Embed Size (px)
Citation preview
Journal of Surgical Oncology 2012;105:342–350
Liver-Directed Therapy for Neuroendocrine Neoplasm Hepatic Metastasis
Prolongs Survival Following Progression After Initial Surgery
AKSHAT SAXENA, BMedSc, TERENCE C. CHUA, BscMed (Hons), MBBS, JING ZHAO, MD, AND
DAVID L. MORRIS, MD, PhD*UNSW Department of Surgery, St George Hospital, Kogarah, Sydney, New South Wales, Australia
Background: Surgery confers the best chance of long-term survival in patients with neuroendocrine neoplasm hepatic metastases (NENHM).
Disease progression invariably occurs in the majority of patients. No previous study has addressed the outcomes after treatment of hepatic
disease progression in patients who initially underwent surgical extirpation of NENHM. This was the principal aim of the current study.
Methods: Seventy-four patients with NENHM underwent surgery for NENHM between December 1992 and December 2009. Of these,
50 patients developed disease progression in the liver. These patients were then treated with specific liver-directed therapies according to
consensus of a multidisciplinary team. The current study evaluates progression-free survival (PFS) and overall survival (OS) following
treatment of hepatic disease progression with specific liver-directed therapies.
Results: No patient was lost to follow up. The median follow-up after treatment of progression was 29 months (range ¼ 2–137). The median
PFS and OS after diagnosis of disease progression were 15 and 48 months, respectively. Specific liver-directed therapies included surgery in
10 patients, radioembolization in 15, cytotoxic chemotherapy in 14, and conservative therapy in 11. Four independent factors associated with
PFS and OS were identified through a multivariate analysis. These were initial progression-free survival (PFS, P ¼ 0.006, HR¼ 0.32), extra-
hepatic disease (OS, P ¼ 0.029, HR ¼ 4.04; PFS, P ¼ 0.004, HR ¼ 4.03), histological grade (PFS, P ¼ 0.006, HR ¼ 4.08), and type of
secondary intervention (PFS, P ¼ 0.024, HR ¼ 0.63).
Conclusion: A multimodality approach towards treatment of disease progression as shown in this study that includes repeat surgery or radio-
embolization has been shown to achieve a superior outcome in the setting of disease progression/recurrence.
J. Surg. Oncol. 2012;105:342–350. � 2011 Wiley Periodicals, Inc.
KEY WORDS: neuroendocrine neoplasm; hepatic metastases; hepatectomy; cryoablation; survival analysis; recurrence;carcinoid
INTRODUCTION
Neuroendocrine neoplasms (NEN) represent a heterogenous group
of rare neoplasms characterized by a relatively indolent clinical
course. They mostly originate from the gastrointestinal tract or tra-
cheobronchopulmonary complex and are generally categorized into
two groups, carcinoids and islet tumors. Although rare, a contempo-
rary analysis of the National Cancer Institute, Surveillance Epidemi-
ology and End Results (SEER) database demonstrated that the
age-related incidence of NEN increased 481% within 30 years,
from 1.09/100,000 in 1973 to 5.25/100,000 in 2004 [1]. The most
common site of metastases from NEN is the liver; between 25–93%
of patients develop neuroendocrine neoplasm liver metastases
(NENHM) throughout their disease process [2–4]. These patients
have a significantly worse prognosis and enhanced symptomatology
related to hormone secretion, pressure on structures, and replacement
of the liver.
Although the optimal management for NENHM remains to
be defined, radical surgery provides symptomatic benefit and is
associated with the best survival outcomes. In expert centres, the
median survival of patients with NENLM who undergo surgery is
between 81 and 125 months, with a 5-year survival in excess of 60%
[2,5–8]. Despite encouraging data in recent years on non-surgical
therapies such as somatostatin analogs [9], radioembolization [10–
12], transarterial embolization [13,14], and systemic peptide receptor
radionucleide therapy [15], patients with unresectable disease or
those managed with non-surgical therapies can generally expect a
5-year survival of <30%. In fact, despite the lack of randomized
data, a recent consensus statement from the European Neuroendo-
crine Tumor Society emphasized that resection of hepatic metastases
should be the first-line treatment in patients within resection criteria
[16].
Unfortunately, although surgery is the only definitive therapy, dis-
ease recurrence or progression following an initial curative attempt
is almost invariable. Studies evaluating surgical management of
NENHM report a median and 5-year progression-free survival is
only 15–25 months and 0–7%, respectively [5,8,17]. Despite a pro-
tracted PFS, the long-term survival is a reflection on ongoing treat-
ment of disease progression that has contributed to the overall
survival (OS) outcome. This aspect of the surgical literature is lack-
ing and is the aim of the current study. We evaluate our institution’s
approach of multimodality treatment of disease progression after ini-
tial hepatic resection of NENHM. The current analysis will hopefully
expand the contemporary literature and elucidate the value of various
therapeutic interventions for progressive disease.
PATIENTS AND METHODS
This retrospective study was approved by an institutional review
board and ethics committee. Seventy-four patients with histologically
confirmed neuroendocrine tumor hepatic metastases (NETHM)
*Correspondence to: Prof. David L. Morris, MD, PhD., Department ofSurgery, St George Hospital, University of New South Wales, Level 3Pitney Building, Gray Street, Kogarah, NSW 2217, Sydney, Australia.Fax: (02) 9113 3997. E-mail: [email protected]
Received 7 May 2011; Accepted 15 September 2011
DOI 10.1002/jso.22114
Published online 17 October 2011 in Wiley Online Library(wileyonlinelibrary.com).
� 2011 Wiley Periodicals, Inc.

underwent resection (with or without cryoablation) between
December 1992 and December 2009. Of these, 50 patients developed
disease progression in the liver during routine post-operative follow-
up. The last time of follow-up for these patients was June 2010. Prior
to surgery, patients were evaluated with a baseline medical history,
clinical examination, serum laboratory tests including measurement
of hormone levels, computed tomography (CT) scan (triple phase),
hepatobiliary ultrasound, magnetic resonance imaging, chest radiog-
raphy, and endocrinopathy-directed evaluation. In more recent years,
Indium-111 octroetide (Octreoscan) was used in some patients to
assist in the radiological evaluation of disease. Patients who under-
went open and close procedures were excluded from this study.
Patients with limited extra-hepatic disease discovered incidentally
during laparotomy were not excluded from this study.
A description of our surgical and cryoablative techniques have
been provided elsewhere [18]. In summary, patients were explored
through a bilateral subcostal incision with vertical midline upward
extension. After a thorough intraoperative exploration and liver ultra-
sound, parenchymal dissection was performed using an ultrasonic
dissector (Cavitron ultrasonic surgical aspirator, CUSA1; Valleylab,
Boulder, CO), with Pringle manoeuvre only in selected patients to
minimize blood loss or to maximize efficacy of cryotherapy. Cryo-
therapy was performed using the LCS 3000 liquid nitrogen system
(Spembly or the Erbe system). Liver resection was the preferred
method for the treatment of large tumors because of the relationship
of cryovolume with cryoshock phenomenon, and the remaining
smaller metastases were treated with a limited resection and/or cryo-
therapy. A more detailed description of our cryotherapy techniques
have been provided elsewhere [19]. Fifteen patients underwent open
and close procedures and were excluded from this study.
Procedures were classified as complete (curative intent) or incom-
plete (palliative intent). In palliative procedures, all patients in the
series had at least 90% of their hepatic disease removed (as calculat-
ed on the basis of preoperative imaging and operative findings).
Complete resection was achieved when there was removal of all
gross metastatic disease (including lymphatic spread).
