24 h72 h48 h24 h0
50
100
150
200
250
300
350
pro-
MM
P-1
0(n
g/m
g ce
llula
r pr
otei
n)
No Dox Dox
R3 shRNA4R3 shRNA2Ctrl shRNA
72 h 24 h 48 h24 h 48 h 72 h72 h48 h24 h
B
0
100
200
300
400
500
Tot
al M
MP
-1(n
g/m
g ce
llula
r pr
otei
n)
No Dox Dox
0
20
40
60
80
100
120
72 h48 h24 h
Tot
al M
MP
-1(n
g/m
g ce
llula
r pr
otei
n) Ctrl AbR3Mab
0
100
200
300
400
500
600
72 h48 h24 h
pro-
MM
P-1
0(n
g/m
g ce
llula
r pr
otei
n) Ctrl AbR3Mab
0
5
10
15
20
25
30
35
72 h48 h24 h
Tot
al M
MP
-10
(ng/
mg
cellu
lar
prot
ein) Ctrl Ab
R3Mab
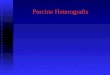
Figure 1. Inhibition of FGFR3reduces the mRNA and proteinexpression of MMP-1 and MMP-10 in RT112 bladder cancer cells.A, doxycycline-inducedknockdown of FGFR3 reducesmRNA levels of MMP-1 andMMP-10. B, doxycycline-inducedknockdown of FGFR3 reducestotal MMP-1 and pro-MMP-10secreted in the conditionedmedium. C, a specific FGFR3-blocking antibody, R3Mab,reduces total MMP-1, pro-MMP-10, and total MMP-10 secreted inthe conditioned medium by RT112cells.
Urinary Pharmacodynamic Markers for R3Mab in Bladder Cancer
www.aacrjournals.org Clin Cancer Res; 20(24) December 15, 2014 6327
on November 11, 2020. © 2014 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 17, 2014; DOI: 10.1158/1078-0432.CCR-13-3336

the ELISA detection of pro-MMP-10 is more sensitive thanthat of MMP-10, and both pro- and enzymes show similarmodulation by FGFR3 inhibition, we focused on pro-MMP-10 protein levels in subsequent studies.
FGFR3 signaling promotes MMP-1 and MMP-10expression mainly through MEK
To study the molecular mechanisms underlying FGFR3regulation of MMP-1 andMMP-10 expression, we activatedFGFR3 signaling in bladder cancer cells with FGF1. We firstanalyzed themRNA levels of the twoMMPs. FGF1 treatmentof RT112 cells induces robust FGFR3 activation in a dose-and time-dependent fashion (36), and higher mRNA levelsof both MMP-1 and MMP-10 were detected after 6 or12-hour incubation (Fig. 2A). Consistent with thesechanges, secreted MMP-1 and pro-MMP-10 proteinsdetected in conditioned media were higher after a 24-hourincubation with FGF1 (Fig. 2B), and accumulated further at48 and 72 hours (data not shown).
To determine whether the induction of MMP-1 andMMP-10 by FGF1 depends on specific FGFR3 signalingmediators, we blocked the two major signaling branchesdownstream of FGFR3 using the PI3K inhibitor Ly294002and the MEK1/2 inhibitor PD325901. In RT112 bladdercancer cells, each inhibitor blocked FGF1-induced activa-
tion of its corresponding target, as assessed by the phos-phorylation of AKT or MAPK, respectively (Fig. 2C). WhilePI3K inhibition elicited minimal effect on the expressionand secretion of MMP-1 and MMP-10 proteins, MEK inhi-bition significantly diminished both basal and FGF1-induced expression of these two proteins (Fig. 2D). Thus,FGFR3 promotesMMP-1 andMMP-10 expression in RT112bladder cancer cells mainly through the MEK-MAPK axis.
R3Mab blocks FGFR3 signaling and reduces humanMMP-1 and MMP-10 protein levels in both bladdertumor xenograft tissues and mouse serum
To evaluate whether MMP-1 and MMP-10 could serveas potential pharmacodynamic markers for FGFR3-tar-geted therapeutics, we studied the effect of R3Mab on theexpression and secretion of these enzymes in vivo. TwoR3Mab-responsive tumor xenograft models, RT112 andUMUC-14, were selected for this study. Weekly intraper-itoneal administration of R3Mab suppressed xenograftgrowth of these models in a dose-dependent manner(Fig. 3A and Supplementary Fig. S5). First, we evaluatedFGFR3 signaling and MMP-1 and MMP-10 protein levelsin tumor xenograft tissues. Compared with the controlantibody, R3Mab markedly reduced the phosphorylationand activation of FRS2 and MAPK, two of the essential
C
FGF1 ++ −+ −+ −+ −−pAKT
AKT
pMAPK
MAPK
Actin
DMSO 10 100 2 20
Ly294(µmol/L)
PD901(nmol/L)
A
6 h 12 h
D
0
10
20
30
40
pro-
MM
P-1
0(n
g/m
g ce
llula
r pr
otei
n) No FGF1
+FGF1
0
150
300
450
MM
P-1
(n
g/m
g ce
llula
r pr
otei
n) No FGF1
+FGF1
0
2
4
6
8
Rel
ativ
e M
MP
-1
mR
NA
leve
l
No FGF1+FGF1
6 h 12 h0
2
4
6
Rel
ativ
e M
MP
-10
mR
NA
leve
l
No FGF1+FGF1
Tot
al M
MP
-1
(ng/
mg
cellu
lar
prot
ein)
B
0
50
100
150
200
250
300
No FGF1
+FGF1
Pro
-MM
P-1
0 (n
g/m
g ce
llula
r pr
otei
n)
0
20
40
60
No FGF1+FGF1
DMSO
DMSO
PD901
10 n
mol/
L
PD901
10 n
mol/
L
PD901
100
nmol/
L
PD901
100
nmol/
LLy
294
2 µm
ol/L
Ly29
4 2
µmol/
L
Ly29
4 20
µmol/
L
Ly29
4 20
µmol/
L
Figure 2. FGF1 signaling stimulatesMMP-1 and MMP-10 expressionthrough MEK. A, FGF1 inducesMMP-1 and MMP-10 mRNAexpression inRT112cells. B, FGF1treatment stimulates MMP-1 andpro-MMP-10 protein expressionand secretion into conditionedmedium by RT112 cells. C,pharmacologic inhibition of FGF1signaling in RT112 cells. RT112cells were treated with PD325901(PD901) and Ly294002 (Ly294) atindicated concentrations for3 hours, followed by FGF1(25 ng/mL) stimulation for 10minutes. Cell lysates weresubjected to Western blotanalysis. D, MEK inhibitor, butnot PI3K inhibitor, blockedFGF1-induced expression andsecretion of MMP-1 andpro-MMP-10 by RT112 cells.
