-
7/28/2019 lp hematomessis melena
1/17
THEORETICAL BACKGROUND
OF
HAEMATEMESIS MELENA
IN TANJUNG WARD ( PDP ) BANJARMASIN ULIN GENERAL HOSPITAL
BY:
Hengki Hanggara
SRN
011016 D3KI
BANJARMASIN MUHAMMADIYAH HEALTH COLLEGE
INTERNASIONAL CLASS OF NURSING DIPLOMA PROGRAM
2013-2014
-
7/28/2019 lp hematomessis melena
2/17
ANATOMY AND PHYSIOLOGY GASTRIC
stomach in the medical language gastric, gastric digestion is
one of the organs
contained in the human body. for more jelasnnya what the stomach
or gastric, I will
discuss the anatomy of the stomach first. not only the anatomy
of the stomach, here I
will discuss the physiology of the stomach or the complete I
will discuss Stomach
Anatomy and Physiology. anatomy and physiology of the stomach
which I discussed
here include: stomach lining, innervation and blood flow to the
stomach, the motor
function of the stomach, the digestive function of the stomach,
the secretion of gastric
function, process of food digestion in the stomach, as well as
enzymes and hormones
that play a role in digestion in the stomach. tall aja yah you
read below about the
anatomy of gastric physiology.
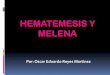
ANATOMY OF GASTRIC
Gastric located at the top of the abdomen, extending from the
bottom surface of the arch to
the left until the region epigastrica costalis an umbilical.
Gastric mostly located below the
bottom of the costae. Gastric roughly J-shaped and has two
holes, and ostium ostium
cardiacum pyloricum, two curvatura,
http://arispurnomo.com/wp-content/uploads/2010/06/lambung.gif
-
7/28/2019 lp hematomessis melena
3/17
curvatura major and lesser curvature, and two walls, Paries
Paries anterior and posterior.
In general, stomach is divided into 3 sections:
1. cardiac / cardiac glands found in the mouth regia heart. It
only secrete mucus2. fundus / gastric located almost in the entire
corpus, which this gland has three main
types of cells, namely:
Cells zigmogenik / chief cell, mesekresi pepsinogen. Pepsinogen
is converted into
pepsin under acidic conditions. These glands secrete stomach
lipase and renin are less
important.
parietal cells, secrete hydrochloric acid and intrinsic factor.
Intrinsic factor required for
absorption of vitamin B12 in the small intestine.
mucous neck cells found in the stomach glands of the neck all.
These cells
secrete mucus barrier thickness of 1 mm and protects the stomach
lining against
damage by HCL or autodigesti.
3. pyloric antrum pylorus lies in regia. This Kelenajr and mucus
secreting gastrin,
a peptide hormone which is influential in the process of stomach
secretion.
Ingestion Food In Stomach
1. MECHANICAL
after food enters the stomach, the peristaltic movements gentle
and berriak called
wave mixing (mixing wave) occurs in the stomach every 15-25
seconds. This wave of
soaking food and mix it with the secretion of stomach glands and
reduce it to a watery
liquid called chyme. Some wave mixing occurs in the fundus,
which is the main
storage area. The food is in the fundus for an hour or more
without mixed with
gastric. During this time, digestion with saliva continue.
During digestion takes place in the stomach, more terrific wave
mixing starts from the
body and is intensified when it reaches the pylorus. Pyloric
spinchter almost always
there but not entirely closed. When food reaches the pylorus,
each wave mixing
pressing small amounts of stomach into the duodenum through the
pyloric spinchter.
Almost all the food is pressed back into the abdomen. The next
wave push on and
push a little more towards the duodenum. Movement forward or
back (forward /
-
7/28/2019 lp hematomessis melena
4/17
backward) of stomach contents is responsible for almost all the
mixing that occurs in
the stomach.
2. CHEMICALPrinciples of activity in the stomach is to begin
digestion of protein. For adults,
primarily through the digestive enzyme pepsin. Pepsin breaks the
peptide bond
between amino acids that make up proteins. Chain protein
consisting of the amino
acids are broken down into smaller fragments called peptides.
Pepsin most effective
in the highly acidic environment in the stomach (pH = 2) and
became inactive in
alkaline environments. Pepsin is secreted into inactive form
called pepsinogen, so it
can not digest the protein in zymogenic cells that produce it.
