Embed Size (px)
Citation preview

Kathleen Reynolds, LMSW, ACSWVice President for Health Integration and Wellness
Health Care Reform: Opportunities and Challenges for
Behavioral Health Safety Net Providers

www.TheNationalCouncil.org
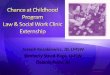
History of Funding for Mental Health and Substance Abuse Services
# o
f P
eo
ple
Se
rve
d
(mil
lio
ns)
Federal/State Funding
(billions)
Current State of Federal Funding and Persons Served
(2007 OMB)
Community Mental Health
Community Primary Care
2
4
6
8
.5 1 1.5 2

www.TheNationalCouncil.org
What Created the U Turn?
> The Impact of Block Grants on Mental Health and Substance Abuse FundingDuring Regan Administration funding went to block
grants to the statesGood at the time Little if any increase to mental health or substance
abuse block grants since

www.TheNationalCouncil.org
Movement to Medicaid as a Source of Funding for Mental Health
> Substance abuse not included> Created entitlement to services for some who
are Medicaid eligible> Less funding for persons without Medicaid

www.TheNationalCouncil.org
ARRA and Health Care Act Funding
> Bureau or Primary Health Care ARRA Funding = $2 Billion +
> SAMHSA – Did not ask for any> Bureau of Primary Health Care Patient
Protection and Affordable Health Act = $11 Billion +
> SAMHSA - $50 Million

www.TheNationalCouncil.org
Patient Protection and Affordable Health Care Act
> Medicaid Expansion> Parity> Accountable Care Organizations> Medicaid/Medicare Medical Home Pilots

www.TheNationalCouncil.org
Accountable Care Organizations
An ACO would have at least one hospital, a minimum of 50 physicians (primary care and specialists), commit to be in business for at least 3-5 years, and serve at least 5,000 patients. If the ACO met pre-established quality goals, it would receive an incentive payment. Penalties would be assessed if care did not meet the established quality goals. Incentive payments and penalties would be split between the members of the ACO. The providers in the ACO would follow best practices, be patient-centered and contribute to the development of best clinical practices to build standards of evidenced-based medicine

www.TheNationalCouncil.org
Behavioral Health Role in an ACO> Opportunity to define the role of behavioral
health in the system• Specialty mental health only • Specialty mental health + physical health• Mental health for all• Other?
> Expand role of mental health substance abuse role in primary care
> Reduce stigma and increase access

www.TheNationalCouncil.org
Behavioral Health Role in ACO
> Challenge to determine who will be the ACO in your area
> Challenge to establish your position in the system if not already there
> Important role for advocacy in the process

www.TheNationalCouncil.org
Medicaid/Medicare Medical Home Pilots
> The Medicaid Medical Home pilots allow states to enroll Medicaid beneficiaries with chronic conditions in medical home pilot projects as early as January 2011. This includes individuals with serious and persistent mental illnesses. Up to $25 million is available for states to plan and implement these projects.
> Beginning in January 2012 Medicare can establish a pilot program that includes community health teams to increase access to comprehensive, community-based, coordinated care.

www.TheNationalCouncil.org
Medical Home Definition
> While definitions of medical homes vary, the most widely accepted definition, supported by the American Academy of Family Physicians, American Academy of Pediatrics, American College of Physicians and the American Osteopathic Association, includes the following principles;
• Personal physician• Physician directed medical practice (team care that collectively takes responsibility
for the ongoing care of patients)• Whole person orientation• Care that is coordinated and/or integrated• Quality and safety (including evidence based care, use of information technology
and performance measurement/quality improvement)• Enhanced access to care• Payment structure that reflects these characteristics beyond the current
encounter-based reimbursement mechanisms (http://www.pcpcc.net/)

www.TheNationalCouncil.org
Medical Homes & Behavioral Health - Opportunities
> Need to insure that “medical” home includes mental health and substance abuse services
> Get services to more people, earlier> Reduce stigma> As part of health care, reduce “stepchild”
phenomena> Improve access to primary care

www.TheNationalCouncil.org
Medical Homes & Behavioral Health - Challenges
> Insure that psycho-social treatment, case management and other key services get integrated into the model
> Insure that those with the most severe issues do not get lost in the system
> Where will the volume of new eligibles go?

