Embed Size (px)
Citation preview
Massive Transfusion and
Massive Transfusion Protocols
Robert T. Russell, MD, MPH
November 2019
Pediatric Trauma Society
Massive Transfusion and
Massive Transfusion Protocols
No Disclosures
Objectives
• Review data associated with massive transfusion in adults and children
• Defining Massive Transfusion
• Predictors for activation
• Outcomes from utilization
• MTP creation
• Resources
• Monitoring response
• Use of simulation
Damage Control Resuscitation
Hemorrhage control
Permissive hypotension
Hemostatic resuscitation
The “Old” Approach
20 mL/kg isotonic crystalloid
Reassess
20 mL/kg isotonic crystalloid
Reassess
20 mL/kg isotonic crystalloidconsider 10-20 mL/kg packed red cells
Crystalloid Based“Resuscitation”
• Dilutional coagulopathy
• Excessive third spacing
• Abdominal compartment syndrome
• Pulmonary edema
• Cerebral edema
• Ileus
• Hypothermia
• Acidosis (hyperchloremia)
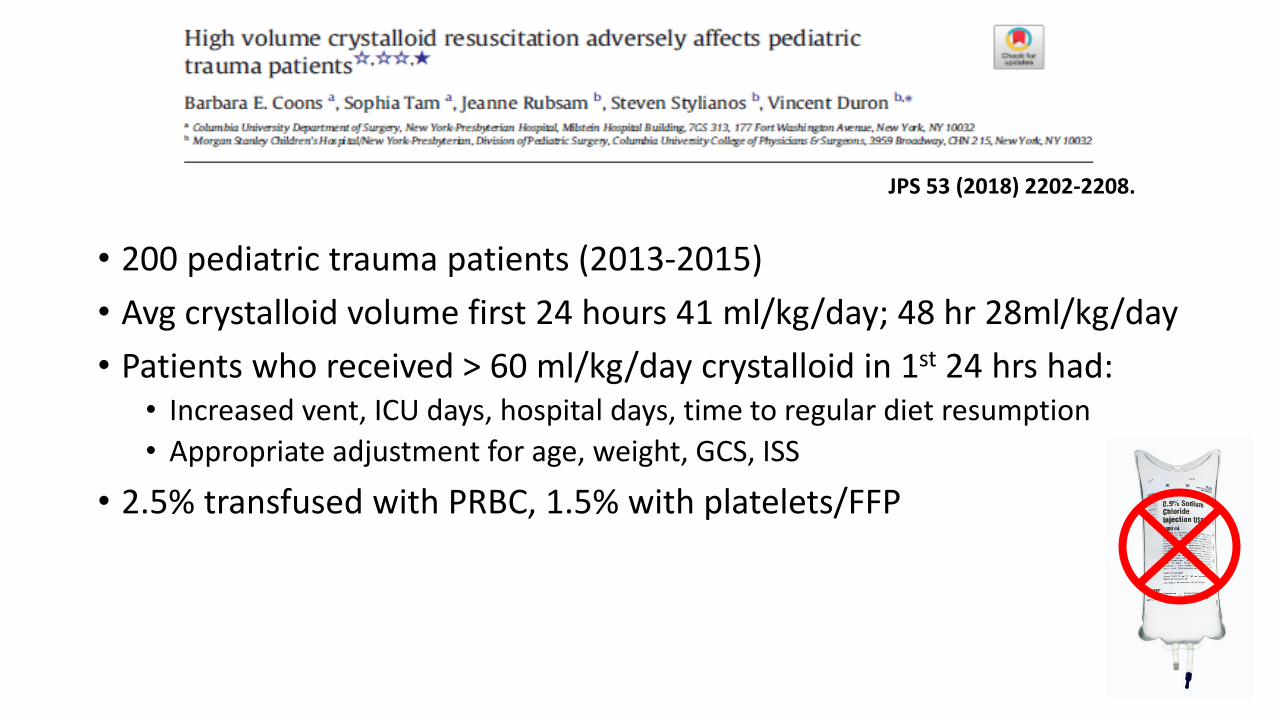
• 200 pediatric trauma patients (2013-2015)
• Avg crystalloid volume first 24 hours 41 ml/kg/day; 48 hr 28ml/kg/day
• Patients who received > 60 ml/kg/day crystalloid in 1st 24 hrs had: • Increased vent, ICU days, hospital days, time to regular diet resumption
• Appropriate adjustment for age, weight, GCS, ISS
• 2.5% transfused with PRBC, 1.5% with platelets/FFP
JPS 53 (2018) 2202-2208.
Massive Transfusion Protocols
• Provide large amounts of blood products to critically injured patients in an immediate and sustained manner
• Predefined ratios of platelets, plasma and RBCs

Defining Massive Transfusion?
