Embed Size (px)
Citation preview

LATROBE REGIONAL HOSPITAL
Annual Report 2019
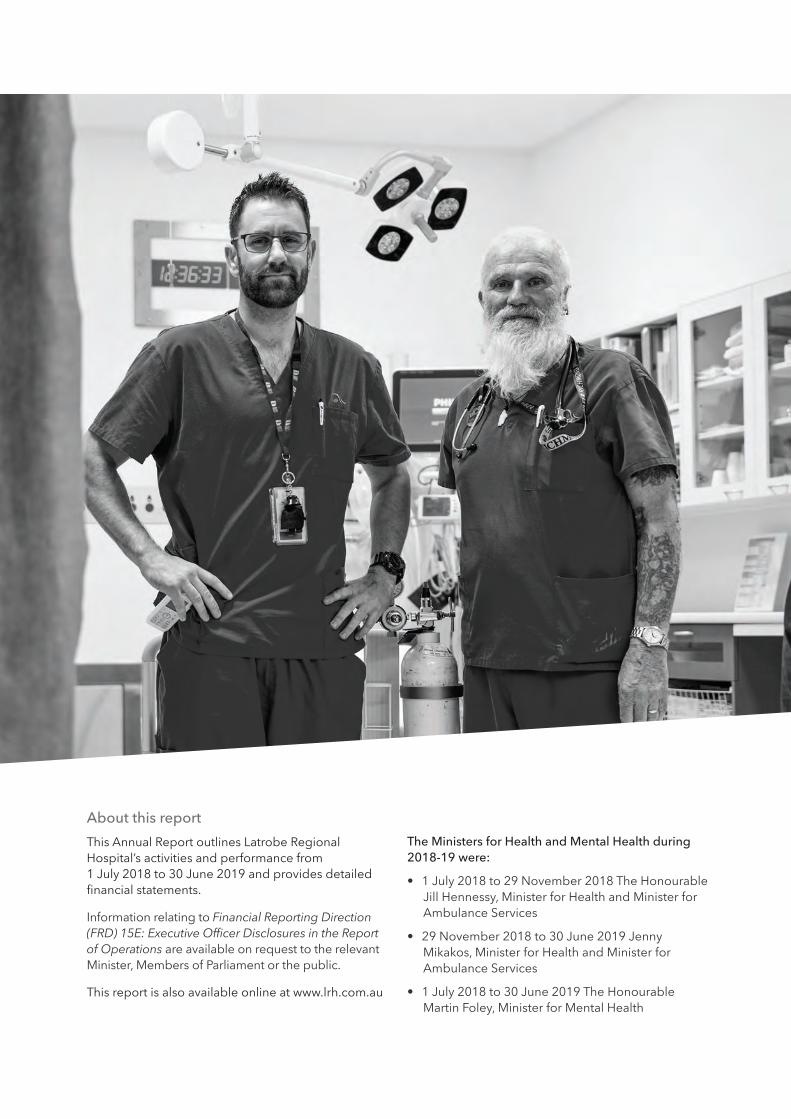
About this report
This Annual Report outlines Latrobe Regional Hospital’s activities and performance from 1 July 2018 to 30 June 2019 and provides detailed financial statements.
Information relating to Financial Reporting Direction (FRD) 15E: Executive Officer Disclosures in the Report of Operations are available on request to the relevant Minister, Members of Parliament or the public.
This report is also available online at www.lrh.com.au
The Ministers for Health and Mental Health during 2018-19 were:
• 1 July 2018 to 29 November 2018 The Honourable Jill Hennessy, Minister for Health and Minister for Ambulance Services
• 29 November 2018 to 30 June 2019 Jenny Mikakos, Minister for Health and Minister for Ambulance Services
• 1 July 2018 to 30 June 2019 The Honourable Martin Foley, Minister for Mental Health

ANNUAL REPORT 2019 | 1
OrbostOrbost Community Mental Health Service
TraralgonLatrobe Regional Hospital
Latrobe Valley Community Health Service
YarramYarram Community Mental Health Service
WonthaggiWonthaggi Community
Mental Health Service
WarragulWarragul Community
Mental Health Service
KorumburraKorumburra Community
Mental Health Service
BairnsdaleBairnsdale Community Mental Health Service
SaleSale Community Mental Health Service
GIPPSLAND
AUSTRALIA
VICTORIA
ContentsOur vision 2
Chair and Chief Executive Report 3
Board of Directors and Committees 6
Executive team 7
Organisational Structure 8
Service indicators 10
Executive Reports 11
Our People 16
Occupational Health and Safety 17
Summary of Financial Results 18
Disclosures required under legislation 21
Additional Information 23
Attestations 24
Statement of Priorities Part A 25
Statement of Priorities Part B 30
Statement of Priorities Part C 33
Other reporting requirements 34
Disclosure Index 35
Financial Report 36
Our storyLatrobe Regional Hospital (LRH) is located 150km east of Melbourne at Traralgon West.
We are a public health service established under the Health Services Act 1988 (Vic). This followed the merger of two public hospitals in Traralgon and Moe and a nursing home in Morwell in 1991.
We provide public hospital services in accordance with the principles of the National Health Care Agreement (Medicare) and the Health Services Act 1988 (Vic).
LRH has 313 beds and treatment chairs and cares for a population of more than 270,000 as a provider of specialist services to the Gippsland region. We offer services such as cardiac care, surgery, medical, renal, emergency care, aged care, obstetrics, mental health, pharmacy, allied health and rehabilitation. Medical and radiation oncology are offered at the Gippsland Cancer Care Centre on site.
LRH is the main provider of acute mental health services in Gippsland with inpatient care at the hospital and community mental health services and teams in the Latrobe Valley, Sale, Bairnsdale, Yarram, Orbost, Korumburra, Warragul and Wonthaggi.
Our Macalister Unit has 10 acute beds for older people with complex needs relating to mental illness as well as 10 nursing home beds.

2 | LATROBE REGIONAL HOSPITAL
our vision
We will be a leading regional health care provider delivering timely accessible, integrated and responsive services to the Gippsland community.
Our values
Person-centred careWe put our patients first in our care, planning and decision-making.
IntegrityWe are honest and respectful in our dealings and accountable for what we do.
ExcellenceWe aim high to ensure our community receives timely and relevant care.
Working togetherWe will respond to challenges together to create a safe, quality health service.

ANNUAL REPORT 2019 | 3
Year in Reviewfrom Chair Linda McCoy and Chief Executive Peter Craighead
This has been a year of change and challenge for our organisation. Our expanded Emergency Department has attracted a record number of presentations and inpatient services have also experienced high demand. Our consulting specialists have also been extremely busy in 2018-19.
It’s a scenario that wasn’t unexpected. We have grappled with the poor health profile of the Gippsland community for many years however our new and expanded facilities are ensuring more people are able to get the care and treatment they need.
Caring for our community
Our forecast 10 per cent increase in the number of Emergency Department presentations has come to fruition and we are pleased 100 per cent of category 1 emergency patients were seen immediately.
There were 41,157 presentations to our ED compared with 36,175 in 2017-18. Overall, 167,157 people were treated at our hospital, an increase of 13,923 on the previous year.
While the larger ED has provided more points of care, our dedicated staff have played a vital role in ensuring patients have access to safe, quality services.
Our commitment to better flow from the ED through to inpatient units and discharge is also making a contribution to improving the experience for patients. We also involve non-clinical staff in discussions about patient flow and draw on their input at Daily Operating System meetings.
Aside from our busy acute schedule, LRH has also been working towards improving outcomes for our community before and after they use our services.
Our Enhanced Maternity Clinic has significantly improved our response to high risk pregnancies by ensuring expectant mums with health issues are supported with multidisciplinary antenatal care. Our Thomson maternity unit has had a busy year with 833 babies delivered including 17 sets of twins.
New smoke free models and policies will guide the reduction, if not the elimination of smoking at all of our sites from September 2019. While we continue to educate and encourage the public not to smoke on our grounds, the emphasis of this new campaign will be on our patients and staff. A quarter of Latrobe Valley residents are regular smokers and we know this has contributed to high chronic diseases in the area.
We are also pleased our Mental Health Service has continued its work towards reducing the rate of harm by suicide, another significant challenge in this community. A Zero Suicide pilot program has commenced in Bairnsdale as has the Hospital Outreach Post-suicidal Engagement (HOPE) project which aims to identify people at risk of suicide and self-harm and provide them with ongoing support when discharged.
Our Koori Liaison Officers have been working to improve care pathways for Aboriginal patients on discharge by linking them in to community services that respond to their needs. We’re proud of our efforts so far to create a welcoming, inclusive health service. Our non-indigenous staff have embraced opportunities to learn about Aboriginal culture during NAIDOC Week activities and throughout the year.
Our people
Increased demand and acuity has posed a challenge to staff across the organisation and at times have contributed to heavy workloads. This year’s influenza season has also taken a toll on the health of our staff and community.
Our heartfelt thanks to our dedicated workforce which has ensured we maintain a high standard of care despite the challenges.

4 | LATROBE REGIONAL HOSPITAL
Recruitment has always been an issue for regional health services and LRH continues to look for innovative ways to recruit and retain our clinical and non-clinical workforce. We are delighted to report our involvement in the creation of a ‘regional training hub’ has been successful in encouraging a number of junior medical officers to stay in Gippsland.
Internally, our Organisational Development Committee (ODC) consisting of staff and management meet regularly to discuss the wellbeing of our employees and implement measures to keep them happy and healthy at work.
Our People Matter Survey results from 2018 have prompted a number of measures to support the physical, mental and emotional wellbeing of our employees including flexible working arrangements, the construction of a walking path around our precinct, zero tolerance for bullying and the appointment of a coordinator to tackle occupational violence and aggression.
This year we were made aware of specific challenges in our mental health service so we engaged the services of an independent consultant to help us identify opportunities for improvement and learn how we may be able to support a positive workplace culture as our organisation continues to grow. Our service and care can only be better for it.
Our work with the local Aboriginal community has gone from strength to strength thanks to the partnerships forged by our Koori Liaison team. This has resulted in renewed interest in our Aboriginal Employment Program which has provided career opportunities across the organisation. We now have 20 staff who identify as Aboriginal or Torres Strait Islander.
Our community continues to connect with us through our Volunteer Program. We now have almost 60 volunteers including a number who have a ‘concierge’ role helping our visitors and patients to navigate their way around our growing precinct while our ever-reliable team of drivers ensure dialysis patients are able to get to and from their regular appointments.
Research, education and training
We have made a substantial commitment to education and training with an extensive schedule of clinical and non-clinical opportunities offered to staff each day.
Our Staff Development Unit and Mental Health Professional Development Unit have amalgamated to form a single Education and Training Unit with the aim of providing opportunities for the development of our staff and assisting with building the capacity of a regional health workforce.
We have also embraced an exciting opportunity to embark on two major research projects involving clinical trials in our region which we hope will improve health outcomes for the Gippsland community. Our work in this space is complemented by the appointment of Human Research Ethics Officer to better coordinate research projects, academic and community involvement.
Regional Leadership
As the largest hospital in Gippsland, LRH has an important role to play in advocating for and supporting smaller health services in the region.
However, in the past 12 months there has been a terrific spirit of collaboration and partnership where services, large and small have had an equal say and contribution to make to a number of projects. This has been particularly true in orthopaedic surgical and rehab pathways and maternity and newborn services.
We have opened a new special care nursery for premature and sick babies from across Gippsland. The nursery, funded through the Victorian Government’s Regional Health Infrastructure Fund, now has the capacity to deliver a high level of neonatal care for up to 10 babies in spacious, family friendly surroundings. We’re working on redeveloping rooms for women and paediatric patients in our Thomson Unit.
Meanwhile, planning is underway for Stage 3A of the hospital’s expansion with the first phase of funding received in this year’s State Budget. The $217 million project will address projected demands for inpatient, surgery and maternity services while creating fit-for-purpose facilities to ensure Gippsland people are able to be treated as close to home as possible.

ANNUAL REPORT 2019 | 5
Acknowledgements
Our thanks go to the many individuals, community groups and businesses that have made a contribution to LRH throughout the year – our staff, volunteers, donors, contractors and suppliers.
In particular, we wish to acknowledge the service of retiring Board Director Ian Gibson. Ian took a special interest in engaging the local community with our health service and worked closely with our Community Advisory Committee. He also made a terrific connection with our employees and was a regular at staff functions.
We must also thank three key members of our Executive team, Amanda Cameron (Chief Operating Officer/Chief Nurse), Dr Simon Fraser (Chief Medical Officer) and Gary Gray (Executive Director Regional Services) who left LRH this year. This highly experienced trio has guided the organisation through challenging times and into an era of excellence in healthcare.
We look forward to the strategic direction of our new Executive team and Board of Directors to take us forward in responding to the health challenges and needs of our community.
Responsible Bodies Declaration
In accordance with the Financial Management Act 1994, I am pleased to present the report of operations for Latrobe Regional Hospital for the year ending 30 June 2018.
Linda McCoyChair, Board of DirectorsTraralgon West27 August 2019

6 | LATROBE REGIONAL HOSPITAL
Board of DirectorsLinda McCoy – Chair
Ian Gibson – Deputy Chair
Leah Young
John Rasa
John Donovan
Chelsea Caple
John Arranga
Dr Bernadette Hickey
Liesl McKay
Board Committees
Audit and Risk
Leah Young (Chair), Linda McCoy (ex-officio), John Donovan, Chelsea Caple (from Nov 2018), Peter Craighead, Don McRae, Mark Wilkins, Michael Glaubitz
Finance
John Donovan (Chair), Linda McCoy (ex-officio), John Arranga, John Rasa (from Oct 2018), Peter Craighead, Don McRae, Michael Glaubitz
Quality
John Rasa (Chair), Linda McCoy (ex-officio), John Arranga, John Donovan (Aug 2018 meeting only), Dr Bernadette Hickey, Peter Craighead, Don McRae, Cayte Hoppner, Dr Philippa Hawkings, Mark Wilkins, Jon Millar, Dr Tricia Wright, Lee Bell/Sharon Rutter, Kenneth Ch’ng, Martin Allen, Angela Scully, Lucie Newberry
Population Health
John Rasa (Chair), Linda McCoy (ex-officio), Ian Gibson, Chelsea Caple, Peter Craighead, Don McRae, Dan Weeks, Frank Evans, Robyn Hayles, Amanda Proposch, Gippsland PHN, Greg Blakeley, Tim Owen, Ben Leigh, David Morgan
Community Advisory Committee
Ian Gibson (Chair to Aug 2018), Chelsea Caple (Chair from Oct 2018), Linda McCoy (ex-officio), Liesl McKay (from Oct 2018), Vicki Hamilton, John Smethurst, Rita Fleming, Ray Watson, Rika Delaney
Appointments and Scope of Practice
Ian Gibson (Chair), Linda McCoy (ex-officio), John Rasa, Leah Young (from Oct 2018), Dr Bernadette Hickey (from Oct 2018), Peter Craighead, Don McRae, Dr Philippa Hawkings, Cayte Hoppner, Mark Jarred, Swarada Kotkar
Remuneration and Executive Performance
Linda McCoy (Chair), Ian Gibson, Leah Young

ANNUAL REPORT 2019 | 7
Executive team
Chief Executive
Peter CraigheadThe Chief Executive is responsible for the development and implementation of operational and strategic planning and quality improvement at LRH in consultation with staff, community and other Gippsland health services.
Chief Operating Officer / Chief Nurse
Don McRae (from August 2018)The COO/Chief Nurse manages a diverse healthcare environment including inpatient, ambulatory and critical services. The role also encompasses financial services, payroll operations and procurement.
Chief Medical Officer
Dr Philippa HawkingsThe CMO provides high-level support on a range of issues including governance, education training and research, medical staff, pharmacy, health information unit and private consulting suites.
Executive Director Mental Health / Chief Mental Health Nurse
Cayte HoppnerThe Executive Director Mental Health/Chief Mental Health Nurse oversees the provision of recovery-oriented, high quality care, the implementation of key mental health reforms and the development of the mental health workforce.
Executive Director People and Culture
Mark WilkinsThe Executive Director People and Culture aims to develop and implement a strategic workforce approach for the promotion of a positive culture, employee engagement and the achievement of organisational and service delivery goals.
Executive Director Information and Regional Services
Jon Millar (from January 2019)This dual role encompasses Chief Information Officer of the Gippsland Health Alliance as well as the Executive Director of Regional Partnerships. The role is responsible for regional ICT and the management and development of opportunities around shared services. Additionally, the Executive Director Information and Regional Services operates as the Chief Procurement Officer for LRH.

8 | LATROBE REGIONAL HOSPITAL
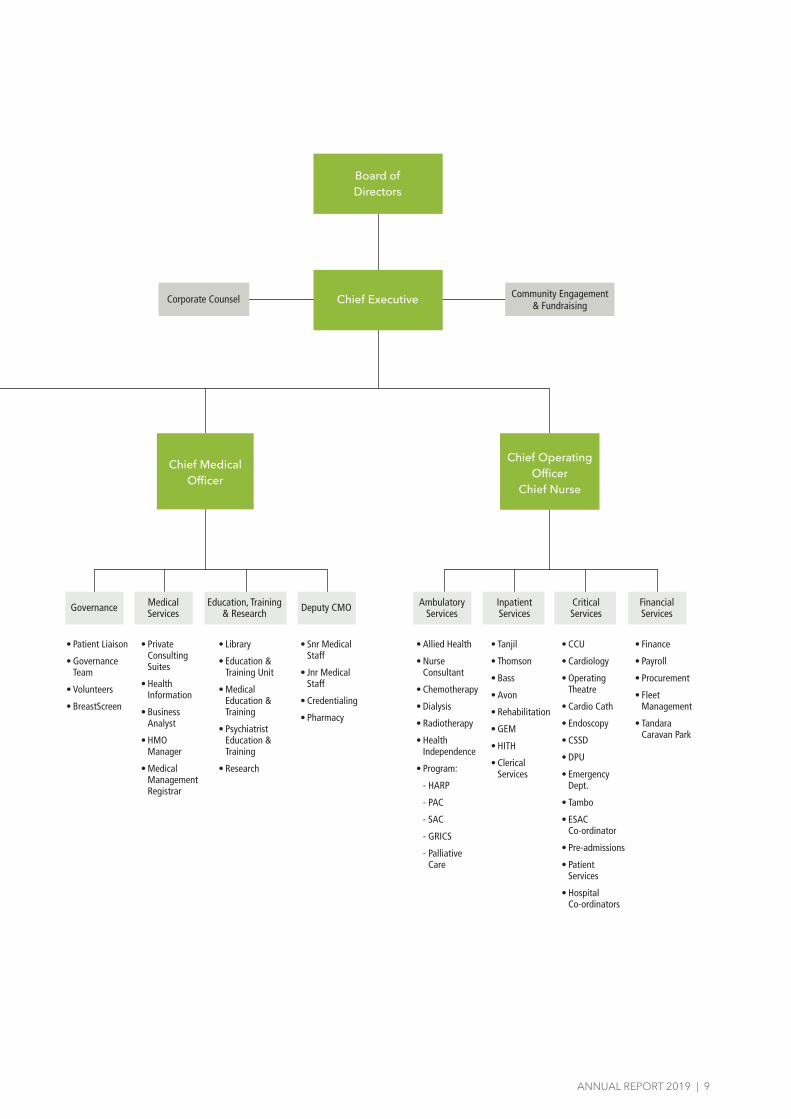
Organisational Structure
Executive Director People & Culture
• Facilities Management
• External Contracts
• Security
• Staff Accommodation
• Risk Management
• Insurance:
- Public Liability
- Industrial Special Risk
Business Services
Support Services
Human Resources
Koori Liaison
• Human Resources
• Industrial Relations
• OH&S
• WorkCover
• Food Services
• Environmental Services
• Cafe
Community Mental Health
Clinical Director
Acute & Bedbased Mental Health
Executive Director Mental Health
Chief Mental Health Nurse
• Consultant Psychiatrists
• Registrars
• Medical Officers
• Adult Mental Health Teams
• Aged Mental Health Team
• Child & Youth Mental Health Team
• Specialist and Therapeutic Programs
• Flynn Unit
• Macalister Unit
• Agnes (Mother & Baby) Unit
• CRCU
• Triage
• Acute Community Intervention Service
• PARCS
• SECU
Executive Director Information and
Regional Services
Information Technology
Gippsland Health Alliance
• Application Management
• Electronic Medical Record
• Information, communication and technology
• Bio-Medical
ANNUAL REPORT 2019 | 9
Community Engagement & Fundraising
Chief Medical Officer
Deputy CMOGovernance Medical Services
Education, Training & Research
• Patient Liaison
• Governance Team
• Volunteers
• BreastScreen
• Private Consulting Suites
• Health Information
• Business Analyst
• HMO Manager
• Medical Management Registrar
• Library
• Education & Training Unit
• Medical Education & Training
• Psychiatrist Education & Training
• Research
• Snr Medical Staff
• Jnr Medical Staff
• Credentialing
• Pharmacy
Ambulatory Services
Inpatient Services
Critical Services
Financial Services
Chief Operating Officer
Chief Nurse
• Allied Health
• Nurse Consultant
• Chemotherapy
• Dialysis
• Radiotherapy
• Health Independence
• Program:
- HARP
- PAC
- SAC
- GRICS
- Palliative Care
• Tanjil
• Thomson
• Bass
• Avon
• Rehabilitation
• GEM
• HITH
• Clerical Services
• CCU
• Cardiology
• Operating Theatre
• Cardio Cath
• Endoscopy
• CSSD
• DPU
• Emergency Dept.
• Tambo
• ESAC Co-ordinator
• Pre-admissions
• Patient Services
• Hospital Co-ordinators
• Finance
• Payroll
• Procurement
• Fleet Management
• Tandara Caravan Park
Chief Executive
Board ofDirectors
Corporate Counsel

10 | LATROBE REGIONAL HOSPITAL
Service indicators
People treated at LRH
2014-15 130,388
2015-16 134,314
2016-17 134,181
2017-18 153,234
2018-19 167,157
Emergency Department presentations
2014-15 31,966
2015-16 33,820
2016-17 33,849
2017-18 36,175
2018-19 41,117
Surgical procedures
2014-15 9645
2015-16 9841
2016-17 10,214
2017-18 10,314
2018-19 10,900
Outpatients
2014-15 65,132
2015-16 65,175
2016-17 64,701
2017-18 68,262
2018-19 74,657

ANNUAL REPORT 2019 | 11
Executive ReportsOur Executive team shares some of its highlights for 2018-19.
Chief Operating Officer / Chief Nurse
• No patient has stayed longer than 24 hours in the Emergency Department despite over 40,000 presentations, an increase of 13 per cent from the previous year.
• There have been sustained high achievements in elective surgery with more patients admitted for surgery than previous years and procedure numbers exceeding our target by more than 500. We performed more than 800 knee, hip or shoulder replacements to Gippsland residents.
• Significant work has been undertaken by the Gippsland Maternity and Newborn Service Planning Project with the establishment of a Regional Maternity and Newborn Planning Committee. One outcome has been the development and implementation of a Gippsland-wide bariatric policy and LRH’s increased capability to care for patients with high Body Mass Index (BMI).
• Involvement in the Better Care Victoria Patient Flow Partnership project resulted in a number of initiatives to improve timely access to care. This has included implementation of a Daily Operating System to improve staff and patient safety and facilitate communication across all areas and levels of the organisation. The project also provided an opportunity to review the management of ‘Fast Track’ in the Emergency Department resulting in improved pathway for patients being treated and discharged home.
• Collaboration with all stakeholders has led to the establishment of a foetal surveillance competency policy and associated procedures for all staff providing maternity care. This will ensure the safest outcomes for mothers and babies.
• Our Nurse Donation Specialist in partnership with DonateLife Victoria has played an important role in the development of robust hospital organ donation protocols and success of new donor pathways in 2019. This comes as we strengthen our successful living bone donor program to become one of the highest donors of bone in Victoria. Community awareness activities particularly about the Donor Register are ongoing.
• The release of the national hip fracture care clinical care standard in 2016 by the Australian Commission on Safety and Quality in Health Care was an opportunity for us to review the care we provide to our patients with hip fracture. Strategies have been implemented to further improve outcomes for this group of patients.
• LRH has expanded the Gippsland Regional Palliative Care Consultancy Service to include South Gippsland and further enhanced the service with a Palliative Care Nurse Practitioner. A key focus of the service is building the skills and capacity of regional health care providers, through the provision of multi-disciplinary specialised education.
• LRH commenced an Enhanced Maternity Clinic which provides multi-disciplinary care in a ‘one stop shop’ environment for women with high risk pregnancies.
• Our infection control team immunised 85 per cent of our staff against influenza.
• LRH has supported the development of its nursing workforce through the introduction and integration of several nurse practitioner roles, including the appointment of our first Nurse Practitioner in Aged Care, expanded Nurse Practitioner positions in the Emergency Department and continued support for Nurse Practitioner Candidates in Oncology and Palliative Care.
• We successfully hosted the Safer Care Victoria Governance Committee of the Older Persons Clinical Network meeting in May, which included presentations on four local quality improvement initiatives relating to older people. This included highlighting the work of the Delirium Collaborative, the role of Residential in Reach program including the Aged Care Nurse Practitioner role, the completion of an organisation-wide environmental audit and our work with our regional partners in achieving timely access to surgery for patients with fractured neck of femur.

