Embed Size (px)
Citation preview

Left Anterior Hemiblock Obscuring the Diagnosisof Right Bundle Branch Blockin Acute Myocardial InfarctionSAMUEL SCLAROVSKY, M.D., RUBEN F. LEWIN, M.D.,
BORIS STRASBERG, M.D. AND JACOB AGMON, M.D., F.A.C.C.
SUMMARY Thirty cases in which transient left anterior hemiblock (LAHB) obscured the diagnosis of rightbundle branch block (RBBB) appearing during the first days of an acute myocardial infarction (AMI) arepresented. Twenty-eight of the patients with AMI had a clear septal wall involvement, while the remaining twohad an anterolateral and lateral wall AMI, respectively. These intraventricular conduction defects developed2-120 hours (mean 64.9 ± 26 hours) after the acute event, and persisted for 24 hours to 7 days (mean 63.135 hours).The ECG was characterized by a pure LAHB with wide QRS complexes and the presence of RBBB was
shown by recording high V, and right-sided chest leads. The vectorcardiogram was also useful in several cases.The clinical course of this type of bifascicular block was transient and benign, with an in-hospital mortality
of 6.7%. No patient developed trifascicular or complete atrioventricular block and, therefore, we conclude thatprophylactic installation of a temporary pacemaker is not indicated in this type of bifascicular block. Thepossible role of extracellular potassium released during acute myocardial necrosis in the pathophysiologicalmechanism of these blocks is discussed.
IT IS ACCEPTED that pure left anterior hemiblock(LAHB) increases the QRS duration no more than0.02 second. Thus, a QRS complex longer than 0.10 or0.1 1 second indicates the presence of other complicat-ing factors, such as severe left ventricular hypertrophy(LVH) and focal blocks due to myocardial infarctionand fibrosis or bundle branch block.'"3 LAHB mayobscure the diagnosis of right bundle block (RBBB),abolishing the S waves in lead I, aVL and the terminalR wave in V,.'-We describe 30 cases of acute myocardial infarction
(AMI) in which LAHB obscured the diagnosis ofRBBB, and present the clinical and electrocar-diographic characteristics, evolution and immediateprognosis.
Materials and MethodsFrom 2500 patients admitted to our Intensive
Coronary Care Unit (ICCU) with definite diagnosis ofAMI, 249 patients had LAHB on admission or duringhospitalization. From this group, 30 patients (12%)developed LAHB, obscuring the diagnosis of RBBB.The diagnosis of AMI was established by a history
of severe chest pains, appearance of new pathologicalQ waves and a typical elevation of cardiac enzymes. A12-lead ECG was taken at least once daily during thehospitalization and the position of the precordial leadswas marked on the patient's chest on arrival to theICCU.
From the Israel and lone Massada Center for Heart Disease,Intensive Coronary Care Unit and Institute for Cardiac Rehabilita-tion, Beilinson Medical Center, Petah-Tikva, Israel.
Address for reprints: J. Agmon, M.D., Director, Massada Centerfor Heart Diseases, Beilinson Medical Center, Petah-Tikva, Israel.
Received June 12, 1978; revision accepted January 11, 1979.Circulation 60, No. 1, 1979.
LAHB was defined electrocardiographically asmarked left-axis deviation (LAD) of -300 or more,with a Q,S% pattern and small R waves in leads II, IIIand aVF.4 LAHB obscuring RBBB was also definedaccording to the criteria of Rosenbaum et al.3: 1)LAHB with increased QRS duration without anyother explicatory cause; and 2) a marked terminaldelay oriented slightly to the right in the transverseplane (R' in aVR, S in V5,, R' in high V, or RV,). Thislate vector measured more than 0.02 second. Thepresence of RBBB was confirmed by recording a highV, lead and right-sided chest leads. In several cases,we used vectorcardiographic (VCG) recordings toconfirm the presence of RBBB.3 The study began atthe time of initial appearance of chest pain.We performed statistical analysis using the t test.
ResultsOur findings are summarized in table 1. Of the 30
patients studied, 19 (63%) were male and 11 (27%)female. Age ranged from 32-80 years (mean 59.4years). The AMI location was anteroseptal in 20 pa-tients and anterior wall in eight. Of the other two pa-tients, one developed an anterolateral and the second alateral wall AMI. Nineteen patients (63.3%) had nocardiac symptoms before the onset of the acute event;six were diabetics and five had a duodenal ulcer. Onepatient had hypertension, another had ischemiccerebrovascular disease and a third had severe chronicobstructive lung disease.The frontal QRS axis before the appearance of the
LAHB obscuring RBBB ranged from -45° to + 120°(mean 4.5 ± 38.8). During the presence of LAHBobscuring RBBB, the QRS axis ranged from -30° to-90° (mean -58 ± 17.5) (figs. 1 and 2). In eightpatients, a mean frontal axis of at least -30° was
26
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from

LEFT ANTERIOR HEMIBLOCK OBSCURING RBBB/Sclarovsky et al.
