Embed Size (px)
Citation preview

Left Ventricular Oufflow Tract Obstruction with Mitral Valve Replacement in Small Ventricular Cavities G. Kimble Jett, M.D., M. Denise Jett, B.A., M.T., Glenn R. Barnhart, M.D., Gerta L. van Rijk-Swikker, M.D., Michael Jones, M.D., and Richard E. Clark, M.D.
ABSTRACT The inference that mitral valve replacement (MVR) may produce left ventricular outflow tract (LVOT) obstruction has been made, but no comparative hemody- namic studies with various types of prostheses have been done. The purpose of the present study was to compare the gradients created across the LVOT with MVR in young sheep with small left ventricular cavities. Mitral valve re- placement was accomplished using cardiopulmonary by- pass and hypothermic cardioplegic arrest. Five animals were used for each of the following valves studied 25-mm Ionescu-Shiley bovine pericardial valve, 25-mm Hancock porcine aortic valve, 2M-6120 2&mm Starr-Edwards ball- valve prosthesis, 25-mm Bjork-Shiley 60-degree flat tilting- disc prosthesis, and 25-mm St. Jude Medical hemidisc valve. Gradients across the LVOT were measured after MVR and then during infusion of isoproterenol hydro- chloride (0.05 p,g/kg/min). Following MVR, only the Starr- Edwards valve produced an LVOT gradient (32 f 23 mm Hg). Substantial gradients after MVR were seen, however, with isoproterenol administration with the Ionescu-Shiley (47 f 4 mm Hg), Hancock (13 f 8 mm Hg), and Starr- Edwards (65 f 30 mm Hg) valves but not with the low- profile valves (Bjork-Shiley and St. Jude Medical). The results of the present study demonstrate that MVR can produce LVOT obstruction. The greatest degree of obstruc- tion was with the high-profile mechanical and biopros- thetic valves.
Replacement of a diseased mitral valve with a prosthetic valve is now easily accomplished with acceptable early and late mortality and morbidity. Although various me- chanical and tissue valves are available, replacement of the valve in a small ventricular cavity limits the choices of acceptable valves [I, 21. Early postoperative deaths associated with low cardiac output have been attributed to left ventricular outflow tract (LVOT) obstruction caused by caged-ball valves (3-91. Low-profile valves were designed to prevent obstruction of the outflow tract in small left ventricular cavities [3, 5). Recent re-
From the Surgery Branch, National Heart, Lung, and Blood Institute, Bethesda, MD.
Presented at the Twenty-first Annual Meeting of The society of Thoracic Surgeons, Phoenix, AZ, Jan 21-23, 1985. Address reprint requests to Dr. Clark, Building 10, Room 2N242, Na- tional Institutes of Health, Bethesda, MD 20205.
ports [lo-131 on bioprosthetic valve replacement have implicated LVOT obstruction to be an important factor contributing to mortality and morbidity.
Despite the frequent references to LVOT obstruction following mitral valve replacement (MVR) with some prostheses, no comparative hemodynamic studies with various prostheses have been done. Most of the reports described necropsy findings, although several measured gradients [ll, 121. The present study was designed to compare the gradients created across the LVOT with MVR using various prostheses of similar size (Starr- Edwards, Bjork-Shiley, St. Jude Medical, Hancock, and Ionescu-Shiley). High-profile as well as low-profile valves were chosen for comparison. Small normal sheep were used because of their small ventricular cavities.
Material and Method Twenty-five sheep 2 months of age and weighing 25 to 30 kg underwent MVR. The same technique was used for MVR regardless of the prosthetic valve placed. Anes- thesia was induced with sodium thiopental (30 mg per kilogram of body weight) and was maintained with halothane following endotracheal intubation and me- chanical ventilation.
The heart was exposed through a left thoracotomy in the fourth intercostal space and suspended in a pericar- dial cradle. Aortic pressure was measured through an Wgauge, 5.1-cm fluid-filled catheter inserted into the proximal ascending aorta. This same catheter later served for infusion of cardioplegic solution. Left ventric- ular and left atrial pressures were also measured through short, fluid-filled catheters inserted directly into the left ventricular apex and left atrial appendage, re- spectively. Cardiac output was determined by the ther- modilution technique utilizing a flow-directed catheter inserted through the femoral vein and positioned in the pulmonary artery. All pressure recordings were made on a Gould Brush 480 multichannel recorder. Baseline hemodynamic measurements were then obtained.
