Embed Size (px)
Citation preview

Clinical Oncology (2006) 18: 129e132doi:10.1016/j.clon.2005.09.008
Original Article
Low-dose Prophylactic Cranial Irradiation in Patientswith Poor Prognosis Small-cell Lung Cancer
A. M. Henry, M. P. Snee
Cookridge Hospital, Hospital Lane, West Yorkshire, UK
ABSTRACT:Aims: In small-cell lung cancer (SCLC), prophylactic cranial irradiation (PCI) provides a survival advantage in goodperformance status patients with limited disease. Its role in those with poor performance status limited disease orextensive disease is unclear. A low-dose PCI schedule has been used in these groups, and outcomes have been analysed.Materials and methods: Retrospective analyses of brain metastasis-free survival and overall survival of patientsreceiving low-dose PCI over a 2-year period.Results: Fifty-six patients were treated, with 55 evaluable due to missing notes for one. No major treatment-relatedtoxicity was observed. Median brain metastasis-free survival and overall survival for the group were 44 and 46 weeks,respectively. The median brain metastasis-free survival were 32 and 50 weeks, and median overall survival were 39 and57 weeks, in those with extensive and limited disease, respectively. A total of 10 patients developed clinical orradiological evidence of brain metastases, four (16%) with limited disease and six (21%) with extensive disease. Thirteen(52%) with limited disease and 10 (36%) with extensive disease survived 1 year.Conclusions: Symptomatic brain metastases occurred less frequently than would be expected, with most patientsdeveloping widespread metastatic disease. Low-dose PCI may benefit these groups, and the results of an ongoing EORTCrandomised-controlled trial in extensive disease should provide more information. Henry, A. M., Snee, M. P. (2006).Clinical Oncology 18, 129e132
ª 2005 The Royal College of Radiologists. Published by Elsevier Ltd. All rights reserved.
Key words: Cranial metastases, prophylactic cranial irradiation (PCI), small-cell lung cancer (SCLC)
Introduction
Small-cell lung cancer (SCLC) makes up 25% of all lungcancers diagnosed. Extensive disease is found in 70% ofpresenting patients. Although disease is initially responsiveto chemotherapy, drug resistance is acquired during thecourse of treatment. Clinically apparent cerebral metasta-ses will develop in about 70% of patients within 2 years [1].Symptomatic brain metastases are more likely to develop inextensive disease compared with limited disease and, onceestablished, respond poorly to cranial irradiation [2].
A meta-analysis of PCI in patients who achieveda complete response to chemotherapy has shown an overallsurvival advantage of about 5% at 3 years [3]. Although thismeta-analysis included a small proportion of patients withextensive disease, PCI is generally only routinely offered topatients with limited disease, achieving a complete re-sponse to chemotherapy [4]. The demographics of themeta-analysis show patients had a median age of 59 years,with over 90% having World Health Organization (WHO)performance status of 1 or over. Therefore, in routinepractice, PCI is generally not offered to people aged over70 years or with WHO performance status of 2 or over.
0936-6555/06/180129C04 $35.00/0 ª 2005 The Royal
Within our centre, a simple low-dose PCI schedule hasbeen used to treat patients with poor prognosis SCLC. Thedefinition of poor prognosis includes those patients withextensive disease achieving a partial or complete responseto chemotherapy, and those with limited disease achievinga partial response to chemotherapy or a complete responsebut poor performance status, aged over 70 years, or both. Aretrospective analysis of outcome, in terms of brainmetastasis-free and overall survival, has been undertaken.
Materials and Methods
The outcome of all patients with SCLC who underwent low-dose PCI (12 Gy given in 2 fractions over 2 days) betweenJuly 1999 and July 2001 was retrospectively analysed.Patients presenting with brain metastases, or those de-veloping brain metastases during chemotherapy, wereexcluded. As discussed previously, low-dose PCI was offeredto patients with extensive disease, achieving a complete orpartial response to chemotherapy. Those patients withlimited disease but not achieving a complete response tochemotherapy or having a poor performance status were
College of Radiologists. Published by Elsevier Ltd. All rights reserved.

130 CLINICAL ONCOLOGY
also offered treatment. Patients with a WHO performancestatus of 4 were not treated. Patients were identified fromplanning clinic records and chemotherapy databases.
Whole-brain cranial irradiation was given after chemo-therapy had been completed, usually within 6 weeks. Thelower field border from tragus to lateral supra-orbital ridgewas marked on the patient in the planning clinic. A lateralparallel-opposed pair of fields was used at a fixed source toskin distance, giving a mid-plane dose of 12 Gy delivered intwo doses over 2 days as an outpatient. Cobalt-60 or 6 MVphotons were used. Steroid cover was not used.
Patients were followed up at 6 weeks in an oncologyclinic. Thereafter, they were seen every 3 months, or morefrequently if clinically indicated. Patients with symptomssuggestive of brain metastases underwent urgent braincomputed tomography. Symptom checklists were not used.
