Upload
ralu-dia
View
223
Download
0
Embed Size (px)
Citation preview
8/2/2019 Life Style Cockerman
1/17
Health Lifestyle Theory and theConvergence of Agency and Structure*
WILLIAM C. COCKERHAM
University of Alabama at Birmingham
Journal of Health and Social Behavior 2005, Vol 46 (March): 5167
This article util izes the agency-struc ture debate as a framework for
constructing a health lifestyle theory. No such theory currently exists, yet the
need for one is underscored by the fact that many daily lifestyle practices involveconsiderations of health outcomes. An individualist paradigm has influenced
concepts of health lifestyles in several disciplines, but this approach neglectsthe structural dimensions of such lifestyles and has limited applicability to the
empirical world. The direction of this article is to present a theory of healthlifestyles that includes considerations of both agency and structure, with an
emphasis upon restoring structure to its appropriate position. The articlebegins by defining agency and structure, followed by presentation of a health
lifestyle model and the theoretical and empirical studies that support it.
51
An important but undeveloped area of theo-retical discourse in medical sociology pertainsto the relative contributions of agency and struc-ture in determining health lifestyles. Medicalsociologists have paid little attention to theagency-structure problem, yet it is clearly centralto theoretical discussions of health and lifestyles(Pescosolido, McLeod, and Alegra 2000;Williams 1995). No contemporary theoretical
perspective denies that either agency or struc-ture is unimportant; rather, the debate centerson the extent to which one or the other isdominant. Proponents of structure emphasizethe power of structural conditions in contouringindividual dispositions and behavior alongsocially prescribed lines, while advocates of
agency accentuate the capacity of individualactors to choose their behavior regardless ofstructural influences. When applied to healthlifestyles, the question is whether the deci-sions people make with respect to diet, exercise,smoking, and the like are largely a matter ofindividual choice or are principally shaped bystructural variables such as social class position
and gender?
THE NEED FOR AHEALTH LIFESTYLE THEORY
It is the purpose of this article to examine theagency-structure debate as a framework forconstructing a health lifestyle theory. No suchtheory currently exists. The need for a healthlifestyle theory is underscored by the fact thatmany daily lifestyle practices involve consid-erations of health outcomes. Perhaps this is truertoday than in the past. Whereas people may havemore or less taken their health for granted in
previous historical eras, this is presently not thecase. Health in late modernity has becomeviewed as an achievementsomething peopleare supposed to work at to enhance their quality
of life or risk chronic illness and premature deathif they do not (Clarke et al. 2003). According toGiddens (1991) and Turner (1992), lifestyle
#2102Jnl of Health and Social BehaviorVol. 46 146105-cockerham
* An earlier version of this article was presented atthe 2003 American Sociological Association meetingin Atlanta, Georgia, and the 2004 joint meeting of theEuropean Society of Health and Medical Sociologyand the Italian Society of Health Sociology, Bologna,Italy. The author would especially like to thankMichael Hughes for his considerable insightsconcerning this article, along with Mark Tausig andthree anonymous reviewers for their comments on anearlier version. Address correspondence to WilliamC. Cockerham, Department of Sociology, Univer-sity of Alabama at Birmingham, 237 Ullman Building,1530 Third Avenue South, Birmingham, AL 35294-3350 (email: [email protected]).
Delivered by Ingenta toUNIVERSITY OF NEVADA, RENO (cid 1060), Univ. of Nevada-Reno (cid 291575), University
of Nevada, Reno (cid 57010993)IP : 127.0.0.1
Tue, 13 Sep 2005 20:50:48
8/2/2019 Life Style Cockerman
2/17
options have become integrated with bodily regi-mens in late modernity and people have becomemore responsible for both the health and designof their own bodies.
This situation originates from changes in
(1) disease patterns, (2) modernity, and (3) socialidentities. The first change is the twentiethcentury epidemiological transition from acuteto chronic diseases as the major source of humanmortality in most areas of the world. Medicinecannot cure these chronic diseases and negativehealth lifestyles promote them. The realizationthat this is a certainty carries with it the reve-lation that the responsibility for ones health ulti-
mately falls on oneself through healthy living(Crawford 1984). Greater personal responsibilitymeans that achieving a healthy lifestyle has
become more of a life or (time of) death option.The second change is the current era of late
modern social alterations creating a newmodernity (Bauman 1992, 2000; Beck 1992;Giddens 1991). While notions of an absolute
break with the past modernity originating withthe industrial age are unconvincing, it is never-
theless clear that society is in a transition to anew social form (Pescosolido and Rubin 2000).This is seen in the new world order evolving outof the collapse of Soviet-style socialism, theexpanding multiculturalization of Europe and
North America, the rise of cultural and sexualpolitics, the multiplicity of family forms,changing patterns of social stratification, andthe increasing use of knowledge as a commodity.
In health matters, we see the decline in the statusand professional authority of physicians throughlessened control over the medical marketplace.We also see greater movement toward the mutual
participation model of the physician-patient rela-tionship that has accelerated with the adventof Internet medicine and the diffusion of medicalknowledge in the public domain (Hardey1999; Warren, Weitz, and Kulis 1998). In thestill-emerging late modern society, where tradi-
tional industrial age centers of power andauthority, such as medicine, are weakening,adopting a healthy lifestyle accords people morecontrol over their life situation.
The third change is that there has also beenmovement in late modernity toward an adjust-ment in the primary locus of social identity.Previously, work or occupation largely deter-mined social class position and a persons way
of life. Beginning in the second half of the twen-tieth century, lifestyle consumer habits have beenincreasingly experienced by individuals in
advanced societies as a primary source of theirsocial identification (Bauman 1992; Crompton1998; Giddens 1991). This situation was made
possible by the rise in economic productivitypromoting a general improvement in living stan-
dards and purchasing power after World War II.The easier acquisition of basic material needsallowed styles of consumption to supercedeoccupation for signifying social similarities anddistinctions for many people (Crompton 1998).Scott (1996), for example, finds that thelifestyles of British manual workers have beenaltered, with major implications for class iden-tification. He observes that social distinctions
in the working class are determined more byconsumption patterns than relationships to themeans of production.
Therefore, as Crompton (1998) points out,the claim that lifestyles have become moresignificant in class formation and social iden-tification needs to be taken seriously. This obser-vation is consistent with Giddenss (1991) asser-tion that lifestyles not only fulfill utilitarianneeds, but also give material form to a partic-
ular narrative of self-identity. An importantlifestyle configuration and the accompanyingsocial marker are those practices affecting healthand the distinctions they also contribute to differ-ences in social identities (Annandale 1998). Atheory of health lifestyles is needed to advanceour understanding of this social phenomenon.
THE INDIVIDUALIST PARADIGM:A CRITIQUE
Much of what we know about lifestyles hasits theoretical origins in the early twentiethcentury work of Max Weber ([1922] 1978).However, Frohlich, Corin, and Potvin (2001:782)observe that the term lifestyle, widely adopted
by researchers in health promotion, socialepidemiology, and other branches of public
health, has taken on a very particular anddifferent meaning from that intended by Weber.Although Webers methodologies often reflectedan individualist and agency-oriented bottom-up approach to the study of social structure, hedid not view patterns of social action as theuncoordinated practices of disconnected indi-viduals (Kalberg 1994; Sibeon 2004). Instead,he saw social action in terms of regularities and
uniformities repeated by numerous actors overtime. His focus was on the way in which peopleact in concert, not individually. The bridge from
52 JOURNAL OF HEALTH AND SOCIAL BEHAVIOR
#2102Jnl of Health and Social BehaviorVol. 46 146105-cockerham
Delivered by Ingenta toUNIVERSITY OF NEVADA, RENO (cid 1060), Univ. of Nevada-Reno (cid 291575), University
of Nevada, Reno (cid 57010993)IP : 127.0.0.1
Tue, 13 Sep 2005 20:50:48
8/2/2019 Life Style Cockerman
3/17
agency to structure for Weber was the idealtype, consisting of structural entities (e.g.,
bureaucracy) or processes (e.g., formal ratio-nality), whose construction allowed him to makegeneral statements about collective forms of
social behavior (Kalberg 1994). For example,in The Protestant Ethic and the Spirit of Capi-talism, Weber (1958) emphasized macrostruc-ture in an essentially top-down fashionshowing how social institutions (Calvinist reli-gion) and widespread belief systems (capitalism)were powerful forces in shaping the thoughtsand behavior of individuals (Sibeon 2004).
Yet, as Frohlich et al. (2001:783) point out:
When lifestyle is currently discussed withinthe socio-medical discourse, there is a decidedtendency for it to be used in reference to indi-vidual behavioural patterns that affect diseasestatus, thereby neglecting its collective (struc-tural) characteristics. This approach is anexample of Archers (1995:4) notion of upwardsconflation, a term she applies to behavioralmodels in which individuals monopolize causal
power that operates in a one-way, upward direc-
tion and seems incapable of acting back to influ-ence individuals. This is seen in the standardapproach to research in public health andepidemiology that treats health behavior andlifestyles as matters of individual choice andtargets the individual to change his or herharmful health practices largely through educa-tion (Lomas 1998; Sweat and Denison 1995).The theoretical models employed in such
research, like the Health Belief Model, the AIDSRisk Reduction Model, the Common SenseModel of Illness Danger, and the Stages ofChange Model, are based on individual
psychology.In their bookEducation, Social Status, and
Health, Mirowsky and Ross (2003) indicate thatneither individual choice nor structural limita-tions can be ignored in studies of health behaviorand lifestyles. They use the term structural
amplification to refer to situations where well-educated individuals accumulate advantages and
poorly educated persons amass disadvantagesthat are bundled over time into cascadingsequences impacting either positively or nega-tively on health. However, Mirowsky and Rossconcentrate more on agency than structure inthis book. Their goal is to show that educationincreases effective agency that, in turn, increases
the control that an individual has over his or herlife, thereby encouraging and enabling a healthylifestyle. Mirowsky and Ross (2003:28) state
that no health scientist has yet invented the drugor written the law that will make individualsdo what those individuals must choose to dothemselves.