Heparin (300 unitskg) was administered, and cannu- lations were performed in the femoral artery for sys- temic arterial perfusion and in the pulmonary artery for venous drainage. A previously placed tape was secured around the pulmonary artery to isolate venous drainage. Cardiopulmonary bypass was initiated and the animal cooled to a body temperature of 25°C. A vent was placed in the left ventricular apex. Once the animal was cooled, the heart was arrested by placing a clamp across the ascending aorta and cardioplegic solution was injected
70

71 Jett et al: LVOT Obstruction with MVR
into the aortic root. The cardioplegic solution consisted of 20 mEq of KCl, 5 mEq of NaHC03, 6.25 gm of man- nitol in 1,000 ml of 2.5% dextrose, and 0.45% NaCl (pH 7.60, 370 mOsm), and was administered at a dose of 10 “Vkg at an aortic pressure of 60 to 100 mm Hg.
The left atrium was opened longitudinally, and the normal mitral valve, chordae tendineae, and papillary muscle heads were excised. The prosthetic valve was inserted and secured with twelve braided, nonabsorb- able, interrupted mattress sutures buttressed with pledgets passed through the atrial aspect of the mitral annulus and prosthetic valve ring. It should be empha- sized that the valves were placed in an annular, not a subannular, position. The bioprosthetic valves were oriented with a strut in the outflow tract to create the greatest possible degree of obstruction. The atriotomy was closed with a continuous monofilament suture, and the heart was evacuated of remaining air. The cross- clamp was removed and the animal warmed to 38°C. The left ventricular vent was removed after resumption of normal sinus rhythm. The animal was separated from cardiopulmonary bypass. Once the animal was in stable condition, hemodynamics were measured. Isoprotere- no1 hydrochloride (0.05 &kg/min) was administered, and the hemodynamic measurements were repeated.
Five animals were used for each of the following valves studied: Ionescu-Shiley bovine pericardial valve, 25 mm (Shiley Laboratories, Inc., Santa Ana, CA); Han- cock porcine aortic valve, 25 mm (Vascor Inc., Anaheim, CA); Starr-Edwards caged-ball valve prosthesis No. 5120-2M, 28 mm (American Edwards Laboratories, 3anta Ana, CA); Bjork-Shiley 60-degree flat-disc pros- thesis, 25 mm (Shiley Laboratories, Inc., Santa Ana, CA); and St. Jude Medical valve No. 25M-101, 25 mm (St. Jude Medical, Inc., St. Paul, MN). It should be em- phasized that the valves were of similar size. Hemody- namic values after MVR were compared with the values obtained prior to valve replacement for each valve used. In addition, hemodynamic values after valve replace- ment were compared between groups having different types of valves. All comparisons were made using the Student t test for paired differences and were considered statistically significant when p was less than 0.05. Data are reported as the mean the standard error of the mean.
Table 1 . Hernodynamics prior to Valve Replacement“
Results The physical characteristics and echocardiographic mea- surements of the study animals were as follows: age, 2.0 2 0.1 months; body weight, 27 5 1 kg; heart weight, 176 5 15 gm; thickness of left ventricular free wall, 12.2 * 0.5 mm; left ventricular systolic diameter, 25.8 * 2.3 nm; and left ventricular diastolic diameter, 36.0 * 2.5
Snm. The ventricular cavities were small but normal for the body sizes. There were no significant differences in hemodynamic values between groups prior to valve in- sertion. Isoproterenol increased cardiac output and heart rate significantly, but did not create a gradient across the LVOT. The preoperative hemodynamic values of all groups combined are shown in Table 1.
