Embed Size (px)
Citation preview

MCS
Mitswmmptrp
*
†
A
1
anagement of Articularartilage Injuries in the Knee
teven J. Hospodar, MD,* and John M. Tokish, MD†
Chondral injuries of the knee are a common source of disability in a military population.These lesions may limit activities of daily living and military duty requirements and maycompromise the readiness of the individual and the unit. The ability to avoid or modifyactivities is often not an option in this population. At the US Air Force Academy, we treatactive duty and retired patients, as well as their dependents. In addition, we care for over4,400 cadets including athletes from 27 intercollegiate sports. This patient populationpresents a considerable experience with these injuries. Treatment of knee chondral lesionsin our population begins with a thorough history and physical examination. Radiographicstudies including x-rays, magnetic resonance imaging, computed tomography scans, andalignment films are often used in the preoperative plan. Lesions are characterized accord-ing to their size and surrounding environment, including quality of surrounding cartilageand mechanical alignment. Based on the preoperative evaluation, we use a variety ofsurgical techniques including microfracture, osteoarticular autograft and allograft trans-plantion, and autologous chondrocyte transplantation. Osteotomies are also used to cor-rect malaligment when necessary. The postoperative regimen is specific and critical to thesuccess of the procedure. With careful attention to preoperative workup, meticuloussurgical technique, and compliance with a specific postoperative regimen, cadets andactive duty members can recover from these injuries and return to activities includingintercollegiate athletics, military readiness, and overseas deployment duties.Oper Tech Sports Med 13:150-156 © 2005 Elsevier Inc. All rights reserved.
KEYWORDS chondral defect, microfracture, osteoarticular autograft and allograft transplanta-tion, autologous chondocyte transplantation, malalignment
duk1mefctc
h“tdlKte
ost orthopedic surgeons in the military practice sportsmedicine. Those who are responsible for caring for the
njured soldier understand the striking similarities betweenhe active soldier and the elite athlete. Both groups are mis-ion oriented, require a high level of function, and are all tooilling to sacrifice long-term health for short-term perfor-ance. The training regimen of the military “combat athlete”ay include routine use of a 50-lb pack, hard landings afterarachute jumps, or regular marches for miles over unevenerrain. With a recent reemphasis on deployment, readinessequires that most members of the active service be in properhysical condition, as measured by service-specific stan-
Department of Orthopaedics, Wilford Hall Medical Center, Lackland AirForce Base, TX.
United States Air Force Academy Hospital, United States Air Force Acad-emy, CO.
ddress reprint requests to John M. Tokish, MD, United States Air ForceAcademy Hospital, 4102 Pinon Drive, Suite 100, USAFA, CO 80840.
aE-mail: [email protected]
50 1060-1872/05/$-see front matter © 2005 Elsevier Inc. All rights reserved.doi:10.1053/j.otsm.2005.10.005
ards. Such standards include running tests that are partic-larly demanding on patients with chondral defects in thenee. Finally, the nation’s military academies have over5,000 officers in training who are required to adhere to theost stringent of physical training programs. In addition,
ach academy has upwards of 25 intercollegiate sports withrequent chondral injuries in the knee. This article will dis-uss our approach in treating these injuries, as well as some ofhe unique complexities that our military population andadets present.
Articular cartilage injuries in the knee are common andave a limited ability to regenerate.1-6 In 1743, Hunter wrote,From Hippocrates to the present age it is universally allowedhat ulcerated cartilage is a troublesome thing and that onceestroyed it is not repaired.”7 Since that time, articular carti-
age injuries have been shown to progress to osteoarthritis.8
nee arthroscopy has led to the identification, diagnosis, andreatment of articular cartilage lesions. There are 3 main cat-gories of techniques available for the treatment of traumatic
rticular cartilage lesions: (1) marrow stimulation (ie, micro-
flttas
abAaw
TTUuitiomrmflSimtpamlprist
mqfidnisocc
CPOcsoptltttm(lf(ctaas
Articular cartilage injuries 151
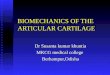
racture, drilling, abrasion chondroplasty) (Fig. 1), (2) cellu-ar induction of chondrogenesis (ie, autologous chondrocyteransplantation [ACT]or autologous chondrocyte implanta-ion), and (3) transplantation of osteochondral allografts orutografts (ie, osteochondral autograft transfer [OATS], mo-aicplasty, osteoarticular allograft placement).
