Embed Size (px)
Citation preview
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
Daniel H Ward DDS
Less is More ‐ Incorporating Minimally Invasive and Bioactive Materials into Your Practice 2020
3
•Emergency Treatment Only
•Limited aerosols
•No anesthetic
•Fear of the Unknown
Dental First Aid Kit
•Fuji IX
Dental First Aid Kit
•Fuji IX
•Fuji Automix LC
Dental First Aid Kit
•Fuji IX
•Fuji Automix LC
•G-aenial Universal Injectable
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
Re‐open for Business
New Protocols●Pre-appointment Questionnaire ●In-Car Check-in●Temperature Check●Closed Reception Area● Fewer In-Office Patients ●Pre-Procedure Rinse●Extended Disinfection●Plexiglass Front Desk Shields●PPE
Impact on Patient & Doctor Finances
Pent‐Up Demand for Aesthetic Treatment
Goal is to Share New Products & Techniques
for Superior Care
Products for a Post‐Covid World30 Products for a Post‐Covid World
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
Technology
•Laser Fluorescence Caries Detection
•Diagnodent
•655 nm laser
•Decay fluoresces
•Numeric display & audible sound
•>30 decay
•Great for patient education & confirmation
MID Diagnostics
Diagnodent
•Stained Grooves •Place tip in occlusal pits
Diagnodent
•Lite Touch Erbium YAG Laser
Hard Tissue Laser
•Tooth Preparation
Hard Tissue Laser
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
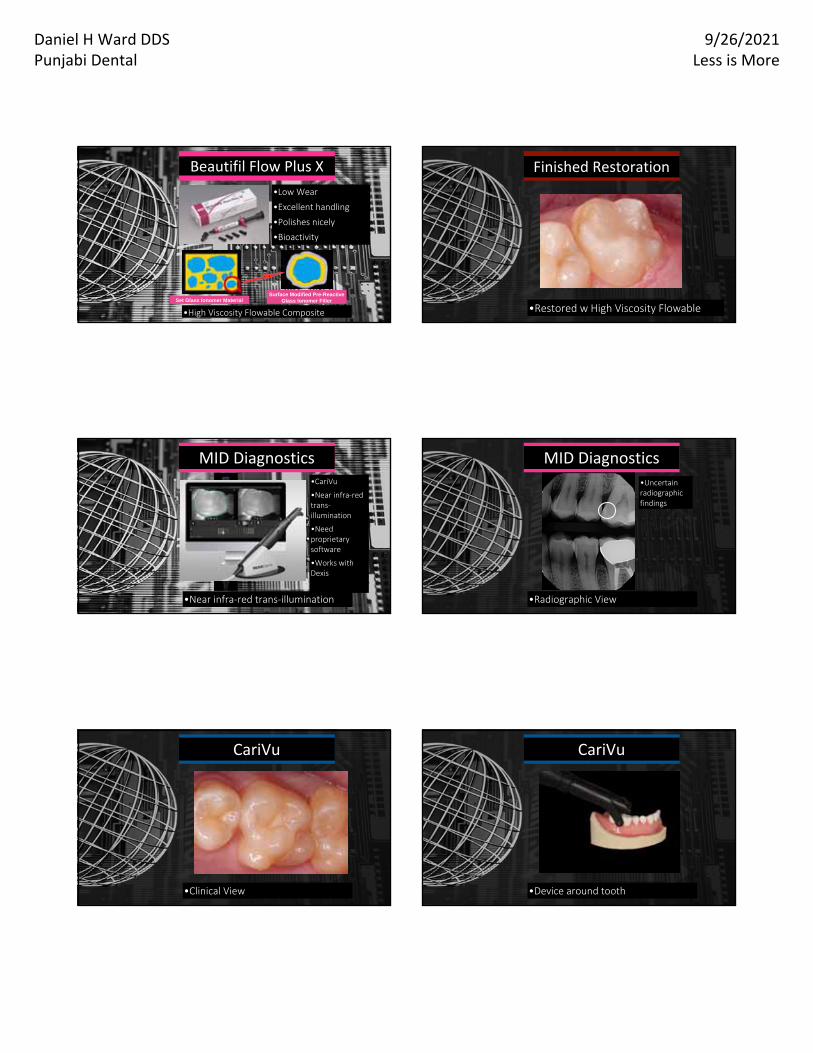
•High Viscosity Flowable Composite
•Low Wear
•Excellent handling
•Polishes nicely
•Bioactivity
Beautifil Flow Plus X
Set Glass Ionomer MaterialSurface Modified Pre-Reactive
Glass Ionomer Filler
•Restored w High Viscosity Flowable
Finished Restoration
•Near infra‐red trans‐illumination
•CariVu
•Near infra‐red trans‐illumination
•Need proprietary software
•Works with Dexis
MID Diagnostics
•Radiographic View
•Uncertain radiographic findings
MID Diagnostics
•Clinical View
CariVu
•Device around tooth
CariVu
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
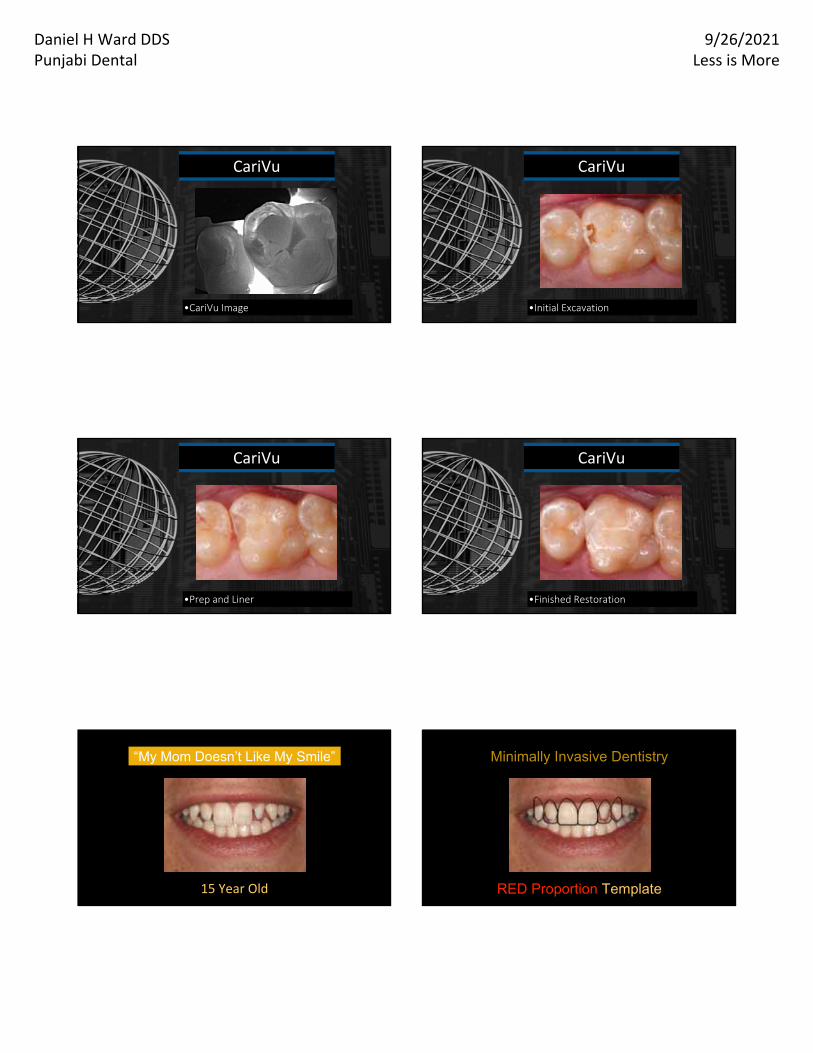
•CariVu Image
CariVu
•Initial Excavation
CariVu
•Prep and Liner
CariVu
•Finished Restoration
CariVu
15 Year Old
“My Mom Doesn’t Like My Smile”
RED Proportion Template
Minimally Invasive Dentistry
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
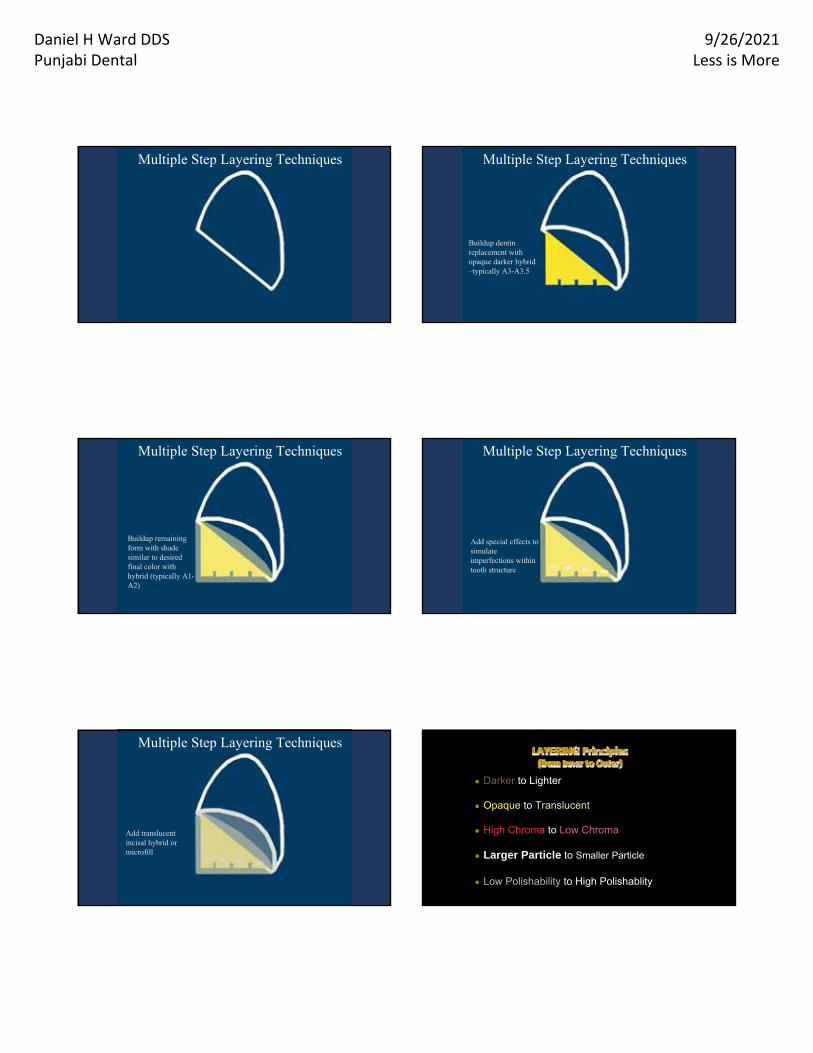
Multiple Step Layering Techniques
Buildup dentin replacement with opaque darker hybrid –typically A3-A3.5
Multiple Step Layering Techniques
Buildup dentin replacement with opaque darker hybrid –typically A3-A3.5
Multiple Step Layering Techniques
Buildup remaining form with shade similar to desired final color with hybrid (typically A1-A2)
Buildup dentin replacement with opaque darker hybrid –typically A3-A3.5
Buildup remaining form with shade similar to desired final color with hybrid (typically A1-A2)
Add special effects to simulate imperfections within tooth structure
Multiple Step Layering Techniques
Buildup dentin replacement with opaque darker hybrid –typically A3-A3.5
Buildup remaining form with shade similar to desired final color with hybrid (typically A1-A2)
Add special effects to simulate imperfections within tooth structure
Add translucent incisal hybrid or microfill
Multiple Step Layering Techniques
● Darker to Lighter
● Opaque to Translucent
● High Chroma to Low Chroma
● Larger Particle to Smaller Particle
● Low Polishability to High Polishablity
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
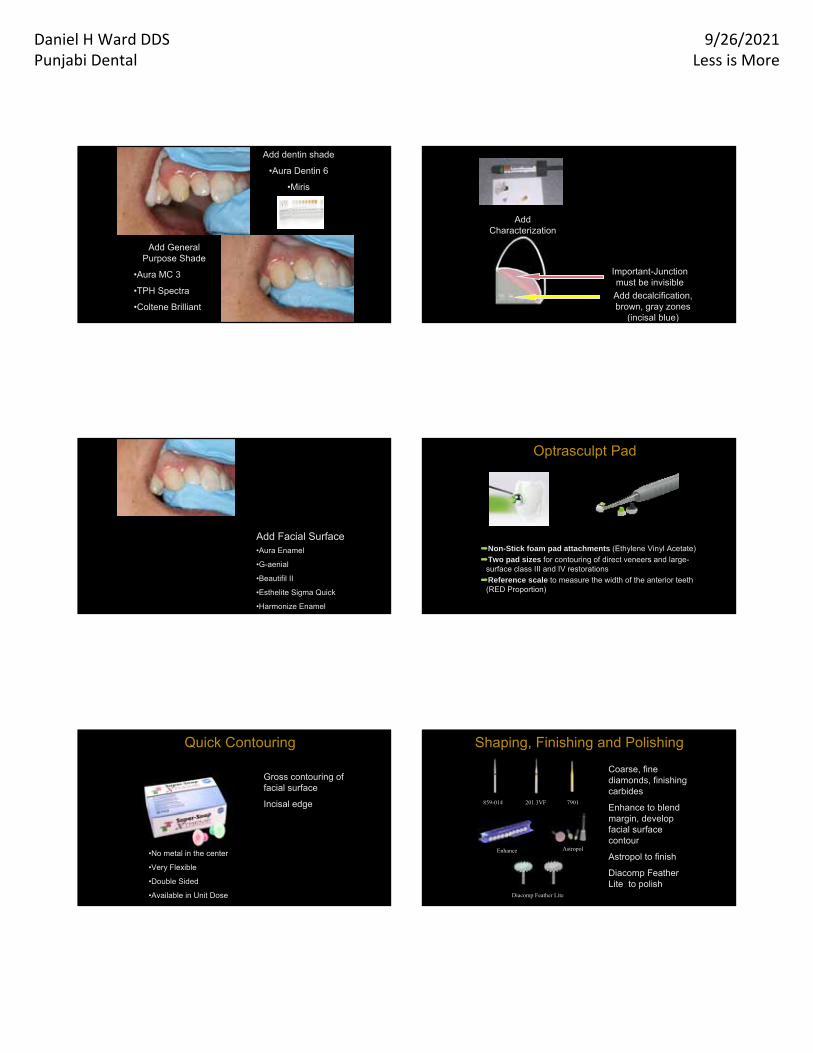
Add dentin shade
•Aura Dentin 6
•Miris
Add General Purpose Shade
•Aura MC 3
•TPH Spectra
•Coltene Brilliant
Add Characterization
Important-Junction must be invisible
Add decalcification, brown, gray zones
(incisal blue)
Add Facial Surface•Aura Enamel
•G-aenial
•Beautifil II
•Esthelite Sigma Quick
•Harmonize Enamel
Optrasculpt Pad
➡Non-Stick foam pad attachments (Ethylene Vinyl Acetate)
➡Two pad sizes for contouring of direct veneers and large-surface class III and IV restorations
➡Reference scale to measure the width of the anterior teeth (RED Proportion)
Gross contouring of facial surface
Incisal edge
Quick Contouring
•No metal in the center
•Very Flexible
•Double Sided
•Available in Unit Dose
859-014
Coarse, fine diamonds, finishing carbides
Enhance to blend margin, develop facial surface contour
Astropol to finish
Diacomp Feather Lite to polish
Astropol
Shaping, Finishing and Polishing
Enhance
7901
Diacomp Feather Lite
201.3VF
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
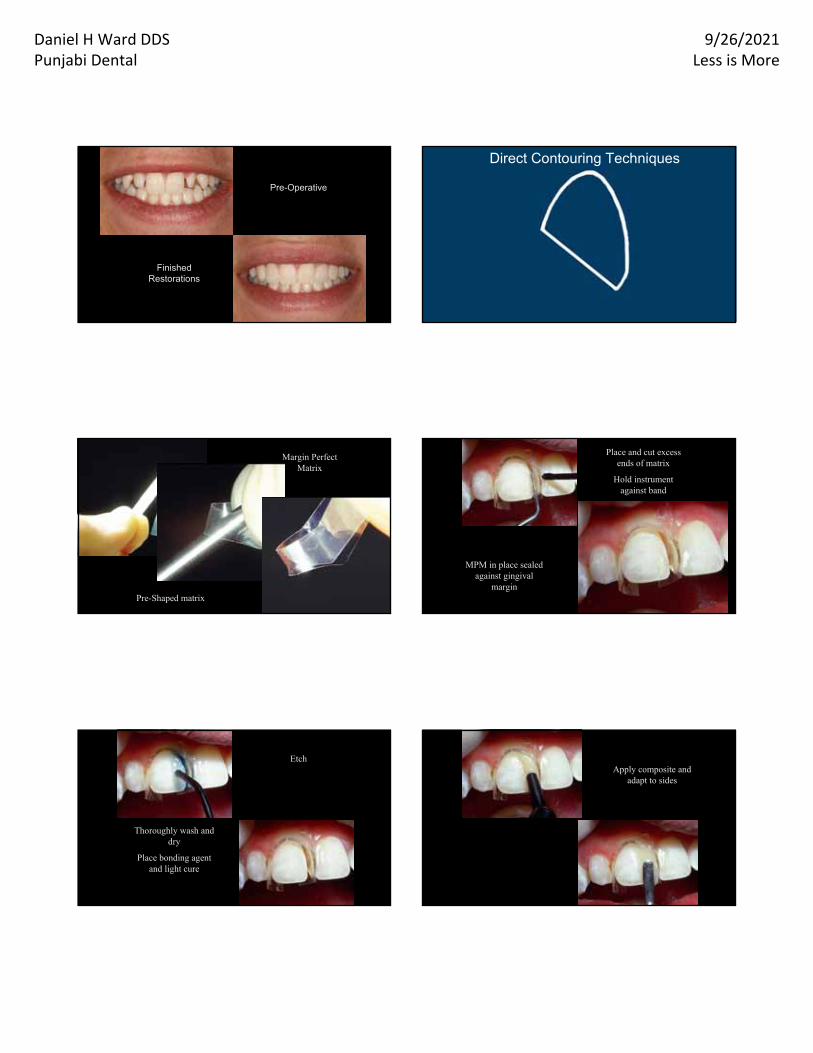
Pre-Operative
Finished Restorations
