Embed Size (px)
Citation preview
12/3/2010
1
LOW BACK PAIN IN PRIMARY CARE
UCSF 5th Annual Primary Care Sports Medicine ConferenceDecember 3, 2010
Carlin Senter, M.D.Assistant Clinical ProfessorPrimary Care Sports MedicineUCSF Orthopaedic Surgery and Internal Medicine
Impact of low back pain• 5th most common reason people go to doctor in the U.S. 1
• 25% of adults reported LBP for at least 1 day in past 3 months when surveyed 2
• 2% of U.S. workforce compensated for back injuries yearly 3
1. Hart LG et al. Spine, 1995.2. Deyo RA et al. Spine, 2006.3. Andersson GB. Lancet, 1999.
Pearls• Kids with LBP ≠ adults with LBP• Identify red flags/non mechanical LBP early• Imaging often unnecessary outside of red flags
• Exercise is key to patients’ prescriptions

12/3/2010
2
LBP in kids ≠ adults• Majority of adults have LBP that cannot be attributed to
identifiable disease or spinal abnormality • Much more common to diagnose a cause in children• Work up pediatric back pain more aggressively than adult
Epidemiology: young athletes with LBP
• Rowing: low back most common site of injury in elite-level junior rowers (32.3% of all injuries) 1
• Gymnastics: 43% of high school injuries involve back 2
• Dancers: 11-18% have low back pain 3
• Figure skaters: 32% female and 35% male complain of LBP 4
1. Smoljanovic T et al. AJSM, 2009.2. Garrick and Requa AJSM, 1980.3. Micheli LJ, Clin Sports Med, 1983.4. Dubravcic-Simunjak S, AJSM, 2003.
History, young athlete• Sport involvement• Relation of pain to sports• Axial vs. peripheral symptoms
• Red flags• Night pain• Immunosuppressant medication• Bowel/ bladder involvement• Systemic symptoms
• Family history• Disc• Connective tissue disorders• Spinal curve disorders
D’Hemecourt PA, AMSSM 19th Meeting, April 2010.
Causes of acute LBP differ by age
Lesion Youth (%)
Adult (%)
P value
Discogenic 11 48 0.05
Spondylolysis or spondylolisthesis
47 5 0.05
Lumbosacral strain 6 27 0.05
Hyperlordotic mechanical back pain
26 0
Spinal stenosis 0 6
Osteoarthritis 0 4
Micheli and Wood. Arch Pediatr Adolesc Med, 1995.
12/3/2010
3
Causes of LBP by age• < 18 y/o spondylolysis• 18 –50 y/o discogenic pain and herniated disc• >50 y/o facet arthropathy, spondylosis/spinal stenosis
Mautner K, AMSSM 19th Meeting, April 2010.
Goal when seeing patient with LBP1. Rule out non-mechanical low back pain
• Serious spine pathology• Non-spine causes of LBP• Substantial neurologic involvement
2. Treat mechanical low back pain (85% of cases)
7-8% of patients with LBP
Causes of LBP in adults• 85% nonspecific, mechanical low back pain• 4% compression fracture• 4% herniated disc
• 3% spinal stenosis• 0.7% cancer• 0.3-5% ankylosing spondylitis• 0.04% cauda equina syndrome• 0.01% spinal infection
MacDonald J. Back Pain in Primary Care, 2009.
