Embed Size (px)
Citation preview
151Journal of Cytology / July 2013 / Volume 30 / Issue 3
Ranajoy Ghosh, saumya R. mallik, sandeep R. mathuR, VenkateswaRan k. iyeR
Department of Pathology, All India Institute of Medical Sciences, New Delhi, India
Address for correspondence: Dr. Sandeep R Mathur, Department of Pathology, 1st Floor Teaching Block, All India Institute of Medical Sciences, New Delhi, India. E-mail: [email protected]
ABSTRACTBackground: Solid pseudopapillary tumor of pancreas (SPTP) is a rare pancreatic tumor of uncertain histogenesis usually affecting young women. Though these tumors have characteristic cytomorphology, it is sometimes difficult to differentiate them from neuroendocrine tumors of the pancreas. We reviewed cases of SPTP to delineate the diagnostic cytological features and also observed utility of CD 99 (MIC 2) immunostaining to aid in the diagnosis of this tumor.
Aims: This study was designed to demonstrate the utility of CD 99 immunostaining along with cytological features for making a pre-operative diagnosis and delineating it from the neuroendocrine tumor of pancreas which is a close mimic.
Materials and Methods: Cytomorphological features of 11 cases of solid pseudopapillary neoplasm diagnosed by pre-operative fine-needle aspiration cytology (FNAC) at our institute were reviewed. Immunocytochemistry for CD 99 was also performed on the smears.
Results: All the cases had cellular smears with monomorphic cells lying singly, as loosely cohesive clusters as well as forming delicate pseudopapillae. Presence of intra and extra-cellular basement membrane material, background foamy macrophages and nuclear grooves were the other salient features. Immunocytochemistry for CD 99 could be performed on eight cases and demonstrated typical paranuclear dot-like positivity.
Conclusions: Pre-operative early diagnosis of SPTP can be made by FNAC which can further be aided by CD 99 immunocytochemistry.
Key words: CD 99; immunohistochemistry; solid pseudopapillary tumor of pancreas.
Introduction
Solid pseudopapillary tumor of the pancreas (SPTP) is a rare neoplasm of unknown histogenesis and low malignant potential first reported by Frantz in 1959.[1] The tumor was known by various names like “solid and cystic tumor”, “solid cystic and papillary epithelial neoplasm”, and “solid and papillary tumor” before the present consensus name solid pseudopapillary tumor of pancreas (SPTP).[2] SPTP is more
common in young females although cases in males are also reported in the literature.[3] Early pre-operative diagnosis is of paramount importance as adequate resection is usually curative.[4] SPT constitutes approximately 3% of the cystic lesions of pancreas[5] and about 60 cases diagnosed by fine-needle aspiration cytology (FNAC) are reported in the literature.[6] The cytomorphology of this tumor is highly characteristic, with features that are distinctive from those of other cystic and solid tumors of the pancreas. However, monomorphic population of discohesive cells and eccentric nuclei sometimes makes it difficult to differentiate from some other pancreatic tumors like the neuroendocrine tumors. It is very important to distinguish this tumor from other pancreatic tumors as these may have similar clinical presentation and radiologic appearance but with different prognosis and treatment. Immunohistochemically these tumors are usually positive for vimentin and α-1 antitrypsins[7] but no specific immunocytochemical markers
CD 99 immunocytochemistry in solid pseudopapillary tumor of pancreas: A study on fine-needle aspiration cytology smears
Access this article online
Website:
www.jcytol.org
Quick Response Code
DOI:
10.4103/0970-9371.117645
Original Article
[Downloaded free from http://www.jcytol.org on Wednesday, October 16, 2013, IP: 36.74.61.1] || Click here to download free Android application for this journal
152
Ghosh, et al.: CD 99 immunocytochemistry in solid pseudopapillary tumor of pancreas
Journal of Cytology / July 2013 / Volume 30 / Issue 3
are present which could be used to distinguish it from other pancreatic tumors. Some other markers like CD56, neurone-specific enolase, progesterone receptor and CD10 may be immunopositive in SPTP[8] but may also be positive in various other tumors.[9]
Here we have studied detailed cytomorphological features of 11 cases of SPTP for accurate pre-operative diagnosis along with use of immunocytochemical marker CD 99 as a specific marker for SPTP with a unique staining pattern.