12 | LATROBE REGIONAL HOSPITAL
• An Advanced Care Planning forum was held at LRH in collaboration with the McCabe Centre and attracted interest from across Gippsland.
• A project to enhance recovery after major surgery has been funded by Gippsland Regional Integrated Cancer Services (GRICS). This project aims to improve recovery by focusing on specific strategies targeted at areas of care before surgery, during surgery and immediately post-surgery.
• We have implemented intentional rounding on Tyers, Tanjil, Nicholson Rehabilitation, GEM and Macalister units. Nursing staff regularly attend to patients and are proactive in identifying their needs.
• A Director of Cancer Services has been appointed and survivorship supportive care using telehealth introduced. We now have a new nurse-led Symptom Urgent Review Clinic (SURC) for patients experiencing pain or other symptoms while undergoing cancer treatment.
• We amalgamated the orthopaedic and surgical units to provide a 40 bed ‘super surgical unit’. We have also refurbished the Tanjil Unit decreasing shared rooms from four patients to two.
Services for women and children are now delivered in one area with the opening of our Women’s, Children and Birthing Unit. The unit includes a new 10 bed Special Care Nursery and refurbished inpatient area for women and children.
Chief Medical Officer
• Collaboration with the regional training hub to promote opportunities designed to enable training within the region is well underway in an effort to retain our medical workforce. In the 2019 intake, LRH had 12 returning junior medical officers. A Gippsland medical workforce management forum has been established to facilitate collaboration and enhance recruitment and retention across the region.
• Victorian Medical Specialist Training (VMST) funding has been granted for registrar training posts in anaesthetics, geriatric medicine, obstetrics and gynaecology, rehabilitation medicine and psychiatry.
• Challenges in recruitment of staff has resulted in increased utilisation of medical locum workforce. A proposal has been accepted to develop a regional approach to engaging short term medical relief staff.
• Associate Professor Solomon Menahem was appointed as Director of Renal Services and is working on strategies to strengthen renal services across the region. Patient flow has already improved.
• A Gippsland cancer service reference group has been established to optimise governance of cancer services across the region. The group is led by our Director of Cancer Services Dr Tricia Wright.
• Telehealth services have expanded across the region, including pre-admission telehealth appointments and in partnership with Monash Health kidney and pancreas transplant units, education sessions at LRH for transplant patients.
• LRH has successfully worked with Health Purchasing Victoria (HPV) to implement an innovative tendering approach for the purchase of IV chemotherapy preparations to treat cancer patients. This has been undertaken in partnership with Central Gippsland Health Service and Bairnsdale Regional Health Service.
• LRH has participated in the Better Care Victoria ‘Choosing Wisely’ Scaling Collaboration focusing on coagulation studies in the Emergency Department. Following the success of the initial project we intend to expand the process to the entire organisation this year.
• A clinical documentation specialist is working to improve documentation and patient outcomes, in addition to WIES utilisation. Engagement with key clinical staff and education for junior medical staff have been critical to facilitating the success of this role.
• LRH has transitioned to version two of the NSQHS and aged care standards.
• Our medical staff have been strongly engaged in the ‘patient flow collaboration’ which has resulted in positive strategy implementation.
• A new position for an Advanced Trainee in Medical Oncology has been created at LRH with the Royal Australasian College of Physicians (RACP) visiting and granting accreditation for the post.
• The RACP Basic Paediatrician training (BPT) committee performed an assessment of LRH BPT training, following changes in senior staffing, and have endorsed ongoing accreditation.
ANNUAL REPORT 2019 | 13
• The College of Intensive Care Medicine (CICM) granted accreditation of Foundation training in Intensive Care Medicine.
• The Royal Australasian College of Medical Administrators have endorsed LRH for training of a second candidate.
• The Staff Development Unit and Mental Health Professional Development Unit were successfully amalgamated into one multidisciplinary education and training unit.
• Digitalisation of the surgical high dependency unit (SHDU) and the ventilation programs has occurred enabling increased access to these programs by staff and supporting excellence in care.
• Two graduate entry streams now exist for Registered and Enrolled Nurses at LRH. Strong interest has been secured for the 2020 intake through promotion at the Federation University Open Day.
• Research activity has expanded across the region with LRH participating in two multi-centre clinical research trials. A Human Research Ethics Committee secretariat has commenced to support this expansion. The LRH HREC now supports all of our regional partners (Central Gippsland Health Service, Bass Coast Health, West Gippsland Healthcare Group, Bairnsdale Regional Health Service)
• A research development day was held in collaboration with our partnering universities, Federation and Monash, to train staff in research methodologies, literature review, HREC application/ERM (ethical review manager) and how to identify research opportunities.
Executive Director Mental Health / Chief Mental Health Nurse
• LRH has recruited three trainees into the psychiatry training program in the Gippsland region.
• LRH has partnered with the new headspace branch in Wonthaggi to deliver services to young people.
• The Mental Health and Police Response program commenced in Bairnsdale in 2019.
• The Occupational Violence and Aggression (OVA) workgroup implemented key initiatives such as lapel cameras, stab vests, post incident support for staff, pre-admission screening for OVA and mandatory training programs.
• Twelve nursing and allied health professionals were recruited into our new two-year Graduate Mental Health Program. The graduates are working across all clinical areas and geographic regions of the service.
• The HOPE - Hospital Outreach Post Suicide program commenced in March 2019 providing support and treatment for people presenting after a suicide attempt.
• Works are progressing on the redevelopment of the Flynn staff base/nurses station and a new building for our community team in Wonthaggi.
• The Agnes Parent Infant Unit is now operating seven days a week to provide additional support for families requiring specialist mental health care in the perinatal period.
• Our new Aboriginal Mental Health Traineeship commenced in our Bairnsdale team.
• The Early Intervention Mental Health Psychosocial Response in partnership with community mental health agency Mind Australia, has commenced operation and delivers a range of short to medium term tailored psychosocial supports. The program aims to help clients of clinical mental health services to self-manage their mental health condition, develop practical life skills for independent living, engage with others and participate in the community.
• A new program to deliver early mental health intervention for the 0-5 age group has begun.
• LRH and the Primary Health Network are collaborating on a regional mental health and suicide prevention plan to deliver a stepped care model in Gippsland and improve coordination of mental health services using an evidence-based approach.
• LRH contributed to the Royal Commission into Mental Health through several roundtables in Melbourne and Traralgon. We also provided our own organisational submission and contributed to a joint submission with other rural and regional services recommending changes to ensure the mental health needs of our rural communities are addressed. LRH also provided a submission to the Aged Care Royal Commission.
• An innovative collaboration has been established with the Foyle Project (Londonderry) and the Helen Hamlyn School of Design to discuss a community approach to suicide prevention and the design of the built environment to prevent suicides in rural regions.

14 | LATROBE REGIONAL HOSPITAL
• Hazelwood Mine Fire Deliverable 85 Project has progressed with community health and a selected GP clinic engaging in mental health education to support people living with mental health issues and chronic disease.
• The Office of the Chief Psychiatrist undertook a successful review of the Macalister Aged Care Nursing Home and an unannounced visit by the Aged Care Quality Commission was also completed with a successful outcome.
• DHHS conducted a review of our residential and extended care services as part of a state-wide review of all facilities.
• New consultant psychiatrists and senior registrars have been recruited in Sale, Bairnsdale and Traralgon.
• Funding for four new full-time graduate level clinical positions to be employed as Community Mental Health System navigators was received.
• LRH has progressed a project to build an interface to support referrals into NDIS for consumers of the mental health service.
• Our seclusion rates are the best in the state in the recent DHHS Performance reports. This is testament to our inpatient staff and their skill and expertise in managing very complex care needs for patients.
• New funding for Intensive Community Care Packages was received. The funding is being used for additional face-to-face support for people with a severe mental illness.
• Expansion of the perinatal mental health program across our community sites and the introduction of new telehealth options is progressing.
Executive Director People and Culture
• We implemented a comprehensive leadership program for identified emerging leaders across the organisation. The program draws on the expertise of internal and external facilitators and covers leadership principles, HR practice, risk management, governance, safety, coaching and mentoring, difficult conversations and mindfulness.
• A new version of electronic on-boarding was implemented enabling prospective staff to complete their recruitment and relevant checks online before commencing employment.
• Senior and junior medical contracts are now developed by HR to improve standardisation of employment practices across LRH.
• The Workplace Support Officer initiative continues to provide enormous benefit to employees and the organisation. Bi-monthly meetings are held by the group as they continue to assist, support and guide LRH staff. Funding has recently been obtained to provided refresher training for Workplace Support Officers.
• We implemented a new supported Aboriginal Traineeship Program in collaboration with our Latrobe City Council partnership. Candidates and their families were invited to attend an information day at LRH to hear more about the traineeship opportunities and tour the organisation. Four aboriginal trainees were recruited in IT, Consulting Suites, Clerical Services and Theatre and continue to be supported in their learnings by a LRH tutor and senior HR staff.
• Support from our workforce and management continues for our Aboriginal Employment Plan. This has made a genuine difference in recruitment and retention. LRH now employs 20 Aboriginal/Torres Strait Islander staff members as we aim to surpass our one per cent target.
• The Aboriginal Telehealth Program continues to grow with all six Gippsland ACCHOS supportive of this initiative. Support is provided by our Telehealth Project Manager and Koori Liaison team leader with appointments scheduled as far away as Lake Tyers and Orbost.
• A Memorandum of Understanding between LRH and Ramahyuck was signed to ensure rural and regional Aboriginal communities in Gippsland receive the best available health treatment in combination with effective holistic social and emotional wellbeing support. Quarterly partnership forums have commenced for developing this partnership, integrating service delivery, sharing ideas and resolving operational problems that arise.
• We purchased a number of artworks by local Gunai Kurnai artists which are now proudly on display around the hospital. Six of these pieces were purchased from Federation Training which resulted in a genuine connection between LRH and the local community. This was celebrated at an official handover ceremony with excellent attendance by LRH management and staff and the local Aboriginal community.

ANNUAL REPORT 2019 | 15
• Wuman Ninje (welcome) signs have been placed at all hospital and community mental health buildings. The response to these signs has been terrific as we continue to ensure LRH provides a safe, welcoming and nurturing environment to Aboriginal patients and their families.
• We are proud to partner and support Latrobe Valley Enterprises for our garden maintenance service.
• There have been improvements to overall maintenance services under a new facilities management contract.
• Back up electrical generators were installed for critical ICT infrastructure that supports regional service provision as well as here at LRH.
• Minor refurbishment of our community mental health service building in Traralgon was completed to accommodate more staff. There were also works to improve amenities at our community residential care units including installation of a garden shed, rotunda with barbecue facilities and an extension to the activities building.
• Work was completed on a new, larger Tanjil inpatient unit.
• Security within our satellite pharmacy was improved with the installation of a new system.
• Our catering services continue to support efforts to improve wellbeing for our busy staff. This year the team rolled out a special indigenous menu for NAIDOC Week and once again supported Active April, AFL Grand Final and Christmas activities.
• LRH has been recognised by the Victorian Government as a healthy workplace and has successfully met statewide benchmarks for physical activity and mental health and wellbeing. Our cafeteria services continue to work towards achieving recognition through the Healthy Workplaces Achievement Program by offering food and drink options that comply with healthy eating guidelines.
• We participated in the Premier’s Active April program with approximately 430 staff attending a staff lunch supported by local fitness businesses and groups. Activities for the month included walking groups, free health checks and mental health mindfulness sessions.
• Our environmental services team continues to provide a clean and hygienic environment for our patients, staff and visitors. The Victorian Healthcare Experience Survey delivered positive results regarding cleanliness throughout the year.
• Our management team is better able to stay on top of occupational health and safety matters with the introduction of a ‘dashboard’ report.
Executive Director Information and Regional Services
• During the financial year the position of Executive Director Regional Services was merged with the Gippsland Health Alliance, Chief Information Officer. This strategic expansion has enabled us to leverage existing relationships and governance structure to enable maximisation and alignment of resources with the anticipated benefits. The role provides greater oversight and integration on core issues, projects, relationships and opportunities in line with DHHS Rural and Regional Health Partnerships Guidelines. ICT Health Alliances are identified as a key service partner in the guidelines.
• We have continued to engage with senior managers from other agencies to collectively oversee the identification, development and implementation of shared services.
• Implementation of a shared procurement and contract management module with West Gippsland Healthcare Group, Central Gippsland Health Service and Bairnsdale Regional Health Service was completed.
• A LRH-operated echocardiograph service for inpatients and outpatients was established. The service is shared between LRH and Central Gippsland Health Service with support from specialists from Alfred Health.
• We have developed a shared partnership matrix documenting partnership services across the Gippsland region and continued work on identifying shared service opportunities in payroll and locum service functions to reduce duplication.
• Phase one of the Electronic Medical Record (EMR) project was implemented in LRH’s Emergency Department. Phase two of the project will see the EMR rolled out across the remaining inpatient setting with the anticipated implementation go-live date of February 2020.
16 | LATROBE REGIONAL HOSPITAL
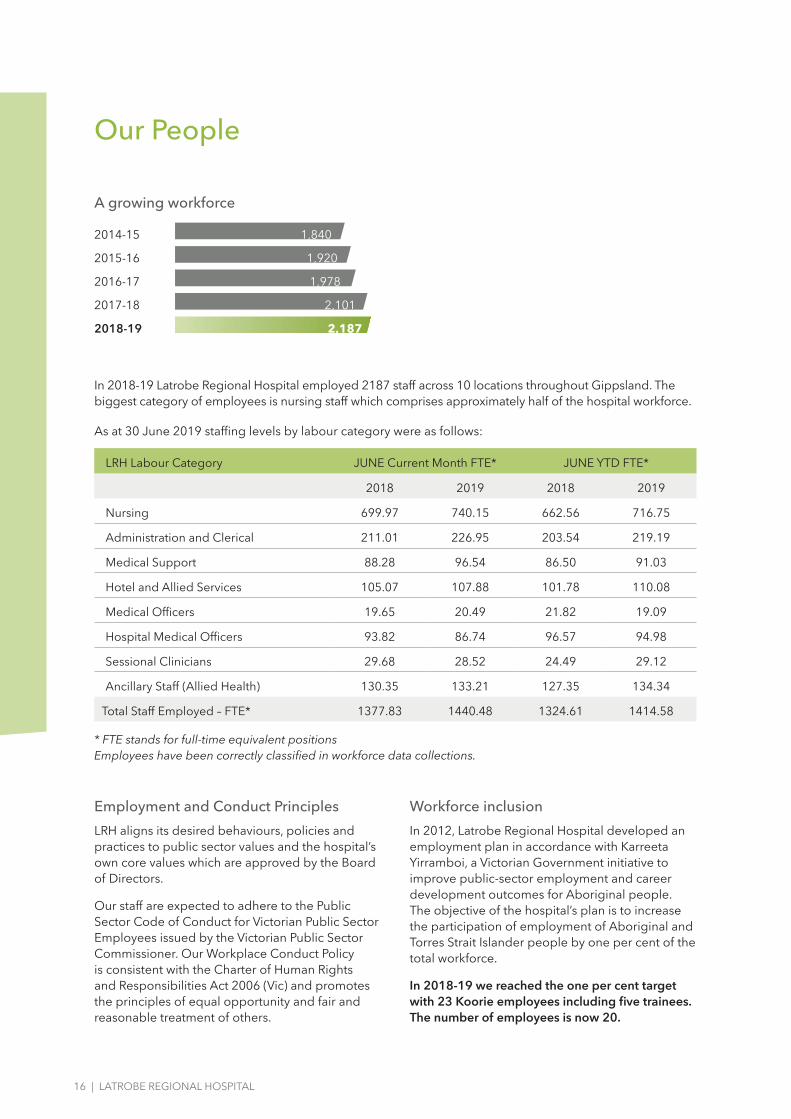
In 2018-19 Latrobe Regional Hospital employed 2187 staff across 10 locations throughout Gippsland. The biggest category of employees is nursing staff which comprises approximately half of the hospital workforce.
As at 30 June 2019 staffing levels by labour category were as follows:
LRH Labour Category JUNE Current Month FTE* JUNE YTD FTE*
2018 2019 2018 2019
Nursing 699.97 740.15 662.56 716.75
Administration and Clerical 211.01 226.95 203.54 219.19
Medical Support 88.28 96.54 86.50 91.03
Hotel and Allied Services 105.07 107.88 101.78 110.08
Medical Officers 19.65 20.49 21.82 19.09
Hospital Medical Officers 93.82 86.74 96.57 94.98
Sessional Clinicians 29.68 28.52 24.49 29.12
Ancillary Staff (Allied Health) 130.35 133.21 127.35 134.34
Total Staff Employed – FTE* 1377.83 1440.48 1324.61 1414.58
* FTE stands for full-time equivalent positions Employees have been correctly classified in workforce data collections.
Our People
Employment and Conduct Principles
LRH aligns its desired behaviours, policies and practices to public sector values and the hospital’s own core values which are approved by the Board of Directors.
Our staff are expected to adhere to the Public Sector Code of Conduct for Victorian Public Sector Employees issued by the Victorian Public Sector Commissioner. Our Workplace Conduct Policy is consistent with the Charter of Human Rights and Responsibilities Act 2006 (Vic) and promotes the principles of equal opportunity and fair and reasonable treatment of others.
Workforce inclusion
In 2012, Latrobe Regional Hospital developed an employment plan in accordance with Karreeta Yirramboi, a Victorian Government initiative to improve public-sector employment and career development outcomes for Aboriginal people. The objective of the hospital’s plan is to increase the participation of employment of Aboriginal and Torres Strait Islander people by one per cent of the total workforce.
In 2018-19 we reached the one per cent target with 23 Koorie employees including five trainees. The number of employees is now 20.
A growing workforce
2014-15 1,840
2015-16 1,920
2016-17 1,978
2017-18 2,101
2018-19 2,187

ANNUAL REPORT 2019 | 17
Occupational Health and SafetyHealth and safety are shared responsibilities at LRH and involve management and staff. Our efforts to prioritise safety have led to a higher level of awareness and understanding of the importance of incident reporting and safety management. Staff are committed to improving safety outcomes for patients and themselves.
Health and Safety IndicatorsThe number of reported health and safety incidents for the year per 100 full-time equivalent staff members was 10.35. In 2017/18 it was 14.98.
The number of ‘lost time’ standard WorkCover claims for the year per 100 full-time equivalent staff members was 1.74. In 2017/18 it was 1.49.
The average cost per claim for the year (including payments to date and an estimate of outstanding claim costs as advised by WorkSafe) are as follows:
Average Claim Cost
Actual
Average Claim Cost
Estimate
Number of
claims
Total 30/06/2019 $17,313.12 $66,627.54 24
Total 30/06/2018 $11,105.52 $63,646.29 21
Total 30/06/2017 $8,201.27 $33,568.92 13
The average claim cost and average claim cost estimates at 30 June 2019 are higher than previous years due to an increase in the number of complex claims with actual claim costs and claim cost estimates above $100,000.
LRH had no staff fatalities during the year.
Occupational Violence and Aggression (OVA)Our Occupational Violence and Aggression (OVA) Working Group which was established in 2013, encourages staff to report incidents of violence and abuse. The group’s role is to develop, implement and evaluate a framework of best practice interventions to reduce the frequency and impact of occupational violence and aggression.
Over the period 2018-19, the following has been achieved:• OVA page updated on the staff intranet –
additional psychological wellbeing content and trauma video uploaded.
• OVA updates in weekly LRH staff newsletter
• ‘Self-Talk’ posters in all staff amenities rooms• revised Home Visiting Policy and Risk Screen
OVA Staff Survey completed• Post Incident Response Protocol and Education
completed• ‘calm down’ and sensory boxes introduced in
staff areas• pre-admission OVA screening project
commenced• new online mandatory OVA training program
introduced• patient safety alerts now being added to patient
records.
Occupational violence statistics for 2018-19
• Workcover accepted claims with an occupational violence cause per 100 FTE = 0.37
• Number of accepted Workcover claims with lost time injury with an occupational violence cause per 1,000,000 hours worked = 1.83
• Number of occupational violence incidents reported = 243
• Number of occupational violence incidents reported per 100 FTE = 22.25
• Percentage of occupational violence incidents resulting in a staff injury, illness or condition = 2.47%
Definitions
Occupational violence – Any incident where an employee is abused, threatened or assaulted in circumstances arising out of, or in the course of their employment.
Incident – An event or circumstance that could have resulted in or did result in harm to an employee.
Accepted Workcover claims – Accepted Workcover claims that were lodged in 2017-18.
Lost time – Defined as greater than one day. Injury, illness or condition – This includes all reported harm as a result of the incident, regardless of whether the employee required time off work or submitted a claim.

