Embed Size (px)
Citation preview

127
Lateral Ankle Exam and Imaging Understanding lateral ankle in-juries requires knowledge of the pertinent anatomy and familiarity with proper physical exam tech-niques. The exam itself is based on understanding the anatom-
L ateral ankle instability is one of the most common traumatic events the foot and ankle surgeon will en-counter. There are approxi-
mately two million acute sprains per year, or about 20,000 a day that are reported. The most common are lat-eral ankle injuries making up approx-imately 85% of sprains.1 The remain-der of “sprains” are less common and include the deltoid or medial ankle sprain, as well as “high ankle sprains,” or injuries of the syndes-mosis. This article will focus on the more common lateral ankle injuries, Continued on page 128
Welcome to Podiatry Management’s CME Instructional program. Podiatry Management Magazine is approved by the Council on Podiatric Medical Education as a provider of continuing education in podiatric medicine. Podiatry Management Magazine has approved this activity for a maximum of 1.5 continuing education contact hours. This CME activity is free from commercial bias and is under the overall management of Podiatry Management Magazine. You may enroll: 1) on a per issue basis (at $29.00 per topic) or 2) per year, for the special rate of $249 (you save $41). You may submit the answer sheet, along with the other information requested, via mail, fax, or phone. You can also take this and other exams on the Internet at www.podiatrym.com/cme. If you correctly answer seventy (70%) of the questions correctly, you will receive a certificate attesting to your earned credits. You will also receive a record of any incorrectly answered questions. If you score less than 70%, you can retake the test at no additional cost. A list of states currently honoring CPME approved credits is listed on pg. 136. Other than those entities currently accepting CPME-approved credit, Podiatry Management cannot guarantee that these CME credits will be acceptable by any state licensing agency, hospital, managed care organization or other entity. PM will, however, use its best efforts to ensure the widest acceptance of this program possible. This instructional CME program is designed to supplement, NOT replace, existing CME seminars. The goal of this program is to advance the knowledge of practicing podiatrists. We will endeavor to publish high quality manuscripts by noted authors and researchers. If you have any questions or comments about this program, you can write or call us at: Program Management Services, P.O. Box 490, East Islip, NY 11730, (631) 563-1604 or e-mail us at [email protected]. Following this article, an answer sheet and full set of instructions are provided (pg. 136).—Editor
www.podiatrym.com FEBRUARY 2020 | PODIATRY MANAGEMENT
with focus on both acute and chron-ic pathology as well as frequently associated injuries. The goal of this article is for the reader to understand the pathology associated with the lateral ankle sprain and learn the cur-rent treatment recommendations and techniques.
Lateral Ankle Injuries: Scope and Stabilization Proper diagnosis and treatment leads to better outcomes.
By Patrick r. Burns, DPM
Surgical PoDiatrycontinuing
Medical Education
Goals and Objectives
1) To understand the pathology associated with the lateral ankle sprain
2) To learn the current treatment recommendations and techniques.
Understanding lateral ankle injuries requires knowledge of the pertinent anatomy and familiarity
with proper physical exam techniques.

Laterally, there are three liga-ments of most concern. Once all other issues are ruled out, the ante-rior talofibular (ATFL), calcaneofib-ular (CFL), and posterior talofibular (PTFL) ligaments are surveyed. The least likely to injure is the PTFL. It is perhaps the strongest, but it also protects the ankle from poste-rior translation, which is much less common as far as mechanism. Be-cause of this, it tends to only be rup-tured in severe injuries such as talus dislocation. The PTFL is difficult to examine clinically but can be seen on MRI images. The CFL is a relatively strong ligament and primarily resists inver-sion forces, particularly when the foot is neutral or dorsiflexed. It orig-inates on the distal fibula and inserts into the calcaneus and plays a role in both ankle and subtalar instabili-
ty. The course of the CFL is easy to palpate from the distal tip of the fib-ula to the lateral wall of the calcane-us and is tested with a talar tilt test or inversion stress clinically. This test is less useful in acute injuries because of guarding but is certainly helpful in cases of chronic insuffi-ciency. Most frequently, the amount of inversion while the foot is in neu-tral is compared to the contralateral side, but it can also be compared on radiographs.
ATFL The ATFL is the most common ligament injury. It is the only intra-capsular ligament and is the weakest of the three lateral ankle ligaments. It is easy to palpate at the anterior edge of the fibula, extending toward the neck of the talus. The ATFL re-sists anterior translation of the talus, but also aids in limiting inversion when the foot is in a plantarflexed position. This ligament is likely to be tender with palpation, and the most common clinical exam is the anterior drawer test. This is typically done
ic structures of the lateral ankle and the related surface anatomy. As with most exams, there should be a systematic approach. In the acute ankle sprain, it may be more difficult as edema and guarding
may interfere, so starting the eval-uation away from the primary area of complaint avoids irritating the lateral ankle and subsequently lim-iting participation in the remaining examination. The exam should be based on a knowledge of injuries associated with inversion or twist-ing-type mechanisms. Edema, ecchymosis, and ankle joint effusion should be noted, and neurovascular status of the inter-mediate dorsal cutaneous and sural sensory distributions should be doc-umented. The exam is then moved to muscle strength, which again may be guarded, but making sure all groups are functioning, paying attention to the peroneal tendons laterally and noting any pathology such as tenderness, loss of power, or subluxation. Bone is next on the
list, palpating the proximal fibula to help rule out high fibular fracture, and a squeeze test at mid-leg will give information about syndesmotic involvement. The lateral process of the talus, anterior process of the calcaneus, base of the fifth metatarsal, and the
Lisfranc complex should all be ex-amined as they all may be associated with the typical lateral ankle/inver-sion mechanism. Finally, attention is now turned to the primary area of concerns and a more thorough exam of the lateral ankle ligaments, remembering they are typically ten-
der so the exam may be limited. The deltoid ligament is first palpated to ensure that there is no medial injury. The lateral ankle ligaments are the last to examine, again remembering anatomic characteristics during pal-pation and the exam (Figure 1).
