Embed Size (px)
Citation preview

T E C H N I Q U E
Meniscus Repair: Update on New TechniquesNICHOLAS A. SGAGLIONE, M.D.Division of Sports Medicine, Department of Orthopaedic Surgery, North Shore University Hospital, andOrthopaedic Associates of Manhasset, Manhasset, New York
� ABSTRACT
Increasing emphasis on the comprehensive reconstruc-tion of the knee and on restoration of knee function afterinjury has heightened the interest in meniscus preserva-tion. The approach to meniscal tears in the active indi-vidual emphasizes tissue repair over resection becausemeniscal tissue preservation has several potential advan-tages that improve the biomechanics and natural historyof knee function over time. The technical approach tomeniscal repair has significantly evolved in the last 10years and continues to expand. Numerous techniques andmultiple devices have been introduced and present theclinician with a vast array of surgical options. More re-cently, case reports documenting morbidities associatedwith the use of newer generation meniscal repair fixatorshave raised concerns regarding these devices andprompted recommendation that repair using suture maybe preferred. An update on meniscus repair techniques ispresented outlining and reviewing the current availableprocedures and implants including postoperative care,preliminary results, and complications. Technical pearlsand pitfalls including optimal indications are reviewedfor several of the repair methods as well as potentialfuture directions in the approach to meniscal disease.Key words: arthroscopic meniscal repair, new tech-niques, implant fixators
� INTRODUCTION
The medial and lateral menisci have been shown to sig-nificantly contribute to optimal knee function by provid-ing an essential biomechanical and structural role in jointload bearing and distribution, stability, congruence, aswell as articular cartilage homeostasis and propriocep-tion.1–6 It is well established that meniscal preservationin the younger active individual presenting with symp-tomatic meniscal disease is important.7–11 Furthermore,
in those patients who are concurrently undergoing ante-rior cruciate ligament stabilization, articular cartilage re-surfacing, or axial realignment osteotomies, the need tomaintain meniscal tissue may be even greater.2,4,12,13 Re-cent advances in the approach to meniscal repair haveheightened the interest in the numerous available surgi-cal options. Evolving techniques, multiple devices, andimproved understanding of the natural history of menis-cal attrition and outcomes of meniscal repair prompt theneed for a current review of the subject.
� HISTORY
King first reported on meniscal disease in an animalmodel study in 1936 and found that in the canine menis-cus, tears in the peripheral vascular zone had the capacityto heal.14 Despite this work, most clinicians advocatedand performed meniscal resection until the 1970s, whenthe introduction and widespread embrace of arthroscopyand expanding research into meniscal vascular and ul-trastructural anatomy and function began to be betterunderstood. The increased emphasis on physical fitnessand conditioning as well as the information and influencegenerated by the media spotlight on sports and injuredathletes has prompted demand for both the preservationof knee function and a more predictable return to prein-jury performance and stressful activity. The parallel em-phasis on and evolution of the treatment of anterior cru-ciate ligament (ACL) deficiency and significantassociation of ACL injury and meniscal tears has furtherturned attention to the repair of meniscal tears.
Clinical reports of meniscal repair by Henning andlonger-term follow-up data published by DeHaven sup-ports the efficacy and success of both open and arthro-scopic approaches to repair.15–18 Increasing work in thelaboratory, in addition to patient follow-up data, has ad-vanced the concept of meniscal preservation and ulti-mately prompted the development of improved meniscalrepair devices.19–22 Various techniques have been de-scribed including open, arthroscopic-assisted, outside-in,inside-out, all-inside, suture-based, and implant or fix-ator based.16,21–24
Address correspondence and reprint requests to Nicholas A. Sgaglione,M.D., Orthopaedic Associates of Manhasset, 800 Community Drive,Manhasset, NY 11030, U.S.A. e-mail: [email protected]
Techniques in Knee Surgery 1(2):113–127, 2002 © 2002 Lippincott Williams & Wilkins, Inc., Philadelphia
113Volume 1, Issue 2

� INDICATIONS ANDCONTRAINDICATIONS
The indications for meniscal repair have been expandingas a better understanding of pathophysiology, repair sitehealing, and biomechanical behavior and performance ofvarious repair techniques and devices is achieved. Ver-tical longitudinal tears located in the red–red and red–white vascularized zones of the meniscal periphery areanatomically optimal for repair14,19 (Fig. 1). The indica-tions and contraindications for meniscal repair are out-lined in Table 1. Asymptomatic tears that are not clini-cally correlative, particularly in patients older than age60 years, with associated articular cartilage degenerativearthritis are clearly not repaired. Patients, who aftercounseling regarding postoperative healing, activity re-strictions, and repair failure rates, decide that resection ispreferable, are not candidates for meniscal repair.
� PREOPERATIVE PLANNING
Preoperative planning begins with the clinical diagnosisof meniscal tears. The history of trauma, hemarthrosis inthe presence of an ACL injury, associated joint-line pain,swelling, and mechanical symptoms of locking andcatching are indicative of a meniscus tear. Physical ex-amination findings include assessment of axial align-ment, antalgia, posttraumatic loss of motion (particularlyextension), pain with squatting in terminal flexion, focaljoint-line point tenderness, pain with axial compressiontesting (in flexion and extension), palpable joint-line click, and effusion. Plain radiographs should be ob-tained in all cases and should include extensionanterior/posterior and medial/lateral views as well as anotch and patella skyline view. In addition, weight-bearing 45° flexion posterior–anterior comparison viewsshould be obtained in cases in which there is any suspi-cion of articular cartilage wear and to accurately assessjoint-space narrowing. Routine magnetic resonance im-aging is often not indicated in the presence of meniscaldisease but may be useful in cases where other ligamen-tous, articular cartilage, or bony disorder (i.e., osteone-
crosis) is suspected. When appropriate and comprehen-sive nonsurgical treatment fails and patient counselingand expectations and proper indications are addressed,surgical intervention is appropriate. More urgent opera-tive intervention is appropriate in cases of displacedmeniscal tears and associated locking.
� SURGICAL TECHNIQUES
PreparationThe author’s preferred technique of meniscus repair isperformed with the patient under local anesthesia withintravenous sedation on an outpatient basis at an ambu-latory surgery center. Preoperative prophylactic intrave-nous antibiotics are not routinely given. When associatedACL reconstruction is carried out, then a femoral nerveregional block anesthesia is used with general endotra-cheal anesthesia or epidural anesthesia. A lateral post(Telos; Fallston, MD, U.S.A.) is preferred to apply val-gus stress and open the medial joint for medial meniscaldisease. If ACL reconstruction or articular cartilage pro-cedures are to be performed, then the meniscal repair is
TABLE 1. Indications and contraindications to meniscal repair
Indications Contraindications
Acute, symptomatic tears Degenerative non-clinically correlative tears in older patientsVertical, longitudinal tears Complex pattern tearsPeripheral, red-red/red-white tears White-white avascular tears> 7–10 millimeters (mm) in length Tears < 5–7 mm in lengthUnstable: > 3 mm of excursion Stable, incomplete tearsNondeformed, viable tissue Degenerative, nonviable tissueConcomitant reconstructive surgery: ACL or articular cartilage
proceduresAssociated infectious, rheumatoid or collagen vascular
diseasesPatient preferred Patient recovery or rehabilitation compliance is an issue
FIG. 1. Meniscal vascular zones.
N. A. Sgaglione
114 Techniques in Knee Surgery