18 | LATROBE REGIONAL HOSPITAL
Summary of Financial Results
2018-19 Financial Result with comparative results for the preceding four financial years
2018/19 $’000
2017/18 $’000
2016/17 $’000
2015/16 $’000
2014/15 $’000
Total Revenue 270,027 274,845 279,989 232,506 207,058
Total Expenses 278,476 260,774 232,147 213,730 205,613
Net Result From Transactions (8,449) 14,071 47,842 18,776 1,445
Total other economic flows (557) 653 (692) - -
Net Result (9,006) 14,724 47,150 18,776 1,445
Total Assets 367,661 292,808 269,281 220,130 196,454
Total Liabilities 69,957 60,148 51,345 49,344 44,452
Net Assets/Total Equity 297,704 232,660 217,936 170,786 152,002
Summary of significant changes in financial position in 2018-19
During the 2018-19 financial year, the Victorian Government through the Department of Health and Human Services (DHHS) provided $47.8 million in operating grants and $179.6 million from State and Commonwealth activity-based funding payments via the Victorian Health Funding Pool.
The Victorian Government also provided $5.1 million towards targeted capital works and equipment.
Other Commonwealth grants through the Pharmaceutical Benefits Scheme, Department of Health and Ageing and Radiology/Oncology Equipment Replacement Program totalled $15.1 million.
Revenue from operating activities showed a decrease of $5.8 million, 2.1 per cent from the previous financial year. Revenue received in 2018-19 included carry-over funding totalling $5 million and is scheduled for disbursement in 2019-20.
Total expenses (excluding depreciation) increased by $16.9 million, 6.8 per cent from 2017-18. Employee expenses increased by $21.8 million (13.3 per cent) supplies and consumables decreased by $1.8 million (3.3 per cent) and other operating expenses decreased by $2.9 million (10.6 per cent).
Operating activities provided a net cash inflow of $10 million. Investing activities which included the redemption of an investment of $29.1 million, increased net cash by $23.7 million. There was also a net cash outflow from financing activities of $44,000.
The overall net result was an increase of $33.7 million in cash held. Cash and cash equivalents at end of financial year totalled $62.5 million.
Our current asset ratio at 30 June 2019 was 1.14, a decrease from 1.22 at 30 June 2018.
Major capital works projects continued during the year, including the refurbishment of the Tanjil and Thomson inpatient units.
Current year funding for current capital projects totals $5.1 million from the Commonwealth and Department of Health and Human Services. Future commitments from hospital reserves total $6.9 million.
There were no events subsequent to balance date which may have had a significant effect on the operations of LRH in subsequent years.

ANNUAL REPORT 2019 | 19
2018-19 Net result from transactions
Reconciliation between the Net result from transactions to the Operating result as agreed in the Statement of Priorities
2018/19 $’000
Net operating result (953)
Capital and specific items
Capital purpose income 5,269
Assets received free of charge 13
Expenditure for capital purpose (920)
Depreciation and amortisation (11,858)
Net result from transactions (8,449)
Consultancies engaged during 2018-2019
A number of consultants were contracted to work for Latrobe Regional Hospital in 2018/19. As required by the Victorian Industry Participation Policy Act 2003, a summary of the extent of contractual costs or consultants is provided below.
2018/19
Number of consultants used to a value greater than $10,000
Total cost of consultants used to a value greater than $10,000
3
$76,423
Number of consultants used to a value less than $10,000
Total cost of consultants used to a value less than $10,000
5
$23,673
(Details of individual consultancies, greater than $10,000 on page 20.)
2018-19 Annual Report – ICT Expenditure Disclosure
The total ICT expenditure incurred during 2018-19 is $6,614,707 (excluding GST) with the details shown below:
Business as usual (BAU) ICT expenditure Non-Business As Usual (non- BAU) ICT expenditure
Total (excluding GST) Total = Operational expenditure and
Capital Expenditure (excluding GST)
Operational expenditure
(excluding GST)
Capital expenditure (excluding GST)
$6,548,141 $66,565 0 $66,565

20 | LATROBE REGIONAL HOSPITAL
Details of individual consultancies
Consultant Purpose of consultancy Start date End Date
Total approved
project fee (excluding
GST)
Expenditure 2018-19
(excluding GST)
Future expenditure
(excluding GST)
KPMG Financial Advisory Services
Development of Governance Documents for the Latrobe Health Assembly
Apr-18 Sept-18 $77,646 $38,823 $ -
3M AustraliaHealth Info Systems Consultancy- Phase 1-2 DRG Assurance Program
Oct-18 Dec-18 $45,173 $27,000 $ -
CWH Mediation and Workplace Relations
Workplace culture review Jun-19 Jun-19 $10,600 $10,600 $ -
Ex-Gratia Expenses
*** Latrobe Regional Hospital has not made any ex-gratia payments during 2018-19.
Financial Management Act 1994
The information requirements listed in the Financial Management Act 1994 (the Act), the Standing Directions of the Minister for Finance under the Act (Section 4 Financial Management Reporting) and Financial Reporting Directions have been

ANNUAL REPORT 2019 | 21
Freedom of Information Act 1982
The Victorian Freedom of Information (FOI) Act 1982 gives a person the right to request information held by government agencies including public hospitals and community health centres.
Information on how to lodge an FOI to Latrobe Regional Hospital, an application form and useful links to the FOI Act and FOI website are available at www.lrh.com.au/important-info/patientinformation/general-patient-information.
FOI requests must be made in writing to:
The Freedom of Information Officer Latrobe Regional Hospital PO Box 424 Traralgon Vic 3844
There are two costs associated with making a FOI request – an application fee and access charges. These charges are set by government regulations.
As of 1 July 2019 the fee is $29.60. Access charges are applied under the Act for processing requests.Access charges are applied according to the nature of the request and may include: search fees ($20 per hour), photocopying (20 cents per page), providing written transcripts of a recorded document ($20 per hour), supervising an inspection of documents ($5 per quarter hour).
In 2018-19 LRH received 350 FOI requests, of which 326 were granted full access. There were no documents for seven requests while 17 were withdrawn.
Building Act 1993
Latrobe Regional Hospital complies with the building and maintenance provisions of the Building Act 1993. We obtain building permits for all new projects where required and an audit of compliance of our certificates of occupancy are completed by a registered building surveyor in June each year. LRH engages a building consultant to audit our fire safety every five years against the requirements of Human Services Fire Risk Management Guidelines.
LRH controls properties located at the corner of Princes Highway and Village Avenue, Traralgon West and within the Princes Street, Washington Street and Garden Grove precinct in Traralgon. LRH owns and occupies an additional six buildings located at the Traralgon West campus which operate as specialist consulting clinics and administration offices and property in Macleod Street Bairnsdale. LRH also provides non-residential health services from 10 properties not under its direct control located throughout Gippsland.
We also control a number of houses and units for accommodation purposes – five owned by LRH and 19 leased from private vendors and not under the control of LRH.
LRH ensures all buildings owned or occupied by staff or patients meet the standards for essential safety measures.
Local Jobs First Act Disclosures
LRH has commenced one project that meets the requirements for a Local Industry Development Plan.
From this project LRH initiated one regional contract with 100% local content and a jobs created/retained profile as shown below.
Disclosures required under Legislation

22 | LATROBE REGIONAL HOSPITAL
Table 3: New LRH Contracts, Jobs Retained and Created
Key Criteria CommitmentComments
(where applicable)
ANZ Value-added activity 100% -
Apprenticeships created 0 -
Apprenticeships retained 0 -
Traineeships created 0 -
Traineeships retained 0 -
Standard Employment created
6.8 -
Standard Employment retained
1.98 -
MPSG Commitment (%) N/A -
LRH had one conversation with the ICN that corresponds with the registration and issue of an Interaction Reference Number.
Statement on National Competition Policy
LRH has observed and complied with all requirements of the Victorian Government policy statement, Competitive Neutrality Policy Victoria, for all significant business activities.
Protected Disclosure Act 2012
Latrobe Regional Hospital has a policy consistent with the requirements of the Protected Disclosure Act 2012 which supports staff to disclose improper or corrupt conduct.
LRH’s General Manager Human Resources was the Protected Disclosure Coordinator for the purpose of the Protected Disclosure Act in 2018-19. LRH had no disclosures notified to the Independent Broad-based Anti-corruption Commission under section 21(2) of the Act.
Carers Recognition Act 2012
The Carers Recognition Act 2012 acknowledges and values the role of carers and the importance of care relationships in the Victorian community.
LRH defines a carer as a consumer or patient’s next of kin, a guardian, family member, delegated community member or significant other as nominated.
We recognise the principles of the Act and have incorporated these into multiple policies including Person Centred Care, Family Meeting and Consumer, Carer and Community Partnerships. Carer Consultants also have an important role to play in our mental health service..
We use our internal feedback systems and the Victorian Healthcare Experience Survey to monitor a carer’s experience.
Environmental Performance
LRH has an Environmental Management Plan with targets to improve performance by minimising consumption of water and energy, encouraging the procurement of sustainable products and services and where possible diverting equipment and furniture from landfill. We have progressed a number of projects aimed at assisting us to meet environmental targets for reduction in energy consumption.
We have begun a project to install 1.5mW of solar panels following the indentification of potential savings during an energy audit of our organisation. The project will offset approximately 20 per cent of LRH’s electricity needs.
A tender is also being prepared for a solar hot water system which will eliminate the need for regular hot water flushing.
LRH is developing a waste minimisation strategy to better categorise and recycle waste.

ANNUAL REPORT 2019 | 23
Additional information available on requestDetails in respect of the items listed below have been retained by the health service and are available to the relevant Ministers, Members of Parliament and the public on request (subject to freedom of information requirements, if applicable):
• Declarations of pecuniary interests have been duly completed by all relevant officers;
• Details of shares held by senior officers as nominee or held beneficially;
• Details of publications produced by the entity about itself, and how these can be obtained;
• Details of changes in prices, fees, charges, rates and levies charged by the Health Service;
• Details of any major external reviews carried out on the Health Service;
• Details of major research and development activities undertaken by the Health Service that are not otherwise covered either in the report of operations or in a document that contains the financial statements and report of operations;
• Details of overseas visits undertaken including a summary of the objectives and outcomes of each visit;
• Details of major promotional, public relations and marketing activities undertaken by the Health Service to develop community awareness of the Health Service and its services;
• Details of assessments and measures undertaken to improve the occupational health and safety of employees;
• A general statement on industrial relations within the Health Service and details of time lost through industrial accidents and disputes, which is not otherwise detailed in the report of operations;
• A list of major committees sponsored by the Health Service, the purposes of each committee and the extent to which those purposes have been achieved;
• Details of all consultancies and contractors including consultants/contractors engaged, services provided, and expenditure committed for each engagement.
Financial Management ComplianceI, Linda McCoy on behalf of the Responsible Body, certify that Latrobe Regional Hospital has complied with the applicable Standing Directions 2018 under the Financial Management Act 1994 and Instructions.
Linda McCoyChair, Board of DirectorsLatrobe Regional Hospital 27 August 2019

24 | LATROBE REGIONAL HOSPITAL
Attestations
Data Integrity
I, Peter Craighead, certify that Latrobe Regional Hospital has put in place appropriate internal controls and processes to ensure that reported data accurately reflects actual performance. Latrobe Regional Hospital has critically reviewed these controls and processes during the year.
Peter CraigheadChief Executive Latrobe Regional Hospital 27 August 2019
Conflict of Interest
I, Peter Craighead, certify that Latrobe Regional Hospital has put in place appropriate internal controls and processes to ensure that it has complied with the requirements of hospital circular 07/2017 Compliance reporting in health portfolio entities (Revised) and has implemented a ‘Conflict of Interest’ policy consistent with the minimum accountabilities required by the VPSC. Declaration of private interest forms have been completed by all executive staff within Latrobe Regional Hospital and members of the board, and all declared conflicts have been addressed and are being managed. Conflict of interest is a standard agenda item for declaration and documenting at each executive board meeting.
Peter CraigheadChief Executive Latrobe Regional Hospital 27 August 2019
Integrity, fraud and corruption
I , Peter Craighead, certify that Latrobe Regional Hospital has put in place appropriate internal controls and processes to ensure that Integrity, fraud and corruption risks have been reviewed and addressed at Latrobe Regional Hospital during the year.
Peter CraigheadChief Executive Latrobe Regional Hospital 27 August 2019

ANNUAL REPORT 2019 | 25
Statement of Priorities Part A
Goals Strategies Health Service Deliverables Actions
Better Health
A system geared to prevention as much as treatment
Everyone understands their own health and risks
Illness is detected and managed early
Healthy neighbourhoods and communities encourage healthy lifestyles
Better Health
Reduce Statewide Risks
Build Healthy Neighbourhoods
Help people to stay healthy
Target health gaps
Evaluate the effectiveness of improving birth outcomes for the newly developed ‘enhanced maternity clinic’ to ensure health is optimised and further opportunities explored.
Achieved. Evaluation, including patient satisfaction survey, has been completed. The Enhanced Maternity Clinic has improved LRH’s response to high risk pregnancies including weight monitoring and dietetics involvement in antenatal care (as per recommendations by RANZCOG Guidelines and NHMRC Clinical Practice Guidelines).
Enhance the recently implemented multidisciplinary paediatric outpatient diabetes service.
Achieved. Clinic now established offering individual and multidisciplinary team appointments. Monash endocrinologists to provide patient reviews on site.
Utilise and embed the tools of the Strengthening Hospital Responses to Family Violence (SHRFV) including implementing the action plan with a focus on training, building skills and knowledge in screening, identifying and responding to FV and expanding the program into the clinical mental health service.
Achieved. SHRFV team continues to undertake organisation-wide education and training. Specialist family violence advisor appointed to build the capacity and capability of clinical mental health services to facilitate earlier recognition and response to family violence. Proposal has been developed to ensure all second year students have completed SHRFV training prior to placement.
Implement the LRH Smoking Reduction Working Group action plan and the smoke free policy and in collaboration with regional health services deliver smoke free sites across Gippsland which encourage and support patients and staff to quit smoking.
Achieved. Commenced implementation of project interventions.
26 | LATROBE REGIONAL HOSPITAL
Goals Strategies Health Service Deliverables Actions
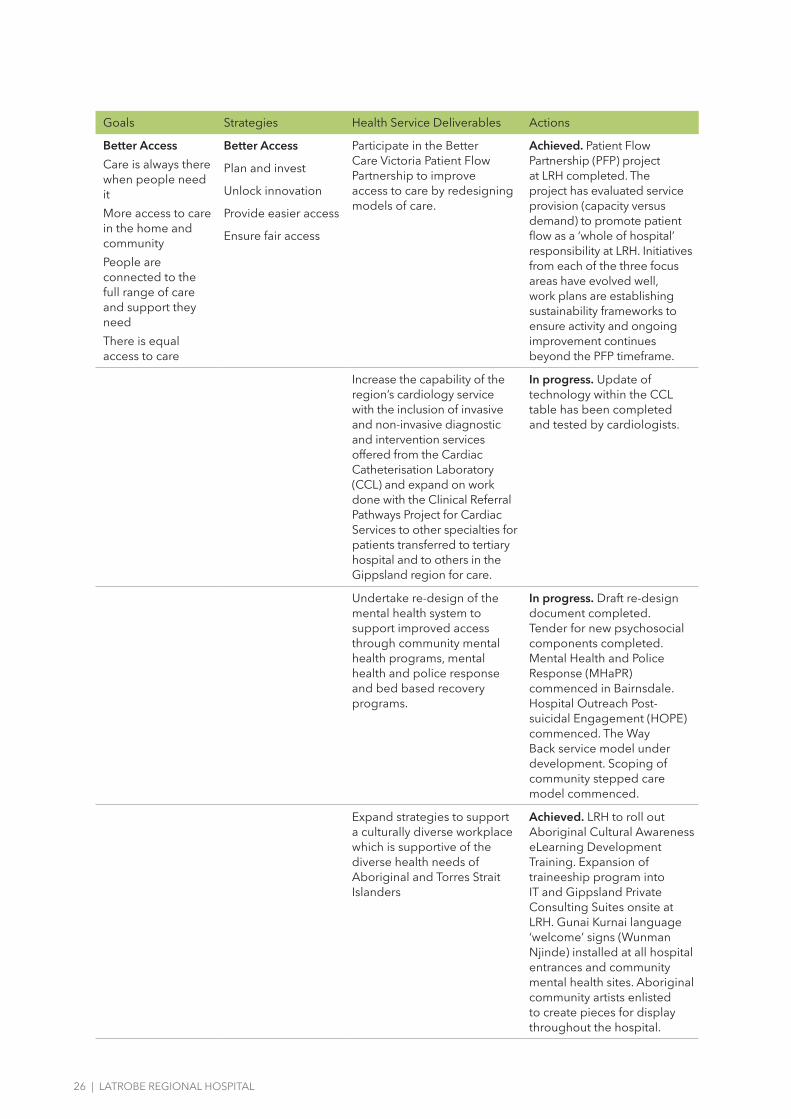
Better AccessCare is always there when people need itMore access to care in the home and communityPeople are connected to the full range of care and support they needThere is equal access to care
Better Access
Plan and invest
Unlock innovation
Provide easier access
Ensure fair access
Participate in the Better Care Victoria Patient Flow Partnership to improve access to care by redesigning models of care.
Achieved. Patient Flow Partnership (PFP) project at LRH completed. The project has evaluated service provision (capacity versus demand) to promote patient flow as a ‘whole of hospital’ responsibility at LRH. Initiatives from each of the three focus areas have evolved well, work plans are establishing sustainability frameworks to ensure activity and ongoing improvement continues beyond the PFP timeframe.
Increase the capability of the region’s cardiology service with the inclusion of invasive and non-invasive diagnostic and intervention services offered from the Cardiac Catheterisation Laboratory (CCL) and expand on work done with the Clinical Referral Pathways Project for Cardiac Services to other specialties for patients transferred to tertiary hospital and to others in the Gippsland region for care.
In progress. Update of technology within the CCL table has been completed and tested by cardiologists.
Undertake re-design of the mental health system to support improved access through community mental health programs, mental health and police response and bed based recovery programs.
In progress. Draft re-design document completed. Tender for new psychosocial components completed. Mental Health and Police Response (MHaPR) commenced in Bairnsdale. Hospital Outreach Post-suicidal Engagement (HOPE) commenced. The Way Back service model under development. Scoping of community stepped care model commenced.
Expand strategies to support a culturally diverse workplace which is supportive of the diverse health needs of Aboriginal and Torres Strait Islanders
Achieved. LRH to roll out Aboriginal Cultural Awareness eLearning Development Training. Expansion of traineeship program into IT and Gippsland Private Consulting Suites onsite at LRH. Gunai Kurnai language ‘welcome’ signs (Wunman Njinde) installed at all hospital entrances and community mental health sites. Aboriginal community artists enlisted to create pieces for display throughout the hospital.

ANNUAL REPORT 2019 | 27
Goals Strategies Health Service Deliverables Actions
Better Care
Target zero avoidable harm
Healthcare that focusses on outcomes
Patients and carers are active partners in care
Care fits together around people’s needs
Better Care
Put Quality First
Join up care
Partner with patients
Strengthen the workforce
Embed evidence
Ensure equal care
Increase the awareness, screening and completion of appropriate Advance Care Directives (ACDs), ensure systems are in place to support staff across the organisation understand current legislation.
Achieved. Advanced care planning audit conducted to assess screening and completion of ACDs. Activities rolled out to close gaps, for example, education program for staff, education to Community Rehabilitation Service Group clients, user friendly packs to encourage completion of ACDs. Health Independence Program providing ACD champion to continue to drive quality activities.
Reduce the rates of avoidable harm by suicide through progressing the implementation of the Zero Suicide Framework across LRH focusing on screening, evidence based interventions, training, care pathways and evaluation. Participate in the place based suicide prevention trials in Latrobe City and Bass Coast Shire.
In progress. Zero Suicide pilot has commenced in Bairnsdale. Hospital Outreach Post-suicidal Engagement (HOPE) clinicians recruited and program commenced.
Implement the evidence based ‘Choosing Wisely’ initiative in partnership with clinicians and consumers through the Better Care Victoria Collaborative.
Achieved. Coagulation study guideline and flowchart developed. Reference tools and visual communication developed and provided to nursing and medical staff with ongoing rollout of education. Input provided into the development of the Electronic Medical Record to prevent the ordering of unnecessary tests. Data as of May 2019 demonstrates a 50% decrease in inappropriate testing of coagulation studies.
Specific 2018-19 priorities (mandatory)
Disability Action Plans
Draft disability action plans are completed in 2018-19.
Submit a draft Disability Action Plan to the department by 30 June 2019 and outline the approach to full implementation of the plan within three years of publication.
Achieved. Draft Disability Action Plan completed.
Volunteer engagement
Ensure that the health service executives have appropriate measures to engage and recognise volunteers.
Undertake a benchmarking exercise with peers and the peak bodies to recognise additional opportunities for volunteer engagement with executive and expand on the current program’s recognition of service to include reporting of the volunteer program within the governance structure and regular articles in the LRH+You
Achieved. LRH Volunteer Coordinator involved in the state-wide network which is benchmarking strategies to improve engagement of volunteers within health services. Engagement strategy being developed for LRH which explores involvement, training and recognition.

28 | LATROBE REGIONAL HOSPITAL
Goals Strategies Health Service Deliverables Actions
Bullying and harassment
Actively promote positive workplace behaviours and encourage reporting. Utilise staff surveys, incident reporting data, outcomes of investigations and claims to regularly monitor and identify risks related to bullying and harassment, in particular include as a regular item in Board and Executive meetings. Appropriately investigate all reports of bullying and harassment and ensure there is a feedback mechanism to staff involved and the broader health service staff.
Provide organisational wide training to promote positive behaviours amongst staff and reduce incidents of workplace bullying and harassment. Increase staff understanding and awareness of legislative and policy requirements and ensure governance via regular reporting through the Organisational Development Committee through to the Executive and Board.
Achieved. Interactive practical training now complements online mandatory training with 362 staff trained across 69 sessions to May 2019. Workplace Support Officers from the staff group deliver presentations to work groups across the organisation. The Organisational Development Committee continues to provide governance and oversight of new strategies.
Occupational violence
Ensure all staff who have contact with patients and visitors have undertaken core occupational violence training, annually. Ensure the department’s occupational violence and aggression training principles are implemented.
Deliver the 2018–19 Occupational Violence and Aggression Prevention Implementation Plan which includes key focus areas of health service design, education, safety devices, policies, workforce development, reporting and monitoring and prevention activities.
In progress. Victorian Government funding received and plans prepared to upgrade the staff base in the Flynn inpatient unit to better monitor patient activity. OVA Coordinator appointed. Sub-committees established to progress projects across the organisation. New De-escalation Engagement and Prevention (DEEP) training has been implemented. Protective vests and search wands introduced.

ANNUAL REPORT 2019 | 29
Goals Strategies Health Service Deliverables Actions
Environmental Sustainability
Actively contribute to the development of the Victorian Government’s:
• policy to be net zero carbon by 2050 and improve environmental
• sustainability by identifying and implementing projects, including
• workforce education, to reduce material environmental impacts with
• particular consideration of procurement and waste management, and
• publicly reporting environmental performance data, including
• measureable targets related to reduction of clinical, sharps and landfill
• waste, water and energy use and improved recycling.
Initiate strategies to deliver a reduction in electricity and gas consumption across the organisation via energy efficiency improvements. Implement sustainable waste management systems to provide better social, environmental and economic value for the organisation and the community.
Achieved. Gas and water efficiency initiatives have commenced with better use of domestic hot water for heating purposes. Plumber engaged to provide specification to introduce solar heating of domestic warm water to reduce CO2 levels. Lighting to be replaced with smart LED. Procurement and installation of solar photovoltaic (PV) electricity generation to be progressed
LGBTI
Develop and promulgate service level policies and protocols, in partnership with LGBTI communities, to avoid discrimination against LGBTI patients, ensure appropriate data collection, and actively promote rights to free expression of gender and sexuality in healthcare settings.
Progress the implementation of the e-Quality Action Plan based on our recent self-assessment and work towards Rainbow Tick accreditation.
In progress. Staff groups established to work towards six Rainbow Tick accreditation standards. Draft inclusiveness statement and training module developed.

