Embed Size (px)
DESCRIPTION
Kidney transplant res guide
Citation preview

Division of Organ Transplantation
Resident Manual
Rhode Island Hospital A Lifespan Partner
Compiled by:
Paul Morrissey, MD Revised: December 2011
Available at: http://intra.lifespan.org/surgery.
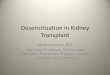
Actuarial Survival
Tacrolimus + Mycophenolate regimen

2
Table of Contents
ORDERS
Admissions to the Transplant Surgical and Medical Services
ORDERS after donor nephrectomy
ORDERS for renal transplant patients
Post-op
MEDICATIONS
Transplantation historical timeline
Immunosuppressive medications – Mechanism of Action
Transplant medications - routine dosing and prescriptions
Steroids
GRAFT DYSFUNCTION
Early considerations after renal transplant
Algorithm for work-up of rising creatinine
Infectious complications
Late complications after transplantation (Ciba)
Clinical rejection
Hyperacute
Acute rejection
Chronic rejection
GENERAL INFORMATION
Success of renal transplantation
Live donor versus Cadaver Renal Transplant (CRT)
Organ Donation
Dialysis Access Game Plan
ASTS WEBSITE (Resident Education in Transplantation) http://www.asts.org/FellowshipTraining/ResidentEducati
on/Resident1.aspx
Administrative issues
Transplant office and clinic
APC 921
444-5285 or 444-8345
Transplant surgeons
Kevin Charpentier 350-3848 (b)
Paul Morrissey 350-1385 (b)
Transplant physicians
Reg Gohh 350-5553 (b)
Terri Montague 350-7227 (b)
Staci Fischer 350-9022 (b)
Transplant Manager
Bette Hopkins-Senecal 350-5523 (b)
Transplant Clinical Coordinators
Nancy McNamara, RN 444-3186
Mary Ellen Espanola, RN 444-3284
Rounds
The team meets at 9:00 (8:30 on Thursday for Journal Club) to
discuss patients. Walk rounds begin at 4:00 PM on 4A or 5ISC.
Clinic (Surgery residents attend one clinic per week)
Tuesday - Dr. Morrissey (1:00 PM)
Friday - Dr. Charpentier (9:30 AM)
Surgery
Renal transplant with Senior Resident or AR-III (cadaveric)
Donors by AR-II; AV access with AR I or II
PD catheters and PermCaths with AR I or II
Resident Duties – Routine care of in-house transplant surgical
patients, discharge summaries, admissions, consultations and in-
house pre-ops.

3
Kidney Donors Donor nephrectomy is unique among surgical procedures as the patient is
undergoing major surgery with all its risks (1% incidence of major
complication, 0.03% incidence of mortality) for no medical benefit.
Therefore, special attention to detail is required for the donor‟s safety.
Eligible donors are in good health, ABO compatible with the recipient
and have normal renal function. Spouses and close friends are potential
unrelated donors. Pre-op testing consists of physical exam, labs, 24-hr.
urine collection for creatinine clearance, renal ultrasound and CT
angiogram (for renal anatomy). The surgery is performed (1)
laparoscopically, (2) mini-open nephrectomy via an anterior-
retroperitoneal approach or (3) via a flank incision (over 11th rib).
POST-OP – Typical course through discharge
Prophylactic Rx: Spirometer, heparin 5000U sc bid x 48 hr
Sequential compression devices (Venodyne boots)
Pain management: PCA for 1-2 days
Clear liquid diet
POD #1
Heplock or KVO I.V. when tolerates adequate P.O.
D/c Foley catheter; d/c Venodyne boots when ambulating
Advance to regular diet as tolerated.
Check CBC, BUN/creatinine
POD #2
Check CBC, BUN/creatinine
POD #3
D/c PCA
Vicodin (or Percocet) for analgesia
Laxative prn (begin P.O., then use suppository if no effect)
D/c to home today or next day
F/U 10-14 days in Transplant Clinic
One week supply of analgesics (usually 20-30 tablets)
Donors
There are two sources of kidneys: either a living donor (relative,
spouse or friend, e.g.) or a deceased donor (brain dead or donor
after circulatory death (DCD)). Live donors are preferred for many
reasons, especially the reduced time on dialysis for the recipient.
Item Live donor Deceased donor
Allograft half-life 12-14 years 8-9 years
Waiting time 2 - 4 months 18 - 48 months
Donor Age 18 - 65 4 - 70
Quality of kidney Excellent Fair to excellent
Immediate function 97 % 50 %
DGF* 2 % 30 %
Hospital LOS 5 - 7 days 5 - 14 days
Surgery Planned Urgent
Immunosuppression Lower doses Standard
Risk of acute rejection 5 - 10 % 15 - 20%
*Delayed graft function – requires dialysis after transplant.
Requirements for live donor renal transplants
1. Compatible blood type – ABO, HLA matching not required
2. Excellent health – low operative risk
3. Normal renal function – 24 hour urine collection, U/S and CT
4. Proper motivation (voluntary donation)
Risks to the Donor
Hyperchloremic metabolic acidosis (Kellum JA. CCM 2002; 30: 259.)
Major complication < 1 % (e.g. - bleeding, injure adjacent structure,
AMI, DVT or PE, significant injury to donor kidney)
Lifetime risk of HTN, ESRD – same as general population.

