Embed Size (px)
Citation preview
Page 1 of 11
Patient Safety and Spanish in the Pharmacy 1
Learning Objectives: 2
After completing this lesson, the pharmacist will be able to: 3
Discuss Hispanic population demographics in Ohio. 4
Discuss the need for language assistance of Limited English Proficiency [LEP] patient 5
populations. 6
Discuss federal standards affecting service of LEP patient populations. 7
Discuss enforcement of federal standards for service of LEP patient populations. 8
Discuss Ohio Board of Pharmacy standards for patient counseling and record keeping. 9
Introduction 10
Patient safety is one of the chief aims of the pharmacists and pharmacy law. Medicine must be 11
safe and effective before it can be prescribed and dispensed. Pharmacists are trained to advise 12
patients in the safe use of medications. Healthcare professionals detect and report incidents of 13
unsafe practices and thereby enhance patient care. 14
Effective communication is a critical part of patient safety. If patients don’t understand how to 15
safety use medication, the results can be disastrous. If pharmacists do not properly communicate 16
with patients, malpractice and administrative disciplinary actions can occur. In particularly 17
serious cases, civil and even criminal actions can arise. Communication between the pharmacist 18
and professional colleagues is likewise important. 19
When communication involves persons speaking differing languages, patient safety can be 20
compromised. Mis-hearing, mis-speaking, and misinterpreting can put patients at serious risk of 21
drug misadventures. LEP affects millions of persons in the United States. This lesson will focus 22
primarily on the interaction between the pharmacist and Spanish-speaking LEP patients. 23
Pharmacy Services Needs for LEP Patients 24
Studies have shown that communicating in a patient’s preferred language, such as Spanish, 25
improves accuracy of medication history collection. Luong-Schwab K, Gillian L, Floyd RA, et 26
al. Bilingual pharmacy technician medication reconciliation at hospital admission reduces 27
omissions of prescribed medications. Presented at ASHP Midyear Clinical Meeting. Anaheim, 28
CA; 2006 Dec 3. 29
Fourteen percent of adults (30 million people) have below-basic health literacy, meaning they are 30
either nonliterate in English or can perform only the most simple and concrete health literacy 31
tasks, such as circling the date of a medical appointment on an appointment slip. Kutner M, 32
Greenberg E, Jin Y, et al. The Health Literacy of America’s Adults: Results from the 2003 33
National Assessment of Adult Literacy. Washington, DC: National Center for Education 34
Statistics; 2006. These patients are clearly able to benefit from meaningful interactions with 35
their pharmacist. 36
Page 2 of 11
Providing a patient with a prescription product accurately labelled and understandable by the 1
patient is critical to assure patient safety and medication adherence. Culturally appropriate 2
educational programs are needed to help all patient, including Hispanic patients, adhere to 3
treatment plans. Hall E, Lee SY, Clark PC, Perilla J. Social Ecology of Adherence to 4
Hypertension Treatment in Latino Migrant and Seasonal Farmworkers. J Transcult Nurs May 5
22, 2014; 1043659614524788. 6
When the pharmacy serves a large Spanish-speaking population and receives federal funds, such 7
as Medicare Part D funds, the pharmacy should be able to provide Spanish language assistance. 8
There is no bright line number or percentage of patients being served to trigger this language 9
requirement. See Office of Minority Health; National Standards on Culturally and Linguistically 10
Appropriate Services (CLAS) in Health Care, Federal Register, Vol. 65, No. 247, Friday, 11
December 22, 2000 Pages 80865 – 80879; and National Standards for Culturally and 12
