Embed Size (px)
Citation preview

http://neurology.thelancet.com Vol 7 January 2008 97
Review
Mitochondria in the aetiology and pathogenesis of Parkinson’s diseaseAnthony HV Schapira
Several biochemical abnormalities have been described in the brains of patients with Parkinson’s disease (PD), including oxidative stress and mitochondrial dysfunction. The identifi cation of specifi c gene mutations that cause PD has reinforced the relevance of oxidative stress and mitochondrial dysfunction in the familial and the sporadic forms of the disease. The proteins that are associated with familial PD—PTEN-induced putative kinase 1 (PINK1), DJ-1, α-synuclein, leucine-rich repeat kinase 2, and, possibly, parkin—are either mitochondrial proteins or are associated with mitochondria, and all interface with the pathways of oxidative stress and free radical damage. Insights into the aetiology and pathogenesis of PD provide hope that drugs or cocktails of drugs that might successfully intervene in the pathogenesis and slow the progression of the disease can be derived from the study of the converging rather than diverging pathways to cell dysfunction and death.
IntroductionThe incidence of Parkinson’s disease (PD) is estimated as 8–18 per 100 000 person-years, and the prevalence is approximately 0·3% of the entire population: PD aff ects more than 1% of those older than 60 years and up to 4% of those older than 80 years.1 PD is, therefore, the second most common neurodegenerative disease after Alzheimer’s disease. The clinical phenotype of PD is homogeneous, and the clinical–pathological correlation can be as high as 98·5% with experienced diagnosticians.2 However, the genotype of PD is heterogeneous, and several genes are known to cause familial PD (table), whereas other genes are associated with parkinsonian syndromes. The aetiology of the PD phenotype is, therefore, multifactorial, which is also likely to apply to most of the, apparently sporadic, idiopathic cases of PD.3 Several biochemical abnormalities that were thought to be relevant to the pathogenesis were seen in the brains of patients with PD before the discovery of the fi rst genetic cause;4 these abnormalities included mitochondrial dysfunction, free-radical-mediated damage, excitotoxicity, and infl ammatory changes. Data on the phenotype and expression of the mutant genes implicated in familial PD have confi rmed the relevance of these biochemical defi cits to the pathogenesis. The link between mitochondrial dysfunction and idiopathic PD was fi rst made after the discovery of mitochondrial complex I defi ciency in the substantia nigra.5 The connection between mitochondria and PD has been reinforced by the fi nding that several of the genes that cause familial PD encode mitochondrial proteins and that mitochondrial toxins can cause PD in animals. Apart from the production of energy substrates by oxidative phosphorylation, mitochondria have a fundamental role in mediating cell death by apoptosis, which has been reviewed in detail elsewhere.6 Many diff erent cellular processes can lead to apoptosis through mitochondrial membrane permeabilisation, and many molecules regulate this pathway. Inevitably, many of the biochemical abnormalities caused by expression of mutant genes that are discussed in this Review might initiate mitochondrial-
mediated apoptosis; however, the abnormalities will be discussed in detail only if they have a direct connection to mitochondria or mitochondrial function beyond the initiation of apoptosis. The contribution of mitochondria to the aetiology and pathogenesis of PD will be reviewed.
Mitochondrial dysfunction in PDThe direct relation between mitochondrial dysfunction and PD came from the post-mortem description of complex I defi ciency in the substantia nigra of patients with PD.5 Subsequently, the defi ciency was also seen in the skeletal muscle and platelets7,8 and there was a decrease in complex I proteins in the substantia nigra of patients with PD.9 The complex I defi ciency in the substantia nigra and platelets has been consistently detected,10–14 whereas the mitochondrial abnormality in skeletal muscle has been more diffi cult to detect reliably.15–
17 The specifi city of the complex I defect in the brains of patients with PD has been supported by the recent fi nding that this is the only respiratory chain protein complex that is aff ected by endogenous oxidative damage and reduced structural stability.18 The substantia nigra in patients with PD is severely depleted of dopaminergic neurons. Tissue homogenates have been analysed in all
Lancet Neurol 2008; 7: 97–109
University Department of Clinical Neurosciences and Institute of Neurology, University College London, London, UK (AHV Schapira)
Correspondence to: Anthony HV Schapira, University Department of Clinical Neurosciences, University College London, Rowland Hill Street, London NW3 2PF, [email protected]
Mode of inheritance Locus Age at onset Lewy bodies Gene product
PARK1/4 AD 4q21 40s Yes α-Synuclein
PARK2 AR 6q25 20s+ No Parkin
PARK3 AD 2p13 60s Yes ··
UCH-L1 AD 4p15 50s Yes Ubiquitin thiolesterase
PINK1 AR 1p35 30s ·· PTEN-induced putative kinase 1
PARK7 AR 1p36 30s ·· DJ-1
LRRK2 AD 12p Variable Yes/no Leucine-rich repeat kinase 2
ATP13A2 AR 1p36 Variable ·· ATPase type 13A2
PARK10 AR 1p32 ·· ·· ··
PARK11 ·· 2q36–q37 ·· ·· ··
AD=autosomal dominant. AR=autosomal recessive.
Table: Genetic causes of parkinsonism

98 http://neurology.thelancet.com Vol 7 January 2008
Review
these studies, and the implication is that the mitochondrial defect cannot be restricted to neurons but also involves glia.
The mitochondrial complex I defi ciency is not present in all patients with PD, either in the brain, platelets, or other tissues. The severity of the defect is about a 35% reduction in activity when the patient group is compared with control populations. However, these studies inevitably report on an aetiologically heterogeneous population (eg, patients with PD who had severe complex I defi ciency and patients with PD who had healthy complex I activity). Furthermore, there are some patients with a substantial complex I defect in whom the defect is directly related to their aetiology, whereas other pathogenetic factors are important in other patients with PD. The small and unselected sample groups might explain why, for example, the mitochondrial abnormality has not been seen consistently in skeletal muscle. The complex I defi ciency in the substantia nigra and platelets implies that it is a systemic defect in a proportion of cases (~25% on the basis of platelet activities) and this might be due to genetic or environmental (endogenous or exogenous) causes.
The complex I defect in patients with PD lowers the threshold of apoptosis mediated by the mitochondria—through a decrease in ATP production and by the generation of free radicals—and sensitises cells to the proapoptotic protein Bax.19
Mitochondrial DNA in patients with PDBecause the mitochondrial DNA (mtDNA) encodes 13 of the 83 respiratory chain protein subunits, including seven of the complex I proteins, mutations in the mtDNA were an obvious early target for analysis. Although there are more deletions in the mtDNA of patients with PD, a comparison with age-matched controls reported no substantial increase.20–22 However, since these early studies, more sensitive techniques have become available to detect the proportion of deleted mtDNA in individual cells. The number of mtDNA deletions in individual neurons in the substantia nigra is substantially increased in patients older than 65 years.23 The deletions within a neuron are clonal and associated with decreased cytochrome oxidase activity, as seen with histochemistry. Another study used similar techniques to investigate the number of deletions in mtDNA in the brains of patients with parkinsonism, widespread Lewy body deposition, and less severe loss of nigral dopaminergic neurons.24 A high proportion of mtDNA deletions (43±9·3%) was seen in controls, which increased with age, and more mtDNA deletions were found in patients with parkinsonism and dementia (52·3±9·3%). These results support the proposal that the human substantia nigra is a site of free-radical-mediated damage to mtDNA, and that this damage is enhanced in parkinsonism.
Sequencing of the mtDNA of patients with PD has generally been done in unselected groups, with and
without a mitochondrial defi ciency.25,26 Although the results of some reports have suggested increased frequency of specifi c mtDNA polymorphisms in patients with PD, this has not been replicated in all studies.27–31 Certain mtDNA haplotypes infl uence PD expression; haplotype J is associated with a signifi cant decrease in risk of PD, which, in turn, is strongly associated with a single nucleotide polymorphism (A10398G).32 The results of a second study showed a 22% decrease in the risk of PD in people with the UKJT haplotype cluster.33 By contrast, a smaller study reported an increased risk of PD in patients with haplotypes J and T.34 Some evidence suggests that mtDNA haplotypes might infl uence cytosolic pH and mitochondrial calcium regulation,35 which could infl uence neuronal function and integrity over time.
Two studies have reported the use of genetic transplantation to investigate the potential of mtDNA from patients with PD to determine the origin of the complex I defect. In one study, platelets from unselected patients with PD were fused and grown in mixed culture.36 In another study, patients with PD were selected on the basis of a peripheral complex I defi ciency,37 and cells from these patients were fused with cells that lack mtDNA (rho–) and grown in mixed or clonal culture. In both studies, the mtDNA that was transferred from the patients with PD caused a complex I defect in the recipient cybrid cells, which suggests that the mtDNA in these patients caused the complex I defi ciency through inherited or somatic mutations. The results of subsequent experiments have suggested that the recipient cells also developed abnormal calcium handling and a lower mitochondrial membrane potential.
A mutation in the mtDNA 12S RNA was seen in a patient with maternally inherited, early-onset PD, deafness, and neuropathy,38 and a deletion in the gene encoding cytochrome b was found in a patient with parkinsonism.39 However, these mutations have not been found in other patients with PD. Another study investigated sequence changes in gene encoding mitochondrially encoded NADH dehydrogenase 5 (MT-
ND5) in the brains of patients with PD and controls; the authors reported an excess of heteroplasmic modifi cations in MT-ND5 in the patients with PD.40 However, this has yet to be replicated.
