Embed Size (px)
Citation preview

Lampi and Reinhart-King, Sci. Transl. Med. 10, eaao0475 (2018) 3 January 2018
S C I E N C E T R A N S L A T I O N A L M E D I C I N E | R E V I E W
1 of 14
M E C H A N O M E D I C I N E
Targeting extracellular matrix stiffness to attenuate disease: From molecular mechanisms to clinical trialsMarsha C. Lampi1 and Cynthia A. Reinhart-King2*
Tissues stiffen during aging and during the pathological progression of cancer, fibrosis, and cardiovascular dis-ease. Extracellular matrix stiffness is emerging as a prominent mechanical cue that precedes disease and drives its progression by altering cellular behaviors. Targeting extracellular matrix mechanics, by preventing or reversing tissue stiffening or interrupting the cellular response, is a therapeutic approach with clinical potential. Major drivers of changes to the mechanical properties of the extracellular matrix include phenotypically converted myofibro-blasts, transforming growth factor (TGF), and matrix cross-linking. Potential pharmacological interventions to overcome extracellular matrix stiffening are emerging clinically. Aside from targeting stiffening directly, alterna-tive approaches to mitigate the effects of increased matrix stiffness aim to identify and inhibit the downstream cellular response to matrix stiffness. Therapeutic interventions that target tissue stiffening are discussed in the context of their limitations, preclinical drug development efforts, and clinical trials.
INTRODUCTIONIncreased tissue stiffness is associated with a diverse array of pathol-ogies, including the two leading causes of death in the United States: cancer and cardiovascular disease (1, 2). Decreased extracellular matrix (ECM) compliance also occurs with fibrosis, advanced age, and di-abetes due to enhanced matrix deposition, cross-linking of existing matrix, and fiber alignment. (3–5). The expansion of the mechano-biology field over the past decade has integrated the engineering and biological landscapes to advance our understanding of the con-tributions of increased ECM stiffness on disease. Although it is well established that changes in tissue mechanics are hallmarks of specif-ic pathological states, more recently, it has become apparent that tissue stiffening can precede disease development and that mechanical cues can drive its progression (6, 7). Hence, mechanomedicine is an emerg-ing field focused on therapeutically targeting tissue mechanics, either by directly altering the mechanical cues presented to cells or by dis-rupting the cellular response to mechanics.
The ECM is a cell-secreted network that surrounds cells and is pri-marily composed of proteoglycans and fibrous proteins, the most abundant being collagen. In addition to providing structural sup-port, the ECM imparts biochemical and mechanical cues that regu-late cell behaviors (8). Tensional, compressive, and shear forces are translated into biochemical signaling cascades through a process known as mechanotransduction, and evidence suggests that cells play an active role in remodeling their matrix to maintain an ECM stress set point through a process known as tensional homeostasis (9). The ECM exhibits viscous and elastic properties, both of which govern cell fate (9). Aberrant increased ECM stiffness, which can be described in terms of the Young’s elastic modulus, is associated with pathological states and is emerging as a critical factor that influences cell behavior (9–11). The elastic modulus represents the ability of a material to resist deformation, and is calculated as the stress applied to the material divided by the resulting strain (9, 10). ECM stiffness sensing is achieved through protein deformation caused by cell-generated force loading on transmembrane integrins adhered to the matrix
(9). Because individual cell types exhibit unique mechanosensitivities that can promote pathological progression, mechano-based thera-pies represent an emerging clinical strategy (12).
Here, we discuss mechanisms that cause ECM stiffening during natural aging and pathological progression. Therapeutic approaches to prevent or reverse matrix stiffening, including their clinical rele-vance, are described. Because elevated ECM stiffness is deleterious in multiple pathologies and difficult to attenuate, we examine several potential cellular targets to disrupt the cellular response to increased matrix mechanics. We describe drug development efforts and chal-lenges of individual cellular targets, as well as the translational potential of available drugs, preclinical studies, and clinical trials. Aberrant ECM mechanical properties play a critical role in numerous pathol-ogies, and thus, mechanomedicine is a therapeutic approach to treat disease with important clinical implications.
TARGETING TISSUE STIFFENING TO LIMIT PATHOLOGICAL PROGRESSIONMyofibroblastsA major cause of increased ECM stiffness during cancer and fibrotic diseases is dysregulated matrix synthesis and remodeling by activated fibroblasts that have dedifferentiated into myofibroblasts (Fig. 1). Remodeling of the tumor stroma and organ fibrosis exhibit striking similarities to the wound healing response, except in the pathological state the response is sustained: Activated fibroblasts do not undergo apoptosis or become quiescent (13). To date, no distinct phenotypic or molecular markers have been identified to distinguish functional differences between cancer-associated fibroblasts (CAFs) and fibrosis- associated fibroblasts (FAFs); therefore, here, CAFs and FAFs are collectively referred to as myofibroblasts (13). Myofibroblasts are a heterogeneous cell population with pathology-specific precursor cells originating from multiple cell sources, including tissue-resident cells, bone marrow, and immune cells (14). The de novo expression of -smooth muscle actin (-SMA) organized into contractile stress fibers is tradition-ally used as the defining myofibroblast molecular marker. However, -SMA–negative proto-myofibroblasts can also exhibit a contrac-tile myofibroblast-like phenotype (15). Other features of activated myofibroblasts include a stellate cell shape compared to the spindle morphology of quiescent cells, increased proliferation and migration,
1Meinig School of Biomedical Engineering, Cornell University, Ithaca, NY 14850, USA. 2Department of Biomedical Engineering, Vanderbilt University, Nashville, TN 37212, USA.*Corresponding author. Email: [email protected]
Copyright © 2018 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works
by guest on August 8, 2019
http://stm.sciencem
ag.org/D
ownloaded from

Lampi and Reinhart-King, Sci. Transl. Med. 10, eaao0475 (2018) 3 January 2018
S C I E N C E T R A N S L A T I O N A L M E D I C I N E | R E V I E W
2 of 14
and the expression of fibroblast activation protein (13). Myofibro-blasts are distinct from fibroblasts that lack a contractile cytoskele-ton and, despite shared expression of -SMA, do not express the same machinery used by smooth muscle cells for reversible Ca2+-mediated contractions (16). Because of the expression of -SMA, myofibro-blasts exert high contractile forces that, combined with excess ECM deposition, stiffen the local microenvironment. Castella et al. (16)
proposed a lock-step model of matrix remod-eling to explain how the unique contractile behavior of myofibroblasts irreversibly re-models the matrix through forces transmit-ted across extremely large, “super-mature” focal adhesions. Sustained Rho/Rho-associated kinase (ROCK) intercellular stress releases tension on ECM fibers; these ECM fibers are then pulled with weaker Ca2+-dependent os-cillatory contractions and stabilized in a re-tracted position by enzymatic cross-linking that stiffens the matrix through an irrevers-ible event. The stiffened ECM further stim-ulates myofibroblast activity through positive feedback loops, including the mechanically driven release of matrix-bound latent trans-forming growth factor (TGF) (17).
Targeting myofibroblasts or their differen-tiation may hold clinical potential to mitigate fibrosis. Historically, a lack of myofibroblast- exclusive molecular biomarkers has limited cell-level targeting approaches. The hetero-geneity of the myofibroblast precursor cell population suggests cell type–specific sen-sitivities to chemical and mechanical stimuli. Unique targeting approaches may be required for cancer and fibrosis applications, which further complicates these efforts. Using com-putational methods, Jia et al. (18) recently iden-tified elevated COL11A1 gene expression as a distinguishing signature of CAFs found across 13 types of epithelial cancer. Although this find-ing is a considerable advance in the identifi-cation of targetable myofibroblast biomarkers, up-regulation was not conserved in noncan-cerous fibrotic tissues or even among all types of cancer, thus revealing that myofibroblast- specific therapies may require high degrees of tailoring (18). Because of the diversity of organs affected by myofibroblast activity, an-other challenge will be localizing drugs to the intended site at therapeutic concentrations, es-pecially when systemic administration routes are used. For example, the unique physiology of the lungs, kidneys, liver, and solid tumors will necessitate specific drug delivery strate-gies (19).
Preclinical studies have demonstrated proof- of-concept success targeting differentiated myofibroblasts to mitigate their fibrotic ac-tivity. The monoclonal antibody C1-3 specifically bound to a transmembrane protein expressed
by hepatic myofibroblasts and selectively induced apoptosis in vivo when conjugated to the fungal toxin gliotoxin (20). Inhibition of myofi-broblast contraction was achieved with the delivery of an -SMA N-terminal peptide (21). The extra domain A–fibronectin (EDA-FN) splice variant, the growth factor TGF, and an intact ECM to gener-ate cellular tension are essential to induce myofibroblast differenti-ation and therefore represent therapeutic targets to mitigate early
Nucleus
Actin Focaladhesion
Integrin LINCcomplex
Latencycomplex
TGFβ AGEcross-link
TG2cross-link
LOXcross-link
Lamins NewECM
ECM
Nucleus Nucleus
F
F
FF
A
B
B
C
C
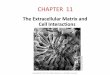
Fig. 1. Putative mechanisms of ECM stiffening and cellular contractile forces generated in response to increased microenvironment stiffness. (A) Matrix cross-linking by lysyl oxidase (LOX), tissue transglutaminase (TG2), and advanced glycation end products (AGEs) in concert with increased matrix deposition are major con-tributors of pathological matrix stiffening. Inside-out and outside-in extracellular matrix (ECM) rigidity sensing is transmitted across cell adhesions composed of integrins and focal adhesion complexes. (B) Actomyosin cell contractility forces are increased in response to elevated matrix stiffness, and traction forces are exerted against the ECM. Cellular force is also propagated across the cell cytoplasm to the nucleus. (C) Stiffness-mediated trac-tion forces transmitted across integrins cause a conformational change in the transforming growth factor (TGF) latency complex to release TGF ligand and activate positive feedback cycles of ECM synthesis and stiff-ening. Solid blue arrows represent directionality of force transmission.
CR
ED
IT: A
. KIT
TER
MA
N/S
CIE
NC
E T
RA
NSL
ATI
ON
AL
ME
DIC
INE
by guest on August 8, 2019
http://stm.sciencem
ag.org/D
ownloaded from

Lampi and Reinhart-King, Sci. Transl. Med. 10, eaao0475 (2018) 3 January 2018
S C I E N C E T R A N S L A T I O N A L M E D I C I N E | R E V I E W
3 of 14
fibrotic states (22). Mechanistic studies have also identified signaling by reactive oxygen species, microRNAs (miRs), chemokines, and cyto-kines as additional mediators of the myofibroblast phenotypic conver-sion that could be targeted therapeutically (23–26). A miR-29 mimic, MRG-201, recently completed a phase 1 clinical trial as an antifibrotic therapy (NCT02603224) (Table 1) (26).
Despite their widely recognized contribution as mediators of fibrotic pathologies and their associated role in cancer progression, paradoxical results from mouse models of cancer indicate an additional layer of complexity associated with myofibroblast targeting (13, 14, 27). In these models, depleting myofibroblasts from the stroma resulted in in-creased tumor aggressiveness and decreased survival (27). Myofibroblast- depleted tumors had decreased collagen content, were less stiff, and had altered immune cell infiltration, indicating that, collectively, the myofibroblast-depleted tumor milieu was drastically different than the untreated tumor stroma (27). Reconciling these data with the
robust body of work indicating pathological roles for myofibroblasts and a stiffened ECM is necessary to appropriately direct therapeutic targeting and identify the factors most critical to tumor aggressive-ness (6, 13).
Growth factorsAberrant overexpression of TGF is common among myofibroblast- driven pathologies. TGF promotes myofibroblast differentiation, cell proliferation, and matrix production. Extracellular TGF ligands bind to its serine/threonine kinase receptor (TGFR1) and activate the ca-nonical SMAD pathways that induce collagen and fibronectin gene expression (28). Simultaneously, TGF signaling inhibits matrix metallo-proteinase (MMP) matrix degradation by inducing the expression of tissue inhibitors of MMPs to drive microenvironment stiffening (29). Notably, cells exert increased contractile pulling forces against their matrix in response to elevated matrix stiffness, which activates
Table 1. Therapeutics in latest clinical trials with primary end points specific to ECM stiffness.
Target Drug name (trade name/company) Category Highest
completed trialCurrent trials relevant
to ECM stiffness References
miR-29 MRG-201(miRagen Therapeutics Inc.) MicroRNA Phase 1 None (26)
NCT02603224
CTGF FG-3019 (Fibrogen) Monoclonal antibody Phase 2 Phase 2(33, 34)
NCT01890265NCT01262001
TGF signalingPirfenidone
(Esbriet/Genentech)Small molecule,
mechanism unknownApproved:
Idiopathic lung fibrosis Phase 1–3
(36)NCT01872689NCT02552849NCT02408744NCT03068234NCT01872689
TGFGC1008
(Fresolimumab/Genzyme) Monoclonal antibody Phase 2 Phase 1–2
(37)NCT01401062NCT02581787NCT01665391
VEGF, FGF, and PDGF receptors
Nintedanib (Ofev/Boehringer Ingelheim)
Small molecule, tyrosine kinase inhibitor
Approved: Idiopathic lung fibrosis Phase 1–3 NCT01284322
LOXL2 GS-6624 (Simtuzumab/Gilead) Monoclonal antibody
Phase 2No efficacy in fibrosis
or cancerNone
(56–58)NCT01472198NCT01759511NCT 01769196
LOX Tetrathiomolybdate Copper chelator Phase 3(Wilson’s disease) Phase 2
(60)NCT00805805NCT00195091NCT01837329
v6 BG00011/STX-100 (Biogen) Monoclonal antibody Phase 2 None (89)NCT01371305
FAK VS-6063/PF-04554878 (Defactinib/Verastem) Small molecule Phase 2 Phase 1–2
(117)NCT02943317NCT02758587NCT02546531NCT02465060
FAK GSK-2256098 (GlaxoSmithKline) Small molecule Phase 1 Phase 1–2
(117)NCT02551653NCT02428270NCT02523014
NF-BBortezomib
(Velcade/Takeda) Small molecule Approved: Multiple myeloma Phase 2 (138, 139)
NCT02370693
by guest on August 8, 2019
http://stm.sciencem
ag.org/D
ownloaded from

