-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
1/75
CALCIUM AND BONECALCIUM AND BONE
METABOLISMMETABOLISM
LECTURE 8LECTURE 8
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
2/75
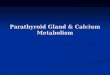
ParatParathyrhyroidoidglandsglands
Four pFour pea-sized glandsea-sized glands
located posterior to thelocated posterior to thethyroid
lobes.thyroid lobes.
They secrete PTH , thatThey secrete PTH , thatplays a major role
inplays a major role in
bonebone remoderemodelllingling
andandcalciumcalciumhomeostasis.homeostasis.
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
3/75
CalciumCalciumCalcium ions play a critical role in
intracellularCalcium ions play a critical role in intracellular
and extracellular eventsand extracellular events
Roles of calciumRoles of calcium::
Skeletal strengthSkeletal strength
euromuscular conductioneuromuscular conduction
Excitation! contraction coupling"Excitation! contraction
coupling"
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
4/75
Role of #T$Role of #T$ #T$ prevents serum calcium from
falling#T$ prevents serum calcium from falling
%y stimulating calcium movement from:%y stimulating calcium
movement from: &ntestinal lumen&ntestinal lumen
renal tu%ular lumenrenal tu%ular lumen 'one fluid
compartment'one fluid compartment
into the %loodinto the %lood
(irect(irecteffects oneffects on %one and kidney%one and kidney
&ndirect&ndirect effects oneffects on
intestineintestine)mediated %y)mediated %y
vitamin (*vitamin (*
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
5/75
Cellular effects of +itamin (Cellular effects of +itamin (
Stimulates calcium and phosphate a%sor%tion fromStimulates
calcium and phosphate a%sor%tion fromthe intestinethe intestine
Regulates %one resor%tion and formationRegulates %one resor%tion
and formation
(ecreases calcium rea%sor%tion in the distal renal(ecreases
calcium rea%sor%tion in the distal renal
tu%ulestu%ules
Represses the transcription and secretion of #T$Represses the
transcription and secretion of #T$
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
6/75
Role of calcitoninRole of calcitonin
#revents a%normal increase in serum Ca and#revents a%normal
increase in serum Ca and
phosphate concentrationphosphate concentration (ecreases %one
resor%tion(ecreases %one resor%tion inhi%its renal tu%ular calcium
rea%sor%tioninhi%its renal tu%ular calcium rea%sor%tion Uncertain
effect on vit ( meta%olism and intestinalUncertain effect on vit (
meta%olism and intestinal
a%sorption of calciuma%sorption of calcium ,ay %e considered as
a counteregulator of #T$,ay %e considered as a counteregulator of
#T$
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
7/75
#-T$.L./&C-L C.(&T&.S#-T$.L./&C-L
C.(&T&.S
$0#ERC-LCE,&-$0#ERC-LCE,&-
$0#.C-LCE,&-$0#.C-LCE,&-
.STE.#.R.S&S.STE.#.R.S&S
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
8/75
$0#ERC-LCE,&-$0#ERC-LCE,&-
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
9/75
Causes:Causes:,alignancy:,alignancy:
,ultiple myeloma,ultiple myeloma
'ony metastases'ony metastases
LymphomaLymphoma
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
10/75
Causes:Causes:Increased bone resorbtion:Increased bone
resorbtion:
HyperparatiroidismHyperparatiroidism
Hypercalcemia in parathyroid cancersHypercalcemia in parathyroid
cancers
HyperthyroidismHyperthyroidism
PheochromocytomaPheochromocytoma
ImmobilizationImmobilization
Vitamina into!icationVitamina into!ication
ddison"s diseaseddison"s disease
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
11/75
Causes:Causes:Increased renal reabsorption or decreased renal
elimination:Increased renal reabsorption or decreased renal
elimination:
Rha%domyolysisRha%domyolysis
Thiazide diureticsThiazide diuretics
#enal $ailure#enal $ailure
Heart $ailureHeart $ailure
%ithium carbonate%ithium carbonate
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
12/75
Causes:Causes:Increased intestinal absorbtion:Increased
intestinal absorbtion:
Vitamina & into!icationVitamina & into!ication
'arcoidosis and other granulomatous diseases'arcoidosis and
other granulomatous diseases
TuberculosisTuberculosis
%ymphomas%ymphomas
I&'I&'
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
13/75
$yperparathyroidism$yperparathyroidism
Increased autonomous production of PTH-Increased autonomous
production of PTH-primary hyperparathyroidismprimary
hyperparathyroidism
