Embed Size (px)
Citation preview
MANAGING PATIENTS WITH HEAVILY PRETREATED METASTATIC BREAST CANCER:BALANCING EFFICACY AND SAFETY
REVIEWS
S1 Chemotherapy in patients with heavilypretreated metastatic breast cancer:overviewChristopher J. Twelves, MD, MB ChB, FRCP, RCPS, andMonica N. Fornier, MD
S5 Approved chemotherapy agents for patientswith metastatic breast cancer previouslyexposed to taxanes and anthracyclinesChristopher J. Twelves, MD, MB ChB, FRCP, RCPS, andMonica N. Fornier, MD
S13 Choosing chemotherapy for patients withmetastatic breast cancer previously exposedto taxanes and anthracyclines: other agentsChristopher J. Twelves, MD, MB ChB, FRCP, RCPS, andMonica N. Fornier, MD
S20 CME Post-Test and Evaluation
Jointly sponsored by:
‘‘No fixed algorithm exists to guidechemotherapy treatment selection inpatients with heavily-pretreatedmetastatic breast cancer. . .’’
Monica N. FornierAssistant MemberBreast Cancer Medicine ServiceMemorial Sloan-Kettering Cancer CenterAssistant ProfessorWeill Medical College of Cornell UniversityNew York Presbyterian HospitalNew York, New York
‘‘[Study] data will help guidetreatment selection, which is based onmany factors, including priortherapies, toxicities, performancestatus, and patient preference.’’
Christopher J. TwelvesProfessor of Clinical Pharmacology
and OncologyLead, Experimental Cancer Medicine CenterUniversity of Leeds & St James’s Institute
of OncologyLeeds, United Kingdom
In affiliation with:
This educational activity is supported by an educational grant from Eisai Inc.
CME-Certified Supplement to: Volume 9 ● Number 5S ● May 2012
Community Oncology Volume 9, Number 5S (pp S1–S20)May 2012

Editor-in-Chief
David H. Henry,MD, FACPPennsylvania HospitalPhiladelphia, PA
Editors
Jame Abraham, MDWest Virginia UniversityMorgantown, WV
Linda D. Bosserman,MD, FACPWilshire OncologyMedical GroupLa Verne, CA
Debra A. Patt,MD, MPHTexas Oncology CancerCenter, Austin, TX
Editorial BoardJohanna Bendell, MDSarah Cannon Research Institute, Nashville, TN
Charles L. Bennett, MD, PhD, MPPUniversity of South Carolina, Columbia, SC
Roy A. Beveridge, MDUS Oncology, Houston, TX
Ralph V. Boccia, MDGeorgetown University, Washington, DC
Matt BrowUS Oncology, Washington, DC
Michael J. Fisch, MD, MPHThe University of TexasMD Anderson Cancer Center, Houston, TX
John A. Fracchia, MDLenox Hill Hospital, New York, NY
James N. George, MDUniversity of Oklahoma Health Sciences CenterOklahoma City, OK
James Gilmore, PharmDGeorgia Cancer Specialists, Atlanta, GA
Patrick Grusenmeyer, ScDHelen F. Graham Cancer Center, Newark, DE
David M.J. Hoffman, MDTower Hematology Oncology Medical GroupBeverly Hills, CA
Jimmie Holland, MDMemorial Sloan-Kettering Cancer CenterNew York, NY
Leslie Rodgers Laufman, MDBlood and Cancer Care of Ohio, Columbus, OH
Stuart M. Lichtman, MDMemorial Sloan-Kettering Cancer Center, Commack, NY
Charles Loprinzi, MDMayo Medical School, Rochester, MN
John L. Marshall, MDLombardi Comprehensive Cancer Center, Washington, DC
Cathy Maxwell, RN, OCN, CCRCAdvanced Medical Specialties, LLC, Miami, FL
Bradley J. Monk, MD, FACOGCreighton University School of Medicine at St. Joseph’sHospital and Medical Center, Phoenix, AZ
Anne Moore, MDWeill Medical College of Cornell University, New York, NY
Deborah A. Nagle, MDBeth Israel Deaconess Medical Center, Boston, MA
Geoffrey R. Norman, PhDMcMaster University, Hamilton, Ontario, Canada
Steven O’Day, MDThe Angeles Clinic & Research Institute, Los Angeles, CA
Theodore A. Okon, MBASupportive Oncology Services, Memphis, TN
Philip A. Philip, MD, PhDBarbara Ann Karmanos Cancer Institute, Detroit, MI
Jondavid Pollock, MD, PhDSchiffler Cancer Center, Wheeling, WV
Nicholas J. Robert, MDUS Oncology, Fairfax, VA
Peter J. Rosen, MDRoy & Patricia Disney FamilyCancer Research Center, Burbank, CA
Myrna R. Rosenfeld, MD, PhDUniversity of Pennsylvania School of Medicine,Philadelphia, PA
Philip Schulman, MDMemorial Sloan-Kettering Cancer Center, Commack, NY
Lee S. Schwartzberg, MD, FACPThe West Clinic, Memphis, TN
David Streiner, PhD, CPsychUniversity of Toronto, Toronto, Ontario, Canada
Debu Tripathy, MDUniversity of Southern California/ NorrisComprehensive Cancer Center, Los Angeles, CA
Steven Tucker, MDPacific Cancer Centre, Singapore, Malaysia
May 2012VOLUME 9, NUMBER 5S
IMNG, LLC60B Columbia Road
Morristown, NJ 07960973.290.8200 tel ● 631.424.8905 fax
Alan Imhoff, President and Publisher
Mary Jo Dales, Editorial Director
Renee Matthews, Managing Editor
John J. Fried, Elizabeth Mechcatie,Matt Stenger, Contributing Writers
Virginia Ingram-Wells, Copy Editor
Yvonne Evans, Production Manager
Peter Murphy, Stuart Williams,National Accounts Managers
Devin Gregorie, National AccountsManager—Oncology Projects
Community Oncology (ISSN 1548-5315) ispublished monthly by IMNG, LLC, 60BColumbia Road, Morristown, NJ 07960.Periodicals postage paid at Morristown, NJ,and additional mailing offices.
Change of Address
Postmaster: send address changes to CommunityOncology, Circulation, IMNG, LLC, 60BColumbia Road, Morristown, NJ 07960.
Recipient: to change your address, [email protected], telephone:973.290.8253, or mail to Community Oncology,Circulation, IMNG, LLC, 60B Columbia Road,Morristown, NJ 07960.

Educational Need Breast cancer is the most commonly diag-nosed malignancy in women in the United States, and up to 30% of women diagnosed with early breast cancer will eventually devel-op advanced disease. Women with metastatic breast cancer (MBC) are increasingly likely to have been exposed to an anthracycline and a taxane in different treatment scenarios, mak-ing subsequent use of these options less likely to be effective. Thus, there is a need for effec-tive, alternative cytotoxic therapies in patients with prior exposure to anthracycline- and taxane-based therapy. This series of articles examines chemotherapy selection for women with heavily pretreated MBC through a review of the evidence for the use of FDA-approved and off-label cytotoxic agents in this setting.
Learning Objectives After completing this educational activity, par-ticipants should be able to:
heavily pretreated MBC, including sequential versus combination chemotherapy
chemotherapy agents and combinations for the treatment of patients with heavily pre-treated MBC
patients with advanced breast cancer that has progressed following treatment with taxanes and anthracyclines
Target AudienceThis activity has been developed for medical oncologists.
CME Accreditation Statement
This activity has been planned and implement-ed in accordance with the Essential Areas and Policies of the Accreditation Council for Con-tinuing Medical Education (ACCME) through the joint sponsorship of Boston University School of Medicine and Continuing Education Alliance. Boston University School of Medi-cine is accredited by the ACCME to provide continuing medical education for physicians. AMA PRA Credit DesignationBoston University School of Medicine desig-nates this enduring material for a maximum of 2.0 AMA PRA Category 1 CreditsTM. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
DisclosuresBoston University School of Medicine asks all individuals involved in the development and presentation of Continuing Medical Education (CME) activities to disclose all relationships with commercial interests. This information is disclosed to CME activity participants. Boston University School of Medicine has procedures to resolve any apparent conflicts of interest. In addition, faculty members are asked to dis-close when any discussion of unapproved use of pharmaceuticals and devices is being dis-cussed. This educational activity may contain discussion of published and/or investigational uses of agents that are not indicated by the US Food and Drug Administration.
AcknowledgmentThis educational activity is supported by an educational grant from Eisai Inc.
FacultyMonica N. Fornier, MDAssistant MemberBreast Cancer Medicine ServiceMemorial Sloan-Kettering Cancer CenterAssistant ProfessorWeill Medical College of Cornell UniversityNew York Presbyterian Hospital New York, New YorkAuthor has nothing to disclose.Author indicates that she does plan to discuss unla-beled/investigational uses of commercial products.
Christopher J. Twelves, MD, MB ChB, FRCP, RCPSProfessor of Clinical Pharmacology and OncologyLead, Experimental Cancer Medicine CenterUniversity of Leeds & St James’s Institute of OncologyLeeds, United KingdomAuthor has received grant research support from Roche. He has also been a consultant for Eisai Inc. and Roche and a speaker for Eisai Inc.Author indicates that he does plan to discuss unla-beled/investigational uses of commercial products.
Course DirectorCarol L. Rosenberg, MDAdjunct Associate Professor of Medicine and PathologyBoston University School of MedicineBoston, MassachusettsCourse director has nothing to disclose.
Planning CommitteeCarol L. Rosenberg, MD, and Ilana Hardesty, of Boston University School of Medicine, have nothing to disclose.Ruth Cohen and Susan J. Moench, PhD, PA-C, of Continuing Education Alliance, have nothing to disclose.
DisclaimerTHESE MATERIALS AND ALL OTHER MA-TERIALS PROVIDED IN CONJUNCTION WITH CONTINUING MEDICAL EDUCA-TION ACTIVITIES ARE INTENDED SOLE-LY FOR PURPOSES OF SUPPLEMENTING CONTINUING MEDICAL EDUCATION PROGRAMS FOR QUALIFIED HEALTH-CARE PROFESSIONALS. ANYONE USING THE MATERIALS ASSUMES FULL RESPON-SIBILITY AND ALL RISK FOR THEIR AP-PROPRIATE USE. TRUSTEES OF BOSTON UNIVERSITY MAKES NO WARRANTIES OR REPRESENTATIONS WHATSOEVER RE-GARDING THE ACCURACY, COMPLETE-NESS, CURRENTNESS, NONINFRINGE-MENT, MERCHANTABILITY, OR FITNESS FOR A PARTICULAR PURPOSE OF THE MATERIALS. IN NO EVENT WILL TRUS-TEES OF BOSTON UNIVERSITY BE LIABLE TO ANYONE FOR ANY DECISION MADE OR ACTION TAKEN IN RELIANCE ON THE MATERIALS. IN NO EVENT SHOULD THE INFORMATION IN THE MATERIALS BE USED AS A SUBSTITUTE FOR PROFES-SIONAL CARE.
Date of original release: May 1, 2012Date of expiration: May 1, 2013Course code: CEE77511Estimated time to complete: 2 hours
Participants wishing to earn CME credit must read the supplement, relate the content ma-terial to the learning objectives, and com-plete the self-assessment questions and the evaluation form online at: www.cealliance.org/credit/CEE77511. After login, please select the following code: CEE77511.
Successful completion of the self-assessment is required to earn CME credit. Successful
at least 70%. The estimated time to complete this activity is 2 hours.
If you have any continuing medical education questions, please contact: [email protected]. For information on the Boston University School of Medicine Privacy Policy, please visit: www.bu.edu/cme/policies/privacy_policy.html.
About This CME Activity
Managing Patients With Heavily Pretreated Metastatic Breast Cancer: Balancing Efficacy and Safety
Information for Authors and Advertisers
Aims and Scope
COMMUNITY ONCOLOGY is an independent journal that publishes peer-reviewed research, review articles and commentary on all aspects ofclinical oncology practice. Article types include original clinical studies inpractice-based settings, state-of-the-art review papers, peer viewpoints,commentaries, and letters to the editor.
For a full and complete guide for authors, go to ees.elsevier.com/co/
For further information, contact the Managing Editor, Renee Matthews,at 240-221-2461 or e-mail, [email protected].
Correspondence
For general, noneditorial enquiries, write to COMMUNITY ONCOLOGY,60B Columbia Road, Morristown, NJ 07960; tel: 973-290-8200; fax:973-290-8250.
Letters to the Editor should be addressed to the Editor-in-Chief, DavidH. Henry, MD, FACP, e-mail: [email protected].
Advertising
For information regarding advertising rates, contact Peter Murphy(tel: 201-529-4020; e-mail: [email protected]) or StuartWilliams (tel: 201-529-4004; e-mail: [email protected]);for information regarding supplements and projects, contact DevinGregorie (tel: 516-381-8613; e-mail: [email protected]).
CME Supplements
For information on CME supplements to COMMUNITY ONCOLOGY,contact Sylvia Reitman of Global Academy for Medical Education,LLC, at e-mail: [email protected].
Annual Subscription Rates
For 12 issues (in US$): Individual $380, Canada $413, International$413; Institutional $380, Canada $413, International, $413; Singlecopy $45.
For further information regarding subscriptions, contact BarbaraCavallaro, e-mail: [email protected]
COMMUNITY ONCOLOGY (ISSN 1548-5315) is published monthlyby International Medical News Group, LLC, 60B Columbia Road,Morristown, NJ 07960.
CopyrightCopyright © 2012 by Elsevier Inc. All rights reserved. No part of thispublication may be reproduced or transmitted in any form or by anymeans, electronic or mechanical, including photocopy, recording, or anyinformation storage and retrieval system, without written permissionfrom the Publisher.
DisclaimerDiscussions, views, opinions, and recommendations as to medicalprocedures, products, choice of drugs, and drug dosages are theresponsibility of the authors or advertisers. No responsibility is assumedby the Publisher, Editor, or Editorial Board for any injury and/ordamage to persons or property as a matter of product liability,negligence, or otherwise or from any use or operation of any methods,products, instructions, or ideas contained in the material herein. Becauseof rapid advances in the medical sciences, independent verification ofdiagnoses and drug dosages should be made. Advertiser and advertisingagency recognize, accept, and assume liability for all content (includingtext, representations, illustrations, opinions, and facts) of advertisementsprinted and also assume responsibility for any claims made against thePublisher arising from or related to such advertisements.
In the event that legal action or a claim is made against the Publisherarising from or related to such advertisements, advertiser and advertisingagency agree to fully defend, indemnify, and hold harmless the Publisherand to pay any judgment, expenses, and legal fees incurred by thePublisher as a result of said legal action or claim. The Publisher reservesthe right to reject any advertising that he feels is not in keeping with thepublication’s standards.
The Publisher is not liable for delays in delivery and/or nondelivery inthe event of Act of God, action by any government or quasi-governmental entity, fire, flood, insurrection, riot, explosion, embargo,strikes (whether legal or illegal), labor or material shortage, transportationinterruption of any kind, work slowdown, or any condition beyond thecontrol of the Publisher that affects production or delivery in anymanner.
This journal is printed on paper meeting the requirements of ANSI/NISO Z39.48-1992 (Permanence of Paper) effective with Volume 1,Issue 1, 2004.
Community Oncology is indexed by EMBASE and the Cumulative Index to Nursing and Allied Health Literature (CINAHL)
May 2012VOLUME 9, NUMBER 5S
A2 COMMUNITY ONCOLOGY � May 2012 www.globalacademycme.com/oncology
Review
Chemotherapy in patients with heavilypretreated metastatic breast cancer:overviewChristopher J. Twelves, MD, MB ChB, FRCP, RCPS,1 and Monica N. Fornier, MD2
1Professor of Clinical Pharmacology and Oncology, Lead, Experimental Cancer Medicine Center, University of Leeds & StJames’s Institute of Oncology, Leeds, United Kingdom; 2Assistant Member at the Breast Cancer Medicine Service of MemorialSloan-Kettering Cancer Center, Assistant Professor at the Weill Medical College of Cornell University, New York Presbyterian
Hospital, New York, NYVolume 9/Numbe
Breast cancer is the most commonly diag-nosed malignancy in women in the UnitedStates. In 2011, an estimated 230,480 new
cases of breast cancer were diagnosed in women—approximately 30% of all new cases of canceramong women—and 39,520 died from breast can-cer, second only to lung cancer.1 Up to 30% ofwomen diagnosed with early breast cancer willeventually develop advanced disease.2
Retrospective evidence suggests that survivalrates for women with metastatic breast cancerhave been improving during the past several de-cades. For example, in an analysis of 834 patientstreated for recurrent breast cancer at M.D. An-derson and stratified from time of disease recur-rence, the estimated risk of death was reduced byapproximately 1%/y from 1974-2000.3 Improve-ment in overall survival (OS) of women with adiagnosis of metastatic breast cancer was observedin a large population-based study that comparedpatients diagnosed in early, and also middle orlatter years of the 1990s; survival improved 30%for those diagnosed late in the decade comparedwith those diagnosed in the early or middle partsof the decade. This improvement was associatedwith use of newer, more effective systemic therapyfor metastatic breast cancer.4
Mauri et al reviewed trials comparing differentchemotherapeutic regimens and/or targeted ther-apy in advanced breast cancer from 1973-2007
Correspondence to: Christopher J. Twelves, MD, MB ChB,FRCP, RCPS, Level 4, Bexley Wing, St James’s UniversityHospital, Beckett Street, Leeds LS9 7TF, UK. Phone: �44 (0)113 20 68186 ([email protected]).Disclosures: Dr Fornier has nothing to disclose.Dr Twelves has received grant research support from Roche.He has also been a consultant for Eisai Inc. and Roche and a
speaker for Eisai Inc.r 5S
and found that stepwise improvements in treat-ment efficacy cumulatively have achieved majorimprovements in survival. Use of anthracyclineregimens resulted in relative risk reductions inmortality of 22%-33% compared with older, single-agent nonanthracyclines. Further reductions inrisk were achieved by use of newer regimens, suchas single-agent taxanes or combinations of an an-thracycline and a taxane.5
The majority of women who develop metastaticdisease do so following previous treatment of earlybreast cancer. Those women with hormone receptor-positive metastatic breast cancer are likely to initiallyreceive endocrine therapy; cytotoxic therapy is, how-ever, recommended for disease that is refractory orhas become resistant to endocrine therapy, and forpatients with rapidly progressive visceral disease.Chemotherapy also is recommended for mostwomen diagnosed with hormone receptor-negativemetastatic breast cancer.6
Patients with metastatic breast cancer in whomchemotherapy is being considered are more andmore likely to have been exposed to an anthracyclineand/or a taxane in different treatment scenarios. An-thracyclines, and increasingly taxanes, are widelyused in the adjuvant setting. Alternatively, theseagents may have been administered as a first- orsecond-line treatment for metastatic disease alone oroccasionally in combination. Therefore, selection ofchemotherapy for women with metastatic disease isinfluenced by treatment history for which significantheterogeneity exists.7 The increasing population ofpatients with anthracycline-/taxane-resistant meta-static disease highlights the need to identify effectivecytotoxic treatment in this setting.
