Embed Size (px)
Citation preview

MEDICAL CONNECTIONS | CONEXIUNI MEDICALEEDITOR IN CHIEF
Koren RumeliaASSISTANT EDITOR IN CHIEF
Bumbuluţ Călin
ASSISTANT EDITORSBlaga VasileAndó Ottó
Oană Cristian SeverEDITORIAL BOARD
Bauer Adalbert (SCM Satu Mare, România)Bidilean Nicolae (Emergency County Hospital,
Satu Mare, România)Boros Melinda (Bucureşti, România)
Borcean Gheorghe (Caransebeş Hospital, România)Brândeu Ioan (Emergency County Hospital,
Satu Mare, România)Cârstea Constantin (CMI Braşov, România)
Cojocaru Manole (Titu Maiorescu University, Bucureşti, România)
Comăneanu Raluca Monica (Titu Maiorescu University, Bucureşti, România)
Cornean-Santa Corina (Emergency County Hospital, Satu Mare, România)
Feciche Bogdan (Emergency County Hospital, Satu Mare, România)
Grosz Gyula (SCM West Satu Mare, România)Gruzman Carlos (Hasharon Hospital,
Tel Aviv, Israel)Horber Orsolya (SCM Praxis Bixad, România)
Lup Liliana (Synevo Satu Mare, România)Kesler Gavriel (Israel)
Kiss Ladislau (Emergency County Hospital, Satu Mare, România)
Mihalca Man Sorina (Emergency County Hospital, Satu Mare, România)
Neumann Gad (Hasharon Hospital, Tel Aviv, Israel)Negru Alina (Centro de Salud Caspe, Zaragoza, Spain)Rath-Wolfson Lea (Hasharon Hospital, Tel Aviv, Israel)
Rădulescu Viorel (CMI Olt, România)Roatiş Marius Dinu (Emergency County Hospital,
Satu Mare, România)Rusu Cristian Bogdan (Emergency County Hospital,
Satu Mare, România)Shvero Kesler Dana (Hadassa University, Jerusalem, Israel)
Trip Gheorghe (Emergency County Hospital, Satu Mare, România)
Zilahi Karoly (SCM Praxis, Bixad, România)Zeidman Aliza (Hasharon Hospital, Tel Aviv, Israel)
Virag Tiberiu (CMI Satu Mare, România)
EDITORCollege of Physicians Satu Mare
Satu Mare, 23 Eroilor Revoluţiei Pl.www.colmedsm.ro,
email: [email protected]
ASSOCIATED EDITORSatu Mare Association of Family Physicians
Affiliated with National Society ofFamily Medicine/General Medicine
Satu Mare, UK 30 Bobocului St.www.amfsm.ro, email: [email protected]
PARTNERSHIPTitu Maiorescu University, Bucharest
Faculty of Medicine and Dental Medicine67A Gheorghe Petraşcu St.
www.utm.ro, email: [email protected]
EXTERNAL PARTNERSHIP Hasharon Hospital, Rabin Medical Center
Affiliated with Sackler School of Medicine, Tel Aviv University, 7 Keren Kayemet St., Petah Tikva 49372, Israel
www.clalit.org.il
EDITORIAL OFFICE 23 Eroilor Revoluţiei Pl., 440055, Satu Mare, Romania, Tel/Fax: 0040261-710456, 0040361-408164
http://www.conexiunimedicale.ro/ISSN online 2068 – 8369
ISSN 1843 – 9306
Journal included in The Schedule of Medical Publications of CMR, 5 credits CMR for subscribersIndexed in Index Copernicus®, CNCSIS B+ Category, Code 944
Medical Connections/Conexiuni Medicale® is a trademark of College of Physicians Satu Mare and Satu Mare Association of Family PhysiciansPrinted at TIPOOFFSET, Fabricii str, No. 93-103, Cluj Napoca, Tel./Fax: 0040264-456071

The Medical Connections/Conexiuni Medicale® is indexed in Journals Master List of Index Copernicus®
B+ Category, Code 944
© Copyright Medical Connections/Conexiuni Medicale, Satu Mare, 2012
No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means without prior permission in writing of Medical Connections/Conexiuni Medicale®. Permission is not
however required to copy abstracts of papers or of articles on condition that a full reference to the source is shown. Correspondence regarding permission to reprint all or part of any article published in this journal
should be addressed to the Editor, e-mail: [email protected]
SCIENTIFIC AND PEER REVIEW BOARD | COLECTIV ŞTIINŢIFIC ŞI DE RECENZIE
Acad. Prof. Univ. as. Dr. Virgil Enătescu(Emergency County Hospital, Satu Mare, Romania)
Acad. Prof. Univ. Dr. Doina Onicescu(Titu Maiorescu University, Faculty of Medicine and Dental Medicine, Bucharest, Romania)
Acad. Senior Scientific Researcher Dr. Sorin Riga(Prof. Dr. Al. Obregia Clinic Hospital of Psychiatry, Bucharest, Romania)
Acad. Senior Scientific Researcher Dr. Dan Riga(Prof. Dr. Al. Obregia Clinic Hospital of Psychiatry, Bucharest, Romania)
Prof. Univ. Dr. Vasile Astărăstoae(Gr. T. Popa University of Medicine and Pharmacy, Iaşi, Romania)
Prof. Univ. Dr. Rumelia Koren(Hasharon Hospital, Rabin Medical Center, Sackler School of Medicine, Tel Aviv University, Israel)
Prof. Univ. Dr. Petru Armeanu(Titu Maiorescu University, Faculty of Medicine and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Ilie Constantin(Victor Babeş University, Faculty of Medicine, Timişoara, Romania)
Prof. Univ. Dr. Gheorghe Ionel Comşa(Ovidius University, Constanţa, Romania)
Prof. Univ. Dr. Constantin Dumitru(Titu Maiorescu University, Faculty of Medicine and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Rivka Gal(Hasharon Hospital, Rabin Medical Center, Sackler School of Medicine, Tel Aviv University, Israel)
Prof. Univ. Dr. Doina Lucia Ghergic(Titu Maiorescu University, Faculty of Medicine and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Tuvia Hadar(Beilinson Hospital, Rabin Medical Center, Sackler Faculty of Medicine, Tel Aviv University, Israel)
Prof. Univ. Dr. Gheorghe Manole(Titu Maiorescu University, Faculty of Medicine and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Dorel Augustin Manu(Titu Maiorescu University, Faculty of Medicine and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Dan Mănăstireanu(Titu Maiorescu University, Faculty of Medicine and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Elena Moldoveanu(Titu Maiorescu University, Faculty of Medicine and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Adriana Stănilă(Victor Papilian Faculty of Medicine, Sibiu, Romania)
Prof. Univ. Dr. Maria Lidia Nica Udangiu(Titu Maiorescu University, Faculty of Medicine and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Dan Florin Ungureanu(Titu Maiorescu University, Faculty of Medicine and Dental Medicine, Bucharest, Romania)
Conf. Univ. Dr. Ghinescu Minerva(Titu Maiorescu University, Bucureşti, România)
Conf. Univ. Dr. Mircea Sorin Sabău(University of Medicine and Pharmacy Târgu Mureş, Romania)
Ş. L. Dr. Anca Ciurea(Iuliu Haţieganu University, Faculty of Medicine, Cluj Napoca, Romania)
As. Univ. Dr. Virgil Radu Enătescu(Eduard Pamfil Universitary Clinic of Psychiatry, Timişoara, Romania)

MEDICAL CONNECTIONS | CONEXIUNI MEDICALEEDITOR ŞEFKoren Rumelia
EDITOR ŞEF ADJUNCTBumbuluţ Călin
EDITORI ADJUNCŢIBlaga VasileAndó Ottó
Oană Cristian SeverCOMITET EDITORIAL
Bauer Adalbert (SCM West Satu Mare, România)Bidilean Nicolae (Spital Judeţean de Urgenţă,
Satu Mare, România)Boros Melinda (Bucureşti, România)
Borcean Gheorghe (Spital Municipal Caransebeş, România)Brândeu Ioan (Spital Judeţean de Urgenţă,
Satu Mare, România)Cârstea Constantin (CMI Braşov, România)
Cojocaru Manole (Universitatea Titu Maiorescu, Bucureşti, România)
Comăneanu Raluca Monica (Universitatea Titu Maiorescu, Bucureşti, România)
Cornean-Santa Corina (Spital Judeţean de Urgenţă, Satu Mare, România)
Feciche Bogdan (Spital Judeţean de Urgenţă, Satu Mare, România)
Grosz Gyula (SCM West Satu Mare, România)Gruzman Carlos (Hasharon Hospital, Tel Aviv, Israel)
Horber Orsolya (SCM Praxis Bixad, România)Lup Liliana (Synevo Satu Mare, România)
Kesler Gavriel (Israel)Kiss Ladislau (Spital Judeţean de Urgenţă,
Satu Mare, România)Mihalca Man Sorina (Spital Judeţean de Urgenţă,
Satu Mare, România)Neumann Gad (Spital Hasharon, Tel Aviv, Israel)
Negru Alina (Centro de Salud Caspe, Zaragoza, Spain)Rath-Wolfson Lea (Spital Hasharon, Tel Aviv, Israel)
Rădulescu Viorel (CMI Olt, România)Roatiş Marius Dinu (Spital Judeţean de Urgenţă,
Satu Mare, România)Rusu Cristian Bogdan (Spital Judeţean de Urgenţă,
Satu Mare, România)Shvero Kesler Dana (Universitatea Hadassa,
Ierusalim, Israel)Trip Gheorghe (Spital Judeţean de Urgenţă,
Satu Mare, România)Zilahi Karoly (SCM Praxis, Bixad, România)
Zeidman Aliza (Spital Hasharon, Tel Aviv, Israel)Virag Tiberiu (CMI Satu Mare, România)
EDITORColegiul Medicilor Satu Mare
Satu Mare, P-ţa Eroilor Revoluţiei nr.23www.colmedsm.ro,
email: [email protected]
EDITOR ASOCIATAsociaţia Medicilor de Familie Satu Mare
Afiliată la Societatea Naţională de Medicina Familiei/Medicină Generală
Satu Mare, str. Bobocului UK 30www.amfsm.ro, email: [email protected]
PPARTENERUniversitatea Titu Maiorescu Bucureşti
Facultatea de Medicină şi Medicină Dentarăstr. Gheorghe Petraşcu 67A
www.utm.ro, email: [email protected]
PARTENER EXTERNHasharon Hospital, Rabin Medical Center
Afiliat la Sackler School of Medicine, Universitatea Tel Aviv7 Keren Kayemet St., Petah Tikva 49372, Israel
www.clalit.org.il
REDACŢIA P-ţa Eroilor Revoluţiei nr 23, 440055, Satu Mare, Romania, Tel/Fax: 0261-710456, 0361-408164
http://www.conexiunimedicale.ro/ISSN online 2068 – 8369
ISSN 1843 – 9306
Revistă inclusă în Nomenclatorul Publicaţiilor Medicale ale CMR, 5 credite CMR pentru abonaţiIndexare în Index Copernicus®, CNCSIS categoria B+, cod 944
Medical Connections/Conexiuni Medicale® este marcă înregistrată a Colegiului Medicilor Satu Mare şi a Asociaţiei Medicilor de Familie Satu MareTipărit la TIPOOFFSET, str. Fabricii, Nr. 93-103, Cluj Napoca, Tel./Fax: 0264-456071

Contents
Editorial ......................................................................................................................................................... 6
original articlEs
Over Expression of Metalloproteinase 1 in Human Colonic Carcinomas and Prognostic ValueRath-Wolfson Lea, Bubis Roy, Shvero Asaf, Ghinescu Minerva, Ram Edward ............................................... 7
Renal Function Monitoring in Urogenital Robot-Assisted Laparoscopic Surgery Performed in General AnaesthesiaMihály Orsolya, Bolboacă Sorana Daniela, Răhăian Rodica, Chira Cipriana, Mihály Zoltan Attila, Coman Ioan ........................................................................................................................................... 13
The Prognostic Value of Serum Amyloid A Levels in Patients with Rheumatoid ArthritisCojocaru Manole, Ghinescu Minerva Claudia, Bălăeţ Constantin, Cojocaru Inimioara Mihaela, Siloşi Isabela ........................................................................................................................................... 19
Parent’s Attitude Toward the Sex Education that Their Children Learn at SchoolJoubran Samia, Marcus Ohad, Iancu Iulian, Hartman Tova, Abraham Weizman, Rath-Wolfson Lea, Ram Edward .......................................................................................................................................... 23
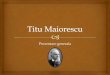
The Ankle-Brachial Index in the Diagnosis of Symptomatic and Asymptomatic Peripheral Arterial DiseaseAdrian Gruici, Elena Ardeleanu, Anca Alexandra Matusz, Rodica Mihăescu, Roxana Alăman, Daniela Gurgus ...................................................................................................................................... 31
Lead Exposure Hematological and Cardiovascular SideRuja Elena, Cocârlă Aristotel ................................................................................................................... 39
Preliminary Study about the Complications Which Can Appear in Restoring an Edentulous Space with Fixed ProsthesisHancu Violeta, Comăneanu Raluca Monica, Barbu Horia Mihail, Rădulescu Diana Eugenia, Filipescu Alina Gabriela, Ghergic Doina Lucia ......................................................................................... 43
May Influence the Epidural Anesthesia the Newborn Hearing Screening?Domuţa Maria, Pascalau Nicoleta, Cotulbea Stan .................................................................................... 49
gEnEral rEviEw
New Therapeutic and Etiologic Perspectives in Recurrent MiscarriageGrigore Mihaela, Mareş Alina ................................................................................................................. 53
casE PrEsEntation
Diagnosis of Digital Nodule by Fine Needle Aspiration Cytology Halpern Marisa, Vigler Mordechai, Rath-Wolfson Lea Schwartz Ariel, Koren Rumelia, Gal Rivka .............. 59
Nephrogenic Adenoma, Report of Two Cases and Review of the LiteratureRath-Wolfson Lea, Schwartz Ariel, Leikin Anna, Koren Rumelia, Gal Rivka .............................................. 63
Substitution of the Ureter with the Appendix in Malignant Melanoma Adjacent to the UreterGoldberg Hanan, Yossepowitch Ofer, Baniel Jack ...................................................................................... 69
A Case of West Nile Meningitis Treated with TamifluSolun Boris, Marcoviciu Dana, Dicker Dror, Shaked Efrat ........................................................................ 73
MEdicinE and art
Imagine all the Pictures Living Other LivesGabrieli Selma, Benzaquen Oshra ........................................................................................................... 77
guidancE for authors ............................................................................................................................... 79

Cuprins
Editorial ....................................................................................................................................................... 83
articolE originalE
Supraexpresia Metaloproteinazei-1 în carcinoamele colonului şi valoarea ei prognosticăRath-Wolfson Lea, Bubis Roy, Shvero Asaf, Ghinescu Minerva, Ram Edward ............................................. 85
Monitorizarea funcţiei renale în intervenţiile laparoscopice uro-genitale asistate robotic, efectuate în anestezie generalăMihály Orsolya, Bolboacă Sorana Daniela, Răhăian Rodica, Chira Cipriana, Mihály Zoltan Attila, Coman Ioan ........................................................................................................................................... 91
Valoarea prognostică a nivelurilor serice de amiloid A la pacienţii cu poliartrită reumatoidăCojocaru Manole, Ghinescu Minerva Claudia, Bălăeţ Constantin, Cojocaru Inimioara Mihaela, Siloşi Isabela ........................................................................................................................................... 97
Atitudinea părinţilor faţă de educaţia sexuală pe care copii lor o primesc de la şcoalăJoubran Samia, Marcus Ohad, Iancu Iulian, Hartman Tova, Abraham Weizman, Rath-Wolfson Lea, Ram Edward ........................................................................................................................................ 101
Importanţa indicelui gleznă-braţ în diagnosticul bolii arteriale periferice simptomatice şi asimptomaticeAdrian Gruici, Elena Ardeleanu, Anca Alexandra Matusz, Rodica Mihăescu, Roxana Alăman, Daniela Gurgus .................................................................................................................................... 109
Expunerea la plumb – efecte secundare hematologice şi vasculareRuja Elena, Cocârlă Aristotel ................................................................................................................. 117
Studiu preliminar asupra complicaţiilor apărute în protezarea fixă a breşelor edentate reduseHancu Violeta, Comăneanu Raluca Monica, Barbu Horia Mihail, Rădulescu Diana Eugenia, Filipescu Alina Gabriela, Ghergic Doina Lucia ....................................................................................... 121
Poate influenţa anestezia epidurală screeningul auditiv al nou-născuţilor?Domuţa Maria, Pascalau Nicoleta, Cotulbea Stan .................................................................................. 127
rEvistă gEnErală
Noi perspective etiologice şi terapeutice asupra bolii abortiveGrigore Mihaela, Mareş Alina ............................................................................................................... 131
PrEzEntarE dE caz
Diagnosticul unui nodul digital prin citologia aspirativă cu ac finHalpern Marisa, Vigler Mordechai, Rath-Wolfson Lea Schwartz Ariel, Koren Rumelia, Gal Rivka ............ 137
Adenomul nefrogenic, prezentare a două cazuri şi o revistă a literaturiiRath-Wolfson Lea, Schwartz Ariel, Leikin Anna, Koren Rumelia, Gal Rivka ............................................ 141
Înlocuirea ureterului cu apendicele în melanomul malign adiacent ureteruluiGoldberg Hanan, Yossepowitch Ofer, Baniel Jack .................................................................................... 145
Un caz de meningită West-Nile tratat cu TamifluSolun Boris, Marcoviciu Dana, Dicker Dror, Shaked Efrat ...................................................................... 149
MEdicină şi artă
Imaginează-ţi toate imaginile prinzând altă viaţăGabrieli Selma, Benzaquen Oshra ......................................................................................................... 153
standardE dE rEdactarE .......................................................................................................................... 154

6
EDITORIAL
After having conquered England in 1066, William the Bastard (only chronicles known as William the Conqueror) made two important things in this order: 1) He built the Tower of London and 2) He ordered the first complete census in history. The order of these actions is extremely important because the Tower was proved to be savior during the census, when the Anglo-Saxons wanted to know more closely the one who disturbed their quiet life and counted their households. Although the King did not graduate London School of Economics, he had the school of life so he had sent two sets of inspectors, some who were census and the others whose task was to control the reviewers. Although the resulting statistic bound in nice leather was more accurate than the Numbers of the Old Testament, in Anglo-Saxon Chronicles is known as the Doomsday Book. That’s because the King then stood and judged the taxes of his subordinates from this database. It is said by malicious chroniclers, that in the last years of his life, when suffering from insomnia, the King used to read from this book. It was certainly a missed act, as Freud would say, as the King was preparing himself to be included in the Last Inquest.
Collecting statistical data is the prior condition for any rational decision on the economy, finance, medicine and society in general. Correct statistical databases are the certainty on which any reasonable estimate of the future is based. Although in essence, the future is unpredictable, using statistics we can partialy control uncertainty and the anxiety it generates. The accumulation of data makes that independent observers, with an open mind, converge to the truth. When they have little data, scientists and statisticians disagree and become subjective; when they have piles of data they agree and are more objective. We continue to illustrate this with an example from medicine.
Since 1937 a small German study noticed a correlation between smoking and lung cancer. But who should take these data seriously when Edward Bernays, Freud’s nephew (from sister), newly hired at American Tobacco, just convinced women to smoke in order to prove their independence and emancipation? The medical world agreed that industrial and car pollution have exclusive guilt. Austin Bradford Hill together with
Richard Doll wanted to check what the main cause of lung cancer was. They interviewed patients with and without lung cancer from 20 hospitals in London. The results, published in 1950, were shockingly clear. Out of 649 men with lung cancer, only 2 did not smoke, and the majority of smokers smoked more than one pack per day. Although it enjoyed excessive media attention, the study did not convince the medical community that accused it as minor, retrospective, not really saying anything about the cause and about the risk for smokers to get lung cancer. For solving this problem, the two have decided to do a prospective study on a considerably higher number of patients. They have interviewed 40,000 British doctors regarding smoking habit and tracked them for five years. The result were clear, smokers had a 24 times higher probability to get lung cancer from smoking, comparing to the non smokers. This time the doctors were convinced, but the statisticians, who found that association between smoking and cancer does not mean causality, opposed. There have been developed all sorts of theories as that a genetic factor induces both your desire to smoke and the lung cancer. At this point of the discussion the intervention of experimental medicine was decisive: “there is no evidence that bronchogenic carcinoma diagnosed after the age of 50 years started at 18 years, average age when people start smoking, and therefore we refuse to talk further on this issue”. Presumed genetic factor should have spread rapidly, especially among smokers, to produce skin cancer in mice but not in humans’ lungs, to decrease with age in those who have quit smoking, be more likely at men than in women, and 60 times more prevalent in those who smoke over 2 packs a day. Too much for a genetic factor, but perfectly feasible for an environmental factor. The main result of this research was that the tobacco industry introduced filter into cigarettes. Most filters contained asbestos! It took other more years of research and controversy till asbestos became a clear role in carcinogenesis. Two generations of smokers had to die until smoking was banned in public places in Europe and America. This was the price paid for the neglect or misuse of statistics.
Sever Cristian Oană, MD
About people And stAtisticAl dAtA

Over Expression Of Metalloproteinase-1 In Human Colonic Carcinomas And Its Prognostic Value 7
Abstract
Colorectal cancer (CRC) represents a serious health problem and the search for additional prognostic factors is on going. In this study we wanted to examine the expression of Matrix Metalloproteinase 1 (MMP-1) by immunohistochemical method in colorectal cancer and its relation to clinicopathological features.
Sixty eight consecutive patients with CRC were treated at our center were chosen to participate. Representative samples from each tumor were stained immunohistochemically for MMP-1. Its intensity expression was graded as positive or negative. Normal colon tissue samples were used for control. In general the survival curve of the positive MMP-1 patients was worse than that of the negative ones, but the difference was not statistically significant (p=0.125). However, survival time was significantly shorter for patients with positive MMP-1 who did not receive chemotherapy treatment than the negative ones, (p=0.019). When considering the gender of the patient, survival time
showed a statistically significant difference between male patients with positive and negative MMP-1 indication (p=0.04), but the difference for female patients was not statistically significant.
It seems that patients with positive MMP-1 would benefit from chemotherapy treatment even if their disease is at a low stage, therefore the immunohistochemical staining for MMP-1 could be relevant in deciding on adjuvant treatment for the individual patient.
Key words: MMP-1, colorectal carcinoma
Introduction
Colon cancer represents a serious health and epidemiologic problem in the developed countries and with the rise in the standard of living its incidence is increasing in the non developed countries. The etiology is thought to co-involve genetic factors as well as environmental-nutritional ones [1].
The prognosis and the treatment are based on the tumor stage and the histological grade. Tumor stage is
ORIgInAL ARTIcLEs
oVeR eXpRession oF MetAllopRoteinAse-1 in HuMAn colonic cARcinoMAs And its pRoGnostic VAlue
Rath-Wolfson Lea1, Bubis Roy2, Shvero Asaf3, Ghinescu Minerva4, Ram Edward5
Department of 1Pathology Hasharon Hospital, Rabin Medical Center, Petah-Tikva, 2Raymond and Beverly School of physics and Astronomy, Tel-Aviv University, 3Sapir Medical Center, Meir Hospital, Kfar Sava, 4Faculty of Medicine, Titu Maiorescu University, Bucharest, Romania, 5Department of Surgery, Hasharon Hospital, Rabin Medical Center, Petah-Tikva, affiliated to Tel-Aviv University, Tel-Aviv, Israel
Address for correspondence:Asaf Shvero, MD Sapir Medical Center, Meir Hospital, Kfar Sava E-mail: [email protected] Received: 09.02.2012 Accepted: 10.07.2012 Med Con October 2012, Vol 7, No 3, 7-12 Running title: MMP-1 in colon cancer The work was communicated at the 2nd International Conference on Pathology (Pathology ’11), September 26-28, 2011, Prague, Czech Republic.

ORIgInAL ARTIcLEs
Rath-Wolfson et al8
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
based on the modified Duke’s system: the depth of infiltration into the intestinal wall, presence/absence of metastases in the regional lymph nodes and presence/absence of metastases in distant organs, like the liver [2]. In stage A, which is penetration of the carcinoma to the sub-mucosa but not further, the five year survival is 90 %. There is a decrease to 50-60 % at stage B when there is penetration into the muscularis propria. The five year survival decreases to 20-25 % in Dukes C when there are metastases to the regional lymph nodes.
The surgical removal of the tumor is a definitive treatment, but, according to the stage there might be recurrence or metastatic spread and therefore adjuvant chemotherapy is added [2].
Lately, the search for additional prognostic factors which could pinpoint those patients who are at greater risk for recurrence or metastases is increasing. There are studies conducted on the proliferating factors, chromosomal abnormalities, oncogene expression, DNA-ploidity etc [2,3].
In colon cancer the most important prognostic factor is the stage, but it is known that the youngest and oldest patient have poorer prognosis as well as obstruction and perforation [4]. Carcinomas of the left colon are more prone to recur [5]. Mucinous antigens like Sialosyl and Sialyl Lewis antigen are known to be worse prognostic factor [6] while patients with strong HLA-DR positive expression had better prognosis [7]. Patients with inflammatory infiltrate of eosinophyls, dendritic cells and lymphocytes had also better survival [8], while vascular and perineural invasion are bad prognostic factors [9]. Allelic loss of chromosome 18Q was shown to be a very bad prognostic factor [10]. DCC was found to be a prognostic factor for colorectal cancer. Positive expression of DCC identifies a subgroup of patients who respond favorably to adjuvant chemotherapy [11,12].
K-Ras, over-expression of p-53, Ras P21 and C-MYC are also well known as prognostic factors [2].
The newer studies concentrate upon the search for enzymes with destructive properties and quantification of its activity in tumors as a prognostic factor.
The destruction of the basement membrane is essential for the progression of the tumor. Different enzymes of the MMP group are suspected to be involved in the penetration of colon cancer into adjacent tissues by digestion of the collagen type IV, which is a major component of the basement membrane [13]. The mechanism of this action is thought to be through activation of the Pro-Gelatinase A.
Matrix metalloproteinases (MMPs) are a family of extracellular endopeptidases with enzymatic activity against protein components of the extracellular matrix.
They are associated with various diseases, such as skeletal dysplasias, coronary artery and heart disease, arthritis and brain disorders. The active form of MMPs exerts a broad proteolytic effect against a wide range of substrates, including proteoglycans, fibronectin, insoluble elastin, type IV and V collagen constituents of basement membrane, and some interstitial tissues [13].
MMPs are known to be involved in early carcinogenesis, tumor growth and, most importantly, tumor invasion and metastasis [14].
The link between MMPs and tumor progression has been examined in breast cancer, head and neck squamous cell carcinoma, and malignant melanoma
[15-17].The aim of this retrospective study on 68 colon
cancer patients was to find out whether the expression of the MMP-1 in the tumor was a prognostic factor dependent/independent on the Duke’s staging and treatment.
Materials and methods
Patients The study included 68 consecutive patients who
were diagnosed and treated for colon cancer at our Hospital. All the patients underwent the same diagnostic and therapeutic protocol. All patients underwent colectomy with or without adjuvant chemotherapy.
This study’s design was approved by our institutional committee
Tumor specimensResected specimens were fixed with 4 % buffered
formalin. Representative sections were embedded in paraffin and stained in Hematoxylin and Eosin (H&E).
ImmunohistochemistryAll the slides available were evaluated by two
pathologists. Representative paraffin blocks of the tumors were
selected for immunohistochemical analysis. Sections cut 4- μm-thick were placed on Super-Frost Plus slides (Sigma, Germany), dried overnight at 37°C and deparaffinized with 2 changes of xylene for 3 minutes each. The preparatory process consisted of the following steps, in succession: the sections were hydrated gradually through graded alcohol, in 100 % ethanol twice for 5 minutes and in 95 % ethanol for 5 minutes; rinsed in distilled water for 1 minute and blocked for endogenous peroxide activity in 3% hydrogen peroxide solution for 10 minutes at room temperature; rinsed in two changes of distilled water and placed in a pressure cooker with pre-boiled citrate buffer at pH 6.0 for antigen retrieval; immediately washed in distilled water and incubated with rabbit polyclonal

ORIgInAL ARTIcLEs
Over Expression Of Metalloproteinase-1 In Human Colonic Carcinomas And Its Prognostic Value 9
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
antibodies for MMP-1. Thereafter, the sections were rinsed again with washing buffer and incubated with Polymer HRP-conjugated broad-spectrum secondary antibody (Polymer Detection Kit, Zymed, California, USA) for 15 minutes at room temperature; rinsed again with washing buffer; and stained with diaminobenzidine solution for 10 minutes at room temperature. Finally, sections were counterstained with Mayer’s hematoxylin for 5 minutes and dehydrated through 95 % ethanol for 1 minute and 100 % ethanol for 2 minutes, cleared with xylene for 2 minutes, and cover slipped with mounting medium.
Immunohistochemical evaluationNormal colonic mucosa served as a positive control
Fig. 1.For negative Control the primary antibody was
omitted in normal colonic mucosa.The slides were evaluated by 2 experienced
pathologists who graded the intensity as positive when the cytoplasm of more than 50 % of the tumor cells was stained and negative when it was less than 50 %.
Statistical Analysis:Mean survival and disease-free survival times were
estimated using Kaplan-Meier analysis to account for censored cases.
The cases were divided into groups according to chemotherapy treatment or according to gender, and the difference in survival curves between patients with positive MMP-1 staining and patients with negative indication was evaluated by means of the log-rank test. Statistical significance was chosen at p<0.05.
Results
The study group consisted of 43 males and 25 females. Table I summarizes the clinicopathological data of the patients. Their age ranged from 42 to 81 years (mean 68.79).
In the male group 16 stained positively for MMP-1 (Fig. 2) and 27 were negative (Fig. 3). In the female group 7 were positive and 18 negative.
Twenty of these cancers were located in the rectum while the others had more proximal locations. Eighteen tumors were graded as well differentiated and 50 were moderately differentiated. 36 patients were stage B while 32 were stage C, with regional lymph node metastases. Adjuvant chemotherapy was administered to 45 patients while 23 did not get any other treatment.
Nine of the 20 rectal cancers were positive for MMP-1 and 11 negative. From the other colonic sites, 48 cases, 14 were positive while 34 were negative.
In the well differentiated tumor group, there were 6 cases positively stained for MMP-1 and 12 negative. In
the moderately differentiated group there were 17 positive cases and 38 negative with no statistically significant difference. In stage B of the disease, 12 had positive MMP-1 stain and 24 were negative. In stage C,
Figure 1. Normal colonic mucosa stained for MMP-1. The brown positive stain is seen in the cytoplasm (x200) [Mucoasă normală de colon colorată pentru MMP-1. Se observă colorare pozitivă maro în citoplasmă (x200)]
Figure 2. Colon cancer with MMP-1 positive stain in the cytoplasm of the tumor cells (x200) [Cancer de colon având coloraţie MMP-1 pozitivă în citoplasma celulelor tumorale (x200)]
Figure 3. Colon cancer with MMP-1 negative stain in the cytoplasm of the tumor cells (x200) [Cancer de colon având coloraţie MMP-1 negativă în citoplasma celulelor tumorale (x200)]

ORIgInAL ARTIcLEs
Rath-Wolfson et al10
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
11 cases were positive while 21 were negative, no statistically significant difference.
Forty five patients received chemotherapy. From these 18 stained positively for MMP-1 and 27 were negative.
At the end of this study 47 patients were alive and 21 died of the disease.
Among those patients who were alive, 23 cases were MMP-1 positive and 45 were negative. Among the dead patients’ group 10 were positive and 11 were negative.
In general the survival of the positive ones was 66±7 months, worse than the negative ones 73.3±4.2 months, but the difference was not statistically significant (p=0.125). Disease free survival in the positive group according to MMP-1 status was 49.3±6.5 and in the negative group 63.6±5, p=0.21, no significant differences. In patients who did not receive chemotherapy treatment, survival time showed a statistically significant difference between patients with positive indication for MMP-1 and negative indication (36.2±9.7 months vs. 66.5±7.7 months, p=0.019) (Fig. 4).
For patients who received chemotherapy treatment, there was no statistically significant difference between patients with positive MMP-1 (mean survival was 75.5±7.5 months) and the negatively stained group (mean survival 73.7±4.3 months), p =0.44 (Fig. 5).
Disease-free survival showed similar findings: a statistically significant difference for patients who did not receive chemotherapy treatment (24.2±3.6 months vs. 55.7±8.2 months, p=0.025) (Fig. 6).
A difference that was not statistically significant for patients who received chemotherapy treatment. For the
Table I. Clinical characteristics of patients by Metalloproteinase
Parameters The wholepopulation
Metalloproteinase
Positive (n=23)
Negative(n=45)
Age(years)-mean 68.79 66.69 69.86Sex
Males 43 16 27Females 25 7 18
Sitecolon 48 14 34rectum 20 9 11
GradeWDC 18 6 12MDC 50 17 38
StageB 36 12 24C 32 11 21
ChemotherapyYes 45 18 27No 23 5 18
StatusAlive 47 13 34Dead 21 10 11
MMP-1 – Metalloproteinase-1; WDC – Well-differentiated adenocarcinoma; MDC – Moderately differentiated adenocarcinoma; NS – No statistical significance.
Figure 4. Kaplan-Meier curve comparing the overall survival of positive and negative expression for MMP-1 in patients who did not receive chemotherapy.The graph represents the statistically significant difference between these patients, p=0.019. (Curba Kaplan-Meier compară supravieţuirea globală pentru expresia pozitivă şi negativă pentru MMP-1 la pacienţii care nu au primit chimioterapie. Graficul reprezintă diferenţa semnificativă statistic între aceşti pacienţi, p=0,019)
Figure 5. Kaplan-Meier curve comparing the overall survival of positive and negative expression for MMP-1 in patients who received chemotherapy. The difference was not statistically significant, p=0.44 (Curba Kaplan-Meier compară supravieţuirea globală pentru expresia pozitivă şi negativă pentru MMP-1 la pacienţii care au primit chimioterapie. Diferenţa nu a fost semnificativă statistic, p=0,44)

ORIgInAL ARTIcLEs
Over Expression Of Metalloproteinase-1 In Human Colonic Carcinomas And Its Prognostic Value 11
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
positively stained group 56.3±7.4 months and for the negative group 65.3±5.6, p=0.45.
When considering the gender of the patient, survival time showed a statistically significant difference between male patients with positive and negative MMP-1 indication (77.4±3.6 months vs. 68.9±8.5 months, p=0.04) (Fig. 7), but the difference for female patients was not statistically significant. In the female group the positively stained tumors, the survival time was 52.6±10.2 months and in the negatively stained group 60.4±7.9 months, p=0.61.
Disease-free survival time showed differences that were not statistically significant for male, positive 50.0±7.9 months, negative 67.3±5.5 months, p=0.09. For female patients, in the positively stained tumors, DFS was 41.9±8.5 months, in the negatively stained DFS was 52.4±8.0, p=0.93.
Dicussion
In this study we examined the expression of MMP-1 in 68 patients who suffered of CRC. The general survival curve of the patients with positive MMP-1 staining was worse than the negative ones, even though there was no statistically significant difference, p =0.125. We found that the survival time of the patients who did not receive chemotherapy treatment and were positive for MMP-1 was worse than for the negative ones, with p=0.019. The survival time also showed a statistically significant difference between male patients with positive MMP-1 staining versus those that did not stain, p=0.04. In the female group the difference was not statistically significant, p=0.61. The disease free survival showed similar findings, with a statistically significant difference for those patients who did not receive chemotherapy treatment, again in favor of those who did not stain positively for MMP-1, p=0.0025.
The major factor upon which the oncologists rely whether to administer chemotherapy is the stage.
In the literature there are studies conducted on various proliferating factors in search for a tool which could pinpoint those patients who are at greater risk for recurrences or metastases, such as chromosomal abnormalities, DNA ploidity etc.[2,3,6,7].
It has been shown that increased expression of MMPs occurs at an early stage of colorectal carcinoma and this provides evidence to support the hypothesis that these molecules have a key role in the early stages of the tumor development [18]. These data are in concordance with it’s proteolytic effect against proteoglycans, fibronectin, collagen IV and V and some types of interstitial tissues [13]. This proteolytic
Figure 6. Kaplan-Meier curve comparing the disease-free survival of positive and negative expression for MMP-1 in patients who did not receive chemotherapy.The graph represents the statistically significant difference between these patients, p=0.45 (Curba Kaplan-Meier compară supravieţuirea fără boală pentru expresia pozitivă şi negativă pentru MMP-1 la pacienţii care nu au primit chimioterapie. Graficul prezintă diferenţa semnificativă statistic între aceşti pacienţi, p=0,45)
Figure 7. Kaplan-Meier curve comparing the survival time of positive and negative expression for MMP-1 in male patients. The graph represents the statistically significant difference between these patients, p=0.04 (Curba Kaplan-Meier compară timpul de supravieţuire pentru expresia pozitivă şi negativă pentru MMP-1 la pacienţii de sex masculin. Graficul prezintă diferenţa semnificativă statistic între aceşti pacienţi, p=0,04)
characteristic of MMP-1 may promote tumor invasion and metastases [14]. So it becomes clear how those patients with positive MMP-1 stain had poorer outcome than those with negative stain.
Studies conducted on malignancies of other organs showed positive MMP-1 expression to be unfavorable. In the thyroid the expression of MMP-1 in patients with invasive well differentiated thyroid carcinoma was consistent with the aggressiveness of the tumor. These findings may predict poorer prognosis and warrant a more aggressive surgical treatment [19].

ORIgInAL ARTIcLEs
Rath-Wolfson et al12
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
In breast cancer Okuyama N et al. [20] concluded that MMP-1 plays a crucial role in breast cancer bone metastasis.
Cheng S et al. [21] found that high MMP-1 mRNA expression was an independent unfavorable prognostic factor, and according to their results suggest that MMP-1 is an important gene implicated in the progression of human breast cancer.
An Z et al. [22] administered orally CT1746, an orally-active synthetic MMP inhibitor to nude mice. They found reduction of the primary tumor mass, total spread and metastasis.
Our main conclusion from this study is that those patients, especially males, with positive MMP-1 stain need to be treated more aggressively even in lower stages of the disease.
References
1. Fletcher CDM. Diagnostic histopathology of tumors. 3th edition, Churchill Livingstone, Elservier, 2007, vol 1, pp. 379-416.
2. Rosai J. Rosai and Ackerman Surgical Pathology. 9th edition, Mosby, New York, vol 1, pp 776-855.
3. Pino MS, Chung DC. The chromosomal instability pathway in colon cancer. Gastroenterology. 2010;138(6):2059-72.
4. Griffin MP, Bergstralh EJ, Coffey RJ, Beart RW Jr, Melton LJ III. Predictors of survival after curative resection of carcinoma of the colon and rectum. Cancer 1987;60:2318-24.
5. Russell AH, Tong D, Dawson LE, Wisbeck W. Adenocarcinoma of the proximal colon. Sites of initial dissemination and patterns of recurrence following surgery alone. Cancer 1984;53(2):360-7.
6. Itzkowitz SH, Bloom EJ, Kokal WA, Modin G, Hakomori S, Kim YS. Sialosyl-Tn. A novel mucin antigen associated with prognosis in colorectal cancer patients. Cancer 1990;66(9):1960-6.
7. Andersen SN, Rognum TO, Lund E, Meling GI, Hauge S. Strong HLA-DR expression in large bowel carcinomas is associated with good prognosis. Br J Cancer 1993;68(1):80-5.
8. Harrison JC, Dean PJ, el-Zeky F, Vander Zwaag R. From Dukes through Jass: pathological prognostic indicators in rectal cancer. Hum Pathol 1994;25(5):498-505.
9. Krasna MJ, Flancbaum L, Cody RP, Shneibaum S, Ben Ari G. Vascular and neural invasion in colorectal carcinoma. Incidence and prognostic significance. Cancer 1988;61(5):1018-23.
10. Jen J, Kim H, Piantadosi S, et al. Allelic loss of chromosome 18q and prognosis in colorectal cancer. N Engl J Med 1994;331(4):213-21.
11. Gal R, Sadikov E, Sulkes J, Klein B, Koren R. Deleted in colorectal cancer protein expression as a possible predictor of response to adjuvant chemotherapy in colorectal cancer patients. Dis Colon Rectum 2004;47(7):1216-24.
12. M. Halpern, D. Kravarusic, R. Bubis, R. Koren. Prediction of Response to preoperative chemoirradiation of rectal cancer by DCC protein expression. Medical Connections 2010;3(19):13-28.
13. Murray GI, Duncan ME, O Neil P, Melvin WT, Fothergill JE. Matrix metalloproteinase-1 is associated with poor prognosis in colorectal cancer. Nat Med 1996;2(4):461-2.
14. Nakopoulou L, Giannopoulou I, Gakiopoulou H, Liapis H, A Tzonou, Davaris PS. Matrix Metalloproteinase-1 and –3 in breast cancer: correlation with progesterone receptors and other clinicopathologic features. Hum Pathol 1999;30:436-42.
15. Murray GI, Duncan ME, O’Neil P, McKay JA, Melvin WT, Fothergill JE. Matrix metalloproteinase-1 is associated with poor prognosis in oesophageal cancer. Jpathol 1998;185(3):256-61.
16. Stetler-Stevenson WG, Liotta LA, Kleiner DE Jr. Extracellular matrix 6: role of matrix metalloproteinases in tumor invasion and metastasis. FASEB J 1993;7(15):1434-41.
17. Tryggvason K, Höyhtyä M, Pyke C. Type IV collagenases in invasive tumors. Breast Cancer Res Treat 1993;24(3):209-18.
18. Jeffery N, McLean MH, El-Omar EM, Murray GI. The matrix metalloproteinase/tissue inhibitor of matrix metalloproteinase profile in colorectal polyp cancers. Histopathology 2009;54(7):820-8.
19. Mizrachi A, Koren R, Hadar T, Yaniv E, Morgenstern S, Shvero J. Expression of MMP-1 in invasive well-differentiated thyroid carcinoma. Eur Arch Otorhinolaryngol 2011;268(1):131-5
20. Okuyama N, Matsumine A, Kosugi R, Wakabayashi H, Uchida A. Matrix metalloproteinase-1 is a crucial bone metastasis factor in a human breast cancer-derived highly invasive cell line. Oncol Rep 2008;20(6):1497-504.
21. Cheng S, Tada M, Hida Y, et al. High MMP-1 mRNA expression is a risk factor for disease-free and overall survivals in patients with invasive breast carcinoma. J Surg Res 2008;146(1):104-9.
22. An Z, Wang X , Willmott N et al. Conversion of highly malignant colon cancer from an aggressive to a controlled disease by oral administration of a metalloproteinase inhibitor. Clin Exp Metastasis 1997;15(2):184-95.

Renal Function Monitoring In Urogenital Robot-Assisted Laparoscopic Surgery Performed In General Anaesthesia 13
Abstract
Introduction: Acute kidney injury as defined by RIFLE (Risk, Injury, Failure, Loss, End-stage) and AKIN (Acute Kidney Injury Network) criteria is a common complication after major surgery and occurs in 36 % of patients admitted to intensive care. The importance of early diagnosis of acute renal injury comes from the fact that renal injury may progress to renal failure, increasing in-hospital mortality and costs despite new treatment or prevention methods. Robotic surgery is the latest minimally invasive surgical method with many advantages. The main disadvantage is its high cost.
The aim of this study was to evaluate renal function by analysis of changes in serum creatinine, in robotic assisted laparoscopic surgery under general anaesthesia.
Materials and methods: We performed a descriptive, observational prospective longitudinal study, which were scheduled for robot-assisted laparoscopic surgery. Acute kidney injury was defined as absolute increase in serum creatinine of 0.3 mg/dl, in accordance with AKIN criteria. 23 male patients scheduled for robotic urogenital interventions, with a mean age of 59 years were included in the study. Surgical interventions performed were: 18 prostatectomies, 3
partial nephrectomies, 1 pieloplasty and 1 cystectomy. The average duration of surgery was 5.23 hours.
Results: Nine patients (representing 39 %) developed acute kidney injury; defined as ≥0.3 mg/dl (27 μmol/l) increase of serum creatinine, renal function, was assessed by repeated measurements of serum creatinine. AKI (acute kidney injury), defined as an absolute increase of serum creatinine of 0.3 mg/dl (26.4 μmol/l) compared to baseline values, 72 hours after surgery, was transient. Serum creatinine on the 4th postoperative day was comparable to baseline levels.
Conclusions: Robotic surgery changes renal function by decreasing renal perfusion due to special circumstances, such as pneumoperitoneum, Trendelenburg position and fluid restriction in prostate surgery. Acute kidney injury is transient in robotic surgery performed under general anaesthesia, and resolves within four days postoperatively.
Keywords: acute kidney injury (AKI), robotic surgery, general anaesthesia, uro-genital organ perfusion, creatinine
Introduction
Acute kidney injury (AKI) is the consensus term used to describe the condition previously known as
ORIgInAL ARTIcLEs
RenAl Function MonitoRinG in uRoGenitAl Robot-Assisted lApARoscopic suRGeRY peRFoRMed in GeneRAl AnAestHesiA
Mihály Orsolya1, Bolboacă Sorana Daniela2, Răhăian Rodica4, Chira Cipriana5, Mihály Zoltán Attila3, Coman Ioan3
1Department of Anaesthesia and Intensive Care II, Cluj County Emergency Hospital, 2”Iuliu Haţieganu” University of Medicine and Pharmacy Cluj-Napoca, Department of Medical Statistics and Informatics, 3Cluj Municipal Hospital, Department of Urology, 4Cluj County Emergency Hospital, Department of Immunology, 5Cluj Napoca Municipal Clinic Hospital, Department of Anaesthesia and Intensive Care
Address for correspondence:Mihaly Orsolya, MD Email: [email protected] Received: 02.08.2012 Accepted: 10.09.2012 Med Con October 2012, Vol 7, No 3, 13-21

ORIgInAL ARTIcLEs
Mihály et al14
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
acute renal failure. AKI, as defined by RIFLE (Risk, Injury, Failure, Loss of function, End-stage) and AKIN (Acute Kidney Injury Network) criteria includes the full spectrum of changes in renal function, while renal failure is considered to be the final stage of AKI. Reducing peri-operative perfusion of urogenital organs increases the risk of ischemia, necrosis and infection. Quite frequently, diagnosis is delayed and is associated with increased morbidity and mortality, which involves prolonged hospitalization, increased costs, and loss of quality of life to the patients affected.
AKI occurs in 36% of patients admitted to the ICU [1] and is a common complication after major cardiovascular surgery [2]. It increases in-hospital mortality and costs in spite of new treatment and intervention methods.
In an effort to reach a consensus on the classification of acute kidney injury, ADQI (Acute Dialysis Quality Initiative Group) developed the RIFLE [3] criteria in 2004, establishing three severity classes: R (risk), I (injury), F (failure) and two outcome classes: L (loss of function), E (End Stage Renal Disease), as shown in Table I.
RIFLE criteria are of clinical importance for diagnosis [4], classification of severity [5], monitoring of AKI progression [6], and for prognosis [7].
For further refinement of the definition of AKI, AKIN [8] (Acute Kidney Injury Network) Table II, proposed new RIFLE criteria in 2007. They establish three stages, consistent with the RIFLE criteria. Stage 1 – Risk, stage 2 – Injury, stage 3 – Failure, Loss and End Stage were considered prognostic factors.
The Da Vinci robotic surgical system, the most advanced robot used in clinical practice, allows a minimally invasive approach and is ideal for urologic surgery [9,10].
The system consists of an ergonomic surgeon console, a patient cart with four interactive robotic arms, a 3D high resolution visualization interface and specific EndoWrist [11] articulated tools. This system is designed to transform, filter and transmit the surgeon’s hand movements into precise movements of the instruments, and is an intuitive interface with high performance surgical skills [12] used in urology, general surgery, gynaecology and thoracic surgery [13].
The advantages [14] of this surgical technique are: reduced bleeding, 3D visualization, superior image
Table I. Risk, Injury, Failure, Loss of function, End Stage Renal Disease, (RIFLE) classification
Classification Glomerular filtration criteria Diuresis criteria
Risk Serum creatinine increases by 1.5 fold, GFR* decreases >25%
<0.5 ml/kg/h over 6 hrs
Injury Serum creatinine increases by 2 fold, GFR decreases >50%
<0.5 ml/kg/h over 12 hrs
Failure Serum creatinine increases by 3 fold, or creatinine ≥4 mg/dl, oracute increase of creatinine >0.5 mg/dl, orGFR decreases >75%
<0.3 ml/kg/h over 24 hrsoranuria over 12 hours
Loss Persistent loss of kidney function >4 weeksESRD End Stage Renal Disease >3 months
* GFR = glomerular filtration rate
Table II. Acute Kidney Injury Network (AKIN) classification
AKIN stage Serum creatinine Diuresis
1 increases 1.5-2 fold, or by 0.3 mg/dl (27 μmol/l)
<0.5 ml/kg/h over 6 hrs
2 increases 2-3 fold <0.5 ml/kg/h over 12 hrs3 increases > 3 fold, or >4 mg/dl (354 μmol/l),
with an acute increase by >0.5 mg/dl (44μmol/l)
<0.3 ml/kg/h over 24 hrs, or anuria over 12 hours

ORIgInAL ARTIcLEs
Renal Function Monitoring In Urogenital Robot-Assisted Laparoscopic Surgery Performed In General Anaesthesia 15
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
quality and EndoWrist instruments with seven degrees of free movement, allowing complex movements in small spaces, reduced postoperative pain, rapid resumption of intestinal transit, reduced complications, smaller scars, reduced hospitalization combined with quick recovery, and nerve sparing, which improves urinary continence and sexual dynamics. The main disadvantage is the high cost [15] of this method, as it increases overall costs by approximately $200, or 20% of global prostatectomy costs [16,17].
The aim of this study was to evaluate renal function in robot-assisted laparoscopic surgery performed under general anaesthesia, by means of repeated serum creatinine measurements.
Materials and Methods
We performed a descriptive, observational prospective longitudinal study, including 23 patients admitted to the Urology Department of Cluj-Napoca Municipal Hospital between May 2010 and February 2012, who were scheduled for robot-assisted laparoscopic surgery.
The patients included were scheduled for urological robot-assisted laparoscopic surgery, with no history of chronic renal disease (RIFLE classification R at most), classified as AKIN [18] stage 1, with stable hemodynamic and breathing.
The study was approved by the Ethics Committee of the Cluj-Napoca Municipal Hospital. All patients included agreed to participate after being duly informed on the implications of their inclusion in the study, and signed an informed consent form. Patients were informed of the type of surgery and anaesthesia they were to receive.
From all patients included the following data were collected: pre-operatively – demographic data (gender, age), comorbidity score (Charlson Comorbidity Index [19], physiological scores (Apache II [20], SOFA [21]), risk of anaesthesia assessed by ASA [22] score. Renal function was assessed by RIFLE and AKIN criteria; during surgery: duration of intervention measured in hours (h), haemorrhage (ml), cardiovascular (average BP over 60 mm Hg) and respiratory (peripheral blood oxygen saturation of 94%) stability. Postoperatively we followed vital signs (BP, pulse, respiration), daily diuresis over 4 days postoperatively, and serum creatinine was sampled daily over the first 4 days postoperatively. Renal function was assessed by analysis of changes in serum creatinine.
Acute kidney injury (AKI) was defined by absolute increase in serum creatinine of 0.3 mg/dl (26.4 μmol/l)
compared to baseline levels within 72 hours after surgery, in accordance with new AKIN criteria.
Statistical analysisQualitative variables were expressed as a percentage,
with a confidence interval of 95% (CI 95%) computed for each percentile, using a method optimized method similar to that presented in the article [23].
Quantitative variables were summarized by arithmetic mean and standard deviation (mean standard deviation) for variables with a normal distribution, and as median plus 25% and 75% quartiles for variables that do not follow a normal distribution. The Kolmogorov-Smirnov test [24,25] was used to assess normality; a probability of less than 5% associated with the Kolmogorov-Smirnov statistic indicated the absence of normal data distribution. The Friedman test was used to identify statistically significant differences between baseline serum creatinine values sampled on day 1, day 2, day 3 and day 4 postoperatively. The aim was to follow the changes in renal function, defined as AKI occurrence robot-assisted laparoscopic surgery performed under general anaesthesia.
Results
Twenty-three patients met the study inclusion criteria and their renal function was assessed against serum creatinine levels. Patients were all male, aged between 22 and 72 years, with a mean age of 59 years (median age = 62 years, 25% percentile = 56 years and 75% percentile = 65 years). Most patients were undergoing prostatectomy (18 patients, 78% CI 95% [57%-91%]). Three patients underwent partial nephrectomies (13%, CI 95% [5%-35%]) and one patient underwent cystectomy and pieloplasty, respectively.
The comorbidity score was between 0 and 10, with a median of 3 (percentile 25% = 2, percentile 75% = 5). Apache score was between 1 and 10, with a median of 6 (25% percentile = 4, 75% percentile = 8). Four patients (17%, CI 95% [5%-39%]) had a SOFA score of 1.
The average duration of surgery was 5.23±1.01 hours, and ranged between 4 and 7 hours. Bleeding volume ranged between 200 and 400 ml, with a median of 250 ml and percentiles values of 25% and 75% of 200 ml and 300 ml, respectively.
Concerning serum creatinine levels, only the baseline and 4th post-op samplings were found to have a normal distribution. A summary of creatinine values is shown in Table III, and the evolution of serum creatinine values per patient is presented in Figure 1.
Applying the Friedman test we identified a significant difference in serum creatinine values

ORIgInAL ARTIcLEs
Mihály et al16
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
investigated (chi-squared test value=19.956, degrees of freedom=4, associated probability test p=0.001). The average basal creatinine proved to differ insignificantly from average serum creatinine levels determined on day 4 postoperatively (t statistic=0.705, 22 degrees of freedom, p=0.488). The results of differences between baseline serum creatinine levels and those measured on different days postoperatively are shown in Table IV.
Nine cases developed acute kidney injury, defined as absolute growth of serum creatinine of 0.3 mg/dl above baseline within 72 hours of surgery (39%, CI95% [18%-61%]). However, this criterion was not maintained on post-op day four.
Discussion
The incidence of this type of renal injury consecutive to robot-assisted laparoscopic surgery has not yet been studied. Some specific features of robot-assisted laparoscopic surgical procedures (pneumoperitoneum, Trendelenburg position and hydration restriction in prostatectomies) reduce splanchnic perfusion and increase the incidence of AKI.
The incidence of AKI in robotic surgery was 39%. In literature AKI is described to occur in 36% of patients admitted to intensive care units [2], in 33.5% of patients undergoing bone marrow transplantation [26], 35.7% in patients with burns [27], 35.9% in liver transplant recipients [28] and 37.4% in septic patients [29].
This is the first study that monitors renal function in robotic surgery performed under general anaesthesia, by means of changes in the levels of serum creatinine. Using implemented statistical methods, it provides evidence that AKI occurs in robot-assisted surgery performed under general anaesthesia, but it also reveals that changes to the renal function are transient.
In the USA, 42% of radical prostatectomies performed in 2006 were done using the robot approach; in 2007 their proportion increased to 60% [30]. Currently, 72% of radical prostatectomies performed in the U.S. are done using Da Vinci robotic surgery and the percentage is growing.
Limitation of the study consisted in the use of serum creatinine to define occurrence of AKI. Proteomic methods were used to identify new serum and urine biomarkers, which promise to provide a prompter
Table III. Descriptive parameters of serum creatinine
StatisticSerum creatinine (mg/dL)
baseline day 1 post-op day 2 post-op day 3 post-op day 4 post-oparithmetic mean 0.98 1.24 1.07 1.01 0.95standard deviation 0.17 0.37 0.25 0.23 0.18minimum 0.72 0.85 0.73 0.75 0.65maximum 1.30 2.10 1.64 1.56 1.40median 0.96 1.08 0.99 0.92 0.94percentile 25% 0.87 0.97 0.90 0.88 0.83percentile 75% 1.10 1.52 1.17 1.10 1.03
Table IV. Wilcoxon test: comparative results in serum creatinine levels measured
Serum creatinine (mg/dL) Z-score p valueday 1* – basal -2.905a 0.004day 2* – basal -1.141 a 0.254day 3* – basal -0.472 a 0.637day 2* – day 1* -3.043b 0.002day 3* – day 1* -3.624b < 0.001day 4 * – day 1* -3.751b < 0.001day 3* – day 2* -1.904b 0.057day 4* – day 2* -2.799b 0.005day 4* – day 3* -2.180b 0.029
a = based on negative ranksb = based on positive ranks*postoperative
Figure 1. Evolution of baseline-to-postoperative serum creatinine levels

ORIgInAL ARTIcLEs
Renal Function Monitoring In Urogenital Robot-Assisted Laparoscopic Surgery Performed In General Anaesthesia 17
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
diagnosis of acute kidney injury. These biomolecules are not yet included in current diagnostic criteria.
Conclusions
Renal function changes in robotic surgery, with a statistically significant difference between serum creatinine on postoperative day 1 and baseline levels (p<0.005).
In most cases (7 out of 9; 77%), peak serum creatinine levels were recorded on first postoperative day; in other cases the peak value was recorded on day 2 after surgery.
There is statistically significant difference (p≤0.002) between serum creatinine values on days 2, 3, and 4 after surgery, compared with those on postoperative day 1, with a pattern of gradual decrease close to baseline levels on postoperative day 4.
AKI appears in robotic surgery, with incidence rates comparable to those known from other major surgical procedures quoted in literature. Renal dysfunction is transient; there is no statistically significant difference between serum creatinine levels on the fourth day after surgery and baseline samples, respectively.
References
1. Bagshaw SM, George C, Dinu I, et al. A multi-centre evaluation of the RIFLE criteria for early acute kidney injury in critically ill pacients. Nephrol Dial Transplant 2008;23:1203-10.
2. Ostermann M, Chang RWS. Acute kidney injury in the intensive care unit according to RIFLE. Crit Care Med. 2007;35:1837-43.
3. Bellamo R, Ronco C, Kellum JA, et al. Acute renal failure: Definition, outcome measures, animal models, fluid therapy and information technology needs. The second International Consensus Conference of the ADQI Group. Crit Care 2004;8:204-12.
4. Kellum JA. Defining and classifying AKI: one set of criteria. Nephrol Dial Transplant 2008;23(5):1471-72.
5. Bagshaw SM, George C, Bellomo R. A comparison of the RIFLE and AKIN criteria for acute kidney injury in critically ill patients. Nephrol Dial Transplant 2008;23(5):1569-74.
6. Ali T, Khan I, Simpson W, et al. Incidence and outcomes in acute kidney injury: a comprehensive population-base study. J Am Soc Nephrol 2007;18(4):1292-8.
7. Chen YC, Jeng CC, Tian YC, et al. Rifle classification
for prdicting in-hospital mortality in critically ill sepsis patients. Shock 2009;31(2):139-45.
8. Levin A, Warnock DG, Mehta RL,et al.Acute Kidney Injury Network Working Group. Improving outcomes from acute kidney injury: report of an initiative. Am J Kidney Dis 2007;50(1):1-4.
9. Davies BL, Hibberd RD, Coptcoat MJ, Wickham JEA. A surgeon robot prostatectomy-a laboratory evaluation. J Med Eng Technol 1989; 13:273-277.
10. Rocco B, Matei DV, Melegari S, et al. Robotic vs open prostatectomy in a laparoscopically naive centre: a matched-pair analysis. BJU Int 2009; 104(7):991-5.
11. Hanly EJ, Zand J, Bachman SL, Marohn MR, Talamini MA. Value of the SAGES learning center in introducing new technology. Surg Endosc 2005; 19(4):477-83.
12. Marescaux J, Leroy J, Gagner M, et al. Transatlantic robot-assisted telesurgery. Nature 2001; 413:379-80.
13. Talamini MA, Chapman S, Horgan S, Melvin WS, for the Academic Robotics Group. A prospective analysis of 211 robotic-assisted surgical procedures. Surg Endosc 2003; 17:1521-4.
14. Giulianotti PC, Coratti A, Angelini M, et al. Robotics in general surgery: personal experience in a large community hospital. Arch Surg 2003; 138:777-84.
15. Marescaux J, Soler L. Image-guided robotic surgery. Semin Laparosc Surg 2004; 11:113–122.
16. Bolenz C, Gupta A, Hotze T, et al. Cost comparison of robotic, laparoscopic, and open radical prostatectomy for prostate cancer. Eur Urol 2010; 57:453-8.
17. Barbash GI, Glied SA. New technology and health care costs: The case of robot-assisted surgery. N Engl J Med 2010; 363:701-4.
18. Lopes A, Fernandes P, Jorge Sofia et al. Acute kidney injury in intensive care unit patients: a comparison between the RIFLE and AKIN classifications. Clin J Am Soc Nephrol 2010;5:402-8.
19. Guzzo TJ, Dluzniewski P, Orosco R, Platz EA, Partin AW, Han M. Prediction of mortality after radical prostatectomy by Charlson comorbidity index. Urology 2010; 76(3):553-7.
20. Wong DT, Crofts SL, Gomez M, McGuire GP, Byrick RJ. Evaluation of predictive ability of APACHE II system and hospital outcome in Canadian intensive care unit patients. Crit Care Med 1995; 23(7):1177-83.
21. Vincent JL, Moreno R, Takala J, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/ failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Cere Med 1996; 22(7):707-10.