Mitral valve replacement resulted in a significant in- crease in left ventricular end-diastolic pressure and a significant decrease in cardiac output in each group studied. None of the valves created a significant end- diastolic gradient across the prosthesis. The administra- tion of isoproterenol caused significant increases in car diac output and heart rate similar to those seen prior to valve replacement. All hemodynamic values for each group after valve insertion are shown in Table 2.
Placement of an Ionescu-Shiley valve in the mitral po- sition created no significant gradient across the LVOT, but the administration of isoproterenol resulted in a gra- dient of 47 ? 4 mm Hg (Figure). The catheter in the left ventricle was repositioned to ensure that catheter en- trapment was not occurring. Presumably, the gradient was prosthesis related, since no gradient was created with isoproterenol provocation prior to valve re- placement .
No gradient was created across the LVOT with place- ment of a Hancock valve. When isoproterenol was given, a gradient of 13 * 8 mm Hg appeared (see Fig- ure). This gradient was significantly less than that created with the Ionescu-Shiley valve.
Placement of a Starr-Edwards mechanical prosthesis resulted in a significant gradient across the LVOT. The gradient increased to 65 f 30 mm Hg with isoproterenol administration (see Figure). However, there were no significant differences in the gradient created between this valve and the Ionescu-Shiley and Hancock valves because of the large standard error.
Mitral valve replacement with a Bjork-Shiley prosthe-
- - - AoP AoP LVP LVP LAP LV-AO
Measurement (mm Hg) (mm Hg) (mm Hg) (mm Hg) (mm Hg) EDG PSG CO (Llmin) HR @eat/min)
Control
Isoproterenol (N = 25) 85/54 f 12/9 65 2 10 85/7 2 5/6 43 f 4 8 f 4 0 0 2.44 f 0.31 97 2 11
(0.05 Kg/kg/min) 94/62 2 14/10 74 f 12 112/4 2 17/4 52 f 10 5 f 3 0 0 3.44 2 0.60 181 ? 20
a Values are mean f standard error of the mean. AoP = aortic pressure; AoP = mean aortic pressure; LVP = left ventricular pressure; = mean left ventricular pressure; LAP = mean left atrial pressure; EDG = end-diastolic gradient; LV-Ao PSG = left ventricular to aortic peak systolic gradient; CO = cardiac output; HR = heart rate.
72 The Annals of Thoracic Surgery Vol 41 No 1 January 1986
Table 2. Hemodynamic Values after Valve Replacementa - - -
AoP AoP . LVP LVP LAP Measurement (mm Hg) (mmHg) (mmHg) (mm Hg) (mm Hg) EDG LV-Ao PSG CO (Umin) HR (beaffmin)
IONESCU-SHILEY IN = 5)
Control 83/48 f 8/5 59 f 6 65/12 c 17/4 37 t 9 15 f 2 2 f 1 2 f 2 1.51 f 0.10 105 f 33 lsoproterenol
