Embed Size (px)
Citation preview


Journal of Translational Medicine and Research
an official journal of the International Association of Surgeons and Gastroenterologists and Oncologists
and of the Romanian Academy of Medical Sciences
Editor-in-Chief Honorary Editors-in-ChiefFounding Editor Masatoshi Makuuchi, Tokyo, Japan
Irinel Popescu, Bucharest Yupei Zhao, China
Founding Editor George A. Calin, Houston, USA
Associate Editors
Tudorel Ciurea, Craiova Vlad Herlea, Bucharest
Radu Deac, Tg. Mures Laurenţiu Micu, Bucharest
Simona Olimpia Dima, Bucharest Carol Stanciu, Iasi
Dan G. Duda, Boston, MA Margit Șerban, Timisoara
Traian Dumitrașcu, Bucharest Kyoichi Takaori, Kyoto, Japan
Carlos Fernandez-del Castillo, Boston, MA Bin Tean Teh, Singapore
Mircea Grigorescu, Cluj Napoca Guido Torzilli, Milan, Italy
Ho-Seong Han, Seoul, Korea Yogesh Vashist, Hamburg, Germany
Andrew X. Zhu, Boston, MA
Editorial Board
Eduard Apetrei, Bucharest Nicolae Ghilezan, Cluj Napoca
Aurel Ardeleanu, Arad Carmen Ginghină, Bucharest
Constantin Arion, Bucharest Anca Grosu, Freiburg, Germany
Nicolae Bacalbașa, Bucharest Theodore S. Hong, Boston, MA
Nabeel Bardeesy, Boston, MA Prodromos Hytiroglou, Thessaloníki, Greece
Hans G. Beger, Ulm, Germany Mircea Ifrim, Bucharest
Gheorghe Benga, Cluj Napoca Vlad Iliescu, Bucharest
Hans Bonnier, Belgium Mihai Ionac, Timisoara
Liliana G. Bordeianou, Boston, MA Constantin Ionescu Târgoviște, Bucharest
Șerban Bubenek, Bucharest Eunice L. Kwak, Boston, MA
Vasile Cândea, Bucharest Mercedes S. Mandell, Aurora, Colorado, USA
Ana Câmpeanu, Bucharest Peter Manu, New York, USA
Mircea Cinteză, Bucharest Naoto Matsuno, Tokyo, Japan
Journal of Translational Medicine and Research, 21 (3), 2016 163

164 Journal of Translational Medicine and Research, 21 (3), 2016
Adrian Covic, Iasi Petru Matusz, Timisoara
Dan Coliţă, Bucharest John T. Mullen, Boston, MA
Sorin Comoroșan, Bucharest Carmen Orban, Bucharest
Daniel Constantinescu, Philadelphia, USA Virgil Păunescu, Bucharest
Ileana Constantinescu, Bucharest Liliana Pâslaru, Bucharest
Daniel Coriu, Bucharest Markus Peck-Radosavljevic, Vienna, Austria
Hiroyuki Daida, Juntendo, Japan Ioan Pop D. Popa, Bucharest
Leon Dănăilă, Bucharest Vlad Ratziu, Paris, France
Mircea Diculescu, Bucharest Dan Sabău, Sibiu
Maria Dorobanţu, Bucharest Bernhard Stamm, Aarau, Switzerland
Gabriela Droc, Bucharest Andrei Stieber, Atlanta, USA
Cristina R. Ferrone, Boston, MA Adrian Streinu Cercel, Bucharest
Daniela Filipescu, Bucharest Alina Tãnase, Bucharest
Cristian Gheorghe, Bucharest Dana Tomescu, Bucharest
Liana Gheorghe, Bucharest Dragos Vinereanu, Bucharest
Gregory Y. Lauwers, Boston, MA Victor Voicu, Bucharest
Thomas CC Yau, Hong Kong
Journal of Translational Medicine and Research is atested and indexed
in Elsevier Bibliographic Databases: SCOPUS
CrossRef (DOI: 10.21614/jtmr)
Printed in Romania, Celsius Publishing House

Journal of Translational Medicine and Research, 21 (3), 2016 165
Journal of Translational Medicine and Research
No. 3 / Vol. 21 / 2016
CONTENTS
EDITORIAL
From the Editor in ChiefIrinel Popescu ................................................................................................................................................... 167
LEADING ARTICLE
Human Cancers: The Interplay Between Protein-Coding Genes and Non-Coding RNAs
George A. Calin ................................................................................................................................................... 168
REVIEW ARTICLE
Thrombotic Complications in Cirrhotic Patients: Balancing Risks and Benefits of Anticoagulation Treatment
Ecaterina Scãrlãtescu, Mercedes S. Mandell, Dana R. Tomescu ........................................................................ 173
ORIGINAL PAPERS
Functional Characterization of 1.1B4 - A Novel Human Insulin Releasing Cell Line and Effect of HDGP (High Density Green Photons) Irradiation on Beta Pancreatic Cells and Human Pancreatic Islets
Petruta Alexandru, Liliana Paslaru, Simona Dima, Anca Nastase, Laura Stoichita, Sorin Comorosan,
Irinel Popescu........................................................................................................................................................ 183
Protective Effect of Green Light Against the Deleterious Effects of UV Irradiation on Cellular SystemsSilviu Polosan, Irinel Popescu, Ileana Farcasanu, Sorin Avramescu, Elena Ionescu, Liliana Paslaru, Marian Apostol, Sorin Comorosan ...................................................................................................................... 193
Study of Serum Intestinal Alkaline Phosphatase in Rosacea
Andreea Merticariu, Luminiåa Marinescu, Cãlin Giurcãneanu .......................................................................... 201

CASE REPORTS
An Unusual Cause of Overt Upper GI Bleeding: Retrograde Jejunogastric IntussusceptionHilmi D. Elsiddig, S.H. Suliman, El.H. Salim Omer, Elnour Mustafa, Mohamed G. Alnedar, Yousif Mohd Khair, S.Z. Ibrahim ......................................................................................................................... 207
Recurrent Giant Phyllodes Tumour in a Young Female: A Case ReportMahim Koshariya, Ashish Sharma, Ajay Gehlot, Surbhi Garg, M.C. Songra, Karan Peepre ............................ 210
ABSTRACTS
Abstracts from the 23rd International Meeting of LICAGEBucharest, Romania, 8-9 September 2016 ........................................................................................................... 215
Abstracts - Author Index ............................................................................................................................................ 237
166 Journal of Translational Medicine and Research, 21 (3), 2016

Journal of Translational Medicine and Research, 21 (3), 2016 167
EDITORIAL
Corresponding author:Irinel Popescu, MD, FACS, FEBS,Professor of Surgery"Dan Setlacec" Center of GeneralSurgery and Liver Transplantation,“Fundeni” Clinical Institute, Sos.Fundeni, 258, 022328, Bucharest,RomaniaE-mail: [email protected]
Back in 1996, as a newly appointed Associate Professor of Surgery, I decidedto start a scientific journal of Fundeni Hospital, the place where I worked,inspired by the long and uninterrupted tradition in research at this largest andarguably the best medical health care institution in Romania. The name of theJournal was Annals of Fundeni Hospital.
In this difficult endeavor, I took as Associate Editor an enthusiastic and verypromising young gastroenterologist, still vascillating between clinical work andbasic research.
His name was George Calin.
The passion for genetics finally prevailed, and George became a worldfamous expert in this field, currently heading an important laboratory at the MD Anderson Institute in Houston (Texas).
Eventually, Annals of Fundeni Hospital, morphed a couple of years ago into,the Journal of Translational Medicine and Research, a journal of the RomanianAcademy of Medical Sciences and of the International Association of Surgeons,Gastroenterologists and Oncologists (IASGO).
Starting with the current issue, George Calin is back, this time as a FoundingEditor of the new (and at the same time old!) journal and as a distinguishedauthor as well.
Welcome back, George, and let’ us work together, as before, in promotingmedical science through JTMR!
Prof. dr. Irinel Popescu
Copyright © Celsius Publishing House
J. Transl. Med. Res 2016;21(3):167-167 DOI: 10.21614/jtmr-21-3-89
From the Editor in Chief

168 Journal of Translational Medicine and Research, 21 (3), 2016
LEADING ARTICLE
Copyright © Celsius Publishing House
J. Transl. Med. Res 2016;21(3):168-172 DOI: 10.21614/jtmr-21-3-90
Human Cancers: The Interplay Between Protein-CodingGenes and Non-Coding RNAs
George A. Calin
Corresponding author:George A Calin, MD, PhDE-mail: [email protected]
ABSTRACT
The discovery of non-coding RNAs (ncRNAs) dramatically changed the understanding ofcancer mechanisms in the last decade. The ncRNAs interplay with protein-coding genes andtheir abnormalities represents one the most unexpected and important discoveries in the cancer field. Cancer initiation, progression and dissemination causally involve the effects ofsmall regulatory ncRNAs named microRNAs, mainly due to deregulation of expression ofcancer protein coding genes. miRNAs can act as oncogenes (activating malignant potential)or tumor suppressors (inhibiting malignant potential) directly on the tumor cells or via communication with tumor microenvironment cells. Understanding the roles of miRNAs andother ncRNAs in malignant cells uncovers a new layer of protein coding and non-coding generegulation; furthermore, provides new markers for early diagnosis and improved prognosis,as well as novel therapeutics for cancer patients. Herein I will expose what is known aboutthe miRNA function and describe examples and the challenges for clinical use of miRNAs inthe near future.Key words: microRNAs, oncogene, tumor suppressor, cancer, diagnosis, therapy
microRNAs are short RNAs involved in physiologic microRNAs are short RNAs involved in physiologic and pathological processes and pathological processes
MicroRNAs are defined as short non-coding RNAs (ncRNAs) of about 19 to 23nucleotides (nt) in length, that are not translated in peptides but regulate protein coding gene expression at the posttranscriptional level (1). PrecursormicroRNAs in the form of hairpin loop structures, located in the nucleus, produce mature microRNAs that act at the cytoplasm level. The binding takesplace at the target messenger RNAs (mRNAs) 3’untranslated regions (UTR), coding sequences or 5´UTR (mRNAs) (2). This leads to degradation of mRNA ortranslation inhibition with consequent target protein expression reduction. It isestimated that miRNAs regulate most part of the human genome, both proteincoding as non-coding; recently, it was found that miRNAs could bind and block
Received: 29.08.2016Accepted: 10.09.2016
Departments of Experimental Therapeutics and Leukemia, The University of Texas M. D. Anderson Cancer Center, Houston, TX, USACenter for RNA Interference and Non-Coding RNAs, The University of Texas MD Anderson Cancer Center, Houston, TX, USA

Human Cancers: The Interplay Between Protein-Coding Genes and Non-Coding RNAs
Journal of Translational Medicine and Research, 21 (3), 2016 169
Human MicroRNAs Examples of clinical correlations Examples of molecular mechanisms let-7 family [TS] Let-7b is reduced in leukemia (ALL, CLL), ovary, Represses cell proliferation and growth(first family of miRs to prove prostate, liver, brain cancers and correlates with let-7f promotes angiogenesisto be conserved between species) poor prognosis; Targets: CCND1, CDC25a, CDC34,
Lets-7i expression is reduced in breast, brain cancers CDK6, DICER, HMGA2, HOXA9, ITGB3,and associated with bad prognosis; let-7i affects MYC, RAS, TLR4chemotherapy potency
miR-15a,miR-16-1 cluster [TS] Downregulated in CLL and associated with good Induces apoptosis in leukemia cells(first family of miRNAs to prove to prognosis miR-16 regulates cell cycle bybe abnormally expressed in cancer) downregulating G0/G1 proteins
Targets: BCL2, CCND1, CDK6, CDC27,HMGA2, MCL1, MYB, VEGF, WNT3A
miR-17, miR-18a, miR-19a, High levels of miR-92a identified in leukemia , miR-17, miR-18a, miR-19a, miR-20a,miR-20a, miR-19b-1, miR-92a1, (CLL, ALL) colorectal and ovary cancers. miR-19b-1miR-17-92 cluster [OG] Associates with poor prognosis. increase tumor growth and tumor(first family of miRNAs proved vascularization;to be oncogenic) miR-20a is anti-apoptotic;
Targets: AIB1 AML1, BIM1, E2F1, E2F2,E2F3, HIF-1A, PTEN, TGFBR2, TSP1
miR-21 [OG] Overexpressed in leukemia (CLL), liver, breast, colon, miR-21 knockdown induces apoptosis(the only microRNA identified lung, pancreas, prostate, stomach, colorectal, brain, in glioblastomaoverexpressed in any type of ovary, tongue, thyroid, uterine, head and neck cancers. miR-21 induces invasion, metastasiscancer analyzed) Poor prognosis, associates with fludarabine refractory in colorectal cancer
CLL Targets: BCL2, CDC25A, MASPIN,PDCD4, PTEN, TPM1, RECK, RASA1
miR-34 family [TS] Downregulated in leukemias and solid cancers miR-34a induces downregulation of E2F (first family to be used for and expression controlled by TP53 in colon cancercancer therapy in clinical trials) Low expression correlates with poor prognosis Targets: BCL2, CCND1, CCNE2, CDK4,
in leukemias CDK6, c-MYC, DLL1, E23, HMGA2,MET, MYC, N-MYC, Notch1, SIRT1
miR-155 [OG] Overexpressed in leukemia (CLL, AML), liver, breast, Pre-B cell proliferation, lymphoblastic(first miRNA to be proved oncogenic pancreas, lung, head and neck, thyroid, tongue leukemia/high-grade lymphoma in miR-155in an mouse transgenic model) carcinomas transgenic mice
Targets: AGTR1, AID, FOXO3A, IKBKE, SHIP-1,SOCS1, TP53INP1Modulates mismatch-repair genes
miR-181 family [TS or OG] Overexpression of miR-181a is reported in pancreas, MYCN regulates transcription of miR-181 cluster(first miRNA family to be involved thyroid cancers , while downregulation in brain cancers. Targets: HOXA11, TCL1in resistance to chemotherapy ) High miR-181a correlates with short interval from
diagnosis to therapy in CLL
Note – TS – tumor suppressor role; OG – oncogene role; the gene symbols are as in NCBI at http://www.ncbi.nlm.nih.gov/. AML, acute myeloid leukemia; CLL, chronic lymphocytic leukemia;
Table 1 - Examples of oncogenic or suppressor microRNAs
the function of longer non-coding RNAs (3). The impor-tance of microRNAs in all physiological or pathologicalcellular processes is supported by the fact that theirstructure is highly conserved among orthologousspecies. Cell cycle regulation, immune system functionality, apoptosis or cell death, cellular aging, differentiation, metabolism and neuronal patterningare all regulated by these short ncRNAs (4,5).
microRNAs alterations are identified microRNAs alterations are identified in all human cancers analyzed to datein all human cancers analyzed to date
Normal levels of expression of mature and/or precursor miRNAs in normal cells versus the abnormal
malignant cells represent the main mechanism of microRNoma (the full spectrum of microRNAs fromhuman genome) alterations (table 1) (6). This is due to numerous reversible or irreversible altered mecha-nisms, such as the epigenetic regulation of miRNAexpression, microRNAs mutated loci, the location ofmiRNAs at aberrant cancer genomic regions, or defectsin miRNA processing proteins including mutations inDicer (an endoribonuclease involved in the productionof mature miRNAs) or Exportin 5 (a protein involved intransport of pre-microRNA out of the nucleus) (7,8).
In 2002, Calin and colleagues reported for the firsttime miRNAs abnormalities in cancer: miR-15a and miR-16-1, that are located at the frequently deleted

