Embed Size (px)
DESCRIPTION
FACTS ABOUT LEPROSY
Citation preview

Leprosy is an infectious disease that causes severe, disfiguring skinsores and nerve
damage in the arms and legs. The disease has been around since ancient times, often
surrounded by terrifying, negative stigmas and tales of leprosy patients being shunned
as outcasts. Outbreaks of leprosy have affected, and panicked, people on every
continent. The oldest civilizations of China, Egypt, and India feared leprosy was an
incurable, mutilating, and contagious disease.
However, leprosy is actually not that contagious. You can catch it only if you come into
close and repeated contact with nose and mouth droplets from someone with untreated
leprosy. Children are more likely to get leprosy than adults.
Today, about 180,000 people worldwide are infected with leprosy, according to the
World Health Organization, most of them in Africa and Asia. About 200 people are
diagnosed with leprosy in the U.S. every year, mostly in the South, California, Hawaii,
and some U.S. territories.
What Causes Leprosy?
Leprosy is caused by a slow-growing type of bacteria calledMycobacterium leprae (M.
leprae). Leprosy is also known as Hansen's disease, after the scientist who
discovered M. leprae in 1873.
What Are the Symptoms of Leprosy?
Leprosy primarily affects the skin and the nerves outside the brain and spinal cord,
called the peripheral nerves. It may also strike the eyes and the thin tissue lining the
inside of the nose.
The main symptom of leprosy is disfiguring skin sores, lumps, or bumps that do not go
away after several weeks or months. The skin sores are pale-colored.
Nerve damage can lead to:
Loss of feeling in the arms and legs
Muscle weakness
It usually takes about 3 to 5 years for symptoms to appear after coming into contact with
the leprosy-causing bacteria. Some people do not develop symptoms until 20 years
later. The time between contact with the bacteria and the appearance of symptoms is
called the incubation period. Leprosy's long incubation period makes it very difficult for
doctors to determine when and where a person with leprosy got infected.

Forms of Leprosy
Leprosy is defined by the number and type of skin sores you have. Specific symptoms
and treatment depend on the type of leprosy you have. The types are:
Leprosy Overview(continued)In this article
What Causes Leprosy?
What Are the Symptoms of Leprosy?
Forms of Leprosy
How Is Leprosy Diagnosed?
How Is Leprosy Treated?
Leprosy Complications
Forms of Leprosy continued...
Tuberculoid. A mild, less severe form of leprosy. People with this type have only one or
a few patches of flat, pale-colored skin (paucibacillary leprosy). The affected area of
skin may feel numb because of nerve damage underneath. Tuberculoid leprosy is less
contagious than other forms.
Lepromatous. A more severe form of the disease. It has widespread skin bumps
and rashes (multibacillary leprosy), numbness, and muscle weakness. The
nose, kidneys, and male reproductive organs may also be affected. It is more
contagious than tuberculoid leprosy.
Borderline. People with this type of leprosy have symptoms of both the tuberculoid and
lepromatous forms.
How Is Leprosy Diagnosed?
If you have a suspicious skin sore, your doctor will remove a small sample of the
abnormal skin and send it to a lab to be examined. This is called a skin biopsy. A skin
smear test may also be done. With paucibacillary leprosy, no bacteria will be detected.
In contrast, bacteria are expected to be found on a skin smear test from a person with
multibacillary leprosy.
How Is Leprosy Treated?

Leprosy can be cured. In the last two decades, more than 14 million people with leprosy
have been cured. The World Health Organization provides free treatment for all people
with leprosy.
Treatment depends on the type of leprosy that you have. Antibiotics are used to treat
the infection. Long-term treatment with two or more antibiotics is recommended, usually
from six months to a year. People with severe leprosy may need to take antibiotics
longer. Antibiotics cannot treat the nerve damage.
Anti-inflammatory drugs are used to control swelling related to leprosy. This may include
steroids, such as prednisone.
Patients with leprosy may also be given thalidomide, a potent medication that
suppresses the body's immune system. It helps treat leprosy skin nodules. Thalidomide
is known to cause severe, life-threatening birth defects and should never be taken
by pregnantwomen.
Leprosy Complications
Without treatment, leprosy can permanently damage your skin, nerves, arms, legs, feet,
and eyes.
Complications of leprosy can include:
Blindness or glaucoma.
Disfiguration of the face (including permanent swelling, bumps, and lumps).
Erectile dysfunction and infertility in men.
Kidney failure.
Muscle weakness that leads to claw-like hands or an inability to flex the feet.
Permanent damage to the inside of the nose, which can lead tonosebleeds and a
chronic, stuffy nose.
Permanent damage to the nerves outside the brain and spinal cord, including those in
the arms, legs, and feet.
Nerve damage can lead to a dangerous loss of feeling. A person with leprosy-related
nerve damage may not feel pain when the hands, legs, or feet are cut, burned, or
otherwise injured.
WebMD Medical Reference
View Article Sources Reviewed by Melinda Ratini, DO, MS on April 23, 2013

© 2013 WebMD, LLC. All rights reserved.
SORCE: http://www.webmd.com/skin-problems-and-treatments/guide/leprosy-symptoms-treatments-history?page=2
LeprosyFrom Wikipedia, the free encyclopedia
For the Biblical term and its varied meanings, see Tzaraath. For other uses, see Leprosy (disambiguation).
Leprosy
A 24-year-old man from Norway, infected with leprosy, 1886.
Classification and external resources
ICD-10 A30
ICD-9 030
OMIM 246300
DiseasesDB 8478

MedlinePlus 001347
eMedicine med/1281 derm/223 neuro/187
NCI Leprosy
Patient UK Leprosy
MeSH D007918
Leprosy / ̍ l ɛ p r ə s i / ,[1] also known as Hansen's disease (HD), is a chronic infection caused by the bacteria Mycobacterium leprae [2] and Mycobacterium lepromatosis.[3] Initially, infections are without symptoms and typically remain this way for 5 to as long as 20 years. [2] Symptoms that develop include granulomas of the nerves,respiratory tract, skin, and eyes.[2] This may result in a lack of ability to feel pain and thus loss of parts of extremities due to repeated injuries. [4] Weakness and poor eyesight may also be present.[4]
The two main types of disease are based on the number of bacteria present: paucibacillary and multibacillary.[4]The two types are differentiated by the number of poorly pigmented, numb skin patches present, with paucibacillary having five or fewer and multibacillary having more than five.[4] The diagnosis is confirmed by findingacid-fast bacilli in a biopsy of the skin or via detecting the DNA by polymerase chain reaction.[4] It occurs more commonly among those living in poverty and is believed to be transmitted by respiratory droplets.[4] It is not very contagious.[4]
Leprosy is curable with treatment.[2] Treatment for paucibacillary leprosy is with the medications dapsone andrifampicin for 6 months.[4] Treatment for multibacillary leprosy consists of rifampicin, dapsone, and clofazimine for 12 months.[4] These treatments are provided for free by the World Health Organization.[2] A number of other antibiotics may also be used.[4] Globally in 2012, the number of chronic cases of leprosy was 189,000 and the number of new cases was 230,000.[2] The number of chronic cases has decreased from some 5.2 million in the 1980s. [2][5][6] Most new cases occur in 16 countries, with India accounting for more than half. [2][4] In the past 20 years, 16 million people worldwide have been cured of leprosy. [2] About 200 cases are reported per year in the United States.[7]
Leprosy has affected humanity for thousands of years. [4] The disease takes its name from the Latin word lepra, which means "scaly", while the term "Hansen's disease" is named after the physician Gerhard Armauer Hansen.[4]Separating people in leper colonies still occurs in countries like India, with more than a thousand;[8] China, with around hundreds;[9] and in Africa.[10] However, most colonies have closed.[10] Leprosy has been associated withsocial stigma for much of history,[2] which remains a barrier to self-reporting and early treatment. World Leprosy Day was started in 1954 to draw awareness to those affected by leprosy.[11]
Contents
[hide]
1 Signs and symptoms 2 Cause
o 2.1 M. leprae o 2.2 Genetics