(0.05 pg/kg/min) 84/47 f 4/5 55 f 4 131/10 t 613 62 2 11 13 ? 3 2 f 2 47 f 4 2.65 f 0.18 169 t 20
HANCOCK (N = 5)
1.35 ? 0.45 101 ? 29 Control 101155 c 1718 57 t 4 91/20 c 21/12 34 f 11 17 f 3 6 f 2 4 f 3 lsoproterenol
(0.05 pg/kg/min) 97/54 f 19/10 63 f 12 104/7 t 30/3 48 f 20 13 ? 2 2 f 1 13 f Sb 2.43 f 0.24 188 f 17
STARR-EDWARDS (N = 5)
Control 98/54 f 15/11 59 ? 13 100123 f 2719 55 c 16 17 c 5 2 -t 1 32 f 23 1.31 ? 0.17 132 t 33 Isoproterenol
(0.5 pg/kg/min) 89/62 c 10110 71 f 6b 132/11 t W 2 61 f 17 15 f 3 2 t 1 65 f 30 2.86 f 0.52 200 f 5
BIORK-SHILEY (N = 5)
Control 89/59 f 7/8 62 t 6 83/25 ? 12/14 37 IT 12 16 c 5 4 c 2 4 ? 4 1.59 f 0.46 132 f 33 lsoproterenol
(0.05 ui?/kdmin) 82/52 c 14/10 61 c 10 80/15 f 11/5b.C 40 f 8 13 f 2 4 f 2 5 t 4b,c 2.47 f 0.52 184 f 24
Control 119/61 f 9/13b.d 75 ? 3b,d.e 105/15 5/10b 41 f 8 28 ? 7 4 f 3 1 f lC 1.44 f 0.40 107 -t 33 lsoproterenol
(0.05 pg/kg/min) 102/56 f 8/9b 68 t 5 109/15 f 6/Zb 47 f 4 19 f 2b.d,e Od,e 10 f 4b,c,d 3.08 ? 0.41 218 f 25 - - -
"Values are mean ? standard error of the mean. AoP = aortic pressure; AoP = mean aortic pressure; LVP = left ventricular pressure; LVP = mean left ventricular pressure; LAP = mean left atrial pressure; EDG = end-diastolic gradient; LV-Ao PSG = left ventricular to aortic peak systolic gradient; CO = cardiac output; HR = heart rate. bp < 0.05 when compared at same intervention to lonescu-Shiley bovine pericardial valve. ' p < 0.05 when compared at same intervention to Starr-Edwards valve. d p < 0.05 when compared at same intervention to Bjork-Shiley valve. ' p < 0.05 when compared at same intervention to Hancock porcine valve.
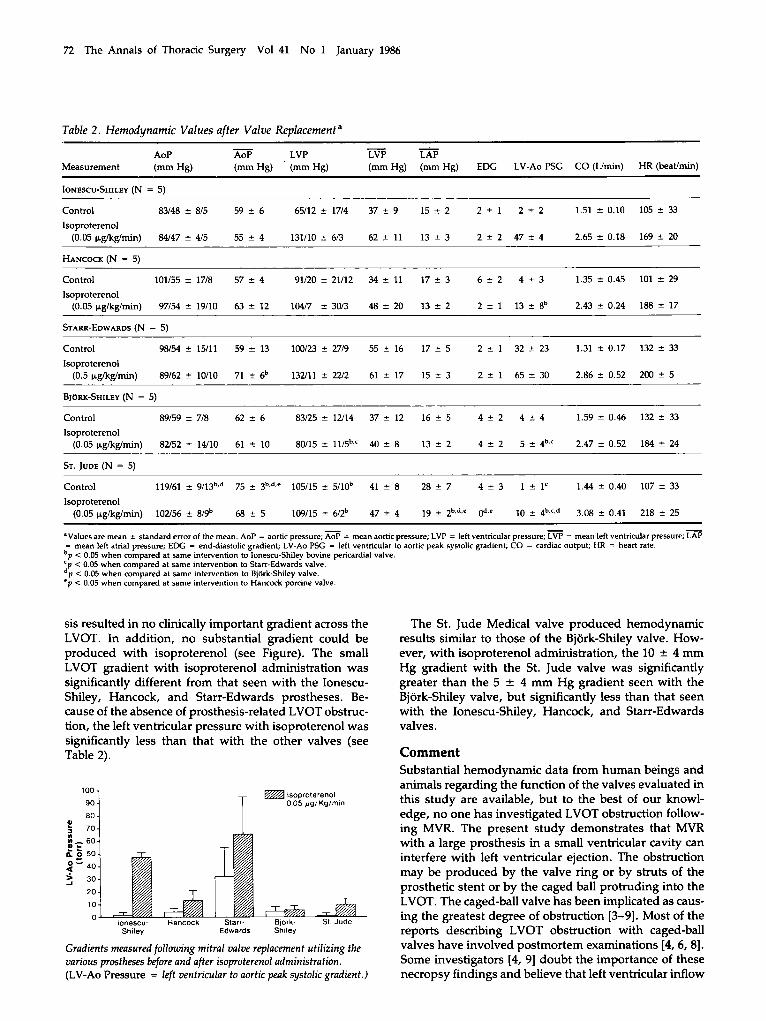
sis resulted in no clinically important gradient across the LVOT. In addition, no substantial gradient could be produced with isoproterenol (see Figure). The small LVOT gradient with isoproterenol administration was significantly different from that seen with the Ionescu- Shiley, Hancock, and Starr-Edwards prostheses. Be- cause of the absence of prosthesis-related LVOT obstruc- tion, the left ventricular pressure with isoproterenol was significantly less than that with the other valves (see Table 2). Comment
The St. Jude Medical valve produced hemodynamic results similar to those of the Bjork-Shiley valve. How- ever, with isoproterenol administration, the 10 * 4 mm Hg gradient with the St. Jude valve was significantly greater than the 5 2 4 mm Hg gradient seen with the Bjork-Shiley valve, but significantly less than that seen with the Ionescu-Shiley, Hancock, and Starr-Edwards valves.