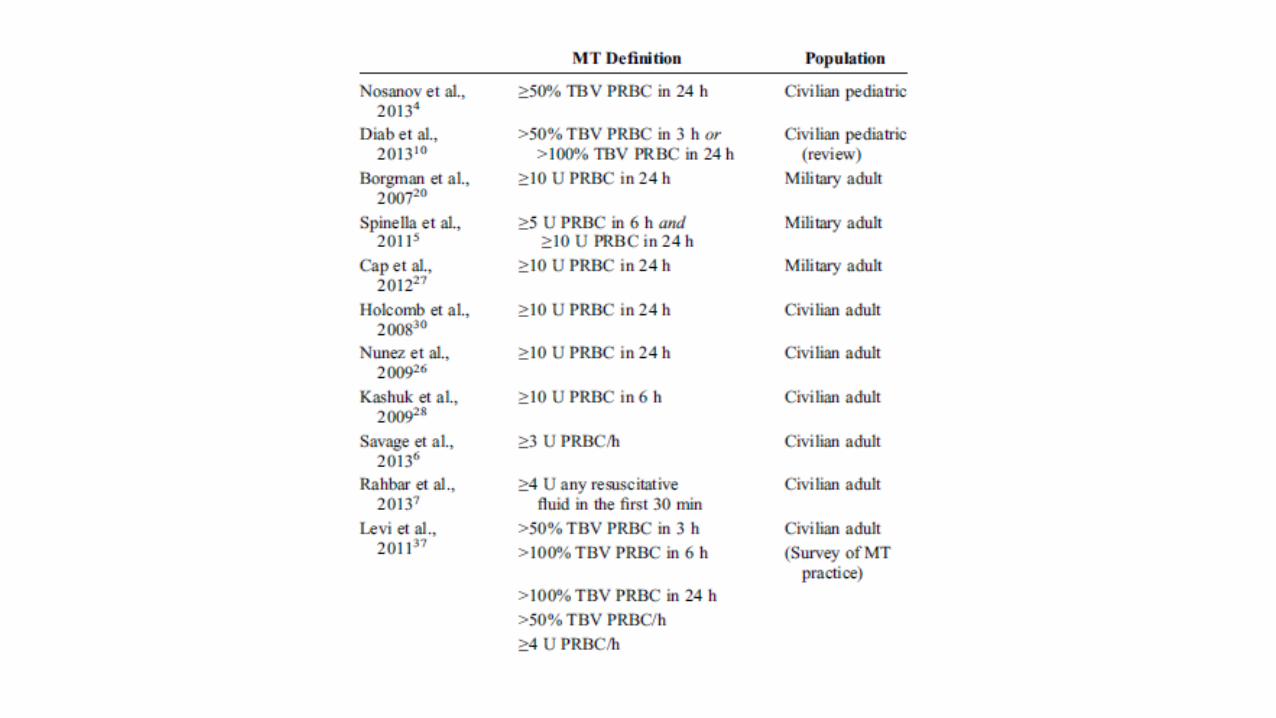
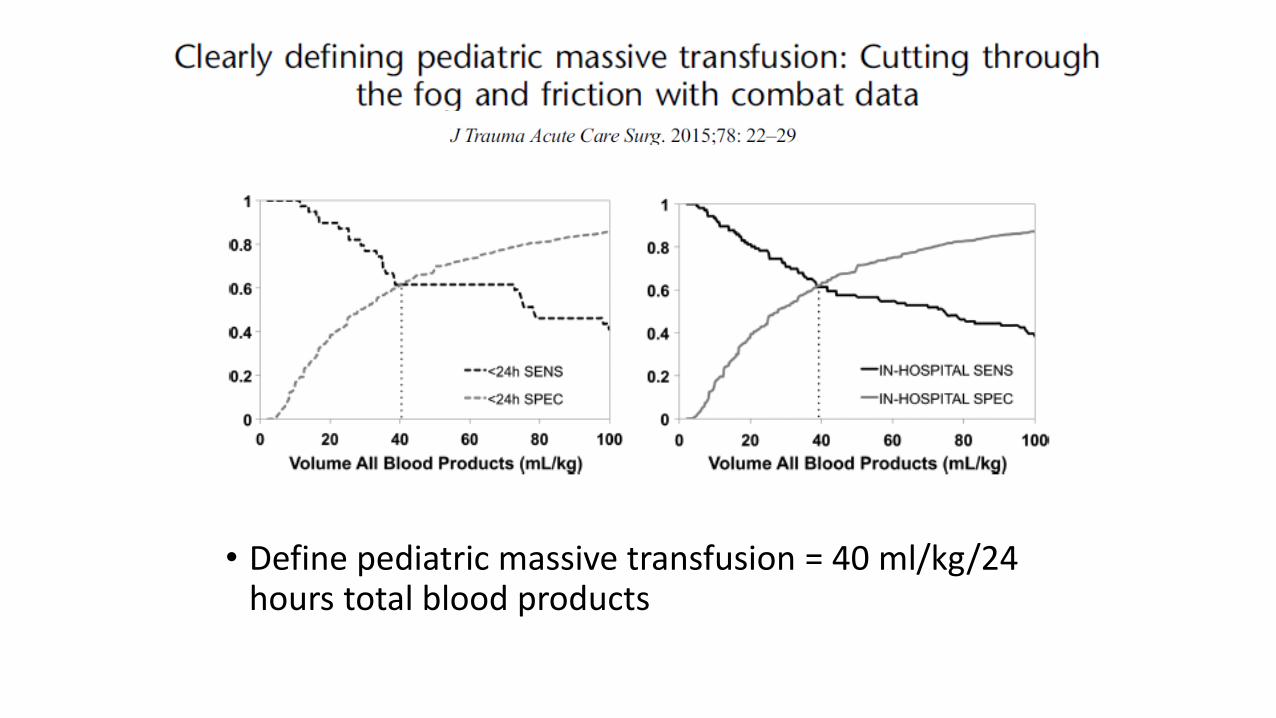
• Define pediatric massive transfusion = 40 ml/kg/24 hours total blood products
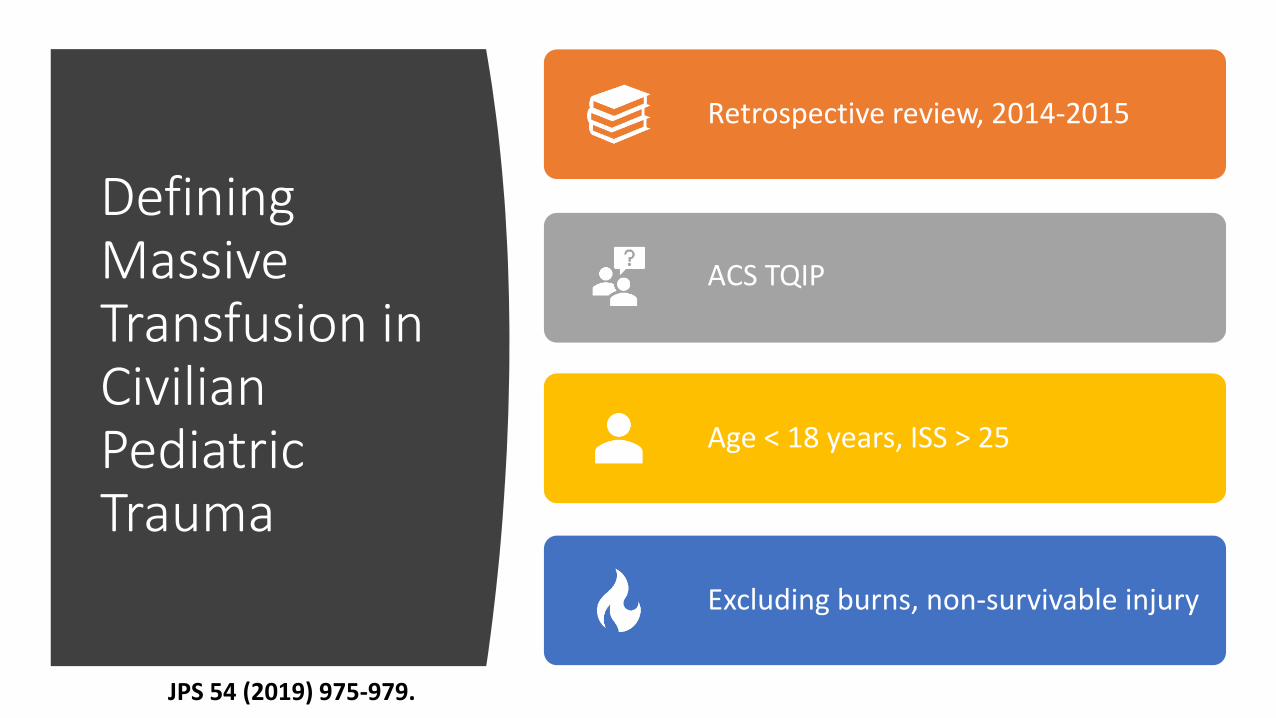
Defining Massive Transfusion in Civilian Pediatric Trauma
Retrospective review, 2014-2015
ACS TQIP
Age < 18 years, ISS > 25