Another development is the production of a mouse model of PD with a conditional knockout approach to disrupt the gene encoding mitochondrial transcription factor A (Tfam) in dopaminergic neurons.41 Tfam knockout mice had a progressive levodopa-responsive motor defi cit from 14 weeks. Pathological examination showed a progressive loss of dopaminergic neurons in the substantia nigra—60% of the neuron density in controls at 12 weeks old to 10% of the neuron density of the controls at 43 weeks—and a parallel decrease in striatal dopamine concentrations. Reduced expression of mtDNA encoded subunit I of cytochrome oxidase was

http://neurology.thelancet.com Vol 7 January 2008 99
Review
reported at 6 weeks, which preceded neuronal loss, and α-synuclein-negative cytoplasmic inclusions were seen in the degenerating dopaminergic cells.
Mitochondrial proteins and familial PDParkinThe gene and proteinPARK2 (parkin) is transcribed ubiquitously, and intracellular localisation studies have reported the association of parkin and the endoplasmic reticulum, Golgi apparatus, synaptic vesicles, and mitochondria.42–44 The function of parkin is unknown but the protein contains several domains for protein–protein interactions and E3 ligase activity. The ligase activity is a function of the ubiquitin proteasomal pathway, and several substrates for parkin ubiquitin ligase activity have been found, including a 22 kDa glycosolated form of α-synuclein, parkin-associated endothelin-receptor-like receptor (Pael-R), and CDCrel-1, a protein involved in cytokinesis that infl uences synaptic vesicle function.45,46 Overexpression of Pael-R causes the protein to become ubiquinated, insoluble, and unfolded, and leads to endoplasmic reticulum stress and cell death.47 The accumulation of insoluble Pael-R has been found in the brains of patients with mutations in the gene encoding parkin (PARK2), which suggests a possible toxic mechanism.
Parkin is constitutively phosphorylated, and the phosphorylation can be modulated by proteasomal dysfunction and endoplasmic reticulum stress.48 The ability of parkin to ubiquinate proteins might be impaired by S-nitrosylation, which might, in turn, be due to excitotoxic-mediated damage.49
The authors of a recent study report that in SHSY-5Y cells, parkin is mostly localised to the mitochondria in dividing cells,50 but redistributes to the Golgi apparatus or the nucleus on diff erentiation. When cells were exposed to uncouplers or inhibitors of respiratory chain activity, including rotenone, parkin was released into the cytosol. Cell cycle blockers induced a similar redistribution of parkin. The transfer of parkin from the mitochondria to the cytosol involved the mitochondrial permeability transition pore. To support the mitochondrial localisation of parkin, Kuroda and co-workers50 showed that the protein could be imported into mitochondria, and cells with parkin mutants translocated less than cells with wild-type parkin. Overexpression of parkin in SHSY-5Y cells increased transcription and translation of mtDNA in dividing cells, mediated by the interaction with mtDNA transcription factor A. The direct association between parkin and mitochondria is of considerable interest and warrants confi rmation and additional examination.
Mutations in PARK2Mutations in PARK2 were fi rst reported in patients with juvenile-onset parkinsonism51 and have subsequently been shown to be the most common cause of PD in
people younger than 20 years,52 although patients with later-onset cases have also been reported.53,54 Patients with mutations in PARK2 often present with symmetrical parkinsonism, slow progression, a good response to levodopa, and early dyskinesias. The fi rst patients to be reported had marked benefi t from sleep, hyper-refl exia, and dystonia; however, these features can be seen in patients with other recessive causes of PD and are not specifi c. Many mutations in PARK2 have been reported, and many are heterozygous sequence changes. A single mutation has been suggested to serve as a risk factor for PD.55 Autopsy examination of the brains of juvenile-onset, parkin-mutation positive patients showed variable pathology, including a lack of Lewy bodies.56 However, Lewy bodies were seen in later-onset cases.53,55
An increase in striatal extracellular dopamine concentrations, reduced synaptic excitability, and mild, non-progressive motor defi cit at 2–4 months were described in a PARK2 knockout mouse.57 No loss of dopaminergic neurons and no inclusion formations were noted. Dopamine-receptor-binding affi nities and concentrations of parkin E3 ligase substrate were normal. PARK2 knockout mice had decreased mitochondrial respiratory chain function in the striatum and reductions in specifi c respiratory chain and antioxidant proteins.58 Midbrain neuronal cultures from PARK2 knockout mice had increased sensitivity to rotenone-induced apoptotic cell death, which was ameliorated by minocycline.59 PARK2 knockout fl ies developed muscle pathology, mitochondrial abnormalities, and apoptotic cell death.60
Mitochondrial function was decreased (complex I and IV activities) in peripheral blood from patients with mutations in PARK2.61
PINK1 (PTEN-induced putative kinase 1)The gene and proteinThe gene encoding PINK1 comprises 8 exons and encodes a ubiquitously expressed, insoluble, 581 amino acid, 63 kDa protein with an 8 kDa amino-terminal, mitochondrial-targeting sequence. The complete protein is transcribed in the nucleus, translated in the cytoplasm, and imported intact into the mitochondria, with subsequent processing and intramitochondrial sorting. There is some evidence that PINK1 is localised to the inner mitochondrial membrane, and part of the structure, probably the C terminus, is exposed to the intermembrane space.62 An early observation was that PINK1 was upregulated in cancer cells by the product of the tumour suppressor gene PTEN.63 PINK1 has a putative serine–threonine protein kinase catalytic domain between residues 156 and 509 that is capable of autophosphorylation.64
The serine–threonine kinase domain of PINK1 has substantial homology with the CG4523 protein in drosophila.65 CG4523 interacts with a protein in the fl y that is a homologue of the mammalian mitochondrial translation-initiating factor 3 (MTIF3), which makes this a candidate protein for interacting with PINK1. Analysis

100 http://neurology.thelancet.com Vol 7 January 2008
Review
of genetic variants of MTIF3 in patients with PD found an allelic association between the C798T polymorphism and PD.65
Mutations in PINK1Mutations in PINK1 are a cause of autosomal recessive PD.66 Mutations have been reported within and outside the kinase domain; however, the localisation of PINK1 to the mitochondria is not aff ected by these mutations.
Several homozygous mutations have been reported in patients with familial PD, indicating that loss of function underlies the pathogenesis. Most patients with mutations in PINK1 have onset of parkinsonism before age 40 years (most in the fourth decade), with features typical of PD: good responses to levodopa and slow progression but early motor complications. Many of these patients have mutations in the kinase region of PINK1, which aff ects activity or substrate recognition,67,68 but some are elsewhere in the protein, including the carboxy terminal.69 In an index case, a homozygous four base insertion at the C terminal (1573–1574 in exon 8) was associated with onset of parkinsonism at 28 years, asymmetrical resting and postural tremor, rigidity in all limbs, falls, dystonia, and sleep benefi t. There was a good response to 300 mg per day levodopa, but dyskinesias occurred after only 3 months. The clinical picture of this mutation, therefore, resembles that of patients with mutations in parkin or DJ-1. The C-terminal W437X mutation enhanced autophosphorylation of PINK1, whereas mutations in the kinase domain did not.62,70 This is consistent with the notion that the C terminal negatively regulates the kinase activity of the wild-type protein.
Post-mortem examination of the brains of patients with mutations in PINK1 showed nigrostriatal cell loss and Lewy body formation.71 PINK1 was seen in a small proportion (5–10%) of Lewy bodies in the brains of patients with PD; PINK1 also localises to the aggrosome during proteasomal inhibition, when there is also increased cleavage of the protein.72 Mutant PINK1 has a similar distribution to Lewy bodies and aggrosomes under the same conditions. Accumulation of aggrosomes is a consequence of mitochondrial recruitment after proteasomal inhibition.
Mutations in PINK1 are rare, and sequence variations are not thought to infl uence common forms of sporadic PD.73,74 In a European study, two of 100 patients with young-onset PD had causative mutations in PINK1: one patient was homozygous and the other patient was compound heterozygous.67 A further fi ve patients had one mutation in PINK1—ie, they were heterozygous compared with two of 200 controls. The patients who were heterozygous for PINK1 mutation had a mean age of onset of 44 years (range 37–47 years), but the group only comprised patients with PD with onset before age 50 years; therefore, this is not indicative of the mean age of onset in carriers in the general population. The
patients who were heterozygous for the causative PINK1 mutations had features typical of young-onset PD.
A study of Italian and German families with PD reported nine patients with PD who were homozygous or compound heterozygous for the C1366T mutation in PINK1, which results in a K456Stop truncation of PINK1.75 This is the most commonly reported mutation of PINK1 in patients with PD and is found in the homozygous form and even as a single heterozygous mutation in the absence of a second identifi able mutation.67,76,77 In the study of the German family, there were two patients with typical PD, six patients who had subtle features of PD, including rigidity or bradykinesia, and six patients with no clinical abnormalities, all of whom were heterozygous for the C1366T mutation. The C1366T mutation reduces PINK1 transcript levels to 10–20% of normal in the homozygous carriers and to 50–60% in the heterozygous carriers.78 A mechanism by which the single mutant allele can increase risk of PD is through a dominant-negative eff ect on the translated truncated protein. The phenotype of heterozygous carriers of PINK1 mutations and whether they have an increased risk of PD was further investigated in an extended German family in whom the index case had a Q456X mutation in exon 775 and 14 family members had mutations in PINK1, including three homozygous individuals, who were aff ected, two heterozygous patients with probable PD, four individuals with possible PD, and fi ve unaff ected carriers. The age of onset was 39–61 years, with relatively mild PD in those with homozygous mutations. The clinical signs in those patients with possible PD were subtle and were noted only on careful neurological examination.
In a study of 80 patients with early-onset PD (<55 years), mutations in PINK1 were found in two homozygous patients and one heterozygous carrier in a Chinese population.79 Mutations in PINK1 were increased (1·2% vs 0·4%) in patients with PD compared with controls and the mutations were associated with reduced mitochondrial membrane potential.80
Patients who are heterozygous for mutations in PINK1 have reduced intensity with 18-fl uorodopa positron emission tomography compared with controls.81 However, there is signifi cant phenotypic variability among the PINK1 heterozygotes, suggesting that other genetic or environmental factors might have a role in disease penetrance. Whether single mutations in PINK1
predispose carriers to PD is a controversial area.