Substantial hemodynamic data from human beings and animals regarding the function of the valves evaluated in this study are available, but to the best of our knowl- edge, no one has investigated LVOT obstruction follow- ing MVR. The present study demonstrates that MVR with a large prosthesis in a small ventricular cavity can interfere with left ventricular ejection. The obstruction may be produced by the valve ring or by struts of the prosthetic stent or by the caged ball protruding into the LVOT. The caged-ball valve has been implicated as caus- ing the greatest degree of obstruction [3-91. Most of the
Shiley Edwards Shiley reports describing LVOT obstruction with caged-ball valves have involved postmortem examinations [4,6, 81. Some investigators (4, 91 doubt the importance of these necropsy findings and believe that left ventricular inflow
100 lsoproterenol 90 0 0 5 pgIKglmin
80 r a 70
2-60
l i 50
3 - 4 0
3 30 20
10
lonescu- Hancock Starr- Blork- S1 Jude
Gradients measured following mitral valve replacement utilizing the various prostheses wore and after isoproterenol administration. (LV-Ao Pressure = left ventricular to aortic peak systolic gradient.)

73 Jett et al: LVOT Obstruction with MVR
obstruction is responsible for the death of the patient with mitral prosthesis-left ventricular disproportion.
We found that LVOT obstruction was substantial in animals with caged-ball valves. Following MVR, all ani- mals had a gradient at rest that increased with isoproter- enol. This degree of obstruction resulted in the inability of 4 of 5 animals in the Starr-Edwards group to maintain adequate arterial pressure and cardiac output after car- diopulmonary bypass. Superior hemodynamic results were observed with the low-profile mechanical valves. A small gradient could be provoked with isoproterenol with the St. Jude valve, perhaps secondary to a valve ring protruding into the LVOT. All of the animals with St. Jude valves were separated from cardiopulmonary bypass without difficulty. It was the fear of LVOT ob- struction caused by caged-ball mechanical prostheses that prompted the design of disc valves [3,5]. Our study confirms the presence of obstruction across the LVOT created by a high-profile, caged-ball valve prosthesis in the mitral position in the ventricular cavities of normal young sheep.
The lack of the need for anticoagulation makes bio- prosthetic valves attractive alternatives to mechanical valves. Their degeneration in young patients, however, has raised questions of their durability [ll, 12). One re- port [14] suggested that the risk of reoperation for tissue valve degeneration is less than the risk of the throm- boembolic complications of mechanical valves. Other re- ports [lo-131 described obstruction to left ventricular emptying when bioprosthetic valves were used in small left ventricular cavities. The obstruction has been seen with bovine pericardial[12] as well as porcine aortic [lo, 11, 131 bioprosthetic valves. The obstruction has been attributed to orientation of a strut into the outflow tract.
We did not observe significant LVOT obstruction fol- lowing MVR with bioprosthetic valves with a strut placed in the outflow tract; however, when isoprotere- no1 was administered, significant gradients were pro- duced with the Ionescu-Shiley and the Hancock biopros- thetic valves. The gradient produced by isoproterenol was presumably related to or caused by the mitral pros- thesis, since no gradient was produced when isoprotere- no1 was administered prior to valve replacement. The left ventricular pressure catheter was repositioned to en- sure that the gradient was not secondary to catheter en- trapment [15]. The gradients created were greater than the increase in cardiac output produced by isoprotere- nol, a finding that suggested that the pressure difference was not merely flow related. The gradient presumably resulted from a small end-systolic left ventricular volume during isoproterenol administration [16-181. It should again be emphasized that a strut was oriented in the outflow tract to enhance the strut-related obstruc- tion. Whether a similar degree of obstruction would re- sult with the strut oriented away from the outflow tract is currently being investigated.