carried out first, and it is the author’s preference to tieand secure the sutures prior to carrying out the ACLprocedure.
The meniscal tear site is essentially identified as asite of suboptimal nonhealing tissue subject to compres-sive, tensile, and shear loads and is unable to adequatelyrespond to those loads. Furthermore, the tear is located inan environment that is fluid filled and subject to motionin multiple planes. The goal of repair is to achieve op-timal strength of fixation and load sharing until biologichealing is adequate for the native meniscal tissue to func-tion under applied mechanical loads. Prior to obtainingfixation, the tear site must be assessed, measured, re-duced, and debrided of nonvital tissue. It is then preparedand freshened to stimulate and promote peripheral nativetissue and to contribute to healing. Stabilization is thenobtained and fixation accomplished either with suturingtechniques or placement of a fixation repair device.Meniscal repair may be supplemented (as needed) withautologous substances in the form of fibrin clot to im-prove the healing environment.
The technique of meniscal repair begins with identi-fying whether the tear is repairable. The site, length,excursion or stability, reducibility, and viability in termsof tissue deformation and extent of damage and frayingare all assessed. Medial meniscal repairs are performedwith valgus stress applied against a lateral post in vary-ing degrees of flexion while lateral repairs are performedwith the patient’s leg in a figure-of-four configuration.Depending upon whether suture or implants or fixatorsare used, then a contralateral approach to the posteriorhorns is used (i.e., posterior horn medial meniscal tearsare approached from a contralateral inferolateral portalwith the suture repair device).
After assessment confirms that the tear is repairable,if the patient will not require an associated ACL recon-struction, then a fibrin clot technique is planned for andimmediate autologous blood is requested and obtainedby the attending anesthesiologist (see Repair Methods:Fibrin Clot Technique). The tear is reduced and the tearedges are geometrically matched to ensure that an ap-propriate reduction can be obtained. It is particularly im-portant to reduce displaced and unstable bucket handletears. A provisional reduction can be obtained and facili-tated using an 18-gauge spinal needle inserted either inan inside-out or outside-in direction.
Preparation of the tear site is begun by gently debrid-ing both the meniscal tear site and edges as well as theperipheral meniscal–capsular junction using a motorizedshaver blade. A low-profile meniscal rasp can also beused and is helpful in preparing the peripheral junction.Vascular access channels can be created using the spinalneedle or a meniscal trephine. Care must be exercised toavoid overly aggressive penetration of the peripheral
meniscal circumferential tissue band and the body of themeniscus fragment to avoid further injuring the tissueand producing stress risers. Trephination and abrasionare particularly important in cases where a repair is per-formed in less vascularized zones. After preparation iscomplete, the specific and preferred repair technique(s)are selected and carried out. Depending upon the methodand device used, the length and vector geometry of thetear site should be assessed to provisionally select thenumber of sutures or fixators that will be needed and alsothe length of the devices that may be needed as far as thesize of the patient, size of the meniscus, distance of thetear from the periphery and capsule, and technique used.
Repair Methods: Open TechniqueOpen repair of the menisci, popularized by DeHaven, isless commonly performed in the era of arthroscopy.17,18
However, in cases of extraarticular ligament reconstruc-tion in which capsular reefing may be concurrently per-formed, especially medially or in cases in which an as-sociated miniarthrotomy may be performed (articularcartilage or meniscal allograft transplantation), open su-turing of meniscal tears is useful. Nonabsorbable 2–0 or-0 interrupted suture is used to repair the meniscus tear toadjacent meniscal tissue or the peripheral capsule.
Repair Methods: ArthroscopicOutside–In TechniqueReported in the literature by Warren and more recentlyby Rodeo, arthroscopic outside-in meniscal repair can becarried out using several methods.22 The outside-in re-pair technique is particularly useful for repairing anteriorhorn or mid-third body tears. After identification andassessment of the tear, a series of 18-gauge spinalneedles placed 3 to 5 mm apart or a corresponding su-ture-passing needle system are passed from outside toinside through the tear, perforating the inner (or superiorfemoral) and outer (or inferior tibial) surfaces. An ab-sorbable monofilament suture may be used such as poly-diaxanone (Ethicon, Somerville, NJ, U.S.A.) and the in-dividual suture strands may be pulled out of thearthroscopic portal and a “mulberry” knot tied, which isthen withdrawn back into the joint and tensioned at andup to the meniscal tear site. More recently various suturematerials can be used in combination with dedicated out-side-in meniscal repair instrumentation. Several nonab-sorbable suture configurations can be placed includinghorizontal and vertical mattress patterns, depending onthe needle passage using a wire loop retriever and place-ment of the suture knot in an extracapsular location. Theoutside-out repair technique requires that a small skinincision be made surrounding the sutures that allows dis-section around the sutures and down to the capsule,
Meniscus Repair
115Volume 1, Issue 2

and which then allows the appropriate tensioning of thesutures down to the capsule and subsequent knot tying(Figs. 2A and 2B).
Repair Methods: ArthroscopicInside-Out TechniquePopularized by Henning, who began performing thetechnique in 1980, inside-out meniscus repair has en-joyed the most clinical experience and documentation inthe literature.12,15,16 It has been referred to as the “goldstandard” against which more recent techniques havebeen compared. The method in general is performed us-ing a series of anatomically matched and contoured(right and left knee) arthroscopic cannulae that are
placed through the arthroscopic portals and up to the tearsite, usually from a contralateral portal. This method re-quires attention to the antegrade direction and vector ofthe cannula and subsequent needle passage to safely re-pair the tear and protect the neurovascular structures.Extra-long suture needles are then passed though thecannulae across the tear and out the posteromedial orposterolateral aspect of the knee. Depending uponwhether a single- or double-lumen cannula system isused, vertical, horizontal, and oblique sutures patternscan be achieved. It is important to safely “capture” andretrieve the needles through accessory posteromedial andposterolateral incisions that are preferably made prior topassage of the needles. The accessory incisions are madewith the knee in 90° of flexion at the level of the jointline, extending one third above the joint but more im-portantly two thirds below the joint. A curved retractor isinserted anterior to and deep to the corresponding sidegastrocnemius, which facilitates protection of the adja-cent soft tissues and allows the passing needles to besafely “bounced” off of the retractor and out the incisionas they exit the capsule. The posteromedial incision ismade just posterior to the medial collateral ligamentabove the level of the sartorius, which is retracted pos-teriorly with the sartorial branch of the saphenous nerve(although anatomic variation may exist) The dissection iscontinued anterior to the semimembranosus and deep tothe medial head of the gastrocnemius muscle bellysweeping the posteromedial capsule. The posterolateralincision is similarly made in flexion, which posteriorizesthe peroneal nerve. The interval used posterolaterally isjust posterior to the lateral collateral ligament and theiliotibial band, staying above and anterior to the bicepsfemoris tendon and muscle fibers of the short head of thebiceps tendon.25 Dissection is continued deep and ante-rior to the lateral head of the gastrocnemius muscle belly,sweeping the posterolateral capsule clear. Upon comple-tion of the placement of a series of sutures through thetear site, the sutures are tied to the corresponding adja-cent suture limb over the capsule while arthroscopicallyviewing the tensioning and seating of the sutures on themeniscal tissue. The medial meniscal repair sutures aretied with the knee in 20° of flexion, while the lateralrepair sutures are tied down with the knee in 90° offlexion, and it is the author’s preference to tension and tiethe sutures prior to performing concomitant proceduressuch as ACL reconstruction.
Repair Methods: All-ArthroscopicFixator TechniqueRecently, multiple meniscal repair devices have becomeavailable that enable an all-arthroscopic approach to sta-bilizing tears. These devices have made meniscal repairtruly arthroscopic, easier, quicker, associated with less
FIG. 2. A, Outside-in arthroscopic photograph. B, Out-side-in technique illustration.
N. A. Sgaglione
116 Techniques in Knee Surgery