Materials and Methods
Eleven cases of SPTPs with pre-operative cytological diagnosis were retrieved from the archives of the cytopathology laboratory of our institute. FNAC was done with 23G needle under ultrasound guidance and in one case EUS-guided aspirate was done. Toluidine blue stain was done for specimen adequacy assessment and preliminary diagnostic interpretation on site. Smears were fixed in 95% alcohol for Papanicolaou stain and air dried for May–Grünwald–Giemsa staining. Detailed cytomorphological evaluation was performed in each case. Alcohol-fixed slides were also used for immunocytochemistry. In five cases, spare alcohol-stained slides were available and immunocytochemistry was done on them. In three cases, a Papanicolaou-stained slide was destained by dipping in xylene for 2-3 h followed by immersing in methanol for 15 minutes. Immunohistochemical staining was done with monoclonal antibody against CD 99 (Dako, Mouse antihuman antibody clone 12E7) using a routine streptavidin-biotin horseradish peroxidase detection system with diaminobenzidine (DAB) as chromogen.
Results
During the period of 2005-2012, 11 patients of SPTP presented to our institute, with age ranging from 13 to 40 years. Only one of the patients was male and rest were all females. The clinical and radiological features of these patients are summarized in Table 1.
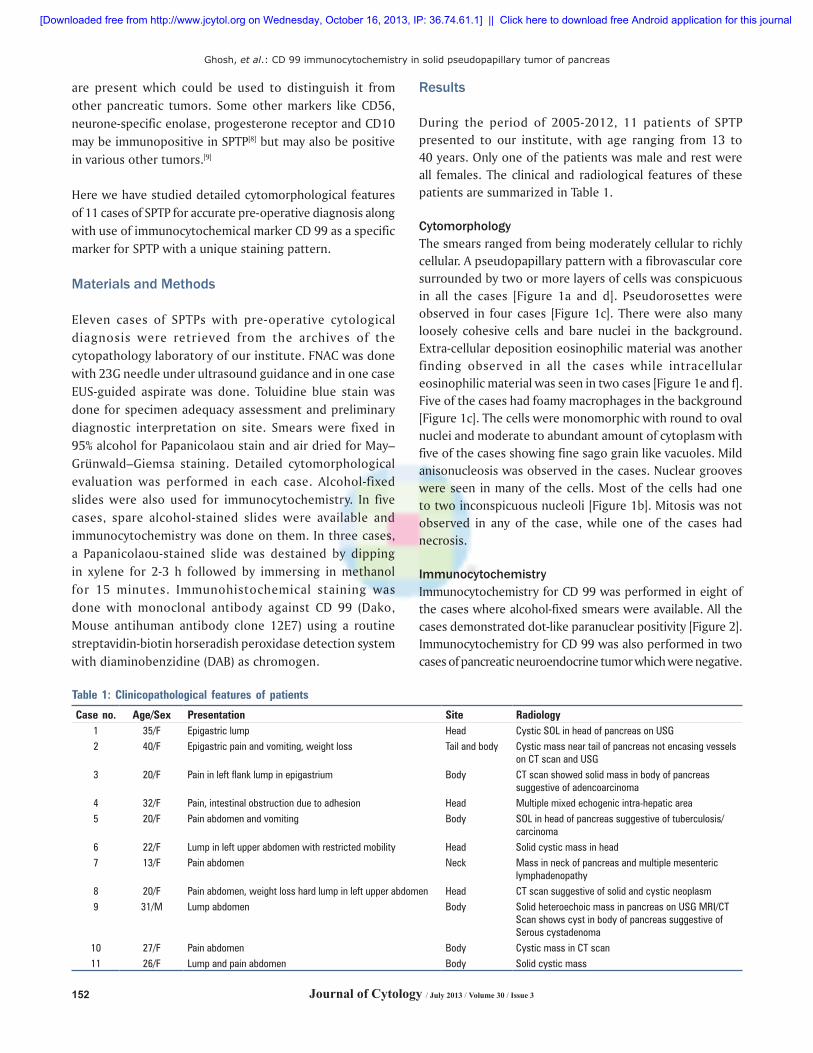
CytomorphologyThe smears ranged from being moderately cellular to richly cellular. A pseudopapillary pattern with a fibrovascular core surrounded by two or more layers of cells was conspicuous in all the cases [Figure 1a and d]. Pseudorosettes were observed in four cases [Figure 1c]. There were also many loosely cohesive cells and bare nuclei in the background. Extra-cellular deposition eosinophilic material was another finding observed in all the cases while intracellular eosinophilic material was seen in two cases [Figure 1e and f]. Five of the cases had foamy macrophages in the background [Figure 1c]. The cells were monomorphic with round to oval nuclei and moderate to abundant amount of cytoplasm with five of the cases showing fine sago grain like vacuoles. Mild anisonucleosis was observed in the cases. Nuclear grooves were seen in many of the cells. Most of the cells had one to two inconspicuous nucleoli [Figure 1b]. Mitosis was not observed in any of the case, while one of the cases had necrosis.