The greatest degree of obstruction created by biopros- thetic valve replacement in our studies was seen with the Ionescu-Shiley bovine pericardial valve. This obser-
vation is difficult to explain, since not only is the strut width narrower than that of the Hancock valve (4 mm versus 7 to 10 mm), but it is slightly lower profile, the strut to sewing ring length being 18 mm for a 25-mm Ionescu-Shiley valve versus 19.4 mm for a 25-mm Han- cock valve, with an implant strut height of 13.1 mm versus 14.2 mm, respectively. Both of these factors should decrease the amount of obstruction across the LVOT.
All of the animals used in our study demonstrated left ventricular dysfunction following MVR as evidenced by an increased left ventricular end-diastolic pressure and decreased cardiac output. This presumably resulted from inadequate myocardial protection during valve re- placement. Our cross-clamp time averaged 20 to 25 min- utes for each study. Only a single dose of cardioplegic solution was used; perhaps this accounted for a degree of the left ventricular dysfunction, since intermittent in- fusion of cardioplegic solution has been shown to be superior [19]. Homogeneous cooling of the heart was not ensured by our method of venous drainage through the pulmonary artery. Better protection might have been achieved with venous drainage at the level of the venae cavae. In addition, perhaps better left ventricular func- tion would have been observed with blood cardioplegia versus an asanguineous solution [20]. The left ventricu- lar dysfunction observed, however, should not alter the validity of our results, although perhaps greater degrees of obstruction might have been seen if better myocardial protection had been achieved.
The results of our study demonstrate that MVR can produce LVOT obstruction. The greatest degree of ob- struction was with the high-profile mechanical and bio- prosthetic valves. The bovine pericardial valve produced greater obstruction than the porcine valve when a strut was oriented in the outflow tract. Although extrapola- tion from an animal experimental study to the clinical setting must be guarded, it would seem justified to use low-profile mechanical valves for MVR in small left ven- tricular cavities.
References 1. Austen WG: Heart valve substitutes. In Johnson RA, Haber
E, Austen WG (eds): The Practice of Cardiology. Boston, Little, Brown, 1980, pp 527-570
2. Roberts WC: Choosing a substitute cardiac valve: type, size, surgeon. Am J Cardiol38633, 1976
3. Kay EB, Suzuki A, Demaney M, Zimmerman HA: Com- parison of ball and disc valves for mitral valve replacement. Am J Cardiol 18:504, 1966
4. Roberts WC, Morrow AG: Mechanisms of acute left atrial thrombosis after mitral valve replacement: pathologic findings indicating obstruction to left atrial emptying. Am J Cardiol 18:497, 1966
5. Cooley DA, Bloodwell RD, Hallman GL: Mitral valve re- placement with a discoid prosthesis. Ann Thorac Surg 3:487, 1967
6. Roberts WC, Morrow AG: Topics in clinical medicine: anatomic studies of hearts containing caged-ball prosthetic valves. Johns Hopkins Med J 121:271, 1967

74 The Annals of Thoracic Surgery Vol 41 No 1 January 1986
7. Roberts WC, Morrow AG: Causes of early postoperative death following cardiac valve replacement. J Thorac Car- diovasc Surg 54A22, 1967
8. Roberts WC, Bulkley BH, Morrow AG: Pathologic anatomy of cardiac valve replacement: a study of 224 necropsy pa- tients. Prog Cardiovasc Dis 15539, 1973
9. Roberts WC Complications of cardiac valve replacement: characteristic abnormalities of prostheses pertaining to any specific site. Am Heart J 103:113, 1982
10. Thiene G, Bortolotti V, Casarotto D, et ak Prosthesis-left ventricle disproportion in mitral valve replacement with the Hancock bioprosthesis: pathological observations. In Se- bening G, Kloverkom WP, Meisner H, Struck E (eds): Bic- prosthetic Cardiac Valves. Munich, Deutsches Herzzen- trum, 1979, p 357