surgical dissection (no accessory incisions), and with lesspain and less need for operating room assistance. Thereare advantages and disadvantages to the use of implantfixators and inside-out suture techniques (Table 2). Vari-ous devices have been introduced since the Bionx Menis-cal Arrow (Bionx Implants Inc., Blue Bell, PA, U.S.A.)was released in 1996 (Table 3).
Arthroscopic meniscal repair fixators are in general,based on a reverse-barbed fish-hook design and are madeof bioabsorbable materials composed of various amountsof polylactic and or polyglycolic acid copolymers. Sev-eral proprietary manufacturing and processing methodsexist in which the polymer materials may be extrudedand machined versus injection molded. The differentpolymer and copolymer configurations including wheth-er the microstructure is crystalline or amorphous as wellthe various processing methods can impart varying bio-mechanical and structural properties as well as hydroly-sis, degradation, and resorption profiles to the im-plants.26
The technique of repairing meniscal tears using fix-ators is similar for most devices in that after preparationof the tear site, and potentially provisional reduction, thetear distance from the periphery is assessed and mea-sured, which allows selection of the appropriately sizedfixator length. The fixator(s) are then inserted perpen-dicular to the tear (vertical, longitudinal tears clearly rep-resent the most optimal tear pattern for repair) and acrossthe tear bridging the two meniscal fragments and stabi-lizing them with the device held in place by the reversebarbs or cross bar on the shaft. It is essential that there beenough meniscal tissue on both sides of the tear in orderfor the device to function optimally, and it follows thatperipheral capsular detachments and meniscal allografts
are not necessarily indications for fixator repairs. Eachdevice is then inserted at 3- to 5-mm intervals. An im-portant pearl is that extreme care must be taken to ensurethat the fixator head is seated flush or countersunk to thesurrounding surface of the meniscus to reduce the chanceof articular cartilage injury (Fig. 3, Table 4).
Repair Methods: Fibrin Clot TechniqueThe technique of insertion of an exogenous autologousfibrin clot is based on the concept of promotion of tearsite healing by introducing blood-associated biologicfactors including platelets that may act as chemical me-diators for tissue repair and as well as an adherent me-chanical scaffold. This may be particularly effective inthe knee where motion, meniscal excursion, and jointfluid can all contribute to reduction in repair tissue for-mation and maturation. Various methods for preparationand insertion of a fibrin clot have been reported.15,19,27
The author’s preferred technique used in cases of iso-lated repair (since in cases of concomitant ACL recon-struction the hemarthrosis that accompanies the tunneldrilling may serve to produce an environment sufficientfor healing) is to obtain 30 to 50 cm3 of blood from thepatient’s intravenous site and then sterilely transfer it toa glass container and stir it with a sintered glass rod.After formation of the clot, the rest of the blood is de-canted off and the clot is blotted dry. Upon completion ofthe repair and with the arthroscopic fluid turned down,the clot is inserted under arthroscopic visualization usinga grasper within a 5-mm diameter cannula with its dia-phragm removed and placed across the portal.22 The clotis then inserted under the repair site adjacent to the tibialsurface of the tear. No specific sutures are used to anchorthe clot, although other authors have reported on tech-niques to suture the fibrin clot into the repair.15
� FIXATOR DEVICES:FIRST GENERATION
Meniscus ArrowThe Meniscus Arrow (Bionx, Blue Bell, PA, U.S.A.),released in 1996, was the first arthroscopic fixator deviceto be popularly used, and a greater experience with thisparticular device exists.28 The original design was “T”shaped with a 1.1-mm-diameter shaft of three lengths(10, 13, and 16 mm) and a 4-mm-long “T” head. Theshafts of the device each have reverse barbs at rightangles to the ‘T‘ head and 90° offset to each other withthe 10-mm device being fully barbed while the 13-mmand 16-mm devices each have 10 mm of barbs and 3-mmand 6-mm lengths of smooth shaft, respectively (Fig. 4).The Arrow can be inserted manually using a curved andvariable insertion cannulae system or a mechanical de-
TABLE 2. Advantages and disadvantages of inside-outsuture and fixator techniques
Advantages of suture and fixator techniques
Inside-out suture Implant fixators
Strength: 70 to 113 Newtons Quick/reduce or time by 1/2Compression across tear site Easy insertionVersatility: vertical suture
patterns Single-handed techniquesExperience: clinically
documented All arthroscopicSafety: outcomes published Bioresorbable
Disadvantages of suture and fixator techniques
Inside-out suture Implant fixators
Time consuming Reduced strengthAccessory incision Limited compressionOR assistant necessary Variable resorption profileNeedle stick risks Foreign body reactionMore dissection/more pain Brittle/breakageArthrofibrosis Chondral injury
Meniscus Repair
117Volume 1, Issue 2

vice known as the “Crossbow” with multiple implantdevices preloaded in a magazine. Material compositionof the original Arrow design was self-reinforced poly-merized levorotatory polylactic acid (PLLA). Specifi-cally the levorotatory “L” stereoisomer preparation,
which is the biologically active form, is highly crystal-line and has been estimated to have a resorption profileof 36 to 60 months. As of late 2000, the Arrow compo-sition was changed to a 96% PLLA combined with 4% ofthe polylactic acid dextrorotatory “D” stereoisomer con-
FIG. 3. Illustration of fixator insertion.
TABLE 3. Meniscal repair fixator devices
Device Sizes Material Resorption
Strength*load
to failure Comments
CONTOURARROW(Bionx Implants Inc.,Blue Bell, PA.)
10, 13 16 mmlength ×1.1 mmdiameter 0.7mm head
Self-ReinforcedCopolymer80% PLLA20% PDLLA
12–24 months 33.6 N(Result for13 mm 1st
GenerationDevice)
Redesigned LowerProfile Head, FullyBarbed Shaft,Copolymer &CrossBow Inserter
SD SorbSTAPLE(Surgical Dynamics,Norwalk, CT.)
7 mm (10 mm)with 4 mmsuture
82% PLLA18% PGA
15 months 31.4 N LowerProfileDesignPending
BIOSTINGER(Linvatec, Largo, FL)
10, 13 16mm× 1.25mmdiameter
Injection-moldedPLLA
36 months 56.6 N (13mm) New Hornet cannulatedinsertion device
FASTENER(Mitek, Westwood,MA)
6 and 8 mm Prolene(polypropylene)or PDS(polydiaxanone)
PDS 6–16 weeks 30 N(8mm Prolene)
12, 24 and 34° curvedinserters
CLEARFIXSCREW (Mitek)
10 mm by 2.0mmdiameter
PLLA 18 months 32.5 N Cannulatedwith variable threadpitch
DART(Arthrex, Naples, FL)
10, 12, 14 mmby 1.3 mmdiameter
AmorphousPDLLACopolymer
9 months Not tested Double reverse barbs:Flexible. New DartStick
STAPLE(Arthrotek, Warsaw, IN)
11 and 13 mm Lactosorb82 % PLLA18 % PGA
12 months 27 N Double pronged fixation
Fast—Fix(Smith & Nephew,Andover, MA)
(2) 5 mmsutureanchors
PLLA orPolyacetal and0—nonabsorbablesuture
NA Not tested Second Generation:vertical mattresssuture possible
RAPIDLOC (Mitek) (2) sutureanchors
PLLA Tophat(POS) &backstopEthibond orPanacrylsuture
NA Not tested Second Generation:Suture deviceCompression possible
*Study reference: 52
N. A. Sgaglione
118 Techniques in Knee Surgery