Lampi and Reinhart-King, Sci. Transl. Med. 10, eaao0475 (2018) 3 January 2018
S C I E N C E T R A N S L A T I O N A L M E D I C I N E | R E V I E W
4 of 14
a feed-forward cycle of matrix production by releasing sequestered TGF from the matrix through mechanical force (17, 30).
A mediator of TGF expression and signaling is connective tissue growth factor (CTGF), which is cyclically expressed through TGF pathways and subsequently acts to induce additional TGF produc-tion (31). CTGF directly binds to TGF to enhance receptor associa-tions and is essential to TGF-mediated fibrotic effects (32). Thus, CTGF drives ECM remodeling and fibrotic pathologies through indi-rect regulation of the myofibroblast phenotype, ECM synthesis, and MMP expression. In vivo murine studies demonstrated prevention and regression of lung fibrosis after treatment with FG-3019, a human monoclonal antibody against CTGF (31). Open-label phase 1 and 2 clinical trials have demonstrated favorable patient tolerability of FG-3019, but clinical efficacy assessed on the basis of healthy tissue compliance will await the results of an ongoing placebo-controlled trial for idiopathic lung fibrosis (NCT01890265) (33, 34).
Because of their dominant role in stimulating proliferation and ECM production, growth factor therapies, especially those targeted against TGF, are a promising avenue to inhibit pathological cycles of ECM synthesis. Targeting TGF is an active area of research for fibro-sis and cancer applications, and therapeutics in development range from in vitro preclinical studies to phase 3 clinical trials (35). Disrupt-ing the pathological role of TGF has been approached from multi-ple angles, including inhibiting receptor-ligand interactions, tyrosine kinase activity, and protein synthesis using peptides, antisense oli-gonucleotides, small-molecule inhibitors, and monoclonal antibodies (35). Once developed, TGF-targeting therapeutics could have widespread applications when repurposed across organ-specific diseases, given the central role of TGF in propagating fibrosis (Table 2). For example, the small-molecule pirfenidone is a breakthrough drug that inhibits TGF pathways and was approved by the U.S. Food and Drug Administration (FDA) in 2014 to treat idiopathic lung fibrosis (36). Pirfenidone is being explored in clinical trials for kidney fibrosis (NCT02408744) and sys-temic sclerosis (NCT03068234). GC1008 is a monoclonal antibody against TGF that is also being actively pursued in clinical trials for its anti-fibrotic effects in cancer (NCT01401062 and NCT02581787) and com-pleted phase 1 trials for kidney sclerosis (NCT00464321) and systemic sclerosis (NCT01284322) (37).
Other growth factors, such as platelet-derived growth factor (PDGF) and vascular endothelial growth factor (VEGF), also contribute to fibrotic development and are potential therapeutic targets (38, 39). Nintedanib, a small-molecule tyrosine kinase inhibitor of VEGF, fibroblast growth factor (FGF), and PDGF receptors, is approved for use in idiopathic lung fibrosis and may hold therapeutic potential for other pathologies, as evidenced by 119 registered clinical trials (clinicaltrials.gov) (40).
A challenge with therapeutically targeting growth factor–mediated ECM synthesis is that the ECM imparts tissue integrity, and regulating ECM turnover is one of many downstream growth factor signaling outcomes. Despite its identification as the key regulator of fibrosis, the pleiotropic effects of TGF impose challenges to its therapeutic target-ing. During cancer, TGF can have both pro- and antitumorigenic effects, and TGF is important for inflammatory regulation (35). Paradoxical roles for growth factors underscore the difficulty of targeting them therapeutically and highlight a necessary role for spatial and temporal control in drug administration.
Short, single-stranded DNA or RNA oligonucleotides called aptamers may represent the future for targeted therapeutics, including growth factor inhibition (41). Although conceptually similar to antibody ap-proaches, aptamers are synthetic oligonucleotides with three-dimensional structure that are produced without animal intermediates and can be designed to engage in distinct, location-specific protein interactions with tailored pharmacokinetics (41). With continued contributions from next-generation sequencing and bioinformatics, improved se-lection methods, and low costs, it is anticipated that aptamers can fill a critical therapeutic niche (41). Currently, pegaptanib (Pfizer), which targets VEGF-165 to inhibit angiogenesis related to macular degen-eration, is the only aptamer on the market; nevertheless, it demon-strates the successful translation of aptamer technology to the clinic for effective, isoform-specific, growth factor targeting (42).
Advanced glycation end productsIn concert with increased ECM deposition, increased cross-linking also contributes to tissue stiffening. Collagen and elastin have low turnover rates, and covalent cross-links by advanced glycation end products (AGEs) that occur from a reaction between reducing sugars and matrix proteins accumulate with aging (10). Hyperglycemic
Table 2. Select FDA-approved drugs with repurposing potential for mechano-based therapeutic interventions.
Drug Trade name Company Disease Target Reference
Pirfenidone Esbriet Genentech Idiopathic lung fibrosis TGF signaling (36)
Nintedanib Ofev Boehringer Ingelheim Idiopathic lung fibrosis VEGF, FGF, and PDGF receptors
(40)
Statins Multiple Multiple Cardiovascular disease Rho, YAP/TAZ (98, 125)
Verteporfin injection Visudyne Novartis Macular degeneration YAP (126)
Bortezomib Velcade Takeda Multiple myeloma NF-B (138, 139)
Ixazomib Nilaro Takeda Multiple myeloma NF-B (139)
Carfilzomib Kyprolis Amgen Multiple myeloma NF-B (138, 139)
Vemurafenib Zelboraf Genentech Melanoma B-Raf (146)
Dabrafenib Tafinlar Novartis Melanoma B-Raf (145, 146)
Cobimetinib Cotellic Genentech Melanoma MEK (146)
Trametinib Mekinist Novartis Melanoma MEK (145, 146)
by guest on August 8, 2019
http://stm.sciencem
ag.org/D
ownloaded from

Lampi and Reinhart-King, Sci. Transl. Med. 10, eaao0475 (2018) 3 January 2018
S C I E N C E T R A N S L A T I O N A L M E D I C I N E | R E V I E W
5 of 14
diabetic individuals have increased susceptibility to glycation and therefore experience accelerated tissue cross-linking (3). Dysregulated enzymatic cross-linking of matrix components also contributes to stiffening. Lysyl oxidase (LOX) and tissue transglutaminase (TG2) are implicated in these processes during cancer, fibrotic progression, and age-related arterial stiffening (43, 44). Breaking or preventing ECM cross-links is an attractive therapeutic approach to stall, reverse, or prevent pathologies that are partially driven by increased matrix stiffness, and appears promising from reports that hepatic stellate cells respond to both the mechanical stiffening and softening of their ECM in situ (45).
Despite initial indications of clinical potential, there are no glycation- related therapeutics on the market. The pioneering AGE breaker, alagebrium, and the AGE inhibitor, aminoguanidine, had contra-dictory clinical trial results, and toxicity risks ultimately prohibited further consideration of their therapeutic use (46). Other therapeu-tics to break or inhibit glycation cross-links have been investigated and are reviewed extensively elsewhere; however, despite a diverse range of candidate compounds, limited clinical success targeting AGEs has been achieved (46). Repeatedly, in vitro results are not replicated in vivo. Progress is hindered by poorly defined mechanisms of tar-get compounds, and the widespread use of bovine serum albumin (BSA) as a model protein does not capture the diversity of glycation cross-links found in vivo. Synthetic AGE-BSA compounds produced in vitro behave differently than native AGEs (47). Toxicity and low efficacy are common outcomes of clinical trials, indicating the need for AGE therapeutics with increased specificity.
In addition to growth factor targeting, preliminary studies sug-gest that aptamers are also effective at ameliorating the deleterious effects of AGEs (48). Aptamer therapy prevented increases in serum AGEs in a diabetic rat model (48). Long-term administration was well tolerated, suggesting that aptamer translation to clinical use may not be hindered by the same toxicological limitations of small-molecule AGE inhibitors and breakers. In light of the challenges to develop drugs against glycation, diet adjustments that reduce circulating AGEs, and evidence that exercise reduces AGE cross-linking in tissues, should also be emphasized for their therapeutic potential and ease of im-plementation (49, 50).
Lysyl oxidaseLOX and TG2 are cell-produced proteins; therefore, enzymatic cross- linking can be targeted at the transcriptional, posttranslational, and catalytic levels. The paradoxical outcomes of LOX activity, and the specific contexts in which it is pro- or antipathogenic, are ongoing areas or research (51). LOX is increasingly considered as a therapeutic target because of its dual role in the formation of the tumor stroma and the premetastatic niche, in addition to its deleterious activity during fibrosis and atherosclerosis. The effectiveness of inhibiting LOX cross-linking to reduce ECM stiffness and improve pathological outcomes has been well established using the competitive inhibitor -aminopropionitrile (BAPN). In the apolipoprotein E (ApoE) knockout mouse model of atherosclerosis, BAPN inhibition of LOX decreased aortic stiffness and atherosclerotic plaque burden (52). BAPN treatment attenuated stiff-ness and reduced malformed microvasculature in murine tumors (53). In a murine model of fibrosis, BAPN inhibited liver fibrosis and pro-moted its reversal (54). Although BAPN is a valuable research tool and validates LOX as a clinical target to prevent pathological pro-gression caused by matrix cross-linking, high toxicity during clini-cal trials precludes its clinical use (55).
Monoclonal antibody inhibition of LOX-like 2 (LOXL2) was pursued by Gilead Sciences with GS-6624, but the culmination of phase 2 clinical trials during late 2016 revealed no benefit for cancer and fibrotic disease patients (NCT01472198; NCT01769196; NCT017595110) (56–58). A sizeable challenge in the race to create effective LOX inhibitors is that the complete crystal structure, which is typically used to guide small- molecule development pipelines, remains unknown for mammalian LOX (59). Therefore, alternative approaches that include inhibiting the LOX transcription factor or preventing posttranslational cleavage of the precursor peptide by BMP-1 have been proposed (59). Treatment with the nonspecific copper chelator tetrathiomolybdate, which de-pletes the LOX catalytic site of copper, resulted in lowered serum LOXL2 concentrations during phase 2 clinical trials in individuals with moderate- to high-risk primary stage breast cancer (NCT00195091) (60). Corresponding murine models demonstrated that copper depletion contributed to antipathogenic ECM remodeling by decreasing LOX, collagen deposition, and collagen fiber length in premetastatic lungs (60). Tetrathiomolybdate has also been pursued in biliary cirrhosis (NCT00805805) and non–small cell lung cancer (NCT01837329). Tetra-thiomolybdate treatment is favorable because of its simple oral ad-ministration route, excellent tolerability, and greater LOX inhibition when compared to BAPN (60).
Tissue transglutaminasePharmacological inhibition of TG2 is in preclinical stages with classical small-molecule competitive, reversible, and irreversible inhibitors (61). A TG2 inhibitor was investigated in Canadian clinical trials where poor efficacy was demonstrated, and an irreversible TG2 inhibitor is in phase 1b clinical trials in Europe, but limited information is available about these efforts (61, 62). TG2 is found in almost all tissues: It is a cytosolic protein with catalytic, G protein, kinase, cell survival, and transcription-regulating roles (44). The ubiquitous nature of TG2 and its multifaceted impact on cell behaviors beyond ECM cross-linking make it a difficult therapeutic target. The challenge of developing effec-tive small-molecule inhibitors is exacerbated by evidence that TG2 exists in multiple conformational states and has several structural domains (44). Therefore, less conventional methods that abolish TG2 activity by limiting its expression are also being pursued. Upstream inhibitors of the extracellular signal–regulated kinase (ERK) pathway that down-regulate TG2 expression and small interfering RNA (siRNA) have successfully demonstrated preclinical potential as antifibrotic therapies (63, 64). TG2 siRNA coupled with liposome delivery yielded effective organ-specific targeting to the liver and lungs in mice (64).
Matrix metalloproteinasesECM homeostasis is an intricate balance of matrix synthesis, modi-fication, and degradation. In vitro models of matrix softening demon-strated a reversion of the myofibroblast phenotype and -SMA expression in activated hepatic stellate cells (45). Paradoxically, dysregulated pro-teolytic activity also contributes to the progression of stiffness-mediated pathologies. Microarray analysis of fibrotic lung biopsies from pa-tients demonstrated that up-regulated expression of matrix proteins occurred in concert with altered degradome expression that included MMP up-regulation (65). Cancer, fibrosis, and cardiovascular disease are all associated with dysregulated MMP activity (66).
Although MMPs are most recognized for their proteolytic activity that directly degrades the ECM, matrix components account for only 20% of MMP substrates, and their ability to cleave and activate growth factors, chemokines, cytokines, and receptors is associated with conflicting
by guest on August 8, 2019
http://stm.sciencem
ag.org/D
ownloaded from