Excluding burns, non-survivable injury
JPS 54 (2019) 975-979.
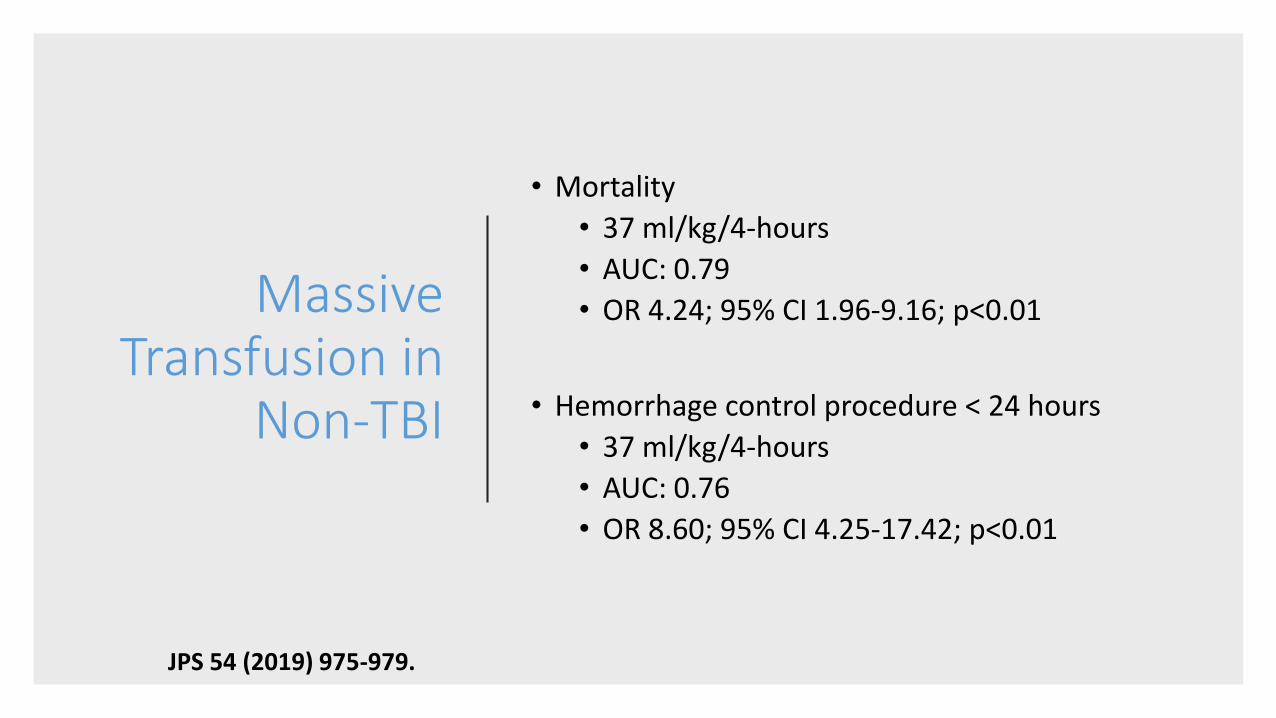
Massive Transfusion in
Non-TBI
• Mortality
• 37 ml/kg/4-hours
• AUC: 0.79
• OR 4.24; 95% CI 1.96-9.16; p<0.01
• Hemorrhage control procedure < 24 hours
• 37 ml/kg/4-hours
• AUC: 0.76
• OR 8.60; 95% CI 4.25-17.42; p<0.01
JPS 54 (2019) 975-979.