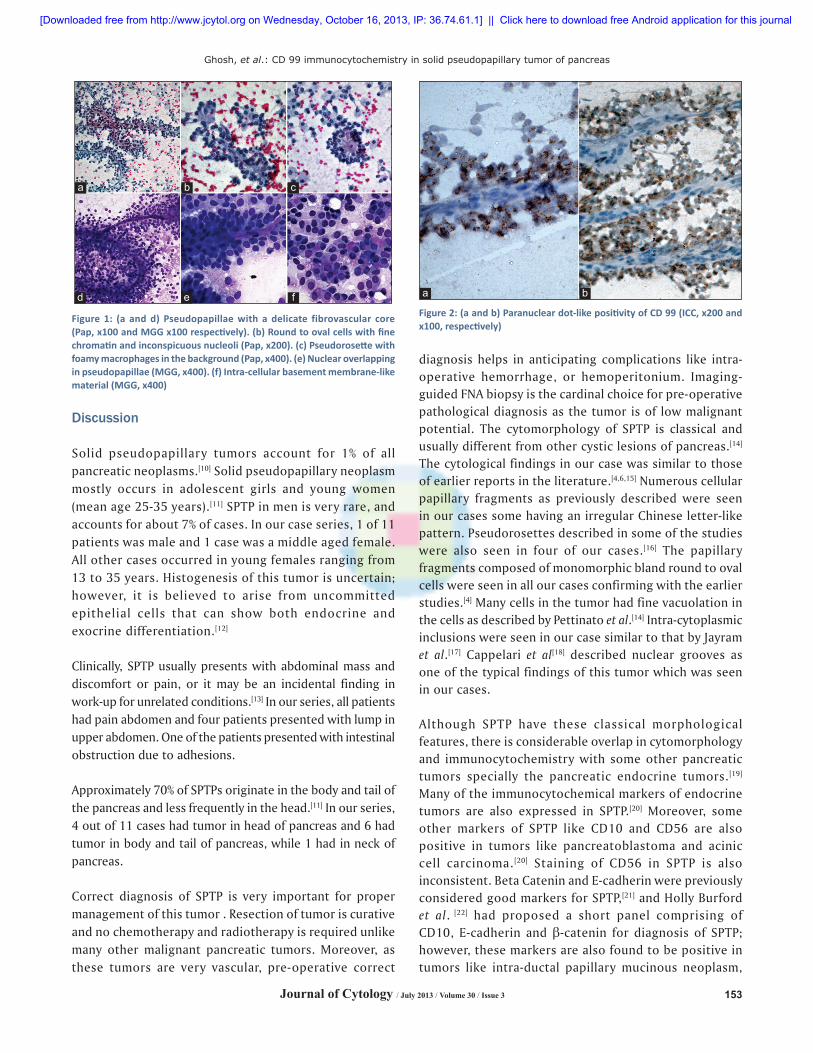
ImmunocytochemistryImmunocytochemistry for CD 99 was performed in eight of the cases where alcohol-fixed smears were available. All the cases demonstrated dot-like paranuclear positivity [Figure 2]. Immunocytochemistry for CD 99 was also performed in two cases of pancreatic neuroendocrine tumor which were negative.