figuration (PDLLA). The PDLLA configuration is moreamorphous and possesses different degradation and me-chanical properties. The 96/4 copolymer imparts aquicker resorption time to the device.26 Further develop-ments introduced in 2002 have included changing thecopolymer to a more flexible and amorphous 80% PLLAand 20% PDLLA, changing the 1.1-mm-thick “T” headto a lower profile rounded 0.7-mm head (Contour Ar-
row), adding barbs to the entire length of the shaft andintroducing a second-generation mechanical Crossbowinserter. These changes have been introduced in responseto issues of retained PLLA fragments not being morequickly resorbed, the brittle and hard character of self-reinforced PLLA, reports of chondral injury from promi-nent fixator heads, and suboptimal fixation strength pro-files (Fig. 4).
FIG. 4. Original and updated Bionx Contour Meniscal Arrow.
TABLE 4. Pearls on use of meniscal fixators
The easier the fixator insertion technique, the more essential the need to prepare the tear siteReduce the tear to avoid gapping, ruffling and lift-up and begin inserting fixators from the center of the tear out to avoid “dog
ears”Use of an outside-in temporary stay suture aids in holding displaced bucket-handle tears reduced in placePay attention to the inner 3-dimensional taper of the meniscus when inserting the implants to avoid cutting or troughing the
tissuePlace the devices perpendicular to the tear using accessory portals as neededConfigure the size of the patient, meniscal structure, tear site and implant length to maximixe strength of the device mechanics
and limit native tissue irritationEnsure that the device is countersunk or flush with the surrounding meniscusAvoid overstuffing the tissue with fixators; place every 3 to 5 mm apartConsider hybrid repair constructsRange knee and arthroscopically view the repairConsider fibrin clot or capsular abrasion in isolated repairs to promote healingAdjust and individualize postoperative rehabilitation
Meniscus Repair
119Volume 1, Issue 2

SD Sorb StapleThis device, released by Surgical Dynamics (Norwalk,CT, U.S.A.) in 1997, consists of two barbed 7-mm fixa-tion posts comprising 82% PLLA/18% PGA linked by a4-mm braided nonabsorbable suture. The copolymer isreportedly resorbed in approximately 15 months. Thedevice provides two points of fixation and is insertedusing a preloaded manual device or a multifire gun. Newupdated design modifications include longer 10-mmfixation posts, and redesigned inserter head with a lowerprofile insertion system with precurved tips.
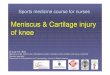
BiostingerThe Linvatec Company (Largo, FL, U.S.A.) introducedthe Biostinger in 1998 as the first cannulated device witha lower profile head. This fixator, which is violet col-ored, making it easier to visualize against tissue, is 1.25mm in diameter and contains four rows of reverse barbson all sides of the shaft and is available in 10-, 13-, and16-mm lengths (Fig. 5A). It comprises 100% PLLA witha resorption profile of 36 to 60 months. Three genera-tions of insertion devices have been introduced with theBiostinger, and improvements in design have recentlyproduced the “Hornet” disposable insertion system,which comes in three dedicated sizes corresponding tothe three available implant sizes, which come preloadedon the color-coded inserters (Fig. 5B).
FastenerMitek (Westwood, MA, U.S.A.) introduced the MitekMeniscal Repair System in 1998, which included theFastener, a “T/J”-shaped fixator device available in twosizes—6 and 8 mm—and two materials, nonabsorbableProlene and absorbable PDS/polydiaxanone (Ethicon),which has a resorption profile of 6 to 16 weeks. TheFastener can be inserted with a curved cannulae systemthat comes in three angled tips: 12, 27, and 34°. TheFastener is unique in that it is one of the few fixatordevices that can be used for repair of peripheral meniscaltears since its design allows for deployment of the lead-ing crosslimb of the device outside the periphery of themeniscus and on the other side of the capsule.
Clearfix ScrewThe Clearfix Screw, also available from Mitek and in-troduced in 1998, is a 2.0-mm-diameter × 10-mm-longheadless screw-in design that allows for countersinkingand has a 0.3-mm variable pitch thread that theoreticallyadds compression across the tear site. The device is madeof PLLA with a resorption profile of up to 18 months. Itis inserted using a cannulated delivery needle-guidedsystem.
DartArthrex (Naples, FL, U.S.A.) released the meniscus re-pair Dart in 1999 as a lower profile headless 1.3-mm-
diameter × 10-mm-long implant that can be countersunk.The barb configuration is one of a double-reverse design,thereby proving improved pull-through as well as pull-out strength and potentially limiting device migration(Fig. 6).
The Dart is placed across the tear site in at least a pairconstruct functioning as two points of fixation. The de-vice is comprised of an amorphous PLLA/PDLLA co-polymer which imparts more flexibility to the fixator andis associated with a 36-week resorption profile. It is in-serted using either a manual or spring-loaded deliverysystem and curved cannulae. Updated technique modifi-cations include the use of a preloaded manual insertiondevice, the Dart Stick, which facilitates placement of theimplants.
FIG. 5. A, Linvatec Biostinger implant. B, LinvatecBiostinger inserters.
N. A. Sgaglione
120 Techniques in Knee Surgery