Du et al.
Clin Cancer Res; 20(24) December 15, 2014 Clinical Cancer Research6328
on November 11, 2020. © 2014 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 17, 2014; DOI: 10.1158/1078-0432.CCR-13-3336

downstream mediators of FGFR3 signaling (Fig. 3B).Concomitantly, both total MMP-1 and MMP-10 proteinlevels in the tumor lysates were decreased significantly inresponse to R3Mab (Fig. 3B).We next evaluated the effect of R3Mab on human
MMP-1 and MMP-10 protein levels in the circulatingblood from xenograft models expressing human bladdertumors. Nude mice with pre-established RT112 tumorswere treated with a low or a high dose of R3Mab (3 or30 mg/kg, respectively), and mouse serum was collectedat 48 or 96 hours after treatment. Human pro-MMP-10protein levels in mouse serum were reduced in a dose-dependent manner in R3Mab-treated group at 48 and 96hours, and the effect was more pronounced in the high-dose group at 96 hours (Supplementary Fig. S6). Weextended the analysis to days 4, 6, and 10 after treatment.Compared with the control antibody, R3Mab substan-tially and significantly suppressed the serum levels ofhuman MMP-1 and pro-MMP-10 throughout the timecourse (Fig. 3C and D). A similar reduction of serumlevels of these two proteins was induced by R3Mabtreatment of mice bearing UMUC-14 tumors (Supple-mentary Fig. S7A and S7B).
To assess whether the modulation of MMPs by R3Mabcorrelates with efficacy, we also analyzed pro-MMP-10levels in three xenograft models whose growth is not affect-ed by R3Mab, namely HT1376, UMUC-4, and SW780(Supplementary Fig. S8A and data not shown). Levels ofpro-MMP-10 were too low to be detected in serum frommice bearing UMUC-4 or HT1376 xenograft tumors (datanot shown).While pro-MMP-10was easily detected inmicewith SW780 tumors, levels of pro-MMP-10 were not affect-ed upon R3Mab treatment as observed in responsive mod-els (Supplementary Fig. S8B).
Together, these data demonstrated that R3Mab-basedinhibition of FGFR3 signaling and tumor growth occurs inconjunction with a substantial and sustained reduction ofMMP-1 and MMP-10 protein expression and secretion,suggesting that these two metalloproteinases could beexplored as potential pharmacodynamic markers of FGFR3pathway inhibition.
MMP-1 and pro-MMP-10 proteins are elevated in theurine of bladder cancer patients
Next, we evaluated MMP-1 and pro-MMP-10 proteinlevels in urine and serum specimens from healthy donors
Ctrl Ab R3Mab
pFRS2
pMAPK
Total MMP-1
Total MMP-10
Actin
223
238
242
246
249
202
208
210
220
226
Animal ID
Total FRS2
Total MAPK
B
Day 10Day 6Day 4
P < 0.0001 P < 0.0001 P < 0.0001
Ctrl Ab R3Mab Ctrl Ab R3Mab Ctrl Ab R3Mab
P < 0.0001
Ctrl Ab R3Mab
P < 0.0005
Ctrl Ab R3Mab
P < 0.0001
Ctrl Ab R3Mab
C
D
0
200
400
600
800
1,000
1,200
1,400
2520151050
VehicleR3Mab, 1 mg/kgR3Mab, 3 mg/kgR3Mab, 10 mg/kgR3Mab, 30 mg/kgR3Mab, 100 mg/kg
A
Fitt
ed tu
mor
vol
ume
(mm
3 )
DayR3Mab
8
6
4
2
0
8
6
4
2
0
12
10
8
6
4
2
0
15.0
12.5
10.0
7.5
5.0
2.5
0.0
20
15
10
5
0
20
15
10
5
0
MM
P-1
0 (n
g/m
L)
MM
P-1
0 (n
g/m
L)
MM
P-1
0 (n
g/m
L)
MM
P-1
(ng
/mL)
MM
P-1
(ng
/mL)
MM
P-1
(ng
/mL)
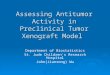
Figure 3. R3Mab attenuates RT112tumor growth, blocks FGFR3signaling and reduces humanMMP-1 and MMP-10 levels inxenograft tumor tissues andmouse serum. A, effect of R3Mabon pre-established RT112 bladderxenograft tumor growth. R3Mabwas administered intraperitoneallyweekly (arrows). n¼ 12 per group.B, effect of R3Mab on FGFR3signaling andMMP levels in tumorxenograft tissues. Mice with pre-established RT112 tumors weregrouped into cohorts of 5 fortreatment with either a controlantibody (Ctrl Ab) or R3Mab(30 mg/kg). Tumors wereharvested at day 7, and lysatesextracted from xenograft tumortissues were subjected toWesternblot analysis. C and D, the kineticsof R3Mab effect on serum levelsof human MMP-1 (C) andpro-MMP-10 (D) in mice bearingRT112 xenograft tumors. n ¼ 10per group.