30 | LATROBE REGIONAL HOSPITAL
Statement of Priorities Part B
Key performance indicator Target 2018-19 result
High Quality and Safe Care
Accreditation
Accreditation against the National Safety and Quality Health Service Standards Accredited Achieved
Compliance with the Commonwealth’s Aged Care Accreditation Standards Accredited Achieved
Infection prevention and control
Compliance with the Hand Hygiene Australia program 80% 81%
Percentage of healthcare workers immunised for influenza 80% 85%
Patient experience
Victorian Healthcare Experience Survey – data submission Full compliance Achieved
Victorian Healthcare Experience Survey – percentage of positive patient experience – Quarter 1 95% 82%
Victorian Healthcare Experience Survey – percentage of positive patient experience responses – Quarter 2 95% 88%
Victorian Healthcare Experience Survey – percentage of positive patient experience responses – Quarter 3 95% 93%
Victorian Healthcare Experience Survey – percentage of very positive responses to questions on discharge care –Quarter 1 75% 71%
Victorian Healthcare Experience Survey – percentage of very positive responses to questions on discharge care –Quarter 2 75% 65%
Victorian Healthcare Experience Survey – percentage of very positive responses to questions on discharge care –Quarter 3 75% 79%
Victorian Healthcare Experience Survey – patients perception of cleanliness – Quarter 1 70% 75%
Victorian Healthcare Experience Survey – patients perception of cleanliness – Quarter 2 70% 81%
Victorian Healthcare Experience Survey – patients perception of cleanliness – Quarter 3 70% 86%
Healthcare associated infections (HAIs)
Number of patients with surgical site infection No outliers Not Achieved
Number of patients with ICU central-line-associated bloodstream infection (CLABSI) Nil Achieved
Rate of patients with Staphylococcus Aureus Bacteraemia (SAB) per occupied bed day ≤1/10,000 0.90
Adverse events
Sentinel events—root cause analysis (RCA) reporting All RCA reports submitted within 30 business days
Achieved
Unplanned readmission hip replacement* Less than 50 cases, below reporting threshold
Annual rate ≤2.5% N/A *
ANNUAL REPORT 2019 | 31
Key performance indicator Target 2018-19 result
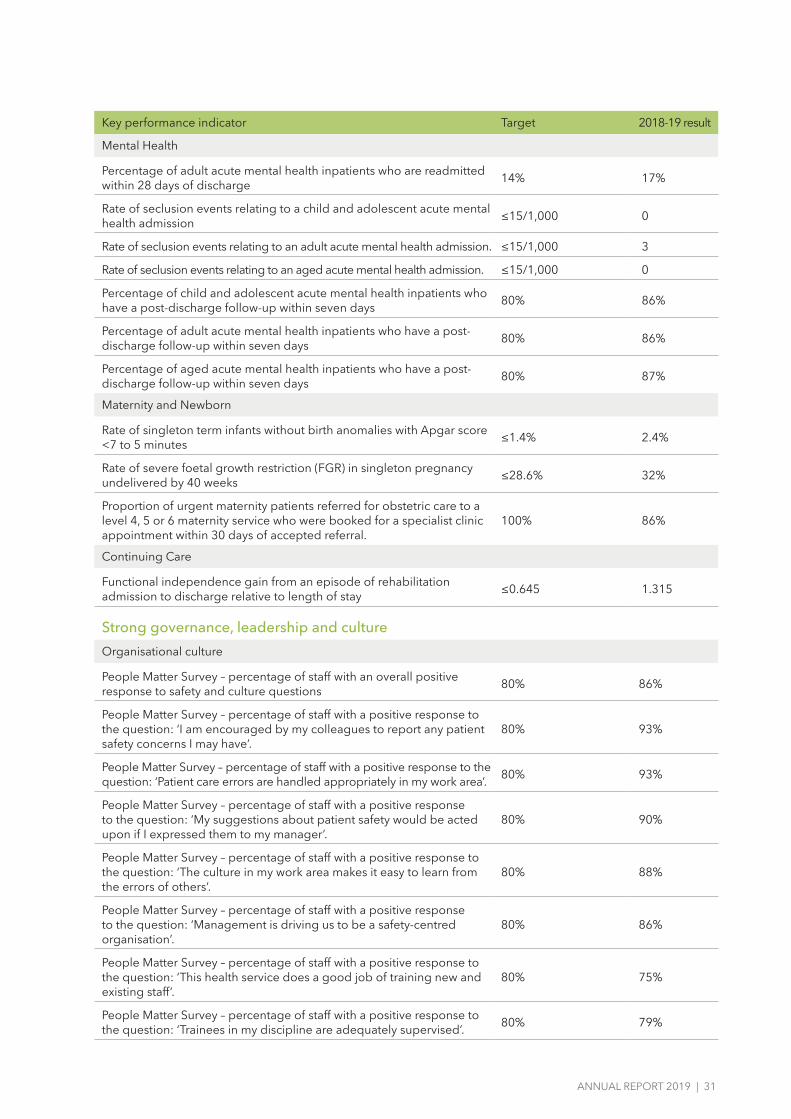
Mental Health
Percentage of adult acute mental health inpatients who are readmitted within 28 days of discharge 14% 17%
Rate of seclusion events relating to a child and adolescent acute mental health admission ≤15/1,000 0
Rate of seclusion events relating to an adult acute mental health admission. ≤15/1,000 3
Rate of seclusion events relating to an aged acute mental health admission. ≤15/1,000 0
Percentage of child and adolescent acute mental health inpatients who have a post-discharge follow-up within seven days 80% 86%
Percentage of adult acute mental health inpatients who have a post-discharge follow-up within seven days 80% 86%
Percentage of aged acute mental health inpatients who have a post-discharge follow-up within seven days 80% 87%
Maternity and Newborn
Rate of singleton term infants without birth anomalies with Apgar score <7 to 5 minutes ≤1.4% 2.4%
Rate of severe foetal growth restriction (FGR) in singleton pregnancy undelivered by 40 weeks ≤28.6% 32%
Proportion of urgent maternity patients referred for obstetric care to a level 4, 5 or 6 maternity service who were booked for a specialist clinic appointment within 30 days of accepted referral.
100% 86%
Continuing Care
Functional independence gain from an episode of rehabilitation admission to discharge relative to length of stay ≤0.645 1.315
Strong governance, leadership and culture
Organisational culture
People Matter Survey – percentage of staff with an overall positive response to safety and culture questions 80% 86%
People Matter Survey – percentage of staff with a positive response to the question: ‘I am encouraged by my colleagues to report any patient safety concerns I may have’.
80% 93%
People Matter Survey – percentage of staff with a positive response to the question: ‘Patient care errors are handled appropriately in my work area’. 80% 93%
People Matter Survey – percentage of staff with a positive response to the question: ‘My suggestions about patient safety would be acted upon if I expressed them to my manager’.
80% 90%
People Matter Survey – percentage of staff with a positive response to the question: ‘The culture in my work area makes it easy to learn from the errors of others’.
80% 88%
People Matter Survey – percentage of staff with a positive response to the question: ‘Management is driving us to be a safety-centred organisation’.
80% 86%
People Matter Survey – percentage of staff with a positive response to the question: ‘This health service does a good job of training new and existing staff’.
80% 75%
People Matter Survey – percentage of staff with a positive response to the question: ‘Trainees in my discipline are adequately supervised’. 80% 79%

32 | LATROBE REGIONAL HOSPITAL
Key performance indicator Target 2018-19 result
People Matter Survey – percentage of staff with a positive response to the question: ‘I would recommend a friend or relative to be treated as a patient here’
80% 84%
Timely access to careEmergency care
Percentage of patients transferred from ambulance to emergency department within 40 minutes 90% 80%
Percentage of Triage Category 1 emergency patients seen immediately 100% 100%
Percentage of Triage Category 1 to 5 emergency patients seen within clinically recommended time 80% 73%
Percentage of emergency patients with a length of stay in the
emergency department of less than four hours 81% 64%
Number of patients with a length of stay in the emergency department greater than 24 hours 0 0
Elective surgery
Percentage of urgency category 1 elective surgery patients admitted within 30 days 100% 100%
Percentage of urgency category 1,2 and 3 elective surgery patients
admitted within the clinically recommended time 94% 98%
Percentage of patients on the waiting list who have waited longer than the clinically recommended time for their respective triage category
5% or 15% proportional improvement from prior year
0.9%
Number of patients on the elective surgery waiting list 900 1091
Number of hospital initiated postponements per 100 scheduled elective surgery admission ≤7/100 3
Number of patients admitted from the elective surgery waiting list 5,446 5,969
Specialist clinics
Percentage of urgent patients referred by a GP or external specialist who attended a first appointment within 30 days 100% 98%
Percentage of routine patients referred by GP or external specialist who attended a first appointment within 365 days 90% 99%
Effective financial managementFinance
Operating result ($M) $1 million -0.95M
Average number of days to paying trade creditors 60 days 39 days
Average number of days to receiving patient fee debtors 60 days 39 days
Public and Private WIES activity performance to target 100% 90.46%
Adjusted current asset ratio 0.7 or 3% improvement from health service base target
1.99
Forecast number of days a health service can maintain its operations with unrestricted available cash (based on end of year forecast) 14 days 110
Actual number of days a health service can maintain its operations with unrestricted available cash, measured on the last day of each month 14 days Achieved
Measures the accuracy of forecasting the Net result from transactions (NRFT) for the current financial year ending 30 June Variance ≤$250,000 Not
Achieved

ANNUAL REPORT 2019 | 33
Statement of Priorities Part C
Funding type 2018-19 Activity Achievement
Acute Admitted
WIES Public 21,822
WIES Private 1,818
WIES DVA 278
WIES TAC 158
Acute Non-Admitted
Emergency Services 41,157
Home Enteral Nutrition 204
Specialist Clinics 28,410
Sub-Acute and Non-Acute Admitted
Sub-acute WIES – Rehabilitation Public 520
Sub-acute WIES – Rehabilitation Private 97
Sub-acute WIES – GEM Public 272
Sub-acute WIES – GEM Private 74
Sub-acute WIES – Palliative Care Public 82
Sub-acute WIES – Palliative Care Private 15
Sub-acute WIES – DVA 42
Transition Care – Bed days 7,296
Transition Care – Home days 4,923
Sub-Acute Non-Admitted
Health Independence Program – Public 33,853
Mental Health and Drug Services
Mental Health Ambulatory 66,851
Mental Health Inpatient – Available bed days 14,132
Mental Health Inpatient – Secure Unit 2,047
Mental Health Residential 3,353
Mental Health Service System Capacity N/A
Mental Health Sub-Acute 6,620
Other
Health Workforce 180
Total Funding

34 | LATROBE REGIONAL HOSPITAL
Other reporting requirements
Safe Patient Care Act 2015
Latrobe Regional Hospital has no matters to report in relation to its obligations under the Safe Patient Care Act 2015.
Compliance with Health Purchasing Victoria (HPV) Health Purchasing Policies
I, Peter Craighead, certify that Latrobe Regional Hospital has put in place appropriate internal controls and processes to ensure that it has complied with all requirements set out in the HPV Health Purchasing Policies including mandatory
HPV collective agreements as required by the Health Services Act 1988 (Vic) and has critically reviewed these controls and processes during the year.
Peter CraigheadChief Executive Latrobe Regional Hospital 27 August 2019

ANNUAL REPORT 2019 | 35
Disclosure Index
Legislation Requirement Page Reference
Ministerial Directions / Report of OperationsCharter and purposeFRD 22H Manner of establishment and the relevant Ministers Inside front, 1FRD 22H Purpose, functions, powers and duties 1FRD 22H Nature and range of services provided 1FRD 22H Activities, programs and achievements for the reporting period 3-5, 11-15FRD 22H Significant changes in key initiatives and expectations for the future 3-5
Management and structureFRD 22H Organisational structure 8-9FRD 22H Workforce data / employment and conduct principles 16FRD 22H Occupational Health and Safety 17
Financial informationFRD 22H Summary of the financial results for the year 18-20FRD 22H Significant changes in financial position during the year 18-20FRD 22H Operational and budgetary objectives and performance against
objectives18-20, 32
FRD 22H Subsequent events 18FRD 22H Details of consultancies under $10,000 19-20FRD 22H Details of consultancies over $10,000 19-20FRD 22H Disclosure of ICT expenditure 19
LegislationFRD 22H Application and operation of Freedom of Information Act 1982 21FRD 22H Compliance with building and maintenance provisions of Building Act 1993 21FRD 22H Application and operation of Protected Disclosure Act 2012 22FRD 22H Statement on National Competition Policy 22FRD 22H Application and operation of Carers Recognition Act 2012 22FRD 22H Summary of the entity’s environmental performance 22FRD 22H Additional information available on request 23
Other relevant directivesFRD 25D Local Jobs First Act disclosures 21-22SD 5.2.4 Financial Management Compliance attestation 23SD 5.2.3 Declaration in Report of Operations 5
AttestationsAttestation on Data Integrity 24Attestation on managing Conflicts of Interest 24Attestation on Integrity, Fraud and Corruption 24
Other reporting requirementsReporting of outcomes from the Statement of Priorities 2018-19 25-33Occupational Violence reporting 17Reporting of compliance Health Purchasing Victoria policy 34Reporting obligations under the Safe Patient Care Act 2015 34

36 | LATROBE REGIONAL HOSPITAL
Financial Report
Declaration Letter 37
Auditor General’s Report 38-39
Comprehensive Operating Statement 40
Balance Sheet 41
Statement of Changes in Equity 42
Cash Flow Statement 43
Notes to the Financial Statements 44

ANNUAL REPORT 2019 I 37
Declaration
Board member’s, accountable officer’s, and chief finance and accounting officer’s declaration
The attached financial statements for Latrobe Regional Hospital have been prepared in accordance with Direction
5.2 of the Standing Directions of the Assistant Treasure under the Financial Management Act 1994, applicable
Financial Reporting Directions, Australian Accounting Standards including Interpretations, and other mandatory
professional reporting requirements.
We further state that, in our opinion, the information set out in the comprehensive operating statement,
balance sheet, statement of changes in equity, cash flow statement and accompanying notes, presents fairly
the financial transactions during the year ended 30 June 2019 and the financial position of Latrobe Regional Hospital at 30 June 2019.
At the time of signing, we are not aware of any circumstance which would render any particulars included
in the financial statements to be misleading or inaccurate.
We authorise the attached financial statements for issue on 27 August 2019.
Linda McCoy
Chair
Peter Craighead
Chief Executive
Michael Glaubitz
Chief Finance & Accounting Officer
Latrobe Regional Hospital
Traralgon West
27 August 2019

38 I LATROBE REGIONAL HOSPITAL

ANNUAL REPORT 2019 I 39
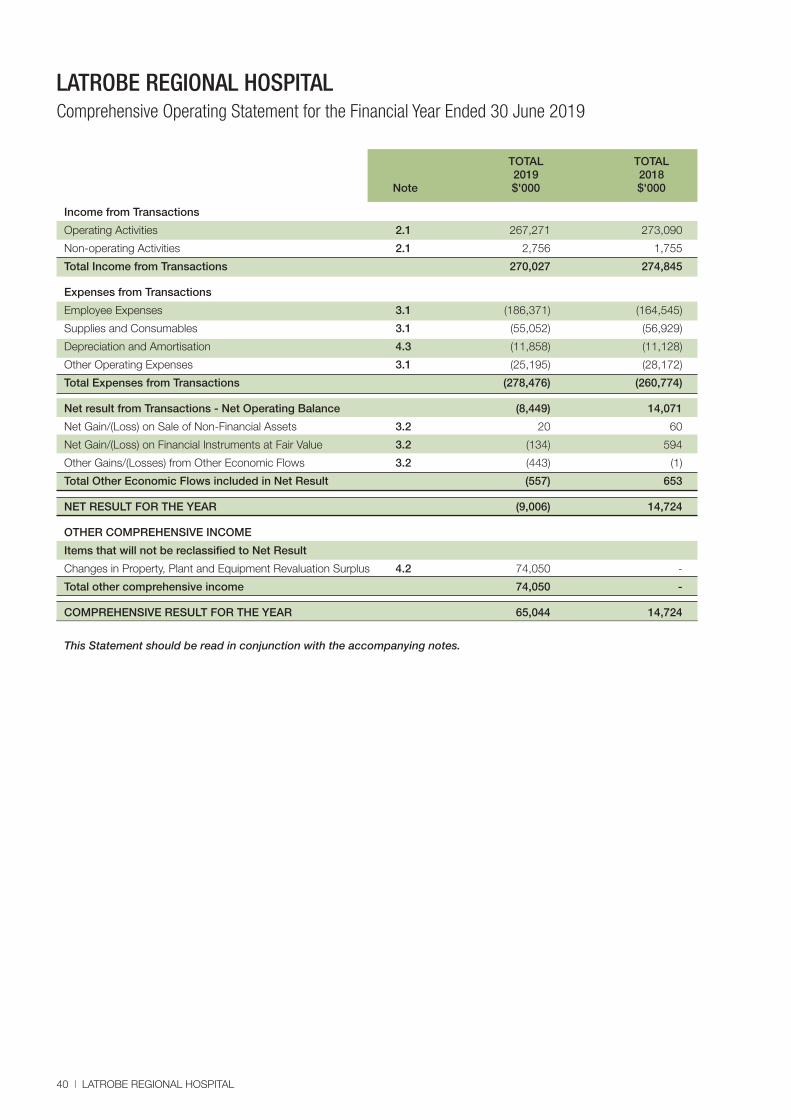
LATROBE REGIONAL HOSPITAL Comprehensive Operating Statement for the Financial Year Ended 30 June 2019
TOTAL TOTAL 2019 2018
Note $'000 $'000
40 I LATROBE REGIONAL HOSPITAL
Income from Transactions
Operating Activities 2.1 267,271 273,090
Non-operating Activities 2.1 2,756 1,755
Total Income from Transactions 270,027 274,845
Expenses from Transactions
Employee Expenses 3.1 (186,371) (164,545)
Supplies and Consumables 3.1 (55,052) (56,929)
Depreciation and Amortisation 4.3 (11,858) (11,128)
Other Operating Expenses 3.1 (25,195) (28,172)
Total Expenses from Transactions (278,476) (260,774)
Net result from Transactions - Net Operating Balance (8,449) 14,071
Net Gain/(Loss) on Sale of Non-Financial Assets 3.2 20 60
Net Gain/(Loss) on Financial Instruments at Fair Value 3.2 (134) 594
Other Gains/(Losses) from Other Economic Flows 3.2 (443) (1)
Total Other Economic Flows included in Net Result (557) 653
NET RESULT FOR THE YEAR (9,006) 14,724
OTHER COMPREHENSIVE INCOME
Items that will not be reclassified to Net Result
Changes in Property, Plant and Equipment Revaluation Surplus 4.2 74,050 -
Total other comprehensive income 74,050 -
COMPREHENSIVE RESULT FOR THE YEAR 65,044 14,724
This Statement should be read in conjunction with the accompanying notes.

ANNUAL REPORT 2019 I 41
LATROBE REGIONAL HOSPITAL Balance Sheet as at 30 June 2019
TOTAL TOTAL 2019 2018
Note $'000 $'000
ASSETS
Current Assets
Cash and Cash Equivalents 6.1 62,549 29,137
Receivables 5.1 5,552 4,906
Investments and Other Financial Assets 4.1 - 28,737
Inventories 1,316 1,383
Prepayments 1,372 1,010
Total Current Assets 70,789 65,173
Non-Current Assets
Receivables 5.1 5,726 4,402
Investments and Other Financial Assets 4.1 20,695 20,379
Property, Plant & Equipment 4.2 (a) 270,451 202,854
Total Non-Current Assets 296,872 227,635
TOTAL ASSETS 367,661 292,808
LIABILITIES
Current Liabilities
Payables 5.2 25,274 19,047
Provisions 3.4 35,897 33,351
Other Current Liabilities 5.3 924 818
Non-Interest Bearing Liabilities 50 50
Total Current Liabilities 62,145 53,266
Non-Current Liabilities
Provisions 3.4 7,572 6,610
Non-Interest Bearing Liabilities 240 272
Total Non-Current Liabilities 7,812 6,882
TOTAL LIABILITIES 69,957 60,148
NET ASSETS 297,704 232,660
EQUITY
Property, Plant & Equipment Revaluation Surplus 4.2 (f) 123,427 49,377
Restricted Specific Purpose Surplus 26,048 21,213
Contributed Capital 26,652 26,652
Accumulated Surpluses 121,577 135,418
TOTAL EQUITY 297, 704 232,660
This Statement should be read in conjunction with the accompanying notes.

42 I LATROBE REGIONAL HOSPITAL
LATROBE REGIONAL HOSPITAL Statement of Changes in Equity for the Financial Year Ended 30 June 2019
Property Plant & Restricted
Equipment Specific Accumulated Revaluation Purpose Contributed Surpluses/
Surplus Surplus Capital (Deficits) Total Note $’000 $’000 $’000 $’000 $’000
Balance at 30 June 2017 49,377 20,339 26,652 121,568 217,936
Net result for the year - - - 14,724 14,724
Transfer to accumulated surplus - 874 - (874) -
Balance at 30 June 2018 49,377 21,213 26,652 135,418 232,660
Net result for the year - - - (9,006) (9,006)
Other comprehensive income for the year 74,050 74,050
Transfer to accumulated surplus - 4,835 - (4,835) -
Balance at 30 June 2019 123,427 26,048 26,652 121,577 297,704
This Statement should be read in conjunction with the accompanying notes.

ANNUAL REPORT 2019 I 43
LATROBE REGIONAL HOSPITAL Cash Flow Statement for the Financial Year Ended 30 June 2019
TOTAL TOTAL 2019 2018
Note $'000 $'000
CASH FLOWS FROM OPERATING ACTIVITIES
Operating grants from government 242,564 232,439
Capital grants from government 5,085 15,527
Patient and resident fees received 3,943 3,837
Donations and bequests received 120 244
GST received from ATO 7,776 7,968
Interest received 894 803
Capital grants from non-government - 656
Capital donations and bequests received 116 115
Other receipts 23,219 23,509
Total receipts 283,717 285,098
Employee expenses paid (167,907) (150,201)
Payment for share of Rural Health Alliance (1,809) (1,713)
Payments for supplies & consumables (103,977) (101,556)
Total payments (273,693) (253,470)
NET CASH FLOW FROM OPERATING ACTIVITIES 8.1 10,024 31,628
CASH FLOWS FROM INVESTING ACTIVITIES
Purchase of investments - (4,000)
Proceeds from disposal of investments 29,102 -
Proceeds from impaired investments - 32
Proceeds from disposal of non-financial assets 30 60
Purchase of non-financial assets (5,395) (16,943)
NET CASH FLOW FROM/(USED IN) INVESTING ACTIVITIES 23,737 (20,851)
CASH FLOWS FROM FINANCING ACTIVITIES
Repayment of borrowings (50) (50)
Receipt of accomodation deposits 306 -
Repayment of accomodation deposits (300) -
NET CASH FLOW USED IN FINANCING ACTIVITIES (44) (50)
NET INCREASE IN CASH AND CASH EQUIVALENTS HELD 33,717 10,727
Cash and cash equivalents at beginning of year 28,832 18,105
CASH AND CASH EQUIVALENTS AT END OF YEAR 6.1 62,549 28,832
This Statement should be read in conjunction with the accompanying notes.