Linguistically Appropriate Services in Health Care. U.S. Department of Health and Human 13
Services. Office of Minority Health. Washington, D.C.: 2001. Available at: 14
minorityhealth.hhs.gov/assets/pdf/checked/finalreport.pdf. Accessed: April 30, 2015. 15
Demographics 16
Over 7,100 different languages are spoken world-wide. See www.ethnologue.com. The most 17
common language is Chinese, with Spanish second and English third. According to an analysis 18
of the United States 2010 Census, of the nearly 300 million residents, over 60 million people 19
(21% of the population) spoke a language other than English at home. In Ohio, over 700,000 20
Hispanic persons spoke Spanish at home. About fifteen percent (15%) of the 700,000 spoke 21
English not well or not at all. 22
In Ohio, Hispanics increased by an estimated 32,263 residents between 2010 and 2013, about 23
nine percent (9%). The Columbus Dispatch, Thursday June 26, 2014. In 2011, the total 24
Hispanic population in Ohio was 362,000, with about half speaking Spanish at home. 25
www.pewhispanic.org/states/state/oh/. By county, Sandusky, Defiance, and Lorain have the 26
greatest percentages, about nine percent (9%). By city, Cleveland (10%), Lorain (25%), and 27
Painesville (22%) are the largest locations. Pharmacists serving patients here are in unique 28
positions to impact Hispanic populations which may require additional language expertise. 29
As pharmacists, we strive to ensure our patients receive prescriptions labelled clearly to enable 30
proper medication use. Pharmacists cringe when given the “use as directed” prescription. 31
Exactly how does a patient safely follow such vague “directions” on a label? How much 32
medication should the patient receive for treatment lasting thirty days or ninety days? 33
How should the pharmacist safely and properly label medications knowing the patient has LEP? 34
While the discussion here will focus primarily on the Spanish-speaking population in Ohio and 35
elsewhere, it could just as easily apply to other LEP populations. As we will see, it is not 36
accurate to conclude that “there is no law” which could impose requirements for a pharmacy or 37
pharmacist to perform duties in a language other than English. Indeed, both Ohio law and 38
Federal law speak to the matter. 39
Page 3 of 11
Language Accommodation Research 1
The Hispanic population has been the focus of some research. See The Hispanic Diabetes 2
Management Program, Impact of Community Pharmacists on Clinical Outcomes, J. Am. Pharm. 3
Assoc. 2011;51:623-626. Research demonstrates the impact that community pharmacists have in 4
improving clinical outcomes in Hispanic patients with diabetes. Patients with higher baseline 5
hemoglobin A1c test values were most likely to show improvement. The Asheville Project: 6
Long-term Clinical and Economic Outcomes of a Community Pharmacy Diabetes Care Program. 7
J. Am. Pharm. Assoc. 2003;43:173–184. A pharmacy school Spanish language initiative 8
resulted in increased Spanish language and cultural competence among students and new 9
graduates. A Spanish Language and Culture Initiative for a Doctor of Pharmacy Curriculum, 10
Am J Pharm Educ. 2011;75:1-8. 11
To assist an LEP patient, the pharmacist might be tempted to use an on-line language translator 12
or other automated software-assisted tool. Unfortunately, these tools have been found to be 13
somewhat unsafe and unreliable. Combining the results of fourteen different computer programs 14
to generate a label in Spanish, one study found an overall error rate of fifty percent (50%). 15
Accuracy of Computer-Generated, Spanish-Language Medicine Labels. Pediatrics 16
2010;125:960-965. doi:10.1542/peds.2009-2530. Translation websites such as Google Translate 17
or Babblefish are often unable to put words into a meaningful context (e.g. “until gone” 18