The goal for each technique is to relieve pain and functionnd to possibly prevent late degenerative changes in the jointy reestablishing the chondral surface. At the United Statesir Force Academy, we routinely offer microfracture, OATS,nd ACT to our young, athletic military patient populationith chondral injuries.
he Military Populationhe United States Air Force Academy (as well as the other 2S service academies) is a unique environment in that grad-ation requirements include a number of physically demand-
ng challenges. These include several running and fitnessests each semester, as well as physical education classes thatnclude unarmed combat, boxing, and/or wrestling. Cadetsften do not have the luxury of opting out of these require-ents, and prolonged waivers for physical limitations are a
are occurrence. In addition, all cadets have daily mandatoryarching formations, must use stairs between classes in the 6oor, ¼-mile long Fairchild Hall (a building at the Unitedtates Air Force Academy), and walk to and from intramural/ntercollegiate facilities over a mile away. All of these require-
ents are considered mandatory military formations, andardiness is not tolerated. Cadets on crutches fall behind theireers quite quickly athletically, but also suffer militarily andcademically for their period of incapacitation. Thus, we asilitary service academy surgeons often see patients with
arge chondral defects who have ignored their symptoms forrolonged periods and who are limited in their availableehabilitation time. In addition, return to less than full activ-ty may jeopardize a military career, so we are assured that theurgical technique and postoperative rehabilitation will be
Figure 1 Example of the microfracture technique. (A) Lateam treated with microfracture. (B) Close view of microof the holes. This patient returned to the national team.
horoughly tested.
In the active duty population, nearly all military airmenust remain “worldwide qualified” for deployment. This
ualification includes a yearly and predeployment physicaltness test. Airmen who have physical ailments like chondralefects in the knee who cannot perform the physical activityecessary to remain worldwide qualified are subject to a Mil-
tary Evaluation Board, which can lead to dismissal from theervice. Current Air Force guidance allows for a total of 1 yearf profiled limitations before an Military Evaluation Board isonvened to evaluate an airman’s fitness for duty. Similaronditions exist in the other branches of the military.
linicalresentation and Workup
ur patients with chondral defects usually present with ahief complaint of pain and limitation of duty. Many report apecific traumatic event, but others report a more insidiousnset that is aggravated by marching, running, or other re-etitive impact use. Patients are often referred for a meniscalear because they often present with physical findings of jointine tenderness, an effusion, and pain at the extremes of mo-ion. A complete examination of both knees is accomplishedo rule out concomitant pathology (instability, meniscalears, ligament deficiency, extensor mechanism dysfunction,echanical malalignment, and so on). Plain radiographs
standing anteroposterior [AP], standing 45° posteroanterior,ateral, Merchant view), a weight-bearing AP long-leg cassetteor mechanical alignment, and magnetic resonance imagingMRI) are obtained. In cases in which a patellar or trochlearhondral defect is suspected, we obtain a limited computedomography (CT) scan with patellofemoral views in 0°, 15°,nd 30° of flexion to evaluate patellofemoral alignment. Inddition to a general evaluation of the imaging studies, wepecifically look for the following:
1. Mechanical axis: we measure this with a line drawnfrom the center of the hip to the center of the ankle.
ion of the femoral condyle in a wrestler on the nationalre showing punctuate bleeding of the base and spacing
rge lesfractu
This line should fall at the base of the lateral tibial spine.