Consequently, health lifestyles are largely
depicted as sets of individually constructedbehaviors, with education serving as the criticalfeature of agency. The elements of a healthylifestyle are described as having nothing incommon with each other except that theyimprove health. In seeking health, stateMirowsky and Ross (2003:199), individualsweave these disparate habits and practices intoa coherent lifestyle designed to preserve and
promote health. While individuals tend to dowhat others like them do, it is individuals whotake otherwise incoherent or diametric prac-tices allocated by subcultural forces andcoalesce them into a healthy lifestyle (Mirowskyand Ross 2003:53).
While Mirowsky and Ross make an impor-tant contribution by highlighting the powerfulrole of education in the selection of healthlifestyles, income and occupational status join
education as the major components of socialclass or socioeconomic status (SES). As Adleret al. (1994) point out, the three variables areinterrelated but not identical nor fully overlap-
ping. The fact that associations between SESand health are found with each of the indica-tors, state Adler et al. (1994:15), suggests thata broader underlying dimension of social strat-ification or social ordering is the potent factor.
Thus, education can also be viewed in combi-nation with the other components of class toconstitute a structural variable that produces top-down distinctions in the quality and form ofhealth lifestyles among individuals, as well as
providing a social context for the practice ofsuch lifestyles. Other structural variables suchas age and gender also produce distinct patternsin health lifestyles (Cockerham 2000a).
Sociological concepts reflecting literally all
theories of social life attest to the fact thatsome-thing(namely structure) exists beyond the indi-vidual to give rise to customary patterns of
behavior. These concepts range from Durkheims([1895] 1950:13) notion of social facts as everyway of acting, fixed or not, capable of exercisingon the individual an external constraint toMeads (1934:155) view of the generalizedother as the organized attitudes of the whole
community and the social process through whichthe community exercises control over theconduct of its individual members.
HEALTH LIFESTYLE THEORY 53
#2102Jnl of Health and Social BehaviorVol. 46 146105-cockerham
Delivered by Ingenta toUNIVERSITY OF NEVADA, RENO (cid 1060), Univ. of Nevada-Reno (cid 291575), University
of Nevada, Reno (cid 57010993)IP : 127.0.0.1
Tue, 13 Sep 2005 20:50:48
8/2/2019 Life Style Cockerman
4/17
Structural influences on health lifestyle prac-tices are seen, for example, in the studies ofDemers and her colleagues (Demers, Bisson,and Palluy 1999; Demers et al. 2002) on alcoholconsumption by married women and univer-
sity students in Canada. This research showsthat class position, the social relationships ofthe people drinking, and the social context ofthe drinking situation have substantial effectson alcohol intake and drinking behavior. It isapparent from our findings, state Demers et al.(2002:422), that the individual cannot beconceptualized as an autonomous actor makingself-governing decisions in a social vacuum.
Another example of structural influences onhealth lifestyles is the antismoking campaign inthe United States. For over 20 years, massiveefforts were made to reduce cigarette smokingthrough educational programs on the hazards ofsmoking. These individual approaches to thecessation of smoking encouraged many to stop,conclude Sweat and Denison (1995:S252),however, not until smoking was banned in many
public places did the prevalence of smoking
significantly decline. This ban had the effectof labeling smokers as social outcasts anddeviants. Antismoking laws, social isolation, andstigma significantly increased smoking cessa-tion far beyond the results of purely individu-alistic approaches (Sweat and Denison1995:S252).
Whereas these studies show structural influ-ences have a significant effect on health lifestyle
practices, there are situations in which structurecan be so overwhelming that agency is renderedineffective. Gareth Williams (2003) reports onthe high mortality of a group of Welsh coalminers in the 1930s. These were men unsungin any chronicle of existence (cited in Williams2003:145). Their lives were severely curtailed
by their punishing work and diet of beggars.However, the unremitting toll of childbirth anddomestic labor impaired the health and short-
ened the lives of the women as much or moreas that of the men. The weight of structuralconditions was so heavy that individual capa-
bilities and capacities were ineffective. This situ-ation, comments Williams (2003:146), providesa salutary reminder of the way in which the
balance between agency, context, and structureis itself highly determined by structural forces.
In more recent research investigating contem-
porary social conditions in a working-classneighborhood in a city in northwest England,Williams observes that the influence of struc-
ture on agency in relation to health lifestyles isstill heavy-handed. He f inds that assuming
people have the freedom to make healthy choicesis out of line with what many people experienceas real possibilities in their everyday lives. The
respondents, concludes Williams (2003:147),understood the behavioural risk factors thatmade ill-health more likely and for which theywere in a limited sense, responsible, but theywere also aware that the risks they faced were
part of social conditions that they could do littleto change.
Consequently, the direction of this article willbe to bring considerations of both agency and
structure into a theory of health lifestyles, witha view to restoring structure to its appropriateposition. While agency is important, it will beargued that structural conditions can act backon individuals and configure their lifestyle
patterns in particular ways. Agency allows themto reject or modify these patterns, but struc-ture limits the options that are available. Thisarticle begins with definitions of agency andstructure, followed by presentation of a health
lifestyle paradigm and the research literaturethat supports it.
AGENCY AND STRUCTURE
The agency-structure issue has been thecentral sociological question since the begin-ning of the discipline. As Archer (1995:1)
explains: The vexatious task of under-standing the linkage between structure andagencywill always retain this centrality becauseit derives from what society intrinsically is. Itis crucial to any scenario ofagency that the actorcould have acted otherwise in particular situa-tions, and that social action takes place withina continuous stream of time subject to the contin-uing possibility of reflexive awareness on the
part of the actor (Bhaskar 1998). Emirbayer and
Mische (1998) suggest, accordingly, that humanagency consists of three different elements: iter-ation (the selective reactivation of past patternsof thought and action),projectivity (the imagi-native generation of possible future trajecto-ries of action in which structures of thought andaction may be creatively reconfigured), and
practical evaluation (the capacity to make prac-tical and normative judgments among alterna-
tive possibilities).Emirbayer and Mische (1998:970) thereforedefine agency as the temporally constructed
54 JOURNAL OF HEALTH AND SOCIAL BEHAVIOR
#2102Jnl of Health and Social BehaviorVol. 46 146105-cockerham
Delivered by Ingenta toUNIVERSITY OF NEVADA, RENO (cid 1060), Univ. of Nevada-Reno (cid 291575), University
of Nevada, Reno (cid 57010993)IP : 127.0.0.1
Tue, 13 Sep 2005 20:50:48
8/2/2019 Life Style Cockerman
5/17
engagement of actors of different structural envi-ronmentsthe temporal-relational contexts ofactionwhich, through the interplay of habit,imagination, and judgment, both reproduces andtransforms those structures in interactive
response to the problems posed by changinghistorical situations. Agency can thus be consid-ered a process in which individuals, influ-enced by their past but also oriented towardthe future (as a capacity to imagine alternative
possibilities) and the present (as a capacity toconsider both past habits and future situationswithin the contingencies of the moment), criti-cally evaluate and choose thei r course of
action (Emirbayer and Mische 1998:963).Sewell (1992:19) provides a definition ofstructures as sets of mutually sustainingschemas and resources that empower orconstrain social action and tend to be reproduced
by that social action. Schemas are transposablerules or procedures applied to the enactmentof social life. Resources are of two types, eitherhuman (e.g., physical strength, dexterity, knowl-edge) or nonhuman (naturally occurring or
manufactured) that can be used to enhance ormaintain power. Sewell equates resources withthe power to influence action consistent withGiddenss (1984) notion of the duality ofstructure as both constraining and enabling. Thisduality, while correct, nonetheless contains acontradiction. The enabling function suggestsresources increase the range and style of optionsfrom which the actor can choose, but constraint
means that resources invariably limit choices towhat is possible. As Bauman (1999) observes,individual choices in allcircumstances areconfined by two sets of constraints: (1) choosingfrom among what is available and (2) social rulesor codes telling the individual the rank orderand appropriateness of preferences.
Although agency theorists maintain thatagency will never be completely determined bystructure, it is also clear that there is no hypo-
thetical moment in which agency actually getsfreeof structure; it is not, in other words, some
pure Kantian transcendental free will (Emir-bayer and Mische 1998:1004). While agencyrefers to the capacity to choose behavior,structure pertains to regularities in social inter-action (e.g., institutions, roles), systematic socialrelationships (e.g., group affiliations, classand other forms of social stratification), and
resources that script behavior to go in particulardirections as opposed to others that might betaken.