4
DECEASED ORGAN DONORS
Brain Dead Donor
Standard criteria donor (SCD) – other than ECD
Expanded criteria donor (ECD)
1. Donor age > 60 years or
2. Donor age > 50 with 2 of the following:
a. Pre-retrieval creatinine > 1.5 mg/dL
b. Death from CVA
c. History of hypertension
Donor after Circulatory Death (DCD)
Donor with irreversible brain injury, family decides on CMO
status, organs (usually kidneys ± liver) are recovered after
extubation and progression to circulatory arrest (5 minutes).
TRANSPLANT RECIPIENT MANAGEMENT - FLUIDS
0.9 % Saline
Volume - most patients get 2-3 L in the OR and cc/cc
replacement of UO thereafter. Hypovolemia is unusual post-
op. The CVP is a rough (though inaccurate) measure;
however aiming for a CVP > 10 is a reasonable guide.
Urine output – most live donors have an initial UO of 200-1000
cc/hr, while a deceased donor with ATN might be expected
to be oliguric.
BP - high normal or slightly elevated BP is best for renal
reperfusion. Even low normal BP can result in ATN and
requirements for dialysis post-op. Goal > 130 mm Hg.
BP MANAGEMENT POST-OP
The short-term effects of hypotension (ATN, DGF) complicate
patient care after renal transplantation. The short-term effects
of hypertension are minimal, especially in this population with
> 85% incidence of hypertension. SBP <100 should be treated
promptly with IV fluids or a vasopressor (Neosynephrine qtt).
Pre-operative β-blockers should be continued as tolerated. .
KIDNEY TRANSPLANT RECIPIENT ORDERS
Expected LOS – 5 days (longer with delayed graft function, DGF)
ORDERS FOR PATIENT CARE
ADMIT to PACU, then 5ISCU
DIAGNOSIS: S/P renal transplant
VITALS: Hourly BP; target SBP > 130. Use neosynephrine PRN
for BP support if SBP and urine output are low.
ACTIVITY: OOB to chair POD #1, then ambulate
NURSING:
Strict I & O
CXR in PACU – R/O pneumothorax if new line placed.
Foley to gravity, d/c Foley catheter on POD #5
MEDS:
Induction: Thymoglobulin (high immune risk or high risk
of DGF) or basiliximab (Simulect).
Immunosuppression: usually tacrolimus (Prograf),
mycophenolate mofetil (CellCept) or EC-MPA (Myfortic)
and steroid taper as below.
Day 1 Solumedrol 250 mg IV times one, then
Prednisone taper as follows:
STANDARD
Day 2-6 Prednisone 30 mg po BID
Day 7-14 Prednisone 20 mg po BID
Day 15-21 Prednisone 10 mg po BID
Day 22-28 Prednisone 10 mg po AM, 5 mg PM
Day 29 onward Prednisone 10 mg po QD.
or
RAPID TAPER
Day 1 Solumedrol 250 mg
Day 2 Prednisone 40 mg po BID
Day 3 Prednisone 20 mg po BID
Day 4 Prednisone 10 mg po BID
Day 5 onward. Prednisone 10 mg po QD

5
POM contains order sets for the donor and recipient. Some
explanations and instructions are given below.
LABS:
Every 6 hours x 24 hours, then q 12 hr on POD#2, then QD.
Tacrolimus level or CsA level QD beginning day after
medication begins.
Ca, Mg, PO4 may become depleted with high volume diuresis.
CBC with differential (lymph count guides Thymoglobulin
dosing)
IV Fluids:
Replacement cc/cc of urine output due to tubular injury
Replacement IVF is ½ NS (similar [Na+] to urine)
D5 ½ NS is “maintenance” until adequate PO intake
Other management issues:
JP Drain – d/c when output < 50 cc/ day
Foley – d/c on POD #5
PCA – d/c on POD # 2
Dressing – change prn and always by POD # 2
Daily weights
CVL – d/c on AM of discharge
RN may draw labs from CVL
Rationale for ancillary medications after renal transplant
Antacids – Ulcer prophylaxis due to steroids and for dyspepsia
due to Cellcept (common side effect)
Bactrim Single Strength – PCP, Nocardia and UTI prophylaxis
Mycelex – Thrush prophylaxis
Ketoconazole - Fungal prophylaxis and CYT p450 3A
inhibition (used when CsA is 1* immunosuppressant).
Valganciclovir - CMV and EBV (Mononucleosis and
lymphoma) prophylaxis.
BP medications – 85% of recipients have HTN. Blood pressure
at the time of discharge is often high (due in part to immuno-
suppression and volume overload) and BP is gradually adjusted
as an outpatient.
Insulin – Type I DM or patients on oral agents at the time of
transplant invariably require insulin therapy on discharge.
Managing BS after transplant is optimally done with a QD
Lantus regimen and Humolog sliding scale transitioned to pre-
meal short-acting insulin. Minimally elevated FSBS (120 –
200s) can initially be controlled with sliding scale insulin and
adding an oral agent or longer-acting preparation as indicated.
Prudent use of peri-operative Lantus (for patients on insulin pre-
transplant) and sliding scale insulin should limit the need for an
insulin drip in most patients.