www.podiatrym.comFEBRUARY 2020 | PODIATRY MANAGEMENT
128
contin
uing
Medica
l Edu
cation
Surgical PoDiatry
Lateral Ankle (from page 127)
Continued on page 129Figure 1: anatomic location and palpation of the aTFl (a) and cFl (B).
a B
The calcaneal fibular ligament is tested by inversion stress during physical examination.
The calcaneal fibular ligament is part of the lateral ankle ligament complex.
need for radiographs, and the Ottawa ankle rules may be of some benefit in decision-mak-ing, trying to limit unnecessary imaging and radiation exposure by as much as 30-40%.2 However, the standard of care with lateral ankle injury generally includes radiograph-
ic evaluation. Radiographs not only aid in the diagnosis of fracture but can be useful for those with chronic instability, looking for biomechan-ical causes such as pes cavus and calcaneal or ankle varus. Pes cavus is commonly associated with lateral ankle instability.
X-Rays Typical radiographs include the anterior-posterior (AP), mortise, and lateral images of the ankle. These images would be utilized to diagnose large fracture issues, but also smaller avulsion types that can be utilized in the diagnosis of spe-cific ligament injuries. The overlap of the tibia and fibula on the mor-tise is at times helpful in syndes-motic injury and should be com-pared to the contralateral ankle. Large fracture and syndesmotic in-jury are out of the scope of this article but obviously should be con-sidered and recognized.
MRI MRI is the standard imaging for lateral ankle sprain and ligament in-jury. This should only be utilized when the information is useful. Most ankle sprains resolve with non-surgi-cal means, and so MRI should only be ordered in cases that either have high suspicion of a larger issue at the initial exam, or those that con-tinue to express symptoms and do not progress at 10-12 weeks post-in-jury and treatment. For most inju-ries, MRI in the early weeks only clouds treatment as the MRI will show edema and torn or attenuated ligaments, which is information al-
by holding the tibia and heel firmly and applying opposing forces at the ankle. If there is an issue with the competency of the ATFL, the ankle will displace anteriorly.
Anterior Drawer Test A positive anterior drawer test re-veals a large “dimple” at the anatom-ic location of the ATFL, signifying its lack of integrity whether it is acute or chronic. This is somewhat contro-versial, however. Since many ankle sprains do not occur when the foot is in a neutral position, the anterior drawer test should be performed with
the foot in slight plantarflexion. That is when the ATFL, from an anatomic standpoint, is engaged to aid the CFL in limiting inversion.
Imaging Imaging is typically the next step. Standard radiographs are com-
mon and include the ankle and foot depending on physical exam find-ings. There is some debate about the
www.podiatrym.com FEBRUARY 2020 | PODIATRY MANAGEMENT
129
continuing
Medical Education
Surgical PoDiatry
Lateral Ankle (from page 128)
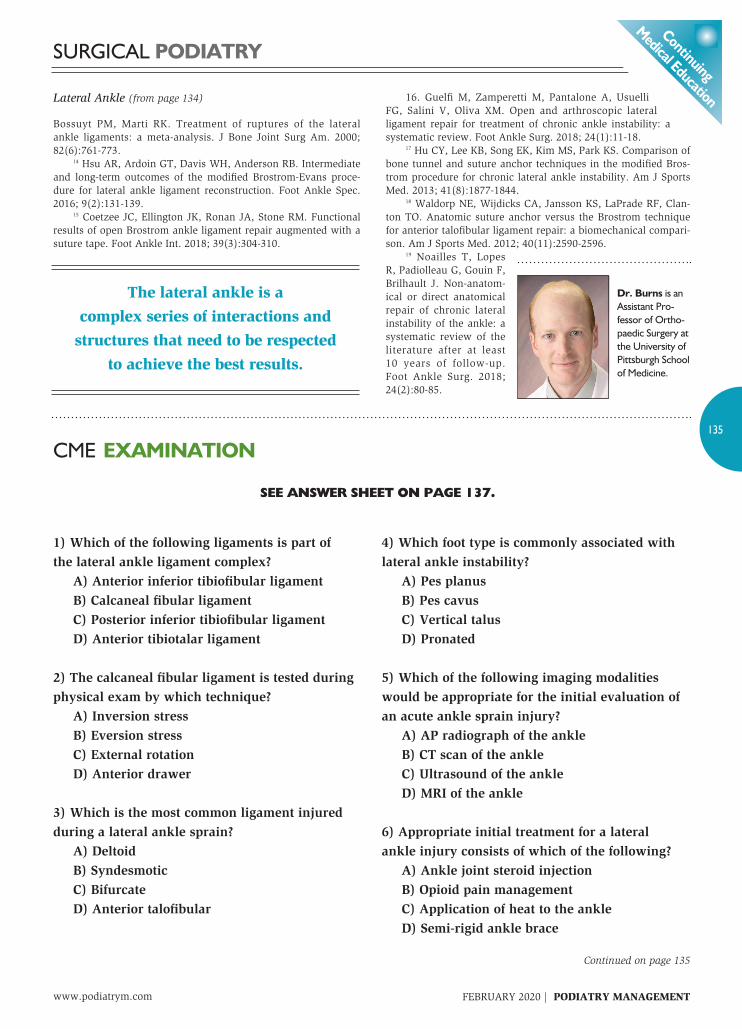
Continued on page 130Figure 3: Mri of normal appearing cFl (a) and attenuated cFl (B). Note this ligament is deep to the peroneal tendons.