StapleThe Meniscal Staple (Arthrotek, Warsaw, IN, U.S.A.)was released in 1999 and delivers fixation via a double-pronged barbed staple available in 11- and 13-mmlengths. The device can be inserted with either a manualcurved cannulae system or a mechanical gun. The Menis-cal Staple is composed of an 82% PLLA and 18% PGAcopolymer with a resorption profile reported to be on theorder of 12 months.
� FIXATOR DEVICES:SECOND GENERATION
The array of available fixators that can be labeled “firstgeneration” all share a similar design. Because of earlycase reports of problems of foreign body synovitis, re-tained and painful fragments, and chondral scuffing andinjury, as well as published laboratory studies indicatingthat these devices provide inferior fixation strength com-pared to vertical mattress-suture configurations, im-
proved designs have been sought.29–45 In response tothese concerns and in the interest of reducing morbiditiesand increasing biomechanical strength, second-generation devices have been released recently that in-corporate all-arthroscopic techniques and hybrid bioab-sorbable fixator/anchor and suture constructs.
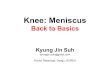
RapidLocMitek released the RapidLoc in 2001 as a meniscal repairsystem that incorporates both suture and fixator. Thedevice is an integrated needle delivery system consistingof a leading 5 × 2.5-mm PLLA (PDS as of 2003) “back-stop” anchor with attached suture that is inserted acrossthe tear site and then extracapsularly. In sequence, asecond attached PLLA anchor (with overlying pre-tied,self-sliding, integrated knot) known as a “tophat” iscinched down on the suture towards the backstop andright up to the tear site, thereby compressing the tearbetween the two anchors connected by the suture. The“tophat,” which is 4.5 mm wide and 0.25 mm thick, isthen seated intraarticularly on the femoral side of themeniscus, and compression across the tear site can beobtained by using an arthroscopic knot pusher to furtherseat the knot (Fig. 7). The delivery needles are availablein straight as well as 12° and 27° curved configurations,and the suture is available in nonabsorbable 2–0 Ethi-bond or extended resorption Panacryl suture (Ethicon).
FasT–FixIn 2001, Smith and Nephew (Andover, MA, U.S.A.) re-leased the FasT-Fix Meniscal Repair System. Some ofthe initial design was in part an expansion of the T-Fixmeniscal repair system introduced by Smith and Nephewin 1994 in that a 5-mm polyacetal anchor bar with at-tached nonabsorbable suture is inserted in an integrated
FIG. 6. Arthrex Dart Implant.
FIG. 7. Mitek RapidLoc device.
Meniscus Repair
121Volume 1, Issue 2

needle delivery system across the tear site and is an-chored extracapsularly. The T-Fix system required ar-throscopic knot tying and each anchor was individuallyplaced. The FasT-Fix system incorporates a design thatincludes two 5-mm polyacetal anchors with attached 0nonabsorbable braided synthetic polyester suture inte-grated in sequence with a preloaded, pretied, self-slidingknot and delivered in an arthroscopic 16.5-gauge inser-tion needle. The integrated delivery needle is available ina straight or a 22-degree curve. The system includesa split-sheath insertion cannula and separate knotpusher/suture cutter. The variable positioning choices forthe needle insertion allow for arthroscopic placement ofvertical mattress suture configurations and in addition,the use of suture placed across the tear site and anchoredextracapsularly introduces compression across the tear.In 2002, design advances included the release of theFasT-Fix system, improved and sharper trochar tippeddelivery needles, waxed-tip suture for easier threading,and more ergonomic and easier-to-use needle deliveryinsertion handpieces and split-sheath cannulae (Fig. 8).
� POSTOPERATIVE PROTOCOLS
Postoperative management begins in the operating roomwith attention to postoperative pain control. Intraarticularbupivacaine mixed with extended-acting morphine is in-jected into the knee, and nonsteroidal antiinflammatorydrugs (NSAIDs) are given intravenously. Postoperativecryotherapy and extended- acting analgesics andNSAIDs are prescribed along with immediate supervisedphysical therapy beginning postoperative day 1. Patientsare instructed to take one aspirin a day as tolerated forprophylaxis against thromboembolic disorders.
The author’s preferred postoperative regimen doesnot deviate much from the protocol used after ACL re-construction (using patellar tendon autografts) and issimilarly followed for isolated meniscal repairs. Patientsare placed in a postoperative brace or knee immobilizerin the operating room locked in extension. The immobi-lizer is used for comfort and to facilitate ambulation andtransfers. It is discontinued when the patient has ad-equate leg control and is comfortable without it or atabout 3 weeks. Weight is allowed in extension initiallyon crutches and then advanced as comfort allows, withfull weight bearing encouraged when antalgia and effu-sion subsides and quadriceps firing is adequate, usuallyat 3 to 4 weeks. Range of motion 0 to 90° is encouragedimmediately on postoperative day 1 (or the night of sur-gery if an associated ACL is performed as the patients inthose cases are placed in a continuous passive motionmachine in the recovery room set 0 to 90°). Progressionof motion, particularly in terminal flexion, is encourageddepending upon the repair site, size, geometry, andstrength. Large, deformed, bucket-handle tears extendingthrough to the posterior horns are progressed moreslowly during the first 2 months from the standpoint ofterminal flexion and loading and squats beyond 90°. Afunctional rehabilitation protocol is followed progressingeach patient dependent upon comfort with range of mo-tion, restoration of strength, and ultimately ability to per-form agility and functional as well as sport-specificdrills.46 Return to sports is usually at 4 to 6 months whenappropriate functional goals are reached and the patientno longer has point tenderness over the repair site.
� COMPLICATIONS
In a review of data obtained through surveying membersof the Arthroscopy Association of North America, Smallreported an overall complication rate incidence of 2.4%in an for meniscal repair.47 This number was noted to behigher in a series reported by Austin and Sherman, inwhich an overall complication rate of 18% was noted tobe associated with arthroscopic meniscal repair and a 7%incidence of saphenous neuropathy and 6% incidence ofFIG. 8. Second-generation device: Fast-Fix.
N. A. Sgaglione
122 Techniques in Knee Surgery

arthrofibrosis.48 It is important to point out that the serieswas collected from patients undergoing surgery between1984 and 1991 and may represent an earlier experiencewith suture repair techniques. In a subsequent prospec-tive series of 8,741 arthroscopies performed by “experi-enced” arthroscopists, the incidence of saphenous neu-ropathy after a meniscal repair was 0.01% and theincidence of complications after meniscal repair (withboth inside-out and outside-in techniques) was actuallylower (1.29%) than for arthroscopic meniscectomy(1.69%).49 More recently, numerous case reports havebeen published outlining the problems that can be en-countered with the use of arthroscopic fixators includingpull-out and pull-through device failure with migrationand breakage, cystic hematoma, foreign body reaction,and chondral injury.23,29–37 Intraoperative and postopera-tive complications after meniscal repair surgery can beclassified as major and minor.50
Major complications can be considered any signifi-cant untoward event that requires a subsequent surgicalprocedure, hospitalization, or significantly changes thepostoperative course of the patient. These include com-mon peroneal, tibial, and saphenous nerve injuries andpopliteal artery and vein injuries. Deep infection, post-operative septic arthritis and arthrofibrosis, sympatheti-cally mediated Type II complex regional pain syn-dromes, and mechanical abrasion of the chondralsurfaces from prominent implants associated with chon-dral injury are also included. Thromboembolic diseaseincluding deep vein thrombosis and pulmonary embo-lism as well as failure of meniscal healing with persistentclinical symptoms of pain, swelling, and mechanicalsymptoms are considered major complications. Minorcomplications can be considered self-limiting, transient,and not associated with any extended or permanent dis-ability and include superficial infection, transient foreignbody reactions and synovitis, retained and/or migratingand painful fixator fragments, and transient soft tissueinflammation.
� RESULTSNumerous studies have been directed towards mechani-cal testing of various suture materials and patterns ofsuture placement.40,42–44,51 More recently, work has beenperformed to assess the behavior of repair devices exvivo and to compare suture to different available fixatordevices.41,52,53 It is important to point out that multiplefactors can affect the laboratory data, including the vari-ous polymer material properties, size, geometry, design,and degradation kinetics. Mechanical testing of pull-out,pull-through, repair site strength, load to failure, cyclictesting, hydrolysis time effects, and animal model versushuman cadaveric aged specimens all can introduce con-
founders that make result interpretation more complex.In general, vertical mattress suture configurations per-form more optimally than horizontal patterns. In addi-tion, most fixators are associated with less mechanicalstrength than suture, specifically vertical mattress non-absorbable suture.40,41,44,52,54
Outcomes after meniscal repair have been publishedfor the various discussed techniques. DeHaven reported100% retrieval of 33 cases with an average age of 18.9years, at average 10.9-year follow-up (range: 10.1–13)treated with open meniscal repair and noted a 79% long-term survival rate. Radiographic analysis revealed that85% of patients noted to have a successful repair out-come had no significant degenerative changes comparedto 43% of patients with recurrent meniscal tearing andpresumably repair failure. It was concluded that in-creased re-tear rates were noted in knees that were ACLdeficient.17,18
Early reports of results after the inside-out repairtechnique were reported by Henning in 260 repairs per-formed in 240 patients, with an average age of 22 yearsat an average follow-up of almost 2 years. ConcomitantACL reconstruction was performed in 80% of cases. Theresults indicated that 62% of repairs were healed on ar-throscopic second look or by arthrogram compared to17% incompletely healed and 21% not healed. Of note,based on clinical and subjective evaluation, 92% of caseswere stable and 80% returned to active sports.16
In a comprehensive review of 117 consecutive in-side-out repairs, by Cannon, 90 cases were reported on;68 repairs with concomitant ACL reconstruction and 22isolated repairs.12 The average age was of the patientswas 27 years. Overall rate of clinical success was 82%,with 93% of the ACL-associated cases successful com-pared to 50% of the isolated cases. Several conclusionswere discussed including that clinical success tends tobe better than arthroscopic assessed (anatomic) and ar-throgram-assessed success. In cases in which rim widthwas up to 2 mm, success was 96% compared to 50%in case of rim widths out to 4 to 5 mm. Tear lengthsof less than 2 cm were associated with success in94%, whereas in cases greater than 4 cm, this droppedto 50%. Lateral repairs (70–100%) fared better than me-dial (34–73%). Age of the patient did not seem to matter,and patients with tears less than 8 weeks old were asso-ciated with 88% success compared to 79% in the“chronic” tears.
Outside-in technique results have been published byRodeo, who found that in 90 patients average 25 years atan average follow-up of 46 months (range: 36–89months), an overall 87% had a successful outcome.22
Failure was noted in 38% of the unstable knees, 15% ofthe stable knees, and 5% of the ACL reconstructedknees. The author concluded that the results after this
Meniscus Repair
123Volume 1, Issue 2