Direct Contouring Techniques
Technique by Dr Paul Belevedere
and Dr. Doug Lambert
Mold Margin Perfect Matrix
Margin Perfect Matrix
Pre-Shaped matrix
Place and cut excess ends of matrix
Hold instrument against band
Use Heliobond to adhere to gingiva
MPM in place sealed against gingival
margin
Etch
Thoroughly wash and dry
Place bonding agent and light cure
Apply composite and adapt to sides
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
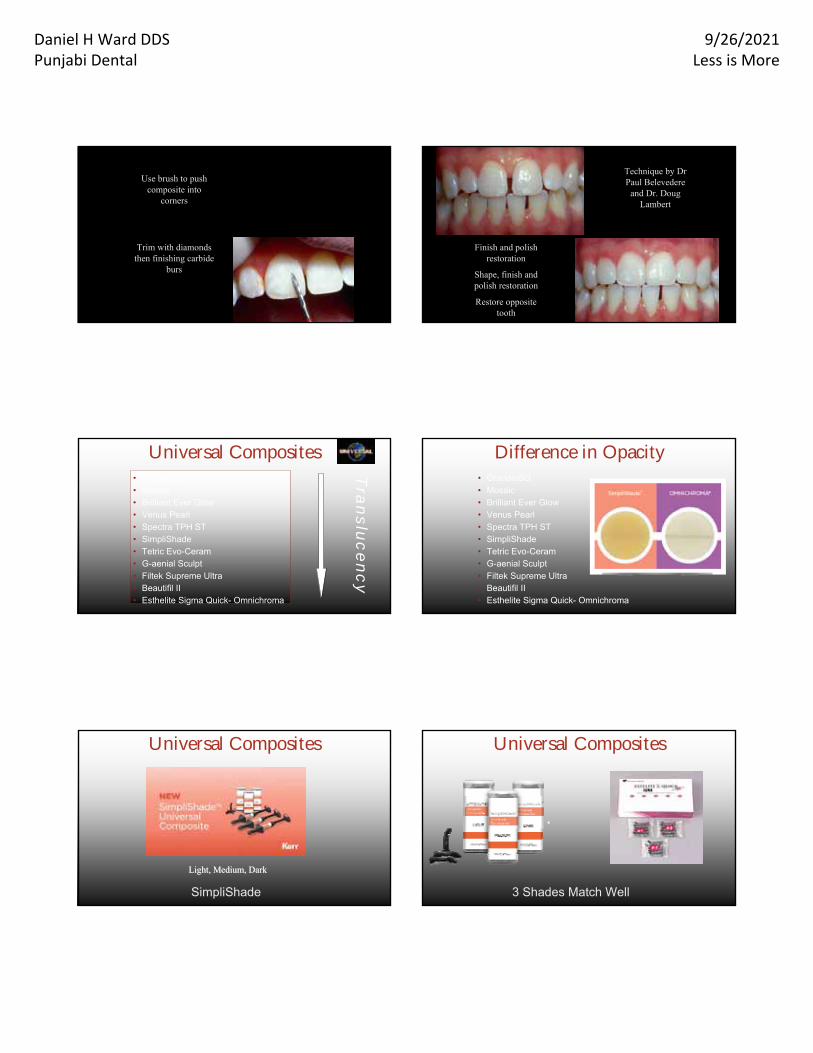
Trim with diamonds then finishing carbide
burs
Use brush to push composite into
corners
Finish and polish restoration
Shape, finish and polish restoration
Restore opposite tooth
Technique by Dr Paul Belevedere
and Dr. Doug Lambert
• GrandioSO• Mosaic• Brilliant Ever Glow• Venus Pearl• Spectra TPH ST• SimpliShade• Tetric Evo-Ceram• G-aenial Sculpt• Filtek Supreme Ultra• Beautifil II• Esthelite Sigma Quick- Omnichroma
Universal CompositesT
ranslu
cency
Difference in Opacity• GrandioSO• Mosaic• Brilliant Ever Glow• Venus Pearl• Spectra TPH ST• SimpliShade• Tetric Evo-Ceram• G-aenial Sculpt• Filtek Supreme Ultra• Beautifil II• Esthelite Sigma Quick- Omnichroma
SimpliShade
Universal Composites
Light, Medium, DarkLight, Medium, Dark
3 Shades Match Well
Universal Composites
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
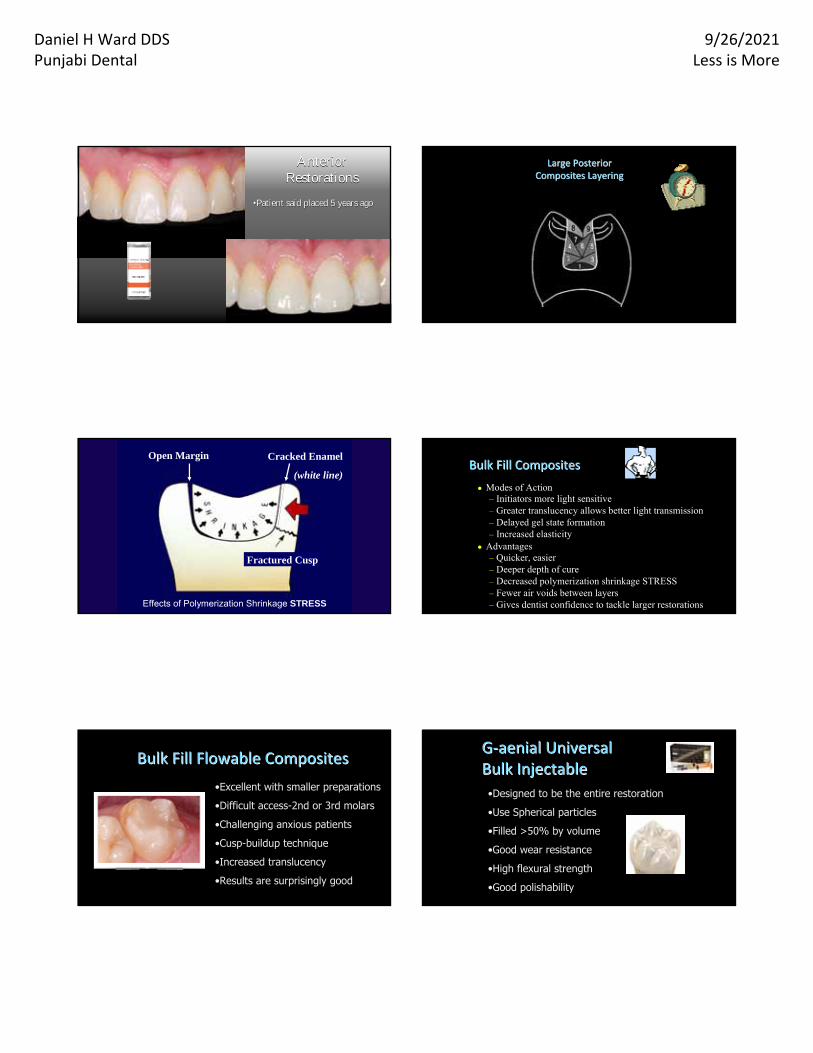
Anterior Restorations
Anterior Restorations
••Patient said placed 5 years ago Patient said placed 5 years ago
Large Posterior Large Posterior Composites LayeringComposites Layering
Open Margin Cracked Enamel
(white line)
Effects of Polymerization Shrinkage STRESS
Fractured Cusp
Bulk Fill CompositesBulk Fill Composites
● Modes of Action– Initiators more light sensitive– Greater translucency allows better light transmission– Delayed gel state formation– Increased elasticity
● Advantages– Quicker, easier– Deeper depth of cure– Decreased polymerization shrinkage STRESS– Fewer air voids between layers– Gives dentist confidence to tackle larger restorations
•Excellent with smaller preparations
•Difficult access-2nd or 3rd molars
•Challenging anxious patients
•Cusp-buildup technique
•Increased translucency
•Results are surprisingly good
Bulk Fill Flowable CompositesBulk Fill Flowable Composites
•Designed to be the entire restoration
•Use Spherical particles
•Filled >50% by volume
•Good wear resistance
•High flexural strength
•Good polishability
GG‐‐aenial Universalaenial UniversalBulk InjectableBulk Injectable
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
•Designed to be the entire restoration
•Use Spherical particles
•Filled >50% by volume
•Good wear resistance
•High flexural strength
•Good polishability
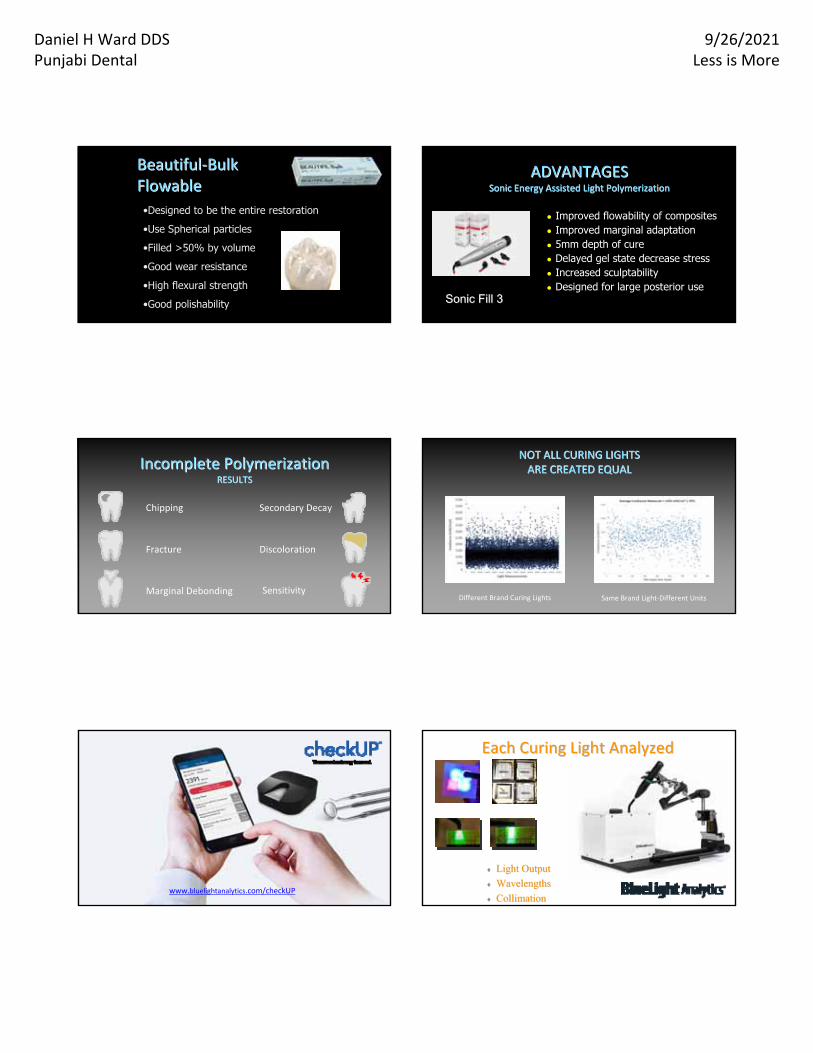
BeautifulBeautiful‐‐Bulk Bulk FlowableFlowable
● Improved flowability of composites● Improved marginal adaptation● 5mm depth of cure● Delayed gel state decrease stress● Increased sculptability● Designed for large posterior use
ADVANTAGESADVANTAGESSonic Energy Assisted Light PolymerizationSonic Energy Assisted Light Polymerization
Sonic Fill 3Sonic Fill 3
Chipping
Fracture Discoloration
Marginal Debonding Sensitivity
Secondary Decay
Incomplete PolymerizationIncomplete PolymerizationRESULTSRESULTS
Same Brand Light‐Different Units
NOT ALL CURING LIGHTS NOT ALL CURING LIGHTS ARE CREATED EQUALARE CREATED EQUAL
Different Brand Curing Lights
www.bluelightanalytics.com/checkUP
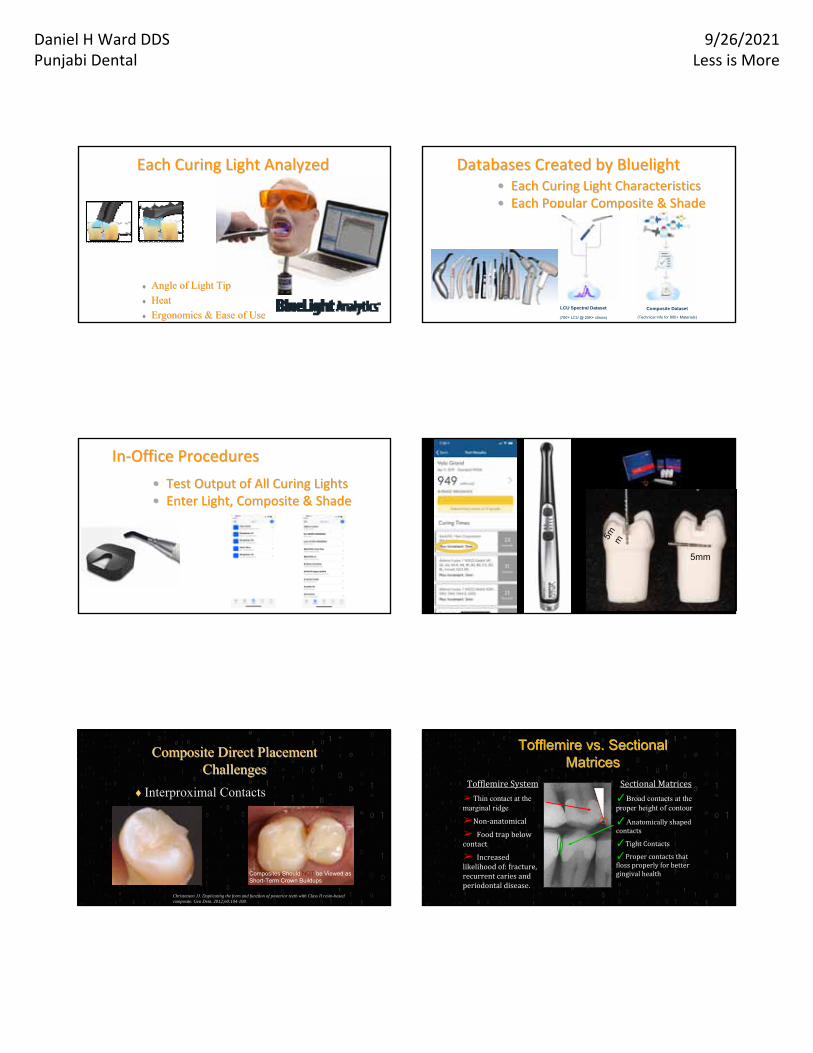
Each Curing Light AnalyzedEach Curing Light Analyzed
Light OutputLight Output
WavelengthsWavelengths
CollimationCollimation
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
Each Curing Light AnalyzedEach Curing Light Analyzed
Angle of Light TipAngle of Light Tip
HeatHeat
Ergonomics & Ease of UseErgonomics & Ease of Use
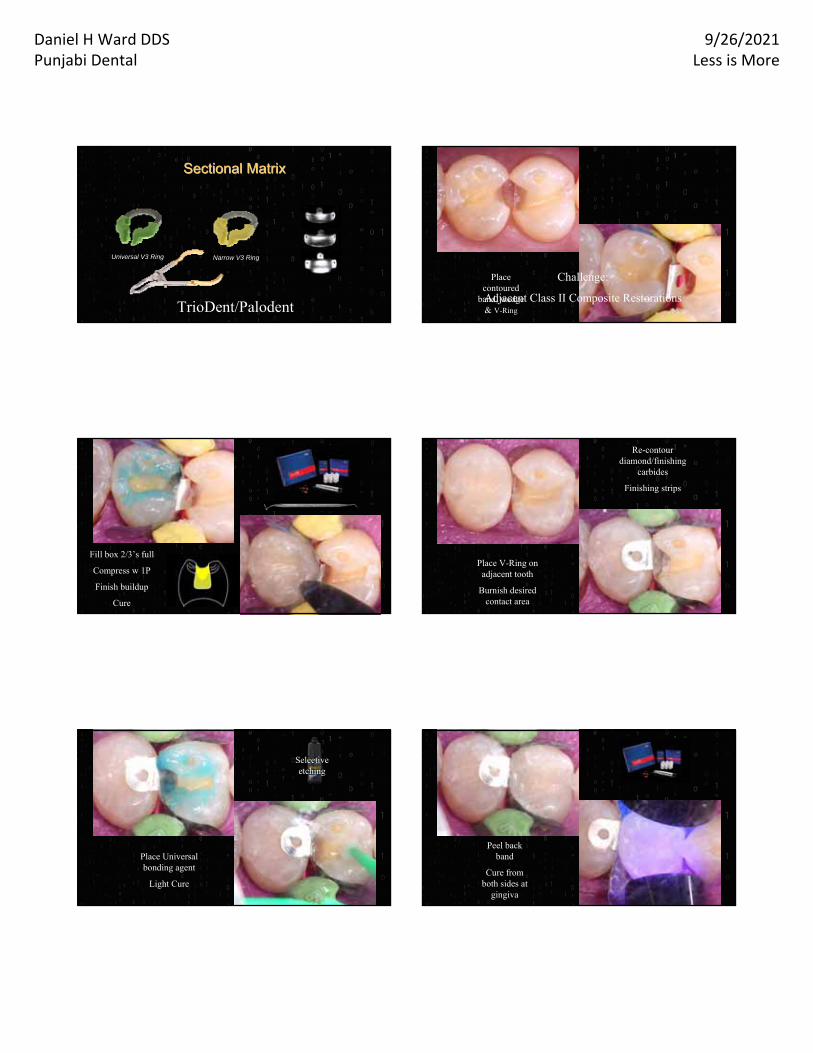
Databases Created by BluelightDatabases Created by Bluelight•• Each Curing Light CharacteristicsEach Curing Light Characteristics•• Each Popular Composite & ShadeEach Popular Composite & Shade
Composite Dataset
(Technical Info for 800+ Materials)
LCU Spectral Dataset
(700+ LCU @ 25K+ clinics)
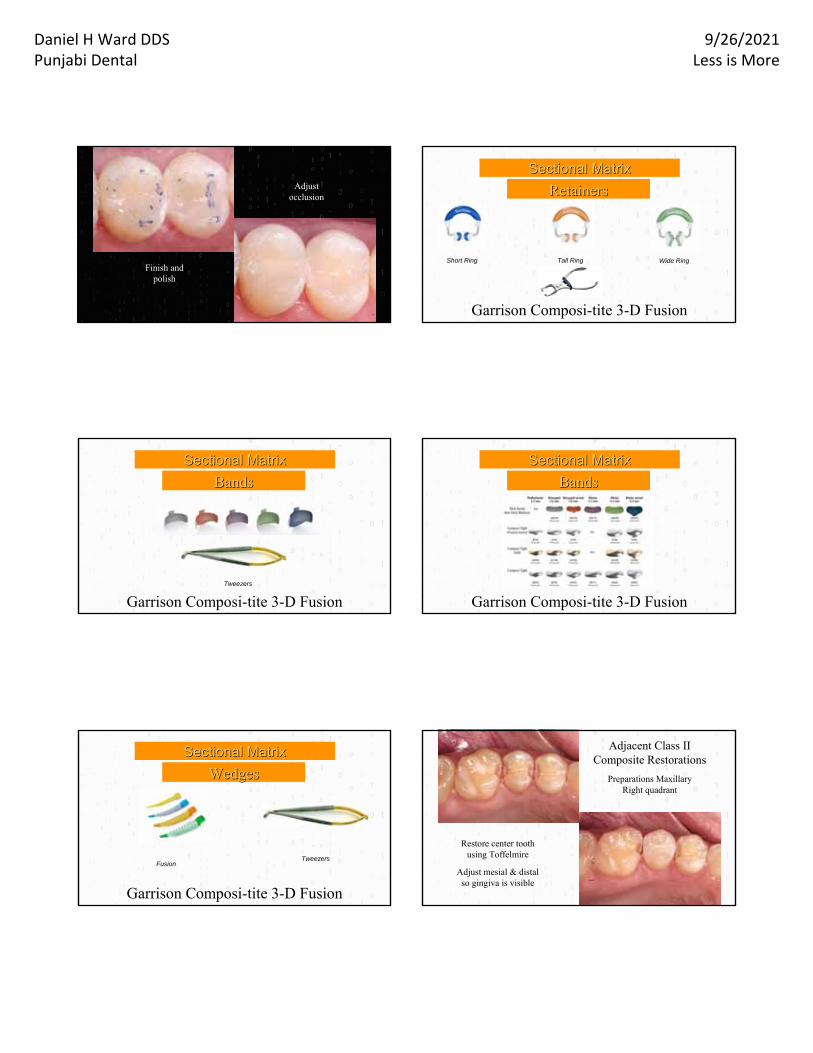
InIn‐‐Office ProceduresOffice Procedures
•• Test Output of All Curing LightsTest Output of All Curing Lights•• Enter Light, Composite & ShadeEnter Light, Composite & Shade
5m m
5mm
Interproximal Contacts
Composite Direct Placement Composite Direct Placement ChallengesChallenges
Christensen JJ. Duplicating the form and function of posterior teeth with Class II resin-based composite. Gen Dent. 2012;60:104-108.