a B
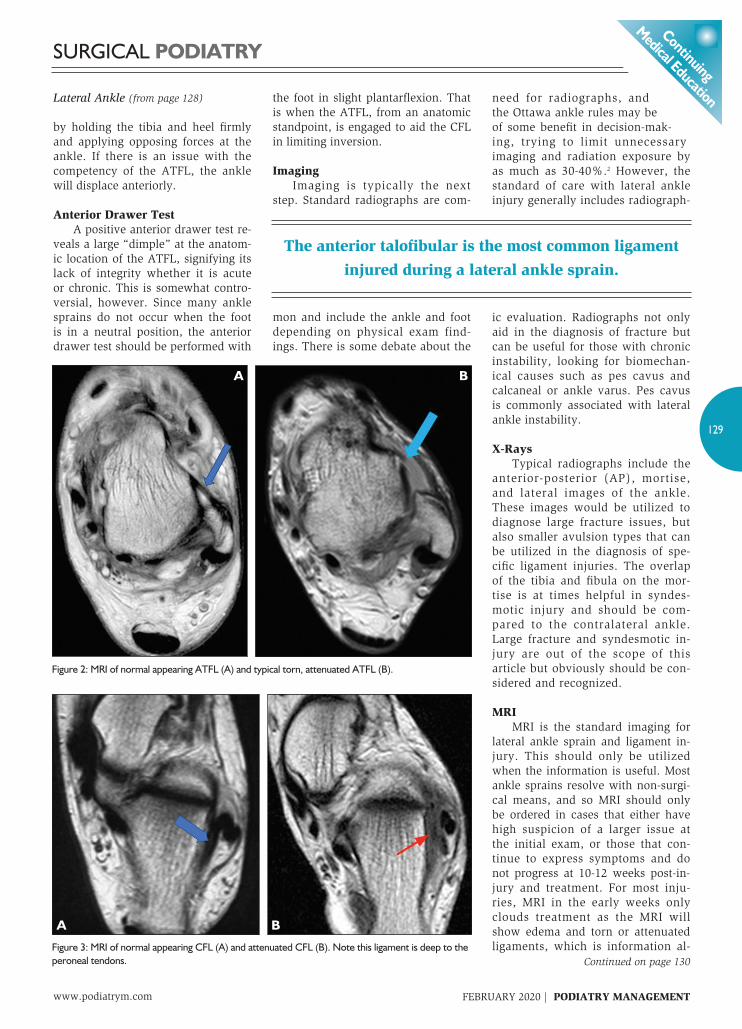
Figure 2: Mri of normal appearing aTFl (a) and typical torn, attenuated aTFl (B).
a B
The anterior talofibular is the most common ligament injured during a lateral ankle sprain.

metrics normalize over 4 months whether supervised or not, and re-in-jury rates between supervised and home programs are debated.6-8
If there is continued instability, pain, reliance on bracing, or other continued symptoms after 12 weeks of supervised treatment, advanced
imaging such as MRI is suggested. The advanced imaging is to help determine the potential cause of the symptoms and to then aid in surgi-cal planning. Arthroscopy is an in-tegral part of most surgical plans. It is a useful tool for diagnosis as well as managing intra-articular patholo-gy. However, MRI has low inter-ob-server reliability in chronic ankle instability, and has been shown that synovitis and osteochondral lesions of the talus may be under-appreci-ated with MRI sensitivity of 21% and 46%, respectively.9 Given that intra-articular pathology is noted to present in as much as 95% of ankle scopes performed during later-al ankle ligament procedures, it has been recommended that arthroscop-ic examination be considered in pa-tients with continued symptoms, even without MRI findings of in-tra-articular lesions.9-11
Ankle Arthroscopy Ankle arthroscopy is a work-horse of lateral ankle injury surgical treatment. Manipulating the camera
ready known from the history and exam. MRI should only be consid-ered when there are continued issues to aid in the diagnosis or treatment of chronic pathology, such as unhealed ligaments, osteochondral defects, or peroneal tendinopathy that may be limiting recovery. When an MRI is obtained, the physician should be able to identi-fy the appropriate anatomy as well as normal and abnormal findings. In particular, one should note the appearance of the ATFL and CFL as well as the peroneal tendons, articu-lar cartilage, and all associated struc-tures of the lateral ankle. The liga-ments should appear as homogenous black structures, with attenuated or partially torn ligament showing signs of edema and thickening or absence of the structure in the case of com-plete tears. The ATFL is best viewed on a modified axial image (Figure 2), while the CFL is best seen on axial and cor-onal images deep to the peroneal ten-dons. The articular surface should be uniform without depression or defect. Peroneal tendons likewise should be uniform black circles on axial imag-es without edema. One should pay close attention to the shape of the peroneal tendons, looking for tendino-sis and tear as well as abnormalities
to the peroneal retinaculum, the presence of te-nosynovitis and low-lying mus-cle belly that may contribute to impingement, subluxation, and the shape of the posterior fibu-lar groove. All of these issues can contribute to continued pain after lateral ankle sprain and may need to be addressed surgically when a patient has not responded to conser-vative management.