Urinary Pharmacodynamic Markers for R3Mab in Bladder Cancer
www.aacrjournals.org Clin Cancer Res; 20(24) December 15, 2014 6329
on November 11, 2020. © 2014 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 17, 2014; DOI: 10.1158/1078-0432.CCR-13-3336

and patients with bladder cancer (acquired from commer-cial sources). In urine samples from healthy donors (n ¼25), MMP-1 was mostly undetectable or below the lowerlimit of quantitation (LLOQ), but pro-MMP-10 was con-sistently detected above the LLOQ, albeit within a low andnarrow range (Fig. 4A). In contrast, both MMP-1 and pro-MMP-10proteinswere detected at significantly higher levelsin urine frompatients with bladder cancer (n¼ 35; Fig. 4A).A different pattern was observed in serum: both metallo-proteinases were detected above the LLOQ in all serumsamples from the same patients; however, there was nodifference in levels detected in healthy donors versuspatients with bladder cancer (Fig. 4B).
As R3Mab has been evaluated in a phase I dose-escalationclinical trial (MFG4991g) conducted in relapsed or refrac-tory, locally advanced, or metastatic solid tumors (Supple-mentary Table S2; ref. 35), analogous measurements ofMMP1andpro-MMP-10weremade in clinical pretreatmenturine and serum specimens (n ¼ 26). All patients withbladder cancer (n¼ 10) enrolled in this study have relapsedor refractory metastatic lesions, and 8 of 10 patients dis-played significantly higher urinary MMP-1 levels, with onlytwo patients having MMP-1 below the LLOQ. In contrast,urinary MMP-1 was undetectable or below the LLOQ in amajority of samples from patients with cancer with othersolid tumors, including colorectal, squamous cell carcino-ma of the head and neck, ovarian, thyroid, esophageal,adrenal, adenoid cystic carcinoma, or carcinoid tumor
(n ¼ 15; Fig. 4A). Similarly, elevated levels of pro-MMP-10 were observed in urine samples from patients withbladder cancer relative to patients with other solid tumors(Fig. 4A). In agreement with observations in the commer-cially procured specimens, there was no difference in serumMMP-1 and pro-MMP-10 levels between patients withbladder cancer or other solid tumors (Fig. 4B). Together,these data demonstrate that these two metalloproteinasesare significantly elevated in bladder cancer patient–derivedurine relative to analogous samples from healthy donors orfrom patients with several other solid tumors. However, wedid not observe a correlation between baseline MMP levelsand either FGFR3 protein expression level (as measuredretrospectively by immunohistochemistry) or clinicalresponse in the MFG4991g phase I trial (38).
R3Mab reduces urinary MMP-1 and pro-MMP-10 levelsin patients with bladder cancer
To examine whether MMP-1 and/or pro-MMP-10 couldbe used as pharmacodynamic biomarkers, patterns oftheir expression were also evaluated in urine samples fromthe MFG4991g phase I clinical trial collected predose, or atcycle 1, day 2 (C1D2), cycle 1, day 4 or 5 (C1D4D5) and,in some cases, at later time points depending on how longthe patient stayed on study and on availability of samples(Fig. 5). In all bladder cancer patients (based on 8 evaluableurine sample pairs), exposure to R3Mab reduced MMP-1levels by >50% (Fig. 5A and B). Assessment of
SerumUrine BA
BLCNon-BLCBLCHealthy0.0001
0.001
0.01
0.1
1
10
100
1,000
Procured samples Ph1 clinical samples
** **
Tot
al M
MP
-1 (
ng/m
L)
n = 10n = 15n = 23n = 3
BLCNon-BLC BLCHealthy0.0001
0.001
0.01
0.1
1
10
100
1,000
pro-
MM
P10
(ng
/mL)
*** *
Ph1 clinical samplesProcured samples
n = 8n = 35n = 25 n = 8
BCLNon-BCL BCLHealth 0.0001
0.001
0.01
0.1
1
10
100
1,000
Tot
al M
MP
-1 (
ng/m
L)
Ph1 clinical samplesProcured samples
n = 10n = 16n = 35n = 5
BLCNon-BLCBLCHealthy0.0001
0.001
0.01
0.1
1
10
100
1,000
Ph1 clinical samplesProcured samples
pro-
MM
P10
(ng
/mL)
n = 10n = 16n = 35n = 5
Figure 4. MMP-1 and pro-MMP-10are elevated in bladder cancer(BLC) patient urine but not inserum. A, levels of MMP-1 andpro-MMP-10 in commerciallyprocured urine samples frompatients with bladder cancer(n ¼ 35) relative to healthy donors(n ¼ 25), or from the MFG4991gphase I clinical trial, includingpatients with bladder cancer(n ¼ 10) and patients with othersolid tumor types (non-BLC,n ¼ 16). Plotted n values arerepresentative of only thosesamples that were detectable(>LOD). The dotted line representsthe LLOQ. B, levels of MMP-1 andpro-MMP-10 in serum areequivalent in healthy donors,bladder cancer patients, and innon–bladder cancer patients.Note: only 5 healthy donor serumsamples were evaluated.
Du et al.