translated into Spanish equivalent of “until the past.”) Further, some automated pharmacy 19
translation programs make such errors as translating the word “once” (meaning “one time”) into 20
the number “eleven” (Spanish translation of the letters o-n-c-e). Pharmacists can appreciate the 21
safety risk of the numerical difference between “eleven” and “one” appearing on the label of a 22
prescription. 23
In New York City, less than forty percent (40%) of 200 randomly selected pharmacies translated 24
prescription labels every day, even though those pharmacies served clients with LEP on a daily 25
basis. Access to multilingual medication instructions at New York City pharmacies. J Urban 26
Health. 2007;84:742–754. In a study of 764 pharmacies in Colorado, Georgia, North Carolina, 27
and Texas, one third (34.9%) of pharmacies reported being unable to provide any translated 28
instructions for medicines. Availability of Spanish prescription labels: a multi-state pharmacy 29
survey. Med Care. 2009;47:707–710. 30
Recognition of Spanish in Ohio Codified Law 31
Ohio law recognizes the utility of Spanish translation in a number of areas. Certain printed 32
materials must include printing in Spanish. Posters directed to human trafficking must be 33
displayed in Spanish, and possibly other languages. See OAC 4713-1-14. The International 34
Certification and Reciprocity Consortium alcohol and drug counselor (ACD) examination is 35
available in Spanish. See OAC 4758-4-01 (B) (5). The Ohio Department of Health is required 36
to publish certain information pertaining to abortion in English and in Spanish. See ORC 37
2317.56 (C). Ohio has an Office of Hispanic-Latino affairs to advise on matters of importance in 38
Ohio. See ORC 121.33. Spanish is also a recognized language for the Ohio driver's license 39
exam. 40
Page 4 of 11
Ohio State Board of Pharmacy – OAC Provisions 1
The Board provides counseling standards for pharmacists and patients, not just those speaking 2
English. Neither the words “Spanish” nor “English” appear in the Ohio pharmacy regulations – 3
other than the requirement by foreign pharmacy school graduates to pass an English-proficiency 4
exam. No particular language is included or excluded. 5
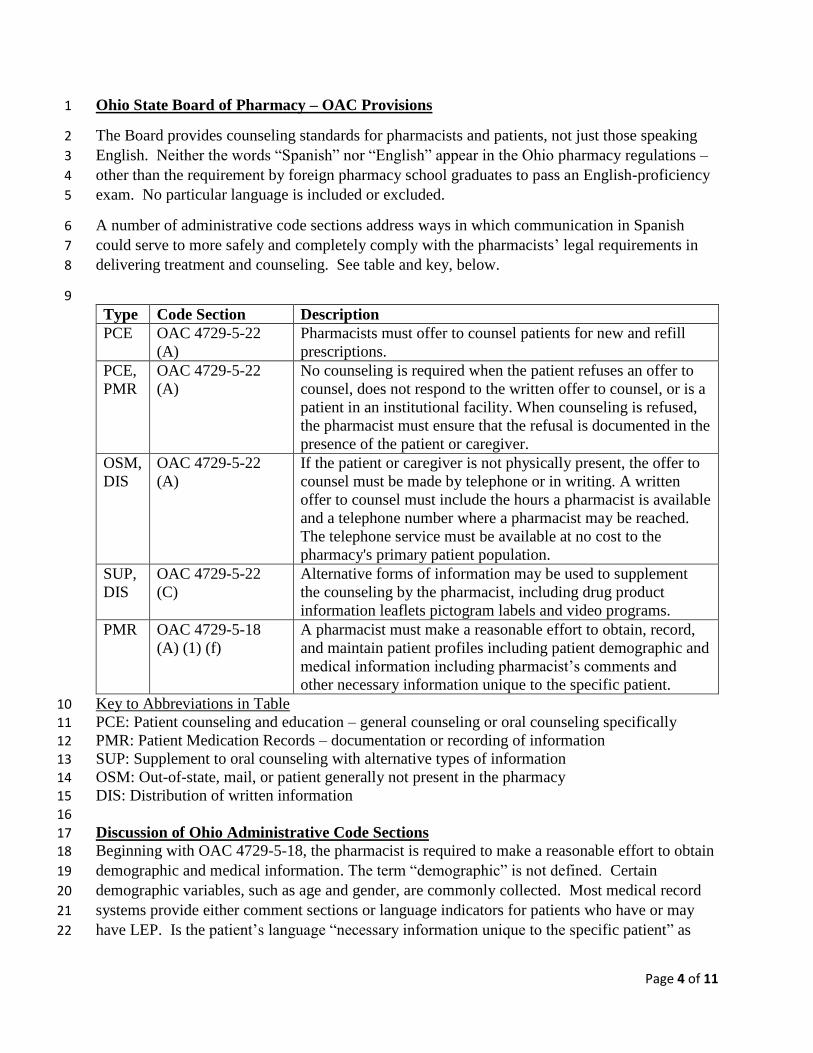
A number of administrative code sections address ways in which communication in Spanish 6
could serve to more safely and completely comply with the pharmacists’ legal requirements in 7
delivering treatment and counseling. See table and key, below. 8
9
Type Code Section Description
PCE OAC 4729-5-22
(A)
Pharmacists must offer to counsel patients for new and refill
prescriptions.
PCE,
PMR
OAC 4729-5-22
(A)
No counseling is required when the patient refuses an offer to
counsel, does not respond to the written offer to counsel, or is a
patient in an institutional facility. When counseling is refused,
the pharmacist must ensure that the refusal is documented in the
presence of the patient or caregiver.
OSM,
DIS
OAC 4729-5-22
(A)
If the patient or caregiver is not physically present, the offer to
counsel must be made by telephone or in writing. A written
offer to counsel must include the hours a pharmacist is available
and a telephone number where a pharmacist may be reached.
The telephone service must be available at no cost to the
pharmacy's primary patient population.
SUP,
DIS
OAC 4729-5-22
(C)
Alternative forms of information may be used to supplement
the counseling by the pharmacist, including drug product
information leaflets pictogram labels and video programs.
PMR OAC 4729-5-18
(A) (1) (f)
A pharmacist must make a reasonable effort to obtain, record,
and maintain patient profiles including patient demographic and
medical information including pharmacist’s comments and
other necessary information unique to the specific patient.
