Embed Size (px)
Citation preview
Thorax (1966), 21, 437.
Metastatic carcinoma of the pleuraP C. MEYER
From the Central Histological Laboratory, Whittington Hospital, London, N.19
Pleural secondaries are a frequent finding atnecropsy in cases of carcinomatosis, and theirpresence is of such prognostic significance thatmuch effort has been made in the field of diag-nostic cytology as applied to the examination ofserous effusions (Foot, 1954; Luse and Reagan,1954a and b; Papanicolaou, 1954; Leuallen andCarr, 1955; Foot, 1956; Myerson, 1956). Therelevant literature has been well reviewed bySpriggs (1957), and a less critical view of theinvestigation is now accepted (Naylor andSchmidt, 1964) than that adopted by Scadding(1955). In recent years special interest has beenshown in the cytological diagnosis of pleuralmesotheliomas (Klempman, 1962; Manguikianand Prior, 1963; Naylor, 1963) out of all propor-tion to the incidence of this condition.The subject of pleural involvement by secon-
dary carcinoma is only briefly mentioned bySpencer (1962), and yet it is of interest since itspathogenesis and the factors influencing theappearance of effusions are poorly understood.
It appeared that a study of necropsy materialin this department would be worth while, althoughcytological material obtained during life wasavailable in only a few of the cases.
METHOD OF STUDY
The histological files of this department containnecropsy material from 52 examples of metastaticcarcinoma of the pleura obtained between theyears 1960 and 1964 inclusive. In each case theanatomical extent of the pleural metastases, theorigin and structure of the tumour, the precisenature of the pleural involvement, and thepresence of inflammation and fibrosis were re-corded together with alterations of the surfaceendothelium and changes in adjacent lung paren-chyma. The distribution and extent of lymphaticmetastases and the presence of hepatic metastaseswere also noted. Serous effusions were examinedduring life in 14 cases and the cytological findingswere reviewed.
RESULTS
Table I shows the distribution of the primarytumours together with the respective cases show-ing visceral pleural involvement only, parietalinvolvement only, and involvement of both layers.
TABLE IDISTRIBUTION OF CASES IN PRESENT SERIES
Pleural InvolvementSite of Primary
Tumour Visceral Parietal and Parietal
Bronchus 3 - 26Breast .. . 5 - 4Pancreas 2 _ 2Stomach.. . 414Caecum. I..Gall-bladder I -
Prostate .. . _Ovary :1. .Unknown .T .. 53
Total ..| 15 136
Table II shows the distribution of the primarytumours in the cases associated with hepaticmetastases. In Table III the cases of bronchialorigin are sub-divided into four groups accord-ing to the presence of unilateral or bilateralpleural involvement and the presence or absenceof hepatic metastases. Table IV shows the distri-bution of the histological types in the 29 casesof bronchial carcinoma. Various aspects ofpleural involvement are illustrated in Figs 1 to 6and are discussed below.
DISCUSSION
In the present series more than half the examplesare of bronchial origin, and the pleural meta-stases must be accepted as usually arising frompulmonary arterial tumour emboli, a fact ofinterest since the importance of arterial invasionby bronchial carcinoma has only fairly recentlybeen recognized (Ballantyne, Clagett, and Mc-Donald, 1957; Pryce and Walter, 1960). Although
437
P. C. Meyer
TABLE IIDISTRIBUTION OF PRIMARY TUMOURS IN CASES
ASSOCIATED WITH HEPATIC METASTASES
Pleural InvolvementSite of Primary
Tumour Visceral Parietal Visceraland Parietal
Bronchus I. 1 - f 12Breast ... .. 5 -22Pancreas 2 _ 2Stomach.. . 31 1 -Caecum .. ..Gall-bladder . . lProstate I1Ovary . .. 04Unknown ..
Total .. 12 1 19
One case of gastric carcinoma unassociated with hepatic secon-daries was an example of retrograde lymphatic spread to the pleura.
2 One case of mammary carcinoma unassociated with hepaticsecondaries was an example of direct neoplastic spread through thechest wall.
I Another case of mammary carcinoma similar to that mentionedabove.
^ The single case of ovarian carcinoma was an example of directneoplastic spread through the diaphragm.
the total number of cases is small, a study ofTable IV indicates that this tendency to pulmon-ary arterial invasion is not the property of aparticular histological type, since the proportionof oat-celled carcinomata (11 out of 29 cases) isin accord with the published figures for theincidence of this type in two large series (Brysonand Spencer (1951) 36-0%; Walter and Pryce(1955) 37-1%). A study of the present materialshowed no evidence that focal pleural secondarieshad arisen by lymphatic permeation of the lungparenchyma, except in peripheral tumours andwhere bronchial carcinomata were accompaniedby very extensive parenchymal and centrifugalperibronchial infiltration.