6
Preferred peri-operative and long-term blood pressure management:
Class Example Note
Beta-blocker Atenolol, Toprol First line
CaCB (Dihydropyridine) Norvasc Second line
Alpha blocker Cardura QHS dosing
Diuretic Lasix Volume overload
Treatment of Hypertensive Urgency vs. Emergency
A hypertensive emergency is a condition in which elevated blood
pressure results in acute target organ damage. The systems primarily
involved are the CNS, the CV system, and the kidneys. In order to
diagnose malignant hypertension, papilledema must be present.
Accelerated Htn is defined as a recent significant increase over
baseline blood pressure that is associated with target organ damage.
Funduscopic exam may show vascular damage (flame-shaped
hemorrhages).
Hypertensive urgency must be distinguished from emergency.
Urgency is defined as severely elevated blood pressure (systolic
>220 mm Hg or diastolic >120 mm Hg) with no evidence of target
organ damage.
Hypertensive emergencies require immediate therapy to decrease
BP within minutes to hours. No evidence suggests a benefit from
rapidly reducing BP in patients with hypertensive urgency. Such
aggressive therapy may harm the patient, resulting in cardiac, renal,
or cerebral hypo-perfusion. Increasing the dose of an existing BP
med or adding another medication is the best approach.
The cardiac presentation of malignant Htn is angina, AMI or CHF.
Neurological presentations are occipital headaches, cerebral infarct,
cerebral hemorrhage, or hypertensive encephalopathy. Hypertensive
encephalopathy is a symptom complex of severe hypertension,
headache, vomiting, visual disturbance, mental status changes,
seizure, and retinopathy with papilledema. Focal signs and
symptoms are uncommon. Renal disease presents as proteinuria,
microscopic hematuria, red blood cell casts, and oliguric renal
failure.
Differential Diagnosis: complications of pregnancy; cocaine;
withdrawal of alcohol, beta-blockers, or alpha-stimulants; renal
artery stenosis, pheo, Ao coarctation, and hyperaldosteronism.
Treatment of Hypertensive Urgency/Emergency – borderline cases
requiring more than gradual increasing of Htn medication.
Labetalol (alpha and beta-blocker) is a safe and effective agent to
consider, provided that the patient does not have asthma, heart
failure, or heart block.
Add 2 vials of Labetalol (40ml) to 250 ml D5W and start at
3ml/min. The BP should start to drop within half an hour. Labetalol
can also be given as a 20mg bolus over 2 minutes; repeated with a
40 mg dose every 10 minutes until the desired BP is reached or 300
mg have been given. Response is usually within 5-10 minutes.
Hypertensive Emergency (Encephalopathy, AMI, CHF or unstable
angina) - Admission to ICU is warranted.
Nitroprusside (Nipride, 0.25 ug/kg/min). It dilates both arteries and
veins and is not associated with tachyphylaxis. It's onset of action is
rapid and minute by minute BP monitoring is required.
Hydralazine 5-25 mg IV, coupled with a beta blocker to prevent
reflex tachycardia is a safe alternative. Hydralazine may be repeated
q4h as necessary.
Esmolol is also a reliable drug in this situation and can be
administered by IV infusion.

7
Timeline of Immunosuppressive Agents in Transplantation
1954 – None available (Identical twin transplant - PBBH)
1959 - Total body irradiation and cancer chemotherapeutics
Fraternal Twins in Boston and Paris are first successful
transplants with immunosuppression.
1960 - 6-mercaptopurine
1961 – Azathioprine (imidazole derivative of 6-MP)
First successful Cadaver Renal Transplant reported.
1962 - Prednisone
1965 – Polyclonal antibodies to T-cells: ALG / ATGAM with
serum obtained from horses, goats, and rabbits.
1975 - Donor specific transfusions given pre-transplant
1975 - OKT3 (mouse monoclonal Ab versus CD3)
CD3 = receptor expressed on all T cells
1978 - Cyclosporine (available clinically in 1983)
1994 - Tacrolimus (FK506)
1995 - Mycophenolate mofetil (Cellcept)
1998 - IL-2R monoclonal Ab (Simulect, Zenapax)
1999 – Thymoglobulin Rabbit – ATG)*
1999 - Sirolimus (Rapamune)
* FDA approved for treatment of rejection versus other agents
approved for the prevention of organ rejection following
renal transplantation.
Drug Protocols and Rationale
Triple Therapy: a three-drug combination for immunosuppression,
which allows for adequate immunosuppression with modest doses
of all three drugs. In theory, side effects of each drug are
minimized. Prograf® (tacrolimus)
Cellcept® (mycophenolate mofetil) of Myfortic (MPA)
Prednisone
Prograf® (tacrolimus)
Imuran® (azathioprine, if Cellcept not tolerated)
Prednisone
Neoral® (cyclosporine)
Azathioprine or Cellcept
Prednisone
Rapamune® may be substituted for Prograf, Neoral or Cellcept
Induction Therapy – Antibody (Simulect, Thymoglobulin (rabbit
antithymocyte globulin) or OKT3) used at the time of the initial
transplant as prophylaxis rather than therapy for acute rejection.
Currently, we offer Ab induction to patients with a PRA > 20%,
repeat transplant, high likelihood of delayed graft function or a plan
to limit other immunosuppression (steroid withdrawal, e.g.).
OKT3 – monoclonal Ab to CD3 (First mAb ever in clinical use.)
Used for the treatment of severe acute rejection. Associated with
cytokine release syndrome (fever, hypotension, CHF).
Basiliximab – chimeric mouse-human mAb to IL-2 receptor (CD25)
Benefit in reducing acute rejection (40% versus 20% at 6
months) and allowing safe steroid minimization.
rATG – polyclonal Ab against many T-cell antigens produced by
immunizing rabbits with human thymocytes. Pre-medicate with
steroids, diphenhydramine (25 mg) and acetaminophen (650 mg) to
prevent cytokine release syndrome.