Non-msk causes of LBP• Pancreatitis• Nephrolithiasis• Aortic aneurysm
12/3/2010
4
Ddx mechanical low back pain• Lumbar sprain or strain – 70%• Degenerative disease – 10%• Herniated disk – 4%
• Compression fracture – 4%• Spinal stenosis – 3%• Spondylolisthesis – 2%• Spondylolysis – 2%• Traumatic fracture – 1%
Red flags for serious spine pathology1. Cancer2. Cauda equina syndrome3. Fracture
4. Infection
Cancer• Age > 50• H/o cancer• Fever
• Unintentional weight loss• Pain awakening from sleep
Cauda equina syndrome• Bowel/bladder incontinence or constipation• Urinary retention most frequent symptom in cauda equina
syndrome (90% sensitivity)

12/3/2010
5
Fracture• Age > 50• Osteoporosis• Steroid use
• Trauma
Infection• Fever• Immunosuppression• IVDU
Other causes of LBP1. Ankylosing spondylitis
• Night pain• Morning stiffness• Sxs improve with exercise• FHx
2. Abdominal aortic aneurysm• Age > 60• Atherosclerosis• Pulsating abdominal mass• Night pain
3. Pyelonephritis/nephrolithiasis4. Pancreatitis
If (+) red flag• Imaging
• XR• MRI• CT
• Labs• ESR, CRP
• Referral to specialist
12/3/2010
6
Rule out substantial neurologic involvement• Abnormal neurologic exam• Symptoms that do not improve with conservative
management• MRI or CT to identify potential surgical candidates
Risk factors for chronic LBP: yellow flags
• Most patients with acute LBP do not develop chronic LBP
• Risk factors for pain > 1 year• Psychiatric comorbidities• Avoiding work, movement, or activity for fear of worsening the
back pain• More generalized pain at baseline• Baseline functional impairment
• Recognizing these can help guide management + expectations
Chou R and Shekelle P. JAMA, 2010.
History, adult• Trauma• Overuse• Location of pain
• Radiation• What makes it better?• What makes it worse?• Red flags
Physical exam back and hip• 9:20am On-Screen Demo with Dr. Luke• Tomorrow 4:15pm Hands On Workshop with me
12/3/2010
7
Imaging lumbar spine• Xray: AP and lateral sufficient
• Oblique if concerned spondy
• CT: good for bone lesions, fractures.• Lots of radiation
• MRI: good for soft tissue, ligaments, discs• Expensive
• SPECT: good for r/o spondylolysis
Case #1• 20 y/o football player and wrestler• R buttock pain late in the season• No specific injury
• No radiation• Rested from practice 1 week, didn’t miss any games• Pain gone by end of season
MacDonald J. Back Pain in Primary Care, 2009.
Case #1 (cont’d)• Pain immediately returned with wrestling• Developed R lateral thigh pain, anterolateral calf pain• Unable to continue wrestling
• No LE weakness, no bowel/bladder symptoms• Pain worse sitting than standing• No PMHx, no FHx of disc disease
Case #1 examination• Standing, back AROM
• Low back pain radiating to RLE with flexion• No pain with extension• Lumbar scoliosis
• Straight leg raise (+) at 45°• Neurologic
• 1+ right patellar reflex, otherwise normal
• Xrays: scoliosis
MacDonald J. Back Pain in Primary Care, 2009.

12/3/2010
8
Ddx flexion-based pain
• Disc pathology: #1 in age 18-50• Discogenic • Herniated disc �
radicular sxs
• Lumbar sprain/strain• Facet joint arthropathy: #1 in age > 50
Lumbar disc herniation• Pain with flexion• Pain reproduced with SLR between 30-70°• 95% occur at L4-5 and L5-S1
• Cause sciatica• 90% improve with non-operative treatment• Resolution of sciatica
• 50% by 1 month• 75% by 6 months
• Imaging: MRI• If no improvement x 4-6 weeks
• If candidate for epidural steroid injection or surgery
Treatment acute low back pain with or without sciatica• Routine imaging: not necessary
• Doesn’t identify the cause• Doesn’t improve outcome• Costs more
• Relative rest• Better results than bed rest
• Self care • The Back Book• Group classes
• Heat for short-term relief
Chou R et al. Ann Intern Med, 2007.
Medications for acute low back pain +/-sciatica• NSAIDs more effective than acetaminophen
• Assess CV and GI risks before rx• Lowest effective dose possible, shortest time period
• Opioids for acute or chronic disabling pain, careful risk/benefit
• Muscle relaxants• TCAs for chronic low back pain• Gabapentin � short-term relief in radiculopathy• Systemic steroids not recommended: no more effective
than placebo
Chou R et al. Ann Intern Med, 2007.