Lampi and Reinhart-King, Sci. Transl. Med. 10, eaao0475 (2018) 3 January 2018
S C I E N C E T R A N S L A T I O N A L M E D I C I N E | R E V I E W
6 of 14
cell processes that promote and inhibit stiffness-mediated pathologies (67). For example, MMPs can release matrix-bound latent TGF, but their expression can also have antifibrotic effects that promote apopto-sis, and MMPs have a critical role in fibrotic resolution (68–70). Evi-dence indicates that MMP activity is mediated by substrate stiffness, suggesting that MMPs can have an evolving role during disease pro-gression (71). MMPs were heavily pursued in clinical trials to over-come cancer metastasis but failed in patients. Therefore, because of the varied, context-specific effects of MMPs and the precedence of major clinical shortcomings, strategies that rely on altering MMP activity to overcome ECM stiffness have to be pursued with caution (72). Therapeutics with high specificity are necessary but are chal-lenging to develop because of similarities between catalytic sites and functional redundancy among the 24 mammalian MMP family mem-bers (72). The success of MMP therapeutic strategies will also rely on correctly identifying the appropriate pathological stage during which to administer the drugs to avoid amplifying MMP disease-promoting effects.
A disintegrin and metalloproteinase/a disintegrin and metalloproteinase with thrombospondin motifsAlthough less well studied than MMPs, microarray analysis from fi-brotic and cancerous tissues identified altered gene expression pro-files of other ECM proteases (65, 73). Subsequent mechanistic studies are elucidating critical roles for both direct and indirect ECM re-modeling by the closely related a disintegrin and metalloproteinase (ADAM) and ADAMs with thrombospondin motifs (ADAMTS) pro-tease family members (74). One notable example is ADAMTS1, which has been identified as an activator of TGF. Up-regulated ADAMTS1 expression increased collagen I production, and administration of a competitive ADAMTS1 peptide prevented fibrotic liver damage in mice (75). In pancreatic cancer, pleiotropic effects of ADAMTS1 in-clude degrading veriscan to create a protumorigenic microenviron-ment, cleaving epithelial-like growth factors to promote metastasis, and recruiting CAFs (76). Similar to MMPs, ADAMs and ADAMTSs can be both tumor promoters and inhibitors, underscoring the im-portance of controlled proteolytic activity to homeostasis (74). The utility of targeting ADAMs and ADAMTSs in the context of ECM remodeling will depend on future studies that identify isoform func-tions that are ECM-specific. Feasibility and safety of generating inhibi-tors against these protease families can be gleaned from early clinical trial pursuits with INCB7839, an inhibitor of ADAM10 and ADAM17, to treat breast cancer and diffuse large B cell non-Hodgkin lymphoma (NCT00820560, NCT00864175, NCT01254136, and NCT02141451) (77).
The contribution of the ECM in promoting cancer malignancy, atherogenesis, and fibrosis is becoming increasingly appreciated, but many questions remain unanswered. Data now indicate that stiffen-ing precedes fibrosis and hypertension, that proliferation and migration increase with increased matrix stiffness, and that epithelial-mesenchymal transition and TGF stimulation are matrix stiffness–dependent (78–81). In addition, similar gene expression profiles observed between cells originating from dense breast tissue and the tumor stroma suggest that mechanically mediated epigenetic regulation may initiate disease (82). If matrix stiffness is a driving factor that causes an even stiffer ECM, then what are the initial mechanisms contributing to prepatho-logical increases in matrix rigidity? As these pathways are unveiled, it is anticipated that new therapeutic targets will also be identified to interrupt matrix stiffening at earlier stages of disease development. Advances in mitigating matrix stiffness directly will likely draw on
clinical successes from other settings where matrix turnover is crit-ical, such as scar and wound healing (62).
INTERRUPTING CELLULAR RESPONSES TO INCREASED ECM STIFFNESSIntegrinsInstead of preventing ECM stiffening, which occurs with advanced age and can precede disease, an alternative approach to overcome the adverse effects of microenvironment stiffening is to inhibit the cellular response to increased matrix mechanics that contributes to pathogen-esis. The ECM activates integrin-mediated signaling pathways to elicit cellular outcomes; therefore, aberrant mechanotransduction can be dis-rupted at the cell-ECM level and at downstream signaling targets.
Integrin targeting is a logical first choice to interrupt ECM mech-anosensing, because these transmembrane adhesion proteins are con-duits of bidirectional signaling, directly connecting extracellular inputs to intracellular outputs. Integrins have been attributed to cancer ma-lignancy, metastasis, and drug resistance, as evidenced by 30 regis-tered clinical trials that include the integrin inhibitor cilengitide (clinicaltrials.gov) (83). In addition, local proteolytic activity of MMP-9 disrupts v3 integrin engagement, resulting in activated stellate cell apoptosis, suggesting an intersection between matrix softening, inte-grin engagement, and fibrotic resolution (70). Studies in fibroblasts indicate that integrin expression alone does not drive the cellular re-sponse to increased substrate mechanics (12). Selecting which integrins to antagonize to ameliorate matrix stiffness sensing is not straight-forward, and the regulation of diverse cellular events that result from integrin binding is an active area of investigation. The integrin sub-unit recruits focal adhesion kinase (FAK) to initiate downstream sig-naling cascades that include Rho, Src, and ERK and therefore is a potential target to mediate matrix stiffness responses (84). In fibroblasts cultured on fibronectin-coated substrates, rigidity sensing through 51-stimulated Rho-mediated contractility and v integrins activated the GEF-H1 Rho pathway, suggesting other potential targets (85).
The current understanding of force sensing across focal adhesions is centered around a shared sequence of events among autonomous adhesions that begins when integrin dimers bind their ECM ligands (86). Extracellular integrin deformation from cytoskeletal forces is dependent on substrate compliance, which then drives the intracel-lular recruitment of scaffolding proteins, actin-binding reinforcement, and the activation of downstream effectors (86). A stiffened ECM is well established to increase Rho-mediated cellular contractile forces that are necessary for protein conformational changes contributing to focal adhesion maturation, and cell-ECM adhesions are stronger on rigid matrices (86). However, the individual contributions of spe-cific integrin dimer pairs to stiffness sensing and mechanotransduction in a multicomponent ECM have not been fully delineated. Fibronectin and collagen are often used interchangeably as ECM proteins during in vitro experiments studying cellular forces despite groundwork that ECM ligand biochemistry, and thus integrin engagement, influ-ences cellular mechanoresponses (87).
Among integrins, the v family has been identified as a possible therapeutic target for fibrotic pathologies, not for their mechanosen-sitive signaling but rather for facilitating ECM deposition. Engagement of the arginine–glycine–aspartic acid sequence on the latency-associated peptide of TGF1 by integrins coupled with traction forces releases TGF1 from a latency complex (17, 88). A phase 2 clinical trial tested BG00011/STX-100, a humanized monoclonal antibody against v6,
by guest on August 8, 2019
http://stm.sciencem
ag.org/D
ownloaded from

Lampi and Reinhart-King, Sci. Transl. Med. 10, eaao0475 (2018) 3 January 2018
S C I E N C E T R A N S L A T I O N A L M E D I C I N E | R E V I E W
7 of 14
for idiopathic lung fibrosis (NCT01371305) (89); however, to date, Biogen has not publicly published the results of the trial. Whether v integrin inhibitors in development for other applications, such as cilengitide for glioblastoma, also have efficacy against TGF1 remains to be established (90). Integrin inhibition is championed when com-pared to other strategies that target TGF1 because it targets a pop-ulation of TGF1 that becomes active as an outcome of pathological stiffening and circumvents the inflammatory reactions that plague systemic TGF inhibition (91).
Rho GTPaseAs a critical regulator of cytoskeletal dynamics and cellular force through the formation of actin stress fibers, dysregulated Rho sig-naling has been causally attributed to pathological cell contractility, motility, gene expression, cell cycle progression, and survival (92, 93). Elevated Rho guanosine triphosphatase (GTPase) signaling and con-tractile traction forces activated by integrin engagement with the ECM is one of the most widely documented downstream consequences of increased ECM stiffness (Fig. 2) (94). However, Rho is considered “un-druggable” from the standpoint of traditional small-molecule inhibitors because of its three-dimensional structure. Classical small- molecule drugs, designed to bind large hydrophobic pockets on target proteins to form stable inhibitor- protein complexes, cannot bind to Rho be-cause it lacks these hydrophobic clefts (95). As an intracellular protein, Rho is also in-accessible to protein biologics, which are too large to cross the plasma membrane (95). Bacterial toxins that interfere with Rho activity through irreversible modi-fication may hold clinical potential if tight control of their potency and localiza-tion can be achieved. The only known bac-terial secreted Rho-specific inhibitors are clostridial C3 enzymes, but they are lim-ited by poor cellular uptake in cell types other than macrophages and monocytes (96). Given these limitations, the Rho path-way has been targeted upstream or down-stream of the mature GTPase to inhibit Rho localization, prevent Rho activation by guanine nucleotide exchange factors (GEFs), and target downstream effectors.
Rho localization is important to its ac-tivation and is regulated by posttransla-tional modification (97). Rho is targeted to the plasma membrane where it main-tains close proximity to GEFs that catalyze the exchange of guanosine diphosphate (GDP) for GTP, which activates Rho in a rapid, switch-like manner (97). Statins are widely prescribed to lower serum cho-lesterol by competitive inhibition of the enzyme HMG-CoA reductase during cho-lesterol synthesis and have been pursued to inhibit Rho (98). Because statins block cholesterol synthesis, they also inhibit pre-nylated protein intermediates, including
geranylgeranyl pyrophosphate, which interferes with Rho local-ization and activation (98). Repurposing statins for clinical use be-yond cholesterol lowering is a potential clinical tool to overcome the effects of matrix stiffening that occurs with age or pathology (Table 2). The statin simvastatin attenuated elevated Rho activity caused by increased matrix stiffness in endothelial cells, reduced contractility, and improved endothelial barrier function (99). In fi-broblasts derived from fibrotic lungs, simvastatin attenuated the myofibroblast phenotype and reduced growth factor expression (100). Despite common deleterious roles for increased matrix stiff-ness and elevated Rho, the benefits of statins in cancer are less clear and even conflicting. Pharmacokinetic differences between lipo-philic and hydrophilic statins, heterogeneity between patient cancers, and data extracted from clinical trials designed with cardiovascular end points, rather than as cancer studies, are cited as causes of the inconsistencies (101). Nevertheless, because the off-target effects of statins extend beyond Rho, and noting that matrix stiffness is one of many factors that compound to drive disease progression, the suc-cess or failure of statin repurposing cannot be attributed to altered Rho activity alone.
GEF-H1
Increased ECM sti�ness
LARG ROCK
Rho
MLCP
MRTF-A
SurvivalMigrationProliferationECM synthesis
ECM
YAP/TAZ
MAPK
NF-κB
MLC
PP
P P
Rho GTP
GDP
Nucleus
F
F
Fig. 2. Increased ECM stiffness activates the Rho-mediated cell contractility pathway. Mechanical force on integrins activates the Rho guanine nucleotide exchange factors (GEFs), GEF-H1 and LARG, to catalyze the exchange of guanosine diphos-phate (GDP) for GTP. The major Rho effector Rho-associated kinase (ROCK) induces actomyosin cell contractility by phosphorylat-ing myosin light chain phosphatase (MLCP) and myosin light chain (MLC). Downstream of Rho activation, myocardin-related transcription factor A (MRTF-A), yes-associated protein (YAP)/transcriptional coactivator with PDZ-binding motif (TAZ), nuclear factor B (NF-B), and mitogen-activated protein kinase (MAPK) pathways regulate gene expression, and Rho ac-tivity has pathological implications on cell survival, migration, proliferation, and ECM synthesis. Solid arrows indicate direc-tion of cellular traction force generation (blue) and Rho-mediated contractility pathway events (black). Dashed black arrows represent cellular responses downstream of Rho-mediated cell contractility.C
RE
DIT
: A. K
ITTE
RM
AN
/SC
IEN
CE
TR
AN
SLA
TIO
NA
L M
ED
ICIN
E
by guest on August 8, 2019
http://stm.sciencem
ag.org/D
ownloaded from