8
TYPICAL IMMUNOSUPPRESSION PLAN
INDUCTION
Basiliximab (Simulect) Dose: 20 mg on POD #0 and #4
Indications: Low immunologic risk, future Thymoglobulin
exposure planned (PAK), high medical risk for over-
immunosuppression
Utility: A meta-analysis of randomized trials. Transplantation
2004; 77: 166.
rATG (Thymoglobulin) Dose: 1.5 mg/kg/d (round to 25 mg increments; maximum dose
150 mg) via CVL
Higher immunologic risk (High PRA, DSA) or high likelihood
of DGF
Usual dose: 1.5 mg/kg on day of surgery and 2 more doses
(4.5 mg/kg)
DGF or high immunologic risk: 1.5 mg/kg for 4-5 doses
(6.0-7.5 mg/kg)
MAINTENANCE
Prograf (Tacrolimus) Dose: Target 7-10 ng/ml first 2 months, 6-8 ng/ml 2-6 months,
5-8 ng/ml after 6 months.
Mycophenolic acid (EC-MPA, Myfortic) Dose: 720 BID
Consider: 540 BID less than 50 kg or 360 BID for elderly
patients, prior GI symptoms, or current leukopenia.
Methylprednisolone / Prednisone Rapid taper (10 mg by day 5) = 500, 250, 40 bid x 1 day, 20
bid x 1 day, 10 bid x 1 day, 10 QD.
Standard taper (10 mg by day 29) = 500, 250, 30 bid x 5
days, 20 bid x 7 d, 10 bid x 7 d, 15 mg/d x 7, then 10 mg/d.
Pancreas: see taper (including methylprednisolone x 3 d) to
10 mg/d on POD #7.
NOTES:
1. Pancreas Transplantation: as above with routine
Thymoglobulin induction.
2. 0-MM allograft: consider no induction, rapid steroid taper or
two-drug regimen.
3. DSA present – consider IVIG at induction and
Plasmapheresis.
PROPHYLAXIS
Bactrim SS – begin post-op day #3 and continue for one year.
Clotrimazole troches – begin post-op day #3 and continue for
one month.
Valganciclovir – 900 mg QD* x 3 months for D+R+, D-R+. Rx
D+R- for six months. D-R- (Donor and Recipient negative
for CMV IgG): obtain serial CMV PCR every 2-4 weeks for
6 months, pre-emptive therapy if PCR > 500 copies.
(*450 mg/d for creatinine > 2.5, leukopenia, $$$ issues or low
body weight.)
Pancreas Transplant - Steroid Taper:
Methylprednisolone 70 mg IV 2XD for one day then
Methylprednisolone 35 mg IV 2XD for one day then
Methylprednisolone 17.5 mg 2XD for one day then
Prednisone 15 mg PO 2XD for one day then
Prednisone 25 mg PO daily for one day then
Prednisone 20 mg PO daily for one day then
Prednisone 10 mg PO daily until discontinued

9
CORTICOSTEROIDS (Prednisone, Solumedrol)
Rapid taper to 10 mg daily
1. Bind intracellular receptors blocking DNA/RNA synthesis
2. Inhibit IL-1 secretion (costimulator); Inhibit MAC chemotaxis
3. Anti-inflammatory
4. Apoptosis at high doses (pulse therapy lympholysis)
5. Toxicity: Steroid side effects
Hypertension, Sodium / fluid retention
Psychosis / emotional instability
Peptic ulcer disease
Delayed growth, Amenorrhea, Osteopenia
Centripetal obesity (Cushingoid appearance)
Glucose intolerance, Hyperlipidemia
Glaucoma / cataracts
Neutrophil dysfunction / sepsis
AZATHIOPRINE (Imuran)
2-3 mg / kg / day
1. Blocks the synthesis of purine nucleotides
2. Toxicity: leukopenia (common), GI upset (rare)
MYCOPHENOLATE MOFETIL (Cellcept)
500 - 1000 mg BID
Enteric Coated - MYCOPHENOLIC ACID (Myfortic)
360 - 720 mg BID
1. Inhibitor of inosine monophosphate dehydrogenase (IMPDH)
2. Blocks de novo synthesis of purine nucleotides
3. Most cells, but not lymphocytes, can make purines via a salvage
pathway
4. Increased activity against Type II IMPDH which is abundant in
active lymphocytes
5. Efficacy: reduced AR to 20% compared to 40% with Imuran
6. Toxicity - leukopenia (common), gastritis, diarrhea.
CYCLOSPORINE (Sandimmune, Neoral)
Dose to achieve trough levels of 100-400 ng/ml
1. Peptide derived from fungus Tolypocladium inflatum
2. Blocks the mRNA (transcription) for IL-2 and INF-g
3. IL-2 formerly called “T cell growth factor” stimulates the
proliferation of T lymphocytes
4. Toxicity: Nephrotoxic in high dose
Hypertension
Neurotoxic (tremor, parethesias)
HyperK+
Renal tubular acidosis
Gout
Excess hair growth
Gum hyperplasia
TACROLIMUS (Prograf, "FK506")
Dose to achieve trough levels or 5-15 ng/ml
1. Macrolide ABx derived from Strep . tsukubaenis
2. Inhibits transcription of IL-2 similar to CsA (Also IL-3, 4, 5,
INF-g, TNF, GM-CSF, IL-2R)
3. Similar toxicity profile to CsA
4. Differences from CsA: More post-transplant diabetes
No cosmetic or lipid SE
Can reverse acute rejection
SIROLIMUS (Rapamune)
Dose to achieve trough levels 5-15 ng/ml
1. Derived from Streptomyces hygroscopicus (Easter Island)
2. Inhibits IL-2 signal; arresting T-cell in G1-S phase
3. Synergistic with CsA or tacrolimus (which fx in G0-G1 phase)
4. Not nephrotoxic (board question) !
5. Toxicity: hyperlipidemia, low cell counts, delayed healing,
lymphocele formation, Pneumonitis
6. Less mutagenic; actually in trials as CA chemotherapeutic