George A. Calin
170 Journal of Translational Medicine and Research, 21 (3), 2016
chromosome 13q14 in chronic lymphocytic leukemia(CLL) are deleted or downregulated in the almost allpatients, indicating that these miRNAs can have a poten-tial tumor suppressors roles (9). In a following report,the same group discovered that a significant number ofmiRNAs are located at genomic regions altered in cancers (such as amplifications or loss of heterozygosityor breakpoints), suggesting miRNAs as a new class ofcancer genes (10). By developing the first microRNAmicroarray and by using large mutational screens, Calinand colleagues reported the first germline mutations inmicroRNAs as well as one of the earliest miRNA expres-sion signature associated with cancer prognosis andevolution (11). Explaining the CLL phenotype, Cimminoand Calin and colleagues reported that both miR-15 andmiR-16 are involved in programmed cell death throughthe targeting of the anti-apoptotic BCL2 messenger RNA(12). This induces low levels of BCL2 with consequentapoptosis and prolonged survival, the phenotypic characteristics of the malignant CD5/CD19-positivemalignant CLL cells.
Further work from all around the world, reported inover 25,000 publications till date present days, deeply dissected the roles of miRNAs in tumors, both in malig-nant cells and in the tumor microenvironment cells(13). Also, mutations within microRNAs were identifiedas more prevalent in malignant cells as compared tonormal cells, which shows that these mutations have arole in the malignant phenotype. An important numberof studies revealed the dual role of microRNAs, that canexert a tumor suppressive role or, on the contrary, atumor promoter (oncogenic) role: let-7 can be down-regulated in lung and breast cancers and stimulate cellgrowth, while in same cancers, miR-17-92 if over-expressed leads to cancer growth (table 1)(5,14). miR-15a and miR-16-1 reduced expression in prostatecancer promoted tumor growth and progression by thelack of repression of FGF-2 and its receptor FGFR1. BothFGF-2 and its receptor act on tumors cells as well as thesurrounding stroma environment to enhance cancer cell survival, proliferation and metastasis and were identified as downregulated also in cancer-associatedfibroblasts (CAFs) from the environment of prostatetumors (13).
microRNA expression signatures frommicroRNA expression signatures fromtumors or body fluids associates withtumors or body fluids associates withpatients’ prognosis and overall survivalpatients’ prognosis and overall survival
The measurement of miRNAs in tumor tissues, plasma, serum and other body fluids represent a newexploratory road for noninvasive biomarkers in cancer
(15,16). MicroRNA expression has been shown to forecast the clinical progression of cancers and other diseases. In CLL, both miR-29c and miR-223 are downregulated in patients who are predicted to have a poorprognosis with a shorter survival, while another impor-tant therapeutic candidate, miR-155 has been shown tobe upregulated in the same category of patients. Also,patients with other hematological diseases like acutemyeloid leukemia who present with high miR-191expression have been reported to have a shorter survival time. Nevertheless, metastasis can be detectedby using as biomarkers serum microRNAs known toinfluence many biological processes and secondarytumor development at additional locations in the body.The concerns about the high stability of miRNAs aremostly disproved by the findings that serum and plasma processing in severe conditions that would normallydegrade most RNAs (such as boiling, extreme pH levels,or extended storage) keep the short RNAs unaltered(16). As an example, serum miR-21 levels were lower inhormone-refractory prostate cancer patients whoresponded to docetaxel-based chemotherapy versusthose with resistant disease. Downregulation of let-7a,miR-17, and miR-34 family was correlated with sensitivity to 5-fluorouacil, adriamycin, or cyclophos-phamide, all commonly used in various chemotherapyregimens (13). The use of miRNA biomarkers is notrestricted only to cancer: for example, the same miR-155 and miR-223 have been implicated inRheumatoid Arthritis (17). It was also demonstrated themiRNA aberrant patterns in cardiac hypertrophy andtheir roles analyzed, including that of miR-21, which isalso one of the most deregulated miRNAs in cancer, suggesting common miRNA pathways involved in signaling pathways shared by both abnormal states (18).
microRNA therapeutics available microRNA therapeutics available for cancer patientsfor cancer patients
Contrary to chemotherapy, antisense oligonucleo-tides, small interfering RNAs, or small molecules, there isone major advantage of using miRNAs: they can targetmultiple genes from the same pathway significantlyreducing the potential development of resistance due tomultiple mutations in various genes from that specificpathway. For instance, miR-15a and miR-16-1, both withreduced expression in CLL, have two anti-apoptotic targets, the oncogenic messenger RNAs for MCL1 andBCL2. Targeting oncogenic miRNAs with anti-miRNAs or antagomiRs, or restoring the tumor suppressor miRNAlevels by using miRNA mimics, although not the “univer-sal panacea” for any type of cancer, could represent in

Human Cancers: The Interplay Between Protein-Coding Genes and Non-Coding RNAs
Journal of Translational Medicine and Research, 21 (3), 2016 171
the near future valid therapeutic options for specific categories of patients (19,20).
In the first miRNA-targeting therapy to reach clinicaltrials in humans, antagomiR-122 (named Miravirsen)was well tolerated by individuals with of hepatitis C(HCV) infection, a risk factor for developing hepato-cellular carcinoma. The use of this antago-miR revealedmild side effects such as diarrhea or headache, beinggenerally well tolerated by patients. Importantly, individuals treated with Miravirsen displayed a significant dose-dependent reduction in HCV RNA levelswithout any signs of viral resistance (21). A liposome-formulated mimic of the tumor suppressor miR-34a,called MRX34, in a Phase I clinical trial in patients withadvanced solid tumors showed manageable toxicity profiles and strong evidence of activity in hepatocellularcarcinomas, renal cell carcinomas and melanomas.Molecular analysis showed dose-dependent repressionof miR-34a target oncogenes, including BCL2, CTNNB1HDAC1, and FOXP1 in the tumors from the treatedpatients (19).
PERSPECTIVESPERSPECTIVES
MiRNAs were discovered in 1993 and rapidlybecame an exciting topic of research during the lastdecade, with the number of published studies growingexponentially. miRNAs and other longer ncRNAs areinvolved not only in cancer-altered pathways but also inmany other deadly diseases such as sepsis (22).Variations of the miRNome have been documented incancer cells with respect to the normal cell counterpart.Similarly to microRNAs, other non-coding RNAs (suchas circular RNAs or long intergenic non-codingRNAs)(23,24) appear deregulated intumors. miRNAs andother ncRNAs have only recently been identified as newdiagnostic and prognostic biomarkers for cancer evolu-tion, and miRNAs based cancer therapy represents atreatment option already in medical practice that has tobe tested for safety and efficacy.
Acknowledgements
Dr. Calin is The Alan M. Gewirtz Leukemia &Lymphoma Society Scholar. Work in Dr. Calin’s laboratoryis supported in part by the NIH/NCI grants1UH2TR00943-01 and 1 R01 CA182905-01, the UT MDAnderson Cancer Center SPORE in Melanoma grant fromNCI (P50 CA093459), Aim at Melanoma Foundation andthe Miriam and Jim Mulva research funds, the UT MDAnderson Cancer Center Brain SPORE (2P50CA127001), aDevelopmental Research award from Leukemia SPORE, aCLL Moonshot Flagship project, a 2015 Knowledge GAP
MDACC grant, an Owens Foundation grant, and theEstate of C. G. Johnson, Jr. We included in the referencelist mostly reviews, so the readers can use additionalmore detailed presentations of specific topics discussedin the present review.
REFERENCESREFERENCES
1. Ambros V. MicroRNA pathways in flies and worms: growth, death, fat,stress, and timing. Cell. 2003 Jun 13;113(6):673-6.
2. Bartel DP. MicroRNAs: genomics, biogenesis, mechanism, and function. Cell. 2004 Jan 23;116(2):281-97.
3. Gregory RI, Shiekhattar R. MicroRNA biogenesis and cancer. CancerRes. 2005 May 1;65(9):3509-12.
4. Berezikov E, Plasterk RH. Camels and zebrafish, viruses and cancer: amicroRNA update. Hum Mol Genet. 2005 Oct 15;14 Spec No. 2:R183-90.
5. Tuna M, Machado AS, Calin GA. Genetic and epigenetic alterations ofmicroRNAs and implications for human cancers and other diseases.Genes Chromosomes Cancer. 2016 Mar;55(3):193-214. doi: 10.1002/gcc.22332. Epub 2015 Dec 9.
6. Berindan-Neagoe I1, Monroig Pdel C, Pasculli B, Calin GA.MicroRNAome genome: a treasure for cancer diagnosis and therapy.CA Cancer J Clin. 2014 Sep-Oct;64(5):311-36. doi: 10.3322/caac.21244. Epub 2014 Aug 7.
7. Calin GA, Croce CM. MicroRNA signatures in human cancers. Nat RevCancer. 2006 Nov;6(11):857-66.
8. Esquela-Kerscher A, Slack FJ. OncomiRs - microRNAs with a role incancer. Nat Rev Cancer. 2006 Apr;6(4):259-69.
9. Calin GA, Dumitru CD, Shimizu M, Bichi R, Zupo S, Noch E, et al.Frequent deletions and down-regulation of micro- RNA genesmiR15 and miR16 at 13q14 in chronic lymphocytic leukemia. ProcNatl Acad Sci U S A. 2002 Nov 26;99(24):15524-9. Epub 2002 Nov14.
10. Calin GA, Sevignani C, Dumitru CD, Hyslop T, Noch E, Yendamuri S, etal. Human microRNA genes are frequently located at fragile sites andgenomic regions involved in cancers. Proc Natl Acad Sci U S A. 2004Mar 2;101(9):2999-3004. Epub 2004 Feb 18.
11. Calin GA, Ferracin M, Cimmino A, Di Leva G, Shimizu M, Wojcik SE, etal. A MicroRNA signature associated with prognosis and progressionin chronic lymphocytic leukemia. N Engl J Med. 2005 Oct 27;353(17):1793-801.
12. Cimmino A, Calin GA, Fabbri M, Iorio MV, Ferracin M, Shimizu M, etal. miR-15 and miR-16 induce apoptosis by targeting BCL2. Proc NatlAcad Sci U S A. 2005 Sep 27;102(39):13944-9. Epub 2005 Sep 15.
13. Berindan-Neagoe I, Calin GA. Molecular pathways: microRNAs, cancercells, and microenvironment. Clin Cancer Res. 2014 Dec 15;20(24):6247-53. doi: 10.1158/1078-0432.CCR-13-2500.
14. Nicoloso MS, Spizzo R, Shimizu M, Rossi S, Calin GA. MicroRNAs-themicro-steering wheel of tumor metastases. Nat Rev Cancer. 2009Apr;9(4):293-302. doi: 10.1038/nrc2619. Epub 2009 Mar 5.
15. Cummins JM, Velculescu VE. Implications of micro-RNA profiling forcancer diagnosis. Oncogene. 2006 Oct 9;25(46):6220-7.
16. Cortez MA, Bueso-Ramos C, Ferdin J, Lopez-Berestein G, Sood AK,Calin GA. MicroRNAs in body fluids-the mix of hormones and biomarkers. Nat Rev Clin Oncol. 2011 Jun 7;8(8):467-77. doi: 10.1038/nrclinonc.2011.76.
17. Churov AV, Oleinik EK, Knip M. MicroRNAs in rheumatoid arthritis:altered expression and diagnostic potential. Autoimmun Rev. 2015Nov;14(11):1029-37. doi: 10.1016/j.autrev.2015.07.005. Epub 2015Jul 8.
18. Small EM, Olson EN. Pervasive roles of microRNAs in cardiovascularbiolobgy. Nature. 2011 Jan 20;469(7330):336-42. doi: 10.1038/nature09783.
19. Ling H, Fabbri M, Calin GA. MicroRNAs and other non-coding RNAsas targets for anticancer drug development. Nat Rev Drug Discov.

George A. Calin
172 Journal of Translational Medicine and Research, 21 (3), 2016
2013 Nov;12(11):847-65. doi: 10.1038/nrd4140.20. Monroig Pdel C, Chen L, Zhang S, Calin GA. Small molecule
compounds targeting miRNAs for cancer therapy. Adv Drug Deliv Rev.2015 Jan;81:104-16. doi: 10.1016/j.addr.2014.09.002. Epub 2014Sep 17.
21. Janssen HL, Reesink HW, Lawitz EJ, Zeuzem S, Rodriguez-Torres M,Patel K, et al. Treatment of HCV infection by targeting microRNA. N EnglJ Med. 2013 May 2;368(18):1685-94. doi: 10.1056/ NEJMoa1209026.Epub 2013 Mar 27.
22. Vasilescu C, Rossi S, Shimizu M, Tudor S, Veronese A, Ferracin M, et
al. MicroRNA fingerprints identify miR-150 as a plasma prognosticmarker in patients with sepsis. PLoS One. 2009 Oct 12;4(10):e7405.doi: 10.1371/journal.pone.0007405.
23. Taft RJ1, Pang KC, Mercer TR, Dinger M, Mattick JS. Non-codingRNAs: regulators of disease. J Pathol. 2010 Jan;220(2): 126-39. doi:10.1002/path.2638.
24. Ling H, Vincent K, Pichler M, Fodde R, Berindan-Neagoe I, Slack FJ, etal. Junk DNA and the long non-coding RNA twist in cancer genetics.Oncogene. 2015 Sep 24;34(39):5003-11. doi: 10.1038/onc.2014.456.Epub 2015 Jan 26..

J. Transl. Med. Res 2016;21(3):173-182 DOI: 10.21614/jtmr-21-3-91
Journal of Translational Medicine and Research, 21 (3), 2016 173
REVIEW ARTICLE
Copyright © Celsius Publishing House
Thrombotic Complications in Cirrhotic Patients: Balancing Risks and Benefits of Anticoagulation Treatment
Ecaterina Scãrlãtescu1, Mercedes S. Mandell2, Dana R. Tomescu1,3
Corresponding author:Dana R. Tomescu, MD, PhDAssociate Professor, University of Medicine and Pharmacy“Carol Davila”, Bucharest, Romania Head of Anesthesiology and IntensiveCare Department III, Fundeni ClinicalInstitute, Fundeni no 258, 022328,Bucharest, RomaniaE-mail: [email protected]
ABSTRACT
The risk of excessive bleeding and thrombotic complications coexist in cirrhotic patients dueto synthetic reduction in both pro and anticoagulants. However, investigators suggest theprevalence and consequences of thrombotic complications are underestimated. There isconvincing evidence that thrombosis causes worsening portal hypertension, hepatic fibrosisand increases patient mortality. New evidence is emerging about the benefits of treating andpreventing thrombotic complications in patients with liver disease. In the absence of well-designed trials, clinical experience has become the most consistent guide to choose anddose anticoagulant drugs in this patient population. Practical use of anticoagulants however,is hindered by the lack of simple methods to monitor drug effect. In this review, we presenta concise appraisal of current evidence on the most commonly studied indications for anti-coagulation in cirrhotic patients. Information about drug action, dosing and monitoring arepresented to provide a basis for clinical decision-making. The ongoing challenges in identifying therapeutic targets for treatment and monitoring drug effects are examined tohighlight important clinical questions that have not yet been fully addressed.Key words: liver cirrhosis; coagulation; bleeding; thrombosis
INTRODUCTIONINTRODUCTION
Health care providers have primarily focused upon the prevention and treat-ment of bleeding episodes in cirrhotic patients (1). A lack of laboratory measuresidentifying thrombosis risk has given clinicians the impression that patients are“auto-anticoagulated” and at low risk of thromboembolic disease (2-4). Onlyrecently have the importance of thrombosis in cirrhotic patients been recognized and investigators think the frequency and severity of the resultingcomplications are still underestimated (5).
Pro and anticoagulant factors play a critical role in forming mechanicallyeffective clot that is limited to the site of injury (2,6). The same balance is
Received: 30.07.2016Accepted: 05.09.2016
1Department of Anesthesiology and Intensive Care III, Fundeni Clinical Institute, Bucharest,Romania2Department of Anesthesiology, University of Colorado Health Sciences Center, Aurora,Colorado, United States3University of Medicine and Pharmacy “Carol Davila”, Bucharest, Romania