Clin Cancer Res; 20(24) December 15, 2014 Clinical Cancer Research6330
on November 11, 2020. © 2014 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 17, 2014; DOI: 10.1158/1078-0432.CCR-13-3336

pharmacodynamic modulation in non–bladder cancerpatients was hampered by the limited number (3/16) ofsamples having sufficient MMP-1 levels at baseline. Whilemost samples were detectable, only 3 were above the lowestlevel of quantitation in the assay. However, in the cases inwhich MMP-1 could be quantified, MMP-1 levels werereduced by >50% (Fig. 5A and B).Unlike MMP-1, all urine samples had detectable pro-
MMP-10 levels for analysis. Pro-MMP-10 was reduced by>50%inhalf of thepatientswithbladder cancer treatedwithR3Mab (4/8 evaluable pairs). In contrast, there was noreduction in pro-MMP-10 in urine samples from patientswith non–bladder cancer (Fig. 5C andD). All of the patientswith bladder cancer that showed reduced levels of pro-MMP-10 were treated at the highest dose (30 mg/kg).However, two other patients in the highest dose cohort didnot show modulation of pro-MMP-10 levels. In contrast,MMP-1 was downmodulated upon antibody treatment inmost dose cohorts including the 8, 15, and 30 mg/kg dosecohorts.A number of MMPs have been postulated as potential
diagnostic and/or prognostic biomarkers in bladder cancer,but the role forMMPs as pharmacodynamic biomarkers haslargely been unexplored (39). To extend our preliminaryobservations, additional analysis was performed to evaluatetwo other MMPs, MMP-3, andMMP-9, which also harbor agroup 1 promoter element similar to MMP-1 and MMP-10(40). Statistical analysis (Mann–Whitney test) indicatedthat MMP-3 (P¼ 0.0251), but not MMP-9 was significantlyhigher in urine frompatients with bladder cancer relative tonon–bladder cancer patients in the MFG4991g phase I
study (Fig. 6A). Similar to pro-MMP-10 and MMP-1 data,no significant difference was detected in serum (Fig. 6B).Pharmacodynamic monitoring of these MMPs showed thatin most but not all cases MMP-3 and MMP-9 were down-modulated by R3Mab similarly to pro-MMP-10 andMMP-1in patient samples where all four MMPs were detectable(Fig. 6C). Together, these data suggested that anti-FGFR3therapy specifically downmodulated urinary, but notserum, MMP levels in patients with bladder cancer. It isworth noting that similar to observations at baseline, nocorrelation between pharmacodynamics measures andeither FGFR3 expression or clinical response was observed(38).
DiscussionBladder cancer is the secondmost commongenitourinary
tract malignancy, accounting for more than 73,000 newcases each year and about 15,000 deaths in 2012 in theUnited States alone (2). The receptor tyrosine kinase,FGFR3, has been postulated as an important oncogenicdriver and potential therapeutic target in this disease basedonmultiple lines of evidence, including a high frequency ofactivating mutations (17–20), aberrant regulation and acti-vation of FGFR3 by gene fusion with TACC3 or BAIAP2L1(21, 22), overexpression of FGFR3 protein in tumor tissues(19, 23), and a large body of preclinical loss-of-functionstudies (23, 27–31). Recent progress toward clinical inves-tigation of experimental agents targeting FGFR3 hasmade itimperative to identify accessible pharmacodynamic bio-markers to gauge target modulation and facilitate clinical
Predo
se
C1D2
C1D4D5
Predo
se
C1D2
C1D4D
50.0001
0.001
0.01
0.1
1
10Bladder cancer Non–bladder cancer
MM
P-1
(ng
/mL)
Predo
se
C1D2
C1D4D
5
Predo
se
C1D2
C1D4D
50
50
100
150Bladder cancer Non–bladder cancer
MM
P-1
(%
pre
dose
)
Predo
se
C1D2
C1D4D
5
Predo
se
C1D2
C1D4D5
0.0001
0.001
0.01
0.1
1
10Bladder cancer Non–bladder cancer
pro-
MM
P-1
0 (n
g/m
L)Pre
dose
C1D2
C1D4D
5
Predo
se
C1D2
C1D4D
50
50
100
150200300400500
Bladder cancer Non–bladder cancer
pro-
MM
P-1
0 (%
pre
dose
)
A C
DB
Figure 5. MMP-1 and pro-MMP-10are reduced upon exposure toR3Mab in patients with bladdercancer in the MFG4991g phase Istudy. A, the overall urinary levelsof MMP-1 are reduced by R3Mabin patients with bladder cancer butnot in non–bladder cancerpatients. B, relative levels ofMMP-1 compared with predose levels.C, the overall urinary levels of pro-MMP-10 are reduced by R3Mab inpatients with bladder cancer butnot in non–bladder cancerpatients. D, relative levels of pro-MMP-10 compared with predoselevels. C1D2, cycle 1 day 2;C1D4D5, cycle 1, day 4 or day 5.
Urinary Pharmacodynamic Markers for R3Mab in Bladder Cancer
www.aacrjournals.org Clin Cancer Res; 20(24) December 15, 2014 6331
on November 11, 2020. © 2014 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 17, 2014; DOI: 10.1158/1078-0432.CCR-13-3336

studies. Here, we report that FGFR3 stimulates MMP-1 andpro-MMP-10 expression and secretion in human bladdercancer cells through the MEK–MAPK pathway. BlockingFGFR3 signaling by a specific anti-FGFR3 human mono-clonal antibody, R3Mab, inhibited human tumor xenograftgrowth in association with a marked reduction in circulat-ing human MMP-1 and pro-MMP-10 levels. Moreover,patients with bladder cancer had an increased level ofurinary MMP-1 and pro-MMP-10 proteins. Importantly, ina phase I dose-escalation study of R3Mab, inhibition ofFGFR3 in patients with relapsed or refractory metastaticbladder cancer resulted in an acute reduction of urinaryMMP-1 and pro-MMP-10 levels. These results unveil animportant role for FGFR3 in regulating MMP-1 and pro-MMP-10 expression and secretion in bladder cancer, andsupport further evaluation of these metalloproteinases aspotential pharmacodynamic markers in future FGFR3-tar-geted clinical studies.