Commun Oncol 2012;9:S1-S4 © 2012 Elsevier Inc. All rights reserved.doi:10.1016/j.cmonc.2012.03.001
May 2012 � COMMUNITY ONCOLOGY S1

Review
S2 COM
Chemotherapy drug resistance is believed to causetreatment failures in � 90% of patients with metastaticcancer; micrometastatic disease resistance also likely limitsthe efficacy of chemotherapy in the adjuvant setting.8
Extensive use of the taxanes and anthracyclines as adju-vant therapy potentially contributes to resistance in thosepatients who subsequently relapse. Even where there is nohistory of prior exposure, de novo resistance to chemo-therapy may be present before treatment. Mechanisms ofresistance to anticancer drugs include reduced apoptosis,altered cell cycle checkpoints, increased metabolism ofdrugs, increased or altered targets, increased repair ofdamage, and intracellular drug compartmentalization.
Case Study: Is this a common clinicalscenario in your practice?A 62-year-old woman diagnosed 7 years ago with a 24 mm,grade II, 1 node positive (stage IIb), estrogen receptor (ER)/progesterone receptor (PR)-positive, human epidermalgrowth factor receptor 2 (HER2)-negative breast cancer wastreated with breast-conserving surgery, followed by wholebreast irradiation and adjuvant chemotherapy with doxorubi-cin and cyclophosphamide (AC) and 5 years of tamoxifen. Oneyear ago, she presented with radiologic evidence of bone me-tastases. Following 2 lines of single-agent endocrine therapy,and development of visceral disease (liver), the patient receivedsingle-agent paclitaxel as first-line chemotherapy for advanceddisease followed by single-agent capecitabine following diseaseprogression. Her Eastern Cooperative Oncology Group(ECOG) performance status is 1 and her most recent CT scanindicates further progression of disease.
Commentary: When patients have metastatic diseaseprogression following 2 lines of endocrine therapy, it may bereasonable to consider additional lines of endocrine therapy,especially where the patient appeared to benefit from themost recent hormonal agent. Development of visceral dis-ease, however, as illustrated by the liver metastases observedin this patient, often provides a tipping point from endocrinetherapy to chemotherapy. Three chemotherapeutic agentscurrently have US Food and Drug Administration (FDA)approval for patients with heavily pretreated breast cancer,including prior exposure to an anthracycline and a taxane:capecitabine, ixabepilone (as a single agent or in combina-tion with capecitabine), and eribulin. Lower level evidenceprovides some support for use of a variety of other cytotoxicagents in this setting. Decision making regarding cytotoxictherapy selection should be individualized according to a num-ber of patient-, disease-, and treatment-related factors. Theaim of this supplement is to review existing evidence to provideguidance on developing treatment plans for patients with ad-vanced breast cancer that has progressed following treatmentwith taxanes and anthracyclines.
Resistance also can occur due to variations in microtubu-
MUNITY ONCOLOGY � May 2012
lar structure, affecting interaction of the drug with itstarget. Tumors may overexpress a particular isoform oftubulin; acquired and intrinsic mutations can affect tubu-lin binding sites, and altered expression of microtubule-associated proteins can occur.9,10
Despite population-based findings of improved out-comes, which are partially attributable to earlier detectionand use of more effective systemic therapies, median sur-vival in patients with metastatic breast cancer is 18-24months,4 and the disease remains incurable.11 The pri-mary goals of treatment focus on prolonging survival,alleviation or prevention of tumor-related symptoms, andmaximizing quality of life.
OS is the recognized “gold standard” endpoint in eval-uating clinical benefits of cancer therapies. However,studies that use OS for evaluation of clinical benefit re-quire large numbers of patients, longer follow-up periods,and may be confounded by subsequent therapies.12 Areview of phase III randomized trials in the setting ofadvanced breast cancer from January 1998-December2007 found OS was used infrequently as the primaryendpoint.13 Moreover, in those trials with OS as theprimary endpoint, none had a positive outcome withrespect to OS. Improved OS as a secondary endpoint wasachieved in 15 trials, a finding that was observed morefrequently in larger trials and those conducted in second-or third-line settings.
Progression-free survival (PFS) frequently is used as asurrogate for OS; however, the relationship between the 2endpoints is disputed. Interestingly, in a review of data fromrecent phase III trials in advanced breast cancer, PFS ac-counted for approximately one-third of OS; nearly two-thirds of patient survival was attributed to duration of survivalafter the disease had progressed.13 When postprogression sur-vival is longer than PFS, many more patients are required toshow statistically superior OS than improved PFS.14
Lack of correlation between PFS and OS was noted byCortazar et al, who reviewed US Food and Drug Adminis-tration (FDA) submission data for 14 randomized clinicaltrials in 9,819 patients with metastatic breast cancer forwhich first-line or second- and third-line indications werebeing sought. PFS was the primary or secondary endpoint.Using a linear regression model, each trial was weighted bysample size and the relationship between PFS and OS in-vestigated. No association between PFS and OS was ob-served. The variation in PFS explained � 10% of the vari-ation in OS, suggesting the relationship between PFS andOS is weak, especially for second- and third-line therapiesfor metastatic breast cancer.15 This may be explained in partby post-trial lines of therapy, especially where a substantialproportion of patients in the control arm are able to receive
the “experimental” therapy at progression.www.globalacademycme.com/oncology
ry do treatmentom M
Twelves & Fornier
No established standardof careNo standard of care exists in se-lecting cytotoxic therapy for pa-tients with heavily pretreatedmetastatic breast cancer.16 Thisconclusion is supported by resultsfrom a recent retrospective cohortstudy evaluating treatment patternsin patients with advanced breastcancer previously exposed to an an-thracycline, a taxane, and capecit-abine.17 Although 61.8% of thesepatients received � 1 additionallines of chemotherapy, a variety ofagents were used in this setting. Inthis context, it is also important tonote that clinical outcome measures,such as response rate and time todisease progression, typically decline as the line of cytotoxictherapy increases. For example, typical outcomes with sin-gle-agent first-line chemotherapy for advanced breast cancerare response rates of 25%-45%, with time to progression of5-8 months. For second- and third-line therapy, responserates decrease from 15%-30% to 0%-20%, respectively, andtime to progression declines from 2-5 months to 1-4months. Few data are available for patients treated with � 4lines of therapy.18
Single-agent chemotherapy options for the treatmentof metastatic breast cancer are included in the NationalComprehensive Cancer Network (NCCN) guidelines as“preferred” or “other” agents. “Preferred” single agents aresummarized by class and include anthracyclines (doxoru-bicin, epirubicin, and pegylated liposomal doxorubicin),taxanes (paclitaxel, docetaxel, and albumin-bound pacli-taxel), antimetabolites (capecitabine and gemcitabine),and other microtubule inhibitors (vinorelbine and eribu-lin). Other single agents recommended are cyclophospha-mide, mitoxantrone, cisplatin, oral etoposide, vinblastine,fluorouracil (continuous infusion), and ixabepilone.6
However, the guidelines do not include recommendationson the order in which these agents should be administeredacross multiple lines of cytotoxic therapy.
NCCN guidelines also include lists of chemotherapycombination regimens: cyclophosphamide/doxorubicin/flu-orouracil; fluorouracil/epirubicin/cyclophosphamide; doxo-rubicin/cyclophosphamide; epirubicin/cyclophosphamide;doxorubicin/docetaxel or doxorubicin/paclitaxel; cyclophos-phamide/methotrexate/fluorouracil; docetaxel/capecitabine;gemcitabine/paclitaxel; and ixabepilone plus capecitabine.
Most trials comparing combination chemotherapy to
SatisfWith
Depression
Anx
FIGURE 1 Symptomsstatus are the 4 primaselection. Reprinted fr
single-agent cytotoxic therapy in advanced breast cancer
Volume 9/Number 5S
have been conducted in the first-line setting and generallyhave demonstrated increased rates of objective responseand longer time to progression with greater toxicity butno improvement in OS in the combination arm.19,20 Thebenefits of sequential single-agent therapy may be com-parable to combination therapy with fewer side effects.6,21
Treatment selection factorsConsiderations in optimal timing of initiation of cytotoxictherapy and continuation are individualized due to biologicvariability of patients and their disease,22 including likeli-hood of resistance to particular cytotoxic agents. Risk assess-ment and treatment choices are guided by a number offactors, which can be classified as disease-related or patient-related. Disease-related factors include disease-free intervalsince primary diagnosis and completion of adjuvant therapy,previous therapies and response to them, hormone receptorstatus and human epidermal growth factor receptor 2(HER2) status of the primary tumor and/or metastatic le-sion, tumor burden (location and extent of metastases), andneed for rapid disease and/or symptom control. Patient-
chologicalStatus
Qualityof Life
SocialFunctioning
Symptomsand SideEffects
PhysicalFunction
Status
Neuropathy
Diarrhea
FamilyInteraction
WRecr
Time WithFriends
Self-Care
FatigueMobility
n
lopecia
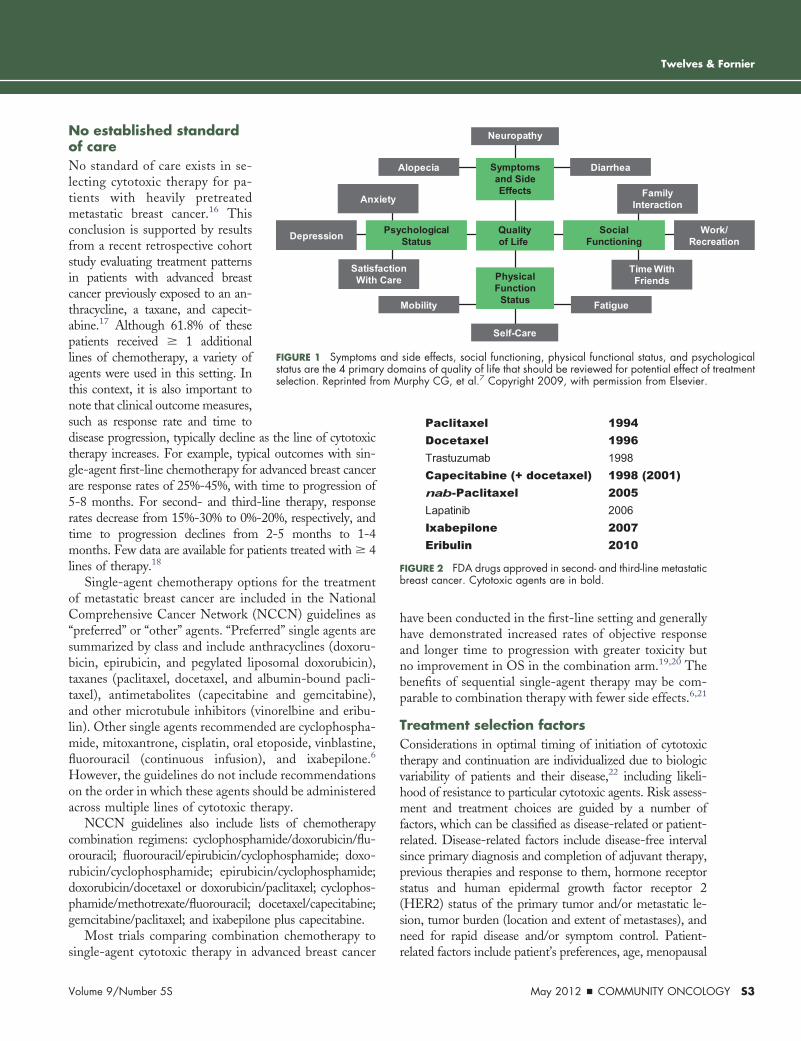
side effects, social functioning, physical functional status, and psycmains of quality of life that should be reviewed for potential effect ofurphy CG, et al.7 Copyright 2009, with permission from Elsevier.
1994199619981998 (2001)2005200620072010
PaclitaxelDocetaxelTrastuzumabCapecitabine (+ docetaxel)nab-PaclitaxelLapatinibIxabepiloneEribulin
FIGURE 2 FDA drugs approved in second- and third-line metastaticbreast cancer. Cytotoxic agents are in bold.
Psy ork/eation
actio Care
iety
A
and hological
related factors include patient’s preferences, age, menopausal
May 2012 � COMMUNITY ONCOLOGY S3

Review
S4 COM
status, comorbidities and performance status, anticipatedside effects of treatment, socioeconomic and psychologicalfactors, and availability and access to treatment.22,23 Thequality of life issues that may have an impact on treatmentselection are illustrated in Figure 1.7
In 2009, the Central European Cooperative OncologyGroup (CECOG) published its third consensus on med-ical treatment of metastatic breast cancer.22 The consen-sus statement acknowledges that few effective treatmentoptions are available to women with metastatic breastcancer who have failed to respond or relapsed after pre-treatment with anthracyclines and taxanes. Based onstudies of agents that have shown activity, consensustreatment recommendations state, “. . . capecitabine,gemcitabine, liposomal doxorubicin, ixabepilone or vi-norelbine, all administered as either monotherapy or incombination with other cytotoxic agents may be beneficialafter failure of anthracyclines and taxanes. Consecutivecytotoxic chemotherapy is worth considering in womenwho have responded to previous regimens, but no defin-itive guidance can be given regarding the optimal agentsor the order they should be administered.”22
Newer approachesNew approaches for treatment of patients with advancedbreast cancer include new drug classes and formulations toovercome drug resistance. Newer formulations of existingclasses of agents are represented by nab-paclitaxel and pegy-lated liposomal doxorubicin, whereas the epothilones andhalichondrins represent new drug classes. Although numer-ous chemotherapeutic options are available for women withheavily pretreated, advanced breast cancer, only a handful ofcytotoxic agents have been FDA-approved as second- orthird-line treatment options for patients with metastaticbreast cancer (Figure 2). The next 2 articles address criteriato guide selection of cytotoxic agents for patients withHER2-negative metastatic breast cancer previously exposedto an anthracycline and a taxane; HER2-targeted therapy isoutside the purview of this review. Most of the studies citedin these articles involve single-agent cytotoxic therapy, al-though several combination chemotherapy regimens will bediscussed. No fixed algorithm exists to guide treatment se-lection, a process based on many factors, including priortherapies, cytologic toxicities, patient performance status,and patient choice and preference.
AcknowledgmentsWriting assistance was provided by Debra Hughes. The authors retainedfull editorial control of the manuscript.
References1. Siegel R, Ward E, Brawley O, Jemal A. Cancer statistics, 2011.
The impact of eliminating socioeconomic and racial disparities on pre-mature cancer deaths. CA Cancer J Clin. 2011;61(4):212-36.
MUNITY ONCOLOGY � May 2012
2. Brewster AM, Hortobagyi GN, Broglio KR, et al. Residual risk ofbreast cancer recurrence 5 years after adjuvant therapy. J Natl CancerInst. 2008;100(16):1179-83.
3. Giordano S, Buzdar AU, Smith TL, Kau SW, Yang Y, Horto-bagyi GN. Is breast cancer survival improving? Trends in survival forpatients with recurrent breast cancer diagnosed from 1974 through2000. Cancer. 2004;100(1):44-52.
4. Chia SK, Speers CH, D’yachkova Y, et al. The impact of newchemotherapeutic and hormone agents on survival in a population-basedcohort of women with metastatic breast cancer. Cancer. 2007;110(5):973-9.
5. Mauri D, Polyzos NP, Salanti G, Pavlidis N, Ioannidis JPA.Multiple-treatments meta-analysis for chemotherapy and targeted ther-apies in advanced breast cancer. J Natl Cancer Inst. 2008;100(24):1780-91.
6. National Comprehensive Cancer Network. NCCN Clinical Prac-tice Guidelines in Oncology™: Breast Cancer. V.2.2011. Available at:http://www.nccn.org. Accessed February 8, 2012.
7. Murphy CG, Seidman AD. Evolving approaches to metastatic breastcancer previously treated with anthracyclines and taxanes. Clin Breast Can-cer. 2009;9(Suppl 2):S58-S65.