I. R.L3 R L F VI V2>~~~~~~~~~~~~ fleIkiS ;I ,.., . ...
I
\1- (/I-r --r '<-I* 4\ rl
+. ,'.j. ii
20.12 .1,g(o4t :I
... ...1
;...
i. ....... .. .
t p.w
L,
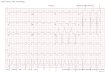
FIGURE 1. Anteroseptal anterior myocardial infarction (first strip) complicated by a transient left anterior hemiblock(LA HB) obscuring right bundle branch block (second strip). Characteristic pattern of disappearance: first the QRS narrows
(third strip), then the LAHB disappears (fourth strip).
present before the appearance of the AMI, but all ofthem had a further left-axis deviation during theLAHB obscuring RBBB (fig. 2). One patient had an
incomplete RBBB. After the disappearance of theLAHB obscuring RBBB, the mean QRS frontal axiswas in the range of 750 to -75° (mean -7 ± 34.7°).The difference between the QRS mean frontal axisbefore and after the appearance and disappearance ofLAHB obscuring RBBB was not statistically signifi-cant (p > 0.05).The QRS complex measured 0.05-0.08 second
(mean 0.066 + 0.009 second) before the LAHBobscuring RBBB; 0.1-0.14 second (mean 0.1110.0097 second) during LAHB obscuring RBBB; and0.06-0.1 second (mean 0.072 ± 0.01 second) afterLAHB obscuring RBBB disappeared. In all patients,QRS duration increased 0.02 second or more duringLAHB obscuring RBBB. The difference of the QRSwidth before the appearance and after the dis-appearance of the LAHB obscuring RBBB wasstatistically significant (p < 0.025).The interval between initial symptoms and the
appearance of the LAHB obscuring RBBB was 2-120hours (mean 64.9 ± 26 hours). The LAHB obscuringRBBB persisted for 24 hours to 7 days (mean 63.1 ±
35 hours). Three patients each developed this type ofconduction defect twice.A commonly observed pattern of disappearance of
the LAHB obscuring RBBB consisted of a narrowingof the QRS in all the cases followed by the dis-appearance of the signs of LAHB in some of them(fig. 2).
In all 30 patients, the demonstration of concealedRBBB was easily obtained with a high V1 recording
(fig. 3), and the VCG gave additional proof of theorigin of the wide QRS (fig. 4). After the QRSnarrowed, it was not possible to show any degree -ofRBBB in unipolar high and right-sided chest leads orin the VCG.
There was no statistically significant differencebetween the heart rates before, during or after theappearance of the LAHB obscuring RBBB (p 0.05).Carotid massage performed in some cases resulted inslowing of the sinus rate without change in the QRSwidth or frontal axis.The in-hospital mortality of this group was 6.7%.
One patient died from cardiogenic shock 96 hoursafter admission to the ICCU and 24 hours after theappearance of the LAHB obscuring RBBB. The sec-ond patient died suddenly, probably from ventricularfibrillation, on the twentieth day of hospitalization.
Apart from pericarditis in two patients and con-gestive heart failure in 10, there were no other com-plications. No patient developed signs of trifascicularblock or complete atrioventricular block.
Discussion
In 1973 Rosenbaum described three cases in whichthe presence of LAHB obscured the diagnosis ofRBBB.3 Another case was described by Heydorn etal.5 Rosenbaum et al.,3 suggested that an increasedQRS duration in the presence of LAHB should be themain clue for suspecting hidden or concealed RBBB;recording additional chest leads one interspace abovethe conventional level or slightly to the right of V1 mayreadily uncover the concealed RBBB (fig. 3). A VCGmay also be helpful in the diagnosis by showing a
L I L2... . I.
';..
17.127O)
18.122945
- j ( ~
19. 127 51
'I; ..
27
--.-t
-.-lI-----I II.- 11
1/,- -- e, .-41-. 1.
- - I--1-1--
I---- 4.--- r. t-- f---
-. --.