Ecaterina Scãrlãtescu et al
174 Journal of Translational Medicine and Research, 21 (3), 2016
present in patients with compensated liver disease.However, coagulation is “rebalanced” by an equalreduction in factors that build and prevent clotting.Physiological insults such as sepsis or kidney dysfunc-tion easily tip this new and fragile balance to causebleeding and/ or thrombotic complications.
New clinical findings show that thrombosis cancause acute hepatic decompensation, disease progres-sion and death in cirrhotic patients (7-9). While treatment with anticoagulants reduces morbidity andmortality associated with thrombotic complications in anumber of diseases, the data about risks and benefitsof anticoagulation in cirrhotic patients is only beginningto accrue. Durable recommendations about indica-tions, dosing and therapeutic safety indices still requiremore information from well-designed studies.
The aim of this review is to provide a concise yetcomprehensive appraisal of current research that outlines the risks and benefits of anticoagulation in cirrhotic patients. We limited our review to the moststudied indications for anticoagulation in cirrhoticpatients. A summary of up to date information aboutthe pharmacology and monitoring of anticoagulants isprovided to assist care providers in clinical decision making. We use the evidentiary base to identify gaps inknowledge that require future work to improve patientoutcomes.
MOST COMMONLY STUDIED INDICATIONSMOST COMMONLY STUDIED INDICATIONSFOR ANTICOAGULATION IN CIRRHOTICFOR ANTICOAGULATION IN CIRRHOTICPATIENTSPATIENTS
Portal vein thrombosis (PVT)
The prevalence of nonmalignant PVT in cirrhosis isestimated at 10-25% (10). Acute PVT can abruptlyincrease portal hypertension leading to decompensa-tion and death. Further, transplantation may not bepossible if clot propagates into the mesenteric veins.Risk factors for PVT are unknown, but variceal bleeding,low platelet count and reduced portal flow velocity areassociated findings (4,11).
Population studies suggest thrombophilic factorsoccur in up to 39% of patients with PVT (12). The mostcommon were Factor V Leiden, prothrombin 20210Amutation and Plasminogen activator inhibitor 4G-4G.The prevalence of thrombophilia in PVT may be under-estimated as standard coagulation profiles often fail toidentify increased clotting and routine screening forthrombophilic factors is rarely performed (12-14).
Differences in opinion about anticoagulation for PVTstem from findings showing that nearly half of affected
patients experience some degree of spontaneousrecanalization (15). However, a systematic reviewshowed a pooled Odds Ratio of 4.16 (95% CI = 1.88 –9.20, P = 0.0004) for complete recanalization in treatedcompared to untreated patients (16). Findings from thesame systematic review showed that bleeding compli-cations were rare and patient death was not due totreatment (16).
The findings show anticoagulation increases portalvein patency and reduces complications due to PVT.Observations from a small randomized controlled trial inadvanced and compensated cirrhosis also suggest thebenefits of routine PVT prophylaxis outweigh the risks(17). The findings are promising, but more outcome datais needed to construct a robust therapeutic safety indexcapable of guiding treatment. Regardless of these limita-tions, many investigators consider current findings convincing enough to recommend anti-coagulation fortreatment and prophylaxis of PVT (17).
Budd-Chiari syndrome (BCS)
Obstruction of outflow between the small hepaticveins and the inferior vena up to the level of the rightatrium is rare in Western countries and usually due tomultiple thrombophilic disorders including myelo-proliferative disease (18). Congenital endoluminalabnormalities explain the higher prevalence in Asiancountries (19). Therapeutic options include anticoagula-tion, recanalization, surgical shunting, transjugular intra-hepatic portosystemic shunting and transplantation.Anticoagulation is a common initial intervention (20).The strategy for anticoagulation is extrapolated fromoutcomes in patients with venous thromboembolism(VTE) due to thrombophilic disorders. However, anti-coagulation as a single therapy is only effective in 10% ofBCS cases (21).
Venous thromboembolism (VTE)
The reported incidence of deep vein thrombosisand pulmonary embolism in hospitalized patients with chronic liver disease varies from 0.5 to 6.3% (4,22).Incidence increased with severity of illness measuredby Child-Pugh (22). Age less than 45 years increasedthe risk in compensated (OR 1.23; 95% CI 1.04 to 1.46)and decompensated patients (OR 1.39; 95% CI 1.15 to1.69)(23).
Investigators suggest VTE is still underestimatedbecause routine screening is rarely performed and standard coagulation tests are not diagnostic (2-4).Patients at increased risk include those with Hepatitis A,B and C in addition to Epstein Barr and Cytomegalovirus(24). Investigators theorize that viral-induced inflamma-

Anticoagulation in the Cirrhotic Patient
Journal of Translational Medicine and Research, 21 (3), 2016 175
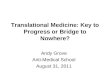
Figure 1 - Two major classes of anticoagulant drugs are the Heparins and Novel Oral Anticoagulants (NOAC).Unfiltered heparins are larger than Low Molecular Weight Heparin (LMWH). Both groups of heparin-based drugsare activated by binding Antithrombin III (AT III). AT-III activated LMWH have higher affinity for factor Xa than for
thrombin. NOAC bind and inactivate either thrombin or factor Xa
tion activates coagulation factors, downregulates anti-coagulants and inhibits fibrinolysis (25).
A pulmonary embolus mortality risk of 35% compared to 16% in noncirrhotic patients and longerhospital stay supports routine surveillance and anti-coagulation for VTE in hospitalized cirrhotic patients(26). Few adverse outcomes in patients with decom-pensated cirrhosis treated for PVT suggest there couldbe a similar risk-benefit profile for treatment of VTE. To date, prophylaxis for VTE requires additional evaluation (2).
Thrombosis-associated hepatic fibrosis
Human and experimental animal evidence linkhepatic microvascular thrombosis with tissue paren-chyma fibrosis (26). A similar relationship betweenmicrovascular clotting and fibrosis has been reported inprogressive lung and kidney diseases and suggests thatin situ small vessel thrombosis may be a common endpathway for a number of pathological conditions (24,25).Recent studies show microvascular thrombosis initiates inflammation and stellate cell activation, two molecularpathways associated with increased thrombin genera-tion and fibrin formation (26,27). Theories implicatingparenchyma extinction also identify microvascularthrombosis as the first step in a cascade leading to fibrosis (27).
Hepatic fibrosis progresses faster in patients withgenetic mutations for Factor V Leiden, protein C deficiency or increased expression of factor VIII than inpatients with hemophilia and Hepatitis C (5,28). Thefibrotic response is slower in experimental animals withinhibition of endothelial-based Tissue Factor and P-selectin (29,30). Evidence suggests multiple sites inthe coagulation cascade initiate inflammation whichstimulates the synthesis of interstitial molecules (31).
The current evidence specifically implicates increasedclot formation as a cause of progressive fibrosis but, it isunknown if anticoagulation will mitigate this response.The evidence is very compelling and clinical trials are thenext logical step.
Use of extracorporeal circuits for life support
Extracorporeal circuits are often used in cirrhoticswithout anticoagulation due to concerns about heparin-induced bleeding risk. Clot accumulation in extra-corporeal circuits is common in cirrhotic patients compared to patients with other causes of renal failure(32). Heparin administration however, failed to increasecircuit patency times and was associated with increasedbleeding complications (33). Other anticoagulants usedto promote extracorporeal circuit patency did not perform better than heparin (34, 35). Citrate anti-coagulation can safely be used in liver transplantpatients, but the filter running time was still limited toapproximately 23 hours (35). There is general agree-ment that the risk of heparinization exceeds the benefitin renal replacement circuits (33).
PHARMACOLOGY AND MONITORING PHARMACOLOGY AND MONITORING OF ANTICOAGULANT DRUGOF ANTICOAGULANT DRUG
Choice of anticoagulant drugs for clinical use in cirrhotic patients is complicated by a lack of well-designed efficacy and safety trials. Current studies incirrhotic patients have not tested for differences inresponse due to factors such as demographic hetero-geneity, severity of illness and etiology of disease.Therefore clinicians often draw from their knowledgeabout the pharmacological behavior of anticoagulantdrugs (fig. 1).

Ecaterina Scãrlãtescu et al
176 Journal of Translational Medicine and Research, 21 (3), 2016
Heparin: unfractioned heparin and low molecular weight heparin
Pharmacology
Unfractionated heparin (UFH) is a naturally occur-ring molecule bound to endothelial cells. Molecules arerepeating disaccharide units that vary between 3000 to30,000 Daltons (36). When given parenterally, UFH,binds Antithrombin III (AT III), inducing conformationalchanges that causes the UFH-AT-III complex to bind andinactivate thrombin and factor Xa (36). Smaller UFH segments complex with AT IIII and inactivate factor Xa,while longer segments are required to inhibit thrombin(37). Duration of action is one to two hours (table 1).
Low molecular weight heparins (LMWH) are formedby chemical or enzymatic breakdown of large UFHmolecular fragments to yield smaller subunits. Purityassays require at least 60% of heparin chains are 8000Daltons or less (37). LMWH form a complex with AT IIIto primarily inhibit factor Xa. The preferential inhibitionof factor Xa produces more predictable anticoagulanteffects than unfractionated heparins.
Duration of action
Steady state drug levels for UFH require 6 hours compared to approximately two to four days for LMWH.The elimination half-life of UFH is 60-150 minutes com-pared to 4.5 hours for LMWH (33). Heparin half-life isdetermined by the rate of cellular uptake, renal excre-tion and binding to Antithrombin III. Human hyaluronicacid receptors for endocytosis (HARE)/ stabilin-2 in liversinusoidal endothelial cells clear UHF and LMWH (38).Affinity for HARE is higher for UFH than LMWH butuptake for both is facilitated by AT III binding. Renal
excretion becomes the primary route of eliminationwhen cellular uptake is saturated (39). In contrast,LMWH is eliminated by the kidneys only after hepaticpartial depolymerization and/or desulfation (40).Therefore renal elimination becomes the primary deter-minant of half-life during continuous treatment (39).
Monitoring heparin-anticoagulation in cirrhosis
The activated partial prothrombin time (aPTT) is astandard measure of UFH anticoagulant effect, butpoorly predicts coagulation inhibition in cirrhosis (41,42). Baseline aPTT values often exceed normal limits in most cirrhotic patients because the assay only measures procoagulant activity which is reduced due tosynthetic failure.
The aPTT does not measure anticoagulant activityand can overestimate bleeding risk, leading to sub-therapeutic dosing. To date there are no evidence-based algorithms to guide UFH dosing that considersthe balance between procoagulant and anticoagulantfactors. Even tests that use a direct measure of throm-bin activity have poor predictability (43,44).
Monitoring is rarely performed in non-cirrhoticpatients taking LMWH due to the relatively large therapeutic safety index. When required, the anti-Xaassay is used to determine therapeutic effect (45,46).The assay is performed by adding patient plasma to aknown excess of factor Xa and AT III. The amount ofremaining Xa is used to extrapolate the degree of coagulation inhibition (46,47).
Results of the anti-Xa assay can be unreliable due toinconsistent sources of commercially available anti-factor Xa substrates and the use of blood samples out-side peak activity. Further, the test presumes patients
Property Unfractionated Heparin Low Molecular Weight HeparinChemical Composition Polysaccharide with repeating Same but less heterogeneous
disaccharide unitsMolecular Weight 3000- 30,000 Daltons 4,000-6,000 DaltonsAdministration Parenteral ParenteralInhibitory activity Primarily Thrombin Primarily XaElimination half-life 1.5 hours I1-2) 4.5 hours (4-6)Metabolism Hepatic (HARE receptors) Hepatic
(HARE receptors and desulfation or depolymerization)Elimination Renal-dose dependent Renal-dose independentStandard Laboratory Monitoring aPTT Antifactor Xa and thrombin generationReversal Protamine Partially reversed by ProtamineAbbreviations: Activated Partial Thromboplastin Time (aPTT), Hyaluronic acid receptors for endocytosis (HARE)
Table 1 - Pharmacokinetic and pharmacodynamic properties of Unfractionated Heparin (UFH) and Low Molecular Weight Heparins (LMWH)

Anticoagulation in the Cirrhotic Patient
Journal of Translational Medicine and Research, 21 (3), 2016 177
have normal AT III levels (41). Most cirrhotic patientsdevelop profound AT III deficiency (<30% activity) dueto hepatic synthetic failure. Therefore, the accuracy ofthe assay declines as the severity of cirrhosis increases(42).
Thrombin generation tests also estimate LMWHanticoagulant effect. The degree of coagulation inhibi-tion measured by the anti-Xa and thrombin generationtests vary and make clinical interpretation difficult (48).Similar discordant findings are also reported in pregnant patients (49). Thrombin generation tests formonitoring are now commonly used as opposed toanti-Xa since the former provides a more detailedpharmokinetic profile.
Newer low molecular weight heparins
Newer LMWH have a narrower range of meanmolecular weights that make the duration of actionmore predictable (50). The ratio of anti-Xa and anti-thrombin activity varies for each LMWH. SmallerLMWH drugs such as Bemiparin (3,600 D) have thehighest anti-Xa to anti-thrombin activity. The relativeproportion of anti-thrombin activity increases withmolecular weight, explaining why Tinzaparin (6,500 D)has the lowest anti-Xa to anti-thrombin activity. Forexample, Tinzaparin has much higher dose dependentanti-thrombin activity compared to Enoxaparin (4,400D) (50).
Lower molecular weight is associated with accumu-lation in renal disease. Tinzaparin has the highestmolecular weight of all marketed LMWH and is leastdependent upon renal excretion (38). Studies in elderlypatients showed less accumulation of Tinzaparin compared to Enoxaparin with a creatinine clearance<20 mL/min (51).
New oral anticoagulants (NOAC)
Pharmacology
New oral anticoagulants are molecular hetero-geneous drugs that bind and inactivate thrombin or Xa(table 2). Dabigatran was the first NOAC released foruse. It directly inhibits thrombin, while Endoxaban,Rivaroxaban and Apixaban inhibit free factor Xa and Xabound to prothrombinase complex (52). The thrombininhibitor, Dabigatran has a larger anticoagulant effect incirrhotic versus control patients compared to the directfactor Xa inhibitors, Rivaroxaban and Apixaban whichwere less potent than in control patients (43).
Advantages of NOAC include oral administration, norequirement for bridging therapy, few drug restrictions,reversal with recombinant prothrombin complexes orspecific agents like Idarucizumab for Dabigatran reversal (53) and no need for monitoring in mostpatient populations (54). Oral administration is particularly advantageous in cirrhotic patients whorequire long term anticoagulant administration (2,55).
Duration of action
The half-life of NOAC vary between 5 and 17 hours(table 2). The shorter half-life of the factor Xa inhibitor,Rivaroxaban (5-9 hours) improves safety. Up to 33% ofthe drug is eliminated unchanged by the kidney while66% is metabolized by the liver before renal elimina-tion. In contrast Dabigatran must be activated by hepatic metabolism (54). The half-life is considerablylonger (12-17 hours) than Rivaroxaban, but the meanplasma terminal half-life is independent of dose whichimproves the ability to predict duration of action.Apixaban is another factor Xa inhibitor with a half-life
NOAC Dabigatran Rivaroxaban ApixabanTrade name Pradaxa, Praxaza, Pradax Xarelto Eliquis
Site of Action thrombin Xa Xa
Bioavailability 3-7% 80-100% 50%
Metabolism Hepatic glucuronidation Hepatic metabolism (66%) CYP3A4 , HepaticCYP2J2 and CYP-independent mechanisms CYP3A4, CYP3A5, CYP1A2
Half-life 12-17 hours 5-9 hours 9-14 hours
Elimination Renal 7% Renal Biliary (75%)GI 87% Metabolized (66%) Renal (25%)
Unchanged (33%)
Monitor: None TCT-based tests Modified chromogenic Modified chromogenic Anti-Xa assay Anti-Xa assay
Reversal 3 and 4 PTC 3 and 4 PTC 3 and 4 PTCIdarucizumab Reversal agents in development Reversal agents in development
Abbreviations: Anticoagulant Drugs (NOAC). Cytochrome P (CYP), Gastrointestinal (GI), Prothrombin Complex (PTC), Thrombin Clotting Time (TCT)
Table 2 - A summary of pharmacokinetic and pharmacodynamic information on Novel Oral