A HEALTH LIFESTYLES PARADIGM
Health lifestyles are defined here as collec-tive patterns of health-related behavior based onchoices from options available to people
according to their life chances (Cockerham2000a). This definition incorporates the dialec-tical relationship between life choices and lifechances proposed by Weber in his lifestyleconcept ([1922:53139] 1978:92639). In aWeberian context, life choices are a proxy foragency and life chances are a form of structure.Whereas health and other lifestyle choices arevoluntary, life chanceswhich primarily repre-sent class positioneither empower or constrainchoices as choices and chances work off eachother to determine behavioral outcomes.
Weber associated lifestyles not with indi-viduals but with status groups, thereby showingthey are principally a collective social phenom-enon. Status groups are aggregates of peoplewith similar status and class backgrounds, andthey originate through a sharing of similarlifestyles. People who wish to be part of a partic-
ular status group are required to adopt the appro-priate lifestyle. Status groups are stratifiedaccording to their patterns of consumption.These patterns not only establish differences
between groups, but they also express differ-ences that are already in place (Bourdieu 1984).Health lifestyles are a form of consumption inthat the health that is produced is used for some-thing, such as a longer life, work, or enhanced
enjoyment of ones physical being (Cock-erham 2000a; dHoutaud and Field 1984). More-over, health lifestyles are supported by an exten-sive health products industry of goods andservices (e.g., running shoes, sports clothing,diet plans, health foods, club and spa member-ships) promoting consumption as an inherentcomponent of participation.
Additionally, as Gochman (1997) pointsout, positive health lifestyle behaviors are the
opposite of risk behaviors. Good nutrition, forexample, is the reverse of bad nutrition. The
binary nature of health lifestyle practices meansthat the outcome generated from the interplayof choices and chances have either positive ornegative effects on health. Gochman alsoobserves that health lifestyles are intended toavoid risk in general and are oriented towardoverall health and fitness. However, while the
term health lifestyle is meant to encompass ageneral way of healthy living, there has beendebate over whether or not there is an overall
HEALTH LIFESTYLE THEORY 55
#2102Jnl of Health and Social BehaviorVol. 46 146105-cockerham
Delivered by Ingenta toUNIVERSITY OF NEVADA, RENO (cid 1060), Univ. of Nevada-Reno (cid 291575), University
of Nevada, Reno (cid 57010993)IP : 127.0.0.1
Tue, 13 Sep 2005 20:50:48
8/2/2019 Life Style Cockerman
6/17
health lifestyle. The best evidence suggeststhat for many people their health lifestyle can
be characterized as either generally positive ornegative. Vickers, Conway, and Hervig (1990)found, for example, in a study of U.S. Navy
personnel that positive health behaviors clus-tered along two dimensions, one promoting well-ness and the other avoiding risk. More recentresearch from Finland provides strong evidencethat associations between health practices arerelated, with people who behave unhealthily inone respect doing so in others and vice versa(Laaksonen, Prttl, and Lahelma 2002).Smoking had the strongest and most consis-
tent associations with other unhealthy lifestylepractices, and multiple unhealthy practices weremost common among lower socioeconomicgroups. A significant body of research attachesthe most positive health lifestyle practices tohigher social strata and women and the mostnegative to lower strata and men (Abel et al.1999; Blaxter 1990; Cockerham 1997, 1999,2000a; Grzywacz and Marks 2001; Link andPhelan 2000).
It therefore appears that health lifestyles arenot the uncoordinated behaviors of disconnectedindividuals, but are personal routines that mergeinto an aggregate form representative of specificgroups and classes. While definitions and ageneral concept of health lifestyles exist in theliterature, an overall theoretical paradigmasnotedis missing. In order to fill this gap andfurther the development of health lifestyle
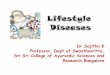
theory, a preliminary paradigm is presented inFigure 1. The arrows between boxes indicatehypothesized causal relationships.
Beginning with box 1, in the top right-handbox in Figure 1, four categories of structuralvariables are listed that have the capacity toshape health lifestyles: (1) class circumstances,(2) age, gender, and race/ethnicity, (3) collec-tivities, and (4) living conditions. Each ofthese categories is suggested by a review of
the research literature.
Class Circumstances
The first category of structural variables isclass circumstances, which is likely the most
powerful influence on lifestyle forms. The closeconnection between class and lifestyles has been
observed since the nineteenth century whenMarx (1960) mentioned lifestyle differences inwriting about politics in the 1850s, and Veblen
([1899] 1994) used the concept of lifestyles asa basis for his theory of the leisure class. Itremained for Weber ([1922] 1978), however,to produce the most insightful account of thelink between lifestyles and socioeconomic status.
Weber (1946) not only found that lifestylesexpressed distinct differences between statusgroups and their adoption was a necessaryfeature of upward social mobility, but he alsoobserved that powerful strata were socialcarriers of particular ways of living. Thesecarrier strata were important causal forces intheir own right as they transmitted class-specificnorms, values, religious ethics, and ways of life
across generations (Kalberg 1994).The seminal study detailing class as the mostdecisive variable in the determination ofhealth lifestyles is Bourdieus (1984)Distinc-tion that included a survey of differences insports preferences and eating habits betweenFrench professionals (upper-middle class) andthe working class. Bourdieu found the workingclass to be more attentive to the strength of themale body than to its shape, and to favor food
that is both cheap and nutritious; in contrast, theprofessional class prefers food that is tasty,healthy, light, and low in calories. As for leisuresports such as sailing, skiing, golf, tennis, andhorseback riding, Bourdieu noted that theworking class not only faces economic barriersto participation, but also barriers in the formof hidden entry requirements of family tradi-tion, obligatory dress and behavior, and early
socialization.Thus, Bourdieu formulated the notion of thedistance from necessity that emerges as a keyexplanation of class differences in lifestyles. He
points out that the more distant a person is fromforaging for economic necessity, the greater thefreedom and time that person has to develop andrefine personal tastes in line with a more priv-ileged class status. Lower social strata, in turn,tend to adopt the tastes consistent with their class
position, in which acquiring items of necessityis paramount.
In Great Britain, Blaxter (1990) found thatimportant differences in health lifestyles
persisted between classes, with the upper andupper-middle classes taking better care oftheir health than the working and lower classes.Blaxter concluded that socioeconomic circum-stances and environment determined the
extent to which health lifestyles were prac-ticed effectively. Consequently, living ahealthy lifestyle was not simply a matter of indi-
56 JOURNAL OF HEALTH AND SOCIAL BEHAVIOR
#2102Jnl of Health and Social BehaviorVol. 46 146105-cockerham
Delivered by Ingenta toUNIVERSITY OF NEVADA, RENO (cid 1060), Univ. of Nevada-Reno (cid 291575), University
of Nevada, Reno (cid 57010993)IP : 127.0.0.1
Tue, 13 Sep 2005 20:50:48
8/2/2019 Life Style Cockerman
7/17
vidual choice, but to a large extent dependedupon a persons social and material environmentfor its success. Other research in Britain alsofound major distinctions in the health lifestylesof the various classes, with less positive lifestyles
practiced the lower the rung a person occupieson the social ladder (Adonis and Pollard 1997;Jarvis and Wardle 1999; Reid 1998). A declinein smoking, for example, has been far greater
among the affluent, but very little change hasbeen observed among the British poor (Jarvisand Wardle 1999).
Elsewhere, in Russia and Eastern Europe,middle-age male members of the working classhave been identified as the majorsocial carriersof a particularly unhealthy overall lifestylefeaturing heavy alcohol consumption and bingedrinking, smoking, high fat diets, and an absenceof exercise (Cockerham 1997, 1999, 2000b;Janec^kov 2001; Ostrowska 2001). This lifestyle
pattern, associated with traditional male social-
izing and limited life opportunities, is norma-tive for many men. The result is high levels ofpremature male mortality due to increased heart
HEALTH LIFESTYLE THEORY 57
#2102Jnl of Health and Social BehaviorVol. 46 146105-cockerham
FIGURE 1. Health Lifestyles Paradigm
Delivered by Ingenta toUNIVERSITY OF NEVADA, RENO (cid 1060), Univ. of Nevada-Reno (cid 291575), University
of Nevada, Reno (cid 57010993)IP : 127.0.0.1
Tue, 13 Sep 2005 20:50:48
8/2/2019 Life Style Cockerman
8/17
disease, alcohol-related accidents, and alcoholpoisonings. In the United States, the poor havebeen found to be especially disadvantagedwith respect to positive health lifestyles, withgreater cigarette consumption, more unhealthy
eating and drinking practices, and less partici-pation in exercise across adulthood (Grzywaczand Marks 2001; Snead and Cockerham 2002;Wickrama et al. 1999).
Overall, the lifestyles of the upper and upper-middle classes are the healthiest. Virtually everystudy confirms this. These classes have thehighest participation in leisure-time sports andexercise, healthier diets, moderate drinking, little
smoking, more physical checkups by physicians,and greater opportunities for rest, relaxation,and coping with stress (Blaxter 1990; Grzywaczand Marks 2001; Jarvis and Wardle 1999; Robertand House 2000; Snead and Cockerham2002).
The upper and upper-middle classes arealso the first to have knowledge of new healthrisks and, because of greater resources, are mostable to adopt new health strategies and practices
(Link and Phelan 2000). The advantaged classesare able to move in a more fluid fashion toembrace new health behaviors, such as adoptinglow cholesterol and low carbohydrate diets.Advantaged classes were able to reduce theirrisk of heart disease (which at one time was highrelative to lower classes) so that lower class indi-viduals are now at greater risk. While educationis obviously a critical factor, it is, as noted, only
one dimension of the broader context of classmembership that enables members of highersocial strata to be healthy.