Lampi and Reinhart-King, Sci. Transl. Med. 10, eaao0475 (2018) 3 January 2018
S C I E N C E T R A N S L A T I O N A L M E D I C I N E | R E V I E W
8 of 14
Rho GEFsGEFs are a therapeutic target to control Rho activity because of their direct role in activating Rho signaling. GEF targeting has the poten-tial to impart Rho-specific inhibition due to the identification of more than 80 GEFs and the diversity of cellular behaviors that result from intricate upstream signaling pathways that converge at Rho (102). GEF inhibitors can be designed to block GEF-Rho interac-tions or target the GEF catalytic site, both of which terminate for-ward movement of the signal cascade. For example, the compound Rhosin blocks a GEF docking site on RhoA, and a class of compounds named Y16 bind to the GEF catalytic site (103, 104). These RhoA in-hibitors were effective in fibroblasts, neuronal cells, and mammary epithelial cells (103, 104). Within the Rho family of GTPases, Rhosin only inhibits RhoA activity without interrupting the function of other Rho GTPase family members, and Y16 binds to just three RhoA GEFs (LARG, p115, and PDZ), demonstrating high specificity with GEF targeting approaches (104). In silico methods were used to discover these two Rho GEF inhibitors and are becoming powerful tools for rational drug discovery. Because the siRNA techniques used to study GEFs in experimental settings are not applicable to clinical transla-tion, there is a need to develop small-molecule inhibitors. However, similar to Rho, GEFs engage in protein-protein interactions and lack large structural pockets, which make them poor candidates for traditional small-molecule inhibitors. The combination of compu-tational methods with data-driven structural knowledge is identify-ing novel surface sites that are energetically favorable on proteins that were previously deemed undruggable, and because of the high clinical need, it is anticipated that these methods will yield addition-al sites to target Rho signaling and the associated GEFs (105). In fi-broblasts, the Rho GEFs LARG and GEF-H1 have been identified as critical mediators of the cellular response to integrin force and there-fore are ideal GEF targets for dampening cell-ECM mechano-transduction (106). As the ability to target Rho signaling expands, a more complete understanding of the expression, function, regula-tion, and activation of individual GEFs in specific cell types will be necessary.
Rho-associated kinaseROCK is the major downstream effector of Rho that drives cell con-tractility and is a mediator of fibrotic pathologies (93, 107). ROCK phosphorylates myosin light chain and myosin light chain phos-phatase to induce the generation of cellular force from actomyosin filament contraction. Recently, a stiffness-dependent role for ROCK in driving fibroblast to myofibroblast conversion in pulmonary fibro-sis was identified, and ROCK inhibition attenuated increased endo-thelial permeability caused by age-related increased intima stiffness (107, 108).
ROCK inhibition can be pursued using traditional small-molecule discovery efforts but is also plagued by nonspecificity. The two most prominent small-molecule ROCK inhibitors, fasudil and Y27632, not only target the adenosine 5′-triphosphate (ATP)–dependent ROCK kinase domain but also show nonspecific interactions with other kinases (109). The effectiveness of fasudil and Y27632 is hypothesized to be partially due to their off-target effects with other kinases (109). In addition to its pathological role, ROCK helps maintain homeostatic vascular tone via vascular smooth muscle cell contraction (109), and ROCK inhibitors such as fasudil can be designed and used with this motivation. However, drugs that are successful in vitro for different clinical applications of ROCK inhibition can also induce unwanted
decreases in blood pressure when transferred to animal models or humans, creating a barrier to their clinical adaptation. Nevertheless, fasudil has been used in Japan since 1995 for the treatment of cere-bral vasospasms, and ROCK inhibitors have been widely investigated to treat a variety of pathologies either alone or as a combination treat-ment (109). Fasudil has an impressive record of safety and efficacy but has not been commercially marketed in the United States. The composition of matter patent on fasudil expired in early 2016, and although its commercial future is unknown, it continues to be eval-uated in preclinical and clinical studies (U.S. Patent 5,942,505). A timely preclinical investigation in mice recently reported that prim-ing with fasudil to inhibit Rho pathway–mediated ECM remodeling markedly improved the efficacy of the current standard-of-care pan-creatic chemotherapies gemcitabine and Abraxane at both the pri-mary tumor and metastatic sites (110).
New ROCK inhibitors, such as ripasudil (a fasudil derivative), have emerged from the clinical need to lower ocular pressure in glaucoma (111). One approach to mitigate the off-target effects of ROCK in-hibitors is the development of “soft inhibitors,” which are designed to degrade into inactive metabolites when not at their target site for improved patient tolerability (112). The soft inhibitor AMA0076, which completed phase 2 clinical trials (NCT02136940 and NCT01693315), is structurally based on Y27632 but exhibits tissue-specific hydrolysis rates in the eye (112). Pharmacological efforts distinguishing the dis-tinct roles of the two ROCK isoforms, ROCK1 and ROCK2, are also in progress (113). The development of small-molecule inhibitors that exhibit greater specificity toward the ROCK family kinases or its spe-cific isoforms are using high-throughput screening and fragment- based approaches (109). New patents for clinical siRNA inhibition of ROCK have also been filed (109).
Focal adhesion kinaseFAK is a cytosolic nonreceptor tyrosine kinase activated by integrin clustering and is a regulator of focal adhesion dynamics and Rho ac-tivity (114). FAK activation is upstream of the Ras–mitogen-activated protein kinase (MAPK) cascade (115). FAK integrates ECM signals from integrins to activate downstream pathways that control adhesion, proliferation, motility, and survival (114). In addition, focal adhesions are sites of actomyosin force transmission to the ECM; therefore, FAK is a potential upstream target to inhibit cellular responses to matrix mechanical cues. Increased matrix stiffness increases phosphorylation of FAK at Tyr397, which is necessary for Src binding, and complete FAK activation through additional phosphorylation (114, 116). Dysregulated FAK-Src signaling is widely appreciated for its role in cancer invasion and metastasis, and consequently, the development of FAK inhibi-tors is concurrently being pursued by GlaxoSmithKline, Novartis, Merck, Takeda, and Pfizer, in addition to efforts by smaller pharma-ceutical companies (117, 118). These inhibitors primarily target the FAK catalytic site and have reached clinical trials as mono- or com-bination therapies (117, 118). Stiffness-induced up-regulated FAK activation is also deleterious in noncancer pathologies. Constitutive phosphorylation of the kinase is found in fibrotic fibroblasts, and FAK signaling potentiates growth factor signaling and the myofibroblast phenotype (119). In addition, mechanically driven FAK-ERK pathways activate the Rho GEF, GEF-H1 (106).
As a druggable protein, FAK suffers from the same limitations as other kinases, namely, similarity in the catalytic domain that imparts nonspecific cross-reactivity of small-molecule inhibitors. Among a subset of kinases, improved selectivity has been demonstrated with
by guest on August 8, 2019
http://stm.sciencem
ag.org/D
ownloaded from

Lampi and Reinhart-King, Sci. Transl. Med. 10, eaao0475 (2018) 3 January 2018
S C I E N C E T R A N S L A T I O N A L M E D I C I N E | R E V I E W
9 of 14
allosteric inhibitors directed to a flexible Aps-Phe-Gly (DFG) amino acid trio at the N terminus of the activation loop (120). In these ki-nases, the DFG portion undergoes dramatic conformational changes as it switches between active and inactive states and has been iden-tified as a domain that imparts selectivity when targeted in the inac-tive state (120). Inhibitors stabilizing a unique -helical conformation of the FAK DFG domain have exhibited robust selectivity and effi-cacy when tested in mice (121). Other recent efforts to target FAK signaling are designed to inhibit scaffolding interactions with down-stream effectors (117). These approaches are advantageous, because they target specific lineages of FAK signaling (117). Another current approach to targeted FAK inhibition prevents autophosphorylation at Tyr397, which is particularly relevant to attenuating aberrant FAK activation caused by increased ECM stiffness (122). For detailed discussions on FAK pharmacological development, the reader is di-rected to reviews by Golubovskaya (117) and Lee et al. (118).
Yes-associated protein/transcriptional coactivator with PDZ-binding motifThe cellular response to increased ECM stiffness also occurs at the transcriptional level. The downstream effectors of the Hippo pathway, yes-associated protein (YAP) and transcriptional coactivator with PDZ-binding motif (TAZ), known for mediating transcriptional reg-ulation of apoptosis and proliferation, are also activated by increased matrix rigidity independent of the canonical Hippo cascade (123). YAP/TAZ activation by matrix stiffness contributes to fibroblast pheno-typic conversion, increased collagen deposition, and cell proliferation by augmenting feed-forward cycles that enhance microenvironment stiffening (124). YAP/TAZ also potentiates TGF signaling (124). Acto-myosin contractility is necessary for stiffness-induced YAP activation, and inhibiting intercellular tension by abrogating Rho activation atten-uates YAP/TAZ nuclear localization (123). The ongoing efforts to de-velop therapeutic Rho antagonists represent an indirect mechanism to inhibit stiffness-mediated YAP/TAZ activation. Already, statins have been identified as strong inhibitors of YAP/TAZ nuclear local-ization due to the crossover between the synthesis of cholesterol in-termediates and the synthesis of geranylgeranyl pyrophosphate for Rho posttranslational modification (125). Direct inhibition of YAP/TAZ has been pursued using small-molecule inhibitors that prevent YAP/TAZ from associating with their target TEA/ATTS domain (TEAD) transcription factors in the nucleus (126). The Novartis photosensi-tizer Visudyne prevented YAP from interacting with TEAD during treatment for macular degeneration, and Visudyne attenuated YAP- mediated oncogenic liver overgrowth in transgenic mouse models (126). A peptide designed to mimic the native inhibition of YAP-TEAD association by vestigial-like family member 4 (VGLL4) inhibited YAP (127). As our understanding of the cross-talk between the Hippo and mechanotransduction pathways and regulation of YAP/TAZ in both normal and pathological settings increases, new therapeutic ap-proaches to target YAP/TAZ will likely emerge. YAP inhibition in he-patic stellate cells impeded the activated cell phenotype in vitro and prevented liver fibrosis in mice, indicating that transcriptional regu-lation may be a method to inhibit tissue stiffening (128). Screens of avail-able drugs have yielded candidates that can be repurposed to inhibit YAP/TAZ, suggesting an accelerated track for druggable efforts.
Myocardin-related transcription factor–AMyocardin-related transcription factor–A (MRTF-A) is another transcriptional coactivator with ECM remodeling implications that
undergoes nuclear localization with increasing matrix stiffness (129). MRTF-A induces fibrogenesis downstream of cellular force genera-tion by Rho activation and actin polymerization (129). In addition to activation by cellular tension, TGF intersects with MRTF-A ac-tivation and also induces its nuclear translocation, further linking matrix stiffness and TGF in a self-propagating cycle (130). The com-pound CCG-1423 inhibited transcription along the Rho/MRTF/serum response factor (SRF) pathway, downstream of Rho activation, by bind-ing to the MRTF-A nuclear localization sequence (131). Although CCG- 1423 suffered from high toxicity, structural insights into the rational design of Rho-mediated transcription inhibitors informed the devel-opment of new compounds with improved cytocompatibility. Atten-uated collagen-I and -SMA expression induced by TGF was achieved in myofibroblasts treated with the second-generation MRTF-A inhib-itors, CCG-100602 and CCG-20397, validating stiffness-mediated Rho transcription as a therapeutic target (129).
Nuclear factor BRho-generated contractile forces initiated by ECM rigidity cues have been identified as regulators of the transcription factor nuclear factor B (NF-B) (132). NF-B is a key regulator of inflammation, con-sistent with the observation that aberrant connective tissue growth in the tumor stroma and fibrosis reflect a dysregulated wound heal-ing process (13, 133). In cell culture experiments, Rho-dependent nuclear localization of NF-B was shown to increase with substrate stiffness and resulted in the expression of the inflammatory markers interleukin-1 (IL-1), IL-8, and MMP9 (132). Nuclear translation of NF-B scaled with ECM stiffness in both nonmetastatic and meta-static breast cancer cells stimulated with tumor necrosis factor– (TNF-) (134). Because cell shape, cytoskeletal tension, and cell-cell adhesions regulate NF-B, Rho can also negatively regulate NF-B independent of stiffness in the presence of other cues and TNF- stimulation (134). Both NF-B and YAP/TAZ activation share depen-dencies on cell shape and ECM stiffness; however, nuclear localization of NF-B is transient and rapid, occurring within hours, whereas mea-surable YAP/TAZ translocation requires days. These data suggest unique sensitivities of transcription factors regulated by ECM-mediated, Rho-generated actomyosin forces (132, 135).
Therapeutic targeting of NF-B for cancer is also applicable to fi-brosis (for example, NF-B contributes to hepatic injury progression to cirrhosis) (136). However, NF-B inhibition is limited by side ef-fects resulting from systemic disruption of the innate immune response and overproduction of the inflammatory cytokine IL-1 (137). FDA- approved therapeutics that inhibit NF-B activity include bortezomib, carfilzomib, and ixazomib, with registered clinical trials to study their efficacy in cancers (138, 139). Initial clinical trials of bortezomib out-side of hematological cancers had disappointing results, but there are currently 848 registered clinical trials for bortezomib, 144 registered for carfilzomib, and 90 for ixazomib, demonstrating the strong clin-ical interest in NF-B inhibitors, with others in preclinical develop-ment (clinicaltrials.gov) (140).
Mitogen-activated protein kinaseForce-dependent integrin activation can initiate MAPK cascades to affect cell survival, gene transcription, and myofibroblast differenti-ation (141, 142). Stiffness-mediated activation of MAPK signaling through ERK is FAK-dependent, consistent with an established role for FAK as an intermediate in integrin-mediated mechanotransduc-tion (106, 115). TGF induces CTGF expression through Ras-ERK
by guest on August 8, 2019
http://stm.sciencem
ag.org/D
ownloaded from