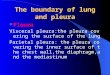
Bilateral pleural involvement by bronchialcarcinoma is clearly related to the presence ofhepatic metastases, consistent with the occurrenceof parenchymal secondaries in the opposite lung.This interpretation of the results shown in TableIII is strengthened by the fact that, of the threecases without hepatic involvement, one was anexample of retrograde lymphatic spread frominfiltrated mediastinal glands (Fig. 1) while an-other was an example of alveolar cell carcinomawith primary foci in both lungs.
Pleural metastases from other primary sites areusually a manifestation of tertiary spread fromestablished hepatic secondaries, a relationshipestablished in Table II. In only one case of mam-mary carcinoma was there evidence of directspread through the chest wall to the parietalpleura, but in two larger series this factor was
TABLE IIIANALYSIS OF CASES OF BRONCHIAL CARCINOMA IN THE
PRESENT SERIES
Unilateral Bilateral
Hepatic metastases present 6..1 6Liver not involved 14 31 2
1 One of thcse cases was an example of retrograde lymphatic spreadfrom infiltrated mediastinal lymphatic nodes.
2 The second case was an example of alveolar cell carcinoma ofmultifocal origin; there were no lymphatic metastases present.
TABLE IVDISTRIBUTION OF CASES OF BRONCHIAL CARCINOMA
ACCORDING TO HISTOLOGICAL TYPE
Histological Type No. of Cases
Oat cell.tUndifferentiated. 5Epidermoid.5Squamous IAdenocarcinoma. 6Alveolar cell. I
important (Porter, 1965; Stoll, 1965). The fre-quency of remote visceral metastases in thesecases at necropsy is also an indication that thedevelopment of the pleural secondaries is usuallya terminal event. There was no significant varia-tion between the histological structure of theprimary tumours and that of their pleural secon-daries.The evolution of a pleural metastasis can only