Data on patients were collected from individual casenotes and death certificates. The following information wascollected: sex, age at diagnosis, stage at diagnosis, WHOperformance status at diagnosis, date of first chemother-apy, type and number of chemotherapy cycles given,response to chemotherapy, use of second-line chemother-apy on relapse, treatment-related toxicity and hospitaladmissions and date of death or last follow-up.
Patient characteristics and outcomes were analysed forthe group as a whole and by stage at presentation. Endpoints were brain metastasis-free survival, defined as timein weeks from the date of first chemotherapy to the clinicalor radiological development of brain metastasis and overallsurvival, defined similarly. KaplaneMeier survival curveswere calculated for both actuarial brain metastasis-freesurvival and overall survival.
Results
A total of 56 patients were treated with low-dose PCI in the2-year period. Thirty-seven (66%) patients were men and 19(34%) were women. Notes for one patient were missing,leaving a total of 55 evaluable patients. In an additionaltwo patients, the initial stage was not recorded, and theywere therefore excluded from the analysis by stage atpresentation.
Table 1 summarises the patient characteristics andoutcomes by stage at presentation. Age distribution,performance status and proportion achieving completeresponse with initial chemotherapy were similar in patientswith limited and extensive disease. Reasons for notdelivering standard PCI in people with limited SCLCachieving a complete response to chemotherapy were ageover 70 years (nZ 6) and WHO performance status of 3, orsignificant co-morbidity (nZ 4). Thoracic radiation wasdelivered more frequently in people with initial limiteddisease: 80% vs 54% in the extensive disease group.
Chemotherapy regimens were CAV (cyclophosphamide,adriamycin, vincristine), ICE (ifosphamide, carboplatin,etoposide), EP (etoposide, cisplatinum), MVP (mitomycin C,vinblastine, cisplatin) and single-agent carboplatin. Onepatient was treated with MVP chemotherapy on the basis of
an initial histology report of non-small-cell lung cancer,which was found to be SCLC on histology review. Thenumber of chemotherapy cycles given ranged from 2 to 6(median four cycles) in both groups. About a quarter ofpatients in both groups underwent treatment with second-line chemotherapy on developing progressive disease. Nopatients experienced significant documented acute toxicityor required hospital admission after PCI.
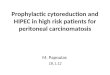
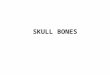
The median brain metastasis-free survival for the groupwas 44 weeks and median overall survival 46 weeks. Whenanalysed by stage at presentation, the median brainmetastasis-free survival and overall survival were 50 vs 32weeks and 57 vs 39 weeks for the limited and extensivedisease groups, respectively (Figs. 1 and 2). A total of 10patients developed clinical or radiological evidence of brainmetastases, four (16%) in the limited disease group and six(21%) in the extensive disease group. Thirteen (52%) withlimited disease and 10 (36%) with extensive diseasesurvived over 1 year.
Discussion
This group of patients has a poor prognosis, and ultimatelytreatment is aimed at relieving or delaying the onset ofdisease-related symptoms rather than improving overallsurvival. Brain metastases cause disabling and distressingsymptoms, which can be difficult to palliate once estab-lished. Isolated brain metastases respond poorly to radio-therapy, with only 50% of patients treated obtainingimprovement or stabilisation of neurological symptoms,and this is often short-lived [2]. Performance status candeteriorate rapidly, precluding further palliative chemo-therapy. The median age of those with limited disease was69 years, with over half the group with performance status2 or over. Low-dose PCI may be of benefit in reducing the
Table 1 e Characteristics and outcomes of patients with small-cell lung cancer receiving low-dose prophylactic cranial irradi-ation according to stage
Limitedstage
Extensivestage
Group total 25 28Median age (range) 69 (51e79)
years67 (49e73)years
Achieving initialcomplete response (%)
10 (40) 9 (32)
Performance status 0e1 (%) 10 (40) 14 (50)Performance status 2C (%) 13 (52) 10 (36)Second-line chemotherapy (%) 6 (24) 8 (29)Thoracic radiation (%) 20 (80) 15 (54)Developing symptomaticbrain metastases (%)
4 (16) 6 (21)
1-year survival (%) 13 (52) 10 (36)Median brain metastasis-freesurvival
50 weeks 32 weeks
Median overall survival 57 weeks 39 weeks

131LOW-DOSE PROPHYLACTIC CRANIAL IRRADIATION IN PATIENTS
risk of developing symptomatic brain metastasis in thispopulation who would not generally be offered PCI even onachieving complete response with initial chemotherapy.Patients with extensive disease have an even higher risk ofdeveloping brain metastases than those with limiteddisease, with published rates of about 70% if surviving 2years [1]. Using this low-dose PCI schedule, symptomaticbrain metastases occurred less frequently (about 20%) thanwould be expected. Most patients died of widespread
Fig. 1 e KaplaneMeier curves demonstrating brain metastasis-freesurvival for both limited and extensive stage groups.
Fig. 2 e KaplaneMeier curves demonstrating overall survival forboth limited and extensive stage groups.
disease rather than isolated spread to the brain only. PCIseemed to be effective in reducing the rate of symptomaticand isolated brain metastasis in these high-risk groups,thereby improving overall palliation.