8. Longley DB, Johnston PG. Molecular mechanisms of drug resis-tance. J Pathol. 2005;205(2):275-92.
9. Morris PG, Fornier MN. Microtubule active agents: beyond thetaxane frontier. Clin Cancer Res. 2008;14(22):7167-72.
10. Rivera E, Gomez H. Chemotherapy resistance in metastaticbreast cancer: the evolving role of ixabepilone. Breast Cancer Res. 2010;12(Suppl 2):S2.
11. Gennari A, Conte P, Rosso R, et al. Survival of metastatic breastcarcinoma patients over a 20 year period. Cancer. 2005;104(8):1742-50.
12. Pazdur R. Endpoints for assessing drug activity in clinical trials.Oncologist. 2008;13(Suppl 2):19-21.
13. Saad E, Katz A, Buyse M. Overall survival and post-progressionsurvival in advanced breast cancer: a review of recent randomized clinicaltrials. J Clin Oncol. 2010;28(11):1958-62.
14. Broglio KR, Barry DA. Detecting an overall survival benefit thatis derived from progression-free survival. J Natl Cancer Inst. 2009;101(23):1642-9.
15. Cortazar P, Zhang JJ, Sridhara R, Justice RL, Pazdur R. Relation-ship between OS and PFS in metastatic breast cancer (MBC): Review ofFDA submission data [abstract 1035]. J Clin Oncol. 2011;29(Suppl).
16. Cardoso F, Bedard PL, Winer EP, et al; ESO-MBC TaskForce. International guidelines for management of metastatic breastcancer: combination vs sequential single-agent chemotherapy. J NatlCancer Inst. 2009;101(17):1174-81.
17. Donato BMK, Burns L, Wiley V, et al. Treatment patterns inpatients with advanced breast cancer who were exposed to an anthra-cycline, a taxane, and capecitabine: a descriptive report. Clin Ther.2010;32(3):546-54.
18. Burstein H. Oral abstract discussion. Presented at: American Soci-ety of Clinical Oncology Annual Meeting; June 4-8, 2010; Chicago, IL.
19. Nielsen DL, Bjerre KD, Jakobsen EH, et al. Gemcitabine plusdocetaxel in patients with predominantly human epidermal growthfactor receptor 2-negative locally advanced or metastatic breast cancer: arandomized, phase III study by the Danish Breast Cancer CooperativeGroup. J Clin Oncol. 2011;29(36):4748-54.
20. Sledge GW, Neuberg D, Bernardo P, et al. Phase III trial ofdoxorubicin, paclitaxel, and the combination of doxorubicin and pacli-taxel as front-line chemotherapy for metastatic breast cancer: an inter-group trial (E1193). J Clin Oncol. 2003;21(4):588-92.
21. Dees EC. Taxane doublets for metastatic breast cancer: do we needanother cytotoxic pair or approach? J Clin Oncol. 2011;29(36):4738-40.
22. Beslija S, Bonneterre J, Burstein HJ, et al. Third consensus on medicaltreatment of metastatic breast cancer. Ann Oncol. 2009;20(11):1771-85.
23. Cardoso F, Fallowfield L, Costa A, Castiglione M, Senkus E;ESMO Guidelines Working Group. Locally recurrent or metastatic
breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treat-ment and follow-up. Ann Oncol. 2011;22(Suppl 6):vi25-vi30.www.globalacademycme.com/oncology
Review
Approved chemotherapy agents forpatients with metastatic breast cancerpreviously exposed to taxanes andanthracyclinesChristopher J. Twelves, MD, MB ChB, FRCP, RCPS,1 and Monica N. Fornier, MD2
1Professor of Clinical Pharmacology and Oncology, Lead, Experimental Cancer Centre, University of Leeds & St James’sInstitute of Oncology, Leeds, United Kingdom; 2Assistant Member at the Breast Cancer Medicine Service of Memorial Sloan-Kettering Cancer Center, Assistant Professor at the Weill Medical College of Cornell University, New York Presbyterian
Hospital, New York, NYVolume 9/Numbe
Patients with metastatic breast cancer whosedisease progresses after treatment with an-thracycline and taxane therapy have limited
approved treatment options. Currently, 3 cyto-toxic agents are US Food and Drug Administra-tion (FDA)-approved for the treatment of pa-tients with heavily pretreated metastatic breastcancer: capecitabine, ixabepilone (as monotherapyin patients resistant to capecitabine, and in com-bination with capecitabine), and eribulin mesylate.This article reviews the efficacy and toxicity datafor each of these agents and regimens.
CapecitabineThe antimetabolite capecitabine is a fluoropyrimi-dine carbamate, an orally administered pro-drugof 5-fluorouracil (5-FU) designed to mimic con-tinuous infusion of 5-FU and deliver drug prefer-entially to tumor tissue. Capecitabine inhibits thy-midylate synthase and interferes with DNA andRNA synthesis.1 Capecitabine monotherapy oftenis considered a treatment of choice in patientswith metastatic breast cancer with prior exposureto an anthracycline and a taxane due to its activityas well as its good overall safety profile and oral routeof administration.2 Additional support for the use ofthis agent is the negligible risk of capecitabine-associated alopecia,3 an adverse effect of chemo-
Correspondence to: Christopher J. Twelves, MD, MB ChB,FRCP, RCPS, Level 4, Bexley Wing, St James’s UniversityHospital, Beckett Street, Leeds LS9 7TF, UK. Phone: �44 (0)113 20 68186 (e-mail: [email protected]).Disclosures: Dr Fornier has nothing to disclose.Dr Twelves has received grant research support from Roche.He has also been a consultant for Eisai Inc. and Roche and a
speaker for Eisai Inc.r 5S
therapy that has a detrimental impact on quality oflife for many patients with breast cancer.4
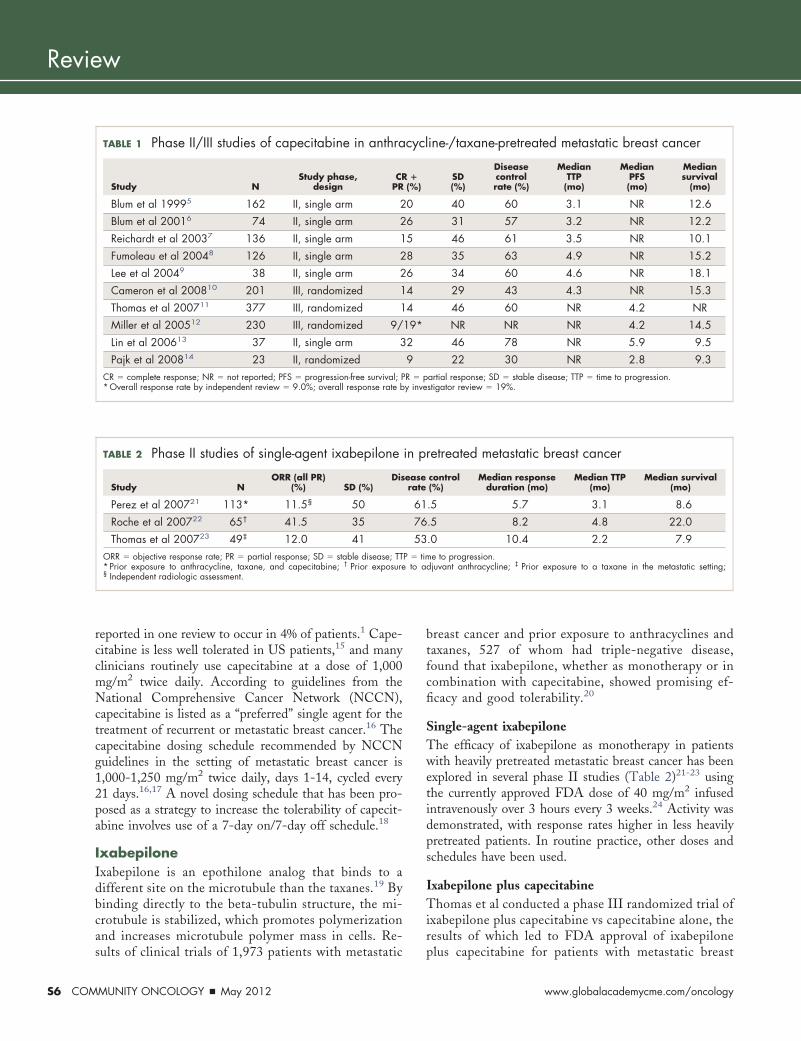
Efficacy data for 3 phase III trials and 7 phaseII trials of capecitabine in patients with metastaticbreast cancer previously treated with anthracy-clines and taxanes are summarized in Table 1.5-14
The capecitabine dose was 1,250 mg/m2 or 1,255mg/m2 twice daily for 14 days every 3 weeks in allof these studies, which have shown overall re-sponse rates (complete response [CR] � partialresponse [PR]) ranging from 9%-32% and diseasecontrol rates of 30%-78% in this heavily pretreatedpopulation. Range in median time to progression(TTP) was 3.1-4.9 months and median progression-free survival (PFS) was 2.8-5.9 months for thosestudies reporting these endpoints. Median overallsurvival (OS) ranged from 9.3-18.1 months.
A systematic review of response and survivaldata for patients with metastatic breast cancertreated with capecitabine as second-line agent orlater (after treatment with anthracyclines and/ortaxanes) from the studies listed in Table 1 re-ported weighted mean values for disease controlrate of 57%; for median TTP, 3.9 months; and formedian OS, 13.5 months.3
Capecitabine generally is well tolerated. Themost frequently reported grade 3/4 nonhemato-logic adverse events were hand-foot syndrome(weighted mean of 16%), and diarrhea (weightedmean of 10%).3 Other reported adverse effectsincluded stomatitis, nausea, and vomiting. Grade3/4 hematologic adverse effects were uncommon,
Commun Oncol 2012;9:S5-S12 © 2012 Elsevier Inc. All rights reserved.doi:10.1016/j.cmonc.2012.03.002
May 2012 � COMMUNITY ONCOLOGY S5
Review
S6 COM
reported in one review to occur in 4% of patients.1 Cape-citabine is less well tolerated in US patients,15 and manyclinicians routinely use capecitabine at a dose of 1,000mg/m2 twice daily. According to guidelines from theNational Comprehensive Cancer Network (NCCN),capecitabine is listed as a “preferred” single agent for thetreatment of recurrent or metastatic breast cancer.16 Thecapecitabine dosing schedule recommended by NCCNguidelines in the setting of metastatic breast cancer is1,000-1,250 mg/m2 twice daily, days 1-14, cycled every21 days.16,17 A novel dosing schedule that has been pro-posed as a strategy to increase the tolerability of capecit-abine involves use of a 7-day on/7-day off schedule.18
IxabepiloneIxabepilone is an epothilone analog that binds to adifferent site on the microtubule than the taxanes.19 Bybinding directly to the beta-tubulin structure, the mi-crotubule is stabilized, which promotes polymerizationand increases microtubule polymer mass in cells. Re-
TABLE 1 Phase II/III studies of capecitabine in anthra
Study NStudy phase,
designCR
PR
Blum et al 19995 162 II, single arm 2
Blum et al 20016 74 II, single arm 2
Reichardt et al 20037 136 II, single arm 1
Fumoleau et al 20048 126 II, single arm 2
Lee et al 20049 38 II, single arm 2
Cameron et al 200810 201 III, randomized 1
Thomas et al 200711 377 III, randomized 1
Miller et al 200512 230 III, randomized 9/
Lin et al 200613 37 II, single arm 3
Pajk et al 200814 23 II, randomizedCR � complete response; NR � not reported; PFS � progression-free survival; P*Overall response rate by independent review � 9.0%; overall response rate b
TABLE 2 Phase II studies of single-agent ixabepilone
Study NORR (all PR)
(%) SD (%)Dis
Perez et al 200721 113* 11.5§ 50
Roche et al 200722 65† 41.5 35
Thomas et al 200723 49‡ 12.0 41ORR � objective response rate; PR � partial response; SD � stable disease; TT* Prior exposure to anthracycline, taxane, and capecitabine; † Prior exposure§ Independent radiologic assessment.
sults of clinical trials of 1,973 patients with metastatic
MUNITY ONCOLOGY � May 2012
breast cancer and prior exposure to anthracyclines andtaxanes, 527 of whom had triple-negative disease,found that ixabepilone, whether as monotherapy or incombination with capecitabine, showed promising ef-ficacy and good tolerability.20
Single-agent ixabepiloneThe efficacy of ixabepilone as monotherapy in patientswith heavily pretreated metastatic breast cancer has beenexplored in several phase II studies (Table 2)21-23 usingthe currently approved FDA dose of 40 mg/m2 infusedintravenously over 3 hours every 3 weeks.24 Activity wasdemonstrated, with response rates higher in less heavilypretreated patients. In routine practice, other doses andschedules have been used.
Ixabepilone plus capecitabineThomas et al conducted a phase III randomized trial ofixabepilone plus capecitabine vs capecitabine alone, theresults of which led to FDA approval of ixabepilone
ine-/taxane-pretreated metastatic breast cancer
SD(%)
Diseasecontrolrate (%)
MedianTTP(mo)
MedianPFS(mo)
Mediansurvival
(mo)
40 60 3.1 NR 12.6
31 57 3.2 NR 12.2
46 61 3.5 NR 10.1
35 63 4.9 NR 15.2
34 60 4.6 NR 18.1
29 43 4.3 NR 15.3
46 60 NR 4.2 NR
NR NR NR 4.2 14.5
46 78 NR 5.9 9.5
22 30 NR 2.8 9.3artial response; SD � stable disease; TTP � time to progression.stigator review � 19%.
retreated metastatic breast cancer
control(%)
Median responseduration (mo)
Median TTP(mo)
Median survival(mo)
.5 5.7 3.1 8.6
.5 8.2 4.8 22.0
.0 10.4 2.2 7.9e to progression.
djuvant anthracycline; ‡ Prior exposure to a taxane in the metastatic setting;
cycl
�(%)
0
6
5
8
6
4
4
19*
2
9R � py inve
in p
easerate
61
76
53P � tim
to a
plus capecitabine for patients with metastatic breast
www.globalacademycme.com/oncology

Twelves & Fornier
cancer resistant to anthracyclines and taxanes.11,24 Inthis pivotal trial, 752 patients were randomized toixabepilone 40 mg/m2 intravenously over 3 hours, day1 plus oral capecitabine 2,000 mg/m2/day, days 1-14,every 3 weeks, or to single-agent oral capecitabine2,500 mg/m2/day, days 1-14, every 3 weeks. Priortreatment must have included an anthracycline-basedregimen, and patients must have also received do-cetaxel-based or paclitaxel-based chemotherapy andexperienced disease progression during therapy orwithin 4 months of the last dose in the metastaticsetting or within 12 months in the adjuvant setting.The primary endpoint was PFS. Patients were stratifiedfor distant metastasis (liver or lung), anthracycline re-sistance, prior chemotherapy for metastatic disease, andstudy site.
For the ixabepilone plus capecitabine arm, an indepen-dent review committee determination of median PFS was5.8 months compared with 4.2 months for those receivingcapecitabine alone (Table 3)25; this difference in PFS wasstatistically significant, but there was no difference in OS.