Follow-up
After discharge from hospital, patients were followed prospective-
ly at monthly intervals for the first 3 months and then at 6-monthly
intervals thereafter with measurement of hormone levels and CT of
the liver. The diagnosis of disease progression was defined as the
earliest radiologic evidence of new tumor recurrence after complete
resection or new tumor growth after incomplete resection. In the cur-
rent series, 60 patients developed disease progression of which 50
developed progressive disease in the liver. Depending on decision
from the multidisciplinary tumor board which was based on the
patient’s performance status, hepatic function, extent of hepatic dis-
ease, and concurrent extrahepatic disease, a management strategy
was decided. Repeat hepatectomy and/or ablation (surgical treat-
ment) were considered the treatment of choice for resectable recur-
rent tumors. For more diffuse disease, non-surgical treatments were
used including somatostatin analogs, selective internal radiation
using yttrium-90 microspheres (SIR-Spheres1, Australia), hepatic
artery embolization/chemoembolization (HAE/HACE), systemic
chemotherapy, hepatic artery chemotherapy, and lipiodol I-131. Best
supportive care represented no attempt at active treatment of disease
with a primary focus on symptomatic management and comfort care.
For patients with more diffuse disease, a change in the treatment
paradigm has taken place. Initially, before the adoption of yttrium-90
microspheres (December 2003) in our department, chemotherapeutic
agents such as systemic chemotherapy, hepatic artery chemotherapy,
and transarterial chemoembolization was used in the management
of more diffuse disease. Since the introduction of yttrium-90
microspheres, radioembolization has been used in the majority of
patients with diffuse disease and chemotherapeutic agents have been
restricted to patients who are unsuitable for radioembolization of
those who have been unresponsive to other treatments. Somatostatin
analogs were used in isolation in patients with symptomatic recur-
rence which was adjudged to be the best managed conservatively.
Patients were observed if they had limited, non-symptomatic disease.
Patients were treated in palliative care if their functional and disease
status precluded any active treatment. Following treatment of pro-
gressive disease, patients were followed up as per the same protocol
as described above.
Data Collection and Statistical Analysis
Patient demographic data, disease-related factors, pathological
factors, and treatment-related factors were collected and analyzed.
The primary endpoint was the time interval between treatment of
initial disease progression to the development of second disease pro-
gression (progression-free survival). The secondary endpoint was the
time interval between the treatment of initial disease progression and
cancer-related death [overall survival(OS)]. Data analyses were per-
formed using SPSS1 for Windows version 17.0 (SPSS, Munich,
Germany). The patient’s characteristics were reported using frequen-
cy and descriptive analyses. The Kaplan–Meier method was used to
analyze progression-free survival and OS. Univariate analysis (log-
rank) was performed to examine the relationship of 14 clinicopatho-
logical and treatment-related factors with progression-free survival
and OS. Multivariate analysis was performed on all factors P < 0.10
using the Cox proportional hazards regression model. The median
time to death was defined as the time where 50% of patients have
died. Follow-up was calculated from the date of treatment of carci-
nomatosis to the date of last follow-up. P < 0.05 was considered
statistically significant.
RESULTS
Between December 1992 and December 2009, a total of
74 patients underwent hepatic resection with or without ablation for
neuroendocrine tumor hepatic metastases. The extent of the initial
hepatectomy is summarized in Table I. Of these, 14 (18%) patients
did not develop disease progression during post-operative follow-up;
this includes two patients in whom radiological recurrence was not
assessed because of death in the early post-operative period (within
2 months). Of the 12 remaining patients, five patients remained dis-
ease-free for more than 3 years after initial hepatectomy and three
patients have remained disease-free between 1–3 years after initial
hepatectomy. The remaining four patients have been followed-up for
less than 1 year.
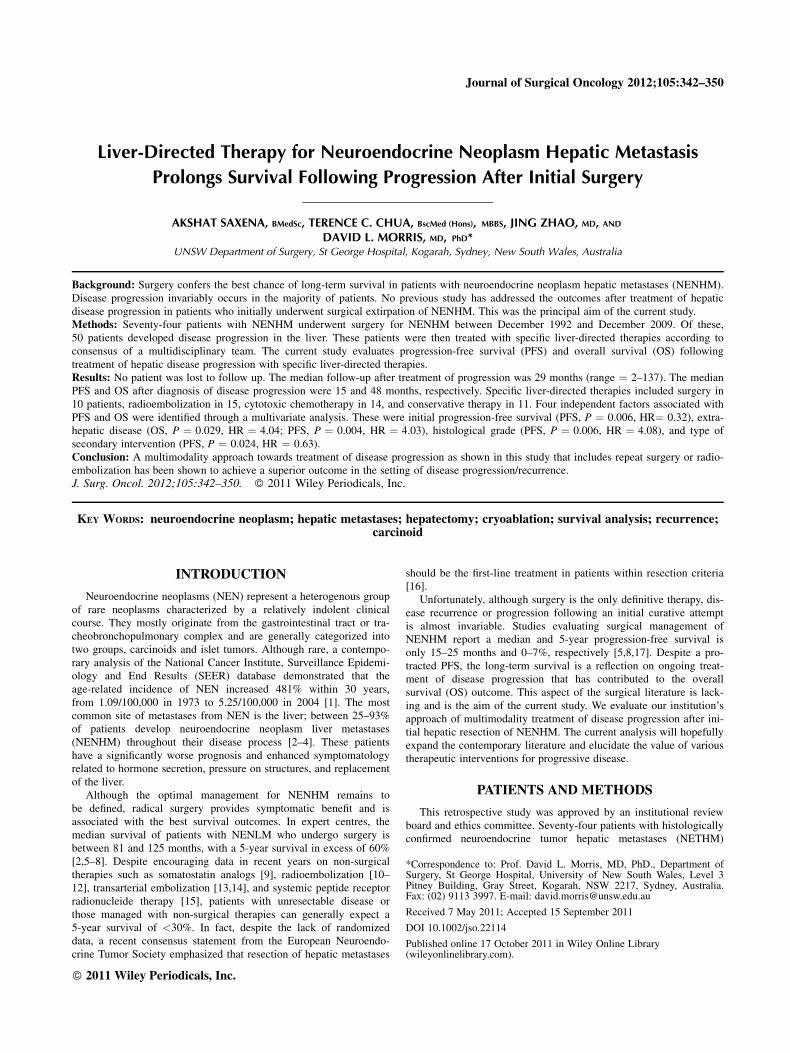
The remaining 60 (82%) patients developed disease progression
at last follow-up after a median interval of 23 months. The most
common site of initial disease progression was the liver in 50 (69%)
patients, bone in five (7%) patients, lung in two (3%) patients, neck
in one (1%) patient, pancreas in one (1%) patient, peritoneum in one
(2%) patient, and heart in one (1%) patient. Four (6%) patients dem-
onstrated disease progression in multiple organ sites simultaneously.
Patients with disease progression in the liver are the principal focus
of the current study. A summary of progression outcomes and subse-
quent treatment outcomes is given in Figure 1.