Ecaterina Scãrlãtescu et al
178 Journal of Translational Medicine and Research, 21 (3), 2016
of 8–15 hours. However, it has the smallest renal clearance of all NOAC drugs (25%). Apixaban andRivaroxaban are metabolized in the liver by theCytochrome P450-dependent isozyme pathway prior toelimination (54).
Monitoring
There are no laboratory assays capable of measuringNOAC anticoagulation effect (55). Dilute thrombin generation time, Ecarin clotting and chromogenic assayscorrelate best with drug concentration, but are notapproved by U.S. regulatory agencies for testing (56). Inaddition, dosing adjustments for age or renal and hepatic disease have not been developed (57).
The Prothrombin Time and Ecarin venom test canbe used to estimate clotting inhibition but are unreliable due to differences in thromboplastin assayagents (58). The diluted thrombin time and Ecarin clotting times only estimate plasma drug concentration(59). Therapeutic ranges are unknown and concentra-tion does not reliably predict activity (56). The resultsfrom in vitro studies found chromogenic anti-Xa assaysmay be better estimates of direct Xa inhibitors eventhough this test underestimates AT III-dependent druglevels in cirrhotic patients (42).
CLINICAL EXPERIENCE WITHCLINICAL EXPERIENCE WITHANTICOAGULATION IN CIRRHOSIS ANTICOAGULATION IN CIRRHOSIS
Experience with PVT
There is growing support for routine use of anti-coagulation in all cirrhotics with newly diagnosed non-malignant PVT. Most clinical experience is derived fromstudies using the LMWH, Enoxaparin. Most patientshad partial or complete resolution of PVT followingtreatment over 7-17 months (60-62). However, limiteddata suggests at least 39% recurrence after treatmentwas stopped.
The natural history of PVT is similar to spontaneouspulmonary embolism where therapeutic benefit is lostafter discontinuing treatment (63). This raises questionsabout treatment strategies and if long term post thrombotic prophylaxis is of benefit. At least one studyshowed de novo PVT could be prevented by prophylac-tic treatment. While it is reasonable to speculate thatprophylaxis could reduce the risk of recurrent PVT, thisassumption requires confirmatory evidence (17).
There is limited experience with newer anticoagu-lant drugs for PVT or other thrombotic complications ofcirrhosis. Anticoagulant drugs are not necessarily inter-changeable even if they belong to the same family ofmedications. A comparison of half-life, duration of
action and type of elimination within each drug groupindicates that each drug has a unique pharmacologicalprofile.
Clinical experience with NOAC in PVT is limited tosmall studies and case reports as cirrhotic patients wereexcluded from commercially sponsored Phase III trials.Use of these products in cirrhotics is considered off-label. Successful treatment of PVT with or withoutmesenteric extension of clot was reported in a series of5 patients and in a separate single case report (64, 65).All patients were Child A, without varices. Resolution ofPVT required six months of therapy. No major bleedingcomplications were reported (66). Mild hepatic impair-ment did not seem to alter the pharmacokinetics ofRivaroxaban. However, moderate hepatic impairmentsignificantly increased plasma levels (67).
The decision to treat PVT with anticoagulantsappears evidence based and has a sound line of scien-tific reasoning (68). However, some investigators arguePVT is probably a distant marker of worse patient survival regardless of successful recanalization and theimportant benchmark is a critical reduction in portalvenous velocity that precedes in situ thrombosis (69).This difference in viewpoints has made it difficult to findconsensus on anticoagulant management of PVT (60).
Experience with BCS
Investigators suggest limiting anticoagulation for BSCto patients without portal hypertension to reduce risk ofbleeding complications and because of a poor long termresponse rate (70). Heparins (UFH and LMWH) appear tohave equal efficacy to Vitamin K antagonists (71).However, Vitamin K antagonists are often preferred dueto ease of long term oral administration. There is limitedevidence for choice of anticoagulants following percuta-neous or surgical recanalization and transplantation. Aretrospective single center study of balloon dilationreported complete clot resolution in 12 of 19 and partialresolution in the remaining 7 BCS patients at 15.9 ±14.4months using Warfarin (72). The antithrombotic effectsof aspirin were equally effective as Vitamin K Antagonistsin patients with thrombophilia due to myeloproliferativedisorders well controlled on hydroxyurea (73). To datethere are no studies using newer LMWH or NOAC in BCS.
Experience with VTE
Evidence suggests VTE prophylaxis improves patientsurvival and reduces length of hospitalization in cirrhotic patients. Early studies found prophylaxis withLMWH or UFH failed to prevent VTE and increasedbleeding complications (44, 74). A reduction in VTE ratehowever, was reported in a larger study cohort

Anticoagulation in the Cirrhotic Patient
Journal of Translational Medicine and Research, 21 (3), 2016 179
comprised of younger hospitalized cirrhotics. The diag-nostic rate was greater in the younger cohort (1.5%vs.0.5%) (75). The findings are consistent with previousobservations showing a relationship between youngerage in cirrhotics and risk of VTE (23). Older age in earlier studies also probably explains the higher number of bleeding episodes (76, 77).
Experience with hepatic fibrosis
There is strong experimental data supporting observations that in situ thrombosis increases the risk ofprogressive fibrosis. However, there are no correspon-ding human trials. Select anticoagulants may have additional properties that modulate ischemia and thefibrotic response. Rats treated with Enoxaparin andNadroparin had significantly less hepatic fibrosis compared to those treated with Tinzaparin (78). A linkbetween Rivaroxaban and inhibition of inflammatorypathways was found in models of ischemic stroke. Betteroutcome in Rivaroxaban treated rats was related todown regulation ICAM-1 expression and the activationof CD68+-immune cells in addition to thrombin inhibi-tion (79).
Vitamin K antagonists (VKA)
Vitamin K antagonists still form a mainstay of therapeutic intervention at many institutions. Warfarinbinds and inactivates Vitamin K epoxide reductase, theenzyme that returns Vitamin K1 to an active form. Thisdepletes Vitamin K1, the substrate needed to activatecoagulation proteins (II, VII, IX, X, protein C, and S).Onset of action is delayed for two to three days untilthere is natural attrition of activated coagulation proteins. Protein C and S levels drop faster than pro-coagulant factors leaves a vulnerable period where therisk of thrombosis is theoretically increased. Short acting anticoagulants with rapid onset are thereforeoften used to initiate anticoagulation during treatmentwith VKA. Treatment requires regular monitoring. Themost common monitoring test is the InternationalNormalized Ratio (INR).
Monitoring
The therapeutic target for INR in cirrhotic patients isoften unclear due to prolongation of the INR caused byreduced procoagulant synthesis (2). A comparison ofassays including INR shows thrombin generation captures more detailed information about the globalcoagulation cascade. However, there was a large variation across a narrow range of INR values even inthrombin generation testing (80).
Shortfalls in clinical monitoring
The prothrombin time was previously used to measure therapeutic effect in patients taking VKA.Different sourcing of assay thromboplastin substratesgave rise to variable test results. The World HealthOrganization endorsed use of a normalized value based upon a single thromboplastin source (81). Theresulting international sensitivity index (ISI) correctsprothrombin times into values that can be comparedover time and between institutions (81,82). The resulting INR values can only be used in patients with-out pre-existing coagulation defects and there is nosimple approach to normalize the INR in cirrhosis (82).
Investigators suggested using plasma from healthyand cirrhotic patients to normalize the INR (82). Eachthromboplastin would have 2 ISI values: one forpatients on VKA and one for cirrhotic patients. Thisshould reduce inter-laboratory variability for INR values. However, it is unlikely that a single ISI for liverwould work equally well in all cirrhotic patients due todifferences in coagulation profiles caused by severity ofillness. The other remaining alternative is to measurefactor levels (2).
Clinical outcomes
There are no large randomized trials and most evidence supporting use of VKA in cirrhotic patientscomes from small single center reports. Treatmentappears to improve PVT with and without thrombophilia(83). Few bleeding complications have been reported following PVT treatment with either VKA or LMWH (84,85). Similar findings were reported in a single centerstudy of VKA thrombosis prophylaxis in liver transplantrecipients (86). Patients with splanchnic thrombosis havebeen safely treated with VKA after initiation treatmentwith LMWH. Patients in this study had an average MELDscore of 13 and the INR was kept between values of 2-3during treatment (87).
A single study found cirrhotic patients with atrialfibrillation experienced more bleeding complicationswhen treated with VKA (88). Bleeding complicationswere mostly due to varices and hemorrhagic stroke.However, a higher prevalence of neurological vascularaccident and hypertension in this population prior toVKA treatment may explain these findings. Endoscopictreatment of varices was not reported. Further, the onlytest that guided VKA administration was the INR andend points for treatment were unclear. The authors stillconcluded however, that the risk compared to benefitof VKA use seemed favorable for patients with earlierstages of cirrhosis (88,89).

Ecaterina Scãrlãtescu et al
180 Journal of Translational Medicine and Research, 21 (3), 2016
CONCLUSIONSCONCLUSIONS
A focus upon the most commonly studied indica-tions for anticoagulation in cirrhotic patients allowed usto compile enough evidence to uncover trends in anti-coagulant treatment and identify knowledge gaps thatcause uncertainty in clinical decision making. We foundgeneral agreement that treatment of thrombosis in cirrhosis reduces morbidity and mortality. Thestrongest evidence came from studies of PVT.
Evidence outlining the risks and benefits of PVT prophylaxis were more controversial. However, thefindings were encouraging and can be considered alaunch point for future investigation. Larger and betterdesigned studies are needed to confirm observationsabout the benefits of anticoagulation prophylaxis andtreatment for PVT and VTE. The ability of some anti-coagulant drugs to modulate the fibrotic response inexperimental animals is an exciting finding that stillneeds translation into human studies.
There are few reliable tests to monitor anti-coagulant activity in cirrhotic patients and standardtests have inherent faults that limit clinical use. Thedesire to monitor anticoagulant effects is driven by thelack of steady state in coagulation synthesis and drugmetabolism and elimination. Developing reliable andvalidated tests for measuring coagulation profiles andtherapeutic effect will be one of the most importantpieces of the puzzle for developing a rational approachto anticoagulation in cirrhosis.
REFERENCESREFERENCES
1. Caldwell S, Intagliata N. Dismantling the myth of "autoanticoagulation"in cirrhosis: an old dogma dies hard. Hepatology. 2012 May;55(5):1634-7.
2. Lisman T1, Kamphuisen PW, Northup PG, Porte RJ. Established and new-generation antithrombotic drugs in patients with cirrhosis -possibilities and caveats. J Hepatol. 2013 Aug;59(2):358-66.
3. Senzolo M, Sartori MT, Lisman T. Should we give thromboprophylaxisto patients with liver cirrhosis and coagulopathy? HPB (Oxford). 2009Sep;11(6):459-64.
4. Hugenholtz GC, Northup PG, Porte RJ, Lisman T. Is there a rationalefor treatment of chronic liver disease with antithrombotic therapy?Blood Rev. 2015 Mar;29(2):127-36.
5. Tripodi A, Anstee QM, Sogaard KK, Primignani M, Valla DC.Hypercoagulability in cirrhosis: causes and consequences. J ThrombHaemost. 2011 Sep;9(9):1713-23.
6. Saner FH, Gieseler RK, Akız H, Canbay A, Görlinger K. Delicate balance of bleeding and thrombosis in end-stage liver disease and livertransplantation. Digestion. 2013;88(3):135-44.
7. Lisman T, Leebeek FW. Hemostatic alterations in liver disease: a reviewon pathophysiology, clinical consequences, and treatment. Dig Surg.2007;24(4):250-8. Epub 2007 Jul 27.
8. Tripodi A, Salerno F, Chantarangkul V, Clerici M, Cazzaniga M,Primignani M, et al. Evidence of normal thrombin generation in cirrhosis despite abnormal conventional coagulation tests.Hepatology. 2005 Mar;41(3):553-8.
9. Gatt A, Riddell A, Calvaruso V, Tuddenham EG, Makris M, Burroughs
AK. Enhanced thrombin generation in patients with cirrhosis-inducedcoagulopathy. J Thromb Haemost. 2010 Sep;8(9):1994-2000.
10. Tsochatzis EA, Senzolo M, Germani G, Gatt A, Burroughs AK.Systematic review: portal vein thrombosis in cirrhosis. AlimentPharmacol Ther. 2010 Feb 1;31(3):366-74.
11. Rodriguez-Castro KI, Simioni P, Burra P, Senzolo M. Anticoagulationfor the treatment of thrombotic complications in patients with cirrho-sis. Liver Int. 2012 Nov;32(10):1465-76.
12. D'Amico M, Pasta F, Pasta L. Thrombophilic genetic factors PAI-1 4G-4G and MTHFR 677TT as risk factors of alcohol, cryptogenic liver cir-rhosis and portal vein thrombosis, in a Caucasian population. Gene.2015 Aug 15;568(1):85-8.
13. Chen H, Qi X, He C, Yin Z, Fan D, Han G. Coagulation imbalance maynot contribute to the development of portal vein thrombosis in patientswith cirrhosis. Thromb Res. 2013 Feb;131(2):173-7.
14. Rossetto V, Spiezia L, Senzolo M, Rodriguez-Castro KI, Maggiolo S,Simioni P. Whole blood rotation thromboelastometry (ROTEM(R))profiles in subjects with non-neoplastic portal vein thrombosis.Thromb Res. 2013 Aug;132(2):e131-4.
15. Sogaard KK, Astrup LB, Vilstrup H, et al. Portal vein thrombosis; riskfactors, clinical presentation and treatment. BMC Gastroenterology.2007; 7(1):1-6.
16. Qi X, De Stefano V, Li H, Dai J, Guo X, Fan D. Anticoagulation for thetreatment of portal vein thrombosis in liver cirrhosis: a systematicreview and meta-analysis of observational studies. Eur J Intern Med.2015 Jan;26(1):23-9.
17. Villa E, Cammà C, Marietta M, Luongo M, Critelli R, Colopi S, et al.Enoxaparin prevents portal vein thrombosis and liver decompensationin patients with advanced cirrhosis. Gastroenterology. 2012 Nov;143(5):1253-60.e1-4.
18. Martens P, Nevens F. Budd-Chiari syndrome. United EuropeanGastroenterol J. 2015 Dec;3(6):489-500.
19. Darwish Murad S, Plessier A, Hernandez-Guerra M, Fabris F, EapenCE, Bahr MJ, et al. Etiology, management, and outcome of the Budd-Chiari syndrome. Ann Intern Med. 2009 Aug 4;151(3):167-75.
20. Seijo S, Plessier A, Hoekstra J, Dell'era A, Mandair D, Rifai K, et al.Good long-term outcome of Budd-Chiari syndrome with a step-wisemanagement. Hepatology. 2013 May;57(5):1962-8.
21. Plessier A, Sibert A, Consigny Y, Hakime A, Zappa M, Denninger MH,et al. Aiming at minimal invasiveness as a therapeutic strategy forBudd-Chiari syndrome. Hepatology. 2006 Nov;44(5):1308-16.
22. Dabbagh O, Oza A, Prakash S, Sunna R, Saettele TM. Coagulopathydoes not protect against venous thromboembolism in hospitalizedpatients with chronic liver disease. Chest. 2010 May;137(5):1145-9.
23. Pincus KJ, Tata AL, Watson K. Risk of venous thromboembolism inpatients with chronic liver disease and the utility of venous thrombo-embolism prophylaxis. Ann Pharmacother. 2012 Jun;46(6):873-8.
24. Crooks MG, Hart SP. Coagulation and anticoagulation in idiopathic pulmonary fibrosis. Eur Respir Rev. 2015 Sep;24(137):392-9.
25. Tian S, Chen SY. Macrophage polarization in kidney diseases.Macrophage (Houst). 2015;2(1). pii: e679.
26. Anstee QM, Goldin RD, Wright M, Martinelli A, Cox R, Thursz MR.Coagulation status modulates murine hepatic fibrogenesis: implica-tions for the development of novel therapies. J Thromb Haemost.2008 Aug;6(8):1336-43.
27. Anstee QM, Dhar A, Thursz MR. The role of hypercoagulability in liverfibrogenesis. Clin Res Hepatol Gastroenterol. 2011 Sep;35(8-9):526-33.
28. Yee TT, Griffioen A, Sabin CA, Dusheiko G, Lee CA. The natural history of HCV in a cohort of haemophilic patients infected between1961 and 1985. Gut. 2000 Dec;47(6):845-51.
29. Rautou PE, Tatsumi K, Antoniak S, Owens AP 3rd, Sparkenbaugh E,Holle LA, et al. Hepatocyte tissue factor contributes to the hyper-coagulable state in a mouse model of chronic liver injury. J Hepatol.2016 Jan;64(1):53-9.
30. Diaz JA, Wrobleski SK, Alvarado CM, Hawley AE, Doornbos NK, LesterPA, et al. P-selectin inhibition therapeutically promotes thrombus resolution and prevents vein wall fibrosis better than enoxaparin andan inhibitor to von Willebrand factor. Arterioscler Thromb Vasc Biol.2015 Apr;35(4):829-37.
31. Levi M, Keller TT, van Gorp E, ten Cate H. Infection and inflammation

