Embed Size (px)
Citation preview

W
Metastatic Melanoma to the HeartBrian C. Allen, MD,a Tan Lucien Mohammed, MD, FCCP,b Carmela D. Tan, MD,c
Dylan V. Miller, MD,d Eric E. Williamson, MD,e and Jacobo S. Kirsch, MDf
aw
sdrcidmt
lmcaptoi
h
Melanoma is a common neoplasm with a propensity tometastasize to the heart. Although cardiac metastasis israrely diagnosed ante mortem, using a multimodality ap-proach, several imaging findings may be seen. Echocardi-ography is often the initial imaging method used to detectcardiac metastases and their complications. On computedtomography, intraluminal filling defects and myocardial/pericardial nodules may be seen. On magnetic resonanceimaging, metastatic melanoma is classically hyperintenseon T1 images and hypointense on T2 images, a result of theT1 shortening of melanin; however, this is seen in aminority of cases. As melanoma metastases are fluorine-18-fluorodeoxyglucose avid, fluorine-18-fluorodeoxyglu-cose positron emission tomography may also be used todetect cardiac metastases.
Melanoma is a common neoplasm with a propensityto metastasize to the heart. Because of absent ornonspecific signs and symptoms of cardiac involve-ment, most metastases are diagnosed post-mor-tem.1,2 However, with clinical suspicion and using amultimodality imaging approach, several imagingfindings have been described. By the time cardiacmetastasis has been diagnosed, most patients are atan advanced stage of their disease. Not infrequently,however, management may be altered, and surgicaltherapies are available.
From the aDepartment of Radiology, Wake Forest Baptist Medical Center,inston Salem, NC; bImaging Institute, Cleveland Clinic, Cleveland, OH;
cPathology and Laboratory Medicine Institute, Cleveland Clinic, Cleve-land, OH; dDepartment of Pathology, Mayo Clinic, Rochester, MN;eDepartment of Radiology, Mayo Clinic, Rochester, MN; and fImagingInstitute, Cleveland Clinic, Florida, Weston, FL.Reprint requests: Brian C. Allen, MD, Department of Radiology, WakeForest Baptist Medical Center, Medical Center Boulevard, Third FloorMRI, Winston Salem, NC 27157-1088. E-mail: [email protected] Probl Diagn Radiol 2012;41:159-164.© 2012 Mosby, Inc. All rights reserved.0363-0188/$36.00 � 0
tdoi:10.1067/j.cpradiol.2011.09.001
Curr Probl Diagn Radiol, September/October 2012
EpidemiologyMelanoma is a common neoplasm with an annualincidence of 18 per 100,000 inhabitants in the USA.3
There are multiple risk factors for developing cutane-ous melanoma, including Caucasian ethnicity, numer-ous melanocytic nevi, positive family history, andexposure to ultraviolet light.4 Metastasis is common,nd up to 30% of patients with cutaneous melanomaill develop metastatic disease.4
Signs and SymptomsMetastatic cardiac melanoma is most commonly clin-ically silent.5 Signs and symptoms are typically non-pecific and may include those of cardiac failure:yspnea, pedal edema, and cough. Tachycardia, dys-hythmia, and chest pain are also seen. To diagnoseardiac metastatic melanoma, there must be a strongndex of suspicion. If patients have signs of cardiacisease, and a known diagnosis of melanoma, noatter how remote, the suspicion should be raised for
he development of metastasis.5
PathologyMelanoma generally spreads via hematogenous routes,but lymphatic and direct extension of disease are alsoencountered.1 Common metastatic sites include theungs, liver, brain, and osseous structures. Of tumors thatetastasize to the heart, melanoma has the highest rate of
ardiac metastasis, although lung and breast carcinomasre more commonly encountered because of the higherrevalence of these cancers.1,2 Although cardiac metas-asis is rarely diagnosed ante mortem, greater than 50%f patients with metastatic melanoma will have cardiacnvolvement as proven in autopsy series.1,2,6
Cardiac metastases are typically multifocal, given theematogenous spread of disease, may involve any por-
ion of the heart, including the epicardium, myocardium,159

dvoco
160
and pericardium, and may also present as an intracavitarymass.