Of the 50 patients, there were 26 (54%) male patients. Two
patients (4%) had been previously diagnosed with multiple endocrine
neoplasia type 1 (MEN-I) and one patient (2%) had been previously
diagnosed with Zollinger–Ellison syndrome. The mean age of
patients at the time of disease recurrence was 58 years (S.D ¼ 12,
median ¼ 59, range ¼ 28–83). Twenty-four (48%) patients pre-
sented with symptoms relating to hormone excess secondary to NEN
Neuroendocrine Neoplasm Hepatic Metastasis 343
Journal of Surgical Oncology
at the time of progression. The site of the primary tumor was the
small bowel in 20 (40%) patients, the pancreas in 18 (36%), the
large bowel/rectum in 4 (8%) patients, the bronchus in 3 (6%)
patients, and unknown in 5 (10%). The primary tumor was classified
as carcinoid in 37 (74%) patients, non-functional islet cell tumor in
five (10%) patients, small cell neuroendocrine tumor in two (4%)
patients, VIPoma in two (4%) patients, gastrinoma in two (4%)
patients, glucagonoma in one (2%) patient, and large cell neuroendo-
crine tumor in one (2%) patient.
Twenty (40%) patients underwent isolated hepatic resection at the
time of their initial surgery and 30 (60%) underwent concomitant
hepatic resection and ablation. The mean size of the largest resected
hepatic neoplasm was 51 � 44 mm (range, 10–260). The median
number of lesions ablated in patients who underwent synchronous
resection and cryoablation was 2 (range, 1–10 lesions). Pathological
examination of initial resection sample revealed that 35 (70%)
patients had well differentiated tumor, five (10%) had moderately
differentiated tumor and nine (18%) had poorly differentiated tumor.
Vascular invasion, lymphatic invasion, and perineural invasion were
then noted in 20 (40%), 30 (60%), and 12 (24%) patients, respective-
ly. Tumor necrosis status was recorded in 41 patients; of these,
14 (34%) were noted to have tumor necrosis present. At the time of
progression, extra-hepatic disease was detected in 20 (40%) patients.
Ten (20%) patients had unilobar hepatic disease and 40 (80%)
patients had bilobar hepatic disease. Replacement of the liver paren-
chyma by tumor was 0–25% in 29 (58%) patients, 26–50% in 19
(38%) patients, and 51–75% in 2 (4%) patients.
Treatment of Hepatic Disease Progression
Fifty patients developed progression of liver disease after initial
surgical extirpation. The mean size of hepatic recurrence in these
patients based on imaging was 3.6 cm (S.D ¼ 3.0). These patients
were managed according to consensus of a multidisciplinary team as
earlier described. Ten (20%) patients were treated with surgery
(Group A). The extent of surgery in these 10 patients is summarized
in Table II. Three patients who underwent surgery were also treated
with concomitant cryoablation. The median number of lesions
treated in patients who underwent surgery was 5 (range, 1–13). Ad-
juvant octreotide analogs were used in three patients who underwent
repeat hepatectomy. Postoperative complications developed in three
patients for an overall morbidity rate of 30%. These were bile leak-
age (n ¼ 1,10%), subphrenic abscess (n ¼ 1,10%), and liver dys-
function (n ¼ 1,10%). Fifteen (30%) patients were treated with
yttrium-90 radioembolization (Group B). Postoperative complica-
tions included fatigue in six patients (40%), non-specific self-limiting
abdominal pain in four (27%), nausea in three (20%), anorexia in
two (13%), vomiting in one (9%), and shortness of breath in
one (9%). The mean hospital stay in patients who underwent
resection and radioembilozation was 14 days (S.D ¼ 12) and 1 day
(S.D ¼ 0.5), respectively.
Fourteen (28%) patients were treated with chemotherapeutic
agents (Group C). Of these, 10 (20%) patients were treated with
systemic chemotherapy, three (6%) with hepatic artery chemotherapy
and one (2%) with transarterial chemoembolization. Eleven (22%)
patients were managed with more conservative measures (Group D).
Of these, seven (14%) patients were managed with medical therapy
using somatostatin analogs, two (4%) were closely observed and two
(%) were managed with best supportive care. A comparison between
TABLE I. Operative Procedures Performed in 74 Patients who Under-
went Hepatic Resection for Neuroendocrine Neoplasm Liver Metastases
Type of procedure performed
Patients
(n ¼ 74)
Right hemihepatectomy 8
Left hemihepatectomy 5
Extended left hemihepatectomy 2
Extended right hemihepatectomy 4
Central resection 6
Bisegementectomy
Segments 2 and 3 12
Segments 3 and 4 1
Segments 5 and 6 3
Segments 7 and 8 2
Segments 6 and 7 2
Segments 2 and 4 1
Segmentectomy
Segment 3 1
Segment 4 2
Segment 7 2
Segment 8 2
Subsegmentectomy
Segment 5 1
Segment 4 1
Multiple hepatic resections
Complex bilobar liver resection 1
2� segmental resection
Segments 4 and 6 2
Segments 5 and 7 1
Segments 3 and 7 1
Segments 3 and 6 1
3� segmental resection
Segments 1, 3, and 5 1
Segments 2, 6, and 7 1
Right hemihepatectomy þ subsegmental (segment 3) 1
Right hemihepatectomy þ subsegmental (segment 2) 1
Wedge (segments 2 and 3) and segmental (segment 6) 2
Left hemihepatectomy and segmental (segment 6) 1
Left hemihepatectomy and subsegmental (7) 1
Bisegmentectomy (segments 2 and 3) and segmental (segment 7) 1
Bisegmentectomy (segments 2 and 3) and subsegmental (segment 4) 1
Bisegmentectomy (segments 5 and 6) and segmental (segment 3) 2
Bisegmentectomy (segments 5 and 6) and segmental (segment 2) 1
Fig. 1. A summary of progression outcomes and subsequent treat-ment outcomes.
344 Saxena et al.
Journal of Surgical Oncology
the baseline characteristics of the four major treatment groups is pro-
vided in Table III. The treatment groups differ in terms of extra-he-
patic disease status (P ¼ 0.005) and the extent of hepatic disease
(P ¼ 0.022).
Overall Survival
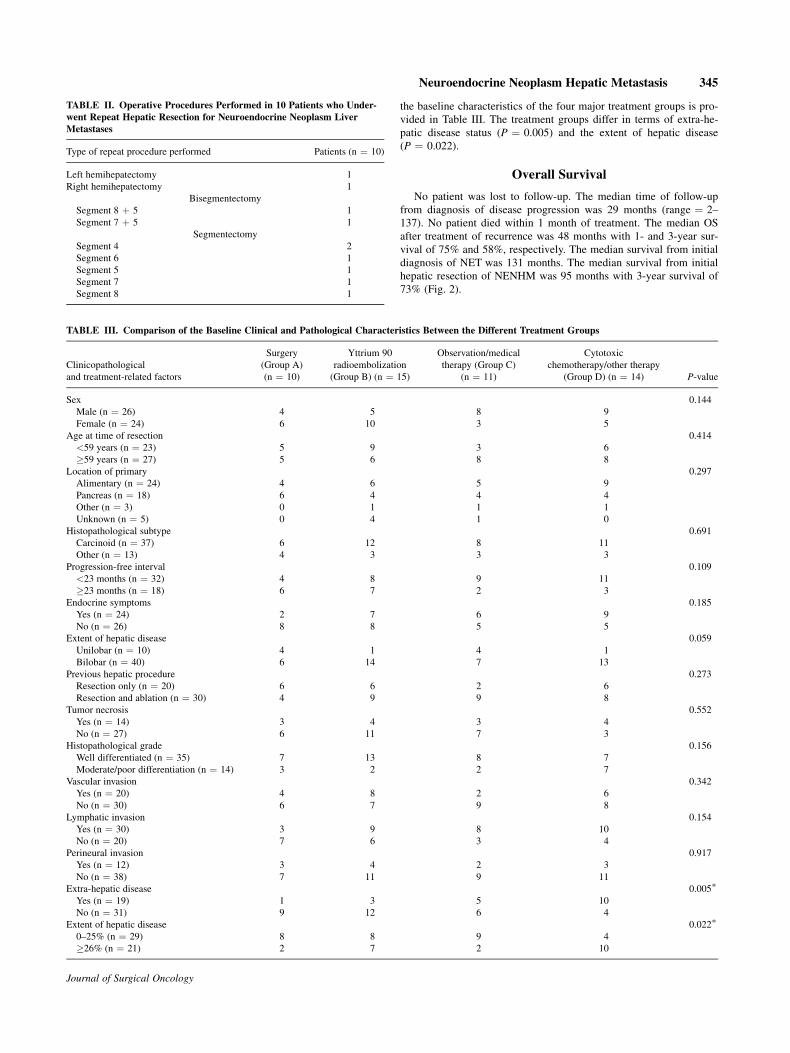
No patient was lost to follow-up. The median time of follow-up
from diagnosis of disease progression was 29 months (range ¼ 2–
137). No patient died within 1 month of treatment. The median OS
after treatment of recurrence was 48 months with 1- and 3-year sur-
vival of 75% and 58%, respectively. The median survival from initial
diagnosis of NET was 131 months. The median survival from initial
hepatic resection of NENHM was 95 months with 3-year survival of
73% (Fig. 2).