ORIgInAL ARTIcLEs
Mihály et al18
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
22. .Khan M, Rooh-ul-Muqim, Zarin M, Khalil J, Salman M.J. Influence of ASA score and Charlson Comorbidity Index on the surgical site infection rates. Coll Physicians Surg Pak. 2010; 20(8):506-9.
23. Jäntschi L, Bolboacă SD. Exact Probabilities and Confidence Limits for Binomial Samples: Applied to the Difference between Two Proportions. The Scientific World Journal. 2010;10:865-78.
24. Kolmogorov A. Confidence Limits for an Unknown Distribution Function. The Annals of Mathematical Statistics 1941;12(4):461-3.
25. Smirnov NV. Tables for estimating the goodness of fit of empirical distributions. Ann Math Statist 1948;19(2):279-81.
26. Lopes JA, Jorge S, Silva S, et al. An assesment of the RIFLE criteria for acute renal failure following myeloablative autologous and allogeneic haematopoietic
cell transplantation. One Marrow Trnsplant 2006;38:395.
27. Lopes JA, Jorge S, Neves FC, et al. An assessment of the RIFLE criteria for acute renal failure in severely burned patients. Nephrol Dial Transplant 2007; 22:285.
28. O’Riordan A, Wong V, McQuillan R, et al. Acute renal disease, as defined by the RIFLE criteria, post-liver transplantation. Am J Transplant 2007; 7:168-76.
29. Lopes JA, Jorge S, Resina C, et al. Prognostic utility of RIFLE for acute renal failure in patiets with sepsis. Crit Care 2007; 11:408.
30. Ho C, Tsakonas E, Tran K, et al. Robot-Assisted Surgery Compared with Open Surgery and Laparoscopic Surgery: Clinical Effectiveness and Economic Analyses [Internet]. Ottawa: Canadian Agency for Drugs and Technologies in Health (CADTH); 2011 (Technology report no. 137).
Translation: Dr. Peter László-Herbert

The Prognostic Value Of Serum Amyloid A Levels In Patients With Rheumatoid Arthritis 19
Abstract
Background: The underlying pathogenic mechanisms in RA are largely unknown. Serum amyloid A (SAA), a kind of apolipoprotein, is one of the acute phase proteins and is primarily synthesized in the liver by activated monocytes and macrophages and secreted into the blood. SAA induces effects by cartilage degradation.
Objectives: We sought to evaluate SAA in patients with RA as compared to healthy subjects and to investigate predictive value of SAA for disease activity.
Materials and method: The concentrations of SAA were investigated in 90 patients (mean of age 36.4±12.7 years, mean of arthritis duration 5.3±4.5 years) and 100 healthy controls (mean of age 35.8±11.2 years). SAA concentration was measured by immunonephelometry. SAA concentrations were expressed in mg/L). The results were statistically analyzed by Student’s t-test and p<0.05 (95% CI) was considered statistically significant. Correlation analyses were performed using Spearman’s rank correlation, and differences between groups were calculated with the Wilcoxon signed rank test.
Results: The SAA was raised, sometimes markedly so. SAA levels were found raised in 24 of 90 patients with RA (26.4%), with ranges from 2.53 to 9.86 mg/L, mean value 8.35±0.72 mg/L vs. normal controls, ranges from 3.12 to 5.28 mg/L, mean value 3.93±0.47 mg/L; p value <0.01. Raised SAA levels in RA may indicate a direct correlation with high disease activity (r=0.67; p<0.001). It was demonstrated significant correlations with other acute-phase measurements such as C-reactive protein (CRP) and the erythrocyte sedimentation rate (ESR) (r=0.54, p<0.01).
Conclusion: These findings suggest that SAA is a more sensitive marker of inflammation than is CRP and ESR. In RA, SAA provides the strongest correlations with disease activity, and changes in serum levels best reflect the clinical course.
Key words: serum amyloid A, rheumatoid arthritis, inflammation, disease activity
Introduction
Serum amyloid A (SAA) is a major acute-phase protein released to circulation in response to injury.
ORIgInAL ARTIcLEs
tHe pRoGnostic VAlue oF seRuM AMYloid A leVels in pAtients WitH RHeuMAtoid ARtHRitis
Cojocaru Manole1,2, Ghinescu Minerva Claudia1, Bălăeţ Constantin1, Cojocaru Inimioara Mihaela3, Siloşi Isabela4
1Titu Maiorescu University, Faculty of Medicine, Department of Physiology, 2Dr Ion Stoia Center for Rheumatic Diseases, Bucharest, 3Carol Davila University of Medicine and Pharmacy, Prof. Gheorghe Marinescu Department of Neurology, Colentina Clinical Hospital, Bucharest, 4University of Medicine and Pharmacy, Department of Immunology, Craiova, Romania
Address for correspondence:Cojocaru Manole MD, PhD 5 Thomas Masaryk St., Sector 2, Postal Code 020983 Bucharest, Romania Email: [email protected] Received: 16.06.2012 Accepted: 15.09.2012 Med Con October 2012, Vol 7, No 3, 19-21

ORIgInAL ARTIcLEs
Cojocaru et al20
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
Rheumatoid arthritis (RA) has a very heterogeneous course. It has been suggested that SAA levels may represent the most sensitive measurement of the acute-phase reaction [1].
SAA induces effects on cartilage degradation. Until relatively recently, the erythrocyte sedimentation rate (ESR) and the serum C-reactive protein (CRP) level were used to monitor inflammation clinically [2].
SAA appeared to be produced by synoviocytes, macrophages and endothelial cells. It is very useful in monitoring disease activity in rheumatologic conditions such as RA. Reactive, secondary amyloidosis is characterized by the extracellular accumulation in various tissues of the amyloid. These deposits are highly insoluble and resistant to proteolysis; they disrupt tissue structure and compromise function. Increases both CRP and SAA have been associated with disease activity [3].
The objectives of this study were to evaluate SAA in patients with RA as compared to healthy subjects and to investigate predictive value of SAA for disease activity.
Materials and method
RA was diagnosed according to the criteria of the American College of Rheumatology. The concentrations of SAA were investigated in 90 patients (mean of age 36.4±12.7 years, mean of arthritis duration 5.3±4.5 years) and 100 healthy controls (mean of age 35.8±11.2 years). We excluded patients who had a medical or surgical illness such as recent infection, trauma and/or a neoplastic disease, in order to remove other confounding factors affecting SAA level. Their SAA levels were quantitatively measured by immunonephelometry using an N-Latex SAA reagent. SAA concentrations were expressed in mg/L). The study was approved by our Local Ethics Committee. All patients gave their written informed consent before inclusion.
Statistical analysis results were reported as mean±SD and they were compared using Student’s t test to continuous variables and chi-square analysis for discontinuous variables. As such, a p value<0.05 was considered significant. Correlation analyses were performed using Spearman’s rank correlation, and differences between groups were calculated with the Wilcoxon signed rank test.
Results
The SAA was raised, sometimes markedly so. SAA levels were found raised in 24 of 90 patients with RA (26.6 %). with ranges from 2.53 to 9.86 mg/L, mean value 8.35±0.72 mg/L vs. normal controls, ranges from 3.12 to 5.28 mg/L, mean value 3.93±0.47 mg/L; p value <0.01. Raised SAA levels in RA may indicate a direct correlation with high disease activity (r=0.67; p<0.001). It was demonstrated significant correlations with other acute-phase measurements such as CRP and ESR (r=0.54, p<0.01).
Discussion
This study demonstrates the value of measuring SAA levels as a reliable surrogate marker of inflammation for RA. In RA, SAA levels provided the strongest correlations with clinical measurements of disease activity, and changes in serum levels best reflected the clinical course [1].
It has been suggested that SAA levels may represent the most sensitive measurement of the acute-phase reaction. Host response to injury and infection is accompanied by a rapid rise in the blood of acute-phase proteins such as SAA. Although SAA has been used as a marker for inflammatory diseases, its role in the modulation of inflammation and immunity has not been defined [2].
The effects of SAA on protease production are interesting because in RA a sustained acute-phase reaction has been strongly associated with progressive joint damage. The value of measuring serum amyloid A
Figure 1. Mean serum amyloid A level in patients with rheumatoid arthritis as compared to healthy controls

ORIgInAL ARTIcLEs
The Prognostic Value Of Serum Amyloid A Levels In Patients With Rheumatoid Arthritis 21
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
levels as a reliable surrogate marker of inflammation represents the most sensitive measurement of the acute-phase reaction in RA. Nonetheless, the potential for SAA will be necessary to further explore these relationships, particularly in patients with less advanced RA [3].
Moreover SAA can stimulate the production by synoviocytes of cartilage-degrading proteases. Under the influence of the inflammatory interleukin (IL)-6, hepatic transcription of the messenger ribonucleic acid (mRNA), SAA may increase 1000-fold when exposed to an inflammatory stimulus. SAA production is induced mainly by interleukine (IL-6, IL-1) and tumour necrosis factor (TNF-a). SAA is mainly synthetisized in the liver, but extrahepatic production has been demonstrated in many species, including in humans [4].
In addition, SAA is implicated as both a beneficial and harmful factor in the inflammatory process. Besides its role in amyloidosis and lipid homeostasis during the acute-phase, SAA has recently been assumed to contribute to bone and cartilage destruction. With respect to being a harmful factor, SAA is the precursor of amyloid A, the deposit of which causes amyloidosis. The findings that SAA is produced locally in arthritic joints suggest a potential role of this acute-phase protein in chronic inflammatory diseases such as RA [5].
Despite these important findings, a precise function of SAA in acute inflammation has not been defined. It is notable that a number of studies suggest a link between SAA and leukocyte infiltration. SAA is chemotactic to leukocytes including monocytes, mast cells, and T lymphocytes during an acute-phase response. There is also accumulating evidence suggesting that SAA possesses cytokine-like activities and is able to induce the production of matrix metalloproteinases (MMPs) [3].
Conclusion
The marked increase of SAA has been used as an important indicator for diagnosis and prognosis of inflammatory diseases. The study’s findings suggested that higher level of SAA is a predictor of exacerbation and may play an important role in the pathogenesis of RA.
SAA leads to production of cartilage-degrading proteases by synoviocytes. The SAA levels correlated with disease activity, and decreased with improvement of clinical disease.
Conflict of interest: The authors who have taken part in this study declared that they do not have anything to disclose regarding funding or conflict of interest with respect to this manuscript.
References
1. Cunnane G, Grehan S, Geoghegan S, et al. Serum amyloid A in the assessment of early inflammatory arthritis. J Rheumatol 2000;27:58-63.
2. Sheldon J. Laboratory testing in autoimmune rheumatic diseases. Best Pract Res Clin Rheumatol 2004,18:249-69.
3. Shovman O, Gilburd B, Shoenfeld Y, et al: The diagnostic utility of anti-cyclic citrullinated peptide antibodies, matrix metalloproteinase-3, rheumatoid factor, erythrocyte sedimentation rate, and C-reactive protein in patients with erosive and non-erosive rheumatoid arthritis. Clin Devel Immunol 2005, 12:(3):197-202.
4. Kushner I. Acute phase proteins. In: BD Rose, editor, UPTODATE. Waltham, MA 2006 [Published as CD and online.]
5. Makovitzky J. The nature of the localized meniscus amyloid. In: Bely M, Apathy A, editors. Amyloid and amyloidosis: proceedings of the IXth International Symposium on Amyloidosis, Budapest, Hungary, 2001. p. 409–11.

CENTER FOR DOCUMENTATION AND CONTINUOUS MEDICAL EDUCATION
SATU MARE
The need to continue and enhance medical programs for the medical personnel from the primary and secondary care network, as well as the social and comunity staff from the health care centers in the county of Satu Mare, is a problem whose solution is the development of the Documentation and Continuous Medical Education Center Satu Mare. Satu Mare College of Physicians in partnership with the Association of Family Physicians Satu Mare, the Dental College Satu Mare, wishes within this project to continue the health educational programs in order to improve health services for vulnerable social groups: disabled, social cases as well as for the population of Satu Mare county.
Necesitatea continuării şi perfecţionării programelor de educaţie medicală a personalului medical din reţeaua de asistenţă primară şi secundară, precum şi a personalului de asistenţă socială şi comunitară din centrele de îngrijire ale judeţului Satu Mare este o problemă a cărei soluţie este dezvoltarea Centrului de Documentare şi Educaţie Medicală Continuă Satu Mare. Colegiul Medicilor Satu Mare în parteneriat cu Asociaţia Medicilor de Familie Satu Mare, Colegiul Medicilor Dentişti Satu Mare, doreşte în cadrul acestui proiect continuarea programelor educaţionale în domeniul sănătăţii în vederea ameliorării serviciiilor de sănătate pentru grupurile sociale vulnerabile: dizabilităţi, cazuri sociale, precum şi pentru populaţia judeţului Satu Mare.

Parent’s Attitude Toward The Sex Education That Their Children Learn At School 23
Abstract
This study’s aim was to examine the parents’ attitudes toward the sex education that their children receive at school. Results showed that most parents think sex education should be mandatory; that the children should be taught to avoid sex until marriage; that sex education does encourage children to have safe sex, but also encourages them to have sex; that issues not directly related to sex should be taught in junior high while issues directly related to intercourse should be taught in high school; and that homosexuality should be taught without defending it as right or wrong. Significant differences were found between Muslim and Christian parents about their attitudes toward sex education.
Keywords: Parental attitudes, sex education, Israeli-Arab sector, Muslims, Christians, School
Introduction
Sexuality is an essential component of healthy development for young people. Despite the widely
recognized importance of sexual health, education to promote it remains a sensitive and sometimes controversial issue [1]. Sex education in schools should treat social and familial values respectfully and professionally [2].
Sexuality is perhaps the most powerful aspect of human life, encompassing not only a physical act of intimacy between two persons, but also the potential for the creation of new life. Sexuality is more than just the simple act of two bodies joining together, more than just a physical thing. Sexuality communicates something to the other and to ourselves about what kind of persons we are [3].
It is indeed ironic that while sex is such an important aspect in our lives, parents, elders and teachers in Israel hardly play any significant role in providing scientific knowledge. Talking about sex is banned in the Arab society in Israel, especially in the Muslim society, and an adolescent cannot freely approach his or her parents for guidance. Those who do seek guidance from their parents are not satisfied because the latter try to evade discussion or are not able to give satisfactory answers [4]. Sex is probably one area of our lives about which we
ORIgInAL ARTIcLEs
pARent’s Attitude toWARd tHe seX educAtion tHAt tHeiR cHildRen leARn At scHool
Joubran Samia1, Marcus Ohad2, Iancu Iulian3,8, Hartman Tova4, Abraham Weizman5,8, Rath-Wolfson Lea6,8, Ram Edward7,8
1The Bruce Rappaport Faculty of Medicine Technion-Institute of Technology and Emek Medical Center, 2Department of Psychology, The Yezreel Valley College, 3The Yavne Mental Health Clinic, 4Department of Education and Gender Bar-Ilan university Israel, 5Geha Mental Health Center, Petah Tikva, Israel, 6Department of Pathology, Hasharon Hospital, Rabin Medical Center, 7Division of General Surgery, Hasharon Hospital, Rabin Medical Center, 8Sackler Faculty of Medicine, Tel Aviv University, Israel
Address for correspondence:Edward Ram Division of General Surgery, Rabin Medical Center-Campus Golda Petach Tikva, Keren Kayemet st.7 Tel:972-3-9372323, Fax: 972-3-9372401 E-mail: [email protected] Received: 04.07.2012 Accepted: 15.09.2012 Med Con October 2012, Vol 7, No 3, 23-30

ORIgInAL ARTIcLEs
Joubran et al24
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
know little, and whatever little we happen to know is learned in bits and pieces through sources such as friends, pornographic films, and books [6,7].
The majority of adolescents do not have access to much information; they receive inaccurate information and these myths and misconceptions are carried throughout their lifetime. There is a need to provide adolescents with information so as to enable them to cope better with the changes sex represents in their lives. Though there is a need to educate adolescents on sex education, parents often oppose to such educational programs due to the fear that imparting sex education may lead to experimentation with sex [7]. Parents can have an important influence on their children’s sexual behaviors. Studies indicate that supportive parent-child relationships and parental monitoring and supervision are associated with delayed sexual activity among children [8].
The state of Israel has some 7.4 million inhabitants. The most prominent characteristic of Israel’s population is its high diversity. Besides the main division of the country’s inhabitants into Jews (80%) and Arabs (20%), there are many more subdivisions.
Because of the importance of the religion as a system of faith and ethics, and above all as a structure of meaning, sexuality occupies the attention of many religions because it provides a powerful way to organize and relate human beings. Religions seek to create order and purpose by relating human beings to wider associations such as families and social collectives [3].
Explaining anatomy and the changes one’s body experiences during puberty is essential for enabling young people to grow up with a healthy self-image. In an era where sexual activity in many countries begins at an early age, Muslim adolescents must be informed to better enable them to deal with peer pressure. Sex education can be taught in a way that informs young people about sexuality in scientific and moral terms [9].
The first sex education program for Arab citizens was published in 1996 by the Ministry of Education. This program discussed family life education and sex education aimed at imparting knowledge, skills, and understanding of how to address the subject of sex. The program has 12 chapters of theoretical subjects and activities that include these topics: sex education and education for good family life, adolescence, the relationship between parents and adolescents, one’s body, decision making, friendship, prejudice, education and assertiveness, peer pressure, tradition and habits, AIDS and sexually transmitted disease [10].
In this study we wanted to see whether there is correlation between the parents’ religion (Moslem or Christian) and their attitude towards sex education.
Materials and Methods
In order to reach this goal we composed a questionnaire which was sent to the parents of the children.
QuestionnaireThe study was based on questionnaires developed
by Blendon R [11] that contained questions which examine the parent’s attitude toward sex education and were divided into several sections. The questionnaire was translated into Arabic (two-way translation) and was proofed by an Arab language specialist. From this questionnaire 5 questions, regarding sexual education at school, were utilized:
1. Should sex education at school be mandatory or optional?
2. Should sex education classes at school teach students to avoid sex until marriage or teach the use of contraception when having sex before marriage?
3. Does sex education encourage children to have sexual intercourse today? And will it encourage them to have safe sexual intercourse (using contraceptives) in the future?
4. To which age groups should different subjects be taught as part of sex education?
5. Is it right or wrong to teach the subject of homosexuality in sex education at school?
ParticipantsThis study continues our previous one [12]. The
participants were 797 Israeli-Arab parents from all over Israel whose age ranged was between 20 and 66 (M=39). Among them were 371 Christians and 426 Muslims, 208 males and 589 females; 533 lived in cities and 264 in rural areas or villages; 483 academics (graduated college or university) and 314 non-academics (graduated high school or less). In addition, 545 of the participants defined themselves as secular or traditional and 252 defined themselves as religious or very religious.
ProcedureThe questionnaires were provided to school
administrators across the country, who sent them to randomly and anonymous selected parents from their schools. The anonymously completed questionnaires were sent back to the investigators by mail. Out of 1,000 questionnaires 797 were returned, response rate of 79.7%, which is a high response rate for the Arab community.
Results
In response to question 1, should sex education in school be mandatory or optional? Results indicated that

ORIgInAL ARTIcLEs
Parent’s Attitude Toward The Sex Education That Their Children Learn At School 25
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
76.1% of the parents believed that sex education should be mandatory and only 23.9% believed it should be optional.
There was no significant correlation between a parent’s belief about mandatory sex education and his or her religion [χ2
(1)=1.87, n.s.]. However, when analyzed by religion there was a weak (Φ=0.16) and significant correlation between Muslim parents’ beliefs about mandatory sex education and their gender [χ2
(1)=10.10, p<0.005]; 78.4% of Muslim females believed that sex education should be mandatory (21.6% believe it should be optional), whereas 62.6% of Muslim males believed that sex education should be mandatory (37.4% believe it should be optional).
There was also a weak (Φ=0.16) and significant correlation between Christian parents’ beliefs about mandatory sex education and their gender [χ2
(1)=7.57, p<0.01]; 81.8% of Christian females believed that sex education should be mandatory (18.2% believe it should be optional), whereas 67.8% of Christian males believed that sex education should be mandatory (32.2% believe it should be optional).
We also found a weak (Φ=0.12) and significant correlation between Christian parents’ beliefs about mandatory sex education and their place of residence [χ2
(1)=5.29, p<0.05]. Among urban-dwelling Christians, 81.2% believed that sex education should be mandatory (18.8% believe it should be optional). Among Christians living in villages, 70% believed that sex education should be mandatory (30% believe it should be optional). There was no significant correlation between Muslim parents’ beliefs about mandatory of sex education and their place of residence [χ2
(1)=2.47, n.s.].There was no significant correlation between
parents’ beliefs about mandatory sex education and their degree of religiousness for either Muslim parents [χ2
(1)=0.05, n.s.] or for Christian parents [χ2
(1)=0.01, n.s.]. There was also no significant correlation between parents’ beliefs about mandatory sex education and their degree of education for either Muslim [χ2
(1)=2.79, n.s.] or for Christian parents [χ2
(1)=0.32, n.s.].Figure 1 summarizes all
these results, weather significant or non significant which clearly demonstrates that most parents, regardless of religious affiliation, place of residence, degree of
religiousness, or educational level, believed that sex education should be mandatory. Belief in mandatory sex education is higher among females than among males for both Muslim and Christian parents.
To the second question, whether sex education classes at school should teach students to avoid sex until marriage or teach the use of contraceptives when having sex before marriage?; 73% of the parents believed that sex education should encourage students to avoid sexual intercourse until marriage, whereas only 23% believed that sex education should provide information about birth control.
There was a weak (Φ=0.18) and significant correlation between parents’ attitude toward their children’s sex education and their religion [χ2
(1)=21.07, p<0.001]. Among Muslim parents, 80% believed that sex education should encourage students to avoid sexual intercourse until marriage and 20% believed it should provide information about birth control. Among Christian parents, 64% believed that sex education should encourage students to avoid sexual intercourse until marriage and 36% believed it should provide information about birth control.
When the two religious groups were analyzed separately, there was a weak (Φ=0.17) and significant correlation between Muslim parents’ attitudes toward their children’s sex education and their degree of religiousness [χ2
(3)=29.55, p<0.001]; 88.1% of the religious Muslims parents believed that sex education should encourage students to avoid sexual intercourse until marriage and 11.9% believed it should provide information about birth control, whereas 74.4% of the secular Muslims parents believed that sex education should encourage students to avoid sexual intercourse until marriage and 25.6% believed it should provide information about birth control.
Figure 1. Parents’ beliefs about whether sex education should be mandatory or a choice as a function of their religion (Muslim or Christian) and among each religion
as a function of their gender (male or female) and their place of residence (city or village)

ORIgInAL ARTIcLEs
Joubran et al26
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
In addition, when analyzed by religion there was a medium (Φ=0.22) and significant correlation between Christian parents’ attitudes toward their children’s sex education and their level of education [χ2
(1)=13.44, p<0.001]. Among Christian parents with an academic background, 76.7% believe sex education should encourage students to avoid sexual intercourse until marriage; 23.3% believed that it should provide information about birth control. Among non-academic Christian parents, 55.7% believed that sex education should encourage students to avoid sexual intercourse until marriage and 44.3% believed it should provide information about birth control.
There was no significant correlation between the parents’ attitudes toward their children’s sex education and their gender neither for Muslim parents [χ2
(1)=3.31, n.s.] nor for Christian parents [χ2
(1)=0.24, n.s.]. There was also no significant correlation between parents’ attitudes toward their children’s sex education and their place of residence either for Muslim parents [χ2
(1)=0.03, n.s.] or for Christian parents [χ2
(1)=0.26, n.s.].Figure 2 summarizes these results which demonstrate
that the majority of parents believed sex education should encourage students to avoid sexual intercourse until marriage.
To the third set of questions asked whether sex education encourages children to have sexual intercourse and whether it will encourage them to have safe sexual intercourse in the future, we found that 66% of the parents believed that teaching sex education does encourage their children to have sexual intercourse and 34% did not; 91.9% of the parents believed that teaching sex education does encourage their children to have safe sexual intercourse in the future (and 8,1% do not).
As to the parents’ belief that teaching sex education will encourage their children to have sexual intercourse, we found no significant correlation between this belief and their religion [χ2
(1)=0.81, n.s.]. When divided into religions, however, there was a weak (Φ=0.19) and significant correlation between the Muslim parents’ belief that teaching sex education will encourage their children to have sexual intercourse and their place of residence [χ2
(1)=11.63, p<0.005]; 75.3% of the Muslims living in the city believed that teaching sex
education will encourage their children to have sexual intercourse and 24.7% did not, whereas 57.4% of the Muslims living in villages believe teaching sex education will encourage their children to have sexual intercourse while 42.6% did not.
There was a weak (Φ=0.24) and significant correlation between Muslim parents’ belief that teaching sex education will encourage their children to have sexual intercourse and their level of education [χ2
(1)=18.98, p<0.001]. Among academic Muslims 81.2% believed that teaching sex education will encourage their children to have sexual intercourse and 18.8% did not, whereas among the non-academic Muslims 58.2% believed that teaching sex education will encourage their children to have sexual intercourse and 41.8% did not.
There was no significant correlation between Christian parents’ beliefs that teaching sex education will encourage their children to have sexual intercourse and their place of residence [χ2
(1)=1.42, n.s.], between Christian parents’ belief that teaching sex education will encourage their children to have sexual intercourse and their level of education [χ2
(1)=2.30, n.s.], between parents’ belief that teaching sex education will encourage their children to have sexual intercourse and their gender neither for Muslim parents [χ2
(1)=3.65, n.s.] nor for Christian parents [χ2
(1)=2.24, n.s.] and between parents’ belief that teaching sex education will encourage their children to have sexual intercourse and their degree of religiousness neither for Muslim parents [χ2
(1)=0.33, n.s.] nor for Christian parents [χ2
(1)=3.34, n.s.].Regarding the parents’ belief that teaching sex
education will encourage their children to have safe sexual intercourse in the future, we found a weak
Figure 2. Parents’ attitudes toward sex education as a function of their religion (Muslim or Christian) and among each religion as a function of their degree of religiousness (religious or secular) and their level of education (academic or non-
academic)

ORIgInAL ARTIcLEs
Parent’s Attitude Toward The Sex Education That Their Children Learn At School 27
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
(Φ=0.10) and significant correlation between this belief and their religion [χ2
(1)=6.25, p<0.05], so that 89.2% of the Muslim parents believed that teaching sex education will encourage their children to have safe sexual intercourse in the future and 10.8% did not, whereas 94.8% of the Christian parents believed that teaching sex education will encourage their children to have safe sexual intercourse in the future and 5.2% did not.
When divided into religions there was a weak (Φ=0.18) and significant correlation between Muslim’s belief about whether teaching sex education will encourage their children to have sexual intercourse and their degree of religiousness [χ2
(1)=9.54, p<0.005]. Among religious Muslims 82.4% believed that teaching sex education will encourage their children to have safe sexual intercourse in the future and 17.6% did not, whereas 93.8% of secular Muslims believed that teaching sex education will encourage their children to have safe sexual intercourse in the future and 6.2% did not.
There was also a weak (Φ=0.12) and significant correlation between Muslims’ belief that teaching sex education will encourage their children to have sexual intercourse and their level of education [χ2
(1)=4.03, p<0.005]. Among the academic Muslims 91.9% believed that teaching sex education will encourage their children to have safe sexual intercourse in the future and 8.1% did not, whereas 84.4% of the non-academic Muslims believed that teaching sex education will encourage their children to have safe sexual intercourse in the future and 15.6% did not.
There was no significant correlation between Christians’ belief that teaching sex education will encourage their children to have safe sexual intercourse in the future and their degree of religiousness [χ2
(1)=0.53,
n.s.], between Christians’ belief that teaching sex education will encourage their children to have safe sexual intercourse in the future and their level of education [χ2
(1)=0.14, n.s.], between parents’ belief that teaching sex education will encourage their children to have safe sexual intercourse in the future and their gender neither for Muslim parents [χ2
(1)=1.27, n.s.] nor for Christian parents [χ2
(1)=1.51, n.s.] and between parents’ belief that teaching sex education will encourage their children to have safe sexual intercourse in the future and their place of residence either for the Muslim parents [χ2
(1)=2.78, n.s.] or for Christian parents [χ2
(1)=0.18, n.s.]; Figure 3 summarizes all these results, significant and non significant.
The fourth question asked about the appropriateness of various content areas for students in elementary, junior high, or high school; parents could respond that a given content area should not be taught at all in school, Table I summarizes these results.
Finally we asked the parents whether sex education should teach that homosexuality is acceptable or should it teach only what homosexuality is without discussing whether it is wrong or acceptable, or should it not be discussed at all.
We found that 13.8% of the parents believed that sex education should teach that homosexuality is acceptable, 49.2% believed that homosexuality should be taught without discussion of whether it is acceptable or wrong, 31.8% believed that sex education should teach that homosexuality is wrong, and 5.2% believed that homosexuality should not be taught at all in sex education. There was a significant difference between Muslim and Christian parents’ beliefs about teaching homosexuality in sex education [U(689)=52193, p<0.01];
Muslim parents (mean rank=363.07) object to teaching about homosexuality in sex education more than Christian parents do (mean rank=323.67).
When analyzed by religion, there was a significant difference between religious and secular Muslims in their beliefs about teaching homosexuality in sex education [U(373)=13483, p<0.001]; religious Muslims (mean rank=209.12) object teaching about homosexuality more than secular Muslims did (mean rank=170.92).
There was also a significant difference between religious and non-religious Christian in their
Figure 3. Parents’ belief that teaching sex education will encourage their children to have sexual intercourse and will encourage their children to have safe sexual
intercourse in the future as a function of their religion (Muslim or Christian) and among each religion as a function of their place of residence (city or village) and their
level of education (academic or non-academic)

ORIgInAL ARTIcLEs
Joubran et al28
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
beliefs about teaching homosexuality in sex education [U(316)=6711, p<0.05]; religious Christians (mean rank=177.26) object to teaching about homosexuality more than non-religious Christians do (mean rank=153.92).
There was no difference based on parents’ gender in their beliefs concerning teaching about homosexuality in sex education either for Muslim parents [U(373)=13835, n.s.] or for Christian parents [U(316)=9446, n.s.].
There was no difference based on parents’ place of residence in their beliefs concerning teaching about homosexuality in sex education either for Muslim parents [U(373)=16512.5, n.s.] or for Christian parents [U(316)=8689.5, n.s.].
There was no difference based on parents’ level of education in their beliefs concerning teaching about homosexuality in sex education either for Muslim parents [U(373)=15695.5, n.s.] or for Christian parents [U(316)=10543.5,n.s.]. Although most parents believe that homosexuality should be taught in sex education without the question of right or wrong, many parents still believe it is wrong to teach about homosexuality in sex education, and among religious parents (both Muslims and Christians) the rate of objection is higher.
Discussion
Education is an intentional structured process to impart knowledge and skills and to influence an individual’s developmental course [13].
Adolescence is a time of increased freedom to make choices, and the ability of the adolescent to confront
these choices and make healthy decisions is crucial to development [14].
Today’s generation of adolescents is the largest in history. Nearly half of the global population is 25 years old and younger. Negative outcomes of early pregnancy and sexually transmitted infections threaten the health of people in the second decade of life more than any other age group [15].
Sex education enables people to acquire knowledge and develop skills which they can use to protect themselves and others [14]. In Islam, sexuality is considered part of one’s identity as a human being: Islam is explicit about many aspects of human sexuality. Also, based on the Hadith demonstrating the Prophet’s willingness to discuss these matters openly, it should be obvious that education about matters related to sex is acceptable [9].Teaching about sex does not in itself offend against modesty, indeed parents are urged not to feel shy or embarrassed about providing necessary information about sex to their children [16].
In Christianity the church is the teacher of moral and ethical norms, with the special mission of guarding and protecting the lofty dignity of marriage and the most serious responsibility of the transmission of human life. Sex education is a basic right and duty of parents and must always be carried out under their attentive guidance, whether at home or in educational centers chosen and controlled by them. The mission to educate demands that Christian parents should present to their children all the topics that are necessary for the gradual maturing of their personality from a Christian and ecclesiastical point of view [17].
Table I. Parents’ beliefs concerning what topics are appropriate at what grade level (elementary, junior high, high school or not at all)
Elementary Junior high High school Not at allContraception 45.5% 41.2% 12.9% 0.5%AIDS 12.1% 61.1% 26.3% 0.5%Sex diseases 6.7% 57.3% 34.8% 1.2%Pregnancy planning 1.4% 28.2% 57.8% 12.6%How to use contraception 1.2% 25% 55.1% 18.7%Postponing sex until older 6.1% 41.6% 47.1% 5.2%Where can I check for sex diseases 5.1% 35% 52.1% 7.7%How to deal sensitive issues 22.6% 60.7% 14.8% 1.8%Postponing sex until marriage 2.8% 37.6% 54.4% 5.2%Limiting my partner 2% 22.7% 54.6% 20.7%Masturbation 12.3% 61.6% 18.6% 7.5%How to talk to teen about sex 22.9% 52.6% 21.7% 2.8%Abortion 2% 24.1% 49.3% 24.6%Sexual values 10.3% 35.5% 45.8% 8.4%Use contraception without parental consent 2% 20.9% 38% 39.1%

ORIgInAL ARTIcLEs
Parent’s Attitude Toward The Sex Education That Their Children Learn At School 29
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
In countries with very diverse populations, such as the United States, the main limitation in developing sex education curricula, particularly in public schools, is the inability to select a universally acceptable moral position [9].
In Israel we face the same problem with a highly diverse population and two nations with different cultures, ethnicities, languages, and religions. The Ministry of Education in Israel is responsible for sex education in schools, so the ministry has numerous sex education curricula for each population sector in Israel. During the years 1973-2005 the sex education unit distributed fifteen programs. Cooperation between the Jewish religious sector and Jewish secular sector was very limited; the two sectors represent very different worldviews and therefore the programs of sex education changed frequently and addressed only a few subjects [18].
In our study we found that the majority of parents of both religions believed that sex education should be mandatory, regardless of their level of education or degree of religiousness. These results are in concordance with those found by McKay [19], who found that in the United States and Canada many parents demand to have sexual education included in the school educational program and believed that it should include various subjects and should be learned at an early age.
We also found that mothers wanted sex education to be mandatory at higher rates than did the fathers. In addition, among mothers we found that urban mothers thought sex education should be a mandatory subject more than rural mothers.
In the Arab population only few women work, most of them are housewives [20].
As a result women in the Arab society spend more time with their children and naturally deal with adolescent problems more than their husbands. It is not surprising that they see sex education as a must, since it might serve as an aid to help them deal with the problems of adolescence. In that same vein, it is not surprising that urban mothers think that sex education should be compulsory at higher rates than rural mothers, given that “sources of temptation” are more available in the city (clubs, cafes, pubs and other places of entertainment) than in the villages.
Parental attitudes in our study were at odds with the findings of Jemmott et al. [21], who demonstrated that sex education programs reduced the frequency of sexual intercourse among adolescents who had already experienced sex. On the other hand, the majority of adolescents in their study who did not yet experience sex and who participated in the program continued to abstain from sex. In either category, students who did have sex were more likely to use contraception. In our
research, most parents were in favor of an educational approach focused on discouraging sexual intercourse before marriage but did not support education that encouraged use of contraception, although this approach was found to be more effective. [12].
The public opinion of the Arab community in Israel supports abstinence as a behavioral goal for adolescence [12]. The majority of parents in our study thought sex education should encourage abstinence until marriage. Previous research has found that withholding information from young people only increases the likelihood that when they do have sexual intercourse it will be unprotected [22], especially if the little information they have learned has been acquired on their own without formal instruction. Considering that the average age at marriage is steadily rising worldwide, rates of premarital sexual intercourse are also increasing [23].
Information about sexual behavior is essential to improve sexual health, to correct myths about sexual behavior, and to postpone the age at which young people first have sex [24].
Teaching sex education does not in itself offend modesty and parents are urged not to feel shy about providing necessary information about sex to their children [25].
In fact, there is evidence that sex and sexual education, which includes dispensing condoms and contraceptives, is superior to abstinence-only education in reducing risky sexual behavior [26].
Initiation of sexual intercourse in adolescence is accompanied by considerable risk of sexually transmitted infections (STIs) and pregnancy. Adolescents have the highest age-specific risk for many STIs [27], and the highest age-specific proportion of unintended pregnancies in the United States [28]. In the Middle East cultural taboos are major obstacles to informed discussion about sexual and reproductive health issues, particularly with regard to adolescents. Premarital sexual relationships are forbidden; silence around the topic stems in part from the high value that society puts on a girl’s virginity before marriage and the belief that talking openly about sexual and reproductive – health might encourage unmarried youth to have premarital sex. Reviews of sex education programs worldwide have concluded that sex education does not encourage early sexual activity, and can actually delay the first intercourse and lead to more consistent contraceptive use and safer sex practice [29].
Conclusion
This study examined Arab Israeli parents’ opinions concerning sex education curriculum in schools attended

ORIgInAL ARTIcLEs
Joubran et al30
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
by their children. The parents agreed on a number of the issues addressed in the survey, but significant differences exist between Muslim and Christian parents. On all topics included in the survey, Muslims exhibited more conservative beliefs than Christians.
The findings reported here are among the few studies conducted on sex education in the Arab society in Israel. This is the first study that examines the differences between an urban Arab population and those living in rural villages and the first to examine the differences between Christians and Muslims.
Acknowledgment: to Abhath – The Society for Developing Academic Research for her support and help caring out this study.
References
1. Bay-Cheng LY. The trouble of teen sex: The construction of adolescent sexuality through school-based sexuality education. Sex Education. 2003;3:61-74.
2. Shtarkshall R, Santelli J, Hirsch J. Sex Education and sexual socialization: Role for educators and parents. Perspectives on Sexual and Reproductive Health. 2007;39:116-9.
3. Ellingson S, Green MC, eds. Religion and Sexuality in Cross-Cultural Perspective. New York: Routledge, 2002.
4. Israel Central Bureau of Statistics, 2004. 5. Tjaden P G. Pornography and sex education. Journal of
Sex Research. 1988;24:208-12. 6. Kumar P. Study of sex-related myths in college students.
Journal of Indian Academy of Applied Psychology, 1993;19:21-4.
7. Iwao Hoshii. Sex in Ethics and Law, (Hardcover, 1987)
8. Miller B C, Benson B, Galbraith D. Family relationships and adolescent pregnancy risk: A research synthesis. Developmental Review. 2001;21:1-38.
9. Muslim Women’s League. An Islamic perspective on sexuality. Retrieved online, 1999. http://www.mwlusa.org/topics/sexuality/sexuality_pos.html
10. Israel Ministry of Education, 1996 11. Blendon R. Sex education in America: General public/
parent’s survey. Cambridge ; Harvard University, 2004. 12. Joubran S, Marcus O, Iancu I et al. Parent’s attitude
toward the sex education that their children learn at school. Medical Connections, in press, 2012.
13. Schneewind K A. Socialization and education: Theoretical perspective. In N. J. Smelser & P. B. Baltes (Eds.). International encyclopedia of social and behavioral sciences (pp. 14507-13) sAmterdam, Elsevier, 2001.
14. Beyth-Marom R, Fischhoff B. Adolescents’ decisions about risks: A cognitive perspective. In T. Schulenberg, J. Maggs & K. Hurrelmann (Eds.), Health risks and developmental transition during adolescence (pp. 110-35). Cambridge: Cambridge University Press, 1997.
15. United Nations Population Fund. The state of the world population: Making – one billion count investing in adolescents’ health rights. New York: UNFPA, 2006.
16. Noibi, D. An Islamic perspective. In R. Thomason (Ed.). Religion, ethnicity and sex education: Exploring the issues (pp. 41-57), London: National Children’s Bureau 1993.
17. Pope Paul VI. Gravissimum educationis 3, The Vatican, 1965
18. The Knesset Research and Information Center. Sex education in the school system, 2010.
19. McKay A, Pietrusiak M, Holowaty, P. Parents’ opinions and attitudes towards sexuality education in the schools. The Canadian Journal of Human Sexuality. 1998;7:139-45.
20. Israel Central Bureau of Statistics, 2009 21. Jemmott B, Jemmott S, Fong T. Abstinence and safer-
sex HIV risk reduction interventions for African-American adolescents: A randomized controlled trial. Journal of the American Medical Association. 1998;279:1529-36.
22. Kirby D. Emerging answers: Research findings on programs to reduce teen pregnancy. Washington, DC; the National Campaign to Prevent Teen and Unplanned Pregnancy, 2007.
23. Ragab A, Mahmoud M. Sex education for young people in Egypt: A community-based study. In The proceeding of a conference; Cairo Demographic Center (pp.559-69), 2006.
24. Wellings K, Collumbine M, Slaymaker E, et al. Sexual behavior in context: A global perspective. Lancet. 2006;368:1706-28.
25. Halstead J. M. Muslims and sex education. Journal of Moral Education. 1997;26:317-30.
26. Harper CC, Henderson AS, Schalet DB, Becker D, Stratton L, Raine TR. Abstinence and teenagers: Prevention counseling practices of health care providers serving high-risk patients in the United States. Perspectives on Sexual and Reproductive Health. 2010;42:25-132.
27. Centers for Disease Control and Prevention. Sexually transmitted disease – surveillance. Atlanta. U.S. Department of Health and Human Services, 2004.
28. Institute of Medicine. The best intention: Unintended pregnancy and the well- being of children and families. Washington, DC, National Academy Press, 1995.
29. Kirby D. Impact of sex and HIV education programs on sexual behaviors of youth in developing and developed countries. Family Health International. 2005;2:1-2.

The Ankle-Brachial Index In The Diagnosis Of Symptomatic And Asymptomatic Peripheral Arterial Disease 31
Abstract
The peripheral arterial disease (PAD), evolving asymptomatic in most of the cases a long period of time, can be detected non-invasively by determining the ankle-brachial index (ABI).
Objectives: We sought to determine the correlations between the data obtained by the ABI measurement and the presence of PAD, to improve the early diagnosis of this disease, particularly in the asymptomatic cases.
Material and method: The study enrolled, between 2007-2011, 314 symptomatic and asymptomatic patients, aged>50 years, mean age 61±7 years, 56% men and 44% women, from family medicine offices of Timiş County. The median follow-up time was 34±6 months. The inclusion criteria were the age between 50-79 years, and the presence of manifest cardiovascular disease or at least one major risk factor for cardiovascular and cerebrovascular disease. ABI was performed using a continuous wave Doppler probe and a sphygmomanometer. They were
evaluated in detail in terms of cardiovascular risk factors and associated pathology.
Results: We obtained normal ABI values, between 0.9-1.3, in 72% of patients, and ABI>1.3 was found in 6% of them, 64% of whom were diabetic. ABI confirmed the PAD diagnosis in 22% of the study group, very useful in detecting asymptomatic cases. The incidence of PAD was higher in the elderly, smokers, diabetics, hypertensives and those associated with many atherosclerosis risk factors. The risk of fatal and nonfatal events in PAD group was almost 2.5 times higher (RR: 2.46 CI: 2.04-3.12). The study showed an inverse association between ABI and the number of events, patients with ABI<0.5 presenting a relative risk for cardiovascular events 5 times higher (RR: 5.52 CI: 3.61-7.65) than those with normal ABI.
Conclusions: The determination of the ankle-brachial index proved to be a non-invasive, cheap an easy-to-perform investigation in the family medicine office, with a great importance in the early diagnosis of the PAD.
Keywords: ankle-brachial index, intima-media thickness, peripheral arterial disease.
ORIgInAL ARTIcLEs
tHe AnKle-bRAcHiAl indeX in tHe diAGnosis oF sYMptoMAtic And AsYMptoMAtic peRipHeRAl ARteRiAl diseAse
Adrian Gruici1, Elena Ardeleanu2, Anca Alexandra Matusz3, Rodica Mihăescu4, Roxana Alăman5,Daniela Gurgus2
1CMI, Timiş County, 2Family Medicine Department, UMFT Victor Babeş, Timişoara, 3Academic Society of Family Medicine, Timişoara, 4Semiology Department, UMFT Victor Babeş, Timişoara, 5Cardiology Department, Cardiovascular Institute, Timişoara
Address for correspondence:Dr. Adrian Gruici Tel: 0745149849 Email: [email protected] Received: 05.03.2012 Accepted: 10.09.2012 Med Con October 2012, Vol 7, No 3, 31-38
This paper is supported by the Sectoral Operational Programme Human Resources Development (SOP HRD) 2007-2013, financed from the European Social Fund and by the Romanian Government under the contract number POSDRU/107/1.5/S/82839

ORIgInAL ARTIcLEs
Gruici et al32
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
Introduction
The atherosclerosis is a system disease that leads frequently to myocardial infarction, stroke, aortic and peripheral arterial diseases (PAD). The PAD, as determined by lower limbs atherosclerosis, is an important marker for generalized atherosclerosis, closely related with cardio- and cerebrovascular events. The incidence of fatal and nonfatal cardiovascular events is up two to three times higher in patients with atherosclerosis in the lower limbs.
The epidemiological studies have revealed that the incidence of PAD in the general population is about 10%, with doubled incidence in patients aged >70 years. Although it has been shown that the PAD is a strong predictive factor for future cardiovascular events, previous studies have shown that only a little percent of the patients are early diagnosed. It has been estimated that for every symptomatic patient, there are approximately three up to four undiagnosed cases. Both symptomatic and silent PAD proved to have high levels of cardiovascular mortality and morbidity. Mostly of the patients with PAD have atherosclerosis elsewhere in the vascular system. The risk of premature death in a patient with PAD is three times higher than of the one without peripheral vascular damage.
The ankle-brachial index (ABI) is currently the most common and useful diagnostic method, used to detect the PAD, including the asymptomatic cases. In addition to its diagnostic value, the ABI can be used in the evaluation of the generalized atherosclerosis. Previous studies have shown that an ABI<0.9 has a specificity >98% for PAD and >92% in the prediction of myocardial infarction and stroke.
The risk for cardiovascular diseases is doubled in individuals with an ABI ≤0.9. This risk is even four times higher in men. Only 23% of the patients are symptomatic, most of the cases evolving asymptomatic. In the elderly, an ABI ≤0.9 indicates the presence of subclinical atherosclerosis and it is a strong predictor of total mortality and of cardiovascular morbidity and mortality in the patients without a history of cardiovascular disease.
Family physicians may and have to play a key-role in the diagnosis and the treatment of the PAD and its risk factors. The determination of the ABI is an efficient diagnostic method of the PAD and must be included in the primary care assistance.
Objectives
We sought to determine the correlations between the data obtained by the ABI measurement and the presence of PAD, to improve the early diagnosis of this disease, particularly in the asymptomatic cases.
We aimed to compare the risk of death by any cause or the risk of major cardiovascular events in patients with PAD than in those without PAD. Another objective was to evaluate the individuals with low ABI in terms of major risk factors for cardiovascular disease.
Previous studies have shown that age, hypertension, smoking, diabetes mellitus, hypercholesterolemia and sedentary lifestyle are the main risk factors for PAD. In this study we investigated the ABI in a risk factors based population.
Material and method
The study enrolled between 2007-2011 patients from 7 family medicine offices of Timiş County. The average follow-up time was 34±6 months. All patients underwent a complete vascular screening at the time of the enrolment for atherosclerotic diseases and cardiovascular risk factors.
The study inclusion criteria were defined as age between 50-79 years and the presence of a manifest cardiovascular disease or at least one major risk factor for cardiovascular and cerebrovascular disease. Hypertension, diabetes mellitus, obesity, dyslipidemia and smoking were defined as cardiovascular risk factors.
Major cardiovascular events were: myocardial infarction and coronary revascularization, stable or unstable angina pectoris, stroke or transient ischemic attack, carotid arteries or lower limbs revascularization and amputations due to PAD during the follow-up time. Hospitalization or outpatient discharge letters and results of relevant laboratory or radiology examinations were collected from the patients who recorded different events.
The exclusion criteria were represented by the patient refusal to participate in the study and those with diseases that required hospitalisation such as various forms of advanced cancer or other life-threatening diseases.
The initial study group included 388 patients aged >50 years, who were investigated by medical history, physical examination, vital signs, ECG, biochemistry, echocardiography, IMT and ABI measurement. Written and informed consent was obtained from all participants. Medical history included data about current use of medication, alcohol intake, current and past smoking behaviour.
Physical examination included the measurement of height, weight, abdominal circumference and body mass index (BMI). The body mass index was calculated as weight to height squared. The obesity was defined as BMI ≥30 kg/m2. The abdominal obesity was defined according to the National Cholesterol Education Program Adult Treatment Panel III (NCEP-ATP III) guide as abdominal circumference >88 cm in women and >102 cm in men.

ORIgInAL ARTIcLEs
The Ankle-Brachial Index In The Diagnosis Of Symptomatic And Asymptomatic Peripheral Arterial Disease 33
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
The blood pressure was measured with a random-zero sphygmomanometer in sitting and after three minutes of standing position, together with a count of the pulse rate. Hypertension was defined as a systolic blood pressure >140 mmHg or a diastolic blood pressure >90 mmHg or current use of antihypertensive drugs for the indication of hypertension. Diabetes mellitus was considered to be present when a subject was currently receiving oral antidiabetic drugs or insulin treatment or had a fasting blood glucose level >126 mg/dl.
For the laboratory analysis we used a CardioChek-PA analyzer with PTS-Panels test strips (Polymer Technology Systems, Inc. – CardioChek 7736 Zionsville Road, Indianapolis, Indiana 46268 USA). The blood samples were collected after an overnight fast and were drawn for glucose, total cholesterol, HDL-cholesterol, LDL-cholesterol, triglycerides and ketones. Dyslipidemia was defined, according to the NCEP-ATP III guide, as total plasma cholesterol >200 mg/dl, triglycerides level >150 mg/dl or the current use of lipid-lowering medication.
The urinalysis was performed using the Arkray AutionCheck II equipment with Arkray AutionSticks EB5 urinary test strips (ARKRAY Europe, B.V., Prof. J. H. Bavincklaan 5 1183 AT Amstelveen, The Netherlands). The urine samples were analyzed for detection of glucose, albumin, creatinine, bilirubin, leukocytes, erythrocytes and nitrites. For microalbuminuria these tests have four levels of interpretation: negative, >30 mg/l, >50 mg/l, >100 mg/l, >150 mg/l. Microalbuminuria was defined according to the 2007 ESC Hypertension Guidelines [1] as presenting the following values: 30-300 mg/24h or albumin/creatinine ratio>22 mg/g (men) or >31 mg/g (women). In our study, microalbuminuria was defined as any different interpretation of the negative.
Signs and symptoms suggestive for peripheral arterial disease include: intermittent claudication (pain of the lower limb muscles appeared at walk and disappeared at rest), no pulse in the leg arteries (pedal artery, posterior tibial artery and popliteal artery), ulcer or gangrene. The asymptomatic peripheral arterial disease was defined as ABI ≤ 0.9 in at least one of the legs, but in the absence of intermittent claudication.
Ankle-Brachial Index (ABI)The presence of atherosclerosis in the lower limbs was
evaluated by measuring the systolic blood pressure (SBP) level of the posterior tibial artery and the pedal artery at both sides with an 8 MHz continuous-wave Doppler probe and a sphygmomanometer (Figure 1). The same test was performed at the brachial arteries [2].
For the calculation of the ABI, we used the highest values obtained [2]. The ratio of the SBP at the ankle to the SBP at the arm was calculated for each leg. In patients with
leg pain during walking and having a normal resting ABI, we used an exercise test to settle the diagnosis [2,3]. The peripheral arterial disease was considered present when the resting ABI was <0.90 or when, post exercise, the ABI decreased at least in one leg with >20% [4,5,6].
Intima-media thickness (IMT)The intima-media thickness (IMT) was measured at
baseline in both carotid arteries, as agreed in the Mannheim consensus [10], with a Sonoscape SSI-8000 high-resolution ultrasonography system, equipped with a 10-Mhz linear array transducer. The subjects were examined in a supine position with the head turned 45° from the side being scanned. When an optimal image was obtained, it was frozen on the R wave of the ECG and stored on the system hard-disk. This procedure was repeated three times for both sides. The intima-media thickness was calculated online by built-in software of the ultrasound system. The mean IMT was calculated for the 6 measurements sites in each patient.
The carotid colour Doppler scanning was performed to detect the hemodynamic severity of the carotid artery stenosis. An artery lumen stenosis of more than 50% of the cross-sectional diameter was considered significant
Statistical analysisDifferences between patients with and without
peripheral arterial disease were represented by using the χ2
Posterior tibial artery Pedal artery
Figure 1. Technique for measuring blood pressure with Doppler probe
Figure 2. Intima-media thickness measurement

ORIgInAL ARTIcLEs
Gruici et al34
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
test and unpaired t-student test. P<0.05 was considered statistically significant. All the confidence intervals were calculated at a rate of 95%.
The logistic regression analyses was performed to evaluate the association of the cardiovascular risk factors (age, sex, hypertension, dyslipidemia, diabetes, smoking, sedentary lifestyle) with the occurrence of the PAD.
The association between the carotid IMT and the ABI had been evaluated by linear regression analysis, adjusted for age and sex. We used the logistic regression to estimate the risk of PAD in patients with increased IMT.
The calculations were performed using the statistical software package Statcalc Epi-Info Version 6.
Results
Of the 365 patients with complete clinical and laboratory data, only 314 presented the study inclusion criteria and were considered eligible for the study. A number of 176 (56% ) were men and a number of 138 (44%) were women. The mean age of the study group was 61±7 years. 98 patients (31.2%), mostly men, presented a history of cardiovascular disease and 39 of them were known with a cerebrovascular disease.
As regarding the risk factors, 180 patients, mostly men, were active smokers or ex-smokers (57.4%), 231 (73.5%) were hypertensives, 108 (34.3%) were diabetics
Table I. Biological data of the study group
Characteristics Study group(n=314)
PAD(n=69)
No PAD(n=245) P value
SBP (mmHg) 150±22 155±21 145±23 <0.001DBP (mmHg) 91±12 96±10 86±11 <0.001BMI (kg/m2) 27.5±4.5 28.2±5.1 27.4±4.4 0.01Total Cholesterol (mg/dl) 205±21 209±24 199±22 0.01HDL (mg/dl) 43±8 40±7 42±6 0.01LDL (mg/dl) 137±14 141±15 133±12 0.01Triglycerides (mg/dl) 150±18 155±21 147±18 0.02IMT (mm) 0.97±0.24 1.12 0.78 <0.001Microalbuminuria (%) 17% 22% 15% <0.001
Table II.Clinical data of the study population
Characteristics Study Group(n=314)
PAD(n=69)
No PAD(n=245) P value
Sex (male %) 176(56) 38(55) 138(56.3) 0.01Age (years) 61±7 63±8 60±3 <0.000150-59 (%) 117(37.2) 14(20.2) 103(42)60-60 (%) 124(39.5) 29(42) 95(38.8)70-79 (%) 73(23.2) 26(37.7) 47(19)HTA 231(73.5) 60(87) 171(70) <0.001Diabetes (%) 108(34.3) 30(43.4) 78(31.8) <0.001Dyslipidemia 167(53.1) 42(60.8) 125(51) <0.001Smokers (%) 180(57.4) 50(72.4) 130(53) <0.0001Intermittent Claudication (%) 32(10.2) 15(22.1) 17(7) <0.0001No peripheral pulse (%) 25(8) 10(14.5) 15(6.1) <0.0001Cardiovascular Events% 98(31.2) 36(52) 62(25.3) <0.0001Cerebrovascular Events% 39(12.4) 17(24.6) 22(9) <0.0001Nr. risk factors (%)
1 56(17.8) 5(7.2) 51(20.8)2 133(42.4) 18(26) 115(47)3 89(28.3) 35(50.7) 54(22)4 36(11.5) 11(16) 25(10) <0.0001

ORIgInAL ARTIcLEs
The Ankle-Brachial Index In The Diagnosis Of Symptomatic And Asymptomatic Peripheral Arterial Disease 35
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
and 167 (53.1%) were known with dyslipidemia. The biological and clinical data of the study group are presented in Tables I and II.
From the study population, 56 patients (17.8%) presented a single risk factor, 133 (42.4%) had two risk factors, 89 (28.3%) had three risk factors and a number of 36 (11.5%) individuals presented even four risk factors for cardiovascular disease.
The medical history revealed that 32 (10.2%) patients presented pain or discomfort in the lower limbs during walking. The pain disappeared in 15 of them after a 10 minutes rest (intermittent claudication). Physical examination showed the absence of the peripheral pulse in the lower limbs in 25 patients (8%) and trophic changes in 19 patients (6.2%).
Determination of the Ankle-Brachial Index (ABI)The values obtained from the ABI measurement
ranged from 0.38 to 1.45, with a mean of 0.98. Normal ABI values, between 0.9-1.3, were recorded in 226 patients (72%). An ABI >1.3 was found in 19 (6%) patients, 12 (64%) of whom were diabetics. An ABI <0.9 we found in 69 patients (22%), without major differences between men and women (Table III).
Mild PAD (ABI: 0.9-0.7) was found in 41 patients (59.4%), moderate PAD (ABI: 0.7-0.5) we found in 19 patients (27.5%). Severe PAD (ABI<0.5) was found in 9 patients (13%, Table IV).
From the 69 patients with PAD, 15 subjects (21.7%) were symptomatic, while in 54 (78.3%) cases we found asymptomatic PAD.
The pathological ABI values were found in elderly, subjects with a lot of risk factors and in those with trophic changes in the lower limbs. Patients with PAD are active or ex-smokers, with associated diseases (HTA, DZ, dyslipidemia). We found a strong statistical difference between the ABI values of the smokers comparing with the nonsmokers.
The probability of PAD increased with the number of the risk factors. From the 69 patients with an ABI<0.9, 46 (66.6%) had three or even more risk factors for cardiovascular disease and 30 (43.4%) of them had diabetes mellitus.
The diabetes was found in only 31.8% of the patients without PAD (Table V).
During the follow-up time, 17 patients died. The deaths were caused by myocardial infarction (6 cases), stroke (3 cases) or other causes (8 cases).
During the follow-up period, we recorded 20 nonfatal cardiovascular events, of whom, 5 presented a myocardial infarction and 7 had a coronary revascularization; 5 patients presented a stroke, 2 cases of revascularization in the lower limbs while 1 subject needed an amputation due to the PAD.
Table III. Values obtained at ABI measurement
No. Ankle-Brachial Index
Nr. of patients
Percentage (%)
1 ABI <0.9 69 222 ABI 0.9-1.3 226 723 ABI >1.3 19 6
Figure 3. Distribution of the study group according to the ABI values
Figure 4. Distribution of the ABI values in the study population
Figure 5. Prevalence of symptomatic and asymptomatic PAD in the study population
Table IV. PAD classification according to the ABI values
No. Ankle-Brachial Index
Nr. of patients
Percentage (%)
1 ABI 0.9-0.7 41 59.52 ABI 0.7-0.5 19 27.53 ABI <0.5 9 13.0
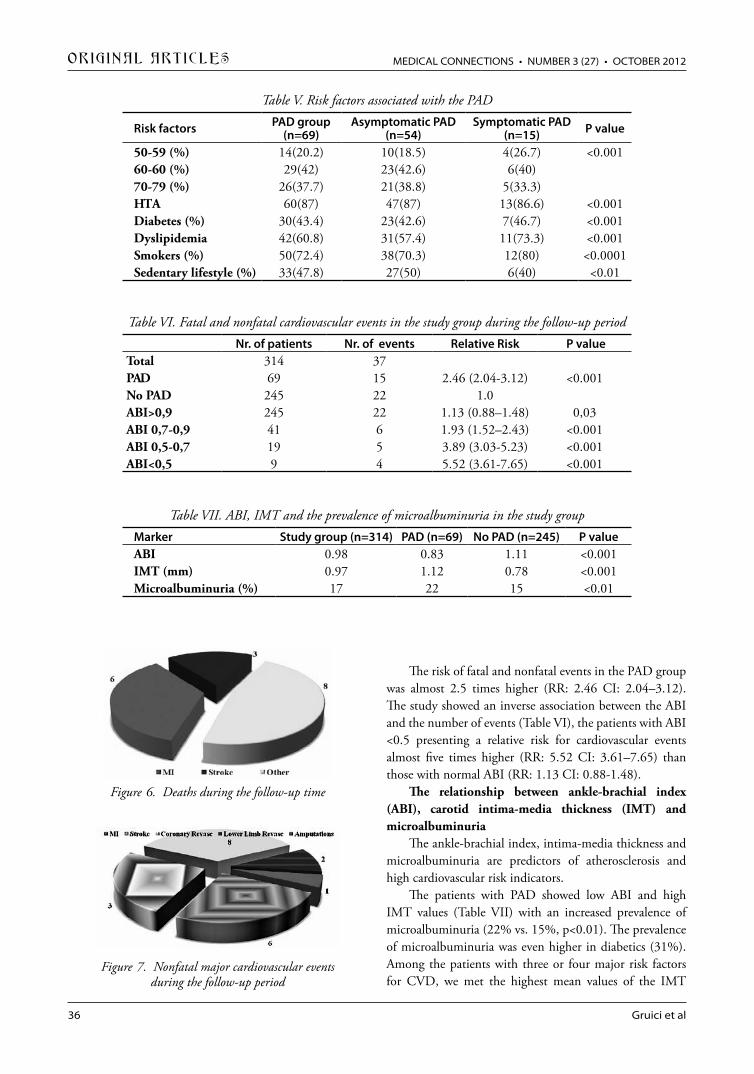
ORIgInAL ARTIcLEs
Gruici et al36
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
The risk of fatal and nonfatal events in the PAD group was almost 2.5 times higher (RR: 2.46 CI: 2.04–3.12). The study showed an inverse association between the ABI and the number of events (Table VI), the patients with ABI <0.5 presenting a relative risk for cardiovascular events almost five times higher (RR: 5.52 CI: 3.61–7.65) than those with normal ABI (RR: 1.13 CI: 0.88-1.48).
The relationship between ankle-brachial index (ABI), carotid intima-media thickness (IMT) and microalbuminuria
The ankle-brachial index, intima-media thickness and microalbuminuria are predictors of atherosclerosis and high cardiovascular risk indicators.
The patients with PAD showed low ABI and high IMT values (Table VII) with an increased prevalence of microalbuminuria (22% vs. 15%, p<0.01). The prevalence of microalbuminuria was even higher in diabetics (31%). Among the patients with three or four major risk factors for CVD, we met the highest mean values of the IMT
Table VI. Fatal and nonfatal cardiovascular events in the study group during the follow-up periodNr. of patients Nr. of events Relative Risk P value
Total 314 37PAD 69 15 2.46 (2.04-3.12) <0.001No PAD 245 22 1.0ABI>0,9 245 22 1.13 (0.88–1.48) 0,03ABI 0,7-0,9 41 6 1.93 (1.52–2.43) <0.001ABI 0,5-0,7 19 5 3.89 (3.03-5.23) <0.001ABI<0,5 9 4 5.52 (3.61-7.65) <0.001
Figure 6. Deaths during the follow-up time
Figure 7. Nonfatal major cardiovascular events during the follow-up period
Table V. Risk factors associated with the PAD
Risk factors PAD group(n=69)
Asymptomatic PAD(n=54)
Symptomatic PAD(n=15) P value
50-59 (%) 14(20.2) 10(18.5) 4(26.7) <0.00160-60 (%) 29(42) 23(42.6) 6(40)70-79 (%) 26(37.7) 21(38.8) 5(33.3)HTA 60(87) 47(87) 13(86.6) <0.001Diabetes (%) 30(43.4) 23(42.6) 7(46.7) <0.001Dyslipidemia 42(60.8) 31(57.4) 11(73.3) <0.001Smokers (%) 50(72.4) 38(70.3) 12(80) <0.0001Sedentary lifestyle (%) 33(47.8) 27(50) 6(40) <0.01
Table VII. ABI, IMT and the prevalence of microalbuminuria in the study groupMarker Study group (n=314) PAD (n=69) No PAD (n=245) P valueABI 0.98 0.83 1.11 <0.001IMT (mm) 0.97 1.12 0.78 <0.001Microalbuminuria (%) 17 22 15 <0.01

ORIgInAL ARTIcLEs
The Ankle-Brachial Index In The Diagnosis Of Symptomatic And Asymptomatic Peripheral Arterial Disease 37
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
Figure 8. Major cardiovascular events in the study population during the follow-up period
Figure 9. Relationship between ABI and IMT
(1.18 mm), the largest frequency of low ABI (25%), and the highest prevalence of microalbuminuria (26%).
The IMT measurement values ranged from 0.41-3.89 mm with an average of 0.97 mm. IMT was considered increased when it exceeded 0.9 mm. A value of IMT >2 mm, obtained from ultrasound measurements, was considered a plaque and was included in the calculation of the average IMT for that patient. At the ultrasound measurement, from the 314 patients enrolled, 166 (53%) presented pathological values of the IMT (>0.9 mm) and the rest of 148 patients had normal values.
The linear regression analysis demonstrated an inverse relationship between the ABI and IMT. Thus an increase of 0.1 mm of the IMT caused a mean reduction of the ABI with 0.034 (CI: 0.024-0.051), slightly more pronounced in men than in women.
Discussion
The peripheral arterial disease is widespread among the elderly, and depending on severity, has an increased risk of death or occurrence of major cardiovascular events [2,3]. In the general population, the incidence of the PAD determined by ABI, range between 5 and 13% [4,5]. In a population with risk factors for atherosclerosis or with manifest cardiovascular disease, also in our study population, the incidence of PAD oscillates between 15 and 40%.
The prevalence of peripheral arterial disease increased with age and with the presence of diabetes, hypertension and smoking habits. The main risk factors in the development of asymptomatic PAD are represented by older age, hypertension, hypercholesterolemia, diabetes, smoking and sedentary lifestyle [6,7,8].
Because the PAD symptoms are largely linked with movement, nonathletes, through their lifestyle, mask the clinical expression of PAD, mainly intermittent claudication [9]. In our study, the AB index confirmed the diagnosis of PAD in 22% of the patients, being very useful in detecting asymptomatic arterial disease. Aggregation of multiple risk factors for atherosclerosis was associated with an increased prevalence of PAD.
The risk of fatal and nonfatal events recorded in patients with PAD was almost 2.5 times higher (RR: 2.46 CI: 2.04-3.12). There is an inverse association between the ABI and the number of events. Thus patients with ABI <0.5 had a relative risk of cardiovascular events by nearly five times higher (RR: 5.52 CI: 3.61-7.65) than those with ABI >0.9 (RR: 1.13 CI: 0.88-1.48).
Our results showed that the ABI is a good predictor of cardiovascular risk both in symptomatic and asymptomatic patients. Its decrease to below 0.9 is associated with the
increasing of the cardiovascular and cerebrovascular morbidity and mortality. This parameter can improve the identification of the high-risk patients [10,11].
Conclusions
The ankle-brachial index proved to be an important indicator of atherosclerosis and a strong prognostic factor of cardiovascular events in high risk patients. The prevalence of peripheral arterial disease was higher in the elderly, smokers, diabetics, hypertensives and those who associate more risk factors for atherosclerosis.
The risk of fatal and nonfatal events recorded in patients with PAD was almost 2.5 times higher (RR: 2.46 CI: 2.04-3.12). An inverse association was observed between the ABI values and the number of events. Thus patients with ABI <0.5 had a relative risk of cardiovascular events by nearly five times higher (RR: 5.52 CI: 3.61-7.65) than those with ABI >0.9 (RR: 1.13 CI: 0.88-1.48).
The study demonstrated an inverse association between the ABI and the intima media thickness. A gradual decrease of the ABI was observed with increasing IMT values.
The determination of the ankle-brachial index proved to be a non-invasive, cheap an easy-to-perform investigation

ORIgInAL ARTIcLEs
Gruici et al38
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
in the family medicine office, with a great importance in the early diagnosis of the PAD.
References
1. Mancia G, De Backer G, Dominiczak A, et all. The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC) 2007 Guidelines for the management of arterial hypertension. European Heart Journal 2007;28:1462-536.
2. Arsenescu I, Stoica A, Matei C, Pop I. Diagnosticul şi tratamentul arteriopatiei obliterante în cabinetul medicului de familie, ISBN 978-973-0-05484-2.
3. Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG, TASC II Working Group, Bell K, Caporusso J, Durand-Zaleski I, Komori K, Lammer J, Liapis C, et all. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). Eur J Vasc Endovasc Surg 2007,33(Suppl 1):1-75.
4. Abela GS. Peripheral Vascular Disease. Basic Diagnostic and Therapeutic Approaches, Lippincot Williams, 2004
5. Apetrei E. Arteriopatiile periferice, Ed. Medicală, Bucureşti, 1986
6. Hirsch AT, Haskal ZJ, Hertzer NR, Bakal CW, Creager MA, Halperin JL, et al. ACC/AHA 2005
Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic). Circulation 2006;113:e463–e654.
7. Ankle Brachial Index Collaboration, Fowkes FG, Murray GD, Butcher I, Heald CL, Lee RJ, Chambless LE, et all. Ankle. brachial index combined with Framingham risk score to predict cardiovascular events and mortality: a meta-analysis. JAMA 2008,300:197-208.
8. Hirsch AT, Criqui MH, Treat-Jacobson D, Regensteiner JG, Creager MA, Olin JW, et all. Peripheral arterial disease detection, awareness, and treatment in primary care. JAMA 2001,286:1317-24.
9. McDermott MM, Greenland P, Liu K, Guralnik JM, Celic L, Criqui MH, et all. The ankle brachial index is associated with leg function and physical activity: the Walking and Leg Circulation Study. Ann Intern Med 2002;136:873–883.
10. Price JF, Tzoulaki I, Lee AJ, Fowkes FG. Ankle brachial index and intima media thickness predict cardiovascular events similarly and increased prediction when combined. J Clin Epidemiol 2007;60(10):1067-75.
11. McDermott MM, Liu K, Criqui MH, Ruth K, Goff D, Saad MF, Wu C, Homma S, Sharrett AR: Ankle-brachial index and subclinical cardiac and carotid disease: the multi-ethnic study of atherosclerosis. Am J Epidemiol 2005;162(1):33-41.