Composites Should NOT be Viewed as Short-Term Crown Buildups
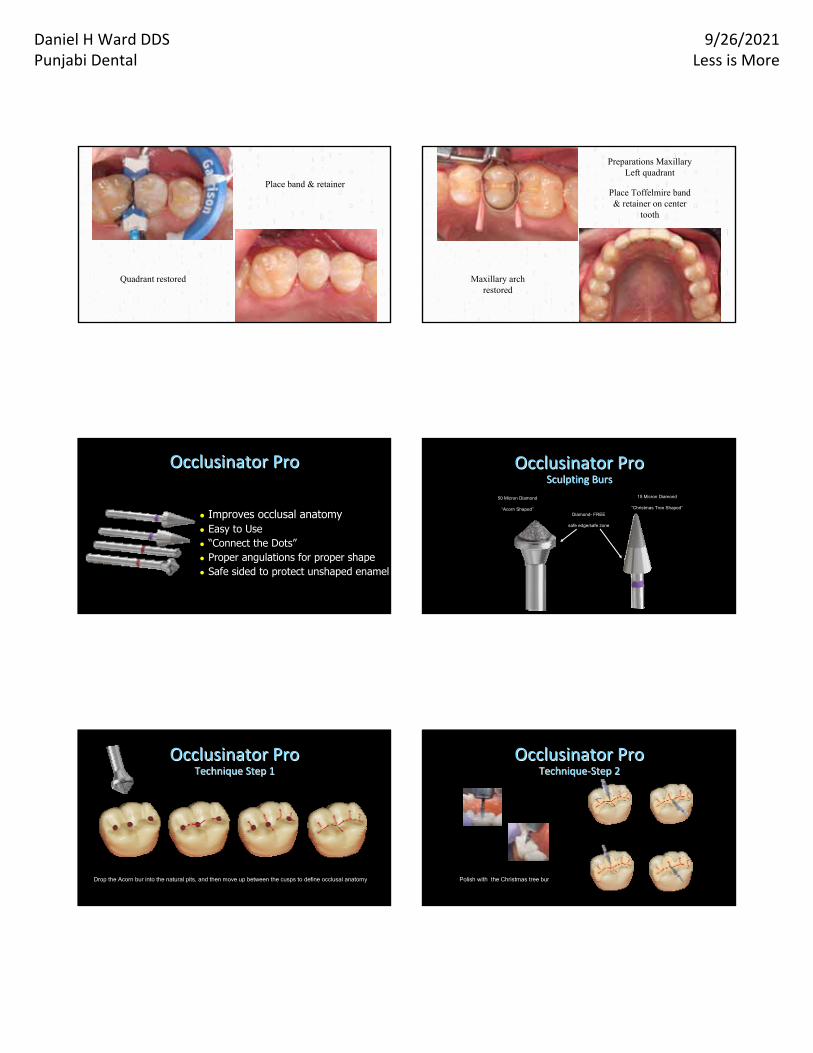
Tofflemire vs. Sectional Tofflemire vs. Sectional MatricesMatrices
Tofflemire System
➢ Thin contact at the marginal ridge
➢Non‐anatomical
➢ Foodtrapbelowcontact
➢ Increasedlikelihoodof:fracture,recurrentcariesandperiodontaldisease.
SectionalMatrices
✓Broad contacts at the proper height of contour
✓Anatomicallyshapedcontacts
✓TightContacts
✓Propercontactsthatflossproperlyforbettergingivalhealth
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
Sectional MatrixSectional Matrix
TrioDent/Palodent
Universal V3 Ring Narrow V3 Ring
Challenge:
Adjacent Class II Composite Restorations
Place contoured
band, wedge & V-Ring
Selective etching
Wash thoroughly
Apply bonding agent
Fill box 2/3’s full
Compress w 1P
Finish buildup
Cure ContacEZ
Re-contour diamond/finishing
carbides
Finishing strips
Place V-Ring on adjacent tooth
Burnish desired contact area
Selective etching
Place Universal bonding agent
Light Cure
Peel back band
Cure from both sides at
gingiva
Place Composite as
before
Light Cure
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
Finish and polish
Adjust occlusion
Sectional MatrixSectional Matrix
RetainersRetainers
Garrison Composi-tite 3-D Fusion
Short Ring Tall Ring Wide Ring
Sectional MatrixSectional Matrix
BandsBands
Garrison Composi-tite 3-D FusionTweezers
Sectional MatrixSectional Matrix
BandsBands
Garrison Composi-tite 3-D Fusion
Sectional MatrixSectional Matrix
WedgesWedges
Garrison Composi-tite 3-D Fusion
Fusion WedgesTweezers
Adjacent Class II Composite Restorations
Restore center tooth using Toffelmire
Adjust mesial & distal so gingiva is visible
Preparations Maxillary Right quadrant
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
Quadrant restored
Place band & retainer
Maxillary arch restored
Place Toffelmire band & retainer on center
tooth
Preparations Maxillary Left quadrant
● Improves occlusal anatomy● Easy to Use● “Connect the Dots”● Proper angulations for proper shape● Safe sided to protect unshaped enamel
Occlusinator ProOcclusinator Pro Occlusinator ProOcclusinator ProSculpting BursSculpting Burs
50 Micron Diamond
“Acorn Shaped”
15 Micron Diamond
“Christmas Tree Shaped”
Diamond- FREE
safe edge/safe zone
Occlusinator ProOcclusinator ProTechnique Step 1Technique Step 1
Drop the Acorn bur into the natural pits, and then move up between the cusps to define occlusal anatomy
Occlusinator ProOcclusinator ProTechniqueTechnique‐‐Step 2Step 2
Polish with the Christmas tree bur

Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
Occlusinator ProOcclusinator ProShaped ToothShaped Tooth
•Total Etch Technique
•Self Etch Technique
•Selective Etch Technique
Improved Dentin Bonding
Total-Etch Technique
Challenges-Technique Sensitivity
Under-etched enamel Over-etched dentinProper moisture-affects bond strengthsMoisture ContaminationProper Evaporation of solventIncompletely filled dentinal tubulesPost-Operative Sensitivity
Air only syringe
Air/water syringe
Evaporating the solvent with dry air
Post-Operative Sensitivity
• Chlorhexidine
•HEMA
Anti-Microbial

Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
Benefits
• Superior antimicrobial activity
• Enhances bond strength • Antimicrobial activity
• Inhibits enzymatic degradation
• Enhanced dentin bond strength
• Reduced micro-leakage
• No soft tissue burning
• Economical
Benefits
Desensitization Prior to Bridge Seating
Under Composite If you would like to try:
Text “Advantage” to:
72345
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
Self-Etch Technique
Challenges-Material Weaknesses
Decreased bond strength & marginal gap formation w/ un-etched enamel
Bond incompatibility to self-cure & dual-cure resins
Hydrolytic degradationEnzymatic collagen attack
Self etching Primer
Solution: “Etching prepared enamel w phosphoric acid promoted better marginal integrity with self-etching bonding agents.”
Marginal Gap Prevention
Souza-Junior EJ, Prieto LT, Araújo CT, Paulillo LA. Selective enamel etching: effect on marginal adaptation of self-etch LED-cured bond systems in aged Class I composite restorations. Oper Dent. 2012;37:195-204.
Solution: Use a self-cure or dual cured dentin bonding agent
Suh BI, Feng L, Pashley DH, Tay FR. Factors contributing to the incompatibility between simplified-step adhesives and chemically-cured or dual -cured composites. Part III. Effect of acidic resin monomers. J Adhes Dent 2003;5:267-282.
Bond Incompatibility with Self and Dual Cured Resins
Solution: Use MDP containing bonding agents which become hydrophobic upon polymerization due to high amount of cross-linkage.
“MDP-containing adhesives form nano-layering at the adhesive interface. Stable MDP-Ca salt deposition along with nano-layering may explain the high stability of MDP-based bonding.”
Yoshida Y, Yoshihara K, Nagaoka N, Hayakawa S, Tori Y, Ogawa T, Osaka A, Van Meerbeek B. Self-assembled nano-layering at the adhesive interface. J Dent Res 2012;9:376-381.
Hydrolytic Degradation
MMP-Matrix Metalloproteases
● MMPs are naturally occurring proteases involved in dentin formation and trapped during odontogenesis
● Not bacteria but proteolytic enzymes found within dentin capable of degrading collagen within newly created adhesive hybrid layers
● Low pH causes dentin to release these inherent MMPs which attack exposed collagen fibrils
Osorio R, Yamauti M. Osorio E., et al. Effect of dentin etching on metalloproteinase-mediated collagen degradation. Eur J Oral Sci 2011;119:79-85.
Enzymatic Collagen Attack
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
MMP-Matrix Metalloproteases
Carrilho et al., JDR 2007;
In-vivo 12 m w/PBNT (Acetone)
Immediate (MPa)Control 29.3 (9.2)CHX 32.7 (7.6)
w/CHX in 12 m
14 mo (MPa)Control 19.0 (5.2)CHX 32.2 (7.2)
Potential MMP Inhibitors
Long Term Dentin Bond Stability
● Chlorhexidine (CHX)
● Hemaseal & Cide
● Benzalkonium Chloride
● MDPB (12-methacryloxydodecalpyridinium bromide)
● GLUMA
Perdigao J, Resi A, Loguercio AD. Dentin Adhesion and MMPs: A Comprehensive Review. J Esthet Restor Dent 2012: 25:219-241.
Disinfect to prevent MMPs
Use Etchant containing 1% Benzalkonium Chloride
TE-Apply 2% Chlorhexidine after acid etching for 30 sec
SE-Apply 2 coats 2% Chlorhexidine prior to application of primer
OR
Long Term Dentin Bond Stability Selective-Etch TechniqueChallenges with Self-
Etching Primers:
Improved Enamel Bonding
But…
Selective-Etch TechniqueChallenges with Self-
Etching Primers:
Poorer Dentin Bonding
THE SolutionSelf‐etch Selective‐etch Total‐etch
Universal Bonding Agents
Challenges-SOLVED
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
Total-etch, self-etch or selective-etch technique
Can be used for direct and indirect restorations
Bond to all indirect substrates-metal, ceramics, zirconia, porcelain and lithium disilicate.
Compatible with light-cured, self-cured and dual-cured composite and luting cements.
Universal Bonding AgentsAll-Bond UniversalTotal-etch, self-etch or selective-etch
Single bottle for direct and indirectrestorations
High bond strengths to metal, ceramics, zirconia, porcelain & lithium disilicate.
Compatible with light-cured, self-cured and dual-cured composite and luting cements since pH is 3.2
Becomes hydrophobic upon setting
Universal Bonding Agents
Universal Bonding AgentsContain MDPContain MDP Contain MDP
Universal Bonding Agents
Having an effect upon a living organism, tissue, or cell.
Biologically active.
Bioactive

Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
121
ORAL ENVIRONMENT
2. ACP: Amorphous Calcium Phosphate – very high quantities
• Is pH driven. Healthy resting saliva has a pH 6.8. Demineralization starts at 5.5 pH.
• Saliva contains calcium and phosphate so it can build hydroxyapatite to keep teeth healthy.
• Hydroxyapatite is major component and essential ingredient of normal bone & teeth. It makes up bone mineral & the matrix of teeth. Hydroxyapatite gives bones and teeth their rigidity.
122
ORAL ENVIRONMENT
2. ACP: Amorphous Calcium Phosphate – very high quantities
• If the mouth is constantly being challenged by acid attacks, saliva cannot keep the balance.
• Result is an environment that favors demineralization
TOOTH
Acid
Calcium
phosphate
Demineralization Remineralization
Google Image Word Search
• Under acidic attack release ions-F, Ca, PO4, Na, Sr, Si, Al, Na, B
• Restorative and Base material
• Pulp capping material
• Cements
• Others
Bioactive
•Self-curing: Acid/Base setting reaction
•Ionic Bonding to tooth Calcium
•NO polymerization shrinkage stress
•More highly filled-reduced wear(compared to RMGI)
•Expansion/contraction similar to tooth
•High Fluoride Release-Bioactive
(The Original Bioactive Dental Material)Glass Ionomer Restoratives
Patient on multiple meds
Glass Ionomer Cervical Caries
Remove decay-place matricesTreat dentin with PAA
Place, shape and wait 2:30
Glass Ionomer Cervical Caries
Shape w very fine diamonds & waterPlace matrix and surface sealant

Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
Class V root caries
Glass Ionomer Cervical Caries
Repair around crown margins
Glass Ionomer Cervical Caries
Internal Cracks
Glass Ionomer Crown Buildup
Class II
Glass Ionomer Pediatrics
Glass Ionomer Sealants
Partially erupted vulnerable tooth
Able to seal before decayed
Long term fluoride affect -Rarely decay
Place
Glass Ionomer Sealants
Partially erupted vulnerable tooth Etch with
phosphoric acid
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
5 Years Later
Glass Ionomer Sealants
Place surface sealant Light cure
Glass Ionomer Closed Sandwich
Gain access to decay using a high
speed
Use slow speed and then spoon excavator
STOP if you feel you will expose pulp
Hilton TJ. Keys to Clinical Success with Pulp Capping: A Review of the Literature. Op Dent 2009;34:615-625.