In our unbiased expression analysis of genes encodingsecretedmolecules, we found that upon FGFR3 knockdownin RT112 bladder cancer cells, MMP-1, and pro-MMP-10were among the most prominently downregulated genes.Our studies further demonstrate that ligand-induced FGFR3activation promotes both mRNA and protein expression ofthese two metalloproteinases, and acute pharmacologicinhibition of canonical FGFR3 signaling markedlydiminishes the level of secreted MMP-1 and pro-MMP-10
in the conditionedmedium. This inhibitory effect is mainlymediated through the FGFR3–MEK–MAPK pathway, butnot the FGFR3-PI3K axis. These results extend earlier studiesby others showing that the expression of several MMP genesis regulatedby somegrowth factors and cytokines inbladdercancer. For example, basic FGF is able to stimulate theexpression of MMP-2 and MMP-9 in HT1376 cells (41),and EGF elicits the rapid induction of MMP-1 andMMP-10mRNA in T24 bladder cancer cells through the Stat3/acti-vator protein-1 (AP-1) family of transcription factors (42).Importantly, in the current study, by selectively blockingFGFR3 function with R3Mab (i.e., a specific anti-FGFR3monoclonal antibody), wewere able to clearly demonstratethat MMP-1 and pro-MMP-10 are bona fide downstreamtargets of FGFR3 signaling in bladder cancer. It is worthnoting that the current study does not exclude the possi-bility that other signaling pathways may also regulate thesetwo MMPs through MAPK or alternative mechanisms inbladder cancers.
To assess whether MMP-1 and pro-MMP-10 could serveas accessible pharmacodynamic biomarkers for FGFR3-tar-geted therapy, we have evaluated the serum and urinarylevels of these two proteins in healthy subjects and inpatients with bladder cancer, as well as in patients withvarious solid cancers enrolled in the MFG4991g phase Istudy of R3Mab. Compared with healthy controls andpatients with non–bladder cancer malignancies, patients
A
B
116 117 121 122 123 126 1270.00
50.00
100.00
150.00
MM
P1 v
alu
es
(% p
redose
)116 117 121 122 123 126 127
0.00
50.00
100.00
150.00
pro
MM
P10 (
% p
redonse
)
116 117 121 122 123 126 1270.00
50.00
100.00
150.00
MM
P3 (
% p
redose
)
116 117 121 122 123 126 1270.00
50.00
100.00
150.00
MM
P9 (
% p
redose
)
Predose C1D2 C1D4/5C
0.001
0.01
0.1
1
10
100
1,000
10,000
MM
P v
alue
s (n
g/m
L)
1
10
100
1,000
MM
P v
alue
s (n
g/m
L)
BLCNon-BLC
MMP-9MMP-3
BLCNon-BLC
Serum
Urine
MMP-9MMP-3
Figure 6. Levels and modulation ofMMP-3 and MMP-9 by R3Mab inthe MFG4991g phase I study.A, urinary MMP-3 is elevated inpatients with bladder cancerrelative to non–bladder cancerpatients in the MFG4991g phase Istudy. On the basis of Mann–Whitney test, P ¼ 0.0251 forMMP-3; P > 0.05 for MMP-9. B, nocorresponding difference of theseMMPs was detected in serum. C,samples (n ¼ 7) with detectablelevels of all four MMPs showedvariablemodulation in response toR3Mab administration. C1D2,cycle 1 day 2; C1D4D5, cycle 1,day 4 or day 5.
Du et al.
Clin Cancer Res; 20(24) December 15, 2014 Clinical Cancer Research6332
on November 11, 2020. © 2014 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 17, 2014; DOI: 10.1158/1078-0432.CCR-13-3336

with advanced bladder cancer showed significantly elevatedurine levels of MMP-1 and pro-MMP-10 protein. In con-trast, the concentration of these two proteins in circulatingblooddisplayednodifference amongst the different groups.This observation is in agreement with several publishedstudies. MMP-1 and MMP-10 mRNA levels have beenreported to be significantly higher in bladder cancers com-pared with normal urothelial tissues (43, 44), and MMP-1and pro-MMP-10 immunoreactivity is evidently stronger intumor cells of both superficial and muscle-invasive bladdercancers (45, 46). In addition, patients with bladder cancerwith an increased urinary MMP-1 protein level are morelikely to have an aggressive tumor of advanced stage andgrade (47, 48). Although published data on urinary pro-MMP-10 in patients with bladder cancer is more limited, arecent study demonstrates that a higher urinary pro-MMP-10 concentration could serve as a potential diagnosticbiomarker when used in combination with a panel of sixother analytes (44). Taken together, the differential expres-sion pattern between patients with bladder cancer andhealthy subjects, the relative ease in acquisition of voidurine samples, and the robust detection of urinary MMP-1and pro-MMP-10 levels suggest that these two metallopro-teinases could serve as useful and clinically relevant non-invasive biomarkers.One important finding of our current study is that in
preclinical bladder cancer xenograft models, R3Mab treat-ment inhibited FGFR3 signaling, attenuated tumor growth,and reducedMMP-1 andpro-MMP-10protein expression intumor lysates as well as in mouse serum. Consistent withthese preclinical studies, our phase I study with 26 patientsdemonstrated that administration of R3Mab led to an acutereduction of urinary MMP-1 by more than 50% in 8 of 8evaluable patients with bladder cancer. The evaluation innon–bladder cancer patients was hampered by the fact thatvery few patients had measureable levels of MMP-1 atbaseline. In the only 3 patients (2 colorectal and 1 headand neck SCC) that were evaluable, MMP-1 was alsomarkedly reduced. It is noteworthy that although a mini-mum threshold level of MMP-1 is required for monitoringpharmacodynamic modulation, the extent of downmodu-lation was not correlated with the baseline values. A similareffect was observed for pro-MMP-10, as R3Mab resulted in adecrease of urinary pro-MMP-10, albeit in only 4 of 8patients with bladder cancer. Interestingly, no modulationof pro-MMP-10 was detected in non–bladder cancerpatients, suggesting that pro-MMP-10 might be more spe-cific for bladder cancer.Additional MMPs were monitored in the clinical study.