o 2.3 Risk factors o 2.4 Transmission
3 Pathophysiology 4 Diagnosis
o 4.1 Endemic areas o 4.2 United States o 4.3 Classification
5 Prevention 6 Treatment 7 Epidemiology
o 7.1 Disease burden 8 History
o 8.1 The Bible 9 Society and culture
o 9.1 Treatment cost o 9.2 Stigma in India o 9.3 Notable cases
10 References 11 External links
Signs and symptoms[edit]
Hands deformed by leprosy, 1990, India
Lepers in Tahiti, circa 1895
Leprosy is primarily a granulomatous disease of the peripheral nerves and mucosa of the upper respiratory tract; skin lesions are the primary external sign. [12] Left untreated, leprosy can be progressive, causing permanent damage to the skin, nerves, limbs, and eyes. Contrary to folklore, leprosy does not cause body parts to fall off, although they can become numb or diseased as a result of secondary infections; these occur as a result of the body's defenses being compromised by
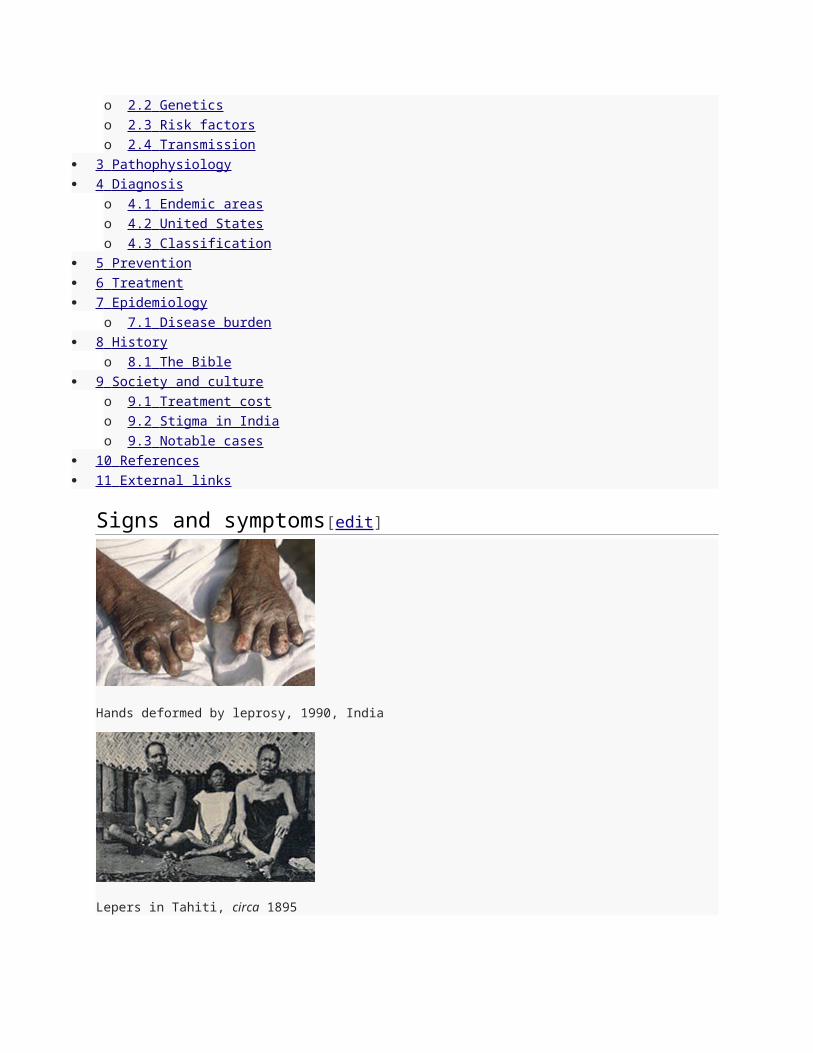
the primary disease.[13][14] Secondary infections, in turn, can result in tissue loss causing fingers and toes to become shortened and deformed, as cartilage is absorbed into the body.[13][14][15]
Cause[edit]
M. leprae[edit]
M. leprae, one of the causative agents of leprosy: As an acid-fastbacterium, M. leprae appears red when
a Ziehl-Neelsen stain is used.
Main article: Mycobacterium leprae
M. leprae and M. lepromatosis are the causative agents of leprosy. M. lepromatosis is a relatively newly identified mycobacterium isolated from a fatal case of diffuse lepromatous leprosy in 2008. [3][12]
An intracellular, acid-fast bacterium, M. leprae is aerobic and rod-shaped, and is surrounded by the waxy cell membrane coating characteristic of the Mycobacterium genus.[16]
Due to extensive loss of genes necessary for independent growth, M. leprae and M. lepromatosis are obligate pathogens, and unculturable in the laboratory, a factor that leads to difficulty in definitively identifying the organism under a strict interpretation of Koch's postulates.[3]
[17] The use of nonculture-based techniques such as molecular genetics has allowed for alternative establishment of causation.
While the causative organisms have to date been impossible to culture in vitro, it has been possible to grow them in animals.
Naturally occurring infection also has been reported in nonhuman primates, including the African chimpanzee, sooty mangabey, and cynomolgus macaque, as well as in armadillos and red squirrels.[18]
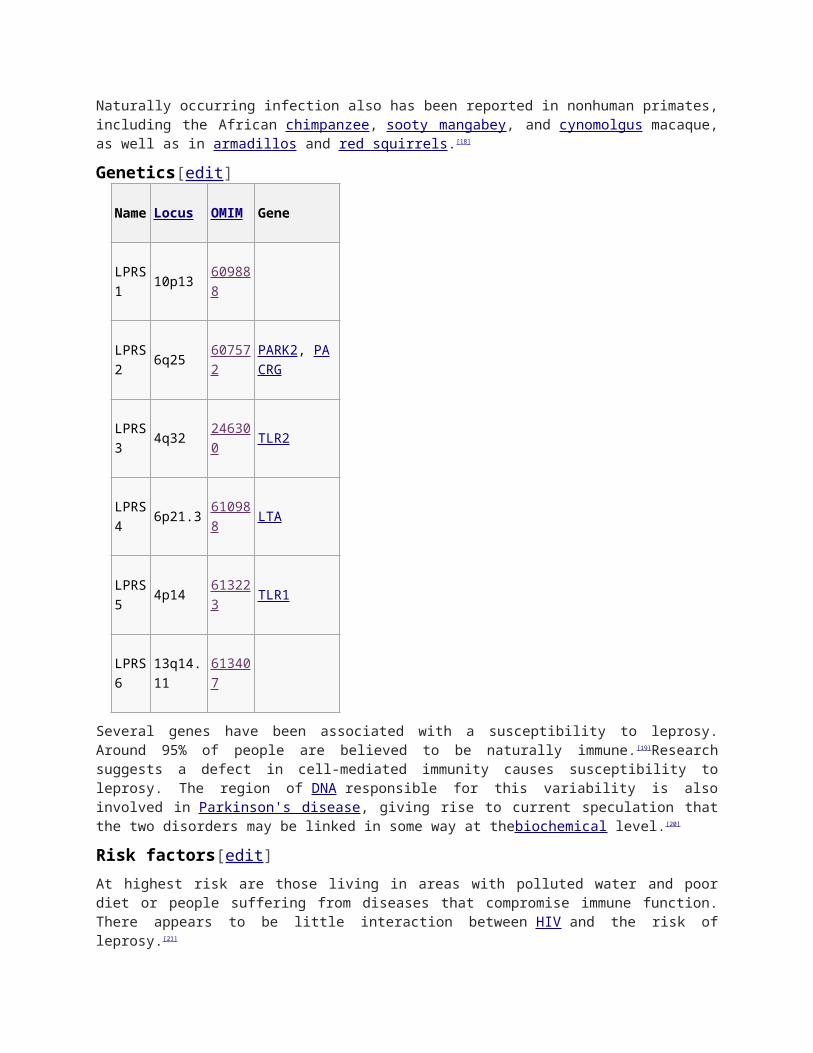
Genetics[edit]
Name
Locus OMIM Gene
LPRS1 10p13 609888
LPRS2 6q25 607572 PARK2, PACRG
LPRS3 4q32 246300 TLR2
LPRS4 6p21.3 610988 LTA
LPRS5 4p14 613223 TLR1
LPRS6 13q14.11 613407
Several genes have been associated with a susceptibility to leprosy. Around 95% of people are believed to be naturally immune.[19]Research suggests a defect in cell-mediated immunity causes susceptibility to leprosy. The region of DNA responsible for this variability is also involved in Parkinson's disease, giving rise to current speculation that the two disorders may be linked in some way at thebiochemical level.[20]
Risk factors[edit]
At highest risk are those living in areas with polluted water and poor diet or people suffering from diseases that compromise immune function. There appears to be little interaction between HIV and the risk of leprosy.[21]
Transmission[edit]
Although the mode of transmission of leprosy remains uncertain, M. leprae is probably spread from person to person in nasal droplets.[6] Leprosy can be transmitted to humans by armadillos.[22]
[23] Leprosy is not known to be either sexually transmitted or highly infectious after treatment. Sufferers are no longer infectious after as few as two weeks of treatment.[19]
Pathophysiology[edit]
The precise mechanism of transmission of leprosy is unknown; however, both prolonged close contact and transmission by nasal droplets are thought to be implicated. [24] In addition to humans, leprosy has been observed in the nine-banded armadillo, (which is among the primary sources of new cases of leprosy in the population of North America), [23] and three species of non-human primates.[25] The bacterium can also be grown in the laboratory by injection into the footpads of mice.[26] Some evidence indicates not all people who are infected with M. leprae develop leprosy, and genetic factors have long been thought to play a role, due to the observation of clustering of leprosy around certain families, and the failure to understand why certain individuals develop lepromatous leprosy while others develop other types of leprosy. [27] Due to genetic factors, an estimated 5% of the population is susceptible to leprosy.[28] This is mostly because the body is naturally immune to the bacteria, and those persons who do become infected experience severe allergic reactions to the disease. However, the role of genetic factors is not entirely clear in determining this clinical expression. In addition, malnutrition and prolonged exposure to infected persons may play a role in development of the overt disease.
The most widely held belief is that the disease is transmitted by contact between infected persons and healthy persons.[29] In general, closeness of contact is related to the dose of infection, which in turn is related to the occurrence of disease. Of the various situations that promote close contact, contact within the household is the only one easily identified, although the incidence among contacts
and the relative risk for them appear to vary considerably in different studies. In incidence studies, infection rates for contacts of lepromatous leprosy have varied from 6.2 per 1000 per year in Cebu, Philippines [30] to 53 per 1000 per year in part of western India to 55.8 per 1000 per year in a part of southern India.[31]
Two exit routes of M. leprae from the human body often described are the skin and the nasal mucosa, although their relative importance is not clear. Lepromatous cases show large numbers of organisms deep in the dermis, but whether they reach the skin surface in sufficient numbers is doubtful.[32]Although reports have been made of acid-fast bacilli being found in the desquamating epithelium (sloughing of superficial layer of skin) of the skin, researchers reported they could not find any acid-fast bacilli in the epidermis, even after examining a very large number of specimens from patients and contacts.[33] Fairly large numbers of M. leprae were found in the superficial keratin layer of the skin of lepromatous leprosy patients, suggesting the organism could exit along with the sebaceous secretions.[34]
The importance of the nasal mucosa was recognized as early as 1898 by Schäffer, in particular that of the ulcerated mucosa.[35] The quantity of bacilli from nasal mucosal lesions in lepromatous leprosy was demonstrated with counts ranging from 10,000 to 10,000,000. [36] The majority of lepromatous patients showed leprosy bacilli in their nasal secretions as collected through blowing the nose.[37] Nasal secretions from lepromatous patients could yield as many as 10 million viable organisms per day.[38]
The entry route of M. leprae into the human body is also not definitively known. The skin and the upper respiratory tract are most likely. While older research dealt with the skin route, recent research has increasingly favored the respiratory route. Experimental transmission of leprosy through aerosols containing M. leprae in immune-suppressed mice was accomplished, suggesting a similar possibility in humans.[39] Successful results have also been reported on experiments with nude mice when M. leprae was introduced into the nasal cavity by topical application. [40] In summary, entry through the respiratory route appears the most probable route, although other routes, particularly broken skin, cannot be ruled out.
In leprosy, both the reference points for measuring the incubation period and the times of infection and onset of disease are difficult to define, the former because of the lack of adequate immunological tools and the latter because of the disease's slow onset. Even so, several investigators have attempted to measure the incubation period for leprosy. The minimum incubation period reported is as short as a few weeks based on the very occasional occurrence of leprosy among young infants.[41] The maximum incubation period reported is as long as 30 years, or over, as observed among war veterans known to have been exposed for short periods in endemic areas, but otherwise living in nonendemic areas. The average incubation period is generally believed to be between three and five years.
SOURCE: http://en.wikipedia.org/wiki/Leprosy
Leprosy (Hansen's disease) facts Leprosy is a slowly developing, progressive disease that damages the skin and nervous
system.
Leprosy is caused by an infection with Mycobacterium leprae or M. lepromatosis bacteria.
Early symptoms begin in cooler areas of the body and include loss of sensation.
Signs of leprosy are painless ulcers, skin lesions of hypopigmented macules (flat, pale areas of
skin), and eye damage (dryness, reduced blinking). Later, large ulcerations, loss of digits, skin
nodules, and facial disfigurement may develop.