10
Immunosuppression - DOSING
DRUG Low dose Moderate High Too much
CsA 80-150 150-250 250-400 Greater 400
Prograf 3-6 ng/ml 6 - 10 10 - 15 Greater than 15
Azathioprine (Imuran): 1-3 mg/kg once daily.
Mycophenolate mofetil (Cellcept, Myfortic): 500 – 1000 mg/ BID
depending on body size, GI side effects (heartburn, gastritis,
diarrhea) and WBC (reduce dose if < 3.0)
Steroids – slow taper to 10 mg/d at one month or rapid taper to 10
mg/d at POD #5 (see orders). If there is no history of acute
rejection continue taper to 5 mg/d after 3-6 months.
TRANSPLANT PRESCRIPTIONS:
Most patients use a mail-order pharmacy and Rx are filled by
our Transplant RNs, otherwise please discharge from the
hospital with a six-month supply of all meds (one month supply
with 5 refills). Pain med (narcotic) scripts must be written.
Immunosuppression
Prograf (tacrolimus) - supplied as 1 and 5 mg capsules
Neoral (cyclosporine) - supplied as 100 and 25 mg capsules
Cellcept - supplied as 250 or 500 mg capsules, 180 or 360 for MPA.
Prednisone - discharge with 10 mg capsules (#100)
Prophylaxis
Axid – QD or bid; Protonix (pantoprazole) if previous Hx of PUD
Bactrim SS (for PCP and UTI) - QD (6 months); then every MWF
Mycelex (for thrush) – QID with meals for 1 month.
Valganciclovir (for CMV) - 450 or 900 mg QD for 3-6 months.
Steroid equivalents
Duration Potency t1/2 Equivalent
Short
Hydrocortisone 1 8-12 hr 20 mg
Intermediate
Prednisone* 4 18-36 5 mg
Methylprednisolone 5** 12-36 4 mg
Long
Dexamethasone 25 36-54 0.75 mg
* Physiologic equivalent is 7.5 mg per day
** For simplicity we usually convert methylprednisolone
(Solumedrol) 1:1 with prednisone when patients can not take PO.
Stress steroids
Stress doses of steroids are not required for mild-moderate medical
illnesses (infections, MI, etc.) or for surgery after transplant (re-
operations, catheter removals, elective general surgery). Patients
require only their usual maintenance dose of prednisone. “Stress
steroids” may be beneficial in severely ill patients on long-term
steroids (sepsis in the ICU, severe asthma attacks, major multiple
trauma victim). Patients with evidence of adrenal insufficiency
(low BP, low sodium, unexplained MS changes, etc.) should
receive stress steroids.
References:
(1) Stress steroids are not required for patients receiving a renal
allograft and undergoing operation. JACS 1995, 180:532.
(2) Corticosteroid therapy in severe illness. NEJM 1997, 337:
1285.