Glass Ionomer Closed Sandwich
Condition enamel only with phosphoric acid for 10 seconds and
wash
Glass Ionomer Closed Sandwich
Place glass ionomerbase
Place Universal Dentin bonding agent Allow to set
Re-prep if needed
Glass Ionomer Closed Sandwich
Place composite and light cureFinish and Polish
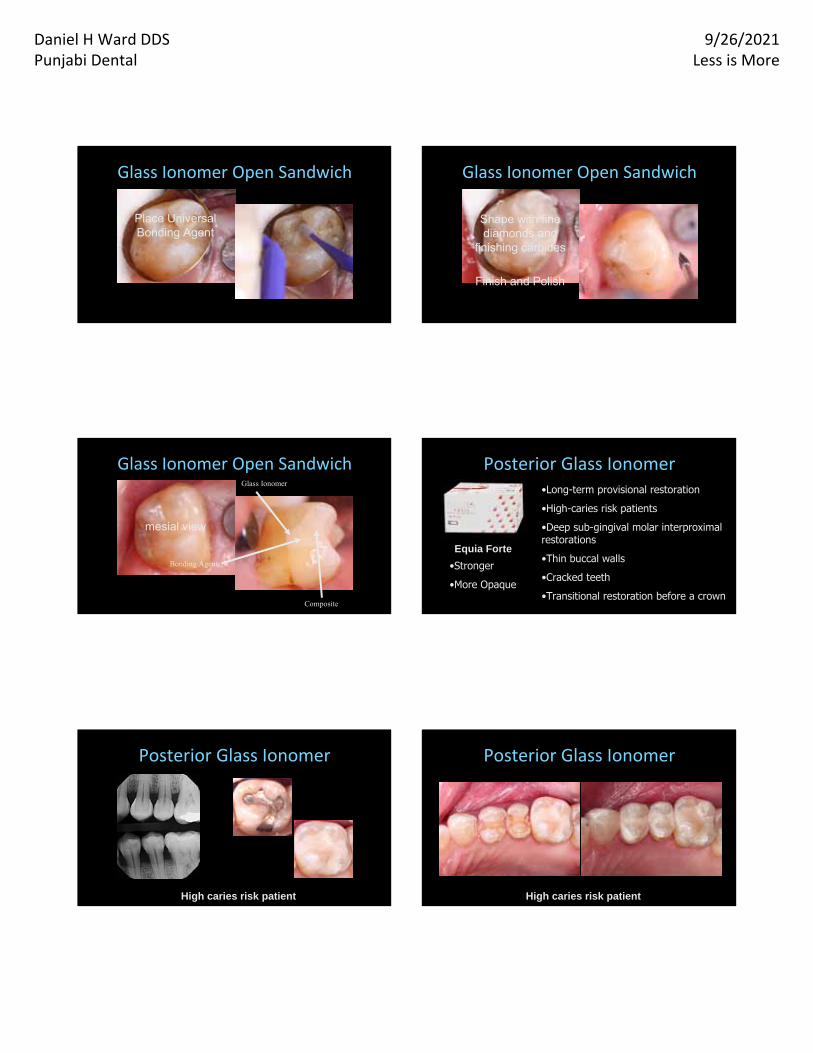
Glass Ionomer Open Sandwich
Preparation with dentin cervical
margin
Etch enamel with phosphoric acid -20 sec
Condition dentin with polyacrylic acid-10 sec
Wash thoroughly
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
Glass Ionomer Open Sandwich
Place glass ionomerbase
Allow to set, then reshape and wash &
dry if needed
Place Universal Bonding Agent
Glass Ionomer Open Sandwich
Buildup tooth with composite
Shape with fine diamonds and
finishing carbides
Finish and Polish
Glass Ionomer Open Sandwich
Straight -contoured Restoration
mesial view
Glass Ionomer
Composite
Bonding Agent
Posterior Glass Ionomer•Long-term provisional restoration
•High-caries risk patients
•Deep sub-gingival molar interproximal restorations
•Thin buccal walls
•Cracked teeth
•Transitional restoration before a crown
Equia Forte
•Stronger
•More Opaque
High caries risk patient
Posterior Glass Ionomer
High caries risk patient
Posterior Glass Ionomer
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
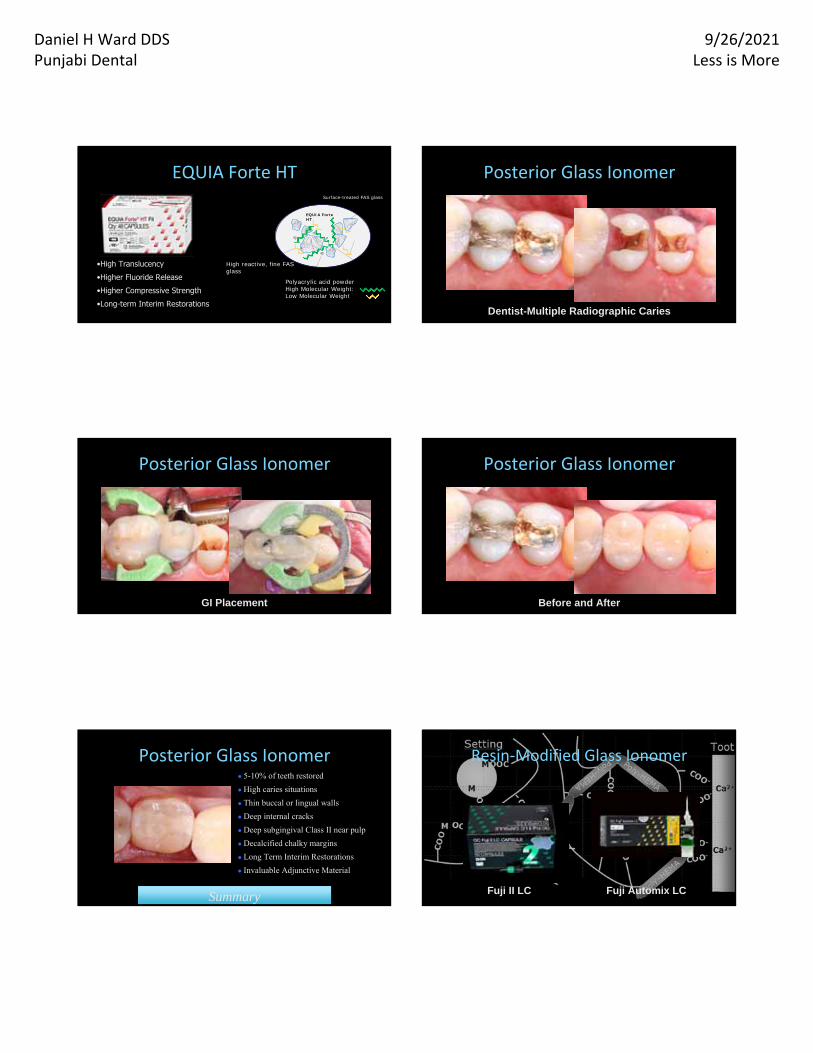
EQUIA Forte HT
•High Translucency
•Higher Fluoride Release
•Higher Compressive Strength
•Long-term Interim Restorations
EQUIA Forte HTSurface-treated FAS glass
High reactive, fine FAS glass
Polyacrylic acid powder High Molecular Weight:Low Molecular Weight
Dentist-Multiple Radiographic Caries
Posterior Glass Ionomer
Posterior Glass Ionomer
GI Placement Before and After
Posterior Glass Ionomer
SummarySummary
● 5-10% of teeth restored
● High caries situations
● Thin buccal or lingual walls
● Deep internal cracks
● Deep subgingival Class II near pulp
● Decalcified chalky margins
● Long Term Interim Restorations
● Invaluable Adjunctive Material
Posterior Glass Ionomer
Fuji II LC
Resin‐Modified Glass Ionomer
Fuji Automix LC
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
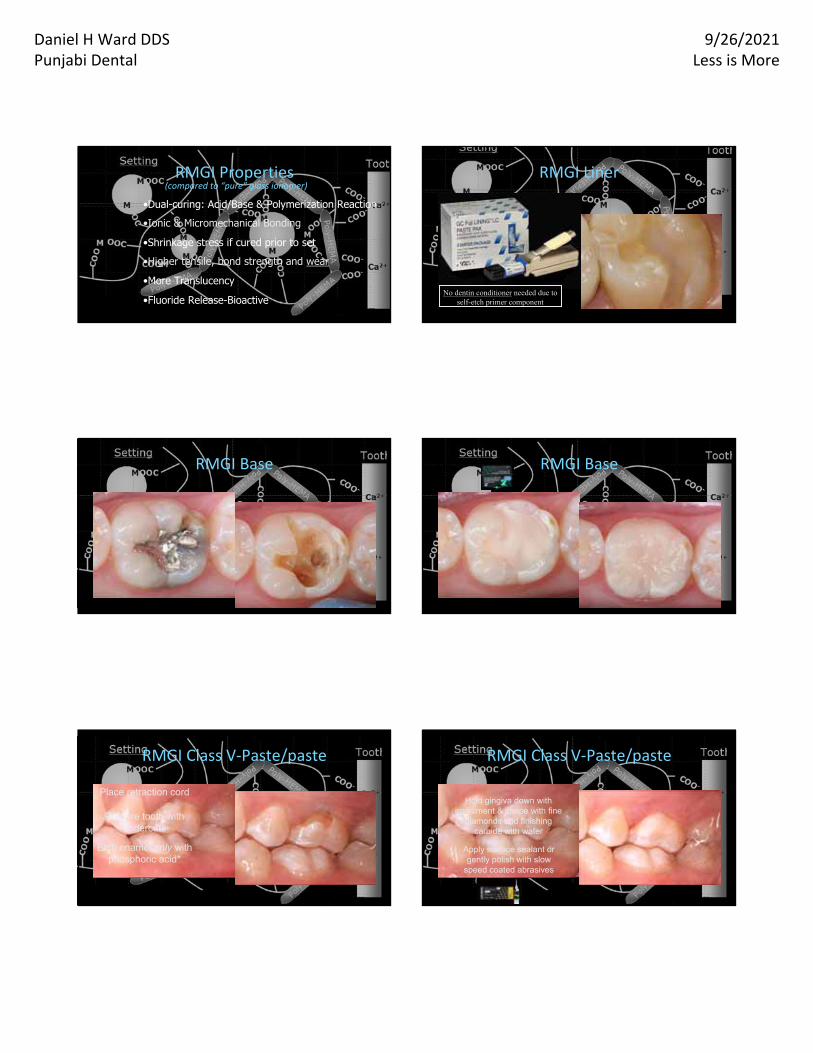
•Dual-curing: Acid/Base & Polymerization Reaction
•Ionic & Micromechanical Bonding
•Shrinkage stress if cured prior to set
•Higher tensile, bond strength and wear
•More Translucency
•Fluoride Release-Bioactive
RMGI Properties(compared to “pure” glass ionomer)
RMGI Liner
No dentin conditioner needed due to self-etch primer component
RMGI Base RMGI Base
Place RMGI & light cure
Re-prepare if necessary
Etch tooth and base with phosphoric acid
Place composite
RMGI Class V‐Paste/paste
Place retraction cord
Prepare tooth with undercuts
Etch enamel only with phosphoric acid*
RMGI Class V‐Paste/paste
Bulk placement
Light cure
Hold gingiva down with instrument & shape with fine
diamonds and finishing carbide with water
Apply surface sealant or gently polish with slow
speed coated abrasives
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
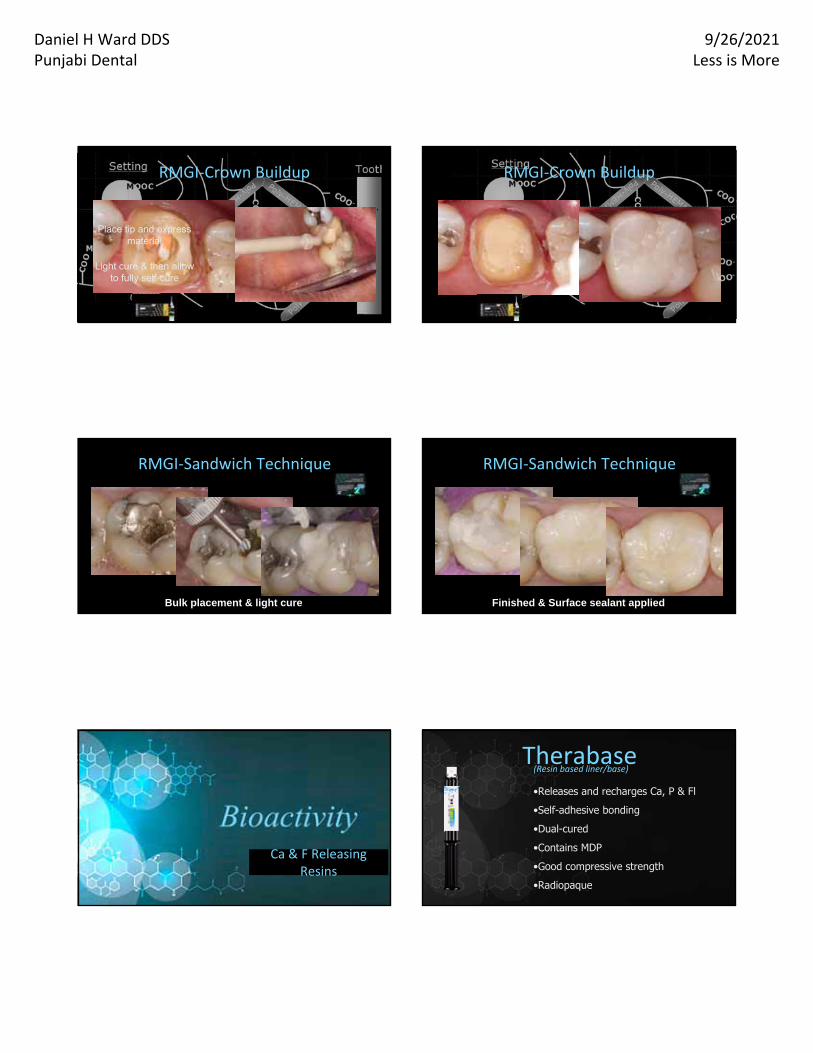
RMGI‐Crown Buildup
Place tip and express material
Light cure & then allow to fully self-cure
Quick preparation & removal of provisional
RMGI‐Crown Buildup
Seated Zirconia CrownCompleted preparation
Bulk placement & light cure
RMGI‐Sandwich Technique
Decayed toothExcavate
thoroughly
Finished & Surface sealant applied
RMGI‐Sandwich Technique
Reshape base-curved floor Placement prior
to curing
Ca & F Releasing Resins
•Releases and recharges Ca, P & Fl
•Self-adhesive bonding
•Dual-cured
•Contains MDP
•Good compressive strength
•Radiopaque
Therabase(Resin based liner/base)
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
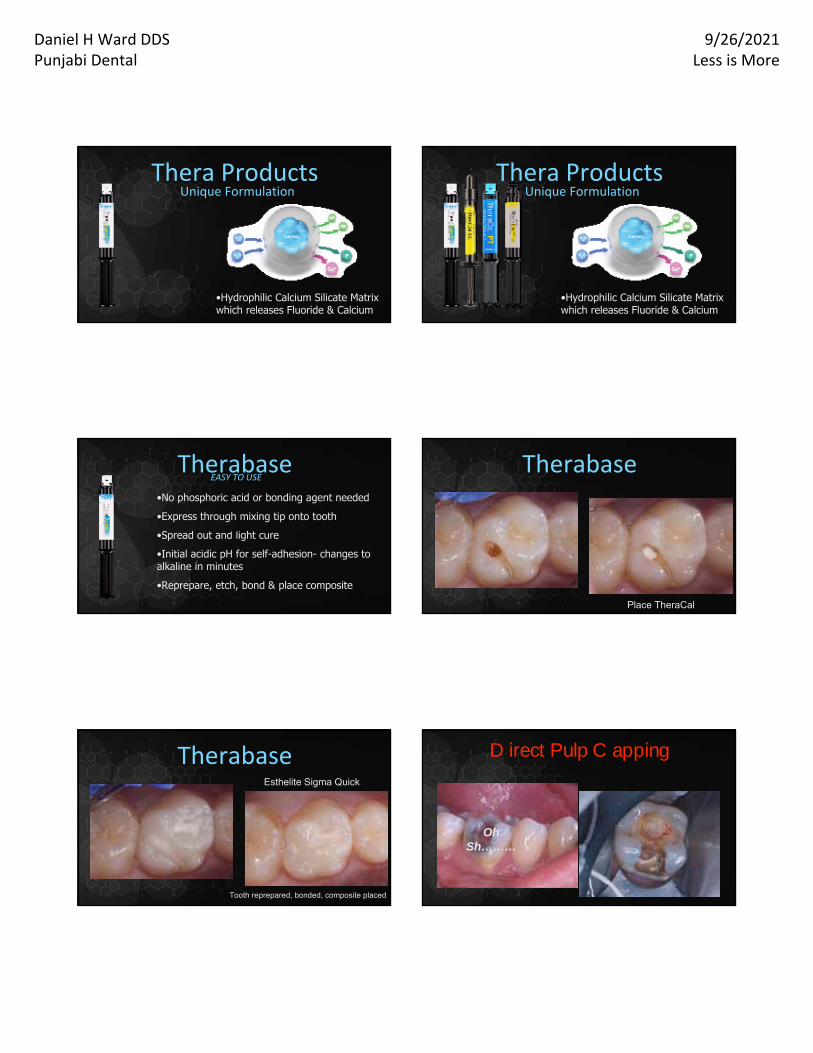
•Hydrophilic Calcium Silicate Matrix which releases Fluoride & Calcium
Thera ProductsUnique Formulation
200 pt
•Hydrophilic Calcium Silicate Matrix which releases Fluoride & Calcium
Thera ProductsUnique Formulation
200 pt
•No phosphoric acid or bonding agent needed
•Express through mixing tip onto tooth
•Spread out and light cure
•Initial acidic pH for self-adhesion- changes to alkaline in minutes
•Reprepare, etch, bond & place composite
TherabaseEASY TO USE
200 pt
Deep decay
Therabase
Place TheraCal
TheraBase placed & cured
Therabase
Tooth reprepared, bonded, composite placed
Esthelite Sigma Quick
Oh Sh………
Direct Pulp Capping
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
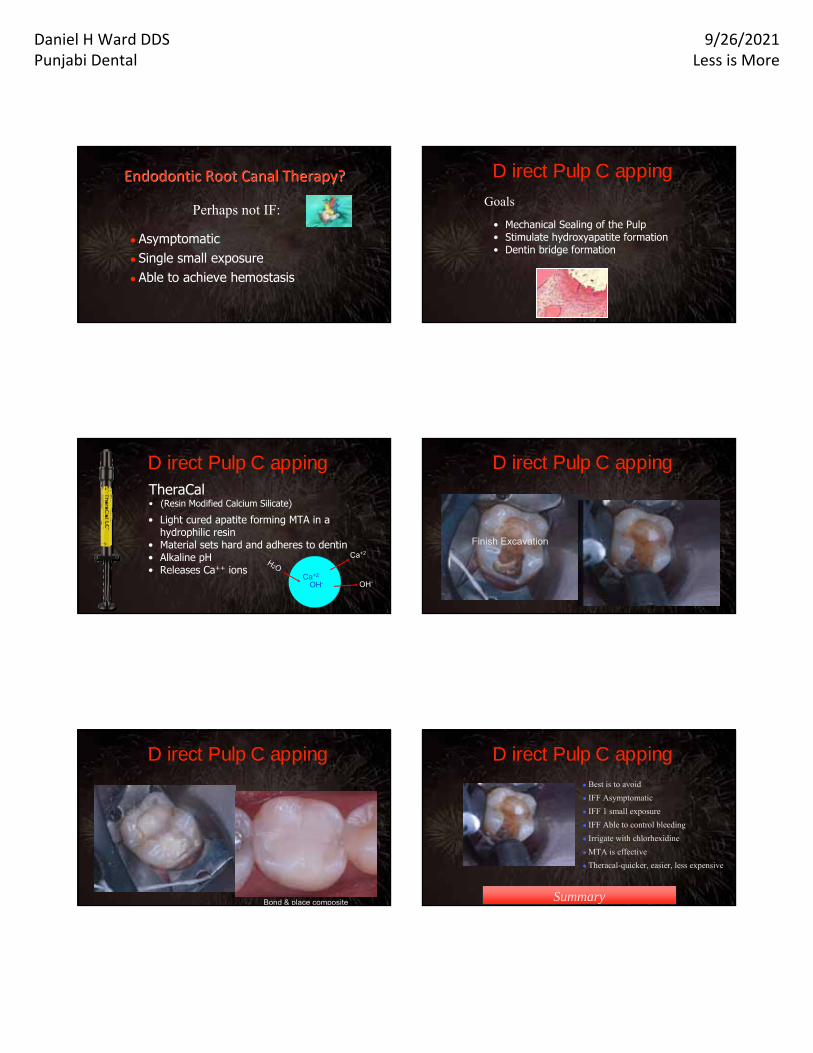
Endodontic Root Canal Therapy?Endodontic Root Canal Therapy?