Anticoagulation in the Cirrhotic Patient
Journal of Translational Medicine and Research, 21 (3), 2016 181
and the coagulation system. Cardiovasc Res. 2003 Oct 15;60(1):26-39.
32. Agarwal B, Shaw S, Shankar Hari M, Burroughs AK, Davenport A.Continuous renal replacement therapy (CRRT) in patients with liverdisease: is circuit life different? J Hepatol. 2009 Sep;51(3):504-9.
33. Chua HR, Baldwin I, Bailey M, Subramaniam A, Bellomo R. Circuitlifespan during continuous renal replacement therapy for combinedliver and kidney failure. J Crit Care. 2012 Dec;27(6):744.e7-15.
34. Goonasekera CD, Wang J, Bunchman TE, Deep A. Factors affecting circuit life during continuous renal replacement therapy in childrenwith liver failure. Ther Apher Dial. 2015 Feb;19(1):16-22.
35. Saner FH, Treckmann JW, Geis A, Lösch C, Witzke O, Canbay A, et al.Efficacy and safety of regional citrate anticoagulation in liver transplantpatients requiring post-operative renal replacement therapy. NephrolDial Transplant. 2012 Apr;27(4):1651-7.
36. Hirsh J, Anand SS, Halperin JL, Fuster V. Mechanism of action andpharmacology of unfractionated heparin. Arterioscler Thromb VascBiol. 2001 Jul;21(7):1094-6.
37. Hirsh J, Warkentin TE, Shaughnessy SG, Anand SS, Halperin JL,Raschke R, et al. Heparin and low-molecular-weight heparin: mecha-nisms of action, pharmacokinetics, dosing, monitoring, efficacy, andsafety. Chest. 2001 Jan;119(1 Suppl):64S-94S.
38. Harris EN, Baggenstoss BA, Weigel PH. Rat and human HARE/stabilin-2 are clearance receptors for high- and low-molecular-weightheparins. Am J Physiol Gastrointest Liver Physiol. 2009 Jun;296(6):G1191-9.
39. Johansen KB, Balchen T. Tinzaparin and other low-molecular-weightheparins: what is the evidence for differential dependence on renalclearance? Exp Hematol Oncol. 2013 Aug 8;2:21.
40. Hoy SM, Scott LJ, Plosker GL. Tinzaparin sodium: a review of its usein the prevention and treatment of deep vein thrombosis and pulmonary embolism, and in the prevention of clotting in the extra-corporeal circuit during haemodialysis. Drugs. 2010 Jul 9;70(10):1319-47.
41. Potze W, Adelmeijer J, Porte RJ, Lisman T. Preserved clot formationdetected by the Thrombodynamics analyzer in patients with cirrhosis.Thromb Res. 2015 May;135(5):1012-6.
42. Potze W, Arshad F, Adelmeijer J, Blokzijl H, van den Berg AP, Porte RJ,et al. Routine coagulation assays underestimate levels of antithrombin-dependent drugs but not of direct anticoagulant drugs in plasma frompatients with cirrhosis. Br J Haematol. 2013 Dec;163(5):666-73.
43. Potze W, Arshad F, Adelmeijer J, Blokzijl H, van den Berg AP, MeijersJC, et al. Differential in vitro inhibition of thrombin generation by anticoagulant drugs in plasma from patients with cirrhosis. PLoS One.2014 Feb 4;9(2):e88390.
44. Shatzel J, Dulai PS, Harbin D, Cheung H, Reid TN, Kim J. Safety andefficacy of pharmacological thromboprophylaxis for hospitalizedpatients with cirrhosis: a single-center retrospective cohort study. JThromb Haemost. 2015 Jul;13(7):1245-53.
45. Egan G, Ensom MH. Measuring anti-factor xa activity to monitor low-molecular-weight heparin in obesity: a critical review. Can J HospPharm. 2015 Jan-Feb;68(1):33-47.
46. Lai S, Coppola B. Use of enoxaparin in end-stage renal disease. KidneyInt. 2013 Sep;84(3):433-6.
47. Bechmann LP, Sichau M, Wichert M, Gerken G, Kröger K, Hilgard P.Low-molecular-weight heparin in patients with advanced cirrhosis.Liver Int. 2011 Jan;31(1):75-82.
48. Senzolo M, Rodriguez-Castro KI, Rossetto V, Radu C, Gavasso S,Carraro P, et al. Increased anticoagulant response to low-molecular-weight heparin in plasma from patients with advanced cirrhosis. JThromb Haemost. 2012 Sep;10(9):1823-9.
49. Chowdary P, Adamidou D, Riddell A, Aghighi S, Griffioen A, Priest P,et al. Thrombin generation assay identifies individual variability inresponses to low molecular weight heparin in pregnancy: implicationsfor anticoagulant monitoring. Br J Haematol. 2015 Mar;168(5):719-27. doi: 10.1111/bjh.13193. Epub 2014 Oct 29.
50. Samama MM, Gerotziafas GT. Comparative pharmacokinetics ofLMWHs. Semin Thromb Hemost. 2000;26 Suppl 1:31-8.
51. Atiq F, van den Bemt PM, Leebeek FW, van Gelder T, Versmissen J. Asystematic review on the accumulation of prophylactic dosages of low-molecular-weight heparins (LMWHs) in patients with renal
insufficiency. Eur J Clin Pharmacol. 2015 Aug;71(8):921-9. 52. Salem JE, Sabouret P, Funck-Brentano C, Hulot JS. Pharmacology and
mechanisms of action of new oral anticoagulants. Fundam ClinPharmacol. 2015 Feb;29(1):10-20.
53. Pollack CV Jr, Reilly PA, Eikelboom J, Glund S, Verhamme P, BernsteinRA, et al. Idarucizumab for Dabigatran Reversal. N Engl J Med. 2015Aug 6;373(6):511-20.
54. Eikelboom JW, Weitz JI. New anticoagulants. Circulation. 2010 Apr6;121(13):1523-32.
55. Bauer KA. Recent progress in anticoagulant therapy: oral directinhibitors of thrombin and factor Xa. J Thromb Haemost. 2011 Jul;9Suppl 1:12-9.
56. Gehrie E, Tormey C. Novel oral anticoagulants: efficacy, laboratorymeasurement, and approaches to emergent reversal. Arch Pathol LabMed. 2015 May;139(5):687-92.
57. van Ryn J, Stangier J, Haertter S, Liesenfeld KH, Wienen W, FeuringM, et al. Dabigatran etexilate--a novel, reversible, oral direct thrombininhibitor: interpretation of coagulation assays and reversal of antico-agulant activity. Thromb Haemost. 2010 Jun;103(6):1116-27.
58. Samama MM. Coagulation Assays in Patients with New OralAnticoagulants (NOACs): Why? When? Drug Development Research.2013;74(8):582-6.
59. Božic-Mijovski M, Malmström RE, Malovrh P, Antovic JP4, Vene N,Šinigoj P, et al. Diluted thrombin time reliably measures low to inter-mediate plasma dabigatran concentrations. Ann Clin Biochem. 2016Jul;53(Pt 4):446-51. doi: 10.1177/0004563215599795. Epub 2015Sep 21.
60. Amitrano L, Guardascione MA, Menchise A, Martino R, Scaglione M,Giovine S, et al. Safety and efficacy of anticoagulation therapy with lowmolecular weight heparin for portal vein thrombosis in patients withliver cirrhosis. J Clin Gastroenterol. 2010 Jul;44(6):448-51.
61. Cui SB, Shu RH, Yan SP, Wu H, Chen Y, Wang L, et al. Efficacy andsafety of anticoagulation therapy with different doses of enoxaparin forportal vein thrombosis in cirrhotic patients with hepatitis B. Eur JGastroenterol Hepatol. 2015 Aug;27(8):914-9.
62. Delgado MG, Seijo S, Yepes I, Achécar L, Catalina MV, García-CriadoA, et al. Efficacy and safety of anticoagulation on patients with cirrho-sis and portal vein thrombosis. Clin Gastroenterol Hepatol. 2012 Jul;10(7):776-83.
63. Couturaud F, Sanchez O, Pernod G, Mismetti P, Jego P, Duhamel E, etal. Six Months vs Extended Oral Anticoagulation After a First Episodeof Pulmonary Embolism: The PADIS-PE Randomized Clinical Trial.JAMA. 2015 Jul 7;314(1):31-40.
64. Martinez M, Tandra A, Vuppalanchi R. Treatment of acute portal veinthrombosis by nontraditional anticoagulation. Hepatology. 2014Jul;60(1):425-6.
65. Intagliata NM, Maitland H, Northup PG, Caldwell SH. Treating thrombosis in cirrhosis patients with new oral agents: ready or not?Hepatology. 2015 Feb;61(2):738-9.
66. Kubitza D, Roth A, Becka M, Alatrach A, Halabi A, Hinrichsen H, et al.Effect of hepatic impairment on the pharmacokinetics and pharmaco-dynamics of a single dose of rivaroxaban, an oral, direct Factor Xainhibitor. Br J Clin Pharmacol. 2013 Jul;76(1):89-98.
67. Simonetto DA, Wysokinski WE, Kamath PS. Use of nontraditional anti-coagulants in portal vein thrombosis: a note of caution. Hepatology.2015 Jun;61(6):2119.
68. Senzolo M. Liver: PVT in cirrhosis, not always an innocent bystander.Nat Rev Gastroenterol Hepatol. 2015 Jan;12(1):11-3.
69. Zocco MA, Di Stasio E, De Cristofaro R, Novi M, Ainora ME, PonzianiF, et al. Thrombotic risk factors in patients with liver cirrhosis: correlation with MELD scoring system and portal vein thrombosisdevelopment. J Hepatol. 2009 Oct;51(4):682-9.
70. Mancuso A. An update on the management of Budd-Chiari syndrome:the issues of timing and choice of treatment. Eur J GastroenterolHepatol. 2015 Mar;27(3):200-3.
71. Menon KV, Shah V, Kamath PS. The Budd-Chiari syndrome. N Engl JMed. 2004 Feb 5;350(6):578-85.
72. Sun J, Zhang Q, Xu H, Huang Q, Shen B, Zu M, et al. Clinical outcomesof warfarin anticoagulation after balloon dilation alone for the treatment of Budd-Chiari syndrome complicated by old inferior venacava thrombosis. Ann Vasc Surg. 2014 Nov;28(8):1862-8.

Ecaterina Scãrlãtescu et al
182 Journal of Translational Medicine and Research, 21 (3), 2016
73. Chinnakotla S, Klintmalm GB, Kim P, Tomiyama K, Klintmalm E, DavisGL, et al. Long-term follow-up of liver transplantation for Budd-Chiarisyndrome with antithrombotic therapy based on the etiology.Transplantation. 2011 Aug 15;92(3):341-5.
74. Gómez Cuervo C1, Bisbal Pardo O, Pérez-Jacoiste Asín MA. Efficacyand safety of the use of heparin as thromboprophylaxis in patientswith liver cirrhosis: a systematic review and meta-analysis. ThrombRes. 2013 Oct;132(4):414-9.
75. Barclay SM1, Jeffres MN, Nguyen K, Nguyen T. Evaluation of pharma-cologic prophylaxis for venous thromboembolism in patients withchronic liver disease. Pharmacotherapy. 2013 Apr;33(4):375-82.
76. Cui J, Wu B, Liu C, Li Z. A systematic review and adjusted indirectcomparison of oral anticoagulants. Orthopedics. 2014 Nov;37(11):763-71.
77. Bauersachs RM. Use of anticoagulants in elderly patients. ThrombRes. 2012 Feb;129(2):107-15.
78. Abdel-Salam OM, Baiuomy AR, Ameen A, Hassan NS. A study ofunfractionated and low molecular weight heparins in a model ofcholestatic liver injury in the rat. Pharmacol Res. 2005 Jan;51(1):59-67.
79. Dittmeier M, Kraft P, Schuhmann MK, Fluri F, Kleinschnitz C.Pretreatment with rivaroxaban attenuates stroke severity in rats by adual antithrombotic and anti-inflammatory mechanism. ThrombHaemost. 2016 Apr;115(4):835-43.
80. Yang ZJ, Sheth SH, Smith CH, Schmotzer AR, Lippello AL, Al-KhafajiA, et al. Plasma from chronic liver disease subjects exhibit differentialability to generate thrombin. Blood Coagul Fibrinolysis. 2015 Oct;26(7):844-7.
81. Bates SM, Weitz JI. Coagulation assays. Circulation. 2005 Jul 26;112(4):e53-60.
82. Tripodi A, Chantarangkul V, Primignani M, Fabris F, Dell'Era A, Sei
C, et al. The international normalized ratio calibrated for cirrhosis(INR(liver)) normalizes prothrombin time results for model forend-stage liver disease calculation. Hepatology. 2007 Aug;46(2):520-7.
83. Werner KT, Sando S, Carey EJ, Vargas HE, Byrne TJ, Douglas DD, etal. Portal vein thrombosis in patients with end stage liver diseaseawaiting liver transplantation: outcome of anticoagulation. Dig Dis Sci.2013 Jun;58(6):1776-80.
84. Cai M, Zhu K, Huang W, Meng X, He K, Zhou B, et al. Portal veinthrombosis after partial splenic embolization in liver cirrhosis: efficacyof anticoagulation and long-term follow-up. Journal of vascular andinterventional radiology. J Vasc Interv Radiol. 2013 Dec;24(12):1808-16.
85. Lai W, Lu SC, Li GY, Li CY, Wu JS, Guo QL, et al. Anticoagulation therapy prevents portal-splenic vein thrombosis after splenectomywith gastroesophageal devascularization. World J Gastroenterol. 2012Jul 14;18(26):3443-50.
86. Widén A, Rolando N, Manousou P, Rolles K, Davidson B, Sharma D,et al. Anticoagulation after liver transplantation: a retrospective auditand case-control study. Blood Coagul Fibrinolysis. 2009 Dec;20(8):615-8.
87. Francoz C, Belghiti J, Vilgrain V, Sommacale D, Paradis V, Condat B, etal. Splanchnic vein thrombosis in candidates for liver transplantation:usefulness of screening and anticoagulation. Gut. 2005 May;54(5):691-7.
88. Lee SJ, Uhm JS, Kim JY, Pak HN, Lee MH, Joung B. The safety andefficacy of vitamin K antagonist in patients with atrial fibrillation andliver cirrhosis. Int J Cardiol. 2015 Feb 1;180:185-91.
89. Efird LM, Mishkin DS, Berlowitz DR, Ash AS, Hylek EM, Ozonoff A, etal. Stratifying the risks of oral anticoagulation in patients with liver disease. Circ Cardiovasc Qual Outcomes. 2014 May;7(3):461-7.