44 I LATROBE REGIONAL HOSPITAL
LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
Note 1: Summary of Significant Accounting Policies
Basis of presentation
These financial statements are in Australian dollars and the historical cost convention is used unless a different measurement basis is specifically disclosed in the note associated with the item measured on a different basis.
The accrual basis of accounting has been applied in preparing these financial statements, whereby assets, liabilities, equity, income and expenses are recognised in the reporting period to which they relate, regardless of when cash is received or paid.
Summary of Significant Accounting Policies
These annual financial statements represent the audited general purpose financial statements for Latrobe Regional Hospital for the year ended 30 June 2019. The report provides users with information about the Hospital’s stewardship of resources entrusted to it.
(a) Statement of compliance
These financial statements are general purpose financial statements which have been prepared in accordance with the Financial Management Act 1994 and applicable AASBs, which include interpretations issued by the Australian Accounting Standards Board (AASB). They are presented in a manner consistent with the requirements of AASB 101 Presentation of Financial Statements.
The financial statements also comply with relevant Financial Reporting Directions (FRDs) issued by the Department of Treasury and Finance, and relevant Standing Directions (SDs) authorised by the Assistant Treasurer.
The Hospital is a not-for profit entity and therefore applies the additional AUS paragraphs applicable to “not-for-profit” Hospitals under the AASBs.
(b) Reporting entity
The financial statements include all the controlled activities of the Hospital.
Its principal address is: Cnr Princes Highway and Village Avenue Traralgon West, Victoria 3844.
A description of the nature of Hospital’s operations and its principal activities is included in the report of operations, which does not form part of these financial statements.
(c) Basis of accounting preparation and measurement
Accounting policies are selected and applied in a manner which ensures that the resulting financial information satisfies the concepts of relevance and reliability, thereby ensuring that the substance of the underlying transactions or other events is reported.
The accounting policies have been applied in preparing the financial statements for the year ended 30 June 2019, and the comparative information presented in these financial statements for the year ended 30 June 2018.
The financial statements are prepared on a going concern basis (refer to Note 8.8 Economic Dependency).
These financial statements are presented in Australian dollars, the functional and presentation currency of the Hospital.
All amounts shown in the financial statements have been rounded to the nearest thousand dollars, unless otherwise stated. Minor discrepancies in tables between totals and sum of components are due to rounding.
The hospital operates on a fund accounting basis and maintains three funds: Operating, Specific Purpose and Capital Funds.
The financial statements, except for cash flow information, have been prepared using the accrual basis of accounting. Under the accrual basis, items are recognised as assets, liabilities, equity, income or expenses when they satisfy the definitions and recognition criteria for those items, that is, they are recognised in the reporting period to which they relate, regardless of when cash is received or paid.
Judgements, estimates and assumptions are required to be made about the carrying values of assets and liabilities that are not readily apparent from other sources. The estimates and underlying assumptions are reviewed on an ongoing basis. The estimates and associated assumptions are based on professional judgements derived from historical experience and various other factors that are believed to be reasonable under the circumstances. Actual results may differ from these estimates.
Revisions to accounting estimates are recognised in the period in which the estimate is revised and also in future periods that are affected by the revision. Judgements and assumptions made by management in the application of AABSs that have significant effects on the financial statements and estimates relate to:
• The fair value of land, buildings and plant and equipment (refer to Note 4.2 Property, Plant and Equipment); • Defined benefit superannuation expense (refer to Note 3.5 Superannuation); • Employee benefit provisions are based on likely tenure of existing staff, patterns of leave claims, future salary movements and future
discount rates (refer to Note 3.4 Employee Benefits in the Balance Sheet); and
Goods and Services Tax (GST)
Income, expenses and assets are recognised net of the amount of associated GST, unless the GST incurred is not recoverable from the Australian Taxation Office (ATO). In this case the GST payable is recognised as part of the cost of acquisition of the asset or as part of the expense.
Receivables and payables are stated inclusive of the amount of GST receivable or payable. The net amount of GST recoverable from, or payable to, the ATO is included with other receivables or payables in the Balance Sheet.

ANNUAL REPORT 2019 I 45
LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
Note 1: Summary of Significant Accounting Policies
Cash flows are presented on a gross basis. The GST components of cash flows arising from investing or financing activities which are recoverable from, or payable to the ATO, are presented as operating cash flow.
Commitments and contingent assets and liabilities are presented on a gross basis.
(d) Jointly controlled operation
Joint control is the contractually agreed sharing of control of an arrangement, which exists only when decisions about the relevant activities require the unanimous consent of the parties sharing control.In respect of any interest in joint operations, Latrobe Regional Hospital recognises in the financial statements:
• its assets, including its share of any assets held jointly; • any liabilities including its share of liabilities that it had incurred; • its revenue from the sale of its share of the output from the joint operation; • its share of the revenue from the sale of any output by the operation; and • its expenses, including its share of any expenses incurred jointly.
Latrobe Regional Hospital is a member of the Gippsland Health Alliance and retains joint control over the arrangement, which it has classified as a joint operation (refer to Note 8.7 Jointly Controlled Operations).
Intersegment Transactions
Transactions between segments within the hospital have been eliminated to reflect the extent of the hospital’s operations as a group.
(e) Equity
Contributed capital
Consistent with the requirements of AASB 1004 Contributions, contributions by owners (that is, contributed capital and its repayment) are treated as equity transactions and, therefore, do not form part of the income and expense of the Hospital.Transfers of net assets arising from administrative restructurings are treated as distributions to or contributions by owners. Transfers of net liabilities arising from administrative restructurings are treated as distributions to owners. Other transfers that are in the nature of contributions or distributions or that have been designated as contributed capital are also treated as contributed capital.
Specific Restricted Purpose Surplus
The Specific Restricted Purpose Surplus is established where the Hospital has possession or title to the funds but has no discretion to amend or vary the restriction and /or condition underlying the funds received.
(f) Comparatives
Where applicable, the comparative figures have been restated to align with presentation in the current year. Figures have been restated in the Comprehensive Operating Statement, Note 2.1, Note 3.1, Note 3.2 and Note 7.1.

46 I LATROBE REGIONAL HOSPITAL
LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
Note 2: Funding Delivery of our Services
The hospital's overall objective is to provide quality health service that supports and enhances the wellbeing of all Victorians.
The hospital is predominantly funded by accrual based grant funding for the provision of outputs.
The hospital also receives income from the supply of services.
Structure:
2.1 Income from Transactions
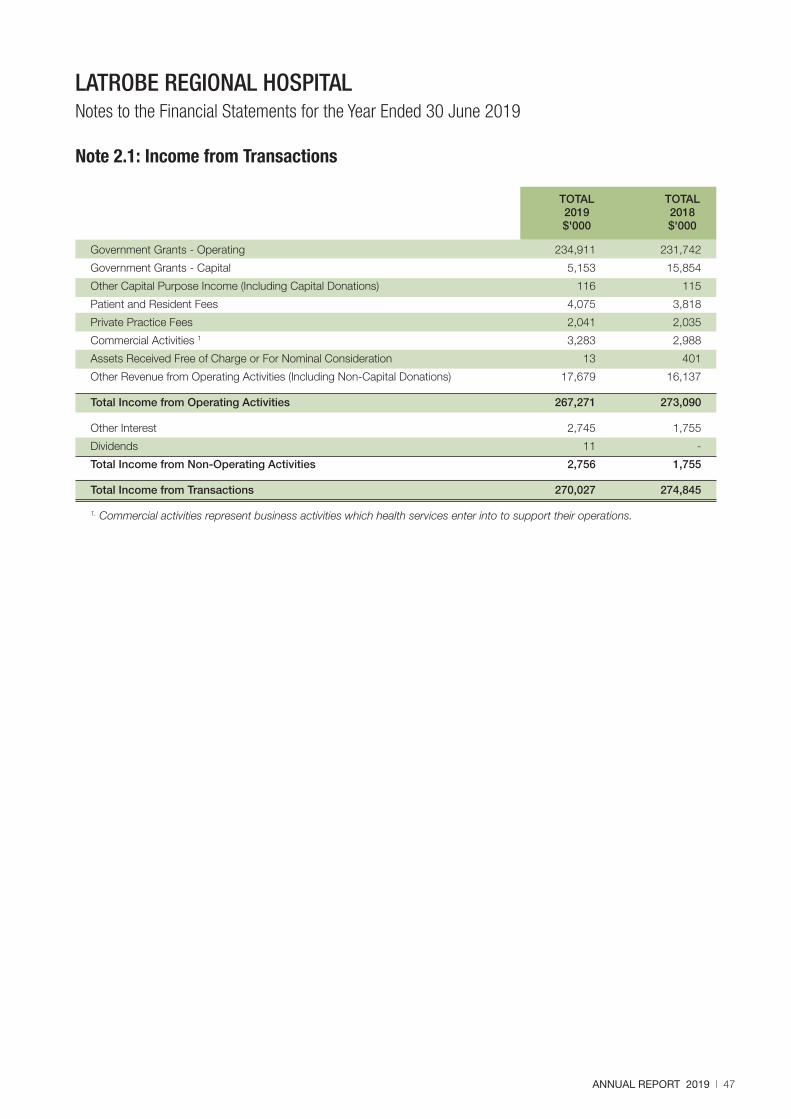
ANNUAL REPORT 2019 I 47
LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
TOTAL TOTAL 2019 2018 $'000 $'000
Government Grants - Operating 234,911 231,742
Government Grants - Capital 5,153 15,854
Other Capital Purpose Income (Including Capital Donations) 116 115
Patient and Resident Fees 4,075 3,818
Private Practice Fees 2,041 2,035
Commercial Activities 1 3,283 2,988
Assets Received Free of Charge or For Nominal Consideration 13 401
Other Revenue from Operating Activities (Including Non-Capital Donations) 17,679 16,137
Total Income from Operating Activities 267,271 273,090
Other Interest 2,745 1,755
Dividends 11 -
Total Income from Non-Operating Activities 2,756 1,755
Total Income from Transactions 270,027 274,845
1. Commercial activities represent business activities which health services enter into to support their operations.
Note 2.1: Income from Transactions

48 I LATROBE REGIONAL HOSPITAL
Revenue recognition
Income is recognised in accordance with AASB 118 Revenue and is recognised as to the extent that it is probable that the economic benefits will flow to Latrobe Regional Hospital and the income can be reliably measured at fair value. Unearned income at reporting date is reported as income received in advance.
Amounts disclosed as revenue is, where applicable, net of returns, allowances and duties and taxes.
Government grants and other transfers of income (other than contributions by owners)
In accordance with AASB 1004 Contributions, government grants and other transfers of income (other than contributions by owners) are recognised as income when the Hospital gains control of the underlying assets irrespective of whether conditions are imposed on the Hospital’s use of the contributions.
The Department of Health and Human Services makes certain payments on behalf of the hospital. These amounts have been brought to account as grants in determining the operating result for the year by recording them as revenue.
Contributions are deferred as income in advance when the Hospital has a present obligation to repay them and the present obligation can be reliably measured.
Non-cash contributions from the Department of Health and Human Services
The Department of Health and Human Services makes some payments on behalf of the hospital as follows: – The Victorian Managed Insurance Authority non-medical indemnity insurance payments are recognised as revenue following
advice from the Department of Health and Human Services. – Long Service Leave (LSL) revenue is recognised upon finalisation of movements in LSL liability in line with the long service leave
funding arrangements set out in the Department of Health and Human Services Hospital Circular.
Patient and resident fees
Patient fees are recognised as revenue on an accrual basis.
Private practice fees
Private practice fees are recognised as revenue at the time invoices are raised, and include recoupments from private practice for the use of hospital facilities.
Revenue from commercial activities
Revenue from commercial activities such as property rental and the cafeteria are recognised on an accrual basis.
Fair value of assets and services received free of charge or for nominal consideration
Resources received free of charge or for nominal consideration are recognised at their fair value when the transferee obtains control over them, irrespective of whether restrictions or conditions are imposed over the use of the contributions, unless received from another hospital or agency as a consequence of a restructuring of administrative arrangements. In the latter case, such transfer will be recognised at carrying amount. Contributions in the form of services are only recognised when a fair value can be reliably determined and the service would have been purchased if not received as a donation.
Other income
Other income is recognised as revenue when received. Other income includes recoveries for salaries and wages and external services provided, and donations and bequests. If donations are for a specific purpose, they may be appropriated to a surplus, such as the specific restricted purpose surplus.
Interest revenue
Interest revenue is recognised on a time proportionate basis that takes into account the effective yield of the financial asset, which allocates interest over the relevant period.
Dividend revenue
Dividend revenue is recognised when the right to receive payment is established. Dividends represent the income arising from the hospital's investments in financial assets.
Note 2.1: Income from Transactions (continued)
LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
Note 3: The Cost of Delivering Services
This section provides an account of the expenses incurred by the hospital in delivering services and outputs. In Section 2, the funds that enable the provision of services were disclosed and in this note the cost associated with provision of services are recorded.
Structure:
3.1 Expenses from Transactions
3.2 Other Economic Flows
3.3 Analysis of Expenses and Revenue by Internally Managed and Restricted Specific Purpose Funds
3.4 Employee Benefits in the Balance Sheet
3.5 Superannuation
ANNUAL REPORT 2019 I 49

50 I LATROBE REGIONAL HOSPITAL
TOTAL TOTAL 2019 2018 $'000 $'000
Salaries and Wages 138,860 121,874 On-costs 33,205 29,131 Agency Expenses 1,246 953 Fee for Service Medical Officer Expenses 11,116 10,390 Workcover Premium 1,944 2,197
Total Employee Expenses 186,371 164,545 Drug Supplies 14,755 14,840 Medical and Surgical Supplies (including Prostheses) 12,864 11,813 Diagnostic and Radiology Supplies 11,341 10,087 Other Supplies and Consumables 16,092 20,189
Total Supplies and Consumables 55,052 56,929 Finance Costs 41 26 Fuel, Light, Power and Water 2,724 2,452 Repairs and Maintenance 626 3,166 Maintenance Contracts 4,479 4,241 Medical Indemnity Insurance 3,794 3,727 Other Administrative Expenses 13,034 13,526 Expenditure for Capital Purposes 497 1,034
Total Other Operating Expenses 25,195 28,172 Depreciation and Amortisation (refer Note 4.3) 11,858 11,128
Total Other Non-Operating Expenses 11,858 11,128
Total Expenses from Transactions 278,476 260,774
Expenses are recognised as they are incurred and reported in the financial year to which they relate.
Note 3.1: Expenses from Transactions
LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
Employee expenses Employee expenses include:
• salaries and wages (including fringe benefits tax, leave entitlements, termination payments); • on costs; • agency expenses; • fee for service medical officer expenses; • workcover premium.
Supplies and consumables Supplies and services costs which are recognised as an expense in the reporting period in which they are incurred. The carrying amounts of any inventories held for distribution are expensed when distributed.
Finance costs Finance costs include:
• interest on bank overdrafts and short-term and long-term borrowings (Interest expense is recognised in the period in which it is incurred);
• amortisation of discounts or premiums relating to borrowings.
Other operating expenses Other operating expenses generally represent the day-to-day running costs incurred in normal operations and include such things as:
• Fuel, light and power; • Repairs and maintenance; • Other administrative expenses; • Expenditure for capital purposes (represents expenditure related to the purchase of assets that are below the capitlisation threshold).
The Department of Health and Human Services also makes certain payments on behalf of the hospital. These amounts have been brought to account as grants in determining the operating result for the year by recording them as revenue and also recording the related expense.
Non-operating expenses Other non-operating expenses generally represent expenditure for outside the normal operations such as depreciation and amortisation, and assets and services provided free of charge or for nominal consideration.

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
ANNUAL REPORT 2019 I 51
TOTAL TOTAL 2019 2018 $'000 $'000
Net gain/(loss) on sale of non-financial assets
Net gain on disposal of property plant and equipment 20 60
Total net gain/(loss) on non-financial assets 20 60
Net gain/(loss) on financial instruments at fair value
Bad debts written off unilaterally 9 4
Net gain/(loss) on disposal of financial instruments (143) 590
Total net gain/(loss) on financial instruments at fair value (134) 594
Other gains/(losses) from other economic flows
Net gain/(loss) arising from revaluation of long service liability (443) (1)
Total other gains/(losses) from other economic flows (443) (1)
Total other gains/(losses) from economic flows (557) 653
Other economic flows are changes in the volume or value of an asset or liability that do not result from transactions. Other gains/(losses) from other economic flows include the gains or losses from: • the revaluation of the present value of the long service leave liability due to changes in the bond interest rates.
Net gain/(loss) on non-financial assets Net gain/(loss) on non-financial assets and liabilities includes realised and unrealised gains and losses as follows: • Revaluation gains/ (losses) of non-financial physical assets (Refer to Note 4.2 Property plant and equipment.) • Net gain/ (loss) on disposal of non-financial assets • Any gain or loss on the disposal of non-financial assets is recognised at the date of disposal.
Net gain/(loss) on financial instruments at fair value Net gain/(loss) on financial instruments at fair value includes: • realised and unrealised gains and losses from revaluations of financial instruments at fair value; • impairment and reversal of impairment for financial instruments at amortised cost refer to Note 4.1 Investments
and other financial assets; and • disposals of financial assets and derecognition of financial liabilities.
Other gains/(losses) from other economic flows Other gains/(losses) include: • the revaluation of the present value of the long service leave liability due to changes in the bond rate movements,
inflation rate movements and the impact of changes in probability factors.
Note 3.2: Other Economic Flows
Note 3.2: Analysis of Expense and Revenue by Internally Managed and Restricted Specific Purpose Funds
TOTAL TOTAL TOTAL TOTAL 2019 2018 2019 2018 $’000 $’000 $’000 $’000
Commercial Activities Pharmacy Services Regional 296 332 296 332 Consulting Suites 744 677 744 677 ICT External Sales 13 9 - 2 Salary Packaging 150 159 454 436 Regional Biomedical 27 25 63 52 External Supply 39 53 48 45 Tandara Caravan Park 330 538 422 511 Lung Function Respiratory Lab 60 34 106 74 Cafeteria 1,150 784 1,150 808 Television Service 5 30 - 51
Total Commercial Activities 2,814 2,641 3,283 2,988
EXPENSE REVENUE

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
52 I LATROBE REGIONAL HOSPITAL
TOTAL TOTAL 2019 2018 $'000 $'000
Current Provisions
Employee Benefits(i)
Accrued Days Off - Unconditional and expected to be settled wholly within 12 months(ii) 510 496 Annual Leave - Unconditional and expected to be settled wholly within 12 months(ii) 13,000 11,298 - Unconditional and expected to be settled wholly after 12 months(iii) 831 1,541 Long Service Leave - Unconditional and expected to be settled wholly within 12 months(ii) 3,000 2,500 - Unconditional and expected to be settled wholly after 12 months(iii) 14,606 13,868 Other - Unconditional and expected to be settled wholly within 12 months(ii) 32 24
31,979 29,727 Provisions Related to Employee Benefit On-Costs - Unconditional and expected to be settled within 12 months(ii) 2,134 1,921 - Unconditional and expected to be settled after 12 months(iii) 1,784 1,703
3,918 3,624 Total Current Provisions 35,897 33,551
Non-Current Provisions Conditional long service leave 6,881 5,969 Provisions related to Employee Benefit On-Costs 691 641
Total Non-Current Provisions 7,572 6,610
Total Provisions 43,469 39,961
(a) Employee Benefits and Related On-Costs Current Employee Benefits and Related On-Costs Unconditional Long Service Leave Entitlement 19,587 18,201 Annual Leave Entitlements 15,694 14,560 Substitution Leave 38 27 Accrued Days Off 578 563 Non-Current Employee Benefits and Related On-Costs Conditional Long Service Leave Entitlements 7,572 6,610
Total Employee Benefits and Related On-Costs 43,469 39,961
(b) Movements in provisions Movement in long service leave: Balance at start of year 24,811 23,063 Provision made during the year - Revaluations 443 (1) - Expense recognising Employee Service 4,784 4,064 Settlement made during the year (2,879) (2,315)
Balance at end of year 27,159 24,811
Notes: (i) Employee benefits consist of amounts for accrued days off, annual leave and long service leave accrued
by employees, not including on-costs. (ii) The amounts disclosed are nominal amounts. (iii) The amounts disclosed are discounted to present values.
Note 3.4: Employee Benefits in the Balance Sheet

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
ANNUAL REPORT 2019 I 53
Note 3.4: Employee Benefits in the Balance Sheet (continued) Employee Benefit Recognition
Provision is made for benefits accruing to employees in respect of wages and salaries, annual leave and long service leave for services rendered to the reporting date as an expense during the period the services are delivered.
Provisions
Provisions are recognised when the hospital has a present obligation, the future sacrifice of economic benefits is probable, and the amount of the provision can be measured reliably.
The amount recognised as a liability is the best estimate of the consideration required to settle the present obligation at reporting date, taking into account the risks and uncertainties surrounding the obligation.
Annual leave and accrued days off
Liabilities for annual leave and accrued days off are recognised in the provision for employee benefits as “current liabilities”, because the hospital does not have an unconditional right to defer settlements of these liabilities.
Depending on the expectation of the timing of settlement, liabilities for wages and salaries, annual leave and accrued days off are measured at:
• Nominal value - if the hospital expects to wholly settle within 12 months; or • Present value - if the hospital does not expect to wholly settle within 12 months.
Long service leave (LSL)
The liability for long service leave (LSL) is recognised in the provision for employee benefits.
Unconditional LSL is disclosed in the notes to the financial statements as a current liability even where the Hospital does not expect to settle the liability within 12 months because it will not have the unconditional right to defer the settlement of the entitlement should an employee take leave within 12 months. An unconditional right arises after a qualifying period.
The components of this current LSL liability are measured at:
• Nominal value - if the Hospital expects to wholly settle within 12 months, and
• Present value - if the Hospital does not expect to wholly settle within 12 months.
Conditional LSL is disclosed as a non-current liability.
Any gain or loss following revaluation of the present value of non-current LSL liability is recognised as a transaction, except to the extent that a gain or loss arises due to changes in estimations e.g. bond rate movements, inflation rate movements and changes in probability factors which are then recognised as other economic flows.
Termination Benefits
Termination benefits are payable when employment is terminated before the normal retirement date or when an employee decides to accept an offer of benefits in exchange for the termination of employment.
On-Costs related to employee benefits
Provision for on-costs, such as workers compensation and superannuation are recognised separately from provisions for employee benefits.