The pathologic diagnosis of metastatic melanoma tothe heart may be problematic. Cytologic examinationof pericardial fluid may be performed; however, this isfrequently nondiagnostic, as cytology is positive inonly 44%-65% of suspected malignant pericardialeffusions.7 For intraluminal cardiac masses, histologiciagnosis may be obtained by ultrasound-guided trans-enous biopsy. This is a safe and efficient way tobtain tissue, while avoiding a thoracotomy. Compli-ation rates range from 1.17% to 1.67%, less than thatf routine cardiac catheterization.8-10
Imaging FeaturesCardiac metastases are typically accompanied by me-tastases in other organs, such as lung and liver. Whendiagnosed by imaging, metastatic melanoma of theheart is typically a lobular mass that may be intracav-itary or may involve the myocardium or pericardium.The right heart is more commonly involved, comparedto the left heart, possibly because the pulmonarymicrocirculation filters hematogenous spread of tu-mor. A recent review of pathology-proven cases ofmetastatic melanoma to the heart reported that of the 7cases found in a surgical pathology file, 6 casesinvolved the right side of the heart, and only 1involved the left ventricle.11
Ultrasound/EchocardiographyBecause of its high sensitivity and widespread avail-ability, transthoracic echocardiography is often thefirst imaging test performed when cardiac metastasesare suspected, or when nonspecific cardiac findings arepresent on physical examination. Limitations of trans-thoracic echocardiography include limited evaluation
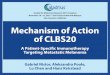
FIG 1. A 56-year-old man with cutaneous melanoma and pathologi-cally proven metastatic melanoma to the right atrial appendage. (A)Transesophageal echocardiogram demonstrates a lobular mass in theright atrial appendage (arrow). (B) Axial, noncardiac-gated, unen-hanced CT was then performed, demonstrating a subtle mass in theright atrial appendage (arrowhead), which would be very difficult toidentify prospectively, given the lack of intravenous contrast. Intrave-nous contrast was not used because of the patient’s renal insufficiency.(C) Fluorine-18-fluorodeoxyglucose positron emission tomography(FDG-PET) demonstrates an FDG avid mass in the right atrial append-
age (arrows). (Color version of figure is available online.)Curr Probl Diagn Radiol, September/October 2012

t
d
frdsodm
ttmFst
of the right ventricle and right atrial appendage, whichare technically challenging because of the substernallocation.12
Transesophageal echocardiography is more sensi-
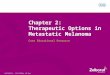
FIG 2. A 78-year-old woman with cutaneous melanoma treated 13years prior, with pathologically proven metastatic melanoma to theright atrium. Intravenous contrast-enhanced axial CT image throughthe heart demonstrates a lobular mass (arrow) within the right atrium,adjacent to the tricuspid valve.
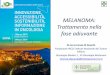
FIG 3. A 53-year-old woman with cutaneous melanoma with dyspneaand pathologically proven metastatic melanoma to the right ventricularoutflow tract. Axial, contrast-enhanced, noncardiac-gated CT imagethrough the pulmonary outflow tract demonstrates triangular soft tissuein the right ventricular outflow tract (arrow).
ive than transthoracic echocardiography and better
Curr Probl Diagn Radiol, September/October 2012
efines lesion size, mobility, and site of attachment.13
The right atrial appendage can also be visualized usingthe transesophageal technique (Fig 1A).13
Common findings of metastatic disease, not specificor melanoma, include dense pericardial bands thateflect inflammation or tumor infiltration. If a massistends the right ventricle, exaggerated paradoxicaleptal motion may be seen. Mitral valve prolapse mayccur when tumors infiltrate the ventricular wall andisrupt normal systolic motion, or when papillaryuscles are involved.12
Computed TomographyComputed tomography (CT) is generally used as astaging examination of the chest, abdomen, and pelvis.The overall sensitivity of CT for metastatic melanomais 58% and the specificity is nearly 70%.14 Althoughhe sensitivity of cardiac metastatic melanoma is low,here are findings that can lead to the diagnosis ofetastatic melanoma on a screening CT examination.or example, although a pericardial effusion is non-pecific, a hemorrhagic pericardial effusion is sugges-ive of a malignant effusion.15 The presence of a
pericardial effusion should heighten scrutiny of thepericardium and myocardium.
