Embed Size (px)
Citation preview

MALPOSITION OF THE MANDIBULAR CONDYLE
PROFESSOR MOGENS GLAHN
The Royal Dental College, Department of Surgery, Aarhus, Denmark. Head: Professor, M.D., Mogens Glahn
TEMPOROMANDIBULAR dysfunction is a miscellaneous group of diseases with only their location and certain symptoms in common, and X-ray examinations rarely provide information which has not been obtained already by clinical examination. However, in some cases radiographs do show us that changes have taken place in the temporomandibular joint. About 15 years ago arthrotomies were performed more commonly than is now considered justifiable.
Malpositions of the mandibular condyle are most often connected with fractures of the condylar neck or luxations, but usually condylar neck fractures heal without symptoms, even when there is gross malposition or luxation of the head. A discussion on simple luxations is not the actual purpose of this com- munication, but one case is described as an example of how some people are able to tolerate disability more than others.
CASE R E P O R T S
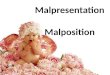
Case I . - -A 3o-year-old female had all her teeth extracted, and afterwards she suspected that her lower jaw was not in its usual position (Fig. x). Her appearance was altered and she had persistent pain in both temporomandibular joints, but she attributed this to the extractions alone and did not see her doctor until five weeks later.
A radiograph confirmed that her mandible had been dislocated, and since simple reduction was impossible, an open reduction was carried out on both sides. The result was satisfactory and post-operatively she could open her mouth sufficiently for dentures to be made (Fig. 2).
When fractures of the condylar neck give rise to secondary symptoms, the patient often complains of limitation of movement which prevents ordinary dental care and sometimes affects normal mastication.
Case 2.--A boy of 14 fell from his bicycle and hit the ground with his chin. Gradually he developed limitation of jaw movement. He applied for treatment two years after the incident and when seen he could open his mouth to a maximum of only 15 mm inter-incisor width. His bite seemed normal.
Tomographic examination proved that he had had a bilateral fracture of the condylar neck. Healing had occurred with considerable shortening of the necks and the condylar heads were also abnormal.
At first it was believed that adhesions and damage to the articular disc were responsible for the restricted movement. A pair of splints were made with a spring in the upper one and these were used for two months. After that treatment the improvement was a mere 3 mm. increase of opening.
However, his radiographs were re-examined and coronoid processes were found to be considerably longer, due to the shortening of the condylar necks.
The normal opening of the jaw includes a forward-downward movement of the coronoid, and as we sometimes see a loss of the free-way space between the temporal fossa and the zygomatic arch in fractures of the malar bone with backward dislocation, the same thing may happen if the coronoid is too large to move down under the lower malar border. A frontal tomographic examination confirmed that this had happened.
33

~4 BRITISH JOURNAL OF ORAL SURGERY
Treatment is simple in such cases : resection of the coronoid on both sides and dilatation exercises to correct the contractors of the chewing muscles.
Case 3.--A 46-year-old man fell on a staircase and for some days afterwards he had a swelling of the right side of the head. The swelling subsided but he developed a clicking sensation in the right temporomandibular joint, limitation of jaw movement and increasing pain in the right temporal region. It was 18 months later before he attended for treatment.
%
FIG. I .
• FI~. 2
Temporomandibular luxation, five weeks old. FIG. 2. After bilateral open reduction.
Radiographs showed that his right condyle was grossly displaced, but not deformed. The reason for this was not clear because there were no signs of an old healed fracture. Furthermore this type of dislocation is not common in fractures--dislocation of the condylar neck.
His principal complaint was that his bite was locked and because his remaining molars were carious they were extracted. He was provided with a set of splints which were completely flat, Within one month he had found his resting position and his symptoms disappeared gradually. Later films showed a normal relationship.
Case 4 . - -The last case concerns a woman of 50 years. Fifteen years before she had complained of clicking and pain in the right temporomandibular joint and recurring dislocations of the jaw, The trouble began in I947 after a condylectomy had been performed. Information regarding the intra-arficular condition and the appearance of the condyle at operation was not available. Post-operatively she had facial pain and was treated by peripheral injections of the trigeminal nerve branches.
In I95O the disc and part of the condylar neck was removed and at a further operation in I95I remnants of the neck were removed. In I953 a resection of the right accessory nerve was carried out and in I96O the insertions of the muscles of mastication were detached and the jaw mobilised to improve movement.
Later on in that same year she had a right trigeminotomy. After that the pain was confined to an old scar anterior to the right ear, but gradually she developed pain in the left temporomandibular joint.
When she applied for treatment in September, I96I, she had constant pain, her jaw deviated to the right, and the mandibular angle was at the level of the ear-lobe (Fig. 3). She had a fair movement of the jaw.

MALPOSITION OF THE MANDIBULAR CONDYLE 35
J
FIG. 3 Right condylectomy. Deviation of
mandible.
FIG. 4 Tomogram of the right temporomandibular
joint. Condyle missing.
FIG. 5 After operation.

3 6 BRITISH JOURNAL OF ORAL SURGERY
Radiographs of the right temporomandibular joint showed the cause of the dis- location of the lower jaw (Fig. 4). The left temporomandibular joint was apparently normal except that movement was restricted. The cause of pain on her left side was thought to be due to the rotation of the left condyle. I f this concept was right, the problem was how to move back the mandible into a normal or near normal position.
Her condition was such that she was willing to accept any form of treatment but actual joint reconstruction was out of the question, because the fossa was filled with scar tissue. I t was decided to divide the coronoid, turn it through I8o ° and replace it like a graft. The jaw was immobilised with Gunning splints and a piece of stent wedged in between them to compensate for changes in the bite. The splints were removed two months post-operatively. Eight months after the operation (Fig. 5) her appearance was improved, she was symptom-free and could open her mouth to the same extent as before the operation.
S u m m a r y . - - T h e s e are a few examples f rom a large group of patients, each of whom may contribute to our knowledge of this complicated functional entity. A careful analysis o f each case is essential, and each case must be judged and treated individually.