Embed Size (px)
Citation preview

Management of Inverted Papilloma of the Temporal Bone1Nicholas Rowan, BS; 1Evelyne Kalyoussef, MD; 2,3James K. Liu, MD, and 1,3Robert W. Jyung, MD
Contact Information:Evelyne Kalyoussef, [email protected]
1Department of Otolaryngology – Head & Neck Surgery, University of Medicine and Dentistry of New Jersey – New Jersey Medical School, Newark, NJ2Department of Neurological Surgery, University of Medicine and Dentistry of New Jersey – New Jersey Medical School, Newark, NJ3Center for Skull Base and Pituitary Surgery, Neurological Institute of New Jersey, University of Medicine and Dentistry of New Jersey – New Jersey Medical School, Newark, NJ
Objective:1.Understand the clinical presentation, etiology, and histopathology of inverting papilloma of the temporal bone2.Discuss current treatment and management of inverting papilloma of the temporal bone as well as considerations for future management
Methods: Inverted papilloma (IP), a benign neoplasm typically arising within the sinonasal tract, has rarely been reported to occur outside the sinonasal tract. Only seventeen cases of temporal bone IP have been reported. We reviewed our two cases of temporal bone IP and discuss their management.
Results: Our first case was a patient with a history of sinonasal IP who had undergone three previous endoscopic resections when she presented with a subepithelial mass extending from the posterior wall of the ear canal . She was found to have extensive bony destruction and underwent a retrolabyrinthine approach with tympanomastoid obliteration. Recurrence was monitored with baseline and follow‐up PET‐CT scans. The second case was a primary lesion with an atypical otoscopic appearance of a granular mass extending from the middle ear through a tympanic membrane perforation. This was managed with a tympanomastoidectomy and clinically followed for recurrence.
Conclusion:Temporal bone IP is a rare neoplasm with no definitive treatment algorithm. We recommend aggressive surgical resection with close postoperative follow‐up. PET‐CT may be useful for identifying multicentric disease at presentation or for early identification of recurrent disease. HPV detection may identify IPs at risk for multicentric or recurrent disease.
Abstract
IntroductionInverted papilloma is a benign neoplasm arising from ectodermally derived sinonasal mucosa of the lateral nasal wall. Although benign, inverted papillomas are often locally aggressive, multicentric, and can be associated with bony destruction and extension into the paranasal sinuses, orbits and anterior skull base. Rarely, inverted papillomas arise at extra‐sinonasal tract sites including the pharynx, lacrimal sac, and temporal bone. Only 18 cases involving the temporal bone, including primary and secondary disease, have been reported since 1987.1‐14 We present two additional cases of extra‐sinonasal disease and an overview of their clinical presentation and surgical management. Furthermore, we review the role of HPV screening in extra‐sinonasal disease and discuss the potential for baseline screening.
Case PresentationsCase #1: A 49‐year‐old woman with a past history of sinonasal inverted papilloma status post three endoscopic resections presented with an eight month history of progressive right‐sided hearing loss. She further reported right sided otorrhea, tinnitus, aural fullness, vertigo, and new onset right‐sided facial twitching. Physical examination revealed right‐sided facial myoclonus, facial nerve paresis (House Brackmann Scale II/VI) and a bluish, blanching mass protruding from the posterior external auditory canal anteriorly, completely obstructing visualization of the tympanic membrane.
CT Scan of the Temporal Bone and MRI (Figures 1&2) demonstrated an expansile mass filling the middle ear cavity with bony erosion of the external auditory canal and the intratemporal facial nerve.
The patient underwent a right radical mastoidectomy and decompression of the facial nerve with tympanomastoid obliteration using abdominal fat. Gross total resection was achieved. The patient did well postoperatively with complete return of facial nerve function. Post‐operative CT Temporal Bone, MRI and PET/CT were negative for persistent or recurrent disease.
Case #2: A 76‐year‐old man with a fifteen‐year smoking history was referred for evaluation of right‐sided chronic otitis media. The patient reported a two year history of decreased hearing and tinnitus in his right ear but denied otalgia, otorrhea, vertigo, trauma, or prior otologic surgery.