TABLE II. Operative Procedures Performed in 10 Patients who Under-
went Repeat Hepatic Resection for Neuroendocrine Neoplasm Liver
Metastases
Type of repeat procedure performed Patients (n ¼ 10)
Left hemihepatectomy 1
Right hemihepatectomy 1
Bisegmentectomy
Segment 8 þ 5 1
Segment 7 þ 5 1
Segmentectomy
Segment 4 2
Segment 6 1
Segment 5 1
Segment 7 1
Segment 8 1
TABLE III. Comparison of the Baseline Clinical and Pathological Characteristics Between the Different Treatment Groups
Clinicopathological
and treatment-related factors
Surgery
(Group A)
(n ¼ 10)
Yttrium 90
radioembolization
(Group B) (n ¼ 15)
Observation/medical
therapy (Group C)
(n ¼ 11)
Cytotoxic
chemotherapy/other therapy
(Group D) (n ¼ 14) P-value
Sex 0.144
Male (n ¼ 26) 4 5 8 9
Female (n ¼ 24) 6 10 3 5
Age at time of resection 0.414
<59 years (n ¼ 23) 5 9 3 6
�59 years (n ¼ 27) 5 6 8 8
Location of primary 0.297
Alimentary (n ¼ 24) 4 6 5 9
Pancreas (n ¼ 18) 6 4 4 4
Other (n ¼ 3) 0 1 1 1
Unknown (n ¼ 5) 0 4 1 0
Histopathological subtype 0.691
Carcinoid (n ¼ 37) 6 12 8 11
Other (n ¼ 13) 4 3 3 3
Progression-free interval 0.109
<23 months (n ¼ 32) 4 8 9 11
�23 months (n ¼ 18) 6 7 2 3
Endocrine symptoms 0.185
Yes (n ¼ 24) 2 7 6 9
No (n ¼ 26) 8 8 5 5
Extent of hepatic disease 0.059
Unilobar (n ¼ 10) 4 1 4 1
Bilobar (n ¼ 40) 6 14 7 13
Previous hepatic procedure 0.273
Resection only (n ¼ 20) 6 6 2 6
Resection and ablation (n ¼ 30) 4 9 9 8
Tumor necrosis 0.552
Yes (n ¼ 14) 3 4 3 4
No (n ¼ 27) 6 11 7 3
Histopathological grade 0.156
Well differentiated (n ¼ 35) 7 13 8 7
Moderate/poor differentiation (n ¼ 14) 3 2 2 7
Vascular invasion 0.342
Yes (n ¼ 20) 4 8 2 6
No (n ¼ 30) 6 7 9 8
Lymphatic invasion 0.154
Yes (n ¼ 30) 3 9 8 10
No (n ¼ 20) 7 6 3 4
Perineural invasion 0.917
Yes (n ¼ 12) 3 4 2 3
No (n ¼ 38) 7 11 9 11
Extra-hepatic disease 0.005�Yes (n ¼ 19) 1 3 5 10
No (n ¼ 31) 9 12 6 4
Extent of hepatic disease 0.022�0–25% (n ¼ 29) 8 8 9 4
�26% (n ¼ 21) 2 7 2 10
Neuroendocrine Neoplasm Hepatic Metastasis 345
Journal of Surgical Oncology
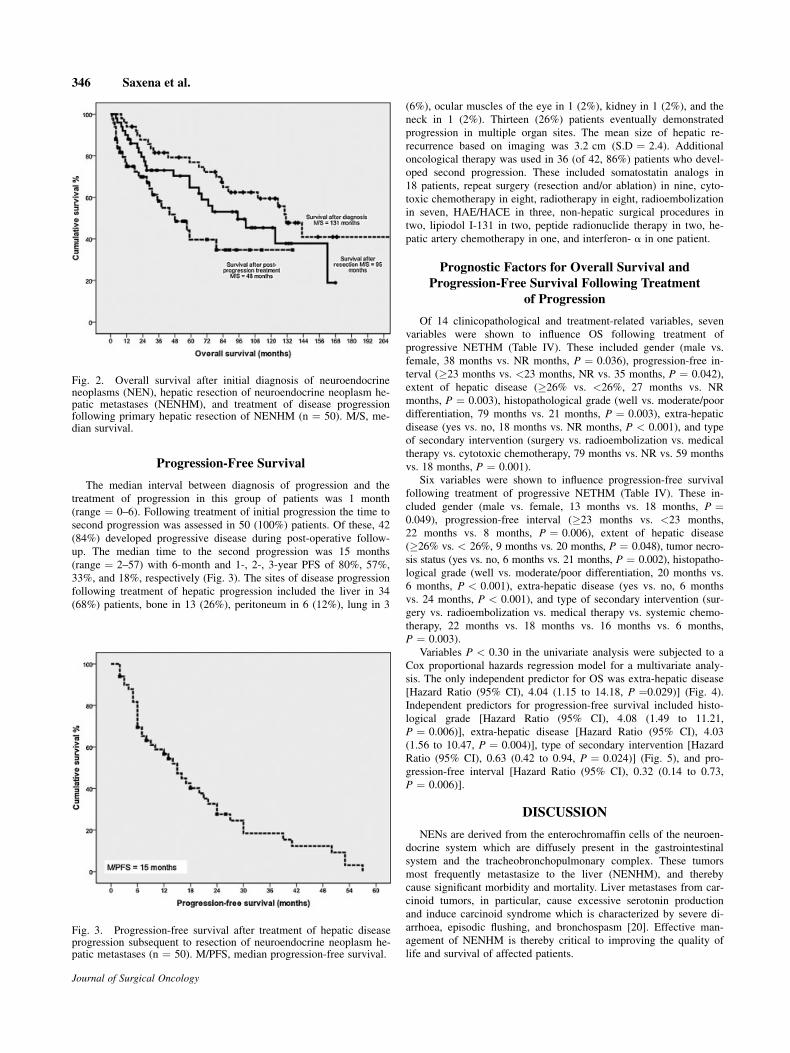
Progression-Free Survival
The median interval between diagnosis of progression and the
treatment of progression in this group of patients was 1 month
(range ¼ 0–6). Following treatment of initial progression the time to
second progression was assessed in 50 (100%) patients. Of these, 42
(84%) developed progressive disease during post-operative follow-
up. The median time to the second progression was 15 months
(range ¼ 2–57) with 6-month and 1-, 2-, 3-year PFS of 80%, 57%,
33%, and 18%, respectively (Fig. 3). The sites of disease progression
following treatment of hepatic progression included the liver in 34
(68%) patients, bone in 13 (26%), peritoneum in 6 (12%), lung in 3
(6%), ocular muscles of the eye in 1 (2%), kidney in 1 (2%), and the
neck in 1 (2%). Thirteen (26%) patients eventually demonstrated
progression in multiple organ sites. The mean size of hepatic re-
recurrence based on imaging was 3.2 cm (S.D ¼ 2.4). Additional
oncological therapy was used in 36 (of 42, 86%) patients who devel-
oped second progression. These included somatostatin analogs in
18 patients, repeat surgery (resection and/or ablation) in nine, cyto-
toxic chemotherapy in eight, radiotherapy in eight, radioembolization
in seven, HAE/HACE in three, non-hepatic surgical procedures in
two, lipiodol I-131 in two, peptide radionuclide therapy in two, he-
patic artery chemotherapy in one, and interferon- a in one patient.