Age, Gender, and Race/Ethnicity
Weber did not consider other stratificationvariables such as age, gender, and race/ethnicity,yet contemporary empirical studies show that
these variables influence health lifestyles. Ageaffects health lifestyles because people tend totake better care of their health as they grow older
by being more careful about the food they eat,resting and relaxing more, and either reducingor abstaining from alcohol use and smoking(Backett and Davison 1995). Exercise, however,is one major health lifestyle activity that declinesand is often lost with advancing age (Grzywacz
and Marks 2001). Yet class can also intersectwith age to produce further differences. Youthfrom lower social strata, for instance, smoke
significantly more their higher strata counter-parts (Jarvis and Wardle 1999). Low incomeelderly, in turn, have been found to make nega-tive changes in their food habits or to disre-gard their diet in response to a negatively
anticipated future, while older people with suffi-cient incomes tend to make positive changeswith their diet as they age (Shifflet 1987; Shif-flett and McIntosh 198687). Structural vari-ables (class and age) were the decisive factorsin each outcome.
Gender is a highly significant variable in thatwomen eat more healthy foods, drink much lessalcohol, smoke less, visit doctors more often for
preventive care, wear seatbelts more frequentlywhen they drive, and, with the exception of exer-cise, have more healthier lifestyles overall thanmen (Abel et al. 1999; Blaxter 1990; Cockerham2000a, 2000b; Denton and Walters 1999;Grzywacz and Marks 2001; Roos et al. 1998;Ross and Bird 1994). Furthermore, in adoles-cence males tend to adopt the health lifestylesof their fathers and females those of theirmothers, thereby establishing the parameters for
the gender-specif ic transmission of healthlifestyles into adulthood (Wickrama et al. 1999).
Whereas gender is an especially powerfulpredictor of health lifestyles, its effects can alsobe moderated by distinctions between classes.There is evidence that people on the higher rungsof the socioeconomic ladder, regardless ofgender, participate more in leisure-time exer-cise, eat healthier foods, and smoke less (Adonis
and Pollard 1997; Blaxter 1990; Reid 1998).This is seen in research in the United States,where Ford et al. (1991) found that lower-classwomen were exceedingly less likely to engagein physical activity (other than housework) thanhigher strata women or males generally. InBritain, Calnan (1987) found that middle-classwomen placed a greater emphasis on the needfor a balanced diet high in fiber and low infats and carbohydrates; working-class women
were significantly more likely to insist onsubstantial meals containing meat and twovegetables.
Race and ethnicity are presumed to be impor-tant, but there is a paucity of research directlycomparing the health lifestyles of different racialand ethnic groups. Black-white comparisonsin the United States show that whites often drink,smoke, exercise, and practice weight control
more than blacks (George and Johnson 2001;Grzywacz and Marks 2001; Johnson and Hoff-mann 2000; Lindquist, Cockerham, and Hwang
58 JOURNAL OF HEALTH AND SOCIAL BEHAVIOR
#2102Jnl of Health and Social BehaviorVol. 46 146105-cockerham
Delivered by Ingenta toUNIVERSITY OF NEVADA, RENO (cid 1060), Univ. of Nevada-Reno (cid 291575), University
of Nevada, Reno (cid 57010993)IP : 127.0.0.1
Tue, 13 Sep 2005 20:50:48
8/2/2019 Life Style Cockerman
9/17
1999), but the extent of the differences has notbeen fully documented. There is evidence thatexercise declines more steeply for blacks thanwhites across the course of adulthood, yet thistendency may be explained by blacks having
more functional health problems and living inless safe neighborhoods (Grzywacz and Marks2001). Most health studies on race addressdifferences in levels of morbidity and mortalityrather than specif ic health practices. Thesestudies often suggest that racial disparities inhealth are largely but not exclusively determined
by class position, with disadvantaged socioe-conomic circumstances and the adverse life
experiences associated with them promotingpoor health (Robert and House 2000; Smaje2000).
Research is also needed that investigates therelationship between health lifestyles anddifferent ethnic groups, including how to bestconceptualize and measure ethnicity (Aspinall2001). Existing studies of ethnicity, like thoseof race, have focused more on overall health
profiles than health lifestyles. Nevertheless,
some of these studies are instructive, as seenin research by Karlsen and Nazroo (2002) onthe respective influences of agency and struc-ture on the health of ethnic minorities in GreatBritain. Ethnic identity was considered a conse-quence of agency, even though it is subject toexternal constraints, because a persons identityis also self-constructed and internally defined.Racial discrimination and harassment, along
with class position, were used to measure theeffects of structure. However, our findingssuggest, state Karlsen and Nazroo (2002:18),that ethnicity as identity does not appear toinfluence health; rather ethnicity as structure
both in terms of racialisation [discrimina-tion/harassment] and class experienceisstrongly associated with health for ethnicminority people living in Britain. When itcomes to health lifestyles, the effects of race and
ethnicity may indeed reside more powerfullyin structure than agency.
Collectivities
Collectivities are collections of actorslinked together through particular social rela-tionships, such as kinship, work, religion, and
politics. Their shared norms, values, ideals, andsocial perspectives constitute intersubjectivethought communities beyond individual
subjectivity that reflect a particular collectiveworld view (Zerubavel 1997). The notion ofthought communities is akin to Meads (1934)concept of the generalized other in that both areabstractions of the perspectives of social collec-
tivities that enter into the thinking of the indi-vidual. Religion and ideology are examples ofcollective perspectives that have implicationsfor health lifestyle choices. This is seen in theusual preference of highly religious persons andgroups to have positive health lifestyles sincetheir beliefs affect their choices of food anddiscourage drinking and smoking, while
promoting exercise and personal hygiene (Brown
et al. 2001). However, the full extent of the rela-tionship between religiosity and health lifestylesis not known because of a lack of relevantstudies. This is an important area that needsfurther research.
Little is known also about ideology and healthlifestyles. Research on the effects of the socialistheritage in contemporary Russia show that
prosocialists (those who are in favor of areturn to socialism as it was before Gorbachev)
have less healthy lifestyles than antisocialists,although neither group demonstrated excep-tionally positive health practices (Cockerham,Snead, and DeWaal 2002). Prosocialists had a
particularly passive approach to health lifestylesthat seemed leftover from Soviet times. Thechoices of individuals in Soviet society wereconfined to a single social and political ideology(communism) and expected to conform to it.
If a person got sick, the state was responsiblefor taking care of that person as a benefit of statesocialism. Individual incentives in health matterswere not encouraged. Thus it could be arguedthat communism was bad for ones health.However, the extent to which ideology gener-ally affects health lifestyles beyond this examplehas not been determined.
Living Conditions
Living conditions are a category of structuralvariables pertaining to differences in the qualityof housing and access to basic utilities (e.g.,electricity, gas, heating, sewers, indoor
plumbing, safe piped water, hot water), neigh-borhood facilities (e.g., grocery stores, parks,recreation), and personal safety. To date, there
has been little research linking living conditionsto health lifestyles but the connection isimportant. Blaxter (1990) found in her nation-
HEALTH LIFESTYLE THEORY 59
#2102Jnl of Health and Social BehaviorVol. 46 146105-cockerham
Delivered by Ingenta toUNIVERSITY OF NEVADA, RENO (cid 1060), Univ. of Nevada-Reno (cid 291575), University
of Nevada, Reno (cid 57010993)IP : 127.0.0.1
Tue, 13 Sep 2005 20:50:48
8/2/2019 Life Style Cockerman
10/17
wide British survey that the conditions withinwhich a person lives has important implicationsfor health-related behavior. Health lifestyles weremost effective in positive circumstances andleast effective under negative conditions. In
the United States, living in disadvantaged neigh-borhoods has been associated with a less posi-tive health status (Browning and Cagney 2002).Other research, as previously noted, shows thatliving in less safe neighborhoods significantlycontributes to the low participation of adult
blacks in vigorous outdoor exercise (Grzywaczand Marks 2001). Consequently, living condi-tions can constrain (or enhance) health lifestyles.
Socialization and Experience
Class circumstances and the other variablesshown in box 1 provide the social context forsocialization and experience as depicted by thearrow leading to box 2. This is consistent withBourdieus (1977) view that dispositions to actare constructed through socialization and expe-
rience, with class position providing the socialconditions for this process. The present para-digm, however, adds the additional structuralcategories depicted in box 1, since they may alsoinfluence the social environment within whichsocialization and experience occur.
Whereas primary socialization represents theimposition of societys norms and values on theindividual by significant others and secondary
socialization results from later training, expe-rience is the learned outcome of day-to-dayactivities that comes about through social inter-action and the practical exercise of agency. Itis through both socialization and experience thatthe actor acquires reflexive awareness and thecapacity to perform agency, but experiencewith respect to life choicesprovides the essen-tial basis for agencys practical and evaluativedimensions to evolve over time. This is espe-
cially the case as people confront new socialsituations and conditions.
Life Choices (Agency)
Figure 1 shows that socialization and expe-rience (box 2) provides the capacity for lifechoices (agency) depicted in box 3. As previ-
ously noted, the term life choices was intro-duced by Weber and refers to the self-directionof ones behavior. It is an English language trans-
lation ofLebensfhrung, which in German liter-ally means conducting or managing ones life.Life choices are a process of agency by whichindividuals critically evaluate and choose theircourse of action. Webers notion of life choices
differs from rational choice theory in that itaccounts for both means-ends rationality as wellas the interpretive process whereby the poten-tial outcomes of choices are imagined, evalu-ated, and reconstructed when necessary (Emir-
bayer and Mische 1998). Weber (1949)maintained that individuals have the capacity tointerpret their situation, make deliberate choices,and attach subjective meaning to their actions.
