Embed Size (px)
Citation preview
http://qhr.sagepub.com/Qualitative Health Research
http://qhr.sagepub.com/content/17/4/501The online version of this article can be found at:
DOI: 10.1177/1049732307299215
2007 17: 501Qual Health ResPádraig Mac Neela, P. Anne Scott, M. Pearl Treacy and Abbey Hyde
Lost in Translation, or the True Text: Mental Health Nursing Representations of Psychology
Published by:
http://www.sagepublications.com
can be found at:Qualitative Health ResearchAdditional services and information for
http://qhr.sagepub.com/cgi/alertsEmail Alerts:
http://qhr.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://qhr.sagepub.com/content/17/4/501.refs.htmlCitations:
What is This?
- Apr 6, 2007Version of Record >>
at UNIVERSITY OF WINDSOR on July 8, 2014qhr.sagepub.comDownloaded from at UNIVERSITY OF WINDSOR on July 8, 2014qhr.sagepub.comDownloaded from
Lost in Translation, or the True Text: Mental Health Nursing Representations of Psychology
Pádraig Mac NeelaNational University of Ireland, Galway
P. Anne ScottDublin City University, Ireland
M. Pearl TreacyAbbey HydeUniversity College Dublin, Ireland
One theme of academic discourse and research in mental health nursing is the exploration and application of psychoso-cial models of nursing practice. Despite this, the influence of disciplinary psychological knowledge on practitioners’ talkabout nursing practice has not been extensively researched. To address this gap, the authors analyzed talk about psy-chological work using transcripts of 10 focus groups involving 59 mental health nurses. Nurses identified a psycholog-ical domain of practice as central to their work. Given the amount of time spent with clients, nurses are the primeresource for psychological work. Psychological talk was organized into three categories related to the nursing processand organizational context and analyzed through empowerment and critical perspectives on power. Although technical(“formal”) and everyday (“informal”) discourses were generally well integrated, the authors question the oral basis tothis body of knowledge in terms of accountability to service users and as a marker of disempowerment.
Keywords: mental health nursing; psychology; empowerment; social representations; lifeworld; qualitativeresearch
The influence of psychological concepts and tech-niques on mental health nursing is evident in pre-
registration training and professional developmenttexts (e.g., Barker, 1997; Thomas, Hardy, & Cutting,1997). Although psychological concepts are seen ascentral, this domain of activity is identified as “nursing”rather than “psychology.” With mental health nursingengaged in an “unending quest for a firm integratedidentity” (Keen, 2003, p. 34), there is a divergence ofviews on the discipline’s future development (e.g.,Barker, 2000; Gournay, 2000). Debate focuses on the rel-ative merits of a control-based, medically oriented model(“psychiatric” nursing) and one that is psychosociallyoriented (“mental health” nursing; Howell & Norman,2000).
The psychosocial model of nursing care drawsextensively on psychological theory and interventions,but the relationship between mental health nursing and psychology has not been unraveled. Although thenurse therapist role (e.g., Bracey, 2002) positionsnurses as providers of formal psychotherapeutic care,
the nurse-client relationship encompasses an informalpsychosocial role through which care is delivered (e.g.,“ordinary me,” Barker, Jackson, & Stevenson, 1999,p. 275). Reflecting the invisibility of nursing care gen-erally (Clark & Lang, 1992), the formal and informaluses mental health nurses make of psychology havebeen largely unstudied.
Social psychological and sociological perspectivesprovide potentially useful analytic tools for exploringthe use of psychological discourse in mental healthnursing. Overall, nursing has been considered a profes-sion affected by disempowerment (e.g., Porter, 1998),standing in distinct power and status relations to other
501
Qualitative Health ResearchVolume 17 Number 4April 2007 501-509
© 2007 Sage Publications10.1177/1049732307299215
http://qhr.sagepub.comhosted at
http://online.sagepub.com
Authors’ Note: This research was supported through the IrishHealth Research Board Research Programme in Nursing DecisionMaking. Correspondence concerning this article should beaddressed to Dr. Pádraig Mac Neela, Department of Psychology,National University of Ireland, Galway, Ireland. Phone number: 35391 495121; fax number: 353 91 521355; e-mail: [email protected]
at UNIVERSITY OF WINDSOR on July 8, 2014qhr.sagepub.comDownloaded from

502 Qualitative Health Research
professional groups. In this context, formal psycholog-ical knowledge can be seen as a tool of oppression,alienating nursing knowledge from credible clinicaldiscourse. Alternatively, given the utility of being ableto name and classify clinical phenomena and practices,psychology can be constructed as a useful languageresource, empowering psychosocial nursing practice.
Empowerment research (e.g., Gilbert, 1995) is use-ful in exploring these two perspectives on nursingknowledge. Kanter (1993) proposed that the perceptionof empowerment is based on a rational evaluation of theenvironment. In addition, the socialization processinfluences the experience of empowerment through theintrojection of attitudes and nursing culture (Farnell &Dawson, 2006; Melia, 1987). In the process perspective(Kanter, 1993), disempowerment arises from structuralconditions in the work environment. The way in whichwork is organized determines nurses’ access to formaland informal power, expressed through access to infor-mation, resources, support, and opportunities for devel-opment (Laschinger, Finegan, Shamian, & Wilk, 2001).The experience of empowerment (psychologicalempowerment) is based on the perception of personalcontrol. This is reflected in levels of competence andautonomy (Spreitzer, 1995), which are, in turn, associ-ated with positive personal and organizational out-comes (e.g., Ellefsen & Hamilton, 2000).