Prognostic Factors for Overall Survival and
Progression-Free Survival Following Treatment
of Progression
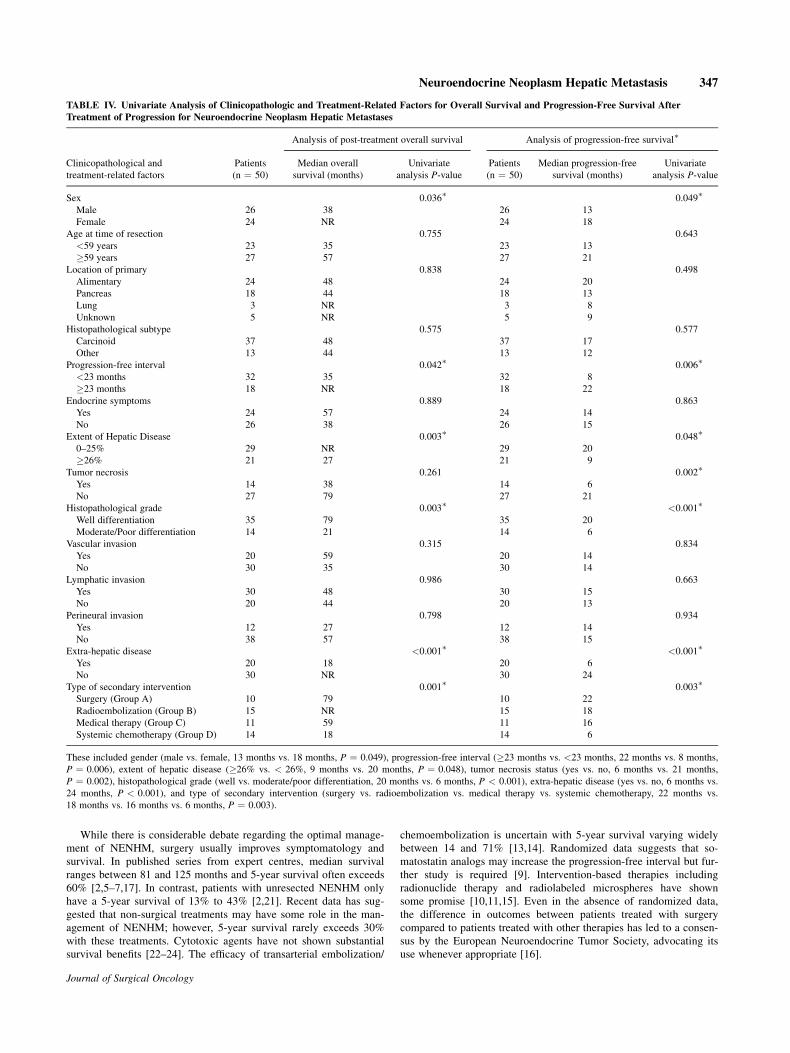
Of 14 clinicopathological and treatment-related variables, seven
variables were shown to influence OS following treatment of
progressive NETHM (Table IV). These included gender (male vs.
female, 38 months vs. NR months, P ¼ 0.036), progression-free in-
terval (�23 months vs. <23 months, NR vs. 35 months, P ¼ 0.042),
extent of hepatic disease (�26% vs. <26%, 27 months vs. NR
months, P ¼ 0.003), histopathological grade (well vs. moderate/poor
differentiation, 79 months vs. 21 months, P ¼ 0.003), extra-hepatic
disease (yes vs. no, 18 months vs. NR months, P < 0.001), and type
of secondary intervention (surgery vs. radioembolization vs. medical
therapy vs. cytotoxic chemotherapy, 79 months vs. NR vs. 59 months
vs. 18 months, P ¼ 0.001).
Six variables were shown to influence progression-free survival
following treatment of progressive NETHM (Table IV). These in-
cluded gender (male vs. female, 13 months vs. 18 months, P ¼0.049), progression-free interval (�23 months vs. <23 months,
22 months vs. 8 months, P ¼ 0.006), extent of hepatic disease
(�26% vs. < 26%, 9 months vs. 20 months, P ¼ 0.048), tumor necro-
sis status (yes vs. no, 6 months vs. 21 months, P ¼ 0.002), histopatho-
logical grade (well vs. moderate/poor differentiation, 20 months vs.
6 months, P < 0.001), extra-hepatic disease (yes vs. no, 6 months
vs. 24 months, P < 0.001), and type of secondary intervention (sur-
gery vs. radioembolization vs. medical therapy vs. systemic chemo-
therapy, 22 months vs. 18 months vs. 16 months vs. 6 months,
P ¼ 0.003).
Variables P < 0.30 in the univariate analysis were subjected to a
Cox proportional hazards regression model for a multivariate analy-
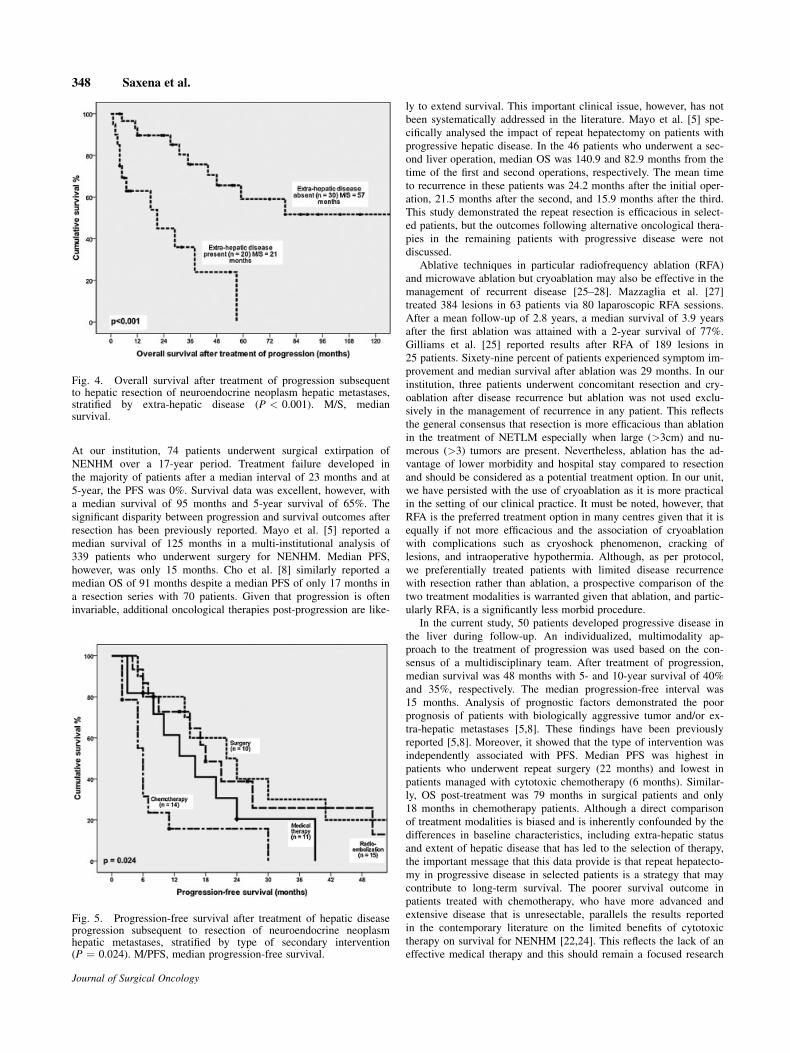
sis. The only independent predictor for OS was extra-hepatic disease
[Hazard Ratio (95% CI), 4.04 (1.15 to 14.18, P ¼0.029)] (Fig. 4).