Lampi and Reinhart-King, Sci. Transl. Med. 10, eaao0475 (2018) 3 January 2018
S C I E N C E T R A N S L A T I O N A L M E D I C I N E | R E V I E W
10 of 14
signaling, and emerging data from mesenchymal stem cell differen-tiation suggest that CTGF expression is, in part, dependent on ECM stiffness (143, 144). Matrix stiffness and Rho activation have already been reported to intersect with MAPK pathway activation. In mam-mary epithelial cells, sustained activation of Rho induced by elevated ECM stiffness activated Ras-ERK signaling to promote increased cell proliferation and invasiveness, both of which are signatures of cancer malignancy (115). Because of the high occurrence of aberrant MAPK signaling in cancer, inhibitors of MAPK pathway intermedi-ates Ras, Raf, MEK (MAPK kinase), and ERK have been pursued; how-ever, intrinsic and acquired drug resistance have emerged as major limitations of these therapies (145). Aberrant signal initiation from receptor tyrosine kinases (RTKs) on the cell surface is one cause of poor long-term success of MAPK pathway inhibitors (145). Matrix- mediated MAPK signaling is initiated through integrins rather than RTKs; therefore, it is possible that sustained therapeutic inhibition could be achieved in the specific context of attenuating ECM stiff-ness effects (115). Combination therapies and new inhibitors are being pursued to circumvent acquired inhibitor resistance and complement the approved MAPK cascade inhibitors: vemurafenib (B-Raf inhibi-tor), dabrafenib (B-Raf inhibitor), cobimetinib (MEK inhibitor), and trametinib (MEK inhibitor) (145, 146).
Alternative splicingVariations in gene expression by alternative splicing were recently found to be regulated by ECM mechanics. Bordeleau et al. (147) reported that expression of the extra domain B–fibronectin (EDB-FN) splice variant, commonly found in tumors and proposed to contribute to tumorigenesis, is regulated by increased matrix stiffness in vitro and in murine models. The splicing event depends on Rho-mediated cell contractility. Alternative splicing of protein kinase C (PKC) BII and VEGF 165b were also identified as matrix stiffness–dependent. The phosphorylation of serine-arginine–rich (SR) proteins that mediate splicing increased with matrix stiffness via phosphoinositide 3-kinase (PI3K)/protein kinase B (AKT) signaling. These data suggest that other splice variant proteins that aberrantly appear in the ECM milieu of stiffened tissues, such as EDA-FN that induces myofibroblast differen-tiation (22, 142), may also be mediated by matrix mechanics through a similar pathway. TGF is often up-regulated in pathologically stiff microenvironments and contributes to splicing events, suggesting that alternative splicing may involve synergistic contributions be-tween mechanical cues and ECM components (148). SR proteins or the PI3K/AKT pathways are potential therapeutic targets to control stiffness-mediated splicing events, in addition to current approach-es using oligonucleotides and small molecules (149).
Nuclear mechanicsThe cell nucleus is mechanically coupled to the actin cytoskeleton by an assembly of proteins that comprise the linker of nucleoskele-ton and cytoskeleton (LINC) complex and by extension to integrins and the ECM (150). Externally applied force, as well as cell-generated intercellular tension, is propagated to the nucleus, which itself is a mechanotransducer (150). Force propagation across the cytoskele-ton occurs orders of magnitude faster than biochemical signaling, and the nucleus is involved in the integration of and response to these mechanical inputs (150). Because cellular DNA is stored in the nu-cleus, transmitted forces that induce changes in protein conformation, alter protein associations, or deform chromatin may have transcrip-tional implications (151).
Lamins are nuclear intermediate filaments that create a struc-tured protein network associated with the interior nuclear mem-brane and are implicated in both nuclear mechanotransduction and matrix stiffening responses (151). Lamin-A content in murine tis-sues increased with matrix stiffness, and nuclear envelope stability and stiffness correlate with increased lamin-A content (152). In addi-tion to transducing force, lamins are scaffolding proteins that interact with transcription factors and bind chromatin (151). Lamin-dependent regulation of the MRTF-A/SRF and YAP/TAZ pathways may explain the excessive ECM production in many laminopathies and demon-strate another mechanism by which ECM protein transcription is regulated by matrix stiffness (153). Therapeutic targets for nuclear mechanotransduction are likely to be discovered in parallel with the development of improved technologies to study subcellular pro-cesses. However, the complexity and delicacy of the nucleus, coupled with our current understanding of mechanotransduction, suggest that the best therapeutic options to intervene lie within already dis-cussed mechanotransduction sensing components. Force transmis-sion to the nucleus requires cells under prestress, which can be modulated by Rho contractility (150). In addition, MRTF-A and YAP/TAZ path-ways can be targeted independent of lamin regulation as already described.
CONCLUSION AND FUTURE OUTLOOKTwo key players emerge from the discussion of potential therapeutic targets to overcome pathological ECM stiffening: TGF and Rho. Their pleiotropic effects converge as they function in concert to pro-mote feed-forward cycles that amplify ECM production and stiffening. However, they also represent elusive therapeutic targets because of their ubiquitous expression and key functions in tissue homeostasis. A common underlying theme is a need for high potency and specific-ity among druggable efforts. Off-target interactions are a major hurdle for developing kinase inhibitors, and high toxicities have been crip-pling to the development of small molecules to prevent or disrupt matrix cross-linking. Moreover, these interventions need to be localized to the organs of interest to further minimize deleterious side effects. Improved specificity is anticipated with the development of aptamer technologies and new approaches to small-molecule drug develop-ment that use multifaceted approaches combining thermodynamics, structural biology, and mathematical computation (41, 105). The iden-tification of inhibitor sites on previously undruggable proteins, in-cluding Rho, should vastly expand the available therapeutic library.
With the recognition of ECM stiffness as a contributing factor to multiple pathologies, the development of clinical technologies to non-invasively measure local tissue mechanics is necessary to achieve earlier diagnoses and better patient outcomes. From an academic perspec-tive, these modalities will contribute to increased understanding of pathological stiffening in its earliest stages at a resolution beyond the current clinical limit and will drive research efforts to identify novel clinical targets—perhaps even preventing full disease manifestation. Building off the strong foundation of the mechanotransduction field and the importance of microenvironment stiffness established over the past two decades, we can now work toward mitigating the effects of increased ECM stiffness in the emerging field of mechanomedicine. As has already been discovered for other pathologies, the most success-ful mechano-based therapeutic interventions for tissue stiffening will likely include combination therapies to reach more than one tar-get and overcome cellular redundancies.
by guest on August 8, 2019
http://stm.sciencem
ag.org/D
ownloaded from

Lampi and Reinhart-King, Sci. Transl. Med. 10, eaao0475 (2018) 3 January 2018
S C I E N C E T R A N S L A T I O N A L M E D I C I N E | R E V I E W
11 of 14
REFERENCES AND NOTES 1. M. B. Barton, R. Harris, S. W. Fletcher, Does this patient have breast cancer? The screening
clinical breast examination: Should it be done? How? JAMA 282, 1270–1280 (1999). 2. S. Sidney, C. P. Quesenberry, M. G. Jaffe, M. Sorel, M. N. Nguyen-Huynh, L. H. Kushi,
A. S. Go, J. S. Rana, Recent trends in cardiovascular mortality in the United States and public health goals. JAMA Cardiol. 1, 594–599 (2016).
3. V. M. Monnier, G. T. Mustata, K. L. Biemel, O. Reihl, M. O. Lederer, D. Zhenyu, D. R. Sell, Cross-linking of the extracellular matrix by the maillard reaction in aging and diabetes: An update on “a puzzle nearing resolution”. Ann. N. Y. Acad. Sci. 1043, 533–544 (2005).
4. A. M. Handorf, Y. Zhou, M. A. Halanski, W.-J. Li, Tissue stiffness dictates development, homeostasis, and disease progression. Organogenesis 11, 1–15 (2015).
5. K. M. Riching, B. L. Cox, M. R. Salick, C. Pehlke, A. S. Riching, S. M. Ponik, B. R. Bass, W. C. Crone, Y. Jiang, A. M. Weaver, K. W. Eliceiri, P. J. Keely, 3D collagen alignment limits protrusions to enhance breast cancer cell persistence. Biophys. J. 107, 2546–2558 (2014).
6. M. W. Pickup, J. K. Mouw, V. M. Weaver, The extracellular matrix modulates the hallmarks of cancer. EMBO Rep. 15, 1243–1253 (2014).
7. B. M. Kaess, J. Rong, M. G. Larson, N. M. Hamburg, J. A. Vita, D. Levy, E. J. Benjamin, R. S. Vasan, G. F. Mitchel, Aortic stiffness, blood pressure progression, and incident hypertension. JAMA 308, 875–881 (2012).
8. C. Frantz, K. M. Stewart, V. M. Weaver, The extracellular matrix at a glance. J. Cell Sci. 123, 4195–4200 (2010).
9. J. D. Humphrey, E. R. Dufresne, M. A. Schwartz, Mechanotransduction and extracellular matrix homeostasis. Nat. Rev. Mol. Cell Biol. 15, 802–812 (2014).
10. J. C. Kohn, M. C. Lampi, C. A. Reinhart-King, Age-related vascular stiffening: Causes and consequences. Front. Genet. 6, 112 (2015).
11. C. Bonnans, J. Chou, Z. Werb, Remodelling the extracellular matrix in development and disease. Nat. Rev. Mol. Cell Biol. 15, 786–801 (2014).
12. T. Yeung, P. C. Georges, L. A. Flanagan, B. Marg, M. Ortiz, M. Funaki, N. Zahir, W. Ming, V. Weaver, P. A. Janmey, Effects of substrate stiffness on cell morphology, cytoskeletal structure, and adhesion. Cell Motil. Cytoskeleton 60, 24–34 (2005).
13. R. Kalluri, The biology and function of fibroblasts in cancer. Nat. Rev. Cancer 16, 582–598 (2016).
14. B. Hinz, S. H. Phan, V. J. Thannickal, A. Galli, M.-L. Bochaton-Piallat, G. Gabbiani, The myofibroblast: One function, multiple origins. Am. J. Pathol. 170, 1807–1816 (2007).
15. F. Klingberg, B. Hinz, E. S. White, The myofibroblast matrix: Implications for tissue repair and fibrosis. J. Pathol. 229, 298–309 (2013).
16. L. F. Castella, G. Gabbiani, C. A. McCulloch, B. Hinz, Regulation of myofibroblast activities: Calcium pulls some strings behind the scene. Exp. Cell Res. 316, 2390–2401 (2010).
17. P.-J. Wipff, D. B. Rifkin, J.-J. Meister, B. Hinz, Myofibroblast contraction activates latent TGF-1 from the extracellular matrix. J. Cell Biol. 179, 1311–1323 (2007).
18. D. Jia, Z. Liu, N. Deng, T. Z. Tan, R. Y.-J. Huang, B. Taylor-Harding, D.-J. Cheon, K. Lawrenson, W. R. Wiedemeyer, A. E. Walts, B. Y. Karlan, S. Orsulic, A COL11A1-correlated pan-cancer gene signature of activated fibroblasts for the prioritization of therapeutic targets. Cancer Lett. 382, 203–214 (2016).
19. S. Yazdani, R. Bansal, J. Prakash, Drug targeting to myofibroblasts: Implications for fibrosis and cancer. Adv. Drug Deliv. Rev. 121, 101–116 (2017).
20. A. Douglass, K. Wallace, R. Parr, J. Park, E. Durward, I. Broadbent, C. Barelle, A. J. Porter, M. C. Wright, Antibody-targeted myofibroblast apoptosis reduces fibrosis during sustained liver injury. J. Hepatol. 49, 88–98 (2008).
21. B. Hinz, G. Gabbiani, C. Chaponnier, The NH2-terminal peptide of –smooth muscle actin inhibits force generation by the myofibroblast in vitro and in vivo. J. Cell Biol. 157, 657–663 (2002).
22. B. Hinz, Masters and servants of the force: The role of matrix adhesions in myofibroblast force perception and transmission. Eur. J. Cell Biol. 85, 175–181 (2006).
23. N. Sampson, R. Koziel, C. Zenzmaier, L. Bubendorf, E. Plas, P. Jansen-Dürr, P. Berger, ROS signaling by NOX4 drives fibroblast-to-myofibroblast differentiation in the diseased prostatic stroma. Mol. Endocrinol. 25, 503–515 (2011).
24. Q. Yao, S. Cao, C. Li, A. Mengesha, B. Kong, M. Wei, Micro-RNA-21 regulates TGF--induced myofibroblast differentiation by targeting PDCD4 in tumor-stroma interaction. Int. J. Cancer 128, 1783–1792 (2011).
25. B. Hinz, G. Gabbiani, Fibrosis: Recent advances in myofibroblast biology and new therapeutic perspectives. F1000 Biol. Rep. 2, 78 (2010).
26. S. O’Reilly, MicroRNAs in fibrosis: Opportunities and challenges. Arthritis Res. Ther. 18, 11 (2016).
27. B. C. Özdemir, T. Pentcheva-Hoang, J. L. Carstens, X. Zheng, C.-C. Wu, T. R. Simpson, H. Laklai, H. Sugimoto, C. Kahlert, S. V. Novitskiy, A. De Jesus-Acosta, P. Sharma, P. Heidari, U. Mahmood, L. Chin, H. L. Moses, V. M. Weaver, A. Maitra, J. P. Allison, V. S. LeBleu, R. Kalluri, Depletion of carcinoma-associated fibroblasts and fibrosis induces immunosuppression and accelerates pancreas cancer with reduced survival. Cancer Cell 25, 719–734 (2014).
28. A. Biernacka, M. Dobaczewski, N. G. Frangogiannis, TGF- signaling in fibrosis. Growth Factors 29, 196–202 (2011).
29. D. R. Edwards, G. Murphy, J. J. Reynolds, S. E. Whitham, A. J. Docherty, P. Angel, J. K. Heath, Transforming growth factor beta modulates the expression of collagenase and metalloproteinase inhibitor. EMBO J. 6, 1899–1904 (1987).
30. C. M. Kraning-Rush, J. P. Califano, C. A. Reinhart-King, Cellular traction stresses increase with increasing metastatic potential. PLOS ONE 7, e32572 (2012).
31. K. E. Lipson, C. Wong, Y. Teng, S. Spong, CTGF is a central mediator of tissue remodeling and fibrosis and its inhibition can reverse the process of fibrosis. Fibrog. Tissue Repair 5, S24 (2012).
32. J. G. Abreu, N. I. Ketpura, B. Reversade, E. M. De Robertis, Connective-tissue growth factor (CTGF) modulates cell signalling by BMP and TGF-. Nat. Cell Biol. 4, 599–604 (2002).
33. G. Raghu, M. B. Scholand, J. de Andrade, L. Lancaster, Y. Mageto, J. Goldin, K. K. Brown, K. R. Flaherty, M. Wencel, J. Wanger, T. Neff, F. Valone, J. Stauffer, S. Porter, FG-3019 anti-connective tissue growth factor monoclonal antibody: Results of an open-label clinical trial in idiopathic pulmonary fibrosis. Eur. Respir. J. 47, 1481–1491 (2016).
34. S. G. Adler, S. Schwartz, M. E. Williams, C. Arauz-Pacheco, W. K. Bolton, T. Lee, D. Li, T. B. Neff, P. R. Urquilla, K. L. Sewell, Phase 1 study of anti-CTGF monoclonal antibody in patients with diabetes and microalbuminuria. Clin. J. Am. Soc. Nephrol. 5, 1420–1428 (2010).
35. R. J. Akhurst, A. Hata, Targeting the TGF signalling pathway in disease. Nat. Rev. Drug Discov. 11, 790–811 (2012).
36. A. S. Selvaggio, P. W. Noble, Pirfenidone initiates a new era in the treatment of idiopathic pulmonary fibrosis. Annu. Rev. Med. 67, 487–495 (2016).
37. J. C. Morris, A. R. Tan, T. E. Olencki, G. I. Shapiro, B. J. Dezube, M. Reiss, F. J. Hsu, J. A. Berzofsky, D. P. Lawrence, Phase I study of GC1008 (fresolimumab): A human anti-transforming growth factor-beta (TGF) monoclonal antibody in patients with advanced malignant melanoma or renal cell carcinoma. PLOS ONE 9, e90353 (2014).
38. C.-H. Heldin, Targeting the PDGF signaling pathway in the treatment of non-malignant diseases. J. Neuroimmune Pharmacol. 9, 69–79 (2014).
39. D. Schuppan, Y. O. Kim, Evolving therapies for liver fibrosis. J. Clin. Invest. 123, 1887–1901 (2013).
40. P. L. McCormack, Nintedanib: First global approval. Drugs 75, 129–139 (2015). 41. J. Barman, Targeting cancer cells using aptamers: Cell-SELEX approach and recent
advancements. RSC Adv. 5, 11724–11732 (2015). 42. E. W. M. Ng, D. T. Shima, P. Calias, E. T. Cunningham Jr., D. R. Guyer, A. P. Adamis,
Pegaptanib, a targeted anti-VEGF aptamer for ocular vascular disease. Nat. Rev. Drug Discov. 5, 123–132 (2006).
43. L. Santhanam, E. C. Tuday, A. K. Webb, P. Dowzicky, J. H. Kim, Y. J. Oh, G. Sikka, M. Kuo, M. K. Halushka, A. M. Macgregor, J. Dunn, S. Gutbrod, D. Yin, A. Shoukas, D. Nyhan, N. A. Flavahan, A. M. Belkin, D. E. Berkowitz, Decreased S-nitrosylation of tissue transglutaminase contributes to age-related increases in vascular stiffness. Circ. Res. 107, 117–125 (2010).
44. N. Agnihotri, K. Mehta, Transglutaminase-2: Evolution from pedestrian protein to a promising therapeutic target. Amino Acids 49, 425–439 (2017).
45. S. R. Caliari, M. Perepelyuk, E. M. Soulas, G. Y. Lee, R. G. Wells, J. A. Burdick, Gradually softening hydrogels for modeling hepatic stellate cell behavior during fibrosis regression. Integr. Biol. 8, 720–728 (2016).
46. A. Nenna, C. Spadaccio, M. Lusini, L. Ulianich, M. Chello, F. Nappi, Basic and clinical research against advanced glycation end products (AGEs): New compounds to tackle cardiovascular disease and diabetic complications. Recent Adv. Cardiovasc. Drug Discov. 10, 10–33 (2015).
47. J. V. Valencia, M. Mone, C. Koehne, J. Rediske, T. E. Hughes, Binding of receptor for advanced glycation end products (RAGE) ligands is not sufficient to induce inflammatory signals: Lack of activity of endotoxin-free albumin-derived advanced glycation end products. Diabetologia 47, 844–852 (2004).
48. S. Maeda, T. Matsui, A. Ojima, M. Suematsu, K. Kaseda, Y. Higashimoto, R. Yamakawa, S. Yamagishi, DNA aptamer raised against advanced glycation end products prevents abnormalities in electroretinograms of experimental diabetic retinopathy. Ophthalmic Res. 54, 175–180 (2015).
49. J. Uribarri, M. Peppa, W. Cai, T. Goldberg, M. Lu, C. He, H. Vlassara, Restriction of dietary glycotoxins reduces excessive advanced glycation end products in renal failure patients. J. Am. Soc. Nephrol. 14, 728–731 (2003).
50. C. Couppé, R. B. Svensson, J.-F. Grosset, V. Kovanen, R. H. Nielsen, M. R. Olsen, J. O. Larsen, S. F. E. Praet, D. Skovgaard, M. Hansen, P. Aagaard, M. Kjaer, S. P. Magnusson, Life-long endurance running is associated with reduced glycation and mechanical stress in connective tissue. Age 36, 9665 (2014).
51. H. E. Barker, T. R. Cox, J. T. Erler, The rationale for targeting the LOX family in cancer. Nat. Rev. Cancer 12, 540–552 (2012).
52. D. Kothapalli, S.-L. Liu, Y. H. Bae, J. Monslow, T. Xu, E. A. Hawthorne, F. J. Byfield, P. Castagnino, S. Rao, D. J. Rader, E. Puré, M. C. Phillips, S. Lund-Katz, P. A. Janmey,
by guest on August 8, 2019
http://stm.sciencem
ag.org/D
ownloaded from