● Asymptomatic● Single small exposure● Able to achieve hemostasis
Perhaps not IF:Goals
• Mechanical Sealing of the Pulp• Stimulate hydroxyapatite formation• Dentin bridge formation
Direct Pulp Capping
TheraCal • (Resin Modified Calcium Silicate)
Direct Pulp Capping
• Light cured apatite forming MTA in a hydrophilic resin
• Material sets hard and adheres to dentin• Alkaline pH• Releases Ca++ ions
Ca+2
OH-
H2O
Ca+2
OH-
Direct Pulp Capping
STOP!
Control bleeding
Water, saline, chlorhexidine, sodium
hypochlorite
Place Theracal & cure
Finish Excavation
Direct Pulp Capping
Cover with RMGI or Therabase
Bond & place composite SummarySummary
● Best is to avoid
● IFF Asymptomatic
● IFF 1 small exposure
● IFF Able to control bleeding
● Irrigate with chlorhexidine
● MTA is effective
● Theracal-quicker, easier, less expensive
Direct Pulp Capping
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
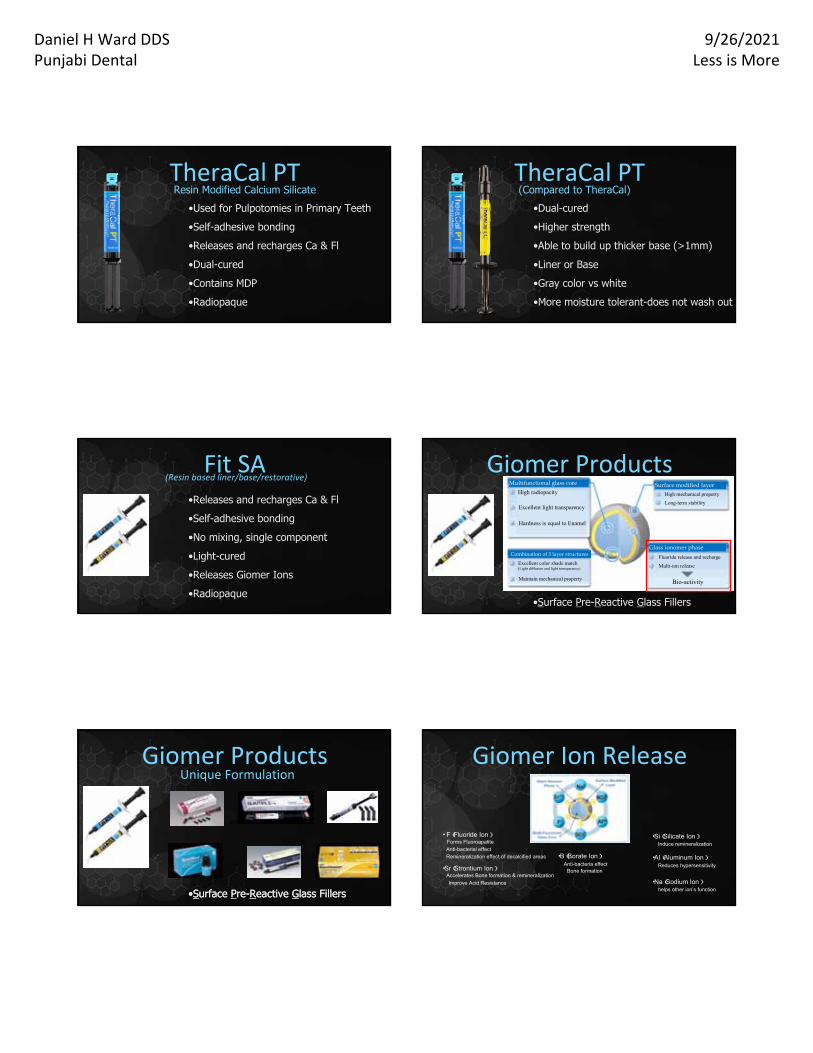
•Used for Pulpotomies in Primary Teeth
•Self-adhesive bonding
•Releases and recharges Ca & Fl
•Dual-cured
•Contains MDP
•Radiopaque
TheraCal PTResin Modified Calcium Silicate
TheraCal PT(Compared to TheraCal)
•Dual-cured
•Higher strength
•Able to build up thicker base (>1mm)
•Liner or Base
•Gray color vs white
•More moisture tolerant-does not wash out
Fit SA•Releases and recharges Ca & Fl
•Self-adhesive bonding
•No mixing, single component
•Light-cured
•Releases Giomer Ions
•Radiopaque
(Resin based liner/base/restorative)
•Surface Pre-Reactive Glass Fillers
Giomer ProductsUnique Formulation
200 pt
Set Glass Ionomer Material Surface Modified Pre-Reactive Glass Ionomer Filler
Surface modified layer
Glass Ionomer phase
Glass Core
Set glass ionomer filler particlesMultifunctional glass core
High radiopacity
Excellent light transparency
Combination of 3 layer structures
Hardness is equal to Enamel
Excellent color shade match(Light diffusion and light transparency)
Maintain mechanical property
Surface modified layer
Glass ionomer phase
High mechanical property
Long-term stability
Fluoride release and recharge
Multi-ion release
Bio-activity
Giomer ProductsUnique Formulation
200 pt
•Surface Pre-Reactive Glass Fillers•Surface Pre-Reactive Glass Fillers
Giomer Ion Release
・ F(Fluoride Ion)Forms Fluoroapatite
Anti-bacterial effectRemineralization effect of decalcified areas
・Sr(Strontium Ion)Accelerates Bone formation & remineralization
Improve Acid Resistance
・AI(Aluminum Ion)Reduces hypersensitivity
・Si(Silicate Ion)Induce remineralization
・B(Borate Ion)Anti-bacteria effect
Bone formation
・Na(Sodium Ion)helps other ion’s function

Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
•No phosphoric acid or bonding agent needed
•Self-adhesive bonding reduces sensitivity
•2 viscosities-F03 (low flow) F10 (runny)
•Express through tip onto tooth
•Leave for 20 seconds-then light cure
•Cover with composite or continue to buildup Transitions from acidic PH (needed for initial bonding) to alkaline PH in minutes* which promotes pu
Transitions from acidic PH (needed for initial bonding) to alkaline PH in minutes* which promotes pu
Fit SAEASY TO USE
Fit SAInstructions
✴Class I Restoration - F03✴Class III and Class IV Restorations - F03✴Class V Restoration - F03✴Lining of Large Restorations - F10 Transitions from acidic PH (needed for initial bonding) to alkaline PH in minutes* which promote
vitality2 Transitions from acidic PH (needed for initial bonding) to alkaline PH in minutes* which p
pulp vitality2
Fit SA
2 Viscosities
F03 (low flow) & F10 (runny)
IndicationsFit SA
Dr. Jack Griffin
F03 CLASS I (MAXILLARY)
F03 CLASS I (MANDIBULAR)
Fit SA
Dr. Jack Griffin
F03 CLASS V
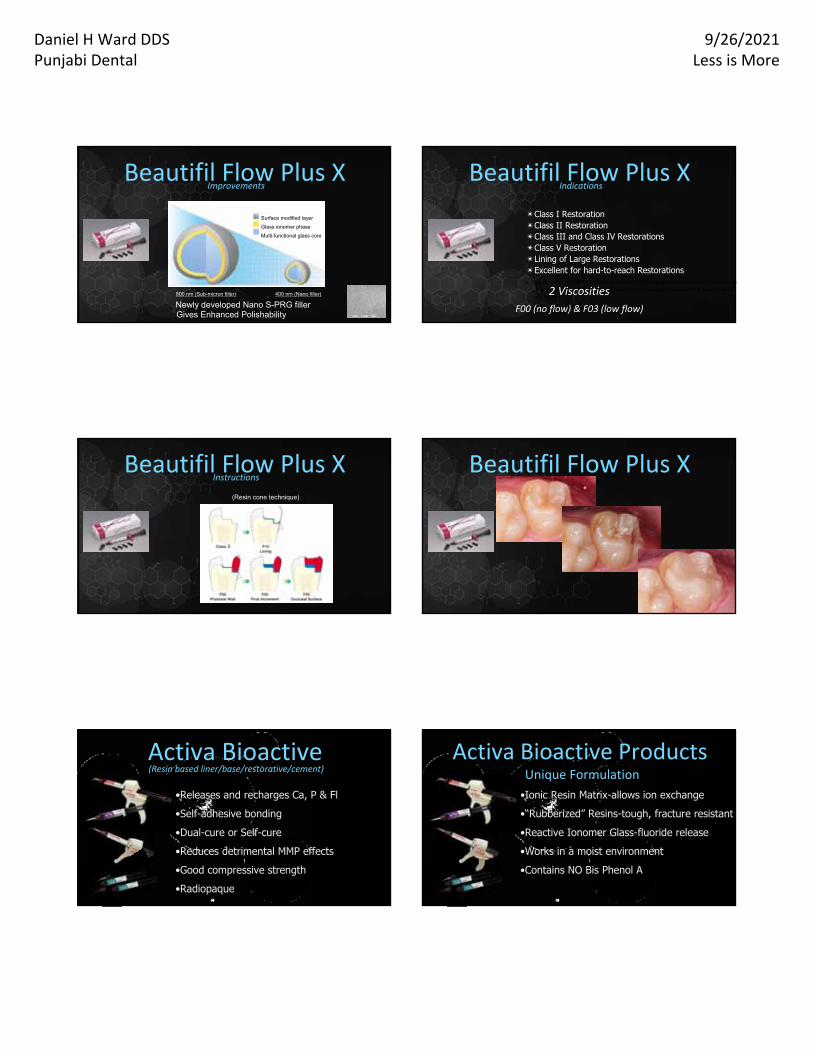
Beautifil Flow Plus X •Releases and recharges Fl
•Can be used as liner, base or restoration
•Light-cured
•Releases Giomer Ions
•Excellent Polishability
•Radiopaque
(High Viscosity Flowable Composite)
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
Beautifil Flow Plus X Improvements
Surface modified layer
Glass ionomer phase
Multi-functional glass core
Newly developed Nano S-PRG filler800 nm (Sub-micron filler) 400 nm (Nano filler)
Gives Enhanced Polishability
✴Class I Restoration ✴Class II Restoration✴Class III and Class IV Restorations ✴Class V Restoration ✴Lining of Large Restorations ✴Excellent for hard-to-reach Restorations Transitions from acidic PH (needed for initial bonding) to alkaline PH in minutes* which promote
vitality2 Transitions from acidic PH (needed for initial bonding) to alkaline PH in minutes* which p
pulp vitality22 Viscosities
F00 (no flow) & F03 (low flow)
IndicationsBeautifil Flow Plus X
Beautifil Flow Plus X Instructions
(Resin cone technique)
Beautifil Flow Plus X
•Releases and recharges Ca, P & Fl
•Self-adhesive bonding
•Dual-cure or Self-cure
•Reduces detrimental MMP effects
•Good compressive strength
•Radiopaque
Activa Bioactive(Resin based liner/base/restorative/cement)
•Ionic Resin Matrix-allows ion exchange
•“Rubberized” Resins-tough, fracture resistant
•Reactive Ionomer Glass-fluoride release
•Works in a moist environment
•Contains NO Bis Phenol A
Activa Bioactive ProductsUnique Formulation
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
Releases Phosphates as pH lowers
ppm
Activa BioactiveIon Release
Releases Calcium as pH lowersRestoration Under Crown
Activa Bioactive Restorative
•Releases and recharges Ca, P & Fl
•Calcium phosphate soluble in monomer
•-Light cured
•Reduces detrimental MMP effects
•Good compressive strength & toughness
•Radiopaque
Activa Presto(High Viscosity Flowable Composite)
•Liners
•Class V restorations
•Class I II III restorations
•Pediatric patients
•Geriatric patients
•Crown buildups
Activa PrestoUses
Class I
Activa Presto Activa Bioactive vs Presto
Hydrophilic
Rubberized Resins
Calcium /Phosphate Enriched Ionic
Resins
Release/Recharge Calcium, Phosphate,
Fluoride
No Bis-GMA or BPA Derivatives
Dual Cure
Contains Glass Ionomer
Injectable/Flowable
Bulk Fill
5 Shades
Light Cure
Contains ModifiedCalcium Phosphate
High viscosity Flowable
2mm Increments
8 Shades

Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
Ca & F Releasing Preventive
200
RECALDENT (ACP-CPP)
ACP-CPP release dependent on pH of the oral environment•Acidic environment-releases more ACP•Stable environment-releases appropriate level
ACP: Amorphous Calcium Phosphate • Active carrier molecule
CPP: Casein Phosphopeptide • Delivery vehicle
• Binds to enamel, pellicle, plaque, and soft tissue
• Binds Calcium and Phosphate
• Milk Protein
201
RECALDENT (ACP-CPP)
ACP: Amorphous Calcium Phosphate • Carrier molecule
CPP: Casein Phosphopeptide• Do not use on patients with a
proven or suspected milk protein allergy or with sensitivity to benzoate preservatives
• Lactose content is less than 0.01%
202
RECALDENT (ACP-CPP)
2. ACP: Amorphous Calcium Phosphate – very high quantities
Provides Ca and PO4
Promotes Remineralization
Prevents mineral lossInhibits
Demineralization
Neutralizes acid from bacteria
Neutralizes & Buffers
Mechanism of ActionMechanism of Action• Binds to enamel, pellicle, plaque, & soft tissue
RECALDENT (ACP-CPP)
Mechanism of ActionMechanism of Action
RECALDENT (ACP-CPP) PRODUCTS
MI Paste MI Paste Plus
MI VarnishMI Paste ONE GC Fuji TRIAGE Plus
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
MI PASTE
● Provides bio-available calcium and phosphate ● Buffers pH● Reduces tooth sensitivity● Aides remineralization● Reduces sensitivity after scaling or tooth whitening● Excellent for dry mouth syndrome● Treats white spot lesions
● After tooth whitening
● For pregnant mothers
● For children 6 & older
● During or after ortho
● Desensitization
● Poor Oral Hygiene
● Extra protection for teeth
MI PASTE USES
MI PASTE PLUS
● Addition of 0.2% NaF (900 ppm)● Provides bio-available calcium and phosphate ● Reduces tooth sensitivity● Aides remineralization● Fluoride increases anti-cariogenic effect● Excellent for dry mouth syndrome● Treats white spot lesions ● Suitable for patients 12 and older
●White spot lesions
● Desensitization
● During or after ortho-12 and older
● Medical compromised patients
● Xerostomia
● High Acid Environment
● High Caries Risk patients
● Extra Protection
MI PASTE PLUSUSES
MI PASTE & MI PASTE PLUS
APPLICATION■ Apply after toothbrushing
■ Rub paste onto tooth & leave for 3 minutes
■ May apply with trays for 3-5 minutes
■ No food or drink for 30 minutes
MI PASTE ONE
● Toothpaste with ACP-CPP, Fluoride & Potassium Nitrate ● Same benefits as MI Paste Plus● Very low in abrasives● Reduces tooth sensitivity● Aides remineralization● Good for tooth erosion and wear● Treats white spot lesions ● Ideal for High-Risk Patients

Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
MI PASTE ONE
APPLICATION
Apply a small, pea-size amount of MI Paste® ONE to your
toothbrush.
For best results, brush for 2 minutes and do not rinse; do not eat or drink for 30 mins after brushing. Use twice
a day.