When should we activate an MTP?
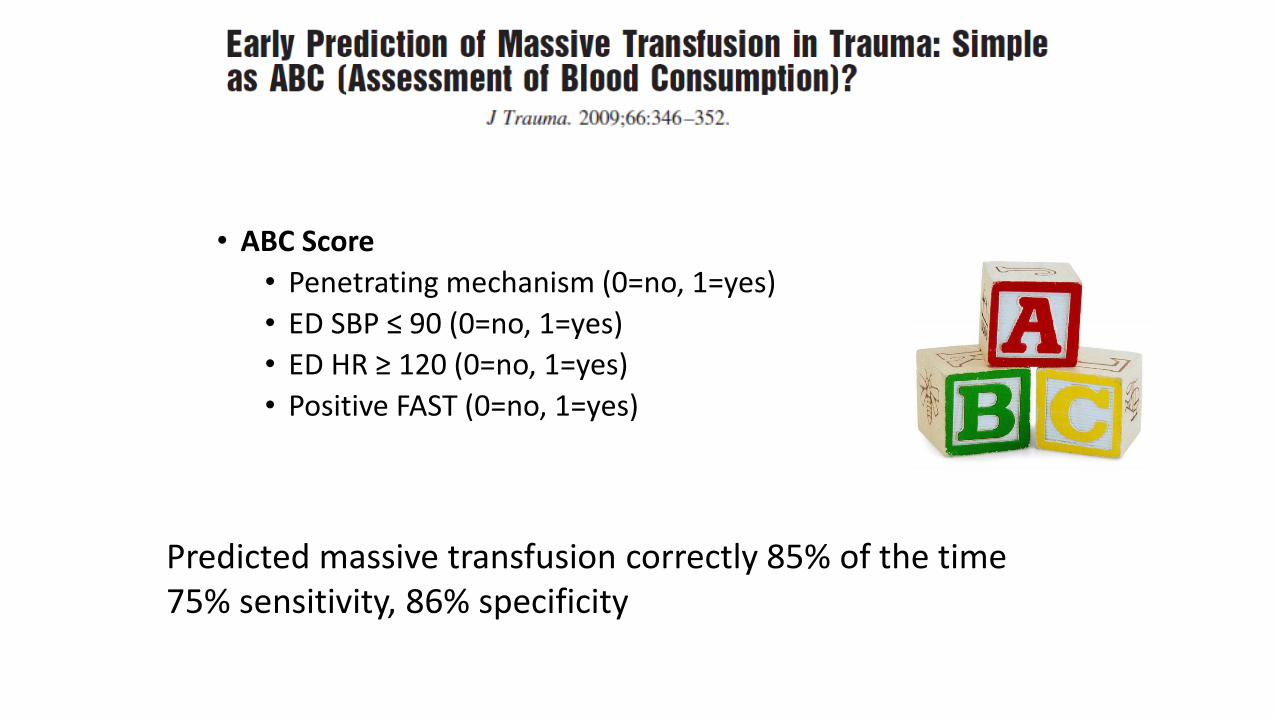
• ABC Score
• Penetrating mechanism (0=no, 1=yes)
• ED SBP ≤ 90 (0=no, 1=yes)
• ED HR ≥ 120 (0=no, 1=yes)
• Positive FAST (0=no, 1=yes)
Predicted massive transfusion correctly 85% of the time75% sensitivity, 86% specificity
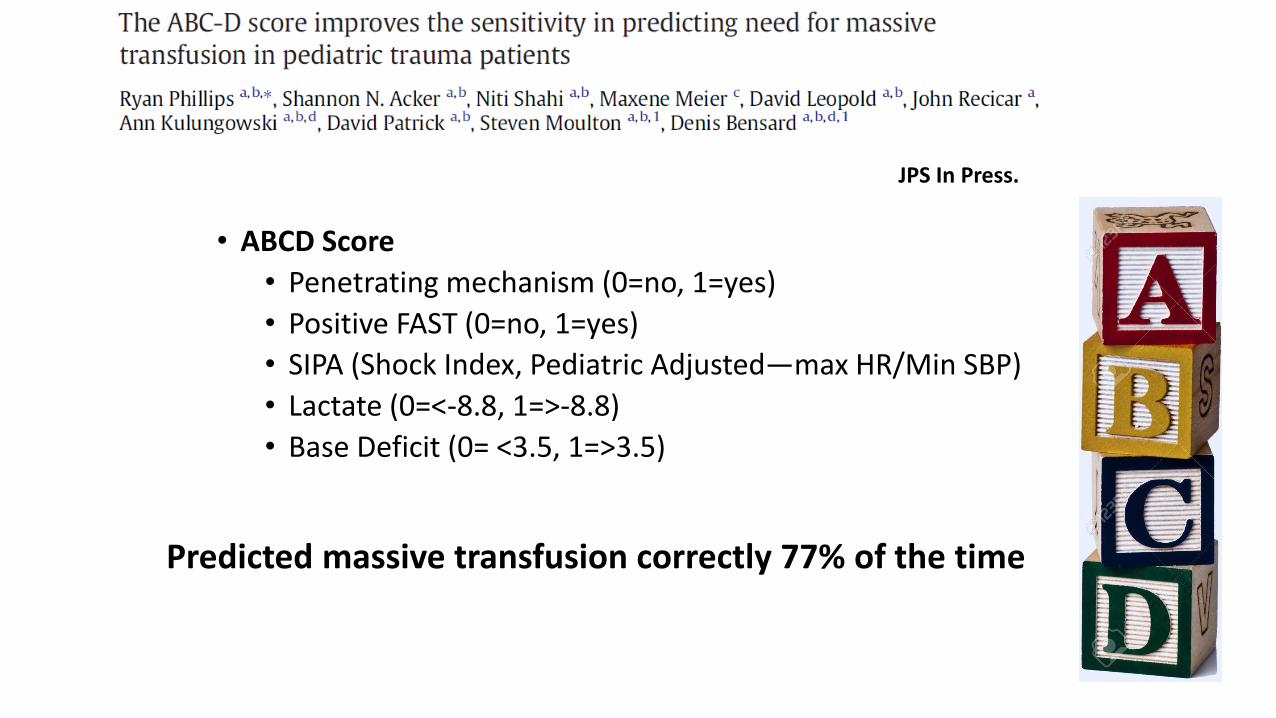
• ABCD Score
• Penetrating mechanism (0=no, 1=yes)
• Positive FAST (0=no, 1=yes)
• SIPA (Shock Index, Pediatric Adjusted—max HR/Min SBP)
• Lactate (0=<-8.8, 1=>-8.8)
• Base Deficit (0= <3.5, 1=>3.5)
JPS In Press.