Microscopic examination of the right ear revealed a small posterior perforation of the tympanic membrane, through which there was extension of polyploid tissue with adjacent neovascularization. An audiogram demonstrated a moderately severe to profound mixed hearing loss with 88% discrimination on the side of the lesion. A CT scan was obtained (Figure 3) demonstrating soft tissue density filling the middle ear cavity. The patient underwent a tympanomastoidectomy and final pathology was consistent with inverted papilloma. A flexible fiberoptic exam failed to reveal intranasal disease or other potential sites of primary disease.The patient did well post‐operatively and was clinically free of disease on physical exam and on repeat CT scan one year post‐operatively.
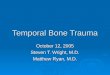
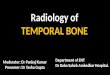
Figure 2. (A) Preoperative Axial T1 with gadolinium MRI Scan Patient #1 demonstrating a 2.8 cm x 2.5 cm x 2.6 cm soft expansile mass involving the right mastoid air cells and extending into the middle ear. (B) Postoperative Axial T1 with gadolinium MRI demonstrating no evidence of residual tumor with tympanomastoid obliteration.
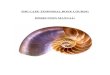
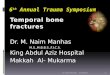
Figure 1. Axial Bone Window (A) and Coronal Soft Tissue Window (B) CT Scan of the Temporal Bone of Patient #1 demonstrating 2.8 cm x 2.5 cm x 2.6 cm soft expansile mass involving the right mastoid cavity. The green arrow demonstrates the mass extending from the external auditory canal (EAC) into the middle ear cavity. The blue arrow demonstrates bony dehiscence of the facial nerve and posterior EAC wall destruction while the red arrow demonstrates destruction of the posterior cranial fossa plate.
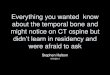
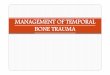
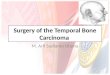
Figure 3. Axial Bone Window (A) and Coronal Bone Window (B) CT Scan of the Temporal Bone of Patient #2 with soft tissue filling the middle ear and surrounding the ossicles.
Conclusions
References
Despite the exceedingly rare presentation of inverted papilloma of the temporal bone, we recommend patients with sinonasal inverting papilloma and otologic complaints undergo work‐up for possible temporal bone involvement. We recommend aggressive surgical resection and PET‐CT for identifying multicentric disease at presentation as well as for follow‐up and early identification of recurrent disease. In regards to HPV detection, the virus’ role remains unclear, however, given the increasing incidence of HPV + related head and neck cancers, we recommend both ISH and PCR analysis in order to increase chance of detection.
DiscussionInverted papillomas (IP) are a well‐defined group of benign neoplasms typically arising within the sinonasal tract but only 18 cases of temporal bone involvement have been reported.1‐13 There are several hypotheses regarding etiology. The first is transmission of primary disease through the eustachian tube to the middle ear1 however recurrent disease at the primary site or contiguous spread of disease has never been shown. A second hypothesis suggests that possible ectopic foci of Schneiderian mucosa, a result of an error during embryological development, are the root cause.4 A third hypothesis proposes a genetic predisposition to account for the disease’s predilection for multicentricity.6 Another proposal suggests influence of progesterone receptors in rapid growth of IP of the temporal2 although in both of our reported cases immunostains for progesterone receptors were negative.
Current literature suggests an association between human papilloma virus (HPV) and IP, however only two cases of the eighteen reported temporal bone cases have shown definite HPV involvement.12, 17‐20 One hypothesis is a “hit and run” phenomenon in which HPV may be the inciting event of transformation, but is not necessary for maintenance of the neoplastic changes.21 Another author suggested a difference in sensitivity for HPV detection between polymerase chain reaction (PCR) and in situ hybridization (ISH),12 however, there is conflicting data on which technique is superior.21 Neither of the cases we report stained positive for HPV types 6, 11, 16, and 18 by ISH.
The clinical presentation of IP of the temporal bone is varied. While IP of the sinonasal tract predominantly affects men, IP of the temporal bone occur with a female‐male ratio of 2:1.13 Of the eighteen cases reported, ten were found to be primary disease. In addition to Case #2 above, six of these previously reported cases were associated with chronic otitis media with complaints of hearing loss in the affected ear.6,9
There is an 82% risk of recurrence in the middle ear if adequate margins are not achieved and thus aggressive surgical resection is the preferred method of treatment. 1, 2,11,22‐24 In addition to resection, postoperative radiation therapy has been previously discussed as an option foraggressive lesions of the temporal bone however there is a lack of evidence to support its efficacy.9
Literature regarding post‐surgical surveillance for recurrent disease is scant. In a study of four patients with positron emission tomography‐computed tomography (PET‐CT) scanning, F‐18‐fluorodeoxyglucose (18FDG) avidity was a reliable indicator of the presence of recurrent disease. Two other studies with small sample sizes showed a potential role for PET‐CT in differentiating benign sinonasal inverting papillomas from those with coexistent malignancy.26,27 In one of our reported cases, PET‐CT displayed 18FDG avidity at the site of tumor recurrence, suggesting that PET‐CT may in fact be an appropriate test for surveillance of extra‐sinonasal disease, however lack of supporting data prompts further investigation of the subject.
