MASSIVE PLEURAL EFFUSION
MASSIVE PLEURAL EFFUSION12ModuleYear 4 (MBS 362)TitleManagement
of Massive Pleural Effusions LecturerDr. Hla MyintAims and
ObjectivesAimsManagement based on when to suspectObjectivesKnow the
common causes of pleural effusionKnow the difference between
transudative and exudative pleural effusionShould know the
principles in the management of unilateral pleural effusion (BTS
2010)Expected to know the clinical manifestations and management of
massive pleural effusionAssumed KnowledgeThe concept of physiology,
pathology and radiology in accordance with the knowledge obtained
from BCS module in Phase I B/ 2nd yearLecture ContentsApproach to a
patient with (massive) pleural effusionManagementClinical
RelevanceFor practical approach and management of patients with
massive pleural effusionReferencesHarrisons principle of Internal
Medicine, 18th EditionInvestigation of A Unilateral Pleural
Effusionin Adults (BTS 2010)Seminar OutlineOBJECTIVESKnow the
common causes of pleural effusionKnow the difference between
transudative and exudative pleural effusionShould know the
principles in the management of unilateral pleural effusion (BTS
2010)Expected to know the clinical manifestations and management of
massive pleural effusion
3Differential Diagnoses of Pleural Effusions HARRISON 18 Ed
Transudative PleuralEffusions1. Congestive heart failure2.
Cirrhosis3. Pulmonary embolization4. Nephrotic syndrome5.
Peritoneal dialysis6. Superior vena cava obstruction7. Myxedema8.
Urinothorax41. Neoplastic diseasesa. Metastatic diseaseb.
Mesothelioma2. Infectious diseasesa. Bacterial infectionsb.
Tuberculosisc. Fungal infectionsd. Viral infectionse. Parasitic
infections3. Pulmonary embolization4. Gastrointestinal diseasea.
Esophageal perforationb. Pancreatic diseasec. Intraabdominal
abscessesd. Diaphragmatic herniae. After abdominal surgeryf.
Endoscopic variceal sclerotherapyg. After liver
transplantDifferential Diagnoses of Pleural EffusionsExudative
Pleural Effusions55. Collagen vascular diseases7. Asbestos
exposurea. Rheumatoid pleuritis8. Sarcoidosisb. Systemic lupus
erythematosus9. Uremiac. Drug-induced lupus10. Meigs' syndromed.
Immunoblastic lymphadenopathy11. Yellow nail syndromee. Sjgren's
syndrome12. Drug-induced pleural diseasef. Granulomatosis with
polyangiitis (Wegener's)a. Nitrofurantoing. Churg-Strauss syndrome
b. Dantrolene6. Post-coronary artery bypass surgeryc.
Methysergided. Bromocriptinee. Procarbazinef. Amiodaroneg.
DasatinibDifferential Diagnoses of Pleural EffusionsExudative
Pleural Effusions613. Trapped lung14. Radiation therapy15.
Post-cardiac injury syndrome16. Hemothorax17. Iatrogenic injury18.
Ovarian hyperstimulation syndrome19. Pericardial disease20.
Chylothorax Differential Diagnoses of Pleural EffusionsExudative
Pleural Effusions7
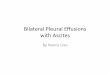
Approach to the diagnosis of pleural effusions. CHF, congestive
heart failure; CT, computed tomography; LDH, lactate dehydrogenase;
PE, pulmonary embolism; TB, tuberculosis; PF, pleural
fluid.HARRISON 18 Ed89
10
11
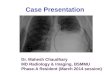
A pleural effusion (arrow) seen on chest computed tomography.
INVESTIGATION OF A UNILATERAL PLEURAL EFFUSIONIN ADULTS (BTS
2010)Clinical assessment and history Aspiration should not be
performed for bilateral effusions in a clinical setting strongly
suggestive of a transudate unless there are atypical features or
they fail to respond to therapy. An accurate drug history should be
taken during clinical assessment.
12Clinical assessment and historyInitial Diagnostic ImagingPlain
radiography Posteroanterior (PA) chest x-rays should be performed
in the assessment of suspected pleural effusion.
13Clinical assessment and historyInitial Diagnostic
ImagingUltrasound Bedside ultrasound guidance significantly
increases the likelihood of successful pleural fluid aspiration and
reduces the risk of organ puncture. Ultrasound detects pleural
fluid septations with greater sensitivity than CT. 14Pleural
aspiration A diagnostic pleural fluid sample should be aspirated
with a fine bore (21G) needle and a 50ml syringe. Bedside
ultrasound guidance improves success rate and reduces complications
[including pneumothorax) and is therefore recommended for
diagnostic aspirations [B].
15Cytology Malignant effusions can be diagnosed by pleural fluid
cytology in about 60% of cases. The yield from sending more than 2
specimens (taken on different occasions) is very low and should be
avoided. Immunocytochemistry should be used to differentiate
between malignant cell types and can be very important in guiding
oncological therapy. 16Tumour markers Pleural fluid and serum
tumour markers do not currently have a role in the routine
investigation of pleural effusions. 17Invasive
investigationsPercutaneous pleural biopsy When investigating an
undiagnosed effusion where malignancy is suspected and areas of
pleural nodularity are shown on contrastenhanced CT, an
image-guided cutting needle is the percutaneous pleural biopsy
method of choice. 18Percutaneous pleural biopsy Abrams needle
biopsies are only diagnostically useful in areas with a high
incidence of TB, although thoracoscopic and image-guided cutting
needles have been shown to have higher diagnostic yield. Invasive
investigations19Thoracoscopy Thoracoscopy is the investigation of
choice in exudative pleural effusions where a diagnostic pleural
aspiration is inconclusive and malignancy is suspected. Invasive
investigations20Bronchoscopy Routine diagnostic bronchoscopy should
not be performed for undiagnosed pleural effusion. Bronchoscopy
should be considered if there is haemoptysis, or clinical or
radiographic features suggestive of bronchial obstruction.Invasive
investigations21Diagnostic algorithm for the investigation of
aunilateral pleural effusion (BTS)
22
Diagnostic algorithm for the investigation of aunilateral
pleural effusion23
Diagnostic algorithm for the investigation of aunilateral
pleural effusion24
Diagnostic algorithm for the investigation of aunilateral
pleural effusion25Parapneumonic Effusion HARRISON 18 EdThe presence
of free pleural fluid can be demonstrated with a lateral decubitus
radiograph, computed tomography (CT) of the chest, or ultrasound.
If the free fluid separates the lung from the chest wall by >10
mm, a therapeutic thoracentesis should be performed. 26Factors
indicating the likely need for a procedure more invasive than a
thoracentesis (in increasing order of importance) include the
following:Loculated pleural fluidPleural fluid pH