Parkin rescues PINK1 mutantsPINK1 knockout fl ies are viabile but sterile or hypofertile, have a motor defi cit, a shorter life-span, an abnormal fl ight muscle with impaired function, disorganised mitochondrial morphology, reduced mitochondrial mass, lower concentrations of ATP, and a small reduction in the number of dopaminergic neurons.82,83 The PINK1 knockout fl ies have increased sensitivity to paraquat and rotenone, which implies that PINK1 participates in the

http://neurology.thelancet.com Vol 7 January 2008 101
Review
defence against oxidative stress. This phenotype is similar to that of PARK2 knockout fl ies; therefore, the rescue of PINK1-related abnormalities by overexpression of parkin, but not vice versa, is interesting. Furthermore, knockouts of both genes do not exacerbate the phenotype. These data suggest that parkin and PINK1 participate in the same pathogenetic pathway, that this pathway is linear, and that PINK1 is upstream of parkin.
DJ-1The gene and proteinDJ-1 is a 23 kDa protein that is expressed in peripheral tissues and parts of the brain, including the striatum, substantia nigra pars compacta, and reticulata in neurons and glia, but is highly expressed in the cerebellum, hippocampus, and olfactory bulb.84 Studies of the intracellular distribution of DJ-1 show that it is found in several pools, including the mitochondria, where it is present in the intermembrane space and matrix.
DJ-1 has several functions, including as an oncogene, a modulator of androgen-receptor-dependent transcription, and as a sensor of oxidative stress.85–87 Oxidative stress and PD-associated mutations did not increase the mitochondrial localisation of DJ-1, although other researchers have shown that DJ-1 might translocate to the outer mitochondrial membrane during oxidative stress.87–89
The deletion or silencing of DJ-1 sensitises cells to oxidative stress, and overexpression of DJ-1 protects cells; this implies a protective role for the protein.90 DJ-1 forms a nuclear complex with RNA-binding proteins and DNA-binding proteins that regulates gene transcription and can prevent apoptotic cell death by α-synuclein or oxidative stress.
Mutations in DJ-1Mutations in the gene encoding DJ-1 (PARK7) are a rare cause of autosomal recessive PD.91 Patients with mutations in PARK7 have young-onset PD, progress slowly, respond well to levodopa, and might have dystonia. Mutations in PARK7 that cause familial PD lead to protein instability or decreased nuclear localisation, decreased transcriptional activation, and decreased protection against apoptosis.92 The L166P mutation is also associated with increased mitochondrial localisation,91 although this was not confi rmed in other studies.84 DJ-1 might also reduce the aggregation of α-synuclein.93
Two members of a Chinese family who developed PD in their 30s had single (C1196T) mutations in PARK7 and PINK1 on separate alleles;94 a 42-year-old sibling with the same genotype was unaff ected. Overexpression of DJ-1 and PINK1 in SHSY-5Y cells showed that both the wild-type and mutant forms of each protein interact, and DJ-1 stabilised PINK1. The wild-type forms of both proteins reduced 1-methyl-4-phenylpyridinium-induced toxicity, whereas the respective mutant proteins lost this ability.
PARK7 knockout mice have motor abnormalities, although there is no change in the number or morphology of neurons in the substantia nigra.95 Substantia nigra neurons from PARK7 knockout mice have enhanced sensitivity to blockade of Na/K ATPase and energy-dependent metabolism;96 furthermore, the PARK7 knockout mice have increased sensitivity to MPTP (1-methyl 4-phenyl 1,2,3,6-tetrahydropyridine) and oxidative stress.97
Other mitochondrial proteins and PD or parkinsonism Mitochondrial DNA polymerase gamma 1 (POLG1)Mitochondrial DNA polymerase gamma (POLG1) is essential for mtDNA synthesis, replication, and repair. The protein is a heterodimer that comprises a 140 kDa α-subunit and a 41 kDa β-subunit, which are encoded by nuclear DNA and imported into the mitochondria where they are located within the inner mitochondrial membrane. The α-subunit is catalytic and contains polymerase and exonuclease activities; the β-subunit helps DNA binding and promotes DNA synthesis.98
Mutations in the gene encoding POLG1 (POLG1) have been reported in a wide range of clinical phenotypes, including autosomal dominant or recessive progressive external ophthalmoplegia and parkinsonism.99 Patients fi rst develop progressive external ophthalmoplegia, with age of onset in the range 10–54 years, and then an asymmetric, levodopa-responsive bradykinetic rigid syndrome with resting tremor between 6 and 40 years later. Additional features of progressive external ophthalmoplegia include variable limb, pharyngeal, or facial weakness, cataracts, ataxia, peripheral neuropathy, and premature ovarian failure.100 Muscle biopsies show changes that are typical of mitochondrial disease: ragged-red, cytochrome-oxidase-negative fi bres and multiple deletions in the mtDNA seen on Southern blotting. Reduced striatal uptake of [18F]β-CFT (2β-carbomethoxy-3β-(4-fl uorophenyl)-8-(2-[18F]fl uoroethyl)nortropane) was seen symmetrically in two patients, and the pathology of another two patients showed severe loss of dopaminergic neurons in the substantia nigra, without Lewy bodies or other α-synuclein aggregates. Two patients with parkinsonism and an axonal peripheral neuropathy without progressive external ophthalmoplegia have also been described; these patients had compound heterozygote mutations in POLG1,101 onset of a bradykinetic rigid syndrome in their 30s, mild to moderate morphological changes in the mitochondria on muscle biopsy, reductions in the activity of complexes I, III, and IV, and a 37% decrease in mtDNA content and multiple deletions. Mutations in various regions of POLG1 have been associated with parkinsonism and result in multiple mtDNA deletions and depletion.100,102
In humans, POLG1 includes a trinucleotide microsatellite CAG repeat that encodes a polyglutamine

102 http://neurology.thelancet.com Vol 7 January 2008
Review
tract in the N-terminal region that is downstream of the presumed mitochondrial-targeting sequence. No changes were seen in the CAG repeat in a series of patients with PD.103 Similarly, no mutations in POLG1 were found in 140 patients with sporadic PD.104 Thus, the parkinsonian phenotype associated with mutations in POLG1 is seen with either myopathy or neuropathy and morphological changes in skeletal muscle.
HtrA2/OmiHtrA2/Omi is a nuclear-derived mitochondrial protein that is located in the intermembrane space and is released into the cytosol after permeabilisation of the mitochondrial membrane, where it binds and inactivates inhibitors of apoptosis. HtrA2/Omi knockout mice have neurodegenerative disease, with features of motor neuron dysfunction, ataxia, and parkinsonism with striatal damage.105 A mutation in HtrA2/Omi (G399S) was found in four patients with late-onset, sporadic PD, and a polymorphism (A141S) was thought to be a risk factor for PD.106 Expression of G399S and A141S in SHSY-5Y cells reduced mitochondrial membrane potential and increased sensitivity to apoptosis induced by staurosporin. HtrA2 is a phosphorylation target of PINK1, and HtrA2 is phosphorylated at a residue adjacent to the residue G399S that is mutated in patients with PD who are carriers of HtrA2.107 Phosphorylation of HtrA2 is decreased in the brains of patients with PD with PINK1 mutations.
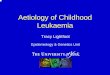
The interaction of known genetic causes of PD and their eff ects on mitochondrial function are summarised (fi gure 1). There is no clinical phenotype within the spectrum of idiopathic PD that predicts an underlying mitochondrial cause.
Non-mitochondrial proteins and mitochondrial dysfunctionMutations and multiplications of α-synuclein are a cause of autosomal dominant PD. α-Synuclein is an important component of Lewy bodies that is enriched in nerve terminals. The mechanisms by which this protein exerts its toxicity are not known but probably include enhanced aggregation; this explanation would fi t with the toxicity of wild-type α-synuclein in cell models and patients with familial PD with multiplications of the gene encoding α-synuclein. Phosphorylation of the serine residue at position 129 is important for mediating toxicity.108 Overexpression of mutant α-synuclein increases oxidative stress and impairs mitochondrial function.109 The A53T mutant, but not wild-type α-synuclein, increased toxicity to dopamine and was suggested to interfere with the incorporation of dopamine into vesicles.110,111 The A53T mutation was further implicated as a contributory factor to toxicity by the diminished eff ect of vesicular monoamine compartmentalisation by reserpine in A53T mutants.112
Transgenic mice that overexpress mutant (A53T or A30P) α-synuclein develop a motor defi cit at 10–15 months followed by rapidly progressive paralysis and death.113 Chromatolytic changes were seen in the neurons of the brain stem and these were more prevalent in A53T mutants (A53T>A30P>wild-type).114 Axonal changes were present in the brain stem and in selective tracts of the spinal cord. α-Synuclein was localised to the presynaptic nerve terminal and mitochondria, and intracytoplasmic aggregates of α-synuclein were present in addition to morphologically abnormal mitochondria and decreased cytochrome oxidase activity. α-Synuclein knockout mice are resistant to the mitochondrial toxins MPTP, malonate, and 3-nitropropionic acid; this protective eff ect might be mediated by the decreased production of free radicals in response to these toxins.115,116 In agreement with this, transgenic mice that overexpress mutant A53T α-synuclein showed increased pathology after exposure to the combination of the pesticides paraquat and maneb, although not separately.117
Mutations in the gene encoding leucine-rich repeat kinase 2 (LRRK2) are a common cause of familial PD, and are found in 5–8% of individuals with a fi rst-degree relative with PD and in 0·4–1·6% of patients with apparently sporadic PD.118–127 G2019S in the kinase domain is the most common mutation and accounts for most of the cases referenced above. Mutations have now been reported in all the main protein domains of leucine-rich repeat kinase 2; however, there is, at present, no distinction between the site of a mutation and a specifi c clinical phenotype. Wild-type leucine-rich repeat kinase 2 autophosphorylates and this might be a mechanism to regulate the protein. Antibodies to leucine-rich repeat kinase 2 have confi rmed the wide distribution of the protein throughout the brain and peripheral tissues:128 leucine-rich repeat kinase 2 is mostly associated with the
DJ-1
UPS
α-Synuclein
Omi/HtrA2
Parkin
LRRK2?