Pepsinogen is converted
into pepsin is not active until he made contact with the
hydrochloric acid secreted by
the parietal cells. Second, cells are protected by mucus
alkaline stomach, especially
after pepsin is activated. Mucus covering the mucosa to form a
barrier between the
gastric mucus
Other enzymes of the stomach is stomach lipase. stomach lipase
breaks down
triglycerides into short chain fatty molecules that are found in
milk. These enzymes
operate well at pH 5-6 and has a limited role in the adult
stomach. Adults are very
dependent on the enzyme that is secreted by the pancreas
(pancreatic lipase) into the
small intestine to digest fat. Stomach also secrete renin which
is important in
digesting milk. Renin and Ca react to milk to produce curds.
Clumping prevents too
frequent passage of milk from the stomach into the duodenum to
the (first part of
small intestine). Renin secretion is not present in stomach in
adults.
-
7/28/2019 lp hematomessis melena
5/17
Enzymes and Hormones Play a Role in Digestion in Stomach
1.Gastrin hormone
Physiological significance of work
1. stimulates the secretion of acid and pepsin 1. facilitate
digestion
2. stimulates the secretion of intrinsic factor 2. facilitate
absorption in the intestine
3. stimulates the secretion of pancreatic enzymes 3. facilitate
digestion
4. stimulates bile flow increased heart 4. facilitate
digestion
5. 5 stimulates insulin secretion. facilitate glucose
metabolism
6. stimulates the movement of stomach and intestines
6.mempermudah mixing
7. facilitate stomach receptive relaxation 7.lambung can easily
increase the volume,
without increasing the pressure
8. increase the resting tone SEB 8. prevent reflux of stomach
mixing time and
pangadukan
9. 9 inhibits gastric emptying. allows mixing the entire
contents of stomach before
passing into the intestine
2. Enzyme pepsin: convert protein into peptone
3. Enzyme rennin: precipitate the casein in milk
4. Lipase: breaks down fats into fatty acids
5. HCl: mmbunuh germs and preserve food
-
7/28/2019 lp hematomessis melena
6/17
I.definition
Haematemesis is vomiting blood and melena are spending faeces or
black feces
caused by the presence of upper gastrointestinal tract bleeding.
Hematemesis color
depending on the length of contact between the blood and the
size of the stomach acid
of bleeding, so it can be colored like coffee or reddish and
lumpy Hematemesis
usually occurs when there is bleeding in the proximal jejunum
and melena may occur
alone or together with hematemesis. At least 50-100 ml of
bleeding, melena
circumstances are found. The amount of blood that comes out
during hematemesis or
melena difficult to use as a benchmark to estimate the size of
the upper tract bleeding
eat. Haematemesis and melena is an emergency situation and need
immediate
treatment in hospital.
II.etiology
Cause of hematemesis melena:
1. Abnormalities in the esophagus
esophageal varices
Patients with hematemesis melena caused by rupture of esophageal
varices, never
complained of pain or pain in epigastrum. In general, the nature
of spontaneous and
massive bleeding arise. Blood spewed blackish in color and does
not freeze because it
mixes with stomach acid
.
Carcinoma of the esophagus
Carcinoma of the esophagus often give complaints than
hematemesis melena. Besides
complaining dysphagia, body care and anemic, just seseklai
patient vomited blood,
and even then not massive. At endoscopy clear picture of
carcinoma that almost
closes the esophagus and bleed easily located in the lower third
of the esophagus.
-
7/28/2019 lp hematomessis melena
7/17
Mallory-Weiss syndrome
arising Before hematemesis preceded severe vomiting that
eventually emerging
bleeding, such as in alcoholics or in early pregnancy. Usually
caused by too frequent
and severe vomiting continuously. If the patient is experiencing
dysphagia may be
caused by esophageal carcinoma.
Esophagitis korosiva
In a study of patients found a woman and a man vomiting blood
after drinking water
hard to solder. From the analysis of the hard water found to
contain citric acid and
HCl acid, which is corrosive to the oral mucosa, esophagus and
stomach. Besides
vomiting blood the patient also complained of pain and burning
in the mouth heat.
Chest and epigastrum.
Esophagitis and esophageal ulcers
Esophagitis when to cause more frequent bleeding is intermittem
or chronic and
usually mild, so more often than hematemsis melena arise. Ulcers
in the esophagus
rarely cause bleeding when compared with stomach and duodenal
ulcers.