The infection is thought to be spread person to person by nasal secretions or droplets. Leprosy
is rarely transmitted from chimpanzees, mangabey monkeys, and nine-banded armadillos to
humans by droplets or direct contact.
Susceptibility to getting leprosy may be due to certain human genes.
Antibiotics are used in the treatment of leprosy.
What is leprosy?Leprosy is a disease caused by the bacteria Mycobacterium leprae, which causes damage to the
skin and the peripheral nervous system. The disease develops slowly (from six months to 40 years!)
and results in skin lesions and deformities, most often affecting the cooler places on the body (for
example, eyes, nose, earlobes, hands, feet, and testicles). The skin lesions and deformities can be
very disfiguring and are the reason that infected individuals historically were considered outcasts in
many cultures. Although human-to-human transmission is the primary source of infection, three
other species can carry and (rarely) transfer M. leprae to humans: chimpanzees, mangabey
monkeys, and nine-banded armadillos. The disease is termed a chronic granulomatous disease,
similar to tuberculosis, because it produces inflammatory nodules (granulomas) in the skin and
nerves over time.
What is the history of leprosy (Hansen's disease)?Unfortunately, the history of leprosy and its interaction with man is one of suffering and
misunderstanding. The newest research suggests that at least as early as 4000 B.C. individuals had
been infected with M. leprae, while the first known written reference to the disease was found on
Egyptian papyrus in about 1550 B.C. The disease was well recognized in ancient China, Egypt, and
India, and there are several references to the disease in the Bible. Because the disease was poorly
understood, very disfiguring, slow to show symptoms, and had no known treatment, many cultures
thought the disease was a curse or punishment from the gods. Consequently, leprosy was left to be
"treated" by priests or holy men, not physicians.
Picture of a person with leprosy (Hansen's disease)