Considering psychology as a disempowering influ-ence is consistent with the idea that formal, rule-basedsystems threaten the implicit and shared sense of mean-ing underpinning everyday group functioning. Theinformal nursing lifeworld (Habermas, 1981) is liableto disruption through oppressive regulation (Hyde et al.,2005). Applied to mental health nursing and psychology,this suggests a role for psychiatric-psychological lan-guage in formalizing and fixing nurses’understanding ofthe patient’s experience. This is potentially disempower-ing if perceived as undermining and subjugating experi-ential nursing knowledge.
Rather than considering psychology a means ofmaking nursing a tool of psychiatric medicine, psycho-logical concepts and techniques can be recast within thevalues of mental health nursing. In his theory of socialrepresentations, Moscovici (1984) proposed that a socialgroup’s collective identity and knowledge are expressedthrough a framework of social representations. A socialrepresentation is an implicit, shared understanding of aphenomenon (Howarth, 2006), which shapes experi-ence through its naming and classification functions.Accumulated, shared knowledge assists in the accultur-ation of novel concepts and terms. The assimilation of
external language terms within the existing network ofthe group’s social representations serves an adaptivefunction. Appropriating psychological terminology andinvesting it with nursing meaning can support theexpression of professional knowledge. Health profes-sionals’ social representations of health have been littleexamined to date, especially in the context of powerrelations (Howarth, 2006).
These perspectives suggest two positions to inves-tigate in considering the relationship of psychologyand mental health nursing: psychology as a disem-powering colonizer of the nursing lifeworld, unwel-come and resisted, and psychology as an empoweringinfluence that is assimilated to the context of nursingcare and made useful to the care of clients.
Method
A purposive sample of 59 mental health nurses tookpart in 10 focus group interviews in 2002 and 2003. Thefocus group interviews were a component researchstudy of the Irish Health Research Board research pro-gram in nursing decision making, carried out with theaim of identifying the nursing contribution to care.Focus groups provided a dynamic means of elicitinggroup representations of concepts of care. Nurses fromeight mental health services took part, reflecting bothurban and rural settings and predominantly situated inDublin and the northeast of Ireland. Focus groupsranged in size between 2 and 12 nurses, comprising clin-icians and a small number of managers.
Nurses in four of the groups worked in hospital-based acute admissions units, three in communityservices, and three were mixed groups. Participantswere invited to take part through contacts in the prac-tice setting, with three inclusion criteria used for par-ticipant selection: registration in the Mental Healthdivision of the nursing register, a minimum of ayear’s experience in clinical practice, and 6 or moremonths’ experience in their particular practice setting.Participating services gave ethical approval to thestudy, and participants gave informed consent with an assurance of anonymity and confidentiality. Theinterviews lasted between 45 and 75 minutes, con-ducted by a moderator and comoderator using a topicguide containing four general questions and follow-up probes: How do nurses conceptualize nursing?What problems do clients present with? How donurses perceive their contribution to care? and Howdo nurses organize their care?
at UNIVERSITY OF WINDSOR on July 8, 2014qhr.sagepub.comDownloaded from
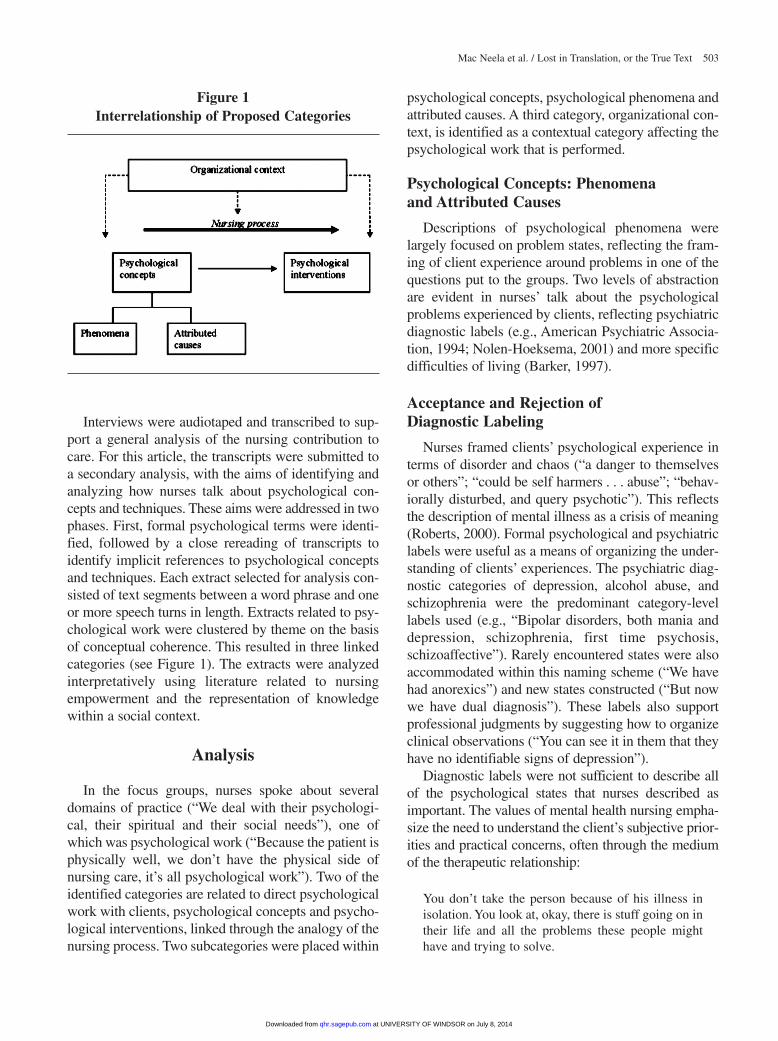
Interviews were audiotaped and transcribed to sup-port a general analysis of the nursing contribution tocare. For this article, the transcripts were submitted toa secondary analysis, with the aims of identifying andanalyzing how nurses talk about psychological con-cepts and techniques. These aims were addressed in twophases. First, formal psychological terms were identi-fied, followed by a close rereading of transcripts toidentify implicit references to psychological conceptsand techniques. Each extract selected for analysis con-sisted of text segments between a word phrase and oneor more speech turns in length. Extracts related to psy-chological work were clustered by theme on the basisof conceptual coherence. This resulted in three linkedcategories (see Figure 1). The extracts were analyzedinterpretatively using literature related to nursingempowerment and the representation of knowledgewithin a social context.