toodc
ITCapdcab
tTaad
tntmps
ctdapmoc
oaterboaawtOpdrtokqr
152 S.J. Hospodar and J.M. Tokish
2. Radiograph evaluation: we ensure that the patient doesnot have degenerative joint changes such as joint spacenarrowing, osteophytes, cystic change, or subchondralsclerosis.
3. MRI evaluation: the MRI is reviewed to determine sizeand location of the lesion, the presence or absence ofsubchondral bone edema or bone loss, kissing lesions(concomitant patellar and trochlear arthritis as well asconcomitant condylar and plateau arthritis), and thequality of the surrounding cartilage.
4. Limited CT scan evaluation: in cases of patellar ortrochlear chondral defects, we evaluate for evidence ofpatellofemoral malalignment. We calculate tilt and sub-luxation as described by Fulkerson.10
Finally, a thorough discussion is undertaken with the pa-ients to ensure they are willing to undergo the rigorous post-perative regimen and that they understand the expectationsf outcome. On completion of the history, physical, and ra-iographic review, we determine if a patient is an appropriateandidate for cartilage restoration techniques.
ndications andreatment Algorithm
andidates for cartilage restoration are generally under 45nd have a well-defined chondral defect in an otherwise well-reserved knee. Although concomitant pathology can be ad-ressed, chondral atrophy, kissing lesions, or degenerativehange is a contraindication for surgery. Mechanical mal-lignment, either femoral-tibial or patellofemoral must alsoe considered in these patients and in general corrected.Microfracture remains the workhorse of our cartilage-res-
oration techniques and is appropriate for many of our cases.he microfracture technique, as described by Steadman etl,9 is a versatile procedure that is not technically demandingnd very effective in both our cadet population and our active
uty force. It is considered our first-line treatment for lesions bhat are small to medium size (less than 2 � 2 cm), haveormal mechanical alignment, and have no significant struc-ural bone loss. Critical to the success of the procedure is aeticulous surgical technique and adherence to a specificostoperative rehabilitation program, which will be de-cribed later.
Microfracture is not as effective in patients with mechani-al malalignment. In patients who present with femoral oribial chondral lesions and who have a mechanical axis that iseviated toward the side of the defect (eg, a varus knee withmedial femoral chondral lesion), a corrective osteotomy iserformed (Fig. 2). In patients with patellofemoral malalign-ent and a patellar or trochlear defect, a Fulkerson osteot-
my is performed in conjunction with the microfracture pro-edure (Fig. 3).
Patients who present with either mechanical malalignmentr an osteochondral defect with more than 5 mm of bone lossre not optimal candidates for microfracture. In these pa-ients, we prefer an OATS procedure (Fig. 4). It has been ourxperience that the structural support of the bone plug canestore a normal bony morphology to the tidemark, andone-to-bone healing is nearly universal. In addition, manyf our patients, especially our cadets, are reluctant to undergotibial osteotomy as a first-line procedure to correct mal-
lignment. Finally, with the structural support of the plug,e are more confident with earlier weight bearing than with
he other techniques. In each of these scenarios, we prefer theATS procedure and have found it effective in returningatients to full activity, although we have concerns about itsurability over time in a mechanically disadvantaged envi-onment. Limitations with the OATS procedure includehe size of the lesion and its location. Donor-site morbidityf autograft OATS may be an ongoing issue of anteriornee pain, especially in the military population that re-uires a great deal of deep-bending activities. Large lesionsequiring more than 4 plugs may lead to donor-site mor-
Figure 2 Correction of malalignment. (A) Mechani-cal malalignment in an active duty patient withchondral defect of the right knee. Note the medialdeviation of the drawn mechanical axis. (B) AP and(C) lateral views show restoration of mechanicalaxis after opening wedge osteotomy. This patienthas returned to full duty including fitness testing.