Independent predictors for progression-free survival included histo-
logical grade [Hazard Ratio (95% CI), 4.08 (1.49 to 11.21,
P ¼ 0.006)], extra-hepatic disease [Hazard Ratio (95% CI), 4.03
(1.56 to 10.47, P ¼ 0.004)], type of secondary intervention [Hazard
Ratio (95% CI), 0.63 (0.42 to 0.94, P ¼ 0.024)] (Fig. 5), and pro-
gression-free interval [Hazard Ratio (95% CI), 0.32 (0.14 to 0.73,
P ¼ 0.006)].
DISCUSSION
NENs are derived from the enterochromaffin cells of the neuroen-
docrine system which are diffusely present in the gastrointestinal
system and the tracheobronchopulmonary complex. These tumors
most frequently metastasize to the liver (NENHM), and thereby
cause significant morbidity and mortality. Liver metastases from car-
cinoid tumors, in particular, cause excessive serotonin production
and induce carcinoid syndrome which is characterized by severe di-
arrhoea, episodic flushing, and bronchospasm [20]. Effective man-
agement of NENHM is thereby critical to improving the quality of
life and survival of affected patients.
Fig. 2. Overall survival after initial diagnosis of neuroendocrineneoplasms (NEN), hepatic resection of neuroendocrine neoplasm he-patic metastases (NENHM), and treatment of disease progressionfollowing primary hepatic resection of NENHM (n ¼ 50). M/S, me-dian survival.
Fig. 3. Progression-free survival after treatment of hepatic diseaseprogression subsequent to resection of neuroendocrine neoplasm he-patic metastases (n ¼ 50). M/PFS, median progression-free survival.
346 Saxena et al.
Journal of Surgical Oncology
While there is considerable debate regarding the optimal manage-
ment of NENHM, surgery usually improves symptomatology and
survival. In published series from expert centres, median survival
ranges between 81 and 125 months and 5-year survival often exceeds
60% [2,5–7,17]. In contrast, patients with unresected NENHM only
have a 5-year survival of 13% to 43% [2,21]. Recent data has sug-
gested that non-surgical treatments may have some role in the man-
agement of NENHM; however, 5-year survival rarely exceeds 30%
with these treatments. Cytotoxic agents have not shown substantial
survival benefits [22–24]. The efficacy of transarterial embolization/
chemoembolization is uncertain with 5-year survival varying widely
between 14 and 71% [13,14]. Randomized data suggests that so-
matostatin analogs may increase the progression-free interval but fur-
ther study is required [9]. Intervention-based therapies including
radionuclide therapy and radiolabeled microspheres have shown
some promise [10,11,15]. Even in the absence of randomized data,
the difference in outcomes between patients treated with surgery
compared to patients treated with other therapies has led to a consen-
sus by the European Neuroendocrine Tumor Society, advocating its
use whenever appropriate [16].
TABLE IV. Univariate Analysis of Clinicopathologic and Treatment-Related Factors for Overall Survival and Progression-Free Survival After
Treatment of Progression for Neuroendocrine Neoplasm Hepatic Metastases
Clinicopathological and
treatment-related factors
Patients
(n ¼ 50)
Analysis of post-treatment overall survival Analysis of progression-free survival�
Median overall
survival (months)
Univariate
analysis P-value
Patients
(n ¼ 50)
Median progression-free
survival (months)
Univariate
analysis P-value
Sex 0.036� 0.049�Male 26 38 26 13
Female 24 NR 24 18
Age at time of resection 0.755 0.643
<59 years 23 35 23 13
�59 years 27 57 27 21
Location of primary 0.838 0.498
Alimentary 24 48 24 20
Pancreas 18 44 18 13
Lung 3 NR 3 8
Unknown 5 NR 5 9
Histopathological subtype 0.575 0.577
Carcinoid 37 48 37 17
Other 13 44 13 12
Progression-free interval 0.042� 0.006�<23 months 32 35 32 8
�23 months 18 NR 18 22
Endocrine symptoms 0.889 0.863
Yes 24 57 24 14
No 26 38 26 15
Extent of Hepatic Disease 0.003� 0.048�0–25% 29 NR 29 20
�26% 21 27 21 9
Tumor necrosis 0.261 0.002�Yes 14 38 14 6
No 27 79 27 21
Histopathological grade 0.003� <0.001�Well differentiation 35 79 35 20
Moderate/Poor differentiation 14 21 14 6
Vascular invasion 0.315 0.834
Yes 20 59 20 14
No 30 35 30 14
Lymphatic invasion 0.986 0.663
Yes 30 48 30 15
No 20 44 20 13
Perineural invasion 0.798 0.934
Yes 12 27 12 14
No 38 57 38 15
Extra-hepatic disease <0.001� <0.001�Yes 20 18 20 6
No 30 NR 30 24
Type of secondary intervention 0.001� 0.003�Surgery (Group A) 10 79 10 22
Radioembolization (Group B) 15 NR 15 18
Medical therapy (Group C) 11 59 11 16
Systemic chemotherapy (Group D) 14 18 14 6
These included gender (male vs. female, 13 months vs. 18 months, P ¼ 0.049), progression-free interval (�23 months vs. <23 months, 22 months vs. 8 months,
P ¼ 0.006), extent of hepatic disease (�26% vs. < 26%, 9 months vs. 20 months, P ¼ 0.048), tumor necrosis status (yes vs. no, 6 months vs. 21 months,
P ¼ 0.002), histopathological grade (well vs. moderate/poor differentiation, 20 months vs. 6 months, P < 0.001), extra-hepatic disease (yes vs. no, 6 months vs.
24 months, P < 0.001), and type of secondary intervention (surgery vs. radioembolization vs. medical therapy vs. systemic chemotherapy, 22 months vs.
18 months vs. 16 months vs. 6 months, P ¼ 0.003).
Neuroendocrine Neoplasm Hepatic Metastasis 347
Journal of Surgical Oncology
At our institution, 74 patients underwent surgical extirpation of
NENHM over a 17-year period. Treatment failure developed in
the majority of patients after a median interval of 23 months and at
5-year, the PFS was 0%. Survival data was excellent, however, with
a median survival of 95 months and 5-year survival of 65%. The
significant disparity between progression and survival outcomes after
resection has been previously reported. Mayo et al. [5] reported a
median survival of 125 months in a multi-institutional analysis of
339 patients who underwent surgery for NENHM. Median PFS,
however, was only 15 months. Cho et al. [8] similarly reported a
median OS of 91 months despite a median PFS of only 17 months in
a resection series with 70 patients. Given that progression is often
invariable, additional oncological therapies post-progression are like-
ly to extend survival. This important clinical issue, however, has not
been systematically addressed in the literature. Mayo et al. [5] spe-
cifically analysed the impact of repeat hepatectomy on patients with
progressive hepatic disease. In the 46 patients who underwent a sec-
ond liver operation, median OS was 140.9 and 82.9 months from the
time of the first and second operations, respectively. The mean time
to recurrence in these patients was 24.2 months after the initial oper-
ation, 21.5 months after the second, and 15.9 months after the third.