All social action in his view takes place incontexts that imply both constraints andopportunities, with the actors interpretive under-standing (Verstehen) of the situation guiding
behavioral choices (Kalberg 1994).
Life Chances (Structure)
Class circumstances and to a lesser degree
the other variables in box 1 constitute lifechances (structure) shown in box 4. Weber wasambiguous about what he meant by life chances,
but the term is usually associated with the advan-tages and disadvantages of relative class situa-tions. Dahrendorf (1979:73) finds that the bestmeaning of life chances in Webers work is thecrystallized probability of finding satisfac-tion for interests, wants and needs, thus the prob-
ability of the occurrence of events which bringabout such satisfaction. Consequently, thehigher a persons position in a class hierarchy,the better the persons life chances (probabili-ties for satisfaction) and vice versa. Dahrendorf(1979:65) adds the following clarification: ForWeber, the probability of sequences of action
postulated in the concept of chance is not merelyan observed and thus calculable probability, butis a probability which is invariably anchored in
structural conditions. Webers thesis is thatchance is socially determined and social struc-ture is an arrangement of chances. Therefore,life chances represent the influence of structurein Webers oeuvre and this paradigm.
Choice and Chance Interplay
The arrows in Figure 1 indicate the dialec-tical interplay between life choices (box 3) andlife chances (box 4). This interaction is
60 JOURNAL OF HEALTH AND SOCIAL BEHAVIOR
#2102Jnl of Health and Social BehaviorVol. 46 146105-cockerham
Delivered by Ingenta toUNIVERSITY OF NEVADA, RENO (cid 1060), Univ. of Nevada-Reno (cid 291575), University
of Nevada, Reno (cid 57010993)IP : 127.0.0.1
Tue, 13 Sep 2005 20:50:48
8/2/2019 Life Style Cockerman
11/17
Webers most important contribution to concep-tualizing lifestyle construction (Cockerham,Abel, and Lschen 1993; Cockerham, Rtten,and Abel 1997). Choices and chances operatein tandem to determine a distinctive lifestyle for
individuals, groups, and classes. Life chances(structure) either constrain or enable choices(agency); agency is not passive in this process,however. As Archer (2003) puts it, whetherconstraints and enablements are exercised ascausal powers is based on agency choosing the
practices to be influenced. Contraints, saysArcher (2003:4), require something toconstrain, and enablements something to
enable. Consequently, people have to considera course of action if their actions are to be eitherconstrained or enabled. People therefore aligntheir goals, needs, and desires with their prob-abilities for realizing them and choose a lifestyleaccording to their assessments of the reality oftheir resources and class circumstances. Unre-alistic choices are not likely to succeed or beselected, while realistic choices are basedupon what is structurally possible.
In this context, choices and chances notonly are connected d ialectically, but areanalytically distinct. Archer (1998:369) articu-lates this point: Because the emergent prop-erties of structures and the actual experiencesof agents are not synchronized (due to thevery nature of society as an open system), thenthere will always be the inescapable need for atwo-part account. Weber provides such a frame-
work. He conceptualizes choice and chance asseparate components in the activation andconduct of a lifestyle, and he merges thedifferent functions of agency and structurewithout either losing their distinctiveness.
Dispositions to Act (Habitus)
Figure 1 shows that the interaction of life
choices and life chances produce individualdispositions toward action (box 5). These dispo-sitions constitute a habitus. The notion of habitusoriginates with Edmund Husserl ([1952]1989:26693) who used the term to describehabitual action that is intuitively followed andanticipated. The concept has been expanded
by Bourdieu (1977:7295) to serve as his coreexplanation for the agency-structure relation-
ship in lifestyle dispositions (Bourdieu1984:169225). Bourdieu (1990:53) defineshabitus as systems of durable, transposable
dispositions, structured structures predisposedto operate as structuring structures, that is, as
principles which generate and organize prac-tices and representations that can be objectivelyadapted to their outcomes without presupposing
a conscious aiming at ends or an express masteryof the operations necessary in order to attainthem. Put another way, the habitus serves as acognitive map or set of perceptions that routinelyguides and evaluates a persons choices andoptions. It provides enduring dispositions towardacting deemed appropriate by a person in partic-ular social situations and settings. Included aredispositions that can be carried out even without
giving them a great deal of thought in advance.They are simply habitual ways of acting whenperforming routine tasks.
The influence of exterior social structures andconditions are incorporated into the habitus, aswell as the individuals own inclinations, pref-erences, and interpretations. The dispositionsthat result not only reflect established norma-tive patterns of social behavior, but they alsoencompass action that is habitual and even intu-
itive. Through selective perception the habitusmolds aspirations and expectations into cate-gories of the probable that impose perceptual
boundaries on dispositions and the potential foraction. As an acquired system of generativeschemes, observes Bourdieu (1990:55), thehabitus makes possible the free production ofall the thoughts, perceptions, actions, inherentin the particular conditions of its production
and only those.When Bourdieu speaks of the internalizationof class conditions and their transformation into
personal dispositions toward action, he isdescribing conditions similar to Webers conceptof life chances that determine materially, socially,and culturally what is probable, possible, orimpossible for a member of a particular socialgroup or class (Swartz 1997:104). Individualswho internalize similar life chances share the
same general habitus because, as Bourdieu(1977:85) explains, they are more likely to havesimilar shared experiences: Though it is impos-sible forallmembers of the same class (or eventwo of them) to have the same experiences, inthe same order, it is certain that each memberof the same class is more likely than any memberof another class to have been confronted withthe situations most frequent for members of that
class. As a result, there is a high degree ofaffinity in health lifestyle choices amongmembers of the same class. Bourdieu holds that,
HEALTH LIFESTYLE THEORY 61
#2102Jnl of Health and Social BehaviorVol. 46 146105-cockerham
Delivered by Ingenta toUNIVERSITY OF NEVADA, RENO (cid 1060), Univ. of Nevada-Reno (cid 291575), University
of Nevada, Reno (cid 57010993)IP : 127.0.0.1
Tue, 13 Sep 2005 20:50:48
8/2/2019 Life Style Cockerman
12/17
while they may depart from class standards,personal styles are never more than a deviationfrom a style of a class that relates back to thecommon style by its difference.
Even though Bourdieu allows agency some
autonomy (e.g., agents are determined only tothe extent that they determine themselves), hisemphasis on structure with respect to routineoperations of the habitus clearly delineates alesser role for agency than the individualisthealth lifestyles paradigm. Some have arguedthat Bourdieu strips agency of much of its crit-ical reflexive character (Bohman 1999).Turner and Wainwright (2003:273) disagree and
find that Bourdieu gives full recognition toagency through his notions of strategy and prac-tices, while illustrating the powerful role ofinstitutions and resources in shaping,constraining, and producing human agency.Simon Williams (1995) also defends Bourdieu
by pointing out that choice is not precluded bythe habitus, and he is able to account for therelative durability of different forms of healthlifestyles among the social classes.
It can also be argued that theprocess of expe-rience rescues Bourdieus concept of habitusfrom the charge of social determinism. Throughexperience, agency acquires new informationand rationales for prompting creativity andchange through the habitus. As Bourdieu (Bour-dieu and Wacquant 1992:133) explains, eventhough experiences confirm habitus, since thereis a high probability that most people encounter
circumstances that are consistent with those thatoriginally fashioned it, the habitus neverthe-less is an open system of dispositions that isconstantly subjected to experiences, and there-fore constantly affected by them in a way thatreinforces or modifies its structures. Thus thehabitus can be creative and initiate changes indispositions.
Bourdieu (1996) calls for the abandonment
of theories that explicitly or implicitly treatpeople as mere bearers (Trgers) of structure.Yet he also maintains that the rejection of mech-anistic theories of behavior does not imply thatwe should bestow on some creative free will theexclusive power to generally constitute the mean-ings of situations and determine the intentionsof others. The dispositions generated by thehabitus tend to be compatible with the behav-
ioral parameters set by the wider society; there-fore, usual and practical modes of behavingnot unpredictable noveltytypically prevail.
Completing the Paradigm
Figure 1 shows that dispositions (box 5)produce practices (action) that are representedin box 6. The practices that result from the
habitus can be based on deliberate calculations,habits, or intuition. Bourdieu (1984) helps usrecognize that practices linked to health lifestylescan be so integrated into routine behavioralrepertories that they can be acted out more orless unthinkingly once established in the habitus.Bourdieu observes that people tend to adoptgeneralized strategies (a sense of the game)oriented toward practical ends in routine situa-tions that they can habitually follow withoutstopping to analyze them. As a routinized featureof everyday life, it is therefore appropriate toview health lifestyles as guided more by a prac-tical than abstract logic (Williams 1995).