A phase III multicenter confirmatory study ran-domly assigned 1,221 patients to ixabepilone 40 mg/m2
IV, day 1 plus capecitabine 2,000 mg/m2, days 1-14every 3 weeks or capecitabine 2,500 mg/m2, days 1-14every 3 weeks alone. The primary endpoint was OS (incontrast to PFS for the pivotal trial), and the study waspowered to detect a 20% reduction in the hazard ratio(HR) for death. There was no significant difference inmedian OS between the 2 groups, 16.4 months forixabepilone plus capecitabine vs 15.6 months for cape-citabine alone; in an adjusted analysis, the difference inOS reached statistical significance (Table 3). Again,
TABLE 3 Pivotal and confirmatory trials of ixabepilon
Pivotal
Capecitabine � ixab(n � 375)
Median OS* (mo) 12.9
HR (95% CI) 0.90 (0
P value 0.1
Adjusted Cox regression† HR (95% CI) 0.87 (0
P value 0.0
Median PFS‡ (mo) 5.8
HR (95% CI) 0.75 (0
P value 0.0HR � hazard ratio; OS � overall survival; PFS � progression-free survival.Hortoabagyi GN, et al25; Sparano JA, et al.26
* Primary endpoint in confirmatory trial; † Baseline prognostic factors: performancendpoint in pivotal trial.
the combination arm had significantly improved PFS,
Volume 9/Number 5S
6.2 months compared with 4.2 months for capecitabinealone (HR, 0.79; P � 0.0005) objective response rate(CR � PR), 43% vs 29%, respectively (P � .0001).26
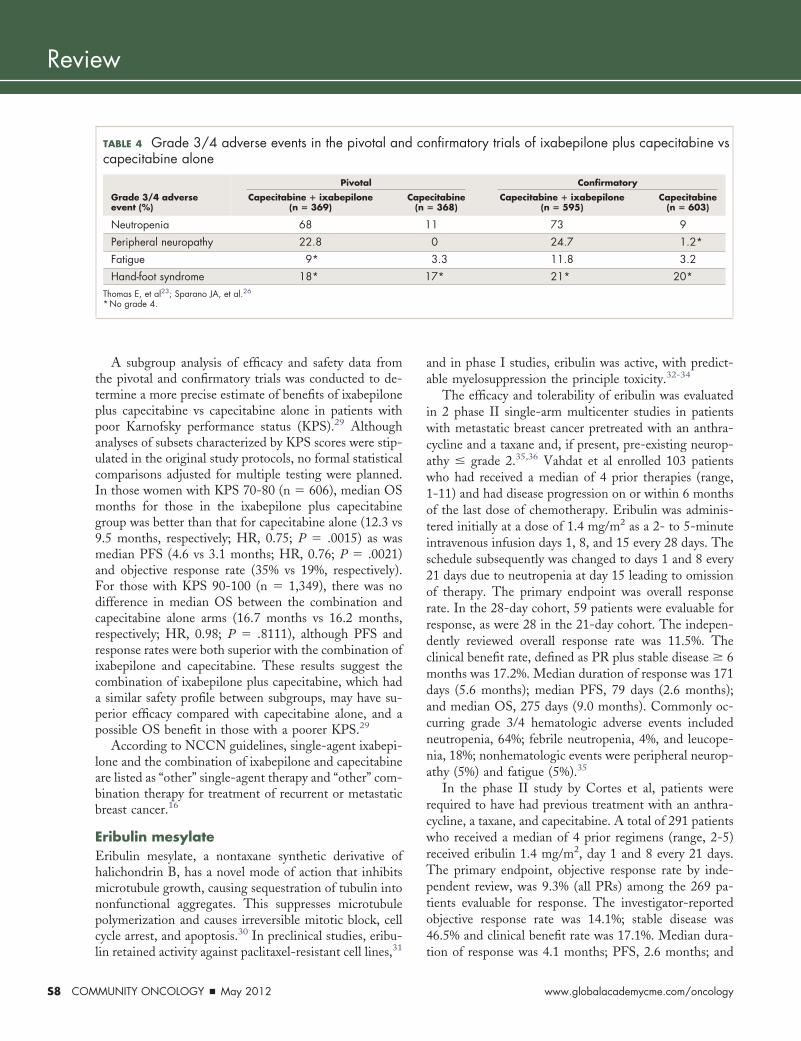
Grade 3/4 treatment-related adverse events commonlyreported in both studies are summarized in Table 4. Inthe pivotal trial, all 33 deaths within 30 days of last dosein patients receiving ixabepilone plus capecitabine wererelated to neutropenia. The risk was greatest in those withbaseline elevation � grade 2 in liver biochemistry; 5 of 16such patients (31%) died, compared with 7 of 353 patients(2%) with baseline � 1 liver dysfunction, leading to astudy protocol amendment excluding those with baseline� 2 liver dysfunction.23 In the confirmatory study, fewerdeaths occurred in the group receiving ixabepilone pluscapecitabine (3%; attributed to sepsis) than capecitabinealone (7%).26
Peripheral neuropathy, which commonly occurred inthe ixabepilone plus capecitabine group in both studies,was managed by dose reduction and delay. Comparedwith the taxanes, treatment interruption of ixabepiloneappears to result in more rapid and complete symptomresolution, suggesting the nature of peripheral neuropathymay be different with the epothilones.27 Vahdat et alconducted a retrospective review of phase II and III clin-ical trials of ixabepilone as monotherapy or in combina-tion with capecitabine (n � 1,540). Pre-existing periph-eral neuropathy was a significant risk factor for increasedgrade 3/4 peripheral neuropathy (HR, 1.44; P � .007),whereas prior therapy with taxanes appeared to decreasethis risk (HR, 0.35; P � .018). Patients with grade � 2peripheral neuropathy resulting from prior taxane usewere excluded from the ixabepilone studies, suggesting a
us capecitabine vs capecitabine alone: OS and PFS
752) Confirmatory (N � 1,221)
e Capecitabine(n � 377)
Capecitabine � ixabepilone(n � 609)
Capecitabine(n � 612)
11.1 16.4 15.6
.05) 0.90 (0.78, 1.03)
0.1162
.02) 0.85 (0.75, 0.98)
0.0231
4.2 6.2 4.4
.88) 0.79 (0.69, 0.90)
0.0005
s, age, number of organ sites, visceral disease, estrogen receptor status; ‡ Primary
e pl
(N �
epilon
.77, 1
936
.74, 1
803
.64, 0
003
e statu
selection bias.28
May 2012 � COMMUNITY ONCOLOGY S7
Review
S8 COM
A subgroup analysis of efficacy and safety data fromthe pivotal and confirmatory trials was conducted to de-termine a more precise estimate of benefits of ixabepiloneplus capecitabine vs capecitabine alone in patients withpoor Karnofsky performance status (KPS).29 Althoughanalyses of subsets characterized by KPS scores were stip-ulated in the original study protocols, no formal statisticalcomparisons adjusted for multiple testing were planned.In those women with KPS 70-80 (n � 606), median OSmonths for those in the ixabepilone plus capecitabinegroup was better than that for capecitabine alone (12.3 vs9.5 months, respectively; HR, 0.75; P � .0015) as wasmedian PFS (4.6 vs 3.1 months; HR, 0.76; P � .0021)and objective response rate (35% vs 19%, respectively).For those with KPS 90-100 (n � 1,349), there was nodifference in median OS between the combination andcapecitabine alone arms (16.7 months vs 16.2 months,respectively; HR, 0.98; P � .8111), although PFS andresponse rates were both superior with the combination ofixabepilone and capecitabine. These results suggest thecombination of ixabepilone plus capecitabine, which hada similar safety profile between subgroups, may have su-perior efficacy compared with capecitabine alone, and apossible OS benefit in those with a poorer KPS.29
According to NCCN guidelines, single-agent ixabepi-lone and the combination of ixabepilone and capecitabineare listed as “other” single-agent therapy and “other” com-bination therapy for treatment of recurrent or metastaticbreast cancer.16
Eribulin mesylateEribulin mesylate, a nontaxane synthetic derivative ofhalichondrin B, has a novel mode of action that inhibitsmicrotubule growth, causing sequestration of tubulin intononfunctional aggregates. This suppresses microtubulepolymerization and causes irreversible mitotic block, cellcycle arrest, and apoptosis.30 In preclinical studies, eribu-
TABLE 4 Grade 3/4 adverse events in the pivotal ancapecitabine alone
Grade 3/4 adverseevent (%)
Pivotal
Capecitabine � ixabepilone(n � 369)
Neutropenia 68
Peripheral neuropathy 22.8
Fatigue 9*
Hand-foot syndrome 18*Thomas E, et al23; Sparano JA, et al.26
*No grade 4.
lin retained activity against paclitaxel-resistant cell lines,31
MUNITY ONCOLOGY � May 2012
and in phase I studies, eribulin was active, with predict-able myelosuppression the principle toxicity.32-34
The efficacy and tolerability of eribulin was evaluatedin 2 phase II single-arm multicenter studies in patientswith metastatic breast cancer pretreated with an anthra-cycline and a taxane and, if present, pre-existing neurop-athy � grade 2.35,36 Vahdat et al enrolled 103 patientswho had received a median of 4 prior therapies (range,1-11) and had disease progression on or within 6 monthsof the last dose of chemotherapy. Eribulin was adminis-tered initially at a dose of 1.4 mg/m2 as a 2- to 5-minuteintravenous infusion days 1, 8, and 15 every 28 days. Theschedule subsequently was changed to days 1 and 8 every21 days due to neutropenia at day 15 leading to omissionof therapy. The primary endpoint was overall responserate. In the 28-day cohort, 59 patients were evaluable forresponse, as were 28 in the 21-day cohort. The indepen-dently reviewed overall response rate was 11.5%. Theclinical benefit rate, defined as PR plus stable disease � 6months was 17.2%. Median duration of response was 171days (5.6 months); median PFS, 79 days (2.6 months);and median OS, 275 days (9.0 months). Commonly oc-curring grade 3/4 hematologic adverse events includedneutropenia, 64%; febrile neutropenia, 4%, and leucope-nia, 18%; nonhematologic events were peripheral neurop-athy (5%) and fatigue (5%).35
In the phase II study by Cortes et al, patients wererequired to have had previous treatment with an anthra-cycline, a taxane, and capecitabine. A total of 291 patientswho received a median of 4 prior regimens (range, 2-5)received eribulin 1.4 mg/m2, day 1 and 8 every 21 days.The primary endpoint, objective response rate by inde-pendent review, was 9.3% (all PRs) among the 269 pa-tients evaluable for response. The investigator-reportedobjective response rate was 14.1%; stable disease was46.5% and clinical benefit rate was 17.1%. Median dura-
nfirmatory trials of ixabepilone plus capecitabine vs
Confirmatory
citabine� 368)
Capecitabine � ixabepilone(n � 595)
Capecitabine(n � 603)
1 73 9
0 24.7 1.2*
3.3 11.8 3.2
7* 21* 20*
d co
Cape(n
1
1
tion of response was 4.1 months; PFS, 2.6 months; and
www.globalacademycme.com/oncology
: the
Twelves & Fornier
median OS, 10.4 months. Grade3/4 toxicities included neutrope-nia (54%; febrile neutropenia,5.5%), leukopenia (14%), and as-thenia/fatigue (10%; no grade 4).A total of 6.9% of patients hadgrade 3 neuropathy (no grade 4).36
Similar results, albeit withhigher rates of hematologic toxic-ities, were obtained in a single-arm, open-label phase II study in80 Japanese patients receiving 1.4mg/m2 eribulin on a 21-day cyclewho had a median of 3 prior reg-imens (range, 1 to 5), including an anthracycline and ataxane. The primary endpoint, overall response rate byindependent review, was 21.3%. An additional 30 patients(37.5%) had stable disease and the clinical benefit rate (ie,CR � PR � stable disease � 6 months) was 27.5%.Median duration of response was 3.9 months; PFS was3.7 months; and OS, 11.1 months. Grade 3/4 neutrope-nia (95.1%; febrile neutropenia, 13.6%) and leukopenia(74.1%) were the most frequently occurring adverseevents; grade 3 peripheral neuropathy was observed in3.7% of patients (no grade 4).37
The open-label, multicenter, randomized phase IIIEisai Metastatic Breast Cancer Study Assessing Physi-cian’s Choice versus E7389 (EMBRACE) study enrolled762 patients with locally recurrent or metastatic breastcancer who received between 2 and 5 previous regimensthat included an anthracycline and a taxane, at least 2 ofwhich were for advanced disease. Patients needed to havedisease progression on or within 6 months of the lastchemotherapy regimen and neuropathy � grade 2.38
Patients were randomly assigned 2:1 to eribulin mesy-late 1.4 mg/m2 as a 2- to 5-minute intravenous bolus ondays 1 and 8 of a 21-day cycle or the control group,treatment of physician’s choice (TPC), a discretionaryselection of any monotherapy (ie, cytotoxic, hormonal, orbiologic therapy) approved for the treatment of cancerand administered according to local practice, if applicable,or supportive care only (palliative treatment or radiother-apy). Patients were stratified by geographic region, priorcapecitabine treatment, and human epidermal growthfactor receptor (HER)2 status. The primary endpoint wasOS in the intent-to-treat population; secondary end-points were PFS, objective response rate, response dura-tion, and safety.
The treatment arms were well balanced, the majorityof the patients being white (92%), and having a goodperformance status (Eastern Cooperative Oncology
ITT populAnthracyc
30
25
20
15
0
5
10% o
f Pat
ient
s
25%
n = 6
Vinore
FIGURE 1 EMBRACE
Group [ECOG] 0 or 1, 91%). Median age was 55 years;
Volume 9/Number 5S
16% had HER2-positive disease, 19% had triple-negativemetastatic breast cancer, and 84% had � 2 organsinvolved, including metastases to the liver, lung, andbone. Ninety-nine percent of the patients had receivedtaxanes and anthracyclines and 73% had also receivedcapecitabine.
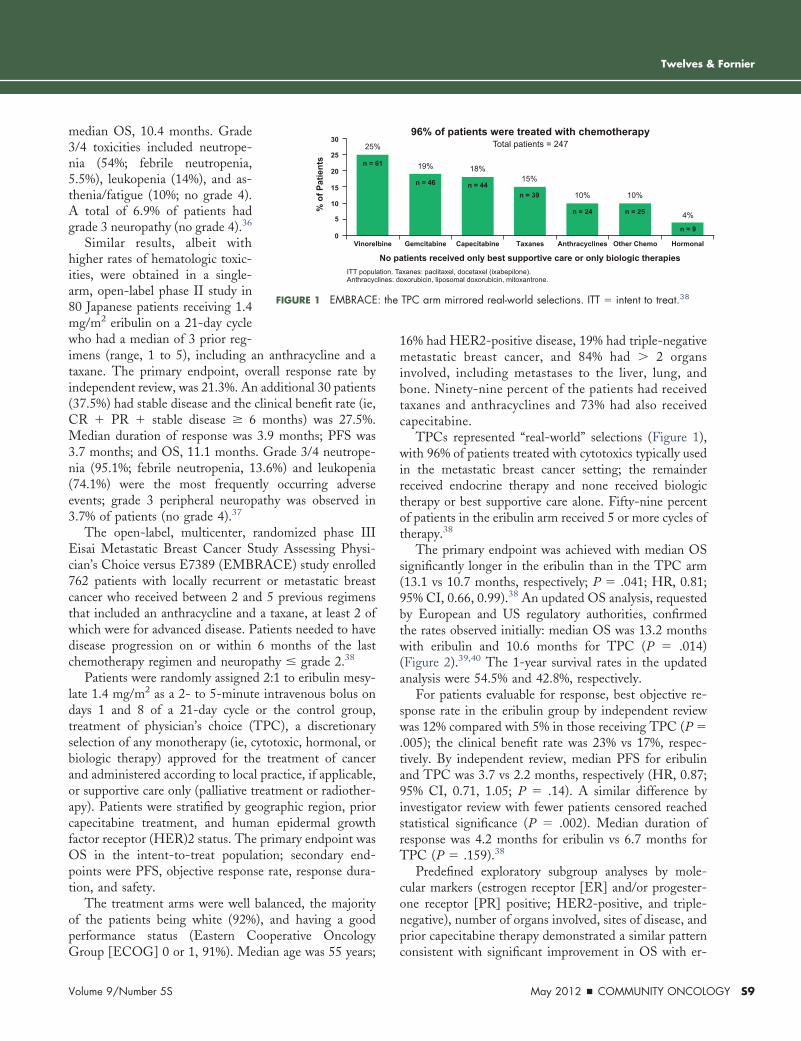
TPCs represented “real-world” selections (Figure 1),with 96% of patients treated with cytotoxics typically usedin the metastatic breast cancer setting; the remainderreceived endocrine therapy and none received biologictherapy or best supportive care alone. Fifty-nine percentof patients in the eribulin arm received 5 or more cycles oftherapy.38
The primary endpoint was achieved with median OSsignificantly longer in the eribulin than in the TPC arm(13.1 vs 10.7 months, respectively; P � .041; HR, 0.81;95% CI, 0.66, 0.99).38 An updated OS analysis, requestedby European and US regulatory authorities, confirmedthe rates observed initially: median OS was 13.2 monthswith eribulin and 10.6 months for TPC (P � .014)(Figure 2).39,40 The 1-year survival rates in the updatedanalysis were 54.5% and 42.8%, respectively.
For patients evaluable for response, best objective re-sponse rate in the eribulin group by independent reviewwas 12% compared with 5% in those receiving TPC (P �.005); the clinical benefit rate was 23% vs 17%, respec-tively. By independent review, median PFS for eribulinand TPC was 3.7 vs 2.2 months, respectively (HR, 0.87;95% CI, 0.71, 1.05; P � .14). A similar difference byinvestigator review with fewer patients censored reachedstatistical significance (P � .002). Median duration ofresponse was 4.2 months for eribulin vs 6.7 months forTPC (P � .159).38
Predefined exploratory subgroup analyses by mole-cular markers (estrogen receptor [ER] and/or progester-one receptor [PR] positive; HER2-positive, and triple-negative), number of organs involved, sites of disease, andprior capecitabine therapy demonstrated a similar pattern
tients received only best supportive care or only biologic therapiesxanes: paclitaxel, docetaxel (ixabepilone).
oxorubicin, liposomal doxorubicin, mitoxantrone.
96% of patients were treated with chemotherapyTotal patients = 247
HormonalOther ChemoGemcitabine Capecitabine Taxanes Anthracyclines
19%
n = 46
18%
n = 4415%
n = 39 10%
n = 25
10%
n = 24 4%
n = 9
TPC arm mirrored real-world selections. ITT � intent to treat.38
No paation. Talines: d
1
lbine
consistent with significant improvement in OS with er-
May 2012 � COMMUNITY ONCOLOGY S9

Review
S10 CO
ibulin; no individual subgroup was identified that ap-peared not to benefit from eribulin. For patients withER/PR-positive (n � 528) and ER/PR-negative (n �187) disease, relative risk reduction was 27% and 34%,respectively; for HER2-positive (n � 123) and HER2-negative (n � 565) disease, it was 24% and 19%, respec-tively. For patients in the triple-negative subgroup (n �144), risk reduction was 29%.41
Two additional exploratory analyses of the patients inthe EMBRACE trial were conducted to determine theinfluence of number of prior regimens and age on OSamong those treated with eribulin. The first comparedOS, PFS, overall response rate, clinical benefit rate, andtoxicity in 4 age cohorts; analyses were stratified by geo-graphic region, HER2 status, and prior capecitabine use.Results suggested survival outcomes with eribulin are in-dependent of age; therefore, age alone should not pre-clude use of this agent. Toxicity was similar in older vsyounger patients.42 In the second analysis, the OS benefitwith eribulin compared with TPC appeared to be greaterfor patients who had received fewer previous treatmentregimens for locally recurrent or metastatic disease: thosereceiving � 3 regimens (n � 571) had a relative riskreduction of 33%, compared with those who had � 3regimens (n � 190); relative risk reduction, 10%.43
Regarding toxicity, there was little difference in thefrequency of adverse events and serious adverse eventsbetween the eribulin and TPC arms.38 In the eribulingroup, neutropenia was the most frequently reportedgrade 3/4 adverse event (45%), but febrile neutropeniaoccurred in only 5% of patients and hematologic toxicities
Time (mo)No. of
Patients at Risk508 406 274 142 54 11 0
052661106178254
Prop
ortio
n of
Pat
ient
s A
live
363024181260
1.00.90.80.70.60.50.40.30.20.10.0
TPC (n = 254)Median 10.6 mo
An updated, unplanned survival analysis conducted when 77% of events had been observed, was
consistent with the primary analysis.