Lead Exposure-Hematological And Cardiovascular Side Effects 39
Abstract
Although lead is one of the most extensively studied pollutants, the health significance of hematological and cardiovascular side effects remain unclear. Anemia and hypertension are manifestations of lead toxicity. However, there are conflicting reports of its prevalence among lead exposed workers, and it is uncertain whether they should be monitored by periodic hemoglobin and blood pressure examinations. To explore the relation between hematological and cardiovascular side effects and lead exposure, we examined the correlation between hemoglobin, hematocrit, blood pressure, electrocardiogram and blood lead levels in 223 workers in a lead acid battery plant. Blood lead levels exceeded 40μg/dl in 56 (25.11%) of the blood samples. The correlation between blood lead levels and hematocrit was weak (r=0.178). Blood lead levels did not correlated with hemoglobin levels, blood pressure values or electrocardiogram changes. We conclude that blood cell count, blood pressure and electrocardiogram are not useful indicators of lead exposure. The discrepancies between the reported correlations remain unexplained and need further study. Any findings of hematological or cardiovascular changes in lead exposed workers should be considered to be due to lead toxicity only after other causes have been excluded.
Keywords: lead exposure, blood lead level, hemoglobin, high blood pressure
Introduction
Chronic lead poisoning remains a major health problem recognized worldwide, despite the toxicity of lead has been known and described since antiquity [1]. Lead has no physiological role in the body, while its harmful effects are innumerable [2].
Lead inhibits the activity of enzymes involved in the heme biosynthesis; affect the stability of erythrocyte membrane, decreases the life time of erythrocytes and produces haemolysis, leading to anaemia [3].
It was shown that lead impairs vessels smooth muscle responsiveness to vasoactive stimuli, resulting in increase of the cholinergic response in dopaminergic cardiac and vascular receptors. The relationship between lead and blood pressure is still under debate and remains a public health problem [4].
The purpose of this study was to asses the dose response relationship at occupational lead exposed people with emphasis on haematological and cardiovascular side effects.
Materials and methods
This research was conducted in a battery manufacturing plant and involved 223 workers, who were continuously exposed to lead.
The main objective was to evaluate the internal lead load of the body through the medium of lead
ORIgInAL ARTIcLEs
leAd eXposuRe-HeMAtoloGicAl And cARdioVAsculAR side eFFects
Ruja Elena¹, Cocârlă Aristotel²
¹Phoenix Diagnostic Clinic, Cluj Napoca, ²University of Medicine and Pharmacy “Iuliu Haţieganu”, Cluj Napoca
Address for correspondence:Ruja Elena, MD, 8 Iuliu Moldovan St, Cluj Napoca E-mail: [email protected] Received: 18.06.2012 Accepted: 15.08.2012 Med Con October 2012 Vol 7, No 3, 39-41

ORIgInAL ARTIcLEs
Ruja et al40
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
biomarkers, in order to assess the health status of the employees working on the production departments.
The blood lead level is the reference indicator used in biological monitoring of occupationally lead exposed workers. Blood lead was measured by means of a direct method using a graphite furnace atomic absorption spectrophotometer SpectraA 110A - Varian.
Physiological and biological tests performed to determine the side effects of lead on the cardiovascular and hematoformator systems were: cell blood count, blood pressure and ECG.
Blood pressure was measured twice in succession with a five minutes interval, using a mercury sphygmomanometer. Hypertension was defined as average systolic blood pressure higher than 140 mmHg and the diastolic blood pressure higher than 90 mmHg. Individuals with normal blood pressure who were using antihypertensive medication were classified as hypertensive.
The employees monitoring took place at the end of the shift, and held out at the occupational medicine office where there were no traces of lead neither in the air nor on surfaces.
Statistical analyzes were performed using SPSS for Windows, version 16. Any values of p less than 0.05 were considered statistically significant.
Results
All 223 employees enrolled in this study were men. The work seniority was 18.13 years in average, with minimum of 0.09 years and a maximum of 37.10 years. All employees worked for 8 hours a day, five days a week.
A total of 56 workers (25.11%) recorded blood lead levels higher then normal limit of 40 μg/dl, and of these 5 (2.24%) had values higher then 60 μg/dl.
The total arithmetic mean of blood lead levels was 36.14 μg/dl with minimum value of 6.44 μg/dl and the highest one of 65 μg/dl.
The highest lead average values of 38.77 μg/dl were recorded in those employees who had seniority over 30 years, while the lowest average of 31.78 μg/dl were recorded in those who worked 5 to 10 years. The maximum blood lead values 65 μg/dl were recorded in groups with work experience of 0-5 years, 10-15 years, 20-30 years, and over 30 years. When applying ANOVA, omnibus F test results showed that there was no significant difference in the blood lead level according to work seniority (p> 0.05).
A total of 18 subjects (8.07%) had haemoglobin levels below the normal values of 14-17 g/dl. The total
arithmetic average of haemoglobin was 15.95 g/dl, range 12.6-19.7 g/dl.
There was no significant correlation between haemoglobin values and blood lead level (p=0.182)
A total of 11 subjects (4.93%) had hematocrit values below the normal of 42-50%. The total arithmetic average of hematocrit was 44.92, range 36-56.
There was a significant positive correlation between blood lead levels and hematocrit values (p=0.029), but this correlation was weak, r=0.178. Only 2.4% of the hematocrit variation was due to changes in blood lead levels. (Coefficient of determination R² is equal to 0.024)
A total of 57 subjects (25.56%) had hypertension. There was no statistically significant correlation between blood lead levels and blood pressure values (p=0.083).
We performed electrocardiograms for 208 of the 233 investigated subjects. We had reported the next type of changes: ventricular extra systoles, right bundle branch block, ST segment changes, sinusal tachycardia in 19 subjects.
There was no significant positive correlation between the blood lead level and the changes recorded on the ECG. (p=0.284).
Discussions
Haemoglobin levels did not correlate with blood lead levels. The discovery of anaemia in a person with a blood lead level up to 80 μg/dl should be considered to be the result of lead toxicity only after other causes of anaemia have been excluded. It has also been reported that periodic haemoglobin determinations are not useful indicators of lead exposure [5]. In a study conducted in Japan, the group of workers whose blood lead levels were lower exhibited significantly lower hematocrit, haemoglobin, and erythrocyte values than the group of workers whose blood lead levels were higher [6]. In our study a significant relationship was found between blood lead levels and low hematocrit levels. The relationship between blood lead levels and anaemia varied according to the exposure dose, time and lifestyle factors such as nutrition, smoking, and alcohol consumption [7].
Many experimental animal studies have shown that chronic exposure to lead can increase systolic and/or diastolic blood pressure in mammals, and several plausible theories for their role in the etiology of hypertension have been proposed. Human studies have generally provided less conclusive evidence for the role of lead in hypertension [8]. It has been reported that long-term occupational exposure was related to a slight

ORIgInAL ARTIcLEs
Lead Exposure-Hematological And Cardiovascular Side Effects 41
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
increase in both systolic and diastolic blood pressure [9]. As in similar studies evaluating the effect of lead exposure on blood pressure [10], our study showed that there was no significant relationship between blood lead levels and systolic and/or diastolic blood pressure.
Conclusions
Blood lead levels did not correlated with hemoglobin levels, blood pressure values or electrocardiogram changes. We conclude that blood cell count, blood pressure and electrocardiogram are not useful indicators of lead exposure. The discrepancies between the reported correlations remain unexplained and need further study. Any findings of hematological or cardiovascular changes in lead exposed workers should be considered to be due to lead toxicity only after other causes have been excluded.
References
1. De Rosa CT, Choudhury H, Peirano WB. An integrated exposure/pharmacokinetic based approach to the assessment of complex exposures: Lead: A case study. Toxicol Ind Health 1991;7(4):231247.
2. U.S. Department of Labour Occupational Safety and Health Administration Screening and surveillance: A guide to OSHA Standards. OSHA 3162.2000;19-20.
3. Clayton GD, Clayton FE. Patty’s Industrial Hygiene and Toxicology. 3th Ed. New York: John Wilez and Sons Inc; 1981,pp:567-9.
4. Goyer R.A. Lead toxicity: from overt to subclinical to subtle health effects. Env Health Perspect 1990;86:177-81.
5. Froom P, Kristal-Boneh E, Benbassat J, Ashkanazi R, Ribak J. Lead exposure in battery-factory workers is not associated with anaemia. J Occup Environ Med 1999;41:120-3.
6. Makino S, Shimizu Y, Takata T. A study on the relationship between blood lead levels and anaemia indicators in workers exposed to low levels of lead. Ind Health 1997;35:537-41.
7. Pala K, Turkkan A, Gucer S, Osman E, Aytekin H. Occupational Lead Expousure: Blood Lead Levels of Apprentices in Bursa, Turkey. Ind Health 2009;47:97-102.
8. Telisman S, Pizent A, Jurasovic J, Cvitkovic P. Load effect on blood pressure in moderately lead exposed male workers. Am J Ind Med 2004;45:446-54.
9. Fenga C, Cacciola A, Martino LB, Calderaro SR, Di Nola C, Verzera A, Trimarchi G, Germanò D. Relationship of blood lead levels to blood pressure in exhaust battery storage workers. Ind Health 2006;44:304-9.
10. Mormontoy W, Gastañaga C, Gonzales G. Blood lead levels among police officers in Lima and Callao, 2004. Int J Hyg Environ Health 2006;209:497-502.

www.conexiunimedicale.roISSN 1843-9306
Revista „Medical Connections / Conexiuni Medicale” are o vizibilitate naţională şi internaţională prin versiunea electronică pe site-ul www.conexiunimedicale.ro (ISSN e-serials 2068–8369), prin indexarea în Journals Master List a bazei de date internaţionale Index Copernicus®, începând cu numerele din anul 2009, precum şi datorită includerii în cadrul schimburilor cu Universitatea Titu Maiorescu, Bucureşti, Facultatea de Medicină şi Medicină Dentară, şi Sackler School of Medicine afliată la Universitatea Tel Aviv, Hasharon Hospital, Centrul Medical Rabin din Israel.
The journal „Medical Connections / Conexiuni Medicale” has a national and international visibility by the publication of it’s electronic version on the website www.conexiunimedicale.ro (ISSN e-serials 2068–8369), and due to the fact that the journal is included in an exchange program between national and international universities such as Titu Maiorescu University, Bucharest, Faculty of Medicine ans Dental Medicine, and Hasharon Hospital, Rabin Medical Center Affiliated with the Sackler School of Medicine, Tel Aviv University. The “Medical Connections / Conexiuni Medicale” is indexed in Journals Master List of Index Copernicus®, isues since 2009.

Preliminary Study About The Complications Which Can Appear In Restoring An Edentulous Space With Fixed Prosthesis 43
Abstract
The partial edentation is one of the most frequent encountered oral pathologies, its restoration being usualy made with integral/partial physiognomical fixed prosthesis.
The incorrect execution or choice of the dental materials to be used for the manufacturing of the restoration, lead to the occurrence of multiple effects: the feeling of discomfort, the mobility of the fixed prosthesis, loosening of the prosthesis, periodontal decompensation, cavities and pulp complications of the abutment teeth, gum retractions and alveolar resorbtions because of the overload of the abutment teeth, perforation of aggregation elements, fracture of the fixed prosthesis mediators, fracture or detachment of the facets, lack of functionality of the prosthesis, gum inflammations, gum coloration, metallic taste.
We studied in a group of 169 patients the negative effects produced by inserting in the mouth of conjunct prosthetic restorations made or adjusted incorrectly.
Treatment success rate in the studied group of patients was 76.92%. 39 cases were considered failures by complications that endanger long-term prognosis of restorations. The frequency of complications, in descending order, was: development of dental caries (20.51%), fracture of esthetic components (19.44%), fracture of metal components (15.38%), gingival and alveolar resorptions (15.38%), gum stains (12.82%), loss of physiognomic appearance (10.25%), gingival bleeding and suppuration (7.69%).
Keywords: partial edentation, fixed prosthesis, iatrogenic, dental materials
Introduction
The partial edentation represents the absence of one to fifteen dento-periodontal units from a dental arch. Through the loss of the dento-periodontal units, on the dental arch will appear discontinuities, named edentulous spaces [1].
The untreated partial edentation determines the development of a subjective and objective symptomatology
ORIgInAL ARTIcLEs
pReliMinARY studY About tHe coMplicAtions WHicH cAn AppeAR in RestoRinG An edentulous spAce WitH FiXed pRostHesis
Hancu Violeta, Comăneanu Raluca Monica, Barbu Horia Mihail, Rădulescu Diana Eugenia, Filipescu Alina Gabriela, Ghergic Doina Lucia
Titu Maiorescu University of Bucharest, Faculty of Dental Medicine
Address for correspondence:Dr. Hancu Violeta Str. Reconstrucţiei, nr.10, bl.29, sc.4, et.1, ap.138, sect.3, 031725, Bucureşti Email: [email protected] This work was cofinanced from the European Social Fund through Sectorial Operational Programme Human Resources Development 2007-2013, project number POSDRU/ CPP107/DMI 1.5/S/77082, “Doctoral Scholarships for eco-economy and bio-economic complex training to ensure the food and feed safety and security of anthropogenic ecosystems”. Received: 27.01.2012 Accepted: 10.09.2012 Med Con October 2012 Vol 7, No 3, 43-47

ORIgInAL ARTIcLEs
Hancu et al44
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
that progressively worsens, as complications appear locally, regionally and at distance. The symptomatology of the partial edentation has a great impact on the essential orofacial functions, such as chewing, phonetics and the physiognomical appearance by losing the vertical dimension of occlusion and the occurrence of dental migration.
The restoration of the reduced partial edentation and the compensation of the affected functions are performed by using fixed prostheses.
Prognosis of fixed prosthetic restorations (RPF) is extremely difficult to assess [1-13], because in the integration of RPF is there a wide range of factors [14].
The incorrect execution or the improper choice of the dental materials used in order to manufacture the restorations, leads to the occurrence of multiple undesired effects such as: the feeling of discomfort, the mobility of the fixed prosthesis, loosening of the prosthesis, periodontal decompensation, cavities and pulp complications of the abutment teeth, gum retractions and alveolar resorbtions because of the overload of the abutment teeth, perforation of aggregation elements, fracture of the fixed prosthesis mediators, fracture or detachment of the facets, lack of functionality of the prosthesis, gum inflammations, gum coloration, metallic taste.
The aim of our study is to analyze the negative effects on 169 patients, generated by the insertion in the oral cavity of prosthetic restorations manufactured or adjusted incorrectly.
Methods
The study was made on 203 patients, whose partial edentations have been restored at least 5 years, patients who addressed theirselves to a number of five different dental offices in Bucharest, in the period of October 2010-January 2012 for various dental reasons. From the study, there has been excluded a number of 34 patients, who had extended partial edentations, restored with removable prosthesis, that means that in the end, just 169 patients were part of the study, patients whose partial edentations were restored worth fixed prosthesis.
Cases in which RPF had at five years functionally, biological and aesthetic integrate appropriate were considered successful and cases where complications endanger long-term prognosis of the restorations were considered failures.
After some authors [4-10] are mainly nine possible causes of failure of the RPF: development of cavities in the abutments which can not be treated without removal of the RPF, need for endodontic treatment at the abutment teeth which can not be performed properly without ablation of RPF, aesthetic deficiencies due
gingival or gum pigmentation, gingival inflammation, periodontal reasons (mobility/loss of bone support on abutment teeth), tooth fracture, broken bridge, fracture of physiognomic material, abrasion on antagonists tooth.
The patients were classified according to age, gender, the location of the edentation, its etiology and type of the complication that led to failure of the prosthetic treatment.
Results
The studied group of patients was made of 54 male patients and 115 female patients. Dividing the patients according to the group of age they belong to, we obtained: 5 male patients and 9 female patients (ages 41-50), 19 male patients and 42 female patients (ages 51-60), 22 male patients and 49 female patients (ages 61-70), 8 male patients and 15 female patients (ages 71-80) (Table I).
Regarding the location of the partial edentation, we observed the existence of 105 edentations at the maxillary level and 64 edentations at the madibular level. The female patients presented a number of 70 maxillary edentations and 45 mandibular edentations, whereas the male patients presented 35 maxillary edentation and 19 mandibular edentation (Table II).
The etiology of the teeth loss was in 78 of the cases the dental caries and its complications, in 60 of the cases the periodontitis and in 31 of the cases iatrogenies (Table III).
The success rate of the treatment on the studied patients was 76, 92%. Thereby, from the 169 cases, 39 patients presented the following complications: the
Table I. The distribution of the patients according to age and gender
PatientsGroups of age
Total41-50 years
51-60 years
61-70 years
71-80 years
Male 5 19 22 8 54Female 9 42 49 15 115Total 14 61 71 23 169
Table II. The classification of the patients according to the location of the edentation
PatientsThe location of the edentation Total
Maxillary Mandible
Male 35 19 54Female 70 45 115Total 105 64 169

ORIgInAL ARTIcLEs
Preliminary Study About The Complications Which Can Appear In Restoring An Edentulous Space With Fixed Prosthesis 45
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
Table III. The edentulous etiology of the studied patients group
The complicated dental caries Periodontitis Iatrogenies
Number of cases 78 60 31
Table IV. Types of found complications
Types of complications found Number of cases
fracture of the physiognomic component 7fracture of the metallic component 6loss of the physiognomic aspect 4gum bleeding and suppurations 3gum coloration 5gum retractions and alveolar resorptions 6evolution of carious processes at the dental abutments level 8
Total 39
Figure 4. The fracture of the physiognomic component, at a metal-ceramic restoration,
due to occlusal factors
Figure 5. The fracture of the physiognomic component, at a metal-ceramic restoration,
due to a design error (the manufacturing of a total prosthesis for the mandible)
Figure 6. The fracture of the metallic component due to an incorrect hardware technique, food retentions due to the incorrect conformation of
the apertures, gum inflammations because of the acrylic component, the loss of physiognomical aspect through visibility of the metal, through
acrylic transparency and due to impregnation of the materials with alimentary dyes
Figure 7. At maxillary level: the fracture of the metallic component due to the incorrect hardware
technique, gingival bleeding due to the inflammation produced by the acrylic component,
alimentary retentions due to the incorrect adjustment of the apertures and the loss of the
physiognomical aspect through the coloration of the acrylate produced by nicotine; At mandibular level: the fracture of the physiognomic component due to
the inefficient retention and gum retraction through the improper outline of the aggregation elements
Figure 8. The fracture of the metallic component due to an incorrect hardware technique
Figure 9. The fracture of the metallic component due the overload produced by the excessive length of
the edentulous space and the fracture of the physiognomic component at the incised level
through insufficient retention and occlusal overload
fracture of the physiognomic component, the fracture of the metallic component, the loss of the physiognomic aspect, gum bleeding and suppurations, gum coloration, gum retractions and alveolar resorptions, the evolution of carious processes at the dental abutments level (Table IV, Figures 4-17).

ORIgInAL ARTIcLEs
Hancu et al46
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
Figure 10. Gum coloration: metal-acrylic restoration (left) and metal-ceramic restoration (right)
Figure 11. Gum suppurations and bleedings: metal-acrylic restoration (left) and metal-ceramic restoration (right)
Figure 12. The fracture of the blunt teeth due to the evolution of carious processes (too large
microprostheses)
Figure 13. Carious process at the level of the blunt teeth (too short microprosthesis)
Figure 14. Gum retractions due to the overload of the abutment teeth
Figure 15. Gum retractions and alveolar resorbtions due to the ruquest of the abutment teeth
Figure 16. Fistula-gangrene complication at the blunt tooth level
Figure 17. Irritating spine at gum level – too large microprosthesis
Discussion
The feeling of discomfort is a common incident observed after the fixation of the prosthetic restorations and may be caused by: the presence of premature contacts or occlusal interferences, the insertion of the prosthesis in an inadequate position, a oversized or reduced occlusal surface [9,10], overpressure on the dento-periodontal support units [4,5], too close contacts with the adjacent teeth, the insufficient protection of
the gum tissues or the accumulation of alimentary debris within the prosthesis, due to its inadequate design [12].
The mobility of the fixed prostheses may occur in case of aggregation elements deformation, dysfunctional occlusal contacts, incorrect cementation, cement solubilisation, carious processes occurring at the abutment teeth (because of poor hygiene, incorrect adjustment of the aperture, too large or too short aggregation elements), the mobility of one or more

ORIgInAL ARTIcLEs
Preliminary Study About The Complications Which Can Appear In Restoring An Edentulous Space With Fixed Prosthesis 47
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
abutment teeth through periodontal decompensation [4,5], the lack of retention of the aggregation elements through incorrect preparations.
The gingival retractions and the alveolar resorbtions may be determined by: overuse of the abutment teeth through the excessive lenght of the spaces, the inadequate conformation of the gum apertures, the improper outline of the aggregation elements [8], the choice of an insufficient number of abutment teeth.
The metallic skeleton of the intermediate teeth can be fractured due to the incorrect technique of hardware and the manipulation of the alloy or through overload of the fixed partial prosthesis due to a very extended space [4].
The physiognomic component fracture of the fixed partial prostheses may occur due to an inefficient retention, occlusal factors or design errors (the manufacturing of total prostheses for the mandible, without regarding its mobility) [6,7].
Conclusions
The studied group consisted mostly of female pacients belongig to the age group 61-70 years.
The location of the edentation was in 62,13% of the cases at the maxillary level. Regarding the etiology of the edentation, in 46% of the cases it has been produced as a result of the caries process evolution, in 36% of the cases because of periodontitis and in 18% of the cases due to iatrogenies.
Treatment success rate in the studied group of patients was 76.92%. 39 cases were considered failures by complications that endanger long-term prognosis of restorations. The frequency of complications, in descending order, was: development of dental caries (20.51%), fracture of esthetic components (19.44%), fracture of metal components (15.38%), gingival and alveolar resorptions (15.38%), gum stains (12.82%), loss of physiognomic appearance (10.25%), gingival bleeding and suppuration (7.69%).
References
1. Bratu D, Nussbaum R. Bazele clinice şi tehnice ale protezării fixe. Ed. Signata, Timişoara, 2001 p 69-108,503-601,1153-246.
2. Shigli K, Hebbal M, Angadi GS. Self-reported assessment of intraoral prostheses among patients attending the prosthodontic department in a dental institute in India. Geriatr Gerontol Int, 2008; 8(2):101-8.
3. Güngör MA, Artunç C, Dündar M. Seven-year clinical follow-up study of Probond ceramic crowns. Quintessence Int, 2007;38(8):456-63.
4. Hirotomi T, Yoshihara A, Ogawa H, et al. Tooth-related risk factors for periodontal disease în community-dwelling elderly people. J Clin Periodontol, 2010;37(6):494-500.
5. Hermann P, Gera I, Borbély J, et al. Periodontal health of an adult population in Hungary: findings of a national survey. J Clin Periodontol, 2009;36(6):449-57.
6. Creugers NH, Kayser AF, van‘t Hof MA. A meta-analysis of durability data on conventional fixed bridges. Community Dent Oral Epidemiol, 1994;22(6):448-52.
7. Goodacre CJ, Bernal G, Rungcharassaeng K, et al. Clinical complications in fixed prosthodontics. J Prost Dent, 2003;90(1):31-41
8. Foster LV. The relationship between failure and design in conventional bridgework from general dental practice. J Oral Rehabil, 1991;18(6):491-95.
9. Napankangas R, Salonen-Kemppi MA, Raustia AM. Longevity of fixed metal ceramic bridge prostheses: a clinical follow-up study. J Oral Rehabil, 2002;29(2):140-5.
10. Lindquist E, Karlsson S. Success rate and failures for fixed partial dentures after 20 years of service: Part I. Int J Prosthodont, 1998;11(2):133-8.
11. Hammerle CH, Ungerer MC, Fantoni PC, et al. Long-term analysis of biologic and technical aspects of fixed partial dentures with cantilevers. Int J Prosthodont, 2000;13(5):409-15.
12. Palotie U, Vehkalahti M. Finnish dentists’ perceptions of the longevity of direct dental restorations. Acta Odont Scand, 2009;67(1):44-9
13. Romanian National Institute of Statistics (2010). Household Income and Expenditure – Q1 2010 [Online]. 2010 Aug 3 [cited 2010 Nov 21] [http://www.seenews.com/news/latestnews /romaniannational instituteofstatistics–householdincomeandexpedi ture-q1-142602/]
14. Moga I, Chifor R, Badea ME, Popa S. Factori implicaţi în eşecurile protezelor parţiale fixe. Clujul Medical, 2011;84(4),603-7.

www.colmedsm.ro
Colegiul MedicilorSatu Mare
Colegiul Medicilor Satu Mare este o persoană juridică autonomă, neguvernamentală, apolitică şi fără scop patrimonial. Este într-o largă accepţiune o organizaţie profesională liberală şi reuneşte peste 626 de medici.
Colegiul Medicilor Satu Mare crede că poate reuşi urmând trei principii: să vorbească doar când are ceva important de spus, să nu critice până când nu are soluţii şi să nu propună decât soluţii rezultate din sfatul colectiv. Forţa Colegiului Medicilor constă în prezentarea în faţa societăţii ca o voce autentică, permanent validată, a tuturor membrilor săi.
Satu Mare College of Physicians is an autonomous legal entity, non-governamental, apolitical and non-profit. In a widley acception it is a liberal professional organization and brings together over 626 doctors.
Satu Mare College of Physicians believes it can succeed by following three principles: to speak only when he has something important to say, to make no critics until he has solutions and to propose only solutions resulted from a of collective advice. The force of Physicians College consist in showing in front of the society an authentic voice, always validated, from all its members.
Eroilor Revoluţiei Pl. no.23, 440055 Satu Mare, Romania.Tel./Fax: +40-261-710456, +40-361-408164, e-mail: [email protected]

May Influence The Epidural Anesthesia The Newborn Hearing Screening? 49
Abstract
Objectives: The main purpose was to determine if the epidural anesthesia has any influence on the results of the screening of the newborns whose birth was by caesarean section on request and if the time of the testing influences the results of the screening.
Materials and methods: 50 newborn babies are taking in the study, 25 born by Cesarean section under epidural anesthesia, 25 born by natural delivery; they are tested at three different times using transient otoacoustic emissions (TEOAE) and automated auditory brainstem response (AABR).
Results: The screening performed in the first four hours of the birth had false positive results, compared with the testing performed after 24 hours. They obtained an index increased of suspicion-statistically significant (p < 0, 05)-in the terms of the influence of the epidural anesthesia on the automatic response of the auditory brainstem (AABR) when the test is performed at less than four hours after birth. Conclusions: The obtained results have importance for the planning of the auditory
screening, especially when it wants the universal testing of the hearing to the newborn.
Keywords: newborn hearing screening, transient otoacoustic emissions (TEOAE), automated auditory brainstem response (AABR), epidural anesthesia
Introduction
Because the hearing deficiency cannot be identified immediately by routine clinical examinations such as observing the behavior [1], they required the application of the objective electro-physiological measurements, transient otoacoustic emissions (TEOAE) and automated auditory brainstem response (AABR), characteristic to the universal screening of the newborn and infant [2,3]. It is aimed at getting the hearing screening results for each newborn, at any time before the external of the hospital [4]. The early identification and intervention therapy before the age of 6 months of the hearing deficiency can prevent severe psychosocial repercussions, educational and linguistic. Therefore, it is vital to isolate and classify the factors that can influence
ORIgInAL ARTIcLEs
MAY inFluence tHe epiduRAl AnestHesiA tHe neWboRn HeARinG scReeninG?
Domuţa Maria1,2, Pascalau Nicoleta1, Cotulbea Stan2
1Faculty of Medicine and Pharmacy, Oradea, România, 2University of Medicine and Pharmacy “Victor Babeş” Timişoara, România
Address for correspondence:Dr. Maria Domuţa Faculty of Medicine and Pharmacy Oradea Piaţa 1 Decembrie 10, 410073 Oradea, România Phone: +40744 779 199 E-mail: [email protected] Received: 01.09.2012 Accepted: 01.10.2012 Med Con October 2012, Vol 7, No 3, 49-52

ORIgInAL ARTIcLEs
Domuţa et al50
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
the success or failure of the program screening of newborn hearing evaluation, such as the epidural anesthesia for the caesarean section birth by request.
The rate of prevalence of hearing loss reported to the worldwide is growing [5], 1-4 of 1000 newborns are born with hearing loss, this being one of the most common congenital anomalies [6]. The current literature suggests that globally about 6 out of 1000 infants present the permanent hearing loss at birth or in the neonatal period [7]. In the consent, the screening application for hearing loss is required to all newborns and a clear understanding of the influence that certain elements postnatal (such as the epidural anesthesia) may have on the implementation of it. It is possible that the epidural anesthesia can depress the functioning of the auditory system and therefore the integrity of the hearing screening, thus causing false positive results [8]. Hence, is the need to determine the auditory results at the newborns of the mothers that practiced the epidural anesthesia for cesarean section by request. The epidural anesthesia is a procedure that involves the injecting of the anesthetic outside the dura mater of the spinal cord and these results in an automatic and partial blockade of the central nervous system. This is often used for the cesarean section by request [9]. It has the advantage of allowing the mother to remain awake, diminishes the risk of aspiration and reduces the effects of the maternal drugs used on the newborns [10]. The long-term effects of the epidural anesthesia, which are rare and minimal, have been well documented [11]; however, it is not well established if the epidural anesthesia affects the auditory system of the newborn.
Based on these data, the goal of this prospective study is to determine if the epidural anesthesia has an influence on the results of the newborns screening whose birth was by caesarean on request.
They have sought to achieve the following objectives: determining the results of the hearing screening at newborn group whose mothers gave birth through cesarean under epidural anesthesia (Group A); comparison of the results of the hearing screening of the Group A with those of the new-born of mothers who have had a natural delivery, without epidural anesthesia (Group B); establish if the time of hearing screening aid has any effect on the screening results.
Materials and Method
This prospective study was presented in the Clinic of Neonatology of the County Clinical Hospital of Emergency Oradea, Stationary III in the period 2009-2010 on a number of 50 newborns at term, between 38 and 42 weeks of gestation. They were divided into two
groups: Group A – 25 newborns whose mothers gave birth by caesarean operation on demand with epidural anesthesia and the B Group – 25 newborns of mothers who have had a natural delivery, without epidural anesthesia.
The criteria of inclusion in the study for the sample of patients were:
– newborns at term, between 38 and 42 weeks of gestation
– normal pregnancy– lack of maternal risk factors (miscarriage) and
fetal (pathology that might require hospitalization on the neonatal intensive care unit, craniofacial abnormalities, intrauterine infections, family history of hearing loss)
– cesarean with epidural anesthesia or normal natural delivery
– lack of the epidural anesthesia during the natural delivery
The device used for testing the hearing was an Echo-Screen type ES/TA produced by Fisher Zoth-Mack Medizintechnick Germany. All newborns were tested using screening methods like transient otoacoustic emissions (TEOAE), reflecting the mechanical activity of the ciliates external cells that produce vibrations transmitted through endocochleare liquids on retrograde way to the external conductive ear, followed by automated auditory brain stem response (AABR).They have thus evaluated the integrity and function of the cochlear cranial nerves (NW VIII) and auditory pathway in the brainstem, at three time intervals: less than 4 hours, between 4 and 6 hours and after 24 hours after birth. They performed the testing in complete silence when the newborn infant was resting or immediately after feeding (no sedation). For both methods of testing, the results were recorded as PASS or REFER to each participant at each testing session.
All information was stored and processed using the program Microsoft® Excel® 2010 (Microsoft® Corporation, USA), being the database of statistical study. As methods of statistical analysis, they have used the Fisher’s exact test, using the medical statistics program MedCalc® version 12.2.1.0 (MedCalc® Software, Mariakerke, Belgium).
Results
The results of the newborn hearing screening participants in the study are included in the Table I. They indicate that a large majority (92%) of the newborns have obtained REFER to the first two sessions TEOAE for the lot A, while 40% have obtained REFER to the first session AABR.

ORIgInAL ARTIcLEs
May Influence The Epidural Anesthesia The Newborn Hearing Screening? 51
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
The session 1 results, although according to some previous reports relating to the epidural anesthesia that is causing delays in the response AABR, must be interpreted with caution due to the vernix in the external conductive ear of the newborn, which can have an influence on the result AABR. The presence of vernix had a similar influence on the AABR also in the Group B. However, there is a statistically significant difference between the two groups (REFER 40% Group A versus 8% of Group B, p=0.018077) which confirms that the epidural anesthesia has had an effect on the results of screening through auditory brain stem response (AABR) in newborns.
Discussions
It is noted a significant improvement in the PASS results of AABR screening at the sessions 2 and 3, indicating that the effects of the anesthesia would be stopped. Moreover, examining the effects of the lidocaine hydrochloride on the auditory brain stem response of the newborn, Diaz and al. [17] they found a significant delay in the central neural component at 90 dB for the experimental group, compared to the control group.
In another study conducted by Bozynski and col. [18] they noted the change of the auditory brain stem response evoked to the newly born test in less than four hours, in comparison with the results at 48 hours or more after the epidural anesthesia with lidocaine; these changes correlate with the concentration in the blood of the lidocaine.
Not the same thing we can say for the screening results through TEOAE, which seem to remain quite high in the sessions 1 and 2 for the both groups, but without statistically significant differences. Significant changes occur in the session 3. The false positive results are obtained when a condition is not present, but the test results indicate that it is present. Owen and al. [14] note
the large number of false positive results obtained when the transient otoacoustic emissions (TEOAE) are made in the first 24 hours after birth. The REFER rates for TEOAE are reported between 5-20% when they are performed earlier than 24 hours after birth and less than 3% when they are carried out in 24-48 hours after birth [15]. The researches conducted by Levi and al. [16] indicate that the TEOAE can be achieved earlier than 48 hours from birth, while the Pennsylvania Health Care Cost Containment Counsel [17] suggests that the TEOAE made after 48 hours are much more reliable. The false positive results may be due to the presence of the vernix in the external conductive ear [18]. The TEOAE findings confirm the documented proves that the screening by otoacoustic emissions (TEOAE) is more reliable at 24 hours after birth, due to the presence of the vernix.
Analyzing Table I we can notice that the TEOAE screening can be maintained positive in the first two sessions (<4 hours, at 4-6 hours) for both groups, probably due to the presence of the vernix in the external conductive ear, this changing only when it was achieved after 24 hours (at discharge). The AABR screening can be maintained positive when it is achieved in the first four hours after birth, with significant differences between the two groups of infants (REFER 40% Group A versus 8% of Group B, p=0,018077) and changes in the next two sessions for all newborns.
In conclusion, although the effective use of TEOAE and AABR as screening measures was well established, it is important to establish the factors that can influence the reliability of these measures. In the current study, the epidural anesthesia seems to have had an influence on the increase of the false positive results when the testing was achieved earlier than four hours after birth.
From the results obtained, they can conclude that the test through TEOAE earlier than four hours after birth, as
Table 1. Results of the hearing screening for the two groups of newborns
Sessions of screening for TEOAE and AABR
Group A (newborns by cesarean with epidural
anesthesia)n=25
Group B (newborns by natural delivery without
epidural anesthesia)n=25
p†
(PASS)p†
(REFER)
Session 1 TEOAESession 1 AABRSession 2 TEOAESession 2 AABRSession 3 TEOAESession 3 AABR
PASS2 (8%)
15 (60%)2 (8%)100%100%100%
REFER23 (92%)10 (40%)23 (92%)
0%0%0%
PASS5 (20%)23 (92%)5 (20%)100%100%100%
REFER20 (80%)2 (8%)
20 (80%)0%0%0%
p=0,417427*p=0,018077*p=0,417427*
p=0.417427*p=0.018077*p=0.417427*
*Fisher’s exact test†p<0,05 proves a statistically significant difference between two groups studied

ORIgInAL ARTIcLEs
Domuţa et al52
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
well as between four and six hours after birth is unfavorable due to the presence of the vernix in the external conductive ear such moments. This finding is confirmed by Korres and al. [19] and the Pennsylvania Health Care Cost Containment Counsel [17], whereby the TEOAE are screening tools viable between 24 and 48 hours after birth, because at that time the external conductive ear would be free of vernix. The index of suspicion regarding the influence of the epidural anesthesia was high.
The conclusions of the present study have significant implications for the implementation of the program of universal screening of the newborn for the hearing deficiency.
The AABR screening is reliable if it is carried out at four hours after birth of the newborns whose birth was achieved under epidural anesthesia. The calendar of the hearing universal screening especially at the children born with epidural anesthesia is important because the use of the epidural anesthesia may lead to the increase of the false positive results, which may lead to the maternal undue anxiety.
The use of TEOAE appears to be significantly influenced by vernix in the first hours after birth, stressing the need to ensure that the fluids from the external conductive ear are actively removed before using the TEOAE and can be implemented as a condition of screening before 24 hours.
References
1. Arehart KH, Yoshinaga-Itano C, Thompson V, Gabbard SA, Brown AS. State the states: The status of universal newborn hearing screening, assessment, and intervention systems in 16 states. Am J Audiol 1998;7:1-14.
2. American Academy of Pediatrics, Joint Committee on Infant Hearing. Year 2007 Position statement: Principles and guidelines for early hearing detection and intervention programs. Pediatrics 2007;120:898-921.
3. HPCSA. Early hearing detection and intervention programmes in South Africa, Position Statement Year (2007). Available from: http://www.hpsca.co.za/hpcsa/default.aspx?id=137 [Last accessed on 2009 Feb 07].
4. Widen J, Bull RW, Folsom RC. Newborn hearing screening: What it means for providers of early intervention services. Infants Young Child 2003;16:249.
5. Swanepoel DC, Delport SD, Swart JG. Universal newborn hearing screening in South Africa. S A Med J 2004;94:634.
6. Pripic I, Mahujla-Stamenkovic V, Bilic I, Haller H. Hearing loss assessed by universal newborn hearing
screening-The new approach. Int J Pediatr Otorhinolaryngol 2007;71:1757-61.
7. Olusanya BO, Newton VE. Global burden of childhood hearing impairment and disease control priorities in developing countries. Lancet 2007;369:1314-7.
8. Gurian EA, Kinnamon DD, Henry JJ, Waisbren SE. Expanded newborn screening for biochemical disorders: The effect of a false-positive result. Pediatrics 2006;117:1915-21.
9. Marquette GP, Mechas T, Charest J. Epidural anesthesia for elective Cesarean section does not influence fetal umbilical artery blood flow indices. Can J Anaesth 1994;41:1053-6.
10. Morrow RJ, Rolbin SH, Ritchie JW, Haley S. Epidural anesthesia and the blood flow velocity in mother and fetus. Can J Anaesth 1989;36:519-22.
11. Marquette GP, Mechas T, Charest J. Epidural anesthesia for elective Cesarean section does not influence fetal umbilical artery blood flow indices. Can J Anaesth 1994;41:1053-6.
12. Diaz M, Graff M, Hiatt M, Friedman S, Ostfeld B, Hegyi T. Prenatal lidocaine and the auditory evoked responses in term infants. Am J Dis Child 1988;142:160-1.
13. Marquette GP, Mechas T, Charest J. Epidural anesthesia for elective Cesarean section does not influence fetal umbilical artery blood flow indices. Can J Anaesth 1994;41:1053-6.
14. Owen M, Webb M, Evans K. Community based universal neonatal hearing screening by health visitors using otoacoustic emissions. Arch Dis Child 2001;84:157-62.
15. Erenberg A, Lemons J, Sia C, Trunkel D, Ziring P. Task Force on Newborn and Infant Hearing. Newborn and Infant Hearing Loss: Detection and Intervention. Pediatrics 1999;103:527-30.
16. Levi H, Adelman C, Geal-Dor M, Elidan J, Eliashar R, Sichel J, et al. Transient evoked otoacoustic emissions in newborns in the first 48 hours after birth. Audiology 1997;36:181-6.
17. Pennsylvania Health Care Cost Containment Council. Review of Senate Bill 938. 2005. Available from: http://www.phc4.org/reports/mandates/SB938/review.htm [Last accessed on 2007 Jun 11].
18. Watkin PM, Baldwin M, Dixon R, Beckman A. Maternal anxiety and attitudes of universal neonatal hearing screening. Br J Audiol 1998;32:27-37.
19. Korres S, Nikolopoulos T, Ferekidis E, Gotzamanoglou Z, Georgiou A, Balatsouras DG. Otoacoustic emissions in universal hearing screening: Which day after birth should we examine the newborns. ORL J Otorhinolaryngol Relat Spec 2003;65:199-201.

New Therapeutic And Etiologic Perspectives In Recurrent Miscarriage 53
Abstract
Habitual abortion affects around 1% to 3% of the fertile couples and represents a very actual problem which has no clear etiopathogenetic mechanism elucidated yet. Uterine anomalies, genetic, endocrine and immunologic factors along with thrombophilia are known to be involved in the etiopathogenesis of the recurrent pregnancy loss cases. Recently there were taken into account also the roles of the glycoproteins and some nuclear hormone receptors as possible causes of this pathology. In the present study we focus on the last trends and studies regarding the etiopathogenesis and treatment of the recurrent pregnancy loss.
Keywords: habitual abortion, recurrent niscarriage, genetic factors, uterine anomalies, thrombophilia, antiphospholipidic antibodies
Declaration of interest: The authors are declining any conflict of interest.
Introduction
The habitual abortion (HA) is defined as the emergence of a number of at least three consecutive spontaneous abortions and is affecting approximately 1%-3% of the couples [1,2]. The primary HA includes patients with consecutive spontaneous abortions
without births in antecedents, and the secondary HA is represented by the recurrent spontaneous abortions occurring after the birth of a viable fetus. There is a series of known factors involved in the etiology of the HA such as: chromosomal abnormalities, endocrine disorders, uterus abnormalities, immunological diseases or trombophilia. However, in over 50% of the cases the etiology is unknown and nowadays there are several studies regarding the involvement of some factors such as the nuclear hormonal receptors or the leptin glycol-protein glycodeline [3].
Genetic CausesThe genetic causes of the HA are involved in a variable
percentage of the disease occurrence, respectively 25-47% of the total cases with HA [4,5]. The etiology of the genetic factors is asserted by the high rate of chromosomal abnormalities revealed by the genetic diagnosis of the pre-implant of the in-vitro fertilization (IVF) for the couples with HA as compared to those without recurrent HA (70.7% versus 45.1%; p<0.0001) [6].
Among the genetic factors we can mention the shortening of the ovocytes telomere induced by the oxidative stress, a phenomena characteristic to advanced maternal age [7]. This anomaly explains the increased incidence of the spontaneous abortion, both of the sporadic one as well as of the recurrent one in women over 35 years old [8].
gEnERAL REVIEW
neW tHeRApeutic And etioloGic peRspectiVes in RecuRRent MiscARRiAGe
Grigore Mihaela¹, Mareş Alina²
¹Gr.T.Popa University of Medicine and Pharmacy Iaşi, ²Medis Medical Center Iaşi
Address for correspondence:Dr. Mihaela Grigore Str. Bălţi 7C, Iaşi, România tel: 0744438024 E-mail:[email protected] Received: 20.06.2012 Accepted: 10.08.2012 Med Con October 2012, Vol 7, No 3, 53-57

gEnERAL REVIEW
Grigore et al 54
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
The studies have shown an increased incidence (3.6%) of the equilibrated translocations to the couples with HA [9]. The couples presenting this type of translocations have a rate of spontaneous abortion of up to 29%, and for 36% of the aborted conceptive products there was evidenced a non-equilibrated translocation [10]. All these observations sustain the need to carry out a high resolution parental caryotype to the couples with antecedents of premature spontaneous abortion with unexplained causes. It is also recommended to the couples with equilibrated translocations and AD antecedents to make within FIV the genetic diagnosis pre-implanting [11].
Together with the translocations, in the etiology of the spontaneous abortion are involved some genetic abnormalities, especially connected to the X chromosome or mutations of the germinal line. The progresses registered in the analysis of the genomic sequence allow nowadays the division of the pre-implanting screening tests in order to discover a singular genetic cause.
Due to the decrease of folic acid plasma levels in the patients with abnormal caryotype of the conception products, the administration of the high dose folic acid is recommended during the peri-conception period [12]. A second therapeutic strategy proposed for the patients with HA as a result of the advanced maternal age is in vitro fertilization (IVF). Pre-implanting genetic diagnosis is required. The purpose of the genetic pre-implanting diagnosis is to exclude the trisomy 21, which frequently observed in woman pregnancies over 35 years old [13,14].
Uterus AbnormalitiesThe relations between HA and the uterus
abnormalities (septate uterus, bicornuate uterus, uterus didelphys) are well known. Recent studies have shown the mechanisms through which the uterus abnormalities can induce spontaneous abortion: the decrease of the vascularization at the level of the uterine septum, increased local inflammatory status, and reduced hormone receptors [15]. The standard treatment for the uterine septum is represented by the hysteroscopic resection. The submucous myomas that are determining a distortion of the uterine cavity can cause HA as well as the decrease of the IVF success. In these cases the hysteroscopic resection can improve the fertility as well as the birth rate [16,17]. Asherman syndrome and the uterine polyps were confirmed as being direct factors for HA, and some studies have suggested the improvement of the pregnancy evolution after the hysteroscopic resection [18]. Thus, the patients with HA must undergo sonohysterographic investigation in order to
diagnose the uterine defects. Together with the standard endovaginal ultrasound scan, another very useful investigation is the 3D ultrasound which allows establishing a correct diagnosis for the pathology of the uterine cavity as well as for the uterine abnormalities [19,20].
Endocrine DiseasesThe untreated diabetes is a well-known cause of
spontaneous abortion. In the subclinical forms of diabetes there is no clear relationship with spontaneous abortion [21]. As for thyroid dysfunction, female patients with HA present more often anti-peroxidase and anti-thyroid globulin antibodies [22]. Non-randomized studies have underlined the fact that the therapy with levotiroxyne can reduce the rate of HA in those female patients with anti-thyroidian antibodies [22].
The syndrome of polycystic ovaries is an endocrine disorder frequently encountered, associated with higher incidence of spontaneous abortion. Correct diagnoses as well as an adequate management are necessary to all patients presenting with polycystic ovaries.
Another endocrine disorder with a role in the emergence of HA is hyperprolactinemia, and the treatment with bromocriptine proved to be very efficient in decreasing the incidence of HA [23]. Thus, it is very useful to determinate the prolactin level of the couples presenting HA and to make all the necessary corrections when the level is high.
The Infectious DiseasesWhile the severe acute infections of bacterial,
parasite or viral nature can determine a sporadic spontaneous abortion, there are no clear data regarding the relationship between chronic bacterial infections and HA. Although for a long time there were speculations about the connections between HA and the infections with Cytomegalovirus, Adenovirus, Chlamydia trachomatis or Mycoplasma hominis, there is no clear evidence of this relationship [24,25]. Moreover, although the bacterial vaginosis was associated with HA, if seems to be connected more to the second trimester abortion than to the first trimester one [26,27].
Congenital TrombophiliaThe studies of the last years have demonstrated a
correlation between the congenital trombophilia and the spontaneous abortion during the first semester of pregnancy and more often, of the second semester of pregnancy. The congenital trombophilia is determined by the mutation of the V factor and by the prothrombin gene; the deficiency of the S or C protein is associated with a high rate of spontaneous abortion or with the

gEnERAL REVIEW
New Therapeutic And Etiologic Perspectives In Recurrent Miscarriage 55
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
obstetrical complications of the preeclampsia or stillbirth. The meta-analysis of 31 studies has reported a connection between the V Leiden factor and recurrent abortion in the first semester of pregnancy, and especially in the second semester [28]. A second meta-analysis on the relationship between the V Leiden factor and the pregnancy complications showed no connection between the factor and the pregnancy losses in the first semester of pregnancy, but proved a real link for the second or third semesters [28]. The recommended treatment to patients with congenital trombophilia and with a history of HA is heparin with low molecular weight or acetylsalicylic acid [30]. Moreover, the obstetricians must be warned upon the risk of developing thromboembolia in these patients during delivery.
Immunological CausesThe syndrome of the antiphospholipide antibodies
is defined as a combination of profound or arterial venous thromboses in their post history, specific obstetrical complications or thrombocytopenia associated with the presence of antiphospholipide antibodies (AAF) [31]. The last criteria includes: high concentration of IgG or IgM anticardiolipine antibodies, increased concentration of IgG or IgM anti-β2-glycoprotein I antibodies or the presence of lupus anticoagulant. The AAF must be identified at least two times within a period of at least 12 weeks. The obstetrical complications include at least one abortion at over 10 weeks of gestation and at least one premature birth before 35 weeks or 3 consecutive spontaneous abortions before 10 weeks of gestation. AAF can be identified through the screening of the antibodies connected directly on the protein epitrophy (β2-glycoprotein-I, prothrombin, V anexine), through indirect determination of the antibodies directed through the proteins of the phospholipids’ matrix (cardiolipins and phosphatidylserine) or through the evaluation of the effects of AAF upon the coagulation or activation in vitro of the prothrombin (lupus anticoagulant) [32].
It was proven that 5-15% of the women with HA have AAF compared to a percentage of 2-5% of the general obstetrical population [33]. These antibodies are closely connected to the fetal losses rather than the embryonic losses [34]. The treatment for the patients with AAF includes heparin with small molecular weight and small doses of acetylsalicylic acid.
In order to explain the role of immunological factors in the spontaneous abortion, a series of studies have suggested the presence of a relation between the high levels of the circulate NK cells and AD. The main theory is the one according to which the excessive activity of the decidual NK cells can affect the
implantation of the blastocysts on the initial placenta determining the abortion. Yamada and his colleagues have shown that a periconceptional high level of activity of the NK cells in the peripheral blood and the percentage of circulating NK cells can signal the ulterior loss of a normal caryotype pregnancy in the female patients with HA [35]. The abnormal interaction between the decidual NK cells and the trofoblast antigens can activate this cytotoxic capacity, determining placenta abnormalities. The decidual NK cells of the placental bed express immunoglobulin-like receptors for NK cells which can be connected to the HLA-C molecules from the trofoblastic cells, a process which normally is initiating the production of angiogenic and growing factors by the NK cells which sustain the trofoblastic invasion. On the contrary, the presence of the haplotypes KIR AA on the decidual NK cells, especially of the KIR activator for the groups HLA-C2 (KIR2DS1), connected to HLA-C2 at the level of the trofoblast, can determine the occurrence of preeclampsia and of HA [36]. For the moment there are no evidences supporting the determination of the circular NK cells at patients with HA or of the therapy of those presenting a high activity of the NK cells.
Celiac DiseaseCeliac disease (sprue) is an immunological disease
characterized by mal-absorption and atrophy of the intestinal villy, modifications that can be avoided through gluten exclusion from food. Some studies have shown the correlation between celiac disease and recurrent abortion. Kotze has reported a bigger prevalence of HA in 76 adult female patients with celiac disease versus an 84 female patients of the control group presenting with the irritable colon syndrome (24.4% versus 11.6%) [37]. He also noticed that the pregnancy prognosis improved for those 12 female patients with celiac disease after treatment, with a decrease of HA from 38.9% up to 5.6% (p=0.045). Similar observations were made by other authors [38]. Thus, the symptomatic celiac disease can be associated with HA and its treatment can reduce the incidence of AD [39].
Discussion
Given the high frequency of genetic causes in the etiopathogenesis of HA, the first recommendation in the evaluation of the couples presenting HA is to make a caryotype of the parents as well as a caryotype analysis of the aborted fetus. The investigation of the placental pathology, in order to discover inclusions of the trofoblast can be very useful when there was no caryotype analysis of the aborted fetus and when there

gEnERAL REVIEW
Grigore et al 56
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
are occurring intermittent euploid abortions at the same gestation age. In the near future, the genomic sequence of the abortions will be an option and would certainly identify X-linked, autosomal recessive and germinal line mutations. The treatment for the female patients with aneuploid spontaneous abortions must include the nutritional supplements with folic acid.
A standard method of approach will remain the investigation of the female patients for uterine abnormalities using sonohysterography and 3D ultrasound. Of course, during prenatal examination the discovered abnormalities should be treated accordingly. In order to exclude some endocrine causes it is recommended to test the level of prolactin, of TSH and of anti-thyroid antibodies. Eventually, the investigations for trombophilia and AAP must be carried for HA with undefined causes, and their presence will need a treatment with heparin low molecular weight and small doses of aspirin.
Conclusions
The HA is affecting 1%-3% of the couples and represents a real problem with multiple unknown elements regarding the etiopathogenic mechanisms. The uterine abnormalities, the genetic, endocrine, immunological factors, and thrombophilia, represent well known factors, which are involved in the etiopathology of recurrent abortions. Presently there are discussions regarding the involvement of the glycoproteins and of some nuclear hormonal receptors in the etiopathology of this disease. The therapeutic strategy included treatment with heparin low molecular weight or with aspirin, although only a small number of results have proven it’s’ efficiency. The HA is an important issue for the health system, reason for which it is imperative to continue the researches in order to clarify the etiology and to improve the conduct.
References
1. Carrington B, Scacks G, Regan L. Recurrent miscarriage: pathophysiology and outcome. Curr Opin Obstet Gynecol 2005;17:591-7.
2. Regan L. Recurrent miscarriage. Br Med J 1991;302:543-4.
3. Toth B, Jeschke U, Rogenhofer N, et al. Recurrent miscarriage: current concepts in diagnosis and treatment. J Reprod Immunol 2010;85:25-32.
4. Nybo Andersen AM, Wohlfahrt J, Christens P, Olsen J, Melbye M. Maternal age and fetal loss: population
based register linkage study. Br Med J 2000;320:1708-12.
5. Stern JJ, Dorfmann AD, Gutierrez-Najar AJ, Cerrillo M, Coulam CB. Frequency of abnormal karyotypes among abortuses from women with and without a history of recurrent spontaneous abortion. Fertil Steril 1996;65:250-3.
6. Rubio C, Simon C, Vidal F, et al. Chromosomal abnormalities and embryo development in recurrent miscarriage couples. Hum Reprod 2003;18:182-8.
7. Keefe DL, Marquard K, Liu L. The telomere theory of reproductive senescence in women. Curr Opin Obstet Gynecol 2006;18:280-5.
8. Habayeb OM, Konje JC. The one-stop recurrent miscarriage clinic: an evaluation of its effectiveness and outcome. Hum Reprod 2004;19:2952-8.
9. Fryns JP, Van Buggenhout G. Structural chromosome rearrangements in couples with recurrent fetal wastage. Eur J Obstet Gynecol Reprod Biol 1998;81;171-6.
10. Stephenson MD, Sierra S. Reproductive outcomes in recurrent pregnancy loss associated with a parental carrier of a structural chromosome rearrangement. Hum Reprod 2006;21:1076-82.
11. Fischer J, Colls P, Escudero T, Munné S. Preimplantation genetic diagnosis (PGD) improves pregnancy outcome for translocation carriers with a history of recurrent losses. Fertil Steril 2010;94(1):283-9.
12. George L, Mills JL, Johansson AL, et al. Plasma folate levels and risk of spontaneous abortion. JAMA 2002;288:1867-73.
13. Hardarson T, Hanson C, Lundin K, et al. Preimplantation genetic screening in women of advanced maternal age caused a decrease in clinical pregnancy rate: a randomized controlled trial. Hum Reprod 2008;23(12):2806-12.
14. Mastenbroek S, Twisk M, van Echten-Arends J, et al. In vitro fertilization with preimplantation genetic screening. N Engl J Med 2007;357:9-17
15. Devi Wold AS, Pham N, Arici A. Anatomic factors in recurrent pregnancy loss. Semin Reprod Med 2006;24:25-32.
16. Fernandez H, Sefrioui O, Virelizier C, Gervaise A, Gomel V, Frydman R. Hysteroscopic resection of submucosal myomas in patients with infertility. Hum Reprod 2001;6:1489-92.
17. Bajeckal N, Li TC. Fibroids, infertility and pregnancy wastage. Hum Reprod 2000;6:614-20.
18. Sanders B. Uterine factors and infertility. J Reprod Med 2006;51:169-76.
19. Grigore M, Cojocaru C, Mares A, Indrei A. Mullerian duct anomalies: clinical issues and 3D ultrasound diagnosis. Gineco.ro 2009;5:100-6.

gEnERAL REVIEW
New Therapeutic And Etiologic Perspectives In Recurrent Miscarriage 57
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
20. Grigore M, Mares A. Applications of 3D-ultrasound in female infertility. Rev Med Chir Soc Med Natur 2009;113(4):1113-9.
21. Mills JL, Simpson JL, Driscoll SG, et al. Incidence of spontaneous abortion among normal women and insulin-dependent diabetic women whose pregnancies were identified within 21 days of conception. N Engl J Med 1988;319:1617-23.
22. Stagnaro-Green A, Glinoer D. Thyroid autoimmunity and the risk of miscarriage. Best Pract Res Clin Endocrinol Metab 2004;18(2):167-81.
23. Hirahara F, Andoh N, Sawai K, Hirabuki T, Uemura T, Minaguchi H. Hyperprolactinemic recurrent mis-carriage and results of randomized bromocriptine treatment trials. Fertil Steril 1998;70(2):246-52.
24. Matovina M, Husnjak K, Milutin N, Ciglar S, Grce M. Possible role of bacterial and viral infections in miscarriages. Fertil Steril 2004;81(3):662-9.
25. Sugiura-Ogasawara M, Ozaki Y, Nakanishi T, Kumamoto Y, Suzumori K. Pregnancy outcome in recurrent aborters is not influenced by Chlamydia IgA and/or G. Am J Reprod Immunol 2005;53:50-3.
26. Ralph SG, Rutherford AJ, Wilson JD. Influence of bacterial vaginosis on conception and miscarriage in the first trimester: cohort study. Br Med J 1999;319:220-3.
27. Oakeshott P, Hay P, Hay S, Steinke F, Rink E, Kerry S. Association between bacterial vaginosis or chlamydial infection and miscarriage before 16 weeks’ gestation: prospective community based cohort study. BMJ 2002;325:1334.
28. Rey E, Kahn SR, David M, Shrier I. Thrombophilic disorders and fetal loss: a meta-analysis. Lancet 2003;361:901-8.
29. Dudding TE, Attia J. The association between adverse pregnancy outcomes and maternal factor V Leiden genotype: a meta-analysis. Thromb Haemost 2004;91:700-11.
30. Ghosh K, Shetty S, Vora S, Salvi V. Successful pregnancy outcomein women with bad obstetric history and recurrent fetal loss due to thrombophilia: effect of
unfractionated heparin and low-molecular wight heparin. Clin Appl ThrombHemost 2008;14:174-9.
31. Miyakis S, Lockshin MD, Atsumi T, et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost 2006;4:295-306.
32. Galli M, Luciani D, Bertolini G, Barbui T. Anti-beta 2-glycoprotein I, antiprothrombin antibodies, and the risk of thrombosis in the antiphospholipid syndrome. Blood 2003;102:2717-23.
33. Branch DW, Gibson M, Silver RM. Clinical practice. Recurrent miscarriage. N Engl J Med 2010;363:1740-7.
34. Rai RS, Clifford K, Cohen H, Regan L. High prospective fetal loss rate in untreated pregnancies of women with recurrent miscarriage and antiphospholipid antibodies. Hum Reprod 1995;10:3301-4.
35. Yamada H, Morikawa M, Kato EH, Shimada S, Kobashi G, Minakami H. Pre-conceptional natural killer cell activity and percentage as predictors of biochemical pregnancy and spontaneous abortion with normal chromosome karyotype. Am J Reprod Immunol 2003;50:351-4.
36. Hiby SE, Walker JJ, O’Shaughnessy KM, et al. Combinations of maternal KIR and fetal HLA-C genes influence the risk of preeclampsia and reproductive success. J Exp Med 2004; 200:957-65.
37. Kotze LM. Gynecologic and obstetric findings related to nutritional status and adherence to a gluten-free diet in Brazilian patients with celiac disease. J Clin Gastroenterol 2004;38(7):567-74.
38. Tata LJ, Card TR, Logan RF, Hubbard RB, Smith CJ, West J. Fertility and pregnancy-related events in women with celiac disease: a population-based cohort study. Gastroenterology 2005;128(4):849-55.
39. Tursi A,Giorgetii G, Brandimarte G, Elisei W. Effect of gluten-free diet on pregnancy outcome in celiac disease patients with recurrent miscarriages. Dig DisSci 2008;53:2925-2928.

Calcified uterine myoma (CT)
Aladdin and the magic lamp
Hydronephrosis (US)
The angry kidney!

Diagnosis Of A Digital Nodule By Fine Needle Aspiration Cytology 59
Abstract
84 year old male with a painless nodule of the 5th digit, left hand, underwent fine needle aspiration cytology (FNAC) of the lesion. Cytologic examination revealed typical birefringent urate crystals diagnostic of gouty tophus. Patient’s serum uric acid was found to be 10mg/dl (normal 3.5-7.2 mg/dl) confirming the diagnosis of gout. FNAC is an easy and minimally invasive procedure for the diagnosis of gouty tophus.
Keywords: gout, fine needle aspiration
Introduction
Gout is a mostly hereditary metabolic disease. The disease is promoted by a purine-rich diet and shows an intermittent course of inflammatory joint manifestations and periods free of symptoms. The pathognomonic sign of the disease is an acute and very painful monarthritis with typical local deposits of uric acid, so-called gouty tophi [1].
We report a rare case in which the diagnosis of gout was made cytologically and was then confirmed by conventional methods of investigation.
Case Report84 year old male presented to the Orthopedic hand
clinic with a 1.5 cm diameter painless nodule of the left hand, 5th digit, distal interphalangeal joint (Fig. 1).
On examination the nodule was not tender but there was a limitation of the distal-interphalangeal joint flexion. Radiograph showed severe destruction of the distal interphalangeal joint (Fig. 2 and 3).
The differential diagnosis included metastasis, primary tumor and gout, although previous history did not reveal any episodic bouts of arthritis. Because the
diAGnosis oF A diGitAl nodule bY Fine needle AspiRAtion cYtoloGY
Halpern Marisa1, Vigler Mordechai2, Rath-Wolfson Lea1, Schwartz Ariel1, Koren Rumelia1, Gal Rivka1
Departments of 1Pathology and 2Orthopedic Surgery, Hasharon Hospital, Rabin Medical Centre, Petah Tikva, affiliated to Sackler Faculty of Medicine, Tel-Aviv University, Israel
Address for correspondence:Prof. Gal Rivka Department of Pathology, Hasharon Hospital, POB 101, Petah-Tikva, Israel. Tel: 972-3-9372390, Fax: 972-3-9372349 E-mail: [email protected] Received: 09.03.2012 Accepted: 10.05.2012 Med Con October 2012, Vol 7, No 3, 59-62
cAsE PREsEnTATIOn
Figure 1. Clinical picture of left hand, 5th digit

Halpern et al60
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012cAsE PREsEnTATIOn
were made in the lesion by the aspirator before the needle was withdrawn. The procedure was repeated twice to ensure that adequate material was obtained for diagnosis. White material was obtained from aspiration and expelled onto glass slides. It was smeared with another slide, fixed with cytospray and stained by hematoxylin and eosin (H&E).
Light microscopy of the slides showed eosinophilic slender needle shaped crystals with pointed ends distributed singly or in groups (Figure 4). They showed strong birefringence under polarized light consistent with monosodium urate crystals (Figure 5).
On further examination the patient’s serum uric acid was 10mg/dl (normal 3.5-7.2 mg/dl) and the diagnosis of gout was confirmed. At two weeks follow up examination, there were no signs of hemorrhage or inflammation of the finger.
Discussion
Gout is a common disease associated with monosodium urate (MSU) crystal deposition in articular or peri-articular tissues and in the urinary tract.
Figure 2. Lateral X-ray of 5th digit – extensive lytic lesion with severe erosion and destruction of
the distal interphalangeal joint
Figure 3. AP X-ray of 5th digit, also depicting the severe destruction of the distal interphalangeal
joint
Figure 4. Hematoxylin & Eosin showing needle shaped crystals
Figure 5. Polarizing microscopy showing birefringence of slender needle shaped crystals
patient was under Coumadin treatment for arrhythmia following cardiac surgery he was sent for FNAC instead of surgical biopsy.
A 23-gauge needle and syringe were placed in a holder for aspiration of palpable lesions. After the needle was placed inside the lesion, negative pressure was applied to the needle with the syringe. Several excursions

Diagnosis Of A Digital Nodule By Fine Needle Aspiration Cytology 61
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012 cAsE PREsEnTATIOn
Generally it progresses through four clinical stages if left untreated: asymptomatic hyperuricemia, acute gout, intercritical or interval gout and chronic tophaceous gout. Although gouty tophi are seen in chronic disease, tophi may be the first sign of the disorder [2].
The diagnosis of gout can be problematic when the presentation is atypical and serum uric acid is borderline value. Occasionally, gout may present as a soft tissue tophus without antecedent painful arthritis or hyperuricemia. Differential diagnosis of articular nodules includes giant cell tumor of tendon sheath, giant cell tumor of bone and metastatic tumor [3]. Demonstration of monosodium urate crystals in FNAC smears from nodular masses establishes the diagnosis of gout unequivocally [4].
The advantages of FNAC over open biopsy and other surgical procedures have made FNAC an increasingly popular procedure. In our case, although the patient was under coumadin treatment, there were no adverse reactions after the FNAC.
Birefringent crystals may be found in gouty tophus (monosodium urate) and in deposits of pseudo gout (Calcium pyrophosphate). Careful examination of the
crystals will reveal distinct differences between the two processes; gout crystals are needle shaped with pointed ends while calcium pyrophosphate crystals are shorter, rhomboid and have blunted or squared ends. Also, gouty crystals are strongly (negatively) birefringent while pseudo gout crystals display weak (positive) birefringence on polarization [3].
Another advantage of FNAC over excision biopsy is that urate crystals are often lost during histological processing because they dissolve in formalin, but they are preserved in FNAC smears that are alcohol fixed.
Agarwal et al. [5] reviewed the literature (2007) and found six published reports of gouty tophi diagnosed by FNAC. These included 17 cases with the clinical diagnosis of: gouty arthritis (5 cases), giant cell tumor (5 cases), metastatic tumor (2 cases), sarcoma (2 cases) arthritis (1 case) and in 2 cases the diagnosis was not given. The uric acid level was high in 5 cases, normal in 7 and low in 2 cases [4,6,7,8,9,10].
Since then another few cases were reported, [11,12,13,14] arriving at a total of 23 cases, Table I.
FNAC is currently replacing other investigations due to its quick, less invasive, simpler and cost effective
Table I. Summary of published reports of gout diagnosed by FNAC
Author Year No. ofcases Anatomic Site Clinical diagnosis
Gal et al 2012 1 5th digit, left hand Metastasis? Gout?Koley et al. [2] 2010 1 bilateral feet and toes, left palm, right elbow, helix of left ear ArthritisGupta et al. [13] 2009 1 left elbow joint and near the lateral malleolus of the left foot Not givenAngeles et al. [12] 2008 1 No data No dataPurohit et al. [11] 2006 1 nodules over extremities Benign neoplastic lesionBhadani et al. [4] 2006 7 Dorsum foot& arm Gout
Hand & foot Gout2nd toe, Rt foot GoutHands & feet Metastatic tumorsLittle finger (Lt) GCTOlecranon (Rt) GCT1st toe (Rt) GCT
Sah et al. [6] 2 Forearms, hands, dorsum feet, lateral malleoli Metastatic tumorsPalmar aspect over base of little finger GCT
Paik et al. [7] 2002 1 Hands, feet, ear helix Rheumatoid arthritis Rege et al. [8] 2000 2 Nodules on B\L malleoli Arthritis
Nodules on dorsum foot, sole, lateral malleolus Gout?Nicol et al. [9] 1997 3 Dorsal ulnar, Rt distal forearm Sarcoma
I & III Metacarpal joints GoutRt foot & ankle Sarcoma
Liu et al. [14] 1996 1 right distal ulnar mass GCTNasser et al. [10] 1994 2 Vertebral level C3 L4 Not given
Forearm nodule Not givenGCT=Giant cell tumor

Halpern et al62
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012cAsE PREsEnTATIOn
technique. The crystal demonstration in FNAC smears is superior to histopathology sections where crystals are more commonly lost during processing. In joint fluid analysis coincident crystals like hydroxyapatite, steroid etc in the joint fluid may cause confusion [8].
Conclusion
FNAC is an easy, minimally invasive and cost effective procedure for diagnosing gouty tophus. It is accurate and should be used before surgical biopsy.
References
1. Ott I, Gartenschläger M, Schmeck S, Baier G. Atypical gout tophi for differential diagnosis of head and neck tumors: case report and review of the literature. HNO 2009;57(12):1280-4.
2. Koley S, Salodkar A, Choudhary S, Bhake A, Singhania K, Choudhury M. Tophi as first manifestation of gout. Indian J Dermatol Venereol Leprol 2010;76(4):393-6.
3. Dodd LG, Major NM. Fine-needle aspiration cytology of articular and periarticular lesions. Cancer 2002;96(3):157-65.
4. Bhadani PP, Sah SP, Sen R, Singh RK. Diagnostic value of fine needle aspiration cytology in gouty tophi: a report of 7 cases. Acta Cytol 2006;50(1):101-4.
5. Agarwal K, Pahuja S, Agarwal C, Harbhanjanka A. Fine needle aspiration cytology of Gouty Tophi with review of literature. J Cytol 2007;24:142-5.
6. Sah SP, Rani S, Mahto R. Fine needle aspiration of gouty tophi: a report of two cases. Acta Cytol 2002;46:784-5.
7. Paik SS, Park MH. Fine needle aspiration cytology of gouty tophus in a patient with rheumatoid arthritis. Acta Cytol 2002;46:1024-5.
8. Rege J, Shet T, Naik L. Fine needle aspiration of tophi for crystal identification in problematic cases of gout. A report of two cases. Acta Cytol 2000;44:433-6.
9. Nicol KK, Ward WG, Pike EJ, Geisinger KR, Capperllari JO, Scott EK. Fine needle aspiration biopsy of gouty tophi; lessons in cost effective patient management. Diagn Cytopathol 1997;17:30-5.
10. Nasser IA, Fayyad LM, Soudi NM, Bardawil RG. Fine needle aspiration cytology in the diagnosis of gouty tophi: the role of Diff-Quick stain in the evaluation of unexpected lesions. Acta Cytol 1994;38:840.
11. Purohit MB, Purohit TM, Tandon RK. FNAC of gouty tophi – a case report. Microbiol 2006;49(1):42-3.
12. Angeles RM, Gong Y. Fine needle aspiration of a subcutaneous gouty tophus. Diagn Cytopathol 2008;36(7):494-5.
13. Gupta A, Rai S, Sinha R, Achar C. Tophi as an initial manifestation of gout. J Cytol 2009;26(4):165-6.
14. Liu K, Moffatt EJ, Hudson ER, Layfield LJ. Gouty tophus presenting as a soft-tissue mass diagnosed by fine-needle aspiration: a case report. Diagn Cytopathol 1996;15(3):246-9.