11
Early Considerations after Renal Transplantation
The one and five year allograft survivals are:
1-year 5-year
Live donor renal transplant - 95 % 88 %
Cadaver renal transplant* - 88 % 70 %
*(immediate function)
Cadaver renal Tx (DGF*) - 70 % 50 %
DGF – delayed graft function defined as oliguria necessitating dialysis
after transplantation.
Surgical considerations
Bleeding - anastomotic, hematuria, peri-graft.
Thrombosis - renal artery or vein (1%)
Ureteral or urethral (Foley) obstruction - use of stent
Urine leak - immediate or delayed (weeks)
Ureteral stricture – weeks to years later
Obstruction by compression (lymphocele, urinoma)
Early renal transplant dysfunction
Immediate function with high output diuresis – due to fluid
overload, osmotic diuresis from inadequate hemodialysis,
intraoperative diuretics, proximal renal tubular injury
Delayed function – due to ischemia-reperfusion injury
Risks: donor age, donor hypotension and vasopressor use,
cold and warm ischemic times
SE: cardiac, pulmonary edema
Cytokine release syndrome with use of ATG
ATN
Hypovolemia (CVP), hypotension, MI, CHF, seizure,
sepsis
Cyclosporine or tacrolimus (CNI) toxicity
Rejection – unusual in the first week after transplantation.
Algorithm: renal transplant dysfunction
Hx and PEx Differential Dx
Weight gain / edema Dehydration
Oliguria Drug toxicity
Hypertension Infection
Allograft pain Hydronephrosis Stricture
Fever, chills, myalgias Rejection Lymphocele
Technical pblm Compression
EVALUATION
Labs: Chem 7, CBC, LFT‟s, CsA or Tacrolimus level, U/A + C &
S, Urine sediment (ATN, PMN).
Pre-biopsy labs: PT, PTT, CBC, T & C 2U, bleeding time.
Usual approach:
Hydrate overnight, thorough history (new meds such as ACEI,
NSAIDs, Abx; recent illness, change in BP, glucose control).
Check labs, urinalysis, and urine sediment.
Renal consult to assist with assessment and perform biopsy.
Ultrasound to R/O technical problem.
Renal biopsy (2 U/S-guided 18G core biopsies of renal cortex).
Common surgical complications after renal transplantation
Ureteral complications (10%) – leak or stricture (obstruction)
Lymphocele (5%) – may be incidental or cause compression
Wound infection (3%), Hernia (3%)
Colon perforation (diverticulitis - 3%)
Pathologic fractures
Tertiary hyperparathyroidism – most resolve in 6-12 months. Some
require cinacalcet or parathyroidectomy (one gland or 3 ½ glands).
Progressive vascular disease including amputation
Cancer – skin, renal and other solid tumors.

12
Infectious complications after transplantation
Early Middle Late
(0 - 6 weeks) (6 weeks - 6 months) (> 6 months)
Wound infection CMV disease PCP*
Line sepsis PCP* Cryptococcus
UTI / urosepsis Candidiasis Pneumonia
Herpes Nocardia UTI
Pneumonia Polyoma virus PML
Thrush EBV Viral infections**
Dialysis access Legionella Mycoplasma
* Incidence <0.1 % with Bactrim prophylaxis.
** CMV most likely in middle period. RSV, HSV, adenovirus, influenza
can occur in middle and late periods.
Routine work-up is based on Hx, PEx, post-op period, etc., but may
include bacterial, fungal, and viral cultures, mycoplasma and acid
fast (TB), Legionella cultures, silver stains for PCP, cryptococcal
Ag.
CMV is diagnosed by rapid spin-amplified viral culture, IgM
antibody, CMV PCR or by inclusion bodies in a tissue biopsy. The
diagnosis is suspected when the triad of leukopenia, unexplained
fevers and flu-like symptoms is noted.
Pneumonia is evaluated by appropriate sputum samples. If these
can not be obtained within 6-12 hours of admission, proceed to
bronchoscopy. PCP is extremely rare with Bactrim prophylaxis.
Polyoma (BK) virus affects the urinary tract and causes renal
transplant dysfunction. The inflammatory infiltrate mimics acute
rejection.
Pneumonia evaluation
Sputum or induced sputum
Bronchoscopy PRN
AFB
Fungal stains and cultures
PCP DFA
Legionella urinary Ag
Histoplasmosis serology (P. Rico and Ohio River Valley)
Coccidioidomycosis (Southwestern USA)
Cryptococcus serum Ag
Nocardia smear and stain
Respiratory viral cultures
CMV – biopsy
Chlamydia
Open lung biopsy - PRN

13
Success Rates for Renal Transplantation
Allograft survival based on donor source and HLA matching.
Graft survival
Category N 1-year 3-year
HLA-ID sibling 1984 97 95
Spouse donor 368 95 85
Other living unrelated 129 97 81
Parent donor 3368 95 82
Cadaver donor 43,341 85 70
CRT with DGF 11,060 70 60
Terasaki et al. High survival rates of kidney transplants from spousal and
unrelated donors. NEJM 1995; 333: 333-6.
Long-term Survival after AMI in Dialysis Patients
Overall mortality after AMI (%)
Category 1-yr 2-yr 3-yr 4-yr
Patients on hemodialysis 59 73 81 90
Dialysis + DM 62 77 86 93
Dialysis + Htn 61 73 81 90
Transplant recipients* 24 30 36 47
Renal Tx + DM 29 36 43 54
* Differences persisted after adjustment for age and other demographic
factors, cause of renal failure, duration of ESRD and coexisting illnesses.
Herzog et al. NEJM 1998; 339: 799-805.
Chronic Renal Failure – A Vasculopathic State (NEJM 1998;
339:841.)
2/3 of ESRD patients have DM or Htn
Reasons are multi-factorial
Renal dysfunction
Chronic inflammatory state
Hyperhomocysteinemia
Syndrome X
Anemia
Chronic volume overload
Elevated oxidized low-density lipoprotein
Secondary hyperparathyroidism
Endothelial cell dysfunction: excess ET-1 and diminished NO
LVH, impaired cardiac microcirculation, tendency to
arrhythmias.

