Embed Size (px)
Citation preview

Breast
Metastatic disease of the breast and local recurrence of breast cancerDeborah M Clements
Philip a Holland
Abstractthe two main aims of the treatment of early breast cancer are to achieve
control of locoregional disease and to treat micrometastatic disease. Pa-
tients often have micrometastatic disease at presentation, but many sub-
jects can be potentially cured by locoregional treatment alone. Prevention
of local recurrence is important. a small percentage of patients develop
metastases from a local recurrence which would not otherwise have
occurred. Local recurrence of breast cancer should occur in <10% of cases
within 10 years of surgery with adequate local and systemic therapies. about
35% of breast cancer cases develop metastatic disease within 10 years of
surgery. Patients with local recurrence in the breast or chest wall may sur-
vive long term with appropriate locoregional therapy. Metastatic breast can-
cer is incurable, but long-term and worthwhile short-term responses can be
achieved by appropriate treatment. some patients with hormone-sensitive
disease survive many years after sequential hormone manipulation. Patients
with hormone-insensitive disease have much shorter survival. In all cases of
recurrent or metastatic disease, a multidisciplinary approach is required to
achieve the primary goal of management: maximize the quality of life with
palliation of symptoms without unnecessary side effects.
Keywords breast cancer; local recurrence; metastatic disease
Local recurrence of breast cancer: basic principles
Local recurrence of breast cancer is recurrent malignancy in the skin or parenchyma of the conserved breast, or skin flaps or scar after mastectomy. Local recurrence represents failure of local therapy. The best form of treatment is prevention i.e. ensuring that initial local treatment is optimal. Local disease can be isolated, but up to 50% of patients have associated systemic relapse. Patients with local recurrence should be fully staged to look for distant metastases because this influences management. Local recurrence is often responsive to therapy, but prognosis depends upon the type and timing of recurrence. Patients with localized recurrences in the breast or chest wall may survive long term if appropriate therapy is instituted. Early local recurrence (<5 years) is associated with an overall poor prognosis.
Deborah M Clements MRCS is a Specialist Registrar in General Surgery
at Royal Gwent Hospital, Newport, UK. Conflicts of interest:
none declared.
Philip A Holland FRCS is a Consultant General and Endocrine Surgeon
at Royal Gwent Hospital, Newport, UK. Conflicts of interest:
none declared.
sUrGerY 25:6 27
Local recurrence after mastectomy
Risk factors include: • high nuclear grade • lymphovascular invasion • heavy node positivity • large tumour size. For patients with these risk factors, radiotherapy to the chest wall soon after surgery reduces the risk of local recurrence.
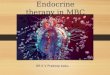
Types of local recurrence • Single-spot recurrences tend to occur late and are not predic-tive of a poor prognosis. • Multiple-spot relapse • Widespread field change recurrence tends to occur early and is associated with a very poor prognosis (Figure 1).
Diagnosis: depending upon the site, local recurrence can be con-firmed by fine-needle aspiration cytology (see Mitchard, CROSS REFERENCES) or biopsy (core, punch).
Treatment of local recurrence without confirmed metastases: surgery alone can provide long-term control if recurrence is focal and occurs many years after mastectomy. If the disease-free interval is short, surgery could be combined with radiotherapy (if not already given) and a change in hormonal therapy (for oestro-gen receptor-positive tumours). Treatment options for multifocal recurrence include: • radiotherapy • more radical excision ± myocutaneous flap • change in hormonal therapy • topical cytotoxic agents. Widespread recurrence is difficult to treat and standard treat-ments are often disappointing. Options include radiotherapy at a high skin dose, intra-arterial chemotherapy and systemic therapy (hormonal or chemotherapy).
Excision of dead tissue, antibiotics (topical, per ora) with anaerobic activity combined with charcoal dressings help to control malodour in locally advanced cases that have progressed to ulceration.
Figure 1 Widespread recurrence of breast cancer after left mastectomy.
6 © 2007 elsevier Ltd. all rights reserved.

Breast
Local recurrence after breast-conserving surgery
The aim of breast-conserving surgery is to preserve a cosmetically acceptable breast while ensuring low rates of local recurrence. Early local recurrence represents significant failure of local treat-ment. Successful treatment depends on adequate surgical excision that leaves minimal residual disease in the breast, which can then be controlled by acceptable doses of radiation (see Falk, CROSS REFERENCES). Patients with close or involved margins require re-excision or mastectomy to ensure clear margins. Without radiother-apy, local recurrence can be expected in up to 40% of cases; after radiotherapy, local recurrences may continue to appear for at least five years, after which new primary tumours predominate. Concur-rent adjuvant systemic treatment (see ‘Adjuvant therapy for breast cancer’, page 272) further reduces the risk of local recurrence.
Risk factors for local recurrence after breast-conserving surgery are listed in Table 1.
Presentation: local recurrence is usually localized in the region of the initial excision of tumour, but some recurrences are diffuse or involve the skin, which sometimes presents with inflamma-tion. Local recurrence may be detected clinically or by surveil-lance mammography. The diagnosis is confirmed by core biopsy, which is guided by ultrasound if the lesion is impalpable.