Key to Abbreviations in Table 10
PCE: Patient counseling and education – general counseling or oral counseling specifically 11 PMR: Patient Medication Records – documentation or recording of information 12 SUP: Supplement to oral counseling with alternative types of information 13 OSM: Out-of-state, mail, or patient generally not present in the pharmacy 14 DIS: Distribution of written information 15
16
Discussion of Ohio Administrative Code Sections 17 Beginning with OAC 4729-5-18, the pharmacist is required to make a reasonable effort to obtain 18
demographic and medical information. The term “demographic” is not defined. Certain 19
demographic variables, such as age and gender, are commonly collected. Most medical record 20
systems provide either comment sections or language indicators for patients who have or may 21
have LEP. Is the patient’s language “necessary information unique to the specific patient” as 22
Page 5 of 11
mentioned in OAC 4729-5-18? If so, the pharmacist must make a reasonable effort to obtain and 1
record that language information. 2
OAC 4729-5-22 (A) is a key section to consider for the pharmacists’ (or supervised pharmacy 3
interns’) counseling requirements. The counseling requirement is for an “offer” to counsel. The 4
patient can refuse the offer, which must be recorded. Can an LEP patient truly “refuse” 5
counseling if the patient’s English proficiency is so limited as to not understand whether and 6
what type of pharmacist counseling is being offered? Does the patient understand that 7
counseling is being offered? All states require some attempt to provide oral counseling and 8
distribution of written materials. To comply with these requirements, pharmacists must 9
effectively communicate with all of their patients, not only patients who are well-educated and 10
fluent in English. 11
Recent Publication by Ohio State Board of Pharmacy 12 Spanish LEP and patient safety issues are of interest not only in states close to Mexico, Puerto 13
Rico, and Cuba. The August 2014 edition of the Ohio State Board of Pharmacy Newsletter 14
described a dosing error by both a pharmacist and a nurse. The case involved an adult dose of 15
carbamazepine oral tablets given to a 4-year-old child. Apparently the adult and child patient 16
had similar names. Of significance was that the child’s parents apparently had a very “limited 17
understanding of English,” and were unable to provide an adequate medical history (in English) 18
that may have prevented the error. As a result, the treatment environment was unsafe. 19
While the parents may not be to blame, a more successful exchange between the parents and the 20
healthcare team may have increased safety and prevented the error. The proverbial “red flag” 21
might have been raised if the pharmacist and nurse noticed the patient had no history of seizures. 22
Both professionals should have noticed that chewable tablets or suspension were not being 23
prescribed, dispensed, and administered for the young child – and further investigated the 24
situation. In hindsight, an interpreter or Spanish-speaking pharmacist or nurse could have 25
greatly reduced the possibility of error. 26
Federal Standards 27
Any individual or entity that receives federal funds, including pharmacies accepting federal 28
funds via Medicare Part-D, must comply with Title VI of the Civil Rights Act of 1964. Title VI 29
prohibits discrimination and ensures that federal money is not used to support health care 30
providers who discriminate on the basis of race, color or national origin. See 42 U.S.C. § 2000d. 31