idity, tibial lesions and posterior femoral lesions are not

eatwtWey
e
pawpcdottv
Faflkotiaakmi
Articular cartilage injuries 153
asily accessible to a perpendicular insertion, and contourreas like the patella are topographically challenging areaso use an OATS technique. We have a limited experienceith allograft OATS procedures and have found them to
ake longer to return to duty than the other techniques.e restrict its use to very large defects and are careful to
xplain to the patient that return to full duty can take aear or more.ACT also plays a role in our population. ACT can be more
asily contoured than an OATS plug, can be used in most all
igure 3 Correction of patellofemoral mal-lignment. (A) Limited CT scan at 30° ofexion in a US Air Force Academy cadet bas-etball player with kissing chondral lesionsf the patella and trochlea showing subluxa-ion of the patella. (B-D) Postoperative x-raysncluding patellofemoral view at 30°, lateral,nd AP views showing correction of the mal-lignment. The osteotomy unloaded theissing lesions, which were then treated withicrofracture. This patient has returned to
ntercollegiate athletics.
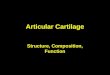
Figure 4 OATS. (A) Medial femoral condylar lesion in US9-mm OATS plug inserted into lesion. (C) Ten months af
the restoration of the chondral surface of the medial condyle.arts of the knee, and is not limited by the size of a lesion. Inddition, the technique can be modified to provide a “sand-ich” of bone, periosteum, cartilage, and another layer oferiosteum to remedy an osteochondral defect with signifi-ant bone loss. In our military population, this techniqueoes have the downside of requiring 2 surgeries, with post-perative recovery from each, and is very expensive relativeo other techniques. In general, we prefer this technique inhe setting of a potential for failed microfracture, such as aery large or uncontained lesion. In this situation, a micro-
rce Academy football player with varus knee. (B) SingleTS, the patient returned to intercollegiate football. Note
Air Foter OA
(Color version of figure is available online.)

ftcpos
MSFutnpAasttptdppmtov
rhctarvmpadpmhpcatcmtaeslt
OWBmthflpdtpOsccdaelamtplppsc
gvttlbewTt
sach9cactmivltit
154 S.J. Hospodar and J.M. Tokish
racture is performed, and an ACT biopsy is taken for use inhe event that the microfracture fails. ACT is our primaryhoice for large patellofemoral lesions with a bone-loss com-onent. As is the case in microfracture, this procedure isptimized with a mechanically normal knee, and we aggres-ively correct patellofemoral malalignment when necessary.
icrofracture:urgical Technique
or smaller (less than 4 cm2 � 2 � 2 cm) lesions in patientsnder 40 years of age, we prefer an isolated microfractureechnique as described by Steadman et al.9 If the leg is not inormal mechanical alignment, a high tibial, distal femoral, oratellar realignment osteotomy is performed concomitantly.nonsterile tourniquet is placed high on the patient’s thigh,
nd the leg is placed in the leg holder. Three standard arthro-copic portals are created. First, a superolateral outflow por-al is placed. A lateral parapatellar portal is made adjacent tohe patellar tendon at the level of the inferior pole of theatella. The inflow cannula and arthroscopic camera are in-roduced, and the medial parapatellar portal is made underirect visualization. A thorough diagnostic arthroscopy iserformed (suprapatellar pouch, medial/lateral gutters,atellofemoral articulation, notch, medial/lateral compart-ents). The articular lesion is adequately defined, and ar-
hroscopic images are recorded. We commonly perform anyther indicated procedures first to maximize arthroscopicisualization.