Increased PTH production as response toIncreased PTH production
as response toprolonged hypocalcemia -prolonged hypocalcemia -
secondarysecondaryhyperparathyroidismhyperparathyroidism (feedback
control is(feedback control ismaintained)maintained)
Autonomous secondary hyperparathyroidism -Autonomous secondary
hyperparathyroidism -tertiary hyperparathyroidismtertiary
hyperparathyroidism
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
14/75
#athology#athology 812 single adenoma812 single adenoma
342 parathyroid hyperplasia342 parathyroid hyperplasia
isolatedisolated
associated with other endocrine abnormalities:associated with
other endocrine abnormalities:
ultiple endocrine neoplasia (!"# types I and II)ultiple
endocrine neoplasia (!"# types I and II)
$% parathyroid carcinoma$% parathyroid carcinoma
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
15/75
,E,E
,E &,E & ,E &&a,E &&a ,E &&%,E
&&%An autosomalAn autosomal
dominant conditiondominant condition
&haracteri'ed by:&haracteri'ed by:
ParathyroidParathyroid
tumourstumours
hyperplasiahyperplasia
Anterior pituitaryAnterior pituitary
adenomaadenoma
PancreaticPancreatic
neuroendocrineneuroendocrine
tumourstumours
An autosomalAn autosomal
dominant conditiondominant condition
&omprises:&omprises:
amilialamilial
medullary thyroidmedullary thyroid
carcinomacarcinoma
PheocromocytomPheocromocytom
aa
ParathyroidParathyroid
tumourstumours
de*ned by thede*ned by the
association of:association of:
edullary thyroidedullary thyroid
carcinomacarcinoma
PheochromocytomaPheochromocytoma
ultiple mucosalultiple mucosalneuromasneuromas
HyperparathyroidismHyperparathyroidism
(parathyroid(parathyroid
hyperplasia)hyperplasia)
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
16/75
Skin and tongue neuromas in ,E syndromeSkin and tongue neuromas
in ,E syndrome
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
17/75
Clinical featuresClinical features ,ost patients are
asymptomatic,ost patients are asymptomatic
5eatures of hypercalcemia5eatures of hypercalcemia
Target organ damage:Target organ damage: 'one'one
6idneys6idneys 7oints7oints /astrointestinal/astrointestinal
6id6id '' // t . h.th
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
18/75
6idneys6idneys 'one'one /astro!/astro!intestinalintestinal
.ther.ther
+enal calculi+enal calculi
"efrocalcinos"efrocalcinos
is- lessis- less
fre,uentfre,uent
+enal+enal
impairment-impairment-
*nal stage*nal stage
IncreasedIncreasedosteoclast actiityosteoclast actiity
and decreasedand decreasedosteoblast actiityosteoblast
actiity
.steoporosis-.steoporosis-a/ects all sites#a/ects all sites#but
predominantbut predominant
loss is inloss is inperipheral corticalperipheral
corticalbonebone
.steitis *brosa.steitis *brosacystica - less thancystica - less
than
$0% of patients$0% of patients&linical:&linical:
-bone painbone pain
-pathologicpathologicfracturesfractures
-bonebonedeformationdeformation
-norexia-norexia
+omiting+omiting
ConstipationConstipation
-%dominal pain-%dominal pain
&ntestinal calculi&ntestinal calculi
#ancreatitis#ancreatitis
,uscle eakness,uscle eakness
Lethargy9 fatigue9Lethargy9 fatigue9depression9
difficultydepression9 difficultyin concentration andin
concentration andpersonality changespersonality changes
-rticular-rticularmanifestationsmanifestations)pseudogout*)pseudogout*
(ental(entalmanifestationsmanifestations
)dental cavities*)dental cavities*
Salivary duct calculiSalivary duct calculi
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
19/75
1one deformation2pinal compression
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
20/75
2aliary duct calculi
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
21/75
ultiple caities# edentations3
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
22/75
Radiologic findingsRadiologic findings
Su%periostal resorption of cortical %one9 %est seenSu%periostal
resorption of cortical %one9 %est seen:: in high! resolution films
of the phalanges orin high! resolution films of the phalanges or in
the skull9 creating ain the skull9 creating a
salsalt!t!andand!!pepperpepper;;appearenceappearence
.steoporosis.steoporosis! predominant loss of cortical
%onepredominant loss of cortical %one
! the mass and the mechanical strength of the tra%ecular %one
arethe mass and the mechanical strength of the tra%ecular %one
arerelatively maintainedrelatively maintained
(ental x!ray ! loss of lamina dura of the teeth(ental x!ray !