Nephrogenic Adenoma, Report Of Two Cases And Review Of The Literature 63
Abstract
Nephrogenic adenoma (NA) is an uncommon benign lesion of the urothelial tract, characterized by a proliferation of tubules, cysts, and papillae lined by cells with low cuboidal to columnar epithelium. NA can be a significant diagnostic pitfall as certain histologic features, such as the presence of enlarged nuclei with prominent nucleoli, degenerative nuclear atypia, tiny tubules simulating signet ring cells, and focal invasion into superficial muscle, when taken out of context can mimic malignancy. Here we report two cases of NA, a male and a female with some worrisome histologic features and review the diagnostic criteria as well as pertinent morphologic malignant mimics of NA.
Keywords: Nephrogenic adenoma, urinary bladder, Cytokeratin-7, Cytokeratin-20, P504S
Introduction
Nephrogenic adenomas (NA) are benign tumor-like lesions of the urothelium. It is a rare lesion of the urinary tract widely considered to be a metaplastic response to urothelial injury [1]. It shows proliferation of glands that can occur at several sites within the
urogenital tract. Although it is benign, the histopathological appearance may sometimes be mistaken for a malignancy, particularly in biopsies around the prostatic urethra. NA is an infrequent lesion of the urinary tract, associated with a previous history of trauma or irritation of the urothelium. Predisposing factors include infections, calculi, surgery, trauma and kidney transplantation [2].
The diagnostic features that are useful in the recognition of this entity are the characteristic mixture of various architectural patterns, associated stromal edema and inflammation, hyaline sheath around tubules, eosinophilic colloid like secretion within tubules, and lack of mitotic activity [3]. Histologically they consists of tubules, cords, individual cells and/or signet ring cells within the urothelium, which can extend into the muscular wall and mimic adenocarcinoma [4]. NA may show papillae as well as a focal solid growth pattern; however, conspicuous diffuse solid growth pattern is extremely uncommon. The cells lining tubules, cysts, and papillae are cuboidal to low columnar with scant pale cytoplasm. Occasional clear cells can be seen especially in the solid areas. Although enlarged nuclei and prominent nucleoli may be observed in some cases, significant nuclear atypia, including
nepHRoGenic AdenoMA, RepoRt oF tWo cAses And ReVieW oF tHe liteRAtuRe
Rath-Wolfson Lea1,2, Schwartz Ariel1,2, Leikin Anna1,2, Koren Rumelia1,2, Gal Rivka1,2
Department of 1Pathology Hasharon Hospital, Rabin Medical Centre Petah Tikva, affiliated to 2Sackler Faculty of Medicine, Tel-Aviv University, Israel
Address for correspondence:Rath- Wolfson Lea, MD Department of Pathology, Hasharon Hospital, Rabin Medical Center, Petah Tikva, Israel Fax: 972-3-9372349 E-mail: [email protected] Received: 11.01.2012 Accepted: 01.02.2012 Med Con October 2012, Vol 7, No 3, 63-67
cAsE PREsEnTATIOn

Rath-Wolfson et al64
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012cAsE PREsEnTATIOn
presence of mitosis, is extremely rare. Nuclear atypia, when present, appears degenerative with indistinct, smudgy chromatin [3, 5]. Many normal structures and pathologic lesions in the genitourinary system can resemble neoplastic processes histologically. Although some, such as NA, can be seen in different locations, most are identified in particular organs and, as such, have unique differential diagnostic considerations specific to that organ [6].
We report two cases of NA and review the literature, focusing on the pathological differential diagnosis and immunohistochemical studies.
Case reports
Case 1A 61 years old male was admitted to the Urology
Department for re-evaluation of bladder tumor. He was suffering from high grade transitional cell carcinoma stage T1 since 2003 and passed several courses of intravesical treatment with BCG following transurethral resection of bladder tumor (TURBT). No lesions were seen on cystoscopy. Random biopsies were taken. On microscopic examination in the lamina propria of the
urinary bladder mucosa there was a focus of small tubules and glands, lined by cuboidal cells (Fig. 1).
The cells did not show any significant atypia, mitoses were not found. The tubules and glands were accompanied by chronic inflammatory infiltrate. Immunohistochemical stains for Pan Cytokeratin, Cytokeratin-7, EMA and P504S were positive in the small tubules. Cytokeratin-20, PSA and Prostatic Specific Acid Phosphatase (PSAP) were negative. Ki-67 was negative in the tubules and positive in some of the lymphocytes (Fig. 2). The differential diagnosis with prostatic adenocarcinoma, adenocarcinoma of the urinary bladder was taken into consideration, but they were ruled out with the help of the immunohistochemical stains, Table I.
These findings were compatible with the diagnosis of NA.
Case 2A 68 years old female, suffering from cystinuria
resulting in chronic renal failure treated on hemodialysis since 2008. In October 2006 was admitted to the urology department with complains of lower abdominal and flank pain, and hematuria. Cystoscopy was performed and revealed foci of ulcerated bladder mucosa with no space occupying lesion. Endoscopically these findings were consistent with the diagnosis of Hunner’s lesion. Hunner’s lesion is a distinctive inflammatory lesion presenting a characteristic deep rupture through the mucosa and submucosa provoked by bladder distension. Biopsies were taken from the ulcerated areas. On microscopic examination, infiltration of tubules lined by epithelial clear cells was seen in the lamina propria, (Fig. 3).
Immunohistochemical stain for Cytokeratin 7 was positive while Cytokeratin 20 was negative. Ki-67 was positive in only in the lymphocytes. These findings were suspicious for Clear Cell Carcinoma but not diagnostic. Other areas showed heavy infiltration of lymphocytes, plasma cells and histiocytes which were stained with CD68 immunostain. She was treated for interstitial cystitis with DMSO that was interrupted because of
Figure 1. Tubular structures are seen on the right side with prominent inflammatory infiltrate on the
left side. H&E x20 (Sunt observate structuri tubulare în partea dreaptă, cu infiltrat proeminent
inflamator în partea stângă. H&E x20)
Table I. The different immunohistochemical stains
Markers Nephrogenic adenoma
Urinary bladder adenocarcinoma
Renal cell carcinoma
Prostate adenocarcinoma
CK 7 + + - -EMA + +/- +/- +/-P504S + - - +CK20 - + - -PSAP - - - +Ki67 - ++ ++ ++

Nephrogenic Adenoma, Report Of Two Cases And Review Of The Literature 65
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012 cAsE PREsEnTATIOn
Figure 2. Immunohistochemical Findings: A. Positive Pan Keratin stain in the small tubules. x20. B. Positive keratin 7 stain in the tubular structures. X20. C. EMA positive stain in the tubules. X20. D. P504S positive stain in the tumoral tubules. X10. E. Very few Ki-67 positive cells, mostly in lymphocytes. F. Keratin 20 showed diffuse negative expression. X20 (Constatări imunohistochimice: A. Colorare pozitivă la Pan Keratină în tubii mici. x20. B. Colorare pozitivă la 7 keratină în structurile tubulare. x20. C. Colorare pozitivă la EMA la nivelul tubilor. x20. D. Colorare pozitivă la P504S în tubii tumorali. x10. E. Foarte puţine celule pozitive Ki-67, în special în limfocite. F. Keratina 20 a arătat expresie negativă difuză. x20)
A. Pan keratin x20 D. P504S x10
B. Keratin 7 x20 E. Ki-67
C. EMA x20 F. Keratin 20 x20
severe irritative changes. On January 2010, six months after the treatment, while she was asymptomatic, a control cystoscopy was performed. A small lesion measuring 2-3mm found at posterior wall of the bladder was biopsied.
On microscopic examination the lesion was composed of small tubules and glands located in the lamina propria near an area of chronic inflammatory infiltrate. Neither atypia nor mitotic figures were seen. Immunohistochemical staining for Cytokeratin-7 and

Rath-Wolfson et al66
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012cAsE PREsEnTATIOn
P504S were positive, Cytokeratin-20 was negative. Ki-67 was positive in only few cells (Table I). These findings were compatible with the diagnosis of NA.
Discussion
The urinary bladder is the most common location for NA, usually the posterior wall. Occasionally it can be found in the renal pelvis, urether, or urethra. It is found in young adults with a male predominance (2:1). About half of the cases are found after genitourinary surgery, including renal transplantation. NA is also associated with calculi, trauma, and cystitis. Usually the lesions are asymptomatic, although patients frequently present with hematuria or dysuria. It may present as a papillary or polyploidy exophytic mass or velvety lesion, which resembles cystoscopically, neoplasia. Sessile forms make up about 25% to 30% of cases. Papillary structures usually measure less than 1 cm, may rarely measure more than 5 cm.
Classic histologic pattern is that of small tubules resembling renal tubules. The tubules are lined by hobnail cells resembling endothelial-lined vascular spaces and are often surrounded by a layer of hyalinized basement membrane.
NA can resemble adenocarcinoma of the urinary bladder or of the prostate and also some urachal benign or malignant tumors [6]. The absence of epithelial stratification and the characteristic eosinophilic, cuboidal, low columnar, or hobnail cells should alert the pathologist to the correct diagnosis.
Immunohistochemical stains for EMA, cytokeratin-7, P504S and PAX-2 are positive. Ki-67 is positive in only few cells. Cytokeratin-20, PSA and Prostatic Specific Acid Phosphatase (PSAP) are negative.
P504S is also positive in NA and in prostatic carcinoma therefore it cannot differentiate between those two lesions [7], but it is negative in clear cell carcinoma of the bladder. PSA is usually positive in prostatic carcinoma and negative in NA, which is frequently negative for basal cell markers and PSAP as well. The characteristic histomorphologic and immunohistochemical features, possibly supplemented by positive PAX2 and/or PAX8 immunostains, which can be used to arrive at the correct diagnosis [8,9].
Careful examination of the H&E stained slides which do not show dysplasia together with PSA and PSAP negativity can exclude the diagnosis of prostatic carcinoma and support the diagnosis of NA [10].
Mazal et al. [11] showed that in renal transplant recipients the sex chromosome status of 46 NA was the same as that of the kidney donor. They suggested that NA is derived from tubular cells of the renal transplant and were not metaplastic proliferations of the recipient’s bladder urothelium. This was supported by the positive immunohistochemical studies for PAX-2 and other peanut agglutinin studies.
Conclusion
Nephrogenic adenoma is a benign lesion with a broad histologic spectrum. NA can sometimes cause diagnostic difficulty in some cases, as certain histologic features, when taken out of context, may simulate the appearance of prostate adenocarcinoma, nested variant of urothelial carcinoma and/or clear cell adenocarcinoma.
Immunohistochemical profile of NA includes positive staining with CK 7, P504S, and PAX-2; negative staining with p63, PSA, PSAP, high-molecular-weight cytokeratin (34βE12) and Ki-67. Whenever in doubt, theses stains should be performed in order to arrive to the correct diagnosis.
References
1. Broecker JS, Steelman CK, Broecker BH, Shehata BM. Nephrogenic Adenoma of the Bladder in a Prune Belly Syndrome Patient: Case Report and Review of the Literature. Fetal Pediatr Pathol. 2011 Aug 15.
2. Martín LL, Cardoso JV, Vivas CM, Muñoz JG, Napurí LF, Enguita CG. Prostatic nephrogenic adenoma. Case report. Arch Esp Urol. 2011;64(5):473-6.
3. Kunju LP. Nephrogenic adenoma: report of a case and review of morphologic mimics. Arch Pathol Lab Med. 2010;134(10):1455-9. 7
Figure 3. Tubular structures lined by clear epithelial cells and chronic inflammation H&E
x20 (Structuri tubulare delimitate de celule epiteliale clare şi inflamaţie cronică H&E x20)

Nephrogenic Adenoma, Report Of Two Cases And Review Of The Literature 67
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012 cAsE PREsEnTATIOn
4. Allan CH, Epstein JI. Nephrogenic adenoma of the prostatic urethra: a mimicker of prostate adenocarcinoma. Am J Surg Pathol. 2001;25(6):802-8.
5. Amin W, Parwani AV. Nephrogenic adenoma. Pathol Res Pract. 2010;206(10):659-62.
6. Hameed O, Humphrey PA. Pseudoneoplastic mimics of prostate and bladder carcinomas. Arch Pathol Lab Med. 2010;134(3):427-43.
7. Gupta A, Wang HL, Policarpio-Nicolas ML, et al. Expression of alpha-methylacyl-coenzyme A racemase in nephrogenic adenoma. Am J Surg Pathol. 2004;28(9):1224-9.
8. Tong G X, Melamed J, and Mansukhani M. PAX2: a reliable marker for nephrogenic adenoma. Mod Pathol 2006;19(3):356–363
9. Tong G X, Weeden E M, Hamele-Bena D. Expression of PAX8 in nephrogenic adenoma and clear cell adenocarcinoma of the lower urinary tract: evidence of related histogenesis? Am J Surg Pathol 2008;32 (9):1380–1387
10. Skinnider BF, Oliva E, Young RH, Amin MB. Expression of alpha-methylacyl-CoA racemase (P504S) in nephrogenic adenoma: a significant immunohistochemical pitfall compounding the differential diagnosis with prostatic adenocarcinoma. Am J Surg Pathol. 2004;28(6):701-5.
11. Mazal PR, Schaufler R, Altenhuber-Müller R, et al. Derivation of nephrogenic adenomas from renal tubular cells in kidney-transplant recipients. N Engl J Med. 2002;347(9):653-9. Erratum in: N Engl J Med 2002;347(17):1390.

Fetus in utero
Or a bodybuilder?
Cortical infarct / atrophy (brain CT)
Or passion for shopping in Italy?....

Substitution Of The Ureter With The Appendix In Malignant Melanoma Adjacent To The Ureter 69
Abstract
A 70 year old female presented with right flank pain of 1 year duration.
CT scan with contrast material showed right hydroureteronephrosis and a heterogeneous soft tissue mass impinging against the right ureter and vena cava. CT guided biopsy of the mass was consistent with malignant melanoma. No evidence of a primary tumor was found.
Chemo-immunotherapy was followed by surgical resection of the mass, the adjacent vena cava and the involved ureter. The inferior vena cava was repaired with a gortex patch and the ureteral gap was substituted with the appendix. Follow-up imaging studies showed clear passage through the reconstructed ureter.
Keywords: Hydroureteronephrosis, Malignant Melanoma, Ureteral gap, Vermiform Appendix
Introduction
Malignant melanoma of unknown origin accounts for a small percentage of all melanoma cases. Metastatic melanoma involving the ureter is extremely rare. We present a case of a woman with a retroperitoneal
melanoma involving the ureter and the surgical treatment that followed. In Israel no review of any similar case has been found.
A 70 year old woman was referred to the Emergency Room due to severe worsening of a right flank pain she was suffering from for the last year. Over the past year, she suffered of repeated episodes of right flank pain with no associated fever, urinary symptoms or other complaints. Her physical examination and blood workup were unremarkable and an abdominal ultrasound scan demonstrated severe right hydroureteronephrosis. A CT scan was obtained showing right hydronephrosis and ureteral dilatation to the level of the proximal ureter where a heterogeneous soft tissue mass was apparent encasing the right ureter as well as the Inferior Vena Cava. The mass was also impinging against the duodenum, merging with the psoas muscle. A chest CT scan was interpreted as normal. Prompted by pain and imaging findings, a percutaneous nephrostomy tube (PCN) was placed into the right kidney. Antegrade pyeloureterography was performed demonstrating extrinsic pressure on the right ureter. A CT guided biopsy from the mass was consistent with malignant melanoma. Remarkably, other 2 benign nevi were removed from her back 3 years before her
substitution oF tHe uReteR WitH tHe AppendiX in MAliGnAnt MelAnoMA AdJAcent to tHe uReteR
Goldberg Hanan, Yossepowitch Ofer, Baniel Jack
Institute of Urology, Rabin Medical Center, Petah Tikva, affiliated to Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
Address for correspondence:Hanan Goldberg MD Institute of Urology Beilinson Hospital, Petah-Tikva, Israel. Tel: 972-3-9376558, Fax: 972-72-2361346 E-mail: [email protected] Received: 04.03.2012 Accepted: 15.06.2012 Med Con October 2012, Vol 7, No 3, 69-71
cAsE PREsEnTATIOn

Goldberg et al70
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012cAsE PREsEnTATIOn
present admission. She had no history of melanoma. A thorough genital and skin assessment by a dermatologist and a gynecologist was unremarkable excluding the possibility that a primary malignant melanoma was overlooked. A PET FDG CT scan revealed abnormal uptake only in the retroperitoneal mass adjacent to the right ureter, Figure 1.
During the six subsequent months, the patient received five courses of Cisplatin, Dacarbazine and IL-2 therapy, which were generally tolerated well. After completing the systemic therapy, resection of the retroperitoneal mass was scheduled. During the procedure, a 3x4 cm mass was identified, completely encasing the inferior vena cava and a portion of the right ureter. The mass was resected to attain negative surgical margins, requiring replacement of a 10 cm vena cava segment with gortex graft. In addition, a 6 cm right proximal ureteral segment was resected along with the mass. To compensate for the gap created in the ureter, the vermiform appendix was harvested along with its subtle blood supply and mobilized to the point where an end to end anastomosis was feasible. Care was taken to ensure a tension free, wide, and watertight anastomosis over a 6 FR self retaining ureteral stent. Of note, the appendix did not show abnormal uptake on PET scan, allowing its safe use as a ureteral substitute.
The postoperative course was uneventful and the patient was discharged on postoperative day 7. Three months after the procedure, a retrograde pyeloureterography study showed clear passage of contrast material through the reconstructed ureter with no signs of obstruction (Figure 2), and the stent was removed.
Figure 1. A PET FDG CT scan revealing abnormal uptake by the retroperitoneal mass adjacent to the right ureter (O scanare PET FDG CT dezvăluie absorbţia anormală a masei retroperitoneale adiacente
ureterului drept)
Figure 2. Retrograde pyelography showing an appendix conduit in the right ureter with clear
passage of contrast material and no obstruction or leak from the anastomosis (Pielografie retrogradă
arătând un conduct apendicular în ureterul drept, cu trecerea clară a materialului de contrast, fără
obstrucţie sau pierderi prin anastomoză)

Substitution Of The Ureter With The Appendix In Malignant Melanoma Adjacent To The Ureter 71
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012 cAsE PREsEnTATIOn
Discussion
Malignant melanoma is one of the most aggressive known skin cancers. The primary risk factors include positive family history, multiple benign or atypical nevi, and history of a previous melanoma. In Western Europe, the incidence of malignant melanoma has been steadily increasing with 10–12 new cases diagnosed per 100,000 [1]. Although melanoma accounts for only 4 percent of all dermatologic cancers, it is associated with unfavorable outcome and the five year survival of patients with metastatic melanoma is 14 percent [1].
Melanocytes, which may give rise to malignant melanoma, derive from the neural crest. These cells migrate during embryological development along the midline and may be found in non cutaneous sites.
Malignant melanoma of unknown origin accounts for 5-10% of all melanoma cases [2]. However, even when melanoma is found in a retroperitoneal location, a primary cutaneous lesion is nearly always documented. Our patient did not have any skin lesion, nor did she have any relevant past history of melanoma. Malignant melanoma arising in the retroperitoneum is extremely rare, and whether this case reflects a primary malignant melanoma or retroperitoneal metastasis from an unknown origin is still an enigma.
To date, metastatic melanoma involving the ureter has been reported very rarely [3]. Common metastatic sites include the liver and cerebrum. Systemic therapeutic strategies in metastatic melanoma include interferon and interleukin-2-based immunotherapy as well as various chemotherapeutic agents. However, if feasible, the patients derive the largest clinical benefit from radical resection of the metastatic lesions [1].
Commonly, surgical repair of long diseased ureteral segment, especially the proximal segment, entails the use of ileal segment or autotransplantation. However, if feasible, interposing the appendix is technically simple and obviates the need for bowel resection. In 1912 Melnikoff was the first to report using the vermiform appendix to substitute an ureteral segment after resection [4]. Since then, others have reported using the appendix to substitute various defects involving the mid or distal ureter in adults or children. In a case report published by Thomas et al. [5] in 2004, the appendix was used as replacement for a 9 cm gap between the proximal ureter and the urinary bladder. The gap resulted from severe retroperitoneal fibrosis. Similar to our case, the appendix was isolated with its mesentery, and an end-to-end anastomosis was created between the proximal ureter and one end of the appendix. The cecal
end of the appendix was anastamosed to the bladder over an ureteral stent. In another case report, Jang et al. [6] interposed the appendix into the ureter in an isoperistaltic orientation from the renal pelvis to the proximal ureter in a patient injured in a motorcycle accident. The appendix derives its blood supply from the appendicular artery, which is a branch of the ileocolic artery. The relatively small caliber of the appendix (2 to 3 mm), which is similar to that of the ureter (2 to 10 mm), enables a secure watertight anastamosis. Moreover, its natural peristalsis and small surface area would decrease the risk of any associated electrolyte imbalance due to urine absorption. Despite its many advantages, the use of the appendix as a ureteral substitute can be limited due to caliber discrepancy, excessive mucous production or if previous appendectomy was performed [7].
Conclusions
To our knowledge this is a novel case of appendiceal substitution of the ureter in the context of malignant melanoma. Use of the appendix as a possible alternative for ureteral substitution, particularly if the mid or proximal ureter is involved, should be considered a viable option.
References
1. Miller AJ, Mihm MC Jr. Melanoma. N Engl J Med. 2006;355(1):51-65.
2. Jayashree PE, Javalgi PA, Hiremash R, Dombale VD, Kansagara MH. Retroperitoneal Malignant Melanoma – A Curiosity. Journal of Clinical and Diagnostic Research. 2011;5(2):372-373
3. Gakis G, Merseburger AS, Sotlar K, Kuczyk MA, Sievert KD, Stenzl A. Metastasis of malignant melanoma in the ureter: possible algorithms for a therapeutic approach. Int J Urol. 2009;16(4):407-9.
4. Melnikoff AE. Sur le replacement de l’uretère par anse isolée de l’intestine grêle. Rev Clin Urol. 1912;1:601.
5. Thomas A, Eng MM, Hagan C, Power RE, Little DM. Appendiceal substitution of the ureter in retroperitoneal fibrosis. J Urol. 2004;171(6 Pt 1):2378.
6. Jang TL, Matschke HM, Rubenstein JN, Gonzalez CM. Pyeloureterostomy with interposition of the appendix. J Urol. 2002;168(5):2106-7.
7. Richter F, Stock JA, Hanna MK. The appendix as right ureteral substitute in children. J Urol. 2000;163(6):1908-12.

Osteoblastic mets in pelvic bones (CT)
who’s afraid of the big white wolf?
Lumbar vertebrae , axial (CT)

A Case Of West-Nile Meningitis Treated With Tamiflu 73
Abstract
West Nile Virus is an arthropod borne virus belonging to the Flaviviridae family and can cause endemic spread infection usually in the Middle East, Africa and Asia. About 1% of the infected individuals develop central nervous system infection. We describe a patient admitted to the hospital during an outbreak of swine flu with fever and meningeal symptoms and successfully treated with TAMIFLU® (an antiviral drug for H1N1 influenza infection). However, lumbar puncture results revealed West Nile virus infection. In the absence of published data about the effect of TAMIFLU® on the West Nile virus we discussed the possible mechanism of action of TAMIFLU® in this setting.
Keywords: West Nile Virus, TAMIFLU®, Olsetamivir, infection
Introduction
West Nile virus (WNV) infection is a wide-spread endemic infection observed in the Middle East, Africa and Asia [1]. In the United States it was first discovered in the summer of 1999 in New York City. Since then, the virus has extended from north to south America, Caribbean, northward into Canada resulting in the
A cAse oF West-nile MeninGitis tReAted WitH tAMiFlu
Solun Boris, Marcoviciu Dana, Dicker Dror, Shaked Efrat
Department of Internal Medicine D, Hasharon Hospital, Rabin Medical Center, Petah Tikva, affiliated to Sackler Faculty of Medicine, Tel-Aviv University, Israel
Address for correspondence:Dr. Dana Marcoviciu, Department of Internal Medicine D, Rabin Medical Center, Hasharon Hospital 7, Keren Kayemet St., Petah Tiqva, Israel Phone: 972-3-9372429, Fax: 972-3-9372427 E-mail: [email protected] Received: 23.05.2012 Accepted: 10.09.2012 Med Con October 2012, Vol 7, No 3, 73-76
cAsE PREsEnTATIOn
largest epidemics of neuroinvasive WNV disease ever reported [2]. WNV is an arthropod-borne virus (arbovirus) belonging to the family Flaviviridae and maintained in a bird-mosquito transmission cycle [3]. Approximately 80% of WNV infections are asymptomatic. Symptomatic persons develop an acute systemic febrile illness presenting as headache, myalgia, arthralgia, rash, or gastrointestinal symptoms. About 1% of the infected individuals develop central nervous system infection, which typically expresses as encephalitis, meningitis, or acute flaccid paralysis [4]. Ninety three percent of the affected patients became ill during dry and warm weather, mainly through July to September. The incidence of severe neuroinvasive disease increases with advanced age and is highest (1.35 cases per 100,000 population) among persons aged 70 years or more [5]. Hospitalization rate and case-fatality ratio are related both to age and neuroinvasive disease [6]. Currently no available human vaccine exist and therefore mosquito protection remains the best way to avoid infection [7].
Case report
A 54 year old woman was admitted to the hospital due to fever, headache and left extremities’ weakness. Her medical history was remarkable for alcohol abuse,

Solun et al74
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012cAsE PREsEnTATIOn
hypertension and an event of intracerebral hemorrhage a year prior to admission. Following rehabilitation therapy she remained in a good performance status.
On admission she was in good mental condition and consciousness. Her temperature was 39.2oC, blood pressure 184/126 mmHg, the pulse rate 111 bpm and regular and oxygen saturation was 94%. The breath and heart sounds were normal, the abdomen was soft, without tenderness, organomegaly, or masses. Neurological examination revealed stiff neck with positive Kernig and Brudzinski signs and mild left side hemiparesis. The remainder of the physical examination was normal.
Laboratory examination showed a white-cell count of 8.480/mm3 with 80.7% neutrophils, 11.9% lymphocytes, 4.6% monocytes, eosinophils 2.1%, basophils 0.7%. The platelet count was 214.000/mm3. Serum globulin level - 3.7g/dL,serum glutamic oxaloacetic transaminase (SGOT) 76 U/L (reference range 7-31), serum glutamic pyruvic transaminase (SGPT) 74.3 U/L (4-34).
Chest X-ray examination was normal. Computed tomography of the brain revealed a number of small hypoechogenous focuses in the peripheral regions of both ventricles. Since at the time of admission there was an outbreak of cases with swine flu, the possibility that the patient had contracted the disease was considered and treatment with capsules containing 75 mg of TAMIFLU® (oseltamivir phosphate, Genentech USA, Inc) was prescribed. However, blood cultures and PCR test for pandemic influenza A (H1N1) received some days later were negative. A lumbar puncture showed: glucose 71mg/dl (blood glucose 157 mg/dl), cell count 56 cells/mm3, with lymphocytic predominance, protein 80 g/dl. Bacteriological examination of the cerebrospinal fluid showed: HSV-1 and HSV-2 negative, West Nile fever ELISA-IgM (Enzyme-Linked Immunosorbent Assay) positive, ELISA-IgG negative. There was no bacterial growth. The treatment with TAMIFLU® was continued for 5 days with significant improvement in her performance and mental status. The patient was discharged on the 7th day of hospitalization.
Discussion
West Nile virus is a single-stranded Ribonucleic Acid (RNA) virus from the family Flaviviridae. Its replication cycle includes NS3 protease, glycoprotein, NS3 helicase, NS5 methyltransferase and NS5 RNA-dependent RNA polymerase, all potential targets for antiviral therapy [8]. The virus entry into different types of cells (macrophages, monocyte and dendritic cells)
proceeds by endocytosis following interaction of E protein with cellular receptors. Consequently, genomic viral RNA moves to the endoplasmic reticulum for viral protein translation and RNA replication. Therefore, any cause for disruption of WNV protein translation and/or RNA replication will block the viral life cycle and will abort infection [9].
Although the majority of the infected individuals are asymptomatic, the virus may affect the central nervous system with symptoms ranging from headache to aseptic meningitis or meningoencephalitis. These symptoms may be occult and occasionally undistinguishable from similar manifestations caused by other viruses. The incidence of central nervous system involvement in endemic areas, including meningoencephalitis, has been observed to be one out of 150 cases with WNV infections [10]. It has been reported that WNV was one of the commonest pathogens of cases with viral meningitis surveyed during 1997 to 2008 in a Baltimore community hospital [11]. Apart from for symptomatic treatment, there is no specific therapy for WNF infections [10].
Although no human vaccine is available, to date a recombinant influenza virus expressing domain III (DIII) of the WNV, E protein has been studied as a possible WNV vaccine candidate in a mouse model [12]. The WNV DIII was cloned in the N-terminal region of the influenza virus neuraminidase destroying the functional activity of the influenza protein. It was shown that one subcutaneous immunization of the mice with the FLU-NA-DIII vaccine resulted in 100% protection against challenge [13].
Possibly positive treatment effect with TAMIFLU® based on the reports that infection with flaviviruses was associated with a decrease in spontaneous locomotors brain activity and with a significant decrease in the level of neurotransmitters, especially dopamine [14]. It was found that TAMIFLU® increased significantly the extracellular dopamine level in medial prefrontal cortex [15].
The another mechanism of TAMIFLU® was by lowering the intracellular pH. Low pH of intracellular vesicles induced irreversible modification in the replication of Influenza A H1N1 virus [16,17]. Infection of host cells by flaviviruses depended on acidic pH with optimal range between 6,3 to 6,9 [18]. We assumed that this might be the primary mechanism of inhibiting WNV replication.
It has been reported that in inflammed areas the number of different enzymes including proteases and neuraminidase increased [19]. Mady et al. [20] examined effects of neuraminidase on antibody

A Case Of West-Nile Meningitis Treated With Tamiflu 75
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012 cAsE PREsEnTATIOn
dependent enhancement (ADE) of flavivirus infection, phenomena that occurs when neutralizing antibodies form complexes with the virus. It was shown that in vivo, during WNV infection neuraminidase and other enzymes modulated the function and expression of human Fc gamma RII receptors, widely detected on monocytes, macrophages, neutrophils, platelets, eosinophils and B cells, thus played an important role in the pathogenesis and development of WNV infection [20].
TAMIFLU® serving as a competitive inhibitor of the activity of the viral neuraminidase (sialidases), found on glycoproteins on the surface of normal host cells. Inhibitors entry act by targeting viral and/or cellular components, through either the inhibition of protein-protein interactions within the viral envelope proteins or between viral proteins and host cell receptors, or through the inhibition of protein-lipid interactions. Since attachment of virus strain requires sialic acid, neuraminidase inhibitors act by targeting the cellular-receptor of sialic acid to which virus particles are attached. Without neuraminidase, infection would be limited to replicate and rarely enough to cause disease [21,22].
Today there is a long list of numerous types of neuraminidases. Since there are no data whether influenza neuraminidase has the same properties as neuraminidase or other enzymes on WNV surface we do not exclude the possible effect of TAMIFLU® on viral neuraminidase of WNV. On the other hand we are aware of the fact that conclusions based on a single patient cannot be definitive about the beneficial effect of TAMIFLU® on WNV meningoencephalitis. Further investigations in this area should be done in order to evaluate the possible effectiveness and benefit of TAMIFLU® in the setting of WNV infection.
Conclusion
West Nile virus is a mosquito-transmitted flavivirus widely distributed in Africa, the Middle East, Asia, southern Europe and was recently introduced to North America and Canada. Most human WNV infections are subclinical but patients with clinical manifestations can range in severity from uncomplicated form to fatal meningoencephalitis. The incidence of severe neuroinvasive disease and death increased with age. Currently no antiviral treatment or appropriate vaccine to cure WNV exists and only supportive care can be administered. Considering the positive experimental results of subcutaneous immunization in mice with the vaccine FLU-NA-DIII, the beneficial effect of
TAMIFLU® on WNV infection in the appropriate cases cannot be excluded. Further studies should be done to evaluate this suggestion.
References
1. Blitvich BJ. Transmission dynamics and changing epidemiology of West Nile virus. Anim Health Res Rev 2008;9(1):71-86.
2. Murray KO, Mertens E, Despres P. West Nile virus and its emergence in th United States of America. Vet Res 2010;41(6):67.
3. Hayes EB, Sejvar JJ, Zaki SR, Lanciotti RS, Bode AV, Campbell GL. Virology, pathology and clinical manifestations of West Nile virus disease. Emerg Infect Dis 2005;11(8):1174-9.
4. Petersen LR, Roehrig JT, Hughes JM. West Nile virus encephalitis. N Engl J Med 2002;347(16):1225-6.
5. Lindsey NP, Staples JE, Lehman JA, Fischer M; Centers for Disease Control and Prevention (CDC). Surveillance for human West Nile virus disease - United States, 1999-2008. MMWR Surveill Summ. 2010;59(2):1-17. Erratum in: MMWR Surveill Summ 2010;59(23):720.
6. Borchardt SM, Feist MA, Miller T, Lo TS. Epidemiology of West Nile virus in the highly epidemic state of North Dakota, 2002-2007. Public Health Rep 2010;125:246-9.
7. Rossi SL, Ross TM, Evans JD. West Nile virus. Clin Lab Med 2010;30:47-65.
8. Chappell KJ, Stoermer MJ, Fairlie DP, Young PR. West Nile Virus NS2B/NS3 protease as an antiviral target. Curr Med Chem 2008;15:2771-84.
9. Sampath A, Padmanabhan R. Molecular targets for flavivirus drug discovery. Antiviral Res 2009;81:6-15.
10. Gyure KA. West Nile virus infections. J Neuropathol Exp Neurol 2009;68:1053-60.
11. Wiberg K, Birnbaum A, Gradon J. Causes and presentation of meningitis in a Baltimore community hospital 1997-2006. South Med J 2008;101:1012-6.
12. Yamshchikov G, Borisevich V, Seregin A, Chaporgina E, Mishina M, Mishin V, Kwok CW, Yamshchikov V. An attenuated West Nile prototype virus is highly immunogenic and protects against the deadly NY99 strain: a candidate for live WN vaccine development. Virology 2004;330:304–312.
13. De Filette M, Ulbert S, Diamond M, Sanders NN. Recent progress in West Nile virus diagnosis and vaccination. Vet Res. 2012;43:16.
14. Misra UK, Kumar S, Kalita J, et al. A study of motor activity and catecholamine levels in different brain

Solun et al76
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012cAsE PREsEnTATIOn
regions following Japanese encephalitis virus infection in rats. Brain Res 2009;1292:136-47.
15. Yoshino T, Nisijima K, Shioda K, Yui K, Kato S. Oseltamivir (Tamiflu) increases dopamine levels in the rat medial prefrontal cortex. Neurosci Lett 2008;438:67-9.
16. Giocondi MC, Ronzon F, Nicolai MC, et al. Organization of Influenza A virus envelope at neutral and low pH. J Gen Virol 2010;91(Pt 2):329-38.
17. Di Trani L, Savarino A, Campitelli L, et al. Different pH requirements are associated with divergent inhibitory effects of chloroquine on human and avian influenza A viruses. Virol J 2007;4:39.
18. Moesker B, Rodenhuis-Zybert IA, Meijerhof T, Wilschut J, Smit JM. Characterization of the Functional Requirements of West Nile Virus Membrane Fusion. J Gen Virol. 2010;91(Pt 2):389-93.
19. LaMarco KL, Diven WF, Glew RH. Experimental alteration of chinchilla middle ear mucosae by bacterial neuraminidase. Ann Otol Rhinol Laryngol 1986;95(3 Pt 1):304-8.
20. Mady BJ, Kurane I, Erbe DV, Fanger MW, Ennis FA. Neuraminidase augments Fc gamma receptor II-mediated antibody-dependent enhancement of dengue virus infection. J Gen Virol 1993;74(Pt 5):839-44.
21. Khan M, Rangari NT, Kalyankar TM, Agarwal PC. Clinical Assessment and Management of Swine Influenza: A Review. International Journal of Research in Pharmaceutical and Biomedical Sciences 2011;2:52-58.
22. Teissier E, Penin F, Pécheur EI. Targeting cell entry of enveloped viruses as an antiviral strategy. Molecules 2010;16(1):221-50.

Imagine All The Pictures Living Other Lives 77
Dr. Selma Gabrieli is a diagnostic imaging specialist in the department of Imaging, Hasharon Hospital, Rabin Medical Center, Petah Tikva. Dr. Oshra Benzaquen is a resident in the same department. Between the interpretations of CT scans and X-ray images and performing ultrasound exams, they try to
spice up the routine by adding an imaginative dimension to the medical images. Lively characters emerge even from the most trivial or gloomy ones. The collection was assembled over a few years.
Photos from the pages: 58, 68, 72, 78, 84, 90, 100, 120, 126, 136, 148 are from this work.
MEDIcInE AnD ART
iMAGine All tHe pictuRes liVinG otHeR liVes
Gabrieli Selma, Benzaquen Oshra
Department of Imaging, Hasharon Hospital, Rabin Medical Center, Petah Tikva, affiliated to Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel

Odontoid process, C2 vertebrae, coronal (CT)
help, GHOST !!
Odontoid process, C2 vertebrae, axial (CT)

79
ScopeThe Medical Connections publishes papers
reporting original clinical and scientific research, which contribute to the advancement of knowledge in all field of medicine. The journal also publishes reviews, editorials and short communications on specific topics. Case reports will be accepted if of great interest and well investigated. Letters to the Editor, especially those mentioning an opinion on an article previously published, or expressing a new finding are welcome. The website address of the Medical Connections is http://www.conexiunimedicale.ro. The journal is published quarterly and papers are accepted for publication in English language. Papers from contributors living abroad and from Romanian authors should be addressed to the editorial office: dr. Bumbuluţ Călin, assitant editor in chief of Medical Connections, Eroilor Revoluţiei Pl. no.23-440055 Satu Mare, Romania. Tel./Fax: +40-261-710456, e-mail: [email protected].
Redundant or duplicate publicationWe ask you to confirm that your paper has not
been published in its current form or a substantially similar form, that it has not been accepted for publication by another journal, and that it is not under consideration by another publication.
Conflicts of interestWe ask authors to state all possible conflicts of
interest, including financial and other relationships. If you are sure that there is no conflict of interest, please state this also. The sources of funding should be acknowledged in your paper.
Permissions to reproduce previously published materialPlease send us copies of permission to reproduce
material (such as illustrations) from the copyright holder.
GuidAnce FoR AutHoRs
gUIDAncE FOR DRAWIng UP
Patient consent formsThe protection of a patient’s right to privacy is
essential. Please send copies of patient’s consent forms on which patients or other subjects of your experiments clearly grant permission for the publication of photographs or other material that might identify them. If the consent form for your research does not specifically include this, please obtain it or remove the identifying material. A statement must be included in the ‘Methods’ section of your paper.
Ethics Committee approvalYou must state clearly in your submission in the
Methods section that you conducted studies on human participants with the approval of the Hospital, or University Ethics Committee etc. Similarly, you must confirm that experiments involving animals adhered to ethical standards.
Copyright assignmentPapers are accepted for publication on the
understanding that exclusive copyright in the paper is assigned to the Publisher. Authors may use material from their paper in other works published by themselves.
SubmissionsAll manuscripts submitted to the Medical
Connections are made available for online review. The journal introduced the electronic submission of manuscripts in Word format, but also accepts manuscripts submitted as attachments to electronic mail (text, figures and tables). Do not send them in PDF format. The word count for electronic submissions is up to 3,500 words for original articles, 2,500 words for case reports, 2,000 for clinical imaging papers, 500 words for letters, and 4,500 words for review articles. Authors should NOT in addition post a hard copy submission to the editorial office, unless they are supplying artwork, letters or if

80
MEDICAL CONNECTIONS • NUMBER 2 (26) • JUNE 2012gUIDAncE FOR DRAWIng UP
les that cannot be submitted electronically, or have been instructed to do so by the editorial office. For those authors who have no option but to submit by mail please send one copy of the article, plus an electronic version on disk or CD-ROM to the Editorial Office, Conexiuni Medicale/Medical Connections, Str. Tudor Vladimirescu no.7-440037 Satu Mare, Romania. Double spacing should be used throughout the manuscript, which should include the following sections, each starting on a separate page: title page, abstract and key words, text, acknowledgements, references, individual tables and legend for figures. Pages should be numbered consecutively, beginning with the title page, and the Arabic numbers should be placed in the top right hand corner of each page.
Presentation of papersTitle pageThe title page should carry the full title of the
paper and a short title to be used as a short ‘running head’ (and which should be so identified and should comprise up to 45 characters). The first name, middle initial and last name of each author should appear. If the work is to be attributed to a department or institution, its full name should be included. Any disclaimers should appear on the title page, as should the name and address of the author responsible for correspondence concerning the manuscript and the name, address and e-mail address of the author to whom requests for reprints should be made (the author should mention if he does not want his e-mail address to be published). Finally, the title page should include the sources of any support for the work in the form of grants, equipment, drugs, or any combination of these.
AbstractsThe second page should carry a structured
abstract of no less than 200 words. Do not use abbreviations, footnotes, or references.
Background & AimsDescribe the importance of the study and the
precise research objective(s) or study question(s). MethodsMethods should include information on the
following aspects of study design when applicable: Design - describe the basic study design, e.g. randomized controlled trial, cross sectional study, cohort study, case series, survey etc; Setting - specify whether the study was conducted in a primary or tertiary care setting, in an ambulatory care clinic or
hospital, in the general community etc; Participants - indicate the number of study subjects and how they were selected, recruited, and assigned to the intervention; Intervention - report the method of administration and duration of the intervention.
ResultsProvide the main outcomes of the study, including
confidence intervals or p values.ConclusionState only conclusions that are directly supported
by the evidence and the implications of the findings. Review articles and case reports should include an unstructured summary.
KeywordsThe abstract should be followed by a list of 3–10
keywords or short phrases which will assist the cross-indexing of the article and which may be published. When possible, the terms used should be from the Medical Subject Headings 262 list of Index Medicus (http://www.nlm.nih.gov/mesh/meshhome.html).
TextFull papers of an original study may be divided
into sections headed Introduction, Methods (including ethical and statistical information), Results and Discussion (including a conclusion). This so-called “IMRAD” structure is not simply an arbitrary publication format, but rather a direct reflection of the process of scientific discovery. Long articles may require subheadings within some sections (especially the Results and Discussion sections) to clarify their content. Other types of articles, such as case reports, reviews, and editorials, are likely to require other formats. Excessive use of abbreviations is not recommended. Outline statistical methods used. Identify drugs and chemicals used by generic name (if trade-marks are mentioned, manufactured name and city should be given).
AcknowledgementsAcknowledgements should be made only to those
who have made a substantial contribution to the study. Authors are responsible for obtaining written permission from people acknowledged by name in case readers infer their endorsement of data and conclusions.
ReferencesReferences should be numbered consecutively in
the order in which they first appear in the text. They should be assigned Arabic numerals, which should be given in brackets, e.g. [12]. References should include the names of all authors when six or fewer; when

81
MEDICAL CONNECTIONS • NUMBER 2 (26) • JUNE 2012 gUIDAncE FOR DRAWIng UP
seven or more, list only the first three names and add et al. References should also include full title and source information. Journal names should be abbreviated as in Index Medicus (http://www.nlm.nih.gov/tsd/serials/terms_cond.html). No more than 90-100 references will be accepted for reviews. For Letters to the Editor, 5-6 references. Avoid or keep as low as possible the use of abstracts as references. Personal communications and unpublished work should not feature in the reference list but should appear in parentheses in the text. Unpublished work accepted for publication but not yet released should be included in the reference list with the words “in press” in parentheses beside the name of the journal concerned.
TablesEach table should be assigned a Roman numeral
(e.g. Table III) and a brief title. Explanatory matter should be placed in footnotes. Explain in footnotes all non-standard abbreviations that are used in each table. Identify statistical measures of variations, such as standard deviation and standard error of the mean. Each table should be cited in the text.
IllustrationsAll graphs, photographs (on glossy paper),
diagrams will be referred to as figures and should be numbered consecutively in the text in Arabic numerals. If a figure has been published before, the original source must be acknowledged and written permission from the copyright holder for both print and electronic formats should be submitted with the material. Figures may be reduced, cropped or deleted at the discretion of the Editor.
Legends for illustrationsCaptions should have an Arabic numeral
corresponding to the illustration to which it refers with a title above and explanatory notes below it. Internal scales should be explained and staining methods for photomicrographs should be identified.
Units of measurementMeasurements of length, height, weight, and
volume should be reported in metric units (meter, kilogram, or litre) or their decimal multiples. Temperatures should be given in degrees Celsius. Blood pressures should be given in mmHg. All hematological and clinical chemistry measurements should be reported in the metric system in terms of the International System of Units (SI).
Abbreviations and symbolsUse only standard abbreviations. Avoid
abbreviations in the title and abstract. The full term
for which an abbreviation stands should precede its first use in the text unless it is a standard unit of measurement.
ReprintsTen reprints of the published articles and two
copies of the Journal will be supplied free of charge. If required in a greater number, they will be available on payment of the necessary cost.
Editorial policyWe welcome all contributions in the field of
medicine. We invite known personalities with expertise and many published papers in a specific field to write reviews and editorials in our journal. We accept original papers and case reports from all countries. The Conexiuni Medicale/Medical Connections offers thorough peer review and immediate publication on acceptance. The redactor-in-chief or one of the first reads the manuscripts received and in about 1-3 weeks decide upon their priority level: some are immediately sent to the reviewers, some are rejected without being sent for review and some are returned to authors with suggestions for improvement before submitting them to reviewers.
Peer-review procedureThe Conexiuni Medicale/Medical Connections
promotes evaluation of all the original papers by two or three independent reviewers, of whom two are international personalities. The peer-review process is essential for ensuring the quality of the scientific information disseminated. The reviewers are asked to evaluate the manuscript by applying the same standards as for the international journals. The reviewers send their comments to the Editor. The Editor will inform the authors about the suggestions made by the referee and ask them to answer the questions and make the required corrections. This information is provided up to three months from the date they submitted the paper to the journal. The revised manuscript should be sent in no more than one month to the Editor. When the Editor receives the corrected version with all changes marked, accompanied by a letter with a point-by-point reply to the reviewers’ comments, he sends those back to the same reviewer, who makes the final recommendation for acceptance or rejection of the manuscript.

82
MEDICAL CONNECTIONS • NUMBER 2 (26) • JUNE 2012gUIDAncE FOR DRAWIng UP
Notice to subscribersThe annual subscription rates for 2011: 80 RON
individual, 160 RON institutional. Foreing subscribers: 75 $ individual, 150 $ institutional. Additional postage: surface mail 20 $, for overseas air mail 40 $. Bank account: Colegiul Medicilor Satu Mare, CUI 9839430, Banca Transilvania, branch Agenţia Golescu Satu Mare, IBAN: RO38 BTRL 0310 1202 K392 62XX (RON) IBAN: RO62 BTRL 0310 2202 K392 62XX (USD) Swift: BTRLRO22. Orders should be sent to the Editorial Office, Eroilor Revoluţiei Pl. no.23-440055 Satu Mare, Romania. Tel./Fax: +40-261-710456 or +40-361-408164, or by e-mail: [email protected].
Notice to advertisersApplications for advertisement space and for rates
should be addressed to the Editorial Office of Conexiuni Medicale/Medical Connections. 2012 advertising rates are Euro 200 full (A4) colour page, 1 issue, and Euro 800 full colour page, 4 issues. Full
colour page on inside front or inside back cover: Euro 350 1 issue, 1400 4 issues. Full colour page ouside back cover: Euro 400 1 issue, 1600 4 issues. Bank account: Colegiul Medicilor Satu Mare, CUI 9839430, Banca Transilvania, branch Agenţia Golescu Satu Mare, IBAN: RO38 BTRL 0310 1202 K392 62XX (RON) IBAN: RO62 BTRL 0310 2202 K392 62XX (USD) Swift: BTRLRO22.
© Copyright Conexiuni Medicale/Medical Connections, Satu Mare, 2012
No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means without prior permission in writing of Conexiuni Medicale/Medical Connections. Permission is not however required to copy abstracts of papers or of articles on condition that a full reference to the source is shown. Correspondence regarding permission to reprint all or part of any article published in this journal should be addressed to the Editor, e-mail: [email protected]

83
EDITORIAL
După ce a cucerit Anglia la anul 1066, William Bastardul (doar în cronici e William Cuceritorul) a făcut două lucruri importante în această ordine: 1) A construit Turnul Londrei şi 2) A ordonat primul recensământ complet din istorie. Ordinea acestor acţiuni este extrem de importantă deoarece Turnul s-a dovedit salvator în timpul recensământului, când anglo-saxonii au vrut să-l cunoască mai îndeaproape pe cel care le-a deranjat tihna şi le-a numărat acareturile. Deşi nu absolvise London School of Economics, Regele avea şcoala vieţii aşa că a trimis două rânduri de inspectori, unii care făceau recensământul şi alţii care îi controlau pe recenzori.Asemănător cu trenurile româneşti din zilele noastre. Deşi statistica rezultată a fost legată frumos în piele şi era mai precisă decât Numerii din Vechiul Testament, în Cronicile Anglo-Saxone este cunoscută drept Cartea Judecăţii de Apoi (Doomsday Book). Asta pentru că Regele a stat apoi şi a judecat impozitele supuşilor pornind de la această bază de date. Se spune de către cronicari răutăcioşi, că în ultimii ani ai vieţii, când suferea de insomnie, Regele citea din această carte. Era desigur un act ratat, cum ar spune Freud, căci Regele se pregătea el însuşi să fie numărat la Judecata de Apoi.
Acumularea de date statistice este condiţia prealabilă obligatorie pentru orice decizie raţională privind economia, finanţele, medicina şi societatea în general. Bazele de date statistice corecte reprezintă certitudinea pe care se bazează orice estimare serioasă a viitorului. Deşi în esenţă, viitorul este imprevizibil, cu ajutorul statisticii putem stăpâni incertitudinea şi, parţial, anxietate pe care o generează. Acumularea de date face ca observatori independenţi, cu mintea deschisă să conveargă spre adevăr. Când au puţine date, oamenii de ştiinţă şi statisticienii nu cad de acord şi sunt subiectivi; când au mormane de date ei cad de acord şi devin obiectivi. Am să ilustrez în continuare acest lucru cu un exemplu din medicină.
Încă din 1937 un studiu german de dimensiuni reduse sesizase existenţa unei corelaţii între fumat şi cancerul pulmonar. Dar cine să-l ia în serios când Eduard Bernays, nepotul de soră al lui Freud şi proaspăt angajat la American Tobacco, tocmai convinsese femeile să fumeze ca să-şi dovedească independenţa şi emanciparea. Lumea medicală era de acord că poluarea industrială şi auto sunt vinovaţii exclusivi. Austin Bradford Hill împreună cu
Richard Doll au vrut să verifice care era totuşi cauza principală a cancerului pulmonar. Ei au intervievat pacienţii cu şi respectiv fără cancer pulmonar din 20 de spitale londoneze. Rezultatele, publicate în 1950, erau şocant de clare. Din 649 de bărbaţi cu cancer pulmonar, doar 2 nu fumau, iar dintre fumători majoritatea fumau mai mult de un pachet pe zi. Cu toate că s-a bucurat de atenţia excesivă a presei, studiul nu a convins comunitatea medicală care l-a acuzat că este minor, retrospectiv şi nu spune de fapt nimic despre cauză şi despre riscul fumătorilor de a face cancer pulmonar. Pentru a tranşa problema cei doi s-au hotărât să facă un studiu prospectiv pe un lot considerabil mai mare. Ei au chestionat un număr de 40.000 de medici britanici privind obiceiul fumatului şi i-au urmărit timp de 5 ani. Rezultatul a fost la fel de clar, fumătorii aveau o probabilitate de 24 de ori mai mare să facă cancer pulmonar, faţă de nefumători. De această dată medicii au fost convinşi, dar s-au opus statisticienii care au considerat că asocierea dintre fumt şi cancer nu înseamnă cauzalitate. Au fost elaborate tot felul de teorii precum că un factor genetic îţi induce atât dorinţa de a fuma cât şi cancerul pulmonar. În acest punct al dezbaterii intervenţia medicinei experimentale a fost decisivă: „nu există nicio dovadă că un carcinom bronhogenic diagnosticat după vârsta de 50 de ani a debutat la 18 ani, vârsta medie la care încep oamenii să fumeze, şi de aceea refuzăm să mai discutăm pe această temă”. Presupusul factor genetic ar fi trebuit să se răspândească rapid mai ales printre fumători, să producă cancer pe pielea şoriceilor dar nu în plămânii oamenilor, să scadă cu vârsta la cei ce s-au lăsat de fumat, să fie mai probabil la bărbaţi decât la femei, şi de 60 de ori mai prevalent la cei ce fumează peste 2 pachete pe zi. Cam mult pentru un factor genetic, dar perfect fezabil pentru un factor de mediu. Principalul rezultat al acestor cercetări a fost faptul că industria tutunului a introdus filtrul la ţigarete. Majoritatea filtrelor conţineau azbest! A fost nevoie de alţi ani de cercetări şi controverse până s-a lămurit rolul azbestului în carcinogeneză. A trebuit să moară două generaţii de fumători până când fumatul a fost interzis în locurile publice în Europa şi America. Acesta a fost preţul plătit pentru neglijarea sau interpretarea greşită a datelor statistice.
Dr. Sever-Cristian Oană
despRe oAMeni şi dAte stAtistice

Renal cyst (US)
Kidney in love
Gallbladder (US)
… and the gallbladder returns love

Over Expression Of Metalloproteinase-1 In Human Colonic Carcinomas And Its Prognostic Value 85
Rezumat
Cancerul colorectal (CCR) reprezintă o problemă gravă de sănătate iar căutarea de factori suplimentari de prognostic este în curs. În acest studiu ne-am dorit examinarea expresiei matricei metaloproteinazei 1 (MMP-1) prin metoda imunohistochimică în cancerul colorectal şi relaţia acesteia cu elementele clinicopatologice.
Au fost aleşi să participe şaizeci şi opt de pacienţi consecutivi cu CCR trataţi la centrul nostru. Eşantioane reprezentative din fiecare tumoră au fost marcate imunohistochimic pentru MMP-1. Intensitatea expresiei a fost clasificată ca fiind pozitivă sau negativă. Au fost folosite pentru control probe de ţesut normal de colon. În general, curba de supravieţuire a pacienţilor MMP-1 pozitivi a fost mai proastă decât a celor negativi, dar diferenţa nu a fost semnificativă statistic (p=0,125). Cu toate acestea, timpul de supravieţuire a fost semnificativ mai scurt pentru pacienţii MMP-1 pozitivi care nu au urmat chimioterapie, decât pentru cei negativi (p=0,019). Atunci când se ia în considerare
sexul pacientului, durata de supravieţuire a arătat o diferenţă semnificativă statistic între pacienţii de sex masculin MMP-1 pozitivi şi respectiv negativi (p=0,04), dar diferenţa pentru pacienţii de sex feminin nu a fost semnificativă statistic.
Se pare că pacienţii MMP-1 pozitivi ar putea beneficia de chimioterapie chiar dacă boala lor este întrun stadiu scăzut, prin urmare colorarea imunohistochimică pentru MMP-1 ar putea fi relevantă pentru luarea deciziei tratamentului adjuvant pentru fiecare pacient în parte.
Cuvinte cheie: MMP-1, carcinom colorectal
Introducere
Cancerul de colon reprezintă o problemă de sănătate şi epidemiologică gravă în ţările dezvoltate, iar prin creşterea nivelului de trai incidenţa sa este în creştere şi în ţările în curs de dezvoltare. Se crede că etiologia sa implică şi factori genetici, precum şi de mediu şi nutriţionali [1].
ORIgInAL ARTIcLEs
supRAeXpResiA MetAlopRoteinAZei-1 În cARcinoAMele colonului şi VAloAReA ei pRoGnosticĂ
Rath-Wolfson Lea1, Bubis Roy2, Shvero Asaf3, Ghinescu Minerva4, Ram Edward5
Departamentul de 1Patologie, Spitalul Hasharon, Centrul Medical Rabin, Petah-Tikva, 2Facultatea de Fizică şi Astronomie Raymond şi Beverly, Universitatea Tel-Aviv, 3Centrul Medical Sapir, Spitalul Meir, Kfar Sava, 4Universitatea Titu Maiorescu, Facultatea de Medicină, Bucureşti, România, 5Departamentul de Chirurgie, Spitalul Hasharon, Centrul Medical Rabin, Petah Tikva, afiliat la Universitatea Tel-Aviv, Tel-Aviv , Israel
Adresa pentru corespondenţă:Asaf Shvero, MD Sapir Medical Center, Meir Hospital, Kfar Sava E-mail: [email protected] Primit: 09.02.2012 Acceptat: 10.07.2012 Med Con October 2012, Vol 7, No 3, 85-89 Titlu scurt: MMP-1 în cancerul de colon Lucrarea a fost comunicată la a 2-a Conferinţă Internaţională în Patologie (Patology ‘11), 26-28 septembrie 2011, Praga, Republica Cehă.

ORIgInAL ARTIcLEs
Rath-Wolfson et al86
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
Prognosticul şi tratamentul se bazează pe stadializarea tumorală şi gradul histologic. Stadializarea tumorală se bazează pe sistemul Duke modificat: adâncimea infiltrării în peretele intestinal, prezenţa/absenţa metastazelor în nodulii limfatici regionali şi prezenţa/absenţa de metastaze în organe la distanţă, cum ar fi ficatul [2]. În stadiul A, în care penetrarea carcinomului este limitată la submucoasă, supravieţuirea la cinci ani este de 90%. Există o scădere la 50-60% în stadiul B, atunci când pătrunderea este în musculara propria. Supravieţuirea la cinci ani scade la 20-25% în stadiul Dukes C, atunci când există metastaze în nodulii limfatici regionali.
Îndepărtarea chirurgicală a tumorii reprezintă tratamentul definitiv, dar în funcţie de stadiu ar putea apare recurenţa sau metastazarea şi prin urmare se adaugă chimioterapia adjuvantă [2].
În ultimul timp, căutarea de factori de prognostic suplimentari care ar putea stabili care sunt pacienţii la risc mare de recurenţă sau metastazare este în creştere. Există studii efectuate asupra factorilor de proliferare, anomaliilor cromozomiale, expresiei oncogenelor, ADN-ploidiei, etc [2,3].
În cancerul de colon cel mai important factor de prognostic este stadiul, dar este cunoscut că pacienţii cei mai tineri şi cei mai în vârstă au prognosticul cel mai prost, precum şi riscul de ocluzie şi perforare [4]. Carcinoamele colonului stâng sunt mai predispuse la recurenţă [5]. Antigenii mucinoşi cum sunt Sialosyl şi antigenul Sialyl Lewis sunt cunoscuţi a fi factori de prognostic negativi [6], în timp ce pacienţii cu expresie HLA-DR pozitivă intensă au avut prognostic mai bun [7]. Pacienţii cu infiltrat inflamator de eozinofile, celulele dendritice şi limfocite au avut de asemenea o supravieţuire mai bună [8], în timp ce invazia vasculară şi perineurală sunt factori de prognostic negativi [9]. Pierderea alelei cromozomului 18Q a fost dovedită a fi un factor de prognostic foarte prost [10]. DCC s-a dovedit a fi un factor de prognostic pentru cancerul colorectal, expresia pozitivă a DCC identificând un subgrup de pacienţi care răspund favorabil la chimioterapie adjuvantă [11,12].
K-Ras, supra-expresia p-53, Ras P21 şi C-MYC sunt de asemenea bine cunoscuţi ca factori de prognostic [2].
Noile studii se concentrează asupra căutării de enzime cu proprietăţi distructive şi cuantificarea activităţii lor în tumori, ca factori de prognostic.
Distrugerea membranei bazale este esenţială pentru progresia tumorii. Diferite enzime ale grupului MMP sunt suspectate a fi implicate în invazia cancerului de colon în ţesuturile adiacente prin digestia colagenului de
tip IV, care este o componentă majoră a membranei bazale [13]. Mecanismul aceastei acţiuni este considerat a fi prin activarea Pro-gelatinazei A.
Metaloproteinazele matriceale (MMPs) sunt o familie de endopeptidaze extracelulare cu activitate enzimatică împotriva componentelor proteice ale matricei extracelulare. Ele sunt asociate cu diferite boli, cum ar fi displaziile scheletale, afecţiuni coronariene şi cardiace, artrită şi tulburări cerebrale. Forma activă a MMPs exercită un larg efect proteolitic împotriva unei game vaste de substraturi, incluzînd proteoglicani, fibronectină, elastină insolubilă, constituenţi de colagen de tip IV şi V a membranei bazale şi unele ţesuturi interstiţiale [13].
MMPs sunt cunoscute a fi implicate în carcinogeneza precoce, creşterea tumorală şi cel mai important, în invazia tumorală şi metastazare [14].
Legătura dintre MMPs şi progresia tumorală a fost investigată în cancerul de sân, carcinomul cu celule scuamoase al capului şi gâtului şi melanomul malign [15 -17].
Scopul acestui studiu retrospectiv pe 68 de pacienţi cu cancer de colon a fost de a afla dacă expresia MMP-1 în tumoră a fost un factor de prognostic dependent/independent de stadializarea Duke şi de tratament.
Materiale şi metode
Pacienţii Studiul a inclus 68 de pacienţi consecutivi care au
fost diagnosticaţi şi trataţi pentru cancer de colon la spitalul nostru. Toţi pacienţii au fost supuşi aceluiaşi protocol diagnostic şi terapeutic. Toţi pacienţii au fost supuşi colectomiei, cu sau fără chimioterapie adjuvantă.
Concepţia acestui studiu a fost aprobată de către comitetul nostru instituţional.
Specimenele tumorale Specimenele rezecate au fost fixate cu formol
tamponat 4%. Secţiuni reprezentative au fost incluse în parafină şi colorate cu hematoxilină şi eozină (H&E).
Imunohistochimie Toate lamele disponibile au fost evaluate de către
doi patologi.Blocurile de parafină reprezentative ale tumorilor au
fost selectate pentru analiza imunohistochimică. Secţiunile de 4 μm grosime au fost plasate pe lame Super-Frost Plus (Sigma, Germania), uscate peste noapte la 37°C şi deparafinizate cu două schimburi de xilen pentru 3 minute fiecare. Procesul de pregătire a constat în etape în succesiunea următoare: secţiunile au fost hidratate treptat prin alcool gradat, în etanol 100% de două ori timp de 5 minute şi în etanol 95% pentru 5 minute,

ORIgInAL ARTIcLEs
Over Expression Of Metalloproteinase-1 In Human Colonic Carcinomas And Its Prognostic Value 87
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
clătite cu apă distilată timp de 1 minut şi blocate pentru activitatea peroxidului endogen în soluţie de 3% peroxid de hidrogen timp de 10 minute la temperatura camerei; clătite în două schimburi de apă distilată şi plasate întro oală sub presiune cu citrat tamponat pre-fiert la pH 6,0 pentru recuperarea antigenului; imediat spălate în apă distilată şi incubate cu anticorpi policlonali de iepure pentru MMP-1. Ulterior, secţiunile au fost clătite din nou cu soluţie tampon de spălare şi incubate cu anticorpi secundari cu spectru larg Polymer HRP-conjugaţi (Kit de detectare Polymer, Zymed, California, SUA) pentru 15 minute la temperatura camerei; clătite din nou cu soluţie tampon de spălare şi colorate cu soluţie de diaminobenzidină timp de 10 minute la temperatura camerei. În cele din urmă, secţiunile au fost contracolorate cu hematoxilină Mayer pentru 5 minute şi deshidratate cu etanol 95% timp de 1 minut şi 100% etanol pentru 2 minute, clarificate cu xilen pentru 2 minute şi acoperite cu mediu de montare.
Evaluarea imunohistochimică Mucoasa normală de colon a servit ca şi control
pozitiv (Fig. 1, pag. 9).Pentru controlul negativ anticorpii primari au fost
omişi în mucoasa colonului normal. Lamele au fost evaluate de către 2 patologi
experimentaţi, care au clasificat intensitatea ca pozitivă atunci când citoplasma a mai mult de 50% din celule tumorale a fost colorată şi negativă când a fost de mai puţin de 50%.
Analiza statisticăDurata medie a supravieţuirii şi supravieţuirea fără
boală au fost estimate folosind analiza Kaplan-Meier pentru a ţine cont de cazurile cenzurate.
Cazurile au fost împărţite în grupe în funcţie de chimioterapie sau în funcţie de sex, iar diferenţa în curbele de supravieţuire între pacienţii având colorare MMP-1 pozitivă şi pacienţii negativi a fost evaluată cu ajutorul testului log-rank. Semnificaţia statistică a fost fixată la p<0,05.
Rezultate
Grupul de studiu a constat din 43 de bărbaţi şi 25 femei. Tabelul I rezumă datele clinicopatologice ale pacienţilor. Vârsta lor a variat de la 42 la 81 de ani (medie 68,79).
În grupul de sex masculin 16 au avut coloraţie pozitivă pentru MMP-1 (Fig. 2, pag. 9) şi 27 au fost negativi (Fig. 3, pag. 9). În grupul de femei 7 au fost pozitive şi 18 negative.
Douăzeci din aceste cancere s-au situat în rect, în timp ce altele au avut mai multe locaţii proximale.
Optsprezece tumori au fost clasificate ca bine diferenţiate iar 50 au fost moderat diferenţiate. Treizeci şi şase de pacienţi au fost în stadiul B, în timp ce 32 de pacienţi au fost în stadiul C, cu metastaze ganglionare regionale. Chimioterapia adjuvantă a fost administrată la 45 de pacienţi, în timp ce 23 nu au primit niciun tratament.
Nouă din cele 20 de cancere rectale au fost pozitive pentru MMP-1 şi 11 negative. Din celelalte localizări colice, 48 de cazuri, 14 au fost pozitive în timp ce 34 au fost negative.
În grupul de tumori bine diferenţiate, au existat 6 cazuri pozitiv colorate pentru MMP-1 şi 12 negative. În grupul cu tumori moderat diferenţiate au fost 17 cazuri pozitive şi 38 negative, fără nicio diferenţă semnificativă. În stadiul B al bolii, 12 au avut coloraţie MMP-1 pozitivă şi 24 au fost negative. În stadiul C 11 cazuri au fost pozitive în timp ce 21 au fost negative, fără nicio diferenţă semnificativă statistic.
Patruzeci şi cinci de pacienţi au primit chimioterapie. Din aceştia, 18 au avut coloraţie pozitivă pentru MMP-1 şi 27 au fost negativi.
La sfârşitul acestui studiu 47 de pacienţi erau în viaţă, iar 21 au decedat datorită bolii.
Tabelul I. Caracteristicile clinice ale pacienţilor în contextul metaloproteinazelor
Parametri Întreaga populaţie
MetaloproteinazePozitive (n=23)
Negative(n=45)
Vârsta (ani)-medie 68,79 66,69 69,86Sex
bărbaţi 43 16 27femei 25 7 18
Localizarecolon 48 14 34rect 20 9 11
GradABD 18 6 12AMD 50 17 38
StadiuB 36 12 24C 32 11 21
Chimioterapieda 45 18 27nu 23 5 18
StatusÎn viaţă 47 13 34Decedat 21 10 11
MMP-1 – Metaloproteinaze-1; ABD – adenocarcinom bine diferenţiat; AMD – adenocarcinom moderat diferenţiat.