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from

VOL 60, No 1, JULY 1979
TABLE 1. Clinical and Electrocardiographic Data of 30Branch Block (RBBB)
Patients with Left Anterior Hemiblock (LAHB) Obscuring Right Bundle
Previous Previous QRS widthSite of cardiac noncardiac (seconds)
Patient Sex Age infarction disease disease B D A
NA F 62 ASW No DI 0.06 0.12 0.08606973
Ex/AnASWASW
57 ASW
5960
32
LWASWASW
69 Ex/An45 ASW48 Ex/An80
50
ASWEx/An
No RAAP DUOMI -No
NoNo
DI/DUDI
No DU/AHNo DUNoNo -
No65 Ex/An OMI69 An/La6363
ASW
ASW
64 ASW
75 ASW71 ASW6872
ASW
ASW59 ASW59 ASW6062
NoO1MI
OMINoNo DINo CVAAPAPNoNo
COPD
Ex/An AP
Ex/An AP
70 ASW
67 Ex/An65 ASW
AP DUNo DI
No -
EJ F 30 ASW No DI 0.06 0.11 0.06
Abbreviations: A = after RBBB; AH = arterial hypertension; An/La = anterolateral wall; AP = angina pectoris; ASW =
anteroseptal wall; B = before RBBB; CHF = congestive heart failure; COPD = chronic obstructive pulmonary disease; CVA =
cerebrovascular accident; D = during RBBB; DI = diabetes mellitus; DU = duodenal ulcer; Ex/An = extensive anterior;LW = lateral wall; No = no previous disease; = old myocardial infarction; RA = rheumatoid arthritis.
marked terminal delay oriented slightly to the right inthe transverse plane (fig. 4). To the best of ourknowledge, such an ECG evolution of LAHB obscur-ing RBBB during the first days of an AMI has notbeen reported.As pointed out by Rosenbaum et al.,3 several other
conditions capable of producing the same ECG find-ing should be excluded: 1) severe left ventricularhypertrophy. This was definitely not present in any ofour patients. 2) Focal blocks (infarction or fibrosis ofthe anterolateral wall of the left ventricle), peri-infarction or intra-infarction block. These terms arenot clearly defined and are used as another ter-
minology for hemiblocks. However, the transientnature of the LAHB obscuring RBBB in our patientsdoes not support the diagnosis of focal blocks, whichseem to be a more permanent phenomenon.6 7 3) InLAHB the passage of the electrical wave from theposterior to the anterior wall may be through the sep-tum; 1, 2 in cases with anteroseptal AMI (28 of ourpatients) the conduction through the septum could bedelayed, causing the wide QRS. However, as shownon the VCG (fig. 4), the actual delay is in the last vec-tor, without the participation of the infarcted septalportion in the last wave front.8 Another characteristicof this group was the typical interval between the onset
VLLSSKSIGRASHALIMFTIURAMFMDJBOBMISVAHIGOKEMGI1SIBPSSSLPB
FM1FFF
M
F
FMF
FMMIFIFF14
0.06
0.060.050.060.08
0.07
0.06
0.08
0.08
0.08
0.060.06
0.06
0.08
0.060.070.060.06
0.070.06
0.060.080.080.080.06
0.080.060.06
0.120.11
0.11
0.11
0.120.10
0.10
0.12
0.10
0.100.120.120.110.140.110.110.13
0.120.110.100.11
0.120.11
0.11
0.10
0.120.100.10
0.10
0.080.060.080.070.070.060.08
0.080.080.060.080.060.080.060.070.080.060.080.060.060.080.080.080.070.08
0.070.06
28 CIRCULATION
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from

LEFT ANTERIOR HEMIBLOCK OBSCURING RBBB/Sclarovsky et al.