2. Abnormalities in stomach
erisova hemorrhagic gastritis
Haematemesis is not massive and arise after patients take drugs
that cause stomach
irritation. Before the patient complained of vomiting heartburn.
Need to be asked also
whether the patient is or frequent use rheumatic drug (NSAID +
steroids) or frequently
drink alcohol or herbal remedies.
Gastric ulcer
Patients experiencing dispepsi include nausea, vomiting,
heartburn hatidan before
hematemesis preceded or stinging pain in epigastrum related to
food. Shortly before
arising hematemesis due to pain and pain is felt more intense.
After vomiting blood
and pain reduced pain. Nature is not so massive hematemesis and
melene more
dominant than hematemesis.
-
7/28/2019 lp hematomessis melena
8/17
Gastric Carcinoma
The incidence of gastric carcinoma in our country is classified
as very rare and
generally comes to treatment already in the advanced phase, and
often complain of
feeling pain, pain in the pit of the stomach often complain of
feeling full quickly and
the body becomes weak. More often complain because melena.
3. Blood diseases: leukemia, DIC (disseminated intravascular
coagulation),
thrombocytopenia purpura and others.
4. Other systemic diseases: uremic, and others.
5. The use of drugs that ulserogenik: class salicylates,
corticosteroids, alcohol, and others.
III.pathophysiology
Bleeding from esophageal varices occurs in approximately one
third of patients with liver
cirrhosis and varices. Mortality caused by first bleeding
episode was 40% to 50%. This
bleeding is one of the leading causes of death in patients with
liver cirrhosis. Bleeding is also
the most common complication of peptic ulcer disease and occurs
in approximately 20% of
patients with ulcers.
-
7/28/2019 lp hematomessis melena
9/17
Patway
-
7/28/2019 lp hematomessis melena
10/17
SIGNS AND SYMPTOMS
1.Intestinal symptoms are not typical such as anorexia, nausea,
vomiting and diarrhea.2. Fever, weight loss, quickly tired.
3. Ascites, and edemo hidratonaks.
4. Jaundice, urine sometimes become older or brownish color.
5. Hematomegali, when it has advanced liver fibrosis can small
becouse. When
clinically found to be the presence of fever, jaundice and
ascites, where the fever
rather than by other causes, added cirrhosis in an active state.
Be careful about the
possible future prekoma and hepatic coma.
6. Vascular abnormalities such as collateral-collateral wall,
koput medusa,
hemorrhoids and esophageal varices.
7. Endocrine disorder which is a sign of hiperestrogenisme
namely:
- Impotence, atrosi testes, gynecomastia, loss axila and pubic
hair.
- Amenorrhea, hyperpigmentation mammary areola
- Spider nevi and erythema
- Hyperpigmentation
8. finger clubbing
Diagnostic examination
1. Anamnesis, physical examination and laboratoryDo anmnesis
rigorous and general condition of the patient when the weak or
decreased consciousness, it can be aloanamnesis. Past medical
history needs to
be asked, such as hepatitis, chronic liver disease, alcoholism,
Gastric diseases,
use of medications ulserogenik and blood diseases such as
leukemia and others.
Usually the upper tract bleeding caused by eating rupture of
esophageal varices
may not find any complaints of pain or pain in the epigastric
region and
hematemesis symptoms occur suddenly. From the results of history
is
predictable amount of bleeding out using practical TAKARA like
how many
glasses, how many cans and others. Physical examination of
patients with
upper tract bleeding meals that need to be considered is the
general condition,
consciousness, pulse, blood pressure, anemia signs and symptoms
ofhypovolemic to quickly note a more serious condition such as a
rejatan or liver
-
7/28/2019 lp hematomessis melena
11/17
failure. Besides, look for signs of portal hypertension and
cirrhosis of the liver,
such as spider naevi, ginekomasti, palmar erythema, caput
Medusae, presence
of collateral, ascites, hepatosplenomegaly and leg edema.
Laboratory tests such
as hemoglobin concentration, hematocrit, leukocytes, remove
blood clots,
blood type and liver function tests be done on a regular basis
to be able to keep
track of patients.
2. radiological examinationRadiological examinations performed
with esofagogram examination for
esophageal area and continued with double contrast examination
of the
stomach and duodenum. emeriksaan was conducted at various
positions,
especially in the area of 1/3 distal esophagus, cardia and
fundus of Gastric to
look for the presence / absence of varicose veins. To get the
expected results,
the radiological examination is recommended as early as
possible, and
preferably as soon as haematemesis stopped.