www.TheNationalCouncil.org
Integration as Part of the Strategy> Integration does not mean return to a medical
model> Provides access to multiple services at one
time and place> Improves the quality of all services> Creates space within the current public sector
for more consumers> Ultimately reduce the early loss of life for
those with a serious and persistent mental illness

MH/Primary Care Integration Options
Function
Minimal
Collaboration
Basic Collaboration
from a Distance
Basic Collaboration On-
Site
Close Collaboration/
Partly Integrated
Fully Integrated/Merged THE CONSUMER and STAFF PERSPECTIVE/EXPERIENCE
Access Two front doors; consumers go to separate sites and organizations for services
Two front doors; cross system conversations on individual cases with signed releases of information
Separate reception, but accessible at same site; easier collaboration at time of service
Same reception; some joint service provided with two providers with some overlap
One reception area where appointments are scheduled; usually one health record, one visit to address all needs; integrated provider model
Services Separate and distinct services and treatment plans; two physicians prescribing
Separate and distinct services with occasional sharing of treatment plans for Q4 consumers
Two physicians prescribing with consultation; two treatment plans but routine sharing on individual plans, probably in all quadrants;
Q1 and Q3 one physician prescribing, with consultation; Q2 & 4 two physicians prescribing some treatment plan integration, but not consistently with all consumers
One treatment plan with all consumers, one site for all services; ongoing consultation and involvement in services; one physician prescribing for Q1, 2, 3, and some 4; two physicians for some Q4: one set of lab work
Funding Separate systems and funding sources, no sharing of resources
Separate funding systems; both may contribute to one project
Separate funding, but sharing of some on-site expenses
Separate funding with shared on-site expenses, shared staffing costs and infrastructure
Integrated funding, with resources shared across needs; maximization of billing and support staff; potential new flexibility
Governance Separate systems with little of no collaboration; consumer is left to navigate the chasm
Two governing Boards; line staff work together on individual cases
Two governing Boards with Executive Director collaboration on services for groups of consumers, probably Q4
Two governing Boards that meet together periodically to discuss mutual issues
One Board with equal representation from each partner
EBP Individual EBP’s implemented in each system;
Two providers, some sharing of information but responsibility for care cited in one clinic or the other
Some sharing of EBP’s around high utilizers (Q4) ; some sharing of knowledge across disciplines
Sharing of EBP’s across systems; joint monitoring of health conditions for more quadrants
EBP’s like PHQ9; IDDT, diabetes management; cardiac care provider across populations in all quadrants
Data Separate systems, often paper based, little if any sharing of data
Separate data sets, some discussion with each other of what data shares
Separate data sets; some collaboration on individual cases
Separate data sets, some collaboration around some individual cases; maybe some aggregate data sharing on population groups
Fully integrated, (electronic) health record with information available to all practitioners on need to know basis; data collection from one source

www.TheNationalCouncil.org
New York SAMHSA Grantees Initiatives> Vocational Instruction Project Community
Service> Fordham Tremont Mental Health Center/Bronx
Lebanon Hospital Center; Post Graduate Center for Mental Health
> Other Initiatives?

www.TheNationalCouncil.org
National Training and Technical Assistance Center for PCBHI
> Awarded to the National Council for Community Behavioral HealthCare
> Four years; $5.3 Million/year> Target Audience
• SAMHSA Grantees• HRSA Grantees• General Public
> Services• Training and Technical Assistance• Knowledge Development• Prevention and Wellness• Workforce Development• Health Reform Monitoring and Updates

Questions?