PINK1 UCHLI
Caspasecascadeactivation
Abnormalphosphorylation
↑O2˙̄Mitochondria
Figure 1: Potential interactions of the genetic causes of Parkinson’s diseaseMutations in PINK1 lead to mitochondrial dysfunction and, in combination with mutations in LRRK2, probably lead to abnormal phosphorylation of proteins, possibly including mitochondrial proteins. Parkin is downstream of PINK1 and might itself cause mitochondrial abnormalities in addition to impaired ubiquitination of proteins. The ubiquitin proteasomal system (UPS) will also be aff ected by mutations in UCHL1 (the gene encoding ubiquitin carboxyl-terminal esterase). The oxidative stress generated by mitochondrial dysfunction will modify α-synuclein aggregation and enhance toxic protofi bril formation. DJ-1 acts as an antioxidant signal molecule, and mutations in DJ-1 are associated with oxidative stress. Mitochondrial-mediated caspase cascade activation will be increased by these processes and by mutations in Omi/HtrA2.

http://neurology.thelancet.com Vol 7 January 2008 103
Review
cytoplasmic membrane rather than a membrane-bound protein and is present in the microsomal and outer mitochondrial membrane fractions (approximately 10% of the protein is associated with the latter).129–131 Leucine-rich repeat kinase 2 has many functions, and the relevance of at least some association with the mitochondria is unclear.132
Mitochondrial toxins and PDAlthough no toxin faithfully reproduces the clinical or pathological phenotype of PD (and there is a similar limitation for genetic models), several compounds induce dopaminergic cell death in human beings and other animals.
MPTP causes dopaminergic cell loss in the substantia nigra and induces parkinsonism in primates and rodents. MPTP is preferentially converted to MPP+ (1-methyl-4-phenylpyridinium) by monoamine oxidase B.133 MPP+ is concentrated by the mitochondria, where it inhibits complex I; MPP+ toxicity also generates free radicals, including nitric oxide.134
Rotenone is a potent and specifi c complex I inhibitor that is commonly used in the USA as a pesticide. Infusion of low doses of rotenone into rodents over 1 month caused nigrostriatal cell death and Lewy-like inclusions.135 Subsequent studies have reported that the damage induced by rotenone is also due to the generation of free radicals and is anatomically more widely distributed than in PD.136 The rotenone model is a useful tool to investigate pathogenetic events in patients with PD and understand the potential interaction of genetic and environmental factors in PD.
Rotenone causes the isoelectric point of DJ-1 to change, with the accumulation of acidic isoforms of DJ-1 in the striatum, substantia nigra, and olfactory bulb.137 Oxidation of DJ-1 was associated with a redistribution of the protein, from a diff use cytoplasmic pattern to localisation in the proximity of the mitochondria. The accumulation of the acidic forms of DJ-1 and its mitochondrial localisation could be prevented in cell culture by incubation with vitamin E. Chronic exposure to rotenone in cell culture induces cytosolic accumulation of α-synuclein,138 which can also be prevented by vitamin E. Systemic infusion of rotenone reduced proteasomal activity by 16–31% in the ventral midbrain but not in the striatum or cortex. Reduced proteasomal activity was seen in rats that had rotenone-induced cell loss, but not in those infused rats with no cell loss, which suggests a possible compensatory protective eff ect.137 Studies in cell culture reported that the eff ect on proteasomal function was mediated by inhibition of complex I; however, concentrations of ATP were unaff ected by rotenone, and proteasomal inhibition was prevented by vitamin E. The eff ect of rotenone on the proteasome is likely to be mediated by free-radical-induced damage. By contrast, fi ve of 25 pesticides induced proteasomal inhibition in cell culture (at concentrations between 10 nM and 10 µM) without
evidence of free-radical generation.139 Both rotenone and MPP+ caused the death of dopaminergic cells through apoptosis, an eff ect that can be blocked by cyclosporine.140
Annonacin is a complex I inhibitor that is found in sour sop, a drink from the Caribbean; when injected into rats, annonacin induces nigral degeneration.141
Cigarette smoking has consistently been associated with reduced risk for PD; smoking might infl uence the function of complex I and the expression of a disease phenotype due to mutations of complex I mtDNA genes.142
The pathogenetic events relevant to PD that are initiated by mitochondrial toxins and mitochondrial dysfunction are shown (fi gure 2).
Mitochondrial dysfunction, oxidative stress, and the ubiquitin proteasomal systemThere is substantial evidence of free-radical-mediated damage to proteins, lipids, and DNA in the substantia nigra of patients with PD,143 but the relationship between free-radical-induced damage and the complex I defect is not fully understood. However, inhibition of complex I or mutation of a complex I subunit results in increased free-radical generation; conversely, enhanced oxidative stress can induce abnormalities of mitochondrial function.144,145 Adult nigral dopaminergic neurons are particularly reliant on voltage-dependent calcium channels, and this reliance is relevant to the interaction between mitochondria and free radicals:146 increased intracellular calcium leads to an increase in mitochondrial-derived free radicals, particularly in the dendrites, which could underlie, at least in part, a predisposition to dying-back neuronal degeneration. The third mechanism of pathogenesis in patients with PD is proteasomal inhibition. Decreased activity and a reduction in the alpha subunits of the 26/20S proteosome seen on immunoblotting of substantia nigra isolates indicate an abnormality in the ubiquitin proteasomal system in patients with PD.147 Giving a proteasomal inhibitor systemically to rodents induces the loss of nigral dopaminergic neurons,148–150 although not all investigators have been able to reproduce these observations.151,152
Proteins are degraded in proteosomes by a series of ATP-dependent peptidases.153 A mitochondrial respiratory chain activity defect results in impaired oxidative phosphorylation and an increase in free-radical generation; the defect aff ects the function of the ubiquitin proteasomal system by limiting its activity and increasing the substrate load of oxidised protein.154 Similarly, a source of free radicals that is independent of the mitochondria will impair respiratory chain function and increase substrate load on the proteasome. Any cause of proteasomal dysfunction will lead to an accumulation of damaged proteins, with a potentially deleterious eff ect on cell function and survival. Thus, there is evidence within the nigra of patients with PD of all the elements of a self-

104 http://neurology.thelancet.com Vol 7 January 2008
Review
amplifying cycle of events that lead to cell death. Precisely where this cycle begins, how it develops, and its rate of progression might vary from one patient to another, and will depend on the primary underlying cause.
Mitochondrial dysfunction, oxidative stress, and abnormalities of the ubiquitin proteasomal system also connect with two other important parts of the pathogenesis of PD: infl ammation and excitotoxicity (fi gure 3).
Therapeutic implicationsThe recognition that mitochondrial dysfunction has a role in the pathogenesis of PD has provided a way to test the hypothesis that drugs that improve mitochondrial function might slow the progression of PD. The fi rst of these studies used co-enzyme Q10, which functions as a component of the respiratory chain that shuttles electrons between complexes I and III and as an antioxidant. The pilot trial reported by Shults and co-workers used a double-blind, placebo-controlled design with 16–23 patients in each arm, to assess the effi cacy of three doses of co-enzyme Q10 (300 mg per day, 600 mg per day, and 1200 mg per day) in patients with early PD.155 During a period of 16 months, the group that received the highest dose progressed at the slowest rate—established by worsening of motor function and activities of daily living (unifi ed Parkinson disease rating scale [UPDRS] parts II
and III)—compared with controls, although much of this benefi t was in the activities of daily living component and was assessed early in the trial. Co-enzyme Q10 was assessed in a futility analysis with historic control data and the total UPDRS score; this analysis failed to show futility, which suggested that the compound was worthy of future study.156 However, the authors called into question the validity of the historic control data in light of recent placebo progression rates in the UPDRS, which suggested futility of treatment with co-enzyme Q10. A small study of 28 patients with PD who were supplemented with 360 mg per day of co-enzyme Q10 showed a mild, symptomatic, motor eff ect over 4 weeks.157 However, a larger study with 300 mg per day supplementation with co-enzyme Q10, which produced the same plasma concentrations as in those patients who were treated with 1200 mg per day in the study by Shults and co-workers, found no symptomatic eff ect on the UPDRS score.158
Creatine, a dietary supplement that is well tolerated in high doses, is another potential treatment that has been investigated for its disease-modifying eff ect on the basis of the evidence of mitochondrial dysfunction in patients with PD: creatine is converted to phosphocreatine, which can transfer its phosphoryl group to ADP to synthesise ATP and, therefore, enhance energy production. Creatine can reduce dopaminergic cell loss in the MPTP-induced rodent model of PD,159 and is one of the compounds investigated in the National Institute of Neurological Disorders and Stroke (NINDS) neuroprotection exploratory trials in Parkinson’s disease (NET-PD) futility studies for
Substantia nigra toxins
↓ATP ↑O2
Complex Ideficiency
Deleted mtDNA
Oxidative stressBioenergetic failure
PTP
Apoptotic cascade Apoptosis Cell death
Protein aggregation
UPS dysfunction
Cell dysfunction↓∆ψm
˙̄
ExcitotoxicityMitochondria
Inflammation
Oxidative stress
Phosphorylation
UPS
Figure 2: Environmental toxins and the pathogenetic pathways to cell death in Parkinson’s diseaseSubstantia nigral toxins, such as MPTP and rotenone, induce complex I defi ciency and increase free-radical generation. The free radicals are probably the source of damage to mtDNA; and toxins and free radicals will both promote a fall in mitochondrial membrane potential (∆ψm), reduce ubiquitin proteasomal system (UPS) activity, and increase protein aggregation, cell dysfunction and death—directly or through apoptosis. These pathogenetic pathways are the same as those identifi ed in the brains of patients with idiopathic PD.
