Embed Size (px)
Citation preview

CASE REPORTS
Late Recurrence and Rapid Evolutionof Severe Hepatopulmonary SyndromeAfter Liver TransplantationMichael J. Krowka,* Gregory A. Wiseman,‡ Jeffery L. Steers,§and Russell H. Wiesner†
Recurrence of hepatopulmonary syndrome (HPS)after orthotopic liver transplantation (OLT) in anadult has never been reported. We describe a23-year-old woman who initially underwent OLTbecause of debilitating and severe HPS associ-ated with nonalcoholic steatohepatitis (NASH).Although the clinical resolution of HPS was welldocumented day 117 post-OLT, the reappearance
of NASH was documented by liver biopsy. Severehypoxemia because of recurrent HPS rapidlyevolved beginning approximately day 700 post-OLT. Retransplantation was attempted, but thepatient died post-OLT of sepsis and/or multiorganfailure.Copyright r 1999 by the American Association forthe Study of Liver Diseases
H epatopulmonary syndrome (HPS) is definedby the triad of (1) arterial hypoxemia
(PaO2 , 70 mm Hg or alveolar-arterial oxygengradient . 20 mm Hg), (2) intrapulmonary vascu-lar dilatations, and (3) chronic liver disease.1-3 Thecurrent criteria used to infer the existence ofpulmonary vascular dilatations include either posi-tive results from a contrast-enhanced transthoracicechocardiography (delayed microbubble opacifica-tion in the left atrium greater than three cardiaccycles after right atrial opacification), or abnormalextrapulmonary uptake of technetium-labeled mac-roaggregated albumin (99mTcMAA) after a lungperfusion scan (brain uptake .5%).3,4 Chronicliver disease has usually implied cirrhotic or noncir-rhotic portal hypertension.2,3
Complete resolution of HPS after orthotopicliver transplantation (OLT) has been well docu-mented, and some investigators consider this syn-drome a valid indication for OLT,5-7 especially inthe pediatric age group.8 We describe the subse-quent recurrence and rapid evolution of severe HPSin a woman approximately 700 days post-OLT whoinitially underwent transplantation for progressivehypoxemia caused by HPS associated with nonalco-holic steatohepatitis (NASH).
Case ReportThe pretransplantation course and posttransplantationclinical resolution of HPS in this patient have beenpreviously reported (Mayo Clinic case no. 3).5 Briefly,this patient underwent OLT at the age of 23 years
because of progressive and severe hypoxemia (PaO2, 53mm Hg standing at rest; 42 mm Hg with exercise,breathing room air) associated with biopsy-proven NASH.Portal hypertension was inferred by the existence ofesophageal varices and splenomegly. Delayed, positive-contrast echocardiography and abnormal extrapul-monary (brain) 99mTcMAA uptake after lung perfusionscanning (23%; normal ,5%) were compatible with theexistence of intrapulmonary vascular dilatations. Thetriad of chronic liver disease, arterial hypoxemia, andpulmonary vascular dilatations fulfilled the publishedcriteria for the diagnosis of HPS.
By day 117 post-OLT, the patient was asymptomatic,no longer required supplemental oxygen, and had nor-mal oxygenation breathing room air, with a PaO2 of 76mm Hg supine and 81 mm Hg standing. The PaO2 whenbreathing 100% oxygen was 576 mm Hg supine and 560mm Hg standing. Brain uptake after a 99mTcMAA lungscan normalized from a pre-OLT uptake of 23% to 2% inthe standing position (Fig. 1). A liver biopsy specimenshowed mild steatohepatitis with marked steatosis. Byday 360 post-OLT, active steatohepatitis with bridgingfibrosis was documented by biopsy.
Beginning approximately day 700 post-OLT and pro-gressing rapidly over the next 60 days, the patient
From the Divisions of *Pulmonary and Critical Care Medicineand †Gastroenterology and Hepatology, ‡Department of DiagnosticRadiology, Mayo Clinic, Rochester, MN; and the §Department ofSurgery, Mayo Clinic, Jacksonville, FL.
Address reprint requests to Michael J. Krowka, MD, Division ofPulmonary and Critical Care Medicine, 200 1st St SW, MayoClinic, Rochester, MN 55905.