ORIgInAL ARTIcLEs
Rath-Wolfson et al88
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
Dintre acei pacienţi care au fost în viaţă, 23 de cazuri au fost MMP-1 pozitive şi 45 au fost negative. În grupul de pacienţi decedaţi 10 au fost pozitivi şi 11 au fost negativi.
În general, supravieţuirea celor pozitivi a fost de 66±7 luni, mai rea decât a celor negativi, 73,3±4,2 luni, dar diferenţa nu a fost semnificativă statistic (p=0,125). Supravieţuirea fără boală în grupul pozitiv în conformitate cu statutul MMP-1 a fost de 49,3±6,5, iar în grupul negativ 63,6±5, p=0,21, fără diferenţe semnificative. La pacienţii care nu au primit chimioterapie, timpul de supravieţuire a arătat o diferenţă semnificativă statistic între pacienţii cu indicaţie pozitivă pentru MMP-1 şi indicaţie negativă (36,2±9,7 luni faţă de 66,5±7,7 luni, p=0,019) (Fig. 4, pag. 10).
Pentru pacienţii care au primit chimioterapie, nu a fost nicio diferenţă semnificativă statistic între pacienţii cu MMP-1 pozitiv (supravieţuirea medie 75,5±7,5 luni) şi grupul negativ (supravieţuirea medie 73,7±4,3 luni), p=0,44 (Fig. 5, pag. 10).
Supravieţuirea fără boală a arătat rezultate similare: o diferenţă semnificativă statistic la pacienţii care nu au primit chimioterapie (24,2±3,6 luni faţă de 55,7±8,2 luni, p=0,025) (Fig. 6, pag. 11).
Diferenţa nu a fost statistic semnificativă pentru pacienţii care au primit chimioterapie. Pentru grupul pozitiv 56,3±7,4 luni, iar pentru grupul negativ 65,3±5,6, p=0,45.
Atunci când se ia în considerare sexul pacientului, timpul de supravieţuire a arătat o diferenţă semnificativă statistic între pacienţii de sex masculin cu indicaţie MMP-1 pozitivă şi negativă (77,4±3,6 luni faţă de 68,9±8,5 luni, p=0,04) (Fig. 7, pag. 11), dar diferenţa pentru pacienţii de sex feminin nu a fost semnificativă statistic. În grupul de sex feminin cu tumori colorate pozitiv, timpul de supravieţuire a fost de 52,6±10,2 luni, iar în grupul negativ 60,4±7,9 luni, p=0,61.
Supravieţuirea fără boală a arătat diferenţe care nu au fost statistic semnificative pentru bărbaţi, pozitivi 50,0±7,9 luni, negativi, 67,3±5,5 luni, p=0,09. Pentru pacienţii de sex feminin, cu tumori colorate pozitiv, durata de supravieţuire fără boală a fost de 41,9±8,5 luni, iar pentru cele colorate negativ a fost de 52,4±8,0, p=0,93.
Discuţie
În acest studiu am analizat expresia MMP-1 la 68 de pacienţi care au suferit de CCR. Curba de supravieţuire generală a pacienţilor având colorare MMP-1 pozitivă a fost mai rea decât la cei negativi, chiar dacă nu au fost
diferenţe semnificative statistic, p=0,125. Am constatat că durata de supravieţuire a pacienţilor care nu au primit chimioterapie şi au fost pozitivi pentru MMP-1 a fost mai rea decât cea pentru cei negativi, p=0,019. Durata de supravieţuire a arătat, de asemenea, o diferenţă semnificativă statistic între pacienţii de sex masculin având colorare MMP-1 pozitivă, comparativ cu cei care nu au coloraţie, p=0,04. În grupul de sex feminin diferenţa nu a fost semnificativă statistic, p=0,61. Supravieţuirea fără boală a aratat rezultate similare, cu o diferenţă semnificativă statistic pentru acei pacienţi care nu au primit chimioterapie, din nou în favoarea celor care nu s-au colorat pozitiv pentru MMP-1, p=0,0025.
Factorul major pe care se bazează cu adevărat medicii oncologi pentru a administra chimioterapie este stadiul.
În literatura de specialitate există studii efectuate pe diferiţi factori de proliferare în căutarea unui instrument care ar putea identifica acei pacienţi care sunt la risc mai mare pentru recidive sau metastaze, cum ar fi anomaliile cromozomiale, ploidia ADN-ului, etc [2,3,6,7].
S-a demonstrat că expresia crescută a MMPs apare întrun stadiu incipient al carcinomului colorectal şi aceasta oferă dovezi pentru a susţine ipoteza că aceste molecule au un rol cheie în primele etape ale dezvoltării tumorii [18]. Datele sunt în concordanţă cu efectul lor proteolitic împotriva proteoglicanilor, fibronectinei, colagenului IV şi V şi unor tipuri de ţesuturi interstiţiale [13]. Această caracteristică proteolitică a MMP-1 poate promova invazia tumorală şi metastazele [14]. Astfel, devine clar modul în care acei pacienţi cu pozitivitate a coloraţiei MMP-1 au avut rezultate mai slabe decât cei având coloraţie negativă.
Studiile efectuate pe tumori maligne ale altor organe au arătat că expresia MMP-1 pozitivă este nefavorabilă. În tiroidă expresia MMP-1 la pacienţii cu carcinom tiroidian bine diferenţiat a fost în concordanţă cu agresivitatea tumorii. Aceste constatări pot prezice prognosticul mai sărac şi justifică un tratament mai agresiv chirurgical [19].
În cancerul de sân Okuyama N şi colab. [20] au concluzionat că MMP-1 joacă un rol crucial în metastazele osoase ale cancerului de sân.
Cheng S şi colab. [21] au constatat că expresia crescută MMP-1 mRNA a fost un factor independent de prognostic nefavorabil, rezultatele lor sugerând că MMP-1 este o genă importantă implicată în progresia cancerului de sân.
An Z şi colab. [22] au administrat pe cale orală CT1746, un inhibitor sintetic oral activ MMP la şoareci. Ei au demonstrat o reducere a masei tumorale primare, răspândirii totale şi metastazării.

ORIgInAL ARTIcLEs
Over Expression Of Metalloproteinase-1 In Human Colonic Carcinomas And Its Prognostic Value 89
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
Concluzia noastră principală din acest studiu este faptul că aceşti pacienţi, în special cei de sex masculin, având colorare MMP-1 pozitivă trebuie să fie trataţi mai agresiv, chiar şi în stadiile precoce ale bolii.
Referinţe
1. Fletcher CDM. Diagnostic histopathology of tumors. 3th edition, Churchill Livingstone, Elservier, 2007, vol 1, pp. 379-416.
2. Rosai J. Rosai and Ackerman Surgical Pathology. 9th edition, Mosby, New York, vol 1, pp 776-855.
3. Pino MS, Chung DC. The chromosomal instability pathway in colon cancer. Gastroenterology. 2010;138(6):2059-72.
4. Griffin MP, Bergstralh EJ, Coffey RJ, Beart RW Jr, Melton LJ III. Predictors of survival after curative resection of carcinoma of the colon and rectum. Cancer 1987;60:2318-24.
5. Russell AH, Tong D, Dawson LE, Wisbeck W. Adenocarcinoma of the proximal colon. Sites of initial dissemination and patterns of recurrence following surgery alone. Cancer 1984;53(2):360-7.
6. Itzkowitz SH, Bloom EJ, Kokal WA, Modin G, Hakomori S, Kim YS. Sialosyl-Tn. A novel mucin antigen associated with prognosis in colorectal cancer patients. Cancer 1990;66(9):1960-6.
7. Andersen SN, Rognum TO, Lund E, Meling GI, Hauge S. Strong HLA-DR expression in large bowel carcinomas is associated with good prognosis. Br J Cancer 1993;68(1):80-5.
8. Harrison JC, Dean PJ, el-Zeky F, Vander Zwaag R. From Dukes through Jass: pathological prognostic indicators in rectal cancer. Hum Pathol 1994;25(5):498-505.
9. Krasna MJ, Flancbaum L, Cody RP, Shneibaum S, Ben Ari G. Vascular and neural invasion in colorectal carcinoma. Incidence and prognostic significance. Cancer 1988;61(5):1018-23.
10. Jen J, Kim H, Piantadosi S, et al. Allelic loss of chromosome 18q and prognosis in colorectal cancer. N Engl J Med 1994;331(4):213-21.
11. Gal R, Sadikov E, Sulkes J, Klein B, Koren R. Deleted in colorectal cancer protein expression as a possible predictor of response to adjuvant chemotherapy in
colorectal cancer patients. Dis Colon Rectum 2004;47(7):1216-24.
12. M. Halpern, D. Kravarusic, R. Bubis, R. Koren. Prediction of Response to preoperative chemoirradiation of rectal cancer by DCC protein expression. Medical Connections 2010;3(19):13-28.
13. Murray GI, Duncan ME, O Neil P, Melvin WT, Fothergill JE. Matrix metalloproteinase-1 is associated with poor prognosis in colorectal cancer. Nat Med 1996;2(4):461-2.
14. Nakopoulou L, Giannopoulou I, Gakiopoulou H, Liapis H, A Tzonou, Davaris PS. Matrix Metalloproteinase-1 and –3 in breast cancer: correlation with progesterone receptors and other clinicopathologic features. Hum Pathol 1999;30:436-42.
15. Murray GI, Duncan ME, O’Neil P, McKay JA, Melvin WT, Fothergill JE. Matrix metalloproteinase-1 is associated with poor prognosis in oesophageal cancer. Jpathol 1998;185(3):256-61.
16. Stetler-Stevenson WG, Liotta LA, Kleiner DE Jr. Extracellular matrix 6: role of matrix metalloproteinases in tumor invasion and metastasis. FASEB J 1993;7(15):1434-41.
17. Tryggvason K, Höyhtyä M, Pyke C. Type IV collagenases in invasive tumors. Breast Cancer Res Treat 1993;24(3):209-18.
18. Jeffery N, McLean MH, El-Omar EM, Murray GI. The matrix metalloproteinase/tissue inhibitor of matrix metalloproteinase profile in colorectal polyp cancers. Histopathology 2009;54(7):820-8.
19. Mizrachi A, Koren R, Hadar T, Yaniv E, Morgenstern S, Shvero J. Expression of MMP-1 in invasive well-differentiated thyroid carcinoma. Eur Arch Otorhinolaryngol 2011;268(1):131-5
20. Okuyama N, Matsumine A, Kosugi R, Wakabayashi H, Uchida A. Matrix metalloproteinase-1 is a crucial bone metastasis factor in a human breast cancer-derived highly invasive cell line. Oncol Rep 2008;20(6):1497-504.
21. Cheng S, Tada M, Hida Y, et al. High MMP-1 mRNA expression is a risk factor for disease-free and overall survivals in patients with invasive breast carcinoma. J Surg Res 2008;146(1):104-9.
22. An Z, Wang X , Willmott N et al. Conversion of highly malignant colon cancer from an aggressive to a controlled disease by oral administration of a metalloproteinase inhibitor. Clin Exp Metastasis 1997;15(2):184-95.
Traducere: Bumbuluţ Călin

Inner Ear , petrous bone (CT)
Can anybody hear barking?
lion’s gate
Inner Ear , petrous bone (CT)

Renal Function Monitoring In Urogenital Robot-Assisted Laparoscopic Surgery Performed In General Anaesthesia 91
Rezumat
Introducere: Leziunea renală acută, definită prin criteriile RIFLE (acronim de la risc-R, injurie-I, insuficiență-L, stadiu final-LE) şi AKIN (Acute Kidney Injury Network), este o complicaţie frecventă după intervenţiile majore, apare la 36% din pacienţii internaţi pe terapie intensivă. Importanţa diagnosticării precoce a leziunii renale acute derivă din faptul că injuria renală poate avansa până la insuficienţă renală, creşte mortalitatea, perioada internării şi costurile spitalizării în ciuda tuturor modalităţilor noi de tratament sau prevenire. Chirurgia robotică este cea mai modernă metodă chirurgicală minim invazivă, cu multiple avantaje. Dezavantajul principal este costul ridicat.
Scopul studiului a fost evaluarea funcţiei renale prin analiza evoluţiei creatininei serice în chirurgia laparoscopică asistată robotic sub anestezie generală.
Material şi metodă: Am efectuat un studiu descriptiv, observaţional longitudinal prospectiv, în care au fost incluşi 23 pacienţi internaţi în Spitalul Municipal Cluj secţia Urologie, în perioada mai 2010 - februarie 2012, programaţi pentru intervenţii chirurgicale urologice laparoscopice asistate robotic. Leziunea renală acută a fost definită prin creşterea absolută a creatininei serice cu 0,3mg/dl, conform criteriilor AKIN.
Rezultate: Au fost incluşi în studiu 23 de pacienţi de sex masculin cu vârsta medie 59 de ani, programaţi pentru intervenţii uro-genitale robotice. Intervenţiile efectuate au fost: 18 prostatectomii radicale, 3 nefrectomii parţiale, 1 cistectomie şi 1 pieloplastie. Durata medie a intervenţiei chirurgicale a fost de 5,23 ore. Nouă pacienţi au prezentat leziune renală acută, reprezentând 39%. Funcţia renală a fost apreciată prin determinări repetate ale creatininei serice. Leziunea renală acută, definită prin creşterea absolută a creatininei serice cu 0,3 mg/dl (26,4 μmol/l) peste valoarea bazală în 72 ore postoperator, conform noilor criteriilor AKIN, a fost tranzitorie. Valorile creatiniei serice din ziua a patra postoperator sunt comparabile cu valorile bazale.
Concluzii: Chirurgia robotică modifică funcţia renală, prin scăderea perfuziei renale, datorită unor condiţii speciale, cum ar fi: pneumoperitoneul, poziţia Trendelenburg şi restricţia de lichide în întervenţiile pe prostată. Leziunea renală acută tranzitorie în chirurgia robotică sub anestezie generală, remite până în ziua a patra postoperator.
Cuvinte cheie: leziune renală acută, chirurgie robotică, anestezie generală, perfuzia organelor uro-genitale, clasificarea RIFLE
ORIgInAL ARTIcLEs
MonitoRiZAReA FuncŢiei RenAle În inteRVenŢiile lApARoscopice uRo-GenitAle AsistAte Robotic, eFectuAte În AnesteZie GeneRAlĂ
Mihály Orsolya1, Bolboacă Sorana Daniela2, Răhăian Rodica4, Chira Cipriana5, Mihály Zoltán Attila3, Coman Ioan3
1Spitalul Clinic Judeţean de Urgenţă Cluj, Secţia ATI, 2Universitatea de Medicină şi Farmacie “Iuliu Haţieganu”, Cluj-Napoca, Catedra Informatică şi Statistică Medicală, 3Spitalul Clinic Municipal Cluj-Napoca, secţia Urologie, 4Spitalul Clinic Judeţean de Urgenţă Cluj, Departamentul Imunologie, 5Spitalul Clinic Municipal Cluj Napoca, Secţia ATI
Adresa de corespondenţă:Dr. Mihály Orsolya Email: [email protected] Primit: 02.08.2012 Acceptat: 10.09.2012 Med Con October 2012, Vol 7, No 3, 91-99

ORIgInAL ARTIcLEs
Mihály et al92
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
Introducere
Tendinţa actuală este de a diferenţia leziunea renală acută de insuficienţa renală acută. Leziunea renală acută, definită prin criteriile RIFLE (acronim de la risc-R, injurie-I, insuficienţă-F, stadiu final-LE) şi AKIN (Acute Kidney Injury Network), cuprinde spectrul integral al modificării funcţiei renale, iar insuficienţa renală reprezintă stadiul final al leziunii renale. Frecvent diagnosticul este tardiv şi se asociază cu creşterea morbidităţii şi mortalităţii, ceea ce implică prelungirea duratei internării, ridicarea costurilor spitalizării şi nu în ultimul rând reducerea calităţii vieţii pacienţilor afectaţi. Reducerea perfuziei organelor uro-genitale perioperator creşte riscul ischemiei, necrozei şi infecţiilor.
AKIN apare la 36% din pacienţii internaţi pe secţiile de terapie intensivă [1] şi este o complicaţie frecventă după intervenţiile chirurgicale majore cardiovasculare [2]. Creşte mortalitatea, perioada internării şi costurile spitalizării în ciuda tuturor modalităţilor noi de tratament sau prevenire.
Pentru a ajunge la un consens în sistemul de clasificare al leziunii renale acute, ADQI (Acute Dialysis Quality Initiative Group) a elaborat criteriile RIFLE în 2004 şi a stabilit trei clase de severitate R (risc), I (injury-leziune), F (failure-insuficienţă) şi două clase de prognostic L (loss-pierderea funcţiei), E (End Stage Renal Disease-boală renală în stadiu final) [3], aşa cum sunt prezentate în Tabelul I.
Criteriile RIFLE au importanţă clinică pentru diagnosticul [4], clasificarea severităţii [5], monitorizarea progresului AKI [6], cu rol prognostic [7].
În 2007 Acute Kidney Injury Network (AKIN) a propus modificarea unor criterii RIFLE [8]. Au stabilit trei stadii, care corespund cu criteriile RIFLE. Stadiul 1- Risc, stadiul 2- I-leziune, stadiul 3- F-insuficienţă, Loss şi End Stage (boală renală în stadiu terminal), au fost considerate factori de prognostic.
Sistemul chirurgical robotic da Vinci, cel mai avansat robot utilizat în practica clinică, permite o abordare minim invazivă, ideală pentru chirurgia urologică [9,10].
Sistemul constă într-o consolă ergonomică pentru chirurg, un cart pentru pacient cu patru braţe robotice interactive, un sistem de vizualizare 3D de înaltă rezoluţie şi instrumente articulate specifice EndoWrist [11]. Acest sistem este conceput să transforme, să filtreze şi să transmită mişcările mâinii chirurgului în mişcări precise ale instrumentelor, fiind o interfaţă intuitivă cu capacităţi chirurgicale de înaltă performanţă [12], utilizat în urologie, chirurgie generală, ginecologie şi chirurgie toracică [13].
Avantajele [14] acestei tehnici chirurgicale sunt: scăderea hemoragiei, vizualizarea 3D, calitate superioară a imaginii, iar instrumentele EndoWrist cu 7 grade de libertate permit mişcări complexe în spaţiu mic, dureri postoperatorii reduse, reluarea rapidă a tranzitului, reducerea complicaţiilor, cicatrici mici, durată mai
Tabel I. Clasificarea RIFLE
Clasificare Criteriu de filtrare glomerulară Criteriu de diureză
Risc Creatinina creşte de 1,5X RFG scade >25% <0,5 ml/kg/h 6 ore
Injury Creatinina creşte de 2X RFG scade >50% <0,5 ml/kg/h 12 ore
Failure Creatinina creşte de 3X sau creat ≥4 mg/dl saucreştere acută creat de >0,5mg/dlRFG scade >75%
<0,3 ml/kg/h 24 oresau
anurie 12 oreLoss Insuficienţa renală acută persistentă = pierderea completă a funcţiei renale> 4 săptămâni
ESRD End Stage Renal Disease Boală cronică de rinichi >3 luni
Tabel II. Clasificarea AKIN
Stadiul akin Creatinina Diureza
1 Creşte de 1,5-2 ori, sau cu 0,3mg/dl (27 μmol/l) <0,5 ml/kg/h 6 ore2 Creşte de 2-3 ori <0,5 ml/kg/h 12 ore3 >3 ori sau >4mg/dl (354 μmol/l) cu o creştere bruscă de >0,5
mg/dl (44μmol/l)<0,3 ml/kg/h 24 ore sau anurie 12 ore

ORIgInAL ARTIcLEs
Renal Function Monitoring In Urogenital Robot-Assisted Laparoscopic Surgery Performed In General Anaesthesia 93
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
redusă de spitalizare cu recuperare rapidă, protejarea filetelor nervoase care influențează continenţa urinară şi dinamica sexuală. Dezavantajul este costul ridicat [15]: creşte costul intervenţiei cu aproximativ 200$, ceea ce reprezintă 20% din costul prostatectomiei [16,17].
Scopul studiului a fost evaluarea funcţiei renale prin analiza evoluţiei creatininei în anestezie generală pentru chirurgia laparoscopică asistată robotic.
Material şi metodă
Am efectuat un studiu descriptiv observaţional longitudinal prospectiv, în care au fost incluşi 23 pacienţi internaţi în Spitalul Clinic Municipal Cluj secţia Urologie, în perioada mai 2010 - februarie 2012, programaţi pentru intervenţii chirurgicale urologice laparoscopice asistate robotic.
Criteriile de includere în studiu au fost: pacienţi programaţi pentru intervenţie urologică robotică, fără afecţiuni renale cronice (clasificarea RIFLE, cel mult R), clasificarea AKIN [18] stadiu 1, stabili hemodinamic şi respirator.
Studiul a fost aprobat de comisia de etică a Spitalului Municipal Cluj. Toţi pacienţii incluşi în studiu şi-au dat acordul participării prin semnarea unui consimţământ informat în care li s-a explicat ce implică prezenţa lor în acest studiu. Pacienţii au fost informaţi privind tipul intervenţiei şi al anesteziei.
De la pacienţii incluşi în studiu au fost culese următoarele date preoperator: date demografice (sex, vârstă), scorul comorbidităţilor (Charlson Comorbidity Index [19]), scorurile fiziologice (Apache II [20], SOFA [21]), riscul anesteziei evaluat prin scorul ASA [22]. Funcţia renală a fost evaluată prin criteriile RIFLE şi AKIN. Intraoperator: durata intervenţiei măsurată în ore (h), cantitatea hemoragiei (ml), stabilitate cardiovasculară (TA medie peste 60mmHg) şi respiratorie (saturaţia în oxigen al sângelui periferic peste 94%). Postoperator: s-au urmărit funcţiile vitale (TA, puls, respiraţia), diureza zilnică 4 zile postoperator şi s-a recoltat zilnic creatinina serică în primele 4 zile postoperator. Funcţia renală a fost evaluată prin analiza evoluţiei creatininei serice.
Leziunea renală acută (AKI) a fost definită prin creşterea absolută a creatininei serice cu 0,3mg/dl (26,4μmol/l) peste valoarea bazală la 72 ore postoperator, conform noilor criteriilor AKIN.
Analiza statisticăVariabilele calitative au fost exprimate procentual,
pentru procente calculându-se intervalul de încredere de 95% (abreviat ca IC 95%) prin aplicarea unei metode optimizate, metodă similară cu cea prezentată în lucrare [23].
Variabilele cantitative au fost sumarizate prin media aritmetică şi deviaţia standard (media±deviaţia standard) pentru variabile cu date normal distribuite şi ca mediană şi cvartilele de 25% şi 75% pentru variabilele cu date care nu au respectat distribuţia normală. Testul Kolmogorov-Smirnov [24,25] a fost utilizat pentru testarea normalităţii; o valoare a probabilităţii asociată statisticii Kolmogorov-Smirnov mai mică de 5% a indicat absenţa distribuţiei normale a datelor. Testul Friedman a fost aplicat pentru a identifica diferenţe semnificative statistic între valorile creatininei serice determinate baseline, la o zi, două zile, trei zile şi respectiv patru zile postoperator.
S-a urmărit modificarea funcţiei renale definită prin apariţia AKI în anestezie generală pentru intervenţii chirurgicale laparoscopice asistate robotic.
Rezultate
Douăzeci şi trei de pacienţi au îndeplinit criteriile de includere în studiu, funcţia lor renală fiind evaluată prin prisma nivelelor creatininei serice. Pacienţii au fost de sex masculin, cu vârsta cuprinsă între 22 şi 72 ani, cu o vârstă medie de 59 ani (mediana vârstei = 62 ani, percentila de 25% = 56 ani şi percentila de 75% = 65 ani). Majoritatea pacienţilor au fost supuşi intervenţiei pe prostată (18 pacienţi, 78% IC 95% [57%-91%]). Trei pacienţi au fost supuşi nefrectomiei parţiale (13%, IC 95% [5%-35%]), iar un pacient a fost supus cistectomiei, respectiv pieloplastiei.
Scorul de comorbiditate a avut valori între 0 şi 10, cu o valoare a medianei de 3 (percentila de 25% = 2, percentila de 75% = 5). Scorul Apache a avut valori între 1 şi 10, cu o valoare a medianei de 6 (percentila de 25% = 4, percentila de 75% = 8). Patru pacienţi (17%, IC 95% [5%-39%]) au avut scorul SOFA egal cu 1.
Durata medie a intervenţiei chirurgicale a fost de 5,23±1,01 ore şi a variat între 4 şi 7 ore. Volumul hemoragiei a variat între 200 şi 400 ml, cu o valoare a medianei de 250 ml şi valori ale percentilelor de 25% şi respectiv de 75% de 200 ml, respectiv 300 ml.
Dintre determinările creatininei serice, doar evaluarea bazală şi cea de la 4 zile postoperator s-au dovedit normal distribuite. Sumarizarea valorilor creatininei este prezentată în Tabelul III, iar evoluţia valorilor creatininei serice per pacient este redată în Figura 1.
Aplicarea testului Friedman a identificat o diferenţă semnificativă statistic între valorile creatininei serice investigate (valoarea statisticii Hi-Pătrat=19,956, grade de libertate=4, valoarea probabilităţii asociate testului p=0,001). Valoarea medie a creatininei bazale s-a dovedit

ORIgInAL ARTIcLEs
Mihály et al94
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
a nu fi semnificativ statistic diferită faţă de valoarea medie a creatininei serice determinată la 4 zile postoperator (statistica t=0,705, 22 grade de libertate, p=0,488). Rezultatele diferenţelor între creatinina serică evaluată bazal şi la diferite zile postoperator sunt prezentate în Tabelul IV.
În nouă cazuri a fost identificată leziune renală acută definită prin creşterea absolută cu 0,3 mg/dL peste valoarea bazală în primele 72 ore de la intervenţie (39%, IC 95% [18%-61%]), criteriu care însă nu s-a păstrat şi la 4 zile postoperator.
Discuţii
Până în prezent, nu a fost studiată incidenţa acestui tip de leziune renală după intervenţii chirurgicale laparoscopice asistate robotic. Unele particularităţi ale intervenţiilor chirurgicale laparoscopice asistate robotic (pneumoperitoneul, poziţia Trendelenburg şi restricţia de hidratare la prostatectomii) reduc perfuzia splahnică şi cresc incidenţa AKI.
Valorile cele mai crescute ale creatininei serice au fost înregistrate în prima zi postoperator, diferenţa fiind semnificativă statistic (p=0,004).
Există o diferenţă semnificativă statistic (p≤0,002) între valorile creatininei serice din zilele 2,3,4 postoperator comparativ cu ziua 1 postoperator, semnificând scăderea trepatată a valorilor până aproape de valoarea bazală în ziua 4 postoperator.
Disfuncţia renală a fost tranzitorie. Începând din ziua a 2-a postoperator diferenţa valorilor creatininei serice comparate cu valoarea bazală nu a mai fost semnificativă statistic (p>0,05).
Incidenţa leziunii renale acute în chirurgia robotică a fost 39%. În literatura de specialitate leziunea renală acută apare în 36% de cazuri la pacienţii internaţi pe terapie intensivă, în 33,5% la pacienţii cu transplant de măduvă osoasă [26], în 35,7% la pacienţii arşi [27], în 35,9% la pacienţii cu transplant hepatic [28] şi 37,4% la pacienţii septici [29].
Este primul studiu care urmăreşte funcţia renală în chirurgia robotică, prin spectrul modificării creatininei
Tabelul III. Parametrii descriptivi ai creatininei serice
StatisticaCreatinina serică (mg/dL)
bazal 1 zi post-op 2 zile post-op 3 zile post-op 4 zile post-op
media aritmetică 0.98 1.24 1.07 1.01 0.95deviaţia standard 0.17 0.37 0.25 0.23 0.18Minimum 0.72 0.85 0.73 0.75 0.65Maximum 1.30 2.10 1.64 1.56 1.40Mediana 0.96 1.08 0.99 0.92 0.94percentila 25% 0.87 0.97 0.90 0.88 0.83percentila 75% 1.10 1.52 1.17 1.10 1.03
Tabelul IV. Testul Wilcoxon: rezultate în compararea creatininei serice
Creatinina serică (mg/dL) Statistica Z Valoarea p1 zi* – bazal -2,905a 0,0042 zile* – bazal -1,141 a 0,2543 zile* – bazal -0,472 a 0,6372 zile* – 1 zi* -3,043b 0,0023 zile* – 1 zi* -3,624b <0,0014 zile* – 1 zi* -3,751b <0,0013 zile* – 2 zile* -1,904b 0,0574 zile* – 2 zile* -2,799b 0,0054 zile* – 3 zile* -2,180b 0,029
a = bazat pe ranguri negativeb = bazat pe ranguri pozitive* post-operator
Figura 1. Evoluţia baseline – postoperator a valorilor creatininei serice

ORIgInAL ARTIcLEs
Renal Function Monitoring In Urogenital Robot-Assisted Laparoscopic Surgery Performed In General Anaesthesia 95
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
serice. Acest studiu dovedeşte prin metode statistice implementate apariţia leziunii renale acute în intervenţiile chirurgicale robotice, dar arată şi caracterul tranzitor al modificărilor funcţiei renale.
În SUA, în 2006 42% dintre prostatectomiile radicale s-au realizat prin abord robotic, în 2007 procentul a crescut la 60% [30]. În acest moment, 72% dintre prostatectomiile radicale din SUA sunt efectuate prin chirurgie robotică cu ajutorul da Vinci, iar procentul este în continuă creştere.
Limitarea studiului este folosirea creatininei serice pentru a defini apariţia leziunii acute renale. Prin metode de proteomică, au fost identificaţi biomarkeri serici şi urinari, care promit un diagnostic mai prompt al leziunii acute renale. Aceste biomolecule nu sunt incluse încă în criteriile de diagnostic.
Concluzii
Funcţia renală se modifică în chirurgia robotică, diferenţa dintre creatinina serică din ziua 1 postoperator şi valoarea bazală este semnificativă statistic (p<0,005).
Leziunea renală acută apare şi după intervenţii chirurgicale robotice, în procent comparabil cu alte intervenţii chirurgicale majore din literatura de specialitate.
Afectarea funcţiei renale este tranzitorie, nu este diferenţă semnificativă statistic între valorile creatininei serice din ziua a patra postoperator şi valorile bazale.
Referinţe
1. Bagshaw SM, George C, Dinu I, et al. A multi-centre evaluation of the RIFLE criteria for early acute kidney injury in critically ill pacients. Nephrol Dial Transplant 2008;23:1203-10.
2. Ostermann M, Chang RWS. Acute kidney injury in the intensive care unit according to RIFLE. Crit Care Med. 2007;35:1837-43.
3. Bellamo R, Ronco C, Kellum JA, et al. Acute renal failure: Definition, outcome measures, animal models, fluid therapy and information technology needs. The second International Consensus Conference of the ADQI Group. Crit Care 2004;8:204-12.
4. Kellum JA. Defining and classifying AKI: one set of criteria. Nephrol Dial Transplant 2008;23(5):1471-72.
5. Bagshaw SM, George C, Bellomo R. A comparison of the RIFLE and AKIN criteria for acute kidney injury in critically ill patients. Nephrol Dial Transplant 2008;23(5):1569-74.
6. Ali T, Khan I, Simpson W, et al. Incidence and outcomes in acute kidney injury: a comprehensive population-base study. J Am Soc Nephrol 2007;18(4):1292-8.
7. Chen YC, Jeng CC, Tian YC, et al. Rifle classification for prdicting in-hospital mortality in critically ill sepsis patients. Shock 2009;31(2):139-45.
8. Levin A, Warnock DG, Mehta RL,et al.Acute Kidney Injury Network Working Group. Improving outcomes from acute kidney injury: report of an initiative. Am J Kidney Dis 2007;50(1):1-4.
9. Davies BL, Hibberd RD, Coptcoat MJ, Wickham JEA. A surgeon robot prostatectomy-a laboratory evaluation. J Med Eng Technol 1989;13:273-277.
10. Rocco B, Matei DV, Melegari S, et al. Robotic vs open prostatectomy in a laparoscopically naive centre: a matched-pair analysis. BJU Int 2009;104(7):991-5.
11. Hanly EJ, Zand J, Bachman SL, Marohn MR, Talamini MA. Value of the SAGES learning center in introducing new technology. Surg Endosc 2005;19(4):477-83.
12. Marescaux J, Leroy J, Gagner M, et al. Transatlantic robot-assisted telesurgery. Nature 2001;413:379-80.
13. Talamini MA, Chapman S, Horgan S, Melvin WS, for the Academic Robotics Group. A prospective analysis of 211 robotic-assisted surgical procedures. Surg Endosc 2003;17:1521-4.
14. Giulianotti PC, Coratti A, Angelini M, et al. Robotics in general surgery: personal experience in a large community hospital. Arch Surg 2003;138:777-84.
15. Marescaux J, Soler L. Image-guided robotic surgery. Semin Laparosc Surg 2004; 11:113-22.
16. Bolenz C, Gupta A, Hotze T, et al. Cost comparison of robotic, laparoscopic, and open radical prostatectomy for prostate cancer. Eur Urol 2010;57:453-8.
17. Barbash GI, Glied SA. New technology and health care costs: The case of robot-assisted surgery. N Engl J Med 2010;363:701-4.
18. Lopes A, Fernandes P, Jorge Sofia et al. Acute kidney injury in intensive care unit patients: a comparison between the RIFLE and AKIN classifications. Clin J Am Soc Nephrol 2010;5:402-8.
19. Guzzo TJ, Dluzniewski P, Orosco R, Platz EA, Partin AW, Han M. Prediction of mortality after radical prostatectomy by Charlson comorbidity index. Urology 2010;76(3):553-7.
20. Wong DT, Crofts SL, Gomez M, McGuire GP, Byrick RJ. Evaluation of predictive ability of APACHE II system and hospital outcome in Canadian intensive care unit patients. Crit Care Med 1995;23(7):1177-83.
21. Vincent JL, Moreno R, Takala J, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to

ORIgInAL ARTIcLEs
Mihály et al96
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
describe organ dysfunction/ failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Cere Med 1996;22(7):707-10.
22. .Khan M, Rooh-ul-Muqim, Zarin M, Khalil J, Salman M.J. Influence of ASA score and Charlson Comorbidity Index on the surgical site infection rates. Coll Physicians Surg Pak. 2010;20(8):506-9.
23. Jäntschi L, Bolboacă SD. Exact Probabilities and Confidence Limits for Binomial Samples: Applied to the Difference between Two Proportions. The Scientific World Journal. 2010;10:865-78.
24. Kolmogorov A. Confidence Limits for an Unknown Distribution Function. The Annals of Mathematical Statistics 1941;12(4):461-3.
25. Smirnov NV. Tables for estimating the goodness of fit of empirical distributions. Ann Math Statist 1948;19(2):279-81.
26. Lopes JA, Jorge S, Silva S, et al. An assesment of the RIFLE criteria for acute renal failure following myeloablative autologous and allogeneic haematopoietic cell transplantation. One Marrow Trnsplant 2006;38:395.
27. Lopes JA, Jorge S, Neves FC, et al. An assessment of the RIFLE criteria for acute renal failure in severely burned patients. Nephrol Dial Transplant 2007;22:285.
28. O’Riordan A, Wong V, McQuillan R, et al. Acute renal disease, as defined by the RIFLE criteria, post-liver transplantation. Am J Transplant 2007;7:168-76.
29. Lopes JA, Jorge S, Resina C, et al. Prognostic utility of RIFLE for acute renal failure in patiets with sepsis. Crit Care 2007;11:408.
30. Ho C, Tsakonas E, Tran K, et al. Robot-Assisted Surgery Compared with Open Surgery and Laparoscopic Surgery: Clinical Effectiveness and Economic Analyses [Internet]. Ottawa: Canadian Agency for Drugs and Technologies in Health (CADTH); 2011 (Technology report no. 137).

The Prognostic Value Of Serum Amyloid A Levels In Patients With Rheumatoid Arthritis 97
Rezumat
Introducere: Mecanismele patogene în poliartrita reumatoidă (PR) sunt incomplet elucidate. Amiloidul A seric (AAS), un tip de apolipoproteină, este una dintre proteinele de fază acută, sintetizată în principal în ficat de monocitele şi macrofagele activate şi eliberată în sânge. AAS produce leziuni prin degradarea cartilajului.
Obiective: Să evaluăm AAS la pacienţi cu PR comparativ cu lotul martor de subiecţi sănătoşi şi să investigăm valoarea predictivă a AAS privind evoluţia bolii.
Materiale şi metodă: Concentraţia de AAS a fost măsurată la 90 pacienţi (vârsta medie 36,4±12,7 ani, durata medie a bolii 5,3±4,5 ani) şi 100 martori sănătoşi (vârsta medie 35,8±11,2 ani). Concentraţia de AAS a fost măsurată prin imunonefelometrie şi exprimată în mg/dl. Rezultatele au fost analizate statistic folosind testul t Student, p<0,05 (95% IC) fiind considerat statistic semnificativ. Pentru analiza corelaţiei s-a folosit testul Spearman, iar diferenţa între grupuri a fost calculată cu testul Wilcoxon.
Rezultate: Concentraţia de AAS a fost uneori crescută marcat. Concentraţiile de AAS a fost crescute
la 24 din 90 pacienţi PR (26,4%) cu limitele între 2,53 şi 9,86 mg/L, valoarea medie 8,35±0,72 mg/L comparativ cu lotul martor cu limitele între 3,12 şi 5,28 mg/L, valoarea medie 3,93±0,47 mg/L; p<0,01. Nivelurile de ASS crescute în PR indică corelaţia directă cu agravarea bolii (r=0,67; p<0,001). S-au demonstrat corelaţii semnificative cu alţi parametri de fază acută ca de exemplu proteina C reactivă (CRP) şi viteza de sedimentare a eritrocitelor (VSH) (r=0,54, p<0,01).
Concluzie: Rezultatele sugerează că AAS este un marker mai sensibil decât CRP şi VSH. În PR, AAS se corelează cel mai strâns cu activitatea bolii, variaţiile în ser reflectă cel mai bine evoluţia clinică.
Cuvinte cheie: amiloidul A seric, poliartrita reumatoidă, inflamaţie, activitatea bolii
Introducere
Amiloidul A seric (AAS) este o proteină importantă de fază acută care se eliberează în circulaţie ca urmare a leziunii. Poliartrita reumatoidă prezintă o evoluţie foarte heterogenă. S-a sugerat că AAS reprezintă cel mai sensibil parametru al reacţiei de fază acută [1].
ORIgInAL ARTIcLEs
VAloAReA pRoGnosticĂ A niVeluRiloR seRice de AMiloid-A lA pAcienŢi cu poliARtRitĂ ReuMAtoidĂ
Cojocaru Manole1,2, Ghinescu Minerva Claudia1, Bălăeţ Constantin1, Cojocaru Inimioara Mihaela3, Siloşi Isabela4
1Universitatea Titu Maiorescu, Facultatea de Medicină, Departamentul de Fiziologie, 2Centrul de Reumatologie Dr. Ion Stoia, Bucureşti, 3Universitatea de Medicină şi Farmacie Carol Davila, Departamentul de Neurologie Prof. Gheorghe Marinescu, Spitalul Clinic Colentina, Bucureşti, 4Universitatea de Medicină şi Farmacie, Departamentul de Imunologie, Craiova, România
Adresa pentru corespondenţă:Cojocaru Manole MD, PhD Str. Thomas Masaryk Nr 5., Sector 2, Cod Poştal 020983 Bucureşti, România Email: [email protected] Primit: 16.06.2012 Acceptat: 15.09.2012 Med Con October 2012, Vol 7, No 3, 97-99

ORIgInAL ARTIcLEs
Cojocaru et al98
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
AAS induce efecte prin degradarea cartilajului. Până relativ recent, viteza de sedimentare a eritrocitelor (VSH) şi concentraţia de proteină C reactivă (CRP) erau folosite pentru monitorizarea clinică a inflamaţiei [2].
AAS este produs de sinoviocite, macrofage şi celule endoteliale. Acesta este foarte util pentru monitorizarea activităţii bolii reumatologice, precum PR. Amiloidoza secundară reactivă se caracterizează prin acumularea extracelulară în diferite ţesuturi de amiloid. Aceste depozite sunt insolubile şi rezistente la proteoliză, distrug structura ţesutului şi compromit funcţia. Creşterea atât de CRP cât şi de AAS a fost asociată cu activitatea bolii [3].
Obiectivele studiului: să evaluăm AAS la pacienţi cu PR comparativ cu subiecţi sănătoşi şi să investigăm valoarea predictivă a AAS pentru activitatea bolii.
Material şi metodă
PR a fost diagnosticată folosind criteriile Colegiului American de Reumatologie. Concentraţiile de AAS au fost determinate la 90 pacienţi (vârsta medie 36,4±12,7 ani, durata medie a bolii 5,3±4,5 ani) şi 100 martori sănătoşi (vârsta medie 35,8±11,2 ani). Au fost excluşi pacienţii care au prezentat afecţiuni medicale sau chirurgicale, infecţii recente, traumatisme şi/sau neoplazii, pentru a înlătura orice factor care ar afecta nivelul de AAS. Concentraţiile de AAS au fost măsurate prin imunonefelometrie folosind reactiv N-Latex pentru AAS. Concentraţiile de AAS au fost exprimate în mg/l. Studiul a fost aprobat de Comitetul de Etică Local. Toţi pacienţii şi-au dat consimţământul informat pentru includerea în studiu. Analiza statistică a rezultatelor a fost raportată ca media±DS, comparate folosind testul t Student pentru variabile continue şi analiza chi-pătrat pentru variabile discontinue. Valoarea p<0,05 a fost considerată semnificativă. Pentru analiza corelaţiei s-a folosit testul Spearman, diferenţele între grupe au fost calculate cu testul Wilcoxon.
Rezultate
La unii dintre pacienţi nivelul de AAS a fost crescut marcat. Nivelurile de AAS au fost găsite crescute la 24 din 90 pacienţi cu PR (26,6%), cu limitele între 0,25 şi 0,98 mg/L, valoarea medie 0,83±0,07 mg/l comparativ cu lotul de martori normali cu limitele între 0,31 şi 0,52
mg/l, valoarea medie 0,39±0,06 mg/l; p<0,01). Nivelurile crescute de AAS în PR indică corelaţia directă cu activitatea bolii (r=0,67; p<0,001). S-au demonstrat corelaţii semnificative cu alţi parametri ai fazei acute precum CRP and ESR (r=0,54, p<0,01).
Discuţii
Studiul demonstrează importanţa măsurării nivelurilor de AAS, marker al inflamaţiei în PR. În PR, nivelurile de AAS indică o corelaţie strânsă cu activitatea clinică a bolii şi variaţiile nivelurilor în ser reflectă cel mai bine evoluţia clinică [1].
S-a sugerat că nivelurile de AAS reprezintă un parametru mai sensibil al reacţiei de fază acută. Răspunsul organismului la injurie şi infecţie se asociază cu creşterea rapidă în sânge a proteinelor de fază acută, precum AAS. Dozarea AAS se foloseşte ca marker pentru bolile inflamatorii, importanţa acestuia în modularea inflamaţiei şi imunităţii nu este încă elucidată complet [2].
Efectele AAS asupra producerii de proteaze sunt importante din cauză că în PR reacţia de fază acută este puternic asociată cu distrugerea progresivă a articulaţiei. Valoarea măsurării nivelului de AAS ca marker al inflamaţiei reprezintă un parametru mai sensibil al reacţiei de fază acută în PR. Se impune să explorăm în viitor această relaţie, în special la pacienţi cu PR mai puţin avansată [3].
În PR, nivelurile de AAS indică corelaţii strânse cu semnele clinice de activitate a bolii, variaţiile nivelurilor serice reflectând cel mai bine evoluţia clinică. În plus, AAS stimulează producerea de către sinoviocite de proteaze care degradează cartilajul. Sub influenţa
Figura 1. Valoarea medie a concentraţiei de amiloid A seric la pacienţi cu poliartrită reumatoidă comparativ cu lotul martor de subiecţi sănătoşi

ORIgInAL ARTIcLEs
The Prognostic Value Of Serum Amyloid A Levels In Patients With Rheumatoid Arthritis 99
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
interleukinei inflamatoare (IL)-6 şi transcrierii hepatice a acidului ribonucleic mesager (mRNA), AAS creşte de 1000 de ori când este prezent un stimul inflamator. Producerea de AAS este indusă în principal de IL-6, IL-1 şi factorul de necroză tumorală (TNF-a). AAS este sintetizat în principal la nivelul ficatului, dar producerea extrahepatică a fost demonstrată la multe specii, precum şi la om [4].
În plus, AAS este implicat atât ca factor benefic cât şi dăunător în procesul inflamator. Alături de rolul în amiloidoză şi homeostazia lipidică în timpul fazei acute, recent s-a observat că AAS contribuie la distrugerea osului şi cartilajului. AAS este precursor al amiloidului A, care depozitându-se determină amiloidoza. Descoperirea că AAS este produs local în artrită sugerează rolul potential al acestei proteine de fază acută în bolile inflamatorii cronice precum PR [5].
În ciuda acestor descoperiri importante, funcţia exactă a AAS în inflamaţia acută nu a fost încă definită. Numeroase studii sugerează o legătură între AAS şi acumularea de leucocite la nivelul inflamaţiei. AAS este chemotactic pentru leucocite, precum monocite, bazofile, limfocite T în timpul răspunsului de fază acută. De asemenea, există numeroase dovezi care indică că AAS posedă activităţi asemănătoare citokinelor, capabile să inducă producerea de metaloproteinaze matriceale (MMP) [3].
Concluzie
Creşterea marcată a amiloidului A seric este folosită ca semn important pentru diagnosticul şi prognosticul bolii inflamatorii. Studiul relevă că nivelul mai crescut
de AAS este un semn al agravării şi joacă un rol important în patogenia PR. AAS duce la producerea de către sinoviocite de proteaze care degradează cartilajul. Nivelurile de AAS se corelează cu activitatea bolii, scad odată cu ameliorarea bolii.
Conflict de interese: autorii care au participat la studiu nu au nimic de declarat privind fondurile sau conflicte de interese în ceea ce priveşte articolul publicat.
Referinţe
1. Cunnane G, Grehan S, Geoghegan S, et al. Serum amyloid A in the assessment of early inflammatory arthritis. J Rheumatol 2000;27:58-63.
2. Sheldon J. Laboratory testing in autoimmune rheumatic diseases. Best Pract Res Clin Rheumatol 2004,18:249-69.
3. Shovman O, Gilburd B, Shoenfeld Y, et al: The diagnostic utility of anti-cyclic citrullinated peptide antibodies, matrix metalloproteinase-3, rheumatoid factor, erythrocyte sedimentation rate, and C-reactive protein in patients with erosive and non-erosive rheumatoid arthritis. Clin Devel Immunol 2005, 12:(3):197-202.
4. Kushner I. Acute phase proteins. In: BD Rose, editor, UPTODATE. Waltham, MA 2006 [Published as CD and online.]
5. Makovitzky J. The nature of the localized meniscus amyloid. In: Bely M, Apathy A, editors. Amyloid and amyloidosis: proceedings of the IXth International Symposium on Amyloidosis, Budapest, Hungary, 2001. p. 409–11.

Bicornate uterus (US)
Abdominal x ray, colon (XR)

Parent’s Attitude Toward The Sex Education That Their Children Learn At School 101
Rezumat
Scopul acestui studiu a fost de a examina atitudinea părinţilor faţă de educaţia sexuală pe care copiii lor o primesc la şcoală. Rezultatele au arătat că majoritatea părinţilor cred că educaţia sexuală ar trebui să fie obligatorie, copii trebuind să fie educaţi să evite contactele sexuale până la căsătorie; că educaţia sexuală încurajează copiii să facă sex în condiţii de siguranţă, dar de asemenea îi încurajează să facă sex; că problemele care nu sunt direct legate de sex ar trebui să fie predate în gimnaziu, în timp ce acelea direct legate de actul sexual ar trebui să fie predate în liceu şi că homosexualitatea ar trebui să fie predată fără a fi definită ca bună sau rea. Au fost constatate diferenţe semnificative între părinţii musulmani şi creştini cu privire la atitudinea lor faţă de educaţia sexuală.
Cuvinte cheie: atitudini parentale, educaţia sexuală, sectorul arab din Israel, musulmani, creştini, şcoală
Introducere
Sexualitatea este o componentă esenţială a dezvoltării sănătoase a tinerilor. În ciuda importanţei
sănătăţii sexuale, recunoscute pe scară largă, educaţia pentru a o promova rămâne o problemă sensibilă şi uneori controversată [1]. Educaţia sexuală în şcoli ar trebui să trateze valorile sociale şi familiale cu respect şi profesionalism [2].
Sexualitatea este probabil cel mai puternic aspect al vieţii umane, care cuprinde nu numai un act de intimitate fizică între două persoane, dar de asemenea şi potenţialul de a crea o nouă viaţă. Sexualitatea este mai mult decât un simplu act de unire a două corpuri, mai mult decât un act fizic. Sexualitatea comunică ceva altora dar şi nouă, despre ce fel de persoane suntem [3].
Este într-adevăr o ironie că în timp ce sexul reprezintă un aspect de asemenea importaţă în vieţile noastre, în Israel părinţii, vârstnicii şi profesorii cu greu pot juca un rol semnificativ în furnizarea de cunoştinţe ştiinţifice. Să vorbeşti despre sex este interzis în societatea arabă din Israel, mai ales în societatea musulmană, iar un adolescent nu-şi poate aborda liber părinţii pentru îndrumare. Cei care caută îndrumare sexuală din partea părinţilor nu sunt satisfăcuţi, deoarece aceştia încerca să se sustragă de la discuţie, sau nu sunt în măsură să dea răspunsuri satisfăcătoare [4]. Sexul este probabil un
ORIgInAL ARTIcLEs
AtitudineA pĂRinŢiloR FAŢĂ de educAŢiA seXuAlĂ pe cARe copii loR o pRiMesc lA şcoAlĂ
Joubran Samia1, Marcus Ohad2, Iancu Iulian3,8, Hartman Tova4, Abraham Weizman5,8, Rath-Wolfson Lea6,8, Ram Edward7,8
1Facultatea de Medicină Bruce Rappaport, Institutul Tehnologic Technion şi Centrul Medical Emek, 2Catedra de Psihologie, Colegiul Valea Yezreel, 3Clinica de Sănătate Mintală Yavne, 4Departamentul de Educaţie şi Sexologie, Universitatea Bar-Ilan Israel, 5Centrul de Sănătate Mentală Geha, Petah Tikva, Israel, 6Departamentul de Patologie, Spitalul Hasharon, Centrul Medical Rabin, 7Divizia de Chirurgie Generală, Spitalul Hasharon, Centrul Medical Rabin, 8Facultatea de Medicină Sackler, Universitatea din Tel Aviv, Israel
Adresa pentru corespondenţă:Edward Ram Division of General Surgery, Rabin Medical Center-Campus Golda Petach Tikva, Keren Kayemet st.7 Tel: 972-3-9372323, Fax: 972-3-9372401 E-mail: [email protected] Primit: 04.07.2012 Acceptat: 15.09.2012 Med Con October 2012, Vol 7, No 3, 101-108

ORIgInAL ARTIcLEs
Joubran et al102
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
domeniu al vieţii noastre despre care ştim foarte puţin şi dacă se întâmplă să ştim câte ceva, este învăţatat trunchiat şi fragmentar de la surse cum ar fi prieteni, filme pornografice şi cărţi [6,7].
Majoritatea adolescenţilor nu au acces la mai multe informaţii; ei primesc informaţii inexacte iar aceste mituri şi concepţii greşite sunt purtate de-a lungul vieţii lor. Există o nevoie de a oferi adolescenţilor informaţii, astfel încât să le permită să facă faţă mai bine schimbăriii pe care sexul îl reprezintă în viaţa lor. Deşi există nevoia de a face educaţie sexuală adolescenţilor, de multe ori părinţii se opun la astfel de programe educaţionale din cauza fricii că oferirea educaţiei sexuale poate duce la experimentare sexuală [7]. Părinţii pot avea o influenţă importantă asupra comportamentelor sexuale ale copiilor lor. Studiile indică faptul că relaţiile de suport părinte-copil precum şi monitorizarea şi supravegherea părintească sunt asociate cu întârzierea activităţii sexuale în rândul copiilor [8].
Statul Israel are aproximativ 7,4 milioane de locuitori. Caracteristica cea mai importantă a populaţiei Israelului este diversitatea sa ridicată. Pe lângă diviziunea principală a locuitorilor ţării în evrei (80%) şi arabi (20%), există mult mai multe subdiviziuni.
Datorită importanţei religiei ca sistem de credinţă şi etică şi mai presus de toate ca structură de existenţă, sexualitatea ocupă atenţia multor religii deoarece aceasta oferă o modalitate puternică de a organiza şi relaţiona fiinţele umane. Religiile încearcă să creeze ordine şi scop prin interrelaţionarea fiinţelor umane în asociaţii mai largi, cum ar fi familiile şi colectivele sociale [3].
Explicarea anatomiei şi a fenomenelor de modificare a corpului în timpul pubertăţii este esenţială pentru a permite tinerilor să crească cu o imagine de sine sănătoasă. Întro eră în care activitatea sexuală în multe ţări începe de la o vârstă fragedă, adolescenţii musulmani trebuie să fie informaţi pentru a le permite să facă faţă mai bine presiunii de grup. Educaţia sexuală poate fi predată întrun mod care să informeze tinerii despre sexualitate din punct de vedere ştiinţific şi moral [9].
Primul program de educaţie sexuală pentru cetăţenii arabi a fost publicat în 1996 de către Ministerul Educaţiei. Acest program a dezbătut educaţia vieţii de familie şi educaţia sexuală, vizând împărtăşirea cunoştinţelor, aptitudinilor, precum şi înţelegerea modului de abordare a subiectului sexual. Programul are 12 capitole de subiecte teoretice şi activităţi care includ aceste subiecte: educaţia sexuală şi educaţia pentru viaţa de familie bună, adolescenţa, relaţia dintre părinţi şi adolescenţi, corpul, procesul de luare a deciziilor, prietenia, prejudecăţile, educaţia şi siguranţa de sine, presiunea celor de aceeaşi generaţie, tradiţia şi obiceiurile, SIDA şi bolile cu transmitere sexuală [10].
În acest studiu am dorit să vedem dacă există o corelaţie între religia părinţilor (musulmani sau creştini) şi atitudinea lor faţă de educaţia sexuală.
Materiale şi metode
Cu scopul de a atinge acest obiectiv am compus un chestionar care a fost trimis părinţilor copiilor.
Chestionar Studiul s-a bazat pe chestionare elaborate de Blendon
R [11], care au conţinut întrebări care examinau atitudinea părintelui faţă de educaţia sexuală, împărţite în mai multe secţiuni. Chestionarul a fost tradus în arabă (traducere dublă) şi a fost aprobat de către un specialist în limba arabă. Din acest chestionar au fost utilizate cinci întrebări în ceea ce priveşte educaţia sexuală în şcoală:
1. Educaţia sexuală în şcoală ar trebui să fie obligatorie sau opţională?
2. Orele de educaţie sexuală în şcoală învaţă elevii să evite sexul până la căsătorie, sau îi învaţă utilizarea de contraceptive pentru sex înainte de căsătorie?
3. Educaţia sexuală încurajează copiii să aibă contact sexual acum şi îi va încuraja să aibă contact sexual protejat (utilizând contraceptivele), în viitor?
4. Pentru care grupe de vârstă ar trebui să fie predate diferite subiecte ca parte a educaţiei sexuale?
5. Este bine sau rău să se predea subiectul homosexualităţii în educaţia sexuală din şcoală?
Participanţii Acest studiu continuă studiul nostru anterior [12].
Participanţii au fost 797 părinţi israeliano-arabi din întregul Israel, cu vârsta cuprinsă între 20 şi 66 de ani (M=39). Printre ei au fost 371 creştini şi 426 musulmani, 208 bărbaţi şi 589 femei; 533 locuiau în oraşe şi 264 în zone rurale sau sate; 483 cu studii academice (absolvent de colegiu sau universitate) şi 314 non-academici (liceu sau mai puţin). În plus, 545 de participanţi s-au definit ca laici sau tradiţionalişti, iar 252 s-au definit ca religioşi sau foarte religioşi.
Procedură Chestionarele au fost furnizate administratorilor
şcolilor din toată ţara, care le-au trimis părinţilor din şcoala lor randomizat şi anonim. Chestionarele completate anonim au fost trimise înapoi investigatorilor prin e-mail. Din 1000 de chestionare au fost returnate 797, rata de răspuns de 79,7% reprezentând o rată de răspuns ridicată pentru comunitatea arabă.
Rezultate
Ca răspuns la întrebarea 1- ar trebui să educaţia sexuală în şcoală să fie obligatorie sau opţională?- rezultatele au indicat că 76,1% dintre părinţi cred că

ORIgInAL ARTIcLEs
Parent’s Attitude Toward The Sex Education That Their Children Learn At School 103
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
educaţia sexuală ar trebui să fie obligatorie şi doar 23,9% cred că ar trebui să fie opţională.
Nu a fost nicio corelaţie semnificativă între credinţa unui părinte despre educaţia sexuală obligatorie şi religia lui/ei [χ2
(1)=1,87, n.s.]. Cu toate acestea, atunci când am analizat în funcţie de religie a existat o corelaţie slabă (Φ=0,16) şi semnificativă între convingerile părinţilor musulmani despre educaţia sexuală şi sexul acestora [χ2
(1)=10,10, p<0,005]; 78,4% din femeile musulmane cred că educaţia sexuală ar trebui să fie obligatorie (21,6% cred că ar trebui să fie opţională), în timp ce 62,6% dintre bărbaţii musulmani cred că educaţia sexuală ar trebui să fie obligatorie (37,4 % cred că ar trebui să fie opţională).
De asemenea, a existat o slabă (Φ=0,16) şi semnificativă corelaţie între convingerile părinţilor creştini despre educaţia sexuală obligatorie şi sexul acestora [χ2
(1)=7,57, p<0,01]; 81,8% din femeile creştine cred că educaţia sexuală ar trebui să fie obligatorie (18,2% cred că ar trebui să fie opţională), în timp ce 67,8% dintre bărbaţii creştini cred că educaţia sexuală ar trebui să fie obligatorie (32,2% cred că ar trebui să fie opţională).
Am găsit, de asemenea, o slabă (Φ=0,12) şi semnificativă corelaţie între convingerile părinţilor creştini despre obligativitatea educaţiei sexuale şi locul de reşedinţă al acestora [χ2
(1)=5,29, p<0,05]. Dintre orăşenii creştini, 81,2% cred că educaţia sexuală ar trebui să fie obligatorie (18,8% cred că ar trebui să fie opţională). Dintre creştinii care trăiesc în sate, 70% cred că educaţia sexuală ar trebui să fie obligatorie (30% cred că ar trebui să fie opţională). Nu a fost nicio corelaţie semnificativă între convingerile părinţilor musulmani despre obligativitatea educaţiei sexuale şi locul de reşedinţă al acestora [χ2
(1)=2,47, n.s.].Nu a fost nicio corelaţie semnificativă între
convingerile părinţilor cu privire la educaţia sexuală obligatorie şi gradul lor de religiozitate, fie pentru părinţii musulmani [χ2
(1)=0,05, n.s.], fie pentru părinţii creştini [χ2
(1)=0,01, n.s.]. Nu a fost, de asemenea, nicio corelaţie semnificativă între convingerile părinţilor cu privire la educaţia sexuală obligatorie şi gradul lor de educaţie, fie pentru musulmani [χ2
(1)=2,79, n.s.], fie pentru părinţii creştini [χ2
(1)=0,32, n.s.].Figura 1 rezumă toate aceste
rezultate, semnificative sau nesemnificative, care demonstrează în mod clar că cei
mai mulţi părinţi, indiferent de apartenenţa religioasă, locul de reşedinţă, gradul de religiozitate sau nivelul de educaţie, cred că educaţia sexuală ar trebui să fie obligatorie. Credinţa în educaţia sexuală obligatorie este mai mare în rândul femeilor decât în rândul bărbaţilor, atât pentru părinţii musulmani cât şi pentru cei creştini.
Pentru a doua întrebare – dacă orele de educaţie sexuală în şcoală învaţă elevii să evite sexul până la căsătorie, sau îi învaţă utilizarea de contraceptive când fac sex înainte de căsătorie? – 73% dintre părinţi cred că educaţia sexuală ar trebui să încurajeze elevii să evite contactul sexual până la căsătorie, în timp ce doar 23% cred că educaţia sexuală ar trebui să furnizeze informaţii cu privire la controlul naşterilor.
A fost o slabă (Φ=0,18) şi semnificativă corelaţie între atitudinea părinţilor faţă de educaţia sexuală a copiilor şi religia lor [χ2
(1)=21,07, p<0,001]. În rândul părinţilor musulmani, 80% cred că educaţia sexuală ar trebui să încurajeze elevii să evite contactul sexual până la căsătorie şi 20% sunt de părere că ar trebui să furnizeze informaţii cu privire la controlul sarcinilor. Printre părinţii creştini, 64% cred că educaţia sexuală ar trebui să încurajeze elevii să evite contactul sexual până la căsătorie şi 36% cred că ar trebui să furnizeze informaţii cu privire la controlul sarcinilor.
Când cele două grupuri religioase au fost analizate separat, a existat o slabă (Φ=0,17) şi semnificativă corelaţie între atitudinile părinţilor musulmani faţă de educaţia sexuală a copiilor lor şi gradul lor de religiozitate [χ2
(3)=29,55, p<0,001]; 88,1% dintre părinţii musulmani religioşi cred că educaţia sexuală ar trebui să încurajeze elevii să evite contactele sexuale până la căsătorie, iar 11,9% cred că ar trebui să furnizeze informaţii cu privire la controlul naşterilor, în timp ce 74,4% din părinţii musulmani seculari cred că educaţia
Figura 1. Convingerile părinţilor despre educaţia sexuală, dacă ar trebui să fie obligatorie sau o alegere, în funcţie de religia lor (musulmană sau creştină) şi în cadrul fiecărei religii în funcţie de sex (masculin sau feminin) şi locul lor de reşedinţă (oraş sau sat)