14
Rejection – Banff Schema (Am J Tx: 2008 8(4):753-60.)
Borderline changes: „Suspicious‟ for acute cellular rejection. No
intimal arteritis is present, but there are foci of mild tubulitis (1–
4 cells/tubular cross-section) and mild inflammation.
Acute/active cellular rejection
T-cell-mediated rejection graded by histopathological findings:
IA Cases with significant interstitial infiltration (>25% of
parenchyma affected) and foci of moderate tubulitis (>4
mononuclear cells/tubular cross section or group of 10 tubular cells)
IB Cases with significant interstitial infiltration (>25% of
parenchyma affected) and foci of severe tubulitis (>10 mononuclear
cells/tubular cross-section or group of 10 tubular cells)
IIA Cases with mild-to-moderate intimal arteritis (v1)
IIB Cases with severe intimal arteritis comprising >25% of the
luminal area (v2)
III Cases with ‘transmural’ arteritis and/or arterial fibrinoid
change and necrosis of medial smooth muscle cells also with
lymphocytic inflammation (v3).
Chronic/sclerosing allograft nephropathy
Fibrosing changes in the allograft, with or without features of true
alloimmune injury to the graft. Histopathological findings
reveal “IFTA” interstitial fibrosis and tubular atrophy which is
graded mild, moderate and severe, usually with features of
glomerular injury or sclerosis.
Humoral rejection (B cell (Ab) mediated):
Allo-Ab may cause immune injury to the allograft kidney. The
diagnosis requires (1) renal transplant dysfunction, (2) presence
of circulating anti-donor Ab (donor specific Ab) and (3) C4d
detected by immunoperoxidase. Evidence of acute cellular with
occult humoral rejection is often identified with late AR
episodes.
Pancreas transplantation
Since the first performance of pancreatic transplantation (PTx) in
1966 the procedure has come of age. As of June 2003, the
International Pancreas Transplant Registry (www.iptr.umn.edu) had
recorded more than 19,600 PTx, out of which over 14,300 were
done in the USA. Most PTx are performed in patients with diabetic
nephropathy requiring kidney transplantation. These patients
already require chronic immunosuppression and a functioning
pancreas transplant provides the most efficacious method for
achieving a normal glucose and hemoglobin A1C. In this setting
there are two options:
SPK - simultaneous pancreas and kidney transplantation
where one deceased donor provides kidney and pancreas or
PAK - pancreas after a previously performed kidney
transplant (PAK), usually after a LDRT.
Less common is pancreas transplant alone (PTA), performed in a
patient without diabetic nephropathy, where the trades off of
achieving normoglycemia with the possible complications of
chronic immunosuppression have to be weighed closely. Each year
in the U.S., approximately 900 SPK and 500 solitary pancreas
transplants are performed (compared with 16,000 kidney Tx).
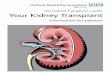
Currently the whole organ obtained from a cadaver donor is used.
The organ is placed in the pelvis opposite to the kidney transplant
and receives its blood supply through the iliac vessels with the
exocrine secretions drained into the small intestine or the bladder.
A newer surgical innovation has been portal venous drainage of the
pancreas allograft. The traditional systemic venous drainage
achieves euglycemia at the expense of hyperinsulinemia. Portal
venous drainage replicates the physiological state and due to the
first pass effect achieves euglycemia with normal insulin levels.

15
Patient survival at one year for 1999-2003 US cadaveric pancreas
transplants was at least 94% in all categories (SPK 95%; PAK 94%;
PTA 98%). After SPK, pancreas graft survival rate at one year for
1996-2000 was 84.7%; kidney graft survival was 92%. For solitary
pancreas transplants, pancreas graft survival at one year was 78.5%
for PAK and 78.2% for PTA.
Indications for pancreas transplantation
1. Presence of insulin-requiring diabetes mellitus*.
2. Ability to tolerate surgery and immunosuppression.
3. Adequate cardiopulmonary function.
4. Absence of organ system failure (other than kidney: creatinine
clearance < 30mL/min for SPK; for PAK > 40 mL/min.).
5. Emotional and psychosocial suitability.
6. Presence of 2 or more diabetic complications
Proliferative retinopathy
Nephropathy (hypertension, proteinuria, decreased GFR)
Peripheral or autonomic neuropathy
Microangiopathy
Accelerated atherosclerosis
Glucose hyperlability, hypoglycemia unawareness
* As a general rule, most candidates have absolute insulin deficiency as
determined by an undetectable c-peptide, rather than a component of
insulin resistance (Type II DM).
Absolute contraindications
1. Insufficient cardiovascular reserve (coronary angiography with
uncorrectable or untreatable CAD, or recent MI).
2. Active infection.
3. History of malignancy treated within the past 3 years (excluding
nonmelanoma skin cancer).
4. Positive HIV serology.
5. Positive hepatitis B surface antigen serology.
6. Active, untreated peptic ulcer disease.
7. Ongoing substance abuse (drug or alcohol).
8. Major ongoing untreated psychiatric illness.
9. Recent history of medical noncompliance.
10. Inability to provide informed consent.
11. Any systemic illness that would severely limit life expectancy or
compromise recovery.
12. Significant, irreversible hepatic or pulmonary dysfunction.
13. Positive lymphocytotoxic cross-match.
Relative contraindications
1. Age less that 18 or greater than 50 years.
2. Recent retinal hemorrhage.
3. Symptomatic cerebrovascular or peripheral vascular disease.
4. Absence of appropriate social support network.
5. Extreme obesity (greater that 150% ideal body weight).
6. Active smoking.
7. Severe, untreatable peripheral vascular (aorto-iliac) disease.
Risk factors
1. History of myocardial infarction, congestive heart failure, or
previous open heart surgery;
2. History of major amputation or peripheral bypass graft;
3. History of cerebrovascular event or carotid endarterectomy;
4. History of hypercoagulable syndrome.