Lampi and Reinhart-King, Sci. Transl. Med. 10, eaao0475 (2018) 3 January 2018
S C I E N C E T R A N S L A T I O N A L M E D I C I N E | R E V I E W
12 of 14
R. K. Assoian, Cardiovascular protection by ApoE and ApoE-HDL linked to suppression of ECM gene expression and arterial stiffening. Cell Rep. 2, 1259–1271 (2012).
53. F. Bordeleau, B. N. Mason, E. M. Lollis, M. Mazzola, M. R. Zanotelli, S. Somasegar, J. P. Califano, C. Montague, D. J. LaValley, J. Huynh, N. Mencia-Trinchant, Y. L. Negrón Abril, D. C. Hassane, L. J. Bonassar, J. T. Butcher, R. S. Weiss, C. A. Reinhart-King, Matrix stiffening promotes a tumor vasculature phenotype. Proc. Natl. Acad. Sci. U.S.A. 114, 492–497 (2017).
54. S. B. Liu, N. Ikenaga, Z.-W. Peng, D. Y. Sverdlov, A. Greenstein, V. Smith, D. Schuppan, Y. Popov, Lysyl oxidase activity contributes to collagen stabilization during liver fibrosis progression and limits spontaneous fibrosis reversal in mice. FASEB J. 30, 1599–1609 (2016).
55. H. R. Keiser, A. Sjoerdsma, Studies on beta-aminopropionitrile in patients with scleroderma. Clin. Pharmacol. Ther. 8, 593–602 (1967).
56. A. B. Benson III, Z. A. Wainberg, J. R. Hecht, D. Vyushkov, H. Dong, J. Bendell, F. Kudrik, A phase II randomized, double‐blind, placebo‐controlled study of simtuzumab or placebo in combination with gemcitabine for the first‐line treatment of pancreatic adenocarcinoma. Oncologist 22, 241-e15 (2017).
57. G. Raghu, K. K. Brown, H. R. Collard, V. Cottin, K. F. Gibson, R. J. Kaner, D. J. Lederer, F. J. Martinez, P. W. Noble, J. W. Song, A. U. Wells, T. P. M. Whelan, W. Wuyts, E. Moreau, S. D. Patterson, V. Smith, S. Bayly, J. W. Chien, Q. Gong, J. J. Zhang, T. G. O’Riordan, Efficacy of simtuzumab versus placebo in patients with idiopathic pulmonary fibrosis: A randomised, double-blind, controlled, phase 2 trial. Lancet Respir. Med. 5, 22–32 (2017).
58. J. R. Hecht, A. B. Benson III, D. Vyushkov, Y. Yang, J. Bendell, U. Verma, A phase II, randomized, double‐blind, placebo‐controlled study of simtuzumab in combination with FOLFIRI for the second‐line treatment of metastatic KRAS mutant colorectal adenocarcinoma. Oncol. 22, 243-e23 (2017).
59. T. R. Cox, A. Gartland, J. T. Erler, Lysyl oxidase, a targetable secreted molecule involved in cancer metastasis. Cancer Res. 76, 188–192 (2016).
60. N. Chan, A. Willis, N. Kornhauser, M. M. Ward, S. B. Lee, E. Nackos, B. R. Seo, E. Chuang, T. Cigler, A. Moore, D. Donovan, M. Vallee Cobham, V. Fitzpatrick, S. Schneider, A. Wiener, J. Guillaume-Abraham, E. Aljom, R. Zelkowitz, J. D. Warren, M. E. Lane, C. Fischbach, V. Mittal, L. Vahdat, Influencing the tumor microenvironment: A phase II study of copper depletion using tetrathiomolybdate in patients with breast cancer at high risk for recurrence and in preclinical models of lung metastases. Clin. Cancer Res. 23, 666–676 (2017).
61. J. W. Keillor, K. Y. P. Apperley, Transglutaminase inhibitors: A patent review. Expert Opin. Ther. Pat. 26, 49–63 (2016).
62. N. L. Occleston, S. O’Kane, N. Goldspink, M. W. J. Ferguson, New therapeutics for the prevention and reduction of scarring. Drug Discov. Today 13, 973–981 (2008).
63. K. C. Olsen, A. P. Epa, A. A. Kulkarni, R. M. Kottmann, C. E. McCarthy, G. V. Johnson, T. H. Thatcher, R. P. Phipps, P. J. Sime, Inhibition of transglutaminase 2, a novel target for pulmonary fibrosis, by two small electrophilic molecules. Am. J. Respir. Cell Mol. Biol. 50, 737–747 (2014).
64. N. Daneshpour, M. Griffin, R. Collighan, Y. Perrie, Targeted delivery of a novel group of site-directed transglutaminase inhibitors to the liver using liposomes: A new approach for the potential treatment of liver fibrosis. J. Drug Target. 19, 624–631 (2011).
65. M. Selman, A. Pardo, L. Barrera, A. Estrada, S. R. Watson, K. Wilson, N. Aziz, N. Kaminski, A. Zlotnik, Gene expression profiles distinguish idiopathic pulmonary fibrosis from hypersensitivity pneumonitis. Am. J. Respir. Crit. Care Med. 173, 188–198 (2006).
66. B. Fingleton, MMPs as therapeutic targets—Still a viable option? Semin. Cell Dev. Biol. 19, 61–68 (2008).
67. K. J. Isaacson, M. Martin Jensen, N. B. Subrahmanyam, H. Ghandehari, Matrix-metalloproteinases as targets for controlled delivery in cancer: An analysis of upregulation and expression. J. Control. Release 259, 62–75 (2017).
68. S. Cabrera, M. Gaxiola, J. L. Arreola, R. Ramírez, P. Jara, J. D’Armiento, T. Richards, M. Selman, A. Pardo, Overexpression of MMP9 in macrophages attenuates pulmonary fibrosis induced by bleomycin. Int. J. Biochem. Cell Biol. 39, 2324–2338 (2007).
69. Q. Yu, I. Stamenkovic, Cell surface-localized matrix metalloproteinase-9 proteolytically activates TGF- and promotes tumor invasion and angiogenesis. Genes Dev. 14, 163–176 (2000).
70. X. Zhou, F. R. Murphy, N. Gehdu, J. Zhang, J. P. Iredale, R. C. Benyon, Engagement of v3 integrin regulates proliferation and apoptosis of hepatic stellate cells. J. Biol. Chem. 279, 23996–24006 (2004).
71. A. Haage, I. C. Schneider, Cellular contractility and extracellular matrix stiffness regulate matrix metalloproteinase activity in pancreatic cancer cells. FASEB J. 28, 3589–3599 (2014).
72. R. E. Vandenbroucke, C. Libert, Is there new hope for therapeutic matrix metalloproteinase inhibition? Nat. Rev. Drug Discov. 13, 904–927 (2014).
73. U. Lendeckel, J. Kohl, M. Arndt, S. Carl-McGrath, H. Donat, C. Röcken, Increased expression of ADAM family members in human breast cancer and breast cancer cell lines. J. Cancer Res. Clin. Oncol. 131, 41–48 (2005).
74. N. Rocks, G. Paulissen, M. El Hour, F. Quesada, C. Crahay, M. Gueders, J. M. Foidart, A. Noel, D. Cataldo, Emerging roles of ADAM and ADAMTS metalloproteinases in cancer. Biochimie 90, 369–379 (2008).
75. K. Bourd-Boittin, D. Bonnier, A. Leyme, B. Mari, P. Tuffery, M. Samson, F. Ezan, G. Baffet, N. Theret, Protease profiling of liver fibrosis reveals the ADAM metallopeptidase with thrombospondin type 1 motif, 1 as a central activator of transforming growth factor beta. Hepatology 54, 2173–2184 (2011).
76. S. Cal, C. López-Otín, ADAMTS proteases and cancer. Matrix Biol. 44–46, 77–85 (2015). 77. S. Friedman, R. Levy, W. Garrett, D. Doval, S. Bondarde, T. Sahoo, D. Lokanatha, P. Julka,
K. Shenoy, R. Nagarkar, G. Bhattacharyya, K. Kumar, S. Nag, P. Mohan, N. Narang, D. Raghunadharao, M. Walia, W. Yao, J. Li, T. Emm, S. Yeleswaram, P. Scherle, R. Newton, Clinical benefit of INCB7839, a potent and selective inhibitor of ADAM10 and ADAM17, in combination with trastuzumab in metastatic HER2 positive breast cancer patients. Cancer Res. 69, 5056 (2009).
78. P. D. Arora, N. Narani, C. A. McCulloch, The compliance of collagen gels regulates transforming growth factor- induction of -smooth muscle actin in fibroblasts. Am. J. Pathol. 154, 871–882 (1999).
79. P. C. Georges, J.-J. Hui, Z. Gombos, M. E. McCormick, A. Y. Wang, M. Uemura, R. Mick, P. A. Janmey, E. E. Furth, R. G. Wells, Increased stiffness of the rat liver precedes matrix deposition: Implications for fibrosis. Am. J. Physiol. Gastrointest. Liver Physiol. 293, G1147–G1154 (2007).
80. R. M. Weisbrod, T. Shiang, L. Al Sayah, J. L. Fry, S. Bajpai, C. A. Reinhart-King, H. E. Lob, L. Santhanam, G. Mitchell, R. A. Cohen, F. Seta, Arterial stiffening precedes systolic hypertension in diet-induced obesity. Hypertension 62, 1105–1110 (2013).
81. S. C. Wei, L. Fattet, J. H. Tsai, Y. Guo, V. H. Pai, H. E. Majeski, A. C. Chen, R. L. Sah, S. S. Taylor, A. J. Engler, J. Yang, Matrix stiffness drives epithelial–mesenchymal transition and tumour metastasis through a TWIST1–G3BP2 mechanotransduction pathway. Nat. Cell Biol. 17, 678–688 (2015).
82. R. A. DeFilippis, H. Chang, N. Dumont, J. T. Rabban, Y.-Y. Chen, G. V. Fontenay, H. K. Berman, M. L. Gauthier, J. Zhao, D. Hu, J. J. Marx, J. A. Tjoe, E. Ziv, M. Febbraio, K. Kerlikowske, B. Parvin, T. D. Tlsty, CD36 repression activates a multicellular stromal program shared by high mammographic density and tumor tissues. Cancer Discov. 2, 826–839 (2012).
83. L. Seguin, J. S. Desgrosellier, S. M. Weis, D. A. Cheresh, Integrins and cancer: Regulators of cancer stemness, metastasis, and drug resistance. Trends Cell Biol. 25, 234–240 (2015).
84. W. Guo, F. G. Giancotti, Integrin signalling during tumour progression. Nat. Rev. Mol. Cell Biol. 5, 816–826 (2004).
85. H. B. Schiller, M.-R. Hermann, J. Polleux, T. Vignaud, S. Zanivan, C. C. Friedel, Z. Sun, A. Raducanu, K.-E. Gottschalk, M. Théry, M. Mann, R. Fässler, 1- and v-class integrins cooperate to regulate myosin II during rigidity sensing of fibronectin-based microenvironments. Nat. Cell Biol. 15, 625–636 (2013).
86. B. D. Hoffman, C. Grashoff, M. A. Schwartz, Dynamic molecular processes mediate cellular mechanotransduction. Nature 475, 316–323 (2011).
87. V. Maruthamuthu, B. Sabass, U. S. Schwarz, M. L. Gardel, Cell-ECM traction force modulates endogenous tension at cell–cell contacts. Proc. Natl. Acad. Sci. U.S.A. 108, 4708–4713 (2011).
88. N. I. Reed, H. Jo, C. Chen, K. Tsujino, T. D. Arnold, W. F. DeGrado, D. Sheppard, The v1 integrin plays a critical in vivo role in tissue fibrosis. Sci. Transl. Med. 7, 288ra79 (2015).
89. H. V. Woodcock, T. M. Maher, The treatment of idiopathic pulmonary fibrosis. F1000Prime Rep. 6, 16 (2014).
90. R. Stupp, M. E. Hegi, T. Gorlia, S. C. Erridge, J. Perry, Y.-K. Hong, K. D. Aldape, B. Lhermitte, T. Pietsch, D. Grujicic, J. P. Steinbach, W. Wick, R. Tarnawski, D.-H. Nam, P. Hau, A. Weyerbrock, M. J. B. Taphoorn, C.-C. Shen, N. Rao, L. Thurzo, U. Herrlinger, T. Gupta, R.-D. Kortmann, K. Adamska, C. McBain, A. A. Brandes, J. C. Tonn, O. Schnell, T. Wiegel, C.-Y. Kim, L. B. Nabors, D. A. Reardon, M. J. van den Bent, C. Hicking, A. Markivskyy, M. Picard, M. Weller, Cilengitide combined with standard treatment for patients with newly diagnosed glioblastoma with methylated MGMT promoter (CENTRIC EORTC 26071-22072 study): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 15, 1100–1108 (2014).
91. N. C. Henderson, D. Sheppard, Integrin-mediated regulation of TGF in fibrosis. Biochim. Biophys. Acta 1832, 891–896 (2013).
92. M. Parri, P. Chiarugi, Rac and Rho GTPases in cancer cell motility control. Cell Commun. Signal. 8, 23 (2010).
93. C. A. Street, B. A. Bryan, Rho kinase proteins—Pleiotropic modulators of cell survival and apoptosis. Anticancer Res. 31, 3645–3657 (2011).
94. D. E. Discher, P. Janmey, Y.-L. Wang, Tissue cells feel and respond to the stiffness of their substrate. Science 310, 1139–1143 (2005).
95. G. L. Verdine, L. D. Walensky, The challenge of drugging undruggable targets in cancer: Lessons learned from targeting BCL-2 family members. Clin. Cancer Res. 13, 7264–7270 (2007).
96. H. Barth, S. Fischer, A. Möglich, C. Förtsch, Clostridial C3 Toxins target monocytes/macrophages and modulate their functions. Front. Immunol. 6, 339 (2015).
97. R. G. Hodge, A. J. Ridley, Regulating Rho GTPases and their regulators. Nat. Rev. Mol. Cell Biol. 17, 496–510 (2016).
98. C.-Y. Wang, P.-Y. Liu, J. K. Liao, Pleiotropic effects of statin therapy: Molecular mechanisms and clinical results. Trends Mol. Med. 14, 37–44 (2008).
by guest on August 8, 2019
http://stm.sciencem
ag.org/D
ownloaded from