The full-thickness cartilage lesion is then debrided (fulladius shaver or curette) until a stable, perpendicular rim ofealthy cartilage is encountered. Careful removal of the cal-ified cartilage layer is performed until small areas of punc-ate bleeding are visualized throughout the lesion. Occasion-lly, an internal osteophyte is encountered and a burr isequired to achieve the proper depth. Care is also taken to notiolate the subchondral bone. We routinely use a 45° Stead-an arthroscopic awl (Linvatec Corporation, Largo, FL) toerforate the subchondral bone. We begin at the periphery,nd the awl is gently tapped through the exposed subchon-ral bone (2-4 mm depth) to create a microfracture of therepared lesion. Similar microfracture holes are placed 3 to 4m apart around the lesion. We work from the adjacentealthy cartilage toward the center of the lesion. The appro-riate depth is confirmed by the presence of fat dropletsoming from the marrow cavity. Several different portals andwl positions are often required to achieve optimal prepara-ion of the lesion, and meticulous attention to technique isritical to the success of the procedure (Fig. 1A). Once theicrofracture is complete, the pump pressure is reduced and
he lesion is assessed for bleeding (Fig. 1B). When bleeding isdequate, the instruments are removed and the joint fluid isvacuated to maximize the formation of the “superclot.” Aterile dressing is applied. A brace is used only if a patel-ofemoral lesion was addressed, in which case it is placed in
he operating room and set at 0° to 20°. tATS: Surgical Techniquee perform a modification of the procedure described by
obic11 and Sgaglione et al,12 either arthroscopically or via ainiarthrotomy. A nonsterile tourniquet is placed high on
he thigh, and the contralateral leg is placed in a well-legolder. The operative knee is ranged to be sure that adequateexion can be achieved. A brief diagnostic arthroscopy iserformed to evaluate the size of the lesion, the availableonor cartilage, and any concomitant pathology (meniscalears, removal of loose bodies, and so on). The additionalathology is addressed at the time of operation before theATS. The chondral defect is located and debrided back to a
table, perpendicular rim of healthy cartilage with a shaver,urette, or arthroscopic knife and is curetted until the sub-hondral bone is exposed. Different sizing guides are used toetermine the number of grafts required to best fill the defectnd whether existing portals or accessory portals will be ad-quate to approach the defect and donor sites perpendicu-arly. Although many smaller lesions can be addressed quitedequately arthroscopically, we do not hesitate to perform ainiarthrotomy on the side of the defect, which greatly aids
he exposure of both the donor and recipient site. It is ourreference to harvest from the periphery of the trochlea ipsi-
ateral to the chondral lesion first, working from distal toroximal. If additional plugs are required, the contralateraleripheral trochlea can be harvested through the same inci-ion. In an arthroscopic technique, single and double plugsan be harvested through the intercondylar notch.
The grafts are harvested and placed sequentially with eachraft press-fit into the lesion before the subsequent graft har-est. We begin with an evaluation of the lesion’s size andopography. We attempt to choose a pattern that will allow uso use the least number of plugs that will completely cover theesion. If possible, we try to keep our largest plug at 9 mmecause this gives us the option to upsize by 1 mm in thevent that a plug needs to be replaced after insertion. Oncee map the lesion, the first of the recipient plugs is taken.his allows us to exactly measure the contour and depth that
he donor plug must fit, optimizing donor-recipient match.We then harvest the first donor plug. The appropriately
ized tubular chisel is placed perpendicular to the donorrticular surface, and the tube is gently tapped 15 mm forhondral defects and 25 mm for osteochondral lesions. Thearvester is sharply twisted 90° clockwise and then sharply0° counterclockwise, which loosens the graft from the can-ellous bone below. Care is taken not to overtoggle the chiselnd risk fracture of the plug. The plug is then removed. Theartilage depth is checked in 4 orthogonal quadrants to de-ect subtle height differences around the plug. These areatched to the corresponding quadrant heights at the recip-
ent sites to ensure an optimal match. The graft is then ad-anced with the T-handle or is gently tapped into place,eaving the graft approximately 1 mm proud. The graft posi-ion is then fine-tuned with the use of an oversized tamp untilt is completely flush with the surrounding cartilage. Theechnique is repeated until the lesion is filled. The knee is
hen put through a range of motion to assess the congruity of
tpdlu
AWavmpucaplspsolpssma
tptwtrtm
lcasiarctssssitosat
sr
PTtdatcfqtate
iucWpcikibttWmic
SCtltllhgafrodo
R
Articular cartilage injuries 155
he recreated articular surface. The recipient plugs may belaced into the donor defects to accelerate healing of theonor sites. The wounds are irrigated and then closed in
ayers and a sterile dressing is applied. A brace is not generallysed.