54 I LATROBE REGIONAL HOSPITAL
LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
TOTAL TOTAL TOTAL TOTAL 2019 2018 2019 2018 $’000 $’000 $’000 $’000
Defined Benefit Plans:i
Other 2 - - -
Defined contribution plans:
HESTA 6,726 6,023 565 498
First State 5,309 4,808 418 396
Other 743 564 219 239
Total 12,780 11,395 1,202 1,133
Paid contribution Contribution Outstanding for the year at Year End
Note 3.5: Superannuation
Employees of the hospital are entitled to receive superannuation benefits and the hospital contributes to both defined benefit and defined contribution plans. The defined benefit plan provides benefits based on years of service and final average salary.
Defined benefit superannuation plans
The amount charged to the Comprehensive Operating Statement in respect of defined benefit superannuation plans represents the contributions made by the Hospital to the superannuation plans in respect of the services of current staff during the reporting period. Superannuation contributions are made to the plans based on the relevant rules of each plan and are based upon actuarial advice.
The Hospital does not recognise any unfunded defined benefit liability in respect of the plans because the hospital has no legal or constructive obligation to pay future benefits relating to its employees; its only obligation is to pay superannuation contributions as they fall due. The Department of Treasury and Finance discloses the State's defined benefits liabilities in its disclosure for administered items.
However superannuation contributions paid or payable for the reporting period are included as part of employee benefits in the Comprehensive Operating Statement of the hospital.
The name, details and amounts that have been expensed in relation to the major employee superannuation funds and contributions made by Latrobe Regional Hospital are disclosed above.
Defined contribution superannuation plans
In relation to defined contribution (i.e. accumulation) superannuation plans, the associated expense is simply the employer contributions that are paid or payable in respect of employees who are members of these plans during the reporting period. Contributions to defined contribution superannuation plans are expensed when incurred.
i The basis for determining the level of contributions is determined by the various actuaries of the defined benefit superannuation plans.
LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
ANNUAL REPORT 2019 I 55
Note 4: Key Assets to Support Service Delivery Latrobe Regional Hospital controls infrastructure and other investments that are utilised in fulfilling its objectives and conducting its activities. They represent the key resources that have been entrusted to the Hospital to be utilised for delivery of those outputs.
Structure:
4.1 Investments and Other Financial Assets
4.2 Property, Plant and Equipment
4.3 Depreciation and Amortisation
LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
56 I LATROBE REGIONAL HOSPITAL
TOTAL TOTAL 2019 2018 $'000 $'000
CURRENT
- Term Deposit
Aust. Dollar Term Deposits > 3 months - 28,737
TOTAL CURRENT - 28,737
NON CURRENT
- Equities and Managed Investment Schemes
Victorian Funds Management Corporation 20,695 19,984
Investments In Listed Shares - 395
TOTAL NON CURRENT 20,695 20,379
TOTAL INVESTMENTS AND OTHER FINANCIAL ASSETS
Represented by:
Health Service Investments 20,695 49,116
TOTAL INVESTMENTS AND OTHER FINANCIAL ASSETS 20,695 49,116
Note 4.1: Investments and Other Financial Assets
Investment recognition
Investments are recognised and derecognised on trade date where purchase or sale of an investment is under a contract whose terms require delivery of the investment within the timeframe established by the market concerned, and are initially measured at fair value, net of transaction costs.
Investments are classified as loans and receivables or available-for-sale financial assets.
The hospital classifies its other financial assets between current and non-current assets based on the Board's intention at balance date with respect to the timing of disposal of each asset.
The hospital assesses at each balance sheet date whether a financial asset or group of financial assets is impaired.
The hospital's investments must comply with Standing Direction 3.7.2 - Treasury Management, including Central Banking System.
All financial assets, except for those measured at fair value through the Comprehensive Operating Statement are subject to annual review for impairment.
De-recognition of financial assets
A financial asset (or, where applicable, a part of a financial asset or part of a group of similar financial assets) is derecognised when:
- the rights to receive cash flows from the asset have expired; or
- the hospital retains the right to receive cash flows from the asset, but has assumed an obligation to pay them in full without material delay to a third party under a ‘pass through’ arrangement; or
- the hospital has transferred its rights to receive cash flows from the asset and either:
a) has transferred substantially all the risks and rewards of the asset; or
b) has neither transferred nor retained substantially all the risks and rewards of the asset, but has transferred control of the asset.
Where the hospital has neither transferred nor retained substantially all the risks and rewards or transferred control, the asset is recognised to the extent of the hospital’s continuing involvement in the asset.
Impairment of financial assets
At the end of each reporting period Latrobe Regional Hospital assesses whether there is objective evidence that a financial asset or group of financial asset is impaired. All financial instrument assets, except those measured at fair value through profit or loss, are subject to annual review for impairment.

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
ANNUAL REPORT 2019 I 57
Note 4.2: Property, Plant & Equipment Initial recognition
Items of property, plant and equipment are measured initially at cost and subsequently re-valued at fair value less accumulated depreciation and impairment loss. Where an asset is acquired for no or nominal cost, the cost is its fair value at the date of acquisition.
The cost of a leasehold improvement is capitalised as an asset and depreciated over the shorter of the remaining term of the lease or the estimated useful life of the improvements.
Theoretical opportunities that may be available in relation to the asset(s) are not taken into account until it is virtually certain that any restrictions will no longer apply. Therefore, unless otherwise disclosed, the current use of these non-financial physical assets will be their highest and best uses.
Land and buildings are recognised initially at cost and subsequently measured at fair value less accumulated depreciation and accumulated impairment loss.
Revaluations of non-current physical assets
Non-current physical assets are measured at fair value and are re-valued in accordance with FRD 103H Non-current physical assets. This revaluation process normally occurs every five years, based upon the asset’s Government Purpose Classification, but may occur more frequently if fair value assessments indicate material changes in values. Independent valuers are used to conduct these scheduled revaluations and any interim revaluations are determined in accordance with the requirements of the FRDs. Revaluation increments or decrements arise from differences between an asset’s carrying value and fair value.
Revaluation increments are recognised in ‘other comprehensive income’ and are credited directly to the asset revaluation surplus, except that, to the extent that an increment reverses a revaluation decrement in respect of that same class of asset previously recognised as an expense in net result, the increment is recognised as income in the net result.
Revaluation decrements are recognised in ‘other comprehensive income’ to the extent that a credit balance exists in the asset revaluation surplus in respect of the same class of property, plant and equipment.
Revaluation increases and revaluation decreases relating to individual assets within an asset class are offset against one another within that class but are not offset in respect of assets in different classes.
Revaluation surplus is not transferred to accumulated funds on de-recognition of the relevant asset, except where an asset is transferred via contributed capital.
In accordance with FRD 103H, Latrobe Regional Hospital’s non-current physical assets were assessed to determine whether revaluation of the non-current physical assets was required.
Fair value measurement
Fair value is the price that would be received to sell an asset or paid to transfer a liability in an orderly transaction between market participants at the measurement date.
For the purpose of fair value disclosures, the hospital has determined classes of assets and liabilities on the basis of the nature, characteristics and risks of the asset or liability and the level of the fair value hierarchy as explained above.
In addition, the hospital determines whether transfers have occurred between levels in the hierarchy by re-assessing categorisation (based on the lowest level input that is significant to the fair value measurement as a whole) at the end of each reporting period.
The Valuer-General Victoria (VGV) is the hospital's independent valuation agency.
The estimates and underlying assumptions are reviewed on an ongoing basis. Valuation hierarchy
In determining fair values a number of inputs are used. To increase consistency and comparability in the financial statements, these inputs are categorised into three levels, also known as the fair value hierarchy. The levels are as follows:
• Level 1 - quoted (unadjusted) market prices in active markets for identical assets or liabilities;
• Level 2 - valuation techniques for which the lowest level input that is significant to the fair value measurement is directly or indirectly observable; and
• Level 3 - valuation techniques for which the lowest level input that is significant to the fair value measurement is unobservable.
Identifying unobservable inputs (level 3) fair value measurements
Level 3 fair value inputs are unobservable valuation inputs for an asset or liability. These inputs require significant judgement and assumptions in deriving fair value for both financial and non-financial assets.
Unobservable inputs shall be used to measure fair value to the extent that relevant observable inputs are not available, thereby allowing for situations in which there is little, if any, market activity for the asset or liability at the measurement date. However, the fair value measurement objective remains the same, i.e., an exit price at the measurement date from the perspective of a market participant that holds the asset or owes the liability. Therefore, unobservable inputs shall reflect the assumptions that market participants would use when pricing the asset or liability, including assumptions about risk.

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
58 I LATROBE REGIONAL HOSPITAL
Note 4.2: Property, Plant & Equipment (continued) Consideration of highest and best use (HBU) for non-financial physical assets
Judgements about highest and best use must take into account the characteristics of the assets concerned, including restrictions on the use and disposal of assets arising from the asset’s physical nature and any applicable legislative/contractual arrangements.
In accordance with paragraph AASB 13.29, the Hospital has assumed the current use of a non-financial physical asset is its HBU unless market or other factors suggest that a different use by market participants would maximise the value of the asset.
Non-specialised land and non-specialised buildings
Non-specialised land and non-specialised buildings are valued using the market approach. Under this valuation method, the assets are compared to recent comparable sales or sales of comparable assets which are considered to have nominal or no added improvement value.
For non-specialised land and non-specialised buildings, an independent valuation was performed by independent valuers Opteon Victoria Specialised Pty Ltd to determine the fair value using the market approach. Valuation of the assets was determined by analysing comparable sales and allowing for share, size, topography, location and other relevant factors specific to the asset being valued. An appropriate rate per square metre has been applied to the subject asset. The effective date of the valuation is 30 June 2019.
Specialised land and specialised buildings
Specialised land includes Crown Land which is measured at fair value with regard to the property’s highest and best use after due consideration is made for any legal or physical restrictions imposed on the asset, public announcements or commitments made in relation to the intended use of the asset. Theoretical opportunities that may be available in relation to the assets are not taken into account until it is virtually certain that any restrictions will no longer apply. Therefore, unless otherwise disclosed, the current use of these non-financial physical assets will be their highest and best use.
During the reporting period, the Hospital held Crown Land. The nature of this asset means that there are certain limitations and restrictions imposed on its use and/or disposal that may impact their fair value.
The market approach is also used for specialised land and specialised buildings although it is adjusted for the community service obligation (CSO) to reflect the specialised nature of the assets being valued. Specialised assets contain significant, unobservable adjustments; therefore these assets are classified as Level 3 under the market based direct comparison approach.
The CSO adjustment is a reflection of the valuer’s assessment of the impact of restrictions associated with an asset to the extent that is also equally applicable to market participants. This approach is in light of the highest and best use consideration required for fair value measurement, and takes into account the use of the asset that is physically possible, legally permissible and financially feasible. As adjustments of CSO are considered as significant unobservable inputs, specialised land would be classified as Level 3 assets.
For Latrobe Regional Hospital, the depreciated replacement cost method is used for the majority of specialised buildings, adjusting for the associated depreciation. As depreciation adjustments are considered as significant and unobservable inputs in nature, specialised buildings are classified as Level 3 for fair value measurements.
An independent valuation of the Hospital’s specialised land and specialised buildings was performed by the Opteon (Victoria) Specialised on behalf of Valuer-General Victoria. The valuation was performed using the market approach adjusted for CSO. The effective date of the valuation is 30 June 2019.
Vehicles
The hospital acquires new vehicles and at times disposes of them before completion of their economic life. The process of acquisition, use and disposal in the market is managed by the Hospital who set relevant depreciation rates during use to reflect the consumption of the vehicles. As a result, the fair value of vehicles does not differ materially from the carrying value (depreciated cost).
Plant and equipment
Plant and equipment (including medical equipment, computers and communication equipment and furniture and fittings) are held at carrying value (depreciated cost). When plant and equipment is specialised in use, such that it is rarely sold other than as part of a going concern, the depreciated replacement cost is used to estimate the fair value. Unless there is market evidence that current replacement costs are significantly different from the original acquisition cost, it is considered unlikely that depreciated replacement cost will be materially different from the existing carrying value.
There were no changes in valuation techniques throughout the period to 30 June 2019.
For all assets measured at fair value, the current use is considered the highest and best use.

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
ANNUAL REPORT 2019 I 59
TOTAL TOTAL 2019 2018 $'000 $'000
Land
Land at Fair Value 6,838 6,142
Total Land 6,838 6,142
Buildings & Improvements
Buildings & Improvements at Fair Value 240,087 200,047
Less Accumulated Depreciation (324) (27,410)
239,763 172,637
Site Improvements at Fair Value 3,389 4,699
Less Accumulated Depreciation (5) (613)
3,384 4,086
Total Buildings & Improvements 243,147 176,723
Leasehold Improvements
Leasehold Improvements at cost 230 230
Less Accumulated Depreciation (220) (209)
Total Leasehold Improvements 10 21
Plant and Equipment
Non Medical Equipment at Fair Value 5,950 5,842
Less Accumulated Depreciation (3,395) (3,003)
2,555 2,839
Computer Equipment at Fair Value 2,530 2,471
Less Accumulated Depreciation (1,809) (1,510)
721 961
Furniture & Fittings at Fair Value 2,362 2,350
Less Accumulated Depreciation (1,694) (1,576)
668 774
Motor Vehicles at Fair Value 142 328
Less Accumulated Depreciation (141) (313)
1 15
Total Plant & Equipment 3,945 4,589
Medical Equipment at Fair Value 35,287 32,391
Less Accumulated Depreciation (22,923) (21,018)
Medical Equipment 12,364 11,373
Work In Progress
Work In Progress At Cost 4,147 4,006
Total Work In Progress 4,147 4,006
TOTAL PROPERTY, PLANT & EQUIPMENT 270,451 202,854
Note 4.2: Property, Plant & Equipment a) Gross carrying amount and accumulated depreciation

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
60 I LATROBE REGIONAL HOSPITAL
Note 4.2: Property, Plant & Equipment (continued) b) Reconciliations of the carrying amounts of each class of asset
Assets Buildings & Plant & Medical Under Leasehold
Land Improvements Equipment Equipment Construction Improvements Total $'000 $'000 $'000 $'000 $'000 $'000 $'000
Balance at 1 July 2017 6,142 112,386 2,791 6,476 68,915 36 196,746
Additions - 11 372 773 16,081 - 17,237
Transfers from Works In Progress - 72,668 2,289 6,033 (80,990) - -
Depreciation and Amortisation (note 4.3) - (8,342) (863) (1,909) - (15) (11,129)
Balance at 1 July 2018 6,142 176,723 4,589 11,373 4,006 21 202,854
Additions - 983 179 326 3,927 - 5,415
Transfers from Works In Progress - 927 5 2,854 (3,786) - -
Disposals - - - (10) - - (10)
Revaluation increments/(decrements) 696 73,354 - - - - 74,050
Depreciation and Amortisation (note 4.3) - (8,840) (828) (2,179) - (11) (11,858)
Balance at 30 June 2019 6,838 243,147 3,945 12,364 4,147 10 270,451
Land and buildings and leased assets carried at valuation The Valuer-General Victoria undertook to re-value all of the hospital's owned and leased land and buildings to determine their fair value. The valuation, which conforms to Australian Valuation Standards, was determined by reference to the amounts for which assets could be exchanged between knowledgeable willing parties in an arm's length transaction. The valuation was based on independent assessments. The effective date of the valuation is 30 June 2019.

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
ANNUAL REPORT 2019 I 61
Carrying Fair value measurement at end amount as at of reporting period using: 30 June 2019 Level 1 (1) Level 2 (1) Level 3 (1)
$’000 $’000 $’000 $’000Land at fair value
Non-Specialised land 2,726 - 2,726 -
Specialised land 4,112 - - 4,112
Total of land at fair value 6,838 - 2,726 4,112
Buildings at fair value
Specialised buildings 243,147 - - 243,147
Total building at fair value 243,147 - - 243,147
Leasehold improvements 10 10
Plant and equipment at fair value
Plant equipment and vehicles at fair value
- Plant, equipment and vehicles 3,945 - - 3,945
Total of plant, equipment and vehicles at fair value 3,945 - - 3,945
Medical equipment at fair value
- Medical equipment 12,364 - - 12,364
Total medical equipment at fair value 12,364 - - 12,364
Assets under construction
Assets under construction 4,147 4,147 - -
Total assets under construction 4,147 4,147 - -
270,451 4,147 2,726 263,578
Note: (i) Classified in accordance with the fair value hierarchy. There have been no transfers between levels during the period.
Note 4.2: Property, Plant & Equipment (continued) (c) Fair value measurement hierarchy for assets
as at 30 June 2019
Carrying Fair value measurement at end amount as at of reporting period using:
30 June 2018 Level 1 (1) Level 2 (1) Level 3 (1) $’000 $’000 $’000 $’000
Land at fair value
Non-Specialised land 2,704 - 2,704 -
Specialised land 3,438 - - 3,438
Total of land at fair value 6,142 - 2,704 3,438
Buildings at fair value
Specialised buildings 176,723 - - 176,723
Total of building at fair value 176,723 - - 176,723
Leasehold Improvements 21 21
Plant and equipment at fair value
Plant equipment and vehicles at fair value
- Vehicles 15 - - 15
- Plant and equipment 4,574 - - 4,574
Total of plant, equipment and vehicles at fair value 4,589 - - 4,589
Medical equipment at fair value
- Medical equipment 11,373 - - 11,373
Total medical equipment at fair value 11,373 - - 11,373
Assets under construction
Assets under construction 4,006 4,006 - -
Total assets under construction 4,006 4,006 - -
202,854 4,006 2,704 196,144
Note: (i) Classified in accordance with the fair value hierarchy. There have been no transfers between levels during the period.
c) Fair value measurement hierarchy for assets
as at 30 June 2018

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
62 I LATROBE REGIONAL HOSPITAL
Note 4.2: Property, Plant & Equipment (continued) (d) Reconciliation of Level 3 fair value
Plant and Medical Land Buildings equipment equipment $’000 $’000 $’000 $’0002019
Opening Balance 3,438 176,744 4,589 11,373
Additions - 1,909 184 3,180
Disposals - - - (10)
Gains/(losses) recognised in Net Result
- Depreciation - (8,850) (828) (2,179)
Items recognised in Other Comprehensive Income
- Revaluation 674 73,354 - -
Closing Balance 4,112 243,157 3,945 12,364
2018
Opening Balance 3,438 112,422 2,791 6,476
Additions - 72,679 2,661 6,806
Gains/(losses) recognised in Net Result
- Depreciation - (8,357) (863) (1,909)
Closing Balance 3,438 176,744 4,589 11,373
Note (i) Classified in accordance with the fair value hierarchy, see Note 1 There have been no transfers between levels during the period.
(i) CSO adjustments of 20% were applied to reduce the market approach value for the Department’s specialised land.
(e) Description of significant unobservable inputs to Level 3 valuations:
Asset Examples of Likely Valuation Significant Inputs Class Asset Types Approach (Level 3 Only)
Specialised Land Land subject to restriction as to use
and/or sale
Community Service Obligation
(CSO) adjustment
Market approach
Non-specialised Land Land without restriction as to use
and/or sale
n.aMarket approach
Specialised buildings Specialised buildings with limited alternative
uses and/or substantial customisation
Cost per square metre/Useful
life
Depreciated replacement cost
approach
Plant and equipment Specialised items with limited alternative
uses and/or substantial customisation
Cost per square metre/Useful
life
Depreciated replacement cost
approach
Medical equipment Specialised items with limited alternative
uses and/or substantial customisation
Cost per square metre/Useful
life
Depreciated replacement cost
approach

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
ANNUAL REPORT 2019 I 63
TOTAL TOTAL 2019 2018 $'000 $'000
Property, Plant & Equipment Revaluation Surplus
Balance at the beginning of the reporting period 49,377 49,377
Revaluation Increment
- Land 696 -
- Buildings 73,354 -
Balance at the end of the reporting period 123,427 49,377
Represented by:
- Land 2,452 1,756
- Buildings 120,975 47,621
123,427 49,377
Note 4.2: Property, Plant & Equipment (continued) (f) Property, Plant and Equipment Revaluation Surplus

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
64 I LATROBE REGIONAL HOSPITAL
TOTAL TOTAL 2019 2018 $'000 $'000
Depreciation
Buildings 8,556 8,171
Site Improvements 284 171
Plant & Equipment
- Medical Equipment 2,179 1,909
- Non Medical Equipment 391 358
- Computers & Communication 305 368
- Furniture & Fittings 118 121
- Motor Vehicles 14 16
Total depreciation 11,847 11,114
Amortisation
Amortisation of leasehold improvements 11 14
Total Amortisation 11 14
Total Depreciation and Amortisation 11,858 11,128
Note 4.3: Depreciation and Amortisation
Depreciation
All infrastructure assets, buildings, plant and equipment and other non-financial physical assets (excluding items under operating leases, assets held for sale, land and investment properties) that have finite useful lives are depreciated.
Depreciation is generally calculated on a straight line basis, at rates that allocate the asset's value, less any estimated residual value over its estimated useful life.
Amortisation
Amortisation is the systematic allocation of the depreciable amount of an asset over its useful life.
The following table indicates the expected useful lives of non-current assets on which the depreciation and amortisation charges are based.
2019 2018
Buildings
- Structure Shell Building Fabric 40 to 45 years 40 to 45 years
- Site Engineering Services and Central Plant 30 to 40 years 30 to 40 years
Central Plant
- Fit Out 20 to 25 years 20 to 25 years
- Trunk Reticulated Building Systems 20 to 25 years 20 to 25 years
Plant & Equipment 10 years 10 years
Computer Equipment 1-5 years 1-5 years
Furniture and Fittings 10 years 10 years
Motor Vehicles 5 years 5 years
Leasehold Improvements 5 to 40 Years 5 to 40 Years
Site Improvements 40 to 45 Years 40 to 45 Years
As part of the buildings valuation, building values were separated into components and each component assessed for its useful life which is represented above.