Intravenous contrast is essential, as the conspicuity
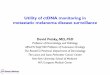
FIG 4. A 66-year-old man with cutaneous melanoma and metastaticmelanoma to the interventricular septum and left lateral free wall.Axial, electrocardiogram-gated, contrast-enhanced CT image of theheart demonstrates focal thickening (arrow) within the interventricularseptum, higher in attenuation than the adjacent myocardium. Asecond, similar-appearing lesion is noted in the myocardium of thelateral free wall of the left ventricle (arrowhead).
of intracardiac and myocardial lesions may be in-
161

mcm
va1mm
sc
ove.
creased when surrounding blood and myocardium areenhanced (Figs 1B, 2, and 3).16 When cardiac involve-
ent is suspected, an electrocardiogram-gated andontrast-enhanced CT is recommended, as sensitivityay be increased (Figs 4, 5, and 6A).17 On CT,
cardiac masses typically enhance and are commonlylobular. They may be intracavitary, myocardial, orpericardial in location (Figs 1-6).
Magnetic Resonance ImagingMagnetic resonance imaging (MRI) is advantageous
FIG 5. A 53-year-old woman with cutaneous melanoma treated 8Electrocardiogram-gated, contrast-enhanced CT demonstrates lobularaxial (A) and coronal (B) images. (C) Axial steady-state free precessionaxis of the heart demonstrates a lobular mass (arrowhead), slightly hyprecovery MR (repetition time msec/echo time msec/inversion timhyperintense, lobular soft tissue (arrowhead) in the atrioventricular gro
because of its superior contrast resolution. MRI pro-
162
ides high-resolution anatomic detail and may clarifynatomic relationships better than ultrasound (FigsA, 5, and 6).18 Tumor extent may better be deter-ined, and surgical/ablative planning is often easier asultiplanar imaging is performed.19
Because melanin is a natural paramagnetic sub-tance and causes T1 shortening, melanoma is classi-ally T1 hyperintense and T2 hypointense.20 However,
only a minority of melanoma metastases demonstratethese classic findings.19,21 T1 signal may be related toactual melanin content in the metastatic deposit.22
Amelanotic melanoma, with less melanin than typical
rs prior, with metastatic melanoma to the atrioventricular groove.issue (arrow) encasing the right coronary artery (arrowhead) on bothrepetition msec/echo time msec, 3.1/1.4) through the horizontal longnse compared to adjacent myocardium. (D) Sagittal double inversion
ec, 1714/67/150) through the aortic root demonstrates slightly
yeasoft tMRI (erintee ms
melanoma, does not share these typical features and
Curr Probl Diagn Radiol, September/October 2012

a
bbdadaactt
Curr Probl Diagn Radiol, September/October 2012
may be isointense to hypointense on T1-weightedimaging (Figs 5 and 6).19 Recently, melanin inversionrecovery imaging has been suggested when metastaticmelanoma is questioned. To achieve this, a standardinversion recovery sequence with an inversion time of200 ms has been described.20 Melanoma will alsodemonstrate diffuse, avid enhancement following in-travenous gadolinium-contrast administration.20
Positron Emission TomographyFluorine-18-fluorodeoxyglucose positron emission to-mography (FDG-PET) is an excellent tool for wholebody staging of melanoma. National guidelines fromthe United States Department of Health and HumanServices recommend FDG-PET for whole body stag-ing in high-risk patients with potentially surgicallyresectable disease.23 The main advantage is in itsbility to detect or exclude distant metastases.24 FDG-
PET/CT is more accurate than FDG-PET or CT alonewith a sensitivity of 98.7% vs 88.9% and 69.7%,respectively.24 Strobel et al. have suggested that sen-sitivity may be improved with a combined, dedicateddiagnostic CT readout, in addition to the FDG-PET/CT. Sensitivity increased from 85% to 98% in wholebody imaging and specificity remained stable, decreas-ing only slightly from 96% to 94%.25
Metastatic deposits are typically FDG avid, but maye difficult to localize because of the inherent meta-olically active myocardium (Figs 1C and 6C). Car-iac uptake is variable not only from 1 patient tonother, but even in the same patient imaged onifferent occasions. Uptake can differ in both the leftnd the right ventricle and can range from backgroundctivity to intense, diffuse accumulation.26,27 For on-ological imaging, to minimize cardiac activity, pa-ients should fast 4-6 hours before FDG administra-ion.27 Pitfalls may include mis-coregistration and
non- or only mildly FDG avid lesions.