Predicted massive transfusion correctly 77% of the time
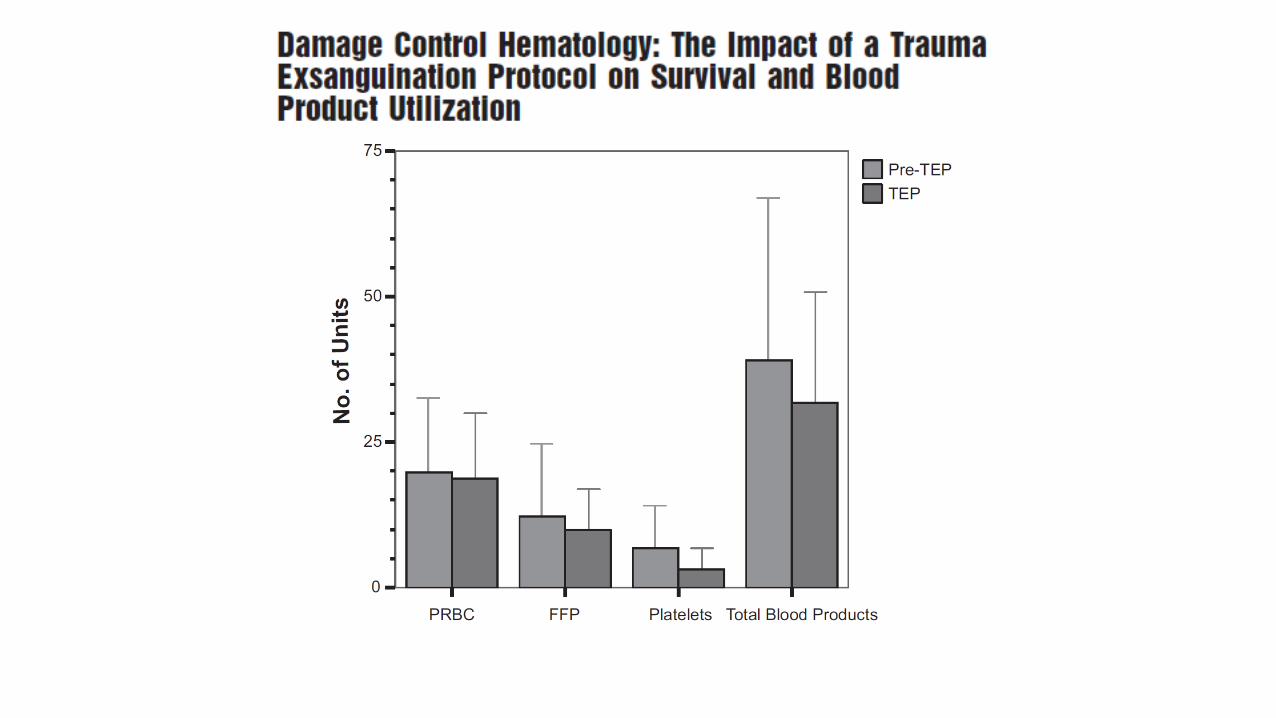
MTP in Adults
• Single center, retrospective, 2004-2006
• All TEP (MTP) activations (N=94)
• Comparison group (2004-2006) (N=117)
• No difference in age, gender, ISS
• 74% reduction in mortality in TEP/MTP group

• Pragmatic Randomized Optimal Platelet and Plasma Ratios
• 1:1:1 = 338; 1:1:2 = 342
• No difference in 24h or 30d mortality
• 1:1:1 vs. 1:1:2
• Hemostasis (86.1 vs 78.1%)
• Less death by exsanguination (9.2 vs 14.6%)Month 2016
Massive Transfusion in Children
• Single center, retrospective, 2005-2014
• ED presentation, RBC administered < 24 hours
• Pre (125) vs post (115) MTP implementation