Analysis
In the focus groups, nurses spoke about severaldomains of practice (“We deal with their psychologi-cal, their spiritual and their social needs”), one ofwhich was psychological work (“Because the patient isphysically well, we don’t have the physical side ofnursing care, it’s all psychological work”). Two of theidentified categories are related to direct psychologicalwork with clients, psychological concepts and psycho-logical interventions, linked through the analogy of thenursing process. Two subcategories were placed within
psychological concepts, psychological phenomena andattributed causes. A third category, organizational con-text, is identified as a contextual category affecting thepsychological work that is performed.
Psychological Concepts: Phenomena and Attributed Causes
Descriptions of psychological phenomena werelargely focused on problem states, reflecting the fram-ing of client experience around problems in one of thequestions put to the groups. Two levels of abstractionare evident in nurses’ talk about the psychologicalproblems experienced by clients, reflecting psychiatricdiagnostic labels (e.g., American Psychiatric Associa-tion, 1994; Nolen-Hoeksema, 2001) and more specificdifficulties of living (Barker, 1997).
Acceptance and Rejection of Diagnostic Labeling
Nurses framed clients’ psychological experience interms of disorder and chaos (“a danger to themselvesor others”; “could be self harmers . . . abuse”; “behav-iorally disturbed, and query psychotic”). This reflectsthe description of mental illness as a crisis of meaning(Roberts, 2000). Formal psychological and psychiatriclabels were useful as a means of organizing the under-standing of clients’ experiences. The psychiatric diag-nostic categories of depression, alcohol abuse, andschizophrenia were the predominant category-levellabels used (e.g., “Bipolar disorders, both mania anddepression, schizophrenia, first time psychosis,schizoaffective”). Rarely encountered states were alsoaccommodated within this naming scheme (“We havehad anorexics”) and new states constructed (“But nowwe have dual diagnosis”). These labels also supportprofessional judgments by suggesting how to organizeclinical observations (“You can see it in them that theyhave no identifiable signs of depression”).
Diagnostic labels were not sufficient to describe allof the psychological states that nurses described asimportant. The values of mental health nursing empha-size the need to understand the client’s subjective prior-ities and practical concerns, often through the mediumof the therapeutic relationship:
You don’t take the person because of his illness inisolation. You look at, okay, there is stuff going on intheir life and all the problems these people mighthave and trying to solve.
Mac Neela et al. / Lost in Translation, or the True Text 503
Figure 1Interrelationship of Proposed Categories
at UNIVERSITY OF WINDSOR on July 8, 2014qhr.sagepub.comDownloaded from

504 Qualitative Health Research
They might have a diagnosis of schizophrenia but ashuman beings they might have seen a death or atrauma, even their child is making a confirmation orwhatever.
Reflecting the emphasis that nursing theorists anddiagnosticians place on the patient’s responses to ill-ness (e.g., Barker, 1997; North American NursingDiagnosis Association [NANDA], 2003), talk aboutmajor diagnostic categories extended into constella-tions of specific psychological difficulties and prob-lems of living (“the symptoms of their illness”). Thesewere described in formal and informal discourses thatcomprise a consistent feature of the nurses’ language.Informal descriptions (e.g., “What means as much tous is the fact that they are not dressed right or theyhaven’t got the money for this”) were provided in addi-tion to problems expressed formally:
low self esteem, poor self worth coming from per-haps a depressed person.
suicidal ideation, bereavement, severe anxiety.
a serious addiction problem or a cognitive problem.The person may have been socially phobic for years.