Lampi and Reinhart-King, Sci. Transl. Med. 10, eaao0475 (2018) 3 January 2018
S C I E N C E T R A N S L A T I O N A L M E D I C I N E | R E V I E W
13 of 14
99. M. C. Lampi, C. J. Faber, J. Huynh, F. Bordeleau, M. R. Zanotelli, C. A. Reinhart-King, Simvastatin ameliorates matrix stiffness-mediated endothelial monolayer disruption. PLOS ONE 11, e0147033 (2016).
100. K. L. Watts, E. M. Sampson, G. S. Schultz, M. A. Spiteri, Simvastatin inhibits growth factor expression and modulates profibrogenic markers in lung fibroblasts. Am. J. Respir. Cell Mol. Biol. 32, 290–300 (2005).
101. S. Pisanti, P. Picardi, E. Ciaglia, A. D’Alessandro, M. Bifulco, Novel prospects of statins as therapeutic agents in cancer. Pharmacol. Res. 88, 84–98 (2014).
102. M. L. Kutys, K. M. Yamada, Rho GEFs and GAPs: Emerging integrators of extracellular matrix signaling. Small GTPases 6, 16–19 (2015).
103. X. Shang, F. Marchioni, N. Sipes, C. R. Evelyn, M. Jerabek-Willemsen, S. Duhr, W. Seibel, M. Wortman, Y. Zheng, Rational design of small molecule inhibitors targeting RhoA subfamily Rho GTPases. Chem. Biol. 19, 699–710 (2012).
104. X. Shang, F. Marchioni, C. R. Evelyn, N. Sipes, X. Zhou, W. Seibel, M. Wortman, Y. Zheng, Small-molecule inhibitors targeting G-protein–coupled Rho guanine nucleotide exchange factors. Proc. Natl. Acad. Sci. U.S.A. 110, 3155–3160 (2013).
105. F. Bai, F. Morcos, R. R. Cheng, H. Jiang, J. N. Onuchic, Elucidating the druggable interface of protein−protein interactions using fragment docking and coevolutionary analysis. Proc. Natl. Acad. Sci. U.S.A. 113, E8051–E8058 (2016).
106. C. Guilluy, V. Swaminathan, R. Garcia-Mata, E. T. O’Brien, R. Superfine, K. Burridge, The Rho GEFs LARG and GEF-H1 regulate the mechanical response to force on integrins. Nat. Cell Biol. 13, 722–727 (2011).
107. S. S. Htwe, B. H. Cha, K. Yue, A. Khademhosseini, A. J. Knox, A. M. Ghaemmaghami, Role of Rho-associated coiled-coil forming kinase isoforms in regulation of stiffness-induced myofibroblast differentiation in lung fibrosis. Am. J. Respir. Cell Mol. Biol. 56, 772–783 (2017).
108. J. Huynh, N. Nishimura, K. Rana, J. M. Peloquin, J. P. Califano, C. R. Montague, M. R. King, C. B. Schaffer, C. A. Reinhart-King, Age-related intimal stiffening enhances endothelial permeability and leukocyte transmigration. Sci. Transl. Med. 3, 112ra122 (2011).
109. C. Hahmann, T. Schroeter, Rho-kinase inhibitors as therapeutics: From pan inhibition to isoform selectivity. Cell. Mol. Life Sci. 67, 171–177 (2010).
110. C. Vennin, V. T. Chin, S. C. Warren, M. C. Lucas, D. Herrmann, A. Magenau, P. Melenec, S. N. Walters, G. del Monte-Nieto, J. R. W. Conway, M. Nobis, A. H. Allam, R. A. McCloy, N. Currey, M. Pinese, A. Boulghourjian, A. Zaratzian, A. A. S. Adam, C. Heu, A. M. Nagrial, A. Chou, A. Steinmann, A. Drury, D. Froio, M. Giry-Laterriere, N. L. E. Harris, T. Phan, R. Jain, W. Weninger, E. J. McGhee, R. Whan, A. L. Johns, J. S. Samra, L. Chantrill, A. J. Gill, M. Kohonen-Corish, R. P. Harvey, A. V. Biankin; Australian Pancreatic Cancer Genome Initiative (APGI), T. R. J. Evans, K. I. Anderson, S. T. Grey, C. J. Ormandy, D. Gallego-Ortega, Y. Wang, M. S. Samuel, O. J. Sansom, A. Burgess, T. R. Cox, J. P. Morton, M. Pajic, P. Timpson, Transient tissue priming via ROCK inhibition uncouples pancreatic cancer progression, sensitivity to chemotherapy, and metastasis. Sci. Transl. Med. 9, eaai8504 (2017).
111. S. K. Wang, R. T. Chang, An emerging treatment option for glaucoma: Rho kinase inhibitors. Clin. Ophthalmol. 8, 883–890 (2014).
112. S. Boland, O. Defert, J. Alen, A. Bourin, K. Castermans, N. Kindt, N. Boumans, L. Panitti, S. Van de Velde, I. Stalmans, D. Leysen, 3-[2-(Aminomethyl)-5-[(pyridin-4-yl)carbamoyl]phenyl] benzoates as soft ROCK inhibitors. Bioorg. Med. Chem. Lett. 23, 6442–6446 (2013).
113. J. Shi, L. Wei, Rho kinases in cardiovascular physiology and pathophysiology: The effect of fasudil. J. Cardiovasc. Pharmacol. 62, 341–354 (2013).
114. F. J. Sulzmaier, C. Jean, D. D. Schlaepfer, FAK in cancer: Mechanistic findings and clinical applications. Nat. Rev. Cancer 14, 598–610 (2014).
115. P. P. Provenzano, D. R. Inman, K. W. Eliceiri, P. J. Keely, Matrix density-induced mechanoregulation of breast cell phenotype, signaling and gene expression through a FAK–ERK linkage. Oncogene 28, 4326–4343 (2009).
116. M. J. Paszek, N. Zahir, K. R. Johnson, J. N. Lakins, G. I. Rozenberg, A. Gefen, C. A. Reinhart-King, S. S. Margulies, M. Dembo, D. Boettiger, D. A. Hammer, V. M. Weaver, Tensional homeostasis and the malignant phenotype. Cancer Cell 8, 241–254 (2005).
117. V. M. Golubovskaya, Targeting FAK in human cancer: From finding to first clinical trials. Front. Biosci. 19, 687–706 (2014).
118. B. Y. Lee, P. Timpson, L. G. Horvath, R. J. Daly, FAK signaling in human cancer as a target for therapeutics. Pharmacol. Ther. 146, 132–149 (2015).
119. Y. Mimura, H. Ihn, M. Jinnin, Y. Asano, K. Yamane, K. Tamaki, Constitutive phosphorylation of focal adhesion kinase is involved in the myofibroblast differentiation of scleroderma fibroblasts. J. Invest. Dermatol. 124, 886–892 (2005).
120. D. K. Treiber, N. P. Shah, Ins and outs of kinase DFG motifs. Chem. Biol. 20, 745–746 (2013).
121. D. Lietha, M. J. Eck, Crystal structures of the FAK kinase in complex with TAE226 and related bis-anilino pyrimidine inhibitors reveal a helical DFG conformation. PLOS ONE 3, e3800 (2008).
122. V. M. Golubovskaya, S. Figel, B. T. Ho, C. P. Johnson, M. Yemma, G. Huang, M. Zheng, C. Nyberg, A. Magis, D. A. Ostrov, I. H. Gelman, W. G. Cance, A small molecule focal
adhesion kinase (FAK) inhibitor, targeting Y397 site: 1-(2-Hydroxyethyl)-3,5,7-triaza-1-azoniatricyclo [3.3.1.13,7]decane; bromide effectively inhibits FAK autophosphorylation activity and decreases cancer cell viability, clonogenicity and tumor growth in vivo. Carcinogenesis 33, 1004–1013 (2012).
123. S. Dupont, L. Morsut, M. Aragona, E. Enzo, S. Giulitti, M. Cordenonsi, F. Zanconato, J. Le Digabel, M. Forcato, S. Bicciato, N. Elvassore, S. Piccolo, Role of YAP/TAZ in mechanotransduction. Nature 474, 179–183 (2011).
124. F. Liu, D. Lagares, K. M. Choi, L. Stopfer, A. Marinković, V. Vrbanac, C. K. Probst, S. E. Hiemer, T. H. Sisson, J. C. Horowitz, I. O. Rosas, L. E. Fredenburgh, C. Feghali-Bostwick, X. Varelas, A. M. Tager, D. J. Tschumperlin, Mechanosignaling through YAP and TAZ drives fibroblast activation and fibrosis. Am. J. Physiol. Lung Cell. Mol. Physiol. 308, L344–L357 (2015).
125. G. Sorrentino, N. Ruggeri, V. Specchia, M. Cordenonsi, M. Mano, S. Dupont, A. Manfrin, E. Ingallina, R. Sommaggio, S. Piazza, A. Rosato, S. Piccolo, G. Del Sal, Metabolic control of YAP and TAZ by the mevalonate pathway. Nat. Cell Biol. 16, 357–366 (2014).
126. Y. Liu-Chittenden, B. Huang, J. S. Shim, Q. Chen, S.-J. Lee, R. A. Anders, J. O. Liu, D. Pan, Genetic and pharmacological disruption of the TEAD–YAP complex suppresses the oncogenic activity of YAP. Genes Dev. 26, 1300–1305 (2012).
127. S. Jiao, H. Wang, Z. Shi, A. Dong, W. Zhang, X. Song, F. He, Y. Wang, Z. Zhang, W. Wang, X. Wang, T. Guo, P. Li, Y. Zhao, H. Ji, L. Zhang, Z. Zhou, A peptide mimicking VGLL4 function acts as a YAP antagonist therapy against gastric cancer. Cancer Cell 25, 166–180 (2014).
128. I. Mannaerts, S. B. Leite, S. Verhulst, S. Claerhout, N. Eysackers, L. F. R. Thoen, A. Hoorens, H. Reynaert, G. Halder, L. A. van Grunsven, The Hippo pathway effector YAP controls mouse hepatic stellate cell activation. J. Hepatol. 63, 679–688 (2015).
129. L. A. Johnson, E. S. Rodansky, A. J. Haak, S. D. Larsen, R. R. Neubig, P. D. R. Higgins, Novel Rho/MRTF/SRF inhibitors block matrix-stiffness and TGF-–induced fibrogenesis in human colonic myofibroblasts. Inflamm. Bowel Dis. 20, 154–165 (2014).
130. M. A. Scharenberg, B. E. Pippenger, R. Sack, D. Zingg, J. Ferralli, S. Schenk, I. Martin, R. Chiquet-Ehrismann, TGF--induced differentiation into myofibroblasts involves specific regulation of two MKL1 isoforms. J. Cell Sci. 127, 1079–1091 (2014).
131. K. Hayashi, B. Watanabe, Y. Nakagawa, S. Minami, T. Morita, RPEL proteins are the molecular targets for CCG-1423, an inhibitor of Rho signaling. PLOS ONE 9, e89016 (2014).
132. S. Ishihara, M. Yasuda, I. Harada, T. Mizutani, K. Kawabata, H. Haga, Substrate stiffness regulates temporary NF-B activation via actomyosin contractions. Exp. Cell Res. 319, 2916–2927 (2013).
133. T. Lawrence, The nuclear factor NF-B pathway in inflammation. Cold Spring Harb. Perspect. Biol. 1, a001651 (2009).
134. J. E. Sero, H. Z. Sailem, R. C. Ardy, H. Almuttaqi, T. Zhang, C. Bakal, Cell shape and the microenvironment regulate nuclear translocation of NF-B in breast epithelial and tumor cells. Mol. Syst. Biol. 11, 790 (2015).
135. M. Aragona, T. Panciera, A. Manfrin, S. Giulitti, F. Michielin, N. Elvassore, S. Dupont, S. Piccolo, A mechanical checkpoint controls multicellular growth through YAP/TAZ regulation by actin-processing factors. Cell 154, 1047–1059 (2013).
136. T. Luedde, R. F. Schwabe, NF-B in the liver—Linking injury, fibrosis and hepatocellular carcinoma. Nat. Rev. Gastroenterol. Hepatol. 8, 108–118 (2011).
137. V. Baud, M. Karin, Is NF-B a good target for cancer therapy? Hopes and pitfalls. Nat. Rev. Drug Discov. 8, 33–40 (2009).
138. B. A. Teicher, K. C. Anderson, CCR 20th anniversary commentary: In the beginning, there was PS-341. Clin. Cancer Res. 21, 939–941 (2015).
139. B. Muz, R. N. Ghazarian, M. Ou, M. J. Luderer, H. D. Kusdono, A. K. Azab, Spotlight on ixazomib: Potential in the treatment of multiple myeloma. Drug Des. Devel. Ther. 10, 217–226 (2016).
140. P. Godwin, A. M. Baird, S. Heavey, M. P. Barr, K. J. O’Byrne, K. Gately, Targeting nuclear factor-kappa b to overcome resistance to chemotherapy. Front. Oncol. 3, 120 (2013).
141. A. Plotnikov, E. Zehorai, S. Procaccia, R. Seger, The MAPK cascades: Signaling components, nuclear roles and mechanisms of nuclear translocation. Biochim. Biophys. Acta Mol. Cell Res. 1813, 1619–1633 (2011).
142. M. Kohan, A. F. Muro, E. S. White, N. Berkman, EDA-containing cellular fibronectin induces fibroblast differentiation through binding to 47 integrin receptor and MAPK/Erk 1/2-dependent signaling. FASEB J. 24, 4503–4512 (2010).
143. G. A. Secker, A. J. Shortt, E. Sampson, Q. P. Schwarz, G. S. Schultz, J. T. Daniels, TGF stimulated re-epithelialisation is regulated by CTGF and Ras/MEK/ERK signalling. Exp. Cell Res. 314, 131–142 (2008).
144. J.-H. Hwang, M. R. Byun, A. R. Kim, K. M. Kim, H. J. Cho, Y. H. Lee, J. Kim, M. G. Jeong, E. S. Hwang, J.-H. Hong, Extracellular matrix stiffness regulates osteogenic differentiation through MAPK activation. PLOS ONE 10, e0135519 (2015).
145. A. A. Samatar, P. I. Poulikakos, Targeting RAS–ERK signalling in cancer: Promises and challenges. Nat. Rev. Drug Discov. 13, 928–942 (2014).
146. R. M. Webster, Combination therapies in oncology. Nat. Rev. Drug Discov. 15, 81–82 (2016).
by guest on August 8, 2019
http://stm.sciencem
ag.org/D
ownloaded from