The federal Department of Health and Human Services (HHS) and the courts have applied this 32
statute to protect national origin minorities who do not speak English well. Lau v. Nichols, 414 33
U.S. 563 (1974), 45 C.F.R. § 80 app. A, Executive Order 13166, 65 Fed. Reg. 50121 (Aug. 11, 34
2000). Pharmacies that receive federal funds must take “reasonable steps to ensure that LEP 35
individuals have meaningful access to their programs and services.” See Federal Laws and 36
Policies to Ensure Access to Health Care Services for People with Limited English Proficiency at 37
www.healthlaw.org. 38
Under Title VI of the Civil Rights Act of 1964 and implementing regulations, failure of a 39
recipient of federal financial assistance to take reasonable steps to provide meaningful access by 40
Page 6 of 11
persons with LEP to covered programs and activities could violate Title VI. See The U.S. 1
Department of Health and Human Services 2013 Language Access Plan - February 26, 2013. 2
www.hhs.gov/open/pres-actions/2013-hhs-language-access-plan.pdf. Accessed: April 30, 2015 3
Where Do Federal Agencies Draw the Line? 4
An objection some pharmacies raise when facing obligations to LEP patients, is that complying 5
with federal rules is too complicated and too expensive. Does filling one prescription for one 6
patient who speaks Vietnamese mean a pharmacist has to become fluent in Vietnamese? Exactly 7
which written materials need to be translated – and into which foreign language(s)? 8
The Department of Health and Human Services (HHS) has developed guidelines for compliance. 9
See 68 Fed. Reg. 47311 (Aug. 8, 2003.) A wealth of LEP information and resources can be 10
found at www.lep.gov. The HHS Office for Civil Rights (OCR) enforces these federal 11
standards. If you or your patients need help filing a complaint or have a question you can email 12
OCR at [email protected]. See http://www.hhs.gov/ocr/office/index.html. 13
A 2009 civil rights complaint filed against mail-order pharmacy Medco alleged that Medco 14
failed to provide LEP members with meaningful access to mail-order pharmacy services and 15
other pharmacy benefit management services. As a result of the federal action, Medco agreed to 16
address the issues to strengthen its provision of language assistance services to LEP members. 17
There is no doubt that HHS standards have been, and will be, enforced for LEP patients 18
receiving prescription drugs. See www.hhs.gov/ocr/civilrights/activities/examples/LEP/. HHS 19
balances the following four factors to ensure meaningful access to pharmacy services: 20
1. The number or proportion of LEP persons who would not receive the HHS pharmacy 21
services absent efforts to remove language barriers; 22
2. The frequency and number of contacts by LEP persons with HHS services; 23
3. The nature and importance of pharmacy services provided by HHS to people's lives; and 24
4. The resources available to the HHS (including cost-benefit analysis) to provide services to 25
LEP persons. 26
In examining these four factors, we notice there is no specific “threshold” number or percentage 27
of LEP persons being served for a possible violation to occur. As the number or proportion 28
increases, the more likely LEP patients are being underserved due to language barriers. 29
The frequency and number of contacts between the LEP patient and their pharmacy are generally 30
quite high. The patient is generally going to have contact with a pharmacist more frequently 31
than a physician or hospital. The “contacts” also include telephonic contacts, such as calls 32