Figure 3: Factors that interact in the pathogenesis of Parkinson’s diseaseMitochondrial dysfunction, and complex I defects in particular, enhance free radical generation, which, in turn, impairs the function of the respiratory chain. Mitochondrial abnormalities decrease the activity of the ubiquitin proteasomal system (UPS), a process that is further exacerbated by the increased substrate load of oxidised protein from oxidative stress. Abnormalities in protein phosphorylation might infl uence the UPS and mitochondrial function. The infl ammation seen in the brains of patients with PD will increase free-radical production including nitric oxide and peroxynitrite. These free radical species will also be enhanced by excitotoxicty, which leads to nitric-oxide-mediated damage to the mitochondria.

http://neurology.thelancet.com Vol 7 January 2008 105
Review
neuroprotection in patients with PD. At a dose of 10 g per day, creatine was well tolerated and satisfi ed the predetermined criterion for non-futility on the basis of time to requirement for symptomatic therapy for 66 patients with early PD.160 The results of another blinded, placebo-controlled study of 2 g per day for 6 months (after a loading dose of 20 g for 6 days), then 4 g per day for 18 months in 31 patients with PD compared with 17 patients given placebo showed no signifi cant diff erence in UPDRS scores or single photon emission computed tomography scan dopamine transporter density.161 However, there was a lower requirement for dopaminergic symptomatic treatment in the patients who received creatine, which could indicate a positive eff ect of creatine.
Antiapoptotic drugs might also function, in part, through a mitochondrial pathway, although this would not be mediated by oxidative phosphorylation. An antiapoptotic agent, TCH346, did not show neuroprotection in patients with early PD.162 However, this negative result could have many explanations beyond simple ineffi cacy of the drug and should not deter further investigations of antiapoptotic drugs but rather stimulate work into better trial designs. Furthermore, drug combinations can be synergistic, particularly if they target diff erent pathogenetic routes. Additional drug strategies that do not target the dopaminergic system are also under development;163 however, such therapies will need to be used in the context of currently available symptomatic treatment.164
ConclusionsThe genetic causes of PD serve to re-enforce the validity of the mitochondria–oxidative stress–proteasomal dys-function axis in the pathogenesis of PD. Mutations and multiplications in the gene encoding α-synuclein enhance the aggregation of the protein, and this is enhanced by free radicals. Overexpression of wild-type and mutant forms of α-synuclein increase oxidative stress and lower the threshold for cell death from toxins such as dopamine and paraquat. Parkin and UCHL1 are part of the ubiquitination process of proteins: parkin, PINK1, and DJ-1 are mitochondrial proteins, and DJ-1 is a free-radical sensor. As reviewed here, the expression of mutant forms of these proteins impairs mitochondrial function and increases susceptibility to a range of endogenous and exogenous toxins. Phosphorylation is also a key component of the pathogenesis of PD: PINK1 and leucine-rich repeat kinase 2 have kinase activity, and phosphorylation of α-synuclein129 enhances its pathogenicity. The importance of these observations is that they highlight the potential pathogenetic pathways that might be initiated by genetic or environmental causes of PD. These pathways are of relevance to the development of compounds that might slow the progression of PD, and compounds that intervene in these pathways can be reasonably assumed to be of potential benefi t to patients with PD with a wide range of
diff erent causes. What is clear is that the identifi cation of the genetic causes of PD and understanding their biochemical consequences has provided insights into the aetiopathogenesis of PD.
There is increasing awareness that synaptic connectivity is important for neuronal function. In many respects, PD might be a dying-back degeneration, and MPTP toxicity might be a good example of this. The function of synaptic mitochondria and their role in calcium homoeostasis might be crucial for the maintenance and survival of the nigrostriatal system, which is worthy of further investigation and might provide opportunities to develop novel therapeutic interventions to protect connectivity.
No specifi c mutation in mtDNA has been consistently associated with PD. If mutations in mtDNA have an eff ect on the pathology of PD, their role is likely to be complex and perhaps involve combinations of sequence changes or specifi c haplotypes that might modify mitochondrial function and render the neuron cell body or synapse more vulnerable to nuclear genetic eff ects or environmental (endogenous or exogenous) infl uences. This, again, is an area worthy of further exploration.Confl icts of interestI have no confl icts of interest
References1 de Lau LM, Breteler MM. Epidemiology of Parkinson’s disease.
Lancet Neurol 2006; 5: 525–35.2 Hughes AJ, Daniel SE, Ben Shlomo Y, Lees AJ. The accuracy of
diagnosis of parkinsonian syndromes in a specialist movement disorder service. Brain 2002; 125: 861–70.
3 Warner TT, Schapira AH. Genetic and environmental factors in the cause of Parkinson’s disease. Ann Neurol 2003; 53 (suppl 3): S16–S23.
4 Schapira AH. Mitochondrial involvement in Parkinson’s disease, Huntington’s disease, hereditary spastic paraplegia and Friedreich’s ataxia. Biochim Biophys Acta 1999; 1410: 159–70.
5 Schapira AH, Cooper JM, Dexter D, et al. Mitochondrial complex I defi ciency in Parkinson’s disease. Lancet 1989; 1: 1269.
6 Kroemer G, Galluzzi L, Brenner C. Mitochondrial membrane permeabilization in cell death. Physiol Rev 2007; 87: 99–163.
7 Bindoff LA, Birch-Machin M, Cartlidge NE, Parker WD Jr, Turnbull DM. Mitochondrial function in Parkinson’s disease. Lancet 1989; 2: 49.
8 Parker WD, Jr, Boyson SJ, Parks JK. Abnormalities of the electron transport chain in idiopathic Parkinson’s disease. Ann Neurol 1989; 26: 719–23.
9 Mizuno Y, Ohta S, Tanaka M, et al. Defi ciencies in complex I subunits of the respiratory chain in Parkinson’s disease. Biochem Biophys Res Commun 1989; 163: 1450–55.
10 Schapira AH, Mann VM, Cooper JM, et al. Anatomic and disease specifi city of NADH CoQ1 reductase (complex I) defi ciency in Parkinson’s disease. J Neurochem 1990; 55: 2142–45.
Search strategy and selection criteria
References for this Review were identifi ed by searches of MEDLINE and of Current Contents with the search terms “mitochondria”, “α-synuclein”, “proteasome”, between 2000 and 2007. References were also identifi ed from relevant articles and through searches of the author’s fi les. Abstracts and reports from meetings were included only when they related directly to previously published work. Only papers published in English were reviewed.

106 http://neurology.thelancet.com Vol 7 January 2008
Review
11 Mann VM, Cooper JM, Daniel SE, et al. Complex I, iron, and ferritin in Parkinson’s disease substantia nigra. Ann Neurol 1994; 36: 876–81.
12 Janetzky B, Hauck S, Youdim MB, et al. Unaltered aconitase activity, but decreased complex I activity in substantia nigra pars compacta of patients with Parkinson’s disease. Neurosci Lett 1994; 169: 126–28.
13 Krige D, Carroll MT, Cooper JM, Marsden CD, Schapira AH. Platelet mitochondrial function in Parkinson’s disease. The Royal Kings and Queens Parkinson Disease Research Group. Ann Neurol 1992; 32: 782–88.
14 Haas RH, Nasirian F, Nakano K, et al. Low platelet mitochondrial complex I and complex II/III activity in early untreated Parkinson’s disease. Ann Neurol 1995; 37: 714–22.
15 Mann VM, Cooper JM, Krige D, et al. Brain, skeletal muscle and platelet homogenate mitochondrial function in Parkinson’s disease. Brain 1992; 115: 333–42.
16 Taylor DJ, Krige D, Barnes PR, et al. A 31P magnetic resonance spectroscopy study of mitochondrial function in skeletal muscle of patients with Parkinson’s disease. J Neurol Sci 1994; 125: 77–81.
17 Penn AM, Roberts T, Hodder J, et al. Generalized mitochondrial dysfunction in Parkinson’s disease detected by magnetic resonance spectroscopy of muscle. Neurology 1995; 45: 2097–99.
18 Keeney PM, Xie J, Capaldi RA, Bennett JP, Jr. Parkinson’s disease brain mitochondrial complex I has oxidatively damaged subunits and is functionally impaired and misassembled. J Neurosci 2006; 26: 5256–64.
19 Perier C, Tieu K, Guegan C, et al. Complex I defi ciency primes Bax-dependent neuronal apoptosis through mitochondrial oxidative damage. Proc Natl Acad Sci USA 2005; 102: 19126–31.
20 Ikebe S, Tanaka M, Ohno K, et al. Increase of deleted mitochondrial DNA in the striatum in Parkinson’s disease and senescence. Biochem Biophys Res Commun 1990; 170: 1044–48.
21 Schapira AH, Holt IJ, Sweeney M, et al. Mitochondrial DNA analysis in Parkinson’s disease. Mov Disord 1990; 5: 294–47.
22 Lestienne P, Nelson I, Riederer P, Reichmann H, Jellinger K. Mitochondrial DNA in postmortem brain from patients with Parkinson’s disease. J Neurochem 1991; 56: 1819.