technique were comparable to results reported after in-side-in repairs and pointed out that it is especially usefulfor repairing tears in the anterior horn region.
The more recent introduction of meniscal repair fix-ators has narrowed the outcome conclusions, and long-term published data remain limited.55–57 Jones et al. re-ported on a retrospective series of 38 patients undergoingmeniscal repair with the Meniscal Arrow (Bionx) at29.7-month follow-up. In 21 cases in which concomitantACL reconstruction was performed, no clinical failures(defined as reoperation) were noted, whereas in 17 iso-lated repair cases, success was noted in 93%. The authorsnoted, however, that there was a 31.6% incidence oftransient local soft-tissue inflammation related to devicemigration, length, prominence, and possible reaction tothe resorbable materials.23 Petsche reported on a singlesurgeon’s experience with the Meniscus Arrows in 29patients with an average age of 29 years available forfollow-up at an average of 24 months after meniscalrepair surgery. He found that there was a 7% incidence offailure, and in five cases mild subcutaneous irritation wasnoted that resolved in all cases within 3 to 7 months.24 Ina published prospective report of 37 patients, average age26.8 years, undergoing repair with the Mitek MeniscalFastener (Mitek, Norwood, Massachusetts) at 1 year fol-low-up, there were 5 reruptures and 32 cases in which theprocedure was interpreted as successful. The authorsconclude that the failure rate was comparable to that ofother studies in the literature and that the healing rate washigh with few associated complications.58
The author’s own unpublished results include a con-secutive series of 109 meniscal repairs performed usingan all-arthroscopic hybrid technique. The technique usedwas a hybrid combination and use of two devices, theMeniscal Arrow (Bionx) and the T-Fix system (Smithand Nephew Endoscopy), a first-generation device com-prising nonabsorbable braided synthetic suture and a5-mm polyacetal suture bar that is inserted and anchoredbeyond the tear extracapsularly. Arthroscopic knots arethen tied to stabilize the tear site between the 3- to 5-mminsertion spacing of two of the implants.59 The studygroup was followed prospectively, with the average age28 years (range: 15–49 years) and the average follow-up3.2 years (range 2 to 4.4 years). The Meniscal Arrow wasused exclusively for the repair in 55% of cases, whereasArrows and the T-Fix were used in 45% of cases. Thedecision to select which cases were treated with the hy-bridized approach was not randomized but rather wasbased on the geometry and extent of the tear, tissue vi-ability, and stability of the repair site. An associatedACL reconstruction was performed in 72 cases (60%),whereas an isolated repair was performed in 37 cases(40%). All isolated repairs were treated with an autolo-gous fibrin clot technique. All patients received uniform
postoperative care with 4 weeks of bracing in extensionbeginning with immediate range of motion 0 to 90° in-creasing beyond that at 4 weeks and partial weight-bearing on crutches for 4 weeks. Return to sports orstressful activity was advised in all cases after the 6months. Result analysis revealed that no difference wasnoted at outcome between the Arrow alone groupcompared to the hybrid group. The overall failure rate,defined as the need to return for meniscal surgery,was 5.5%, with the isolated repair cases noted to havefour failures (10.8%), whereas in the ACL reconstructedcases, there was a failure rate of 2.7% (two cases).No significant differences were noted between thesegroups. Several conclusions were drawn, including thatsatisfactory success could be obtained with an all-arthroscopic technique, that hybridized methods thatincorporate suture and fixators may improve clinicalresults, and that isolated repair outcomes can approachthe results noted with repair in association with ACLsurgery.
In conclusion, review of most published study resultsreveals that clinical success after meniscal repair is com-parable whether open, inside-out, outside-in, or all-arthroscopic fixator methods are used. In all studies,those cases of meniscal repair that are performed in con-junction with an ACL reconstruction clearly are associ-ated with a higher rate of healing and more optimal clini-cal success than cases of isolated meniscal repair. Thismay be due to several factors including the release ofmarrow elements from osseous tunnel drilling that pro-mote healing, the pain associated with a more complexsurgery that “slows down” the patient postoperatively,thereby protecting the repair and the effect of ligamen-tous stabilization of the knee. There appears to be a sig-nificant potential for transient soft-tissue inflammationassociated with some of the fixator devices; however, asmore clinical experience is accrued and as the devicesand polymer materials improve, these problems may be-come reduced.
� SUMMARYMeniscal repair in select active individuals with repair-able meniscal tears should be performed whenever indi-cations are met and appropriate patient counseling re-garding outcomes is addressed. Far more meniscalresections will nonetheless be carried out compared tomeniscal repairs. As the techniques and devices continueto improve, the decision to select one technique or tech-niques over another should ultimately be based on thesound evaluation of and experience associated with aparticular device and its safety and potential efficacy.Surgeon preference and comfort with what works winsout over certain learning curve issues. Overall indica-
N. A. Sgaglione
124 Techniques in Knee Surgery