Copyright r 1999 by the American Association for the Study ofLiver Diseases
1074-3022/99/0505-0014$3.00/0
Liver Transplantation and Surgery, Vol 5, No 5 (September), 1999: pp 451-453 451
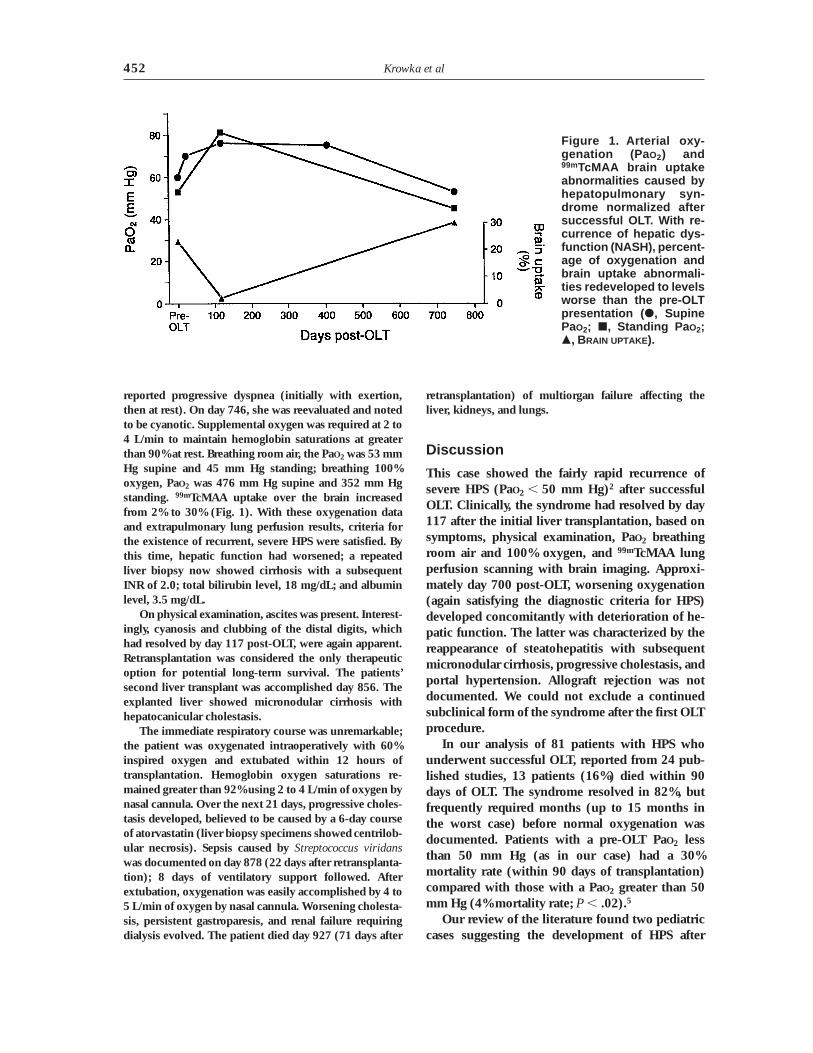
reported progressive dyspnea (initially with exertion,then at rest). On day 746, she was reevaluated and notedto be cyanotic. Supplemental oxygen was required at 2 to4 L/min to maintain hemoglobin saturations at greaterthan 90% at rest. Breathing room air, the PaO2 was 53 mmHg supine and 45 mm Hg standing; breathing 100%oxygen, PaO2 was 476 mm Hg supine and 352 mm Hgstanding. 99mTcMAA uptake over the brain increasedfrom 2% to 30% (Fig. 1). With these oxygenation dataand extrapulmonary lung perfusion results, criteria forthe existence of recurrent, severe HPS were satisfied. Bythis time, hepatic function had worsened; a repeatedliver biopsy now showed cirrhosis with a subsequentINR of 2.0; total bilirubin level, 18 mg/dL; and albuminlevel, 3.5 mg/dL.
On physical examination, ascites was present. Interest-ingly, cyanosis and clubbing of the distal digits, whichhad resolved by day 117 post-OLT, were again apparent.Retransplantation was considered the only therapeuticoption for potential long-term survival. The patients’second liver transplant was accomplished day 856. Theexplanted liver showed micronodular cirrhosis withhepatocanicular cholestasis.
The immediate respiratory course was unremarkable;the patient was oxygenated intraoperatively with 60%inspired oxygen and extubated within 12 hours oftransplantation. Hemoglobin oxygen saturations re-mained greater than 92% using 2 to 4 L/min of oxygen bynasal cannula. Over the next 21 days, progressive choles-tasis developed, believed to be caused by a 6-day courseof atorvastatin (liver biopsy specimens showed centrilob-ular necrosis). Sepsis caused by Streptococcus viridanswas documented on day 878 (22 days after retransplanta-tion); 8 days of ventilatory support followed. Afterextubation, oxygenation was easily accomplished by 4 to5 L/min of oxygen by nasal cannula. Worsening cholesta-sis, persistent gastroparesis, and renal failure requiringdialysis evolved. The patient died day 927 (71 days after
retransplantation) of multiorgan failure affecting theliver, kidneys, and lungs.
Discussion
This case showed the fairly rapid recurrence ofsevere HPS (PaO2 , 50 mm Hg)2 after successfulOLT. Clinically, the syndrome had resolved by day117 after the initial liver transplantation, based onsymptoms, physical examination, PaO2 breathingroom air and 100% oxygen, and 99mTcMAA lungperfusion scanning with brain imaging. Approxi-mately day 700 post-OLT, worsening oxygenation(again satisfying the diagnostic criteria for HPS)developed concomitantly with deterioration of he-patic function. The latter was characterized by thereappearance of steatohepatitis with subsequentmicronodular cirrhosis, progressive cholestasis, andportal hypertension. Allograft rejection was notdocumented. We could not exclude a continuedsubclinical form of the syndrome after the first OLTprocedure.