This study demonstrated the repeat resection is efficacious in select-
ed patients, but the outcomes following alternative oncological thera-
pies in the remaining patients with progressive disease were not
discussed.
Ablative techniques in particular radiofrequency ablation (RFA)
and microwave ablation but cryoablation may also be effective in the
management of recurrent disease [25–28]. Mazzaglia et al. [27]
treated 384 lesions in 63 patients via 80 laparoscopic RFA sessions.
After a mean follow-up of 2.8 years, a median survival of 3.9 years
after the first ablation was attained with a 2-year survival of 77%.
Gilliams et al. [25] reported results after RFA of 189 lesions in
25 patients. Sixety-nine percent of patients experienced symptom im-
provement and median survival after ablation was 29 months. In our
institution, three patients underwent concomitant resection and cry-
oablation after disease recurrence but ablation was not used exclu-
sively in the management of recurrence in any patient. This reflects
the general consensus that resection is more efficacious than ablation
in the treatment of NETLM especially when large (>3cm) and nu-
merous (>3) tumors are present. Nevertheless, ablation has the ad-
vantage of lower morbidity and hospital stay compared to resection
and should be considered as a potential treatment option. In our unit,
we have persisted with the use of cryoablation as it is more practical
in the setting of our clinical practice. It must be noted, however, that
RFA is the preferred treatment option in many centres given that it is
equally if not more efficacious and the association of cryoablation
with complications such as cryoshock phenomenon, cracking of
lesions, and intraoperative hypothermia. Although, as per protocol,
we preferentially treated patients with limited disease recurrence
with resection rather than ablation, a prospective comparison of the
two treatment modalities is warranted given that ablation, and partic-
ularly RFA, is a significantly less morbid procedure.
In the current study, 50 patients developed progressive disease in
the liver during follow-up. An individualized, multimodality ap-
proach to the treatment of progression was used based on the con-
sensus of a multidisciplinary team. After treatment of progression,
median survival was 48 months with 5- and 10-year survival of 40%
and 35%, respectively. The median progression-free interval was
15 months. Analysis of prognostic factors demonstrated the poor
prognosis of patients with biologically aggressive tumor and/or ex-
tra-hepatic metastases [5,8]. These findings have been previously
reported [5,8]. Moreover, it showed that the type of intervention was
independently associated with PFS. Median PFS was highest in
patients who underwent repeat surgery (22 months) and lowest in
patients managed with cytotoxic chemotherapy (6 months). Similar-
ly, OS post-treatment was 79 months in surgical patients and only
18 months in chemotherapy patients. Although a direct comparison
of treatment modalities is biased and is inherently confounded by the
differences in baseline characteristics, including extra-hepatic status
and extent of hepatic disease that has led to the selection of therapy,
the important message that this data provide is that repeat hepatecto-
my in progressive disease in selected patients is a strategy that may
contribute to long-term survival. The poorer survival outcome in
patients treated with chemotherapy, who have more advanced and
extensive disease that is unresectable, parallels the results reported
in the contemporary literature on the limited benefits of cytotoxic
therapy on survival for NENHM [22,24]. This reflects the lack of an
effective medical therapy and this should remain a focused research
Fig. 4. Overall survival after treatment of progression subsequentto hepatic resection of neuroendocrine neoplasm hepatic metastases,stratified by extra-hepatic disease (P < 0.001). M/S, mediansurvival.
Fig. 5. Progression-free survival after treatment of hepatic diseaseprogression subsequent to resection of neuroendocrine neoplasmhepatic metastases, stratified by type of secondary intervention(P ¼ 0.024). M/PFS, median progression-free survival.
348 Saxena et al.
Journal of Surgical Oncology

initiative in NEN. Although our study demonstrated a significant dif-
ference in outcomes based on treatment modality, these data must be
interpreted with caution. It must be noted that the relatively small
sample size (n ¼ 50) of the current study may have precluded a fair
and robust comparison of the treatment modalities. Small numbers
can produce statistically fragile results in which a small difference in
patients can produce a large effect on the results. A large, prospec-
tive study would be clearly beneficial but is hampered by the rarity
of NENHM.
Recent developments in intervention-based therapies have greatly
expanded the therapeutic options available to treat unresectable
NENHM. Radioembolization using yttrium-90 microspheres is a po-
tential treatment option. It exploits the arterial system that intrahe-
patic malignancies derive their blood supply from compared to
normal liver parenchyma that is supplied mainly by the portal
vein. Microspheres when injected selectively into the hepatic artery
lodge in the tumor microvasculature. Yttrium-90 is a pure b emitter
that consequently delivers a high radiation dose to the tumors
with sparing of the normal liver parenchyma. Published series
have demonstrated that Y90 radioembolization is safe, can produce a
radiological response in up to 63% of patients, and can achieve me-
dian survival of 28–70 months [10–12]. In our series, 15 patients
with unresectable disease after surgery were treated with this
therapy, attaining a median PFS of 16 months. More importantly, the
5-year survival of these patients is 73%. Comparing this modality of
Y90 treatment of hepatic progression with repeat hepatectomy that
achieves a 5-year survival of 68%, the comparable long-term out-
come has suggested that radioembolization and surgery achieves
similar outcome as a secondary treatment for hepatic progression
after initial curative surgery. Although this data appears promising,
the relatively small number of patients (15 in the repeat surgery
group and 10 in the radioembolization group) is a limitation and
further evidence is required before any clear conclusions may be
derived.
The role of conservative strategies in the management of
NENHM requires further study. In the current series 11 patients were
managed with conservative therapy including seven with somatostat-
in analogs. The median PFS and OS were 16 months and 79 months,
respectively. Somatostatin analogs confer anti-symptom effects by
blocking somatostatin receptors, and may exert anti-tumor effects by
inhibiting growth factors, modulating the immune system, and inhib-
iting angiogenesis. The recent PROMID study demonstrated that so-
matostatin analogs compared to placebo, delayed progression from
6 months to 14.6 months[9]. The patients in this treatment group
often had advanced bilobar liver disease (82%) and extra-hepatic dis-
ease (36%). Hence, despite being unresectable and nor suitable for
radioembolization, the use of somatostatin analogs alone may have
delayed further progression. However, there are also patients with
rapidly progressing disease on conservative therapy. Favorable tumor
biology seems imperative for long-term survival with this therapy.
Identification of the patient subgroup that will most likely benefit
from careful observation or medical therapy can avoid unnecessary
treatments and cost.
Although it has not been extensively used at our institution, pep-
tide receptor radionuclide therapy has been of recent clinical interest.
This delivers targeted radiation to tumor by utilizing the ability of
somatostatin analogs to bind somatostatin receptors which are over-
expressed by the tumor. In the largest series of 1,772 treatments of177Lu-octreotate administered in 504 patients with metastases in the
liver and bone, 46% had an objective tumor response. Median time
to progression and OS were 40 and 46 months, respectively [15].
Given that our study demonstrates that the relative incidence of bone
metastases from NEN increases with time, this treatment modality is
likely to become increasingly important and may further improve
post-progression outcomes.