loss of lamina dura of the teeth
#lain a%dominal radiograph for renal stones )for prognostic
reasons*#lain a%dominal radiograph for renal stones )for prognostic
reasons*
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
23/75
Bone resorptionBone resorption
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
24/75
Bone resorptionBone resorption
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
25/75
Bone resorptionBone resorption
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
26/75
ormal %one $yperparathyroid
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
27/75
Bone resorption in the skullBone resorption in the skull
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
28/75
'one resorption in the skull'one resorption in the skull
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
29/75
Loss of lamina dura of theLoss of lamina dura of the
teethteeth
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
30/75
"oninasie methods to estimate bone"oninasie methods to estimate
bone
mineral density:mineral density:
- 45A (dual-energy 6- ray- 45A (dual-energy 6- ray
absorptiometry)absorptiometry)
- 5- ray- 5- ray
- bone scanning- bone scanning
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
31/75
#articular clinical forms#articular clinical forms
#regnancy#regnancy ChildrenChildren ElderlyElderly
2pontaneous2pontaneous
abortionabortion
Increased riskIncreased risk
of perinatalof perinataldeathdeath
- intense bone- intense bone
modi*cationsmodi*cations
- decreaseddecreasedperformance in schoolperformance in
school
-personality changespersonality changes
ainly neurologicalainly neurological
symptomssymptoms
- lethargy- lethargy
- confusion#- confusion#
depressiondepression
-dyspepsia# nausea#-dyspepsia# nausea#dehydrationdehydration
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
32/75
La%oratory findingsLa%oratory findings
Hypercalcemia - both total and ioni'ed calcium areHypercalcemia
- both total and ioni'ed calcium areeleatedeleated
2erum phosphorus leel is: low-normal or low2erum phosphorus leel
is: low-normal or low
HyperchloremiaHyperchloremia metabolic acidosismetabolic
acidosis
!leation of the alkaline phosphatase leel!leation of the
alkaline phosphatase leel
HypomagnesemiaHypomagnesemia
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
33/75
&maging studies&maging studies
77Tc- sestamibi scanning77Tc- sestamibi scanning
"on- inasie:"on- inasie:
- &T- &T
- +I- +I
- 8ltrasound- 8ltrasound
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
34/75
#arathyroid adenoma#arathyroid adenoma
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
35/75
#arathyroid adenoma#arathyroid adenoma
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
36/75
#arathyroid adenoma
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
37/75
TreatmentTreatment
3"SUR/ER0 )parathyroidectomy*3"SUR/ER0 )parathyroidectomy*
Removal of the adenomaRemoval of the adenoma &f there is
parathyroid hyperplasia! < = gland are removed9 leaving a&f
there is parathyroid hyperplasia! < = gland are removed9 leaving
a
remnant tissue sufficient to prevent hypocalcemiaremnant tissue
sufficient to prevent hypocalcemia
The recurence rate of hypercalcemia is high in pacients ith
parathyroidThe recurence rate of hypercalcemia is high in pacients
ith parathyroid
hyperplasia )especially in those ith one of the ,E
syndromes*hyperplasia )especially in those ith one of the ,E
syndromes* &n such cases the remnant parathyroid can %e removed
from the neck&n such cases the remnant parathyroid can %e
removed from the neck
and implanted in forearm musclesand implanted in forearm
muscles
Complications:Complications:
(amage to the recurent laryngeal nerve(amage to the recurent
laryngeal nerve &nadvertent removal or devitali>ation of all
parathyroid tissue9 producing&nadvertent removal or
devitali>ation of all parathyroid tissue9 producing
permanent hypoparathyroidism"permanent hypoparathyroidism"
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
38/75
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
39/75
TreatmentTreatment
&ndications for surgery:&ndications for surgery:! serum
Ca markedly elevated )?339@! 3@mgAdl*! serum Ca markedly elevated
)?339@! 3@mgAdl*
! previous episode of life!threatening hypercalcemia! previous
episode of life!threatening hypercalcemia
! creatinine clearance BD2 than normal! creatinine clearance BD2
than normal! renal lithiasis! renal lithiasis
! urinary calcium markedly elevated! urinary calcium markedly
elevated)?4DDmgA@4h*)?4DDmgA@4h*
! %one mass is su%stantially reduced! %one mass is su%stantially
reduced
! young pacient )B1D years*! young pacient )B1D years*
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
40/75
TreatmentTreatment@" ,edical treatment in@" ,edical treatment
in
hyperparathyroidism:hyperparathyroidism:
! prior to surgery! prior to surgery
! inopera%le cases or refusal of surgery! inopera%le cases or
refusal of surgery
! parathyroid crisis! parathyroid crisis
! tumoral hypercalcemia! tumoral hypercalcemia
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
41/75
$ypercalcemia treatement$ypercalcemia treatement&nitial
management:&nitial management: +igourous
rehydratation:+igourous rehydratation:
Saline
Restore renal functionRestore renal function
Chronic therapyChronic therapy
&ntravenous %isphosphonates )pammidronate or >oledronic
acid*! inhi%it osteoclast&ntravenous %isphosphonates
)pammidronate or >oledronic acid*! inhi%it osteoclast%one
resorption%one resorption normalisation of Ca levelsnormalisation
of Ca levels
Calcitonin! synthetic salmon calcitonin )antiresorptive
agent*Calcitonin! synthetic salmon calcitonin )antiresorptive
agent*
/lucocorticoids in high doses:/lucocorticoids in high doses:
(ecrease renal Ca elimination(ecrease renal Ca elimination
&nhi%it a series of osteolithic factors&nhi%it a series of
osteolithic factors -re the first line of treatment for
hypercalcemia in patients ith multiple mieloma9-re the first line
of treatment for hypercalcemia in patients ith multiple
mieloma9
lymphoma9 sarcoidosis or intoxication ith vitamin (A -"lymphoma9
sarcoidosis or intoxication ith vitamin (A -"
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
42/75
$0#.C-LCE,&-$0#.C-LCE,&-
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
43/75
CausesCauses
$ypoparathyroidism$ypoparathyroidism (ecreased vit ((ecreased
vit (levelslevels
(iminished Ca release(iminished Ca releasefrom %onefrom %one
Circulating CaCirculating Cacomplexioncomplexion
(estruction of parathyroid(estruction of
parathyroidglands:glands:
-utoimmune-utoimmunesurgicalsurgicalRadiationRadiation&nfiltration&nfiltrationfailure
of parathyroidfailure of parathyroiddevelopment
)(i/eorgedevelopment )(i/eorgesyndrome*syndrome*deposition of
metals )iron9deposition of metals )iron9copper9 aluminium*copper9
aluminium*
Resistance to #T$ action:Resistance to #T$
action:pseudohypoparathyroidismpseudohypoparathyroidismrenal
insufficencyrenal insufficencymedications that %lockmedications
that %lockosteoclastic %one resorptionosteoclastic %one
resorption)calcitonin9 %isphosphonates)calcitonin9
%isphosphonates**
+itamin (+itamin (deficiencydeficiency
-cute-cute
pancreatitispancreatitis
-cute systemic-cute systemicillnessillness
$ereditary$ereditaryvitamin (!vitamin (!