Informal, nontechnical language coexisted with for-mal terminology, often used to describe the patient’scapacity for personal independence (e.g., “when some-one is not well and beginning to become more dis-tressed, not sleeping so good”; “one lady in particularand she just swings”). Informal talk was used todescribe clinical cues in terms of problem states (e.g.,distress and poor sleep) alongside talk about diagnosis.
As well as being endorsed, formal terminology wasrejected (e.g., “You say somebody might have depres-sion or schizophrenia or whatever it is. It doesn’t meanthat much to us”). Some nursing authors regard diag-nosis as a form of colonization that oppresses auton-omy and knowledge (e.g., Powers, 2002), but thenursing diagnosis movement has also been active (e.g.,NANDA, 2003). In keeping with this dualism, focusgroup participants used diagnostic labels but, at thesame time, considered that they fog the clear consider-ation of difficulties (“People present maybe under themask of maybe depression”).
Causes of Psychological Phenomena
Psychological paradigms present plausible (if mutu-ally inconsistent) causes of mental health difficulties.Predominant explanations among focus group partici-pants included motivations (e.g., psychodynamics,
humanistic psychology) and learned responses (behav-ioral psychology). Nurses frequently invoked conceptswith links to psychological theory when making causalattributions about clients. For example, a problem-solving narrative was used to frame engagement withcare recipients as a rational, technical activity (“It is [a]huge problem solving approach with them and maybetheir family as to what the real problem is. . . . So youproblem solve that”). Diagnostic categories were usedto anchor attributions in a consensual representation.For example, the alcoholism script was invoked toexplain problematic drinking (“He is an alcoholic andhe just wants a drink, do you know, he thinks it willcure all ails”).
The influence of psychological concepts can beseen in the causal narratives used in explaining behav-ior. A problem might be amenable to more than onepsychological causal hypothesis (“because maybe theyare so low they cannot express what it is that is actu-ally is causing the problem or are in denial of it”). Twoexplanations are offered here to account for lack ofinsight, based on mood (“because they are so low”)and drawing on psychodynamic defenses (“in denial”).
From a critical perspective, the nurses’ use of psy-chological talk positions them as vehicles for psycho-logical disciplinary knowledge (Foucault, 1977,1980). Nonetheless, psychological concepts supportnursing assessment. In the extract below, a behavioralmodel of self-harm directs assessment toward identi-fying precipitating environmental factors:
If it is somebody that is deliberately self harming,you would want to know everything . . . from everylevel of resource . . . in relation to what is actuallyhappening prior to these acts of self harm or what, ifit is a first time, what instigated it.
The concept of stress was invoked to account forseveral phenomena, consistent with previous researchwith mental health nurses, which has identifiedimplicit use of psychological theories of stress (e.g.,Carradice, Shankland, & Beail, 2002). Stress was seento contribute to mental health problems: “That sense ofphobia is still there and it is a precursor, it’s a stressorin their life that may have led to this depression.”Stressors are located as external to the person or asinternal but beyond control (“It could be marital diffi-culties, financial, family, lack of family support”). Inthe case of self-harm, “stressors [are] involved thatwould make them do this.”
The account given of motivation in one focusgroup recalls Freud’s (1915/1957) hydraulic model of
at UNIVERSITY OF WINDSOR on July 8, 2014qhr.sagepub.comDownloaded from

motivation, in which a buildup of tension impels actionto occur. In this case, the narrative regarding a typicalday in a psychiatric institution used motivation as anorienting theme to justify a directive nursing role:
When you are involved in looking after psychiatricpatients their motivation is a high thing . . . it’s just try-ing to motivate them . . . get them up in the morning,get them to tidying themselves up . . . some of them arequite content to sit all day and do nothing really.
In the face of a power imbalance in the nurse-clientrelationship, the nurse used a consensually understoodpsychological case type (an amotivational state) to justify direct action at odds with the clients’ prefer-ences. At the other end of the motivational spectrum,instinctual pressure (Freud, 1915/1957) underlies anaccount of aggression brewing up and boiling over(“Their form is going off and they are going to getaggressive . . . usually the next thing he strikes out”).
Psychological Therapeutic Interventions
Nurses identified psychological techniques as inte-gral to mental health practice (“You definitely need to listen well to a patient, and another role that youassume in a way is a counselor”). Communicationskills were identified as a nursing strength arising fromtheir distinctive role in delivering care (“We have vastcommunication skills, because we’re the ones dealingwith the patient day in day out”). Communication itselfis described in informal terms (“You’re just listening tothem, having a conversation with them, hearing what’sgoing on with them”). As with talk about phenomenaand causes, psychological techniques were describedin both formal and informal terms.
The psychotherapeutic role is regarded as authenti-cally therapeutic but often occurs in the course of doingsomething else and is not named “therapy” at the time:
There is a lot of stuff that we do that is intrinsicallytherapeutic . . . ordinary things we do that [show] wecare enough about them. . . . We undervalue stuffthat we do all the time.
Formalizing psychological work through the useof a special terminology allows that contribution to benamed. A number of interventions are given formalstatus, with reference to cognitive, behavioral, andcounseling models:
Problem solving therapies, relaxation . . . where youhave a lot of anxiety . . . bereavement counseling,family therapy, or ADHD assessment.