Eribulin (n = 508)Median 13.2 mo
HR, 0.805; 95% CI 0.677, 0.958; nominal P = .014
FIGURE 2 EMBRACE: Median OS was 13.2 months in the eribulinarm vs 10.6 months in the TPC group. TPC � treatment of physi-cian’s choice. Courtesy of Christopher Twelves, MD.
resulted in discontinuation of � 1% of patients. Periph-
MMUNITY ONCOLOGY � May 2012
eral neuropathy was the most common adverse eventleading to discontinuation from eribulin (5%); for thosewho developed grade 3/4 peripheral neuropathy but con-tinued treatment, this improved to grade 2 or better inlater cycles following delays and dose reductions. Asthe-nia/fatigue occurred at a similar level with eribulin (grade3, 8%; grade 4, 1%) and TPC (grade 3, 10%; no grade 4).
Ongoing trials involving eribulin mesylate in the treat-ment of metastatic breast cancer include a phase III studyof eribulin vs capecitabine as second-line therapy withcoprimary endpoints of PFS and OS,44 a phase II study oferibulin vs ixabepilone with a primary endpoint of rates ofoccurrence of peripheral neuropathy,45 and a phase Ib/IItrial of eribulin in combination with capecitabine.46 Ac-cording to the NCCN Breast Cancer Guidelines, eribulinis listed as a “preferred” single agent for the treatment ofwomen with recurrent or metastatic breast cancer.16
ConclusionsThe FDA-approved single agents, capecitabine, ixabepi-lone, and eribulin, and the combination of capecitabinewith ixabepilone, represent advances in the treatment ofpatients with heavily pretreated metastatic breast cancer.In phase II studies, overall response rates ranged from9%-32% for capecitabine, 12%-42% for ixabepilone, and9.3%-12% for eribulin. In these studies, the most com-mon nonhematologic grade 3/4 adverse effects for thesingle agents are hand-foot syndrome and diarrhea forcapecitabine; peripheral neuropathy and asthenia/fatiguefor ixabepilone; and asthenia/fatigue and peripheral neu-ropathy for eribulin.
A pivotal phase III trial of capecitabine plus ixabepi-lone compared to capecitabine alone, with PFS as theprimary endpoint, did not show improved OS (12.9months, P � .19), but median PFS was superior (5.8months, P � .0003); a confirmatory trial, with OS as theprimary endpoint, had similar findings. By contrast, in theEMBRACE study, eribulin significantly improved OS(13.1 months, P � .041 in the initial analysis; 13.2months, P � .014 in updated analysis) compared withTPC with benefit also in PFS (3.7 months, P � .14 [byindependent review] or 3.6 months, P � .002 [by inves-tigator review]).
In the setting of prior exposure to an anthracycline anda taxane, the EMBRACE trial for the first time presentsevidence of increased survival in women treated witheribulin compared with the “real-world” TPC, which in-cluded agents typically used in the metastatic breast can-cer setting. These data will help guide treatment selection,which is based on many factors, including prior therapies,
toxicities, performance status, and patient preference.www.globalacademycme.com/oncology

Twelves & Fornier
AcknowledgmentsWriting assistance was provided by Debra Hughes. The authors retainedfull editorial control of the manuscript.
References1. Murphy CG, Seidman AD. Evolving approaches to metastatic
breast cancer previously treated with anthracyclines and taxanes. ClinBreast Cancer. 2009;9(Suppl 2):S58-S65.
2. O’Shaughnessy JA, Blum J, Moiseyenko V, et al. Randomized,open-label, phase II trial of oral capecitabine (Xeloda®) vs. a referencearm of intravenous CMF (cyclophosphamide, methotrexate and 5-flu-orouracil) as first-line therapy for advanced/metastatic breast cancer.Ann Oncol. 2001;12(9):1247-54.
3. Oostendorp LJM, Stalmeier PFM, Donders AR, et al. Efficacyand safety of palliative chemotherapy for patients with advanced breastcancer pretreated with anthracyclines and taxanes: a systematic review.Lancet Oncol. 2011;12(11):1053-61.
4. Lemieux J, Maunsell E, Provencher L. Chemotherapy-inducedalopecia and effects on quality of life among women with breast cancer:a literature review. Psycho-Oncology. 2008;17(4):217-28.
5. Blum JL, Jones SE, Buzdar AU, et al. Multicenter phase II studyof capecitabine in paclitaxel-refractory metastatic breast cancer. J ClinOncol. 1999;17(2):485-93.
6. Blum JL, Dieras V, Lo Russo PM, et al. Multicenter, Phase IIstudy of capecitabine in taxane-pretreated metastatic breast carcinomapatients. Cancer. 2001;92(7):1759-68.
7. Reichardt P, Von Minckwitz G, Thuss-Patience PC, et al. Mul-ticenter phase II study of oral capecitabine (Xeloda®) in patients withmetastatic breast cancer relapsing after treatment with a taxane-contain-ing therapy. Ann Oncol. 2003;14(8):1227-33.
8. Fumoleau P, Largillier R, Clippe C, et al. Multicentre, phase IIstudy evaluating capecitabine monotherapy in patients with anthracy-cline- and taxane-pretreated metastatic breast cancer. Eur J Cancer.2004;40(4):536-42.
9. Lee SH, Lee J, Park J, et al. Capecitabine monotherapy in patientswith anthracycline- and taxane-pretreated metastatic breast cancer. MedOncol. 2004;21(3):223-31.
10. Cameron D, Casey M, Press M, et al. A phase III randomizedcomparison of lapatinib plus capecitabine versus capecitabine alone inwomen with advanced breast cancer that has progressed on trastuzumab:updated efficacy and biomarker analysis. Breast Cancer Res Treat. 2008;112(3):533-43.
11. Thomas ES, Gomez HL, Li RK, et al. Ixabepilone plus cape-citabine for metastatic breast cancer progressing after anthracycline andtaxane treatment. J Clin Oncol. 2007;25(33):5210-17.
12. Miller KD, Chap LI, Holmes FA, et al. Randomized phase IIItrial of capecitabine compared with bevacizumab plus capecitabine inpatients with previously treated breast cancer. J Clin Oncol. 2005;23(4):792-9.
13. Lin PC, Wang WS, Yang MH, et al. Sequential therapy withcapecitabine followed by vinorelbine/cisplatin in patients with anthra-cycline/taxane-refractory metastatic breast cancer. J Chin Med Assoc.2006;69(7):304-9.
14. Pajk B, Cufer T, Canney P, et al. Anti-tumor activity of cape-citabine and vinorelbine in patients with anthracycline- and taxane-pretreated metastatic breast cancer: findings from the EORTC 10001randomized phase II trial. Breast. 2008;17(2):180-5.
15. Haller DG, Cassidy J, Clarke SJ, et al. Potential regional differ-ences for the tolerability profile of fluoropyrimidines. J Clin Oncol.2008;26(13):2118-23.
16. National Comprehensive Cancer Network. NCCN ClinicalPractice Guidelines in Oncology™: Breast Cancer. V.2.2011. Availableat: http://www.nccn.org. Accessed February 8, 2012.
17. Bajetta E, Procopio G, Celio L, et al. Safety and efficacy of twodifferent doses of capecitabine in the treatment of advanced breastcancer in older women. J Clin Oncol. 2005;23(10):2155-61.
18. Traina TA, Theodoulou M, Feigin K, et al. Phase I study of a
novel capecitabine schedule based on the Norton-Simon mathematicalVolume 9/Number 5S
model in patients with metastatic breast cancer. J Clin Oncol.2008;26(11):1797-802.
19. Morris PG, Fornier MN. Microtubule active agents: beyond thetaxane frontier. Clin Cancer Res. 2008;14(22):7167-72.
20. Roché HH, Sparano J, Valero V, et al. Ixabepilone (Ixa) andcapecitabine (C) in patients (pts) with triple-negative breast cancer(TNBC): a retrospective analysis of phase 2 and phase 3 clinical studies[abstract 299P]. Ann Oncol. 2010;21(Suppl 8):viii103.
21. Perez E, Lerzo G, Pivot X, et al. Efficacy and safety of ixabepi-lone (BMS-247550) in a phase II study of patients with advanced breastcancer resistant to an anthracycline, a taxane, and capecitabine. J ClinOncol. 2007;25(23):3407-14.
22. Roché H, Yelle L, Cognetti F, et al. Phase II clinical trial ofixabepilone (BMS-247550), an epothilone B analog, as first-line therapyin patients with metastatic breast cancer previously treated with anthra-cycline chemotherapy. J Clin Oncol. 2007;25(23):3415-20.
23. Thomas E, Tabernero J, Fornier M, et al. Phase II clinical trialof ixabepilone (BMS-247550), an epothilone B analog, in patients withtaxane-resistant metastatic breast cancer. J Clin Oncol. 2007;25(23):3399-406.
24. U.S. Food and Drug Administration. Available at: www.accessdata.fda.gov/scripts/cder/drugsatfda/. Accessed February 6, 2012.
25. Hortobagyi GN, Gomez HL, Li RK, et al. Analysis of overallsurvival from a phase III study of ixabepilone plus capecitabine versuscapecitabine in patients with MBC resistant to anthracyclines and tax-anes. Breast Cancer Res Treat. 2010;122(2):409-18.
26. Sparano JA, Vrdoljak E, Rixe O, et al. Randomized phase IIItrial of ixabepilone plus capecitabine versus capecitabine in patients withmetastatic breast cancer previously treated with an anthracycline and ataxane. J Clin Oncol. 2010;28(20):3256-63.
27. Swain SM, Arezzo J. Neuropathy associated with microtubuleinhibitors: diagnosis, incidence and management. Clin Adv HematolOncol. 2008;6(6):455-67.
28. Vadhat LT, Thomas E, Roche H, et al. Ixabepilone (Ixa)-associated peripheral neuropathy (PN): retrospective review of data fromphase II and III clinical trials [abstract 320P]. Ann Oncol. 2010;21(Suppl8):viii.
29. Roché H, Conte P, Perez EA, et al. Ixabepilone plus capecit-abine in metastatic breast cancer patients with reduced performancestatus previously treated with anthracyclines and taxanes: a pooled anal-ysis by performance status of efficacy and safety data from 2 phase IIIstudies. Breast Cancer Res Treat. 2011;125:755-65.
30. Towle MJ, Salvato KA, Wels BF, et al. Eribulin induces irre-versible mitotic blockade: implications of cell-based pharmacodynamicsfor in vivo efficacy and intermittent dosing conditions. Cancer Res.2011;71:496-505.
31. Kuznetsov G, TenDyke K, Yu MJ, Littlefield B. Antiprolifera-tive effects of halichondrin B analog eribulin mesylate (E7389) againstpaclitaxel-resistant human cancer cells in vitro [abstract C58]. Presentedat: AACR-NCI-EORTC International Conference: Molecular Targetsand Cancer Therapeutics; October 22-26, 2007; San Francisco, CA.Available at: http://www.aacrmeetingabstracts.org/cgi/content/meeting_abstract/2007/3_Molecular_Targets_Meeting/C58?maxtoshow�&hits�10&RESULTFORMAT�&author1�Kuznetsov&andorexactfulltext�and&searchid�1&FIRSTINDEX�0&sortspec�relevance&resourcetype�HWCIT. Accessed February 15, 2012.
32. Desai KK, Goel S, Mita A, et al. Dose escalation and pharma-cokinetic (pk) study of E7389, a microtubule-binding drug in patients(pts) with advanced solid tumors [abstract 3090]. J Clin Oncol. 2005;23(Suppl):214s.
33. Rubin EH, Rosen L, Rajeev V, et al. Phase I study of E7389administered by 1 hour infusion every 21 days [abstract 2054]. J ClinOncol. 2005;23(Suppl):148s.
34. Synold TW, Morgan RJ, Newman EM, et al. A phase I phar-macokinetic and target validation study of the novel anti-tubulin agentE7389: a California Cancer consortium trial [abstract 3036]. J ClinOncol. 2005;23(Suppl):200s.
35. Vahdat LT, Pruitt B, Fabian CJ, et al. Phase II study of eribulinmesylate, a halichondrin B analog, in patients with metastatic breast
May 2012 � COMMUNITY ONCOLOGY S11

Review
S12 CO
cancer previously treated with an anthracycline and a taxane. J ClinOncol. 2009;27(18):2954-61.
36. Cortes J, Vahdat L, Blum JL, et al. Phase II study of thehalichondrin B analog eribulin mesylate in patients with locally ad-vanced or metastatic breast cancer previously treated with an anthracy-cline, a taxane, and capecitabine. J Clin Oncol. 2010;28(25):3922-8.
37. Aogi K, Iwata H, Masuda N, et al. A phase II study of eribulinin Japanese patients with heavily pretreated metastatic breast cancer.Ann Oncol. 2011 [Epub ahead of print].
38. Cortes J, O’Shaughnessy J, Loesch D, et al. Eribulin mono-therapy versus treatment of physician’s choice in patients with metastaticbreast cancer (EMBRACE): a phase 3 open-label randomised study.Lancet. 2011;377(9769):914-23.
39. Eribulin [package insert]. Woodcliff Lake, NJ: Eisai Inc; 2011.40. Twelves C, Loesch D, Blum J, et al. Updated survival analysis of
a phase III study (EMBRACE) of eribulin mesylate versus treatment ofphysicians’ choice in subjects with locally recurrent metastatic breastcancer previously treated with an anthracycline and a taxane. Presentedat: 33rd San Antonio Breast Cancer Symposium; December 8-12, 2010;San Antonio, TX. Abstract P6-14-18.
41. Twelves C, Akerele C, Wanders J, et al; Study 305 investigators.
Eribulin mesylate (E7389) vs treatment of physician’s choice (TPC) inpatients (pts) with metastatic breast cancer (MBC): subgroup analysesMMUNITY ONCOLOGY � May 2012
from the EMBRACE study [abstract 275O]. Ann Oncol. 2010;21(Suppl8);viii96.
42. Twelves C, Vahdat LT, Cortes J, et al. The relationship betweenage and survival outcomes for eribulin in metastatic breast cancer [ab-stract 1060]. J Clin Oncol. 2011;29:(Suppl).
43. Blum JL, Twelves CJ, Akerele C, et al. Impact of the number ofprior chemotherapy regimens on overall survival (OS) among subjectswith locally recurrent or metastatic breast cancer treated with eribulinmesylate: results from the phase III EMBRACE study. Presented at:33rd San Antonio Breast Cancer Symposium; December 8-12, 2010;San Antonio, TX. Abstract P6-13-01.
44. Twelves C, Cortes J, Vahdat LT, et al. Phase III trials of eribulinmesylate (E7389) in extensively pretreated patients with locally recur-rent or metastatic breast cancer. Clin Breast Cancer. 2010;10(2):160-3.
45. NCT00879086. A phase II, multicenter, randomized, open-labelstudy comparing eribulin mesylate and ixabepilone in causing or exac-erbating neuropathy in patients with advanced breast cancer. Availableat: www.Clinicaltrials.gov. Accessed February 6, 2012.
46. NCT01323530. A phase Ib/2, multicenter, randomized, open-label, dose-escalation and confirmation study of eribulin in combination
with capecitabine. Available at: www.Clinicaltrials.gov. Accessed Feb-ruary 6, 2012.www.globalacademycme.com/oncology
Review
Choosing chemotherapy for patients withmetastatic breast cancer previously exposedto taxanes and anthracyclines: other agentsChristopher J. Twelves, MD, MB ChB, FRCP, RCPS,1 and Monica N. Fornier, MD2
1Professor of Clinical Pharmacology and Oncology, Lead, Experimental Cancer Medicine Center, University of Leeds &St James’s Institute of Oncology, Leeds, United Kingdom; 2Assistant Member at the Breast Cancer Medicine Service ofMemorial Sloan-Kettering Cancer Center, Assistant Professor at the Weill Medical College of Cornell University, New York
Presbyterian Hospital, New York, NYVolume 9/Numbe
Many options exist for the treatment ofpatients with heavily pretreated meta-static breast cancer. In addition to the 3
agents—capecitabine, ixabepilone (single agent andwith capecitabine), and eribulin mesylate (discussedin the previous article)—approved by the US Foodand Drug Administration (FDA) for use in patientswith metastatic breast cancer previously treated witha taxane and an anthracycline, a number of otheragents have shown efficacy in this population. Thesecytotoxic agents include vinorelbine, gemcitabine,pegylated liposomal doxorubicin, nab-paclitaxel,pemetrexed, irinotecan, and platinum salts (ie, car-boplatin, cisplatin).* Of these single agents, onlygemcitabine and nab-paclitaxel are FDA-approvedfor use in patients with breast cancer, although nei-ther is specifically indicated for the treatment ofwomen with metastatic breast cancer and prior ex-posure to both an anthracycline and a taxane.1-8
Lack of a standard of care and the wide varietyof cytotoxic options used in the treatment ofwomen with heavily pretreated metastatic breastcancer are well illustrated by the control arm of theEisai Metastatic Breast Cancer Study AssessingPhysician’s Choice versus E7389 (EMBRACE)trial, which evaluated single-agent eribulin vs thesingle-agent choice of the treating physician.9 In
*All of the agents discussed herein are used off-label for treat-ment of patients with metastatic breast cancer previouslytreated with anthracyclines and taxanes.