Journal of Translational Medicine and Research, 21 (3), 2016 183
ORIGINAL PAPER
Copyright © Celsius Publishing House
J. Transl. Med. Res 2016;21(3):183-192 DOI: 10.21614/jtmr-21-3-92
1Institute of Biochemistry of the Romanian Academy, Bucharest, Romania2Center of Digestive Diseases and Liver Transplantation, Fundeni Clinical Institute,Bucharest, Romania3Romanian Academy, Bucharest, Romania
Received: 20.06.2016Accepted: 30.08.2016
ABSTRACT
The human pancreatic beta cell 1.1B4 is a novel human hybrid cell line formed by electrofusionof primary culture of human pancreatic islets with PANC-1. Our analysis of functional parametersof this cell line (insulin expression and secretion, glucose responsiveness, staining with humanspecific antibodies) confirmed the human identity and the inherited properties of functional betacells. Irradiation with HDGP (High Density Green Photons) of two beta pancreatic cells lines(1.1B4 and INS-1E) and of human pancreatic islets induced modifications in insulin and pro-insulin expression and secretion.Key words: human pancreatic beta cells 1.1B4, human pancreatic islets, HDGP, insulin
INTRODUCTION INTRODUCTION
In mammalian organisms, the only hypoglycemic hormone is insulin, produced in Beta cells of pancreatic Langerhans islets. The most part of isletsare Beta cells (65-90%, forming the core of the islet) (1).
Diabetes is characterized by a masive decrease of beta cells number correlated with functional impairement. To cure diabetes, at present, thebest therapeutic possibility is pancreatic islets transplantation. They are purchased from dead donors. After isolation, islets are difficult to maintainin culture for long time and their in vitro proliferation rate is very low (2).
The Beta cells are rather delicate and susceptible to functional deficitsor to stressful actions as isolation and trasplantation. The maintenance ofbeta cells viability and function is critically important.
The aim of this study was to find if the HDGP irradiation might induce, in
Corresponding author:Prof. dr. Liliana PaslaruFundeni Clinical Institute022328, Bucharest, RomaniaE-mail: [email protected]
Functional Characterization of 1.1B4 - A Novel Human InsulinReleasing Cell Line and Effect of HDGP (High Density GreenPhotons) Irradiation on Beta Pancreatic Cells and HumanPancreatic Islets
Petruta Alexandru1, Liliana Paslaru2, Simona Dima2, Anca Nastase2, Laura Stoichita2, Sorin Comorosan2,3, Irinel Popescu2,3

Petruta Alexandru et al
184 Journal of Translational Medicine and Research, 21 (3), 2016
normal culture conditions, functional modificationsin pancreatic beta cells and in pancreatic islets.
Recent studies revealed that light may be used formodulation and control of biological function, in the production of biopharmaceuticals and in bio-medicine (3).
Our previous studies demonstrated that irradiationwith High Density Green Photons (HDGP) have complexpleiotropic effects on matter: generation of a new localmacromolecular architecture with a protective roletoward subsequent aggressions, modification of trans-membranar transport, etc (4-8).
Stimulation of cell proliferation under green lightLED irradiation and various effects of green lightlaser irradiation on different substrates were alsodescribed (9-13).
MATERIALS AND METHODSMATERIALS AND METHODS
Cell cultures
A human pancreatic 1.1B4 hybrid cell line, a ratinsulinoma cell line INS-1E and human pancreatic isletswere used in our study for characterization and comparison respectively and for HDGP irradiationeffects. INS-1E cells were a kind gift of Peter van derSluijs (Department of Cell Biology, University MedicalCenter, Utrecht, Netherlands) while 1.1B4 cells wereobtained from ECACC (European Collection of CellCultures).
The human pancreatic beta cell 1.1B4 is a novelhuman hybrid cell line formed by electrofusion of primary culture of human pancreatic islets with PANC-1. It is an insulin secreting cell line, developed byMc Cluskey et al (14) with application in the study of pancreatic cell biology (15). Both cell lines weremaintained in RPMI-1640 medium containing 11,1mM glucose supplemented with 10% FBS and 1% anti-biotics.
Human primary pancreatic islets were obtainedfrom Prodo Laboratories Inc USA. PIM (S), PIM (ABS),PIM (G) culture media and experimental protocols werealso purchased by Prodo Laboratories.
The islets were cultured on inserts in 24 well platesor in suspension in different type of media (PIM, CMRL,RPMI) and irradiated with HDGP.
Immunostaining
1.1B4 and INS1E cell lines and the pancreatic isletswere plated on 3.5 mm poly-L-lysine – coated cover
slips in RPMI-1640 or in CMRL medium. After 48h, thecells were either starved in media without glucose for 2hours and then stimulated with 2.8 mM and 28 M glucose or cultured in media with 11.1 mM glucose.During insulin secretion the cells and islets were irradi-ated with HDGP for different periods of time (minutes).Cells and islets were fixed with 4% para-formaldehydeand permeabilized with Triton-X 100 treatment. Theprimary antibodies were: anti-insulin (Santa Cruz, C-12), anti-insulin (Santa Cruz, H86, Cell Signaling L6B10and AbCam 181547), anti-peptid C (AbCam 8297) anti-calnexin (Santa Cruz), anti-syntaxin 4 (Santa Cruz, C16)anti-GLUT2 (Santa Cruz, C19) and GRP94 (Santa Cruz sc 32249) Nuclei were stained with DAPI. The secondaryantibodies were conjugated with AlexaFluor 488 orAlexaFluor 594 (Invitrogen). The cells were analyzed byApoTome (Zeiss) microscope.
ELISA
For the analysis of insulin and proinsulin secretion,1.1B4, INS-1E cells and pancreatic islets were culturedin 6 - or 24 well plates, starved for 2h and than stimu-lated with 14 mM, and 28 mM glucose for 24h. The culture medium and the cells were harvested for ELISAtest (MERCODIA ELISA kit for human insulin and pro-insulin and mouse/rat insulin and pro-insulin).
Western blot
For western blotting the cells (stimulated with glucose and irradiated or not with HDGP) were lysedand the same protein quantity was loaded on poly-acrylamide gels. The proteins were transferred on anitrocellulose membrane and immunoblotted withanti-insulin antibodies (H-86, insulin B, Santa Cruz, andL6B10) and C-peptid C, (Cell Signalling).
High density green photon source and irradiation
Cells under different culture conditions and the pancreatic islets were irradiated with a source of HDGP.As a source of HDGP, a pure monochromatic light emitting diodes (LED) was used (16V, 20W, 1000 lumens,Everredtronics, E 20 WG 120 C). Diodes were mountedon ventilated copper radiators. A monochromatic greenlight with absorption peak centered at λ-520 nm wasobtained, with intensities up to 140 mW/cm2, spectralwidth 10 nm. Time of cells irradiation varied between 1-60 min, at different intervals of time (e.g 5 minutes, 10min, 2 x 10 minutes /24 hrs of incubation).

Functional Characterization of 1.1B4 - A Novel Human Insulin Releasing Cell Line and Effect of HDGP Irradiation on Beta Pancreatic Cells and Human Pancreatic Islets
Journal of Translational Medicine and Research, 21 (3), 2016 185
RESULTS RESULTS
Characterization of PANC 1.1B4 cell line
1. Cell cultures analysis demonstrated that 1.1B4cells grew as monolayers, maintained a stable growthrate and the phenotype during passages as previouslydescribed (14).
2. Immunofluorescence experiments demonstratedthat 1.1B4 cells exhibitcytoplasmic positive staining forhuman insulin (using different human anti-insulin anti-bodies), C-peptide, calnexin, syntaxin 4, GLUT2 andGRP94 (fig. 1 a,b,c, fig. 4).
3. For comparation, a rat insulinoma beta cellsline INS-1E4 stained for insulin, calnexin, syntaxin ispresented (fig. 2, a,b).
4. The insulin secretory response to different con-centrations of glucose demonstrated the functionalintegrity of 1.1B4 cells. Comparative experimentsrevealed that for the same glucose concentration, theinsulin secretion of 1.1B4 is much lower than in INS-1E
(fig. 3a). Stimulation of 1.1B4 cell lines with increasingglucose concentrations, 2.8, 14 and 28 mM showed anincreasing level of insulin, when measured at 24h (fig. 3b).
5. In our study we observed an interesting behaviorof 1.1B4 cells: in certain culture conditions appearsaselective enhancement of insulin expression. This obser-vation was demonstrated by staining the cells with 3 different anti-insulin antibodies (fig. 4 a,b,c).
Additionaly, to demonstrate this peculiar aspectinsulin expression of insulin in of 1.1B4 culture we present images where in the same culture, calnexinexpression is almost identical but insulin expression isvariable (fig. 5 a,b,c).
The effect of HDGP irradiation on 1.1B4 and INS-1E beta cells
In our experimental conditions, after HDGP irradia-tion a modification of intracellular and extracellularinsulin level was observed in 1.1B4 and INS-1 cells.
a
b
C
Figure 1 - Insulin, calnexin (a), insulin, syntaxin (b), GLUT2 and GRP 94 (c) expression in 1.1B4 cells

Petruta Alexandru et al
186 Journal of Translational Medicine and Research, 21 (3), 2016
a
b
Figure 2 - Insulin, calnexin (a) and insulin syntaxin exression in INS-1E rat insulinoma cells
Figure 3 - (a) Comparative ELISA analysis of insulin secretion in 1.1B4 and INS-1E cell lines. (b) Determination by ELISA of insulin secretion of 1.1B4 cells at 24 hrs after stimulation with 2.8, 14 and 28 mM glucose (the second phase of secretion)
a b
Figure 4 a - Selective expression of insulin stained with 3 different antibodiesInsulin B (antibodies Santa Cruz) InsulinH86 (antibodies Santa Cruz)

Functional Characterization of 1.1B4 - A Novel Human Insulin Releasing Cell Line and Effect of HDGP Irradiation on Beta Pancreatic Cells and Human Pancreatic Islets
Journal of Translational Medicine and Research, 21 (3), 2016 187
Figure 4 c - Selective expression of insulin stained with 3 different antibodies (c) Insulin (Abcam antibodies 18154), C-peptid (Abcam antibodies 8297 )
Figure 4 b - Selective expression of insulin stained with 3 different antibodiesInsulin (Cell Signalling antibodies L6B10), C-peptid (Cell Signalling antibodies)
Augmentation of insulin was detected by immuno-fluorescence (fig. 6 a,b) and Western Blotting (fig. 7 a,b, c).
The effect of HDGP irradiation on humanprimary pancreatic islets
Microscopy analysis and dithizone staining demon-strated the integrity of pancreatic islet (fig. 8).
Double immunofluorescence staining of whole islets
for insulin/glucagon demostrated the functionality ofislets (fig. 9).
Irradiation of pancreatic islets with HDGP inducedaugmentation of intracellular and extracelllar insulinand pro-insulin (fig. 10 a,b).
Augmentation under 28 mM glucose suggests a correct processing of proinsulin toinsulin and C-peptid and a possible protective effect of green lightin chronic hyperglycemia.

Petruta Alexandru et al
188 Journal of Translational Medicine and Research, 21 (3), 2016
Figure 5 - Identical expression of calnexin but selective expression of insulin in 1.1B4 cells (a,b,c)
a
b
c
Figure 6 a - HDGP effects on 1.1B4 cell line

Functional Characterization of 1.1B4 - A Novel Human Insulin Releasing Cell Line and Effect of HDGP Irradiation on Beta Pancreatic Cells and Human Pancreatic Islets
Journal of Translational Medicine and Research, 21 (3), 2016 189
Figure 6 b - HDGP effects on INS-1E cell line
Figure 7 - Western blot analysis of insulin stimulation in INS-1E (a,b) and 1.1B4 (c) cells irradiated with HDGP
a b c
d e f
Figure 8- Human pancreatic islets cultured on inserts (a,b,f ), in suspension (c,d,e) and dithizone staining (d,e)

Petruta Alexandru et al
190 Journal of Translational Medicine and Research, 21 (3), 2016
Figure 9 - Immunofluorescence staining of whole islets for insulin (green), glucagon (red) and nuclei (blue)
Figure 10 - Intracelllar and extracelllar modfications of insulin (a) and pro-insulin in control and HDGP irradiated human primary pancreatic islets (b)
a b

Functional Characterization of 1.1B4 - A Novel Human Insulin Releasing Cell Line and Effect of HDGP Irradiation on Beta Pancreatic Cells and Human Pancreatic Islets
Journal of Translational Medicine and Research, 21 (3), 2016 191
CONCLUSIONSCONCLUSIONS
Our results regarding the characterization of 1.1B4 cells (culture and growth, insulin expression andsecretion, staining with human specific antibodies, glucose responsiveness, etc) confirmed the human identity and the inherited properties of functional betacells.
We consider that the 1.1B4 cell line presents goodattributes which recommend it to be used for furtherstudies of human beta cells and pancreatic islet trans-plantation.
The mechanism of stimulatory action of green photons on cellular systems is still unknown andremains to be elucidate. Nevertheless, our preliminaryresults present a stimulation of insulin expression byHDGP irradiation in two beta cell lines. One possibleexplanation could be that modification of insulin levelappears as a result of green light energy interactionwith voltage-gated ion channels. Consequently, we suggest that the study of this type of HDGP treatmenthas to be continued; it could be used with promisingresults in cell cultures, prior to transplantation or inother regenerative medicine procedures.
Founding source
This study was financially supported by theRomanian Program for Research, Development and
Innovation, research grant PN ID 139/5.10.2011, PNII-PT-PCCA 90/2011 and POSDRU/186/3.2/S/155295.
Acknowledgements
We are indebted to Dr. Norica Nichita for her criticalreading of the manuscript.
REFERENCESREFERENCES
1. Skelin M, Rupnik M, Cencic A. Pancreatic beta cell lines and theirapplications in diabetes mellitus research. ALTEX. 2010;27(2):105-13.
2. Scharfmann R, Rachdi L, Ravassard P. Concise review: in search ofunlimited sources of functional human pancreatic beta cells. Stem CellsTransl Med. 2013 Jan;2(1):61-7. doi: 10.5966/sctm.2012-0120. 3.Kim B, Lin MZ. Optobiology: optical control of biological processes viaprotein engineering. Biochem Soc Trans. 2013 Oct;41(5):1183-8. doi: 10.1042/BST20130150.
4. Comorosan S, Polosan S, Jipa S, Popescu I, Marton G, Ionescu E, etal. Green light radiation effects on free radicals inhibition in cellular andchemical systems. J Photochem Photobiol B. 2011 Jan 10;102(1):39-44. doi: 10.1016/j.jphotobiol.2010.09.003. Epub 2010 Sep 21.
5. Comorosan S, Polosan S, Popescu I, Ionescu E, Mitrica R, CristacheL, et al. State Structural studies on serum albumins under green lightirradiation. Eur Biophys J. 2010 Oct;39(11):1483-91. doi: 10.1007/s00249-010-0606-y. Epub 2010 May 16.
6 . Farcasanu IC, Mitrica R, Cristache L, Nicolau I, Ruta LL, Paslaru L, etal. Optical manipulation of Saccharomyces cerevisiae cells reveals thatgreen light protection against UV irradiation is favored by low Ca2+and requires intact UPR pathway. FEBS Lett. 2013 Nov 1;587(21):3514-21. doi: 10.1016/j.febslet.2013.09.008. Epub 2013 Sep 19.
7. Mitrica R, Popescu I, Paslaru L, Badila D, Polosan S, Cristache L, et al.High-density green photons effects on NaCl solutions detected by redblood cells membranes. Digest Journal of Nanomaterials andBiostructures. 2012;7(1):227-35.
8. Comorosan S, Popescu I, Polosan S, Parvu C, Ionescu E, Paslaru L, etal. Conformational changes and metastable states induced in proteins
Figure 11 - Intracelllar and extracelllar modfications of glucagon in control and HDGP irradiated human primary pancreatic islets stimulated with glucose: 14 mM (a) and 28 mM (b)
a b