• MT: > 40 ml/kg RBC or >80 mg/kg total blood products in 24-hours
• MT were more severely injured and coagulopathic
• No difference in mortality
• ↓ Time to plasma and platelet administration
• ↑ Plasma and PLT:RBC ratios
Month 2016
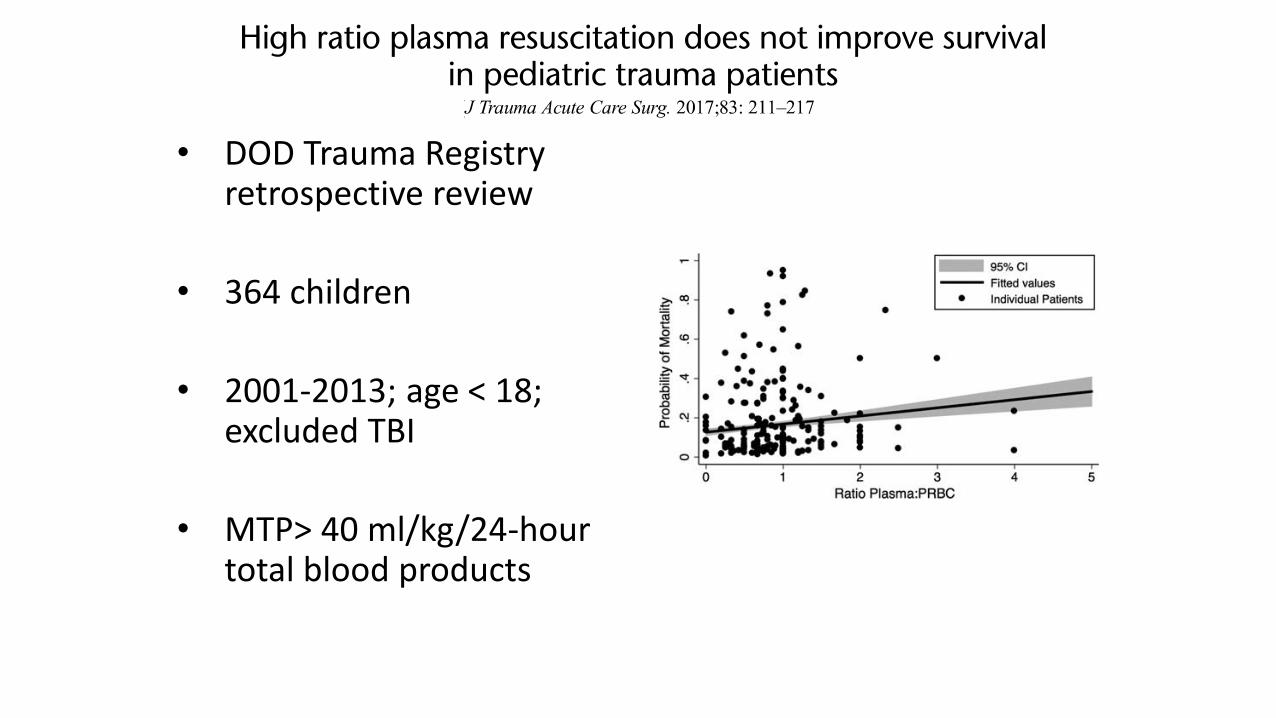
• DOD Trauma Registry retrospective review
• 364 children
• 2001-2013; age < 18; excluded TBI
• MTP> 40 ml/kg/24-hour total blood products
Month 2016
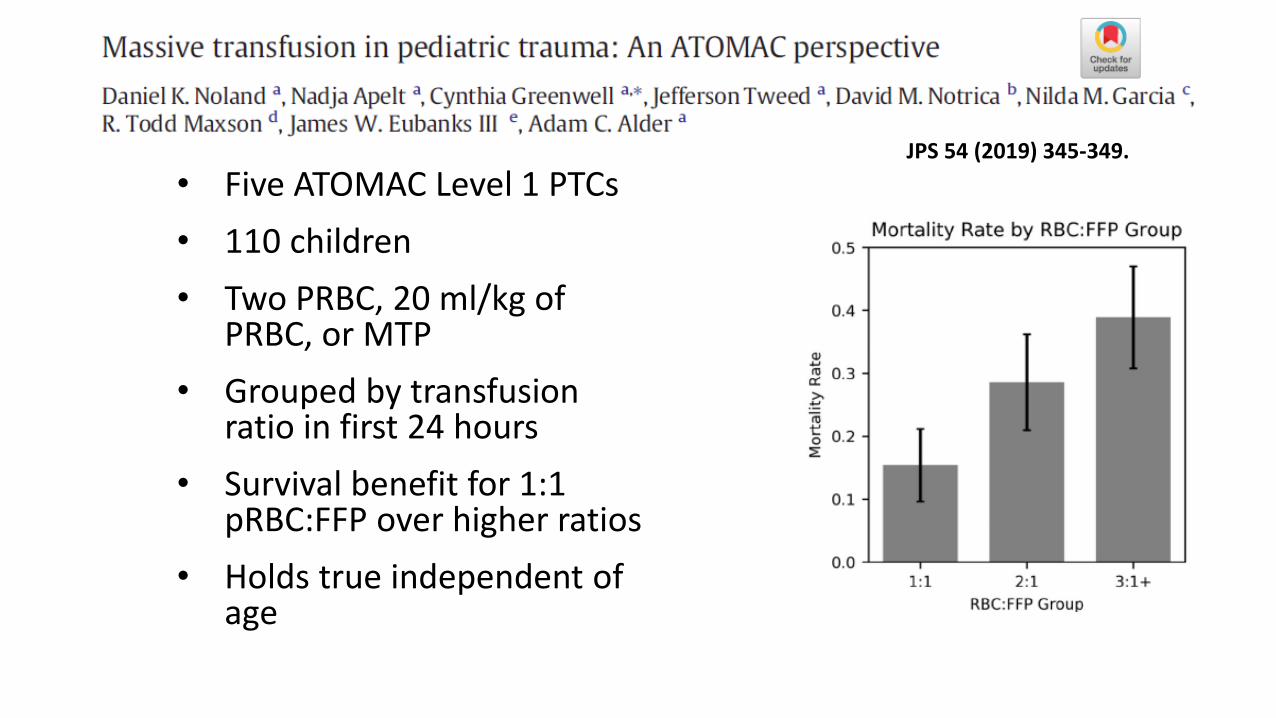
• Five ATOMAC Level 1 PTCs
• 110 children
• Two PRBC, 20 ml/kg of PRBC, or MTP
• Grouped by transfusion ratio in first 24 hours
• Survival benefit for 1:1 pRBC:FFP over higher ratios
• Holds true independent of age
Month 2016
JPS 54 (2019) 345-349.