23 Kraytsberg Y, Kudryavtseva E, McKee AC, et al. Mitochondrial DNA deletions are abundant and cause functional impairment in aged human substantia nigra neurons. Nat Genet 2006; 38: 518–20.
24 Bender A, Krishnan KJ, Morris CM, et al. High levels of mitochondrial DNA deletions in substantia nigra neurons in aging and Parkinson disease. Nat Genet 2006; 38: 515–17.
25 Ozawa T, Tanaka M, Ino H, et al. Distinct clustering of point mutations in mitochondrial DNA among patients with mitochondrial encephalomyopathies and with Parkinson’s disease. Biochem Biophys Res Commun 1991; 176: 938–46.
26 Ikebe S, Tanaka M, Ozawa T. Point mutations of mitochondrial genome in Parkinson’s disease. Brain Res Mol Brain Res 1995; 28: 281–95.
27 Shoff ner JM, Brown MD, Torroni A, et al. Mitochondrial DNA variants observed in Alzheimer disease and Parkinson disease patients. Genomics 1993; 17: 171–84.
28 Lucking CB, Kosel S, Mehraein P, Graeber MB. Absence of the mitochondrial A7237T mutation in Parkinson’s disease. Biochem Biophys Res Commun 1995; 211: 700–04.
29 Kosel S, Grasbon-Frodl EM, Hagenah JM, Graeber MB, Vieregge P. Parkinson disease: analysis of mitochondrial DNA in monozygotic twins. Neurogenetics 2000; 2: 227–30.
30 Richter G, Sonnenschein A, Grunewald T, Reichmann H, Janetzky B. Novel mitochondrial DNA mutations in Parkinson’s disease. J Neural Transm 2002; 109: 721–29.
31 Vives-Bauza C, Andreu AL, Manfredi G, et al. Sequence analysis of the entire mitochondrial genome in Parkinson’s disease. Biochem Biophys Res Commun 2002; 290: 1593–601.
32 van der Walt JM, Nicodemus KK, Martin ER, et al. Mitochondrial polymorphisms signifi cantly reduce the risk of Parkinson disease. Am J Hum Genet 2003; 72: 804–11.
33 Pyle A, Foltynie T, Tiangyou W, et al. Mitochondrial DNA haplogroup cluster UKJT reduces the risk of PD. Ann Neurol 2005; 57: 564–67.
34 Ross OA, McCormack R, Maxwell LD, et al. mt4216C variant in linkage with the mtDNA TJ cluster may confer a susceptibility to mitochondrial dysfunction resulting in an increased risk of Parkinson’s disease in the Irish. Exp Gerontol 2003; 38: 397–405.
35 Kazuno AA, Munakata K, Nagai T, et al. Identifi cation of mitochondrial DNA polymorphisms that alter mitochondrial matrix pH and intracellular calcium dynamics. PLoS Genet 2006; 2: e128.
36 Swerdlow RH, Parks JK, Miller SW, et al. Origin and functional consequences of the complex I defect in Parkinson’s disease. Ann Neurol 1996; 40: 663–71.
37 Gu M, Cooper JM, Taanman JW, Schapira AH. Mitochondrial DNA transmission of the mitochondrial defect in Parkinson’s disease. Ann Neurol 1998; 44: 177–86.
38 Thyagarajan D, Bressman S, Bruno C, et al. A novel mitochondrial 12SrRNA point mutation in parkinsonism, deafness, and neuropathy. Ann Neurol 2000; 48: 730–36.
39 Rana M, de C, I, Diaz F, Smeets H, Moraes CT. An out-of-frame cytochrome b gene deletion from a patient with parkinsonism is associated with impaired complex III assembly and an increase in free radical production. Ann Neurol 2000; 48: 774–81.
40 Parker WD, Jr, Parks JK. Mitochondrial ND5 mutations in idiopathic Parkinson’s disease. Biochem Biophys Res Commun 2005; 326: 667–69.
41 Ekstrand MI, Terzioglu M, Galter D, et al. Progressive parkinsonism in mice with respiratory-chain-defi cient dopamine neurons. Proc Natl Acad Sci USA 2007; 104: 1325–30.
42 Kubo SI, Kitami T, Noda S, et al. Parkin is associated with cellular vesicles. J Neurochem 2001; 78: 42–54.
43 Shimura H, Hattori N, Kubo S, et al. Immunohistochemical and subcellular localization of parkin protein: absence of protein in autosomal recessive juvenile parkinsonism patients. Ann Neurol 1999; 45: 668–72.
44 Stichel CC, Augustin M, Kuhn K, et al. Parkin expression in the adult mouse brain. Eur J Neurosci 2000; 12: 4181–94.
45 Shimura H, Hattori N, Kubo S, et al. Familial Parkinson disease gene product, parkin, is a ubiquitin-protein ligase. Nat Genet 2000; 25: 302–05.
46 Zhang Y, Gao J, Chung KK, et al. Parkin functions as an E2-dependent ubiquitin- protein ligase and promotes the degradation of the synaptic vesicle-associated protein, CDCrel-1. Proc Natl Acad Sci USA 2000; 97: 13354–59.
47 Imai Y, Soda M, Inoue H, et al. An unfolded putative transmembrane polypeptide, which can lead to endoplasmic reticulum stress, is a substrate of Parkin. Cell 2001; 105: 891–902.
48 Yamamoto A, Friedlein A, Imai Y, et al. Parkin phosphorylation and modulation of its E3 ubiquitin ligase activity. J Biol Chem 2005; 280: 3390–99.
49 Chung KK, Thomas B, Li X, et al. S-nitrosylation of parkin regulates ubiquitination and compromises parkin’s protective function. Science 2004; 304: 1328–31.
50 Kuroda Y, Mitsui T, Kunishige M, et al. Parkin enhances mitochondrial biogenesis in proliferating cells. Hum Mol Genet 2006; 15: 883–95.
51 Kitada T, Asakawa S, Hattori N, et al. Mutations in the parkin gene cause autosomal recessive juvenile parkinsonism. Nature 1998; 392: 605–08.
52 Lucking CB, Durr A, Bonifati V, et al. Association between early-onset Parkinson’s disease and mutations in the parkin gene. N Engl J Med 2000; 342: 1560–67.
53 Farrer M, Chan P, Chen R, et al. Lewy bodies and parkinsonism in families with parkin mutations. Ann Neurol 2001; 50: 293–300.
54 Lohmann E, Periquet M, Bonifati V, et al for the French Parkinson’s Disease Genetics Study Group; European Consortium on Genetic Susceptibility in Parkinson’s Disease. How much phenotypic variation can be attributed to parkin genotype? Ann Neurol 2003; 54: 176–85.
55 Pramstaller PP, Schlossmacher MG, Jacques TS, et al. Lewy body Parkinson’s disease in a large pedigree with 77 Parkin mutation carriers. Ann Neurol 2005; 58: 411–22.
56 Hayashi S, Wakabayashi K, Ishikawa A, et al. An autopsy case of autosomal-recessive juvenile parkinsonism with a homozygous exon 4 deletion in the parkin gene. Mov Disord 2000; 15: 884–88.

http://neurology.thelancet.com Vol 7 January 2008 107
Review
57 Goldberg MS, Fleming SM, Palacino JJ, et al. Parkin-defi cient mice exhibit nigrostriatal defi cits but not loss of dopaminergic neurons. J Biol Chem 2003; 278: 43628–35.
58 Palacino JJ, Sagi D, Goldberg MS, et al. Mitochondrial dysfunction and oxidative damage in parkin-defi cient mice. J Biol Chem 2004; 279: 18614–22.
59 Casarejos MJ, Menendez J, Solano RM, et al. Susceptibility to rotenone is increased in neurons from parkin null mice and is reduced by minocycline. J Neurochem 2006; 97: 934–46.
60 Greene JC, Whitworth AJ, Kuo I, et al. Mitochondrial pathology and apoptotic muscle degeneration in Drosophila parkin mutants. Proc Natl Acad Sci USA 2003; 100: 4078–83.
61 Muftuoglu M, Elibol B, Dalmizrak O, et al. Mitochondrial complex I and IV activities in leukocytes from patients with parkin mutations. Mov Disord 2004; 19: 544–48.
62 Silvestri L, Caputo V, Bellacchio E, et al. Mitochondrial import and enzymatic activity of PINK1 mutants associated to recessive parkinsonism. Hum Mol Genet 2005; 14: 3477–92.
63 Unoki M, Nakamura Y. Growth-suppressive eff ects of BPOZ and EGR2, two genes involved in the PTEN signaling pathway. Oncogene 2001; 20: 4457–65.
64 Nakajima A, Kataoka K, Hong M, Sakaguchi M, Huh NH. BRPK, a novel protein kinase showing increased expression in mouse cancer cell lines with higher metastatic potential. Cancer Lett 2003; 201: 195–201.
65 Abahuni N, Gispert S, Bauer P, et al. Mitochondrial translation initiation factor 3 gene polymorphism associated with Parkinson’s disease. Neurosci Lett 2007; 414: 126–9.
66 Valente EM, Abou-Sleiman PM, Caputo V, et al. Hereditary early-onset Parkinson’s disease caused by mutations in PINK1. Science 2004; 304: 1158–60.
67 Valente EM, Salvi S, Ialongo T, et al. PINK1 mutations are associated with sporadic early-onset parkinsonism. Ann Neurol 2004; 56: 336–41.
68 Hatano Y, Li Y, Sato K, et al. Novel PINK1 mutations in early-onset parkinsonism. Ann Neurol 2004; 56: 424–27.
69 Rohe CF, Montagna P, Breedveld G, et al. Homozygous PINK1 C-terminus mutation causing early-onset parkinsonism. Ann Neurol 2004; 56: 427–31.