The four most common practices measuredin studies of health lifestyles are alcohol use,smoking, diet, and exercise. These are shown in
box 7 along with other practices such as phys-ical checkups and automobile seatbelt use that
comprise typical forms of action taken or nottaken. The practices themselves may be positiveor negative, but they nonetheless comprise a
persons overall pattern of health lifestyles asrepresented in box 8. It is important to note thatthese practices sometimes have a complexity oftheir own. Smoking tobacco in any form is nega-tive, but moderate alcohol use reduces the riskof heart disease more so than heavy drinking
(which promotes it) and abstinence (Klatsky1999). Eating fruits and vegetables is positive,but consuming meat can be either positive ornegative depending on how it is cooked and itsfat content. Relatively vigorous leisure-timeexercise has more health benefits than phys-ical activity at work because the latter is subjectto stress from job demands and time sched-ules, while walking and other everyday formsof exercise have some health value (Dunn et
al. 1999). However, measures of leisure-timeexercise may not fully represent the physicalactivities of women who take care of childrenand do housework (Ainsworth 2000). It is there-fore necessary that researchers take the multi-faceted features of health lifestyle practices intoaccount when analyzing them
Action (or inaction) with respect to a partic-ular health practice leads to its reproduction,
modification, or nullification by the habitusthrough a feedback process. This is shown inFigure 1 by the arrow showing movement
62 JOURNAL OF HEALTH AND SOCIAL BEHAVIOR
#2102Jnl of Health and Social BehaviorVol. 46 146105-cockerham
Delivered by Ingenta toUNIVERSITY OF NEVADA, RENO (cid 1060), Univ. of Nevada-Reno (cid 291575), University
of Nevada, Reno (cid 57010993)IP : 127.0.0.1
Tue, 13 Sep 2005 20:50:48
8/2/2019 Life Style Cockerman
13/17
from box 8 back to box 5. This is consistent withBourdieus (1977, 1984) assertion that whendispositions are acted upon they tend to repro-duce or modify the habitus from which they arederived. As conceptualized by Bourdieu, the
habitus is the centerpiece in the health lifestyleparadigm.
MEASURING HEALTH LIFESTYLES
Although individuals make health lifestylechoices, the aggregate influence of collectiveentities and conditions on these choices alsoneeds to be measured if the reality of everydaylife is to be captured. This strategy presentsmethodological issues since approaches empha-sizing the effects of structure on individuals mayoverlook the creativity of social agents. Con-versely, microsociological approaches thatconcentrate on individuals may underestimatethe effects of structure on personal choices.Qualitative methods such as participant obser-vation have to be alert to patterned health
practices and the collective basis for thosepatterns. However, as Sibeon (2004) observes,there are limits to what can be achieved bymicrolevel methods in addressing agency-struc-ture questions, since such methods are notequipped theoretically or methodologically tomeasure macrophenomena.
Bourdieu (1984) selected correspondenceanalysis for his lifestyle research. Correspon-
dence analysis is a method to organize data,investigate similarities and differences betweencategories of variables, and graphically depictrelationships (Greenacre and Blasius 1993). Itis similar to cluster analysis, but it identifiescomplex patterns of behavior in relation tosociodemographic variables more efficiently andquickly, while reducing the potential for insta-
bility by using a fixed algorithm. Correspon-dence analysis produces plots showing how
dependent variables (e.g., lifestyle practices)cluster in particular relationships with inde-
pendent variables (e.g., structural variables suchas class, age, gender, and race), and it also illus-trates the relative strengths and weaknesses ofthose relationships according to their spatialdistance from each other. Bourdieu (1984)formulated his concept of social space as astructure using correspondence analysis to merge
a space of social positions and space oflifestyles into one space that can be displayedand interpreted simultaneously.
A limitation of correspondence analysis isthat it can be used only for displaying relation-ships, not hypothesis testing. Since many vari-ables that have been discussed are interrelated,statistical techniques are required for testing
hypotheses that measure the relationships thathave predictive power exclusive of the effectsof the other variables. Several statistical models(e.g., regression analysis, path or structural equa-tion modeling) exist that can accomplish this.
However, determining the effects of structureon health lifestyle practices requires the con-struction of independent variables having collec-tive properties indicative of such structures.
Measuring class effects is a challenge becausethe usual socioeconomic variables of income,education, and occupational prestige can also
be depicted as individual characteristics. Oneapproach is to apply class categories to thefamily/household rather than therespondent/individual. The status of the person(or perhaps persons) in the family/householdwith the highest level of labor-market partici-
pation can be conceptualized as providing a
master social status to the household repre-senting its collective position vis--vis themarketplace (Erickson and Goldthorpe 1992).This outcome is evident when the parentssocialstanding is passed to their children and thehousehold as a whole is accorded a particularsocial position in the community. Education canalso be measured with respect to the prestige ofthe institution attended, so that the status asso-
ciated with an individuals education can beconsidered a reflection of the institution ratherthan the individual. An index of living condi-tions can be constructed from the percentage ofhouseholds in particular neighborhoods orcensus tracts with basic utilities, indoor
plumbing, and hot water, as well as thepercentage of parks, recreational facilities,restaurants, and grocery stores. Variables suchas these are not the properties of similar indi-
viduals, but those of structures that constrain orenable individuals in their health lifestylechoices.
In order to determine the relative effects ofindividual and structural characteristics on adependent variable, multilevel analysis usingvarious hierarchical regression techiques (e.g.,multilevel regression models, HLM, VARCL,MLn) is required (Luke 2004). Briefly stated,
multilevel analysis examines the interactionbetween variables that describe individuals atone level (level 1), structural entities at the next
HEALTH LIFESTYLE THEORY 63
#2102Jnl of Health and Social BehaviorVol. 46 146105-cockerham
Delivered by Ingenta toUNIVERSITY OF NEVADA, RENO (cid 1060), Univ. of Nevada-Reno (cid 291575), University
of Nevada, Reno (cid 57010993)IP : 127.0.0.1
Tue, 13 Sep 2005 20:50:48
8/2/2019 Life Style Cockerman
14/17
(level 2), and sequentially higher levels, if neces-sary, depending on the variables conceptual posi-tion in a structural hierarchy. By comparingchanges in the regression equations, the relativeeffects of each level of variables on health
lifestyle practices can be simultaneouslydetermined.
CONCLUSION
A central theme of this article is that the indi-vidualistic paradigm of health lifestyles is toonarrow and unrealistic because it fails toconsider structural influences on health lifestylechoices. In order to correct this course andformulate a theory where none currently exists,a health lifestyle model is presented that accordsstructure a role that is consistent with its influ-ence in the empirical world. There are timeswhen structure outweighs but does not negateagency and other times when structure over-whelms agency, and these situations need to
be included in concepts explaining health
lifestyle practices. A macrosocial orientationdoes not mean that action is structurally prede-termined; rather, it recognizes that socialstructures influence the thoughts, decisions, andactions of individuals (Sibeon 2004).
The theoretical paradigm presented in thisarticle is strongly influenced by Weber and Bour-dieu. Although Bourdieu, in particular, has hiscritics, his notion of habitus nevertheless repre-
sents a novel and logical conceptualization ofthe internalization of external structures in themind and perceptual processes of the individual.The result is a registry of dispositions to act inways that are practical and invariably consistentwith the socially approved behavioral pathwaysof the larger social order or some class or grouptherein.
The theoretical model of health lifestylespresented here states that four categories of (1)
structural variables, especially (a) class circum-stances, but also (b) age, gender, and race/ethnicity, (c) collectivities, and (d) living condi-tions, provide the social context for (2) social-ization and experience that influence (3) lifechoices (agency). These structural variables alsocollectively constitute (4) life chances (struc-ture). Choices and chances interact and commis-sion the formation of (5) dispositions to act
(habitus), leading to (6) practices (action),involving (7) alcohol use, smoking, diet, andother health-related actions. Health practices
constitute patterns of (8) health lifestyles whosereenactment results in their reproduction (ormodification) through feedback to the habitus.This theory is an initial representation of thehealth lifestyle phenomenon and is subject to
verification, change, or rejection through empir-ical application. It is a beginning for theoreticalformulations concerning a major aspect of day-to-day social behavior for which no other theorynow exists.
REFERENCES
Abel, Thomas, Esther Walter, Steffen Niemann, andRolf Weitkunat. 1999. The Berne-MunichLifestyle Panel. Sozial- und Prventivmedizin44:91106.
Adler, Nancy E., Thomas Boyce, Margaret A.Chesney, Sheldon Cohen, Susan Folkman, RobertL. Kahn, and S. Leonard Syme. 1994. Socioe-conomic Status and Health: The Challenge ofthe Gradient.American Psychologist10:1524.
Adonis, Andrew and Stephen Pollard. 1997. AClass Act: The Myth of Britains Classless Society.
London: Penguin.Ainsworth, Barbara E. 2000. Issues in the Assess-
ment of Physical Activity in Women. ResearchQuarterly for Exercise and Sport71:3750.
Annandale, Ellen. 1998. The Sociology of Health andMedicine: A Critical Introduction. Cambridge,United Kingdom: Polity Press.
Archer, Margaret S. 1995.Realist Social Theory: TheMorphogenetic Approach. Cambridge, UnitedKingdom: Cambridge University Press.
. 1998. Realism and Morphogensis. Pp.35681 in Critical Realism, edited by MargaretArcher, Roy Bhaskar, Andrew Collier, TonyLawson, and Alan Norrie. London: Routledge.
. 2003. Structure, Agency and the InternalConversation. Cambridge, United Kingdom:Cambridge University Press.
Aspinall, Peter J. 2001. Operationalising the Collec-tion of Ethnicity Data in Studies of the Sociologyof Health and Illness. Sociology of Health andIllness 23:82982.