FIG 6. A 43-year-old woman with cutaneous melanoma and meta-static melanoma to the right atrium. (A) Axial, electrocardiogram-gated, contrast-enhanced CT through the heart demonstrates lobularsoft tissue (arrow) in the right atrium. (B) Axial steady-state freeprecession MR (repetition time msec/echo time msec, 3.1/1.4)through the heart demonstrates a lobular right atrial nodule (arrow),slightly hyperintense to adjacent myocardium. (C) Fused fluorine-18FDG-PET/CT image through the heart demonstrates a focus of hyper-metabolism (arrow) corresponding to the soft-tissue nodule. (Color
version of figure is available online.)163

im
2
2
2
2
2
TreatmentIn the majority of cases, cardiac metastases occur inpatients with advanced tumor burden and diffusemetastatic involvement, which typically excludes pa-tients from aggressive surgical management. For aminority of patients, surgical resection may be anoption, typically employed to prevent rapid cardiacdecompensation or to reduce tumor burden for subse-quent chemotherapy.28 Patients with limited systemicnvolvement or those with an indolent clinical courseay also benefit from surgical resection.
ConclusionsMelanoma is a common neoplasm with a high propen-sity for metastasizing to the heart. Because patients’signs and symptoms are often nonspecific, clinicalsuspicion is paramount. Echocardiography is often theinitial imaging modality. CT, MRI, and FDG-PETmay also be used to detect and define cardiac involve-ment.
REFERENCES1. Young JM, Goldman IR. Tumor metastasis to the heart.
Circulation 1954;9:220-9.2. Glancy DL, Roberts WC. The heart in malignant melanoma. A
study of 70 autopsy cases. Am J Cardiol 1968;21:555-71.3. Garbe C, Leiter U. Melanoma epidemiology and trends. Clin
Dermatol 2009;27:3-9.4. NIH Consensus Conference. Diagnosis and treatment of early
melanoma. JAMA 1992;268:1314-9.5. Bortolotti U, Tursi V, Milano A, et al. Intracardiac metastatic
melanoma: Report of a case mimicking a right atrial myxoma,with a review of the literature. Tex Heart Inst J 1990;17:136-8.
6. Liébana ES, González DJ, Martín M, et al. Atypical presen-tation of cardiac metastasis of amelanotic melanoma. IntJ Cardiovasc Imaging 2009;25:343-4.
7. Wilkes JD, Fidias P, Vaickus L, et al. Malignancy-relatedpericardial effusion. 127 cases from the Roswell Park CancerInstitute. Cancer 1995;76:1377-87.
8. Savoia P, Fierro MT, Zaccagna A, Bernengo MG. Metastaticmelanoma of the heart. J Surg Oncol 2000;75:203-7.
9. Malouf JF, Thompson RC, Maples WJ, Wolfe JT. Diagnosisof right atrial metastatic melanoma by transesophageal echo-cardiographic-guided transvenous biopsy. Mayo Clin Proc1996;71:1167-70.