Since the disease often appeared in family members, some people thought it was hereditary; other
people noted that if there was little or no contact with infected individuals, the disease did not infect
others. Consequently, some cultures considered infected people (and occasionally their close
relatives) as "unclean" or as "lepers" and ruled they could not associate with uninfected people.
Often infected people had to wear special clothing and ring bells so uninfected people could avoid
them.
The Romans and the Crusaders brought the disease to Europe, and the Europeans brought it to the
Americas. In 1873, Dr. Hansen discovered bacteria in leprosy lesions, suggesting leprosy was an
infectious disease, not a hereditary disease or a punishment from the gods. However, patients with
the disease were still ostracized by many societies and cared for only at missions by religious
personnel. Patients with leprosy were encouraged or forced to live in seclusion up to the 1940s,
even in the U.S. (for example, the leper colony on Molokai, Hawaii, that was established by a priest,
Father Damien and another colony established at Carville, La.), often because no effective
treatments were available to patients at that time.
Because of Hansen's discovery of M. leprae, efforts were made to find treatments that would stop or
eliminate M. leprae; in the early 1900s to about 1940, oil from Chaulmoogra nuts was used with
questionable efficacy by injecting it into patients' skin. At Carville in 1941, promin, a sulfone drug,
showed efficacy but required many painful injections. Dapsone pills were found to be effective in the
1950s, but soon (1960s-1970s), M. lepraedeveloped resistance to dapsone. Fortunately, drug trials
on the island of Malta in the 1970s showed that a three-drug combination
(dapsone,rifampicin [Rifadin], and clofazimine [Lamprene]) was very effective in killingM. leprae. This
multi-drug treatment (MDT) was recommended by the WHO in 1981 and remains, with minor
changes, the therapy of choice. MDT, however, does not alter the damage done to an individual
by M. lepraebefore MDT is started.
Currently, there are several areas (India, East Timor) of the world where the WHO and other
agencies (for example, the Leprosy Mission) are working to decrease the number of clinical cases of
leprosy and other diseases such as rabies and schistosomiasis that occur in remote regions.
Although researchers hope to eliminate leprosy like smallpox, endemic (meaning prevalent or
embedded in a region) leprosy makes complete eradication unlikely. In the U.S., leprosy has
occurred infrequently but is considered endemic in Texas, Louisiana, Hawaii, and the U.S. Virgin
Islands by some investigators.
Leprosy is often termed "Hansen's disease" by many clinicians in an attempt to have patients forgo
the stigmas attached to being diagnosed with leprosy.
What causes leprosy?Leprosy is caused mainly byMycobacterium leprae, a rod-shaped bacillus that is an obligate
intracellular (only grows inside of certain human and animal cells) bacterium. M. leprae is termed an
"acid fast" bacterium because of its chemical characteristics. When special stains are used for
microscopic analysis, it stains red on a blue background due to mycolic acid content in its cell walls.
The Ziehl-Neelsen stain is an example of the special staining techniques used to view the acid-fast
organisms under the microscope.
Currently, the organisms cannot be cultured on artificial media. The bacteria take an extremely long
time to reproduce inside of cells (about 12-14 days as compared to minutes to hours for most
bacteria). The bacteria grow best at 80.9 F-86 F, so cooler areas of the body tend to develop the
infection. The bacteria grow very well in the body's macrophages (a type of immune system cell) and
Schwann cells (cells that cover and protect nerve axons). M. lepraeis genetically related
to M. tuberculosis (the type of bacteria that cause tuberculosis) and other mycobacteria that infect
humans. As with malaria, patients with leprosy produce anti-endothelial antibodies (antibodies
against the lining tissues of blood vessels), but the role of these antibodies in these diseases is still
under investigation.
In 2009, investigators discovered a new Mycobacterium species, M. lepromatosis, which causes
diffuse disease (lepromatous leprosy). This new species (determined by genetic analysis) was found
in patients located in Mexico and the Caribbean islands.
What are the risk factors for leprosy?Comment on thisShare Your Story
People at highest risk are those who live in the areas where leprosy is endemic (parts of India,
China, Japan, Nepal, Egypt, and other areas) and especially those people in constant physical
contact with infected people. In addition, there is some evidence that genetic defects in the immune
system may cause certain people to be more likely to become infected (region q25 on chromosome
6). Additionally, people who handle certain animals that are known to carry the bacteria (for
example, armadillos, African chimpanzee, sooty mangabey, and cynomolgus macaque) are at risk of
getting the bacteria from the animals, especially if they do not wear gloves while handling the
animals.
What are leprosy symptoms and signs?Comment on thisRead 1 Comment Share Your Story
Unfortunately, the early signs and symptoms of leprosy are very subtle and occur slowly (usually
over years). The symptoms are similar to those that may occur with syphilis, tetanus,
andleptospirosis. Numbness and loss of temperature sensation are some of the first symptoms that
patients experience. As the disease progresses, the sensations of touch, then pain, and eventually
deep pressure are decreased or lost. Signs that occur, such as relatively painless ulcers, skin
lesions of hypopigmented macules (flat, pale areas of skin), and eye damage (dryness, reduced
blinking) are experienced before the large ulcerations, loss of digits, and facial disfigurement
develop. This long-term developing sequence of events begins and continues on the cooler areas of
the body (for example, hands, feet, face, and knees).
Are there different forms (classifications) of leprosy?There are multiple forms of leprosy described in the literature. The forms of leprosy are based on the
person's immune response to M. leprae. A good immune response can produce the so-called
tuberculoid form of the disease, with limited skin lesions and some asymmetric nerve involvement. A