Table 1: Clinicopathological features of patients
Case no. Age/Sex Presentation Site Radiology1 35/F Epigastric lump Head Cystic SOL in head of pancreas on USG2 40/F Epigastric pain and vomiting, weight loss Tail and body Cystic mass near tail of pancreas not encasing vessels
on CT scan and USG3 20/F Pain in left flank lump in epigastrium Body CT scan showed solid mass in body of pancreas
suggestive of adencoarcinoma4 32/F Pain, intestinal obstruction due to adhesion Head Multiple mixed echogenic intra-hepatic area5 20/F Pain abdomen and vomiting Body SOL in head of pancreas suggestive of tuberculosis/
carcinoma6 22/F Lump in left upper abdomen with restricted mobility Head Solid cystic mass in head7 13/F Pain abdomen Neck Mass in neck of pancreas and multiple mesenteric
lymphadenopathy8 20/F Pain abdomen, weight loss hard lump in left upper abdomen Head CT scan suggestive of solid and cystic neoplasm9 31/M Lump abdomen Body Solid heteroechoic mass in pancreas on USG MRI/CT
Scan shows cyst in body of pancreas suggestive of Serous cystadenoma
10 27/F Pain abdomen Body Cystic mass in CT scan11 26/F Lump and pain abdomen Body Solid cystic mass
[Downloaded free from http://www.jcytol.org on Wednesday, October 16, 2013, IP: 36.74.61.1] || Click here to download free Android application for this journal
153
Ghosh, et al.: CD 99 immunocytochemistry in solid pseudopapillary tumor of pancreas
Journal of Cytology / July 2013 / Volume 30 / Issue 3
Discussion
Solid pseudopapillary tumors account for 1% of all pancreatic neoplasms.[10] Solid pseudopapillary neoplasm mostly occurs in adolescent girls and young women (mean age 25-35 years).[11] SPTP in men is very rare, and accounts for about 7% of cases. In our case series, 1 of 11 patients was male and 1 case was a middle aged female. All other cases occurred in young females ranging from 13 to 35 years. Histogenesis of this tumor is uncertain; however, it is believed to arise from uncommitted epithelial cells that can show both endocrine and exocrine differentiation.[12]
Clinically, SPTP usually presents with abdominal mass and discomfort or pain, or it may be an incidental finding in work-up for unrelated conditions.[13] In our series, all patients had pain abdomen and four patients presented with lump in upper abdomen. One of the patients presented with intestinal obstruction due to adhesions.
Approximately 70% of SPTPs originate in the body and tail of the pancreas and less frequently in the head.[11] In our series, 4 out of 11 cases had tumor in head of pancreas and 6 had tumor in body and tail of pancreas, while 1 had in neck of pancreas.
Correct diagnosis of SPTP is very important for proper management of this tumor . Resection of tumor is curative and no chemotherapy and radiotherapy is required unlike many other malignant pancreatic tumors. Moreover, as these tumors are very vascular, pre-operative correct
diagnosis helps in anticipating complications like intra-operative hemorrhage, or hemoperitonium. Imaging-guided FNA biopsy is the cardinal choice for pre-operative pathological diagnosis as the tumor is of low malignant potential. The cytomorphology of SPTP is classical and usually different from other cystic lesions of pancreas.[14] The cytological findings in our case was similar to those of earlier reports in the literature.[4,6,15] Numerous cellular papillary fragments as previously described were seen in our cases some having an irregular Chinese letter-like pattern. Pseudorosettes described in some of the studies were also seen in four of our cases.[16] The papillary fragments composed of monomorphic bland round to oval cells were seen in all our cases confirming with the earlier studies.[4] Many cells in the tumor had fine vacuolation in the cells as described by Pettinato et al.[14] Intra-cytoplasmic inclusions were seen in our case similar to that by Jayram et al.[17] Cappelari et al[18] described nuclear grooves as one of the typical findings of this tumor which was seen in our cases.