regarding refills, adherence, or adverse drug reactions. It has been discussed at length elsewhere 33
that the pharmacist is the most accessible healthcare professional. 34
Steps to Consider Now 35
A number of practical approaches, individually or in combination, can enhance patient safety and 36
assist the pharmacy to meet federal LEP requirements. 37
Page 7 of 11
1. BYOI – Bring your own interpreter: Of course, LEP patients can rely on family or 1
friends to translate materials from the pharmacy. The risk is that such well-meaning 2
helpers are often untrained in a medical profession and may not understand medical terms 3
or translate accurately. Also, the patient’s privacy is clearly compromised to some 4
degree by involving a third party. Further, the patient may be very uncomfortable 5
discussing some pharmacy topics in the presence of a friend or family member. Consider 6
a young woman needing to rely on her father to explain the proper use of birth control 7
methods. Consider a man relying on his daughter to explain the possible effect of 8
prolonged erection or priapism while taking sildenafil. 9
2. Supply an employee interpreter: It stands to reason that if a pharmacy finds itself awash 10
in an identified LEP population, hiring one or more pharmacy technicians who speak the 11
language might make a lot of sense. Consider a hospital or pharmacy located in 12
Minnesota or California amidst a large population of Hmong patients. Johnson, Sharon 13
K. Hmong health beliefs and experiences in the western health care system. J Transcult 14
Nurs 13.2 (2002): 126-132. Providing a Hmong pharmacist or pharmacy technician in 15
these areas would be a tremendous resource for the healthcare team. 16
3. Rely on colleagues: If the local physician’s receptionist speaks the Hmong language, the 17
receptionist might be willing to help with medication counseling, provided it does not 18
interfere with her own employment duties. Of course, some sort of coordination between 19
the pharmacy and the language resource is advisable to avoid conflicts which may 20
produce frustration. 21
4. Have the pharmacist or technician learn and use the foreign language: Learning a foreign 22
language while practicing pharmacy can raise scheduling problems and be time 23
consuming. Becoming fluent requires study and practice. While such a goal is laudable, 24
it is likely not going to be a first line approach to assisting LEP populations. 25
5. Have the patient learn and use English: Clearly, learning a new language is easier for 26
younger patients. For adults, this is likely not going to be a first line approach to 27
assisting LEP populations. Where there is a willing student, regardless of age, there are 28
usually a number of community resources available to learn English as a second language 29
(ESL). 30
6. Commercial on-demand translation services: When a pharmacy or hospital knows it will 31
have a daily and ongoing demand for translating services, these services may be provided 32
in-house or may be outsourced. For example, the Cleveland Clinic serves a number of 33
patients speaking Arabic, and uses three-way conference calls to communicate between 34
English providers and Arabic patients. Placing the term “translation services” in your 35
favorite search engine will return a list of literally hundreds of available telephonic 36
translation services. Computer language translators should be used with caution, if at all. 37
7. Boards of Pharmacy can adopt standards: California Senate Bill SB 472 was signed by 38
Governor Arnold Schwarzenegger on October 11, 2007. The Bill required that by January 39