Distancing from these models also occurs, resonat-ing with disempowerment and the devaluing of nurs-ing work by nurses themselves (Varcoe, Rodney, &McCormick, 2003), which is indicative of demoral-ization (Habermas, 1981):
Moderator: You are not involved in anxiety therapyor those type of therapies, specific therapies?N1: Not in depth, no.N2: Like indirectly we do anxiety management every day.
The nurses in this exchange might simply wish to dis-tinguish their role performance from that of counseloror psychotherapist, having assimilated certain psycho-logical terms and given them a nursing meaning.However, framing their contribution as “not in depth”suggests a lack of self-belief or competence (Spreitzer,1995). The nurses were hesitant to claim clinical credi-bility in knowing what anxiety management is and howto do it, a phenomenon that can be understood in termsof the educational and occupational socialization ofnurses (Melia, 1987).
Behaviorism and Counseling Discourses
Behavioral and counseling frameworks provided ameans of conceptualizing nursing intervention strate-gies. Behaviorist thinking was embedded in nurses’talk (“The behavioral disorders that we have to dealwith”) and helped them to organize personal experi-ence (“You are desensitized to a point”). This modelwas also used to justify the approach taken to care. Inthe following extract, two nurses draw on a consensu-ally endorsed representation, with an informal descrip-tion summarized and validated through formalterminology (“reinforcing positively”):
N1: Support is very important. . . . The encourage-ment, and just generally positive things that youwould do to yourself on a regular daily basis, likejust move people along.N2: Reinforcing positively. It is very, very important.
Promotion of personal independence is identifiedas a key aim of mental health nursing. Informal talkabout independence-promoting interventions paral-lels the cognitive goal-setting approach (Beck, Rush,Shaw, & Emery, 1979):
Say something like depression or even in schizophre-nia, where a person would be saying I should be outworking . . . I should be doing this, and we would scaledown their occupational needs, you don’t need to be at
Mac Neela et al. / Lost in Translation, or the True Text 505
at UNIVERSITY OF WINDSOR on July 8, 2014qhr.sagepub.comDownloaded from

506 Qualitative Health Research
work but you need to be occupied, you need to bedoing things around the house, your own personalhygiene, or cutting the grass, but you don’t need to dothings that are taxing.
Apart from a behaviorist, directive approach, nurses’psychological work was framed in terms of humanis-tic counseling:
You would have a range of other supportive nursecounselors as well . . . counseling where the majorthrust would be to treat both individuals and theirfamilies with major mental health problems.
The diversity of the nursing role threatened theintegrity of the counseling relationship, as a nursemight do other work with clients:
In an ideal world I would not want that to be happening—for them to be meeting me in that contextand I would be having some limited contact with themand then have a counseling relationship with them.
Although providing a useful language resource,counseling also posed a definitional problem that thenurses resolved by qualifying the use of counselingterms. Respondents said they used counseling, that ithas a formal place in educational curricula, but sawthe counseling they provided as distinctive:
Another role that you assume in a way is a counselor,like it is not professional counseling, but you are acounselor to an extent.
You would be a kind of—so called counselor.
Language terms chosen from counseling practicewere used (“We are using maybe counseling skills toreflect and empathize with the client”). The use of empa-thy is commonly seen as a form of relating to the patient.The technical representation of empathy, tied to counsel-ing skills, has been seen as a distancing strategy to pro-tect the nurse by professionalizing the response tosuffering (Morse, Bottorff, Anderson, O’Brien, &Solberg, 1992). The labeling function of diagnostic talkis another example of distancing. Nonetheless, as notedabove, labeling was also rejected and the patient under-stood on his or her own terms. The principle of nonjudg-mental support, also associated with counseling, wasclaimed for nursing:
We are also quite non-judgmental in so far as youbecome . . . you wouldn’t be as judgmental as say ayounger person would or a person from a different dis-cipline . . . but probably it might be unique to nursing.
Both critical and functional explanations can beapplied to understanding why talk about counseling isframed through qualifiers such as “in a way,” “to anextent,” and “so called.” It is unclear whether nurseslack confidence to claim the meaning of counseling asunderstood in the professional literature or if counsel-ing has a particular and novel meaning in mental healthnursing. Providing counseling, but “only in a way,”indicates a state of disempowerment, a demoralizationof professional identity (Habermas, 1981). Taking amore positive view, this might reflect the appropriationof linguistic tools as the closest fit for clinical workwith no “official” name, useful for interprofessionalcommunication and amenable for representation(Moscovici, 1984) within a nursing context.
Organizational Context
Nurses’ psychological work is contextualized bythe complex organizational environment of care.Nurses stand in power and status relations to otherprofessional groups (Hogg & Abrams, 1988). This isreflected in two themes attached to this category,referral to psychology services and formalizing psy-chological skills.
Referral to psychology services. Mental healthnurses’ psychological skills might not be sufficient tomeet the client’s needs (“Sometimes they need furtherhelp . . . some kind of therapy, like psychotherapy,behavioral therapy”). Nurses were gatekeepers foraccess to psychological services (“We would put thatin motion”) based on monitoring and clinical judgmentof the client’s state. The process of referral involvestransfer of responsibility to the psychologist (“some-body who can deal with that who specializes in thattype of thing”). Successful handling of the referralprocess (to “get them a date”) involves negotiationskills. The nurse has limited autonomy, as referrals areapproved by the medical consultant (“They are onlybrought in on the consultant’s word, kind of”), and thenurse’s judgment can be overridden:
You may think this patient would benefit frombereavement counseling . . . the consultant mightthink, “Well no I don’t think that they need that,” forwhatever reason . . . if it was a nursing decision wewould refer them straight away.