In our analysis of 81 patients with HPS whounderwent successful OLT, reported from 24 pub-lished studies, 13 patients (16%) died within 90days of OLT. The syndrome resolved in 82%, butfrequently required months (up to 15 months inthe worst case) before normal oxygenation wasdocumented. Patients with a pre-OLT PaO2 lessthan 50 mm Hg (as in our case) had a 30%mortality rate (within 90 days of transplantation)compared with those with a PaO2 greater than 50mm Hg (4% mortality rate; P , .02).5
Our review of the literature found two pediatriccases suggesting the development of HPS after
Figure 1. Arterial oxy-genation (Pa O2) and99mTcMAA brain uptakeabnormalities caused byhepatopulmonary syn-drome normalized aftersuccessful OLT. With re-currence of hepatic dys-function (NASH), percent-age of oxygenation andbrain uptake abnormali-ties redeveloped to levelsworse than the pre-OLTpresentation ( d, SupinePaO2; j, Standing Pa O2;m, BRAIN UPTAKE ).
Krowka et al452

OLT. Crary et al9 documented hypoxemia (hemo-globin saturations of 80% to 90%) and abnormalextrapulmonary uptake of 99mTc MAA in associa-tion with chronic allograft rejection 31⁄2 yearspost-OLT in a 5-year-old girl who underwenttransplantation for extrahepatic biliary atresia. Post-mortem injection of the pulmonary arteries withbarium sulfate showed microscopic arteriovenouscommunications. DeGoyet et al10 described a childwith biliary atresia who underwent transplantationfor HPS. Within 6 months of transplantation, theseinvestigators reported a recurrence of HPS associ-ated with the development of portal vein thrombo-sis. Surgical correction of the portal vein thrombo-sis by hepatic revascularization resulted in completeresolution of hypoxemia.
A genetic predisposition to HPS would appearplausible in our case. The pulmonary circulationappeared to be affected by an insult (HPS) associ-ated with the native liver, normalization of oxygen-ation followed with an unrelated allograft, andrecurrence of similar pulmonary vascular patho-physiologic characteristics with allograft dysfunc-tion. The recurrence of NASH in this case sug-gested a systemic (genetic?) process that may haveaffected a susceptible hepatic allograft and hostpulmonary vasculature. The post-OLT recurrence(or de novo development) of HPS associated withhepatic allograft failure appears rare and may berelated to the type of liver disease pre-OLT.
This case showed the clinical resolution andlate, but rapid, recurrence of severe HPS aftersuccessful OLT. Genetic predisposition, directlyaffecting the pulmonary vascular bed and possiblyrelated to the initial hepatic pathological state in
the allograft, may be a factor in the pathophysi-ologic course of recurrent HPS.
References
1. Lange PA, Stoller JK. The hepatopulmonary syndrome.Ann Intern Med 1995;122:521-529.
2. Herve P, Lebrec D, Brenot F, Simmoneau G, HumbertM, Sitbon O, Duvoux P. Pulmonary vascular disorders inportal hypertension. Eur Respir J 1998;11:1153-1166.
3. Scott VL, Dodson SF, Kang Y. The hepatopulmonarysyndrome. Surg Clin North Am 1999;79:23-41.
4. Abrams GA, Nanda NC, Dubovsky EV, Krowka MJ,Fallon MB. Use of macroaggregated lung perfusionscan to diagnose hepatopulmonary syndrome: A newapproach. Gastroenterology 1998;114:305-310.
5. Krowka MJ, Porayko MK, Plevak DJ, Pappas SC,Steers JL, Krom RAF, Wiesner RH. Hepatopulmonarysyndrome with progressive hypoxemia as an indicationfor liver transplantation: Case reports and literaturereview. Mayo Clin Proc 1997;72:44-53.
6. Laberge JM, Brandt ML, Lebeque P, Moulin D, Veyke-mans F, Paradis K, et al. Reversal of cirrhosis-relatedpulmonary shunting in two children by orthotopic livertransplantation. Transplantation 1992;53:1135-1138.
7. Van Obbergh L, Carlier M, de Clety SC, Sokal E,Renotte MT, Veyckemans F, et al. Liver transplantationand pulmonary gas exchange in hypoxemic children.Am Rev Respir Dis 1993;148:1408-1410.
8. United Network for Organ Sharing. Amended UNOSPolicy 3.6 (Amended Appendix 3B ‘‘Indications for livertransplantation in children.’’) Approved by the UNOSBoard of Directors June 25, 1998.
9. Crary GS, Burke BA, Alford BA, duCret RP. Pulmonaryarteriovenous shunting in a child with cirrhosis of theliver. Am J Dis Child 1989;143:749-751.
10. De Goyet JV, Gibbs P, Clayput P, Reding R, Sokal EM,Otte JB. Original extrahepatic approach for hepaticportal revascularization and relief of portal hypertensionrelated to late portal vein thrombosis after pediatric livertransplantation. Transplantation 1996;62:71-75.
Recurrence of Hepatopulmonary Syndrome 453





