Deriving firm conclusions from retrospective data isfraught with difficulty. Ascertaining actual of death fromdeath certificates, hospital notes, or both, can be unreli-able and inaccurate, as dying patients are often managed inprimary care and are also unlikely to undergo postmortemexaminations. It is likely that a significant proportion of thispopulation have occult brain metastases at death. Anongoing EORTC study randomising patients with extensivedisease and initial response to chemotherapy to PCI orsupportive care alone should provide more information onthe benefits of PCI in this group. After treatment in theEORTC study, participants are seen regularly to checksystematically for symptoms of brain metastases, docu-ment quality-of-life scores and carry out contrast-enhancedcomputed tomography, magnetic resonance imaging, orboth, if there is suspicion of brain metastases. Regularcomputed tomography surveillance is not required, as it hasnot been shown to be of benefit in detecting early SCLCbrain metastases [5].
The main drawback in using PCI routinely in this group ofoften poor performance status patients is the associatedacute and late treatment-related toxicity. Acute sideeffects of PCI include rigors, nausea and vomiting,headache, anorexia and lethargy. These can be treatedsymptomatically and are generally self-limiting. Thisschedule seems to be well tolerated, with none of thepatients experiencing significant documented acute toxic-ity or requiring hospital admission. Few patients in thesegroups survive in the long term. Studies in good-prognosispatients show that some will develop dementia, but a directlink with cranial irradiation has not been supported byprospective studies. A significant proportion of patientswith SCLC have abnormalities on neuropsychological testingand computed tomography scanning before PCI, reflectingthe significant comorbidities seen in this population. Onlyone study has examined quality of life, albeit in onlya proportion of the study group [6]. No significant differ-ences were seen between those patients who received PCIand those who did not in the 12 months after treatment.
Many different radiation schedules are used to deliverPCI. A trend for decreased brain metastasis rates withhigher doses of radiation [3], with a dose response up to30e35 Gy is noted [7]. In this poor-prognosis group,schedules should be short and, within the EORTC study,treatment can be delivered as 20 Gy in 5 fractions or 30 Gyin 10e12 fractions. We use a hypofractionated schedule,and the biologically effective dose is about 20 Gy fortumour effects and 48 Gy for late effects, assuming a/b ratios of 10 and 2 Gy, respectively. This schedule may notdeliver the optimal biological dose to eradicate micro-metastatic disease, and may have increased risks of lateeffects compared with longer fractionation schedules. Itrepresents a compromise between theoretical biologicaloptimisation and practical implementation within a busydepartment.

132 CLINICAL ONCOLOGY
As discussed, the role of PCI in extensive SCLC iscurrently under investigation in a randomised-controlledEORTC trial with participants randomised into PCI or nointervention arms. The primary end point is brainmetastasis-free survival, with secondary end points ofquality of life, overall survival and toxicity, includingcognitive impairment. This study will provide morecomprehensive information on the general effects ofcranial irradiation, and may provide the answer towhether PCI has a significant role to play in extensivedisease.
Acknowledgements. The authors would like to thank Dr Dearb-haile O’Donnell for helpful comments on the paper and Dr JulianAdlard for the production of figures.
Author for correspondence: Dr AnnM.Henry, Consultant in ClinicalOncology, Cookridge Hospital, Hospital Lane, Leeds LS10 1JJ, UK.Tel:C44-113-267-3411; Fax:C44-113-392-7576; E-mail: [email protected]
Received 19 January 2005; received in revised form 12 September2005; accepted 15 September 2005
References
1 Van Oosterhout AG, Van de Pol, Ten Velde G, Twijnstra A.Neurologic disorders in 203 consecutive patients with small celllung cancer: results of a longitudinal study. Cancer 1996;77:1434e1441.
2 Postmus PE, Haaxma-Reiche H, Gregor A, et al. Brain-onlymetastases of small cell lung cancer: efficacy of whole brainradiotherapy. An EORTC Phase II study. Radiother Oncol 1998;46:29e32.
3 Auperin A, Arriagada R, Pignon JP, et al. Prophylactic cranialirradiation for patients with small cell lung cancer (SCLC) incomplete remission (CR). N Engl J Med 1999;341:476e484.
4 COIN Guidelines on the non-surgical management of lung cancer.The Royal College of Radiologists’ Clinical Oncology InformationNetwork, Feb 1999.
5 Hardy J, Smith I, Cherryman G, et al. The value of computedtomography (CT) scan surveillance in the detection and manage-ment of brain metastases in patients with small cell lung cancer.Br J Cancer 1990;62:684e686.
6 Gregor A, Cull A, Stephens RJ, et al. Prophylactic cranialirradiation is indicated following complete response to inductiontherapy in small cell lung cancer: results of a multi-centrerandomized trial. Eur J Cancer 1997;33:1752e1758.
7 Suwinski R, Lee SP, Withers HR. Doseeresponse relationship forprophylactic cranial irradiation in small cell lung cancer. Int JRadiat Oncol Biol Phys 1998;40:797e806.