Backett, Kathryn C. and Charlie Davison. 1995.Lifecourse and Lifestyle: The Social and CulturalLocation of Health Behaviours. Social Scienceand Medicine 40:62938.
Bauman, Zygmunt. 1992. Intimations of Post-modernity. London: Routledge.
. 1999.In Search of Politics. Stanford, CA:Stanford University Press.
. 2000. Liquid Modernity. Cambridge,United Kingdom: Polity Press.
Beck, Ulrich. 1992. Risk Society: Towards a NewModernity. Translated by Mark Ritter. London:Sage.
64 JOURNAL OF HEALTH AND SOCIAL BEHAVIOR
#2102Jnl of Health and Social BehaviorVol. 46 146105-cockerham
Delivered by Ingenta toUNIVERSITY OF NEVADA, RENO (cid 1060), Univ. of Nevada-Reno (cid 291575), University
of Nevada, Reno (cid 57010993)IP : 127.0.0.1
Tue, 13 Sep 2005 20:50:48
http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0303-8408()44L.91[aid=6535165]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0303-8408()44L.91[aid=6535165]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0141-9889()23L.829[aid=6535162]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0141-9889()23L.829[aid=6535162]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0141-9889()23L.829[aid=6535162]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0277-9536()40L.629[aid=786509]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0277-9536()40L.629[aid=786509]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0277-9536()40L.629[aid=786509]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0141-9889()23L.829[aid=6535162]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0141-9889()23L.829[aid=6535162]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0277-9536()40L.629[aid=786509]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0277-9536()40L.629[aid=786509]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0303-8408()44L.91[aid=6535165]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0303-8408()44L.91[aid=6535165]8/2/2019 Life Style Cockerman
15/17
Bhaskar, Roy. 1998. The Possibility of Naturalism.3d ed. London: Routledge.
Blaxter, Mildred. 1990. Health and Lifestyles.London: Routledge.
Bohman, James. 1999. Practical Reason and CulturalConstraint: Agency in Bourdieus Theory of Prac-tice. Pp. 12952 in Bourdieu: A Cr iticalReader, edited by Richard Shusterman. Oxford,United Kingdom: Blackwell.
Bourdieu, Pierre. 1977. Outline of a Theory ofPractice. Translated by Richard Nice. Cambridge,United Kingdom: Cambridge University Press.
. 1984.Distinction. Translated by RichardNice. Cambridge, MA: Harvard University Press.
. 1990. The Logic of Practice. Translated byRichard Nice. Stanford, CA: Stanford Univer-
sity Press.. 1996. The Rules of Art. Translated by Susan
Emanuel. Cambridge, United Kingdom:Cambridge University Press.
Bourdieu, Pierre and Loc J. D. Wacquant. 1992.AnIntroduction to Reflexive Sociology. Chicago, IL:University of Chicago Press.
Brown, Tamara L., Gregor y S. Parks, Rick S.
Zimmerman, and Clarenda M. Phillips. 2001.The Role of Religion in Predicting Adolescent
Alcohol Use and Problem Drinking.Journal ofStudies on Alcohol65:696706.
Browning, Christopher and Kathleen A. Cagney.
2002. Neighborhood Structural Disadvantage,Collective Efficacy, and Self-Rated PhysicalHealth in an Urban Setting.Journal of Healthand Social Behavior 43:38399.
Calnan, Michael. 1987.Health and Illness. London:Tavistock.
Clarke, Adele E., Janet K. Shim, Laura Mamo,
Jennifer Ruth Fosket, and Jennifer R. Fishman.2003. Biomedicalization: Technoscientific Trans-formations of Health, Illness, and U.S. Biomedi-cine.American Sociological Review 68:16194.
Cockerham, William C. 1997. The Social Deter-minants of the Decline of Life Expectancy inRussia and Eastern Europe: A Lifestyle Expla-nation. Journal of Health and Social Behavior38:13148.
. 1999.Health and Social Change in Russiaand Eastern Europe. London: Routledge.
. 2000a. The Sociology of Health Behaviorand Health Lifestyles. Pp. 15972 inHandbookof Medical Sociology, 5th ed., edited by ChloeBird, Peter Conrad, and Allen M. Fremont. Upper
Saddle River, NJ: Prentice-Hall.. 2000b. Health Lifestyles in Russia. Social
Science and Medicine 51:131324.Cockerham, William C., Thomas Abel, and Gnther
Lschen. 1993. Max Weber, Formal Rationality,
and Health Lifestyles. The Sociological Quar-
terly 34:41335.Cockerham, William C., Alfred Rtten, and Thomas
Abel. 1997. Conceptualizing Contemporary
Health Lifestyles: Moving beyond Weber. TheSociological Quarterly 38:32142.
Cockerham, William C., M. Christine Snead, andDerek F. DeWaal. 2002. Health Lifestyles inRussia and the Socialist Heritage. Journal ofHealth and Social Behavior 43:4255.
Crawford, Robert. 1984. A Cultural Account ofHealth: Control, Release, and the Social Body.Pp. 60103 inIssues in the Political Economy ofHealth Care, edited by John McKinley. New York:Tavistock.
Crompton, Rosemary. 1998. Class and Stratification.2d ed. Oxford, United Kingdom: Polity Press.
Dahrendorf, Ralf. 1979.Life Chances. Chicago, IL:University of Chicago Press.
Demers, Andre, Jocelyn Bisson, and Jzabelle
Palluy. 1999. Wives Convergence with TheirHusbands Alcohol Use: Social Conditions asMediators. Journal of Studie s of Alcohol60:36877.
Demers, Andre, Sylvia Kairouz, Edward M. Adlaf,Louis Glickman, Brenda Newton-Taylor, andAlain Marchand. 2002. Multilevel Analysis ofSituational Drinking among Canadian Under-graduates. Social Science and Medicine55:41524.
Denton, Margaret and Vivienne Walters. 1999.Gender Differences in Structural and BehavioralDeterminants of Health: An Analysis of the SocialProduction of Health. Social Science and Medi-cine 48:122135.
dHoutaud, A. and Mark G. Field. 1984. TheImage of Health: Variations in Perception by SocialClass in a French Population. Sociology of Healthand Illness 6:3059.
Dunn, Andrea L., Bess H. Marcus, James B. Kampert,Melissa E. Garcia, Harold W. Kohl III, and Steven
N. Blair. 1999. Comparison of Lifestyle andStructural Interventions to Increase PhysicalActivity and Cardiorespiratory Fitness.Journalof the American Medical Association 281:32734.
Durkheim, Emile. [1895] 1950. The Rules of Socio-logical Method. New York: Free Press.
Emirbayer, Mustafa and Ann Mische. 1998. WhatIs Agency? American Journal of Sociology103:9621023.
Erickson, Robert E. and John H. Goldthorpe. 1992.The Constant Flux: A Study of Class Mobility in Industrial Society. Oxford, United Kingdom:Clarendon Press.
Ford, Earl S., Robert K. Merritt, Gregory W. Heath,Kenneth E. Powell, Richard A. Washburn, AndreaKriska, and Gwendolyn Halle. 1991. PhysicalActivity Behaviors in Lower and Higher Socioe-conomic Status Populations.American Journalof Epidemiology 133:124656.
Frohlich, Katherine L., Ellen Corin, and LouisePotvin. 2001. A Theoretical Proposal for the Rela-
tionship between Context and Disease. Sociologyof Health and Illness 23:77697.
George, Valerie A. and Paulette Johnson. 2001.