Hierarchical decision making (Coombs & Ersser,2004) could lead to the nursing voice being dis-counted in decision making about care. This was notin the interests of service users:
at UNIVERSITY OF WINDSOR on July 8, 2014qhr.sagepub.comDownloaded from
I think nurses should be able to say “Okay, I thinkthis person needs anxiety management so I will justgo along and refer them to whoever” . . . instead ofhaving to wait and go through the medical team.
Professional development. Varied views were exp-ressed in relation to professional education and trainingprograms. One view was that formal training was notnecessary to attain expert status, experiential knowl-edge being sufficient (“Some of the staff would havedone challenging behavior courses, others wouldn’t,but they are all experts on challenging behavior”). Theresponsibility that comes with autonomous practicewas off-putting to some nurses; for example,
I did a course there recently in psychosocial inter-ventions . . . some of the people that were there hadtheir own caseload. . . . They were independent prac-titioners . . . but we are not. . . . nor would I person-ally want to work as an independent practitioner. Ifeel we take on what we feel we capably cope with,but that is it.
This extract illustrates that independence as an indi-vidual practitioner was not valued by all, with a prefer-ence for continued independence of the collectivegroup (“we”), through which the delivery of care couldbe shaped. Increased formalization could affect nurses’ability to protect the professional identity and lifeworld(Varcoe et al., 2003). The language of formalized roleswas favored by other nurses (“It would be nice . . . ifyou could have a speciality like, you know, an anxietymanagement nurse”). The formalization of a psycho-logical role here is accommodated within a nursing pro-fessional identity rather than a psychological identity,such as “cognitive therapist.” Nurses working in a com-munity setting tended to talk in a more autonomousmanner and valued individual autonomy.
Discussion
Mental health nurses’ talk about their clinical workreveals a crucial role for disciplinary and implicitpsychological knowledge. Nurses did not see them-selves as psychologists but talked about psychologi-cal concepts and techniques that were used to assessand address clients’ problems. They talked aboutmonitoring psychological status and the use of psy-chological labels and interventions, and they judgedwhen to refer clients to psychology services. Giventhe time they spend with clients, nurses are the primeresource for psychological work in mental health
services. However, many nursing decisions mightmore properly be seen as nursing recommendations,as they need to be endorsed through physician deci-sion making.
Assimilation of psychological knowledge to thevalues framework and everyday discourse of mentalhealth nursing helps to address significant clinicalproblems and describe nursing work. These functionsinclude
• the formal use of psychological techniques and thedescription of nursing work,
• making sense of clients’ experience through diag-nostic terms and symptoms,
• using the interoperability and perceived legitimacyof psychological discourse to lend further technicalcredibility to nursing work, and
• positioning nursing care as psychosocial and distinctfrom medical treatment.
Nonetheless, a complex relationship is illustratedby phenomena such as
• ambiguity toward formalizing psychological work,• use and rejection of diagnostic labels, and• doing psychological work but seeing it as an inade-
quate performance.
Empowerment perspectives are useful in explain-ing the pattern of use of psychological knowledge.For example, the description of having a counselingrole “in a way” indicates a low sense of competenceand psychological empowerment (Spreitzer, 1995).In this sense, psychology is a foreign term, with animperfect fit to describe the nursing work to which itrefers. However, nurses used formal psychologicalterminology extensively to describe and explainpeople’s problems and associated nursing care. Thiskind of talk was complemented by descriptions andexplanations based on informal, everyday language.
A dual discourse about care has been identified pre-viously (e.g., “biculturalism”; Powers, 2002, p. 959).In the present case, psychological experience was pre-sented both through a label-based lingua franca of psy-chiatric care and a complementary everyday nursingdiscourse that fulfills other functions. Informal psycho-logical language is closer to how service users speak,assisting nurses in the role of “ordinary me” (Barker et al., 1999, p. 275), a “tourist guide” and “cultural broker” who helps the person negotiate the system ofcare (Varcoe et al., 2003, p. 967). Nonetheless, the lackof formality in much nursing language raises a questionabout transparency of decision making. Much nursing
Mac Neela et al. / Lost in Translation, or the True Text 507
at UNIVERSITY OF WINDSOR on July 8, 2014qhr.sagepub.comDownloaded from

508 Qualitative Health Research
knowledge is not written down or else requires decod-ing, and this is potentially problematic in terms ofaccountability to service users about the decisionsmade regarding their care.
Considered in terms of empowerment, informal lan-guage use implies disempowerment of nurses fromdecision making in which technical discourse holdssway. The focus group participants spoke about thehierarchical distribution of power favoring psychiatricmedicine. There was wariness of diagnostic terms andof formalizing psychosocial practice, reflecting con-cerns about psychology and psychiatry as a colonizinginfluence (Habermas, 1981). Because it threatensnurses’ professional identity, it is rational that nursesshould resist disempowerment. Informal language is ameans of communicating psychological knowledgethat nurses can control. The appropriation of everydaylanguage for clinical nursing discourse can be consid-ered a form of resistance, leading to a separate form ofclinical knowledge for everyday decision making.