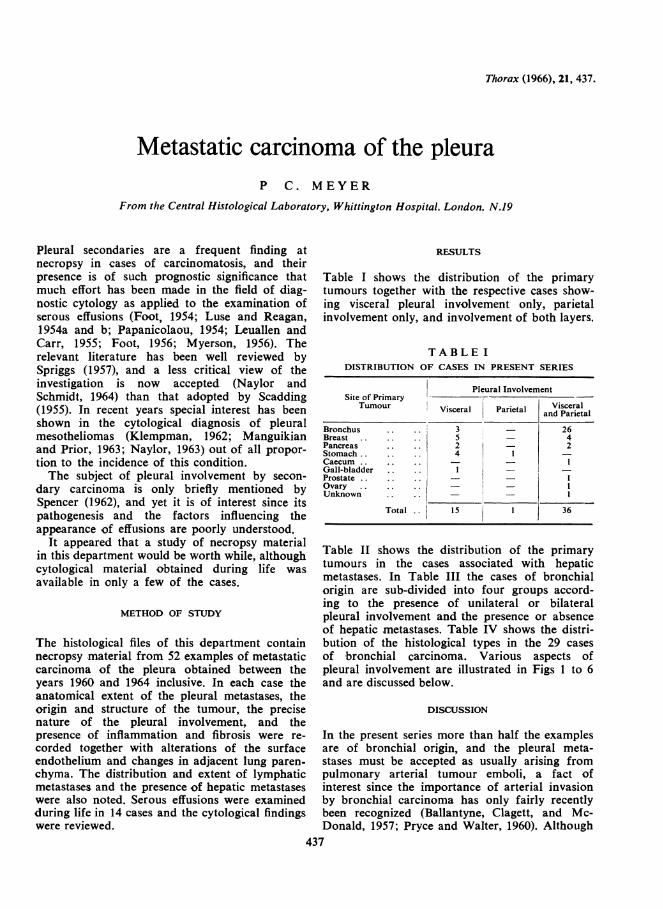
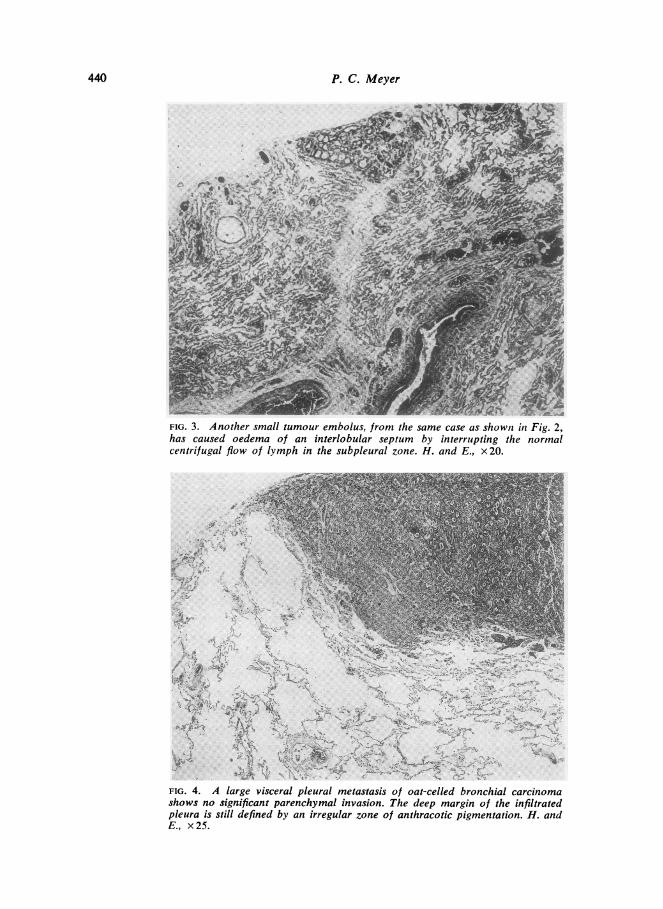
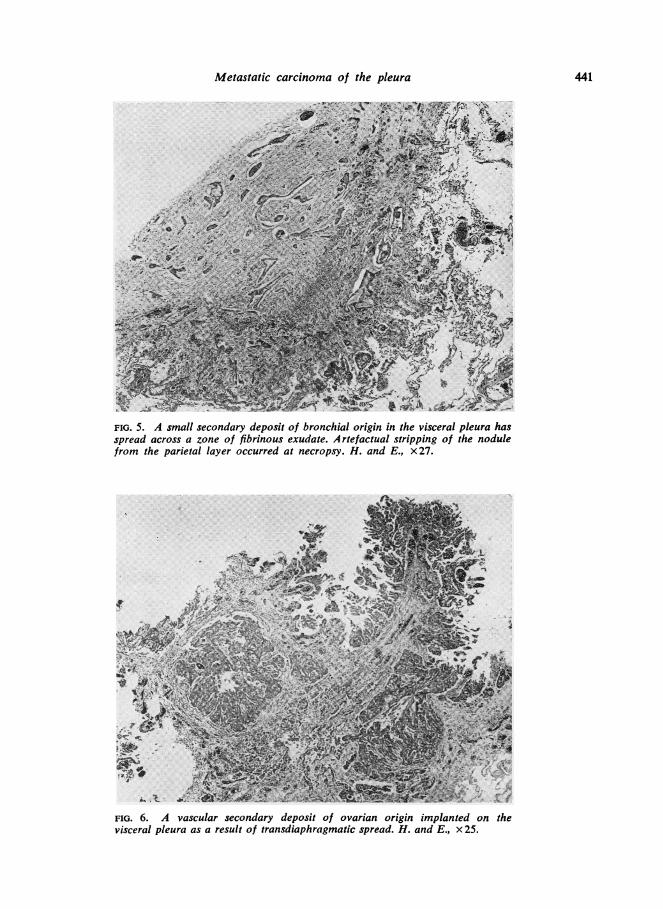
be deduced by comparison of individual tumourfoci in a number of cases. One of the earliestexamples of pleural involvement in which thetumour foci were both small and scanty is shown(Fig. 2) where pleural metastases of gastric originwere clearly the result of pulmonary arterialembolism; the small tumour focus (Fig. 3) hadinterrupted the normal centrifugal flow of lymphin the subpleural zone causing oedema of aninterlobular septum. In the absence of inflamma-tory reaction the pleural endothelium is oftenpreserved for an appreciable time, as in Fig. 4,where a metastasis, 0-8 cm. in diameter, of bron-chial origin shows no significant parenchymalinvasion. This occurs invariably in the presenceof inflammation; in Fig. 5 a secondary deposit ofbronchial origin in the visceral pleura has in-vaded the parietal layer through a zone of fibrin-ous exudate. Inflammatory changes adjacent topleural metastases were found to be variable inintensity and distribution and were frequentlyabsent. When present they were apparently relatedto pneumonic changes in the adjoining lungparenchyma. The same comments apply to the
438
Metastatic carcinoma of the pleura
FIG. I. Extensive retrograde lymphatic spread of a small bronchial carcinomafrom infiltrated mediastinal lymphatic nodes without nodule formation in thevisceral pleura. H. and E., x 25.