3. endoscopic examinationWith the various types fiberendoskop,
the endoscopic examination is essential
to determine the exact place of origin and the source of
bleeding. Another
advantage is the endoscopic examination can be carried out
taking photos for
documentation, fluid aspiration and biopsy for examination
sitopatologik. At
the upper tract bleeding dining ongoing, endoscopic examination
can be done
as early as possible after the emergency or haematemesis
stopped.
4. Liver ultrasonography and scanningExamination with ultrasound
or liver scan can detect chronic liver disease suchas cirrhosis of
the liver that may cause upper tract bleeding eat. This
examination requires specialized equipment and personnel that
until now only
large city there areonly
complications:hypovolemic
shock
Anemia
-
7/28/2019 lp hematomessis melena
12/17
management
Treatment of patients with upper gastrointestinal tract bleeding
should diraat as
early as possible and preferably in a hospital for careful
monitoring and better
aid. Treatment of patients with upper tract bleeding meals
include:
1. Supervision and treatment of general
Patients should be rested absolute, drugs that cause sedative
effects of
morphine, meperidine and paraldehyde should be avoided.
Patients fasted for bleeding is still going on and when
thebleeding stops can
be given liquid food
. infusion directly mounted and diberilan physiological saline
solution for
blood is not yet available.
Monitoring of blood pressure, pulse, awareness of patients and
if necessary
mounted monitor CVP.
The level of hemoglobin and hematocrit should be made to follow
the state
of bleeding.
Blood transfusion is needed for menggati blood loss and
maintain
hemoglobin levels of 50-70% of the normal price.
Provision of hemostatic drugs such as vitamin K, 4 x 10 mg /
day,
karbasokrom (Adona AC), antacids and H2 receptor antagonist
group
(cimetidine or ranitidine) is useful for tackling bleeding.
Do klisma lavemen with plain water or with the administration of
antibiotics
are not absorbed by the gut, the gut sterilization tindadakan.
These actions
were taken to prevent the increase in ammonia production by
intestinal
bacteria, and this can lead to hepatic encephalopathy.
-
7/28/2019 lp hematomessis melena
13/17
2. Installation of a naso-gastric tubeNaso gastric tube fitting
ends are to Gastric fluid aspiration, lavage (Gastric
kumbah) with water, and the provision of drugs. The supply of
water in
Gastric will cause vasoconstriction kumbah local so expect a
decrease in
gastric mucosal blood flow, thus the bleeding will stop. Kumbah
Gastric will
be repeated using water as much as 100-150 ml until a clear
colorless liquid
aspiration and if necessary, action can be repeated every 1-2
hours.
Endoscopic examination can be done immediately after aspiration
of Gastric
fluid was clear.
3. Giving pitresin (vasopressin)Pitresin vasokoktriksi have any
effect, the administration pitresin per infusion
would result kontriksi and splanchnic blood vessels thereby
reducing portal
vein pressure, thus expected variceal bleeding can be stopped.
Keep in mind
that pitresin can menrangsang smooth muscle of coronary
vasoconstriction
that can happen, because it must be careful with the use of
these drugs,
especially in patients with ischemic heart disease. Because it
needs anelectrocardiogram examination and history taking to the
possibility of
coronary artery disease / ischemic.
4. SB balloon Tube InstallationSB balloon tube was installed for
people with variceal bleeding due to
rupture. SB tube installation should be done after the patient
calm and
cooperative, so that patients can be informed and explained the
meaning of
the use of these tools, how to installation and follow-up work
possibilities
that could arise at the time and during installation. Some
researchers get good
results with the use of the SB tube in tackling eating upper
tract bleeding due
to rupture of esophageal varices. SB tube mounting complications
such as
severe lacerations and rupture of the esophagus, airway
obstruction were
never found.
-
7/28/2019 lp hematomessis melena
14/17
5. Sclerotic material usageSclerotic material morrhuate sodium
by 5 ml of 5% or 3% as much sotrdecol
3 ml with the help of a flexible fiberendoskop injected varicose
veins on the
surface and then pressed with SB balloon tube. This action does
not require
general narcotics and can be repeated several times. This
treatment has been
gaining in popularity and is one of the new treatment in
tackling eating upper
tract bleeding caused by rupture of esophageal varices.