poor immune response can result in the lepromatous form, characterized by extensive skin and
symmetric nerve involvement. Some patients may have aspects of both forms. Currently, two
classification systems exist in the medical literature: the WHO system and the Ridley-Jopling
system. The Ridley-Jopling system is composed of six forms or classifications, listed below
according to increasing severity of symptoms:
Indeterminate leprosy: a few hypopigmented macules; can heal spontaneously, this form
persists or advances to other forms
Tuberculoid leprosy: a few hypopigmented macules, some are large and some become
anesthetic (lose pain sensation); some neural involvement in which nerves become enlarged;
spontaneous resolution in a few years, persists or advances to other forms
Borderline tuberculoid leprosy: lesions like tuberculoid leprosy but smaller and more numerous
with less nerve enlargement; this form may persist, revert to tuberculoid leprosy, or advance to
other forms
Mid-borderline leprosy: many reddish plaques that are asymmetrically distributed, moderately
anesthetic, with regional adenopathy (swollen lymph nodes); the form may persist, regress to
another form, or progress
Borderline lepromatous leprosy: many skin lesions with macules (flat lesions) papules (raised
bumps), plaques, and nodules, sometimes with or without anesthesia; the form may persist,
regress or progress to lepromatous leprosy
Lepromatous leprosy: Early lesions are pale macules (flat areas) that are diffuse and
symmetric; later many M. leprae organisms can be found in them. Alopecia (hair loss) occurs;
often patients have no eyebrows or eyelashes. As the disease progresses, nerve involvement
leads to anesthetic areas and limb weakness; progression leads toaseptic necrosis (tissue
death from lack of blood to area), lepromas (skin nodules), and disfigurement of many areas,
including the face. The lepromatous form does not regress to the other less severe forms.
Histoid leprosy is a clinical variant of lepromatous leprosy that presents with clusters of
histiocytes (a type of cell involved in the inflammatory response) and a grenz zone (an area of
collagen separating the lesion from normal tissue) seen in microscopic tissue sections.
The Ridley-Jopling classification is used globally in evaluating patients in clinical studies. However,
the WHO classification system is more widely used; it has only two forms or classifications of
leprosy. The 2009 WHO classifications are simply based on the number of skin lesions as follows:
Paucibacillary leprosy: skin lesions with no bacilli (M. leprae) seen in a skin smear
Multibacillary leprosy: skin lesions with bacilli (M. leprae) seen in a skin smear
However, the WHO further modifies these two classifications with clinical criteria because "of the
non-availability or non-dependability of the skin-smear services. The clinical system of classification
for the purpose of treatment includes the use of number of skin lesions and nerves involved as the
basis for grouping leprosy patients into multibacillary (MB) and paucibacillary (PB) leprosy."

Investigators state that up to about four to five skin lesions constitutes paucibacillary leprosy, while
about five or more constitutes multibacillary leprosy.
Multidrug therapy (MDT) with three antibiotics (dapsone, rifampicin, and clofazimine) is used for
multibacillary leprosy, while a modified MDT with two antibiotics (dapsone and rifampicin) is
recommended for paucibacillary leprosy and composes most current treatments today (see
treatment section below). Paucibacillary leprosy usually includes indeterminate, tuberculoid, and
borderline tuberculoid leprosy from the Ridley-Jopling classification, while multibacillary leprosy
usually includes the double (mid-) borderline, borderline lepromatous, and lepromatous leprosy.
How is leprosy transmitted?Researchers suggest that M. leprae are spread person to person by nasal secretions or droplets.
However, the disease is not highly contagious like the flu. They speculate that infected droplets
reach other peoples' nasal passages and begin the infection there. Some investigators suggest the
infected droplets can infect others by entering breaks in the skin. M. leprae apparently cannot infect
intact skin. Rarely, humans get leprosy from the few animal species mentioned above. Occurrence
in animals makes it difficult to eradicate leprosy from endemic sources. Routes of transmission are
still being researched for leprosy. Recent genetic studies have demonstrated that several genes
(about seven) are associated with an increased susceptibility to leprosy; some researchers now
conclude that susceptibility to leprosy may be partially inheritable.
How is leprosy diagnosed?The majority of cases of leprosy are diagnosed by clinical findings, especially since most current
cases are diagnosed in areas that have limited or no laboratory equipment available.
Hypopigmented patches of skin or reddish skin patches with loss of sensation, thickened peripheral
nerves, or both clinical findings together often comprise the clinical diagnosis. Skin smears or biopsy
material that show acid-fast bacilli with the Ziehl-Neelsen stain or the Fite stain (biopsy) can
diagnose multibacillary leprosy, or if bacteria are absent, diagnose paucibacillary leprosy. Other
tests can be done, but most of these are done by specialized labs and may help a clinician to place
the patient in the more detailed Ridley-Jopling classification and are not routinely done (lepromin
test, phenolic glycolipid-1 test, PCR, lymphocyte migration inhibition test or LMIT). Other tests such
as CBC test, liver function tests, creatinine test, or a nerve biopsy may be done to help determine if
other organ systems have been affected.
What is the treatment for leprosy?Comment on thisShare Your Story
The majority of cases (mainly clinically diagnosed) are treated with antibiotics. The recommended
antibiotics, their dosages, and length of time of administration are based on the form or classification
of the disease and whether or not the patient is supervised by a medical professional. In general,
paucibacillary leprosy is treated with two antibiotics, dapsone and rifampicin, while multibacillary
leprosy is treated with the same two plus a third antibiotic, clofazimine. Usually, the antibiotics are
given for at least six to 12 months or more.