11. Sanders SP, Levey RJ, Freed MD, et a1 Use of porcine xeno- grafts in children and adolescents. Am J Cardiol 46:429, 1980
12. Galioto FM, Midgley FM, Kapur S, et a1 Early failures of Ionescu-Shiley bioprosthesis after mitral valve replacement in children. J Thorac Cardiovasc Surg 83306, 1982
13. Valente M, Bartolotti V, Arbustini R, et al: Glutaraldehyde- preserved porcine bioprosthesis: factors affecting perfor- mance as determined by pathologic studies. Chest 83607, 1983
14. Shore DF, De Leval MR, Stark J: Valve replacement in chil- dren: biologic versus mechanical valves. In Cohen LG, Gal- lucci V (eds): Cardiac Bioprostheses: Proceedings of the Second International Symposium. New York, Yorke Med- ical, 1982, pp 238-247
15. Morrow AG, Vasko JS, Henney RP, Brawley RK: Can outflow obstruction be induced within the normal left ven- tricle? Am J Cardiol 16540, 1965
16. Krasnow N, Rolett EL, Yurchak PM, et al: Isoproterenol and cardiovascular performance. Am J Med 37514, 1964
17. Hamson DC, Glick G, Goldblatt A, Braunwald E Studies on cardiac dimensions in intact, unanesthetized man: IV. Effects of isoproterenol and methoxamine. Circulation 24 186,1964
18. White RI, Criley JM, Lewis KB, Ross RS: Experimental pro- duction of intracavitary pressure differences. Am J Cardiol 19:806, 1967
19. Nelson R, Fey K, Follette DM. The critical importance of intermittent infusion of cardioplegic solution during aortic cross-clamping. Surg Forum 2724, 1976
20. Follette DM, Fey KH, Becker H, et al: Superiority of blood
cardioplegia over asanguineous cardioplegia: experimental and clinic study. Circulation 59,60:Suppl2:11, 1979
Discussion DR. scorn STEWART (Rochester, NY): A little more than a decade ago, my associates undertook a clinical study of LVOT obstruc- tion caused by mitral valve prostheses, and the conclusion of that report continues to influence our choice in the selection of the replacement for the mitral valve. They reviewed the clinical course of 26 patients with isolated mitral valve stenosis who had undergone MVR. Each patient had had an adequate preoperative echocardiogram. The width of the LVOT in the echocardiogram was measured between the ventricular septum above and the anterior leaflet of the mitral valve below at the onset of systole.
Among the 26 patients, 12 had an LVOT greater than 20 mm in width, and 14, an LVOT less than 20 mm in width. Each of the patients in the group of 12 received the Starr-Edwards ball prosthesis. There was a single death in that group. Seven of the patients who had a narrow LVOT also received the same high- profile valve prosthesis, and 5 died, a mortality of 71%. Four of those 5 died of low cardiac output syndrome. In contrast, the remaining 7 patients with a narrowed LVOT received a low- profile disc valve. There was a single death in that group, the result of intraoperative myocardial infarction.
This was an uncontrolled, retrospective clinical study. How- ever, the circumstantial evidence strongly suggested to us that a high-profile valve in an LVOT proved narrow by echocardiog- raphy was a major cause of early operative death. As a result of that study, echocardiography of the LVOT continues to be an important part of our preoperative assessment of patients with mitra valve disease. If an LVOT is less than 20 mm in width, we select a low-profile valve when a reconstructive procedure is not possible. Dr. Jett, did you have the opportunity to examine the LVOT
in your experimental model with echocardiography to visualize the dynamics of the outflow tract obstruction observed?
DR. jm: We did not measure the phasic diameters of the LVOT. We did measure the short-axis midventricular diameters preoperatively by echocardiography when the chest was closed. The mean end-systolic diameter was 25 mm, and the mean end-diastolic diameter was 36 mm. These dimensions correspond to those of a normal human heart from a person of 0.75 mz weighing approximately 15 kg.