Petruta Alexandru et al
by green light. Eur. Phys. J. B. 2015;88:8.9. Paslaru L, Nastase A, Stefan L, Florea R, Sorop A, Ionescu E, et al.
Stimulatory and possible antioxidant effects of High Density GreenPhotons (HDGP) on cellular systems. J Med Life. 2014 Oct-Dec;7(4):619-22.
10. Halevy O, Piestun Y, Rozenboim I, Yablonka-Reuveni Z. In ovoexposure to monochromatic green light promotes skeletal muscle
cell proliferation and affects myofiber growth in posthatch chicks.Am J Physiol Regul Integr Comp Physiol. 2006 Apr;290(4):R1062-70.
11. Rozenboim I, El Halawani ME, Kashash Y, Piestun Y, Halevy O. Theeffect of monochromatic photostimulation on growth and develop-ment of broiler birds. Gen Comp Endocrinol. 2013 Sep 1;190:214-9.doi: 10.1016/j.ygcen.2013.06.027. Epub 2013 Jul 15.
12. AlGhamdi KM, Kumar A, Moussa NA. Low-level laser therapy: a useful technique for enhancing the proliferation of various cultured
cells.Lasers Med Sci. 2012 Jan;27(1):237-49. doi: 10.1007/s10103-011-0885-2. Epub 2011 Jan 28.
13. Anwer AG, Gosnell ME, Perinchery SM, Inglis DW, Goldys EM. Visible532 nm laser irradiation of human adipose tissue-derived stem cells:effect on proliferation rates, mitochondria membrane potential andautofluorescence. Lasers Surg Med. 2012 Nov;44(9):769-78. doi:10.1002/lsm.22083. Epub 2012 Oct 9.
14. McCluskey JT, Hamid M, Guo-Parke H, McClenaghan NH, Gomis R,Flatt PR. Development and functional characterization of insulin-releasing human pancreatic beta cell lines produced by electrofusion.J Biol Chem. 2011 Jun 24;286(25):21982-92. doi: 10.1074/ jbc.M111.226795. Epub 2011 Apr 22.
15. Natalicchio A. Culture, passaging, nucleic acids and proteins extraction1.1B4 cell line. Universita degli studi di Bari Aldo Moro-Corso in biotec-nologie applicate alla fisiopatologia endocrina. Anno Accademico.2015/2016.
192 Journal of Translational Medicine and Research, 21 (3), 2016

Journal of Translational Medicine and Research, 21 (3), 2016 193
ORIGINAL PAPER
Copyright © Celsius Publishing House
J. Transl. Med. Res 2016;21(3):193-200 DOI: 10.21614/jtmr-21-3-93
Protective Effect of Green Light Against the DeleteriousEffects of UV Irradiation on Cellular Systems
Silviu Polosan1, Irinel Popescu2,3, Ileana Farcasanu4, Sorin Avramescu4, Elena Ionescu3, Liliana Paslaru2, Marian Apostol5 and Sorin Comorosan6
Corresponding author:Prof. Dr. Sorin ComorosanE-mail: [email protected]
ABSTRACT
A different type of experimental set-up is developed, in which cellular systems irradiated withultraviolet (UV) light are protected through a simultaneous irradiation with high density greenphotons. The noxious UV-effects and their protection by green light (GL) are investigated onSaccharomyces cerevisiae (Sc) – cells, cultivated and measured under rigorous conditions. Aseries of physical determinations, atomic force microscopy, impedance spectroscopy and circular dichroism, revealed that the alterations induced by UV in the cellular culture were clearly reduced through the simultaneous GL irradiation. The biochemical activities of superoxide dismutase and catalase that “scavenge” free radicals in eukaryotic cells, severelydamaged by UV, were almost completely restored by a previously protected GL- irradiation. Thefree radicals inhibition by high density photons, in the green band of visible spectrum, as a firstrevealed antioxidant effect of electromagnetic (EMF)-field, is analyzed in the context of a suggested tentative physical model.Key words: free radicals, green light irradiation, protein polarization
INTRODUCTION INTRODUCTION
The significant damages induced by ultraviolet (UV) radiation at biologicaland environmental level turned lately into a debated social concern (1) and ahighlight scientific medical problem (2). The noxious effects are discussed in biol-ogy by the oxidative stress and the free radicals generation. In chemistry a “freeradical” is defined as an atom or molecule with an unpaired electron. One of theforms of reactive oxygen species (ROS) is the “activated” oxygen singlet state (O-O:), with the resulted oxidative damage, described in chemical lingo. At the lipidslevel chain breakage and cross-linkage, at the protein level fragmentation and
Received: 15.06.2016Accepted: 24.08.2016
1National Institute of Materials Physics, Bucharest, Romania3Fundeni Clinical Institute, Bucharest, Romania 3Romanian Academy of Medical Sciences4Faculty of Chemistry, University of Bucharest, Romania5Department of Theoretical Physics, Institute of Nuclear Physics, Magurele, Romania6Interdisciplinary Research Group, Romanian Academy, Fundeni Clinical InstituteBucharest, Romania

194 Journal of Translational Medicine and Research, 21 (3), 2016
Silviu Polosan et al
aggregation, at the nucleic acids level deletions andmutations are the main described effects.
But a biophysical mechanism underlying all theseUV-damaging effects is still lacking. Eukaryotic cellshave developed a series of defense mechanisms tocope with UV-aggression, mainly “scavenger enzymes”that neutralize free radicals. Regarding exogenous protection, our resources are scarce and less efficient,since we fight free radicals mainly with chemicals. Ourgroup reported a series of different results in this field,revealing an antioxidant effect of electromagnetic field(EMF). We use the term different in the meaning of thephysicist Philip Anderson (3) instead of the ubiquitous“new”, prevailing in modern scientific literature. A phenomenon/reaction/property is different when itplaces what is already known in an alternative perspec-tive. The occurrence of EMF as a new player will changethe relationship between the antioxidant effectsalready present. The present study focuses mainly onthis difference. We developed a special experimentusing green light (GL) irradiation sources (powerfulmonochromatic light-emitting diodes) that generatehigh-density green photons (HDGP). The protectiveexperimental set-up represents UV-sample irradiation,perpendicular up-bottom, with a simultaneous GL-sample irradiation, perpendicular bottom-up. Ourresults revealed an antioxidant effect of GL on cells subjected to lethal doses of UV, proved on cell viability(4) and a clear GL-protective effect, proved on the structure of proteins subjected to denaturing doses ofUV (5). We report here a chemical and physical investi-gation, as a new basis for the GL-protective effects, ona laboratory Saccharomyces cerevisiae (Sc) strain. Atheoretical analysis of the biological and ecologicalimplications raised by our experimental results is developed.
MATERIALS AND METHODSMATERIALS AND METHODS
UV and green light irradiation
2 mL cells (2 X 108/mL) were irradiated on Petri dishes (φ 30 mm). The light beam was collimated tocover the entire surface of the target. UV irradiationwas carried out using a Vilbert Lourmat UV lamp,model VL-204 G, 16 W, emitting at λ = 254 nm. A spe-cial geometry is arranged in order to deliver irradiationfluxes at 11.0 J m-2 s-1, in set-ups of 4 min exposure.The GL irradiation was carried out with 1 light-emitting-diode (16 V, 200 W, 1000 lumens, Ever Red Tronics, E20Wg 120C) mounted on a copper ventilated radiator. Acollimated monochromatic light λ = 520 nm with 15
mW/cm intensity, 95 mV incident on the target area was used. The protective experimental set-up represents UV-sample irradiation, perpendicular up-bottom, with a simultaneous GL-sample irradiation,perpendicular bottom-up.
Strains and culture conditions
The Saccharomyces cerevisiae strain used in thisstudy BY4741 (MATa; his3Δ1; leu2Δ0; met15Δ0; ura3Δ0)was obtained from EUROSCARF (www.euroscarf.de).Strains were grown in standard YPD or SD (syntheticdextrose) medium supplemented with the necessaryamino acids. Overnight pre-cultures were inoculated infresh media at density 106 cells/mL, then grown withshaking (200 rpm, 28°C) to midlogarithmic phase (5 x106 cells/mL) in SD medium. Cells were washed with 0.1M MES/Tris (2-N-morpholino ethanesulfonic acid/2-amino-2-hydroxymethyl-propane-1,3-diol), pH 6.5and resuspended in SD medium to 2 x 108 cells/mL. Cellgrowth was checked at time intervals by determiningoptical density of cellular suspension at 660 nm(Shimadzu UV-vis spectrophotometer, UV mini 1240).
Atomic force microscopy
20 µL of cellular suspension, 108 mL-1 in SDC (synthetic dextrose complete) medium, were placedon a quartz plate and slowly evaporated at room temperature. The taping mode was selected as themost suitable for imaging of soft biological samples.The AFM- NT-MDT NTEGRA Prima instrument wasused.
Impedance spectroscopy
A Zahner IM6 Khronach (Germany) electrochemicalunit with <0.0025% frequency stability was used, witha miniaturized electrochemical cell (50µl) with two platinum electrodes bands (1mm width, 0.1 mm thick-ness). The Cole-Cole plot reveals the dependence atlow values for the in-phase and out-of-phase compo-nents of impedance. The main parameters are RΩ-solution resistance, Rct-charge transfer resistance andCd-double layer capacity.
Circular dichroism
Measurements were performed on a Jasco J815dichroism equipment, using a water-cooled thermos-tated Peltier device with 0.1°C accuracy, in the 163-900nm range, on Hellma Suprasyl quartz cuvette 0.1 cm

Journal of Translational Medicine and Research, 21 (3), 2016 195
Protective Effect of Green Light Against the Deleterious Effects of UV Irradiation on Cellular Systems
path, with a 108 cell solution in deionized water. In orderto obtain the dichroism signal from intracellular proteins of cells with a known hard membrane as Sc-cells, the cellular culture was previously immerged in10 mL bi-distilled water for 10 minutes.
Enzyme assay
For enzymatic assays, cells were washed with 0.1 MMES/Tris, pH 6.5, and concentrated to 1 x 109 cells/mL.Aliquots (100 µL) were prepared in 1.5 mL tubes, andcell lysis was achieved with acid-washed glass beads(Sigma) by vortex mixing (3 min, 4°C). Cellular debriswas removed by two centrifugation steps (10,000 rpm,2 min, 4°C). The supernatant was collected after eachspin, and the resultant crude lysate was assayed.Enzyme activity was normalized to total cell protein,determined by Bradford method (6). SOD (superoxidedismutase) - activity was determined as described in(7). CAT (catalase) – activity was determined usingSigma Catalase Assay Kit. The hydrogen peroxide sub-strate remaining after the action of catalase is checkedspectrophotometrical at 520 nm. Glyceraldehyde-phosphate dehydrogenase (GPDH) is determined asdescribed in (8).
RESULTS RESULTS
Atomic Force Microscopy (AFM) is a powerful tech-nique used to obtain images of cells at high resolution.The technique may uncover physical properties in thecell walls surroundings, as well as subtle biochemicaldetails concerning cell walls polysaccharide surface andinner layers microtubules protein structure. We haveapplied AFM for revealing the Sc- cell wall transforma-tion induced by UV- irradiation and by GL- protection.The measurements were performed on evaporated cellsuspension at room temperature in air, according to themethod used for electroporation (9).
Cell membranes act as physiological barriers to thesurrounding medium. Extensive studies on the bilayerstructures in the cellular proteins walls revealed complex mechanisms linked to the liquid contact withthe bilayer, the location close to the hydrophobic bilayer core and the asymmetry in density distributionas result of molecular dynamics. Cellular water, as apolar molecule, may cross the cell membrane by osmosis. Due to this process, in our control samples,under the slow room temperature evaporation water isexcluded by diffusion outside the cell. As a consequencedeflections are observed at the cellular walls level (fig. 1a). Under UV-irradiation, the membranes inner
layers proteins are unfolded, through a well-studied bio-chemical mechanism. The unfolded process grows progressively, devoid of ruptures. Therefore the surfaceof the UV-irradiated sample appears smooth and rounded (fig. 1b). This interpretation of the proteinsunfolding mechanism is consistent with the CD measurements, performed in similar experimental conditions. Under GL, the membrane inner layers proteins are only partially unfolded, leaving more cellular canaliculi open (fig. 1c).
a
b
c
Figure 1- Effects of Sc-cells irradiations with UV and GL. a) AFM- 3D image of a control sample. Under evaporation the waterleaves the cellular structures, creating holes in the cells surfaces. b) AFM- 3D image of an UV irradiated sample. UV irradiation will
preclude water evaporation (liquid holding recovering kinetics) due to the cells membranes protein modifications. The cellular surfaces
appear swollen and rounded. c) AFM- 3D image of an UV+GL irradiated sample. The cellular structure under GL protection
exhibits a water depleted surface close to the control

196 Journal of Translational Medicine and Research, 21 (3), 2016
Silviu Polosan et al
Our results correlate with the now classic observa-tions of Fröhlich, concerning coherent electrically polarlongitudinal vibration in biological systems (10). Thesevibrations may generate endogenous (EM)-fields, thatrecently have been detected in a broad frequency spec-trum. Coupling the electromagnetic (EM)-fields with theUV and GL photons may generate energetic distur-bances, resulting in local nanomechanical displace-ments. Pelling (11) detected these phenomena on Sc-cell membranes by AFM, a result that may be connect-ed with our observed AFM- cell membranes modifica-tions.
Electrical Impedance Spectroscopy (EIS)
Recent advances in impedance spectroscopy, basedon cellular technologies, have provided physical type ofinformation concerning cellular long-term behavior(12). We used electrical impedance spectroscopy (EIS)to reveal transport properties of ions across cellularmembranes, at a fixed applied potential in the low frequency domain (100 KHz). The involved model considers cell membranes as RC-circuits and the inter-nal medium as cellular resistance. Under UV-irradiationthe complex impedance (Z*=Z′−iZ″) of control sampledecreases significantly, as the charge current increases.This is the effect of free radicals generation under
UV irradiation. During GL-irradiation the compleximpedance takes intermediary values, revealing a tendency to restore normal conditions (fig. 2), as a consequence of the antioxidant effect of GL.
Since our results reveal differences in the low frequency domain, the electrical processes are duemainly to membrane transport property and less to theintracellular environment (table 1).
We investigate also the electrical impedance of thecellular lysates, irradiated with GL, in order to detect theprotein structure modifications that may account for therecorded UV- protective effects. We represent theresults by the conventional Bode plot: the absolutevalue of the impedance (IZI) and the phase shift (θ) areplotted with log frequency. A sharp decrease of cellularlysate impedance is observed after GL- irradiation (fig. 3a) as well as a net modification of phase angle
Figure 2 - Impedance plots in the complex plane for Sc-cells suspension. The inlet represents the complex impedances of control sample, UV and UV+GL irradiated cells samples. Impedance values for the UV+GL irradiated cells show intermediate levels, between the control sample and UV irradiated cells, revealing a
protective effect of GL against UV-irradiation
Table 1- Impedance parameters for the UV and UV + GL samples
Impedance (Ω) Sample UV UV+GL
RΩ 928 894 905
RΩ+Rct 987 952 963
RΩ+Rct-2σ2Cd 1023 975 1003
RΩ+Rct/2 957 923 934