dependent ricketsdependent rickets)type 3 and @*)type 3 and
@*
.steomalacia.steomalacia
&nhi%ition of %one&nhi%ition of
%oneresorptionresorption
&ncreased uptake&ncreased uptakeof calcium intoof
calcium into%one: osteo%lastic%one: osteo%lasticmetastases9
hungrymetastases9 hungry%one syndrome%one syndrome
&ncreased al%umin&ncreased al%uminin alcalosisin
alcalosis
-cute pancreatitis-cute pancreatitis)a%normal #T$ and)a%normal
#T$ and
vitamin (vitamin (meta%olism*meta%olism*
#hosphate infusion#hosphate infusion
Rapid tumor lysisRapid tumor lysisCrush inFury ithCrush inFury
ithmyonecrosismyonecrosis
,ultiple %lood,ultiple %loodtransfusion!transfusion!complexing
%y citratecomplexing %y citrate
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
44/75
Clinical featuresClinical featuresNeuromuscular
manifestationsNeuromuscular manifestations Other
manifestationsOther manifestations
ParesthesiasParesthesiasNumness an! tin"lin" aroun! the mouth#
in theNumness an! tin"lin" aroun! the mouth# in thefin"er tips# in
the feetfin"er tips# in the feet
Tetan$Tetan$
The tetan$ attack e"ins %ith pro!romalThe tetan$ attack e"ins
%ith pro!romalparesthesias follo%e! $ spasms of the muscles
ofparesthesias follo%e! $ spasms of the muscles ofthe
e&tremities an! facethe e&tremities an! face
'$per(entilation'$per(entilation
Patients ma$ h$per(entilatePatients ma$ h$per(entilate
h$pocapniah$pocapnia alkalosisalkalosis
%orsen h$pocalcemia )increase! in!in" of ionic Ca to%orsen
h$pocalcemia )increase! in!in" of ionic Ca to
plasma proteins*plasma proteins*
A!rener"ic s$mptomsA!rener"ic s$mptoms
An&iet$# tach$car!ia# s%eatin"# pallorAn&iet$#
tach$car!ia# s%eatin"# pallor
Con(ulsionsCon(ulsionsMuch more common in $oun"+ t%o t$pes,Much
more common in $oun"+ t%o t$pes,
-enerali.e! form of tetan$+-enerali.e! form of tetan$+
T$pical epileptiform sei.ure )%ith EE- chan"es*T$pical
epileptiform sei.ure )%ith EE- chan"es*
Latent tetan$ si"ns )Ch(ostek/s si"n# Trousseau/s si"n*Latent
tetan$ si"ns )Ch(ostek/s si"n# Trousseau/s si"n*
E&trap$rami!al si"ns )classic parkinsonism* 0 in
patientsE&trap$rami!al si"ns )classic parkinsonism* 0 in
patients%ith chronic h$pocalcemia%ith chronic h$pocalcemia
Posterior lenticular cataractPosterior lenticular
cataractPro!uces total opacit$ of thePro!uces total opacit$ of
thelens )in opposition to senilelens )in opposition to
senilecataract %hich islimite! to acataract %hich islimite! to
ase"ment of the lens *+ treatin"se"ment of the lens *+
treatin"h$pocalcemia halts theh$pocalcemia halts
thepro"ressionpro"ression
Car!iac manifestationsCar!iac manifestations
Prolon"ation of 1T# resistanceProlon"ation of 1T# resistanceto
!i"italis# h$potension#to !i"italis# h$potension#refractor$ C'2
%ithrefractor$ C'2 %ithcar!iome"al$car!iome"al$
Dental manifestationsDental manifestations
Anormalities in enamelAnormalities in
enamelformationformation
Dela$e! 3 asent !ental eruptionDela$e! 3 asent !ental
eruption
Anormal root formationAnormal root formation
Malasorption s$n!romeMalasorption s$n!rome
Steatorrhea in lon"4stan!in"Steatorrhea in
lon"4stan!in"untreate! !iseaseuntreate! !isease
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
45/75
TrousseauGs signTrousseauGs sign
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
46/75
La%oratory findingsLa%oratory findings
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
47/75
La%oratory findingsLa%oratory findings
$$yypocalcemiapocalcemia)B39D mmolAl*)B39D mmolAl*
$$yyperperphphososphphoremiaoremia)?39D mmolAl*)?39D mmolAl*