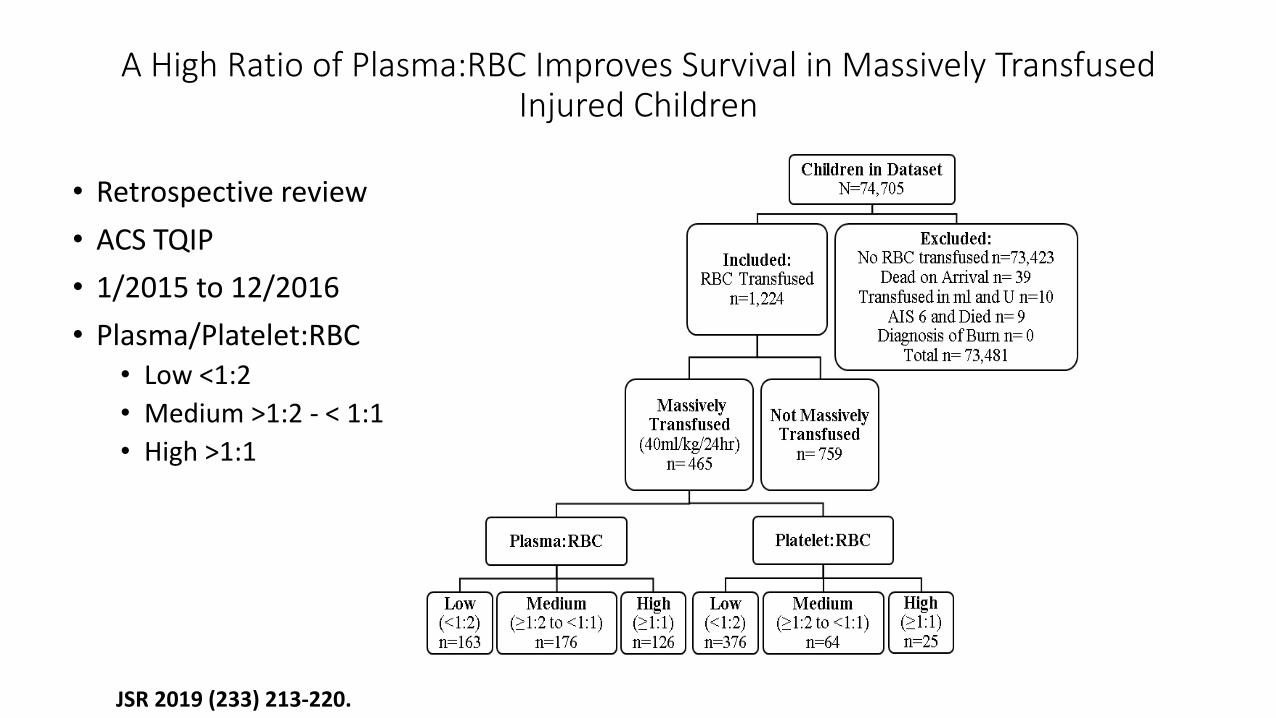
A High Ratio of Plasma:RBC Improves Survival in Massively Transfused Injured Children
• Retrospective review
• ACS TQIP
• 1/2015 to 12/2016
• Plasma/Platelet:RBC• Low <1:2
• Medium >1:2 - < 1:1
• High >1:1
JSR 2019 (233) 213-220.
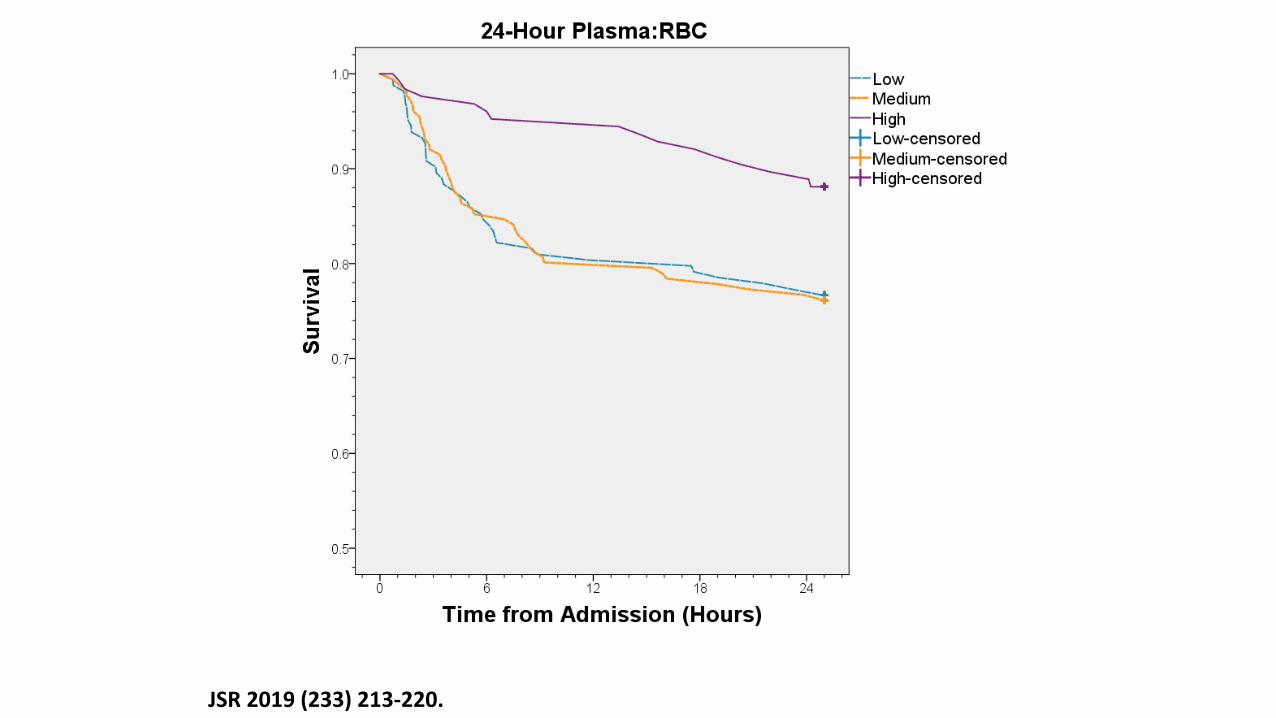
JSR 2019 (233) 213-220.