4 '4N
Z 4
K .
FIG. 2. Tumour embolus of gastric origin occluding a small pulmonary arteryimmediately subjacent to the pleura. H. and E., x 120.
439
P. C. Meyer..,_.........- te,,,n. 1s
FIG. 3. Another small tumour embolus, from the same case as shown in Fig. 2,has caused oedema of an interlobular septum by interrupting the normalcentrifugal flow of lymph in the subpleural zone. H. and E., x20.
½
1*.
4A;1
w..l.
Se./
U~~
FIG. 4. A large visceral pleural metastasis of oat-celled bronchial carcinomashows no significant parenchymal invasion. The deep margin of the infiltratedpleura is still defined by an irregular zone of anthracotic pigmentation. H. andE., x25.
440
, - -,#- '.j.f. el .1.
.. .. '4 1%
, 1.
4
'I.. 1,.4 1
,, ,f,A,91I .
:. t .
,z.
C ..
Metastatic carcinoma of the pleura 441
A'y.Xw [email protected].,-..:c...-,4wi>-r -4
-UW.-~~~~~* P i..
"Att
I~~~~~~~~~~~~~~A A
FIG. 5. A small secondary deposit of bronchial origin in the visceral pleura hasspread across a zone of fibrinous exudate. A rtefactual stripping of the nodulefrom the parietal layer occurred at necropsy. H. and E., x27.
It tf49,'. 4jF tw @e ; | E t^ g * _<~~~~~~~.-:p;, e ~k~f A
"<#'~~~~~~~~~~~~~~tRrtin4v~ ~ ~ '#I /~~~A~~~~~~~~~~~~~~~~~~~~~~~~~4~~ ~ ~ ~ ~
FIG. 6. A vascular secondary deposit of ovarian origin implanted on thevisceral pleura as a result of transdiaphragmatic spread. H. and E., x 25.
P. C. Meyer
occurrence of pleural fibrosis, but the presence ofpreformed fibrous adhesions predisposes to rapidneoplastic spread across the pleural cavity. Thisoccurs regardless of the aetiology of such adhe-sions.
In the present series the development of aserous effusion was related closely to neoplasticinfiltration of mediastinal glands; the extent ofpleural involvement by nodular metastases boreno such relationship. The example illustrated (Fig.1) is of interest in view of the association betweenmassive bilateral effusions and an absence ofnodular metastases. These findings are in accordwith the view that the fluid outflow from apleural effusion is via lymphatics (Stewart, 1963);they also explain the fact that pleural effusionsdo not develop in cases where the pleura is in-volved by secondary sarcoma because of the usualabsence of lymphatic metastases.A pleural effusion was present in 31 out of 52
cases in the present series, and a grossly haemor-rhagic effusion was present in only nine of these.The presence of a haemorrhagic effusion is ofgreat diagnostic importance but the reason for itsoccurrence was often not clear. In a few cases thesource of the haemorrhage was obviously fromvascular papillary tumours (Fig. 6), but moreoften the neoplastic infiltration was restricted tothe deeper layer of the pleura where occlusion ofsmall venules occurred; this process resulted invascular engorgement of the superficial layer andhaemorrhage through the endothelial surface ina manner analogous to that occurring in pachy-meningitis interna haemorrhagica (Russell andCairns, 1934). There was no evidence for anyinflammatory basis for such haemorrhage, assuggested by Willis (1960), and it was, more-over, of interest that in many cases there hadclearly been a substantial time interval betweenthe final occurrence of haemorrhage and death.This was indicated by the fact that many effu-sions encountered at necropsy were transparentand dark brown due to the presence of abundantdegraded blood pigment. It appeared, therefore,that the more gross neoplastic pleural infiltrationwas often associated with a diminished haemor-rhagic tendency.Although specimens of pleural fluid were exam-
ined during life in only 14 cases, some points ofinterest emerge on review of the cytological find-ings. Thus a preponderance of endothelial cellsoccurred in only two cases and in the remaindersuch cells were scanty or absent. This was re-flected by a notable absence of endothelial-cellhyperplasia in the histological material and
establishes that the absence of endothelial cellsfrom a pleural fluid is not a differential diagnosticpoint in favour of tuberculosis, in contrast to theview of Widal and Ravaut (1900). The variablecytological features of pleural effusions associatedwith bronchial carcinoma and with more distantprimary tumours have been emphasized byHinson (1961) and were confirmed in the presentstudy. Malignant cells were present in 11 out of14 cases and were often numerous, althoughin one case only two cells could be identifiedafter prolonged search of a film. The presence ofred cells was established microscopically in everycase except one, although the effusions weremacroscopically free from blood in six cases.