Antibiotics can treat paucibacillary leprosy with little or no residual effects on the patient.
Multibacillary leprosy can be kept from advancing, and living M. leprae can be essentially eliminated
from the person by antibiotics, but the damage done before antibiotics are administered is usually
not reversible. Recently, the WHO suggested that single-dose treatment of patients with only one
skin lesion with rifampicin,minocycline (Minocin), or ofloxacin (Floxin) is effective. Studies of other
antibiotics are ongoing. Each patient, depending on the above criteria, has a schedule for their
individual treatment, so treatment schedules should be planned by a clinician knowledgeable about
that patient's initial diagnostic classification.
The role for surgery in the treatment of leprosy occurs after medical treatment (antibiotics) has been
completed with negative skin smears (no detectable acid-fast bacilli) and is often only needed in
advanced cases. Surgery is individualized for each patient with the goal to attempt cosmetic
improvements and, if possible, to restore limb function and some neural functions that were lost to
the disease.
What are the complications of leprosy?The complications of leprosy depend on how quickly the disease is diagnosed and effectively
treated. Very few complications occur if the disease is treated early enough, but the following is a list
of complications that can occur when diagnosis and treatment is either delayed or started late in the
disease process:
Sensory loss (usually begins in extremities)
Permanent nerve damage (usually in extremities)
Muscle weakness
Progressive disfigurement (for example, eyebrows lost, disfigurement of the toes, fingers, and
nose)
In addition, the sensory loss causes people to injure body parts without the individual being aware
that there is an injury; this can lead to additional problems such as infections and poor wound
healing.
How is leprosy prevented?Prevention of contact with droplets from nasal and other secretions from patients with untreated M.
leprae infection currently is a way recommended to avoid the disease. Treatment of patients with
appropriate antibiotics stops the person from spreading the disease. People who live with individuals
who have untreated leprosy are about eight times as likely to develop the disease, because
investigators speculate that family members have close proximity to infectious droplets. Leprosy is
not hereditary, but recent findings suggest susceptibility to the disease may have a genetic basis.
Many people get exposed to leprosy throughout the world, but the disease in not highly contagious;
researchers suggest that over 95% of exposures result in no disease, and further studies suggest
that susceptibility may be based, in part, by a person's genetic makeup. In the U.S., there are about

200-300 new cases diagnosed per year, with most coming from exposures during foreign travel. The
majority of worldwide cases are found in the tropics or subtropics (for example, Brazil, India, and
Indonesia). The WHO reports about 500,000 to 700,000 new cases per year worldwide, with curing
of about 14 million cases since 1985.
There is no commercially available vaccine available to prevent leprosy. However, there are reports
of using BCG vaccine, the BCG vaccine along with heat-killed M. leprae organisms, and other
preparations that may be protective or help to clear the infection or to shorten treatment. Except for
BCG in some countries, these preparations are not readily available.
Animals (chimpanzees, mangabey monkeys, and nine-banded armadillos) rarely transfer M.
leprae to humans; nonetheless, handling such animals in the wild is not advised. These animals are
a source for endemic infections.
What is the prognosis (outcomes) of leprosy?The prognosis of leprosy varies with the stage of the disease when first diagnosed and treated. For
example, early diagnosis and treatment limits or prevents tissue damage so the person has a good
outcome. However, if the patient's disease has progressed to more advanced disease, the
complications listed below can markedly affect the patient's lifestyle, and thus the condition has a fair
to poor prognosis.
Where can I find more information on leprosy?"Leprosy," Medscape.com
http://emedicine.medscape.com/article/
220455-overview
"Leprosy Elimination," World Health Organization
http://www.who.int/lep/mdt/en/
"Hansen's Disease," Centers for Disease Control and Prevention
http://www.cdc.gov/nczved/divisions/dfbmd/
diseases/hansens_disease/technical.html
REFERENCES:
Han, X., K. Sizer, E. Thompson, et al. "Comparative Sequence Analysis of Mycobacterium leprae and
the New Leprosy-Causing Mycobacterium lepromatosis." J Bacteriol. 191.19 (2009): 6067-6074.
Zhang, F., W. Huang, S. Chen, et al. "Genomewide Association Study of Leprosy." N Engl J Med.
361.27 (2009): 2609-2618.
SOURCE: http://www.medicinenet.com/leprosy/patient-comments-362.htm

Leprosy (Hansen's disease): Technical InformationOn this Page
Clinical Features
Etiologic Agent Incidence Sequelae Transmission Risk Groups Surveillance
Trends Challenges Opportunities More information
More Information Additional Information
Clinical FeaturesThis chronic infectious disease usually affects the skin and peripheral nerves but has a wide range of
possible clinical manifestations. Patients are classified as having paucibacillary or multibacillary
Hansen's disease. Paucibacillary Hansen's disease is milder and characterized by one or more
hypopigmented skin macules. Multibacillary Hansen's disease is associated with symmetric skin
lesions, nodules, plaques, thickened dermis, and frequent involvement of the nasal mucosa resulting in
nasal congestion and epistaxis.
Etiologic AgentMycobacterium leprae, a bacillus that multiplies very slowly and mainly affects the skin, nerves, and
mucous membranes, is the organism responsible for Hansen’s disease. The organism has never been
grown in bacteriologic media or cell culture, but has been grown in mouse foot pads.
IncidenceIn 2008, the number of new cases detected worldwide was 249,007. In 2007, 109 cases occurring in
the United States were reported to CDC. In 2008, Brazil, India, and Indonesia had 77% of all cases
reported to the World Health Organization (WHO). Over 94% of all reported cases are reported from 17
countries.
SequelaeWorldwide, 1-2 million persons are permanently disabled as a result of Hansen's disease. However,
persons receiving antibiotic treatment or having completed treatment are considered free of active
infection.
Top of Page
Transmission