1, 2011, California adopt a standardized prescription drug label. Specifically, the Bill 40
tasked the California State Board of Pharmacy to design such a standardized, patient-41
centered, prescription drug label and mandate its use by state pharmacies on all 42
prescription medication dispensed in California. The Bill required the Board of 43
Page 8 of 11
Pharmacy to specifically consider the needs of patients with LEP in designing the new 1
standardized drug label. The Medication Label Subcommittee of the California Board of 2
Pharmacy is in the process of implementing SB 472. Under California regulations, 3
pharmacies must at a minimum provide interpreting services to all LEP patients. This 4
may be done by pharmacy staff members or through telephone interpreting. This must be 5
available for all hours that the pharmacy is open. 6
8. Non-text communication aids: Drawings or other visual aids may be used. A model or 7
drawing of a timeline or clock with movable hands may effectively communicate dose 8
timing for some patients. Where doses change daily, such as doses of warfarin and 9
levothyroxine, calendars may offer assistance. 10
9. Use of products and props: When explaining something that is inherently spatial, a prop 11
can be worth a thousand words. For example, explaining how to give an injection can be 12
done more simply and effectively with a syringe and needle than text alone. 13
Conclusion 14
Breakdowns in communication between the pharmacist and patient can lead to serious problems 15
and result in unsafe use of medication. Introducing a language barrier only increases safety 16
concerns. Though not all pharmacists need to become fluent in a foreign language, they do have 17
to be mindful of applicable administrative and federal standards. It is reasonable to expect that 18
pharmacists will increasingly have interactions and opportunities to serve LEP patients. 19
Immigration patterns, and the prospect of communicating via the internet with patients from 20
different cultures, may create new safety, compliance and liability concerns. 21
Page 9 of 11
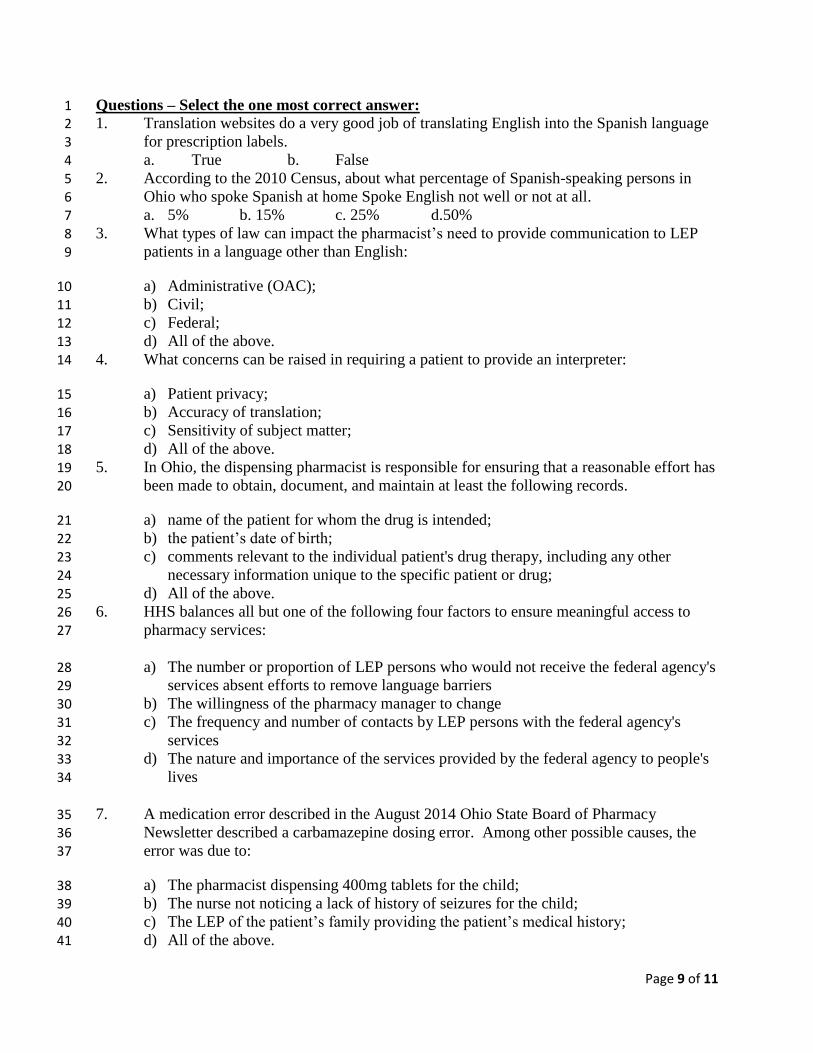
Questions – Select the one most correct answer: 1 1. Translation websites do a very good job of translating English into the Spanish language 2
for prescription labels. 3 a. True b. False 4
2. According to the 2010 Census, about what percentage of Spanish-speaking persons in 5 Ohio who spoke Spanish at home Spoke English not well or not at all. 6 a. 5% b. 15% c. 25% d.50% 7
3. What types of law can impact the pharmacist’s need to provide communication to LEP 8 patients in a language other than English: 9
a) Administrative (OAC); 10 b) Civil; 11 c) Federal; 12
d) All of the above. 13 4. What concerns can be raised in requiring a patient to provide an interpreter: 14
a) Patient privacy; 15
b) Accuracy of translation; 16 c) Sensitivity of subject matter; 17
d) All of the above. 18 5. In Ohio, the dispensing pharmacist is responsible for ensuring that a reasonable effort has 19
been made to obtain, document, and maintain at least the following records. 20
a) name of the patient for whom the drug is intended; 21 b) the patient’s date of birth; 22
c) comments relevant to the individual patient's drug therapy, including any other 23
necessary information unique to the specific patient or drug; 24
d) All of the above. 25 6. HHS balances all but one of the following four factors to ensure meaningful access to 26
pharmacy services: 27
a) The number or proportion of LEP persons who would not receive the federal agency's 28 services absent efforts to remove language barriers 29