Treatment of local recurrence after breast-conserving surgery in the absence of metastatic disease is usually mastectomy ± change in systemic therapy.
Axillary recurrence
Level-III axillary dissection is associated with recurrence rates of <2% at ten years, but represents overtreatment for node- negative cancers. Operable recurrences after axillary sampling or sentinel node biopsy should be excised and combined with level-III axillary dissection. Inoperable axillary recurrence is uncommon, but can be associated with axillary vein thrombosis, lymphoedema and brachial plexus infiltration. Palliative radio-therapy ±systemic therapy may be helpful, but rarely produces longlasting control of the disease.
Metastatic breast cancer
Metastatic breast cancer usually presents as a distant recur-rence from a previously treated cancer of the breast. A minority
Risk factors for local recurrence after breast-conserving surgery
Certain Less certain
Involved surgical margins Lymphovascular invasion
Young age High grade of tumour
No radiotherapy extensive intraductal component
Multicentric disease
Table 1
sUrGerY 25:6 27
of patients with breast cancer have metastatic disease at initial presentation. Breast cancer produces a variable natural course and effect on survival when it metastasizes compared to other cancers that metastasize. There is no evidence that detecting and treating asymptomatic metastases improves survival. Metastatic breast cancer is incurable, but long-term and worthwhile short-term responses can be achieved by appropriate treatment. Some patients with hormone-sensitive disease survive many years after sequential hormone manipulation; patients with hormone-insensitive disease have much shorter survivals. Patients with a long disease-free interval (>2 years after primary diagnosis) and favourable sites of recurrence survive much longer than patients who have a short disease-free interval or recurrence at other sites (e.g. lung, liver, brain). The median survival from symptomatic metastatic breast cancer is 2–3 years.
A multidisciplinary approach is required to achieve the primary goal of management i.e. maximize quality of life with palliation of symptoms without unnecessary side effects. Local or distant recurrent disease is extremely distressing; patients should have access to appropriate support and the local Palliative Care Team.
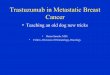
Sites of metastasesCommon sites for metastatic disease include bone (Figure 2), lung, liver and brain. Lobular cancers have a propensity to meta-stasize to the skin, gastrointestinal tract, gynaecological organs, meninges, peritoneum and retroperitoneum. Lobular cancers can cause a retroperitoneal type syndrome with hydronephrosis, but without hydroureter. Gastrointestinal involvement can produce a linitis plastica-type appearance of the stomach.
Presentation of metastatic diseaseThe presentation of metastatic disease is variable and depends upon the volume and site of the disease. Initially, the symptoms may be non-specific (weight loss, anorexia, nausea). More spe-cific symptoms or signs that may suggest the site of metastasis include headache, bone pain, breathlessness or jaundice.
Investigations in patients with known or suspected metastatic diseaseRoutine and selective investigations are shown in Table 2.
TreatmentSystemic therapy (endocrine therapy, chemotherapy, immuno-therapy) is first-line treatment, and choice depends on: • biology of the disease • status of the oestrogen receptor • status of human epidermal growth factor receptor-2 (HER2) • site of metastases • age • fitness. In general, endocrine therapy is slower at inducing a response but, once a response is induced, it can be sustained for longer. Chemotherapy induces a response more rapidly, but the duration of response is shorter than that seen with endocrine therapy.
In general: • good prognosis and oestrogen receptor-positive disease is best
treated by hormonal treatment • poor prognosis and oestrogen receptor-negative disease
usually requires chemotherapy
7 © 2007 elsevier Ltd. all rights reserved.

Breast
Figure 2 appearance of bone metastases shown by bone
scintigraphy. Hotspots in the thoracolumbar spine, ribs,
right shoulder and pelvis are observed.
Investigations for metastatic disease
Routine
• Primary cancer details (histological type, grade, receptors
(oestrogen, progesterone, Her2)
• Blood tests (full blood count, liver function tests, bone
profile, tumour markers (e.g. Ca15.3, carcinoembryonic
antigen)
• Chest radiograph
• Bone scintigraphy (Figure 2) plus plain radiographs of
symptomatic areas or hotspots
• Ultrasound of liver
Selective use
• Ct of chest, abdomen or head
• MrI of spine to detect marrow infiltration when radiographs
and bone scintigraphy may be normal/equivocal or if a
solitary hotspot is found on bone scintigraphy
• aspiration of pleural effusion or ascites
• In most cases a diagnosis can be made using non-invasive
tests, but a biopsy of a suspected area is done occasionally
Table 2
sUrGerY 25:6 27
• endocrine therapy causes fewer side effects than chemotherapy, but troublesome symptoms can occur.
Endocrine treatment: objective responses to endocrine agents are seen in 30% of all patients and 50–60% of those with oes-trogen receptor-positive tumours. Response rates for second-line agents are ≈25%, and for third-line agents 10–15%. Aromatase inhibitors are more efficacious and better tolerated than tamoxi-fen in postmenopausal women.
