Lower motor neuron lesions
LOWER MOTOR NEURON AND LESIONS
Introduction
Lower motor neuron:Come out from the brainstem/spinal cord
nuclei.Connect with skeletal motor end plate on skeletal muscle
fiberThey are the common final motor pathway
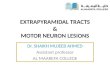
Contribution of lower motor neuron
Muscle spindle
axonLower motor neuron synapses with upper motor neuron,Such
as
LOWER MOTOR NEURONS COMMON PATHWAY
Muscle spindle is sensory organExtra fusal fibers are
contractile unit motor neuron innervates extra fusal fibers motor
neurons innervates muscle spindleIa fibers conduct information from
muscle spindleInformation -> The proprioceptionIa fibers synapse
with MN within spinal cord , the degree of contraction increase( MN
stimulates extra fusal fibers)
-
4 MN -> NMJ -> Ca +2 influx -> AP-> actin-myosin
function-> muscle contraction
Muscle spindle / intra fusal fibers-> stretch receptors
Deep tendon reflex
Strech on tendon-> EFF ->I -> spinal cord-> MN ->
NMJ-> muscle contraction
When over stetch of tendon ->
Golgi tendon organ-> I b fibers -> SC -> innhibitory
inter neuron ->
Lesions may occur in these sites of lower motor neurons
Lower motor neuron lesionsCranial motor nuclei lesions belong to
lower motor neuron lesions CAUSES WHICH MAY DAMAGE THE MOTOR NUCLEI
IN MID BRAINTumor HemorrhageSudden movements of head Damage of both
Occulomotor and Trochlear nuclei will result in impairment of
occular movements
CAUSES WHICH MAY DAMAGE THE MOTOR NUCLEI OF PONSTumorPontine
hemorrhageCAUSES WHICH MAY DAMAGE THE MOTOR NUCLEI IN MEDULLA
OBLONGATARaised pressure in posterior cranial fossa >
Glossopharyngeal motor nuclei > Motor nuclei of vagus >
Hypoglossal nucleiLateral medullary syndrome > Abducent nuclei
> Nucleus ambiguusMedial medullary syndrome > Hypoglossal
nuclei Ipsilateral paralysis of tongue
Occurs when the axon of a neuron is crush or cut across.
Injuries of the axons
Neurapraxia- Due to blockage of nerve conduction.Axonotmesis-
Disruption of nerve cell axon.- Endoneurium is intact.- With
Wallerian degeneration.Neurotmesis- Most serious nerve injury.-
Both the nerve and the nerve sheath are disrupted.
Seddons ClassificationDegree of
injuryMyelinAxonEndo-neuriumPeri-neuriumEpi-neuriumI+/-IINoYesYesNoNoIIINoYesYesYesNoIVNoYesYesYesYesVYesYesYesYesYesSutherlands
classificationNormally innervated muscles respond to stimulation by
the application of interrupted current.Galvanic or direct current
causes contraction only when the current is turned on or turned
off.When the lower motor neuron is cut,After 7 days - No any
muscular response to interrupted electrical stimulation 7 days
after nerve section. (But it will be stillresponding to direct
current.)After 10 days -the response to direct current also
ceases.This change in muscle response to electrical stimulation is
known as the Reaction Of DegenerationReaction Of Degeneration
Reaction Of DegenerationBecause of interruption of the efferent
part of reflex pathways, tendon reflexes are abolished.
Hyporeflexia
Loss Of Reflexes
01 Motor end plate Myasthenia gravis
The immune system inappropriately produce antibodies that bind
to and block some Ach receptors thereby decreasing the number of
functional of skeletal muscles. More receptors are lost. Thus
muscles become increasing weaker, fatigue more easily, and many
eventually cease to function.Effects on muscles02. Muscle spindle
Interruption of motor , pathways anywhere between the motor area of
the cerebral cortex and the muscles produce muscles
paralysis.Inability to move a part of the body is called as
paralysis. In some diseases damage may be confined to lower motor
neurons, and the result in paralysis may be purely flaccid. Such
lesions are accompanied by muscular wasting(atrophy), muscle
twitching(fasciculation), and contracture of opposing muscles. eg:-
poliomyelitis
Effects on muscles When lower motor neurons are destroyed or
their continuity is interrupted , the muscles supplied by them loss
their tone, called as flaccid. (lower motor neuron paralysis)
Flaccid paralysis Destruction of nerve supply. (motor
nerve)Abnormal excitability Sensitive to circulating
AcetylcholineIrregular contraction of individual fiber
(fibrillation )Muscular Atrophy
Jerky visible contraction of group of muscle fibers.Pathological
discharge of spinal motor neuron.Muscular Fasciculation
This is a shortening of the paralyzed muscles.It occurs more
often in the antagonist muscles whose action is no longer opposed
by the paralyzed muscles.Muscular ContractureLower motor neurons
lesionsCauses- Trauma Infection Vascular disorders Degenerative
disease Neoplasm
fDestroy the cell bodies in anterior gray matter or its axon in
anterior root of spinal nerve28Principal Features of UMNL &
LMNLUMNL: (1) No muscle wasting, except from disuse ( disuse
atrophy)(3) Spasticity ( hypertonia ) , called clasp-knife
spasticity (4) Clonus present (5) Brisk ( exaggerated ) tendon
jerks (6) Extensor plantar reflex , Babinski sign ( dorsiflexion of
the big toe and fanning out of the other toes ) (7) Absent
abdominal reflexes (8) No fasciculations(9) No fibrillation
potential in EMG
{ LMNL: (1) Marked muscle wasting (atrophy ) (3) Flacidity
(Hypotonia ) , hence given the name flaccid paralysis (4) No
clonus(5) Diminished or absent tendon reflexes(6) Absent plantar
reflex (normally it is flexor ) . (7) Absent abdominal reflexes(8)
Fasciculations may occur . (9) Fibrillation potentials present
.
THANK YOU
Presented by 3rd group