MI Paste® ONE MI Paste Plus®MI Paste®
pH 7.1 7.2 7.2CPP-ACP 10% 10% 10%
Ca2+
content 11.6mg/g 11.7mg/g 11.7mg/g
PO4 content 7.0mg/g 7.0mg/g 7.0mg/g
Fluoride 1,100 ppm NaF 900 ppm NaF -KNO3 5%Silica Yes - -
Surfactant Yes - -
Composition
MI VARNISH
● Ads benefits of bio-available calcium and phosphate to fluoride varnish
GC FUJI TRIAGE EP
● Ads benefits of bio-available calcium and phosphate to high fluoride releasing glass ionomer
● Inhibits biofilm formation● Helps prevent caries caused by acid and bacteria
AGEAPPROPRIATE
RESTORATIONS
• Xerostomia• Root exposures• Difficulty maintaining oral hygiene• Some unable to tolerate long
appointments• Difficulty coming to office
• Fixed Income
US Population is Aging
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
Multiple Medications
Aging Population Challenges‐Xerostomia
Aging Population Challenges‐Xerostomia
“40% of all prescription drugs have dry mouth listed in the PDR as a possible side effect”
Chalmers J. Personal Communication. 2006.Chalmers J. Personal Communication. 2006.
Aging Population Challenges‐Xerostomia
In a published study of 131 different prescribed medications the most common side effect cited was xerostomia.
Smith RG, Burtner AP. Oral sideSmith RG, Burtner AP. Oral side--effects of the most frequently prescribed drugs. Spec effects of the most frequently prescribed drugs. Spec Care Dent. 1994;14:96Care Dent. 1994;14:96--102. 102.
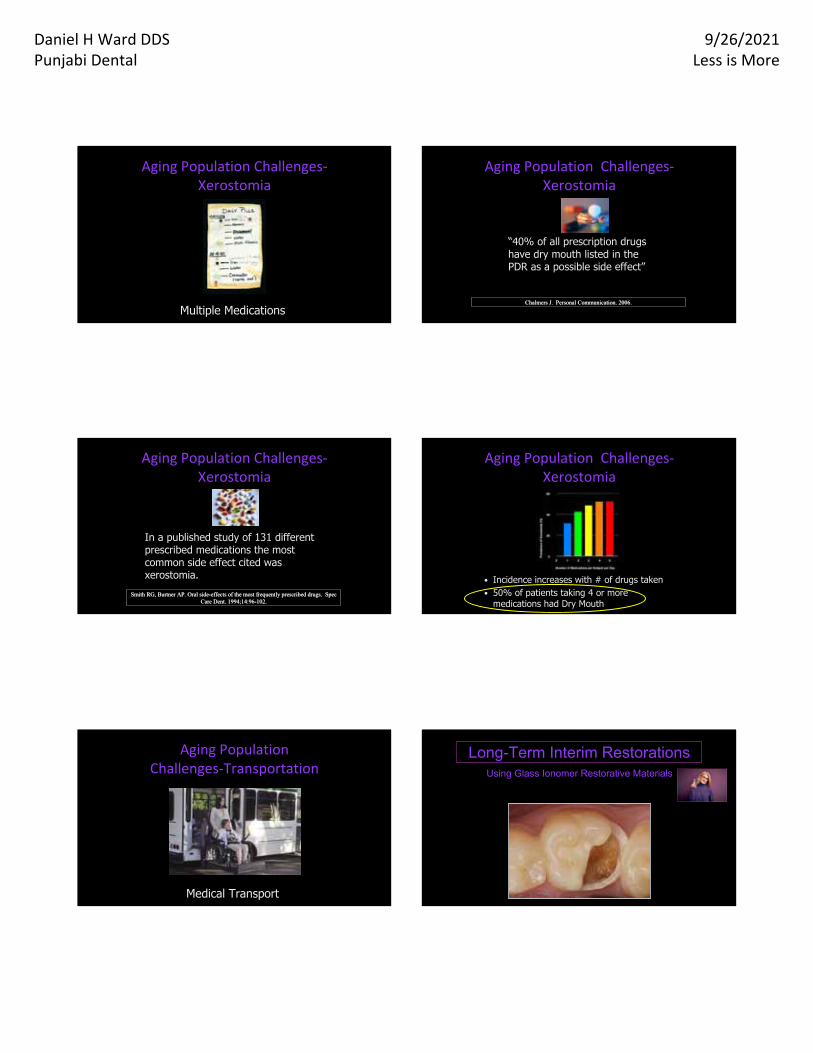
Aging Population Challenges‐Xerostomia
• Incidence increases with # of drugs taken• 50% of patients taking 4 or more
medications had Dry Mouth
Medical Transport
Aging Population Challenges‐Transportation
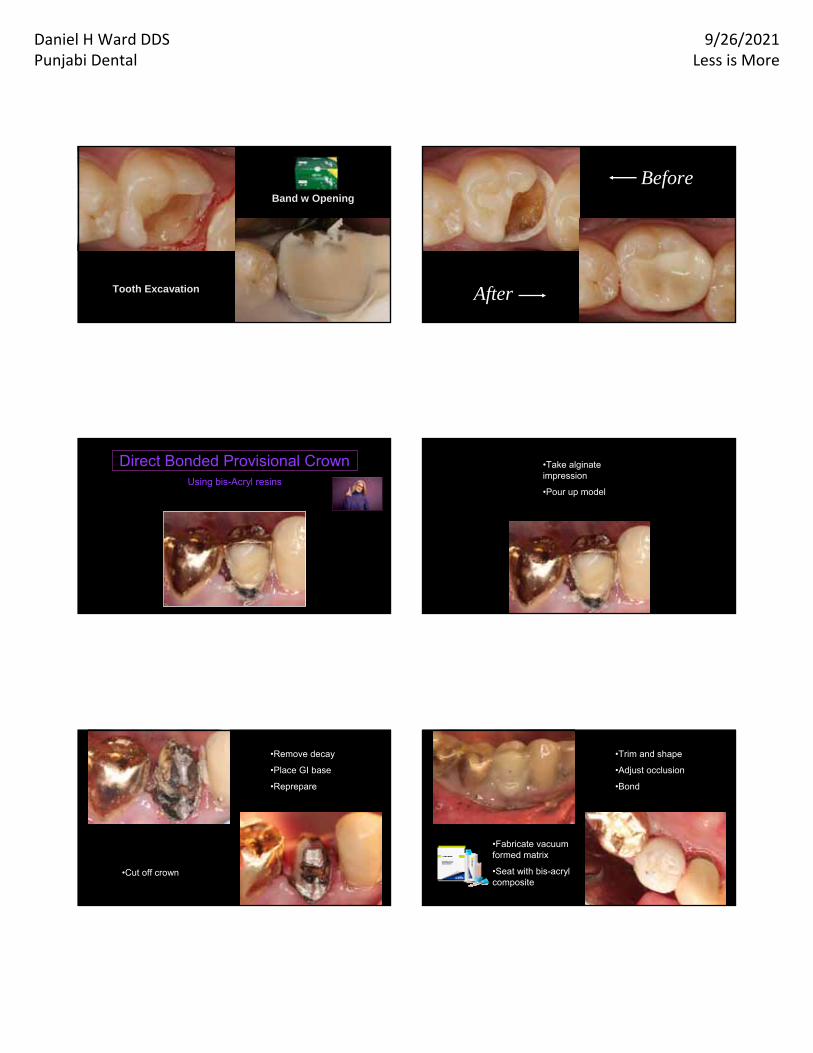
Long-Term Interim RestorationsUsing Glass Ionomer Restorative Materials
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
Tooth Excavation
Band w Opening
Before
After
Direct Bonded Provisional CrownUsing bis-Acryl resins
•Take alginate impression
•Pour up model
•Cut off crown
•Remove decay
•Place GI base
•Reprepare
•Fabricate vacuum formed matrix
•Seat with bis-acryl composite
•Trim and shape
•Adjust occlusion
•Bond
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
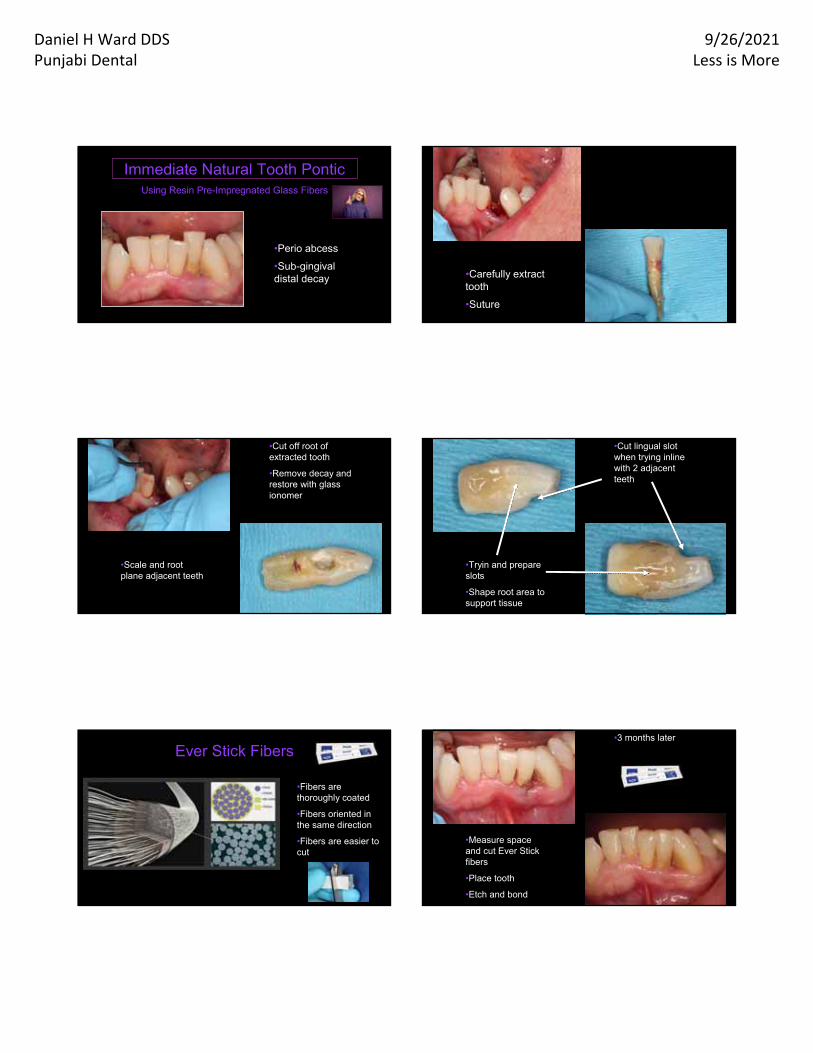
•Perio abcess
•Sub-gingival distal decay
Immediate Natural Tooth PonticUsing Resin Pre-Impregnated Glass Fibers
•Carefully extract tooth
•Suture
•Scale and root plane adjacent teeth
•Cut off root of extracted tooth
•Remove decay and restore with glass ionomer
•Tryin and prepare slots
•Shape root area to support tissue
•Cut lingual slot when trying inline with 2 adjacent teeth
•Fibers are thoroughly coated
•Fibers oriented in the same direction
•Fibers are easier to cut
Ever Stick Fibers
•Measure space and cut Ever Stick fibers
•Place tooth
•Etch and bond
•3 months later
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
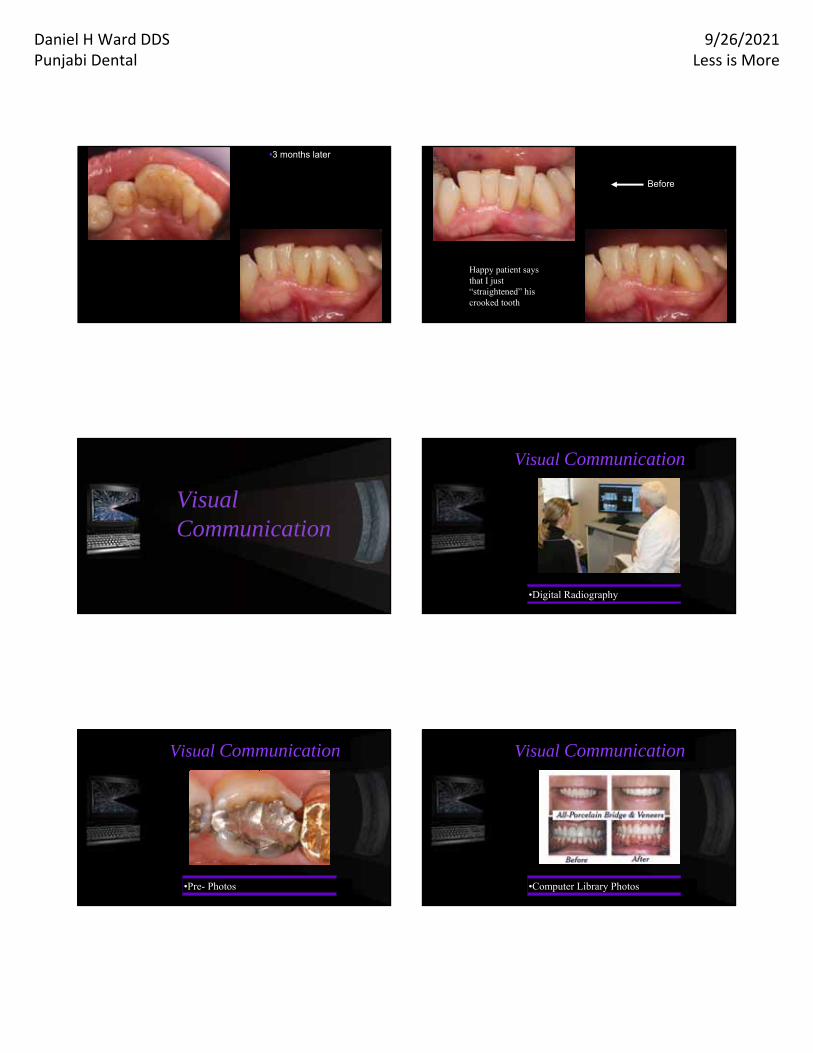
•3 months later
Before
Happy patient says that I just “straightened” his crooked tooth
Visual Communication
•Digital Radiography•Digital Radiography
Visual Communication
•Pre- Photos
Visual Communication
•Computer Library Photos
Visual Communication
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
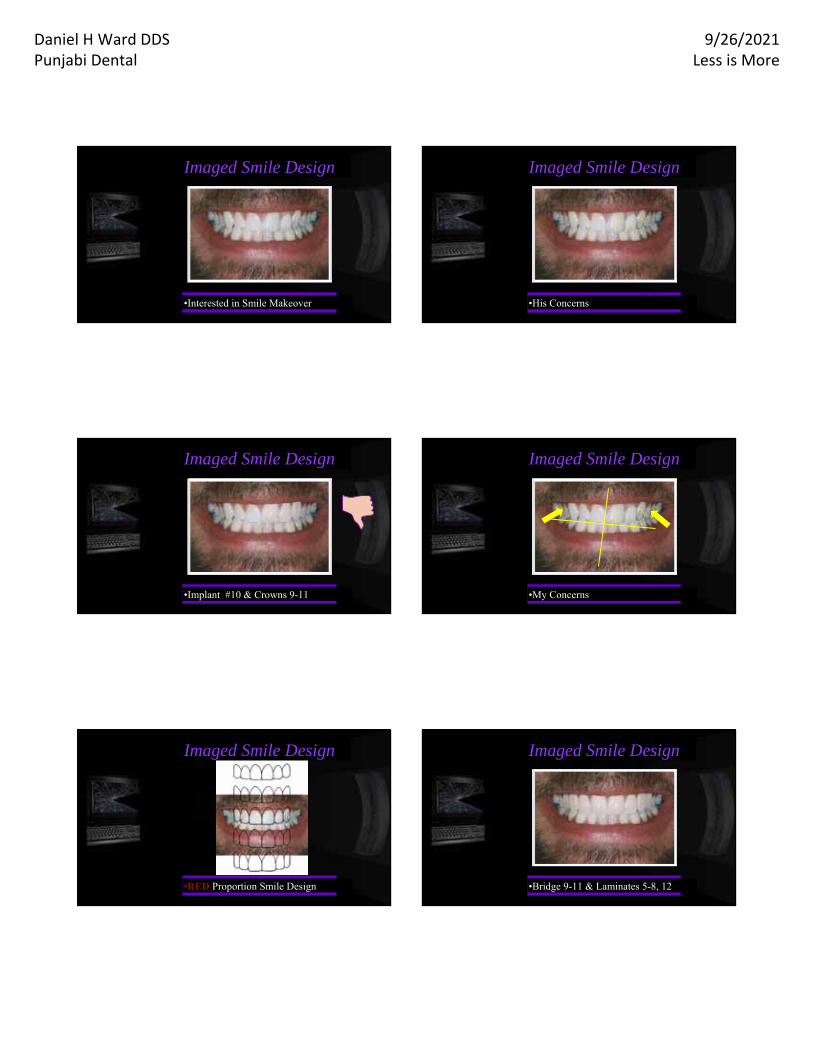
Imaged Smile Design
•Interested in Smile Makeover •His Concerns
Imaged Smile Design
Imaged Smile Design
•Implant #10 & Crowns 9-11 •My Concerns
Imaged Smile Design
•RED Proportion Smile Design
Imaged Smile Design Imaged Smile Design
•Bridge 9-11 & Laminates 5-8, 12

Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
Imaged Smile Design
•Cost
Imaged Smile Design
•Bridge 9-11 & Laminates 6-8
Imaged Smile Design
•Preparations
Imaged Smile Design
•Lab Prosthesis
Imaged Smile Design
•Finished Smile
•DSD App
•I Pad I Phone App
•Smile Frame
•Proportional
•Personality Library Shapes
Visual Communication
•Digital Smile Design App
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
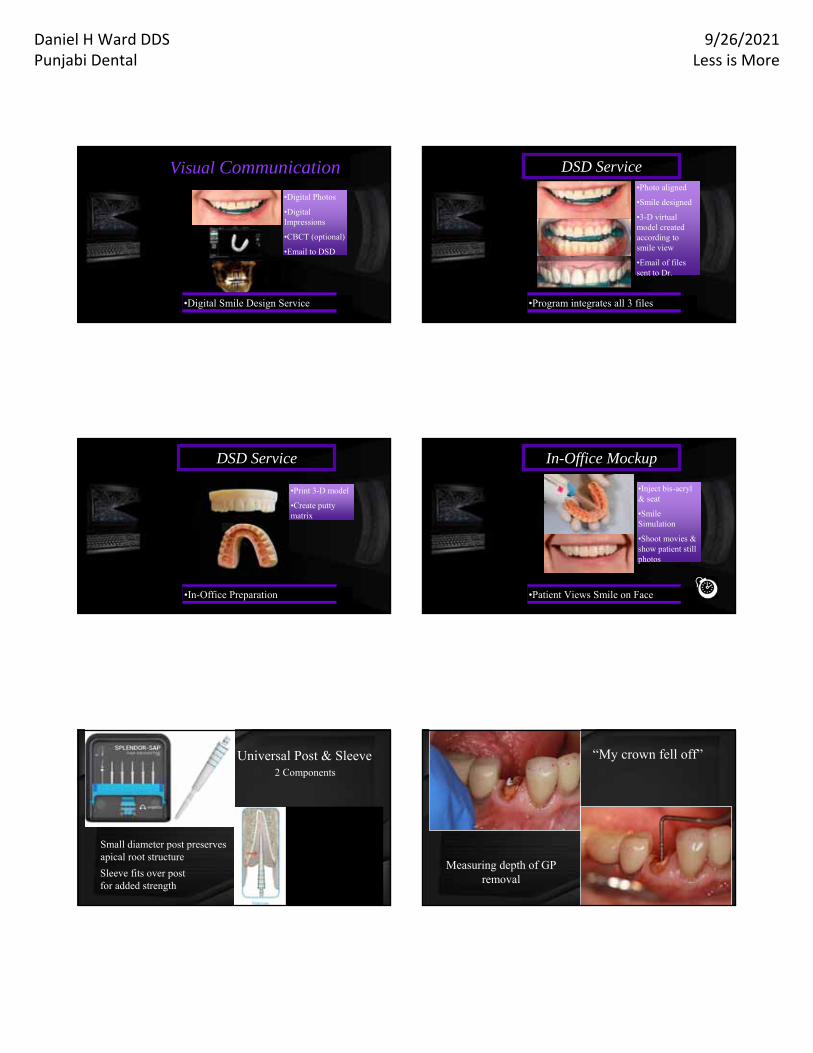
•Digital Photos
•Digital Impressions
•CBCT (optional)
•Email to DSD
Visual Communication
•Digital Smile Design Service
•Photo aligned
•Smile designed
•3-D virtual model created according to smile view
•Email of files sent to Dr.