Lateral Ankle Injury Treatment The mainstay of lateral ankle in-jury is non-operative, with most pa-
tients responding to initial splinting, immobilization, rest, ice, anti-in-flammatory modalities, and physical therapy. Early, controlled mobiliza-tion with functional rehabilitation generally allows patients to return to work 2-4 times faster than those
treated with initial sur-gery or casting with simi-lar functional outcomes.3-4 Therapy typically consists of range-of-motion exercis-es, stretching, strengthen-ing, and proprioceptive or balance and control exer-cises. The proprioceptive exercises have been shown to be particularly useful for prevention of re-injury in patients with a sprain and for primary prevention of injury.5
Rehabilitation under di-rect supervision compared with home exercise pro-grams has been shown to improve short-term patient recorded outcomes—in-cluding pain, strength, and instability. However, these
www.podiatrym.comFEBRUARY 2020 | PODIATRY MANAGEMENT
130
contin
uing
Medica
l Edu
cation
Surgical PoDiatry
Lateral Ankle (from page 129)
Continued on page 131Figure 5: Typical portals and surface anatomy for ankle arthroscopy.
Figure 4: comparison of 2.0mm lens (top) and 4.0 mm lens (bottom).
Pes cavus is commonly associated with lateral ankle instability.

jority of access and tend to be the safest. The anterome-dial is typically the first and is placed at the level of the ankle joint line just medial to the tibialis ante-rior tendon. The incision is vertical and deepened with a hemostat to the level of the joint capsule. A tro-char and cannula are then introduced through this incision and the capsule is entered. The trochar is removed and the camera and lens are placed through the cannula. Once the joint is visualized, ini-tial inspection can be performed taking note of synovitis, cartilage lesions, or other abnormalities. The camera light is then utilized to help transilluminate the skin of the later-al ankle joint to aid in the position-ing of the anteriolateral incision. An 18 gauge needle can then be introduced into the ankle joint just lateral to the long extensor tendons to help directly visualize the access of this portal. This ensures instru-ments placed through this portal have direct line access to the joint and pathology. When confirmed, the incision is made vertically, tak-ing care to avoid veins and the in-termediate dorsal cutaneous nerve which are being transilluminated from below.
Both the camera and shaver are now able to be moved through the joint, inspecting and removing pathology as needed. Arthroscopy will frequently encounter synovitis, both chronic and acute, as well as adhesions, meniscoid bodies, osteo-chondral pathology, loose bodies, and other ligament issues (Figure 6). One common pathology noted laterally is the Bassett ligament, a prominent low extension of the an-terior inferior tibiofibular ligament. Most consider this a normal ana-tomic variant, but with ankle in-stability can be an area of impinge-
and lens is a specialized skill that allows for intra-articular diagnosis and treatment as well as an adjunct to many ligament repair techniques. The most common arthroscope sizes are the 4.0 mm and 2.7 mm diameter lenses. There are pros and cons with both. The obvious issue is the size. Some surgeons like the 2.7 mm scope as the ankle is con-sidered a “small” joint, and it is felt to fit better and is easier to manipu-late within the joint. The down side is availability. Although becoming more com-mon, not all facilities carry the smaller scope sizes in-house. An-other issue is length. Some 2.7 mm scope lenses are short which may pose an issue during the procedure, limiting access to the extremes of the joint. If utilizing a 2.7 mm scope lens, one must be sure of its avail-ability as well as being sure it is a “long” version. As an aside, take caution with the 2.7 mm long ar-throscope lens in training situations as the lens is easier to bend or break during manipulation. In contrast, the larger 4.0 mm is the most common size in ortho-pedics and is readily available. It is also much sturdier for training and manipulation as well as providing a significantly larger field of view for only a small increase in diameter. The 4.0 mm system tends to also be slightly heavier compared with the smaller 2.7 mm version and, for some, more awkward to hold and learn to manipulate (Figure 4). If
available, utilizing both to see which works best for the surgeon would be valuable. Arthroscopy is typically per-formed as the initial portion of sur-gery for lateral ankle repair. All per-tinent superficial anatomy and inci-sions should be marked before the arthroscopy as there can be distor-
tion of the soft tissue with extrav-asation of fluid. The medial border of the tibialis anterior tendon, the lateral border of the long exten-sor tendons, the distal fibula, and the intermediate dorsal cutaneous nerve should be outlined (Figure 5). If possible, the surgeon should also try to limit the amount of time of the arthroscopic portion of the sur-gery as this can help limit the fluid distortion. The most common utilized por-tals for ankle arthroscopy are the an-teromedial and anterolateral portals. There are additional portals for select pathology but these two allow a ma-
www.podiatrym.com FEBRUARY 2020 | PODIATRY MANAGEMENT
131
continuing
Medical Education
AP radiograph of the ankle would be appropriate for the initial evaluation of an acute
ankle sprain injury.