In conclusion, the disparity between PFS and OS after resection
of NENHM underscores the need for an effective strategy to treat
disease progression to achieve the longest survival possible. These
data show that individualised treatment of hepatic progression after
resection of NENHM is associated with excellent overall outcomes.
Although repeat surgery and Y90 radioembolization were shown in
the current series to be efficacious in achieving long-term survival,
further investigation of this important clinical issue is clearly
necessary.
REFERENCES
1. Yao JC, Hassan M, Phan A, et al.: One hundred years after‘‘carcinoid’’: Epidemiology of and prognostic factors for neuro-endocrine tumors in 35,825 cases in the United States. J ClinOncol 2008;26:3063–3072.
2. Chamberlain RS, Canes D, Brown KT, et al.: Hepatic neuroen-docrine metastases: Does intervention alter outcomes? J AmColl Surg 2000;190:432–445.
3. Modlin IM, Lye KD, Kidd M: A 5-decade analysis of 13,715carcinoid tumors. Cancer 2003;97:934–959.
4. Quaedvlieg PF, Visser O, Lamers CB, et al.: Epidemiology andsurvival in patients with carcinoid disease in The Netherlands.An epidemiological study with 2391 patients. Ann Oncol 2001;12:1295–1300.
5. Mayo SC, de Jong MC, Pulitano C, et al.: Surgical managementof hepatic neuroendocrine tumor metastasis: Results from aninternational multi-institutional analysis. Ann Surg Oncol 2010;17:3129–3136.
6. Frilling A, Li J, Malamutmann E, et al.: Treatment of liver me-tastases from neuroendocrine tumours in relation to the extentof hepatic disease. Br J Surg 2009;96:175–184.
7. Schurr PG, Strate T, Rese K, et al.: Aggressive surgery im-proves long-term survival in neuroendocrine pancreatic tumors:An institutional experience. Ann Surg 2007;245:273–281.
8. Cho CS, Labow DM, Tang L, et al.: Histologic grade is corre-lated with outcome after resection of hepatic neuroendocrineneoplasms. Cancer 2008;113:126–134.
9. Rinke A, Muller HH, Schade-Brittinger C, et al.: Placebo-controlled, double-blind, prospective, randomized study on theeffect of octreotide LAR in the control of tumor growth inpatients with metastatic neuroendocrine midgut tumors: A re-port from the PROMID Study Group. J Clin Oncol 2009;27:4656–4663.
10. Saxena A, Chua TC, Bester L, et al.: Factors predictingresponse and survival after yttrium-90 radioembolization ofunresectable neuroendocrine tumor liver metastases: A criticalappraisal of 48 cases. Ann Surg 2010;251:910–916.
11. Kennedy AS, Dezarn WA, McNeillie P, et al.: Radioemboliza-tion for unresectable neuroendocrine hepatic metastases usingresin 90Y-microspheres: Early results in 148 patients. Am JClin Oncol 2008;31:271–279.
12. Rhee TK, Lewandowski RJ, Liu DM, et al.: 90Y Radioemboli-zation for metastatic neuroendocrine liver tumors: Preliminaryresults from a multi-institutional experience. Ann Surg 2008;247:1029–1035.
13. Gupta S, Johnson MM, Murthy R, et al.: Hepatic arterial embo-lization and chemoembolization for the treatment of patientswith metastatic neuroendocrine tumors: Variables affectingresponse rates and survival. Cancer 2005;104:1590–1602.
14. Eriksson BK, Larsson EG, Skogseid BM, et al.: Liver emboliza-tions of patients with malignant neuroendocrine gastrointestinaltumors. Cancer 1998;83:2293–2301.
15. Kwekkeboom DJ, de Herder WW, Kam BL, et al.: Treatmentwith the radiolabeled somatostatin analog [177Lu-DOTA0,-Tyr3]octreotate: Toxicity, efficacy, and survival. J Clin Oncol2008;26:2124–2130.
16. Plockinger U, Rindi G, Arnold R, et al.: Guidelines for thediagnosis and treatment of neuroendocrine gastrointestinaltumours. A consensus statement on behalf of the European
Neuroendocrine Neoplasm Hepatic Metastasis 349
Journal of Surgical Oncology

Neuroendocrine Tumour Society (ENETS). Neuroendocrinology2004;80: 394–424.
17. Sarmiento JM, Heywood G, Rubin J, et al.: Surgical treatmentof neuroendocrine metastases to the liver: A plea for resectionto increase survival. J Am Coll Surg 2003;197:29–37.
18. Chua TC, Saxena A, Chu F, et al.: Clinicopathological determi-nants of survival after hepatic resection of hepatocellularcarcinoma in 97 patients-experience from an Australian hepato-biliary unit. J Gastrointest Surg 2010;14:1370–1380.
19. Yan TD, Padang R, Morris DL: Longterm results and prognosticindicators after cryotherapy and hepatic arterial chemotherapywith or without resection for colorectal liver metastases in 224patients: Longterm survival can be achieved in patients withmultiple bilateral liver metastases. J Am Coll Surg 2006;202:100–111.
20. Moertel CG: Karnofsky memorial lecture. An odyssey in theland of small tumors. J Clin Oncol 1987;5:1502–1522.
21. Janson ET, Holmberg L, Stridsberg M, et al.: Carcinoid tumors:Analysis of prognostic factors and survival in 301 patients froma referral center. Ann Oncol 1997;8:685–690.
22. Arnold R, Rinke A, Schmidt C, et al.: Endocrine tumours ofthe gastrointestinal tract: Chemotherapy. Best Pract Res ClinGastroenterol 2005;19:649–656.
23. Sutcliffe R, Maguire D, Ramage J, et al.: Management ofneuroendocrine liver metastases. Am J Surg 2004;187:39–46.
24. O’Toole D, Hentic O, Corcos O, et al.: Chemotherapy forgastro-enteropancreatic endocrine tumours. Neuroendocrinology2004;80:79–84.
25. Gillams A, Cassoni A, Conway G, et al.: Radiofrequency abla-tion of neuroendocrine liver metastases: The Middlesex experi-ence. Abdom Imaging 2005;30:435–441.
26. Reddy SK, Clary BM: Neuroendocrine liver metastases. SurgClin North Am 2010;90:853–861.
27. Mazzaglia PJ, Berber E, Milas M, et al.: Laparoscopic radiofre-quency ablation of neuroendocrine liver metastases: A 10-yearexperience evaluating predictors of survival. Surgery 2007;142:10–19.
28. Elvin A, Skogseid B, Hellman P: Radiofrequency ablation ofneuroendocrine liver metastases. Abdom Imaging 2005;30:427–434.
350 Saxena et al.
Journal of Surgical Oncology
![Neuroendocrine Neoplasms of the Pancreas: The Pathological …€¦ · neoplasm of the pancreas, accounting for approximately 1–2% of all pancreatic neoplasms [1, 2]. The incidence](https://img.dokumen.tips/doc/110x75/5f6d4c375d58c6724b1aebea/neuroendocrine-neoplasms-of-the-pancreas-the-pathological-neoplasm-of-the-pancreas.jpg)

![Mucinous Neoplasm: A Case Report A Rare Case of Low-grade ... · cell adenocarcinoma, or neuroendocrine carcinoma [3]. Mucinous adenocarcinoma accounts for Mucinous adenocarcinoma](https://img.dokumen.tips/doc/110x75/5d66f73588c993283a8b59a1/mucinous-neoplasm-a-case-report-a-rare-case-of-low-grade-cell-adenocarcinoma.jpg)