10. Deckers JW, Hare JM, Baughman KL. Complications oftransvenous right ventricular endomyocardial biopsy in adultpatients with cardiomyopathy: A seven-year survey of 546consecutive diagnostic procedures in a tertiary referral center.J Am Coll Cardiol 1992;19:43-7.
11. Wood A, Markovic SN, Best PJ, et al. Metastatic malignantmelanoma manifesting as an intracardiac mass. Cardiovasc
Pathol 2010;19:153-7.164
12. Ports TA, Schiller NB, Strunk BL. Echocardiography of rightventricular tumors. Circulation 1977;56:439-47.
13. Obeid AI, al Mudamgha A, Smulyan H. Diagnosis of rightatrial mass lesions by transesophageal and transthoracic echo-cardiography. Chest 1993;103:1447-51.
14. Swetter SM, Carroll LA, Johnson DL, Segall GM. Positronemission tomography is superior to computed tomography formetastatic detection in melanoma patients. Ann Surg Oncol2002;9:646-53.
15. Díaz ML, Villanueva A, Bastarrika G, et al. Non-electrocar-diogram-gated multidetector-row computed tomography find-ings of cardiac pathology in oncologic patients. Curr ProblDiagn Radiol 2009;38:206-17.
16. Burn PR, Chinn R, King DM. Right atrial metastatic mela-noma detected by dynamic contrast enhanced spiral CT. Br JRadiol 1999;72:395-6.
17. Bleiweis MS, Georgiou D, Brundage BH. Detection of intra-cardiac masses by ultrafast computed tomography. Am J CardImaging 1994;8:63-8.
18. Freedberg RS, Kronzon I, Rumancik WM, et al. The contri-bution of magnetic resonance imaging to the evaluation ofintracardiac tumors diagnosed by echocardiography. Circula-tion 1988;77:96-103.
19. Mousseaux E, Meunier P, Azancott S, et al. Cardiac metastaticmelanoma investigated by magnetic resonance imaging. MagnReson Imaging 1998;16:91-5.
20. Crean AM, Juli C. Diagnosis of metastatic melanoma to theheart with an intrinsic contrast approach using melanin inver-sion recovery imaging. J Comput Assist Tomogr 2007;31:924-30.
21. Isiklar I, Leeds NE, Fuller GN, et al. Intracranial metastaticmelanoma: Correlation between MR imaging characteristicsand melanin content. AJR 1995;165:1503-12.
22. Premkumar A, Marincola F, Taubenberger J, et al. Metastaticmelanoma: Correlation of MRI characteristics and histopa-thology. J Magn Reson Imaging 1996;6:190-4.
23. National Guideline C; PET imaging in melanoma: Recom-mendations. http://www.guideline.gov. Accessed 9/1/2011.
4. Reinhardt MJ, Joe AY, Jaeger U et al. Diagnostic performanceof whole body dual modality 18F-FDG PET/CT imaging forN- and M-staging of malignant melanoma: Experience with250 consecutive patients. J Clin Oncol 2006;24:1178-87.
5. Strobel K, Dummer R, Husarik DB, et al. High-riskmelanoma: Accuracy of FDG PET/CT with added CT mor-phologic information for detection of metastases. Radiology2007;244:566-74.
6. Orcurto MV, Delaloye AB, Letovanec I, et al. Detection of anasymptomatic right-ventricle cardiac metastasis from a small-cell lung cancer by F-18-FDG PET/CT. J Thorac Oncol2009;4:127-30.
7. Rosenbaum SJ, Lind T, Antoch G, et al. False-positive FDGPET uptake—The role of PET/CT. Eur Radiol 2006;16:1054-65.
8. Houmsse M, Raman SV, Leier CV, et al. Metastatic mela-noma of the left ventricle: Cardiac imaging in the diagnosisand surgical approach. Int J Cardiovasc Imaging 2004;20:
523-6 [Discussion 527-8].Curr Probl Diagn Radiol, September/October 2012