Overall, nurses shifted easily between formal andinformal discourses. Formal psychological terms, withmeaning derived both from nursing and psychology,were successfully integrated with informal psycholog-ical language. The assimilation of formal terminologyacross the group suggests a set of social representa-tions (Moscovici, 1984) of the knowledge required tonurse. Nursing representations comprise an original,applied psychological understanding, based on formaland informal elements. Key concepts in psychology,such as unconditional positive regard, are placedwithin a nursing tradition, a theme reflected in trainingand professional development literature. An informal,nontechnical nursing language resource empowersnurses by establishing a rival source of knowing that isrelatively close to clients’ own discourse.
Whether diagnostic terms are regarded as a tool ofoppression or a lingua franca required in mental healthwork or as genuinely useful, nurses work within a sys-tem that values diagnosis. Disempowerment from for-mal clinical discourse reduces nurses’ potentialcontribution to patient care. Disempowerment is oftendescribed as rooted in structural factors. The chancesof change are adversely affected by ambiguity amongnurses toward roles and training that formalize theirpsychological work. Evidence-based care is central tomental health policy and “of direct concern to mentalhealth nurses” (Paley, Myers, Patrick, Reid, & Shapiro,2003, p. 494). Evaluation studies of psychosocialtraining programs (e.g., Forrest, Masters, & Milne,2004) suggest that coursework affirms rather thanundermines existing clinical skills. Increased access to
formal power can be obtained for carrying out a for-malized version of a role the nurse had been doing any-way (Forrest et al., 2004).
Psychology is potentially both an empowering anda disempowering influence. Each perspective con-tributes to describing how and explaining why psy-chology is used in mental health nursing. The qualifieduse of counseling terms might indicate disempower-ment (not measuring up to the counseling role) or sig-nify that nursing counseling is distinct and original.Ultimately, dual, formal-informal psychological dis-course should be considered in terms of its impact ondecisions about patient care. Empowerment-basedanalyses of nursing have largely emerged from areasother than mental health nursing, highlighting therelevance of an empowerment-based analysis of lan-guage use across different areas of nursing. Psycho-social work is the “official” purpose, to some degree,of mental health nursing but is less so in many othernursing specializations. This suggests that the languageof psychological care would be even more reliant on infor-mal language resources in other branches of nursing.
This unraveling of the nursing-psychology relation-ship was based solely on nursing talk and requiresextension. For example, service user perspectives andobservational work to examine the use of psychologyin the individual and group decision-making process.As a component part of nursing care and a key issue inprofessional debates within mental health nursing, thelargely undocumented psychological work of nursesrequires further articulation and critical scrutiny. Thebenefits of using psychological knowledge in nursingincluded clinical utility, professional identity, and orga-nizational status. From a critical perspective, psycho-logical knowledge is subject to a “struggle overmeaning” (Howarth, 2006, p. 74). Nurses have a partic-ular form of talking about psychological problems andnursing care, but the absence of formal nursing dis-course contributes to nursing invisibility in technicaldiscourse. In practice, however, rather than being “lostin translation,” psychological talk was useful in describ-ing mental health care. Despite the utility of psychol-ogy as a vehicle of expression, nurses’ lack ofconfidence in describing some aspects of their psycho-logical work suggests a negative impact on empower-ment and control.
References
American Psychiatric Association. (1994). Diagnostic and statis-tical manual of mental disorders (4th ed.). Washington, DC:Author.
at UNIVERSITY OF WINDSOR on July 8, 2014qhr.sagepub.comDownloaded from
Barker, P. (1997). Assessment in psychiatric and mental healthnursing: In search of the whole person. Cheltenham, UK:Stanley Thornes.
Barker, P. (2000). Commentaries and reflections on mental healthnursing in the UK at the dawn of a new millennium:Commentary 1. Journal of Mental Health, 9, 617-619.
Barker, P., Jackson, S., & Stevenson, C. (1999). What are psychi-atric nurses for?: Developing a theory of essential nursing practice. Journal of Psychiatric and Mental Health Nursing, 6,273-282.
Beck, A. T., Rush, J., Shaw, B. F., & Emery, G. (1979). Cognitivetheory of depression. New York: Guilford.
Bracey, A. (2002). Finding the patient within: Managing the tran-sitions from student nurse, to patient, to nurse therapist.Group Analysis, 35, 135-151.
Carradice, A., Shankland, M. C., & Beail, N. (2002). A qualitativestudy of the theoretical models used by UK mental health nursesto guide their assessments with family caregivers of people withdementia. International Journal of Nursing Studies, 39, 17-26.
Clark, J., & Lang, N. M. (1992). Nursing’s next advance: Aninternational classification for nursing practice. InternationalNursing Review, 39, 109-112.
Coombs, M., & Ersser, S. J. (2004). Medical hegemony in decision-making: A barrier to interdisciplinary working inintensive care? Journal of Advanced Nursing, 46, 245-252.