Although SPTP have these classical morphological features, there is considerable overlap in cytomorphology and immunocytochemistry with some other pancreatic tumors specially the pancreatic endocrine tumors.[19] Many of the immunocytochemical markers of endocrine tumors are also expressed in SPTP.[20] Moreover, some other markers of SPTP like CD10 and CD56 are also positive in tumors like pancreatoblastoma and acinic cell carcinoma.[20] Staining of CD56 in SPTP is also inconsistent. Beta Catenin and E-cadherin were previously considered good markers for SPTP,[21] and Holly Burford et al. [22] had proposed a short panel comprising of CD10, E-cadherin and β-catenin for diagnosis of SPTP; however, these markers are also found to be positive in tumors like intra-ductal papillary mucinous neoplasm,
Figure 1: (a and d) Pseudopapillae with a delicate fibrovascular core (Pap, x100 and MGG x100 respectively). (b) Round to oval cells with fine chromatin and inconspicuous nucleoli (Pap, x200). (c) Pseudorosette with foamy macrophages in the background (Pap, x400). (e) Nuclear overlapping in pseudopapillae (MGG, x400). (f) Intra-cellular basement membrane-like material (MGG, x400)
a b c
fedFigure 2: (a and b) Paranuclear dot-like positivity of CD 99 (ICC, x200 and x100, respectively)
a b
[Downloaded free from http://www.jcytol.org on Wednesday, October 16, 2013, IP: 36.74.61.1] || Click here to download free Android application for this journal

154
Ghosh, et al.: CD 99 immunocytochemistry in solid pseudopapillary tumor of pancreas
Journal of Cytology / July 2013 / Volume 30 / Issue 3
pancreatoblatoma and acinic cell carcinoma.[23-25] To rule out the other morphologic mimics of SPTPs, a relatively specific and consistent marker which is expressed on FNA smears should be used.
CD 99 immunoreactivity in SPTP has been reported recently in two studies on histopathology sections. CD 99 was demonstrated to have a characteristic paranuclear dot-like positivity in these studies.[26,27] They reported that this positivity pattern was quite classical of SPTP among the different pancreatic tumors as it was negative in pancreatoblastoma, adenocarcinoma and acinic cell carcinoma. In pancreatic endocrine tumors, it was either negative or had a membranous pattern of positivity.[28] Similar to our study, the studies on tissue sections had 100% of the SPTP positive for CD 99 [Table 2]. There has been no published study which has evaluated utility of CD 99 on FNA smears. In our series, CD 99 staining in cytology smears also demonstrated a similar result with paranuclear dot-like positivity in the eight SPTP cases while negative in two endocrine tumors. Though, in this study we performed immunocytochemistry in Papanicolaou-stained slide by de-staining. The cell block is ideal as it gives better cellularity and allows performance of more tests in the same sample. A major limitation of this study is the number of cases especially only two neuroendocrine tumors were included in the study for comparison. Immunocytochemistry on larger number of cases may have been better and helped to establish predictive values, our study is thus mainly a descriptive study of this unique immunocytochemical property.
SPTP is a tumor of low malignant potential where early diagnosis and resection is curative. This is the first study to demonstrate the paranuclear dot-like expression of CD 99 on FNA smears. This may help especially to differentiate from the other close cytological differential diagnosis like pancreatic endocrine tumors. CD 99 immunocytochemistry thus may be used as a good adjunct to cytomorphology for diagnosis of SPTP where there is an overlap with other entities on imaging and morphology. The pathophysiology for this unique staining pattern however is still to be established.
References
1. Frantz VK. Tumors of the pancreas. In: Atlas of tumor pathology, 1st series. Washington, DC, USA: US Armed Forces Institute of Pathology; 1959. p. 32-3.
2. Adamthwaite JA, Verbeke CS, Stringer MD, Guillou PJ, Menon KV. Solid pseudopapillary tumor of the pancreas: Diverse presentation, outcome and histology. J Pancreas 2006;7:635-42.
3. Mohan H, Bal A, Punia RP, Attri AK. Solid and cystic papillary epithelial neoplasm of the pancreas. J Postgrad Med 2006;52:141-2.
4. Naresh KN, Borges AM, Chinoy RF, Soman CS, Krishnamurthy SC. Solid and Papillary epithelial neoplasm of the pancreas. Diagnosis by fine needle aspiration cytology in four cases. Acta Cytol 1995;39:489-93.
5. Solcia E, Capella C, Kloppel G. Tumors of the pancreas. Atlas of Tumor Pathology, third series, Fascicle 20, Washington D.C. Armed Forces Institute of Pathology, 1995.Rosai J, Sobin LH, editors.
6. Bardales RH, Centeno B, Mallery JS, Lai R, Pochapin M, Guiter G, et al. Endoscopic ultrasound-guided fine-needle aspiration cytology diagnosis of solid-pseudopapillary tumor of pancreas : A rare neoplasm of elusive origin but characteristic cytomorphology features. Am J Clin Pathol 2004;121:654-62.