CT: Surgical Techniquee perform the procedure as described by Sgaglione et al12
nd Peterson et al.13 The autologous chondrocytes are har-ested at a prior arthroscopic procedure and cultured (12illion cells per 4 to 6 cm2 defect). A nonsterile tourniquet islaced high on the thigh. The patient is supine with a bumpnder the hip of the affected extremity. Any additional pro-edures (ie, high tibial osteotomy, Fulkerson realignment,nd so on) are performed before the ACT portion of therocedure. The limb is exsanguinated, and a small parapatel-
ar arthrotomy is performed. The full-thickness cartilage le-ion is excised using a no. 15 blade and a curette to a stable,erpendicular rim. The debridement is carried down to theubchondral bone without causing any bleeding. If bleedingccurs, it is treated with an epinephrine-soaked sponge. Theesion is then measured by its longest diameter and its longesterpendicular diameter. Sterile paper (from the wrapping onurgical gloves) is then placed overlying the lesion, and aterile pen is used to outline the lesion (placing the pen 1-3m beyond the outline of the lesion). The paper is then cut,
nd the template is created.A second longitudinal incision is generated just distal to
he pes anserine. The paper template is placed over the ex-osed periosteum, and a fresh no. 15 blade is used to incisehe periosteum. Once the template has been circumscribedith the knife, a mark is placed on the periosteum to identify
he cambium layer. A sharp periosteal elevator is then used toemove the periosteal flap. Care is taken to avoid small cen-ral defects in the periosteal flap. The periosteal flap is re-oved, and a saline-soaked gauze is placed into the wound.We then proceed to fix the periosteal flap to the chondral
esion perimeter. The cambium layer of the flap faces the sub-hondral bone and 6-0 vicryl on a P-1 cutting needle is used toffix the flap to the cartilage. Mineral oil can facilitate passage ofuture and prevent periosteal bunching of tissue. Sutures arenitially placed to anchor the flap in 4 corners, and then suturesre spaced 3 to 4 mm apart. A 6- to 8-mm opening shouldemain at the 12 o’clock position for injection of the autologousells. The flap is tested first with a normal saline insufflation intohe space between the periosteal flap and bone layers through ayringe-soft catheter setup to check that there is no leakage. Thealine is then aspirated from under the periosteum. Fibrin glueealant is then applied around the periphery of the flap to furthereal the construct. The cells are resuspended in the vial and thennjected beneath the periosteal flap. The catheter is placed dis-ally and then withdrawn as the cells are injected. The superiorpening is closed with additional suture and fibrin glue to en-ure that the injected cells are properly sealed between the bonend periosteum. The 2 incisions are closed in layers, and the
ourniquet is let down. The wounds are dressed in the usualterile fashion. A brace is applied if we addressed a patellofemo-al lesion and is set at a range of 0° to 20° flexion.
ostoperative Rehabilitationhe postoperative rehabilitation program is a critical part of our
reatment of these lesions. We are currently involved in a ran-omized clinical trial comparing microfracture, OATS, and ACTnd thus have a standardized rehabilitation program for the 3echniques. We use a continuous passive motion (CPM) ma-hine in the recovery room and continue it for 8 hours per dayor 8 weeks. The range of motion is begun from 30° to 70° but isuickly increased to full passive range of motion as tolerated byhe patient. The initial rate is usually set to 1 cycle per minutend can be adjusted for patient comfort. If the patient is unableo use the CPM, the patient is instructed to passively flex andxtend the knee 500 times at 3 separate times of the day.