tions for the use of one technique over another may bedependent also on the types of tear that are repaired. Ingeneral, meniscal fixators and implants should be usedfor vertical, longitudinal red–white tears that are not pe-ripheral detachments and are associated with at least a 2-to 3-mm rim width to provide optimal barb–tissue con-tact. Inside-out or outside-in suture may be best used forrepair of more complex tear patterns or less vasculartears with less optimal tissue viability or with significantdeformity or deformation as seen in large displacedbucket-handle tears. In addition, in cases of peripheralcapsular detachment of the meniscus or in repairingmeniscal allografts, suture should be used. Outside-intechniques may be particularly useful in cases of anteriorhorn, mid one-third tears, or in radial tears that extend tothe periphery (Table 5).
The future remains bright, as on the horizon, devel-opments in the area of polymer science will continue toprovide better resorbable devices that will have safer andmore bioinert degradation profiles that are more biologi-cally specific to meniscal tissue and the temporal profilesof meniscal healing.26 The use of biologic and/or non-biologic adhesives may prove to be promising, and initialwork using amphibian-derived adhesives for treatment ofmeniscal tears in a large-animal model has demonstratedoptimal mechanical strength and sealant characteristics.(Zoltan S. Meniscus repair using frog glue. Presented atthe 68th Annual Meeting of the American Academy ofOrthopaedic Surgeons Specialty Day Meeting of theAmerican Orthopaedic Society for Sports Medicine, SanFrancisco, CA, 2001). Laboratory work in the area ofgrowth factors may provide a platform in which repairdevices may soon have incorporated within them bioac-tive factors and anabolic polypeptides. Through controlof dosing, delivery, and release mechanisms, these fac-tors may promote and enhance healing, thereby speedingup recovery and simplifying postoperative protocols.
Eventually, these methods may extend and expand theindications for repair to avascular tear sites. Much workis being done in the area of tissue engineering and mo-lecular genetics.60 Gene-enhanced methods of repairingmeniscal tears are being worked on in the laboratory withthe use of genes virally transferred to transfected fibro-chondrocytes that are expanded in culture and producecatabolic agents such as insulin growth factor (Grande D.Gene enhanced tissue engineering repair of the meniscus.Presented at the 27th Annual Meeting of the AmericanOrthopaedic Society for Sports Medicine, Keystone, CO,2001). The cells or tissue construct are then implantedinto the tear site defects to promote healing. The use ofbiologic extracellular matrices such as porcine small in-testine submucosa to promote a meniscal healing re-sponse through angiogenesis and host cell proliferation isalso being investigated.61 Finally, the use of photody-namic devices in conjunction with reactive chemical“dyes” has been reported and may be applied to areas ofmeniscal disease to covalently bond collagen fibers andproduce a seal and/or reduce propagation of a tearthrough “tissue welding” (Jackson R, personal commu-nication, 2002). These methods represent the potentialfuture of orthopedics and may one day be a reality inclinical orthopedic practice.
� CONCLUSIONS
1. As the emphasis on comprehensive knee reconstruc-tion increases, and the importance of meniscal struc-ture and function is further documented, the indica-tions for meniscal repair are expanding.
2. Meniscal repair techniques have continued to signifi-cantly evolve, and numerous implant fixators areavailable that have improved surgical options.
3. Outside-in, inside-out, and all arthroscopic fixatormethods remain popular and are each associated withadvantages and disadvantages and successful out-comes. Hybridized techniques may be used to com-bine the best of all techniques in select cases.
4. Second-generation implant devices that combine su-ture and arthroscopic implant anchors may result in arepair construct that affords compression across thetear, thereby improving tensile strength.
5. Postoperative care should be individualized depend-ing upon the tear site, size, tissue viability, repairstrength, and device used.
6. The future of meniscal repair may include biologicmanipulation of healing through bioactive peptidesand growth factors that may be delivered via incor-poration in repair sutures or fixator implants. Gene-enhanced tissue engineering may have a role in theapproach to meniscal disease.
TABLE 5. Repair techniques indications
Outside-in sutures Anterior horn tearsMid-third tearsRadial tearsComplex tears
Inside-out sutures Posterior horn tearsMid-third tearsDisplaced bucket-handle tearsPeripheral capsular tearsMeniscal allografts
Fixator implants Posterior horn tearsTears with > 2 to 3 mm rim
widthVertical, longitudinal tears
Suture-based and devices Posterior horn tears(2ND generation devices) Mid-third tears
Bucket handle tearsRadial tears
Meniscus Repair
125Volume 1, Issue 2