Options for premenopausal women with oestrogen receptor-positive tumours • First-line treatments—tamoxifen alone or in combina-tion with a luteinizing hormone-releasing hormone (LHRH) analogue. • Second-line treatments after tamoxifen—LHRH analogue alone or in combination with an aromatase inhibitor (LHRH analogue leads to postmenopausal hormone status).
Options for postmenopausal women with oestrogen receptor-positive tumours • First-line treatments—non-steroidal aromatase inhibitors (e.g. letrozole or anastrozole). • Second-line treatments—tamoxifen, pure antioestrogen (fulvestrant). • Third-line treatments—pure antioestrogen, steroidal aro-matase inhibitors (exemestane), tamoxifen, megoestrol acetate, medroxyprogesterone acetate.
Chemotherapy: the side effects of treatment are undesirable, but intensive chemotherapy regimens are associated with the highest response rates, improved quality of life and improved survival compared with less intensive regimens. Overall response rates to chemotherapy are 40–60% with a median time to relapse of 6–10 months. Subsequent courses of chemotherapy have a response rate of <25%.
Until very recently, most oncologists used an anthracy-cline-containing regimen in the adjuvant setting i.e. 6 cycles of 5-fluorouracil, epirubicin, cyclophosphamide (FEC). Guidance by the National Institute for Health and Clinical Excellence (NICE) published in 2006 resulted in a change of practice. FEC is used for grade-3 node-negative cancers, but patients with node-positive cancers now receive 3 cycles of FEC followed by 3 cycles of the taxane docetaxel. Chemotherapy is also used in the metastatic setting but regimens cannot be repeated. • First-line chemotherapy (no previous chemotherapy)— anthracycline containing regime (e.g. FEC). • First-line chemotherapy (previous anthracycline therapy given)—taxane (e.g. docetaxel). • Second-line chemotherapy—capecitabine, vinorelbine (p.o.).
Immunotherapy: between 25% and 30% of breast cancers over-express the oncoprotein HER2. The humanized murine antibody trastuzumab has antitumour activity against cells that over-express HER2. Trastuzumab is licensed, in combination with a taxane, for metastatic breast cancer in patients with HER2- positive tumours who have not received chemotherapy for met-astatic breast cancer, and in whom anthracycline treatment is inappropriate. It is also licensed as monotherapy in patients who have received at least two chemotherapy regimens including, where appropriate, an anthracycline and a taxane. Compared
8 © 2007 elsevier Ltd. all rights reserved.

Breast
to paclitaxel alone, the addition of trastuzumab to paclitaxel significantly increases the: • median time to disease progression • median time to treatment failure • median duration of response • complete and partial responses. Treatment is given intravenously at three-weekly intervals and continues until resistance to treatment is apparent. Trastuzumab is associated with cardiotoxicity and cardiac failure (particularly if used with an anthracycline) and candidates should undergo careful cardiac assessment and monitoring (see Arrowsmith, CROSS REFERENCES). Patients responding to trastuzumab appear to have a higher incidence of symptomatic brain meta-stases. The improved survival achieved with trastuzumab (which does not cross the blood–brain barrier) may allow brain meta-stases enough time to develop and become clinically evident.
Other palliative treatments for specific problems • Pain control using analgesics and nerve blocks where appro-priate. Localized bone pain should be treated by radiotherapy: a single dose is often sufficient. Analgesics combined with bisphosphonates are the mainstay of treatment for more wide-spread bone pain. • Orthopaedic surgery. Pathological fractures should be antici-pated and avoided if possible. Wider use of bisphosphonates has greatly reduced bone-related complications (e.g. pain, hypercalcae-mia, fractures). Established fractures are treated by surgical fixation and radiotherapy. Prophylactic surgery should be considered if metastases occur in weightbearing areas (e.g. neck or shaft of femur). • Drainage of ascites, drainage of pleural effusion combined with chemical or surgical pleurodesis.
sUrGerY 25:6 27
• Treatment of brain metastases with corticosteroids and whole-brain radiotherapy.
Assessment of response to treatmentSubjective measurements include assessment of symptoms such as general wellbeing, anorexia, nausea, pain and mobility. Improve-ment in symptoms may not correlate with an objective response.
Objective measurements may include monitoring of tumour markers, bone profile or liver function tests depending upon the disease pattern. The criteria for objective assessment by clinical and/or radiological measurements of tumours are laid down by the International Union Against Cancer. The response categories are complete response, partial response, stable disease and progressive disease. ◆
CRoSS ReFeRenCeS
arrowsmith Je, Dawson aJ. advanced cardiovascular monitoring. Surgery
2006; 24(10): 333–6.
Falk s. Principles of cancer treatment by radiotherapy. Surgery 2006;
24(2): 62–5.
Mitchard Jr, romain Ke, shepherd Na. Principles and techniques of
biopsy with special reference to fine-needle aspiration cytology.
Surgery 2005; 23(2): 43–7.
FuRTheR ReAdIng
Dixon M. aBC of breast diseases, 3rd edn. Oxford: Blackwell, 2006.
NICe technology appraisal guidance 109. Docetaxel for the adjuvant
treatment of early node-positive breast cancer. september 2006.
www.nice.org.uk / TA109
9 © 2007 elsevier Ltd. all rights reserved.