HEALTH LIFESTYLE THEORY 65
#2102Jnl of Health and Social BehaviorVol. 46 146105-cockerham
Delivered by Ingenta toUNIVERSITY OF NEVADA, RENO (cid 1060), Univ. of Nevada-Reno (cid 291575), University
of Nevada, Reno (cid 57010993)IP : 127.0.0.1
Tue, 13 Sep 2005 20:50:48
http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0022-1465()43L.383[aid=6535096]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0022-1465()43L.383[aid=6535096]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0022-1465()43L.383[aid=6535096]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0022-1465()38L.131[aid=1983724]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0022-1465()38L.131[aid=1983724]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0277-9536()51L.1313[aid=6535160]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0277-9536()51L.1313[aid=6535160]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0277-9536()51L.1313[aid=6535160]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0038-0253()34L.413[aid=6535159]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0038-0253()34L.413[aid=6535159]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0038-0253()34L.413[aid=6535159]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0038-0253()38L.321[aid=1983722]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0038-0253()38L.321[aid=1983722]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0038-0253()38L.321[aid=1983722]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0022-1465()43L.42[aid=6535158]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0022-1465()43L.42[aid=6535158]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0022-1465()43L.42[aid=6535158]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0096-882X()60L.368[aid=6535157]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0096-882X()60L.368[aid=6535157]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0277-9536()55L.415[aid=6535156]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0277-9536()55L.415[aid=6535156]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0277-9536()48L.1221[aid=6089284]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0277-9536()48L.1221[aid=6089284]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0277-9536()48L.1221[aid=6089284]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0141-9889()6L.30[aid=838394]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0141-9889()6L.30[aid=838394]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0141-9889()6L.30[aid=838394]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0098-7484()281L.327[aid=77208]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0098-7484()281L.327[aid=77208]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0098-7484()281L.327[aid=77208]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0002-9602()103L.962[aid=838934]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0002-9602()103L.962[aid=838934]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0002-9262()133L.1246[aid=6535155]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0002-9262()133L.1246[aid=6535155]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0002-9262()133L.1246[aid=6535155]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0141-9889()23L.776[aid=6535154]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0141-9889()23L.776[aid=6535154]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0141-9889()23L.776[aid=6535154]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0277-9536()48L.1221[aid=6089284]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0277-9536()48L.1221[aid=6089284]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0141-9889()23L.776[aid=6535154]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0141-9889()23L.776[aid=6535154]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0002-9262()133L.1246[aid=6535155]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0002-9262()133L.1246[aid=6535155]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0002-9602()103L.962[aid=838934]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0002-9602()103L.962[aid=838934]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0098-7484()281L.327[aid=77208]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0098-7484()281L.327[aid=77208]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0141-9889()6L.30[aid=838394]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0141-9889()6L.30[aid=838394]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0277-9536()48L.1221[aid=6089284]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0277-9536()48L.1221[aid=6089284]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0096-882X()60L.368[aid=6535157]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0096-882X()60L.368[aid=6535157]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0277-9536()55L.415[aid=6535156]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0277-9536()55L.415[aid=6535156]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0022-1465()43L.42[aid=6535158]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0022-1465()43L.42[aid=6535158]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0038-0253()38L.321[aid=1983722]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0038-0253()38L.321[aid=1983722]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0038-0253()34L.413[aid=6535159]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0038-0253()34L.413[aid=6535159]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0022-1465()38L.131[aid=1983724]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0022-1465()38L.131[aid=1983724]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0277-9536()51L.1313[aid=6535160]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0277-9536()51L.1313[aid=6535160]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0022-1465()43L.383[aid=6535096]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0022-1465()43L.383[aid=6535096]8/2/2019 Life Style Cockerman
16/17
Weight Loss Behaviors and Smoking in CollegeStudents of Diverse Ethnicity.American Journalof Health Behavior 25:11524.
Giddens, Anthony. 1984. The Constitution of Society:Outline of the Theory of Structuration. Berkeley:University of California Press.
. 1991.Modernity and Self-Identity: Self andSociety in the Late Modern Age. Stanford, CA:Stanford University Press.
Gochman, David S. 1997. Health Behavior Research,Cognate Disciplines, Future Identity, and an Orga-nizing Matrix: An Integration of Perspectives.Pp. 395425 in Handbook of Health Behavior,vol. 4, edited by David Gochman. New York:Plenum.
Greenacre, Michael and Jrg Blasius, eds. 1993.
Correspondence Analysis in the Social Sciences.London: Academic Press.
Grzywacz, Joseph G. and Nadine F. Marks. 2001.Social Inequalities and Exercise during Adult-hood: Toward an Ecological Perspective.Journalof Health and Social Behavior 42:20220.
Hardey, Michael. 1999. Doctor in the House: TheInternet as a Source of Lay Knowledge and theChallenge to Expertise. Sociology of Health andIllness 21:82035.
Husserl, Edmund. [1952] 1989.Ideas Pertaining toa Pure Phenomenology and to a Phenomenolog-ical Philosophy. Translated by R. Rojecwicz andA. Schuwer. London: Kluwer Academic.
Janec^kov, Hana. 2001. Transformation of the HealthCare System in the Czech RepublicA Socio-logical Perspective. Pp. 34764 in The BlackwellCompanion to Medical Sociology, edited byWilliam Cockerham. Oxford, United Kingdom:Blackwell.
Jarvis, Martin J. and Jane Wardle. 1999. Social
Patterning of Individual Health Behaviours: TheCase of Cigarette Smoking. Pp. 24056 in SocialDeterminants of Health , edited by MichaelMarmot and Richard G. Wilkinson. Oxford,United Kingdom: Oxford University Press.
Johnson, Robert A. and John P. Hoffmann. 2000.Adolescent Cigarette Smoking in the U.S.Racial/Ethnic Subgroups: Findings from theNational Education Longitudinal Study.Journalof Health and Social Behavior 41:392407.
Kalberg, Stephen. 1994.Max Webers Comparative-Historical Sociology. Chicago, IL: University ofChicago Press.
Karlsen, Saffron and James Y. Nazroo. 2002. Agencyand Structure: The Impact of Ethnic Identity andRacism on the Health of Ethnic Minority People.Sociology of Health and Illness 24:120.
Klatsky, Arthur L. 1999. Moderate Drinking andReduced Risk of Heart Disease.Alcohol Researchand Health 23:1523.
Laaksonen, Mikko, Ritva Prttl, and Eero Lahelma.
2002. Sociodemographic Determinants of Mul-tiple Unhealthy Behaviours. ScandinavianJournal of Public Health 30:17.
Lindquist, Christine, William C. Cockerham, andSean-Shong Hwang. 1999. Drinking Patternsin the American Deep South.Journal of Studieson Alcohol60:66366.
Link, Bruce and Jo Phelan. 2000. Evaluating theFundamental Cause Explanation for Social Dispar-ities in Health. Pp. 3347 in Handbook ofMedical Sociology, 5th ed., edited by Chloe E.Bird, Peter Conrad, and Allen M. Fremont. UpperSaddle River, NJ: Prentice-Hall.
Lomas, Jonathan. 1998. Social Capital and Health:Implications for Public Health and Epidemiology.Social Science and Medicine 47:118188.
Luke, Douglas A. 2004.Multilevel Modeling. Thou-sand Oaks, CA: Sage.
Marx, Karl. 1960.Politische Schriften [Political Writ-
ings]. Edited by H. Lieber. Stuttgart, Germany:Enke.
Mead, George Herbert. 1934.Mind, Self and Society.Chicago, IL: University of Chicago Press.
Mirowsky, John and Catherine E. Ross. 2003.Educa-tion, Social Status, and Health. New York: Aldinede Gruyter.
Ostrowska, Nina. 2001. In and Out of Communism:The Macrosocial Context of Health in Poland.Pp. 33446 in The Blackwell Companion toMedical Sociology, edited by William Cockerham.Oxford, United Kingdom: Blackwell.
Pescosolido, Bernice A., Jane McLeod, and MargaritaAlegra. 2000. Confronting the Second SocialContract: The Place of Medical Sociology inResearch and Policy for the Twenty-First Century.Pp. 41126 inHandbook of Medical Sociology,5th ed., edited by Chloe Bird, Peter Conrad, andAllen M. Fremont. Upper Saddle River, NJ: Pren-tice-Hall.
Pescosolido, Bernice A. and Beth A. Rubin. 2000.
The Web of Group Affiliations Revisited: SocialLife, Postmodernism, and Sociology.AmericanSociological Review 65:5276.
Reid, Ivan. 1998. Class in Britain. Cambridge, UnitedKingdom: Polity Press.
Robert, Stephanie A. and James S. House. 2000.Socioeconomic Inequalities in Health: AnEnduring Sociological Problem. Pp. 7997 inHandbook of Medical Sociology, 5th ed., editedby Chloe E. Bird, Peter Conrad, and Allen M.Fremont. Upper Saddle River, NJ: Prentice-Hall.
Roos, Eva, Eero Lahelma, Mikko Virtanen, RitvaPrttl, and Pirjo Pietinen. 1998. Gender,Socioeconomic Status and Family Status as Deter-minants of Food Behaviour. Social Science andMedicine 46:151929.
Ross, Catherine E. and Chloe E. Bird. 1994. SexStratification and Health Lifestyle: Consequencesfor Mens and Womens Perceived Health.Journalof Health and Social Behavior 35:16178.
Scott, John. 1996. Stratification and Power: Struc-
tures of Class, Status, and Command. Cambridge,United Kingdom: Polity Press.
Sewell, William H. 1992. A Theory of Structure:
66 JOURNAL OF HEALTH AND SOCIAL BEHAVIOR
#2102Jnl of Health and Social BehaviorVol. 46 146105-cockerham
Delivered by Ingenta toUNIVERSITY OF NEVADA, RENO (cid 1060), Univ. of Nevada-Reno (cid 291575), University
of Nevada, Reno (cid 57010993)IP : 127.0.0.1
Tue, 13 Sep 2005 20:50:48
http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=1087-3244()25L.115[aid=6535153]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=1087-3244()25L.115[aid=6535153]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=1087-3244()25L.115[aid=6535153]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0022-1465()42L.202[aid=6535152]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0022-1465()42L.202[aid=6535152]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0022-1465()42L.202[aid=6535152]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0141-9889()21L.820[aid=1937269]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0141-9889()21L.820[aid=1937269]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0141-9889()21L.820[aid=1937269]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0022-1465()41L.392[aid=2331022]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0022-1465()41L.392[aid=2331022]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0022-1465()41L.392[aid=2331022]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0141-9889()24L.1[aid=3035319]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0141-9889()24L.1[aid=3035319]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=1535-7414()23L.15[aid=6535151]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=1535-7414()23L.15[aid=6535151]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=1535-7414()23L.15[aid=6535151]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=1403-4948()30L.1[aid=6535150]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=1403-4948()30L.1[aid=6535150]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=1403-4948()30L.1[aid=6535150]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0096-882X()60L.663[aid=6535149]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0096-882X()60L.663[aid=6535149]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0096-882X()60L.663[aid=6535149]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0277-9536()47L.1181[aid=131713]http://www.ingentaselect.com/rpsv/cgi-bin/linker?ext=a&reqidx=0277-9536()4