12/3/2010
9
Non-pharmacologic treatment of chronicLBP• Acupuncture• Exercise therapy (PT)• Massage• Yoga• Cognitive-behavioral therapy
• Progressive relaxation• Spinal manipulation
Berman BM. NEJM, 2010.
Case #2• 73 y/o woman with LBP x 4 months• Radiates to buttocks � knees• No trauma
• (-) red flags• Used to walk 2 miles/day but now only 2 blocks due to
pain• Pain relieved with sitting• Pain worse walking downhill
Ddx extension-based pain (tennis, golf)
• Lumbar strain/sprain• Spondylolysis/spondylolisthesis
• Isthmic spondy in young• Degenerative spondy in elderly
• Spinal stenosis• Facet joint arthropathy
Diagnosis: Spinal stenosis or neurogenic claudication
• Physical exam usually normal, imaging not necessary usually• Treatment
• Flexion-biased core stabilization exercise program• Epidural steroid injection• Surgical decompression +/- fusion
Cody RC. AMSSM 19th Meeting, April 2010.
12/3/2010
10
Case #3• 16 y/o RHD male baseball pitcher• Increased left-sided LBP• Worse with throwing, especially late in the delivery• Rested x 2 weeks � helped
• Pain comes back as soon as returns to pitching
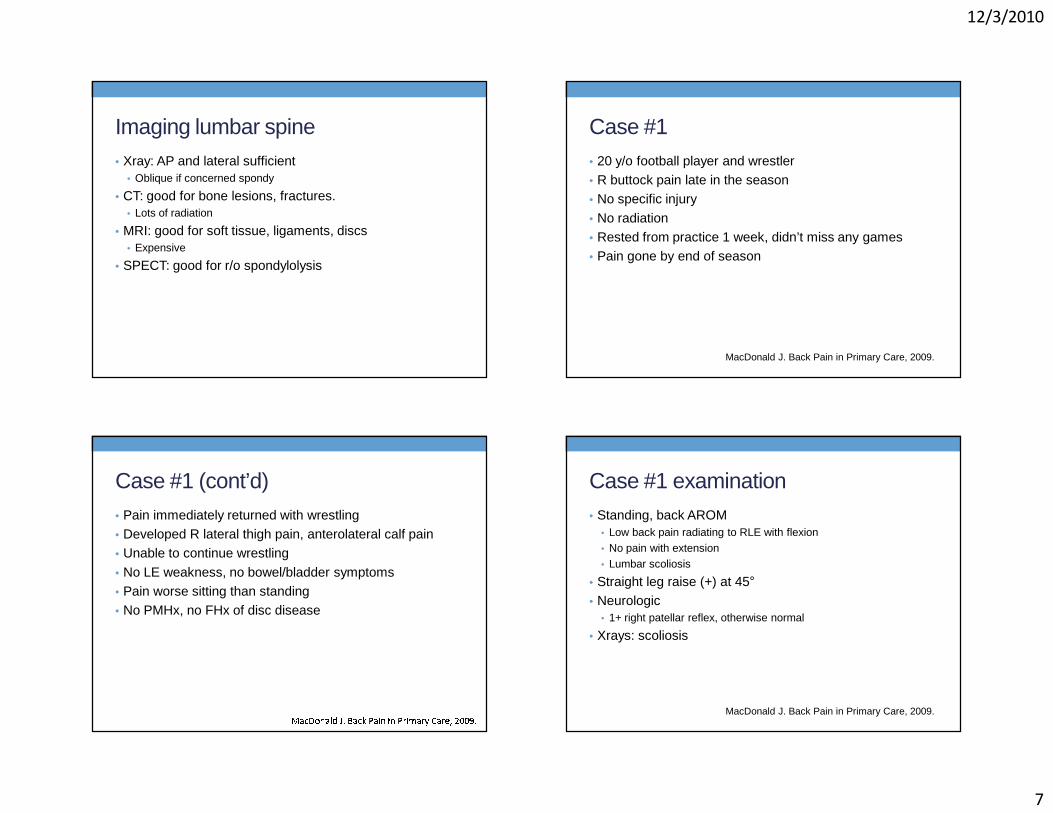
Physical examinationINSPECTION• 6’, 180 pounds• Posture within normal
limitsPALPATION• Minimal tenderness of TS,
LS standingRANGE OF MOTION• Extension 30° mild midline
pain LS; Flexion 60°OTHER TESTS• 1 leg-hyperextension test
positive• Neurological status normal
Differential diagnosis• Age < 18, extension-based back pain
• Spondylolysis• Spondylolisthesis• Lumbar sprain/strain
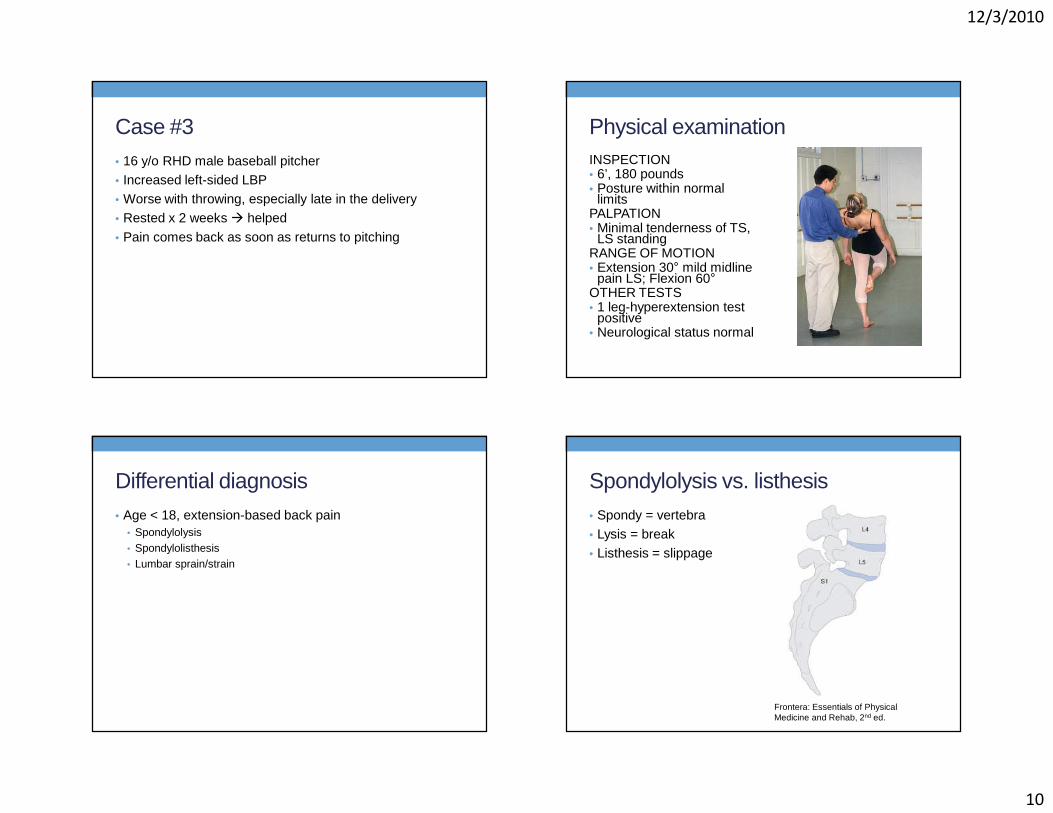
Spondylolysis vs. listhesis• Spondy = vertebra• Lysis = break• Listhesis = slippage
Frontera: Essentials of Physical Medicine and Rehab, 2nd ed.