Data Conclusions
• Tough question to study in retrospective fashion, heterogeneity of populations, rarity of event
• Those receiving massive transfusion and increased product are more severely injured
• Older children get more plasma and have higher plasma:PRBC ratios
• Children that get more higher plasma:pRBCratios may have improved survival, fewer vent days, but similar ICU LOS
• Ratio of platelets:pRBCs did not seem to affect mortality, vent days or LOS
A Survey of Pediatric Massive Transfusion Protocol Polices
• 46 Children’s hospitals
• Physician discretion was the most common activation criteria (89%)
• Most sites targeted equal ratios of plasma: PRBCs; 15% of respondents used antifibrinolytics
• Wide variation in MTPs among pediatric hospitals
• Activation criteria and products administered
Transfusion Med. 2016 Feb; 26(1): 49-56.
Development of MTP at your hospital
• Consider your local environment, resources, data to inform the process
• Trauma Program
• High Risk Surgeries—trauma, craniofacial, spinal fusion
• Blood Bank—evaluate potential availability of products, supply chain
• Utilize Pediatric Trauma Society Resources
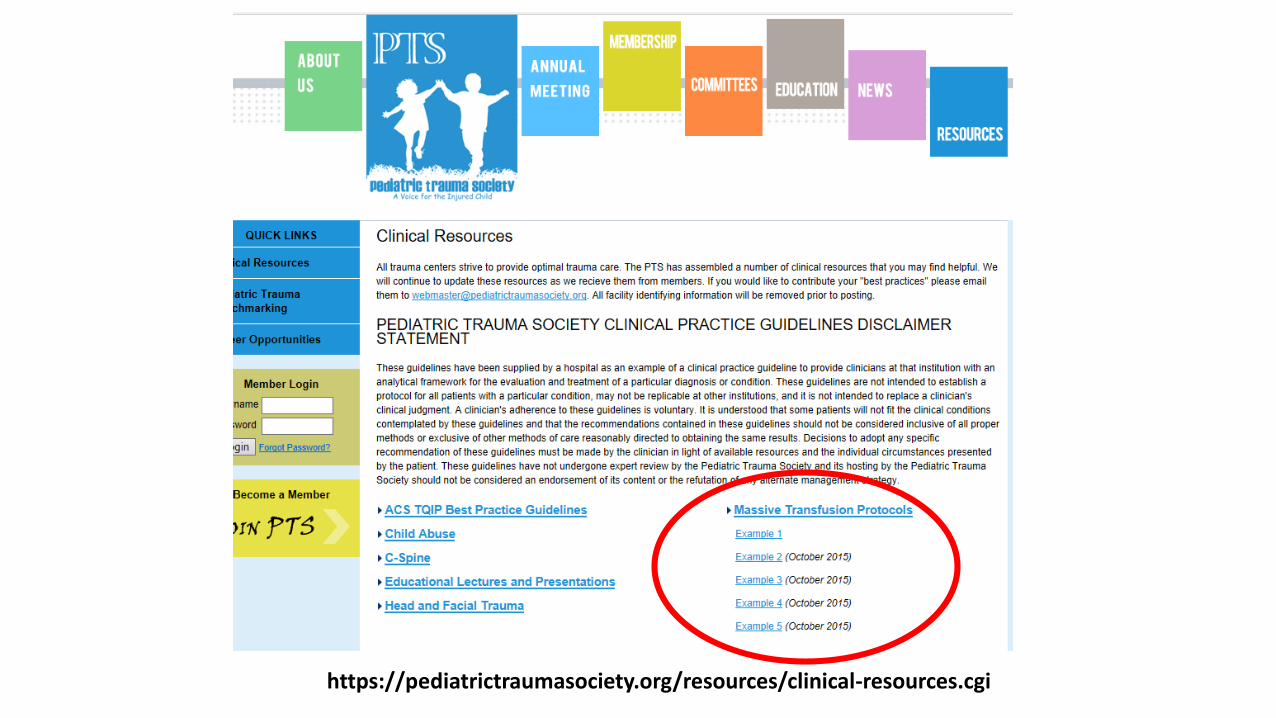
https://pediatrictraumasociety.org/resources/clinical-resources.cgi
Who should be engaged in the process?
Surgery/Trauma
Emergency Medicine/NICU/PICU
Blood Bank
Anesthesia
Nursing
Transport Services
Communications
Conclusions
Highlighted data surrounding
• Pediatric MTP definition
• MTP activation triggers
• Outcomes of MTP in children
Creation and implementation of MTP





