,agnesiu,agnesiumm levels! normalA lolevels! normalA lo
#T$ level:#T$ level: Lo in true hypoparathyroidismLo in true
hypoparathyroidism
Elevated in pseudo!hypoparathyroidismElevated in
pseudo!hypoparathyroidism
ormal in pseudo!pseudo!hypoparathyroidismormal in
pseudo!pseudo!hypoparathyroidism
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
48/75
$ypoparathyroidism$ypoparathyroidismCausesCauses:: Surgical
removal of the parathyroid glands ! the most commonSurgical removal
of the parathyroid glands ! the most common
cause )surgery of the neck*"cause )surgery of the neck*"
Hdiopathic hypoparathyroidism! polyglandular
endocrinopathiesHdiopathic hypoparathyroidism! polyglandular
endocrinopathies)adrenal insufficiency*)adrenal insufficiency*
5amilial hypoparathyroidism! uncommon5amilial
hypoparathyroidism! uncommon
(i/eorge syndrome:(i/eorge syndrome: (ysmorphia(ysmorphia
Cardiac deffectsCardiac deffects &mmune
defficiency&mmune defficiency
$ypoparathyroidism$ypoparathyroidism
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
49/75
#seudohypoparathyroidism#seudohypoparathyroidism &t is a
herita%le disorder&t is a herita%le disorder
Target organs unresponsive to #T$Target organs unresponsive to
#T$
Caracteri>ed %y:Caracteri>ed %y: $ypocalcemia$ypocalcemia
$yperphosphoremia$yperphosphoremia Elevated #T$ levelsElevated #T$
levels
Characteristic somatic phenotype knon asCharacteristic somatic
phenotype knon as Alri"ht/sAlri"ht/shere!itar$
osteo!$stroph$here!itar$ osteo!$stroph$
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
50/75
#seudo!pseudo!#seudo!pseudo!hypoparathyroidismhypoparathyroidism
Skeletal defectsSkeletal defects
o la%oratory a%normalitieso la%oratory a%normalities
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
51/75
Skeletal !efects5 Alri"ht/sSkeletal !efects5 Alri"ht/s
here!itar$ osteo!$stroph$here!itar$ osteo!$stroph$
Short statureShort stature
Round faceRound face
Short neckShort neck
'rachydactyly )short digits*'rachydactyly )short digits*
Shortened metatarsals! most often the fourth and fifthShortened
metatarsals! most often the fourth and fifth
Su%cutaneous ossificationsSu%cutaneous ossifications
Reduced intelligenceReduced intelligence
Con!itionCon!ition ClinicalClinical PT'PT' CaCa PP 6it D6it D
-enetic-enetic
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
52/75
Con!ition Clinicalaspectaspect
PT' Ca P 6it D -enetic
'$poparath$roi!ism'$poparath$roi!ism NN LL LL '' LL NN
Pseu!oh$poPTPseu!oh$poPT
t$pe 7at$pe 7a
SkeletalSkeletal!efects!efects
'' LL '' LL -enetic-enetic!efect from!efect from
mothermother
Pseu!oh$poPTPseu!oh$poPT
t$pe 7t$pe 7
NN '' LL '' LL -enetic-enetic!efect from!efect from
mothermother
Pseu!oh$poPTPseu!oh$poPT
t$pe 8t$pe 8 NN
''
LL
''
LL
99
Pseu!opseu!oh$poPseu!opseu!oh$poparath$roi!ismparath$roi!ism
SkeletalSkeletal!efects!efects
NN NN NN NN -enetic-enetic!efect from!efect from
fatherfather
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
53/75
#seudohypoparathyroidism I clinical
features#seudohypoparathyroidism I clinical features
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
54/75
#seudohypoparathyroidism#seudohypoparathyroidism
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
55/75
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
56/75
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
57/75
Calcifications in the %rain! CT imageCalcifications in the
%rain! CT image
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
58/75
$ypocalcemia treatment$ypocalcemia treatment