70 Beilina A, Van Der BM, Ahmad R, et al. Mutations in PTEN-induced putative kinase 1 associated with recessive parkinsonism have diff erential eff ects on protein stability. Proc Natl Acad Sci USA 2005; 102: 5703–08.
71 Gandhi S, Muqit MM, Stanyer L, et al. PINK1 protein in normal human brain and Parkinson’s disease. Brain 2006; 129: 1720–31.
72 Muqit MM, Abou-Sleiman PM, Saurin AT, et al. Altered cleavage and localization of PINK1 to aggresomes in the presence of proteasomal stress. J Neurochem 2006; 98: 156–69.
73 Healy DG, Abou-Sleiman PM, Ahmadi KR, et al. The gene responsible for PARK6 Parkinson’s disease, PINK1, does not infl uence common forms of parkinsonism. Ann Neurol 2004; 56: 329–35.
74 Groen JL, Kawarai T, Toulina A, et al. Genetic association study of PINK1 coding polymorphisms in Parkinson’s disease. Neurosci Lett 2004; 372: 226–29.
75 Hedrich K, Hagenah J, Djarmati A, et al. Clinical spectrum of homozygous and heterozygous PINK1 mutations in a large German family with Parkinson disease: role of a single hit? Arch Neurol 2006; 63: 833–38.
76 Bonifati V, Rohe CF, Breedveld GJ, et al. Early-onset parkinsonism associated with PINK1 mutations: frequency, genotypes, and phenotypes. Neurology 2005; 65: 87–95.
77 Rogaeva E, Johnson J, Lang AE, et al. Analysis of the PINK1 gene in a large cohort of cases with Parkinson disease. Arch Neurol 2004; 61: 1898–904.
78 Grunewald A, Breedveld GJ, Lohmann-Hedrich K, et al. Biological eff ects of the PINK1 c.1366C>T mutation: implications in Parkinson disease pathogenesis. Neurogenetics 2007; 8: 103–09.
79 Tan EK, Yew K, Chua E, et al. PINK1 mutations in sporadic early-onset Parkinson’s disease. Mov Disord 2006; 21: 789–93.
80 Abou-Sleiman PM, Muqit MM, McDonald NQ, et al. A heterozygous eff ect for PINK1 mutations in Parkinson’s disease? Ann Neurol 2006; 60: 414–19.
81 Khan NL, Valente EM, Bentivoglio AR, et al. Clinical and subclinical dopaminergic dysfunction in PARK6-linked parkinsonism: an 18F-dopa PET study. Ann Neurol 2002; 52: 849–53.
82 Park J, Lee SB, Lee S, et al. Mitochondrial dysfunction in Drosophila PINK1 mutants is complemented by parkin. Nature 2006; 441: 1157–61.
83 Clark IE, Dodson MW, Jiang C, et al. Drosophila pink1 is required for mitochondrial function and interacts genetically with parkin. Nature 2006; 441: 1162–66.
84 Zhang L, Shimoji M, Thomas B, et al. Mitochondrial localization of the Parkinson’s disease related protein DJ-1: implications for pathogenesis. Hum Mol Genet 2005; 14: 2063–73.
85 Nagakubo D, Taira T, Kitaura H, et al. DJ-1, a novel oncogene which transforms mouse NIH3T3 cells in cooperation with ras. Biochem Biophys Res Commun 1997; 231: 509–13.
86 Takahashi K, Taira T, Niki T, et al. DJ-1 positively regulates the androgen receptor by impairing the binding of PIASx alpha to the receptor. J Biol Chem 2001; 276: 37556–63.
87 Taira T, Saito Y, Niki T, et al. DJ-1 has a role in antioxidative stress to prevent cell death. EMBO Rep 2004; 5: 213–18.
88 Canet-Aviles RM, Wilson MA, Miller DW, et al. The Parkinson’s disease protein DJ-1 is neuroprotective due to cysteine–sulfi nic acid-driven mitochondrial localization. Proc Natl Acad Sci USA 2004; 101: 9103–08.
89 Bandopadhyay R, Kingsbury AE, Cookson MR, et al. The expression of DJ-1 (PARK7) in normal human CNS and idiopathic Parkinson’s disease. Brain 2004; 127: 420–30.
90 Yokota T, Sugawara K, Ito K, et al. Down regulation of DJ-1 enhances cell death by oxidative stress, ER stress, and proteasome inhibition. Biochem Biophys Res Commun 2003; 312: 1342–48.
91 Bonifati V, Rizzu P, van Baren MJ, et al. Mutations in the DJ-1 gene associated with autosomal recessive early-onset parkinsonism. Science 2003; 299: 256–59.
92 Xu J, Zhong N, Wang H, et al. The Parkinson’s disease-associated DJ-1 protein is a transcriptional co-activator that protects against neuronal apoptosis. Hum Mol Genet 2005; 14: 1231–41.
93 Shendelman S, Jonason A, Martinat C, Leete T, Abeliovich A. DJ-1 is a redox-dependent molecular chaperone that inhibits alpha-synuclein aggregate formation. PLoS Biol 2004; 2: e362.
94 Tang B, Xiong H, Sun P, et al. Association of PINK1 and DJ-1 confers digenic inheritance of early-onset Parkinson’s disease. Hum Mol Genet 2006; 15: 1816–25.
95 Goldberg MS, Pisani A, Haburcak M, et al. Nigrostriatal dopaminergic defi cits and hypokinesia caused by inactivation of the familial Parkinsonism-linked gene DJ-1. Neuron 2005; 45: 489–96.
96 Pisani A, Martella G, Tscherter A, et al. Enhanced sensitivity of DJ-1-defi cient dopaminergic neurons to energy metabolism impairment: role of Na+/K+ ATPase. Neurobiol Dis 2006; 23: 54–60.
97 Kim RH, Smith PD, Aleyasin H, et al. Hypersensitivity of DJ-1-defi cient mice to 1-methyl-4-phenyl-1,2,3,6- tetrahydropyrindine (MPTP) and oxidative stress. Proc Natl Acad Sci USA 2005; 102: 5215–20.
98 Filosto M, Mancuso M, Nishigaki Y, et al. Clinical and genetic heterogeneity in progressive external ophthalmoplegia due to mutations in polymerase gamma. Arch Neurol 2003; 60: 1279–84.
99 Schapira AH. Mitochondrial disease. Lancet 2006; 368: 70–82.100 Luoma P, Melberg A, Rinne JO, et al. Parkinsonism, premature
menopause, and mitochondrial DNA polymerase gamma mutations: clinical and molecular genetic study. Lancet 2004; 364: 875–82.
101 Davidzon G, Greene P, Mancuso M, et al. Early-onset familial parkinsonism due to POLG mutations. Ann Neurol 2006; 59: 859–62.
102 Mancuso M, Filosto M, Oh SJ, DiMauro S. A novel polymerase gamma mutation in a family with ophthalmoplegia, neuropathy, and Parkinsonism. Arch Neurol 2004; 61: 1777–79.
103 Taanman JW, Schapira AH. Analysis of the trinucleotide CAG repeat from the DNA polymerase gamma gene (POLG) in patients with Parkinson’s disease. Neurosci Lett 2005; 376: 56–59.
104 Hudson G, Schaefer AM, Taylor RW, et al. Mutation of the linker region of the polymerase gamma-1 (POLG1) gene associated with progressive external ophthalmoplegia and Parkinsonism. Arch Neurol 2007; 64: 553–57.

108 http://neurology.thelancet.com Vol 7 January 2008
Review
105 Martins LM, Morrison A, Klupsch K, et al. Neuroprotective role of the Reaper-related serine protease HtrA2/Omi revealed by targeted deletion in mice. Mol Cell Biol 2004; 24: 9848–62.
106 Strauss KM, Martins LM, Plun-Favreau H, et al. Loss of function mutations in the gene encoding Omi/HtrA2 in Parkinson’s disease. Hum Mol Genet 2005; 14: 2099–111.
107 Plun-Favreau H, Klupsch K, Moisoi N, et al. The mitochondrial protease HtrA2 is regulated by Parkinson’s disease-associated kinase PINK1. Nat Cell Biol 2007; 9: 1243–52.
108 Chen L, Feany MB. Alpha-synuclein phosphorylation controls neurotoxicity and inclusion formation in a Drosophila model of Parkinson disease. Nat Neurosci 2005; 8: 657–63.
109 Hsu LJ, Sagara Y, Arroyo A, et al. Alpha-synuclein promotes mitochondrial defi cit and oxidative stress. Am J Pathol 2000; 157: 401–10.
110 Tabrizi SJ, Orth M, Wilkinson JM, et al. Expression of mutant alpha-synuclein causes increased susceptibility to dopamine toxicity. Hum Mol Genet 2000; 9: 2683–89.
111 Abeliovich A, Schmitz Y, Farinas I, et al. Mice lacking alpha-synuclein display functional defi cits in the nigrostriatal dopamine system. Neuron 2000; 25: 239–52.
112 Orth M, Tabrizi SJ, Tomlinson C, et al. G209A mutant alpha synuclein expression specifi cally enhances dopamine induced oxidative damage. Neurochem Int 2004; 45: 669–76.
113 Lee MK, Stirling W, Xu Y, et al. Human alpha-synuclein-harboring familial Parkinson’s disease-linked Ala-53→Thr mutation causes neurodegenerative disease with alpha-synuclein aggregation in transgenic mice. Proc Natl Acad Sci USA 2002; 99: 8968–73.
114 Martin LJ, Pan Y, Price AC, et al. Parkinson’s disease alpha-synuclein transgenic mice develop neuronal mitochondrial degeneration and cell death. J Neurosci 2006; 26: 41–50.
115 Klivenyi P, Siwek D, Gardian G, et al. Mice lacking alpha-synuclein are resistant to mitochondrial toxins. Neurobiol Dis 2006; 21: 541–48.