6. surgeryWhen prevention efforts fail and the above bleeding
bleeding persists, then
surgery may be considered. Base surgery is performed are:
ligation of
esophageal varices, esophageal transection, shortcuts
porto-Kaval. Effective
operation is recommended after 6 weeks the bleeding stopped and
improved
function.
Prognosis
In general, people with eating upper tract bleeding caused by
rupture of
esophageal varices that have poor liver function / disturbed so
that every large
and small hemorrhage resulted in severe liver failure. Many
factors affect the
prognosis of patients such as age, hemoglobin level, blood
pressure during
treatment, and others. The mortality rate of patients with upper
tract bleeding
meals influenced by factors when treated hemoglobin, occurs /
absence of
rebleeding, heart conditions, such as jaundice, encefalopati and
Child class
criteria.
Given the high mortality and difficulty in tackling eating
Sakuran bleeding
should be considered sections the preventive actions primarily
to prevent liver
cirrhosis.
-
7/28/2019 lp hematomessis melena
15/17
Nursing Diagnosis (Carpenito Juall Lynda)
1. Risk of hypovolemic shock related to with hemorrhage
dilambung
2. Ineffective breathing pattern related to decreased lung
expansion.
3. Nutritional changes (less than requirements) related to with
the inability to
process (digest) food.
4.Anxiety associated with less knowledge of disease
treatment.
5. Activity intolerance related to weakness
C. intervention
1. Nursing Diagnosis. I: Risk of bleeding associated with
hypovolemic shock
dilambung
outcome Not happening hypovolemic shock
Results Criteria: - Perdrahan reduced / stopped
- pulse charging regularly and strong (60-100 x / mnt)
- Decreased blood pressure (110/70 - 120/80 mmHg)
- Akral warm
Action Plan
a. TTV observations and signs of hypovolemic shock every 30
minutes
R / Early detection of changes in patient's condition so as to
determine the
appropriate course of action.
b. If there are signs of hypovolemic shock give the head lower
than feet ..
R / Prevent the occurrence of hypoxia
c. Observation of fluid intake and output
R / Maintaining fluid balance needs remains inadequated. Observe
for bleeding
R / Early detection of changes in patient condition
e. Collaboration with the medical team in the delivery of plasma
expander
R / Replacing the plasma out of blood from vomiting and bowel
movements
2. II Nursing Diagnosis: Ineffective breathing pattern related
to decreased lungexpansion.
outcome Shortness of breath decreases
-
7/28/2019 lp hematomessis melena
16/17
Results Criteria: - normal respiratory frequency (RR 16-20 x /
min).
- There is no additional breath sounds.
- Kx is not hypoxic.
Action Plana. TTV observations client (especially RR).
R / tk Knowing tightness scale Kx.
b. Auscultation of breath sounds Kx.
R / Knowing whether there is an additional breath sounds.
c. Give posisiyang comfortable on Kx as semi-Fowler.
R / Reduce pain.
d. Collaboration with a team of doctors in providing drug
teraepi.
R / Implement independent function.
Nursing Diagnosis. III: Changes in nutrition (lack of necessity)
relating to the inability to
process (digest) food.
outcome patient needs are met
Results Criteria: - There is no abdominal tenderness
- Nausea / vomiting is reduced
- BB increased
- Appetite increased
Action Plan
a. Weigh Kx BB every day.
R / As an indicator / Kx adequate nutritional status or not.
b. HE Erikan on Kx and families about the importance of food /
nutrition for themselves Kx.
R / Kx dapatkooperatif and want to eat.
c. Kx motivation to want to eat.
R / Increase appetite.
d. Collaboration with a team of dietitians in nutrition.
R / Implement independent function
-
7/28/2019 lp hematomessis melena
17/17
References
Smeltzer, Suzanne C. 2002.Buku Ajar Keperawatan Medikal-Bedah
Brunner & Suddarth
volume 2. Jakarta: EGC.
Wilkinson, Judith M. 2007.Buku Saku Diagnosis Keperawatan.
Jakarta: EGC.
.
M. Syaifoellah Noer. Prof. dr, dkk.,Ilmu Penyakit Dalam, FKUI,
Jakarta, 1996.
Marlyn E. Doenges dkk,Rencana Asuhan Keperawatan, Edisi 3, EGC,
Jakarta. 2000.
Lynda Juall Carpenito,Diagnosa Keperawatan, Edisi 8, EGC,
Jakarta, 1999.