7. Pelosi G, Iannucci A, Zamboni G, Bresaola E, Iacono C, Serio G. Solid and cystic papillary neoplasm of the pancreas: A clinico-cytopathologic and immunocytochemical study of five new cases diagnosed by fine-needle aspiration cytology and a review of the literature. Diagn Cytopathol 1995;13:233-46.
8. Yu PF, Hu ZH, Wang XB, Guo JM, Cheng XD, Zhang YL, et al. Solid pseudopapillary tumor of the pancreas: A review of 553 cases in Chinese literature. World J Gastroenterol 2010;14:1209-14.
9. Klimstra DS. Nonductal neoplasms of the pancreas. Mod Pathol 2007;20:S94-112.
10. Salla C, Chatzipantelis P, Konstantinou P, Karoumpalis I, Pantazopoulou A, Dappola V. Endoscopic ultrasound-guided fine-needle aspiration cytology diagnosis of solid pseudopapillary tumor of the pancreas: A case report and literature review. World J Gastroenterol 2007;13:5158-63.
11. Kosmahl M, Pauser U, Peters K, Sipos B, Luttges J, Kremer B, et al. Cystic neoplasms of the pancreas and tumor-like lesions with cystic features: A review of 418 cases and a classification proposal. Virchows Arch 2004;445:168-78.
12. Mendelson G. Papillary cystic tumor of pancreas: An enigma. Am J Clin Pathol 1992;98:476-7.
13. Hamilton SR, Aaltonen LA, Editors. World Health Organization Classification of Tumors. Pathology and Genetics of Tumors of the Digestive System. Lyon: IARC Press; 2000. p. 246-8.
14. Pettinato G, Di Vizio D, Manivel JC, Pambuccian SE, Somma P, Insabatao L. Solid-pseudopapillary tumor of the pancreas: A neoplasm with highly distinct and characteristic cytological features. Diagn Cytopathol 2002;27:325-34.
15. Al-Kaisi N, Sieger EE. Fine Needle aspiration cytology of the pancreas. Acta Cytol 1989;33:145-52.
16. Mehta N, Modi L, Patel T, Shah M. Study of cytomorphology of solid pseudopapillary tumor of pancreas and its differential diagnosis. J Cytol 2010;27:118-22.
17. Jayram G, Chaturvedi KU, Jindal RK, Venugopal S, Kapoor R. Papillary cystic neoplasm of pancreas Report of a case diagnosed by fine needle aspiration cytology. Acta Cytol 1990;34:429-33.
18. Cappellari JO, Geisinger KR, Albertson DA, Wolfman NT, Kute TE. Malignant papillary cystic tumor of pancreas. Cancer 1990;66:193-8.
19. Liu BA, Li ZM, Su ZS, She XL. Pathological differential diagnosis of solid-pseudopapillary neoplasm and endocrine tumors of the pancreas. World J Gastroenterol 2010;16:1025-30.
20. Notohara K, Hamazaki S, Tsukayama C, Nakamoto S, Kawabata K, Mizobuchi K, et al. Solid-pseudopapillary tumor of the pancreas:
Table 2: Studies on CD 99 staining in SPTP
Number of SPTPs
Number of cases positive for CD 99
Guo et al.[27] 62 62Li et al.[26] 37 37Present study 8 8
[Downloaded free from http://www.jcytol.org on Wednesday, October 16, 2013, IP: 36.74.61.1] || Click here to download free Android application for this journal
155
Ghosh, et al.: CD 99 immunocytochemistry in solid pseudopapillary tumor of pancreas
Journal of Cytology / July 2013 / Volume 30 / Issue 3
immunohistochemical localization of neuroendocrine markers and CD10. Am J Surg Pathol 2000;24:1361-71.
21. Abraham SC, Klimstra DS, Wilentz RE, Yeo CJ, Conlon K, Brennan M, et al. Solid-pseudopapillary tumors of the pancreas are genetically distinct from pancreatic ductal adenocarcinomas and almost always harbor beta-catenin mutations. Am J Pathol 2002;160:1361-9.