1. Stone, D.M., et al., Inverted papilloma of the middle ear and mastoid. Otolaryngol Head Neck Surg, 1987. 97(4): p. 416-8.2.Seshul, M.J., et al., Nasal inverted papilloma with involvement of middle ear and mastoid. Arch Otolaryngol Head Neck Surg, 1995. 121(9): p. 1045-8.3.Chhetri, D.K., et al., Pathology forum. Quiz case 2. Schneiderian-type papilloma of the middle ear. Arch Otolaryngol Head Neck Surg, 2001. 127(1): p. 79, 80-2.4.Kaddour, H.S. and C.J. Woodhead, Transitional papilloma of the middle ear. J Laryngol Otol, 1992. 106(7): p. 628-9.5.Roberts, W.H., D.L. Dinges, and M.G. Hanly, Inverted papilloma of the middle ear. Ann Otol Rhinol LarMyngol, 1993. 102(11): p. 890-2.6.Wenig, B.M., Schneiderian-type mucosal papillomas of the middle ear and mastoid. Ann Otol Rhinol Laryngol, 1996. 105(3): p. 226-33.7.Bold, E.L., et al., Adenomatous lesions of the temporal bone immunohistochemical analysis and theories of histogenesis. Am J Otol, 1995. 16(2): p. 146-52.8.Jones, M.E., et al., Clinical and molecular pathology of aggressive Schneiderian papilloma involving the temporal bone. Head Neck, 1998. 20(1): p. 83-8.9.Pou, A.M. and J.T. Vrabec, Inverting papilloma of the temporal bone. Laryngoscope, 2002. 112(1): p. 140-2.10.Altug, T., O. Sunar, and H. Bilgin, [Inverted papilloma. Apropos of a multicentric case]. Rev Laryngol Otol Rhinol (Bord), 1989. 110(3): p. 299-301.11.de Filippis, C., et al., Primary inverted papilloma of the middle ear and mastoid. Otol Neurotol, 2002. 23(4): p. 555-9.12.Marioni, G., et al., Detection of human papillomavirus in temporal bone inverted papilloma by polymerase chain reaction. Acta Otolaryngol, 2003. 123(3): p. 367-71.13.Blandamura, S., et al., Temporal bone and sinonasal inverted papilloma: the same pathological entity? Arch Otolaryngol Head Neck Surg, 2003. 129(5): p. 553-6.14.Kainuma, K., et al., Inverted papilloma of the middle ear: a case report and review of the literature. Acta Otolaryngol, 2011. 131(2): p. 216-20.15.Hyams, V.J., Papillomas of the nasal cavity and paranasal sinuses. A clinicopathological study of 315 cases. Ann Otol Rhinol Laryngol, 1971. 80(2): p. 192-206.16.Ferlito, A., K.O. Devaney, and A. Rinaldo, Association between Schneiderian papilloma of the temporal bone and carcinoma: a critical review of the literature. Acta Otolaryngol, 2004. 124(2): p. 121-3.17.Cheung, F.M., et al., Schneiderian papillomas and carcinomas: A retrospective study with special reference to p53 and p16 tumor suppressor gene expression and association with HPV. Ear Nose Throat J, 2010. 89(10): p. E5-E12.18.Katori, H., A. Nozawat, and M. Tsukuda, Relationship between p21 and p53 expression, human papilloma virus infection and malignant transformation in sinonasal-inverted papilloma. Clin Oncol (R Coll Radiol), 2006. 18(4): p. 300-5.19.McKay, S.P., et al., Human papillomavirus (HPV) transcripts in malignant inverted papilloma are from integrated HPV DNA. Laryngoscope, 2005. 115(8): p. 1428-31.20.Kraft, M., et al., Significance of human papillomavirus in sinonasal papillomas. J Laryngol Otol, 2001. 115(9): p. 709-14.
A B
A B
A B
B