Correspondence to: Christopher J. Twelves, MD, MB ChB,FRCP, RCPS, Level 4, Bexley Wing, St James’s UniversityHospital, Beckett Street, Leeds LS9 7TF, UK. Phone: �44 (0)113 20 68186 (e-mail: [email protected]).Disclosures: Dr Fornier has nothing to disclose. Dr Twelveshas received grant research support from Roche. He has alsobeen a consultant for Eisai Inc. and Roche and a speaker for
Eisai Inc.r 5S
the treatment of physician’s choice (TPC) arm ofthe study, vinorelbine, gemcitabine, taxanes, an-thracyclines, and other chemotherapies were ad-ministered to 25%, 19%, 15%, 10%, and 10% ofpatients, respectively. While all these agents orclasses of agents have demonstrated activity asfirst-line treatment for metastatic breast cancer,the data for patients with prior exposure to bothan anthracycline and a taxane are less robust.
A recent systematic review evaluated efficacyand safety data from phase II and phase III clinicalstudies of the single agents, capecitabine, gemcit-abine, vinorelbine, and liposomal doxorubicin inthe setting of heavily pretreated breast cancer.10 Acritical criterion for inclusion in the review wasthat at least 80% of patients enrolled in the studyhad previous exposure to both an anthracyclineand a taxane. The agents and studies included inthis systematic review as well as additional agents/studies also meeting this inclusion criterion are thefocus of this article. Despite inclusion in the sys-tematic analysis of Oostendorp et al,10 data on theefficacy and safety of some of these agents, par-ticularly gemcitabine and liposomal doxorubicin,in the setting of heavily pretreated metastaticbreast cancer are limited, with evidence morescarce for agents not included in the systematicreview. Also mentioned here are studies of otheragents that are often used in the setting of heavilypretreated breast cancer, but do not meet the strictinclusion criterion regarding pretreatment history.Hence, the lower level of evidence for the use ofthese latter cytotoxic therapies, especially as singleagents, in the setting of anthracycline/taxane-pretreated metastatic breast cancer is emphasized.
Commun Oncol 2012;9:S13-S19 © 2012 Elsevier Inc. All rights reserved.doi:10.1016/j.cmonc.2012.03.003
May 2012 � COMMUNITY ONCOLOGY S13

Review
S14 CO
Single-agents studied in the setting of prioranthracycline- and taxane-exposedmetastatic breast cancerGemcitabineGemcitabine, an analogue of cytidine, is an antimetabo-lite prodrug that is activated through intracellular phos-phorylation and involved in the inhibition of DNA syn-thesis.11 Three phase II studies of gemcitabine in patientswith anthracycline- and taxane-resistant breast cancer re-ported response rates of 17% to 22.6% at doses of 800 to1,000 mg/m2 days 1, 8, and 15 every 28 days.12-14 How-ever, in another phase II study of this population, the overallresponse rate was 0% following administration of gemcit-abine at a 1,200 mg/m2 dose on the same schedule, althoughthe disease-control rate and median time to progression(TTP) were 26% and 1.9 months, respectively.15
In a systematic review including 3 of these studies,13-15
weighted mean values for disease-control rate (ie, overallresponse rate plus stable disease rate) and overall survival(OS) were 35% and 9.8 months, respectively.10 Seriousnausea and/or vomiting were reported in 14% of patientsin 1 study15 and serious fatigue in 5%-9% of patients in 2studies.14,15 Rates of grade 3/4 neutropenia ranged from12%-18%. Although guidelines from the National Com-prehensive Cancer Network (NCCN) list gemcitabine asa “preferred” single agent for the treatment of recurrent ormetastatic breast cancer,16 the authors of the systematicreview “found only limited evidence for the effectivenessof gemcitabine” in this specific setting.10
VinorelbineVinorelbine is an antimicrotubule agent that interferes incellular replication by causing abnormalities in microtu-bule formation, although its mechanism of action is dis-tinct from other agents, such as the taxanes, which targetmicrotubules.17 In 9 clinical studies of single-agent vi-norelbine conducted in patients with advanced breast can-cer pretreated with an anthracycline and a taxane, overallresponse rates were 13%-35%.10,18-26 Representative re-sults were observed in the most recently conducted studywhere vinorelbine was administered at a dose of 25 mg/m2
on days 1, 8, 15, and 22 every 4 weeks to 26 patientspreviously treated with anthracyclines and taxanes.18 Theoverall response rate, median TTP, and median OS were20.8%, 3.7 months, and 10.4 months, respectively.
In a systematic review of all 9 studies, weighted meanvalues for disease-control rate and OS were 49% and 12.6months, respectively.10 Serious fatigue was reported in13% of patients in 1 study25 and 16% of patients werereported to experience serious alopecia in another.26 Highrates of grade 3/4 neutropenia (eg, � 50%) have been
reported. According to guidelines from the NCCN, vi-MMUNITY ONCOLOGY � May 2012
norelbine is listed as a “preferred” single agent for thetreatment of recurrent or metastatic breast cancer.16
PemetrexedPemetrexed is an antifolate metabolite that interferes withthe synthesis of DNA and RNA by interfering with thenucleotide synthesis.27 Two phase II studies of pemetrexedin patients with refractory metastatic breast cancer con-ducted in the past decade have shown overall response ratesof 8% to 9% at a dose of 500 mg/m2 every 3 weeks,28,29 withmanageable toxicities including fatigue, dyspnea, anorexia,nausea, chest pain, and grade 3/4 neutropenia.17
O’Shaughnessy et al enrolled 80 patients with meta-static breast cancer previously treated with � 3 regimenscontaining anthracyclines, taxanes, and capecitabine andadministered intravenous pemetrexed 500 mg/m2 on day1 of a 21-day cycle. Following a protocol amendment, 60patients received concurrent folic acid and vitamin B12
supplements to minimize toxicity related to pemetrexed.Overall response rate was 8% and stable disease, 36%.Median TTP was 2.9 months, and median OS, 8.2months. Grade 3/4 toxicities were primarily hematologic;grade 4 neutropenia occurred in 10% of patients, andgrade 3 neutropenia and leukopenia in 29% and 21% ofpatients, respectively. The effect of supplementation ontoxicity was not clear.28
Another study of pemetrexed 500 mg/m2 administeredas a 10-minute intravenous infusion on day 1 every 21days in 79 patients who had experienced progressive dis-ease following treatment with anthracycline and a taxanehad a response rate of 9%; 43 received folic acid andvitamin B12 supplementation. A median of 4 cycles wasadministered. The median duration of response was 5.5months. Median PFS was 3.1 months, and median sur-vival was 10.5 months. Grade 3/4 toxicities included neu-tropenia (36.4%). Toxicity appeared to be amelioratedwith vitamin supplementation.29
Taxane or anthracycline retreatment inpatients with metastatic breast cancerpreviously exposed to an anthracyclineand a taxaneAlthough many patients with early-stage breast cancerreceive adjuvant anthracycline/taxane-based chemother-apy, evidence is limited for rechallenging those patientswho experience a prolonged disease-free survival intervalfollowing completion of adjuvant chemotherapy with 1 orboth of these agents following diagnosis of metastaticdisease.30 Most of the available data are from single-center cohort studies, or subgroup analyses and retrospec-tive reviews of phase III studies. Only 1 phase III trial
examined the strategy of anthracycline rechallenge, andwww.globalacademycme.com/oncology

Twelves & Fornier
nearly all of the patients in that study were not “heavily-pretreated” as the majority had not received prior cyto-toxic therapy for advanced disease.31 Nevertheless, thecumulative dose of anthracycline in standard adjuvantchemotherapy regimens is below the 450-550 mg/m2 and800-900 mg/m2 for doxorubicin and epirubicin, respec-tively,32,33 and liposomal anthracycline formulations areassociated with a reduced risk of cardiotoxicity.34 Poten-tial options for rechallenge with a taxane include using thesame agent, a different member of the drug class, or analternative formulation such as albumin-bound paclitaxel,with the caveat that cumulative toxicity may be an issue.
Pegylated liposomal doxorubicinThe mechanisms of action of pegylated liposomal doxo-rubicin and conventional doxorubicin are the same; theyboth interfere with DNA replication through multipleprocesses, including DNA intercalation and inhibition ofthe enzyme topoisomerase II.35,36 The encapsulation ofconventional doxorubicin in a polyethylene glycol (pegy-lated) liposomal formulation was developed to improvethe therapeutic index of doxorubicin. Uptake of this agentby the reticuloendothelial system is impaired and theserum half-life of the drug is prolonged. Pegylated lipo-somal doxorubicin is less cardiotoxic than conventionaldoxorubicin.34 Due to wider tissue distribution, this for-mulation is associated with lower rates of myelotoxicity,alopecia, and gastrointestinal toxicity, although rates ofhand-foot syndrome and mucositis are increased.
Keller et al conducted a phase III study in which 301women with advanced breast cancer were randomly as-signed to 1 of 3 treatment arms: pegylated liposomaldoxorubicin (50 mg/m2 every 28 days); vinorelbine (30mg/m2 weekly); or mitomycin C (10 mg/m2 day 1 andevery 28 days) plus vinblastine (5 mg/m2 day 1, 14, 28,and 42) every 6 to 8 weeks. One hundred fifty patientsreceived pegylated liposomal doxorubicin. All patients inthe study had been previously treated with a taxane and83% of patients had prior exposure to an anthracy-cline.10,37 Disease-control rate, median PFS, and medianOS for patients in the pegylated liposomal doxorubicinarm were 10%, 2.9 months, and 10.4 months, respec-tively. Similar PFS and OS results were observed forpatients in the comparator arm (ie, patients receivingvinorelbine or mitomycin plus vinblastine). The toxicityprofile of pegylated liposomal doxorubicin in this studyincluded an increased incidence of nausea, vomiting, fa-tigue, hand-foot syndrome, and stomatitis. According toguidelines from the NCCN, pegylated liposomal doxoru-bicin is listed as a “preferred” single agent for the treat-ment of recurrent or metastatic breast cancer.16 Never-
theless, the authors of the systematic review “found onlyVolume 9/Number 5S
limited evidence for the effectiveness of liposomal doxo-rubicin” in this specific setting.10
nab-PaclitaxelThe mechanism of action of nab-paclitaxel is the same aspaclitaxel; it interferes with cellular replication by stabi-lizing microtubules.17 However, in the nab-paclitaxel for-mulation, paclitaxel is coated with nanoparticles of albu-min to increase its solubility and enhance its delivery tothe tumor. Compared with the conventional formulationof paclitaxel, nab-paclitaxel is solvent-free and has ashorter infusion time.38 Blum et al conducted a phase IIstudy involving nab-paclitaxel 100 mg/m2 days 1, 8, and15 every 28 days in 106 women with metastatic breastcancer who had undergone a median of 3 prior regimens(range, 0-7) whose disease had progressed during treat-ment with taxanes or had relapsed within 12 months ofadjuvant taxane therapy. Seventy-five percent of thesepatients had received an anthracycline in the adjuvantsetting. Objective partial responses were observed in 14%of patients, and stable disease of at least 16 weeks induration was observed in 12%. Median PFS was 3 monthsand median OS, 9.2 months. Survival probability at 12months was 39%. Rate of OS was similar in those whoresponded or had stable disease.38
Nab-paclitaxel was well tolerated without steroids orgranulocyte colony-stimulating factor prophylaxis. Grade3 neutropenia occurred in 14% of patients and grade 4,4%. Grade 3 sensory neuropathy was observed in 8% ofpatients. For those who developed treatment-limiting pe-ripheral neuropathy, a treatment delay of 1-2 weeks wasrecommended prior to reinitiating treatment with nab-paclitaxel at a reduced dose.38 Other reported adverseevents included fatigue, nausea, and alopecia. According toguidelines from the NCCN, nab-paclitaxel is listed as a“preferred” single agent for the treatment of recurrent ormetastatic breast cancer.16
Other single agents studied in the setting ofheavily pretreated metastatic breast cancerIrinotecanIrinotecan is an inhibitor of topoisomerase I, an enzymeinvolved in the cleavage and resealing of DNA strandsduring the DNA replication process.39 To assess the ef-ficacy and tolerability of 2 schedules of irinotecan, womenwith metastatic breast cancer whose disease had pro-gressed after 1 to 3 chemotherapy regimens were random-ized in a multicenter phase II study to 100 mg/m2 for 4weeks followed by a 2-week rest (n � 52; the “weekly”arm) or 240 mg/m2 every 3 weeks (n � 51, the “every-3-weeks” arm), both in 6-week cycles.40 In this study,
approximately 60% of patients received prior treatmentMay 2012 � COMMUNITY ONCOLOGY S15
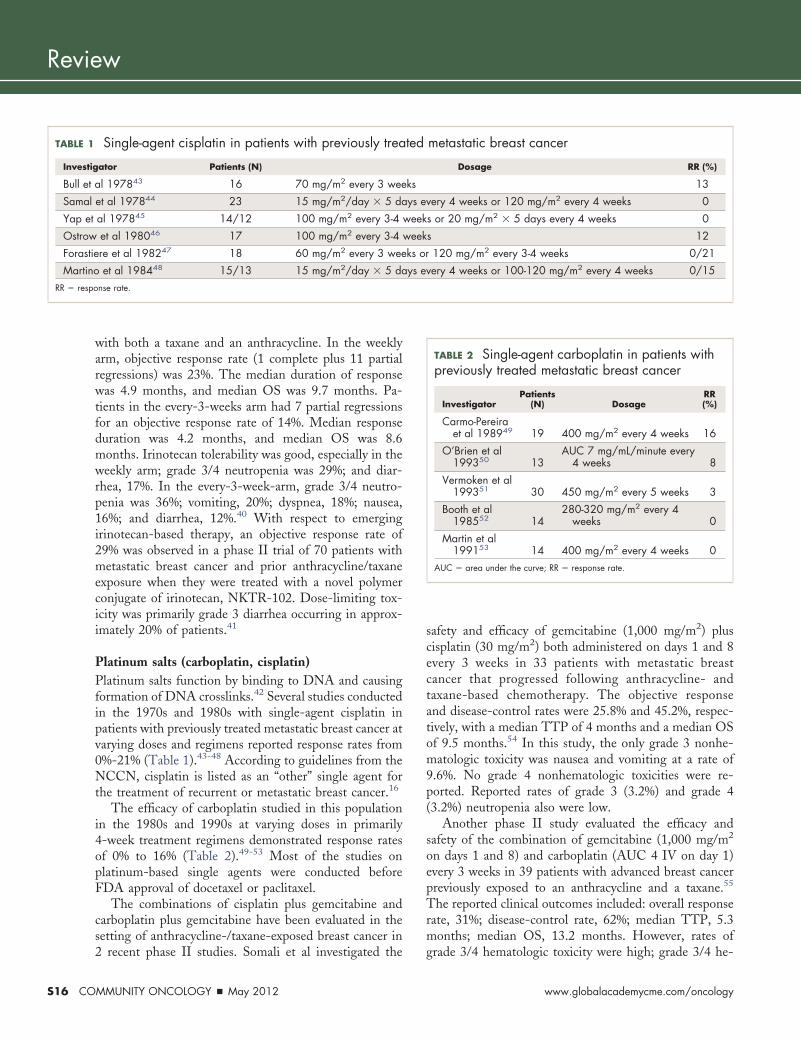
Review
S16 CO
with both a taxane and an anthracycline. In the weeklyarm, objective response rate (1 complete plus 11 partialregressions) was 23%. The median duration of responsewas 4.9 months, and median OS was 9.7 months. Pa-tients in the every-3-weeks arm had 7 partial regressionsfor an objective response rate of 14%. Median responseduration was 4.2 months, and median OS was 8.6months. Irinotecan tolerability was good, especially in theweekly arm; grade 3/4 neutropenia was 29%; and diar-rhea, 17%. In the every-3-week-arm, grade 3/4 neutro-penia was 36%; vomiting, 20%; dyspnea, 18%; nausea,16%; and diarrhea, 12%.40 With respect to emergingirinotecan-based therapy, an objective response rate of29% was observed in a phase II trial of 70 patients withmetastatic breast cancer and prior anthracycline/taxaneexposure when they were treated with a novel polymerconjugate of irinotecan, NKTR-102. Dose-limiting tox-icity was primarily grade 3 diarrhea occurring in approx-imately 20% of patients.41
Platinum salts (carboplatin, cisplatin)Platinum salts function by binding to DNA and causingformation of DNA crosslinks.42 Several studies conductedin the 1970s and 1980s with single-agent cisplatin inpatients with previously treated metastatic breast cancer atvarying doses and regimens reported response rates from0%-21% (Table 1).43-48 According to guidelines from theNCCN, cisplatin is listed as an “other” single agent forthe treatment of recurrent or metastatic breast cancer.16
The efficacy of carboplatin studied in this populationin the 1980s and 1990s at varying doses in primarily4-week treatment regimens demonstrated response ratesof 0% to 16% (Table 2).49-53 Most of the studies onplatinum-based single agents were conducted beforeFDA approval of docetaxel or paclitaxel.