Ellefsen, B., & Hamilton, G. (2000). Empowered nurses?: Nursesin Norway and the USA compared. International NursingReview, 47, 106-120.
Farnell, S., & Dawson, D. (2006). “It’s not like the wards”:Experiences of nurses new to critical care—A qualitativestudy. International Journal of Nursing Studies, 43, 319-331.
Foucault, M. (1977). Discipline and punish: The birth of theprison. London: Allen Lane.
Foucault, M. (1980). Power/knowledge, selected interviews andother writings 1972-1977. New York: Pantheon.
Forrest, S., Masters, H., & Milne, V. (2004). Evaluating theimpact of training in psychosocial interventions: A stake-holder approach to evaluation—Part II. Journal of Psychiatricand Mental Health Nursing, 11, 202-212.
Freud, S. (1957). Instincts and their vicissitudes. In J. Strachey(Ed.), The standard edition of the psychological works ofSigmund Freud (Vol. 14). London: Hogarth. (Original workpublished 1915)
Gilbert, T. (1995). Nursing: Empowerment and the problem ofpower. Journal of Advanced Nursing, 21, 865-871.
Gournay, K. (2000). Commentaries and reflections on mentalhealth nursing in the UK at the dawn of a new millennium:Commentary 2. Journal of Mental Health, 9, 621-623.
Habermas, J. (1981). The theory of communicative action. London:Beacon.
Hogg, M. A., & Abrams, D. (1988). Social identifications.Oxford, UK: Routledge.
Howarth, C. (2006). A social representation is not a quiet thing:Exploring the critical potential of social representationstheory. British Journal of Social Psychology, 45, 65-86.
Howell, V., & Norman, I. (2000). Steering a steady course in anera of compulsory treatment: Taking mental health nursinginto the millennium. Journal of Mental Health, 9, 605-616.
Hyde, A., Treacy, M. P., Scott, P. A., Butler, M., Drennan, J., Irving,K., et al. (2005). Modes of rationality in nursing documentation:
Biology, biography and the “voice of nursing.” Nursing Inquiry,12, 66-77.
Kanter, R. M. (1993). Men and women of the corporation. NewYork: Basic Books.
Keen, T. M. (2003). Post-psychiatry: Paradigm shift or wishfulthinking?—A speculative review of future possibles for psy-chiatry. Journal of Psychiatric and Mental Health Nursing,10, 29-37.
Laschinger, H. K., Finegan, J., Shamian, J., & Wilk, O. (2001).Impact of structural and psychological empowerment on jobstrain in nursing work settings: Expanding Kanter’s model.Journal of Nursing Administration, 31, 260-272.
Melia, K. (1987). Learning and working: The occupationalsocialisation of nurses. London: Tavistock.
Morse, J., Bottorff, J., Anderson, G., O’Brien, B., & Solberg, S.(1992). Beyond empathy: Expanding expressions of caring.Journal of Advanced Nursing, 17, 809-821.
Moscovici, S. (1984). The phenomenon of social representations.In R. M. Farr & S. Moscovici (Eds.), Social representations(pp. 3-69). Cambridge, UK: Cambridge University Press.
Nolen-Hoeksema, S. (2001). Abnormal psychology. New York:McGraw-Hill.
North American Nursing Diagnosis Association. (2003). Nursingdiagnoses: Definitions and classification. Philadelphia:NANDA International.
Paley, G., Myers, J., Patrick, S., Reid, E., & Shapiro, D. A.(2003). Practice development in psychological interventions:Mental health nurse involvement in the conversational modelof psychotherapy. Journal of Psychiatric and Mental HealthNursing, 10, 494-498.
Porter, S. (1998). Social theory and nursing practice. Basingstoke,UK: Palgrave Macmillan.
Powers, P. (2002). A discourse analysis of nursing diagnosis.Qualitative Health Research, 12, 945-965.
Roberts, G. (2000). Narratives and severe mental illness: Whatplace do stories have in an evidence-based world? Advancesin Psychiatric Treatment, 6, 432-441.
Spreitzer, G. (1995). Psychological empowerment in the work-place: Dimensions, measurement, and validation. Academy ofManagement Journal, 38, 1442-1462.
Thomas, B., Hardy, S., & Cutting, P. (1997). Principles and prac-tice of mental health nursing. London: C. V. Mosby.
Varcoe, C., Rodney, P., & McCormick, J. (2003). Health carerelationships in context: An analysis of three ethnographies.Qualitative Health Research, 13, 957-973.
Pádraig Mac Neela, PhD, is a lecturer in the Department ofPsychology, National University of Ireland, Galway.
P. Anne Scott, PhD, is Deputy President of Dublin City University,Ireland, and a professor of Nursing at the same institution.
M. Pearl Treacy, PhD, MSc, BA (Hons) Soc, RGN, is a profes-sor of Nursing in the School of Nursing, Midwifery and HealthSystems, University College Dublin, Ireland.
Abbey Hyde, PhD, is a senior lecturer and Head of Teaching andLearning in the School of Nursing, Midwifery and HealthSystems, University College Dublin, Ireland.
Mac Neela et al. / Lost in Translation, or the True Text 509
at UNIVERSITY OF WINDSOR on July 8, 2014qhr.sagepub.comDownloaded from