Surgical PoDiatry
Lateral Ankle (from page 130)
Continued on page 132
Figure 6: intraoperative arthroscopic findings typical with ankle sprain pathology. Synovitis (a), adhesions (B), and a Bassett ligament (c).
a B
c

a curvilinear parallel to the distal border of the fibula and 2) a longi-tudinal over the distal 3cm of the fibula, bisecting the fibula, then ex-
tending distally over the sinus tarsi area. Both of these incisions allow access to the two most common injured ligaments (Figure 7). Deci-sions about the placement, many times, depends on other pathology and the need for access to the pero-neal tendons. The ATFL is the most common repaired lateral ankle ligament, with much literature to support its repair with generally good to excellent re-sults.13-15 Through the years, there have been many techniques de-
scribed to repair the AFTL. Most are open procedures, although arthroscopic-assisted and now completely arthroscopic tech-niques have been described.12,16
In either case, repair of the ATFL typically involves utilizing bone anchors along the anterior edge of the distal tip of the fib-ula corresponding to the ATFL attachment (Figure 8). The num-ber and size of bone anchors can vary depending on surgeon pref-erence but have allowed for eas-ier and improved strength versus
ment and is typically removed when encountered. Arthroscopy has become a vital part of lateral ankle sprain treat-ment. Having arthroscopic skills adds to the surgeon’s armamentar-ium. Shavers can be utilized to re-move excessive soft tissue, synovi-um, loose bodies, and cartilage. Ar-throscopic burrs help with removing prominent exostosis and spurs, as well as helping to clear soft tissue coverage to access subchondral bone for arthroscopic assisted ligament repair. Awls and drills can be placed to provide micro-fracture, and there are numerous soft tissue cutters and graspers to aid in repair. Bone can also be exposed along the anterior border of the distal fibula to aid in placement of anchors for ATFL re-pair. With continued advancements and innovations, more surgeons are successfully utilizing arthroscopy to place anchors in the lateral talus, with outcomes similar to those for open repair.12
For most surgeons, arthroscopy
is utilized as an adjunct, and ac-tual ligament repair is done as an open procedure. Traditionally, lat-eral ankle injuries and lateral ankle
stability have been treat-ed with open techniques. They can be divided into primary repair and sec-ondary repairs. Primary ligament repair essentially tightens or augments the normal ligament anatomy. Most often this is repair of the ATFL, and at times the CFL. The two most common incisions to access the lat-eral ankle ligaments are 1)
www.podiatrym.comFEBRUARY 2020 | PODIATRY MANAGEMENT
132
contin
uing
Medica
l Edu
cation
Surgical PoDiatry
Lateral Ankle (from page 131)
Continued on page 133
A semi-rigid ankle brace is an appropriate initial treatment for a lateral ankle injury.
Figure 7: Most common open lateral ankle ligament surgical approaches, curvilinear along distal edge of fibula (a), and longitudinal bisection of distal fibula (B).
a B
Figure 8: Examples of aTFl repair with non-absorbable suture (a), bone anchors in distal fibula with non-absorbable suture (B), and aTFl repair augmented with non-absorbable “brace” (c).
a
B c

Once the ATFL is repaired, anchors can be placed from the lateral talar neck to the dis-tal fibula superficial to the primar-ily repaired ATFL to lend support. For the CFL, an anchor is typically
placed in the origin at the distal fib-ula with the foot held in appropriate position; then the distal portion is attached to the lateral wall of the calcaneus deep to the peroneals to mimic the native ligament.
Post-Operative Recovery Post-operative recovery for pri-mary repair continues to evolve, with repairs becoming stronger. With the advent of bracing, non-weight-bear-ing is typically three weeks, with pro-gression from that point along with rehabilitation. For patients with failed prima-ry repair, larger BMI, or in patients with connective tissue disorders, secondary repair is a consideration. Secondary repair involves utilizing either autograft or allograft tendon to stabilize the lateral ankle com-plex. As with most surgery, there are many described techniques, dif-ferent tendons, and different drill-hole configurations, all with the goal of stabilizing the ankle when the
traditional bone tunnels from years past.15,17-18
Sutures are then utilized to re-pair the ligament directly, in an an-atomic fashion. During the repair, most surgeons remove a small por-tion of the injured or chronically dis-eased ATFL to have a “fresh edge” and to allow for some advancement to perhaps aid in increasing healing and stability. The extensor retinacu-lum may be included as well to add strength and provide more tissue for the repair. The CFL is frequently injured during these injuries and can be a large part of chronic instability, so in many cases, it is repaired sur-gically as well. At the very least,
the CFL should be tested with an inversion test to reveal competen-cy. If incompetent, repair again can be anatomic, although just slightly more difficult. One thing to remem-ber is that the CFL is deep to the peroneal tendons, so there is slight-ly more dissection required to ac-cess the anatomy. Once identified, the CFL is frequently loose and an-atomically different from the AFTL (Figure 9). The CFL is much more tendon-like in appearance and shape. Unlike the broad, thin ATFL, the CFL is thick and more cord-like but can be repaired di-
rectly in a similar fashion with just non-absorbable suture or bone anchors taking care to shorten and achieve a more stable ankle after repair. Recently, along with anatom-ic primary repair, augmentation
has become common and almost a mainstay in lateral ankle stabili-zation procedures. This technique comprises the more typical anatomic repair but at the same time applies a “brace” to augment the natural
structures.15,17-18 This technique en-tails additional bone anchors with non-absorbable suture or tape, used not to replace the anatomy, but to augment the repair. The native liga-ments and anatomy are still able to function and allow for propriocep-tion and support, but the “brace” is seen more as a preventative struc-ture in the event the lateral ankle sprain and inversion forces over-come the body’s own composition. For the “brace” technique, again there are several described tech-niques, and some depend on the de-ficiencies about the ankle ligaments.
www.podiatrym.com FEBRUARY 2020 | PODIATRY MANAGEMENT
133
continuing
Medical Education
The intermediate dorsal cutaneous nerve is the most common injured nerve
during ankle arthroscopy.
Surgical PoDiatry
Lateral Ankle (from page 132)
Continued on page 134
Figure 10: intraoperative example of a lateral ankle ligament secondary repair. Note the amount of dissection required, sacrifice of a portion of the peroneus brevis and fibula bone hole required.