Similar to MMP-1 and pro-MMP-10, urinary MMP-3, andto a lesser extent, MMP-9, were also elevated in bladderrelative to non–bladder cancer patients. In a majority ofpatients, there was a similar pattern of downmodulationof these MMPs by R3Mab despite some noticeable differ-ences. This observation could be partially due to the factthat these MMPs all have a proximal AP-1 binding sitein their promoters (40); conceivably, R3Mab-mediatedinhibition of the MEK-MAPK-AP-1 axis may result in
decreased transcription of these genes. Indeed, in 4T1breast cancer cells, the pan-FGFR inhibitor TKI258 sup-presses the transcription of MMP-1, -3, -9, and -10 simul-taneously (49).
The matrix metalloproteinases degrade extracellularmatrix components and activate growth factors, contribut-ing to tumor growth, progression, and metastasis (50).Several MMPs have been postulated to be diagnostic orprognostic markers in bladder cancer (39, 50). Our currentstudy demonstrates that FGFR3 signaling directly regulatesMMP-1 and pro-MMP-10 expression and secretion in blad-der cancer through the MEK–MAPK pathway. UrinaryMMP-1 and pro-MMP-10 levels were reduced substantiallyby R3Mab treatment in both preclinical models andpatients with bladder cancer. This is the first study, to ourknowledge, that identifies urinaryMMP-1 and pro-MMP-10as potential pharmacodynamic biomarkers. While weobserved clear pharmacodynamic modulation in responseto R3Mab administration, there did not appear to be acorrelation betweenmodulation and dose or FGFR3 expres-sion level or clinical benefit (as assessed by time on study ordisease progression). The lack of correlation could be due tosmall sample size and/or a change in FGFR3 expressionlevels during disease progression or prior drug treatment.Although this phase I study was not powered to assesspredictive biomarkers, the data presented here warrantfurther investigation in larger studies using these potentiallyactionable pharmacodynamic biomarkers that can be usedin the clinic in a noninvasive manner to stratify patientswith elevated MMP-1 and pro-MMP-10 profiles and poten-tially monitor therapeutic response.
Disclosure of Potential Conflicts of InterestJ. Qing, X. Du, B.C. Lin, Q.-R. Wang, H. Li, E. Ingalla, J. Tien, I. Rooney,
A. Ashkenazi, and E. Penuel are employees of Genentech. No other potentialconflicts of interest were disclosed.
Authors' ContributionsConception and design: B.C. Lin, A. Ashkenazi, E. Penuel, J. QingDevelopment of methodology: X. Du, B.C. LinAcquisitionofdata (provided animals, acquired andmanagedpatients,provided facilities, etc.): X. Du, B.C. Lin, Q.-R. Wang, H. Li, E. Ingalla,J. Tien, I. RooneyAnalysis and interpretation of data (e.g., statistical analysis, biosta-tistics, computational analysis): X. Du, B.C. Lin, Q.-R. Wang, H. Li,E. Ingalla, J. Tien, A. Ashkenazi, E. Penuel, J. QingWriting, review, and/or revision of the manuscript: B.C. Lin, J. Tien,I. Rooney, A. Ashkenazi, E. Penuel, J. QingAdministrative, technical, or material support (i.e., reporting or orga-nizing data, constructing databases): B.C. Lin, J. TienStudy supervision: J. Tien, I. Rooney, J. Qing
AcknowledgmentsThe authors thank Zora Modrusan for microarray profiling and Jinfeng
Liu for the informatics analysis of the array data. The authors also thankMarkDavis and Genentech’s FGFR3 development team for designing and con-ducting the phase I clinical trial of R3Mab.
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received December 11, 2013; revised September 18, 2014; acceptedOctober 2, 2014; published OnlineFirst October 17, 2014.
Urinary Pharmacodynamic Markers for R3Mab in Bladder Cancer
www.aacrjournals.org Clin Cancer Res; 20(24) December 15, 2014 6333
on November 11, 2020. © 2014 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 17, 2014; DOI: 10.1158/1078-0432.CCR-13-3336

References1. JemalA,BrayF,CenterMM, Ferlay J,WardE, FormanD.Global cancer
statistics. CA Cancer J Clin 2011;61:69–90.2. Siegel R, Naishadham D, Jemal A. Cancer statistics. CA Cancer J Clin
2012;62:10–29.3. Eswarakumar VP, Lax I, Schlessinger J. Cellular signaling by fibroblast
growth factor receptors.CytokineGrowthFactorRev2005;16:139–49.4. Beenken A,Mohammadi M. The FGF family: biology, pathophysiology
and therapy. Nat Rev Drug Discov 2009;8:235–53.5. Turner N, Grose R. Fibroblast growth factor signalling: from develop-
ment to cancer. Nat Rev Cancer 2010;10:116–29.6. Chesi M, Nardini E, Brents LA, Schrock E, Ried T, Kuehl WM,
et al. Frequent translocation t(4;14)(p16.3;q32.3) in multiple mye-loma is associated with increased expression and activatingmutations of fibroblast growth factor receptor 3. Nat Genet1997;16:260–4.
7. Moreau P, Facon T, Leleu X, Morineau N, Huyghe P, Harousseau JL,et al. Recurrent 14q32 translocations determine the prognosis ofmultiple myeloma, especially in patients receiving intensive chemo-therapy. Blood 2002;100:1579–83.
8. Chang H, Stewart AK, Qi XY, Li ZH, Yi QL, Trudel S. Immunohis-tochemistry accurately predicts FGFR3 aberrant expression and t(4;14) in multiple myeloma. Blood 2005;106:353–5.
9. Majewski IJ, Mittempergher L, Davidson NM, Bosma A, Willems SM,Horlings HM, et al. Identification of recurrent FGFR3 fusion genes inlung cancer through kinome-centred RNA sequencing. J Pathol2013;230:270–6.