The combinations of cisplatin plus gemcitabine andcarboplatin plus gemcitabine have been evaluated in thesetting of anthracycline-/taxane-exposed breast cancer in
Single-agent cisplatin in patients with previously trea
ator Patients (N)
al 197843 16 70 mg/m2 every 3 wee
et al 197844 23 15 mg/m2/day � 5 da
al 197845 14/12 100 mg/m2 every 3-4
et al 198046 17 100 mg/m2 every 3-4
re et al 198247 18 60 mg/m2 every 3 wee
et al 198448 15/13 15 mg/m2/day � 5 danse rate.
2 recent phase II studies. Somali et al investigated the
MMUNITY ONCOLOGY � May 2012
safety and efficacy of gemcitabine (1,000 mg/m2) pluscisplatin (30 mg/m2) both administered on days 1 and 8every 3 weeks in 33 patients with metastatic breastcancer that progressed following anthracycline- andtaxane-based chemotherapy. The objective responseand disease-control rates were 25.8% and 45.2%, respec-tively, with a median TTP of 4 months and a median OSof 9.5 months.54 In this study, the only grade 3 nonhe-matologic toxicity was nausea and vomiting at a rate of9.6%. No grade 4 nonhematologic toxicities were re-ported. Reported rates of grade 3 (3.2%) and grade 4(3.2%) neutropenia also were low.
Another phase II study evaluated the efficacy andsafety of the combination of gemcitabine (1,000 mg/m2
on days 1 and 8) and carboplatin (AUC 4 IV on day 1)every 3 weeks in 39 patients with advanced breast cancerpreviously exposed to an anthracycline and a taxane.55
The reported clinical outcomes included: overall responserate, 31%; disease-control rate, 62%; median TTP, 5.3months; median OS, 13.2 months. However, rates of
metastatic breast cancer
Dosage RR (%)
13
very 4 weeks or 120 mg/m2 every 4 weeks 0
s or 20 mg/m2 � 5 days every 4 weeks 0
s 12
120 mg/m2 every 3-4 weeks 0/21
very 4 weeks or 100-120 mg/m2 every 4 weeks 0/15
TABLE 2 Single-agent carboplatin in patients withpreviously treated metastatic breast cancer
InvestigatorPatients
(N) DosageRR(%)
Carmo-Pereiraet al 198949 19 400 mg/m2 every 4 weeks 16
O’Brien et al199350 13
AUC 7 mg/mL/minute every4 weeks 8
Vermoken et al199351 30 450 mg/m2 every 5 weeks 3
Booth et al198552 14
280-320 mg/m2 every 4weeks 0
Martin et al199153 14 400 mg/m2 every 4 weeks 0
AUC � area under the curve; RR � response rate.
TABLE 1 ted
Investig
Bull et ks
Samal ys e
Yap et week
Ostrow week
Forastie ks or
Martino ys eRR � respo
grade 3/4 hematologic toxicity were high; grade 3/4 he-
www.globalacademycme.com/oncology
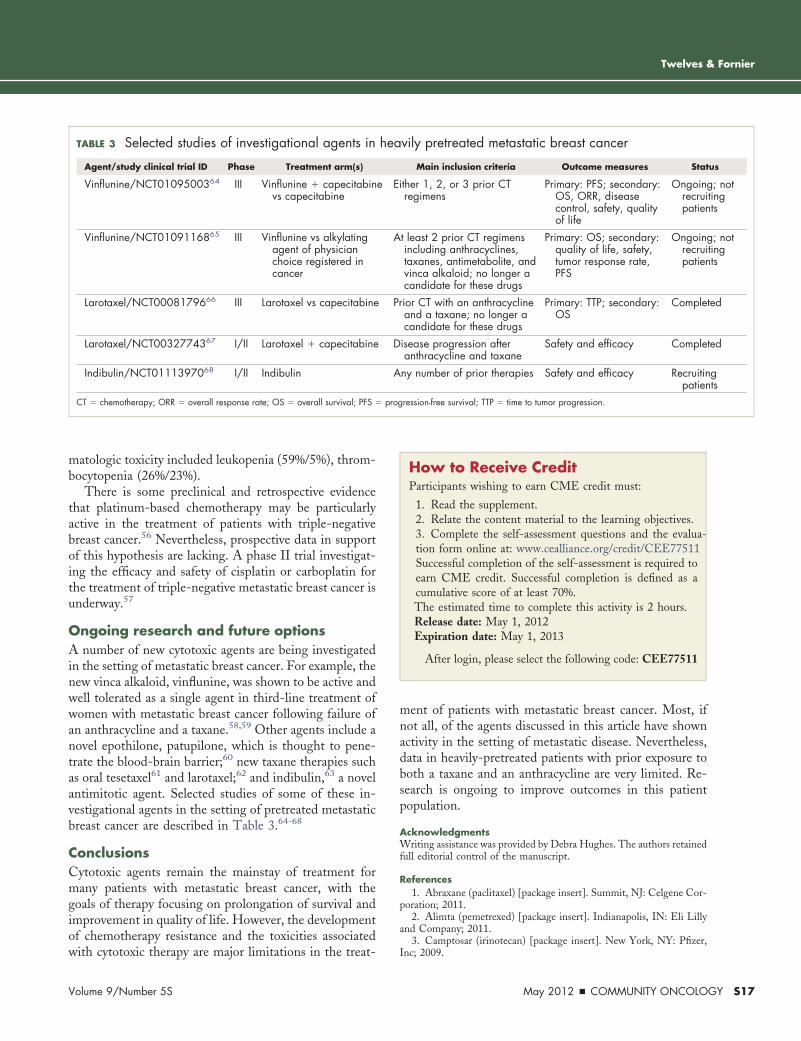
Twelves & Fornier
matologic toxicity included leukopenia (59%/5%), throm-bocytopenia (26%/23%).
There is some preclinical and retrospective evidencethat platinum-based chemotherapy may be particularlyactive in the treatment of patients with triple-negativebreast cancer.56 Nevertheless, prospective data in supportof this hypothesis are lacking. A phase II trial investigat-ing the efficacy and safety of cisplatin or carboplatin forthe treatment of triple-negative metastatic breast cancer isunderway.57
Ongoing research and future optionsA number of new cytotoxic agents are being investigatedin the setting of metastatic breast cancer. For example, thenew vinca alkaloid, vinflunine, was shown to be active andwell tolerated as a single agent in third-line treatment ofwomen with metastatic breast cancer following failure ofan anthracycline and a taxane.58,59 Other agents include anovel epothilone, patupilone, which is thought to pene-trate the blood-brain barrier;60 new taxane therapies suchas oral tesetaxel61 and larotaxel;62 and indibulin,63 a novelantimitotic agent. Selected studies of some of these in-vestigational agents in the setting of pretreated metastaticbreast cancer are described in Table 3.64-68
ConclusionsCytotoxic agents remain the mainstay of treatment formany patients with metastatic breast cancer, with thegoals of therapy focusing on prolongation of survival andimprovement in quality of life. However, the developmentof chemotherapy resistance and the toxicities associated
TABLE 3 Selected studies of investigational agents in
Agent/study clinical trial ID Phase Treatment arm(s)
Vinflunine/NCT0109500364 III Vinflunine � capecitabinvs capecitabine
Vinflunine/NCT0109116865 III Vinflunine vs alkylatingagent of physicianchoice registered incancer
Larotaxel/NCT0008179666 III Larotaxel vs capecitabine
Larotaxel/NCT0032774367 I/II Larotaxel � capecitabine
Indibulin/NCT0111397068 I/II Indibulin
CT � chemotherapy; ORR � overall response rate; OS � overall survival; PFS �
with cytotoxic therapy are major limitations in the treat-
Volume 9/Number 5S
ment of patients with metastatic breast cancer. Most, ifnot all, of the agents discussed in this article have shownactivity in the setting of metastatic disease. Nevertheless,data in heavily-pretreated patients with prior exposure toboth a taxane and an anthracycline are very limited. Re-search is ongoing to improve outcomes in this patientpopulation.
AcknowledgmentsWriting assistance was provided by Debra Hughes. The authors retainedfull editorial control of the manuscript.
References1. Abraxane (paclitaxel) [package insert]. Summit, NJ: Celgene Cor-
poration; 2011.2. Alimta (pemetrexed) [package insert]. Indianapolis, IN: Eli Lilly
and Company; 2011.3. Camptosar (irinotecan) [package insert]. New York, NY: Pfizer,
vily pretreated metastatic breast cancer
Main inclusion criteria Outcome measures Stat
ither 1, 2, or 3 prior CTregimens
Primary: PFS; secondary:OS, ORR, diseasecontrol, safety, qualityof life
Ongoingrecruipatien
t least 2 prior CT regimensincluding anthracyclines,taxanes, antimetabolite, andvinca alkaloid; no longer acandidate for these drugs
Primary: OS; secondary:quality of life, safety,tumor response rate,PFS
Ongoingrecruipatien
ior CT with an anthracyclineand a taxane; no longer acandidate for these drugs
Primary: TTP; secondary:OS
Complet
isease progression afteranthracycline and taxane
Safety and efficacy Complet
ny number of prior therapies Safety and efficacy Recruitinpatien
ression-free survival; TTP � time to tumor progression.
How to Receive CreditParticipants wishing to earn CME credit must:
1. Read the supplement.2. Relate the content material to the learning objectives.3. Complete the self-assessment questions and the evalua-tion form online at: www.cealliance.org/credit/CEE77511Successful completion of the self-assessment is required toearn CME credit. Successful completion is defined as acumulative score of at least 70%.The estimated time to complete this activity is 2 hours.Release date: May 1, 2012Expiration date: May 1, 2013
After login, please select the following code: CEE77511
hea
us
e E ; nottingts
A ; nottingts
Pr ed
D ed
A gts
prog
Inc; 2009.
May 2012 � COMMUNITY ONCOLOGY S17
Review
S18 CO
4. Carboplatin [package insert]. Sellersville, PA: Teva Pharmaceu-ticals USA; 2011.
5. Doxil (doxorubicin) [package insert]. Raritan, NJ: Ortho BiotechProducts, LP; 2008.
6. Gemzar (gemcitabine) [package insert]. Indianapolis, IN: Eli Lillyand Company; 2010.
7. Navalbine (vinorelbine) [package insert]. Research Triangle Park,NC: GlaxoSmithKline; 2002.
8. Platinol (cisplatin) [package insert]. Princeton, NJ: Bristol-MyersSquibb Company; 2010.
9. Cortes J, O’Shaughnessy J, Loesch D, et al. Eribulin monotherapyversus treatment of physician’s choice in patients with metastatic breastcancer (EMBRACE). A phase 3 open-label randomized study. Lancet.2011;377(9769):914-23.
10. Oostendorp LJM, Stalmeier PFM, Donders AR, et al. Efficacyand safety of palliative chemotherapy for patients with advanced breastcancer pretreated with anthracyclines and taxanes: a systematic review.Lancet Oncol. 2011;12(11):1053-61.
11. Mini E, Nobili S, Caciagli B, Landini I, Mazzei T. Cellularpharmacology of gemcitabine. Ann Oncol. 2006;17(Suppl 5):v7-12.
12. Valerio MR, Cicero G, Armata MG, et al. Gemcitabine (G) inpretreated breast cancer (BC) [abstract 1953]. Proc Am Soc Clin Oncol.2001;20
13. Rha SY, Moon YH, Jeung HC, et al. Gemcitabine monotherapyas salvage chemotherapy in heavily pretreated metastatic breast cancer.Breast Cancer Res Treat. 2005;90(3):215-221.
14. Modi S, Currie VE, Seidman AD, et al. A phase II trial ofgemcitabine in patients with metastatic breast cancer previously treatedwith an anthracycline and taxane. Clin Breast Cancer. 2005;6(1):55-60.
15. Smorenburg CH, Bontenbal M, Seynaeve C, et al. Phase II studyof weekly gemcitabine in patients with metastatic breast cancer relapsingor failing both an anthracycline and a taxane. Breast Cancer Res Treat.2001;66(1):83-7.
16. National Comprehensive Cancer Network. NCCN ClinicalPractice Guidelines in OncologyTM: Breast Cancer. V.2.2011. Availableat: http://www.nccn.org. Accessed February 8, 2012.
17. Murphy CG, Seidman AD. Evolving approaches to metastaticbreast cancer previously treated with anthracyclines and taxanes. ClinBreast Cancer. 2009;9(Suppl 2):S58-65.
18. Seo HY, Lee HJ, Woo OH, et al. Phase II study of vinorelbinemonotherapy in anthracycline and taxane pre-treated metastatic breastcancer. Invest New Drug. 2011;29(2):360-5.
19. Papaldo P, Fabi A, Ferretti G, et al. A phase II study onmetastatic breast cancer patients treated with weekly vinorelbine with orwithout trastuzumab according to HER2 expression: changing the nat-ural history of HER2-positive disease. Ann Oncol. 2006;17(4):630-6.
20. Toi M, Saeki T, Aogi K, et al. Late phase II clinical study ofvinorelbine monotherapy in advanced or recurrent breast cancer previ-ously treated with anthracyclines and taxanes. Jpn J Clin Oncol. 2005;35(6):310-5.
21. Jara-Sánchez C, Martín M, García-Sáenz JA, et al. Vinorelbineas a 96-hour continuous infusion in heavily pretreated patients withmetastatic breast cancer: a cooperative study by the GEICAM group.Clin Breast Cancer. 2003;3(6):399-404.
22. Zelek L, Barthier S, Riofrio M, et al. Weekly vinorelbine is aneffective palliative regimen after failure with anthracyclines and taxanesin metastatic breast carcinoma. Cancer. 2001;92(9):2267-72.
23. Udom DI, Vigushin DM, Linardou H, et al. Two weekly vi-norelbine: administration in patients who have received at least two priorchemotherapy regimes for advanced breast cancer. Eur J Cancer. 2000;36(2):177-82.
24. Livingston RB, Ellis GK, Gralow JR, et al. Dose-intensivevinorelbine with concurrent granulocyte colony-stimulating factor sup-port in paclitaxel-refractory metastatic breast cancer. J Clin Oncol. 1997;15(4):1395-400.
25. Pajk B, Cufer T, Canney P, et al. Anti-tumor activity of cape-citabine and vinorelbine in patients with anthracycline- and taxane-
pretreated metastatic breast cancer: findings from the EORTC 10001randomized phase II trial. Breast. 2008;17(2):180-5.MMUNITY ONCOLOGY � May 2012
26. Martín M, Ruiz A, Muñoz M, et al. Gemcitabine plus vinore-lbine versus vinorelbine monotherapy in patients with metastatic breastcancer previously treated with anthracyclines and taxanes: final results ofthe phase III Spanish Breast Cancer Research Group (GEICAM) trial.Lancet Oncol. 2007;8(3):219-25.
27. Shih C, Habeck LL, Mendelsohn LG, et al. Multiple folateenzyme inhibition: mechanism of a novel pyrrolopyrimidine-based an-tifolate LY-231514 (MTA). Adv Enzyme Regul. 1998;38:135-52.
28. O’Shaughnessy J, Clark RS, Blum JL, et al. Phase II study ofpemetrexed in patients pretreated with an anthracycline, a taxane, andcapecitabine for advanced breast cancer. Clin Breast Cancer. 2005;6(2):143-9.
29. Llombart-Cussac A, Theodoulou M, Rowland K, et al. Pem-etrexed in patients with locally advanced or metastatic breast cancer whohad received previous anthracycline and taxane treatment: phase IIstudy. Clin Breast Cancer. 2006;7(5):380-5.
30. Palmieri C, Krell J, James CR, et al. Rechallenging with anthra-cyclines and taxanes in metastatic breast cancer. Nat Rev Clin Oncol.2010;7(10):561-74.
31. Sparano JA, Makhson AN, Semiglazov VF, et al. Pegylatedliposomal doxorubicin plus docetaxel significantly improves time toprogression without additive cardiotoxicity compared with docetaxelmonotherapy in patients with advanced breast cancer previously treatedwith neoadjuvant-adjuvant anthracycline therapy: results from a ran-domized phase III trial. J Clin Oncol. 2009;27(27):4522-9.
32. Ryberg M, Nielsen D, Skovsgaard T, et al. Cardiotoxicity: ananalysis of 469 patients with metastatic breast cancer. J Clin Oncol.1998;16(11):710-7.
33. Von Hoff D, Layard MW, Basa P, et al. Risk factors fordoxorubicin-induced congestive heart failure. Ann Intern Med. 1979;91(5):710-1.
34. Coleman RE, Biganzoli L, Canney P, et al. A randomized phaseII study of two different schedules of pegylated liposomal doxorubicin inmetastatic breast cancer (EORTC-10993). Eur J Cancer. 2006;42(7):882-7.
35. Furlan RL, Garrido LM, Brumatti G, et al. A rapid and sensitivemethod for the screening of DNA intercalating antibiotics. Biotech Lett.2002;24:1807-13.
36. Pommier Y, Leo E, Zhang H, Marchand C. DNA topoisom-erases and their poisoning by anticancer and antibacterial drugs. ChemBiol. 2010;17(5):421-33.
37. Keller AM, Mennel RG, Georgoulias VA, et al. Randomizedphase III trial of pegylated liposomal doxorubicin versus vinorelbine ormitomycin C plus vinblastine in women with taxane-refractory advancedbreast cancer. J Clin Oncol. 2004;22(19):3893-901.