Although the mode of transmission of Hansen's disease remains uncertain, most investigators think
thatM. leprae is usually spread from person to person in respiratory droplets.
Top of Page
Risk GroupsClose contacts of patients with untreated, active, predominantly multibacillary disease, and persons
living in countries with highly endemic disease are at risk of contracting Hansen’s disease.
Top of Page
SurveillanceHansen's disease is nationally notifiable in the United States.
Top of Page
TrendsPrevalence has remained relatively stable in the United States. Cases appear to be predominantly
related to immigration. Worldwide, the number of cases are decreasing, however, there are pockets of
high prevalence in certain countries.
Top of Page
ChallengesMulti-drug therapy has not been implemented in many endemic areas. Early case finding is difficult in
many areas where the disease is most prevalent. Nerve damage must be recognized and managed.
Relapse rate after completion of short course multi-drug therapy may rise.
Top of Page
OpportunitiesOpportunities exist for participation in Hansen's disease elimination activities in endemic-disease
countries, and for Mycobacterium research in the Laboratory Research Branch of the National Hansen's
Disease Program.
SOURCE: http://www.cdc.gov/nczved/divisions/dfbmd/diseases/hansens_disease/technical.html#
BackgroundLeprosy is a chronic infection caused by the acid-fast, rod-shaped bacillusMycobacterium leprae. Leprosy can be considered 2 connected diseases that primarily affect superficial tissues, especially the skin and peripheral nerves. Initially, a mycobacterial infection causes a wide array of cellular immune responses. These immunologic events then elicit the second part of the disease, a peripheral neuropathy with potentially long-term consequences.
The social and psychological effects of leprosy, as well as its highly visible debilities and sequelae (as seen in the image below), have resulted in a historical stigma associated with leprosy. To minimize the
prejudice against those with leprosy, the condition is also known as Hansen disease, named after G.A. Hansen, who is credited with the 1873 discovery of M leprae. This mycobacterium grows extremely slowly and has not been successfully cultured in vitro.
Hands with Z-thumbs, clawing, contractures, and shortening of fingers due to repetitive injury and healing. Ho Chi Minh City, Vietnam. (Courtesy of D. Scott Smith, MD)
In the 1990s, the World Health Organization (WHO) launched a campaign to eliminate leprosy as a public health problem by 2000. Elimination, as defined by the WHO, was defined as a reduction of patients with leprosy requiring multidrug therapy to fewer than 1 per 10,000 population. This goal was achieved in terms of global prevalence by 2002, but 15 of the 122 countries where leprosy was endemic in 1985 still have prevalence rates of greater than 1 per 10,000 population.[1]
Although multidrug regimens have been used globally to cure nearly 14 million patients with leprosy since 1985, the number of new leprosy cases remained relatively unchanged from 1980 to 2000, ranging from 500,000-700,000 worldwide per year.[2] Access and delivery of antibiotics continues to be a problem in the most endemic nations. With the precise transmission mechanism of leprosy still unknown and a lack of an effective vaccine, leprosy will probably continue to pose an ongoing public health problem in the coming decades.
The goal of the WHO by the end of 2015 is to reduce the rate of new cases with grade-2 disabilities worldwide by at least 35%. This will be carried out by enforcing activities to decrease the delay in diagnosing the disease and actuate treatment with multidrug therapy. This will also have the impact of reducing transmission of the disease in the community.[2]
PathophysiologyLeprosy can manifest in different forms, depending on the host response to the organism.
Individuals who have a vigorous cellular immune response to M leprae have the tuberculoid form of the disease that usually involves the skin and peripheral nerves. The number of skin lesions is limited, and they tend to be dry and hypoesthetic. Nerve involvement is usually asymmetric. This form of the disease is also referred to as paucibacillary leprosy because of the low number of bacteria in the skin lesions (ie, < 5 skin lesions, with absence of organisms on smear). Results of skin tests with antigen from killed organisms are positive in these individuals.
Individuals with minimal cellular immune response have the lepromatous form of the disease, which is characterized by extensive skin involvement. Skin lesions are often described as infiltrated nodules and plaques, and nerve involvement tends to be symmetric in distribution. The organism grows best at 27-30°C; therefore, skin lesions tend to develop in the cooler areas of the body, with sparing of the groin, axilla, and scalp. This form of the disease is also referred to as multibacillary leprosy because of the large number of bacteria found in the lesions (ie, >6 lesions, with possible visualization of bacilli on smear). Results of skin tests with antigen from killed organisms are nonreactive.
Patients may also present with features of both categories; however, over time, they usually evolve to one or the other (indeterminate or borderline leprosy). Interestingly, most individuals who are exposed to leprosy never develop the disease.
Classification of leprosy: Leprosy has 2 classification schemas: the 5-category Ridley-Jopling system and the simpler and more commonly used WHO standard.
Ridley-Jopling: Depending on the host response to the organism, leprosy can manifest clinically along a spectrum bounded by the tuberculoid and lepromatous forms of the disease. Most patients fall into the intermediate classifications, which include borderline tuberculoid leprosy, midborderline leprosy, and borderline lepromatous leprosy. The classification of the disease typically changes as it evolves during its progression or management. The Ridley-Jopling system is used globally and forms the basis of
clinical studies of leprosy. It may also be more useful in guiding treatment regimens and assessing risk of acute complications. Physical findings in each subtype are presented in the Clinical section.
WHO system: The WHO recommends classifying leprosy according to the number of lesions and the presence of bacilli on a skin smear. This method is useful in countries where biopsy analysis in unavailable.
o Paucibacillary leprosy is characterized by 5 or fewer lesions with absence of organisms on smear. Paucibacillary leprosy generally includes the tuberculoid and borderline lepromatous categories from the Ridley-Jopling system.
o Multibacillary leprosy is marked by 6 or more lesions with possible visualization of bacilli on smear. Lepromatous leprosy, borderline lepromatous leprosy, and midborderline leprosy on the Ridley-Jopling scale are included in the multibacillary leprosy category.
EpidemiologyFrequency
United StatesAn average of 150-250 cases are diagnosed each year in the United states.[1]
In 2010, according to the Registry of National Hansen’s Disease Programs (NHDP), 205 new cases of leprosy were detected in the United States.[3]
In 2010 WHO reports, 169 new cases of leprosy were detected. The number of new cases of MB leprosy reported was 105. The number of females among the new cases was 53, and 6 cases in children were reported. No cases of relapse were reported in 2010.[2]
Most cases of leprosy in the United States are found in immigrants, although endemic foci exist in parts of Louisiana, Florida, and Texas along the Gulf of Mexico; in Mexican and Asian California populations; and in Spanish Americans in New York City. Around 75% of these detected leprosy cases involve patients who have lived in foreign countries, primarily Asia, Africa, and Latin America.[3]
Some cases among native US citizens can be accounted for by exposure to leprosy overseas. Some cases can be attributed to a contact with a known case of leprosy or exposure to infected armadillos.
Based on genetic analysis studies, wild armadillos and many patients with leprosy in the southern United States are infected with the same strain of M leprae.[4]Leprosy may be a zoonosis in the southern United States because armadillos are a large reservoir for this disease.
Nonetheless, history of exposure cannot be verified in many patients.[3]
InternationalAccording to WHO figures and as reported by 130 countries, the global annual detection rates have declined from 2004-2010, when 407,791 and 228,474 new cases were reported, respectively (see the images below). The prevalence registered worldwide at the beginning of 2010 was 192,246 cases. Of the new cases, 95% were detected worldwide during 2010 in the following countries: Angola, Bangladesh, Brazil, China, Democratic Republic of the Congo, India, Ethiopia, Indonesia, Madagascar, Mozambique, Myanmar, Nepal, Nigeria, Philippines, Sri Lanka, Sudan, and United Republic of Tanzania.[2] These countries still exhibit pockets of high endemicity.
Leprosy prevalence rates, data reported to WHO as of beginning January 2011. Courtesy of WHO, Leprosy: Global
situation, http://www.who.int/lep/situation/en/, accessed March 14, 2013. Leprosy new case detection rates, data reported to WHO as of beginning January 2011. Courtesy of WHO, Leprosy: Global situation, http://www.who.int/lep/situation/en/, accessed March 14, 2013.
Mortality/Morbidity
Leprosy is rarely fatal, and the primary consequence of infection is nerve impairment and debilitating sequelae. According to one study, 33-56% of newly diagnosed patients already displayed signs of impaired nerve function.[5] According to estimates, 3 million people who have completed multidrug therapy for leprosy have sustained disability due to nerve damage. Although both lepromatous leprosy and tuberculoid leprosy involve the skin and peripheral nerves, tuberculoid leprosy has more severe manifestations. Nerve involvement results in loss of sensory and motor function, which may lead to frequent trauma and amputation. The ulnar nerve is most commonly involved.
Damage in the following nerves is associated with characteristic impairments in leprosy:o Ulnar and median - Clawed hando Posterior tibial - Plantar insensitivity and clawed toeso Common peroneal -Foot dropo Radial cutaneous, facial, and greater auricular nerves (may also be involved; as seen in the image
below) Patient with facial nerve palsy and contractures of the hand. Daloa, Ivory Coast. (Courtesy of D. Scott Smith, MD)
Infiltration by bacteria may lead to destruction of nasal cartilage (lepromatous leprosy), ocular involvement, and diffuse thickening of the skin. Advanced cases of leprosy involve the loss of eyebrows and lashes, but these deformities are less common today.
Worldwide, leprosy is considered the most common cause of crippling of the hand, which is caused by ulnar nerve involvement.[6] Peroneal nerve involvement can lead to foot drop, posterior tibial nerve involvement, and clawed toes.
Race
Leprosy was once endemic worldwide, and no racial predilection is known. In the late 1800s, the incidence of leprosy in northern Europe and North America dropped dramatically, and the disease is now reported primarily in tropical areas.
Sex
Leprosy is generally more common in males than in females, with a male-to-female ratio of 1.5:1. In some areas in Africa, the prevalence of leprosy among females is equal to or greater than that in males.[2]
Age