ORIgInAL ARTIcLEs
Joubran et al104
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
sexuală ar trebui să încurajeze elevii să evite contactele sexuale până la căsătorie şi 25,6% sunt de părere că ar trebui să furnizeze informaţii cu privire la controlul naşterilor.
În plus, atunci când s-a analizat în funcţie de religie a existat corelaţie medie (Φ=0,22) şi semnificativă între atitudinea părinţilor creştini faţă de educaţia sexuală a copiilor lor şi nivelul lor de educaţie [χ2
(1)=13,44, p<0,001]. Dintre părinţii creştini cu educaţie academică, 76,7% cred că educaţia sexuală ar trebui să încurajeze elevii să evite contactul sexual până la căsătorie; 23,3% cred că ar trebui să furnizeze informaţii cu privire la controlul naşterilor. Dintre părinţii creştini fără educaţie academică, 55,7% consideră că educaţia sexuală ar trebui să încurajeze elevii să evite contactul sexual până la căsătorie, iar 44,3% cred că ar trebui să furnizeze informaţii cu privire la controlul naşterilor.
Nu a fost nicio corelaţie semnificativă între atitudinea părinţilor faţă de educaţia sexuală a copiilor lor şi sexul acestora, fie pentru părinţii musulmani [χ2
(1)=3,31, n.s.], fie pentru părinţii creştini [χ2
(1)=0,24, n.s.]. Nu a fost, de asemenea, nicio corelaţie semnificativă între atitudinea părinţilor faţă de educaţia sexuală a copiilor lor şi locul lor de reşedinţă, fie pentru părinţii musulmani [χ2
(1)=0,03, n.s.], fie pentru părinţii creştini [χ2
(1)=0,26, n.s.].Figura 2 rezumă aceste rezultate, care demonstrează
faptul că majoritatea părinţilor cred că educaţia sexuală ar trebui să încurajeze elevii să evite contactul sexual până la căsătorie.
La al treilea set de întrebări, dacă educaţia sexuală încurajează copiii să aibă relaţii sexuale şi dacă aceasta îi va încuraja să aibă contact sexual în condiţii de siguranţă în viitor, am constatat că 66% dintre părinţi cred că educaţia sexuală îi încurajează pe copii să aibă contact sexual şi 34% nu; 91,9% dintre părinţi cred că educaţia sexuală încurajează copiii sa aibă relaţii sexuale în condiţii de siguranţă în viitor (iar 8,1% nu).
În ceea ce priveşte credinţa părinţilor că predarea educaţiei sexuale va încuraja copiii lor să aibă relaţii sexuale, nu am găsit nicio corelaţie semnificativă între această credinţă şi religia lor [χ2
(1)=0,81, n.s.]. Când am analizat pe religii, cu toate acestea, a existat o slabă (Φ=0,19) şi semnificativă corelaţie între credinţa părinţilor musulmani că educaţia sexuală va încuraja copiii lor să aibă relaţii sexuale şi locul lor de reşedinţă [χ2
(1)=11,63,
p<0,005]; 75,3% din musulmanii care trăiesc la oraş cred că educaţia sexuală va încuraja copiii să aibă contact sexual, iar 24,7% nu, în timp ce 57,4% din musulmanii care trăiesc în sate cred că predarea educaţiei sexuale va încuraja copiii să aibă contact sexual, în timp ce 42,6% nu.
A fost o corelaţie slabă (Φ=0,24) şi semnificativă între credinţa părinţilor musulmani că educaţia sexuală va încuraja copiii să aibă relaţii sexuale şi nivelul de educaţie [χ2
(1)=18,98, p<0,001]. Printre musulmani cu studii universitare 81,2% consideră că educaţia sexuală va încuraja copiii să aibă contact sexual, iar 18,8% nu, în timp ce în rândul musulmanilor fără studii universitare 58,2% cred că educaţia sexuală va încuraja copiii să aibă relaţii sexuale, iar 41,8% nu.
Nu a fost nicio corelaţie semnificativă între convingerile părinţilor creştini că educaţia sexuală va încuraja copiii să aibă relaţii sexuale şi locul de reşedinţă al acestora [χ2
(1)=1,42, n.s.], între credinţa părinţilor creştini că educaţia sexuală va încuraja copiii să aibă relaţii sexuale şi nivelul lor de educaţie [χ2
(1)=2,30, n.s.], între credinţa părinţilor că educaţia sexuală va încuraja copiii să aibă relaţii sexuale şi sexul acestora, fie pentru părinţii musulmani [χ2
(1)=3,65, n.s.], fie pentru părinţii creştini [χ2
(1)=2,24, n.s.] şi între credinţa părinţilor că educaţia sexuală va încuraja copiii să aibă relaţii sexuale şi gradul lor de religiozitate, fie pentru părinţii musulmani [χ2
(1)=0,33, n.s.], fie pentru părinţii creştini [χ2
(1)=3,34, n.s.].În ceea ce priveşte credinţa părinţilor că educaţia
sexuală va încuraja copiii să aibă contact sexual în condiţii de siguranţă în viitor, am găsit o slabă (Φ=0,10) şi semnificativă corelaţie între această credinţă şi religia lor [χ2
(1)=6,25, p<0,05], astfel că 89,2% dintre părinţii musulmani cred că educaţia sexuală va încuraja copiii să aibă relaţii sexuale în condiţii de siguranţă în viitor iar 10,8% nu, în timp ce 94,8% din părinţii creştini cred că
Figura 2. Atitudinea părinţilor faţă de educaţia sexuală în funcţie de religia lor (musulmană sau creştină) şi în cadrul fiecărei religii în funcţie de gradul lor de religiozitate (religios sau laic), precum şi de nivelul lor de educaţie (academic sau non-academic)

ORIgInAL ARTIcLEs
Parent’s Attitude Toward The Sex Education That Their Children Learn At School 105
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
educaţia sexuală va încuraja copiii să aibă contact sexual în condiţii de siguranţă în viitor, iar 5,2% nu.
Când s-a analizat pe religii a existat o slabă (Φ=0,18) şi semnificativă corelaţie între credinţa musulmanilor că educaţia sexuală va încuraja copiii să aibă relaţii sexuale şi gradul lor de religiozitate [χ2
(1)=9,54, p<0,005]. Dintre musulmanii religioşi 82,4% cred că educaţia sexuală va încuraja copiii să aibă contact sexual în condiţii de siguranţă în viitor, iar 17,6% nu, în timp ce 93,8% dintre musulmanii seculari cred că educaţia sexuală va încuraja copiii să aibă în condiţii de siguranţă contact sexual în viitor, iar 6,2% nu.
A fost, de asemenea, o slabă (Φ=0,12) şi semnificativă corelaţie între credinţa musulmanilor că educaţia sexuală va încuraja copiii să aibă relaţii sexuale şi nivelul lor de educaţie [χ2
(1)=4,03, p<0,005]. Dintre musulmanii cu studii universitare 91,9% cred că educaţia sexuală va încuraja copiii să aibă contact sexual în condiţii de siguranţă în viitor, iar 8,1% nu, în timp ce 84,4% din musulmanii fără studii universitare cred că educaţia sexuală va încuraja copiii să aibă contact sexual protejat în viitor, iar 15,6% nu.
Nu a existat nicio corelaţie semnificativă între credinţa creştinilor că educaţia sexuală va încuraja copiii să aibă contact sexual în condiţii de siguranţă în viitor şi gradul lor de religiozitate [χ2
(1)=0,53, n.s.], între credinţa creştinilor că educaţia sexuală va încuraja copiii să aibă contact sexual în condiţii de siguranţă în viitor şi nivelul lor de educaţie [χ2
(1)=0,14, n.s.], între credinţa părinţilor că educaţia sexuală va încuraja copiii să aibă relaţii sexuale în condiţii de siguranţă în viitor şi sexul acestora, fie pentru părinţii musulmani [χ2
(1)=1,27, n.s.], fie pentru părinţii creştini [χ2
(1)=1,51, n.s.] şi între credinţa părinţilor că educaţia sexuală va încuraja copiii să aibă relaţii sexuale în condiţii de siguranţă în viitor şi locul lor de reşedinţă,
fie pentru părinţii musulmani [χ2(1)=2,78, n.s.], fie pentru
părinţii creştini [χ2(1)=0,18, n.s.]; Figura 3 rezumă toate
aceste rezultate, semnificative şi nesemnificative. La a patra întrebare -despre oportunitatea
conţinutului pe diferite domenii pentru elevii din şcoala elementară, gimnaziu sau liceu, părinţii ar putea răspunde că un anumit domeniu de conţinut nu ar trebui să fie predat deloc la şcoală; Tabelul I rezumă aceste rezultate.
În cele din urmă am întrebat părinţii dacă educaţia sexuală ar trebui să înveţe că homosexualitatea este acceptabilă, sau ar trebui să înveţe numai ceea ce este homosexualitatea fără a discuta dacă este greşită sau acceptabilă, sau acest subiect nu ar trebui să fie discutat deloc.
Am constatat că 13,8% dintre părinţi cred că educaţia sexuală ar trebui să înveţe că homosexualitatea este acceptabilă, 49,2% cred că homosexualitatea ar trebui să fie predată fără a discuta dacă este acceptabilă sau rea, 31,8% cred că educaţia sexuală ar trebui să înveţe că homosexualitatea este greşită, iar 5,2% cred că homosexualitatea nu trebuie să fie predată deloc. A existat o diferenţă semnificativă între credinţele părinţilor musulmani şi creştini despre predarea homosexualităţii în educaţia sexuală [U(689)=52193, p<0,01]; părinţii musulmani (rangul mediu=363,07) au obiectat la predarea homosexualităţii în educaţia sexuală mai mult decât părinţii creştini (rangul mediu=323,67).
Atunci când am analizat după religie, a existat o diferenţă semnificativă între musulmanii religioşi şi laici în credinţele lor despre predarea homosexualităţii în educaţia sexuală [U(373)=13483, p<0,001]; musulmanii religioşi (rangul mediu=209,12) au obiectat la predarea homosexualităţii mai mult decât musulmanii laici (rangul mediu=170,92).
A fost, de asemenea, o diferenţă semnificativă între creştinii religioşi şi non-religioşi în credinţele lor despre
predarea homosexualităţii în învăţământul sexual [U(316)=6711, p<0,05]; creştinii religioşi (rangul mediu=177,26) au obiectat la predarea homosexualităţii mai mult decât au făcut-o creştinii non-religioşi (rangul mediu=153,92).
Nu a fost nicio diferenţă pe baza sexului părinţilor în credinţele lor în ceea ce priveşte predarea homosexualităţii în educaţia sexuală, fie pentru părinţii musulmani [U(373)=13835, n.s.], fie pentru părinţii creştini [U(316)=9446, n.s.].
Figura 3. Credinţa părinţilor că educaţia sexuală va încuraja copiii să aibă contact sexual şi va încuraja copiii să aibă contact sexual în condiţii de siguranţă în viitor, în funcţie de religia lor (musulmană sau creştină) şi in cadrul fiecărei religii în funcţie de locul de reşedinţă al acestora (oraş sau sat) şi nivelul lor de educaţie (academică sau non-academică)

ORIgInAL ARTIcLEs
Joubran et al106
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
Nu a fost nicio diferenţă pe baza locului de reşedinţă a părinţilor în credinţele lor în ceea ce priveşte homosexualitatea în educaţia sexuală, fie pentru părinţii musulmani [U(373)=16512,5, n.s.], fie pentru părinţii creştini U(316)=8689,5, n.s.].
Nu a fost nicio diferenţă în funcţie de nivelul de educaţie al părinţilor în credinţele lor cu privire la homosexualitate în educaţia sexuală, fie pentru părinţii musulmani [U(373)=15695,5, ns], fie pentru părinţii creştini [U(316)=10543,5, ns]. Deşi majoritatea părinţilor cred că homosexualitatea ar trebui să fie predată în învăţământul sexual fără a se pune întrebarea dacă este corectă sau greşită, mulţi părinţi încă mai cred că este greşit să se predea homosexualitatea în educaţia sexuală, iar în rândul părinţilor religioşi (atât musulmani cât şi creştini) rata opoziţiei este mai mare.
Discuţie
Educaţia este un proces intenţional structurat pentru a împărtăşi cunoştinţe şi abilităţi, precum şi pentru a influenţa cursul de dezvoltare al unui individ [13].
Adolescenţa este o perioadă de libertate crescută de a face alegeri, iar capacitatea adolescentului de a se confrunta cu aceste alegeri şi să ia decizii sănătoase este crucială pentru dezvoltare [14].
Generaţia de astăzi a adolescenţilor este cea mai mare din istorie. Aproape jumătate din populaţia mondială are 25 de ani sau mai puţin. Rezultatele negative ale sarcinii precoce şi ale infecţiilor cu transmitere sexuală ameninţă
sănătatea oamenilor în al doilea deceniu de viaţă mai mult decât în altă grupă de vârstă [15].
Educaţia sexuală permite oamenilor să dobândească cunoştinţe şi să-şi dezvolte abilităţi pe care le pot utiliza pentru a se proteja pe ei şi pe alţii [14]. În Islam, sexualitatea este considerată parte a identităţii unei fiinţe umane: Islamul este explicit cu privire la multe aspecte ale sexualităţii umane. De asemenea, pe baza Hadith-ului care demonstrează disponibilitatea Profetului de a discuta aceste aspecte în mod deschis, ar trebui să fie evident faptul că educaţia cu privire la problemele legate de sex este acceptabilă [9]. Predarea despre sexualitate în sine nu ofensează modestia, iar părinţii sunt îndemnaţi să nu se simtă jenaţi sau timizi faţă de copii lor cu privire la furnizarea de informaţii necesare despre sex [16].
În creştinism biserica este învăţătorul normelor morale şi etice, cu misiunea specială de a păzi şi proteja demnitatea înaltă al căsătoriei şi responsabilitatea cea mai serioasă de perpetuare a vieţii umane. Educaţia sexuală este un drept de bază şi datoria părinţilor, trebuind să fie întotdeauna efectuată sub îndrumarea atentă a acestora, fie la domiciliu, fie în centre educaţionale alese şi controlate de ei. Misiunea de a educa solicită părinţilor creştini să prezinte copiilor lor toate subiectele care sunt necesare pentru maturizarea treptată a personalităţii lor din punct de vedere creştin şi ecleziastic [17].
În ţările cu populaţii foarte diverse, cum ar fi Statele Unite ale Americii, principala limită în dezvoltarea programelor de educaţie sexuală, în special în şcolile publice, este incapacitatea de a selecta o poziţie universal acceptabilă moral [9].
Tabel I. Convingerile părinţilor cu privire la ce subiecte sunt potrivite fiecărui nivel de clasă (elementară, gimnaziu, liceu, sau deloc)
Şcoală elementară Gimnaziu Liceu Deloc
Contracepţia 45.5% 41.2% 12.9% 0.5%SIDA 12.1% 61.1% 26.3% 0.5%Boli sexuale 6.7% 57.3% 34.8% 1.2%Planificarea sarcinii 1.4% 28.2% 57.8% 12.6%Cum să utilizeze metode contraceptive 1.2% 25% 55.1% 18.7%Amânarea sexului până la o vârstă mai mare 6.1% 41.6% 47.1% 5.2%Unde pot verifica pentru boli sexuale 5.1% 35% 52.1% 7.7%Cum să se ocupe chestiuni sensibile 22.6% 60.7% 14.8% 1.8%Amânarea sexului până la căsătorie 2.8% 37.6% 54.4% 5.2%Limitarea partenerul meu 2% 22.7% 54.6% 20.7%Masturbare 12.3% 61.6% 18.6% 7.5%Cum să vorbeşti cu adolescentul despre sex 22.9% 52.6% 21.7% 2.8%Avort 2% 24.1% 49.3% 24.6%Valorile sexuale 10.3% 35.5% 45.8% 8.4%Să utilizeze metode contraceptive fără consimţământul parental 2% 20.9% 38% 39.1%

ORIgInAL ARTIcLEs
Parent’s Attitude Toward The Sex Education That Their Children Learn At School 107
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
În Israel ne confruntăm cu aceeaşi problemă a unei populaţii foarte diverse şi a două naţiuni, având culturi, etnii, limbi şi religii diferite. Ministerul Educaţiei din Israel este responsabil pentru educaţia sexuală în şcoli, astfel încât ministerul are numeroase programe de educaţie sexuală pentru fiecare sector al populaţiei din Israel. Pe parcursul anilor 1973-2005 unitatea de educaţie sexuală a furnizat cincisprezece programe. Cooperarea între sectorul evreiesc religios şi sectorul evreiesc secular a fost foarte limitată; cele două sectoare reprezentând viziuni foarte diferite asupra lumii şi prin urmare programele de educaţie sexuală s-au schimbat frecvent, adresându-se doar câtorva subiecte [18].
În studiul nostru am constatat că majoritatea părinţilor de ambe religii cred că educaţia sexuală ar trebui să fie obligatorie, indiferent de nivelul lor de educaţie sau de gradul de religiozitate. Aceste rezultate sunt în concordanţă cu cele găsite de către McKay [19], care a constatat că în Statele Unite şi Canada mulţi părinţi cer ca educaţia sexuală să fie inclusă în programul şcolar de educaţie, că ar trebui să includă subiecte diverse şi că ar trebui aplicată de la o vârstă fragedă.
Am constatat de asemenea ca mamele ar fi dorit ca educaţia sexuală să fie obligatorie la o rată mai mare decât taţii. În plus, în rândul mamelor am constatat că mamele din mediul urban gândesc că educaţia sexuală ar trebui să fie un subiect obligatoriu mai mult decât mamele din mediul rural.
În populaţia arabă puţine femei muncesc, cele mai multe dintre ele fiind casnice [20]. În consecinţă, femeile în societatea arabă petrec mai mult timp cu copiii lor şi bineînţeles au de a face cu probleme adolescenţei mai mult decât soţii lor. Nu este surprinzător faptul că ele văd educaţia sexuală ca o necesitate, deoarece ar putea servi ca sprijin pentru a le ajuta să se ocupe de problemele adolescenţei. În această ordine de idei, nu este surprinzător faptul că mamele din mediul urban cred că educaţia sexuală ar trebui să fie obligatorie la rate mai mari decât mamele din mediul rural, având în vedere că “sursele de ispită” sunt mult mai disponibile în oraş (cluburi, cafenele, pub-uri şi alte locuri de divertisment ), decât în sate.
Atitudinile parentale în studiul nostru sunt în concordanţă cu concluziile lui Jemmott şi colab. [21], care au demonstrat că programele de educaţie sexuală au redus frecvenţa actelor sexuale în rândul adolescenţilor care au experimentat deja sexul. Pe de altă parte, majoritatea adolescenţilor din studiul lor, care nu experientaseră încă sexul şi care au participat la program, au continuat să se abţină de la sex. În oricare categorie, elevii care au facut sex au fost mult mai predispuşi să utilizeze metode contraceptive. În cercetarea noastră, majoritatea părinţilor au fost în favoarea unei abordări educative axate pe descurajarea
contactului sexual înainte de căsătorie, dar nu au sprijinit educaţia care încuraja utilizarea de contraceptive, deşi această abordare s-a dovedit a fi mult mai eficientă [12].
Opinia publică a comunităţii arabe din Israel susţine abstinenţa ca un obiectiv comportamental pentru adolescenţă [12]. Majoritatea părinţilor în studiul nostru cred că educaţia sexuală ar trebui să încurajeze abstinenţa până la căsătorie. Cercetări anterioare au constatat că reţinerea informaţiilor faţă de tineri creşte doar probabilitatea ca, atunci cand aceştia vor avea contact sexual, acesta va fi neprotejat [22], mai ales dacă puţinele informaţii pe care le-au învăţat au fost dobândite pe cont propriu, fără instruire formală. Având în vedere că media de vârstă la căsătorie este în creştere în mod constant la nivel mondial, rata de relaţii sexuale înainte de căsătorie este de asemenea în creştere [23].
Informaţia despre comportamentul sexual este esenţială pentru îmbunătăţirea sănătăţii sexuale, pentru a corecta mituri despre comportamentul sexual şi să amâne vârsta la care tinerii au prima relaţie sexuală [24].
Predarea educaţiei sexuale în sine nu ofensează modestia, iar părinţii sunt îndemnaţi să nu se simtă timizi cu privire la furnizarea de informaţii necesare despre sex cu copiii lor [25].
De fapt, există dovezi că sexul şi educaţia sexuală, care include distribuirea de prezervative şi contraceptive, este superioară educaţiei pentru abstinenţă în reducerea comportamentului riscant sexual [26].
Iniţierea activităţii sexuale în adolescenţă este însoţită de un risc considerabil pentru boli cu transmisie sexuală (BTS) şi sarcini. Adolescenţii au cel mai mare risc specific de vârstă pentru multe BTS [27], precum şi cea mai mare proporţie specifică vârstei de sarcini neintenţionate, în Statele Unite [28]. În tabuurile culturale din Orientul Mijlociu sunt obstacole majore pentru discuţia informată despre problemele de sănătate sexuală şi reproductivă, în special în ceea ce priveşte adolescenţii. Relaţiile sexuale premaritale sunt interzise; tăcerea în jurul subiectului provine în parte din valoarea maximă pe care societatea o pune pe virginitatea fetei înainte de căsătorie şi convingerea că discuţia deschisă despre sănătatea sexuală şi reproductivă ar putea încuraja tinerii necăsătoriţi să aibă sex premarital. Recenzii ale programelor de educaţie sexuală din întreaga lume au ajuns la concluzia că educaţia sexuală nu încurajează activitatea sexuală timpurie şi poate întârzia de fapt primul contact sexual şi să conducă la utilizarea mai bună a contraceptivelor şi la un act sexual mai sigur [29].
Concluzie
Acest studiu a analizat opiniile părinţilor arabo-israelieni în ceea ce priveşte curriculum-ul educaţiei

ORIgInAL ARTIcLEs
Joubran et al108
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
sexuale în şcolile frecventate de copiii lor. Părinţii au fost de acord asupra unei serii de aspecte abordate în sondaj, însă au existat diferenţe semnificative între părinţii musulmani şi creştini. La toate subiectele incluse în sondaj, musulmanii au exprimat credinţe mult mai conservatoare decât creştinii.
Constatările raportate aici sunt printre puţinele studii efectuate asupra educaţiei sexuale în societatea arabă din Israel. Acesta este primul studiu care analizează diferenţele între populaţia arabă urbană şi cea care trăieşte în zonele rurale, precum şi primul care examinează diferenţele dintre creştini şi musulmani.
Mulţumiri pentru Abhath-Societatea pentru Dezvoltarea Cercetărilor Academice, pentru sprijinul şi ajutorul dat în desfăşurarea acestui studiu.
Referinţe
1. Bay-Cheng LY. The trouble of teen sex: The construction of adolescent sexuality through school-based sexuality education. Sex Education. 2003;3:61-74.
2. Shtarkshall R, Santelli J, Hirsch J. Sex Education and sexual socialization: Role for educators and parents. Perspectives on Sexual and Reproductive Health. 2007;39:116-9.
3. Ellingson S, Green MC, eds. Religion and Sexuality in Cross-Cultural Perspective. New York: Routledge, 2002.
4. Israel Central Bureau of Statistics, 2004. 5. Tjaden P G. Pornography and sex education. Journal of
Sex Research. 1988;24:208-12. 6. Kumar P. Study of sex-related myths in college students.
Journal of Indian Academy of Applied Psychology, 1993;19:21-4.
7. Iwao Hoshii. Sex in Ethics and Law, (Hardcover, 1987) 8. Miller B C, Benson B, Galbraith D. Family
relationships and adolescent pregnancy risk: A research synthesis. Developmental Review. 2001;21:1-38.
9. Muslim Women’s League. An Islamic perspective on sexuality. Retrieved online, 1999. http://www.mwlusa.org/topics/sexuality/sexuality_pos.html
10. Israel Ministry of Education, 1996 11. Blendon R. Sex education in America: General public/
parent’s survey. Cambridge; Harvard University, 2004. 12. Joubran S, Marcus O, Iancu I et al. Parent’s attitude
toward the sex education that their children learn at school. Medical Connections, in press, 2012.
13. Schneewind K A. Socialization and education: Theoretical perspective. In N. J. Smelser & P. B. Baltes (Eds.). International encyclopedia of social and behavioral sciences (pp. 14507-13) sAmterdam, Elsevier, 2001.
14. Beyth-Marom R, Fischhoff B. Adolescents’ decisions about risks: A cognitive perspective. In T. Schulenberg, J. Maggs & K. Hurrelmann (Eds.), Health risks and developmental transition during adolescence (pp. 110-35). Cambridge: Cambridge University Press, 1997.
15. United Nations Population Fund. The state of the world population: Making one billion count investing in adolescents’ health rights. New York: UNFPA, 2006.
16. Noibi, D. An Islamic perspective. In R. Thomason (Ed.). Religion, ethnicity and sex education: Exploring the issues (pp. 41-57), London: National Children’s Bureau 1993.
17. Pope Paul VI. Gravissimum educationis 3, The Vatican, 1965 18. The Knesset Research and Information Center. Sex
education in the school system, 2010. 19. McKay A, Pietrusiak M, Holowaty, P. Parents’ opinions
and attitudes towards sexuality education in the schools. The Canadian Journal of Human Sexuality. 1998;7:139-45.
20. Israel Central Bureau of Statistics, 2009 21. Jemmott B, Jemmott S, Fong T. Abstinence and safer-
sex HIV risk reduction interventions for African-American adolescents: A randomized controlled trial. Journal of the American Medical Association. 1998;279:1529-36.
22. Kirby D. Emerging answers: Research findings on programs to reduce teen pregnancy. Washington, DC; the National Campaign to Prevent Teen and Unplanned Pregnancy, 2007.
23. Ragab A, Mahmoud M. Sex education for young people in Egypt: A community-based study. In The proceeding of a conference; Cairo Demographic Center (pp.559-69), 2006.
24. Wellings K, Collumbine M, Slaymaker E, et al. Sexual behavior in context: A global perspective. Lancet. 2006;368:1706-28.
25. Halstead J. M. Muslims and sex education. Journal of Moral Education. 1997;26:317-30.
26. Harper CC, Henderson AS, Schalet DB, Becker D, Stratton L, Raine TR. Abstinence and teenagers: Prevention counseling practices of health care providers serving high-risk patients in the United States. Perspectives on Sexual and Reproductive Health. 2010;42:25-132.
27. Centers for Disease Control and Prevention. Sexually transmitted disease surveillance. Atlanta. U.S. Department of Health and Human Services, 2004.
28. Institute of Medicine. The best intention: Unintended pregnancy and the well- being of children and families. Washington, DC, National Academy Press, 1995.
29. Kirby D. Impact of sex and HIV education programs on sexual behaviors of youth in developing and developed countries. Family Health International. 2005;2:1-2.
Traducere: Bumbuluţ Călin

The Ankle-Brachial Index In The Diagnosis Of Symptomatic And Asymptomatic Peripheral Arterial Disease 109
Rezumat
Boala arterială periferică (BAP), evoluând asimptomatic în marea majoritate a cazurilor o lungă perioadă de timp, poate fi depistată neinvaziv prin determinarea indicelui gleznă-braţ (IGB).
Scopul lucrării: Am urmărit corelaţiile dintre datele obţinute prin determinarea IGB şi prezenţa BAP, în scopul îmbunătăţirii diagnosticului precoce al afecţiunii, în special al cazurilor asimptomatice.
Material şi metodă: Studiul s-a desfăşurat între 2007-2011 şi a inclus 314 persoane simptomatice sau asimptomatice, cu vârsta peste 50 ani, vârstă medie 61±7 ani, 56% bărbaţi şi 44% femei. Perioada medie de urmărire a fost de 34±6 luni. Acestora li s-a determinat IGB folosind un dispozitiv Doppler, ei fiind supuşi şi unei evaluări detaliate din punct de vedere al factorilor de risc cardiovasculari şi al patologiei asociate.
Rezultate: Valori normale ale IGB între 0,9 şi 1,3 s-au obţinut la 72% din pacienţi şi IGB peste 1,3
a fost întâlnit la 6% din pacienţi, 64% din aceştia fiind diabetici. IGB a confirmat diagnosticul de BAP la 22% din pacienţi, fiind foarte util în detectarea cazurilor asimptomatice de arteriopatii. Prevalenţa BAP a fost mai mare la vârstnici, fumători, diabetici, hipertensivi şi la cei care au asociat mai mulţi factori de risc pentru ateroscleroză. Riscul de evenimente fatale şi nonfatale din grupul pacienţilor cu BAP a fost de aproape 2,5 ori mai mare (RR:2,46 CI:2,04–3,12). S-a observat o asociere inversă între IGB şi numărul de evenimente, pacienţii cu IGB<0,5 prezentând un risc relativ de evenimente cardiovasculare de 5 ori mai mare (RR:5,52 CI:3,61–7,65) faţă de cei cu IGB>0,9.
Concluzii: Determinarea IGB s-a dovedit a fi o investigaţie neinvazivă, accesibilă şi uşor de efectuat în cadrul cabinetului de MF, având o mare importanţă în diagnosticul precoce al BAP.
Cuvinte cheie: indice gleznă-braţ, boală arterială periferică, grosimea intima-medie carotidiană
ORIgInAL ARTIcLEs
iMpoRtAnŢA indicelui GleZnĂ-bRAŢ În diAGnosticul bolii ARteRiAle peRiFeRice siMptoMAtice şi AsiMptoMAtice
Adrian Gruici1, Elena Ardeleanu2, Anca Alexandra Matusz3, Rodica Mihăescu4, Roxana Alăman5,Daniela Gurgus2
1CMI, Timişoara, 2UMFT Victor Babeş, Timişoara, 3Societatea Academică de Medicină de Familie, Timişoara, 4UMFT Victor Babeş, Timişoara, 5Institutul de Boli Cardiovasculare, Timişoara
Adresa pentru corespondenţă:Dr. Adrian Gruici Tel: 0745149849 Email: [email protected] Primit: 05.03.2012 Acceptat: 10.09.2012 Med Con October 2012, Vol 7, No 3, 109-116
Acest studiu este efectuat în cadrul Programului Operaţional Sectorial pentru Dezvoltarea Resurselor Umane (POSDRU) 2007-2013, finanţat din Fondul Social European şi Guvernul României prin contractul nr. POSDRU/107/1.5/S/82839

ORIgInAL ARTIcLEs
Gruici et al110
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
Introducere
Ateroscleroza este o boală de sistem care conduce frecvent la infarct miocardic, accident vascular cerebral, boli ale aortei şi ale arterelor periferice. Boala arterială periferică determinată de ateroscleroza localizată la nivelul membrelor inferioare este un important marker pentru ateroscleroza generalizată şi este strâns asociată cu evenimente cardio- şi cerebrovasculare.
Incidenţa evenimentelor cardiovasculare fatale şi nonfatale este de două-trei ori mai mare la pacienţii cu ateroscleroză la nivelul membrelor inferioare.
Studiile epidemiologice au evidenţiat că prevalenţa bolii arteriale periferice (BAP) în rândul populaţiei generale este de 10%, acest procent dublându-se în cazul pacienţilor cu vârsta peste 70 de ani. Deşi s-a demonstrat că BAP este un factor de prognostic puternic pentru evenimente cardiovasculare viitoare, studiile anterioare au arătat că doar o mică parte din pacienţii cu BAP sunt diagnosticaţi. S-a estimat că pentru fiecare pacient cu BAP simptomatică există alte aproximativ 3-4 cazuri cu BAP nediagnosticată. Atât cazurile de BAP simptomatice cât şi cele silenţioase s-au dovedit a avea un nivel crescut de mortalitate şi morbiditate cardiovasculară. Pacienţii cu BAP prezintă adesea ateroscleroză în alte segmente ale sistemului vascular. Riscul de deces prematur al unui pacient cu BAP este de trei ori mai mare decât al unuia fără afectare vasculară periferică.
Indicele gleznă-braţ este în prezent cea mai frecventă şi utilă metodă de diagnostic folosită pentru depistarea BAP, inclusiv a cazurilor asimptomatice. În plus faţă de valoarea sa diagnostică, indicele gleznă-braţ (IGB) poate fi utilizat şi în evaluarea aterosclerozei generalizate. Studii anterioare au arătat că un IGB≤0,9 are o specificitate de 98% pentru BAP şi o specificitate de 92% pentru predicţia ischemiei miocardice şi a accidentului vascular cerebral.
S-a demonstrat că indivizii cu un IGB≤0,9 sunt de două ori mai predispuşi la boli cardiovasculare, iar bărbaţii cu IGB≤0,9 prezintă un risc de patru ori mai mare de a dezvolta boli cerebrovasculare. Se apreciază că doar 23% din pacienţi sunt simptomatici, marea majoritate a cazurilor de BAP evoluând asimptomatic. În rândul vârstnicilor, un IGB≤0,9 indică prezenţa aterosclerozei subclinice şi este un puternic predictor al mortalităţii totale şi al morbidităţii şi mortalităţii cardiovasculare în rândul celor fără antecedente de boli cardiovasculare.
Medicii de familie pot şi trebuie să joace un rol cheie în diagnosticul şi tratamentul BAP şi ai factorilor săi de risc. Determinarea IGB este o metodă eficientă de diagnostic al BAP şi trebuie inclusă în standardul asistenţei medicale primare.
Obiective
Am urmărit corelaţiile dintre datele obţinute prin determinarea IGB şi prezenţa BAP, în scopul îmbunătăţirii diagnosticului precoce al afecţiunii, în special al cazurilor asimptomatice.
Ne-am propus să comparăm riscul de deces de orice cauză sau riscul de evenimente cardiovasculare majore la pacienţii cu BAP faţă de cei fără BAP.
Un alt obiectiv a constat în evaluarea indivizilor cu IGB scăzut din punct de vedere al factorilor de risc majori pentru boală cardiovasculară. Studiile anterioare au arătat că vârsta înaintată, hipertensiunea arterială, fumatul, diabetul zaharat, hipercolesterolemia şi stilul de viaţă sedentar sunt principalii factori de risc pentru apariţia BAP. În studiul de faţă am investigat IGB întro populaţie prezentând factori de risc pentru BAP.
Material şi metodă
Studiul s-a desfăşurat între 2007-2011 şi a inclus 388 pacienţi de la 9 cabinete de medicină de familie din judeţul Timiş. Perioada medie de urmărire a fost de 34±6 luni. Toţi pacienţii au fost investigaţi neinvaziv pentru boli determinate de ateroscleroză şi factori de risc majori pentru boli cardio- şi cerebrovasculare.
Criteriile de includere în studiu au fost reprezentate de vârstă, între 50-79 ani şi prezenţa unei boli cardiovasculare manifeste sau cel puţin a unui factor de risc major pentru boli cardio- şi cerebrovasculare. Ca factori de risc au fost consideraţi: fumatul, hipertensiunea arterială, diabetul zaharat şi dislipidemia.
Evenimente cardiovasculare majore au fost considerate: infarctul miocardic şi revascularizarea coronariană, angina pectorală stabilă sau instabilă, accidentul vascular cerebral, atacul ischemic tranzitor, revascularizarea la nivelul arterelor carotide sau a membrelor inferioare, precum şi amputaţii datorită BAP în timpul perioadei de urmărire. Scrisorile medicale, biletele de externare, rezultatele analizelor de laborator şi ale investigaţiilor imagistice au fost reţinute de la pacienţii care au prezentat diferite evenimente de interes.
Criteriile de excludere le-au constituit refuzul de a participa la studiu, precum şi afecţiuni care necesită spitalizare, ca de exemplu, diferitele forme de cancer avansat sau alte afecţiuni ameninţătoare de viaţă.
Lotul de studiu iniţial a inclus 388 pacienţi cu vârsta>50 ani, cărora li s-a efectuat o anamneză amănunţită, examen clinic obiectiv, determinarea semnelor vitale, ECG, ecocardiografie, analize de laborator, determinarea indicelui gleznă-braţ şi a grosimii intima-medie carotidiană. Consimţământul

ORIgInAL ARTIcLEs
The Ankle-Brachial Index In The Diagnosis Of Symptomatic And Asymptomatic Peripheral Arterial Disease 111
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
informat a fost obţinut de la fiecare pacient în parte. Anamneza a inclus date despre antecedentele personale patologice, antecedentele heredo-colaterale, medicaţia curentă, consumul de alcool, foşti sau actuali fumători.
Examenul fizic a inclus măsurarea înălţimii, greutăţii, a circumferinţei abdominale şi a indicelui de masă corporală. Pacienţii cu IMC>30kg/m2 au fost consideraţi obezi. Obezitatea abdominală a fost definită conform ghidului National Cholesterol Education Program Adult Treatment Panel III (NCEP-ATP III) ca circumferinţa abdominală >88 cm la femei şi >102 cm la bărbaţi. Tensiunea arterială a fost măsurată cu un tensiometru aneroid în clinostatism şi după 3 minute de ortostatism, împreună cu pulsul periferic. Hipertensiunea arterială a fost definită ca TA sistolică >140 mmHg şi/sau TA diastolică >90 mmHg la două măsurători diferite sau dacă pacientul urma tratament cu medicaţie antihipertensivă. Diabetul zaharat a fost considerat prezent când pacientul urma tratament cu antidiabetice orale sau preparate de insulină, sau a avut glicemia a jeune >126 mg/dl. Au fost încadraţi ca fumători toţi cei care fumează sau au fumat cel puţin o ţigaretă pe zi.
Analizele de laborator. Probele de sânge au fost analizate cu ajutorul unui echipament CardioChek-PA şi al testerelor PTS-Lipid panels (Polymer Technology Systems, Inc. – CardioChek 7736 Zionsville Road, Indianapolis, Indiana 46268 USA), care au oferit rezultate pentru: colesterol total, HDL-colesterol, LDL-colesterol, trigliceride, glicemie şi corpi cetonici. Dislipidemia a fost definită conform ghidului NCEP-ATP III ca valoarea colesterolului total >240 mg/dl, LDL-colesterol >160 mg/dl, sau HDL-colesterol <40 mg/dl, sau utilizarea medicaţiei hipolipemiante.
Examenul de urină a fost efectuat cu ajutorul echipamentului Arkray AutionCheck II şi al testerelor urinare Arkray AutionSticks EB5 (ARKRAY Europe, B.V., Prof. J. H. Bavincklaan 5 1183 AT Amstelveen, The Netherlands). Probele de urină au fost analizate pentru detectarea de glucoză, proteine, creatinină, bilirubină, leucocite, hematii şi nitriţi. Pentru microalbuminurie aceste testere prezintă 5 niveluri de interpretare: negativ, >30 mg/l, >50 mg/l, >100 mg/l, >150 mg/l. Microalbuminuria se defineşte, conform Ghidului HTA al ESH şi ESC din 2007 [1], ca având următoarele valori: 30-300mg/24h sau raport albumină/creatinină>22mg/g (bărbaţi) sau >31mg/g (femei). În studiul nostru, microalbuminuria a fost definită ca orice valoare diferită de cea negativă.
Semnele şi simptomele sugestive pentru boala arterială periferică includ: claudicaţia intermitentă (durere la nivelul musculaturii membrului inferior apărută la mers şi care a dispărut în repaus); absenţa pulsului la nivelul arterelor membrului inferior (artera pedioasă,
artera tibială posterioară sau artera poplitee), ulcer sau gangrenă. Boala arterială periferică asimptomatică a fost definită ca un IGB <0,9 la cel puţin unul dintre membrele inferioare, dar în absenţa claudicaţiei intermitente.
Determinarea indicelui gleznă-braţ (IGB) s-a efectuat cu pacientul în clinostatism după 5 minute de repaus, cu ajutorul unei sonde Doppler continuu cu o frecvenţă de 8 Mhz şi un tensiometru. Se măsoară TA sistolică la nivelul arterelor brahiale [2]. La calculul IGB se foloseşte cea mai mare din valorile obţinute [2]. Se plasează manşeta tensiometrului la nivelul gambei, cât mai aproape de gleznă. Se măsoară TA sistolică la nivelul arterei tibiale posterioare şi la artera pedioasă la ambele membre. Pentru calculul IGB se foloseşte cea mai mare dintre valorile obţinute pentru fiecare membru. Raportul dintre TA sistolică la nivelul gleznei şi TA sistolică la nivelul braţului reprezintă indicele gleznă-braţ şi se calculează pentru fiecare picior în parte. Pacienţii care au acuzat durere la nivelul membrului inferior, apărută la mers, dar cu IGB de repaus normal, au fost supuşi unui test de efort pentru a clarifica diagnosticul [2,3]. Boala arterială periferică a fost diagnosticată când IGB de repaus a fost <0,9, sau dacă, după efort, IGB a scăzut cu >20% din valoarea de repaus la cel puţin un picior [4,5,6].
Determinarea grosimii intima-medie carotidiene (IMT) s-a efectuat la ambele artere carotide, conform
Artera tibială posterioară Artera pedioasă
Figura 1. Tehnica de măsurare a TA la nivelul membrului inferior cu ajutorul sondei Doppler
Figura 2. Tehnica măsurării ecografice a IMT

ORIgInAL ARTIcLEs
Gruici et al112
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
consensului de la Mannheim [10], cu un ecograf Sonoscape SSI-8000, echipat cu o sondă liniară de 10 Mhz. Pacienţii au fost investigaţi în clinostatism, cu capul înclinat la 45° în partea opusă arterei examinate. Când s-a obţinut o imagine longitudinală optimă, a fost “freezată” pe unda R a ECG şi salvată pe hard-disk-ul ecografului. Această procedură s-a repetat de 3 ori pentru fiecare parte. Grosimea intima-medie a fost calculată de un program preinstalat pe ecograf. IMT a rezultat din media celor 6 măsurători efectuate la fiecare pacient.
Explorarea Doppler color a fost utilizată pentru determinarea severităţii hemodinamice a stenozelor arterei carotide. Au fost considerate semnificative stenozele luminale >50% din diametrul secţiunii transversale.
Analiza statistică
Diferenţele dintre pacienţii cu şi fără boală arterială periferică au fost reprezentate cu ajutorul testelor χ2 şi t-student nepereche. P<0,05 a fost considerat semnificativ statistic. Toate intervalele de încredere au fost calculate la un nivel de 95%.
Asocierea posibililor factori de risc (vârstă, sex, hipertensiune, diabet, dislipidemie, sedentarism, fumat) cu apariţia BAP simptomatică şi asimptomatică a fost reprezentată prin analiza de regresie logistică multivariată.
S-au efectuat analizele de regresie uni- şi multivariate Cox pentru calculul riscurilor relative corespunzătoare asocierii BAP cu alţi factori de risc şi al morbidităţii şi mortalităţii cardiovasculare.
Tabel I. Date biologice ale populaţiei de studiu
Caracteristici Lot studiu(n=314)
BAP(n=69)
Fără BAP(n=245) valoareP
TAS (mmHg) 150±22 155±21 145±23 <0,001TAD (mmHg) 91±12 96±10 86±11 <0,001IMC (kg/m2) 27,5±4,5 28,2±5,1 27,4±4,4 0,01Colesterol total (mg/dl) 205±21 209±24 199±22 0,01HDL (mg/dl) 43±8 40±7 42±6 0,01LDL (mg/dl) 137±14 141±15 133±12 0,01Trigliceride (mg/dl) 150±18 155±21 147±18 0,02IMT (mm) 0,97±0,24 1,12 0,78 <0,001Microalbuminurie (%) 17% 22% 15% <0,001
Tabel II. Datele clinice ale lotului studiu
Caracteristici Lot studiu(n=314)
BAP(n=69)
Fără BAP(n=245) valoareaP
Sex (bărbaţi %) 176(56) 38(55) 138(56,3) 0,01Vârstă (ani) 61±7 63±8 60±3 <0,000150-59 (%) 117(37,2) 14(20,2) 103(42)60-60 (%) 124(39,5) 29(42) 95(38,8)70-79 (%) 73(23,2) 26(37,7) 47(19)HTA 231(73,5) 60(87) 171(70) <0,001Diabet Zaharat (%) 108(34,3) 30(43,4) 78(31,8) <0,001Dislipidemie 167(53,1) 42(60,8) 125(51) <0,001Fumători (%) 180(57,4) 50(72,4) 130(53) <0,0001Claudicaţie intermitentă (%) 32(10,2) 15(22,1) 17(7) <0,0001Absenţa puls perif. (%) 25(8) 10(14,5) 15(6,1) <0,0001Ev. Cardiovasculare % 98(31,2) 36(52) 62(25,3) <0,0001Ev.Cerebrovasculare% 39(12,4) 17(24,6) 22(9) <0,0001Nr. factori de risc (%)
1 56(17,8) 5(7,2) 51(20,8)2 133(42,4) 18(26) 115(47)3 89(28,3) 35(50,7) 54(22)4 36(11,5) 11(16) 25(10) <0,0001

ORIgInAL ARTIcLEs
The Ankle-Brachial Index In The Diagnosis Of Symptomatic And Asymptomatic Peripheral Arterial Disease 113
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
Asocierea dintre IGB şi IMT a fost realizată cu ajutorul analizei de regresie liniară, ajustată în funcţie de vârstă şi sex. Am utilizat analiza de regresie logistică pentru a stabili riscul de BAP la pacienţii cu IMT>0,9 mm.
Calculele au fost efectuate cu ajutorul pachetului de programe statistice StatCalc Epi-Info versiunea 6.
Rezultate
Caracteristicile lotului de pacienţi la includerea în studiu
Din lotul iniţial de 388 de pacienţi, 365 au prezentat date complete la analizele clinice şi paraclinice. Criteriile de includere în studiu au fost întrunite de un număr de 314 pacienţi pentru care s-au efectuat analize statistice. Dintre aceştia 176 (56%) au fost bărbaţi, restul populaţiei fiind reprezentat de 138 femei (44%). Vârsta medie a lotului de studiu a fost 61±7 ani. 98 pacienţi (31,2%), majoritatea bărbaţi, au prezentat în antecedente cel puţin un episod de boală cardiovasculară iar 39 (12,4%) au fost cunoscuţi cu boală cerebrovasculară.
În ceea ce priveşte factorii de risc întâlniţi la lotul de studiu, 180 pacienţi (57,4%), în majoritate bărbaţi, sunt foşti sau actuali fumători, 231 (73,5%) sunt cunoscuţi hipertensivi, 108 (34,3%) aflaţi în evidenţă la Centrul de Diabet, iar 167 (53,1%) cunoscuţi cu dislipidemie sau aflaţi sub tratament cu hipolipemiante. Datele clinice şi biologice ale lotului de studiu sunt prezentate în tabelele I şi II.
Din lotul total, 56 pacienţi (17,8%) au prezentat un singur factor de risc, 133 (42,4%) au prezentat doi factori de risc, 89 (28,3%) au prezentat trei factori de risc şi un număr de 36 (11,5%) pacienţi au prezentat chiar patru factori majori de risc pentru boală cardiovasculară.
În urma anamnezei, 32 (10,2%) pacienţi au acuzat durere sau disconfort la nivelul membrelor inferioare, apărute la mers. Dintre aceştia, 15 au relatat dispariţia durerii după 10 minute de repaus (claudicaţie intermitentă). Examenul fizic a evidenţiat absenţa pulsului periferic la nivelul membrelor inferioare la 25 de pacienţi (8%) şi modificări trofice la 19 de pacienţi (6,2%). BAP a fost mult mai frecventă la pacienţii la care pulsul la artera pedioasă sau tibială posterioară a fost absent, sau care au prezentat claudicaţie intermitentă.
Determinarea indicelui gleznă-braţ la lotul de studiuValorile obţinute la măsurarea IGB au variat între
0,38-1,45 cu o medie de 0,98. Valori normale ale IGB între 0,9 şi 1,3 s-au înregistrat la 226 (72%) pacienţi. IGB >1,3 s-a întâlnit la un număr de 19 (6%) pacienţi, 12 (64%) din aceştia fiind diabetici. IGB<0,9 a fost întâlnit la 69 pacienţi (22%), fără diferenţe majore între bărbaţi şi femei (Tabel III).
Tabel III.Valorile obţinute la determinarea indicelui gleznă-braţ
Nr. crt. Indice gleznă braţ Nr. pacienţi Procent (%)1 IGB<0,9 69 222 IGB 0,9-1,3 226 723 IGB >1,3 19 6
Figura 3. Repartizarea lotului de studiu în funcţie de valorile obţinute la determinarea IGB
Figura 4. Distribuţia valorilor obţinute la măsurarea IGB în populaţia studiului
Tabel IV. Clasificarea BAP în funcţie de valorile IGB la lotul de studiu
Nr.crt. Indice gleznă-braţ Nr. pacienţi Procent (%)1 IGB 0,9-0,7 41 59,52 IGB 0,7-0,5 19 27,53 IGB <0,5 9 13,0
Figura 5. Repartiţia pacienţilor cu BAP în funcţie de simptomatologie

ORIgInAL ARTIcLEs
Gruici et al114
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
Tabel VI. Evenimentele cardiovasculare majore fatale şi nonfatale apărute la lotul de studiu în perioada de urmărire
Nr. pacienţi Nr. evenimente Risc relativ Valoare pTotal 314 37BAP 69 15 2,46 (2,04-3,12) <0,001Fără BAP 245 22 1,0IGB>0,9 245 22 1,13 (0,88–1,48) 0,03IGB 0,7-0,9 41 6 1,93 (1,52–2,43) <0,001IGB 0,5-0,7 19 5 3,89 (3,03-5,23) <0,001IGB<0,5 9 4 5,52 (3,61-7,65) <0,001
Tabel V. Factorii de risc asociaţi cu BAP simptomatică şi asimptomatică
Factori de risc Lot BAP(n=69)
BAP asimptomatică(n=54)
BAP simptomatică(n=15) Valoare P
50-59 (%) 14(20,2) 10(18,5) 4(26,7) <0,00160-60 (%) 29(42) 23(42,6) 6(40)70-79 (%) 26(37,7) 21(38,8) 5(33,3)HTA 60(87) 47(87) 13(86,6) <0,001Diabet Zaharat (%) 30(43,4) 23(42,6) 7(46,7) <0,001Dislipidemie 42(60,8) 31(57,4) 11(73,3) <0,001Fumători (%) 50(72,4) 38(70,3) 12(80) <0,0001Sedentarism (%) 33(47,8) 27(50) 6(40) <0,01
Tabel VII. IGB, IMT şi prevalenţa microalbuminuriei la lotul de studiuMarker Lot studiu (n=314) BAP (n=69) Fără BAP (n=245) Valoare pABI 0.98 0.83 1.11 <0.001IMT (mm) 0.97 1.12 0.78 <0.001Microalbuminuria (%) 17 22 15 <0.01
BAP uşoară (IGB:0,9-0,7) a fost întâlnită la 41 pacienţi (59,4%), BAP moderată (IGB: 0,7-0,5) la 19 (27,5%) şi BAP severă (IGB<0,5) la 9 pacienţi (13%, Tabel IV).
Dintre cei 69 de pacienţi cu BAP, 15 (21,7%) au prezentat BAP simptomatică, iar 54 (78,3%) BAP asimptomatică.
S-a observat scăderea valorilor IGB odată cu înaintarea în vârstă, cu numărul crescut de factori de risc asociaţi şi modificările trofice apărute la nivelul membrelor inferioare. Pacienţii cu BAP sunt foşti sau actuali fumători, având mai multe boli asociate (HTA, DZ, dislipidemie). Am întâlnit o diferenţă statistică importantă între IGB la fumători comparativ cu nefumători. Probabilitatea de a dezvolta BAP simptomatică sau asimptomatică a crescut odată cu numărul factorilor de risc prezenţi. Dintre cei 69 de pacienţi cu IGB<0,9, 46 (66,6%) au prezentat trei sau mai mulţi factori de risc majori pentru BCV şi 30 (43,4%) au prezentat DZ. Incidenţa DZ în rîndul celor fără BAP a fost de doar 31,8% (Tabel V).
În timpul perioadei de urmărire 17 pacienţi au decedat. Decesele au fost cauzate de IMA (6 cazuri), AVC (3 cazuri) sau de alte cauze (8 cazuri).
S-au înregistrat 20 evenimente cardiovasculare nonfatale majore în perioada de urmărire: infarct miocardic (5 cazuri), revascularizare coronariană (7 cazuri), accident vascular cerebral (5 cazuri), revascularizare la nivelul membrelor inferioare (2 cazuri), precum şi un caz de amputaţie datorită BAP în timpul perioadei de urmărire.
Riscul relativ de evenimente înregistrate în grupul pacienţilor cu BAP a fost de aproape 2,5 ori mai mare (RR: 2,46 CI: 2,04–3,12). Există o asociere inversă între IGB şi numărul de evenimente cardiovasculare (Tabel VI). Astfel pacienţii cu IGB<0,5 au prezentat un risc relativ de evenimente de aproape cinci ori mai mare (RR: 5,52 CI: 3,61–7,65) decât cei cu IGB>0,9 (RR: 1,13 CI: 0,88–1,48).
Relaţia dintre indicele gleznă-braţ (IGB), grosimea intima-medie carotidiană (IMT) şi microalbuminurie
Indicele gleznă-braţ, grosimea intima-medie şi microalbuminuria sunt factori predictori ai aterosclerozei şi indicatori ai riscului cardiovascular înalt.
Pacienţii cu BAP au prezentat valori scăzute ale IGB<0,9, valori crescute ale IMT>0,9 mm (Tabel VII)

ORIgInAL ARTIcLEs
The Ankle-Brachial Index In The Diagnosis Of Symptomatic And Asymptomatic Peripheral Arterial Disease 115
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
şi o prevalenţă crescută a microalbuminuriei (22% faţă de 15%, p<0,01). Prevalenţa microalbuminuriei a fost chiar mai mare la diabetici (31%). În rândul pacienţilor cu trei sau patru factori de risc majori pentru BCV s-au întâlnit cele mai mari valori medii ale IMT (1,18 mm), cea mai mare frecvenţă a IGB scăzut (25%) şi cea mai mare prevalenţă a microalbuminuriei (26%).
Valorile obţinute la măsurarea IMT au fost cuprinse între 0,41-3,89 mm cu o medie de 0,97 mm. IMT a fost considerat crescut când a depăşit 0,9 mm. O valoare a IMT>2 mm, obţinută la măsurătorile ecografice, a fost considerată ca reprezentând o placă de aterom şi a fost inclusă în calculul valorii medii a IMT pentru acel pacient. La măsurarea ultrasonografică a IMT, din cei 314 pacienţi incluşi în studiu, 166 (53%) au prezentat valori>0,9 mm şi la 148 (47%) s-au obţinut valori normale ale IMT.
Analiza de regresie liniară a demonstrat existenţa unei relaţii de inversă proporţionalitate între IGB şi grosimea intimei-medie. Astfel o creştere de 0,1 mm a IMT determină o reducere medie a IGB cu 0,034 (CI: 0,024-0,051), uşor mai pronunţată la bărbaţi decât la femei. O scădere treptată a IGB a fost observată odată cu creşterea IMT.
Discuţii
Boala arterială periferică este foarte răspândită în rândul persoanelor în vârstă şi în funcţie de severitatea ei prezintă un risc crescut de deces sau de apariţie a unor evenimente cardiovasculare majore [2,3]. În populaţia generală, incidenţa BAP, determinată prin IGB, se situează între 5 şi 13% [4,5]. La o populaţie cu factori de risc pentru ateroscleroză sau cu boli cardiovasculare manifeste, asemenea populaţiei din studiul nostru, incidenţa BAP oscilează între 15 şi 40%.
Prevalenţa bolii arteriale periferice a crescut marcat odată cu vârsta pacienţilor şi suplimentar în grupul fumătorilor, al celor cu diabet zaharat şi hipertensiune arterială.
Principalii factori de risc în dezvoltarea BAP asimptomatice sunt reprezentaţi de vârsta înaintată, hipertensiune, hipercolesterolemie, diabetul zaharat, fumatul şi stilul de viaţă sedentar [6,7,8]. Deoarece simptomatologia BAP este legată în mare parte de mişcare, sedentarii prin stilul lor de viaţă maschează expresia clinică a BAP, în principal claudicaţia intermitentă [9]. În studiul nostru indicele gleznă-braţ a confirmat diagnosticul de BAP la 22% din pacienţi, fiind foarte util în detectarea cazurilor asimptomatice de arteriopatii. Cumulul mai multor factori de risc pentru ateroscleroză s-a asociat cu o prevalenţă crescută a BAP.
Figurea 6. Decesele survenite în perioada de urmărire
Figura 7. Evenimentele nonfatale majore înregistrate în perioada de urmărire
Figura 8. Evenimentele cardiovasculare majore apărute la populaţia din lotul de studiu în perioada de urmărire
Figurea 9. Relaţia între IGB şi IMT

ORIgInAL ARTIcLEs
Gruici et al116
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
Riscul de evenimente fatale şi nonfatale înregistrate în grupul pacienţilor cu BAP a fost de aproape 2,5 ori mai mare (RR: 2,46 CI: 2,04-3,12). Există o asociere inversă între IGB şi numărul de evenimente. Astfel pacienţii cu IGB<0,5 au prezentat un risc relativ de evenimente cardiovasculare de aproape cinci ori mai mare (RR: 5,52 CI: 3,61-7,65) decât cei cu IGB>0,9 (RR: 1,13 CI: 0,88-1,48).
Rezultatele noastre au dovedit că IGB este un bun predictor al riscului cardiovascular atât la pacienţii simptomatici, cât şi la cei asimptomatici. Scăderea sa sub pragul de 0,9 se asociază cu creşterea morbidităţii şi mortalităţii cardio- şi cerebrovasculare. Utilizarea acestui parametru poate îmbunătăţi identificarea pacienţilor cu risc înalt [10,11].
Concluzii
Indicele gleznă-braţ s-a dovedit a fi un indicator important al aterosclerozei şi un puternic factor prognostic de evenimente cardiovasculare la pacienţii cu risc înalt. Prevalenţa bolii arteriale periferice a fost mai mare la vârstnici, fumători, diabetici, hipertensivi şi la cei care au asociat mai mulţi factori de risc pentru ateroscleroză.
Riscul de evenimente fatale şi nonfatale înregistrate în grupul pacienţilor cu BAP a fost de aproape 2,5 ori mai mare (RR: 2,46 CI: 2,04-3,12). S-a observat o asociere inversă între valorile IGB şi numărul de evenimente. Astfel, pacienţii cu IGB<0,5 au prezentat un risc relativ de evenimente cardiovasculare de aproape cinci ori mai mare (RR: 5,52 CI: 3,61-7,65) decât cei cu IGB>0,9 (RR: 1,13 CI: 0,88-1,48).
Studiul a demonstrat existenţa unei relaţii de inversă proporţionalitate între IGB şi grosimea intima-medie. O scădere treptată a IGB a fost observată cu creşterea IMT.
Determinarea IGB s-a dovedit a fi o investigaţie neinvazivă, accesibilă şi uşor de efectuat în cadrul cabinetului de medicină de familie, având o mare importanţă în diagnosticul precoce al BAP.
Referinţe
1. Mancia G, De Backer G, Dominiczak A, et all. The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension
(ESH) and of the European Society of Cardiology (ESC) 2007 Guidelines for the management of arterial hypertension. European Heart Journal 2007;28:1462-536.
2. Arsenescu I, Stoica A, Matei C, Pop I. Diagnosticul şi tratamentul arteriopatiei obliterante în cabinetul medicului de familie, ISBN 978-973-0-05484-2.
3. Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG, TASC II Working Group, Bell K, Caporusso J, Durand-Zaleski I, Komori K, Lammer J, Liapis C, et all. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). Eur J Vasc Endovasc Surg 2007,33(Suppl 1):1-75.
4. Abela GS. Peripheral Vascular Disease. Basic Diagnostic and Therapeutic Approaches, Lippincot Williams, 2004
5. Apetrei E. Arteriopatiile periferice, Ed. Medicală, Bucureşti, 1986
6. Hirsch AT, Haskal ZJ, Hertzer NR, Bakal CW, Creager MA, Halperin JL, et al. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic). Circulation 2006;113:e463–e654.
7. Ankle Brachial Index Collaboration, Fowkes FG, Murray GD, Butcher I, Heald CL, Lee RJ, Chambless LE, et all. Ankle. brachial index combined with Framingham risk score to predict cardiovascular events and mortality: a meta-analysis. JAMA 2008,300:197-208.
8. Hirsch AT, Criqui MH, Treat-Jacobson D, Regensteiner JG, Creager MA, Olin JW, et all. Peripheral arterial disease detection, awareness, and treatment in primary care. JAMA 2001,286:1317-24.
9. McDermott MM, Greenland P, Liu K, Guralnik JM, Celic L, Criqui MH, et all. The ankle brachial index is associated with leg function and physical activity: the Walking and Leg Circulation Study. Ann Intern Med 2002;136:873–883.
10. Price JF, Tzoulaki I, Lee AJ, Fowkes FG. Ankle brachial index and intima media thickness predict cardiovascular events similarly and increased prediction when combined. J Clin Epidemiol 2007;60(10):1067-75.
11. McDermott MM, Liu K, Criqui MH, Ruth K, Goff D, Saad MF, Wu C, Homma S, Sharrett AR: Ankle-brachial index and subclinical cardiac and carotid disease: the multi-ethnic study of atherosclerosis. Am J Epidemiol 2005;162(1):33-41.

Lead Exposure-Hematological And Cardiovascular Side Effects 117
Rezumat
Deşi plumbul este unul dintre cei mai studiaţi poluanţi, semnificaţia clinică a efectelor adverse asupra sistemelor hematoformator şi cardiovascular rămâne neclară. Anemia şi hipertensiunea arterială sunt manifestări clinice ale toxicităţii plumbului. Cu toate acestea, există rapoarte contradictorii în ceea ce priveşte prevalenţa acestora în rândul lucrătorilor expuşi de plumb şi este incert dacă determinarea hemoglobinei şi a valorilor tensionale ar trebui să fie incluse în monitorizarea clinică periodică a muncitorilor expuşi la plumb. Pentru a verifica relaţia dintre expunerea la plumb şi efectele adverse hematologice şi cardiovasculare am studiat corelaţia dintre valorile hemoglobinei, hematocritului, tensiunii arteriale, respectiv modificările electrocardiogramei şi nivelul de plumb din sânge, înregistrate la un număr de 223 de muncitori angajaţi întro fabrică producătoare de acumulatori auto. Un număr de 56 de subiecţi (25,11%) au avut nivelul de plumb din sânge mai mare de 40μg/dl. Corelaţia dintre valoarea plumbemiei şi a hematocritului a fost slabă (r=0,178). Nu au existat corelaţii semnificative statistic între valorile plumbemiei şi cele ale hemoglobinei, tensiunii arteriale sau modificările înregistrate pe electrocardiogramă. Putem concluziona că determinările hemoglobinei, hematocritului, tensiunii arteriale şi efectuarea electrocardiogramei nu sunt indicatori utili pentru monitorizarea expunerii la plumb. Discrepanţele
dintre corelaţiile raportate sunt inexplicabile şi acest subiect rămâne deschis cercetărilor ulterioare. Orice modificări ale parametrilor hematologici sau cardiovasculari înregistrate în rândul lucrătorilor expuşi la plumb ar trebui să fie considerate manifestări ale toxicităţii plumbului numai după ce au fost excluse alte cauze.
Cuvinte cheie: expunere la plumb, plumbemie, hemoglobină, hipertensiune arterială
Introducere
Saturnismul continuă să rămână o problemă majoră de sănătate recunoscută pe plan internaţional, în ciuda faptului că toxicitatea plumbului a fost cunoscută şi descrisă încă din antichitate [1]. Plumbul nu are nici un rol fiziologic în organism, în timp ce efectele sale nocive sunt nenumărate [2].
Plumbul inhibă activitatea enzimelor implicate în biosinteza hemului, afectează stabilitatea membranei eritrocitare, scade perioada de viaţă a hematiilor, produce hemoliză, ceea ce duce la apariţia anemiei [3].
S-a demonstrat faptul că plumbul alterează receptivitatea musculaturii netede a vaselor faţă de stimulii vasoactivi, ducând la creşterea consecutivă a răspunsului receptorilor colinergici şi dopaminergici cardiaci şi vasculari. Relaţia între plumb şi tensiunea arterială este încă în dezbatere, rămânând o problemă de sănătate publică [4].
ORIgInAL ARTIcLEs
eXpuneReA lA pluMb - eFecte secundARe HeMAtoloGice şi cARdioVAsculARe
Ruja Elena¹, Cocârlă Aristotel²
¹Clinica de Diagnostic Phoenix, Cluj Napoca, ²Universitatea de Medicină şi Farmacie „Iuliu Haţieganu” Cluj Napoca, Spitalul Clinic Judeţean Cluj, Secţia Clinică de Medicina Muncii
Adresa pentru corespondenţă:Dr. Ruja Elena Strada Iuliu Moldovan nr 8, Cluj Napoca E-mail: [email protected] Primit: 18.06.2012 Acceptat: 15.08.2012 Med Con October 2012 Vol 7, No 3, 117-119

ORIgInAL ARTIcLEs
Ruja et al118
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
Scopul acestui studiu a fost evaluarea relaţiei doză răspuns în expunerea ocupaţională la plumb, cu accent pe efectele hematologice şi cardiovasculare.
Material şi metodă
Acest studiu a fost realizat întro întreprindere producătoare de acumulatori auto şi a cuprins un număr de 223 de subiecţi care au avut expunere permanentă la plumb.
Obiectivul principal a fost evaluarea încărcării interne cu plumb prin intermediu biomarkerilor, în vederea evaluării stării de sănătate a angajaţilor care lucrează în secţiile de producţie.
Indicatorul de referinţă utilizat în monitorizarea biologică a persoanelor expuse profesional la plumb este reprezentat de nivelul plumbemiei. Metoda prin care s-a determinat concentraţia plumbului în sânge a fost absorbţia atomica pe cuptor de grafit, iar aparatul utilizat a fost SpectraA 110A - Varian.
Testele fiziologice şi biologice efectuate pentru a determina efectele plumbului asupra sistemelor hematoformator şi cardiovascular au fost: hemoleucograma, determinarea tensiunii arteriale şi electrocardiograma. Tensiunea arterială a fost măsurată de două ori la interval de cinci minute, folosind un tensiometru cu mercur. Hipertensiunea arterială a fost definită ca valori ale tensiunii arteriale sistolice mai mari de 140 mmHg şi ale tensiunii arteriale diastolice mai mari de 90 mmHg. Indivizii care au avut valori normale ale tensiunii arteriale dar care erau sub tratament antihipertensiv au fost consideraţi hipertensivi.
Monitorizarea angajaţilor a avut loc la ieşirea acestora din schimb şi s-a desfăşurat în cabinetul de medicina muncii din cadrul întreprinderii, încăperea fiind lipsită de urme de plumb atât în aer cât şi pe suprafeţe.
Analizele statistice au fost realizate cu ajutorul programului SPSS pentru Windows, versiunea 16. Orice valori ale lui p mai mici decât 0,05 au fost considerate semnificative statistic.
Rezultate
Toţi cei 223 de angajaţi incluşi în studiu au fost bărbaţi. Vechimea medie în muncă a variat între 0,09 ani şi 37,10 ani, cu o medie de 18,13 ani. Toţi angajaţii au lucrat 8 ore pe zi, în medie 5 zile pe săptămână.
Un număr de 56 muncitori (25,11%) au avut valorile plumbemiei peste limita normală de 40 μg/dl, iar dintre aceştia 5 (2,24%) au avut valori peste 60 μg/dl.
Valoarea medie a plumbemiei a fost de 36,14 μg/dl, cu minima de 6,44 μg/dl şi maxima de 65 μg/dl.
Cea mai mare valoare medie a plumbemiei 38,77 μg/dl s-a înregistrat la cei care au avut vechime în muncă mai mare de 30 de ani, iar cea mai mică valoare medie 31,78 μg/dl la cei cu vechime între 5-10 ani. Valorile maxime ale plumbemiei de 65 μg/dl au fost înregistrate la grupele cu vechime în muncă de 0-5 ani, 10-15 ani, 20-30 ani şi peste 30 ani. La aplicarea testului ANOVA simplu, rezultatele testului F omnibus au arătat că nivelul plumbemiei nu diferă semnificativ statistic (p=0,087) în funcţie de vechimea în muncă.
Un număr de 18 subiecţi (8,07%) au înregistrat valori ale hemoglobinei sub limita normală 14-17 g/dl. Valorea medie a hemoglobinei a fost de 15,95 mg/dl, cu minima 12,6 mg/dl şi maxima 19,7 mg/dl.
Nu a existat o corelaţie semnificativă statistic între valorile plumbemiei şi cele ale hemoglobinei (p=0,182).
Un număr de 11 subiecţi (4,93%) au prezentat valori ale hematocritului sub limita normală 42-50%. Valoarea medie a hematocritului a fost 44,92%, minima de 36%, iar maxima 56%.
Între valorile plumbemiei şi valorile hematocritului s-a constatat că există o corelaţie pozitivă, semnificativă statistic (p=0,029), dar această corelaţie a fost slabă, r=0,178. Un procent de 2,4% din variaţia variabilei hematocrit s-a datorat variaţiei variabilei plumbemie. (Coeficientul de determinare R² este egal cu 0,024).
Un număr de 57 subiecţi (25,56%) au avut hipertensiune arterială. Nu a existat o corelaţie semnificativă statistic între valorile plumbemiei şi cele ale tensiunii arteriale (p=0,083).
La 208 subiecţi din cei 223 investigaţi s-a efectuat electrocardiograma. La un număr de 19 subiecţi s-au semnalat modificări ale traseului înregistrat de tip: extrasistole ventriculare, bloc de ramură dreaptă, modificări ale segmentului ST, tahicardie sinusală.
Nu a existat o corelaţie semnificativă statistic între valorile plumbemiei şi modificările înregistrate pe traseul electrocardiogramei (p=0,284).
Discuţii
Valorile hemoglobinei nu s-au corelat cu nivelul de plumb din sânge. Diagnosticul anemiei la o persoană cu un nivel al plumbemiei mai mic de 80 μg/dl ar trebui să fie considerat a fi rezultatul toxicităţii plumbului numai după ce alte cauze de anemie au fost excluse. De asemenea unele studii au arătat că determinările periodice ale hemoglobinei nu sunt indicatori utili în monitorizarea expunerii la plumb [5]. Întrun studiu efectuat în Japonia, grupul de lucrători a căror

ORIgInAL ARTIcLEs
Lead Exposure-Hematological And Cardiovascular Side Effects 119
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
plumbemie a fost în limite normale a înregistrat valori ale hematocritului, hemoglobinei şi hematiilor semnificativ statistic mai mici decât grupul muncitorilor care au avut valori ale plumbemiei peste limita maximă admisă [6]. În studiul nostru o corelaţie semnificativă statistic a fost găsită între valorile plumbemiei şi nivelurile hematocritului. Numeroase studii au arătat că relaţia dintre plumbemie şi valorile scăzute ale hemoglobinei variază în funcţie de doză şi de timpul de expunere, precum şi de stilul de viaţă (alimentaţie, fumat şi consum de alcool) [7].
Multe studii experimentale pe animale au arătat că expunerea cronică la plumb poate creşte tensiunea arterială sistolică şi diastolică la mamifere, fiind propuse mai multe teorii plauzibile privind rolul plumbului în patogeneza hipertensiunii [8]. Studiile la om au furnizat în general dovezi mai puţin concludente în acest sens [9]. Expunerea profesională la plumb pe termen lung poate fi corelată cu o creştere uşoară, atât a tensiunii arteriale sistolice cât şi diastolice [10]. Asemenea studiilor similare care au evaluat efectului expunerii la plumb asupra tensiunii arteriale, studiul nostru a arătat că nu a existat o relaţie semnificativă statistic între nivelul de plumb din sânge şi valorile tensiunii arteriale sistolice şi/sau diastolice.
Concluzii
Determinările hemoglobinei, hematocritului, tensiunii arteriale şi efectuarea electrocardiogramei nu sunt indicatori utili pentru monitorizarea expunerii la plumb. Discrepanţele dintre corelaţiile raportate sunt inexplicabile şi acest subiect rămâne deschis cercetărilor ulterioare. Orice modificări ale parametrilor hematologici sau cardiovasculari înregistrate în rândul lucrătorilor expuşi de plumb ar trebui să fie considerate manifestări ale toxicităţii plumbului numai după ce au fost excluse alte cauze.
Referinţe
1. De Rosa CT, Choudhury H, Peirano WB. An integrated exposure/pharmacokinetic based approach to the assessment of complex exposures: Lead: A case study. Toxicol Ind Health 1991;7(4):231247.
2. U.S. Department of Labour Occupational Safety and Health Administration Screening and surveillance: A guide to OSHA Standards. OSHA 3162.2000;19-20.
3. Clayton GD, Clayton FE. Patty’s Industrial Hygiene and Toxicology. 3th Ed. New York: John Wilez and Sons Inc; 1981,pp:567-9.
4. Goyer R.A. Lead toxicity: from overt to subclinical to subtle health effects. Env Health Perspect 1990;86:177-81.
5. Froom P, Kristal-Boneh E, Benbassat J, Ashkanazi R, Ribak J. Lead exposure in battery-factory workers is not associated with anaemia. J Occup Environ Med 1999;41:120-3.
6. Makino S, Shimizu Y, Takata T. A study on the relationship between blood lead levels and anaemia indicators in workers exposed to low levels of lead. Ind Health 1997;35:537-41.
7. Pala K, Turkkan A, Gucer S, Osman E, Aytekin H. Occupational Lead Expousure: Blood Lead Levels of Apprentices in Bursa, Turkey. Ind Health 2009;47:97-102.
8. Telisman S, Pizent A, Jurasovic J, Cvitkovic P. Load effect on blood pressure in moderately lead exposed male workers. Am J Ind Med 2004;45:446-54.
9. Fenga C, Cacciola A, Martino LB, Calderaro SR, Di Nola C, Verzera A, Trimarchi G, Germanò D. Relationship of blood lead levels to blood pressure in exhaust battery storage workers. Ind Health 2006;44:304-9.
10. Mormontoy W, Gastañaga C, Gonzales G. Blood lead levels among police officers in Lima and Callao, 2004. Int J Hyg Environ Health 2006;209:497-502.