b) The willingness of the pharmacy manager to change 30 c) The frequency and number of contacts by LEP persons with the federal agency's 31
services 32
d) The nature and importance of the services provided by the federal agency to people's 33 lives 34
7. A medication error described in the August 2014 Ohio State Board of Pharmacy 35 Newsletter described a carbamazepine dosing error. Among other possible causes, the 36
error was due to: 37
a) The pharmacist dispensing 400mg tablets for the child; 38 b) The nurse not noticing a lack of history of seizures for the child; 39 c) The LEP of the patient’s family providing the patient’s medical history; 40 d) All of the above. 41
Page 10 of 11
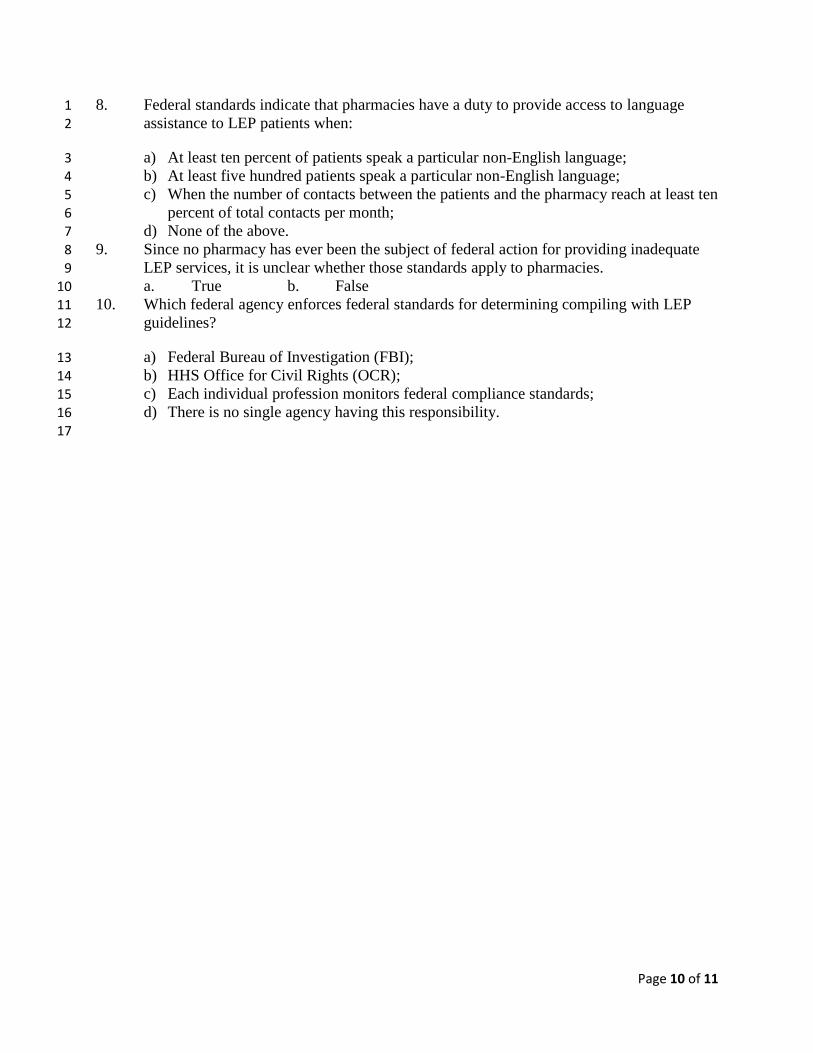
8. Federal standards indicate that pharmacies have a duty to provide access to language 1
assistance to LEP patients when: 2
a) At least ten percent of patients speak a particular non-English language; 3 b) At least five hundred patients speak a particular non-English language; 4
c) When the number of contacts between the patients and the pharmacy reach at least ten 5 percent of total contacts per month; 6
d) None of the above. 7 9. Since no pharmacy has ever been the subject of federal action for providing inadequate 8
LEP services, it is unclear whether those standards apply to pharmacies. 9
a. True b. False 10 10. Which federal agency enforces federal standards for determining compiling with LEP 11
guidelines? 12
a) Federal Bureau of Investigation (FBI); 13 b) HHS Office for Civil Rights (OCR); 14 c) Each individual profession monitors federal compliance standards; 15
d) There is no single agency having this responsibility. 16 17
Page 11 of 11
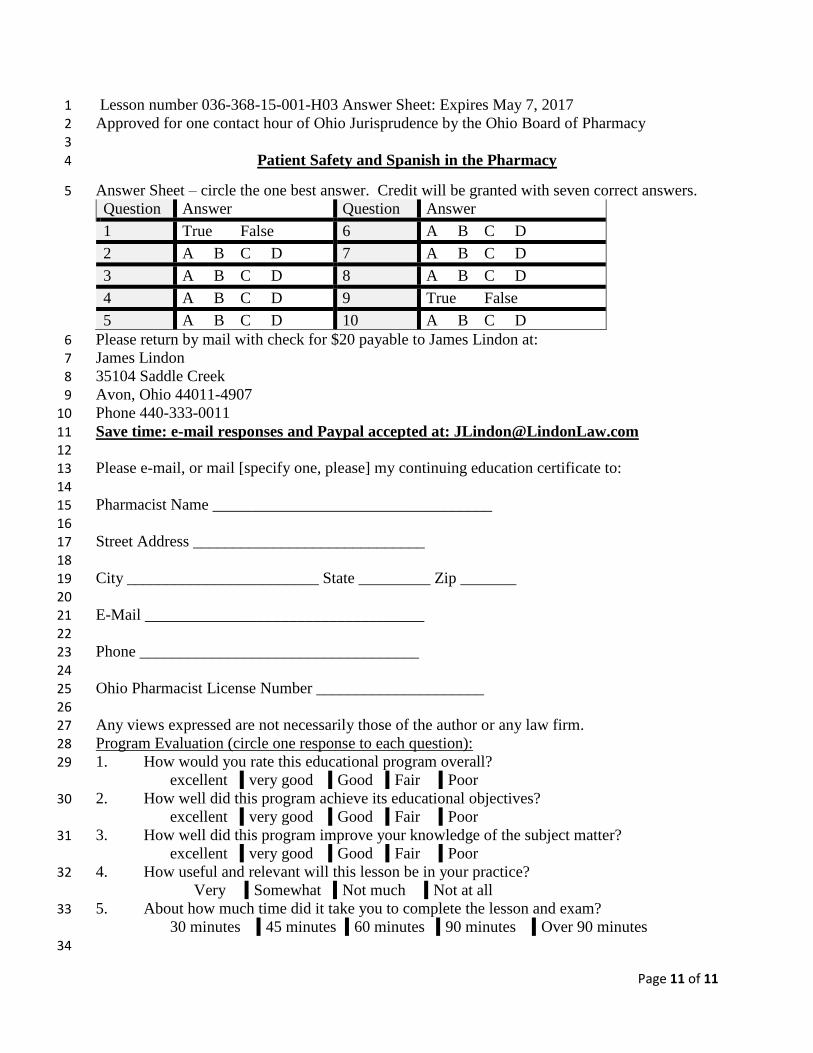
Lesson number 036-368-15-001-H03 Answer Sheet: Expires May 7, 2017 1
Approved for one contact hour of Ohio Jurisprudence by the Ohio Board of Pharmacy 2 3
Patient Safety and Spanish in the Pharmacy 4
Answer Sheet – circle the one best answer. Credit will be granted with seven correct answers. 5 Question Answer Question Answer
1 True False 6 A B C D
2 A B C D 7 A B C D
3 A B C D 8 A B C D
4 A B C D 9 True False
5 A B C D 10 A B C D
Please return by mail with check for $20 payable to James Lindon at: 6 James Lindon 7
35104 Saddle Creek 8 Avon, Ohio 44011-4907 9
Phone 440-333-0011 10
Save time: e-mail responses and Paypal accepted at: [email protected] 11 12
Please e-mail, or mail [specify one, please] my continuing education certificate to: 13 14
Pharmacist Name ___________________________________ 15 16 Street Address _____________________________ 17
18
City ________________________ State _________ Zip _______ 19 20 E-Mail ___________________________________ 21
22 Phone ___________________________________ 23
24 Ohio Pharmacist License Number _____________________ 25
26 Any views expressed are not necessarily those of the author or any law firm. 27 Program Evaluation (circle one response to each question): 28 1. How would you rate this educational program overall? 29
excellent very good Good Fair Poor
2. How well did this program achieve its educational objectives? 30 excellent very good Good Fair Poor
3. How well did this program improve your knowledge of the subject matter? 31 excellent very good Good Fair Poor
4. How useful and relevant will this lesson be in your practice? 32 Very Somewhat Not much Not at all
5. About how much time did it take you to complete the lesson and exam? 33 30 minutes 45 minutes 60 minutes 90 minutes Over 90 minutes
34





