16
Care for the Pancreas Transplant Recipient
POST-OP – Typical course through discharge
Immediate Postop Orders:
-Basic orders: NPO, IVF, SCD/TEDs, Foley, NGT, Clinical
Nutrition consult, OOB and ambulate > TID with help
starting POD 1, Physical therapy consult, case management,
may take meds with sips, clamp NGT for 1hr after meds
-Daily Labs: Chem 10, Amylase, Lipase, CBC w/Diff,
Tacrolimus level (if tacrolimus has been started)
-Radiology: First thing in the AM patient should have an
abdominal US and put in the comment that it should be the
pancreas transplant protocol. Must call ultrasound first
thing in the AM to make sure patient is scheduled first.
-Medications:
Fluconazole 100mg IV 1XD
Bactrim SS PO 1XD
Valcyte 900mg PO 1XD (Adjust based on GFR)
Tacrolimus PO 2XD (dose to be determined)
Myfortic or Cellcept IV 2XD (Ask re: dose)
Steroid taper as follows:
POD 1 – Methylprednisolone 70mg IV 2XD
POD 2 - Methylprednisolone 35mg IV 2XD
POD 3 - Methylprednisolone 17.5mg IV 2XD
POD 4 – Prednisone PO 15mg 2XD
POD 5 - Prednisone PO 25mg 1XD
POD 6 - Prednisone PO 20mg 1XD
POD 7 - Prednisone PO 10mg 1XD
Aspirin 81mg PO
Heparin 5000 units SQ 3XD
Zofran PRN
Scopolamine patch PRN
PCA for pain
Home beta blocker and statin meds
POD#2:
-Induction with Thymoglobulin (1-2mg/kg) dose.
Premedicate 30 -60 min before with solumedrol, Tylenol
650mg PR, and 50mg IV Benadryl. Run Thymo over 6 hrs.
-DC arterial line.
POD#3:
-Flag to 4A/4AE if clinically appropriate
POD#4:
-Induction with Thymoglobulin (see POD#2)
POD#5-7:
-DC home with services
**Refer to the pancreas transplant manual on the Lifespan intranet
for a more detailed description of the procedure and protocols.

17
GAME PLAN FOR HEMODIALYSIS ACCESS
Renal replacement therapy
Hemodialysis (HD): Catheter, fistula or graft (PTFE)
Peritoneal dialysis (CAPD)
Renal transplantation (Cadaver or Live Donor)
CAPD (developed in the 1970‟s) is available to individuals with the
direction and ability (physical and emotional) to perform dialysis at
home. Most patients prefer HD. Less than 10% opt for CAPD in RI
Evaluation for hemodialysis access includes:
Pulse – Bilateral brachial artery and radial artery pulses
Suitable vein
Superficial – cephalic or basilic
Deep – basilic vein in upper arm
Two questions must be answered before access surgery:
1. Is the patient medically stable for surgery?
No CHF, chest pain, K+ > 6.5, sepsis, etc.
2. What access operation should be done?
Wrist fistula, BCF, Basilic vein fistula (TPBVF), leg loop,
AV graft, PermCath or consider peritoneal dialysis.
Access considerations
Prefer non-dominant arm in case of paresthesia or steal.
Ask the RN to place a “red band” on the arm indicating “No IV
placement or blood draws”.
Transposed basilic vein fistula if no superficial vein noted on
exam.
Ultrasound or venogram multiple prior access procedures or
evidence of central stenosis (arm swelling, collateral veins,
etc.).
Graft (6-mm PTFE or Bovine carotid artery) considered if
dialysis required in fewer than 6 weeks, no reasonable vein, or
patient with limited life expectancy. (NEJM 2009; 360:2191).
OPTIONS:
Fistula: RCF, BCF below the antecubital fossa, BCF above
the elbow, TPBVF (transposed basilic vein fistula).
Graft: Forearm loop, upper arm, subclavian artery, femoral.
Catheter: highest likelihood of sepsis, clotting, inadequate
flow.
Uncommon (last resort) options:
Translumbar or transhepatic catheter
HERO: hybrid AVG-central catheter.
Work-up: CBC, Chem 7, EKG OR. Dialysis access is an
“urgent” surgery; only acute medical issues (CHF, hyperkalemia >
6.5, active angina, new arrhythmia, active bleeding, etc.) require
investigation or treatment prior to surgery.
Note:
Patients on routine dialysis should have a recent K+.
Patients with dialysis access problems (poor flow, incomplete
dialysis treatment prior to surgery); those with a history of high K+
or patients not yet on dialysis should have the K+ checked on the
day of surgery.
Cardiac pacers: when possible document the type, make and
model of the pacer. This information is useful for re-programming
after surgery. Consider placing access on the opposite side of the
pacer as SCV stenosis is fairly common 2* to pacing wires.