SUMMARY
In an analysis of necropsy material from 52examples of metastatic carcinoma of the pleura itwas found that over half of the cases were ofbronchial origin and that the pleural secondarieshad arisen from pulmonary arterial tumouremboli. Pleural metastases of bronchial originoccurred relatively early in the course of thedisease, whereas in other visceral primary tumoursthoir appearance was a terminal development.Bilateral pleural involvement was related to thepresence of hepatic metastases. Pleural secondar-ies may become large without evidence of paren-chymal invasion, but in the presence of inflam-mation or of preformed fibrous adhesions thereis rapid spread across the pleural cavity. Effu-sions developed as a result of neoplastic infiltra-tion of mediastinal lymph nodes and were notrelated to the extent cf pleural involvement bynodular metastases. There was evidence that thelater stages of pleural involvement by secondarycarcinoma were often associated with a dimin-ished haemorrhagic tendency.
I am indebted to Mr. G. W. Moore for the photo-micrographs and to Miss H. Pallan for secretarialwork. My thanks are also due to Dr. S. Robinsonfor reading the paper.
REFERENCES
Ballantyne, A. J., Clagett, 0. T., and McDonald, J. R. (1957). Vascularinvasion in bronchogenic carcinoma. Thorax, 12, 294.
Bryson, C. C., and Spencer, H. (1951). Carcinoma of the bronchus.Quart. J. Med., 20, 173.
Foot, N. C. (1954). Identification of types and primary sites of meta-static tumours from exfoliated cells in serous fluids. Amer. J.Path., 30. 661.(1956). Identification of cells in exudates and effusates. Anti. N.Y.Acad. Sci., 63, 1324.
Ttinsonn K. F. W. (19651). 'Examination of pleural fluid. Practitioner,186, 260.
442

Metastatic carcinoma of the pleura
Klempman, Sarah (t962'. The exfoliative cytology of diffuse pleuralmesothelioma. Cancer (Philad.), 15, 691.
Leuallen, E. C., and Carr, D. T. (1955). Pleural effusion. A statisticalstudy of436 patients. New Engl. J. Med., 252, 79.
Luse, Sarah A., and Reagan, J. W. (1954a). A histocytological studyof effusions. 1, Effusions not associated with malignant tumors.Cancer (Philad.), 7, 1155.- (1954b). A histocytological study of effusions. 2, Effu-sions associated with malignant tumors. Ibid., 7, 1167.
Manguikian, B., and Prior, J. T. (1963). Mesotheliomas of the pleura.Arch. Path., 75, 236.
Myerson, R. M. (1956). Pleural effasion. A statistical analysis of 100cases in which thoracentesis was performed. Delaware med. J., 28,87.
Naylor, B. (1963). The exfoliative cytology of diffuse malignantmesothelioma. J. Path. Bact., 86, 293.and Schmidt, R. W. (1964). The case for exfoliative cytology ofserous effusions. Lancet, 1, 71 1.
Papanicolaou, G. N. (1954). Atlas of Exfoliative Cytology. Common-wealth Fund, Harvard University Press, Cambridge, Mass.
Porter, E. H. (1965). Pleural effusion and breast cancer (letter). B;it.med..J., 1, 251.
Pryce, D. M., and Walter, J. B. (1960). The frequency of gross vascularinvasion in lung cancer with special reference to arterial invasion.J. Path. Bact., 79, 141.
Russell, Dorothy S., and Cairns, H. (1934). Subdural false membraneor haematoma (pachymeningitis interna haemorrhagica) in car-cinomatosis and sarcomatosis of the dura mater. B-ain,57, 32.
Scadding, J. G. (1955). Pleurisy. Practitioner, 175, 685.Spencer, H. (1962). Pathology ofthe Lung. Pergamon Press, London.Spriggs, A. I. (1957). The Cytology of Effusions in the Pleural, Peri-
cardial and Peritoneal Cavities. Heinemann, London.Stewart, P. B. (1963). The rate of formation and lymphatic removal
of fluid in pleural effusions. J. clin. Invest., 42, 258.Stoll, B. A. (1965). Pleural effusion and breast cancer (letter). Brit.
med. J., 1, 658.Walter, J. B., and Pryce, D. M. (1955). The histology of lung cancer.
Thorax, 10, 107.Widal and Ravaut (1900). Applications cliniques de l'etude histolo-
gique des 6panchements sero-fibrineux de la plbvre (pleuresiestuberculeuses). C.R. Soc. Biol. (Paris), 52, 648.
Willis, R. A. (1960). Pathology of Tumours, 3rd ed. ButterworthsLondon.
443