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
ANNUAL REPORT 2019 I 65
Note 5: Other Assets and Liabilities This section sets out those assets and liabilities that arose from the hospital’s operations
Structure:
5.1 Receivables
5.2 Payables
5.3 Other Liabilities

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
66 I LATROBE REGIONAL HOSPITAL
TOTAL TOTAL 2019 2018 $'000 $'000
Note 5.1: Receivables
CURRENT
Contractual
Inter hospital debtors 870 1,053
Trade debtors 1,542 508
Patient fees 646 642
Accrued investment income - 27
Sundry Debtors 1,685 1,773
Less allowance for doubtful debts
Trade Debtors (7) (13)
Patient Fees (28) (39)
4,708 3,951
Statutory
GST Receivable 844 955
844 955
TOTAL CURRENT RECEIVABLES 5,552 4,906
NON CURRENT
Statutory
Long Service Leave - Department of Health and Human Services 5,726 4,402
TOTAL NON-CURRENT RECEIVABLES 5,726 4,402
TOTAL RECEIVABLES 11,278 9,308
(a) Movement in the Allowance for doubtful debts
Balance at beginning of year 52 56
Amounts written off during the year 9 2
Decrease in allowance recognised in net result (26) (6)
Balance at end of year 35 52
Receivables recognition Receivables consist of: - contractual receivables, which consists of debtors in relation to goods and services and accrued investment income; and - statutory receivables, which includes predominantly amounts owing from the Victorian Government and Goods and Services Tax (“GST”) input tax credits recoverable. Receivables that are contractual are classified as financial instruments and categorised as loans and receivables. Statutory receivables are recognised and measured similarly to contractual receivables (except for impairment), but are not classified as financial instruments because they do not arise from a contract. Receivables are recognised initially at fair value and subsequently measured at amortised cost less any accumulated impairment. Trade debtors are carried at nominal amounts due and are due for settlement within 30 days from the date of recognition. In assessing impairment of statutory (non-contractual) financial assets, which are not financial instruments, professional judgement is applied in assessing materiality using estimates, averages and other computational methods in accordance with AASB 136 Impairment of Assets. Trade debtors are carried at nominal amounts due and are due for settlement within 30 days from the date of recognition. The hospital is not exposed to any significant credit risk exposure to any single counterparty or any group of counterparties having similar characteristics. Trade receivables consist of a large number of customers in various geographical areas. Based on historical information about customer default rates, management consider the credit quality of trade receivables that are not past due or impaired to be good.
Doubtful debts Collectability of debts is reviewed on an ongoing basis, and debts which are known to be uncollectible are written off. A provision for doubtful debts is recognised when there is objective evidence that the debts may be collected and bad debts are written off when identified. Those bad debts considered as written off by mutual consent are classified as a transaction expense. Bad debts not written off by mutual consent and the allowance for doubtful debts are classified as other economic flows included in net result.
Impairment losses of contractual receivables Refer to Note 7.1c Contractual receivables at amortised costs for the Hospital's contractual impairment losses.
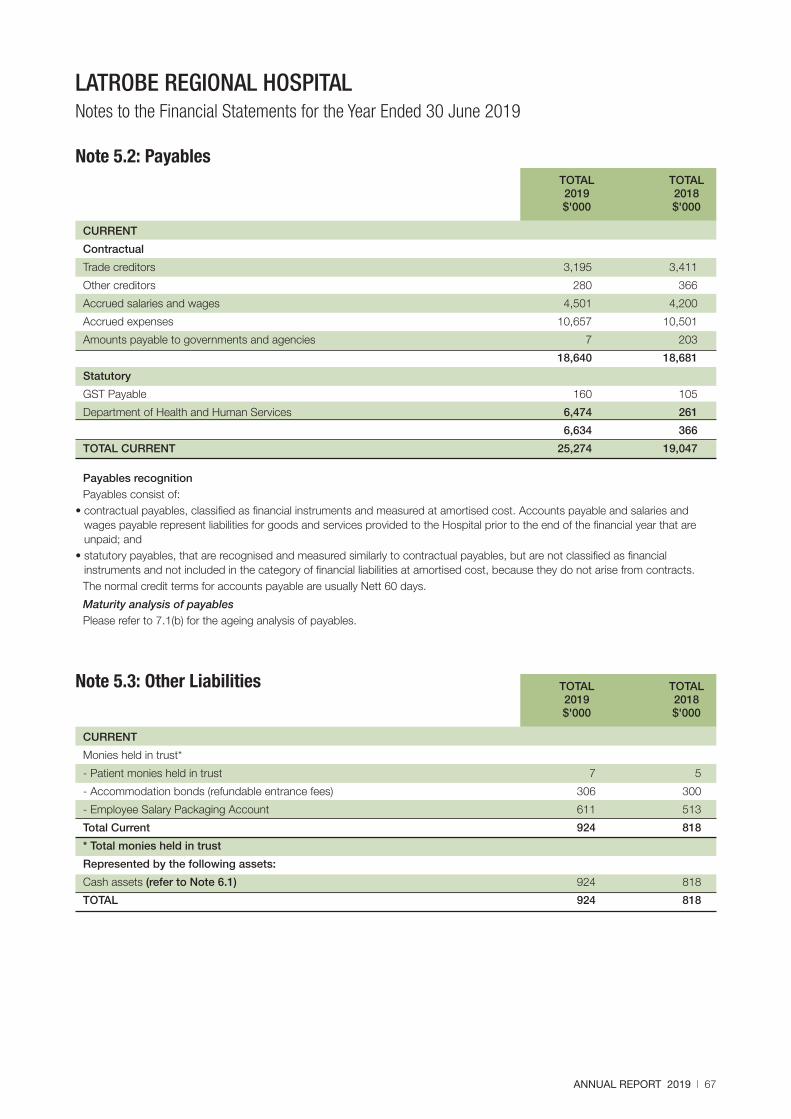
ANNUAL REPORT 2019 I 67
LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
TOTAL TOTAL 2019 2018 $'000 $'000
CURRENT
Contractual
Trade creditors 3,195 3,411
Other creditors 280 366
Accrued salaries and wages 4,501 4,200
Accrued expenses 10,657 10,501
Amounts payable to governments and agencies 7 203
18,640 18,681
Statutory
GST Payable 160 105
Department of Health and Human Services 6,474 261
6,634 366
TOTAL CURRENT 25,274 19,047
Note 5.2: Payables
Payables recognition Payables consist of:
• contractual payables, classified as financial instruments and measured at amortised cost. Accounts payable and salaries and wages payable represent liabilities for goods and services provided to the Hospital prior to the end of the financial year that are unpaid; and
• statutory payables, that are recognised and measured similarly to contractual payables, but are not classified as financial instruments and not included in the category of financial liabilities at amortised cost, because they do not arise from contracts. The normal credit terms for accounts payable are usually Nett 60 days.
Maturity analysis of payables Please refer to 7.1(b) for the ageing analysis of payables.
TOTAL TOTAL 2019 2018 $'000 $'000
CURRENT
Monies held in trust*
- Patient monies held in trust 7 5
- Accommodation bonds (refundable entrance fees) 306 300
- Employee Salary Packaging Account 611 513
Total Current 924 818
* Total monies held in trust
Represented by the following assets:
Cash assets (refer to Note 6.1) 924 818
TOTAL 924 818
Note 5.3: Other Liabilities

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
68 I LATROBE REGIONAL HOSPITAL
Note 6: How we finance our operations This section provides information on the sources of finance utilised by Latrobe Regional Hospital during its operations, along with interest expenses (the cost of borrowings) and other information related to financing activities of the Hospital.
This section includes disclosures of balances that are financial instruments (such as borrowings and cash balances). Note: 7.1 provides additional, specific financial instrument disclosures.
Structure:
6.1 Cash and Cash Equivalents
6.2 Commitments for Expenditure

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
ANNUAL REPORT 2019 I 69
TOTAL TOTAL 2019 2018 $'000 $'000
Cash at Bank 61,625 28,319
Patient Trust Account (refer to Note 5.3) 313 305
Employee Salary Packaging Account (refer to Note 5.3) 611 513
Total Cash and Cash Equivalents 62,549 29,137
Represented by:
Cash as per Cash Flow Statement 62,549 28,832
Cash for Monies Held in Trust
- Cash at Bank - 305
Total Cash and Cash Equivalents 62,549 29,137
Note 6.1: Cash and Cash Equivalents
Cash and cash equivalents recognised on the balance sheet comprise cash on hand and in banks, deposits at call and highly liquid investments (with an original maturity of three months or less), which are held for the purpose of meeting short term cash commitments rather than for investment purposes, which are readily convertible to known amounts of cash and are subject to insignificant risk of changes in value.

70 I LATROBE REGIONAL HOSPITAL
LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
Note 6.2: Commitments Commitments for expenditure
TOTAL TOTAL 2019 2018 $'000 $'000
Capital expenditure commitments
Payable:
Land and Buildings 2,365 261
Plant and Equipment 50 517
Total capital expenditure commitments 2,415 778
Not later than one year 2,415 778
Total 2,415 778
Operating expenditure commitments
Payable:
Maintenance Services Contracts 10,069 2,033
Total operating expenditure commitments 10,069 2,033
Not later than one year 2,896 1,441
Later than 1 year and not later than 5 years 7,173 592
TOTAL 10,069 2,033
Cancellable Operating Lease Commitments
Commitments in relation to leases contracted for at the reporting date:
Operating leases 2,233 330
Total Cancellable Operating Lease Commitments 2,233 330
Operating Leases
Operating Leases- Motor Vehicles
Cancellable
Not later than one year 638 330
Later than 1 year and not later than 5 years 1,595 -
Sub Total 2,233 330
Operating Leases- Other
Cancellable
Not later than one year 171 103
Later than 1 year and not later than 5 years 165 164
Sub Total 336 267
Total Operating Lease Commitments 2,569 597
Total Lease Commitments 2,569 597
Total Commitments (inclusive of GST) other than public private partnerships 15,053 3,408
less GST recoverable from the Australian Tax Office (1,368) (310)
Total Commitments (exclusive of GST) other than public private partnerships 13,685 3,098
Commitments
Commitments for future expenditure include operating and capital commitments arising from contracts. These commitments are disclosed at their nominal value and are inclusive of the GST payable. In addition, where it is considered appropriate and provides additional relevant information to users, the net present values of significant individual projects are stated. These future expenditures cease to be disclosed as commitments once the related liabilities are recognised on the balance sheet.

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
ANNUAL REPORT 2019 I 71
Note 7: Risks, Contingencies and Valuation Uncertainties The hospital is exposed to risk from its activities and outside factors. In addition, it is often necessary to make judgements and estimates associated with recognition and measurement of items in the financial statements. This section sets out financial instrument specific information, (including exposures to financial risks) as well as those items that are contingent in nature or require a higher level of judgement to be applied, which for the health service is related mainly to fair value determination.
Structure:
7.1 Financial Instruments
7.2 Contingent Assets and Contingent Liabilities

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
72 I LATROBE REGIONAL HOSPITAL
Financial instruments arise out of contractual agreements that give rise to a financial asset of one entity and a financial liability or equity instrument of another entity. Due to the nature of the Hospital's activities, certain financial assets and financial liabilities arise under statute rather than a contract. Such financial assets and financial liabilities do not meet the definition of financial instruments in AASB 132 Financial Instruments: Presentation.
Note 7.1: Financial Instruments
(a) Financial instruments: categorisation Financial Financial Assets at Liabilities at
Amortised Cost Amortised Cost Total $’000 $’000 $’000
Contractual Contractual Financial Financial
Assets - Loans Liabilities at & Receivables Amortised Cost Total
$’000 $’000 $’000
2019
Contractual Financial Assets
Cash and Cash Equivalents 62,549 - 62,549
Trade Debtors & Other Receivables 4,708 - 4,708
Other Financial Assets- Managed Investment 20,695 - 20,695
Total Financial Assets 87,952 - 87,952
Financial Liabilities
Payables & Borrowings - 19,854 19,854
Total Financial Liabilities - 19,854 19,854
2018
Contractual Financial Assets
Cash and Cash Equivalents 29,137 - 29,137
Trade Debtors & Other Receivables 3,951 - 3,951
Other Financial Assets- Term Deposit 28,737 - 28,737
Other Financial Assets- Managed Investment 19,984 - 19,984
Other Financial Assets- Shares In Listed Companies 395 - 395
Total Financial Assets 82,204 - 82,204
Financial Liabilities
Payables & Borrowings - 15,621 15,621
Total Financial Liabilities - 15,621 15,621
The carrying amount excludes statutory receivables (i.e. GST receivable and DHHS receivable) and statutory payables (i.e. revenue in advance and DHHS payable)
From 1 July 2018, Latrobe Regional Hospital applies AASB 9 and classifies all of its financial assets based on the business model for managing the asset's contractual terms. Categories of financial assets under AASB 9:-
Financial assets at amortised cost Financial assets are measured at amortised costs if both of the following criteria are met and the assets are not designated as fair value through net result: • the assets are held by the hospital to collect the contractual cash flows, and • the assets’ contractual terms give rise to cash flows that are solely payments of principal and interests. These assets are initially recognised at fair value plus any directly attributable transaction costs and subsequently measured at amortised cost using the effective interest method less any impairment. The Department recognises the following assets in this category: • cash and deposits; • receivables (excluding statutory receivables); • term deposits; and • certain debt securities.

ANNUAL REPORT 2019 I 73
LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
Note 7.1: Financial Instruments (continued)
Categories of financial assets previously under AASB 139
Loans and receivables and cash are financial instrument assets with fixed and determinable payments that are not quoted on an active market. These assets and liabilities are initially recognised at fair value plus any directly attributable transaction costs. Subsequent to initial measurement, loans and receivables are measured at amortised cost using the effective interest method, less any impairment.
Latrobe Regional Hospital recognises the following assets in this category: - cash and deposits - term deposits - investment in managed investment schemes - receivables (excluding statutory receivables)
Financial liabilities at amortised cost are initially recognised on the date they are originated. They are initially measured at fair value plus any directly attributable transaction costs. Subsequent to initial recognition, these financial instruments are measured at amortised cost with any difference between the initial recognised amount and the redemption value being recognised in profit and loss over the period of the interest-bearing liability, using the effective interest rate method.
Latrobe Regional Hospital recognises the following assets in this category: - payables (excluding statutory payables) - borrowings
Derecognition of financial assets: A financial asset (or, where applicable, a part of a financial asset or part of a group of similar financial assets) is derecognised when the rights to receive cash flows from the asset have expired.
Derecognition of financial liabilities: A financial liability is derecognised when the obligation under the liability is discharged, cancelled or expires.
Impairment of financial assets: At the end of each reporting period, the Hospital assesses whether there is objective evidence that a financial asset or group of financial assets is impaired. All financial instrument assets, except those measured at fair value through profit or loss, are subject to annual review for impairment.
The allowance is the difference between the financial asset's carrying amount and the present value of estimated future cash flows, discounted at the effective interest rate. In assessing impairment of statutory (non-contractual) financial assets, which are not financial instruments, professional judgement is applied in assessing materiality using estimates, averages and other computational methods in accordance with AASB 136 Impairment of Assets.

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
74 I LATROBE REGIONAL HOSPITAL
Carrying Nominal Less than 3 Months 1-5 Amount Amount 1 Month - 1 Year Years
Note $’000 $’000 $’000 $’000 $’000
2019
Financial Liabilities
At amortised cost
Payables 5.2 18,640 18,640 18,640 - -
Other Financial Liabilities
- Accomodation Deposits 5.3 306 306 306 - -
- Other 908 908 611 57 240
Total Financial Liabilities 19,854 19,854 19,557 57 240
2018
Financial Liabilities
At amortised cost
Payables 5.2 18,681 18,681 18,681 - -
Other Financial Liabilities
- Accommodation Deposits 5.3 300 300 300 - -
- Other 840 840 513 55 272
Total Financial Liabilities 19,821 19,821 19,494 55 272
Maturity Dates
Ageing analysis of financial liabilities excludes the types of statutory financial liabilities (i.e. GST Payable)
Note 7.1: Financial Instruments (continued) (b) Maturity analysis of Financial Liabilities as at 30 June
The following table discloses the contractual maturity analysis for the Hospital's financial liabilities. For interest rates applicable to each class of liability refer to individual notes to the financial statements.
(c) Contractual receivables at amortised costs
Less than 1-3 3 Months 1-5 Current 1 Month Months - 1 Year Years Total $’000 $’000 $’000 $’000 $’000 $’000
1 July 2018
Expected loss rate 0% 0% 0% 72% 28% 100%
Gross carrying amount of contractual receivables 3,343 115 469 61 15 4,003
Loss allowance - - - (37) (15) (52)
30 June 2019
Expected loss rate 0% 0% 0% 0% 100% 100%
Gross carrying amount of contractual receivables 3,706 701 67 149 120 4,743
Loss allowance - - - - (35) (35)
Impairment of financial assets under AASB 9 - applicable from 1 July 2018
From 1 July 2018, the Hospital has been recording the allowance for expected credit loss for the relevant financial instruments, replacing AASB 139’s incurred loss approach with AASB 9’s Expected Credit Loss approach. Subject to AASB 9 impairment assessment include the Hospital's contractual receivables, statutory receivables and its investment in debt instruments.
Equity instruments are not subject to impairment under AASB 9. Other financial assets mandatorily measured or designated at fair value through net result are not subject to impairment assessment under AASB 9. While cash and cash equivalents are also subject to the impairment requirements of AASB 9, the identified impairment loss was immaterial.

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
ANNUAL REPORT 2019 I 75
Note 7.1: Financial Instruments (continued) (c) Contractual receivables at amortised costs (continued)
2018 2017 $'000 $'000
Balance at beginning of the year 56 89
Opening retained earnings adjustment on adoption of AASB 9 - -
Opening loss allowance 56 89
Modification of contractual cash flows on financial assets - -
Decrease in provision recognised in the net result -6 -33
Reversal of provision of receivables written off during the year as uncollectible 2 -
Reversal of unused provision recognised in the net result - -
Balance at end of the year 52 56
Contractual receivables at amortised cost
The Hospital applies AASB 9 simplified approach for all contractual receivables to measure expected credit losses using a lifetime expected loss allowance based on the assumptions about risk of default and expected loss rates. The Hospital has grouped contractual receivables on shared credit risk characteristics and days past due and select the expected credit loss rate based on the Department’s past history, existing market conditions, as well as forward‑looking estimates at the end of the financial year.
On this basis, the Hospital determines the opening loss allowance on initial application date of AASB 9 and the closing loss allowance at end of the financial year as disclosed above.
Reconciliation of the movement in the loss allowance for contractual receivables
Credit loss allowance is classified as other economic flows in the net result. Contractual receivables are written off when there is no reasonable expectationof recovery and impairment losses are classified as a transaction expense. Subsequent recoveries of amounts previously written off are credited against the same line item. In prior years, a provision for doubtful debts is recognised when there is objective evidence that the debts may not be collected and bad debts are written off when identified. A provision is made for estimated irrecoverable amounts from the sale of goods when there is objective evidence that an individual receivable is impaired. Bad debts considered as written off by mutual consent.
Statutory receivables and debt investments at amortised cost (AASB 2016-8.4)
The Hospital's non-contractual receivables arising from statutory requirements are not financial instruments. However, they are nevertheless recognised and measured in accordance with AASB 9 requirements as if those receivables are financial instruments.
The Hospital also has investments in: VFMC.
Both the statutory receivables and investments in debt instruments are considered to have low credit risk, taking into account the counterparty’s credit rating, risk of default and capacity to meet contractual cash flow obligations in the near term. As the result, the loss allowance recognised for these financial assets during the period was limited to 12 months expected losses. No loss allowance recognised at 30 June 2018 under AASB 139. No additional loss allowance required upon transition into AASB 9 on 1 July 2018.
Note 7.2: Contingent Assets and Contingent Liabilities
There are no known Contingent Assets or Contingent Liabilities held by the hospital at balance date.

76 I LATROBE REGIONAL HOSPITAL
LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
Note 8: Other Disclosures This section includes additional material disclosures required by accounting standards or otherwise, for the understanding of this financial report.
Structure:
8.1 Reconciliation of Net Result for the Year to Net Cash Flow from Operating Activities
8.2 Responsible Persons
8.3 Remuneration of Executives
8.4 Related Parties
8.5 Remuneration of Auditors
8.6 Events occurring after the Balance Sheet date
8.7 Jointly Controlled Operations
8.8 Economic Dependency
8.9 AASBs Issued that are not yet Effective
8.10 Glossary

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
ANNUAL REPORT 2019 I 77
TOTAL TOTAL 2019 2018 $'000 $'000
Net Result For The Year (9,006) 14,724
Non-Cash Movements:
Depreciation and Amortisation 11,858 11,128
Non Cash Grants (15) (294)
Write Down of Inventories 91 (59)
Gain on Disposal of Assets (20) -
Assets Received Free of Charge (13) -
Net Gain/(Loss) on Disposal of Financial Instruments 396 -
Net Gain/(Loss) Arising from Revaluation of Long Service Liability 443 -
Provision for Doubtful Debts (9) (4)
Movements Included in Investing & Financing Activities:
Movement in Capital Payables (8) 1,060
Interest & Distributions Received on Long Term Investments (1,235) (1,446)
Reclassification of Investment Revenue - (559)
Reversal of Impaired Investment - (32)
Movements in Assets and Liabilities:
Change in Operating Assets and Liabilities
Increase in Receivables (1,970) (695)
(Increase)/Decrease in Prepayments (364) 164
Increase in Payables 6,227 3,109
Increase in Provisions 3,508 4,096
Decrease in Other Liabilities 74 538
Decrease/(Increase) in Inventories 67 (102)
NET CASH INFLOW/(OUTFLOW) FROM OPERATING ACTIVITIES 10,024 31,628
Note 8.1: Reconciliation of Net Result for the Year to Net Cash Inflow/(Outflow) from Operating Activities

78 I LATROBE REGIONAL HOSPITAL
LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
Note 8.2: Responsible Persons Disclosures
In accordance with the Ministerial Directions issued by the Assistant Treasurer under the Financial Management Act 1994, the following disclosures are made regarding responsible persons for the reporting period.
Period
Responsible Ministers:
The Honourable Jill Hennessy, Minister for Health, Minister for Ambulance Services 1/7/2018 - 29/11/2018
The Honourable Jenny Mikakos, Minister for Health, Minister for Ambulance Services 29/11/2018 - 30/6/2019
The Honourable Martin Foley, Minister for Mental Health 1/7/2018 - 30/6/2019
The Honourable Martin Foley, Minister for Housing, Disability and Ageing 1/7/2018 - 29/11/2018
The Honourable Luke Donnellan, Minister for Child Protection, Minister for Disability, Ageing and Carers 29/11/2018 - 30/6/2019
Governing Boards
Linda McCoy (Chair) 1/7/2018 - 30/6/2019
Ian Gibson (Deputy Chair) 1/7/2018 - 30/6/2019
John Rasa 1/7/2018 - 30/6/2019
John Donovan 1/7/2018 - 30/6/2019
Leah Young 1/7/2018 - 30/6/2019
Chelsea Caple 1/7/2018 - 30/6/2019
John Arranga 1/7/2018 - 30/6/2019
Liesl McKay 1/7/2018 - 30/6/2019
Bernadette Hickey 1/7/2018 - 30/6/2019
Accountable Officers
Peter Craighead 1/7/2018 - 30/6/2019
Income Band
$20,000 - $29,999 8 6
$50,000 - $59,999 1 1
$400,000 - $409,999 0 1
$430,000 - $439,999 1 0
Total Numbers 10 8
2019 2018
$’000 $’000
Total remuneration received or due and receivable by Responsible Persons from the reporting entity amounted to: $685 $615
Remuneration of Responsible Persons
The number of Responsible Persons are shown in their relevant income bands:
Consolidated
2019 2018
No. No.
Amounts relating to the Governing Board Members and Accountable Officer are disclosed in the Hospital's financial statements.
Amounts relating to the Responsible Ministers are reported within the Department of Parliamentary Service's Financial Report.

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
ANNUAL REPORT 2019 I 79
Total Remuneration 2019 2018 $'000 $'000
Short-term Benefits 1,073 850
Post-employment Benefits 103 81
Other Long-term Benefits 9 92
Termination Benefits 48 -
Total Remuneration i 1,233 1,023
Total Number of Executives 6 5
Total Annualised Employee Equivalent ii 4.7 4.3
The number of executive officers, other than Ministers and Accountable Officers, and their total remuneration during the reporting period are shown in the table below. Total annualised employee equivalent provides a measure of full time equivalent executive officers over the reporting period.
Remuneration of Executive Officers (including Key Management Personnel Disclosed in Note 8.4)
i The total number of executive officers includes persons who meet the definition of Key Management Personnel (KMP) of Latrobe Regional Hospital under AASB 124 Related Party Disclosures and are also reported within Note 8.4 Relates Parties.
ii Annualised employee equivalent is based on working 38 ordinary hours per week over the reporting period.
Short-term Employee Benefits
Salaries and wages, annual leave or sick leave that are usually paid or payable on a regular basis, as well as non-monetary benefits such as allowances and free or subsidised goods or services.
Post-employment Benefits
Pensions and other retirement benefits paid or payable on a discrete basis when employment has ceased.
Other Long-term Benefits
Long service leave, other long-service benefit or deferred compensation.
Termination Benefits
Termination of employment payments, such as severance packages.
Other factors
Several factors affected total remuneration payable to executives over the year. A number of employment contracts were completed and renegotiated and an executive officer resigned in the past year. This has had an impact on remuneration figures for the termination benefits category.
Note 8.3: Remuneration of Executives

80 I LATROBE REGIONAL HOSPITAL
LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
Note 8.4: Related Parties The hospital is a wholly owned and controlled entity of the State of Victoria. Related parties of the hospital include: • All key management personnel (KMP) and their close family members; • Cabinet ministers (where applicable) and their close family members; • Jointly controlled operation- A member of the Gippsland Health Alliance; • All hospitals and public sector entities that are controlled and consolidated into the State of Victoria financial statements. KMPs are those people with the authority and responsibility for planning, directing and controlling the activities of Latrobe Regional Hospital, directly or indirectly. The Board of Directors and the Executive Directors of Latrobe Regional Hospital are deemed to be KMPs.
Entity Key Management Personnel Position Title
Latrobe Regional Hospital Peter Craighead Chief Executive Officer
Latrobe Regional Hospital Don McRae Chief Operating Officer/Chief Nurse
Latrobe Regional Hospital Philippa Hawkings Chief Medical Officer
Latrobe Regional Hospital Jon Millar Executive Director of Information and Regional Services
Latrobe Regional Hospital Cayte Hoppner Executive Director of Mental Health/ Chief Mental Health Nurse
Latrobe Regional Hospital Mark Wilkins Executive Director People and Culture
Latrobe Regional Hospital Linda McCoy Board Chair
Latrobe Regional Hospital Ian Gibson Board Member
Latrobe Regional Hospital John Rasa Board Member
Latrobe Regional Hospital John Donovan Board Member
Latrobe Regional Hospital Leah Young Board Member
Latrobe Regional Hospital Chelsea Caple Board Member
Latrobe Regional Hospital John Arranga Board Member
Latrobe Regional Hospital Liesl McKay Board Member
Latrobe Regional Hospital Bernadette Hickey Board Member
The compensation detailed below is reported in $'000 and excludes the salaries and benefits the Portfolio Ministers receive. The Minister’s remuneration and allowances is set by the Parliamentary Salaries and Superannuation Act 1968, and is reported within the Department of Parliamentary Services’ Financial Report.
2019 2018 Compensation ($’000) ($’000)
Short term employee benefits 1,730 1,430
Post-employment benefits 131 16
Other long-term benefits 9 92
Other long-term benefits 48 -
Total 1,918 1,638
Significant transactions with government-related entities
Latrobe Regional Hospital received funding from the Department of Health and Human Services of $225 million (2018: $233 million).
Expenses incurred by the Hospital in delivering services and outputs are in accordance with Health Purchasing Victoria requirements. Goods and services including procurement, diagnostics, patient meals and multi-site operational support are provided by other Victorian Health Service Providers on commercial terms.
Professional medical indemnity insurance and other insurance products are obtained from a Victorian Public Financial Corporation.
The Standing Directions of the Minister for Finance require the Hospital to hold cash (in excess of working capital) in accordance with the State's centralised banking arrangements. All borrowings are required to be sourced from Treasury Corporation Victoria unless an exemption has been approved by the Minister for Health and Human Services and the Treasurer.

LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
ANNUAL REPORT 2019 I 81
Note 8.4: Related Parties (continued) Transactions with key management personnel and other related parties
Given the breadth and depth of State government activities, related parties transact with the Victorian public sector in a manner consistent with other members of the public e.g. stamp duty and other government fees and charges. Further employment of processes within the Victorian public sector occur on terms and conditions consistent with the Public Administration Act 2004 and Codes of Conduct and Standards issued by the Victorian Public Sector Commission. Procurement processes occur on terms and conditions consistent with the Victorian Government Procurement Board requirements.
Outside of normal citizen type transactions with the Hospital, there were no related party transactions that involved KMPs, their close family members and their personal business interests. No provision has been required, nor any expense recognised, for impairment of receivables from related parties. There were no related party transactions with Cabinet Ministers required to be disclosed in 2019.
There were no related party transactions required to be disclosed for the Latrobe Regional Hospital Board of Directors and Executive Directors in 2019.
2019 2018 Entity ($’000) ($’000) Treasury Corporation Victoria 280 542 Department of Treasury and Finance 198 - Alfred Health 2,461 2,472 Bairnsdale Regional Health Service 128 - Gippsland Southern Health Service 260 263 Central Gippsland Health Service 762 485 Department of Health and Human Services (not grant related) - 41 Department of Health and Human Services (grants) 224,982 233,000 Monash Health 218 196 West Gippsland Healthcare Group 573 483 Transport Accident Commission 324 122 Victorian Managed Insurance Authority 334 - Gippsland Health Alliance 3,096 3,075
2019 2018 Entity ($’000) ($’000) Monash Health 1,468 1,495 Alfred Health 315 - Ambulance Victoria 1,610 605 Bairnsdale Regional Health Service 280 284 Bass Coast Regional Health Service 364 343 Central Gippsland Health Service 1,873 1,875 Department of Health and Human Services - 2 Koo Wee Rup Regional Health Services 340 334 Omeo District Health 136 126 Orbost Regional Health 170 167 South Gippsland Hospital 448 418 West Gippsland Healthcare Group 790 793 Yarram and District Health Service 305 309 Victorian Managed Insurance Authority 3,950 3,819 Gippsland Health Alliance 3,831 8,413
Payments made to the following for 2019 ($'000)
During the year, the hospital had the following government-related entity transactions:
Revenue received from the following for 2019 ($'000)

82 I LATROBE REGIONAL HOSPITAL
LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
Note 8.4: Related Parties (continued)
2019 2018 Entity ($’000) ($’000) Alfred Health 518 195 Bairnsdale Regional Health Service 14 1 Gippsland Southern Health Service 39 56 Central Gippsland Health Service 403 156 Department of Health and Human Services (grants) 5,738 4,931 Monash Health 33 35 West Gippsland Healthcare Group 201 178 Transport Accident Commission 183 32 Gippsland Health Alliance 347 199
2019 2018 Entity ($’000) ($’000) Monash Health 236 329 Alfred Health 146 - Ambulance Victoria 291 151 Bairnsdale Regional Health Service 38 29 Bass Coast Regional Health Service 80 55 Central Gippsland Health Service 167 334 Department of Health and Human Services 6,670 - Koo Wee Rup Regional Health Services 55 59 Omeo District Health 17 16 Orbost Regional Health 42 15 South Gippsland Hospital 89 58 West Gippsland Healthcare Group 141 210 Yarram and District Health Service 46 55 Gippsland Health Alliance 335 294
Payments made to the following for 2019 ($'000)
Outstanding Revenue at year end from the following:
Note 8.5: Remuneration of Auditors TOTAL TOTAL 2019 2018 $'000 $'000
Victorian Auditor-General’s Office
Audit and review of financial statements 55 55
Note 8.6: Events occurring after the Balance Sheet date There are no events occurring after the Balance Sheet Date.

ANNUAL REPORT 2019 I 83
LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
Note 8.7: Jointly Controlled Operations and Assets
Ownership Interest Name of Entity 2019 2018
% %
Gippsland Health Alliance 21.36% 21.60%
Interest in IT Alliance
Summarised Financial information of Jointly Controlled Assets & Liabilities
During 2009/10, the Alliance members signed a new agreement, which was effective 1 July 2009, which determines the interest in the Gippsland Health Alliance as a ‘jointly controlled asset’. Accounting for a ‘jointly controlled asset’ requires the member hospital's to now recognise its share of the Alliance’s assets and liabilities, together with any income and expenditure arising, under the respective line item in the member Hospital’s financial statements from the year ending 30 June 2010 onwards. This arrangement is now known as a Joint Operation.
The Hospital's interest in assets employed in the above jointly controlled operations and assets is detailed below. The amounts are included in the financial statements and consolidated financial statements under their respective asset and liability categories:
TOTAL TOTAL 2019 2018 $'000 $'000
Current Assets
Cash and Cash Equivalents 1,680 1,968
Receivables 292 233
Other Current Assets 556 558
Total Current Assets 2,528 2,759
Non Current Assets
Property, Plant and Equipment 24 31
Total Non Current Assets 24 18
Share of Total Assets 2,552 2,790
Current Liabilities
Payables 225 150
Other Current Liabilities 1,261 1,658
Total Current Liabilities 1,486 1,808
Share of Total Liabilities 1,486 1,808
Net Assets 1,066 982
Reconciliation of jointly controlled assets:
Share of funds at beginning of the reporting period 982 936
Contributions made in current reporting period - -
Share of current year Surplus/(Deficit) 84 46
Share of funds at end of reporting period 1,066 982
The Latrobe Regional Hospital's interest in revenues and expenses resulting from jointly controlled operations are detailed below:
Revenues
GHA revenue 2,934 2,816
Total Revenue 2,934 2,816
Expenses
Information Technology and Administrative Expenses 2,843 2,766
Depreciation 7 4
Total Expenses 2,850 2,770
Net result 84 46
Contingent Liabilities and Capital Commitments
There are no known contingent liabilities or capital commitments held by the jointly controlled operations at balance date.

84 I LATROBE REGIONAL HOSPITAL
LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
Note 8.8: Economic Dependency Latrobe Regional Hospital is dependent on the Department of Health and Human Services for the majority of its revenue used to operate the entity. At the date of this report, the Board of Directors has no reason to believe the Department of Health and Human Services will not continue to support the Hospital.
Applicable for annual Impact on public reporting period sector entity
Standard/ Interpretation Summary beginning on financial statements
AASB 15 Revenue from Contracts with Customers
The changes in revenue recognition requirements in AASB 15 may result in changes to the timing and amount of revenue recorded in the financial statements. Revenue from grants that are provided under an enforceable agreement that have sufficiently specific obligations, will now be deferred and recognised as the performance obligations attached to the grant are satisfied.
There’s most likely no material effect to the hospital.
The core principle of AASB 15 requires an entity to recognise revenue when the entity satisfies a performance obligation by transferring a promised good or service to a customer. Note that amending standard AASB 2015 8 Amendments to Australian Accounting Standards - Effective Date of AASB 15 has deferred the effective date of AASB 15 to annual reporting periods beginning on or after 1 January 2018, instead of 1 January 2017 for Not-for-Profit entities.
1 Jan 2019
AASB 2018-4 Amendments to Australian Accounting Standards - Australian Implementation Guidance for Not-for-Profit Public-Sector Licensors
AASB 2018-4 provides additional guidance for not-for-profit public sector licenses, which include:
• Matters to consider in distinguishing between a tax and a license, with all taxes being accounted for under AASB 1058;
• IP licenses to be accounted for under AASB 15; and
• Non-IP, such as casino licenses, are to be accounted for in accordance with the principles of AASB 15 after first having determined whether any part of the arrangement should be accounted for as a lease under AASB 16.
AASB 2018-4 amends AASB 15 and AASB 16 to provide guidance for revenue recognition in connection with taxes and Non-IP licences for Not-for-Profit entities.
1 Jan 2019
Note 8.9: AASBs issued that are not yet effective Certain new Australian Accounting Standards have been published that are not mandatory for the 30 June 2019 reporting period. Department of Treasury and Finance assesses the impact of all these new standards and advises the Hospital of their applicability and early adoption where applicable.
As at 30 June 2019, the following standards and interpretations had been issued by the AASB but were not yet effective. They become effective for the first financial statements for reporting periods commencing after the stated operative dates as detailed in the table below. The Hospital has not and does not intend to adopt these standards early.

ANNUAL REPORT 2019 I 85
LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
Applicable for annual Impact on public reporting period sector entity
Standard/ Interpretation Summary beginning on financial statements
AASB 2016-8 Amendments to Australian Accounting Standards - Australian Implementation Guidance for Not-for-Profit Entities
This standard clarifies the application of AASB 15 and AASB 9 in a not-for-profit context. The areas within these standards that are amended for not-for-profit application include:
AASB 9
• Statutory receivables are recognised and measured similarly to financial assets.
AASB 15
• The ‘customer’ does not need to be the recipient of goods and/or services;
• The “contract” could include an arrangement entered into under the direction of another party;
• Contracts are enforceable if they are enforceable by legal or ‘equivalent means’;
• Contracts do not have to have commercial substance, only economic substance; and
• Performance obligations need to be ‘sufficiently specific’ to be able to apply AASB 15 to these transactions.
AASB 2016-8 inserts Australian requirements and authoritative implementation guidance for not-for-profit-entities into AASB 9 and AASB 15.
This Standard amends AASB 9 and AASB 15 to include requirements to assist not-for-profit entities in applying the respective standards to particular transactions and events.
1 Jan 2019
AASB 16 Leases The assessment has indicated that most operating leases, with the exception of short term and low value leases will come on to the balance sheet and will be recognised as right of use assets with a corresponding lease liability.
In the operating statement, the operating lease expense will be replaced by depreciation expense of the asset and an interest charge.
The Hospital has identified 3-4 leases which will be reclassified from operating leases to finance leases.
The key changes introduced by AASB 16 include the recognition of most operating leases (which are currently not recognised) on balance sheet.
1 Jan 2019
Note 8.9: AASBs issued that are not yet effective (continued)

86 I LATROBE REGIONAL HOSPITAL
LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
Applicable for annual Impact on public reporting period sector entity
Standard/ Interpretation Summary beginning on financial statements
AASB 2018-8 Amendments to Australian Accounting Standards - Right of Use Assets of Not-for-Profit entities
Under AASB 1058, not-for-profit entities are required to measure right-of-use assets at fair value at initial recognition for leases that have significantly below-market terms and conditions.
For right-of-use assets arising under leases with significantly below market terms and conditions principally to enable the entity to further its objectives (peppercorn leases), AASB 2018-8 provides a temporary option for Not-for-Profit entities to measure at initial recognition, a class or classes of right-of-use assets at cost rather than at fair value and requires disclosure of the adoption.
The State has elected to apply the temporary option in AASB 2018-8 for not-for-profit entities to not apply the fair value provisions under AASB 1058 for these right-of-use assets.
In making this election, the State considered that the methodology of valuing peppercorn leases was still being developed.
This is unlikely to effect the hospital.
This standard amends various other accounting standards to provide an option for not-for-profit entities to not apply the fair value initial measurement requirements to a class or classes of right of use assets arising under leases with significantly below-market terms and conditions principally to enable the entity to further its objectives. This Standard also adds additional disclosure requirements to AASB 16 for not-for-profit entities that elect to apply this option.
1 Jan 2019
AASB 1058 Income of Not-for-Profit Entities
Grant revenue is currently recognised up front upon receipt of the funds under AASB 1004 Contributions.
The timing of revenue recognition for grant agreements that fall under the scope of AASB 1058 may be deferred. For example, revenue from capital grants for the construction of assets will need to be deferred and recognised progressively as the asset is being constructed.
The impact on current revenue recognition of the changes is the potential phasing and deferral of revenue recorded in the operating statement.
There’s unlikely to be a material effect to the Hospital’s grants and revenue figures.
AASB 1058 will replace the majority of income recognition in relation to government grants and other types of contributions requirements relating to public sector not-for-profit entities, previously in AASB 1004 Contributions.
The restructure of administrative arrangement will remain under AASB 1004 and will be restricted to government entities and contributions by owners in a public sector context,
AASB 1058 establishes principles for transactions that are not within the scope of AASB 15, where the consideration to acquire an asset is significantly less than fair value to enable not-for-profit entities to further their objective.
1 Jan 2019
Note 8.9: AASBs issued that are not yet effective (continued)

ANNUAL REPORT 2019 I 87
LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
Note 8.10: Glossary of terms and style conventions Amortisation Amortisation is the expense which results from the consumption, extraction or use over time of a non-produced physical or intangible asset.
Comprehensive result The net result of all items of income and expense recognised for the period. It is the aggregate of operating result and other comprehensive income.
Commitments Commitments include those operating, capital and other outsourcing commitments arising from non-cancellable contractual or statutory sources.
Current grants Amounts payable or receivable for current purposes for which no economic benefits of equal value are receivable or payable in return.
Depreciation Depreciation is an expense that arises from the consumption through wear or time of a produced physical or intangible asset. This expense reduces the ‘net result for the year’. Employee benefits expenses Employee benefits expenses include all costs related to employment including wages and salaries, fringe benefits tax, leave entitlements, redundancy payments, defined benefits superannuation plans, and defined contribution superannuation plans.
Financial asset A financial asset is any asset that is:
• cash; • an equity instrument of another entity; • a contractual or statutory right: – to receive cash or another financial asset from another entity; or – to exchange financial assets or financial liabilities with another entity under conditions that are potentially favorable to the entity;
or • a contract that will or may be settled in the entity’s own equity instruments and is: – a non-derivative for which the entity is or may be obliged to receive a variable number of the entity’s own equity instruments; or – a derivative that will or may be settled other than by the exchange of a fixed amount of cash or another financial asset for a fixed
number of the entity’s own equity instruments.
Financial instrument A financial instrument is any contract that gives rise to a financial asset of one entity and a financial liability or equity instrument of another entity. Financial assets or liabilities that are not contractual (such as statutory receivables or payables that arise as a result of statutory requirements imposed by governments) are not financial instruments.
Financial liability A financial liability is any liability that is:
• A contractual obligation: – to deliver cash or another financial asset to another entity; or – to exchange financial assets or financial liabilities with another entity under conditions that are potentially unfavorable to the
entity; or • A contract that will or may be settled in the entity’s own equity instruments and is: – a non-derivative for which the entity is or may be obliged to deliver a variable number of the entity’s own equity instruments; or – a derivative that will or may be settled other than by the exchange of a fixed amount of cash or another financial asset for a fixed
number of the entity’s own equity instruments. For this purpose the entity’s own equity instruments do not include instruments that are themselves contracts for the future receipt or delivery of the entity’s own equity instruments.
Financial statements A complete set of financial statements comprises:
• Balance sheet as at the end of the period; • Comprehensive operating statement for the period; • A statement of changes in equity for the period; • Cash flow statement for the period; • Notes, comprising a summary of significant accounting policies and other explanatory information; • Comparative information in respect of the preceding period as specified in paragraph 38 of AASB 101 Presentation of Financial
Statements; and • A statement of financial position at the beginning of the preceding period when an entity applies an accounting policy
retrospectively or makes a retrospective restatement of items in its financial statements, or when it reclassifies items in its financial statements in accordance with paragraphs 41 of AASB 101.

88 I LATROBE REGIONAL HOSPITAL
LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
Note 8.10: Glossary of terms and style conventions (continued) Grants and other transfers Transactions in which one unit provides goods, services, assets (or extinguishes a liability) or labour to another unit without receiving approximately equal value in return. Grants can either be operating or capital in nature. While grants to governments may result in the provision of some goods or services to the transferor, they do not give the transferor a claim to receive directly benefits of approximately equal value. For this reason, grants are referred to by the AASB as involuntary transfers and are termed non-reciprocal transfers. Receipt and sacrifice of approximately equal value may occur, but only by coincidence. For example, governments are not obliged to provide commensurate benefits, in the form of goods or services, to particular taxpayers in return for their taxes. Grants can be paid as general purpose grants which refer to grants that are not subject to conditions regarding their use. Alternatively, they may be paid as specific purpose grants which are paid for a particular purpose and/or have conditions attached regarding their use.
General government sector The general government sector comprises all government departments, offices and other bodies engaged in providing services free of charge or at prices significantly below their cost of production. General government services include those which are mainly non-market in nature, those which are largely for collective consumption by the community and those which involve the transfer or redistribution of income. These services are financed mainly through taxes, or other compulsory levies and user charges.
Interest expense Costs incurred in connection with the borrowing of funds includes interest on bank overdrafts and short-term and long-term liabilities, amortisation of discounts or premiums relating to liabilities, interest component of finance leases repayments, and the increase in financial liabilities and non-employee provisions due to the unwinding of discounts to reflect the passage of time. Interest income Interest income includes unwinding over time of discounts on financial assets and interest received on bank term deposits and other investments.
Joint Arrangements A joint arrangement is an arrangement of which two or more parties have joint control. A joint arrangement has the following characteristics:
• The parties are bound by a contractual arrangement. • The contractual arrangement gives two or more of those parties joint control of the arrangement
A joint arrangement is either a joint operation or a joint venture.
Liabilities Liabilities refers to interest-bearing liabilities mainly raised from public liabilities raised through the Treasury Corporation of Victoria, finance leases and other interest-bearing arrangements. Liabilities also include non-interest-bearing advances from government that are acquired for policy purposes.
Net acquisition of non-financial assets (from transactions) Purchases (and other acquisitions) of non-financial assets less sales (or disposals) of non-financial assets less depreciation plus changes in inventories and other movements in non-financial assets. It includes only those increases or decreases in non-financial assets resulting from transactions and therefore excludes write-offs, impairment write-downs and revaluations.
Net result Net result is a measure of financial performance of the operations for the period. It is the net result of items of income, gains and expenses (including losses) recognised for the period, excluding those that are classified as ‘other comprehensive income’. Net result from transactions/net operating balance Net result from transactions or net operating balance is a key fiscal aggregate and is income from transactions minus expenses from transactions. It is a summary measure of the ongoing sustainability of operations. It excludes gains and losses resulting from changes in price levels and other changes in the volume of assets.
Net worth Assets less liabilities, which is an economic measure of wealth. Non-financial assets Non-financial assets are all assets that are not ‘financial assets’. It includes inventories, land, buildings, infrastructure, road networks, land under roads, plant and equipment, investment properties, cultural and heritage assets, intangible and biological assets.
Non-profit institution A legal or social entity that is created for the purpose of producing or distributing goods and services but is not permitted to be a source of income, profit or other financial gain for the units that establish, control or finance it.
Payables Includes short and long term trade debt and accounts payable, grants, taxes and interest payable.

ANNUAL REPORT 2019 I 89
LATROBE REGIONAL HOSPITAL Notes to the Financial Statements for the Year Ended 30 June 2019
Note 8.10: Glossary of terms and style conventions (continued) Public financial corporation sector Public financial corporations (PFCs) are bodies primarily engaged in the provision of financial intermediation services or auxiliary financial services. They are able to incur financial liabilities on their own account (e.g. taking deposits, issuing securities or providing insurance services). Estimates are not published for the public financial corporation sector.
Public non-financial corporation sector The public non-financial corporation (PNFC) sector comprises bodies mainly engaged in the production of goods and services (of a non-financial nature) for sale in the market place at prices that aim to recover most of the costs involved (e.g. water and port authorities). In general, PNFCs are legally distinguishable from the governments which own them.
Receivables Includes amounts owing from government through appropriation receivable, short and long term trade credit and accounts receivable, accrued investment income, grants, taxes and interest receivable.
Sales of goods and services Refers to income from the direct provision of goods and services and includes fees and charges for services rendered, sales of goods and services, fees from regulatory services and work done as an agent for private enterprises. It also includes rental income under operating leases and on produced assets such as buildings and entertainment, but excludes rent income from the use of non-produced assets such as land. User charges includes sale of goods and services income.
Supplies and services Supplies and services generally represent cost of goods sold and the day-to-day running costs, including maintenance costs, incurred in the normal operations of the Department.
Transactions Revised Transactions are those economic flows that are considered to arise as a result of policy decisions, usually an interaction between two entities by mutual agreement. They also include flows in an entity such as depreciation where the owner is simultaneously acting as the owner of the depreciating asset and as the consumer of the service provided by the asset. Taxation is regarded as mutually agreed interactions between the government and taxpayers. Transactions can be in kind (e.g. assets provided/given free of charge or for nominal consideration) or where the final consideration is cash.
Style conventions Figures in the tables and in the text have been rounded. Discrepancies in tables between totals and sums of components reflect rounding. Percentage variations in all tables are based on the underlying unrounded amounts. The notation used in the tables is as follows: zero, or rounded to zero (xxx.x) negative numbers 201x year period 201x-1x year period

Photo credits: • Phill Mackie, Scribblevision• Kim Keltie Photography• Celine Foenander, LRH
Design and layout: • Wendy McEwan, Italicherry Design
(Report of Operations)• Phil Smith Design (Financial Report)

Village Avenue, Traralgon West PO Box 424 Traralgon, Victoria 3844
Tel 03 5173 8000 Fax 03 5173 8444
ABN 18 128 843 652
www.lrh.com.au
Latrobe Regional Hospital is located on the traditional land of the Braiakaulung clan of the Gunaikurnai Nation.
Better health services close to homeThat’s our commitment to you





