Lampi and Reinhart-King, Sci. Transl. Med. 10, eaao0475 (2018) 3 January 2018
S C I E N C E T R A N S L A T I O N A L M E D I C I N E | R E V I E W
14 of 14
147. F. Bordeleau, J. P. Califano, Y. L. Negrón Abril, B. N. Mason, D. J. LaValley, S. J. Shin, R. S. Weiss, C. A. Reinhart-King, Tissue stiffness regulates serine/arginine-rich protein-mediated splicing of the extra domain B-fibronectin isoform in tumors. Proc. Natl. Acad. Sci. U.S.A. 112, 8314–8319 (2015).
148. E. Balza, L. Borsi, G. Allemanni, L. Zardi, Transforming growth factor regulates the levels of different fibronectin isoforms in normal human cultured fibroblasts. FEBS Lett. 228, 42–44 (1988).
149. K.-q. Le, B. S. Prabhakar, W.-j. Hong, L.-c. Li, Alternative splicing as a biomarker and potential target for drug discovery. Acta Pharmacol. Sin. 36, 1212–1218 (2015).
150. N. Wang, J. D. Tytell, D. E. Ingber, Mechanotransduction at a distance: Mechanically coupling the extracellular matrix with the nucleus. Nat. Rev. Mol. Cell Biol. 10, 75–82 (2009).
151. G. R. Fedorchak, A. Kaminski, J. Lammerding, Cellular mechanosensing: Getting to the nucleus of it all. Prog. Biophys. Mol. Biol. 115, 76–92 (2014).
152. J. Swift, I. L. Ivanovska, A. Buxboim, T. Harada, P. C. D. P. Dingal, J. Pinter, J. D. Pajerowski, K. R. Spinler, J.-W. Shin, M. Tewari, F. Rehfeldt, D. W. Speicher, D. E. Discher, Nuclear lamin-A scales with tissue stiffness and enhances matrix-directed differentiation. Science 341, 1240104 (2013).
153. A. T. Bertrand, S. Ziaei, C. Ehret, H. Duchemin, K. Mamchaoui, A. Bigot, M. Mayer, S. Quijano-Roy, I. Desguerre, J. Lainé, R. Ben Yaou, G. Bonne, C. Coirault, Cellular microenvironments reveal defective mechanosensing responses and elevated YAP signaling in LMNA-mutated muscle precursors. J. Cell Sci. 127, 2873–2884 (2014).
Funding: The authors acknowledge support from the NSF (award number 1435755) to C.A.R.-K. and the NIH (award number HL 127499) to C.A.R.-K. We also acknowledge support from a NSF Graduate Research Fellowship (award number 2013155462), a Cornell Sloan Foundation Fellowship, and a Ford Foundation Fellowship awarded to M.C.L. Competing interests: The authors declare that they have no competing interests.
Submitted 12 June 2017Accepted 8 December 2017Published 3 January 201810.1126/scitranslmed.aao0475
Citation: M. C. Lampi, C. A. Reinhart-King, Targeting extracellular matrix stiffness to attenuate disease: From molecular mechanisms to clinical trials. Sci. Transl. Med. 10, eaao0475 (2018).
by guest on August 8, 2019
http://stm.sciencem
ag.org/D
ownloaded from

mechanisms to clinical trialsTargeting extracellular matrix stiffness to attenuate disease: From molecular
Marsha C. Lampi and Cynthia A. Reinhart-King
DOI: 10.1126/scitranslmed.aao0475, eaao0475.10Sci Transl Med
ARTICLE TOOLS http://stm.sciencemag.org/content/10/422/eaao0475
CONTENTRELATED
http://stm.sciencemag.org/content/scitransmed/11/501/eaau2814.fullhttp://stm.sciencemag.org/content/scitransmed/10/464/eaat3487.fullhttp://stm.sciencemag.org/content/scitransmed/10/462/eaat2039.fullhttp://stm.sciencemag.org/content/scitransmed/10/454/eaan1230.fullhttp://stm.sciencemag.org/content/scitransmed/10/453/eaaq0997.fullhttp://stke.sciencemag.org/content/sigtrans/11/532/eaar2566.fullhttp://stm.sciencemag.org/content/scitransmed/4/160/160ps24.fullhttp://stm.sciencemag.org/content/scitransmed/7/301/301ra130.fullhttp://stm.sciencemag.org/content/scitransmed/9/384/eaai8504.fullhttp://stm.sciencemag.org/content/scitransmed/3/112/112ra122.fullhttp://stm.sciencemag.org/content/scitransmed/7/288/288ra79.fullhttp://stm.sciencemag.org/content/scitransmed/9/400/eaan2966.full
REFERENCES
http://stm.sciencemag.org/content/10/422/eaao0475#BIBLThis article cites 153 articles, 31 of which you can access for free
PERMISSIONS http://www.sciencemag.org/help/reprints-and-permissions
Terms of ServiceUse of this article is subject to the
is a registered trademark of AAAS.Science Translational Medicinetitle licensee American Association for the Advancement of Science. No claim to original U.S. Government Works. TheScience, 1200 New York Avenue NW, Washington, DC 20005. 2017 © The Authors, some rights reserved; exclusive
(ISSN 1946-6242) is published by the American Association for the Advancement ofScience Translational Medicine
by guest on August 8, 2019
http://stm.sciencem
ag.org/D
ownloaded from