TABLE 1. (Continued)
Last vectorMean frontal axis duration in
(degrees) Time of onset Duration "high" V1B D A (hours) (hours) (seconds) Complications
-15 -60 0 48 48 0.04
0.030.050.050.040.03
0.030.04
0.040.02
0.02
0.050.050.030.050.040.030.050.040.03
0.030.03
0.040.03
0.03
0.030.03
0.04
0.04
0.05
CHF
CHF
CHF
CHF
CHF
Cardiogenic shock; death
CHF
CHF; pericarditisLate death; pericarditis
CHF
CHF
of the AMI and the LAHB obscuring RBBB, whichmost of the patients developed after 24-48 hours ofthe hyperacute stage of the AMI.Most of the bifascicular blocks occurring in AMI
tend to appear during the first hours, and are con-sidered to be of ischemic origin. Intraventricular con-duction defects appearing relatively late seem to beless severe and their mortality is lower.9The pathophysiology of these late blocks is still un-
clear. Jackrel et al.10 reported that irreversibleatrioventricular conduction disturbances after ligationof the anterior septal artery are caused by the presenceof total cross-sectional necrosis of the His bundle, andthat reversible atrioventricular conduction distur-bances are caused by the effect of increased ex-tracellular potassium released by necrotic myocardial
cells on viable conducting fibers. The distal His bundleand proximal bundle branches are more susceptible tothe depolarizing effect of extracellular potassium thanthe more proximal conducting tissue. The potassiumrelease from necrotic myofibers is greatest 24 hoursafter the AMI and the necrotic area gradually losespotassium until the fourth day after the AMI. Thisphenomenon has been described by Hackel and co-workers.'1 The transient nature of these blocks may beexplained on the basis of this pathophysiologicalmechanism and, therefore, they may be considered as
metabolic blocks.The mortality in our series (6.7%) is relatively low,
even lower than the mortality reported with acuteLAHB alone.'2-14 This is in agreement with therelatively lower mortality observed in transient late
30450
-15-30
0
60
30-45-4560
-3060
-30
0
0
-15-30-30
0
30-30-15120
60
-1500
-15
-75-30-60-45-75-90
-45
-90-90
-75-75-90-60
-45
-60
-45-45-60-45-45-30-45-45-60-45-45-45-60-60
3000
-30-3045
-30-75-30-3045750
-30
00
0
-45-30-4560
-450
-15-45-30
15300
722
84644848
3672
104721203672
48
727296
4848
48
72367296
7296
1083648
7296797224
24
969624
96489648
168724512024
4224
72964824
4824
24
7272
29
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from

VOL 60, No 1, JULY 1979
bifascicular blocks9 and in contrast to the considerablyhigher mortality of the bifascicular blocks appearingearly in the course of AMI.'2 '4 These findings supportthe assumption that LAHB obscuring RBBB is benignand has a better prognosis than other types of acuteblocks appearing in the early phase of AMI. Further-more, because of the lack of progression to
MG25- 1-76
L I
26-1-76730
-t -a- --t----t- -tItt
141-4-
26-1 76 27-1-76 31-1-%14°Q 730 740
4----iT--.i...... ...
L 2 t~
R~~ ~~~ _: :iI.
L $ > = - < - t ~~~~I-
.........
_ 4 --- ----------
.....I
V th let.
V44t,
repreKsenting left anterior hemiblock (LA H8B) obscuring
right bundle branch block (P888). In thefifth strip, LAHBper.siKsts while the has di.sappeared (narrow QRS).
P.B. E.J.
VI normal
;- / V 1
>.r\qj ,11 -,^VI high
VI low
FIGURE 3. Right bundle branch block. The precordial leadis located one interspace above the normal V1 (V1 high) intwo patients.
trifascicular block (bifascicular block and PRprolongation) or complete atrioventricular block andthe transient nature of these blocks, prophylacticpacemaker installation is not indicated in these cases.
FIGURE 4. Vectorcardiogram (VCG) in a patient with leftanterior hemiblock (LA HB) obscuring right bundle branchblock (PRBB) showing: top) anterior wall infarction withnormal axis without RBBB; center) 36 hours later,appearance of LAHB (frontal (F) plane) and terminal slowvector slightlv oriented to the right (horizontal (H) plane)compatible with RBBB; bottom) LAHB and RBBB dis-appear. S = sagittal plane.
30 CIRCULATION
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from

LEFT ANTERIOR HEMIBLOCK OBSCURING RBBB/Sclarovsky et al.
.. -- -L I:1:: i
VI ' High"
VI"' Normal"
:
- r - e -2eII- II1 I 1 i-I i----4- --I ----t1T1'
+ -l' ~~~I ' -ss-IIj --- - -_-_ _ ___tl----- l-t-I~-~----------_~~1..- -_I-,ii___ _
~~~~- ]-t _- lj;_
- ::1-1 -.1.-1 1:111111 i ix IIitHz
FIGURE A1. Normal and high V1 recorded simultaneously in a patient with left anterior hemiblockobscuring right bundle branch block.