DSD Service
•Program integrates all 3 files
•Print 3-D model
•Create putty matrix
DSD Service
•In-Office Preparation
•Inject bis-acryl & seat
•Smile Simulation
•Shoot movies & show patient still photos
In-Office Mockup
•Patient Views Smile on Face
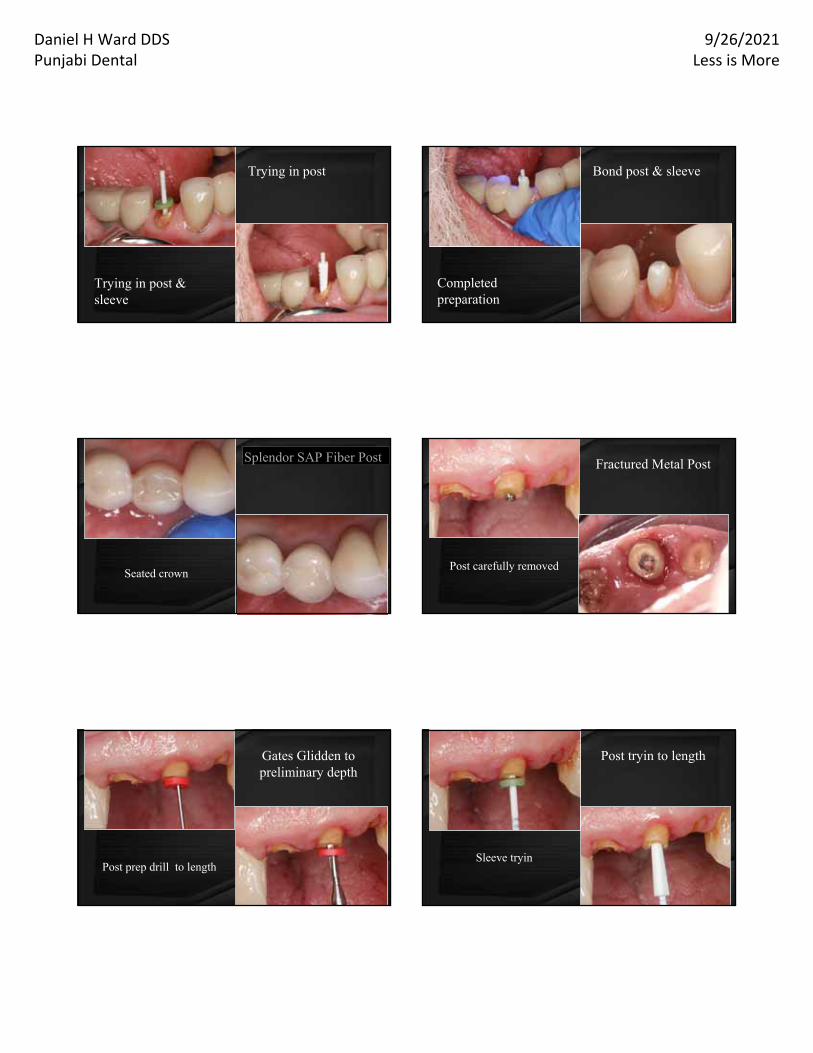
Universal Post & Sleeve
Small diameter post preserves apical root structure
Sleeve fits over post for added strength
2 Components
“My crown fell off”
Measuring depth of GP removal
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
Trying in post
Trying in post & sleeve
Bond post & sleeve
Completed preparation
Provisional crownSeated crown
Splendor SAP Fiber PostSplendor SAP Fiber Post Fractured Metal Post
Post carefully removed
Gates Glidden to preliminary depth
Radiograph confirmation
Post prep drill to length
Post tryin to length
Sleeve tryin
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
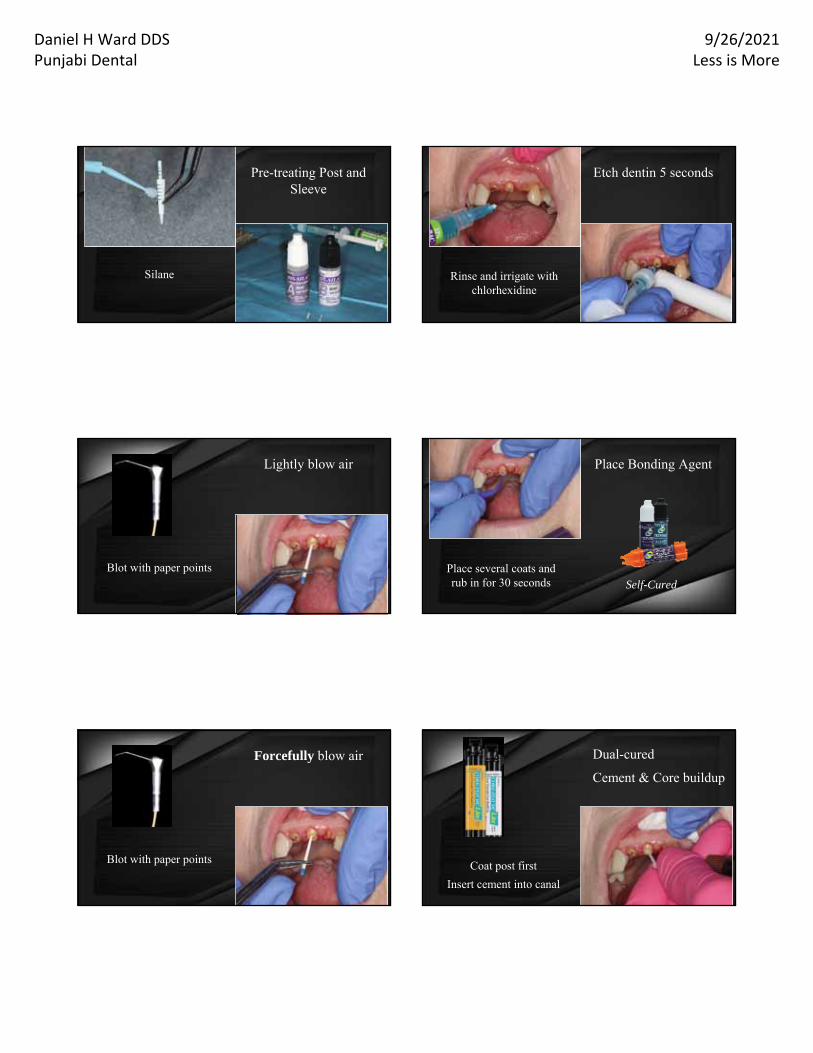
Pre-treating Post and Sleeve
Silane
Etch dentin 5 seconds
Rinse and irrigate with chlorhexidine
Lightly blow air
Blot with paper points
Place Bonding Agent
Place several coats and rub in for 30 seconds Self-Cured
Forcefully blow air
Blot with paper pointsCoat post first
Insert cement into canal
Dual-cured
Cement & Core buildup

Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
Quickly insert post into canal
Coat top of post and quickly insert sleeve
Buildup core
Light Cure & Wait 3 minutes
Cutoff extra post length
Prepare tooth
Completed Preparation
Splendor SAP Fiber PostSplendor SAP Fiber Post
Radiograph
• Preparations-Even & Adequate Reduction
• Cementation Procedures different for each material
• Cement may affect Color
• Cannot adjust intaglio surface of crown
• Post-seating fractures or debonding
• REQUIRES HIGHER SKILLS & ATTENTION TO DETAIL
All-Ceramic RestorationChallengesChallenges
High Strength Monolithic Zirconia (tetragonal 3Y-TZP*)
• Posterior molars
• Grinders
• Blockout dark tooth
• Always decontaminate intaglio surface
• Conventional cementation-RMGI
• Bond w short or non-retentive preps*3 mole-percent yttrium-stabilized tetragonal
zirconia polycrystals
tetragonal
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
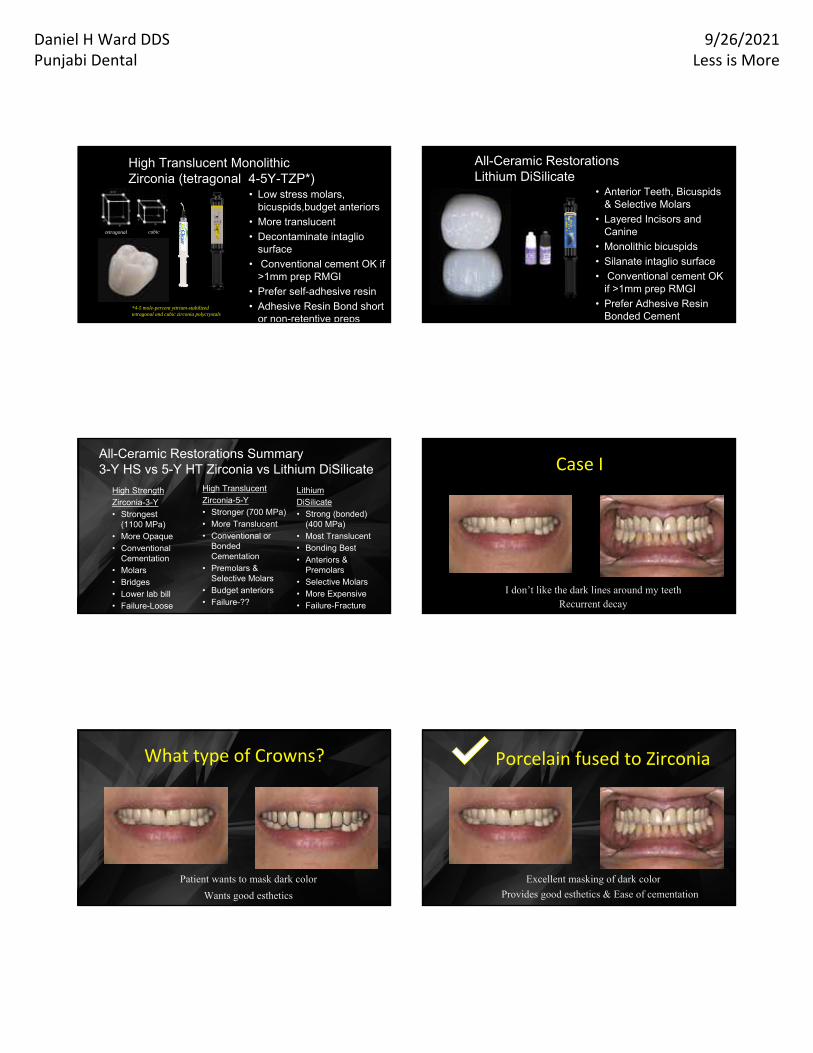
High Translucent Monolithic Zirconia (tetragonal 4-5Y-TZP*)
• Low stress molars, bicuspids,budget anteriors
• More translucent
• Decontaminate intaglio surface
• Conventional cement OK if >1mm prep RMGI
• Prefer self-adhesive resin
• Adhesive Resin Bond short or non-retentive preps
*4-5 mole-percent yttrium-stabilized tetragonal and cubic zirconia polycrystals
tetragonal cubic
All-Ceramic RestorationsLithium DiSilicate
• Anterior Teeth, Bicuspids & Selective Molars
• Layered Incisors and Canine
• Monolithic bicuspids
• Silanate intaglio surface
• Conventional cement OK if >1mm prep RMGI
• Prefer Adhesive Resin Bonded Cement
High Strength Zirconia-3-Y• Strongest
(1100 MPa)• More Opaque• Conventional
Cementation• Molars• Bridges• Lower lab bill• Failure-Loose
All-Ceramic Restorations Summary3-Y HS vs 5-Y HT Zirconia vs Lithium DiSilicate
Lithium DiSilicate• Strong (bonded)
(400 MPa)• Most Translucent• Bonding Best• Anteriors &
Premolars• Selective Molars • More Expensive• Failure-Fracture
High Translucent Zirconia-5-Y• Stronger (700 MPa)• More Translucent• Conventional or
Bonded Cementation
• Premolars & Selective Molars
• Budget anteriors• Failure-??
I don’t like the dark lines around my teethRecurrent decay
Case I
What type of Crowns?
Patient wants to mask dark color
Wants good esthetics
Porcelain fused to Zirconia
Excellent masking of dark color
Provides good esthetics & Ease of cementation
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
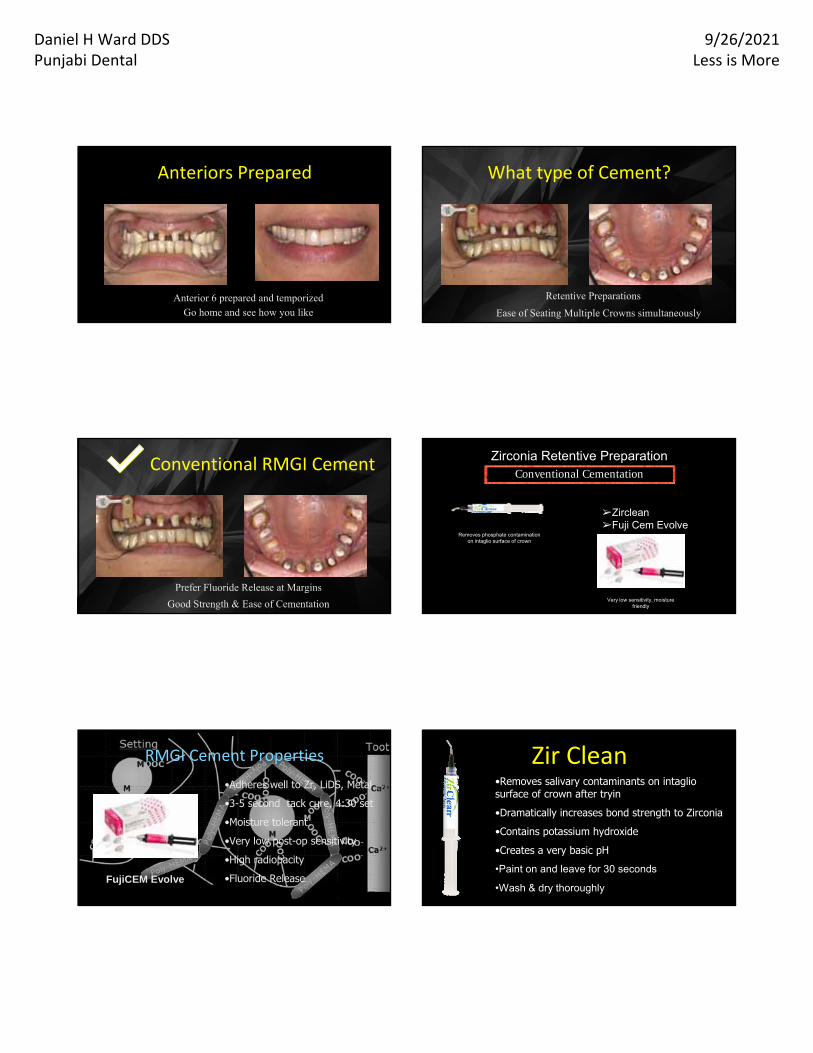
Anterior 6 prepared and temporizedGo home and see how you like
Anteriors Prepared What type of Cement?