Abdominal x ray, colon (XR)
Mesentric panniculitis (CT)
gingerbread man

Preliminary Study About The Complications Which Can Appear In Restoring An Edentulous Space With Fixed Prosthesis 121
Rezumat
Edentaţia parţială reprezintă una din cele mai frecvente patologii orale întâlnite, restaurarea sa făcându-se uzual cu ajutorul protezelor dentare fixe integral/parţial fizionomice.
Realizarea incorectă sau alegerea necorespunzătoare a materialelor dentare utilizate în confecţionarea restaurărilor duce la apariţia unor multiple efecte nedorite precum: senzaţia de disconfort, mobilitatea protezei fixe, descimentarea, decompensarea parodontală, carii şi complicaţii pulpare la nivelul dinţilor stâlpi, retracţii gingivale şi resorbţii alveolare ca urmare a suprasolicitării dinţilor stâlpi, perforarea elementelor de agregare, fractura intermediarilor protezei fixe, fractura sau desprinderea faţetelor, lipsa de funcţionalitate a construcţiei protetice, inflamaţii gingivale, coloraţii gingivale, gust metalic.
Am studiat pe un lot compus din 169 de pacienţi efectele negative generate de inserarea în cavitatea bucală a unor restaurări protetice conjuncte confecţionate sau adaptate incorect.
Rata de succes a tratamentului la lotul de pacienţi studiat a fost de 76,92%. 39 de cazuri au fost considerate eşecuri prin apariţia complicaţiilor care periclitau prognosticul pe termen lung al restaurărilor. Frecvenţa complicaţiilor apărute, în ordine descrescătoare, a fost: evoluţia proceselor carioase la nivelul bonturilor dentare (20,51%), fractura componentei fizionomice (19,44%), fractura componentei metalice (15,38%), retracţii gingivale şi resorbţii alveolare (15,38%), coloraţii gingivale (12,82%), pierderea aspectului fizionomic (10,25%), sângerări şi supuraţii gingivale (7,69%).
Cuvinte cheie: edentaţie parţială, proteză dentară fixă, iatrogenie, materiale dentare
Introducere în temă şi scopuri
Edentaţia parţială reprezintă absenţa uneia până la maxim 15 unităţi dento-parodontale de pe o arcadă dentară. Prin pierderea unităţilor dento-parodontale pe arcada dentară apar discontinuităţi, denumite breşe (spaţii) edentate [1].
ORIgInAL ARTIcLEs
studiu pReliMinAR AsupRA coMplicAŢiiloR ApĂRute În pRoteZAReA FiXĂ A bReşeloR edentAte Reduse
Hancu Violeta, Comăneanu Raluca Monica, Barbu Horia Mihail, Rădulescu Diana Eugenia, Filipescu Alina Gabriela, Ghergic Doina Lucia
Universitatea Titu Maiorescu Bucureşti, Facultatea de Medicină Dentară
Adresa pentru corespondenţă:Dr. Hancu Violeta Str. Reconstrucţiei, nr.10, bl.29, sc.4, et.1, ap.138, sect.3, 031725, Bucureşti Email: [email protected] Primit: 27.01.2012 Acceptat: 10.09.2012 Med Con October 2012 Vol 7, No 3, 121-125 Această lucrare a fost cofinanţată din Fondul Social European prin Programul Operaţional Sectorial Dezvoltarea Resurselor Umane 2007-2013 în cadrul Proiectului POS DRU/CPP 107/DMI 1.5/S/77082 “Burse doctorale de pregătire ecoeconomică şi bioeconomică complexă pentru siguranţa şi securitatea alimentelor şi furajelor din ecosisteme antropice”.

ORIgInAL ARTIcLEs
Hancu et al122
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
Edentaţia parţială neprotezată determină dezvoltarea unei simptomatologii subiective şi obiective care se agravează progresiv, pe măsura apariţiei complicaţiilor locale, regionale şi la distanţă. Simptomatologia edentaţiei parţiale interesează funcţiile esenţiale ale sistemului orofacial, precum funcţia masticatorie, fonetică şi aspectul fizionomic prin pierderea dimensiunii verticale de ocluzie şi apariţia migrărilor dentare.
Restaurarea edentaţiei parţiale reduse şi compensarea funcţiilor afectate se realizează cu ajutorul protezelor fixe. Prognosticul pe termen lung al restaurărilor protetice fixe (RPF) este extrem de dificil de evaluat [1-13], deoarece în integrarea RPF există există o gamă largă de factori implicaţi [14].
Realizarea incorectă sau alegerea necorespunzătoare a materialelor dentare utilizate în confecţionarea restaurărilor duce la apariţia unor multiple efecte nedorite precum: senzaţia de disconfort, mobilitatea protezei fixe, descimentarea, decompensarea parodontală, carii şi complicaţii pulpare la nivelul dinţilor stâlpi, retracţii gingivale şi resorbţii alveolare ca urmare a suprasolicitării dinţilor stâlpi, perforarea elementelor de agregare, fractura intermediarilor protezei fixe, fractura sau desprinderea faţetelor, lipsa de funcţionalitate a construcţiei protetice, inflamaţii gingivale, coloraţii gingivale, gust metalic.
Scopul studiului nostru constă în analiza pe un lot de pacienţi a complicaţiilor care au dus la eşecul RPF.
Metode
În studiu a fost luat un lot de 203 pacienţi cu edentaţii parţiale protezate de minim 5 ani care s-au adresat unui număr de 5 cabinete stomatologice din Bucureşti în perioada octombrie 2010-ianuarie 2012 din diverse motive stomatologice. Din studiu au fost excluşi un număr de 34 de pacienţi care prezentau edentaţii parţiale întinse protezate mobilizabil, astfel încât lotul analizat a cuprins în final 169 de pacienţi cu edentaţii parţiale protezate fix.
Cazurile în care RPF prezentau la 5 ani o integrare corespunzătoare din punct de vedere funcţional, biologic şi estetic au fost considerate de succes, iar cazurile în care au apărut complicaţii care periclitau prognosticul pe termen lung al restaurărilor au fost considerate eşecuri.
După autorii de specialitate [4-10] există în principal nouă posibile cauze de eşec ale RPF: apariţia şi dezvoltarea cariilor la nivelul bonturilor care nu pot fi tratate fără ablaţia RPF, necesitatea efectuării unui tratament endodontic la nivelul dinţilor stâlpi, care nu poate fi efectuat corect fără ablaţia RPF, descimentarea RPF, deficienţe estetice datorate retracţiilor gingivale, inflamării gingivale sau pigmentării gingivale, cauze
parodontale (mobilitate/pierderea suportului osos la nivelul dinţilor stâlpi), fractura dinţilor stâlpi, fractura corpului de punte, fractura materialului de placare fizionomic, abrazia dinţilor antagonişti ai RPF.
Lotul a fost clasificat în funcţie de grupa de vârstă, sex, localizarea şi etiologia edentaţiei, precum şi tipul de complicaţie care a dus la eşecul tratamentului protetic.
Rezultate
Lotul de pacienţi studiat a cuprins un număr de 54 de pacienţi de sex masculin şi 115 pacienţi de sex feminin. În grupa de vârstă 41-50 ani s-au încadrat 14 pacienţi dintre care 5 pacienţi de sex masculin şi 9 pacienţi de sex feminin, în grupa de vârstă 51-60 ani s-au încadrat 61 de pacienţi (19 bărbaţi şi 42 femei), în grupa de vârstă 61-70 ani s-au încadrat 71 de pacienţi (49 de femei şi 22 bărbaţi), iar în grupa de vârstă 71-80 ani s-au încadrat 23 de pacienţi (dintre care 15 pacienţi de sex feminin şi 8 de sex masculin) (Tabel I).
În ceea ce priveşte localizarea edentaţiei parţiale, la lotul studiat am depistat prezenţa unui număr de 105 edentaţii la nivel maxilar şi a 64 edentaţii la nivel mandibular. La pacientele din lotul studiat am depistat 70 de edentaţii maxilare şi 45 de edentaţii mandibulare, iar la pacienţi, 35 de edentaţii maxilare şi 19 mandibulare (Tabel II).
Etiologia pierderii dinţilor a fost în 78 de cazuri caria dentară şi complicaţiile ei, în 60 de cazuri parodontopatia şi în 31 de cazuri iatrogenia (Tabel III).
Rata de succes a tratamentului la lotul de pacienţi studiat a fost de 76,92%. Astfel, din cele 169 de cazuri
Tabel I. Distribuţia lotului de pacienţi pe grupe de vârstă şi sex
PacienţiGrupa de vârstă
Total41-50 ani
51-60 ani
61-70 ani
71-80 ani
sex masculin 5 19 22 8 54sex feminin 9 42 49 15 115total 14 61 71 23 169
Tabel II. Clasificarea lotului studiat în funcţie de localizarea edentaţiei
PacienţiLocalizarea edentaţiei Total
Maxilar Mandibulă
sex masculin 35 19 54sex feminin 70 45 115total 105 64 169

ORIgInAL ARTIcLEs
Preliminary Study About The Complications Which Can Appear In Restoring An Edentulous Space With Fixed Prosthesis 123
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
ale lotului, la 39 pacienţi am constatat prezenţa complicaţiilor reprezentate de: fractura componentei fizionomice, fractura componentei metalice, pierderea aspectului fizionomic, sângerări şi supuraţii gingivale, coloraţii gingivale, retracţii gingivale şi resorbţii alveolare, evoluţia proceselor carioase la nivelul bonturilor dentare (Tabel IV, Figurile 4-17).
Tabel III. Clasificarea lotului de pacienţi în funcţie de etiologia edentaţiei
Caria dentară complicată Parodontopatia Iatrogenia
Număr de cazuri 78 60 31
Tabel IV. Tipuri de complicaţii depistate
Tipuri de complicaţii depistate Număr de cazuri
fractura componentei fizionomice 7fractura componentei metalice 6pierderea aspectului fizionomic 4sângerări şi supuraţii gingivale 3coloraţii gingivale 5retracţii gingivale şi resorbţii alveolare 6evoluţia proceselor carioase la nivelul bonturilor dentare 8
Total 39
Figura 4. Fractura componentei fizionomice la o restaurare metalo-ceramică datorată
factorilor ocluzali
Figura 5. Fractura componentei fizionomice la o restaurare metalo-ceramică datorită erorii de concepţie (confecţionarea unei punţi totale
la nivel mandibular)
Figura 6. Fractura componentei metalice datorită tehnicii incorecte de turnare, retenţii alimentare datorită conformării incorecte a ambrazurilor, inflamaţii gingivale produse de spina iritativă reprezentată de componenta acrilică, pierderea
aspectului fizionomic prin vizibilitatea metalului prin transparenţa acrilatului şi ca urmare a impregnării
materialului acrilic cu coloranţi alimentari
Figura 7. La nivel maxilar: fractura componentei metalice datorită tehnicii incorecte de turnare,
sângerare gingivală la sondare datorată inflamării produse de componenta acrilică fizionomică, retenţii alimentare ca urmare a conformării
incorecte a ambrazurilor şi pierderea aspectului fizionomic prin colorarea acrilatului produsă de
nicotină; la nivel mandibular fractura componentei fizionomice datorită retenţiei
ineficiente şi retracţii gingivale prin conturul necorespunzător al elementelor de agregare
Figura 8. Fractura componentei metalice datorate tehnicii incorecte de turnare
Figura 9. Fractura componentei metalice datorită suprasolicitării produse de lungimea
excesivă a breşei edentate şi fractura componentei fizionomice la nivel incizal prin retenţie insuficientă şi suprasolicitare ocluzală

ORIgInAL ARTIcLEs
Hancu et al124
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
Discuţii
Senzaţia de disconfort este un incident frecvent constatat după fixarea restaurărilor protetice şi poate fi cauzată de prezenţa unor contacte premature sau interferenţe ocluzale, inserţia protezei într-o poziţie inadecvată, o suprafaţă ocluzală supradimensionată sau redusă [9,10], suprapresiune asupra unităţilor dento-parodontale de sprijin [4,5], contacte prea strânse cu
dinţii învecinaţi, protejarea insuficientă a ţesuturilor gingivale sau acumularea resturilor alimentare la nivelul piesei protetice datorită designului inadecvat [12].
Mobilitatea protezelor fixe poate apărea în cazul deformării elementelor de agregare, contactelor ocluzale disfuncţionale, cimentării incorecte, solubilizării cimentului, proceselor carioase apărute la nivelul dinţilor stâlpi (prin igienă defectuoasă, conformare incorectă a ambrazurilor, elemente de agregare prea largi sau prea
Figura 10. Coloraţii gingivale în cazul unei restaurări metalo-acrilice (stânga) şi a unei restaurări metalo-ceramice (dreapta)
Figura 11. Supuraţii şi sângerări gingivale în cazul unei restaurări metalo-acrilice (stânga) şi metalo-ceramice (dreapta)
Figura 12. Fractura bonturilor dentare ca urmare a evoluţiei proceselor carioase
(microproteze prea largi)
Figura 13. Proces carios la nivelul bontului dentar (microproteză prea scurtă)
Figura 14. Retracţii gingivale ca urmare a suprasolicitării dinţilor stâlpi
Figura 15. Retracţii gingivale şi resorbţii alveolare ca urmare a solicitării dinţilor stâlpi
Figura 16. Fistulă – complicaţie a gangrenei de la nivelul bontului dentar
Figura 17. Spină iritativă la nivel gingival – microproteză prea largă

ORIgInAL ARTIcLEs
Preliminary Study About The Complications Which Can Appear In Restoring An Edentulous Space With Fixed Prosthesis 125
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
scurte), mobilizării unuia sau mai multor dinţi stâlpi prin decompensare parodontală [4,5], lipsei de retenţie a elementelor de agregare prin preparări incorecte.
Retracţiile gingivale şi resorbţiile alveolare pot fi determinate de: suprasolicitarea dinţilor stâlpi prin lungimea excesivă a breşelor, conformarea inadecvată a ambrazurilor gingivale, conturul necorespunzător al elementelor de agregare [8], alegerea unui număr insuficient de dinţi stâlpi.
Scheletul metalic al intermediarilor se poate fractura ca urmare a tehnicii incorecte de turnare şi de manipulare a aliajului sau prin suprasolicitarea protezei parţiale fixe datorită unei breşe prea întinse [4].
Fractura componentei fizionomice a protezelor parţiale fixe se poate datora retenţiei ineficiente, factorilor ocluzali sau erorilor de concepţie (confecţionarea punţilor totale la nivelul arcadei inferioare, neţinând cont de flexibilitatea mandibulei) [6,7].
Concluzii
Lotul studiat a cuprins preponderent pacienţi de sex feminin aparţinând grupei de vârstă 61-70 ani.
Localizarea edentaţiei a fost în 62,13% din cazuri la nivel maxilar. Din punct de vedere al etiologiei edentaţiei, în 46% din cazuri aceasta s-a produs ca urmare a evoluţiei proceselor carioase, în 36% din cazuri ca efect al parodontopatiei şi în 18% din cazuri a fost iatrogenă.
Rata de succes a tratamentului la lotul de pacienţi studiat a fost de 76,92%. 39 de cazuri au fost considerate eşecuri prin apariţia complicaţiilor care periclitau prognosticul pe termen lung al restaurărilor. Frecvenţa complicaţiilor apărute, în ordine descrescătoare, a fost: evoluţia proceselor carioase la nivelul bonturilor dentare (20,51%), fractura componentei fizionomice (19,44%), fractura componentei metalice (15,38%) retracţii gingivale şi resorbţii alveolare (15,38%), coloraţii gingivale (12,82%), pierderea aspectului fizionomic (10,25%), sângerări şi supuraţii gingivale (7,69%).
Referinţe
1. Bratu D, Nussbaum R. Bazele clinice şi tehnice ale protezării fixe. Ed. Signata, Timişoara, 2001 p 69-108,503-601,1153-246.
2. Shigli K, Hebbal M, Angadi GS. Self-reported assessment of intraoral prostheses among patients
attending the prosthodontic department in a dental institute in India. Geriatr Gerontol Int, 2008;8(2):101-8.
3. Güngör MA, Artunç C, Dündar M. Seven-year clinical follow-up study of Probond ceramic crowns. Quintessence Int, 2007;38(8):456-63.
4. Hirotomi T, Yoshihara A, Ogawa H, et al. Tooth-related risk factors for periodontal disease în community-dwelling elderly people. J Clin Periodontol, 2010;37(6):494-500.
5. Hermann P, Gera I, Borbély J, et al. Periodontal health of an adult population in Hungary: findings of a national survey. J Clin Periodontol, 2009;36(6):449-57.
6. Creugers NH, Kayser AF, van‘t Hof MA. A meta-analysis of durability data on conventional fixed bridges. Community Dent Oral Epidemiol, 1994;22(6):448-52.
7. Goodacre CJ, Bernal G, Rungcharassaeng K, et al. Clinical complications in fixed prosthodontics. J Prost Dent, 2003;90(1):31-41
8. Foster LV. The relationship between failure and design in conventional bridgework from general dental practice. J Oral Rehabil, 1991;18(6):491-95.
9. Napankangas R, Salonen-Kemppi MA, Raustia AM. Longevity of fixed metal ceramic bridge prostheses: a clinical follow-up study. J Oral Rehabil, 2002;29(2):140-5.
10. Lindquist E, Karlsson S. Success rate and failures for fixed partial dentures after 20 years of service: Part I. Int J Prosthodont, 1998;11(2):133-8.
11. Hammerle CH, Ungerer MC, Fantoni PC, et al. Long-term analysis of biologic and technical aspects of fixed partial dentures with cantilevers. Int J Prosthodont, 2000;13(5):409-15.
12. Palotie U, Vehkalahti M. Finnish dentists’ perceptions of the longevity of direct dental restorations. Acta Odont Scand, 2009;67(1):44-9
13. Romanian National Institute of Statistics (2010). Household Income and Expenditure – Q1 2010 [Online]. 2010 Aug 3 [cited 2010 Nov 21] [http://www.seenews.com/news/latestnews /romaniannational inst i tuteofs tat i s t ics–householdincomeand expediture-q1-142602/]
14. Moga I, Chifor R, Badea ME, Popa S. Factori implicaţi în eşecurile protezelor parţiale fixe. Clujul Medical, 2011;84(4),603-7.

Metal implant, femoral bone (CT)
Retropharyngeal abcess ( neck CT)
I think I found my lizard ….

May Influence The Epidural Anesthesia The Newborn Hearing Screening? 127
Rezumat
Obiective: Scopul principal a fost de a stabili dacă anestezia epidurală are vreo influenţă asupra rezultatelor screeningului nou-nascuţilor a căror naştere a fost prin cezariană la cerere şi dacă momentul efectuării testării influenţează rezultatele screeningului.
Materiale şi metode: 50 de nou-născuţi sunt luaţi în studiu, 25 născuţi prin cezariană sub anestezie epidurală, 25 născuţi pe cale vaginală; sunt testaţi la trei momente diferite folosind otoemisiuni acustice tranzitorii evocate (TEOAE) şi potenţiale evocate automate (AABR).
Rezultate: Screeningul efectuat în primele patru ore de la naştere a avut rezultate fals pozitive, comparativ cu testarea efectuată după 24 de ore. A fost obţinut un indice crescut de suspiciune semnificativ statistic (p<0,05) în ceea ce priveşte influenţa anesteziei epidurale asupra răspunsului automat auditiv al trunchiului cerebral (AABR), atunci când testul este efectuat la mai puţin de patru ore după naştere.
Concluzii: Rezultatele obţinute au importanţă pentru planificarea efectuării screening-ului auditiv, mai
ales cand se doreşte testarea universală a auzului la nou-născut.
Cuvinte cheie: screening-ul auditiv al nou născutului, otoemisii acustice tranzitorii (TEOAE), potenţiale evocate automate (AABR), anestezie epidurală
Introducere
Deoarece deficienţa auzului nu poate fi identificată imediat prin examene clinice de rutină cum ar fi observarea comportamentului [1], se impune aplicarea măsurătorilor electrofiziologice obiective, otoemisiunile acustice tranzitorii evocate (TEOAE) şi potenţialele evocate automate (AABR), caracteristice screeningului universal al nou-născutului şi sugarului [2,3]. Acesta vizează obţinerea de rezultate auditive de screening pentru fiecare nou-născut, în orice moment înainte de externarea din spital [4]. Identificarea precoce şi intervenţia terapeutică înainte de vârsta de 6 luni a deficienţei de auz poate preveni repercusiunile severe psihosociale, educaţionale şi lingvistice. De aceea, este vital de a izola şi clasifica factorii care pot influenţa succesul sau eşecul programului de screening audiologic
ORIgInAL ARTIcLEs
poAte inFluenŢA AnesteZiA epiduRAlĂ scReeninG-ul AuditiV Al nou-nĂscuŢiloR?
Domuţa Maria1,2, Pascalau Nicoleta1, Cotulbea Stan2
1Facultatea de Medicină şi Farmacie Oradea, România, 2Universitatea de Medicină şi Farmacie “Victor Babeş” Timişoara, România
Adresa pentru corespondenţă:Dr. Maria Domuţa Facultatea de Medicină şi Farmacie Oradea Piaţa 1 Decembrie 10, 410073, Oradea, România Tel: +40744 779 199 E-mail : [email protected] Primit: 01.09.2012 Acceptat: 01.10.2012 Med Con October 2012, Vol 7, No 3, 127-130

ORIgInAL ARTIcLEs
Domuţa et al128
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
al nou-născutului, cum ar fi anestezia epidurală pentru naşterea prin cezariană la cerere.
Rata de prevalenţă a pierderii auzului raportată la nivel mondial este tot mai mare [5]. Între unul şi patru din o mie de nou-născuţi se nasc cu hipoacuzie, aceasta fiind una din cele mai comune anomalii congenitale [6]. Literatura actuală sugerează că la nivel global aproximativ 6 din 1000 de sugari prezintă pierderea permanentă a auzului la naştere sau în perioada neonatală [7].
În consecinţă, este necesară aplicarea screeningului pentru hipoacuzie la toţi nou-născuţii şi o înţelegere clară a influenţei pe care anumite elemente postnatale (cum ar fi anestezia epidurală) o pot avea asupra punerii în aplicare a acestuia. Este posibil ca anestezia epidurală să poate deprima funcţionarea sistemului auditiv şi prin urmare integritatea screening-ului auzului, cauzând astfel rezultate fals pozitive [8]. De aici nevoia de a determina rezultatele audiologice la nou-născuţii mamelor la care s-a practicat anestezie epidurală pentru cezariană la cerere.
Anestezia epidurală este o procedură care presupune injectarea anestezicului în afara durei mater a măduvei spinării şi acest lucru duce la o blocadă autonomă şi parţială a sistemului nervos central. Aceasta este frecvent utilizată pentru cezariana la cerere [9]. Ea are avantajul de a permite mamei să rămână trează, diminueaza riscul de aspiraţie maternă şi reduce efectele drogurilor asupra nou-născuţilor [10]. Efectele pe termen lung ale anesteziei epidurale, care sunt rare şi minime, au fost bine documentate [11]; cu toate acestea, nu este bine stabilit dacă anestezia epidurală afectează sistemul auditiv al nou-născutului.
Pornind de la aceste date, scopul acestui studiu prospectiv este de a stabili dacă anestezia epidurală are o influenţă asupra rezultatelor screeningului nou-nascuţilor a căror naştere a fost prin cezariană la cerere.
S-a urmărit atingerea următoarelor obiective: determinarea rezultatelor screeningului auditiv în grupul nou-nascuţilor a căror mame au născut prin cezariană sub anestezie epidurală (lotul A); compararea rezultatelor screeningului auditiv al lotului A cu cele ale nou-născuţilor din mame care au avut o naştere vaginală, fără anestezie epidurală (lotul B); stabilirea dacă momentul efectuării screeningului auditiv are vreun efect asupra rezultatelor de screening.
Materiale şi metodă
Acest studiu prospectiv s-a desfăsurat în cadrul Clinicii de Neonatologie a Spitalului Clinic Judeţean de Urgenţă Oradea Staţionar III, în perioada 2009-2010 pe un număr de 50 nou-născuţi la termen, între 38 şi 42
săptămâni de gestaţie. Aceştia au fost împărţiţi în două loturi: lotul A - 25 nou-născuţi a căror mame au născut prin operaţie cezariană la cerere cu anestezie epidurală şi lotul B - 25 nou-născuţi din mame care au avut o naştere vaginală, fără anestezie epidurală.
Criteriile de includere în studiu pentru eşantionul de pacienţi au fost:
– nou-născuţi la termen, între 38 şi 42 săptămâni de gestaţie
– sarcină normală– lipsa factorilor de risc materni (avort spontan) şi
fetali (patologie care să necesite internarea pe secţia de terapie intensivă neonatală, anomalii craniofaciale, infecţii intrauterine, istoric familial de pierdere a auzului)
– cezariană cu anestezie epidurală sau naştere vaginală normală
– lipsa anesteziei epidurale în timpul naşterii vaginale.
Aparatul folosit pentru testarea auzului a fost un Echo-Screen de tip ES/TA produs de Fisher Zoth-Mack Medizintechnick Germania. Toţi nou-născuţii au fost testaţi utilizând ca metode de screening otoemisiuni acustice tranzitorii evocate (TEOAE), ce reflectă activitatea mecanică a celulelor ciliate externe care produc vibraţii transmise prin lichidele endocohleare pe cale retrogradă spre conductul auditiv extern, urmate de potenţiale evocate auditive automate (AABR). S-a evaluat astfel integritatea şi funcţia nervilor cranieni cohleari (NV VIII) şi calea auditivă din trunchiul cerebral, la trei intervale de timp: sub 4 ore, între 4 şi 6 ore şi după 24 de ore după naştere. Testarea s-a efectuat în deplină linişte, când nou-născutul se odihnea sau imediat după hrănire (fără sedare). Pentru ambele metode de testare, rezultatele au fost înregistrate, ca PASS sau REFER pentru fiecare participant la fiecare sesiune de testare.
Toate informaţiile au fost stocate şi prelucrate cu ajutorul programului Microsoft® Excel® 2010 (Microsoft® Corporation, SUA), constituind baza de date a studiului statistic. Ca metode de analiză statistică a fost folosit Fisher’s exact test, utilizând programul de statistică medicală MedCalc® versiunea 12.2.1.0 (MedCalc® Software, Mariakerke, Belgium).
Rezultate
Rezultatele screeningului auditiv al nou-născuţilor participanţi la studiu sunt incluse în Tabelul I. Acestea indică că o mare majoritate (92%) a nou-născuţilor au obţinut REFER la primele două sesiuni TEOAE pentru lotul A, în timp ce 40% au obţinut REFER la prima sesiune AABR.

ORIgInAL ARTIcLEs
May Influence The Epidural Anesthesia The Newborn Hearing Screening? 129
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
Rezultatele sesiunii 1, deşi sunt în conformitate cu unele rapoarte anterioare referitoare la anestezia epidurală care cauzează întârzieri în răspunsul AABR, trebuie să fie interpretate cu precauţie, datorită prezenţei vernixului în conductul auditiv extern al nou-născutului, care poate avea o influenţă asupra rezultatului AABR. Prezenţa vernixului a avut o influenţă similară asupra AABR şi în lotul B. Însă există o diferenţă semnificativă statistic între cele două loturi (REFER 40% lotul A versus 8% lotul B, p=0,018077) care confirmă că anestezia epidurală a avut un efect asupra rezultatelor de screening prin potentiale evocate auditive (AABR) la nou-născuţi.
Discuţii
Se remarcă o îmbunătăţire semnificativă în rezultatele PASS de screening AABR la sesiunile 2 şi 3, indicând faptul că efectele anesteziei ar fi încetat. De altfel, examinând efectele clorhidratului de lidocaină asupra răspunsului auditiv al trunchiul cerebral la nou-născut, Diaz şi colab. [12] au constatat o întârziere semnificativă în componenta neuronală centrală la 90 dB pentru grupul experimental, în comparaţie cu grupul control.
Întrun alt studiu realizat de Bozynski şi colab. [13] s-a constatat modificarea răspunsului auditiv al trunchiul cerebral evocat la nou-născuţii testaţi la mai puţin de patru ore, în comparaţie cu rezultatele la 48 de ore sau mai mult, după anestezia epidurală maternă cu lidocaină; aceste schimbări se corelează cu concentraţia în sânge a lidocainei.
Nu acelaşi lucru se poate spune pentru rezultatele screeningului prin TEOAE, care par să rămână destul de ridicate în sesiunile 1 şi 2 pentru ambele grupuri, însă fără diferenţe semnificative statistic. Schimbări semnificative apar la sesiunea 3. Owen şi colab. [14]
remarcă numărul mare de rezultate fals pozitive obţinute atunci când otoemisiunile acustice tranzitorii evocate (TEOAE) sunt realizate în primele 24 de ore după naştere. Ratele de REFER pentru TEOAE sunt raportate între 5-20% atunci când sunt efectuate mai devreme de 24 de ore după naştere şi mai puţin de 3% atunci când sunt efectuate la 24-48 ore de la naştere [15]. Cercetările efectuate de către Levi şi colab. [16] indică faptul că TEOAE pot fi realizate mai devreme de 48 de ore de la naştere, în timp ce Pennsylvania Health Care Cost Containment Counsel [17] sugerează că TEOAE realizate după 48 de ore sunt mult mai de încredere. Rezultatele fals pozitive se pot datora prezenţei vernixului în conductul auditiv extern [18]. Constatările TEOAE confirmă dovezile documentate că screeningul prin otoemisiuni acustice (TEOAE) este mult mai fiabil la 24 de ore după naştere, din cauza prezenţei vernixului.
Analizând Tabelul I se poate remarca că screeningul TEOAE se menţine pozitiv în primele două sesiuni (<4 ore, la 4-6 ore) pentru ambele loturi, probabil din cauza prezenţei vernixului în conductul auditiv extern, acesta schimbându-se doar când a fost realizat după 24 de ore (la externare). Screeningul AABR se menţine pozitiv când este realizat în primele patru ore după naştere, cu diferenţe semnificative între cele două loturi de nou-născuţi (REFER 40% lotul A versus 8% lotul B, p=0,018077) şi se schimbă în următoarele două sesiuni pentru toţi nou-născuţii.
În concluzie, deşi utilizarea eficientă a TEOAE şi AABR ca măsuri de screening a fost bine stabilită, este important să se stabilească factorii care pot influenţa fiabilitatea acestor măsuri. În studiul actual, anestezia epidurală pare să fi avut o influenţă referitoare la creşterea rezultatelor fals pozitive atunci când testarea s-a realizat mai devreme de patru ore după naştere.
Din rezultatele obţinute se poate concluziona că testarea prin TEOAE mai devreme de patru ore după
Tabelul I Rezultatele screeningului auditiv pentru cele două loturi de nou-născuţi
Sesiuni de screening pentru TEOAE şi AABR
Lotul A (nou-născuţi prin cezariană cu anestezie
epidurală)n=25
Lotul B (nou-născuţi prin naştere vaginală fără anestezie epidurală)
n=25
p†
(PASS)p†
(REFER)
Sesiunea 1 TEOAESesiunea 1 AABRSesiunea 2 TEOAESesiunea 2 AABRSesiunea 3 TEOAESesiunea 3 AABR
PASS2 (8%)
15 (60%)2 (8%)100%100%100%
REFER23 (92%)10 (40%)23 (92%)
0%0%0%
PASS5 (20%)23 (92%)5 (20%)100%100%100%
REFER20 (80%)2 (8%)
20 (80%)0%0%0%
p=0,417427*p=0,018077*p=0,417427*
p=0.417427*p=0.018077*p=0.417427*
*Fisher’s exact test†p<0,05 dovedeşte o diferenţă statistic semnificativă între loturile studiate

ORIgInAL ARTIcLEs
Domuţa et al130
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
naştere, precum şi între patru şi şase ore după naştere este nefavorabilă din cauza prezenţei vernixului în conductul auditiv extern în astfel de momente. Această constatare este confirmată de Korres şi colab. [19] şi Pennsylvania Health Care Cost Containment Counsel [17] potrivit cărora TEOAE sunt instrumente de screening viabile între 24 si 48 de ore de la naştere, pentru că la acel moment conductul auditiv extern ar fi liber de vernix. Indicele de suspiciune cu privire la influenţa anesteziei epidurală a fost ridicat.
Concluziile studiului actual au implicaţii semnificative pentru punerea în aplicare a programului de screening universal al nou-născutului pentru deficienţa auzului.
Screeningul prin AABR este fiabil dacă este efectuat la patru ore după naştere la nou-născuţii a căror naştere s-a realizat sub anestezie epidurală. Calendarul screeningului universal al auzului în special la copiii născuţi cu anestezie epidurală este important deoarece utilizarea anesteziei epidurale ar putea duce la creşterea rezultatelor fals pozitive, ceea ce poate duce la anxietatea nejustificată maternă.
Utilizarea TEOAE pare să fie influenţată în mod semnificativ de vernix în primele ore după naştere, subliniind necesitatea de a asigura faptul că fluidele din conductul auditiv extern sunt eliminate în mod activ înainte de utilizarea TEOAE şi poate fi implementat ca o condiţie de screening înainte de 24 de ore.
Rerferinţe
1. Arehart KH, Yoshinaga-Itano C, Thompson V, Gabbard SA, Brown AS. State the states: The status of universal newborn hearing screening, assessment, and intervention systems in 16 states. Am J Audiol 1998;7:1-14.
2. American Academy of Pediatrics, Joint Committee on Infant Hearing. Year 2007 Position statement: Principles and guidelines for early hearing detection and intervention programs. Pediatrics 2007;120:898-921.
3. HPCSA. Early hearing detection and intervention programmes in South Africa, Position Statement Year (2007). Available from: http://www.hpsca.co.za/hpcsa/default.aspx?id=137 [Last accessed on 2009 Feb 07].
4. Widen J, Bull RW, Folsom RC. Newborn hearing screening: What it means for providers of early intervention services. Infants Young Child 2003;16:249.
5. Swanepoel DC, Delport SD, Swart JG. Universal newborn hearing screening in South Africa. S A Med J 2004;94:634.
6. Pripic I, Mahujla-Stamenkovic V, Bilic I, Haller H. Hearing loss assessed by universal newborn hearing screening-The new approach. Int J Pediatr Otorhinolaryngol 2007;71:1757-61.
7. Olusanya BO, Newton VE. Global burden of childhood hearing impairment and disease control priorities in developing countries. Lancet 2007;369:1314-7.
8. Gurian EA, Kinnamon DD, Henry JJ, Waisbren SE. Expanded newborn screening for biochemical disorders: The effect of a false-positive result. Pediatrics 2006;117:1915-21.
9. Marquette GP, Mechas T, Charest J. Epidural anesthesia for elective Cesarean section does not influence fetal umbilical artery blood flow indices. Can J Anaesth 1994;41:1053-6.
10. Morrow RJ, Rolbin SH, Ritchie JW, Haley S. Epidural anesthesia and the blood flow velocity in mother and fetus. Can J Anaesth 1989;36:519-22.
11. Marquette GP, Mechas T, Charest J. Epidural anesthesia for elective Cesarean section does not influence fetal umbilical artery blood flow indices. Can J Anaesth 1994;41:1053-6.
12. Diaz M, Graff M, Hiatt M, Friedman S, Ostfeld B, Hegyi T. Prenatal lidocaine and the auditory evoked responses in term infants. Am J Dis Child 1988;142:160-1.
13. Marquette GP, Mechas T, Charest J. Epidural anesthesia for elective Cesarean section does not influence fetal umbilical artery blood flow indices. Can J Anaesth 1994;41:1053-6.
14. Owen M, Webb M, Evans K. Community based universal neonatal hearing screening by health visitors using otoacoustic emissions. Arch Dis Child 2001;84:157-62.
15. Erenberg A, Lemons J, Sia C, Trunkel D, Ziring P. Task Force on Newborn and Infant Hearing. Newborn and Infant Hearing Loss: Detection and Intervention. Pediatrics 1999;103:527-30.
16. Levi H, Adelman C, Geal-Dor M, Elidan J, Eliashar R, Sichel J, et al. Transient evoked otoacoustic emissions in newborns in the first 48 hours after birth. Audiology 1997;36:181-6.
17. Pennsylvania Health Care Cost Containment Council. Review of Senate Bill 938. 2005. Available from: http://www.phc4.org/reports/mandates/SB938/review.htm [Last accessed on 2007 Jun 11].
18. Watkin PM, Baldwin M, Dixon R, Beckman A. Maternal anxiety and attitudes of universal neonatal hearing screening. Br J Audiol 1998;32:27-37.
19. Korres S, Nikolopoulos T, Ferekidis E, Gotzamanoglou Z, Georgiou A, Balatsouras DG. Otoacoustic emissions in universal hearing screening: Which day after birth should we examine the newborns. ORL J Otorhinolaryngol Relat Spec 2003;65:199-201.

New Therapeutic And Etiologic Perspectives In Recurrent Miscarriage 131
Rezumat
Boala abortivă afectează aproximativ 1%-3% din cupluri şi reprezintă o problemă de mare actualitate cu multiple necunoscute încă în ceea ce priveşte mecanismele etiopatogenice. Anomaliile uterine, factorii genetici, endocrini, imunologici şi trombofilia reprezintă factori cunoscuţi a fi implicaţi în etiopatogenia avortului recurent. Actual se discută şi despre implicarea glicoproteinelor şi a unor receptori hormonali nucleari în etiopatogenia acestei afecţiuni. Prezentăm noile tendinţe şi studii referitoare la etiopatogenia şi conduita în cazul avortului recurent.
Cuvinte cheie: boala abortivă, factori genetici, anomalii uterine, trombofilie, anticorpi antifosfolipidici
Declaraţie de interese: autorii declină orice conflict de interese
Introducere
Boala abortivă (BA) se defineşte ca apariţia unui număr de cel puţin trei avorturi spontane consecutive şi afectează aproximativ 1%-3% din cupluri [1,2]. BA primară include paciente cu avorturi spontane consecutive şi fără naşteri în antecedente, iar BA secundară este reprezentată de avorturi spontane recurente ce survin după naşterea unui făt viabil. Există
o serie de factori cunoscuţi a fi implicaţi în etiologia BA şi anume: anomalii cromozomiale, disfuncţii endocrine, anomalii uterine, afecţiuni imunologice sau trombofilia. Cu toate acestea, în peste 50% din cazuri etiologia rămâne necunoscută, iar în prezent se cercetează implicarea unor factori precum receptori hormonali nucleari sau leptineglicoproteina glicodelină [3].
Cauze geneticeCauzele genetice ale BA sunt implicate întrun
procent variabil cuprins între 25-47% din totalul cazurilor cu BA [4,5]. Etiologia factorilor genetici este argumentată de rata crescută a anomaliilor cromozomiale depistate prin diagnosticul genetic preimplantare din cadrul fertilizării in vitro (FIV) la cuplurile cu BA comparativ cu cele fără BA recurente (70,7% versus 45,1%; p<0,0001) [6].
Printre factorii genetici se numără scurtarea telomerelor ovocitelor indusă de stresul oxidativ, fenomen caracteristic vârstei materne avansate [7]. Această modificare explică incidenţa crescută a avortului spontan, atât a celui sporadic cât şi a celui recurent, la femeile peste 35 de ani [8].
Studiile au demonstrat o incidenţă crescută (3,6%) a translocaţiilor echilibrate la cuplurile cu BA [9]. Cuplurile cu acest tip de translocaţie au o rată a avortului spontan de până la 29%, iar la 36% dintre produşii de concepţie avortaţi s-a pus în evidenţă o translocaţie
gEnERAL REVIEW
noi peRspectiVe etioloGice şi teRApeutice AsupRA bolii AboRtiVe
Grigore Mihaela¹, Mareş Alina²
1UMF „Gr.T.Popa” Iaşi, ²Centrul Medical Medis Iaşi
Adresa pentru corespondenţă:Dr. Mihaela Grigore Str. Bălţi 7C, Iaşi, România tel: 0744438024 E-mail:[email protected] Primit: 20.06.2012 Acceptat: 10.08.2012 Med Con October 2012, Vol 7, No 3, 131-135

gEnERAL REVIEW
Grigore et al 132
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
neechilibrată [10]. Aceste constatări argumentează necesitatea efectuării unui cariotip parental de înaltă rezoluţie la cuplurile cu antecedente de avort spontan precoce de cauză neexplicată. De asemenea, se recomandă la cuplurile cu translocaţii echilibrate şi antecedente de BA să se efectueze în cadrul FIV diagnosticul genetic preimplantaţional [11].
Pe lângă translocaţii, în etiologia avortului spontan sunt implicate şi anomalii genetice în special legate de cromosomul X sau mutaţii ale liniei germinale. Progresele înregistrate în analiza secvenţei genomice permit acum secvenţierea probelor din screeningul preimplantaţional pentru a descoperi o cauză genetică singulară.
Datorită scăderii nivelului folaţilor la pacientele cu cariotip anormal al produşilor de concepţie, se recomandă suplimentarea preconcepţională a folaţilor [12]. O a doua strategie terapeutică propusă pentru pacientele cu BA ca urmare a vârstei materne înaintate este FIV cu diagnostic genetic preimplantare. Prin acest diagnostic genetic preimplantaţional se urmăreşte excluderea trisomiilor frecvent depistate la sarcinile obţinute după vârsta de 35 de ani [13,14].
Anomaliile uterineRelaţia dintre BA şi malformaţiile uterine (uter
septat, uter bicorn, uter didelf ) este binecunoscută. Studii recente au elucidat mecanismele prin care anomaliile uterine pot induce avortul spontan: scăderea vascularizaţiei la nivelul septului uterin, status inflamator local crescut, reducerea receptorilor hormonali [15]. Tratamentul standard pentru septul uterin este reprezentat de rezecţia perhisteroscopică. Mioamele submucoase care determină o distorsiune a cavităţii uterine pot cauza BA şi scăderea ratei de succes pentru FIV; şi în aceste cazuri rezecţia histeroscopică poate îmbunătăţi fertilitatea şi rata de naşteri [16,17]. De asemenea, sindromul Asherman şi polipii uterini au fost confirmaţi drept factori cauzali pentru AR, iar unele studii au sugerat îmbunătăţirea evoluţiei sarcinii după rezecţia histeroscopică [18]. Prin urmare, pacientele cu BA trebuie investigate prin sonohisterografie pentru a diagnostica defectele uterine. Pe lângă ecografia standard endovaginală, extrem de utilă este ecografia 3D deoarece permite stabilirea unui diagnostic de fineţe pentru patologia cavităţii uterine precum şi pentru malformaţiile uterine [19,20].
EndocrinopatiileDiabetul zaharat netratat reprezintă o cauză bine
cunoscută de avort spontan. Nu aceeaşi relaţie de cauzalitate există însă între formele subclinice de diabet şi avortul spontan [21]. În ceea ce priveşte disfuncţia tiroidiană, pacientele cu AR prezintă mai frecvent anticorpi anti-peroxidază şi anti-tiroglobulină [22]. Studii nerandomizate au evidenţiat faptul că terapia cu
levotiroxină poate reduce rata de BA la pacientele cu anticorpi antitiroidieni prezenţi [22].
Sindromul ovarelor polichistice este o afecţiune endocrină frecvent întâlnită şi care se asociază cu o incidenţă mai mare a avortului spontan. Un diagnostic corect precum şi o conduită adecvată sunt necesare la toate pacientele cu sindromul ovarelor polichistice.
O altă disfuncţie endocrină cu rol în apariţia BA este hiperprolactinemia, iar tratamentul cu bromocriptină s-a dovedit a fi eficient în scăderea incidenţei BA [23]. Prin urmare, este util de determinat nivelul prolactinei la cuplurile cu BA şi de corectat atunci când acesta este crescut.
Bolile infecţioaseÎn timp ce infecţiile acute severe de etiologie
bacteriană, parazitară sau virală pot determina avort spontan sporadic, nu există date clare care să stabilească relaţia dintre portajul bacterian cronic de la nivelul tractului genital şi BA. Deşi mult timp s-a speculat legătura dintre BA şi infecţia cu citomegalovirus, adenovirus, Chlamydia trachomatis sau Mycoplasma hominis, nu există în prezent dovezi clare ale acestei relaţii de cauzalitate [24,25]. Mai mult, deşi vaginoza bacteriană a fost asociată cu BA, această asociere pare să fie mai degrabă legată de avortul de trimestru al doilea decât de cel din primul trimestru de sarcină [26,27].
Trombofiliile congenitaleStudiile efectuate în ultimii ani au demonstrat o
corelaţie între trombofilia congenitală şi avortul spontan din primul şi mai ales al doilea trimestru de sarcină. Trombofilia congenitală determinată de mutaţia factorului V, a genei protrombinei precum şi deficienţa proteinei S sau C, se asociază cu o frecvenţă crescută a avortului spontan sau a complicaţiilor obstetricale de tipul preeclampsie sau oprire în evoluţie a sarcinii. Metaanaliza a 31 de studii a raportat o legătură între factorul V Leiden şi avortul recurent din trimestrul I şi în special cel din trimestrul al doilea [28]. O a doua metaanaliză a relaţiei dintre factorul V Leiden şi complicaţiile sarcinii nu a evidenţiat nicio legătură între acesta şi pierderile din primul trimestru, dar a demonstrat o relaţie clară cu oprirea în evoluţie a sarcinii în trimestrul II sau III [28]. Tratamentul recomandat la pacientele cu trombofilie congenitală şi cu istoric de BA este cu heparină cu greutate moleculară mică, sau cu acid acetilsalicilic [30]. În plus, obstetricienii trebuie să fie avizaţi asupra riscului de apariţie a trombemboliei la aceste paciente în cursul naşterii.
Cauze imunologiceSindromul anticorpilor antifosfolipidici se defineşte
ca o combinaţie de antecedente de tromboze venoase profunde sau arteriale, complicaţii obstetricale specifice

gEnERAL REVIEW
New Therapeutic And Etiologic Perspectives In Recurrent Miscarriage 133
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
sau trombocitopenie alături de confirmarea de laborator a prezenţei anticorpilor antifosfolipidici (AAF) [31]. Ultimul criteriu include: titruri medii sau mari de anticorpi Ig G sau Ig M anticardiolipinici, titrul crescut de anticorpi Ig G sau Ig M anti-β2-glicoproteină I, sau prezenţa anticoagulantului lupic. AAF trebuie identificaţi la mai mult de două determinări la un interval de cel puţin 12 săptămâni. Complicaţiile obstetricale includ cel puţin o sarcină oprită în evoluţie la peste 10 săptămâni de gestaţie, cel puţin o naştere prematură înainte de 35 de săptămâni, sau cel puţin 3 avorturi spontane consecutive înainte de 10 săptămâni de gestaţie. AAF pot fi identificaţi prin screeningul anticorpilor legaţi direct de epitopii proteinelor (β2-glicoproteina-I, protrombina, anexina V), prin depistarea indirectă a anticorpilor îndreptaţi contra proteinelor matricii fosfolipidice (cardiolipina şi fosfatidilserina), sau prin evaluarea efectelor AAF asupra coagulării, sau activarea in vitro a protrombinei (anticoagulantul lupic) [32].
S-a demonstrat că 5-15% dintre femeile cu BA au AAF comparativ cu 2-5% din populaţia obstetricală generală [33]. Aceşti anticorpi sunt în legătură strânsă mai degrabă cu pierderile fetale decât cu cele embrionare [34]. Tratamentul pacientelor cu AAF necesită atât heparine cu greutate moleculară mică cât şi doze mici de aspirină.
În scopul argumentării implicării factorilor imunologici în avortul spontan o serie de studii au sugerat existenţa unei relaţii între nivelurile ridicate ale celulelor NK circulante şi BA. Principala teorie este aceea conform căreia activitatea excesivă a celulelor NK deciduale poate afecta implantarea blastocistului sau placentaţia iniţială, determinând avortul. Yamada şi colegii săi au arătat faptul că un nivel crescut periconcepţional al celulelor cu activitate NK în sângele periferic şi procentul de celule NK circulante pot semnala pierderea ulterioară a unei sarcini cu cariotip normal la pacientele cu BA [35]. Interacţiunea anormală dintre celulele NK deciduale şi antigenele trofoblastului poate activa această capacitate citotoxică, determinând anomalii de placentaţie. Celulele NK deciduale din patul placentar exprimă receptori imunoglobulin-like pentru celulele NK care se pot lega de moleculele de HLA-C de pe celulele trofoblastice, proces care, în mod normal, declanşează elaborarea de către celulele NK a unor factori angiogenetici şi de creştere care susţin invazia trofoblastică. Dimpotrivă, prezenţa haplotipurilor KIR AA pe celulele NK deciduale, în special a activatorului KIR pentru grupele HLA-C2 (KIR2DS1), legate de HLA-C2 la nivelul trofoblastului poate determina apariţia preeclampsiei şi a BA [36]. Acesta reprezintă încă un domeniu deschis cercetării. Momentan nu există însă
nicio dovadă a utilităţii determinării nivelului celulelor NK circulante la pacientele cu AR sau a terapiei celor cu o activitate crescută a celulelor NK.
Boala celiacăBoala celiacă este o afecţiune imunologică caracterizată
prin malabsorbţie şi atrofia vililor intestinali, modificări care pot fi remise prin excluderea glutenului din alimentaţie. Ultimele studii arată corelaţia dintre boala celiacă şi avortul recurent. Kotze a raportat o prevalenţă mai mare a BA la 76 de paciente adulte cu boală celiacă versus 84 paciente din grupul de control cu sindrom de colon iritabil (24,4% versus 11,6%) [37]. De asemenea, el a observat că prognosticul sarcinilor s-a îmbunătăţit la 12 paciente cu boală celiacă după tratament, cu o reducere a BA de la 38,9% până la 5,6% (p=0,045). Observaţii similare au fost efectuate şi de alţi autori [38]. Prin urmare, boala celiacă simptomatică poate fi asociată cu BA, iar tratamentul acesteia poate reduce incidenţa BA [39].
Discuţii
Dată fiind frecvenţa mare a cauzelor genetice în etiopatogenia BA, o primă recomandare în evaluarea cuplurilor cu AR este aceea de a efectua un cariotip al părinţilor precum şi cariotiparea produşilor de avort. Investigarea patologiei placentare pentru a descoperi incluzii ale trofoblastului poate fi utilă atunci când nu s-a efectuat cariotiparea produsului avortat şi atunci când se produc avorturi euploide intermitente la aceeaşi vârstă de gestaţie. În viitorul apropiat secvenţierea genomică a produşilor de avort va deveni o opţiune şi va identifica cu siguranţă mutaţii X-linkate, autosomal recesive şi ale liniei germinale. Tratamentul pentru pacientele cu avorturi spontane aneuploide trebuie să includă suplimentarea nutriţională cu folaţi.
Ca metodă standard de abordare rămâne investigarea pacientelor pentru anomalii uterine prin sonohisterografie şi ecografie 3D. Bineînţeles, înainte de programarea unei noi sarcini, anomaliile depistate necesită un tratament corespunzător. Pentru eliminarea unor cauze endocrine se recomandă testarea nivelului prolactinei, al TSH-ului şi a anticorpilor antitiroidieni. În cele din urmă, investigaţiile pentru depistarea trombofiliei şi a AAP trebuie efectuate în BA de cauză neprecizată, iar evidenţierea acestora necesită tratament cu heparină cu greutate moleculară mică sau doze mici de aspirină.
Concluzii
Boala abortivă afectează 1%-3% din cupluri şi reprezintă o problemă de mare actualitate cu încă multiple necunoscute în ceea ce priveşte mecanismele

gEnERAL REVIEW
Grigore et al 134
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
etiopatogenice. Anomaliile uterine, factorii genetici, endocrini, imunologici, trombofilia reprezintă factori cunoscuţi a fi implicaţi în etiopatogenia avortului recurent. Actual se discută şi despre implicarea glicoproteinelor şi a unor receptori hormonali nucleari în etiopatogenia acestei afecţiuni. Strategia terapeutică include tratamentul cu derivaţi de heparină cu greutate moleculară mică sau cu aspirină, deşi numai un număr limitat de trialuri au demonstrat eficienţa acestora.
Boala abortivă este o problemă importantă de sănătate, motiv pentru care este imperioasă continuarea cercetărilor pentru clarificarea etiologiei şi îmbunătăţirea conduitei.
Referinţe
1. Carrington B, Scacks G, Regan L. Recurrent miscarriage: pathophysiology and outcome. Curr Opin Obstet Gynecol 2005;17:591-7.
2. Regan L. Recurrent miscarriage. Br Med J 1991;302:543-4.
3. Toth B, Jeschke U, Rogenhofer N, et al. Recurrent miscarriage: current concepts in diagnosis and treatment. J Reprod Immunol 2010;85:25-32.
4. Nybo Andersen AM, Wohlfahrt J, Christens P, Olsen J, Melbye M. Maternal age and fetal loss: population based register linkage study. Br Med J 2000;320:1708-12.
5. Stern JJ, Dorfmann AD, Gutierrez-Najar AJ, Cerrillo M, Coulam CB. Frequency of abnormal karyotypes among abortuses from women with and without a history of recurrent spontaneous abortion. Fertil Steril 1996;65:250-3.
6. Rubio C, Simon C, Vidal F, et al. Chromosomal abnormalities and embryo development in recurrent miscarriage couples. Hum Reprod 2003;18:182-8.
7. Keefe DL, Marquard K, Liu L. The telomere theory of reproductive senescence in women. Curr Opin Obstet Gynecol 2006;18:280-5.
8. Habayeb OM, Konje JC. The one-stop recurrent miscarriage clinic: an evaluation of its effectiveness and outcome. Hum Reprod 2004;19:2952-8.
9. Fryns JP, Van Buggenhout G. Structural chromosome rearrangements in couples with recurrent fetal wastage. Eur J Obstet Gynecol Reprod Biol 1998;81;171-6.
10. Stephenson MD, Sierra S. Reproductive outcomes in recurrent pregnancy loss associated with a parental carrier of a structural chromosome rearrangement. Hum Reprod 2006;21:1076-82.
11. Fischer J, Colls P, Escudero T, Munné S. Preimplantation genetic diagnosis (PGD) improves
pregnancy outcome for translocation carriers with a history of recurrent losses. Fertil Steril 2010;94(1):283-9.
12. George L, Mills JL, Johansson AL, et al. Plasma folate levels and risk of spontaneous abortion. JAMA 2002;288:1867-73.
13. Hardarson T, Hanson C, Lundin K, et al. Preimplantation genetic screening in women of advanced maternal age caused a decrease in clinical pregnancy rate: a randomized controlled trial. Hum Reprod 2008;23(12):2806-12.
14. Mastenbroek S, Twisk M, van Echten-Arends J, et al. In vitro fertilization with preimplantation genetic screening. N Engl J Med 2007;357:9-17
15. Devi Wold AS, Pham N, Arici A. Anatomic factors in recurrent pregnancy loss. Semin Reprod Med 2006;24:25-32.
16. Fernandez H, Sefrioui O, Virelizier C, Gervaise A, Gomel V, Frydman R. Hysteroscopic resection of submucosal myomas in patients with infertility. Hum Reprod 2001;6:1489-92.
17. Bajeckal N, Li TC. Fibroids, infertility and pregnancy wastage. Hum Reprod 2000;6:614-20.
18. Sanders B. Uterine factors and infertility. J Reprod Med 2006;51:169-76.
19. Grigore M, Cojocaru C, Mares A, Indrei A. Mullerian duct anomalies: clinical issues and 3D ultrasound diagnosis. Gineco.ro 2009;5:100-6.
20. Grigore M, Mares A. Applications of 3D-ultrasound in female infertility. Rev Med Chir Soc Med Natur 2009;113(4):1113-9.
21. Mills JL, Simpson JL, Driscoll SG, et al. Incidence of spontaneous abortion among normal women and insulin-dependent diabetic women whose pregnancies were identified within 21 days of conception. N Engl J Med 1988;319:1617-23.
22. Stagnaro-Green A, Glinoer D. Thyroid autoimmunity and the risk of miscarriage. Best Pract Res Clin Endocrinol Metab 2004;18(2):167-81.
23. Hirahara F, Andoh N, Sawai K, Hirabuki T, Uemura T, Minaguchi H. Hyperprolactinemic recurrent mis-carriage and results of randomized bromocriptine treatment trials. Fertil Steril 1998;70(2):246-52.
24. Matovina M, Husnjak K, Milutin N, Ciglar S, Grce M. Possible role of bacterial and viral infections in miscarriages. Fertil Steril 2004;81(3):662-9.
25. Sugiura-Ogasawara M, Ozaki Y, Nakanishi T, Kumamoto Y, Suzumori K. Pregnancy outcome in recurrent aborters is not influenced by Chlamydia IgA and/or G. Am J Reprod Immunol 2005;53:50-3.

gEnERAL REVIEW
New Therapeutic And Etiologic Perspectives In Recurrent Miscarriage 135
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012
26. Ralph SG, Rutherford AJ, Wilson JD. Influence of bacterial vaginosis on conception and miscarriage in the first trimester: cohort study. Br Med J 1999;319:220-3.
27. Oakeshott P, Hay P, Hay S, Steinke F, Rink E, Kerry S. Association between bacterial vaginosis or chlamydial infection and miscarriage before 16 weeks’ gestation: prospective community based cohort study. BMJ 2002;325:1334.
28. Rey E, Kahn SR, David M, Shrier I. Thrombophilic disorders and fetal loss: a meta-analysis. Lancet 2003;361:901-8.
29. Dudding TE, Attia J. The association between adverse pregnancy outcomes and maternal factor V Leiden genotype: a meta-analysis. Thromb Haemost 2004;91:700-11.
30. Ghosh K, Shetty S, Vora S, Salvi V. Successful pregnancy outcomein women with bad obstetric history and recurrent fetal loss due to thrombophilia: effect of unfractionated heparin and low-molecular wight heparin. Clin Appl ThrombHemost 2008;14:174-9.
31. Miyakis S, Lockshin MD, Atsumi T, et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost 2006;4:295-306.
32. Galli M, Luciani D, Bertolini G, Barbui T. Anti-beta 2-glycoprotein I, antiprothrombin antibodies, and the risk of thrombosis in the antiphospholipid syndrome. Blood 2003;102:2717-23.
33. Branch DW, Gibson M, Silver RM. Clinical practice. Recurrent miscarriage. N Engl J Med 2010;363:1740-7.
34. Rai RS, Clifford K, Cohen H, Regan L. High prospective fetal loss rate in untreated pregnancies of women with recurrent miscarriage and antiphospholipid antibodies. Hum Reprod 1995;10:3301-4.
35. Yamada H, Morikawa M, Kato EH, Shimada S, Kobashi G, Minakami H. Pre-conceptional natural killer cell activity and percentage as predictors of biochemical pregnancy and spontaneous abortion with normal chromosome karyotype. Am J Reprod Immunol 2003;50:351-4.
36. Hiby SE, Walker JJ, O’Shaughnessy KM, et al. Combinations of maternal KIR and fetal HLA-C genes influence the risk of preeclampsia and reproductive success. J Exp Med 2004; 200:957-65.
37. Kotze LM. Gynecologic and obstetric findings related to nutritional status and adherence to a gluten-free diet in Brazilian patients with celiac disease. J Clin Gastroenterol 2004;38(7):567-74.
38. Tata LJ, Card TR, Logan RF, Hubbard RB, Smith CJ, West J. Fertility and pregnancy-related events in women with celiac disease: a population-based cohort study. Gastroenterology 2005;128(4):849-55.
39. Tursi A,Giorgetii G, Brandimarte G, Elisei W. Effect of gluten-free diet on pregnancy outcome in celiac disease patients with recurrent miscarriages. Dig DisSci 2008;53:2925-2928.