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
59/75
Acute h$pocalcemia treatmentAcute h$pocalcemia treatment -im: to
prevent laryngeal stridor and convulsions-im: to prevent laryngeal
stridor and convulsions #atent airay is assured#atent airay is
assured
&ntravenous calcium gluconate 3D!@DmL )JDmg calciumA3Dml*9
given sloly&ntravenous calcium gluconate 3D!@DmL )JDmg
calciumA3Dml*9 given sloly)maximum 3DmLAmin*)maximum 3DmLAmin*
#lasma calcium levels checked regularly and the infusion rate
adFustedK target#lasma calcium levels checked regularly and the
infusion rate adFustedK target
level: "1!JmgAdLlevel: "1!JmgAdL Caution in pacients taking
digitalis )EC/ monitoring reMuired* Caution in pacients taking
digitalis )EC/ monitoring reMuired*
+itamin ( should %e initiated as soon as possi%leK+itamin (
should %e initiated as soon as possi%leK
Nhen possi%le9 oral calcium is given )@DDmg every @ hoursK
gradually increasing toNhen possi%le9 oral calcium is given )@DDmg
every @ hoursK gradually increasing to1DDmg every @ hours*K if
serum calcium level falls %elo "1mgAdL9 intravenous1DDmg every @
hours*K if serum calcium level falls %elo "1mgAdL9 intravenous
administration is restartedadministration is restarted
-nticonvulsive agents )pheno%ar%ital* may %e helpful in patients
ith convulsionsK-nticonvulsive agents )pheno%ar%ital* may %e
helpful in patients ith convulsionsK
#henothia>ine drugs )chlorproma>ine* should %e avoided I
they may induce severe#henothia>ine drugs )chlorproma>ine*
should %e avoided I they may induce severedyskinesiadyskinesia
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
60/75
Chronic h$pocalcemia treatmentChronic h$pocalcemia treatment
.ral calcium in a dose of 3"1 !
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
61/75
OSTEOPO:OSISOSTEOPO:OSIS
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
62/75
-symptomatic reduction in the Muantity of %one-symptomatic
reduction in the Muantity of %one
&ts presence is not usually appreciated until minimal&ts
presence is not usually appreciated until minimaltrauma causes a
fractureKtrauma causes a fractureK
,ost common sites of osteoporotic fractures:,ost common sites of
osteoporotic fractures: #roximal femur#roximal femur (istal radius
)CollesG fracture*(istal radius )CollesG fracture*
+erte%ral+erte%ral $umerus$umerus Ri%sRi%s #elvis#elvis
$ypogonadism$ypogonadism #remature menopause#remature
menopause
, l h di, l h di
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
63/75
,ale hypogonadism,ale hypogonadism
Lo estrogensAamenorrheaLo estrogensAamenorrhea
HyperprolactinemiaHyperprolactinemiaanore!ia ner(osaanore!ia
ner(osa
athletic amenorrheaathletic amenorrhea
Endocrine disordersEndocrine disorders )ushing"s
syndrome)ushing"s syndrome*H de$iciency*H de$iciency
hyperparathyroidismhyperparathyroidism
acromegaly +ith hypogonadismacromegaly +ith hypogonadism
hyperthyroidismhyperthyroidism
/& disorders/& disorders alabsorptionalabsorption
*astrectomy*astrectomy
(rugs(rugs Systemic corticoids )?< months*Systemic corticoids
)?< months*
Chemotherapy )gonadal damage*Chemotherapy )gonadal
damage*-nticonvulsivants-nticonvulsivants-romatase inhi%itors for
%reast cancer-romatase inhi%itors for %reast cancer
utritionalutritional calcium or vitamin ( deficitcalcium or
vitamin ( deficitsmoking9 alcohol9 coffesmoking9 alcohol9
cofferestrictive dietsrestrictive diets
/enetic/enetic
.ther.ther &mmo%ili>ation&mmo%ili>ationincreased
phisical activityincreased phisical activity