12/3/2010
11
Lumbar spine xrays: AP and lateralLumbar spine xrays: right and left oblique
Additional imaging• SPECT scan
• High sensitivity for spondylolysis• Lower specificity
• Facet arthritis, infection, osteoid osteoma
• Can identify stress injury before fx occurs
• Ionizing radiation
• CT or MRI to diagnose and stage the lesion• Acute or chronic
Treatment• Physical therapy• Activity Modification / Rest x 3 months• Avoid aggravating activity
Controversial• Modify activities only vs Bracing

12/3/2010
12
Take-home points• Kids with LBP ≠ adults with LBP• Identify red flags/non mechanical LBP early• Imaging often unnecessary outside of red flags
• Exercise is key to patients’ prescriptions THANK YOUCarlin Senter, M.D.UCSF Orthopaedics and Internal [email protected]
References1. Andersson GB. Epidemiological features of chronic low back pain. Lancet. 1999;354:581-5.2. Berman BM, Langevin HM, Witt CM, Dubner R. Acupuncture for chronic low back pain. N Engl J Med.
2010 Jul 29;363(5):454-61.3. Campbell RS, Grainger AJ, Hide IG, Papastefanou S, Greenough CG. Juvenile spondylolysis: a
comparative analysis of CT, SPECT and MRI. Skeletal Radiol. 2005 Feb;34(2):63-73.4. Chou R, Qaseem A, Snow V, Casey D, Cross JT Jr, Shekelle P, Owens DK; Clinical Efficacy
Assessment Subcommittee of the American College of Physicians; American College of Physicians; American Pain Society Low Back Pain Guidelines Panel. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007 Oct 2;147(7):478-91.
5. Chou R and Shekelle P. Will this patient develop persistent disabling low back pain? The Rational Clinical Examination. JAMA. 2010 April 2(303):1295-1302.
6. Cody RC. Back pain in the aging athlete: pathophysiology and evidence-based treatment. AMSSM 19th Annual Meeting, April 21, 2010.
7. D’Hemecourt PA. Pediatric back pain: Acute and chronic issues. AMSSM 19th Annual Meeting, April 21, 2010.
8. Dagenais S, Tricco AC, Haldeman S. Synthesis of recommendations for the assessment and management of low back pain from recent clinical practice guidelines. Spine J. 2010 Jun;10(6):514-29.
9. Dahm KT, Brurberg KG, Jamtvedt G, Hagen KB. Advice to rest in bed versus advice to stay active for acute low-back pain and sciatica. Cochrane Database Syst Rev. 2010 Jun 16;(6):CD007612.
References10. Deyo RA, Mirza SK, Martin BI. Back pain prevalence and visit rates: estimates from U.S.
national surveys, 2002. Spine. 2006;31:2724-7.11. Gregory PL, Batt ME, Kerslake RW, Webb JK. Single photon emission computerized
tomography and reverse gantry computerized tomography findings in patients with back pain investigated for spondylolysis. Clin J Sport Med. 2005 Mar;15(2):79-86.
12. Hart LG, Deyo RA, Cherkin DC. Physician office visits for low back pain. Frequency, clinical evaluation, and treatment patters from a U.S. national survey. Spine. 1995;20:11-9.
13. Leone A, Cianfoni A, Cerase A, Magarelli N, Bonomo L. Lumbar spondylolysis: a review. Skeletal Radiol. 2010 May 4.
14. MacDonald J, Back Pain in Primary Care, UCSF 4th Annual Primary Care Sports Medicine Conference, Dec 13 2009.
15. Mautner, K. Back pain in the young adult: pathophysiology and evidence-based treatment. AMSSM 19th Annual Meeting, April 21, 2010.
16. Smoljanovic T, Bojanic I, Hannafin JA, Hren D, Delimar D, Pecina M. Traumatic and overuse injuries among international elite junior rowers. Am J Sports Med. 2009 Jun;37(6):1193-9.
17. Tsirikos AI, Garrido EG. Spondylolysis and spondylolisthesis in children and adolescents. J Bone Joint Surg Br. 2010 Jun;92(6):751-9.
18. Vanwye WR. Nonspecific low back pain: evaluation and treatment tips. J Fam Pract. 2010 Aug;59(8):445-8.





