Leprosy can occur at any age, but, in developing countries, the age-specific incidence of leprosy peaks in children younger than 10 years, who account for 20% of leprosy cases. Leprosy is very rare in infants; however, they are at a relatively high risk of acquiring leprosy from the mother, especially in cases of lepromatous leprosy or midborderline leprosy.
SOURCE: http://emedicine.medscape.com/article/220455-overview#a0199
Leprosy
Share on facebook Share on twitter Bookmark & Share Printer-friendly version
Leprosy is a disease that has been known since biblical times. This infectious disease causes skin sores,
nerve damage, and muscle weakness that gets worse over time.
Causes
Leprosy is caused by the bacterium Mycobacterium leprae. It is not very contagious and it has a long
incubation period (time before symptoms appear), which makes it hard to know where or when someone
caught the disease. Children are more likely than adults to get the disease.
Leprosy has two common forms: tuberculoid and lepromatous. Both forms produce sores on the skin.
However, the lepromatous form is most severe. It causes large lumps and bumps (nodules).
Leprosy is common in many countries worldwide, and in temperate, tropical, and subtropical climates.
About 100 cases per year are diagnosed in the United States. Most cases are in the South, California,
Hawaii, and U.S. islands.
Effective medications exist. Isolating people with this disease in "leper colonies" is not needed.
Drug-resistant Mycobacterium leprae and an increased numbers of cases worldwide have led to global
concern about this disease.
Symptoms
Symptoms include:
Skin lesions that are lighter than your normal skin coloro Lesions have decreased sensation to touch, heat, or pain
o Lesions do not heal after several weeks to months
Muscle weakness
Numbness or lack of feeling in the hands, arms, feet, and legs
Exams and Tests
Lepromin skin test can be used to tell the two different forms of leprosy apart, but it is not used to
diagnose the disease
Skin lesion biopsy
Skin scraping examination

Treatment
A number of different antibiotics (including dapsone, rifampin, clofazamine, fluoroquinolones, macrolides,
and minocycline) are used to kill the bacteria that cause the disease. More than one antibiotic is often
given together.
Aspirin, prednisone, or thalidomide is used to control inflammation.
Outlook (Prognosis)
Diagnosing the disease early is important. Early treatment limits damage, prevents a person from
spreading the disease, and allows the person to have a normal lifestyle.
Possible Complications
Disfigurement
Muscle weakness
Permanent nerve damage in the arms and legs
Sensory loss
People with long-term leprosy may lose the use of their hands or feet due to repeated injury because they
lack feeling in those areas.
When to Contact a Medical Professional
Call your health care provider if you have symptoms of leprosy, especially if you have had contact with
someone who has the disease. Cases of leprosy in the United States need to be reported to the Centers
for Disease Control and Prevention.
Prevention
Prevention consists of avoiding close physical contact with untreated people. People on long-term
medication become noninfectious (they do not transmit the organism that causes the disease).
Alternative Names
Hansen's disease
References
Renault CA, Ernst JD. Mycobacterium leprae. In: Mandell GL, Bennett JE, Dolin R, eds. Principles and
Practice of Infectious Diseases. 7th ed. Philadelphia, PA: Elsevier Churchill Livingstone; 2009:chap 251.
Ernst JD. Leprosy (Hansen's ). In: Goldman L, Ausiello D, eds. Goldman's Cecil Medicine. 24th ed.
Philadelphia, PA: Saunders Elsevier; 2011:chap 334.
Update Date: 9/1/2013
Updated by: Jatin M. Vyas, MD, PhD, Assistant Professor in Medicine, Harvard Medical School; Assistant
in Medicine, Division of Infectious Disease, Department of Medicine, Massachusetts General Hospital.
Also reviewed by David Zieve, MD, MHA, Bethanne Black, and the A.D.A.M. Editorial team.

SOURCE: http://www.nlm.nih.gov/medlineplus/ency/article/001347.htm
Classification of Leprosy and the clinical symptoms
Disease Clinical Features
Indeterminate leprosyThey are the first type of skin lesions characterized by hypo-pigmented spots
The lesions undergo healing spontaneously
Paucibacillary (tuberculoid leprosy)
A large red patch with well-defined raised borders or a large hypo pigmented asymmetrical lesion.
Lesion is dry and hairlessInfectivity is minimal at this stageLoss of sensation is seenNerves become thick followed by loss of functionIt either progresses to the borderline stage or spontaneously get cured
Borderline borderline leprosyCharacterized by small and numerous skin lesions
The disease goes back to the tuberculoid stage or progresses to the next stage
Borderline borderline leprosySeveral small, irregular red lesions are seen
Moderate sensory loss is seenIt either goes back to the previous stage or progresses to the next
Borderline lepromatous leprosySeveral lesions such as plaques, macules, papules, and nodules are seen
Lesions have a characteristic inverted saucer like appearance
Multibacillary Hansen’s disease (lepromatous leprosy)
Early symptoms:
Several lesions such as plaques, macules, papules, and nodules are seenNasal congestion, discharge and bleeding is seenInflammation of the leg and anklesProgressive symptoms:Thickening of the dermis (skin) in the forehead and ear lobesLoss of eyebrows and eyelashesEye defects such as glaucoma and blindness are seenNodules in the legs break and form ulcersEnlargement of the breast and sterility occurs in the malesInternal infection results in the enlargement of the liver and lymph nodesLoss of sensation in the peripheral nerves. Deformation of the fingers and toes results due to painless repeated trauma
Leprosy is classified into several types based on the bacterial load present in the lesions, the extent of skin and nerve involvement and based on the presence of deformities. Several types of classification like Madrid classification, Ridley & Jopling classification Indian Classification, WHO classification , Field Worker's Classification etc.
Based on the 2 commonly used classifications, leprosy is classified into six types based
on the clinical features (Ridley & Jopling classification):The type of the disease is a reflection of the immune status of the host.
The first sign of the disease is the feeling of numbness or loss of sensation for temperature (heat) followed by touch and pain which usually begins at the extremities. The skin lesions appear later during the course of the disease.
The Indian classification has an additional type, the neuritic type, which is bacteriologically negative and shows neural involvement without any skin lesions.
Read more: Leprosy / Hansens Disease - Classifications & Clinical Symptoms http://www.medindia.net/patients/patientinfo/leprosy_classification.htm#ixzz3SZBKN8dd