22. Burford H, Baloch Z, Liu X, Jhala D, Siegal GP, Jhala N. E-cadherin/beta-catenin and CD10: A limited immunohistochemical panel to distinguish pancreatic endocrine neoplasm from solid pseudopapillary neoplasm of the pancreas on endoscopic ultrasound-guided fine-needle aspirates of the pancreas. Am J Clin Pathol 2009;132:831-9.
23. Chetty R, Serra S, Salahshor S, Alsaad k, Shih W, Blaszyk H, et al. Expression of Wnt-signaling pathway proteins in intraductal papillary mucinous neoplasms of the pancreas: A tissue microarray analysis. Hum Pathol 2006;37:212-7.
24. Abraham SC, Wu TT, Klimstra DS, Finn LS, Lee JH, Yeo CJ, et al. Distinctive molecular genetic alterations in sporadic and familial adenomatouss polyposisassociated pancreatoblastomas: Frequent alterations in the APC/ beta-catenin pathway and chromosome 11p. Am J Pathol 2001;159:1619-27.
25. Abraham SC, Wu TT, Hruban RH, Lee JH, Yeo CJ, Conlon K, et al. Genetic and immunohistochemical analysis of pancreatic acinar cell carcinoma: frequent allelic loss on chromosome 11p and alterations in the APC/beta-catenin pathway. Am J Pathol 2002;160:953-62.
26. Li L, Li J, Hao C, Zhang C, Mu K, Wang Y, et al. Immunohistochemical evaluation of solid pseudopapillary tumors of the pancreas: The expression pattern of CD99 is highly unique. Cancer Lett 2011;310:9-14.
27. Guo Y, Yuan F, Deng H, Wang HF, Jin XL, Xiao JC. Paranuclear dot-like immunostaining for CD99: A unique staining pattern for diagnosing solid-pseudopapillary neoplasm of the pancreas. Am J Surg Pathol 2011;35:799-806.
28. Goto A, Niki T, Terado Y, Fukushima J, Fukayama M Prevalence of CD99 protein expression in pancreatic endocrine tumors (PETs). Histopathology 2004;45:384-92.
How to cite this article: Ghosh R, Mallik SR, Mathur SR, Iyer VK. CD 99 immunocytochemistry in solid pseudopapillary tumor of pancreas: A study on fine-needle aspiration cytology smears. J Cytol 2013;30:151-5.
Source of Support: Nil, Conflict of Interest: None declared.
Author Help: Online submission of the manuscripts
Articles can be submitted online from http://www.journalonweb.com. For online submission, the articles should be prepared in two files (first page file and article file). Images should be submitted separately.
1) First Page File: Prepare the title page, covering letter, acknowledgement etc. using a word processor program. All information related to your identity
should be included here. Use text/rtf/doc/pdf files. Do not zip the files.2) Article File: The main text of the article, beginning with the Abstract to References (including tables) should be in this file. Do not include any information
(such as acknowledgement, your names in page headers etc.) in this file. Use text/rtf/doc/pdf files. Do not zip the files. Limit the file size to 1 MB. Do not incorporate images in the file. If file size is large, graphs can be submitted separately as images, without their being incorporated in the article file. This will reduce the size of the file.
3) Images: Submit good quality color images. Each image should be less than 4 MB in size. The size of the image can be reduced by decreasing the
actual height and width of the images (keep up to about 6 inches and up to about 1800 x 1200 pixels). JPEG is the most suitable file format. The image quality should be good enough to judge the scientific value of the image. For the purpose of printing, always retain a good quality, high resolution image. This high resolution image should be sent to the editorial office at the time of sending a revised article.
4) Legends: Legends for the figures/images should be included at the end of the article file.
[Downloaded free from http://www.jcytol.org on Wednesday, October 16, 2013, IP: 36.74.61.1] || Click here to download free Android application for this journal




![[PPT]SCREENING · Web viewRontgen, Sitologi, Tekanan darah - Usaha identifikasi pada seseorang terhadap kemungkinan adanya penyakit / faktor resiko dengan menggunakan pemeriksaan,](https://img.dokumen.tips/doc/110x75/5ae6ea677f8b9a87048e9227/pptscreening-viewrontgen-sitologi-tekanan-darah-usaha-identifikasi-pada-seseorang.jpg)