10. Liao RG, Jung J, Tchaicha J, Wilkerson MD, Sivachenko A,Beauchamp EM, et al. Inhibitor-sensitive FGFR2 and FGFR3mutations in lung squamous cell carcinoma. Cancer Res 2013;73:5195–205.
11. Kuroso K, Imai Y, Kobayashi M, Yanagimoto K, Suzuki T, Kojima M,et al. Immunohistochemical detection of fibroblast growth factorreceptor 3 in human breast cancer: correlation with clinicopatholog-ical/molecular parameters and prognosis. Pathobiology 2010;77:231–40.
12. Glenisson M, Vacher S, Callens C, Susini A, Cizeron-Clairac G, LeScodan R, et al. Identification of new candidate therapeutic targetgenes in triple-negative breast cancer. Genes Cancer 2012;3:63–70.
13. Singh D, Chan JM, Zoppoli P, Niola F, Sullivan R, Castano A, et al.Transforming fusions of FGFR and TACC genes in human glioblasto-ma. Science 2012;337:1231–5.
14. Parker BC, Annala MJ, Cogdell DE, Granberg KJ, Sun Y, Ji P, et al. Thetumorigenic FGFR3-TACC3 gene fusion escapes miR-99a regulationin glioblastoma. J Clin Invest 2013;123:855–65.
15. Goriely A, Hansen RM, Taylor IB, Olesen IA, Jacobsen GK, McGowanSJ, et al. Activating mutations in FGFR3 and HRAS reveal a sharedgenetic origin for congenital disorders and testicular tumors.NatGenet2009;41:1247–52.
16. Goebell PJ, Knowles MA. Bladder cancer or bladder cancers? Genet-ically distinct malignant conditions of the urothelium. Urol Oncol2010;28:409–28.
17. Cappellen D, De Oliveira C, Ricol D, de Medina S, Bourdin J, Sastre-Garau X, et al. Frequent activating mutations of FGFR3 in humanbladder and cervix carcinomas. Nat Genet 1999;23:18–20.
18. vanRhijnBW,Montironi R, Zwarthoff EC, Jobsis AC, vanderKwast TH.Frequent FGFR3 mutations in urothelial papilloma. J Pathol 2002;198:245–51.
19. Tomlinson DC, Baldo O, Harnden P, Knowles MA. FGFR3 proteinexpression and its relationship to mutation status and prognosticvariables in bladder cancer. J Pathol 2007;213:91–8.
20. Al-Ahmadie HA, Iyer G, Janakiraman M, Lin O, Heguy A, Tickoo SK,et al. Somatic mutation of fibroblast growth factor receptor-3 (FGFR3)defines a distinct morphological subtype of high-grade urothelialcarcinoma. J Pathol 2011;224:270–9.
21. Williams SV, Hurst CD, Knowles MA. Oncogenic FGFR3 gene fusionsin bladder cancer. Hum Mol Genet 2013;22:795–803.
22. WuYM,SuF, Kalyana-SundaramS,KhazanovN, AteeqB,CaoX, et al.Identification of targetable FGFR gene fusions in diverse cancers.Cancer Discov 2013;3:636–47.
23. Gomez-Roman JJ, Saenz P, Molina M, Cuevas Gonzalez J, EscuredoK, Santa Cruz S, et al. Fibroblast growth factor receptor 3 is over-expressed in urinary tract carcinomas and modulates the neoplasticcell growth. Clin Cancer Res 2005;11:459–65.
24. Plowright EE, Li Z, Bergsagel PL, ChesiM, Barber DL, BranchDR, et al.Ectopic expression of fibroblast growth factor receptor 3 promotesmyeloma cell proliferation and prevents apoptosis. Blood 2000;95:992–8.
25. Chesi M, Brents LA, Ely SA, Bais C, Robbiani DF, Mesri EA, et al.Activated fibroblast growth factor receptor 3 is an oncogene thatcontributes to tumor progression in multiple myeloma. Blood 2001;97:729–36.
26. Bernard-Pierrot I, Brams A, Dunois-Larde C, Caillault A, Diez deMedina SG, Cappellen D, et al. Oncogenic properties of the mutatedforms of fibroblast growth factor receptor 3b. Carcinogenesis 2006;27:740–7.
27. Martinez-Torrecuadrada J, Cifuentes G, Lopez-Serra P, Saenz P,Martinez A, Casal JI. Targeting the extracellular domain of fibroblastgrowth factor receptor 3 with human single-chain Fv antibodies inhi-bits bladder carcinoma cell line proliferation. Clin Cancer Res2005;11:6280–90.
28. Tomlinson DC, Hurst CD, Knowles MA. Knockdown by shRNA iden-tifies S249Cmutant FGFR3 as a potential therapeutic target in bladdercancer. Oncogene 2007;26:5889–99.
29. Qing J, Du X, Chen Y, Chan P, Li H, Wu P, et al. Antibody-basedtargeting of FGFR3 in bladder carcinoma and t(4;14)-positive multiplemyeloma in mice. J Clin Invest 2009;119:1216–29.
30. Lamont FR, Tomlinson DC, Cooper PA, Shnyder SD, Chester JD,Knowles MA. Small molecule FGF receptor inhibitors block FGFR-dependent urothelial carcinomagrowth in vitro and in vivo. Br J Cancer2011;104:75–82.
31. Gust KM, McConkey DJ, Awrey S, Hegarty PK, Qing J, BondarukJ, et al. Fibroblast growth factor receptor 3 is a rational thera-peutic target in bladder cancer. Mol Cancer Ther 2013;12:1245–54.
32. Novartis. A dose escalation study in adult patients with advanced solidmalignancies. Available from: http://clinicaltrials.gov/ct2/show/NCT01004224.