Retentive Preparations
Ease of Seating Multiple Crowns simultaneously
Conventional RMGI Cement
Prefer Fluoride Release at Margins
Good Strength & Ease of Cementation
Zirconia Retentive Preparation
➢Zirclean➢Fuji Cem Evolve
Removes phosphate contamination on intaglio surface of crown
Conventional Cementation
Very low sensitivity, moisture friendly
RMGI Cement Properties
FujiCEM Evolve
•Adheres well to Zr, LiDS, Metal
•3-5 second tack cure, 4:30 set
•Moisture tolerant
•Very low post-op sensitivity
•High radiopacity
•Fluoride Release
Zir Clean•Removes salivary contaminants on intaglio surface of crown after tryin
•Dramatically increases bond strength to Zirconia
•Contains potassium hydroxide
•Creates a very basic pH
•Paint on and leave for 30 seconds
•Wash & dry thoroughly
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
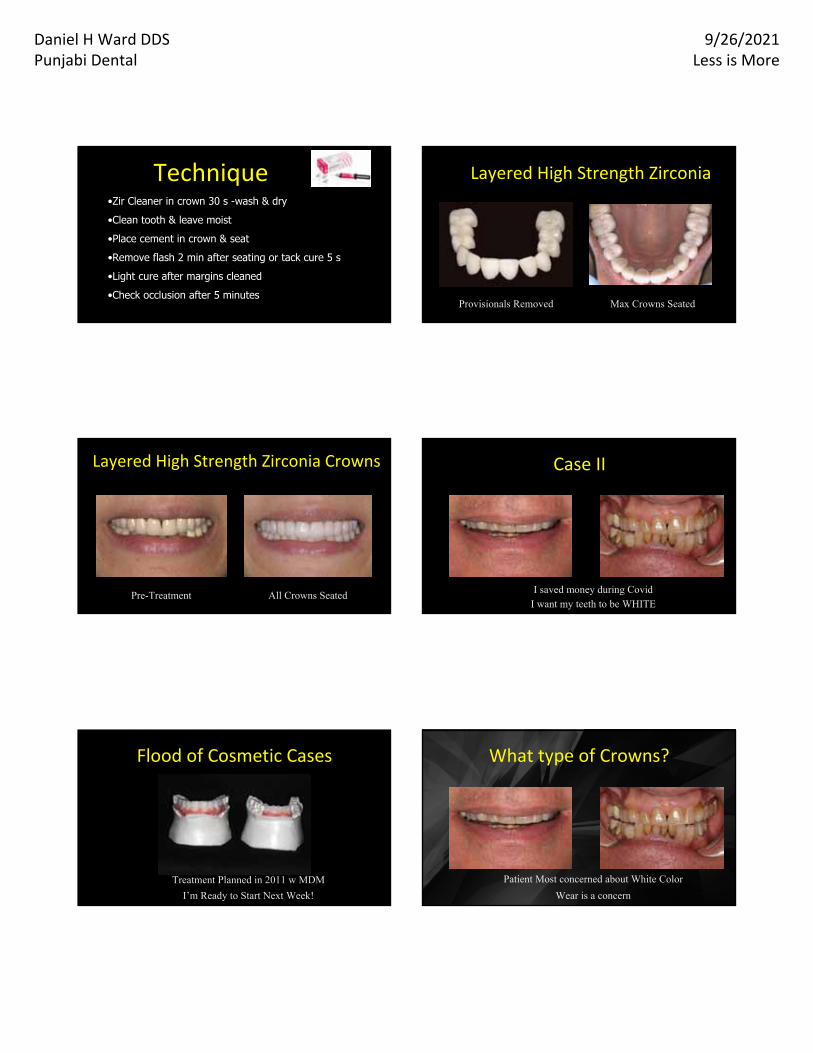
•Zir Cleaner in crown 30 s -wash & dry
•Clean tooth & leave moist
•Place cement in crown & seat
•Remove flash 2 min after seating or tack cure 5 s
•Light cure after margins cleaned
•Check occlusion after 5 minutes
Technique Layered High Strength Zirconia
Provisionals Removed Max Crowns Seated
Layered High Strength Zirconia Crowns
Pre-Treatment All Crowns Seated
Case II
I saved money during CovidI want my teeth to be WHITE
Flood of Cosmetic Cases
Treatment Planned in 2011 w MDM
I’m Ready to Start Next Week!
What type of Crowns?
Patient Most concerned about White Color
Wear is a concern
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
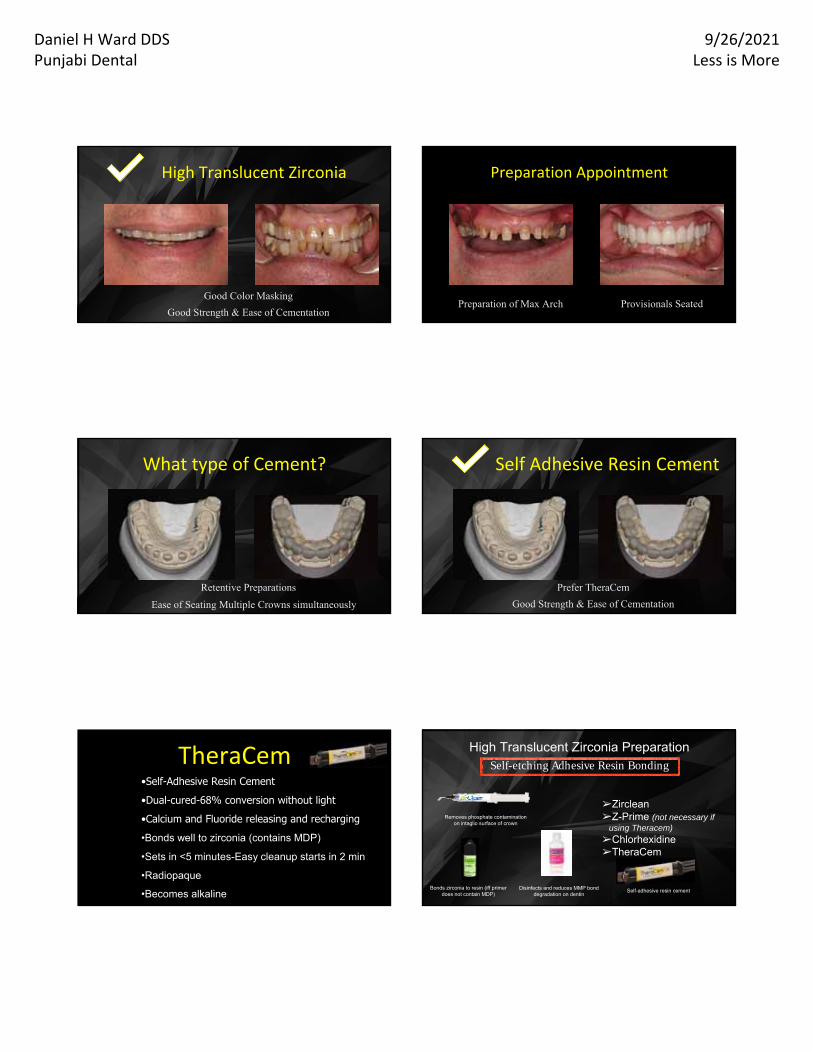
High Translucent Zirconia
Good Color Masking
Good Strength & Ease of Cementation
Preparation Appointment
Preparation of Max Arch Provisionals Seated
What type of Cement?
Retentive Preparations
Ease of Seating Multiple Crowns simultaneously
Self Adhesive Resin Cement
Prefer TheraCem
Good Strength & Ease of Cementation
TheraCem•Self-Adhesive Resin Cement
•Dual-cured-68% conversion without light
•Calcium and Fluoride releasing and recharging
•Bonds well to zirconia (contains MDP)
•Sets in <5 minutes-Easy cleanup starts in 2 min
•Radiopaque
•Becomes alkaline
High Translucent Zirconia Preparation
➢Zirclean➢Z-Prime (not necessary if
using Theracem)
➢Chlorhexidine➢TheraCem
Removes phosphate contamination on intaglio surface of crown
Disinfects and reduces MMP bond degradation on dentin
Self-etching Adhesive Resin Bonding
Bonds zirconia to resin (iff primer does not contain MDP)
Self-adhesive resin cement
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
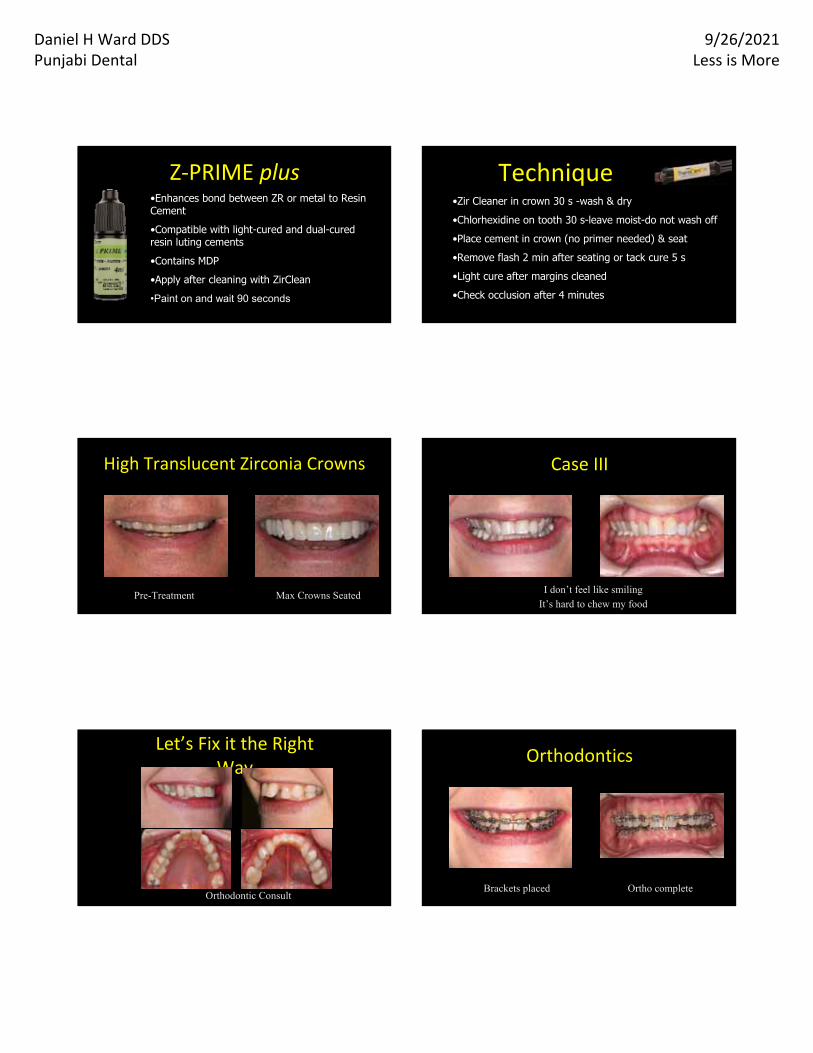
Z‐PRIME plus•Enhances bond between ZR or metal to Resin Cement
•Compatible with light-cured and dual-cured resin luting cements
•Contains MDP
•Apply after cleaning with ZirClean
•Paint on and wait 90 seconds
•Zir Cleaner in crown 30 s -wash & dry
•Chlorhexidine on tooth 30 s-leave moist-do not wash off
•Place cement in crown (no primer needed) & seat
•Remove flash 2 min after seating or tack cure 5 s
•Light cure after margins cleaned
•Check occlusion after 4 minutes
Technique
High Translucent Zirconia Crowns
Pre-Treatment Max Crowns Seated
Case III
I don’t feel like smilingIt’s hard to chew my food
Let’s Fix it the Right Way
Orthodontic Consult
Orthodontics
Brackets placed Ortho complete

Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
Smile Design
RED Proportion Template MDM (Master Diagnostic Model)
What type of Crowns?
Most Interested in Best Esthetics
Appreciates Beautiful Smile
Layered Lithium Disilicate
Best Appearance
Patient is Easy to Work with
Max Preparations
Desired Shade Prep Stump Shade
What type of Cement?
Retentive Preparations
Want to select shade of cement
Adhesive Resin Cement
Prefer Duo-Link w Universal Primer to bond Lithium Disilicate
Superior Strength
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
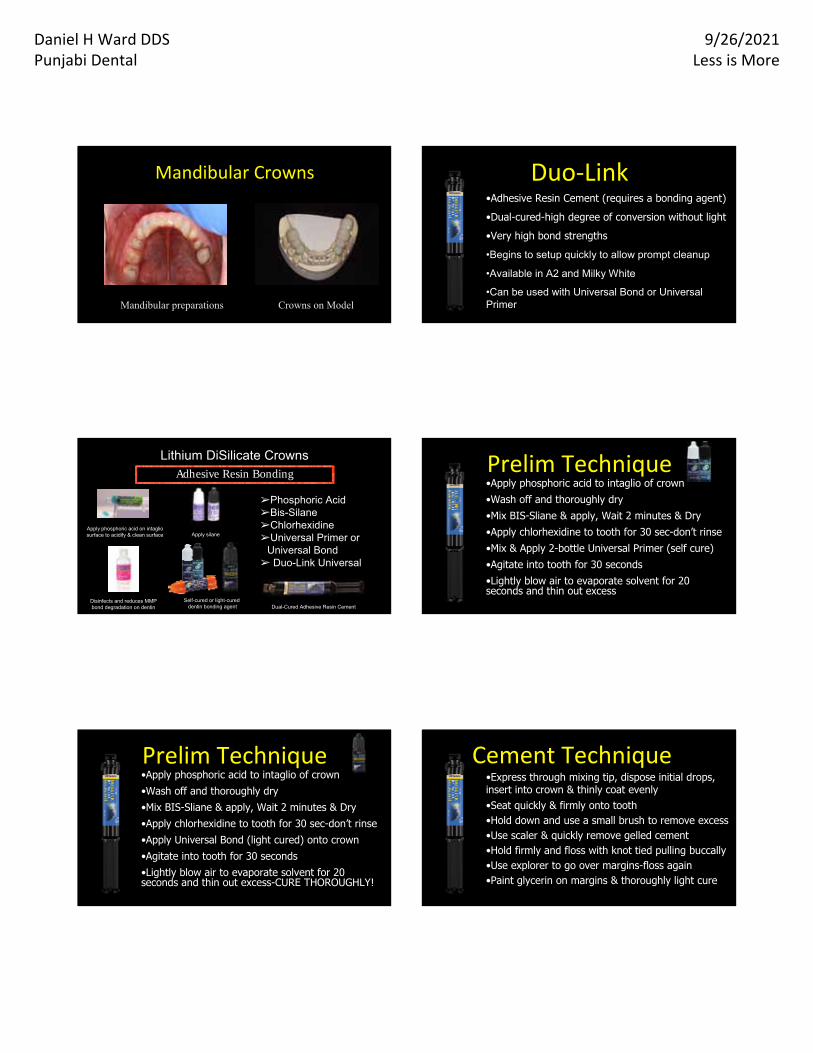
Mandibular Crowns
Mandibular preparations Crowns on Model
Duo‐Link•Adhesive Resin Cement (requires a bonding agent)
•Dual-cured-high degree of conversion without light
•Very high bond strengths
•Begins to setup quickly to allow prompt cleanup
•Available in A2 and Milky White
•Can be used with Universal Bond or Universal Primer
Lithium DiSilicate Crowns
➢Phosphoric Acid➢Bis-Silane➢Chlorhexidine➢Universal Primer or
Universal Bond➢ Duo-Link Universal
Apply phosphoric acid on intaglio surface to acidify & clean surface
Disinfects and reduces MMP bond degradation on dentin
Adhesive Resin Bonding
Apply silane
Self-cured or light-cureddentin bonding agent Dual-Cured Adhesive Resin Cement
Prelim Technique•Apply phosphoric acid to intaglio of crown•Wash off and thoroughly dry•Mix BIS-Sliane & apply, Wait 2 minutes & Dry•Apply chlorhexidine to tooth for 30 sec-don’t rinse•Mix & Apply 2-bottle Universal Primer (self cure)•Agitate into tooth for 30 seconds•Lightly blow air to evaporate solvent for 20 seconds and thin out excess
•Apply phosphoric acid to intaglio of crown•Wash off and thoroughly dry•Mix BIS-Sliane & apply, Wait 2 minutes & Dry•Apply chlorhexidine to tooth for 30 sec-don’t rinse•Apply Universal Bond (light cured) onto crown•Agitate into tooth for 30 seconds •Lightly blow air to evaporate solvent for 20 seconds and thin out excess-CURE THOROUGHLY!
Prelim Technique Cement Technique•Express through mixing tip, dispose initial drops, insert into crown & thinly coat evenly•Seat quickly & firmly onto tooth•Hold down and use a small brush to remove excess•Use scaler & quickly remove gelled cement•Hold firmly and floss with knot tied pulling buccally•Use explorer to go over margins-floss again•Paint glycerin on margins & thoroughly light cure
Daniel H Ward DDSPunjabi Dental
9/26/2021Less is More
Lithium Disilicate Crowns
Pre-Treatment Crowns Seated
Jenny Wohlberg Ceramist
All-Ceramic Results
High Strength Zirconia
High Translucent Zirconia
Lithium Disilicate
You Can Achieve Excellent
WITH SKILL & PLANNING!
E-Mail Questions to:[email protected] Daniel Ward DDS












![Minimally invasive non-surgical vs. surgical approach for ...dictable [12]. More recently, minimally invasive surgical therapy (MIST), modified minimally invasive surgical therapy](https://img.dokumen.tips/doc/110x75/5eddda76ad6a402d6669115c/minimally-invasive-non-surgical-vs-surgical-approach-for-dictable-12-more.jpg)