After failed non-operative management of a lateral ankle injury, ankle joint synovectomy would
be best addressed with ankle arthroscopy.
a BFigure 9: intraoperative picture of attenuated cFl (a), and “brace” type repair (B).

la M, Visuri T, Mattile VM. Surgical ver-sus functional treatment for acute rup-tures of the lateral ligament complex of the ankle in young men: a randomized controlled trial. J Bone Joint Surg Am. 2010; 92(14):2367-2374. 4 Kannus P, Renstrom P. Treatment for acute tears of the lateral ligaments of the ankle. Operation, cast, or early con-trolled mobilization. J Bone Joint Surg Am. 1991; 73(2):305-312. 5 Rivera MJ, Winkelmann ZK, Powder CJ, Games KE. Proprioceptive training for the prevention of ankle sprains: an evi-dence-based review. J Athl Train. 2017; 52(11):1065-1067. 6 Holme E, Magnusson SP, Becher K, Bieler T, Aagaard P, Kjaer M. The effect of supervised rehabilitation on strength, postural sway, position sense and re-inju-ry risk after acute ankle ligament sprain. Scand J Med Sci Sports. 1999; 9(2):104-109. 7 Hupperets MD, Verhagen EA, van Mechelen W. Effect of unsupervised home based proprioceptive training on recur-rences of ankle sprain: randomized con-trolled trial. BMJ. 2009; 339:2684. 8 Feger MA, Herb CC, Faser JJ, Glavi-ano N, Hertel J. Supervised rehabilitation versus home exercise in the treatment of acute ankle sprains: a systematic review. Clin Sports Med. 2015; 34(2):329-346. 9 Cha SD, Kin HS, Chung ST, Yoo JH,
Park JH, Kim JH, Hyunh JW. Intra-artic-ular lesions in chronic lateral ankle in-stability: comparison of arthroscopy with magnetic resonance imaging findings. Clin Orthop Surg. 2012; 4(4):293-299. 10 Komenda GA, Ferkel RD. Ar-throscopic findings associated with the unstable ankle. Foot Ankle Int. 1999; 20(11):708-713. 11 Ferkel RD, Chams RN. Chronic lat-eral instability: arthroscopic findings and long-term results. Foot Ankle Int. 2007; 28(1):24-31. 12 Brown AJ, Shimozono Y, Hurley ET, Kennedy JG. Arthroscopic versus open repair of lateral ankle ligament for chronic lateral ankle instability: a me-ta-analysis. Knee Surg Sports Traumatol Arthrosc. (2018) https://doi.org/10.1007/s00167-018-5100-6 13 Pijnenburg AC, Van Dijk CN,
patient’s anatomy has failed or just cannot be corrected due to size or connective tissue compromise. When utilizing tendon in this man-
ner, it can be classified as anatomic or non-anatomic (Figure 10). Anatomic secondary repairs rep-resent a construct that, when com-plete, mimics the body’s original anatomy in the design, attachment, and function. Non-anatomic second-ary lateral ankle repair is a construct that when complete aids in ankle stability but may not allow “normal” function as the attachments and ori-entation do not follow native anat-omy. This can lead to altered me-chanics and possible long-term issues such as arthritis.19 Secondary repairs have a potential of making an ankle too stiff, and require a larger incision, larger surgery, lingering recovery, and the comorbidity of sacrificing native tendon function if autograft is utilized in the repair. With the ad-vent of improved primary repair tech-niques, there is less need for second-ary repairs.
Lateral Ankle Pathology Lateral ankle pathology is one of the most common issues facing foot and ankle surgeons. Lateral ankle sprains are typically treated non-surgically and generally do well with functional rehabilitation and without need for surgical interven-tion. Surgery is generally only con-sidered with continued pain, insta-bility, issues with proprioception, or other pathology such as tendon and cartilage injury. Understanding the appropriate exam and imaging modalities is a must. Once surgery is planned, ankle arthroscopy has been an indispensable adjunct, aid-ing in diagnosis and management of
intra-articular problems which are frequently associated. Techniques have evolved to allow the primary repair and even augmentation of the lateral ankle ligaments to be performed through
smaller incisions, or even ar-throscopically. With bone anchors and non-absorbable suture material, rehabilitation is earlier and more tolerated. These techniques have also limited the need for the more traditional secondary procedures as well. Although there are still some cases based on anatomy and history that require such procedures, trying to keep the repair anatomic may provide better outcomes and limit secondary osteoarthritis. As with any surgery, one must take into
consideration the entire pathology, which may consist of tendon issues or anatomic deformities that would need to be addressed as well. The lateral ankle is a complex series of interactions and structures that need to be respected to achieve the best results. PM
References 1 Waterman BR, Owens BD, Davey S, Zacchilli MA, Belmont PJ. The epidemiol-ogy of ankle sprains in the United States. J Bone Joint Surg. 2010; 92(13):2279-2284. 2 Bachmann LM, Kolb E, Koller MT, Steurer J, ter Riet G. Accuracy of the Otta-wa ankle rules to exclude fractures of the ankle and mid-foot: systematic review. BMJ. 2003; 326:417. 3 Pihlajamaki H, Hietaniemi K, Paavo-
www.podiatrym.comFEBRUARY 2020 | PODIATRY MANAGEMENT
134
contin
uing
Medica
l Edu
cation
Surgical PoDiatry
Lateral Ankle (from page 133)
A mini bone anchor with non-absorbable suture material is an acceptable
way to anchor the ATFL to the distal fibula during lateral ankle ligament repair.