Touchdown weight bearing with the assistance of crutchess required for 8 weeks. For patellar or trochlear lesions, wese a hinged knee brace set at 0° to 20° to limit patellofemoralontact at all times when the patient is not in the CPM.eight bearing is allowed as tolerated in these patients with
atellar or trochlear lesions in full extension once quadricepsontrol is achieved. Limited strength training is also begunmmediately with straight leg raises and double-leg one-thirdnee bends (operative side remains touchdown weight bear-
ng only). At 2 weeks, the patient may begin the stationaryike or deep-water pool exercises (running with the assis-ance of a flotation vest). Resistance exercises (elastic bandherapy) and full weight bearing are begun after 8 weeks.
eight training may be started as early as 16 weeks. Patientsay return to cutting sports at 4 to 6 months postoperatively
f they have achieved a satisfactory range of motion, quadri-eps mass and control, and have no effusion.
ummaryhondral lesions are a common source of disability in mili-
ary members. These lesions compromise activities of dailyiving, require limit duty requirements, and may compromisehe readiness of the individual and the unit. The ability toimit or modify activities is often not an option in this popu-ation. The diagnosis of a chondral defect requires a carefulistory and physical examination with additional radio-raphic imaging. A number of operative techniques are avail-ble to treat these lesions including OATS, ACT, and micro-racture. Each of these techniques combined with a specificehabilitation program have been successful in the treatmentf chondral lesions of the knee. Further study is necessary toifferentiate between techniques and to evaluate long-termutcomes.14
eferences1. Curl WW, Krome J, Gordon ES, et al: Cartilage injuries: A review of
31,516 knee arthroscopies. Arthroscopy 13:456-460, 19972. Brittberg M, Lindahl A, Ohlsson C, et al: Treatment of deep cartilage
defects in the knee with autologous chondrocyte transplantation.
N Engl J Med 331:889-895, 1994
1
1
1
1
1
156 S.J. Hospodar and J.M. Tokish
3. Convery FR, Akeson WH, Keown GH: The repair of large osteochon-dral defects. An experimental study in horses. Clin Orthop Relat Res82:253-262, 1972
4. DePalma AF, McKeever CD, Subin SD: Process repair of articular car-tilage demonstrated by histology an autoradiography with tritiated thy-midine. Clin Orthop Relat Res 48:229-242, 1966
5. Frisbie DD, Trotter GW, Powers BE, et al: Arthroscopic subchondralbone plate microfracture technique augments healing of large chondraldefects in the radial carpal bone and medial femoral condyle of horses.Vet Surg 4:242-255, 1999
6. Meyers MH, Akeson W, Convery R: Resurfacing of the knee with freshosteochondral allografts. J Bone Joint Surg Am 71:704-713, 1989
7. Hunter W: On the structure and diseases of articulating cartilages.Philos Trans R Soc 9:267, 1743
8. Buckwalter JA, Mow VC, Ratcliffe A: Restoration of injured or degen-
erated articular cartilage. J Am Acad Orthop Surg 36:192-201, 19949. Steadman JR, Rodkey WG, Singleton SB, et al: Microfracture techniquefor full-thickness chondral defects: Technique and clinical results.Oper Tech Orthop 7:300-304, 1997
0. Fulkerson J: Anteromedialization of the of the tibial tuberosity forpatellofemoral malalignment. Clin Orthop Relat Res 177:129-133,1983
1. Bobic V: Arthroscopic osteochondral autograft transplantation in ante-rior cruciate ligament reconstruction: A preliminary clinical study.Knee Surg Sports Traumatol Arthrosc 3:262-264, 1996
2. Sgaglione NA, Miniaci A, Gillogly SD, et al: Update on advanced sur-gical techniques in the treatment of traumatic focal articular cartilagelesions in the knee. Arthroscopy 18:9-32, 2002
3. Peterson L, Minas T, Brittberg M, et al: Two to Nine year outcomes afterautologous chondrocyte transplantation of the knee. Clin Orthop RelRes 374:212-234, 2000
4. Minas T, Peterson L: Advanced techniques in autologous chondrocyte
transplantation. Clin Sports Med 18:13-44, 1999