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
64/75
,easurement of %one mass,easurement of %one mass
The most accurate and used method isThe most accurate and used
method isdual energy O!ray a%sorptiometry )(EO-*9dual energy O!ray
a%sorptiometry )(EO-*9ith the loest radiation exposure"ith the
loest radiation exposure"
,easurements of spine and hip %one,easurements of spine and hip
%onemass are the %est predictors of fracturemass are the %est
predictors of fractureriskrisk
Reading a %one densitometryReading a %one densitometry
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
65/75
Reading a %one densitometryReading a %one
densitometryreportreport
T! score: compares patientGs %one mass toT! score: compares
patientGs %one mass toyoung normal su%Fects %one massyoung normal
su%Fects %one mass
P! score: compares patientGs %one mass toP! score: compares
patientGs %one mass toage! matched normal su%Fects"age! matched
normal su%Fects"
',( )%one mineral density*: the actual',( )%one mineral
density*: the actual%one density value expressed in gAcm@%one
density value expressed in gAcm@
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
66/75
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
67/75
T scoreT score
? !3? !3 ormalormal
!3 to !@"1!3 to !@"1 .steopenia.steopenia
B!@"1B!@"1 .steoporosis.steoporosis
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
68/75
Clinical manifestationsClinical manifestations
$eight loss! due to verte%ral compression$eight loss! due to
verte%ral compressionfracturesfractures
Spinal deformity! kyphosisSpinal deformity! kyphosis
#ain appears in 3A< of pacients ith verte%ral#ain appears in
3A< of pacients ith verte%ralfracturesfractures
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
69/75
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
70/75
6yphosis due to osteoporosis6yphosis due to osteoporosis
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
71/75
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
72/75
5actors influencing fracture risk5actors influencing fracture
risk Skeletal factors:Skeletal factors:
'one age'one age 'one si>e'one si>e
'one mineral density and Muality'one mineral density and Muality
Extrinsic factors )falling risk*:Extrinsic factors )falling
risk*:
&mpaired vision&mpaired vision
(iminished muscle strenght(iminished muscle strenght
europathyeuropathy #resence of small animals in household#resence
of small animals in household
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
73/75
TreatmentTreatment
#revention ! for all ages:#revention ! for all ages:
Regular physical activity of reasona%le intensityRegular
physical activity of reasona%le intensity
-deMuate nutrient intake-deMuate nutrient intake Correct calcium
intakeCorrect calcium intake
Treatment of hypogonadism )hormone replacement*Treatment of
hypogonadism )hormone replacement*
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
74/75
TreatmentTreatment -ntiresor%tive agents:-ntiresor%tive
agents:
CalciumCalcium +itamin ( and calcitriol+itamin ( and
calcitriol
EstrogenEstrogen
CalcitoninCalcitonin 'isphosphonates'isphosphonates
'one! forming agents:'one! forming agents:
5luoride5luoride -ndrogens-ndrogens #arathyroid
hormone#arathyroid hormone
-
7/21/2019 Lecture 9, Calcium and Bone Metabolism
75/75
5ollo!up5ollo!up
#eriodic height measurements#eriodic height measurements
-nnual evaluation of ',(-nnual evaluation of ',(
'iannual la% tests )%one turnover'iannual la% tests )%one
turnovermarkers*markers*