Continued on page 135
Utilization of peroneus brevis for ligament reconstruction is an example of a secondary lateral
ankle ligament repair.
16. Guelfi M, Zamperetti M, Pantalone A, Usuelli FG, Salini V, Oliva XM. Open and arthroscopic lateral ligament repair for treatment of chronic ankle instability: a systematic review. Foot Ankle Surg. 2018; 24(1):11-18. 17 Hu CY, Lee KB, Song EK, Kim MS, Park KS. Comparison of bone tunnel and suture anchor techniques in the modified Bros-trom procedure for chronic lateral ankle instability. Am J Sports Med. 2013; 41(8):1877-1844. 18 Waldorp NE, Wijdicks CA, Jansson KS, LaPrade RF, Clan-ton TO. Anatomic suture anchor versus the Brostrom technique for anterior talofibular ligament repair: a biomechanical compari-son. Am J Sports Med. 2012; 40(11):2590-2596. 19 Noailles T, Lopes R, Padiolleau G, Gouin F, Brilhault J. Non-anatom-ical or direct anatomical repair of chronic lateral instability of the ankle: a systematic review of the literature after at least 10 years of follow-up. Foot Ankle Surg. 2018; 24(2):80-85.
Dr. Burns is an assistant Pro-fessor of Ortho-paedic Surgery at the university of Pittsburgh School of Medicine.
Bossuyt PM, Marti RK. Treatment of ruptures of the lateral ankle ligaments: a meta-analysis. J Bone Joint Surg Am. 2000; 82(6):761-773. 14 Hsu AR, Ardoin GT, Davis WH, Anderson RB. Intermediate and long-term outcomes of the modified Brostrom-Evans proce-dure for lateral ankle ligament reconstruction. Foot Ankle Spec. 2016; 9(2):131-139. 15 Coetzee JC, Ellington JK, Ronan JA, Stone RM. Functional results of open Brostrom ankle ligament repair augmented with a suture tape. Foot Ankle Int. 2018; 39(3):304-310.
Lateral Ankle (from page 134)
continuing
Medical Education
135
www.podiatrym.com FEBRUARY 2020 | PODIATRY MANAGEMENT
Surgical PoDiatry
1) Which of the following ligaments is part of the lateral ankle ligament complex? A) Anterior inferior tibiofibular ligament B) Calcaneal fibular ligament C) Posterior inferior tibiofibular ligament D) Anterior tibiotalar ligament
2) The calcaneal fibular ligament is tested during physical exam by which technique? A) Inversion stress B) Eversion stress C) External rotation D) Anterior drawer
3) Which is the most common ligament injured during a lateral ankle sprain? A) Deltoid B) Syndesmotic C) Bifurcate D) Anterior talofibular
4) Which foot type is commonly associated with lateral ankle instability? A) Pes planus B) Pes cavus C) Vertical talus D) Pronated
5) Which of the following imaging modalities would be appropriate for the initial evaluation of an acute ankle sprain injury? A) AP radiograph of the ankle B) CT scan of the ankle C) Ultrasound of the ankle D) MRI of the ankle
6) Appropriate initial treatment for a lateral ankle injury consists of which of the following? A) Ankle joint steroid injection B) Opioid pain management C) Application of heat to the ankle D) Semi-rigid ankle brace
cME EXaMination
See anSwer Sheet on page 137.
Continued on page 135
The lateral ankle is a complex series of interactions and
structures that need to be respected to achieve the best results.

FEBRUARY 2020 | PODIATRY MANAGEMENT
136
PM’scME Program
Welcome to the innovative continuing Education Program brought to you by Podiatry Management Magazine. Our journal has been approved as a sponsor of continuing Medical Education by the council on Podiatric Medical Education.
now it’s even easier and more convenient to enroll in PM’s cE program! You can now enroll at any time during the year and submit eligible exams at any time during your enrollment period. cME articles and examination questions from past issues of Podiatry Management can be found on the internet at http://www.podiatrym.com/cme. Each lesson is approved for 1.5 hours continuing education contact hours. Please read the testing, grading and payment instructions to decide which method of participa-tion is best for you. Please call (631) 563-1604 if you have any questions. a personal operator will be happy to assist you. Each of the 10 lessons will count as 1.5 credits; thus a maximum of 15 cME credits may be earned during any 12-month period. You may select any 10 in a 24-month period.
The Podiatry Management Magazine CME program is approved by the Council on Podi-atric Education in all states where credits in instructional media are accepted. This article is approved for 1.5 Continuing Education Contact Hours (or 0.15 CEU’s) for each examination successfully completed.
PM’s privacy policy can be found at http:// podiatrym.com/privacy.cfm.
This cME is valid for cPME-approved credits for three (3) years from the date of publication.
$
cME EXaMinationcon
tinuin
g
Medica
l Edu
cation
7) After failed non-operative management of a lateral ankle injury, which associated pathology would be best addressed with ankle arthroscopy? A) Ankle joint synovectomy B) Peroneal tendon debridement C) Deltoid ligament repair D) CFL repair
8) Which is the most common injured nerve during ankle arthroscopy? A) Sural nerve B) Medial dorsal cutaneous nerve C) Intermediate dorsal cutaneous nerve D) Saphenous nerve
9) Which of the following is an acceptable way to anchor the ATFL to the distal fibula during lateral ankle ligament repair? A) 4.0 cannulated screw B) Compression bone staple C) Absorbable suture material through
bone holes D) Mini bone anchor with non-absorbable
suture material
10) Which is an example of a secondary lateral ankle ligament repair? A) Open repair of anterior talofibular
ligament with bone anchors B) Arthroscopic repair of anterior talofibular
ligament C) Utilization of peroneus brevis for
ligament reconstruction D) Open repair of calcaneal fibular ligament
with bone anchors
See anSwer Sheet on page 137.