� REFERENCES
1. Kettlekamp D, Jacobs A. Tibiofemoral contact area: deter-mination and implications. J Bone Joint Surg 1972;54:349–56.
2. Levy M, Torzilli P, Warren R. The effect of medial men-iscectomy on anterior–posterior motion of the knee. J BoneJoint Surg 1982;64:883–8.
3. Radin E, de Lamotte F, Maquet P. Role of the menisci inthe distribution of stress in the knee. Clin Orthop 1984;185:290–4.
4. Shoemaker S, Markolf K. The role of the meniscus in theanterior–posterior stability of the loaded anterior cruciatedeficient knee: effects of partial versus total excision.J Bone Joint Surg 1986;68:71–9.
5. Beaupre A, Choukroun R, Guidouin R, et al. Knee menisci:correlation between microstructure and biomechanics. ClinOrthop 1986;208:72–5.
6. Sommerlath K, Gillquist J. Knee function after meniscusrepair and total meniscectomy: a 7-year follow-up study.Arthroscopy 1987;3:166–9.
7. Jorgensen U, Holm S, Lauridsen F, et al. Long termfollow-up of meniscectomy in athletes: a prospective lon-gitudinal study. J Bone Joint Surg [Br] 1987;69:80–3.
8. Johnson R, Kettelkamp D, Clark W. Factors effecting lateresults after meniscectomy. J Bone Joint Surg [Am] 1974;56:719–29.
9. Tenuta J, Arciero R. Arthroscopic evaluation of meniscalrepairs: factors that effect healing. Am J Sports Med 1994;22:797–802.
10. Hede A, Larsen E, Sandberg H. Partial versus total men-iscectomy. J Bone Joint Surg [Br] 1992;74:118–21.
11. Fauno P, Nielsen A. Arthroscopic partial meniscectomy: along term follow-up. Arthroscopy 1992;8:345–9.
12. Cannon W, Vittori J. The incidence of healing in an ar-throscopic meniscal repairs in ACL-reconstructed kneesversus stable knees. Am J Sports Med 1992;20:176–81.
13. Belzer J, Cannon W. Meniscal tears: treatment in the stableand unstable knee. J Am Acad Orthop Surg 1993;1:41–7.
14. King D. The function of semilunar cartilages. J Bone JointSurg 1936;18:1069–76.
15. Henning C, Lynch M, Yearout K, et al. Arthroscopicmeniscal repair using an exogenous fibrin clot. Clin Or-thop 1990;252:64–72.
16. Scott G, Jolly B, Henning C. Combined posterior incisionand arthroscopic intra-articular repair of the meniscus.J Bone Joint Surg [Am] 1986;68:847–61.
17. DeHaven K, Lohrer W, Lovelock J. Long term results ofopen meniscal repair. Am J Sports Med 1995;23:524–30.
18. DeHaven K. Meniscus repair. Am J Sports Med 1999;27:242–50.
19. Arnoczky S, Warren R, Spivak J. Meniscal repair using an
exogenous fibrin clot. An experimental study in dogs.J Bone Joint Surg 1988;70:1209–17.
20. Gillquist J, Messner K. Long-term results of meniscal re-pair. Sports Med Arthro 1993;1:159–63.
21. Eggli S, Wegmuller H, Kosina J, et al. Long term results ofarthroscopic meniscal repair: an analysis of isolated tears.Am J Sports Med 1995;23:715–20.
22. Rodeo S. Arthroscopic meniscal repair with use of theoutside-to-inside technique. J Bone Joint Surg [Am] 2000;82:127–41.
23. Jones H, Lemos M, Wilk R, et al. Two-year follow-up ofmeniscal repair using a Bioabsorbable Arrow. Arthroscopy2002;18:64–9.
24. Petsche T, Selesnick H, Rochman A. Arthroscopic menis-cal repair with Bioabsorbable Arrows. Arthroscopy 2002;18:246–53.
25. Bach B, Bush-Joseph C. The surgical approach to lateralmeniscal repair. Arthroscopy 1992;8:269–73.
26. Ciccone W, Motz C, Bentley C, et al. Bioabsorbable im-plants in orthopaedics: new developments and clinical ap-plications. J Am Acad Orthop Surg 2001;9:280–8.
27. Port J, Jackson D, et al. Meniscal repair supplemented withexogenous fibrin clot and autologous cultured marrowcells in the goat model. Am J Sports Med 1996;24:547–55.
28. Albrecht-Olsen P, Kristensen G. Meniscus bucket-handlefixation with an absorbable Biofix Tack: development of anew technique. Arthroscopy 1993;1:104–6.
29. Anderson K, Marx R, Hannafin J, et al. Chondral injuryfollowing meniscal repair with a biodegradable implant.Arthroscopy 2000;16:749–53.
30. Ganko A, Engebretsen L. Subcutaneous migration ofmeniscal arrows after failed meniscus repair. Am J SportsMed 2000;28:252–3.
31. Hechtman K, Uribe J. Cystic hematoma formation follow-ing use of a Biodegradable Arrow for meniscal repair.Arthroscopy 2000;15:207–10.
32. Hutchinson M, Ash S. Failure of a Biodegradable MeniscalArrow. Am J Sports Med 1993;27:101–3.
33. Oliverson T, Lintner D. Biofix Arrow appearing as a sub-cutaneous foreign body. Arthroscopy 2000;16:652–5.
34. Ross G, Grabill J, McDevitt E. Chondral injury aftermeniscal repair with Bioabsorbable Arrows. Arthroscopy2000;16:754–6.
35. Menche D, Phillips G, Pitman M, et al. Inflammatory for-eign-body reaction to an arthroscopic bioabsorbableMeniscal Arrow repair. Arthroscopy 1999;15:770–2.
36. Song E, Lee K, Yoon T. Aseptic synovitis after meniscalrepair using the biodegradable Meniscus Arrow. Arthros-copy 2001;17:77–80.
37. Whitman T, Diduch D. Transient posterior knee pain withthe Meniscal Arrow. Arthroscopy 1998;14:762–3.
38. Albrecht-Olsen P, Kristensen G. The meniscus tack versus
N. A. Sgaglione
126 Techniques in Knee Surgery

horizontal suture in arthroscopic meniscus repair: a pro-spective randomized study with arthroscopic evaluation.Arthroscopy 1999;7:268–73.
39. Albrecht-Olsen P, Lind T, Kristensen G, et al. Failurestrength of a new Meniscus Arrow repair technique: bio-mechanical comparison with horizontal suture. Arthros-copy 1997;13:183–7.
40. Boenisch U, Faber K, Ciarelli M, et al. Pull-out strengthand stiffness of meniscal repair using absorbable arrows orTi-Cron vertical and horizontal loop sutures. Am J SportsMed 1999;27:626–31.
41. Becker R, Schroder, Starke C, et al. Biomechanical inves-tigations of different meniscal repair implants in compari-son with horizontal sutures on human meniscus. Arthros-copy 2001;17:439–44.
42. Post W, Akers S, Kish V, et al. Load to failure of commonmeniscal repair techniques: effects of suture techniquesand suture material. Arthroscopy 1997;13:731–6.
43. Rimmer M, Nawana N, Keene G, et al. Failure strengths ofdifferent meniscal suturing techniques. Arthroscopy 1995;11:146–50.
44. Seil R, Rupp S, Kohn D. Cyclic testing of meniscal sutures.Arthroscopy 2000;5:505–10.
45. Song E, Lee K, Yoon T. Biomechanical test comparing theload to failure of the biodegradable meniscus arrow versusmeniscal suture. Arthroscopy 1999;15:726–32.
46. Barber F. Accelerated rehabilitation for meniscus repairs.Arthroscopy1997;10:206–10.
47. Small N. Complications in arthroscopy: the knee and otherjoints. Arthroscopy 1986;2:253–8.
48. Austin K, Sherman O. Complications of arthroscopicmeniscal repair. Am J Sports Med 1993;21:864–9.
49. Small N. Complications in arthroscopic surgery performed
by experienced arthroscopists. Arthroscopy 1988;4:215–21.
50. Rodeo S, Forster R, Weiland A. Neurological complica-tions due to arthroscopy. J Bone Joint Surg [Am] 1993;75:917–26.
51. Albrecht-Olsen P, Kristensen G, Burgaard P, et al. Thearrow versus horizontal suture in arthroscopic meniscusrepair. Knee Sports Trauma Arthro 1999;7:268–73.
52. Barber F, Herbert M. Meniscal repair devices. Arthroscopy2000;16:613–8.
53. Arnoczky S, Lavagnino M. Tensile fixation strengths ofabsorbable meniscus repair devices as a function of hydro-lysis time: an in-vitro experiment study. Am J Sports Med2001;29:118–23.
54. Dervin G, Downing K, Keene G, et al. Failure strengths ofsuture versus biodegradable arrow for meniscal repair: anin-vitro study. Arthroscopy 1997;13:296–300.
55. Lombardi J. Second-look arthroscopy with removal of bio-absorble tacks. Am J Orthop 2000;Feb.:125–7.
56. Hurel C, Mertens F, Verdonk R. Biofix resorbable Menis-cus Arrow for meniscal ruptures: results of a 1-year fol-low-up. Knee Surg Sports Trauma Arthro 2000;8:46–52.
57. Cohen B, Tasto J. Meniscal Arrow. Tech Orthop1998;13:164–9.
58. Laprell H, Stein V, Petersen W. Arthroscopic all-insidemeniscus repair using a new refixation device: a prospec-tive study. Arthroscopy 2002;18:387–93.
59. Coen M, Caborn D. An anatomic evaluation of T-Fix su-ture device placement for arthroscopic all-inside meniscalrepair. Arthroscopy 1999;15:275–80.
60. Goto H, Shuler F, Lamsam C, et al. Transfer of LacZmarker gene to the meniscus. J Bone Joint Surg [Am]1999;81:918–25.
61. Badylak S, Arnoczky S, Plouar P, et al. Naturally occurringextracellular matrix as a scaffold for musculoskeletal re-pair. Clin Orthop 1999;367S:333–43.
Meniscus Repair
127Volume 1, Issue 2