Mick Jager ?!
Renal cysts (US)
Aneurysm, cycle of willis (brain CT)

Diagnosis Of A Digital Nodule By Fine Needle Aspiration Cytology 137
Rezumat
Un bărbat de 84 de ani, cu un nodul nedureros al degetului V al mâinii stângi, a fost supus aspiraţiei cu ac fin pentru citologia leziunii (fine needle aspiration cytology-FNAC). Examenul citologic a evidenţiat cristale birefringente tipice de uraţi pentru diagnosticul de tof gutos. Acidul uric seric al pacientului a fost de 10mg/dl (normal 3,5-7,2 mg/dl), confirmând diagnosticul de gută. FNAC este o procedură uşoară şi minim invazivă pentru diagnosticul de tofi gutoşi.
Cuvinte cheie: guta, aspiraţie cu ac fin
Introducere
Guta este în majoritatea cazurilor o boală metabolică ereditară. Boala este promovată de o dietă bogată în purine şi prezintă o evoluţie intermitentă cu manifestări inflamatorii articulare şi perioade libere de simptome. Semnul patognomonic al bolii este o monartrită acută şi foarte dureroasă, cu depozite locale tipice de acid uric, aşa-numiţii tofi gutoşi [1].
Raportăm un caz rar în care diagnosticul a fost făcut citologic şi apoi confirmat prin metode convenţionale de investigare.
Prezentarea cazului Un bărbat de 84 de ani s-a prezentat la clinica de
ortopedie cu un nodul nedureros la articulaţia interfalangiană distală a degetului V al mâinii stângi, cu dimensiuni variind între 1-1,5 cm diametru (Fig. 1).
La examinarea nodulului, acesta nu a fost moale, dar a existat o limitare la linia de flexiune a articulaţiei distale interfalangiene. Radiografia a arătat distrugerea severă a articulaţiei interfalangiene distale (Fig. 2 şi 3).
Diagnosticul diferenţial a inclus metastazele, tumoră primară şi gută, deşi antecedentele nu au
diAGnosticul unui nodul diGitAl pRin citoloGiA AspiRAtiVĂ cu Ac Fin
Halpern Marisa1, Vigler Mordechai2, Rath-Wolfson Lea1, Schwartz Ariel1, Koren Rumelia1, Gal Rivka1
Departamentele de 1Patologie şi 2Chirurgie Ortopedică, Spitalul Hasharon, Centrul Medical Rabin, Petah Tikva, afiliat la Facultatea de Medicină Sackler, Universitatea Tel-Aviv, Israel
Adresa pentru corespondenţă:Prof. Gal Rivka Department of Pathology, Hasharon Hospital, POB 101, Petah-Tikva, Israel. Tel: 972-3-9372390, Fax: 972-3-9372349 E-mail: [email protected] Primit: 20.01.2012 Acceptat: 15.04.2012 Med Con October 2012, Vol 7, No 3, 137-140
cAsE PREsEnTATIOn
Figura 1. Aspectul clinic al degetului V al mâinii stângi

Halpern et al138
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012cAsE PREsEnTATIOn
evidenţiat nicio criză episodică de artrită. Deoarece pacientul a fost sub tratament cu coumadin pentru aritmie după chirurgie cardiacă a fost trimis pentru FNAC în loc de biopsie chirurgicală.
Un ac de 23 gauge şi o seringă au fost plasate întrun suport de aspiraţie al leziunilor palpabile. După ce acul a fost plasat în partea laterală a leziunii, a fost aplicată
presiune negativă asupra acului cu seringă. Au fost efectuate mai multe curse ale aspiratorului în leziune înainte de retragerea acului. Procedura a fost repetată de două ori pentru a ne asigura că a fost obţinut pentru diagnostic material adecvat. Prin aspiraţie a fost obţinut un material alb care a fost expus pe lamele de sticlă. Acesta a fost întins cu o altă lamelă, fixat cu cytospray şi colorat cu hematoxilină şi eozină (H&E).
Microscopia cu lumină a lamelelor a arătat ristale eozinofilice subţiri în formă de ace cu capetele ascuţite, distribuite individual sau în grupuri (Figura 4). Ele au aratat o birefringenţă puternică în lumină polarizată corespunzând cristalelor de urat monosodic (Figura 5).
La o examinare suplimentară, acidul uric seric al pacientului a fost de 10mg/dl (valori normale 3,5-7,2 mg/dl), confirmându-se diagnosticul de gută. La examinarea de urmărire la două săptămâni, nu au existat semne de hemoragie sau inflamaţie a degetului.
Discuţie
Guta este o boală comună asociată cu depunerea de cristale de urat monosodic (MSU), în ţesuturile
Figura 2. Radiografie laterală a degetului V – leziune litică extinsă cu eroziune severă şi
distrugerea articulaţiei interfalangiene distale
Figura 3. Radiografie AP a degetului V arătând de asemenea distrugerea severă a articulaţiei
interfalangiene distale
Figura 4. Coloraţie hematoxilină & eozină arătând cristale în formă de ace
Figura 5. Microscopia în lumină polarizată arată birefringenţa cristalelor în formă de ace subţiri

Diagnosis Of A Digital Nodule By Fine Needle Aspiration Cytology 139
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012 cAsE PREsEnTATIOn
articulare sau periarticulare şi în tractul urinar. În general, progresează prin patru etape clinice dacă nu este tratată: hiperuricemie asimptomatică, gută acută, gută intercritică sau de interval şi gută tofică cronică. Deşi tofii gutoşi sunt observaţi în boala cronică, ei pot fi primul semn al bolii [2].
Diagnosticul de gută poate fi problematic atunci când prezentarea este atipică şi acidul uric seric este la valoarea limită. Ocazional, guta se poate prezenta ca un tof de ţesut moale, fără antecedente de artrită dureroasă sau hiperuricemie. Diagnosticul diferenţial al nodulilor articulari include tumora cu celule gigante a tecii tendonului, tumora cu celule gigant a osului şi tumori metastatice [3]. Demonstrarea de cristale de urat monosodic prin FNAC în frotiurile din mase nodulare stabileşte diagnosticul de gută fără echivoc [4].
Avantajele FNAC faţă de biopsia deschisă şi alte proceduri chirurgicale au făcut din FNAC o procedură din ce în ce mai populară. În cazul nostru, cu toate că pacientul a fost sub coumadină, nu au existat reacţii adverse după FNAC.
Cristalele birefringente pot fi găsite în tofii gutoşi (urat monosodic) şi în depozitele de pseudogută (pirofosfat de
calciu). Examinarea atentă a cristalelor va dezvălui diferenţe distincte între cele două procese: cristalele din gută sunt în formă de ac cu capete ascuţite pe când cristalele de pirofosfat de calciu sunt mai scurte, rombice şi au capete boante sau pătrate. De asemenea, cristalele gutoase sunt puternic (negativ) birefringente, pe când cristalele din pseudogută au o birefringenţă slabă (pozitivă) la polarizare [3].
Un alt avantaj al FNAC faţă de excizia bioptică: cristalele de uraţi sunt adesea pierdute în timpul prelucrării histologice deoarece se dizolvă în formol, dar ele sunt păstrate în frotiurile de FNAC care sunt fixate cu alcool.
Agarwal şi colab. [5] au trecut în revistă literatura (2007) şi au găsit şase rapoarte publicate de tofi gutoşi diagnosticaţi prin FNAC. Acestea au inclus 17 cazuri cu diagnostic clinic de artrită gutoasă (5 cazuri), tumori cu celule gigant (5 cazuri), tumori metastatice (2 cazuri), sarcom (2 cazuri), artrită (1 caz), iar în 2 cazuri diagnosticul nu a fost determinat. Nivelul acidului uric a fost ridicat în 5 cazuri, normal în 7 şi scăzut în 2 cazuri [4,6,7,8,9,10].
De atunci, alte câteva cazuri au fost raportate, [11,12,13,14] ajungându-se la un total de 23 de cazuri (Tabelul I).
Tabel I. Rezumatul rapoartelor publicate de gută, diagnosticate prin FNAC Autor An Nr de cazuri Localizarea anatomică Diagnosticul clinic Gal et al 2012 1 deget V mana stângă metastaze? gută? Koley et al. [2] 2010 1 picioarele şi degetele bilatera, palma stângă, cotul
drept, helixul urechii stângi artrită
Gupta et al. [13] 2009 1 articulaţia cotului stâng şi în apropiere de maleola laterală a piciorului stâng
nu a fost dat
Angeles et al. [12] 2008 1 nu există date nu există date Purohit et al. [11] 2006 1 noduli la extremităţi leziune neoplastică benignă Bhadani et al. [4] 2006 7 picior dorsal şi braţ gută
mână şi picior gută deget II picior drept gută mâinile şi picioarele tumori metastatice degetul mic stâng GCT olecran drept GCT deget I picior drept GCT
Sah et al. [6] 2 antebraţe, mâini, picior dorsal, maleola laterală tumori metastatice aspect palmar peste baza degetului mic GCT
Paik et al. [7] 2002 1 mâini, picioare, helixul urechii artrită reumatoidă Rege et al. [8] 2000 2 noduli pe maleola B\L artrită
noduli pe piciorul dorsal, solear, maleola laterală Nicol et al. [9] 1997 3 dorsal ulnar, antebrat distal drept guta?
articulaţiile I şi II metacarpiene sarcom piciorul şi glezna dreaptă gută
Liu et al. [14] 1996 1 masă ulnară dreaptă distală sarcom Nasser et al. [10] 1994 2 vertebre la nivelul C3 L4 GCT
nodul al antebraţului nu a fost dat GCT=Giant cell tumor

Halpern et al140
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012cAsE PREsEnTATIOn
FNAC înlocuieşte în prezent, alte investigaţii datorită rapidităţii, invazivităţii reduse, tehnicii mai simple şi cost-eficiente. Evidenţierea cristalelor în frotiurile FNAC este superioră secţiunilor histopatologice în cazul cărora cristalele sunt mai frecvent pierdute în timpul procesării. În analiza lichidului articular cristalele simultane cum ar fi hidroxiapatita, steroizi, etc pot provoca confuzie [8].
Concluzie
FNAC este o procedură simplă, minim invazivă şi cost-eficientă pentru diagnosticarea tofilor gutoşi. Are acurateţe şi ar trebui să fie utilizată înainte de biopsia chirurgicală.
Referinţe
1. Ott I, Gartenschläger M, Schmeck S, Baier G. Atypical gout tophi for differential diagnosis of head and neck tumors: case report and review of the literature. HNO 2009;57(12):1280-4.
2. Koley S, Salodkar A, Choudhary S, Bhake A, Singhania K, Choudhury M. Tophi as first manifestation of gout. Indian J Dermatol Venereol Leprol 2010;76(4):393-6.
3. Dodd LG, Major NM. Fine-needle aspiration cytology of articular and periarticular lesions. Cancer 2002;96(3):157-65.
4. Bhadani PP, Sah SP, Sen R, Singh RK. Diagnostic value of fine needle aspiration cytology in gouty tophi: a report of 7 cases. Acta Cytol 2006;50(1):101-4.
5. Agarwal K, Pahuja S, Agarwal C, Harbhanjanka A. Fine needle aspiration cytology of Gouty Tophi with review of literature. J Cytol 2007;24:142-5.
6. Sah SP, Rani S, Mahto R. Fine needle aspiration of gouty tophi: a report of two cases. Acta Cytol 2002;46:784-5.
7. Paik SS, Park MH. Fine needle aspiration cytology of gouty tophus in a patient with rheumatoid arthritis. Acta Cytol 2002;46:1024-5.
8. Rege J, Shet T, Naik L. Fine needle aspiration of tophi for crystal identification in problematic cases of gout. A report of two cases. Acta Cytol 2000;44:433-6.
9. Nicol KK, Ward WG, Pike EJ, Geisinger KR, Capperllari JO, Scott EK. Fine needle aspiration biopsy of gouty tophi; lessons in cost effective patient management. Diagn Cytopathol 1997;17:30-5.
10. Nasser IA, Fayyad LM, Soudi NM, Bardawil RG. Fine needle aspiration cytology in the diagnosis of gouty tophi: the role of Diff-Quick stain in the evaluation of unexpected lesions. Acta Cytol 1994;38:840.
11. Purohit MB, Purohit TM, Tandon RK. FNAC of gouty tophi – a case report. Microbiol 2006;49(1):42-3.
12. Angeles RM, Gong Y. Fine needle aspiration of a subcutaneous gouty tophus. Diagn Cytopathol 2008;36(7):494-5.
13. Gupta A, Rai S, Sinha R, Achar C. Tophi as an initial manifestation of gout. J Cytol 2009;26(4):165-6.
14. Liu K, Moffatt EJ, Hudson ER, Layfield LJ. Gouty tophus presenting as a soft-tissue mass diagnosed by fine-needle aspiration: a case report. Diagn Cytopathol 1996;15(3):246-9.
Traducere: Bumbuluţ Călin

Nephrogenic Adenoma, Report Of Two Cases And Review Of The Literature 141
Rezumat
Adenomul nefrogenic (NA), este o leziune mai puţin frecventă benignă a tractului urotelial, caracterizat printr-o proliferare la nivelul tubilor, chistelor şi papilelor marginite de celule cuboidale joase până la epiteliu columnar. NA poate fi o capcană semnificativă de diagnostic întrucât anumite caracteristici histologice cum ar fi prezenţa nucleelor mărite cu nucleoli proeminenţi, atipii nucleare degenerative, mici tubi simulând celule în inel cu pecete, precum şi invazia focală în muşchiul superficial, atunci când scoase din context, pot mima malignitatea. Raportăm două cazuri de NA, un bărbat şi o femeie prezentând unele caracteristici histologice îngrijorătoare şi revizuim criteriile de diagnostic, precum şi malignităţile morfologice pertinente pe care le care imită NA.
Cuvinte cheie: adenom nefrogenic, vezica urinară, Cytokeratin-7, Cytokeratin-20, P504S
Introducere
Adenoamele nefrogenice (NA) sunt leziuni benigne de tip tumoral ale uroteliului. Este o leziune rară a tractului urinar considerată în general a fi un răspuns
metaplazic la leziunea urotelială [1]. Prezintă o proliferare ale glandelor care poate apare în mai multe locuri în cadrul tractului urogenital. Deşi este benign, aspectul histopatologic poate fi uneori confundat cu o malignitate, în special în biopsiile din jurul uretrei prostatice. NA este o leziune rară a tractului urinar, asociată cu antecedente de traumatisme sau iritaţii ale uroteliului. Factorii predispozanţi includ infecţii, calculi, intervenţii chirurgicale, traumatisme şi transplant renal [2].
Elementele de diagnostic care sunt utile în recunoaşterea acestei entităţi sunt un amestec caracteristic de modele arhitecturale variate, edem stromal asociat şi inflamaţie, teci hialine în jurul tubilor, secreţii eozinofilice de tip coloidal între tuburi şi lipsa activităţii mitotice [3]. Histologic se compune din tubi, cordoane, celule individuale şi/sau celule în inel cu pecete în cadrul uroteliului, care se pot extinde în peretele muscular şi mimează adenocarcinomul [4]. NA poate prezenta papile, precum şi un model de creştere focală solid; cu toate acestea, evident modelul de creştere solidă difuză este extrem de neobişnuit. Celulele care delimitează tubii, chisturile şi papilele sunt cuboidale, columnare joase, cu citoplasmă redusă palidă. Ocazional pot fi văzute celule clare în special în zonele solide. Deşi
AdenoMul neFRoGenic, pReZentARe A douĂ cAZuRi şi o ReVistĂ A liteRAtuRii
Rath-Wolfson Lea1,2, Schwartz Ariel1,2, Leikin Anna1,2, Koren Rumelia1,2, Gal Rivka1,2
Departamentul de 1Patologie, Spitalul Hasharon, Centrul Medical Rabin, Petah Tikva, afiliat la 2Facultatea de Medicină Sackler, Universitatea Tel-Aviv, Israel
Adresa pentru corespondenţă:Rath- Wolfson Lea, MD Department of Pathology, Hasharon Hospital, Rabin Medical Center, Petah Tikva, Israel Fax: 972-3-9372349 E-mail: [email protected] Primit: 11.01.2012 Acceptat: 01.02.2012 Med Con October 2012, Vol 7, No 3, 141-144
cAsE PREsEnTATIOn

Rath-Wolfson et al142
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012cAsE PREsEnTATIOn
pot fi observate în unele cazuri nuclee mărite şi nucleoli proeminenţi, atipiile nucleare semnificative, inclusiv prezenţa mitozei, sunt extrem de rare. Atipia nucleară atunci când este prezentă, apare ca degenerare cu cromatină indistinctă, neclară [3,5]. Multe structuri normale şi leziuni patologice în sistemul genito-urinar pot semăna histologic cu procesele neoplazice. Deşi unele, precum NA, pot fi văzute în locaţii diferite, majoritatea sunt identificate în anumite organe şi ca atare au consideraţii unice de diagnostic diferenţial specifice acelui organ [6].
Raportăm două cazuri de NA şi o revistă a literaturii de specialitate, concentrându-ne pe diagnosticul diferenţial patologic şi studiile imunohistochimice.
Prezentare de cazuri
Cazul 1 Un bărbat de 61 de ani a fost internat în
Departamentul de Urologie pentru reevaluarea unei tumori de vezică urinară. El suferea de un carcinom cu celule tranziţionale de grad înalt, stadiu T1 din anul 2003, trecând prin mai multe cure de tratament intravezical cu BCG, după rezecţia transuretrală a tumorii vezicale (TURBT). La cistoscopie nu au fost observate leziuni. Au fost prelevate biopsii aleatorii. În urma unei examinări microscopice în lamina propria a mucoasei vezicii urinare a existat o concentrare de tubi mici şi glande, delimitate de celule cuboidale (Fig. 1, pag. 64).
Celulele nu au prezentat nicio atipie semnificativă şi nu au fost găsite mitoze. Tubii şi glandele au fost însoţite de infiltrat inflamator cronic. Coloraţiile imunohistochimice pentru Pan Cytokeratin, Cytokeratin-7, EMA şi P504S au fost pozitive în tubii mici. Cytokeratin-20, PSA şi Fosfataza Acidă Prostatică Specifică (PSAP) au fost negative. Ki-67 a fost negativă în tubi şi pozitivă în unele limfocite (Fig. 2, pag. 65). A fost luat în considerare diagnosticul diferenţial cu adenocarcinomul de prostată, adenocarcinomul vezicii urinare, dar acestea au fost excluse cu ajutorul colorării imunohistochimice, Tabelul I.
Aceste constatări au fost compatibile cu diagnosticul de AN.
Cazul 2 O femeie de 68 de ani, suferind de cistinurie cu
evoluţie spre insuficienţă renală cronică tratată cu hemodializă din 2008. În octombrie 2006 a fost internată pe secţia de Urologie cu dureri abdominale inferioare şi în flanc şi hematurie. A fost efectuată cistoscopia, fiind relevate focare de mucoasă vezicală ulcerată fără leziuni ocupante de spaţiu. Endoscopic aceste constatări au fost în concordanţă cu diagnosticul de leziune Hunner. Leziunea Hunner este o leziune inflamatorie distinctivă care prezintă o ruptură profundă caracteristică prin mucoasă şi submucoasă provocate de distensia vezicii urinare. Au fost prelevate biopsii din zonele ulcerate. La examinarea microscopică a fost observată infiltrarea tubilor delimitate de celule epiteliale clare în lamina propria, (Fig. 3, pag. 66).
Colorarea imunohistochimică pentru Cytokeratin 7 a fost pozitivă în timp ce pentru Cytokeratin 20 a fost negativă. Ki-67 a fost pozitivă numai în limfocite. Aceste constatări au ridicat suspiciunea de carcinom cu celule clare, dar nu diagnostice. Alte zone au arătat infiltrare masivă de limfocite, celule plasmatice şi histiocite care au fost imunocolorate cu CD68. Tratamentul pentru cistita interstiţială cu DMSO a fost întrerupt din cauza unor modificări severe iritative. În ianuarie 2010, la şase luni după tratament în timp ce era asimptomatică, a fost efectuată cistoscopia de control. A fost biopsiată o mică leziune de 2-3mm găsită pe peretele posterior al vezicii urinare.
La examenul microscopic leziunea a fost compusă din mici tubi şi glande situate în lamina propria lângă o zonă de infiltrat inflamatoriu cronic. Nu au fost observate nici atipii, nici elemente mitotice. Coloraraţiile imunohistochimice pentru Cytokeratin-7 şi P504S au fost pozitive, Cytokeratin-20 a fost negativă. Ki-67 a fost pozitivă în doar câteva celule (Tabelul I). Aceste descoperiri au fost compatibile cu diagnosticul de NA.
Tabelul I. Diferite coloraţii imunohistochimice
Markeri Adenom nefrogenic
Adenocarcinom al vezicii urinare
Carcinom cu celule renale
Adenocarcinom de prostata
CK 7 + + - -EMA + +/- +/- +/-P504S + - - +CK20 - + - -PSAP - - - +Ki67 - ++ ++ ++

Nephrogenic Adenoma, Report Of Two Cases And Review Of The Literature 143
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012 cAsE PREsEnTATIOn
Discuţie
Vezica urinară este cea mai comună localizare pentru NA, de obicei peretele posterior. Ocazional poate fi găsit în pelvisul renal, ureter, sau uretră. Se găseşte la adulţii tineri, cu o predominenţă a sexului masculin (2:1). Aproximativ jumătate din cazuri sunt găsite după o intervenţie chirurgicală genito-urinară, inclusiv transplant renal. NA este de asemenea asociat cu calculi, traume şi cistită. De obicei leziunile sunt asimptomatice, cu toate că pacienţii prezintă frecvent hematurie sau disurie. Se poate prezenta ca o masă exofitică papilară sau poliploidică sau ca o leziune catifelată, care seamănă cistoscopic cu neoplazia. Formele sesile constituie circa 25% până la 30% din cazuri. Structurile papilare măsoară de obicei mai puţin de 1 cm, rareori mai mult de 5 cm.
Modelul histologic clasic este acela al tubilor mici asemănători cu tubii renali. Tubii sunt delimitaţi de cuiburi de celule asemănătoare cu endoteliul spaţiilor vasculare şi sunt adesea înconjuraţi de un strat de membrană bazală hialinizată.
NA poate semăna cu adenocarcinomul vezicii urinare sau de prostată şi de asemenea cu unele tumori benigne sau maligne de uracă [6]. Absenţa stratificării epiteliale şi caracteristicile celulare eozinofilice, cuboidale, columnare joase, sau celulele ţintă, ar trebui să alerteze patologul pentru diagnosticul corect.
Coloraţiile imunohistochimice pentru EMA, cytokeratin-7, P504S şi PAX-2 sunt pozitive. Ki-67 este pozitivă doar în câteva celulele. Cytokeratin-20, PSA şi Fosfataza Acidă Prostatică Specifică (PSAP) sunt negative.
P504S este de asemenea pozitiv în NA şi în carcinomul de prostată, prin urmare nu poate face diferenţa între cele două leziuni [7], dar este negativ in carcinomul cu celule clare al vezicii urinare. PSA este de obicei pozitiv în carcinomul de prostată şi negativ în NA, care este frecvent negativ pentru markeri bazocelulari şi de asemenea pentru PSAP. Elementele caracteristice histomorfologice şi imunohistochimice, eventual completate de coloraţiile PAX2 şi/sau PAX8 pozitive, pot fi folosite pentru diagnosticul corect [8,9].
Examinarea atentă a lamelor colorate H&E care nu prezintă displazie, împreună cu negativitatea PSA şi PSAP, pot exclude diagnosticul de carcinom de prostată şi susţin diagnosticul de NA [10].
Mazal şi colab. [11] au arătat că la pacienţii cu transplant renal statusul cromozomilor sexuali 46 NA a fost aceeaşi ca cea a donatorului. Ei au sugerat că NA derivă din celule tubulare ale transplantului renal şi nu au fost proliferări metaplazice ale uroteliului vezicii
primitorului. Acest lucru a fost susţinut de studii imunohistochimice pozitive pentru PAX-2 şi alte studii de aglutinare.
Concluzie Adenomul nefrogenic este o leziune benignă, cu un
larg spectru histologic. NA poate provoca uneori dificultăţi de diagnostic în unele cazuri, precum anumite caracteristici histologice care atunci când scoase din context, pot simula aspectul de adenocarcinom de prostată, variante de carcinom urotelial inclavat şi/sau adenocarcinom cu celule clare.
Profilul imunohistochimic al NA include colorare pozitivă la CK 7, P504S şi PAX-2; colorare negativă cu p63, PSA, PSAP, cytokeratină cu greutate moleculară înaltă (34βE12) şi Ki-67. Ori de câte ori există îndoieli, aceste coloraţii ar trebui să fie efectuate cu scopul de a ajunge la un diagnostic corect.
Referinţe
1. Broecker JS, Steelman CK, Broecker BH, Shehata BM. Nephrogenic Adenoma of the Bladder in a Prune Belly Syndrome Patient: Case Report and Review of the Literature. Fetal Pediatr Pathol. 2011 Aug 15.
2. Martín LL, Cardoso JV, Vivas CM, Muñoz JG, Napurí LF, Enguita CG. Prostatic nephrogenic adenoma. Case report. Arch Esp Urol. 2011;64(5):473-6.
3. Kunju LP. Nephrogenic adenoma: report of a case and review of morphologic mimics. Arch Pathol Lab Med. 2010;134(10):1455-9. 7
4. Allan CH, Epstein JI. Nephrogenic adenoma of the prostatic urethra: a mimicker of prostate adenocarcinoma. Am J Surg Pathol. 2001;25(6):802-8.
5. Amin W, Parwani AV. Nephrogenic adenoma. Pathol Res Pract. 2010;206(10):659-62.
6. Hameed O, Humphrey PA. Pseudoneoplastic mimics of prostate and bladder carcinomas. Arch Pathol Lab Med. 2010;134(3):427-43.
7. Gupta A, Wang HL, Policarpio-Nicolas ML, et al. Expression of alpha-methylacyl-coenzyme A racemase in nephrogenic adenoma. Am J Surg Pathol. 2004;28(9):1224-9.
8. Tong G X, Melamed J, and Mansukhani M. PAX2: a reliable marker for nephrogenic adenoma. Mod Pathol 2006;19(3):356–363
9. Tong G X, Weeden E M, Hamele-Bena D. Expression of PAX8 in nephrogenic adenoma and clear cell adenocarcinoma of the lower urinary tract: evidence of related histogenesis? Am J Surg Pathol 2008;32 (9):1380–1387

Rath-Wolfson et al144
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012cAsE PREsEnTATIOn
10. Skinnider BF, Oliva E, Young RH, Amin MB. Expression of alpha-methylacyl-CoA racemase (P504S) in nephrogenic adenoma: a significant immunohistochemical pitfall compounding the differential diagnosis with prostatic adenocarcinoma. Am J Surg Pathol. 2004;28(6):701-5.
11. Mazal PR, Schaufler R, Altenhuber-Müller R, et al. Derivation of nephrogenic adenomas from renal tubular cells in kidney-transplant recipients. N Engl J Med. 2002;347(9):653-9. Erratum in: N Engl J Med 2002;347(17):1390.
Traducere: Bumbuluţ Călin

Substitution Of The Ureter With The Appendix In Malignant Melanoma Adjacent To The Ureter 145
Rezumat
O femeie 70 de ani s-a prezentat cu dureri în flancul drept, cu durată de 1 an.
CT cu substanţă de contrast a arătat hidroureteronefroză dreaptă şi o masă heterogenă de ţesut moale, cu efect de masă asupra ureterului drept şi a venei cave. Biopsia CT ghidată a masei a fost concordantă cu un melanom malign. Nu au fost găsite dovezi ale tumorii primare.
Chimio-imunoterapia a fost urmată de rezecţia chirurgicală a masei, a venei cave adiacente şi a ureterului implicat. Vena cavă inferioară a fost reparată cu un plasture gortex, iar porţiunea ureterală lipsă a fost înlocuită cu apendicele. Studiile imagistice de urmărire au aratat pasajul liber prin ureterul reconstruit.
Cuvinte cheie: hidroureteronefroză, melanom malign, lipsă ureterală, apendice vermiform
Introducere
Melanomul malign de origine necunoscută reprezintă un procent mic din toate cazurile de melanom. Melanomul metastatic care implică ureterul este extrem de rar. Prezentăm cazul unei femei cu un
melanom retroperitoneal care implică ureterul şi tratamentul chirurgical urmat. În Israel nu a mai fost descris un caz similar.
O femeie de 70 de ani a fost trimisă la serviciul de urgenţă ca urmare a înrăutăţirii severe a durerii în flancul drept de care suferea în ultimul an. Ea prezenta episoade recurente de durere în flancul drept fără febră asociată, simptome urinare sau alte manifestări. Examenul fizic şi analizele sangvine nu au evidenţiat elemente patologice, iar ecografia abdominală a arătat o hidroureteronefroză dreaptă severă. O CT a arătat hidronefroză dreaptă şi dilatare ureterală la nivelul ureterului proximal, unde o masă heterogenă de ţesut moale exercita un efect de masă aparent pe ureterul drept şi vena cavă inferioară. De asemenea, masa exercita efect asupra duodenului, fuzionând cu muşchiul psoas. CT toracic a fost interpretat ca fiind normal. Datorită durerii şi constatărilor imagistice, un tub de nefrostomie percutană (PCN) a fost plasat în rinichiul drept. A fost efectuată o pieloureterografie demonstrând presiune extrinsecă pe ureterul drept. O biopsie CT ghidată în masă a fost în concordanţă cu un melanom malign. De remarcat, alţi doi nevi benigni au fost eliminaţi de pe spatele ei cu trei ani înainte de internarea prezentă. Nu a avut antecedente de melanom. O evaluare atentă
ÎnlocuiReA uReteRului cu Apendicele În MelAnoMul MAliGn AdiAcent uReteRului
Goldberg Hanan, Yossepowitch Ofer, Baniel Jack
Institutul de Urologie, Centrul Medical Rabin, Petah Tikva, afiliat la Facultatea de Medicina Sackler, Universitatea din Tel Aviv, Tel Aviv, Israel
Adresa pentru corespondenţă:Hanan Goldberg MD Institute of Urology Beilinson Hospital, Petah-Tikva, Israel. Tel: 972-3-9376558, Fax: 972-72-2361346 E-mail: [email protected] Primit: 04.03.2012 Acceptat: 15.06.2012 Med Con October 2012, Vol 7, No 3, 145-147
cAsE PREsEnTATIOn

Goldberg et al146
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012cAsE PREsEnTATIOn
genitală şi cutanată efectuată de un dermatolog şi un ginecolog a exclus posibilitatea ca un melanom malign primar să fi fost neobservat. O scanare PET, FDG, CT a relevat absorbţie anormală doar în masa retroperitoneală adiacentă ureterului drept (Figura 1, pag. 70).
În timpul următoarelor şase luni pacienta a urmat cinci cure de cisplatin, dacarbazine şi IL-2 care au fost în general bine tolerate. După terminarea tratamentului sistemic a fost programată rezecţia masei retroperitoneale. În timpul procedurii a fost identificată masa de 3x4 cm, încastrând complet vena cavă inferioară şi o porţiune a ureterului drept. Masa a fost rezecată cu margini de siguranţă chirurgicale necesitând înlocuirea unui segment de 10 cm de venă cavă cu grefă gortex. În plus, un segment proximal ureteral drept de 6 cm a fost rezecat împreună cu masa. Pentru a compensa spaţiul creat în ureter a fost recoltat apendicele vermiform împreună cu vascularizaţia lui şi mobilizat până la punctul în care anastomoza termino-terminală a fost fezabilă. Au fost luate măsuri de precauţie pentru a asigura lipsa tensiunii, anastomoza fiind largă şi etanşă peste 6 FR de autoretenţie a stentului ureteral. De notat că apendicele nu a arătat rate de absorbţie anormale la scanarea PET, permiţând utilizarea acestuia în condiţii de siguranţă ca şi substitut ureteral.
Evoluţia postoperatorie a fost lipsită de evenimente, iar pacienta a fost externată în a şaptea zi postoperator. La trei luni după procedură, o explorare retrogradă pieloureterografică a arătat trecerea clară de material de contrast prin ureterul reconstruit, fără semne de obstrucţie (Figura 2, pag. 70), iar stentul a fost eliminat.
Discuţie
Melanomul malign este unul dintre cele mai agresive tipuri de cancer de piele cunoscute. Factorii primari de risc includ istoricul pozitiv familial, nevi multipli benigni sau atipici şi antecedente de melanom. În Europa de Vest, incidenţa melanomului malign a fost în creştere constantă cu 10-12 cazuri noi diagnosticate la 100.000 de locuitori [1]. Deşi melanomul reprezintă doar 4% din toate cazurile de cancer dermatologic, este asociat cu prognostic nefavorabil, iar supravieţuirea pacienţilor cu melanom metastatic la cinci ani este de 14% [1].
Melanocitele care pot da naştere melanomului malign derivă din creasta neurală. Aceste celule migrează în timpul dezvoltării embrionare de-a lungul liniei mediane şi pot fi găsite în locaţii non-cutanate.
Melanomul malign de origine necunoscută reprezintă 5-10% din toate cazurile de melanom [2]. Cu toate acestea, chiar dacă melanomul este localizat
retroperitoneal, o leziune cutanată primară este aproape întotdeauna documentată. Pacienta noastră nu avea nicio leziune a pielii şi nici nu avea antecedente de melanom. Melanomul malign care apare retroperitoneal este extrem de rar şi este încă o enigmă dacă acest caz reprezintă un melanom malign primar sau metastaze retroperitoneale de origine necunoscută.
Până în prezent, melanomul metastatic care implică ureterul a fost raportat foarte rar [3]. Localizările comune ale metastazelor sunt ficatul şi creierul. Strategiile terapeutice sistemice în melanomul metastatic sunt imunoterapia bazată pe interferon şi interleukina-2, precum şi diverşi agenţi chimioterapici. Cu toate acestea, dacă este accesibilă, pacienţii obţin cel mai mare beneficiu clinic prin rezecţia radicală a leziunilor metastatice [1].
Frecvent, repararea chirurgicală a ureterului afectat de mult timp, în special a segmentului proximal, presupune utilizarea segmentului ileal sau autotransplantul. Cu toate acestea, în cazul în care este posibilă, interpunerea apendicelui este simplă din punct de vedere tehnic şi elimină necesitatea rezecţiei intestinale. În 1912 Melnikoff a fost primul care a raportat utilizarea apendicelui vermiform pentru înlocuirea unui segment ureteral după rezecţie [4]. De atunci şi alţi autori au raportat utilizarea apendicelui pentru înlocuirea diferitelor defecte implicând ureterul mediu sau distal la adulţi sau copii. Întro prezentare de caz publicată de Thomas şi colab. [5] în 2004, apendicele a fost folosit ca înlocuitor pentru o porţiune de 9 cm între ureterul proximal şi vezica urinară. Defectul a rezultat din fibroza retroperitoneală severă. Ca şi în cazul nostru, apendicele a fost izolat cu mezenterul său şi a fost creată o anastomoză termino-terminală între ureterul proximal şi un capăt al apendicelui. Capătul cecal al apendicelui a fost anastamozat la vezica urinară peste un stent ureteral. Întro altă prezentare de caz, Jang şi colab. [6] interpun apendicele în ureter întro orientare isoperistaltică dinspre pelvisul renal spre ureterul proximal la un pacient rănit întrun accident de motocicletă. Apendicele este irigat cu sânge din artera apendiculară, care este o ramură a arterei ileocolice. Calibrul relativ mic al apendicelui (2-3 mm), care este similar cu cel al ureterului (2-10 mm), permite o anastomoză etanşă. Mai mult, peristaltismul natural şi suprafaţa reduc riscul oricărui dezechilibru electrolitic datorat absorbţiei urinii. În ciuda numeroaselor sale avantaje, utilizarea apendicelui ca substitut ureteral poate fi limitată din cauza discrepanţei calibrului, producţiei excesive de mucus, sau în cazul în care apendicectomia a fost efectuată anterior [7].

Substitution Of The Ureter With The Appendix In Malignant Melanoma Adjacent To The Ureter 147
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012 cAsE PREsEnTATIOn
Concluzii
După cunoştinţa noastră acesta este un caz nou de înlocuire apendiculară a ureterului în contextul unui melanom malign. Utilizarea apendicelui ca o posibilă alternativă pentru substituţie ureterală, mai ales dacă ureterul mijlociu sau proximal este implicat, ar trebui să fie considerată ca o opţiune viabilă.
Referinţe
1. Miller AJ, Mihm MC Jr. Melanoma. N Engl J Med. 2006;355(1):51-65.
2. Jayashree PE, Javalgi PA, Hiremash R, Dombale VD, Kansagara MH. Retroperitoneal Malignant Melanoma
– A Curiosity. Journal of Clinical and Diagnostic Research. 2011;5(2):372-373
3. Gakis G, Merseburger AS, Sotlar K, Kuczyk MA, Sievert KD, Stenzl A. Metastasis of malignant melanoma in the ureter: possible algorithms for a therapeutic approach. Int J Urol. 2009;16(4):407-9.
4. Melnikoff AE. Sur le replacement de l’uretère par anse isolée de l’intestine grêle. Rev Clin Urol. 1912;1:601.
5. Thomas A, Eng MM, Hagan C, Power RE, Little DM. Appendiceal substitution of the ureter in retroperitoneal fibrosis. J Urol. 2004;171(6 Pt 1):2378.
6. Jang TL, Matschke HM, Rubenstein JN, Gonzalez CM. Pyeloureterostomy with interposition of the appendix. J Urol. 2002;168(5):2106-7.
7. Richter F, Stock JA, Hanna MK. The appendix as right ureteral substitute in children. J Urol. 2000;163(6):1908-12.
Traducere: Bumbuluţ Călin

US(Collapsed lung with surrounding pleural effusion (US)(ריאה בתמט ותפליט פלאורלי בסמוך
Collapsed lung with surrounding pleural effusion (US)

A Case Of West-Nile Meningitis Treated With Tamiflu 149
Rezumat
Virusul West Nile este un virus având ca vector artropodele, aparţinând familiei Flaviviridae şi care poate provoca infecţii endemice, de obicei în Orientul Mijlociu, Africa şi Asia. Aproximativ 1% din persoanele infectate dezvoltă infecţii ale sistemului nervos central. Descriem cazul unei paciente internate în timpul unui focar de gripă porcină, cu febră şi simptome meningeale, tratate cu succes cu TAMIFLU® (un medicament antiviral pentru infecţia gripală H1N1). Cu toate acestea, rezultatele puncţiei lombare au demonstrat o infecţie cu virusul West Nile. În lipsa unor date publicate despre efectul TAMIFLU® asupra virusului West Nile discutăm posibilitatea unui mecanism de acţiune al TAMIFLU® în această situaţie.
Cuvinte cheie: Virusul West Nile, TAMIFLU®, Olsetamivir, infecţie
Introducere
Infecţia cu virusul West Nile (VWN) este o infecţie endemică observată în Orientul Mijlociu, Africa şi Asia [1]. În Statele Unite a fost descoperită pentru prima dată în vara anului 1999 în New York. De atunci, virusul s-a extins din America de Nord la cea de Sud, Caraibe, spre nord în Canada, determinând cea mai mare epidemie de
un cAZ de MeninGitĂ West-nile tRAtAt cu tAMiFlu
Solun Boris, Marcoviciu Dana, Dicker Dror, Shaked Efrat
Departmentul de Medicină Internă D, Spitalul Hasharon, Centrul Medical Rabin, Petah Tikva, afiliat la Facultatea de Medicină Sackler, Universitatea Tel-Aviv, Israel
Adresa pentru corespondenţă:Dr. Dana Marcoviciu, Department of Internal Medicine D, Rabin Medical Center, Hasharon Hospital 7, Keren Kayemet St., Petah Tiqva, Israel Phone: 972-3-9372429, Fax: 972-3-9372427 E-mail: [email protected] Primit: 23.05.2012 Acceptat: 10.09.2012 Med Con October 2012, Vol 7, No 3, 149-152
cAsE PREsEnTATIOn
boli neuroinvazive cu VWN raportată vreodată [2]. VWN este un virus având ca vector artropodele (arbovirus), aparţinând familiei Flaviviridae şi menţinut întrun ciclu de transmitere păsări-ţânţari [3]. Aproximativ 80% din infecţiile VWN sunt asimptomatice. Persoanele simptomatice dezvoltă o boală sistemică acută febrilă, cu dureri de cap, mialgii, artralgii, erupţii cutanate, sau simptome gastro-intestinale. Aproximativ 1% din persoanele infectate dezvoltă infecţii ale sistemului nervos central, care de obicei se manifestă ca encefalită, meningită, sau paralizie acută flască [4]. Nouăzeci şi trei la sută din pacienţii afectaţi se îmbolnăvesc în timpul anotimpului uscat şi cald, în principal în perioada iulie-septembrie. Incidenţa bolii neuroinvazive severe creşte cu vârsta, fiind cea mai mare (1,35 cazuri la 100.000 de locuitori) în rândul persoanelor cu vârsta de 70 ani sau mai mult [5]. Rata de spitalizare şi raportul cazuri-fatalitate sunt legate atât de vârstă, cât şi de boala neuroinvazivă [6]. În prezent nu este disponibil niciun vaccin uman şi prin urmare protecţia îmotriva ţânţarilor rămâne cel mai bun mod de a preveni infectarea [7].
Prezentare de caz
O femeie în vârstă de 54 de ani a fost internată datorită febrei, cefaleei şi slăbiciunii extremităţilor

Solun et al150
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012cAsE PREsEnTATIOn
stângi. Antecedentele ei au fost semnificative pentru abuzul de alcool, hipertensiune arterială şi un eveniment de hemoragie intracerebrală cu un an înainte. După tratamentul de reabilitare a rămas întrun status bun de performanţe.
La internare a fost întro stare mentală bună şi conştientă. Temperatura ei a fost de 39,2oC, tensiunea arterială 184/126 mmHg, puls regulat 111 bpm, iar saturaţia de oxigen de 94%. Respiraţia şi zgomotele cardiace au fost normale, abdomenul moale, fără sensibilitate, organomegalie, sau mase. Examenul neurologic a relevat rigiditatea gâtului cu semnele Kernig şi Brudzinski pozitive şi hemipareză uşoară stângă. Restul examenului fizic a fost normal.
Examenele de laborator au aratat un număr de celule albe de 8.480/mm3 cu 80,7% neutrofile, 11,9% limfocite, 4,6% monocite, eozinofile 2,1%, bazofile 0,7%. Numărul de trombocite a fost de 214.000/mm3. Nivelul seric de globuline a fost 3,7g/dL, transaminaza glutamic oxalacetică serică (SGOT) 76 U/L (nivel de referinţă 7-31), transaminaza glutamic piruvică serică (SGPT) 74,3 U/L (4-34).
Radiografia toracică a fost normală. Tomografia computerizată a creierului a relevat un număr de focare hipoecogene mici în regiunile periferice ale ambilor ventriculi. Deoarece la momentul internării a existat un focar de cazuri cu gripă porcină, a fost luată în considerare posibilitatea ca pacienta să fi contractat boala, fiind iniţiat tratamentul cu TAMIFLU® capsule de 75 mg (fosfat de oseltamivir, Genentech USA, Inc). Cu toate acestea, culturile de sânge şi testul PCR pentru gripa pandemică A (H1N1) primite câteva zile mai târziu, au fost negative. O puncţie lombară a arătat: glucoză 71mg/dl (glicemie 157 mg/dl), numărul de celule 56 celule/mm3, cu predominanţă limfocitară, proteine 80 g/dl. Examenul bacteriologic al lichidului cefalorahidian a aratat: HSV-1 şi HSV-2 negative, IgM pentru febra Nilului de Vest ELISA (Enzyme-linked immunosorbent assay) pozitive, IgG ELISA negative. Nu s-au dezvoltat bacterii. Tratamentul cu TAMIFLU® a continuat timp de 5 zile, cu îmbunătăţirea semnificativă a performanţei şi stării psihice. Pacienta a fost externată în a 7-a zi de spitalizare.
Discuţie
Virusul West Nile este un acid ribonucleic (ARN) mono-catenar, din familia Flaviviridae. Ciclul său de replicare include proteaza NS3, glicoproteina, helicaza NS3, metiltransferaza NS5 şi ARN-polimeraza ARN NS5 dependentă, toate ţinte potenţiale pentru terapia antivirală [8]. Intrarea virusului în diferite tipuri de
celule (macrofage, celule dendritice şi monocite) debutează prin endocitoză în urma interacţiunii proteinei E cu receptorii celulari. Consecutiv, ARN-ul viral genomic se mută în reticulul endoplasmic pentru translaţia proteinelor virale şi replicarea ARN. Prin urmare, orice cauză de întrerupere a translaţiei proteice VWN şi/sau replicării ARN va bloca ciclului de viaţă viral şi va sista infecţia [9].
Deşi majoritatea persoanelor infectate sunt asimptomatice, virusul poate afecta sistemul nervos central, cu simptome variind de la dureri de cap la meningita aseptică sau meningoencefalită. Aceste simptome pot fi oculte şi uneori neputând fi diferenţiate de manifestări cauzate de alte virusuri. Incidenţa implicării sistemului nervos central în zonele endemice, incluzând meningoencefalita, a fost observată a fi una din 150 de cazuri de infecţii VWN [10]. S-a raportat că VWN a fost unul din cei mai frecvenţi agenţi patogeni în cazuri de meningită virală observate între 1997 şi 2008 întrun spital comunitar din Baltimore [11]. În afară de tratamentul simptomatic, nu există terapie specifică pentru infecţiile cu WNF [10].
Deşi nu este disponibil niciun vaccin uman, până în prezent a fost studiat un candidat posibil pentru vaccin un virus gripal recombinant care să exprime proteina E, domeniul III (DIII) din VWN, întrun model pe cobai [12]. DIII al VWN a fost clonat în regiunea N-terminală a neuraminidazei virusului gripal, distrugând activitatea funcţională a proteinelor gripale. S-a demonstrat că o imunizare subcutanată la cobai cu vaccinul FLU-NA-DIII a dus la protecţie 100% [13].
Posibilul efect pozitiv al tratamentului cu TAMIFLU® se bazează pe rapoartele că infecţia cu flavivirusuri a fost asociată cu o scădere spontană a activităţii cerebrale locomotorii, precum şi cu o scădere semnificativă a nivelului neurotransmiţătorilor, mai ales dopamina [14]. S-a constatat că TAMIFLU® a crescut în mod semnificativ nivelul extracelular de dopamină în cortexul prefrontal medial [15].
Alt mecanism al TAMIFLU® a fost prin scăderea pH-ului intracelular. PH-ul scăzut al veziculelor intracelulare induce modificarea ireversibilă în replicarea virusului gripei A H1N1 [16,17]. Infecţia celulelor gazdă de către flavivirusuri depinde de pH-ul acid cu intervalul optim între 6,3 şi 6,9 [18]. Am presupus că acesta ar putea fi mecanismul primar de inhibare a replicării VWN.
S-a raportat că în zonele inflamate numărul diferitelor enzime incluzând proteaze şi neuraminidaza a crescut [19]. Mady şi colab. [20] au examinat efectele neuraminidazei pe amplificarea dependentă de anticorpi (ADA) a infecţiei cu flavivirus, fenomen care apare când

A Case Of West-Nile Meningitis Treated With Tamiflu 151
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012 cAsE PREsEnTATIOn
anticorpii neutralizanţi formează complexe cu virusul. A fost demonstrat că in vivo, în timpul infecţiei VWN, neuraminidaza şi alte enzime modulează funcţia şi expresia receptorilor Fc gamma RII umani, depistaţi pe scară largă în monocite, macrofage, neutrofile, eozinofile, trombocite şi celule B, jucând astfel un rol important în patogeneza şi dezvoltarea infecţiei VWN [20].
TAMIFLU® serveşte ca inhibitor competitiv al activităţii neuraminidazei virale (sialidaze), pe glicoproteinele de pe suprafaţa celulelor gazdă normale. Inhibitorii de intrare acţionează ţintind componenetele virale sau/şi celulare, fie prin inhibarea interacţiunii proteo-proteice în proteinele de înveliş virale sau între proteinele virale şi receptorii celulei gazdă, fie prin inhibarea interacţiunii proteo-lipidice. Deoarece fixarea tulpinii virale necesită acid sialic, inhibitorii de neuraminidază acţionează prin ţintirea receptorilor celulari de acid sialic la care particulele virale sunt ataşate. Fără neuraminidază, infecţia ar fi limitată pentru reproducere şi rareori suficientă pentru a provoca boala [21,22].
Astăzi există o listă lungă de numeroase tipuri de neuraminidaze. Deoarece nu există date dacă neuraminidaza gripală are aceleaşi proprietăţi ca şi neuraminidaza sau alte enzime de pe suprafaţa VWN, nu excludem efectul posibil al TAMIFLU® pe neuraminidaza virală a VWN. Pe de altă parte, suntem conştienţi de faptul că orice concluzii bazate pe un singur caz nu pot fi definitive cu privire la efectul benefic al TAMIFLU® în meningoencefalita VWN. Ar trebui făcute investigaţii suplimentare în acest domeniu cu scopul de a evalua posibila eficienţă şi beneficiile TAMIFLU® în tratamentul infecţiei VWN.
Concluzie
Virusul West Nile este un flavivirus transmis prin ţânţari, cu o distribuţie largă în Africa, Orientul Mijlociu, Asia, Europa de Sud, fiind introdus recent în America de Nord şi Canada. Cele mai multe infecţii umane VWN sunt subclinice, dar pacienţii cu manifestări clinice pot varia în severitate de la forma simplă la meningoencefalita fatală. Incidenţa bolii neuroinvazive severe şi decesul au crescut cu vârsta. În prezent, nu există niciun tratament antiviral sau vaccin adecvat pentru a vindeca VWN, putând fi administrată doar îngrijire suportivă. Având în vedere rezultatele experimentale pozitive de imunizare subcutanată la cobai cu vaccinul FLU-NA-DIII, nu poate fi exclus efectul benefic al TAMIFLU® în infecţia VWN în anumite cazuri. Ar trebui făcute în continuare studii pentru a evalua această sugestie.
Referinţe
1. Blitvich BJ. Transmission dynamics and changing epidemiology of West Nile virus. Anim Health Res Rev 2008;9(1):71-86.
2. Murray KO, Mertens E, Despres P. West Nile virus and its emergence in th United States of America. Vet Res 2010;41(6):67.
3. Hayes EB, Sejvar JJ, Zaki SR, Lanciotti RS, Bode AV, Campbell GL. Virology, pathology and clinical manifestations of West Nile virus disease. Emerg Infect Dis 2005;11(8):1174-9.
4. Petersen LR, Roehrig JT, Hughes JM. West Nile virus encephalitis. N Engl J Med 2002;347(16):1225-6.
5. Lindsey NP, Staples JE, Lehman JA, Fischer M; Centers for Disease Control and Prevention (CDC). Surveillance for human West Nile virus disease - United States, 1999-2008. MMWR Surveill Summ. 2010;59(2):1-17. Erratum in: MMWR Surveill Summ 2010;59(23):720.
6. Borchardt SM, Feist MA, Miller T, Lo TS. Epidemiology of West Nile virus in the highly epidemic state of North Dakota, 2002-2007. Public Health Rep 2010;125:246-9.
7. Rossi SL, Ross TM, Evans JD. West Nile virus. Clin Lab Med 2010;30:47-65.
8. Chappell KJ, Stoermer MJ, Fairlie DP, Young PR. West Nile Virus NS2B/NS3 protease as an antiviral target. Curr Med Chem 2008;15:2771-84.
9. Sampath A, Padmanabhan R. Molecular targets for flavivirus drug discovery. Antiviral Res 2009;81:6-15.
10. Gyure KA. West Nile virus infections. J Neuropathol Exp Neurol 2009;68:1053-60.
11. Wiberg K, Birnbaum A, Gradon J. Causes and presentation of meningitis in a Baltimore community hospital 1997-2006. South Med J 2008;101:1012-6.
12. Yamshchikov G, Borisevich V, Seregin A, Chaporgina E, Mishina M, Mishin V, Kwok CW, Yamshchikov V. An attenuated West Nile prototype virus is highly immunogenic and protects against the deadly NY99 strain: a candidate for live WN vaccine development. Virology 2004;330:304–312.
13. De Filette M, Ulbert S, Diamond M, Sanders NN. Recent progress in West Nile virus diagnosis and vaccination. Vet Res. 2012;43:16.
14. Misra UK, Kumar S, Kalita J, et al. A study of motor activity and catecholamine levels in different brain regions following Japanese encephalitis virus infection in rats. Brain Res 2009;1292:136-47.
15. Yoshino T, Nisijima K, Shioda K, Yui K, Kato S. Oseltamivir (Tamiflu) increases dopamine levels in the rat medial prefrontal cortex. Neurosci Lett 2008;438:67-9.

Solun et al152
MEDICAL CONNECTIONS • NUMBER 3 (27) • OCTOBER 2012cAsE PREsEnTATIOn
16. Giocondi MC, Ronzon F, Nicolai MC, et al. Organization of Influenza A virus envelope at neutral and low pH. J Gen Virol 2010;91(Pt 2):329-38.
17. Di Trani L, Savarino A, Campitelli L, et al. Different pH requirements are associated with divergent inhibitory effects of chloroquine on human and avian influenza A viruses. Virol J 2007;4:39.
18. Moesker B, Rodenhuis-Zybert IA, Meijerhof T, Wilschut J, Smit JM. Characterization of the Functional Requirements of West Nile Virus Membrane Fusion. J Gen Virol. 2010;91(Pt 2):389-93.
19. LaMarco KL, Diven WF, Glew RH. Experimental alteration of chinchilla middle ear mucosae by bacterial
neuraminidase. Ann Otol Rhinol Laryngol 1986;95(3 Pt 1):304-8.
20. Mady BJ, Kurane I, Erbe DV, Fanger MW, Ennis FA. Neuraminidase augments Fc gamma receptor II-mediated antibody-dependent enhancement of dengue virus infection. J Gen Virol 1993;74(Pt 5):839-44.
21. Khan M, Rangari NT, Kalyankar TM, Agarwal PC. Clinical Assessment and Management of Swine Influenza: A Review. International Journal of Research in Pharmaceutical and Biomedical Sciences 2011;2:52-58.
22. Teissier E, Penin F, Pécheur EI. Targeting cell entry of enveloped viruses as an antiviral strategy. Molecules 2010;16(1):221-50.
Traducere: Bumbuluţ Călin

Imagine All The Pictures Living Other Lives 153
Dr. Selma Gabrieli este un specialist în diagnosticul imagistic, în cadrul Departamentului de Imagistică al Spitalului Hasharon, Centrul Medical Rabin, Petah Tikva. Dr. Oshra Benzaquen este rezident în cadrul aceluiaşi departament. Între interpretările scanărilor CT, a imaginilor radiografice şi efectuarea examinărilor ecografice, ei încearcă să îndepărteze rutina prin adăugarea unei dimensiuni imaginative aspectelor medicale. Caractere pline de viaţă emerg chiar din cele mai banale sau sumbre imagini. Colecţia a fost alcătuită în decursul câtorva ani.
Fotografiile de la paginile: 58, 68, 72, 78, 84, 90, 100, 120, 126, 136, 148 sunt din această lucrare.
MEDIcInE AnD ART
iMAGineAZĂ-Ţi toAte iMAGinile pRinZÂnd AltĂ ViAŢĂ
Gabrieli Selma, Benzaquen Oshra
Departmentul de Imagistică, Spitalul Hasharon, Centrul Medical Rabin, Petah Tikva, afiliat la Facultatea de Medicină Sackler, Universitatea din Tel Aviv, Israel

ScopRevista Conexiuni Medicale publică lucrări de
cercetare care contribuie la progresul din toate domeniile medicinei. Revista publică de asemenea reviste generale, editoriale şi scurte comunicări pe domenii specifice. Prezentările de caz sunt acceptate dacă prezintă interes crescut şi sunt bine investigate. Scrisorile către editor, în special cele care prezintă o opinie privind un articol publicat anterior sau care prezintă noi date, sunt de asemenea binevenite. Adresa web a revistei este http://www.conexiunimedicale.ro. Revista este publicată trimestrial, articolele sunt acceptate în limba engleză sau română, având cel puţin traducerea în limba engleză a rezumatului şi cuvintelor cheie. Lucrările pot fi trimise pe adresa: dr. Bumbuluţ Călin, editor şef adjunct, Conexiuni Medicale, P-ţa. Eroilor Revoluţiei nr. 23, cod 440055, Satu Mare, Romania. Tel./Fax: +40-261-710456, e-mail: [email protected].
Republicarea articolelorVă rugăm să confirmaţi că lucrarea dumneavoastră
nu a mai fost publicată în forma prezentată sau într-o formă asemănătoare, sau că nu a fost acceptată pentru publicare într-o altă revistă.
Conflicte de intereseRugăm autorii să declare posibilele conflicte de
interese, inclusiv cele de natură financiară. Dacă nu există conflicte de interese, vă rugăm să precizaţi acest lucru. Sursele de finanţare trebuie precizate în lucrarea dumneavoastră.
Permiterea de a reproduce materialepublicate anteriorVă rugăm să ne trimiteţi o copie a acceptului de
reproducere (de exemplu al ilustraţiilor) de la deţinătorul dreptului de copyright.
Formularele de accept ale pacienţilorProtecţia drepturilor pacienţilor este esenţială; vă
rugăm să ne trimiteţi formularele de accept ale pacienţilor sau subiecţilor studiului dumneavoastră,
stAndARde de RedActARe
prin care aceştia permit publicarea fotografiilor sau altor materiale care ar putea să îi identifice. Dacă formularele de accept nu prevăd acest lucru vă rugăm să rugăm obţineţi acordul, sau îndepărtaţi posibilitatea de identificare. O declaraţie în acest sens trebuie inclusă în secţiunea „Metode” a lucrării.
Aprobarea Comitetului de EticăPrecizaţi la secţiunea „Metode” faptul că desfăşuraţi
studii asupra subiecţilor umani cu aprobarea Spitalului, Comitetului de Etică al Universităţii, etc. În mod similar, confirmaţi dacă experimentele asupra animalelor corespund standardelor etice.
Asumarea dreptului de copyrightLucrările acceptate pentru publicare au implicit
drepturile de copyright cedate către editor. Autorii pot utiliza materiale din lucrările lor în alte articole proprii.
Propunerea pentru publicareToate manuscrisele propuse pentru publicare în
Conexiuni Medicale vor fi în format compatibil pentru efectuarea recenziei online. Revista acceptă manuscrise propuse în formă electronică, în format Word (text, figuri şi tabele). Nu trimiteţi lucrări în format PDF. Acceptăm lucrări care nu depăşesc 3.500 de cuvinte pentru articole originale, 2.500 pentru prezentări de caz, 2.000 pentru prezentări de imagini clinice, 500 pentru scrisori către editor şi 4.500 de cuvinte pentru reviste generale. Autorii NU vor trimite prin poştă sub formă de hârtie propunerea pentru publicare, decât dacă este vorba de scrisori sau dacă se solicită astfel din partea redacţiei. Dacă nu există altă opţiune decât trimiterea prin poştă, vă rugăm să expediaţi şi versiunea electronică pe disketă sau CD-ROM pe adresa redacţiei: Conexiuni Medicale, P-ţa. Eroilor Revoluţiei nr. 23, cod 440055, Satu Mare, România. Utilizaţi text la două rânduri şi includeţi următoarele secţiuni: pagina de titlu, rezumatul şi cuvintele cheie, textul, mulţumiri, referinţe, tabele şi figuri. Paginile vor fi numerotate consecutiv, începând cu pagina de titlu, numerele arabe fiind plasate în colţul din dreapta sus al fiecărei pagini.

Prezentarea lucrăriiPagina de titluCuprinde titlul întreg şi titlul scurt format din
maxim 45 de caractere, numele şi prenumele fiecărui autor; dacă lucrarea aparţine unui departament sau unei instituţii, va fi menţionat numele acestuia în întregime. De asemenea numele, e-mail-ul şi adresa autorului împuternicit pentru corespondenţă, sursele de finanţare sau suport utilizate sub forma burselor, echipamentelor, medicamentelor, sau orice combinaţie a acestora.
RezumatulPagina a doua va cuprinde rezumatul cu minim 200
de cuvinte; nu utilizaţi abrevieri, note de subsol, sau referinţe.
Introducere în temă şi scopuriDescrieţi importanţa studiului şi obiectivul
(obiectivele) precise ale cercetării sau întrebarea (întrebările) pe care le ridică studiul.
MetodeIncludeţi informaţii privind următoarele aspecte ale
studiului dacă sunt utilizate: proiectul – descrieţi elementele de bază ale studiului, de exemplu studiu controlat randomizat, studiu cross-secţional, de cohortă, de urmărire, serii de cazuri, etc; procedura – specificaţi dacă a fost desfăşurat în sistem de îngrijire primar sau terţiar, în ambulator sau spital, în comunitate, etc; participanţi – indicaţi numărul subiecţilor şi cum au fost selectaţi, recrutaţi şi desemnaţi pentru intervenţie; intervenţia – metoda de administrare şi durata intervenţiei.
RezultatePrezentaţi principalele rezultate ale studiului,
inclusiv intervalurile de confidenţă sau valorile p.ConcluziiEnunţaţi doar concluziile susţinute direct de dovezi,
precum şi importanţa descoperirilor. Revistele generale şi prezentările de caz vor include un rezumat nestructurat.
Cuvinte cheieRezumatul va fi urmat de o listă de 3–10 cuvinte
cheie sau fraze scurte care vor ajuta la indexare. Dacă este posibil, utilizaţi termeni proveniţi din lista Index Medicus cu 262 subiecte medicale/Medical Subject Headings 262 (http://www.nlm.nih.gov/mesh/meshhome.html).
TextulUn studiu original va fi divizat în secţiuni denumite
Introducere, Metode, Rezultate şi Discuţii (incluzând concluziile), după formula „IMRAD”. Articolele lungi pot necesita subsecţiuni (în special la Rezultate şi Discuţii) pentru clarificare. Alte tipuri de articole precum prezentări de caz, reviste generale, editoriale, pot urma alt format. Nu recomandăm utilizarea excesivă
a abrevierilor. Folosiţi metode de calcul statistic standardizate. Nominalizaţi medicamentele şi substanţele chimice utilizând numele generic (dacă sunt menţionate mărcile înregistrate, se furnizează numele producătorului şi oraşul).
MulţumiriVor fi adresate celor care au adus contribuţii
importante la studiu.ReferinţeVor fi numerotate între paranteze drepte cu
numerale arabe, succesiv în ordinea în care sunt menţionate în text. Referinţele vor include numele autorilor până la al şaselea autor, dacă sunt mai mulţi, enumeraţi primii trei şi apoi adăugaţi „et al”. Referinţele vor include titlul complet şi sursa informaţiei; numele revistelor va fi abreviat conform Index Medicus (http://www.nlm.nih.gov/tsd/serials/terms_cond.html); nu se acceptă mai mult de 90-100 referinţe; pentru scrisori către redacţie se acceptă 5-6 referinţe. Folosiţi ca şi referinţe cât mai puţine rezumate. Comunicările personale şi lucrările nepublicate nu vor fi menţionate la referinţe şi vor apare în text între paranteze. Lucrările nepublicate dar aflate în curs de publicare vor fi incluse în referinţe cu menţiunea „in press” între paranteze, lângă numele revistei implicate.
TabeleFiecare tabel va fi numerotat cu numerale romane,
cu un titlu scurt deasupra, la subsolul lor vor fi trecute notele explicative, menţionându-se abrevierele nestandardizate utilizate; nominalizaţi valorile statistice care variază precum deviaţia standard şi eroarea standard a medianei. Fiecare tabel va fi citat în text.
FiguriToate graficele, fotografiile, diagramele vor fi
considerate ca figuri şi vor fi numerotate succesiv în text cu numerale arabe. Dacă o figură a fost publicată anterior, sursa va fi citată cu mulţumiri, menţionându-se permisiunea deţinătorului de copyright. Figurile pot fi reduse, grupate sau şterse la dorinţa editorului. Legenda figurii va fi plasată la subsolul ei; va fi explicată scala utilizată, respectiv metodele de colorare microscopică.
Unităţi de măsurăMăsurătorile lungimii, înălţimii, greutăţii şi
volumului vor fi făcute în sistem metric sau multipli decimali. Temperaturile vor fi exprimate în grade Celsius. Tensiunea va fi măsurată în mmHg. Toate măsurătorile hematologice vor fi exprimate în Sistemul Internaţional de Unităţi (SI).
Abrevieri şi simboluriUtilizaţi doar abrevieri standard. Evitaţi abrevierile
în titlu şi rezumat. Cuvântul va preceda abrevierea la

prima utilizare în text, cu excepţia unităţilor de măsură standard.
RetipăririSunt oferite gratuit zece copii ale articolului publicat
şi două ale revistei. Dacă sunt necesare mai multe copii, sunt disponibile contra cost.
Politica editorialăApreciem toate contribuţiile în domeniul medicinei.
Invităm personalităţi recunoscute cu expertiză şi articole din diverse domenii să publice reviste generale şi editoriale în revista noastră. Acceptăm de asemenea lucrări originale şi prezentări de caz din toate ţările. Conexiuni Medicale vă oferă o recenzie atentă şi publicarea imediată după acceptare. Redactorii vor citi primii lucrarea, decizând în decurs de 1-3 săptămâni în funcţie de nivelul de prioritate: unele sunt trimise imediat recenzorilor, unele pot fi respinse, iar unele sunt returnate autorilor cu sugestii de îmbunătăţire înainte de expedierea spre recenzori.
Procedura peer-reviewConexiuni Medicale practică o evaluare a tuturor
lucrărilor originale de către doi sau trei recenzori independenţi, din care doi sunt personalităţi internaţionale. Procesul peer-review este esenţial pentru asigurarea calităţii informaţiei ştiinţifice. Recenzorii sunt rugaţi să evalueze manuscrisul aplicând aceleaşi standarde ca şi pentru reviste internaţionale; comentariile sunt trimise editorului, care va informa autorii asupra acestor sugestii, rugându-i să răspundă la întrebări şi să facă necesarele corecţii. Aceste informări sunt făcute în cel mult trei luni de la propunerea de publicare. Manuscrisul revizuit de autori va fi reexpediat editorului în cel mult o lună. La primirea de către editor a versiunii corectate, însoţită de o scrisoare de răspuns punctuală la comentariile recenzorilor, se retrimite manuscrisul aceloraşi recenzori, care vor face recomandarea finală pentru acceptarea sau respingerea acestuia.
AbonamentePreţul unui abonament anual pentru 2012 este: 80
RON individual, 160 RON pentru instituţii, plătiţi în contul Colegiului Medicilor Satu Mare RO38 BTRL 0310 1202 K392 62XX, cod fiscal 9839430, cu menţiunea „pentru abonament Conexiuni Medicale”. Solicitarea abonării poate fi trimisă prin poştă: P-ţa. Eroilor Revoluţiei nr. 23, cod 440055, Satu Mare, Romania. Tel./Fax: 0261-710456, 0361-408164, sau prin e-mail: [email protected].
PublicitateCererile pentru spaţiu publicitar vor fi adresate
redacţiei Conexiuni Medicale. Preţurile (plătite în lei la cursul BNR) pentru publicitate pe 2012 sunt 200 euro pagina (A4) color, un număr şi 800 euro patru numere; coperta interioară faţă sau spate: 350 euro un număr, 1400 euro patru numere; coperta exterioară spate: 400 euro un număr, 1600 euro patru numere. Cont bancar: Colegiul Medicilor Satu Mare, CUI 9839430, Banca Transilvania, agenţia Golescu Satu Mare, IBAN: RO38 BTRL 0310 1202 K392 62XX.
© Copyright Conexiuni Medicale/Medical Connections, Satu Mare, 2012
Nicio parte a acestei publicaţii nu poate fi reprodusă, stocată sau transmisă sub orice formă sau prin orice mijloace, fără permisiunea prealabilă în scris a revistei Conexiuni Medicale. Permisiunea nu este necesară pentru a copia rezumate sau articole dacă este indicată sursa, cu citarea completă a referinţei. Solicitarea privind permisiunea de a retipări toată revista sau o parte a ei, va fi adresată editorului prin e-mail: [email protected]
Revista Conexiuni Medicale apare trimestrial prin efortul logistic şi financiar al Colegiului Medicilor Satu Mare şi Asociaţiei Medicilor de Familie Satu Mare, în cadrul proiectului comun al Centrului de Documentare şi Educaţie Medicală Continuă Satu Mare.