33. Novartis, H.O.G.a. A Phase II trial of Dovitinib in Bacillus Calmette-Guerin(BCG) refractory urothelial carcinoma patients with tumorfibroblast growth factor receptor 3(FGFR3) mutations or overex-pression. Available from: http://clinicaltrials.gov/ct2/show/NCT01732107.
34. Gavine PR, Mooney L, Kilgour E, Thomas AP, Al-Kadhimi K, Beck S,et al. AZD4547: an orally bioavailable, potent, and selective inhibitor ofthe fibroblast growth factor receptor tyrosine kinase family. CancerRes 2012;72:2045–56.
35. Genentech. Trial evaluating the safety and pharmacokinetics ofMFGR1877S in patients with advanced solid tumors. Available from:http://clinicaltrial.gov/ct2/show/NCT01363024.
36. Du X, Wang QR, Chan E, Merchant M, Liu J, French D, et al. FGFR3stimulates stearoyl CoA desaturase 1 activity to promote bladdertumor growth. Cancer Res 2012;72:5843–55.
37. Dijkgraaf GJ, Alicke B, Weinmann L, Januario T, West K, Modrusan Z,et al. Small molecule inhibition of GDC-0449 refractory smoothenedmutants and downstreammechanismsof drug resistance. Cancer Res2011;71:435–44.
38. O'Donnell PH, Goldman JW,GordonMS, Shih K, Choi YJ, LuD, et al. APhase I dose-escalation study of MFGR1877S, a human monoclonalanti-fibroblast growth factor receptor 3 (FGFR3) antibody, in patients(pts) with advanced solid tumors. Eur J Cancer 2012;48:Supplement 6,191–2.
39. Szarvas T, vomDorp F, Ergun S, RubbenH.Matrix metalloproteinasesand their clinical relevance in urinary bladder cancer. Nat Rev Urol2011;8:241–54.
40. Yan C, Boyd DD. Regulation of matrix metalloproteinase gene expres-sion. J Cell Physiol 2007;211:19–26.
41. Miyake H, Yoshimura K, Hara I, Eto H, Arakawa S, Kamidono S.Basic fibroblast growth factor regulates matrix metalloproteinases
Du et al.
Clin Cancer Res; 20(24) December 15, 2014 Clinical Cancer Research6334
on November 11, 2020. © 2014 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 17, 2014; DOI: 10.1158/1078-0432.CCR-13-3336

production and in vitro invasiveness in humanbladder cancer cell lines.J Urol 1997;157:2351–5.
42. Itoh M, Murata T, Suzuki T, Shindoh M, Nakajima K, Imai K, et al.Requirement of STAT3 activation for maximal collagenase-1(MMP-1) induction by epidermal growth factor and malignantcharacteristics in T24 bladder cancer cells. Oncogene 2006;25:1195–204.
43. Wallard MJ, Pennington CJ, Veerakumarasivam A, Burtt G, Mills IG,Warren A, et al. Comprehensive profiling and localisation of the matrixmetalloproteinases in urothelial carcinoma. Br J Cancer 2006;94:569–77.
44. Goodison S, Chang M, Dai Y, Urquidi V, Rosser CJ. A multi-analyteassay for the non-invasive detection of bladder cancer. PLoS ONE2012;7:e47469.
45. Nakopoulou L, Gakiopoulou H, Zervas A, Giannopoulou I,Constantinides C, Lazaris AC, et al. MMP-3 mRNA and MMP-3 andMMP-1 proteins in bladder cancer: a comparison with clinicopatho-logic features and survival. Appl Immunohistochem Mol Morphol2001;9:130–7.
46. Seargent JM, Loadman PM, Martin SW, Naylor B, Bibby MC, Gill JH.Expression of matrix metalloproteinase-10 in human bladder transi-tional cell carcinoma. Urology 2005;65:815–20.
47. Nutt JE, Mellon JK, Qureshi K, Lunec J. Matrix metalloproteinase-1 isinduced by epidermal growth factor in human bladder tumour cell linesand is detectable in urine of patients with bladder tumours. Br JCancer1998;78:215–20.
48. Durkan GC, Nutt JE, Rajjayabun PH, Neal DE, Lunec J, Mellon JK.Prognostic significance of matrix metalloproteinase-1 and tissueinhibitor of metalloproteinase-1 in voided urine samples from patientswith transitional cell carcinoma of the bladder. Clin Cancer Res2001;7:3450–6.
49. Dey JH, Bianchi F, Voshol J, Bonenfant D, Oakeley EJ, Hynes NE.Targeting fibroblast growth factor receptors blocks PI3K/AKT signal-ing, induces apoptosis, and impairs mammary tumor outgrowth andmetastasis. Cancer Res 2010;70:4151–62.
50. Roy R, Yang J, Moses MA. Matrix metalloproteinases as novel bio-markers and potential therapeutic targets in human cancer. J ClinOncol 2009;27:5287–97.
www.aacrjournals.org Clin Cancer Res; 20(24) December 15, 2014 6335
Urinary Pharmacodynamic Markers for R3Mab in Bladder Cancer
on November 11, 2020. © 2014 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 17, 2014; DOI: 10.1158/1078-0432.CCR-13-3336

2014;20:6324-6335. Published OnlineFirst October 17, 2014.Clin Cancer Res Xiangnan Du, Benjamin C. Lin, Qian-Rena Wang, et al. CancerBiomarkers of FGFR3-Targeted Therapy in Patients with Bladder MMP-1 and Pro-MMP-10 as Potential Urinary Pharmacodynamic
Updated version
10.1158/1078-0432.CCR-13-3336doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2014/10/18/1078-0432.CCR-13-3336.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/20/24/6324.full#ref-list-1
This article cites 47 articles, 15 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/20/24/6324.full#related-urls
This article has been cited by 2 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/20/24/6324To request permission to re-use all or part of this article, use this link
on November 11, 2020. © 2014 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst October 17, 2014; DOI: 10.1158/1078-0432.CCR-13-3336