Addendum
Since the manuscript was submitted we haveobserved four additional cases of LAHB obscuringRBBB. One of the patients was studied withsimultaneous two- and three-channel ECGs. Normaland high V1 were recorded simultaneously, showingfrom the fifth beat a shift of the QRS width and ter-minal left-superior forces obscuring RBBB. No R'wave was observed before the QRS of the fifth beat
VI
V3
V6
(fig. A1). Simultaneous precordial leads V1, V3, Vffwere also recorded (fig. A2). The first beat shows awide QRS with a terminal S wave in VB; the secondand third beats show a narrowed QRS without thecharacteristic pattern of LAHB obscuring RBBB. Thefourth and fifth beats show RBBB again and then theblock disappears. There is no differences in PR or RRintervals during the appearance or the disappearanceof LAHB obscuring RBBB. The same ECG picturewas noted in all leads.
.1; 1- 1 :1 -..1::1 .1.- 1.:.1'X W 1---- --- --'-X'''- --.1: :1 I ' 1 [--1- 1 - 1 -: -1---1 -- 1 1-- 1 -:1- -t S i -'-1'' 1: .1.':'1''.1':'1. '''''. 11.1:-::
OP __a- [---- 1- - i l l l l l l 1-0 7
.....
::: t: t _ ~ ~ ~ ~ ~ ~ ~ ~ ~~~~~.. ----l:::::::l:::::::+:: :: :---- -- --} --.-+- ,
f t~~~~~~~~~~~~~~~~~~~~~-- -t11 i11 ; 3---
, t l {- - t t ... .....t..:.1:: ........
-l--- ---- .lt-tSh-l--S-ltl~~~~~~~........ :t1 ; 1,1 .-.1 ...1. -, '. .. - .. - 1- 1:_IGR A2Sa p
FIGURE A2. Simultaneous precordial leads V,. V3 and V6, from the same patient as in figure Al.-
I
3 1
I hL_I 7 v
I: J:
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from

CIRCULATION
References
1. Rosenbaum MB, Elizari MV, Lazzari JO: Los Hemibloqueos.Buenos Aires, Paidos, 1968
2. Rosenbaum MB, Elizari MV, Lazzari JO: The Hemiblocks.Oldsmar, Florida, Tampa Tracings, 1970
3. Rosenbaum MB, Yeshuron J, Lazzari JO, Elizari MV: Leftanterior hemiblock obscuring the diagnosis of right bundlebranch block. Circulation 48: 298, 1973
4. Rosenbaum MB: The hemiblocks: diagnostic criteria andclinical significance. Mod Concepts Cardiovasc Dis 39: 141,1970
5. Heydorn WH, Nelson WP, Fitterer JD, Floyd GD, Strevey TE:Congenital aneurysm of the sinus of Valsalva protruding intothe left ventricle. J Thorac Cardiovasc Surg 71: 839, 1976
6. Grant RP: Clinical Electrocardiography. The Spatial VectorApproach. New York, McGraw-Hill, 1957
7. Shadaksharappa KS, Kalbfleisch JM, Conrad LL, Sarkar NK:Recognition and significance of intraventricular block due tomyocardial infarction (peri-infarction block). Circulation 37:
VOL 60, No 1, JULY 1979
20, 19688. Witham CA: A System of Vectocardiographic Interpretation.
Chicago, Year Book Medical Publishers Inc, 1975, ch 99. Lie KI, Wellens HJ, Schuilenburg RM, Becker AE, Durrer D:
Factors influencing prognosis of bundle branch block com-
plicating acute anteroseptal infarction. Circulation 50: 935,1974
10. Jackrel J, Miller JA, Schechter FG, Minkowitz S, Stuckey JH:Atrioventricular conduction following ligation of the anteriorseptal artery in the dog. Am J Cardiol 25: 552, 1970
11. Hackel DB, Wagner G, Ratlif NB, Cies A, Estes EH Jr.:Anatomic studies of the cardiac conduction system in acutemyocardial infarction. Am Heart J 83: 77, 1972
12. Col JJ, Weinberg SL: The incidence and mortality of intra-ventricular conduction defects in acute myocardial infarction.Am J Cardiol 29: 344, 1972
13. Gann D, Balachandran PK, Sherif NE, Samet P: Prognosticsignificance of chronic versus acute bundle branch block inacute myocardial infarction. Chest 67: 298, 1975
14. Basualdo CAE, Haraphongse M, Rossall RE: Intraventricularblocks in acute myocardial infarction. Chest 67: 75, 1975
32
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from

S Sclarovsky, R F Lewin, B Strasberg and J Agmonmyocardial infarction.
Left anterior hemiblock obscuring the diagnosis of right bundle branch block in acute
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1979 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.60.1.26
1979;60:26-32Circulation.
http://circ.ahajournals.org/content/60/1/26the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from