The author(s) certify that they have NO affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; member-ship, employment, consultancies, stock ownership, or other equity interest), or non-financial interest (such as personal or professional relationships, affiliations, knowledge, or beliefs) in the subject matter or materi-als discussed in this manuscript.

Please print clearly...Certificate will be issued from information below.
Name ____________________________________________________________________ Email address______________________________Please Print: FirST Mi laST
address_____________________________________________________________________________________________________________
city__________________________________________________ State_______________________ Zip________________________________
charge to: _____Visa _____ Mastercard _____ american Express
card #________________________________________________Exp. Date____________________ Zip for credit card_________________
note: credit card is the only method of payment. checks are no longer accepted.
Signature__________________________________ Email address_________________________ Daytime Phone_______________________
State license(s)___________________________ is this a new address? Yes________ No________
check one: ______ i am currently enrolled. (if faxing or phoning in your answer form please note that $2.95 will be charged to your credit card.)
______ i am not enrolled. Enclosed is my credit card information. Please charge my credit card $29.00 for each exam submitted. (plus $2.95 for each exam if submitting by fax or phone).
______ i am not enrolled and i wish to enroll for 10 courses at $249.00 (thus saving me $41 over the cost of 10 individual exam fees). i understand there will be an additional fee of $2.95 for any exam i wish to submit via fax or phone.
note: if you are mailing your answer sheet, you must complete all info. on the front and back of this page and mail with your credit card information to: Program Management services, P.o. Box 490, East islip, ny 11730.
tEsting, graDing anD PayMEnt instructions (1) Each participant achieving a passing grade of 70% or higher on any examination will receive an official computer form stating the number of cE credits earned. This form should be safeguarded and may be used as documentation of credits earned. (2) Participants receiving a failing grade on any exam will be notified and permitted to take one re-examination at no extra cost. (3) all answers should be recorded on the answer form below. For each question, decide which choice is the best answer, and cir-cle the letter representing your choice. (4) complete all other information on the front and back of this page. (5) choose one out of the 3 options for testgrading: mail-in, fax, or phone. To select the type of service that best suits your needs, please read the following section, “Test grading Options”.
tEst graDing oPtions Mail-In Grading To receive your cME certificate, complete all information and mail with your credit card information to: Program Management services, P.o. Box 490, East islip, ny 11730. PLEasE Do not sEnD WitH signaturE rEQuirED, as tHEsE WiLL not BE accEPtED.
EnroLLMEnt ForM & ansWEr sHEEt
$
There is no charge for the mail-in service if you have al-ready enrolled in the annual exam cME program, and we receive this exam during your current enrollment period. if you are not en-rolled, please send $29.00 per exam, or $249 to cover all 10 exams (thus saving $41 over the cost of 10 individual exam fees).
Facsimile Grading To receive your cME certificate, complete all information and fax 24 hours a day to 1631-532-1964. Your cME certificate will be dated and mailed within 48 hours. This service is available for $2.95 per exam if you are currently enrolled in the annual 10-exam cME program (and this exam falls within your enrollment period), and can be charged to your Visa, Mastercard, or american Express. if you are not enrolled in the annual 10-exam cME program, the fee is $29 per exam.
Phone-In Grading You may also complete your exam by using the toll-free service. call 1-800-232-4422 from 10 a.m. to 5 p.m. EST, Monday through Friday. Your cME certificate will be dated the same day you call and mailed within 48 hours. There is a $2.95 charge for this service if you are currently enrolled in the annual 10-exam cME program (and this exam falls within your enrollment period), and this fee can be charged to your Visa, Mastercard, american Express, or Discover. if you are not current-ly enrolled, the fee is $29 per exam. When you call, please have ready: 1. Program number (Month and Year) 2. The answers to the test 3. credit card information
Over, please
continuing
Medical Education
Enrollment/testing informationand answer sheet
137
www.podiatrym.com FEBRUARY 2020 | PODIATRY MANAGEMENT
in the event you require additional cME information, please contact PMS, inc., at 1-631-563-1604.
138
www.podiatrym.comFEBRUARY 2020 | PODIATRY MANAGEMENT
contin
uing
Medica
l Edu
cation
EnroLLMEnt ForM & ansWEr sHEEt (continued)
$
Medical Education Lesson Evaluation Strongly Strongly agree agree Neutral Disagree disagree [5] [4] [3] [2] [1]
1) This cME lesson was helpful to my practice ____
2) The educational objectives were accomplished ____
3) i will apply the knowledge i learned from this lesson ____
4) i will makes changes in my practice behavior based on this lesson ____
5) This lesson presented quality information with adequate current references ____
6) What overall grade would you assign this lesson? a B c D
7) This activity was balanced and free of commercial bias.
Yes _____ No _____
8) What overall grade would you assign to the overall management of this activity? a B c D
How long did it take you to complete this lesson?
______hour ______minutes
What topics would you like to see in future cME lessons ? Please list :__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
1. a B c D
2. a B c D
3. a B c D
4. a B c D
5. a B c D
6. a B c D
7. a B c D
8. a B c D
9. a B c D
10. a B c D
circle:
EXaM #2/20Lateral ankle injuries: scope and stabilization
(Burns)





