38. Blum JL, Savin MA, Edelman G, et al. Phase II study of weeklyalbumin-bound paclitaxel for patients with metastatic breast cancerheavily pretreated with taxanes. Clin Breast Cancer. 2007;7(11):850-6.
39. Xu Y, Shapiro CL. Rationale for mitomycin and irinotecanuse in advanced breast cancer. Oncology (Williston Park). 2003;17(5Suppl 5):25-28.
40. Perez EA, Hillman DW, Mailliard JA, et al. Randomized phaseII study of two irinotecan schedules for patients with metastatic breastcancer refractory to an anthracycline, a taxane, or both. J Clin Oncol.2004 Jul 15;22(14):2849-55.
41. Awada A, Chan S, Jerusalem G, et al. Significant efficacy in aphase 2 study of NKTR-102, a novel polymer conjugate of irinotecan, inpatients with pre-treated metastatic breast cancer (MBC) [abstract P6-11-01]. Presented at: 33rd Annual San Antonio Breast Cancer Sympo-sium; December 8-12, 2010; San Antonio, TX.
42. Gonzalez VM, Fuertes MA, Alonso C, Perez JM. Is cisplatin-induced cell death always produced by apoptosis? Mol Pharmacol. 2001;59(4):657-63.
43. Bull T, Anderson ME, Lippmann JG. A phase II trial of cis-dichlorodiammine platinum II in breast and ovarian carcinomas. ProcAm Assoc Cancer Res. 1978;19:Abstract 345.
44. Samal B, Vaitheviclus V, Singlekowenia A. Cis-diamminedi-
chloroplatinum (CDDP) in advanced breast and colorectal carcinoma[abstract 164]. Proc Am Soc Clin Oncol. 1978;19:347.www.globalacademycme.com/oncology
Twelves & Fornier
45. Yap HY, Salem P, Hortobagyi GN, et al. Phase II study ofcis-dichlorodiammineplatinum(II) in advanced breast cancer. CancerTreat Rep. 1978;62(3):405-8.
46. Ostrow S, Egorin M, Aisner J, et al. High-dose cis-diamminedichloroplatinum therapy in patients with advanced breastcancer: pharmacokinetics, toxicity, and therapeutic efficacy. Cancer ClinTrials. 1980 Spring;3(1):23-7.
47. Forastiere AA, Hakes TB, Wittes JT, et al. Cisplatin in thetreatment of metastatic breast carcinoma. A prospective randomizedtrial of two dosage schedules. Am J Clin Oncol. 1982;5(3):243-7.
48. Martino S, Samal BA, Singhakowinta A, et al. A phase II studyof cis-diamminedichloroplatinum II for advanced breast cancer. J CancerRes Clin Oncol. 1984;108(3):354-6.
49. Carmo-Pereira J, Olivera-Costa F, Henriquez E, et al. Carbo-platin as primary chemotherapy for disseminated breast carcinoma: Aphase II study [abstract P0971]. Presented at: 5th European Conferenceon Clinical Oncology; September 3-7, 1989; London, UK. 8:43.
50. O’Brien ME, Talbot DC, Smith IE. Carboplatin in the treat-ment of advanced breast cancer: a phase II study using pharmacokineti-cally guided dose schedule. J Clin Oncol. 1993;11(11):2112-7.
51. Vermoken JB, Gundersen S, Clavel M, et al. Randomized phaseII trial of iproplatin and carboplatin in advanced breast cancer. TheEORTC Early Clinical Trials Group and the EORTC data center. AnnOncol. 1993;4(4):303-306.
52. Booth BW, Weiss RB, Korzun AH, et al. Phase II trial ofcarboplatin in advanced breast carcinoma: a Cancer and LeukemiaGroup B Study. Cancer Treat Rep. 1985;69(7-8):919-20.
53. Martin M, Diaz-Rubio E, Casado A, et al. Phase II study ofcarboplatin in advanced breast cancer: preliminary results. Semin Oncol.1991;18(1 Suppl 2):23-7.
54. Somali I, Alacacioglu A, Tarhan MO, et al. Cisplatin plusgemcitabine chemotherapy in taxane/anthracycline-resistant metastaticbreast cancer. Chemotherapy. 2009;55(3):155-60.
55. Laessig D, Stemmler HJ, Vehling-Kaiser U, et al. Gemcitabineand carboplatin in intensively pretreated patients with metastatic breastcancer. Oncology. 2007;73(5-6):407-14.
56. Sirohi B, Arnedos M, Popat S, et al. Platinum-based chemo-
therapy in triple-negative breast cancer. Ann Oncol. 2008 Nov;19(11):1847-52.Volume 9/Number 5S
57. NCT00483223. A Phase II study of cisplatin or carboplatin fortriple-negative metastatic breast cancer and evaluation of p63/p73 as abiomarker of response. Available at: www.Clinicaltrials.gov. AccessedFebruary 8, 2012.
58. Fumoleau P, Cortes-Funes H, Taleb AB, et al. Phase 2 study ofsingle-agent IV vinflunine as third-line treatment of metastatic breastcancer after failure of anthracycline-/taxane-based chemotherapy. Am JClin Oncol. 2009 [Epub ahead of print].
59. Ng JS. Vinflunine: review of a new vinca alkaloid and its poten-tial role in oncology. J Oncol Pharm Pract. 2011;17(3):209-24.
60. Bystricky B, Chau I. Patupilone in cancer treatment. Expert OpinInvestig Drugs. 2011;20(1):107-17.
61. Saif MW, Sarantopoulos J, Patnaik A, et al. Testaxel, a new oraltaxane, in combination with capecitabine: a phase I, dose-escalationstudy in patients with advanced solid tumors. Cancer Chemother Phar-macol. 2011;68(6):1565-73.
62. Metzger-Filho O, Moulin C, de Azambuja E, Ahmad A. La-rotaxel: broadening the road with new taxanes. Expert Opin InvestigDrugs. 2009;18(8):1183-9.
63. Wienecke A, Bacher G. Indibulin, a novel microtubule inhibitor,discriminates between mature neuronal and nonneuronal tubulin. CancerRes. 2009;69(1):171-7.
64. NCT01095003. Trial of vinflunine plus capecitabine in advancedbreast cancer. Available at: www.Clinicaltrials.gov. Accessed February 8,2012.
65. NCT01091168. Trial of vinflunine versus alkylating agent inmetastatic breast cancer. Available at: www.Clinicaltrials.gov. AccessedFebruary 8, 2012.
66. NCT00081796. Breast cancer trial of RPR109881 versus cape-citabine in male or female patients with advanced breast cancer. Avail-able at: www.Clinicaltrials.gov. Accessed February 8, 2012.
67. NCT00327743. Combination study of a new taxane and cape-citabine in patients with metastatic breast cancer. Available at: www.Clinicaltrials.gov. Accessed February 8, 2012.
68. NCT01113970. Study of a novel indibulin dosing schedule for the
treatment of metastatic breast cancer. Available at: www.Clinicaltrials.gov.Accessed February 8, 2012.May 2012 � COMMUNITY ONCOLOGY S19
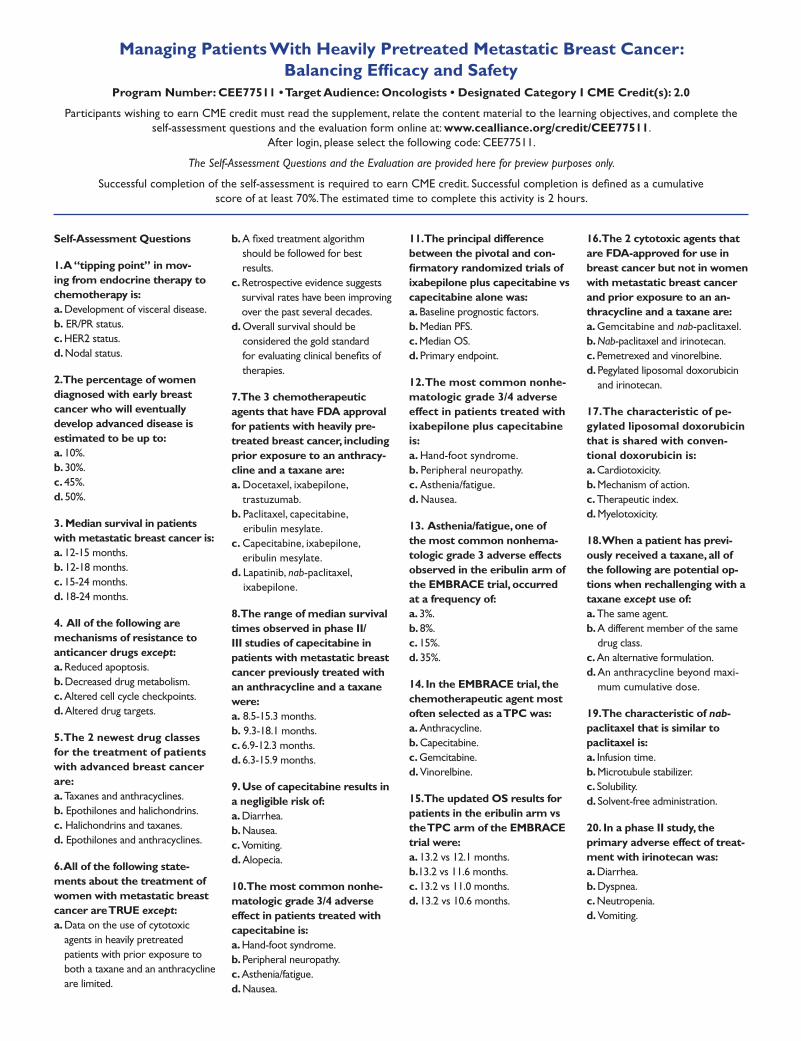
Self-Assessment Questions
1. A “tipping point” in mov-ing from endocrine therapy to chemotherapy is: a. Development of visceral disease. b. ER/PR status. c. HER2 status. d. Nodal status.
2. The percentage of women diagnosed with early breast cancer who will eventually develop advanced disease is estimated to be up to: a. 10%. b. 30%. c. 45%. d. 50%.
3. Median survival in patients with metastatic breast cancer is: a. 12-15 months. b. 12-18 months. c. 15-24 months. d. 18-24 months.
4. All of the following are mechanisms of resistance to anticancer drugs except: a. Reduced apoptosis. b. Decreased drug metabolism. c. Altered cell cycle checkpoints. d. Altered drug targets.
5. The 2 newest drug classes for the treatment of patients with advanced breast cancer are: a. Taxanes and anthracyclines. b. Epothilones and halichondrins. c. Halichondrins and taxanes. d. Epothilones and anthracyclines.
6. All of the following state-ments about the treatment of women with metastatic breast cancer are TRUE except: a. Data on the use of cytotoxic
agents in heavily pretreated patients with prior exposure to both a taxane and an anthracycline are limited.
b. should be followed for best results.
c. Retrospective evidence suggests survival rates have been improving over the past several decades.
d. Overall survival should be considered the gold standard
therapies.
7. The 3 chemotherapeutic agents that have FDA approval for patients with heavily pre-treated breast cancer, including prior exposure to an anthracy-cline and a taxane are: a. Docetaxel, ixabepilone,
trastuzumab.b. Paclitaxel, capecitabine,
eribulin mesylate.c. Capecitabine, ixabepilone,
eribulin mesylate. d. Lapatinib, nab-paclitaxel,
ixabepilone.
8. The range of median survival times observed in phase II/III studies of capecitabine in patients with metastatic breast cancer previously treated with an anthracycline and a taxane were: a. 8.5-15.3 months. b. 9.3-18.1 months. c. 6.9-12.3 months. d. 6.3-15.9 months.
9. Use of capecitabine results in a negligible risk of: a. Diarrhea. b. Nausea. c. Vomiting. d. Alopecia.
10. The most common nonhe-matologic grade 3/4 adverse effect in patients treated with capecitabine is: a. Hand-foot syndrome. b. Peripheral neuropathy. c. Asthenia/fatigue. d. Nausea.
11. The principal difference between the pivotal and con-firmatory randomized trials of ixabepilone plus capecitabine vs capecitabine alone was: a. Baseline prognostic factors. b. Median PFS. c. Median OS. d. Primary endpoint.
12. The most common nonhe-matologic grade 3/4 adverse effect in patients treated with ixabepilone plus capecitabine is: a. Hand-foot syndrome. b. Peripheral neuropathy. c. Asthenia/fatigue. d. Nausea.
13. Asthenia/fatigue, one of the most common nonhema-tologic grade 3 adverse effects observed in the eribulin arm of the EMBRACE trial, occurred at a frequency of: a. 3%. b. 8%. c. 15%. d. 35%.
14. In the EMBRACE trial, the chemotherapeutic agent most often selected as a TPC was: a. Anthracycline. b. Capecitabine. c. Gemcitabine. d. Vinorelbine.
15. The updated OS results for patients in the eribulin arm vs the TPC arm of the EMBRACE trial were: a. 13.2 vs 12.1 months. b.13.2 vs 11.6 months. c. 13.2 vs 11.0 months. d. 13.2 vs 10.6 months.
16. The 2 cytotoxic agents that are FDA-approved for use in breast cancer but not in women with metastatic breast cancer and prior exposure to an an-thracycline and a taxane are: a. Gemcitabine and nab-paclitaxel. b. Nab-paclitaxel and irinotecan. c. Pemetrexed and vinorelbine.d. Pegylated liposomal doxorubicin
and irinotecan.
17. The characteristic of pe-gylated liposomal doxorubicin that is shared with conven-tional doxorubicin is: a. Cardiotoxicity. b. Mechanism of action. c. Therapeutic index. d. Myelotoxicity.
18. When a patient has previ-ously received a taxane, all of the following are potential op-tions when rechallenging with a taxane except use of: a. The same agent. b. A different member of the same
drug class.c. An alternative formulation.d. An anthracycline beyond maxi-
mum cumulative dose.
19. The characteristic of nab-paclitaxel that is similar to paclitaxel is: a. Infusion time. b. Microtubule stabilizer. c. Solubility. d. Solvent-free administration.
20. In a phase II study, the primary adverse effect of treat-ment with irinotecan was: a. Diarrhea. b. Dyspnea. c. Neutropenia. d. Vomiting.
Managing Patients With Heavily Pretreated Metastatic Breast Cancer: Balancing Efficacy and Safety
Participants wishing to earn CME credit must read the supplement, relate the content material to the learning objectives, and complete the self-assessment questions and the evaluation form online at: www.cealliance.org/credit/CEE77511.
After login, please select the following code: CEE77511.
The Self-Assessment Questions and the Evaluation are provided here for preview purposes only.
score of at least 70%. The estimated time to complete this activity is 2 hours.

EVALUATION
1. As a result of this session, I am better able to: a. Discuss the approaches to the treatment of heavily pre-
treated metastatic breast cancer, including sequential versus combination chemotherapy.
(5 = Strongly Agree, 1 = Strongly Disagree) 5 4 3 2 1
agents and combinations for the treatment of patients with heavily pretreated metastatic breast cancer.
(5 = Strongly Agree, 1 = Strongly Disagree) 5 4 3 2 1
c. Devise evidence-based treatment plans for patients with advanced breast cancer that has progressed following treat-ment with taxanes and anthracyclines.
(5 = Strongly Agree, 1 = Strongly Disagree) 5 4 3 2 1
2. The objectives were related to the purpose of the activity. (5 = Stongly Agree, 1 = Strongly Disagree) 5 4 3 2 1
3. The content of this learning activity was clearly written.
(5 = Strongly Agree, 1 = Strongly Disagree) 5 4 3 2 1
4. Did you perceive any commercial bias in this activity? Yes No
If you answered Yes for Question 4, please explain:
5. My level of knowledge about managing patients with heavily pretreated breast cancer prior to this activity was adequate. (5 = Strongly Agree, 1 = Strongly Disagree) 5 4 3 2 1
6. My level of knowledge about managing patients with heavily pretreated breast cancer was enhanced by this activity. (5 = Strongly Agree, 1 = Strongly Disagree) 5 4 3 2 1
7. My overall competence in managing patients with heavily pre-treated breast cancer prior to this activity was adequate. (5 = Strongly Agree, 1 = Strongly Disagree) 5 4 3 2 1
8. My overall competence in managing patients with heavily pre-
treated breast cancer was enhanced by this activity. (5 = Strongly Agree, 1 = Strongly Disagree) 5 4 3 2 1
9. I would recommend this activity to others. Yes No
If you answered No for Question 9, please explain:
10. This activity will assist in the improvement of my (check all that apply):
Competence Performance Patient outcomes
11. I plan to make changes to my clinical practice as a result of this activity. Yes No
Yes. Please give 1 example:
No. Please explain:
12. If you answered Yes to Question 11, what is your level of
commitment to making the changes stated above? Very committed Somewhat committed Not very committed
13. What are the barriers you face in your current practice set-ting that may impact patient outcomes? (check all that apply)
Lack of evidence-based guidelines Guidelines not applicable to my current practice/patients Lack of time Organizational/institutional
Patient adherence Treatment-related adverse events Other
If Other, please explain:
14. Please rank each of the educational formats below in order of preference from 1 (highest) to 8 (lowest).
Association Meetings Grand Rounds Home Study (CD-ROM) Home Study (printed) Internet-Based Case Studies Symposia Teleconferences Webinars
15. Please indicate topics for future activities:
I certify that I have completed this activity and the actual time I spent was:1.5 hours 2.0 hours 2.5 hours