116 Dauer W, Kholodilov N, Vila M, et al. Resistance of alpha-synuclein null mice to the parkinsonian neurotoxin MPTP. Proc Natl Acad Sci USA 2002; 99: 14524–29.
117 Norris EH, Uryu K, Leight S, et al. Pesticide exposure exacerbates alpha-synucleinopathy in an A53T transgenic mouse model. Am J Pathol 2007; 170: 658–66.
118 Farrer M, Stone J, Mata IF, et al. LRRK2 mutations in Parkinson disease. Neurology 2005; 65: 738–40.
119 Gilks WP, Abou-Sleiman PM, Gandhi S, et al. A common LRRK2 mutation in idiopathic Parkinson’s disease. Lancet 2005; 365: 415–16.
120 Zabetian CP, Samii A, Mosley AD, et al. A clinic-based study of the LRRK2 gene in Parkinson disease yields new mutations. Neurology 2005; 65: 741–44.
121 Deng H, Le W, Guo Y, et al. Genetic and clinical identifi cation of Parkinson’s disease patients with LRRK2 G2019S mutation. Ann Neurol 2005; 57: 933–34.
122 Di Fonzo A, Rohe CF, Ferreira J, et al. A frequent LRRK2 gene mutation associated with autosomal dominant Parkinson’s disease. Lancet 2005; 365: 412–15.
123 Kachergus J, Mata IF, Hulihan M, et al. Identifi cation of a novel LRRK2 mutation linked to autosomal dominant parkinsonism: evidence of a common founder across European populations. Am J Hum Genet 2005; 76: 672–80.
124 Hernandez D, Paisan RC, Crawley A, et al. The dardarin G 2019 S mutation is a common cause of Parkinson’s disease but not other neurodegenerative diseases. Neurosci Lett 2005; 389: 137–39.
125 Nichols WC, Pankratz N, Hernandez D, et al. Genetic screening for a single common LRRK2 mutation in familial Parkinson’s disease. Lancet 2005; 365: 410–12.
126 Aasly JO, Toft M, Fernandez-Mata I, et al. Clinical features of LRRK2-associated Parkinson’s disease in central Norway. Ann Neurol 2005; 57: 762–65.
127 Di Fonzo A, Tassorelli C, De Mari M, et al. Comprehensive analysis of the LRRK2 gene in sixty families with Parkinson’s disease. Eur J Hum Genet 2006; 14: 322–31.
128 Giasson BI, Covy JP, Bonini NM, et al. Biochemical and pathological characterization of Lrrk2. Ann Neurol 2006; 59: 315–22.
129 Gloeckner CJ, Kinkl N, Schumacher A, et al. The Parkinson disease causing LRRK2 mutation I2020T is associated with increased kinase activity. Hum Mol Genet 2006; 15: 223–32.
130 Smith WW, Pei Z, Jiang H, et al. Leucine-rich repeat kinase 2 (LRRK2) interacts with parkin, and mutant LRRK2 induces neuronal degeneration. Proc Natl Acad Sci USA 2005; 102: 18676–81.
131 West AB, Moore DJ, Biskup S, et al. Parkinson’s disease-associated mutations in leucine-rich repeat kinase 2 augment kinase activity. Proc Natl Acad Sci USA 2005; 102: 1684247.
132 Schapira AH. The importance of LRRK2 mutations in Parkinson disease. Arch Neurol 2006; 63: 1225–28.
133 Singer TP, Salach JI, Castagnoli N Jr, Trevor A. Interactions of the neurotoxic amine 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine with monoamine oxidases. Biochem J 1986; 235: 785–89.
134 Hantraye P, Brouillet E, Ferrante R, et al. Inhibition of neuronal nitric oxide synthase prevents MPTP-induced parkinsonism in baboons. Nature Med 1996; 2: 1017–21.
135 Betarbet R, Sherer TB, MacKenzie G, et al. Chronic systemic pesticide exposure reproduces features of Parkinson’s disease. Nat Neurosci 2000; 3: 1301–06.
136 Hoglinger GU, Feger J, Prigent A, et al. Chronic systemic complex I inhibition induces a hypokinetic multisystem degeneration in rats. J Neurochem 2003; 84: 491–502.
137 Betarbet R, Canet-Aviles RM, Sherer TB, et al. Intersecting pathways to neurodegeneration in Parkinson’s disease: eff ects of the pesticide rotenone on DJ-1, alpha-synuclein, and the ubiquitin-proteasome system. Neurobiol Dis 2006; 22: 404–20.
138 Sherer TB, Betarbet R, Stout AK, et al. An in vitro model of Parkinson’s disease: linking mitochondrial impairment to altered alpha-synuclein metabolism and oxidative damage. J Neurosci 2002; 22: 7006–15.
139 Wang XF, Li S, Chou AP, Bronstein JM. Inhibitory eff ects of pesticides on proteasome activity: implication in Parkinson’s disease. Neurobiol Dis 2006; 23: 198–205.
140 Seaton TA, Cooper JM, Schapira AH. Cyclosporin inhibition of apoptosis induced by mitochondrial complex I toxin. Brain Res 1998; 809: 12–17.
141 Champy P, Hoglinger GU, Feger J, et al. Annonacin, a lipophilic inhibitor of mitochondrial complex I, induces nigral and striatal neurodegeneration in rats: possible relevance for atypical parkinsonism in Guadeloupe. J Neurochem 2004; 88: 63–69.
142 Smith PR, Cooper JM, Govan GG, Harding AE, Schapira AH. Smoking and mitochondrial function: a model for environmental toxins. Q J Med 1993; 86: 657–60.
143 Jenner P. Oxidative stress in Parkinson’s disease. Ann Neurol 2003; 53 (suppl 3): S26–S36.
144 Thomas PK, Cooper JM, King RH, et al. Myopathy in vitamin E defi cient rats: muscle fi bre necrosis associated with disturbances of mitochondrial function. J Anat 1993; 183: 451–61.
145 Schapira AH. Oxidative stress in Parkinson’s disease. Neuropathol Appl Neurobiol 1995; 21: 3–9.
146 Chan CS, Guzman JN, Ilijic E, et al. ‘Rejuvenation’ protects neurons in mouse models of Parkinson’s disease. Nature 2007; 447: 1081–86.
147 McNaught KS, Belizaire R, Isacson O, Jenner P, Olanow CW. Altered proteasomal function in sporadic Parkinson’s disease. Exp Neurol 2003; 179: 38–46.
148 McNaught KS, Perl DP, Brownell AL, Olanow CW. Systemic exposure to proteasome inhibitors causes a progressive model of Parkinson’s disease. Ann Neurol 2004; 56: 149–62.
149 Schapira AH, Cleeter MW, Muddle JR, et al. Proteasomal inhibition causes loss of nigral tyrosine hydroxylase neurons. Ann Neurol 2006; 60: 253–55.
150 Zeng BY, Bukhatwa S, Hikima A, Rose S, Jenner P. Reproducible nigral cell loss after systemic proteasomal inhibitor administration to rats. Ann Neurol 2006; 60: 248–52.
151 Manning-Bog AB, Reaney SH, Chou VP, et al. Lack of nigrostriatal pathology in a rat model of proteasome inhibition. Ann Neurol 2006; 60: 256–60.
152 Bove J, Zhou C, Jackson-Lewis V, et al. Proteasome inhibition and Parkinson’s disease modeling. Ann Neurol 2006; 60: 260–64.
153 Voges D, Zwickl P, Baumeister W. The 26S proteasome: a molecular machine designed for controlled proteolysis. Annu Rev Biochem 1999; 68: 1015–68.
154 Hoglinger GU, Carrard G, Michel PP, et al. Dysfunction of mitochondrial complex I and the proteasome: interactions between two biochemical defi cits in a cellular model of Parkinson’s disease. J Neurochem 2003; 86: 1297–307.

http://neurology.thelancet.com Vol 7 January 2008 109
Review
155 Shults CW, Oakes D, Kieburtz K, et al. Eff ects of coenzyme Q10 in early Parkinson disease: evidence of slowing of the functional decline. Arch Neurol 2002; 59: 1541–50.
156 The NINDS NET-PD Investigators. A randomized clinical trial of coenzyme Q10 and GPI-1485 in early Parkinson disease. Neurology 2007; 68: 20–28.
157 Muller T, Buttner T, Gholipour AF, Kuhn W. Coenzyme Q10 supplementation provides mild symptomatic benefi t in patients with Parkinson’s disease. Neurosci Lett 2003; 341: 201–04.
158 Storch A, Jost WH, Vieregge P, et al. Randomized, double-blind, placebo-controlled trial on symptomatic eff ects of coenzyme Q10 in Parkinson’s disease. Arch Neurol 2007; 64: 938–44.
159 Matthews RT, Ferrante RJ, Klivenyi P, et al. Creatine and cyclocreatine attenuate MPTP neurotoxicity. Exp Neurol 1999; 157: 142–49.
160 The NINDS NET-PD Investigators. A randomized, double-blind, futility clinical trial of creatine and minocycline in early Parkinson disease. Neurology 2006; 66: 664–71.
161 Bender A, Koch W, Elstner M, et al. Creatine supplementation in Parkinson disease: a placebo-controlled randomized pilot trial. Neurology 2006; 67: 1262–64.
162 Olanow CW, Schapira AH, LeWitt PA, et al. TCH346 as a neuroprotective drug in Parkinson’s disease: a double-blind, randomised, controlled trial. Lancet Neurol 2006; 5: 1013–20.
163 Schapira AH, Bezard E, Brotchie J, et al. Novel pharmacological targets for the treatment of Parkinson’s disease. Nat Rev Drug Discov 2006; 5: 845–54.
164 Schapira AH. Treatment options in the modern management of Parkinson disease. Arch Neurol 2007 ; 64: 108:3-8.