Journal of Translational Medicine and Research, 21 (3), 2016 197
Protective Effect of Green Light Against the Deleterious Effects of UV Irradiation on Cellular Systems
(fig. 3b) indicating a shift toward a pseudo capacitybehavior, due to the orientation of polarized proteins on the electrode surface. All these results, well corrobo-rated with the circular dichroism data, clearly suggestthe protein polarization effect under GL - irradiation(generation of P* - polarized protein as reported previously (13).
Circular dichroism
Circular dichroism determines the difference inabsorbance between the L (left) and R (right) circularlypolarized light components [ΔA= (AL-AR)] reported interms of ellipticity (θ) in degrees, (θ)=tan-1(b/a), where band a are the minor and major axes of the resultingellipse, with θ=32.98 ΔA. The main unit used in proteinsstudies is MRE (mean residue ellipticity), the molarellipticity of the molecules divided by the number ofmonomer units, computed as MRE = θ/10 rl, where θ isthe recorded CD (mdeg) r - the number of amino-acidsresidues and l - the path length (cm) of the specter cell.From it the α-helix content may be computed by refer-ring the mean residue ellipticity for a helix of r-amidesto the mean residue ellipticity of an infinite helix, oralternatively by fitting the recorded CD - curves with aspecific Provencer-Glockner soft. This is the standardtechnique to analyze protein CD-spectra.
Conformational changes under UV-irradiation and(UV+GL)- irradiation are reflected in the CD spectra ofyeast cells. These spectra exhibit a negative band at 224nm characteristic for the α-helix structure and a positiveband at 197 nm due to π-π* transition. The UV- irradia-tion induces an unfolding process altering the geometryof polypeptide backbones and accordingly decreaseselipticity. Clear differences were observed, particularly
within the regions of 195 nm and 222 nm (fig. 4)recorded.
For evaluation of the yeast sample circular dichroismthe CONTIN3 method was used. This algorithm usesridge regression to fit a linear combination of spectra ofknown composition to match a spectrum of unknowncomposition. The CD spectra of 16 proteins whose secondary structures are known from X-ray diffractiondata.
The protein secondary structures derived from thisfit are alpha-helix, beta-strands and turns. The typicalstandard deviation for this fit is 0.06.
In our case, the MRW for the yeasts is 107.13 Da,sample concentration C = 0.0012 mg/ml with 171residues. With these data we present the CD fitting for
Figure 3 - a) Bode diagram: impedance modulus vs frequency of Sc- cellular lysate under GL- irradiation. b) Bode diagram: phase vs frequency of Sc- cellular lysate under GL- irradiation
a b
Figure 4 - Recording of circular dichroism in Sc-cells UV - irradiation induced a cellular protein unfolding
with a decrease of π-π* and n→π* transitions. The MRE is drastically reduced. The protection effect of GL is clear

198 Journal of Translational Medicine and Research, 21 (3), 2016
Silviu Polosan et al
the (UV+GL) irradiated cells (fig. 5a) and the CD fittingfor the U-irradiated cells (fig. 5b).
The fractional composition of cellular lysate secondary structure in terms of alpha-helix, beta-sheet, turns derived from the respecting fittings arelisted in the table 2.
In the control cells, the recorded α-helical contentwas 44.7%, β-sheet 19.6%, turns 21% and unorderedstructure 19%. UV irradiation induced a irreversibledenaturation process with a higher loss of α-helix content, from 44.7 % to 18.9%, as compared with control values. In the UV+GL combined irradiation thecells presented a smaller reduction in the α-helical content from 44.7% to 27.9% with an unchanged β-sheet control.
The small decrease in the α-helical content, recordedin the (UV+GL) - irradiated samples, suggests a morecompact and rigid conformation of the GL - protectedyeast cells.
Cellular antioxidant defenses include severalenzymes, capable of removing oxygen radicals and theirproducts. Sc - cells possess two main intracellular such“scavenger” enzymes.
• Superoxide dismutase (SOD), mithocondriallylocated, MnSod (encoded by SOD2 gene) and
cytoplasmically located Cu/ZnSod (encoded bySOD1 gene).
• Catalase (CAT) catalyses the breakdown of H2O2
to O2 and H2O. Sc- cells have two catalyse types:A, peroxisome located (encoded by CTA1 gene)and cytosolic located, T protein (encoded by CTT1gene).
SOD is involved in a dismutation reaction in which asingle reactant is converted into two different products.The oxidized SODox reacts with the O2 - superoxide ion toform O2 and the reduced enzyme SODred. This in turnreacts with a second superoxide and two protons togenerate hydrogen peroxide and regenerate SODox. Acoupling with CAT achieves a second dismutation, converting hydrogen peroxide in H2O and O2 (fig. 5). Inthis context, our GL - protection experimental set-upsreveal an interesting biochemical result. Under UV- irradiation both “scavenger” enzymes are drasticallyinhibited. The decrease of SOD activity induces adecrease of H2O2 production and, by consequence, asevere decrease of CAT activity through low substrateenzymatic inhibition (fig. 6). Catalase performs anothertype of “protecting” reaction, through a peroxidativemechanism, reshuffling the toxic compounds (phenols,formic, acid, alcohols) derived from the debris generatedby the powerful UV-oxidation: H2O2+RH2=2H2O+R.
The UV inactivation on SOD and CAT enzymes maybe interpreted from a biochemistry viewpoint, by themodification of protein structure resulting in the loss ofenzymic activity.
Our experimental results derived from AFM, impedance and circular dichroism all indicate a proteinunfolding, inducing a modification of the enzymaticactivity. The GL - irradiation through its protective
Figure 5 - a) The CONTIN3 - fitting for (UV+GL)- irradiated Sc - cells.b) The CONTIN3 - fitting for the UV- irradiated Sc - cells.
ba
Cells α-helix β-sheet Turns Unordered
Control 0.447 0.196 0.21 0.191
UV 0.189 0.124 0.180 0.284
GL+UV 0.279 0.194 0.191 0.341
Table 2 - The fractional composition of cellular lysate secondarystructure

Journal of Translational Medicine and Research, 21 (3), 2016 199
Protective Effect of Green Light Against the Deleterious Effects of UV Irradiation on Cellular Systems
activity may restore the native architecture and most ofthe lost enzymatic functions.
This is a different, significant biological effect, particularly with respect to the large value of the difference between the UV- denatured and the GL-protected samples. As far as we know this is the firstreported result in which the activity of an enzyme,several damaged by UV-denaturation may be com-pletely restored by a physical technique. A series ofmedical developments, derived from the “free radicalsscavenger” property of GL may be considered, partic-ularly for viral and degenerative diseases. Noninvasiveexplorations, with optical fibers centered on the greenband in visible domain, are easily conceivable in themodern medical technologies.
DISCUSSIONDISCUSSION
This paper presents a series of different experimen-tal results with practical as well as basic implications. Theantioxidant proprieties of green photons may find largepractical perspectives. The cellular protection of specificbiological specimens (e.g. stem cells) may have impor-tant applications in regenerative medicine.
At the basic level the antioxidant effects of EMFraise a series of fundamental questions connected withbiochemical energetics. The canonical knowledge ofcellular energy generation, storage and subsequentintra/extra- cellular migration, is mainly based on thechemical potential concept. The introduction of the
field notion, with all its powerful theoretical and experimental techniques, brought up by the up-to-datephysics, may open new research avenues in thisdomain. Hence the different nature of our approach.
It is well known that the UV - light has an oxidanteffect on the living cells, producing free radicals. Never-theless this significant effect, with large biological as wellas ecological implications, is presented only in qualitativebiochemical language. A rigorous biophysical/physicaldiscussion is still lacking. In this context, our data opennew perspectives in this direction.
The protective effect of intense GL against UV-induced oxidation observed in this studyappears different since, under normal conditions, most biologicalstructures (with the exception of green light receptors,not studied here) do not/weakly absorb green light.Therefore, the protective effect cannot be discussed interms of electronic excitations. Moreover, the observedprotective effect becomes effective after several minutes (20-30 min) of GL - irradiation, therefore thescales involved here are much larger than the corres-ponding electronic excitations (nanoseconds or shorte.To explain the protective effect of GL, against oxidationthrough UV-light, we suggest the hypothesis that elec-tric polarization effects are responsible for the observedexperimental results.
As known from literature, very large macro-molecules may exhibit different metastable configura-tions with conformational transitions between them(15). These type of large molecules are generally
Figure 6 - Enzyme activity of superoxide dismutase (SOD), catalase (CAT) and glyceraldehyde-P-dehydrogenase(GAPDH) under UV-irradiation and GL-protection

200 Journal of Translational Medicine and Research, 21 (3), 2016
Silviu Polosan et al
considered as metastable states (16, 17).It is likely that GL, with its lower photon energy may
induce local polarization of the medium, with impor-tant consequences for the cohesion forces leading totighter bound states with lower energy. These type ofprocesses are well-known and studied (18).
The oxidant effect of UV-light is understood by thephotopolarization of electrons, leading to free radicals,since the energy levels in the affected biological struc-tures match the UV-photon energy. It is also known thatthe GL is very weakly absorbed, in normal conditions,by the biological structures, de-voided of green lightreceptors, which indicates an absence of electronic-transition processes. It is then likely that GL, (as well aslonger wavelength light) with its lower photon energymay induce local polarization of the medium. This mayhave important consequences for the local cohesionforces, with changes in the electronic structure, leadingto a tighter bound-state with lower energy. The rele-vant highest occupied molecular orbitals (HOMO) mayget lower through such re-arrangement, so that the disruptive effects of UV-light are diminished. This mayalso explain the anti-oxidant effect of GL- as recorded inour experimental results. It is worth noting that sucheffects of the GL are effective especially over relevantlengths of the biological structures comparable with theGL-wavelength, so that, although similar protectiveeffects may be expected from longer- wavelength photons, these are reduced appreciably. In our previousstudies (19) we have confirmed experimentally this theoretical prediction- irradiations with blue and yellowrecorded lower values.
When a biomolecule is irradiated with green light,whose electric field component oscillates with a frequency of 514x1014 Hz, the electronic clouds of theatoms are distorted and oscillate on that frequency withrespect to the positively charged nuclei. As a conse-quence electric dipoles are induced on the atoms andthe permanent dipole moments of the biomolecule (inour case the peptide groups of cellular proteins) aremodified.
As a result the Coulomb- and dipole interactionsinside the biomolecule are changed, which may drivean adjustment of the secondary and tertiary structurein order to minimize the electrostatic energy. A modifi-cation of the surface charge distribution may occur.
The polarization of the molecules with changes inthe surface charge distribution may induce modifica-tions of their interactions in solution, leading to the formation of macromolecular structures (clusters,macromolecular chains).
This aggregation process may lead to the stabiliza-
tion of the tertiary and quaternary structures into amore rigid conformation, stable and less sensitive todisturbances.
It is worth considering at this juncture some charac-teristics of green photons. The maximum intensity ofthe black- body radiation is positioned approximately atthe GL, GL is capable to penetrate the oceans depthsand transport the energy for the many (mostlyunknown biological processes occurring at that leveland last but not least Nature is green.
Acknowledgements
This work was supported by National Research Planof Romania, Grant Bios-ADN 81-082, Grant TDRCPP 22-136 and grant UEFISCD 139/2011.
REFERENCES REFERENCES
1. Vaclav S. Global Catastrophes and Trends. Cambridge: MIT-Press;2009.
2. Oxidative Stress Reduction. International Conference, Institute Pasteur,Paris, ISANH Antioxidants. 2015.
3. Anderson P. More is Different, Princeton Series in Physics, PrincetonUniversity Press- Princeton and Oxford; 2001.
4. Comorosan S, Kappel W, Constantinescu I, Gheorghe M, Ionescu E,Pîrvu C, et al. Green light effects on biological systems: a new biophysical phenomenon. J Biol Phys. 2009 Aug;35(3):265-77. doi:10.1007/s10867-009-9164-x. Epub 2009 Jun 19.
5. Comorosan S, Polosan S, Popescu I, Ionescu E, Mitrica R, CristacheL, et al. Structural studies on serum albumins under green light irradiations. Eur Biophys J. 2010 Oct;39(11):1483-91. doi: 10.1007/s00249-010-0606-y. Epub 2010 May 16.
6. Bradford MM. A rapid and sensitive method for the quantitation ofmicrogram quantities of protein utilizing the principle of protein-dyebinding. Anal Biochem. 1976 May 7;72:248-54.
7. Spitz DR, Oberley LW. An assay for superoxide dismutase activity inmammalian tissue homogenates. Anal Biochem. 1989 May 15;179(1):8-18.
8. Scheek RM, Slater EC. Preparation and properties of rabbit-muscleglyceraldehyde- phosphate dehydrogenase with equal binding parameters for the third and fourth NAD+molecules. Biochim BiophysActa. 1978 Sep 11;526(1):13-24.
9. Suchodolskis A, Stirke A, Timonina A, Ramanaviciene A,Ramanavicius A. Baker's yeast transformation studies by atomic forcemicroscopy. Advanced Science Letters. 2011;4:171-3.
10. Frohlich H. Long-range coherence and energy storage in biologicalsystems. Intern. J. Quantum Chem. 1968;2:641-9.
11. Pelling AE, Sehati S, Gralla EB, Valentine JS, Gimzewski JK. Localnano-mechanical motion of the cell wall of Saccharomyces cerevisiae.Science. 2004 Aug 20;305(5687):1147-50.
12. Kin FL. Review on impedance detection of cellular responses inmicro/nano environment. Micromachines. 2014;5:1-12.
13. Comorosan S, Popescu I, Polosan S, Pirvu C, Ionescu E, Paslaru L, etal. Conformational changes and metastable states induced in proteinsby green light Eur.Phys.J.-B. 2015;88:8.
14. Coe MR, Lee Clerc JA. Soc Antioxidants vrs. Green light protection. J.Am. Oil Chem. 1935;12:231.
15. Rehan M, Mattice WL, Suter UE. Rotational Isomeric State Models inMacromolecular Systems. Advances in Polymer Science. 1997;131.
16. Mattice WL, Suter UW. Conformational theory of large molecules. N.Y.:Wiley; 1994.
17. Keller A, Cheng S. The role of metastability in polymer phase transi-tion. Polymer. 1998;39:4461.
18. Cheng S ZD, Keller A. The role of metastability in polymer phase transition, concept, principles and experimental observations. AnnRev Material Science. 1998;28:533-62.
19. Comorosan S. Progress in theoretical biology. Biological Observables.Academic Press. 1976;194.

Journal of Translational Medicine and Research, 21 (3), 2016 201
ORIGINAL PAPER
Copyright © Celsius Publishing House
J. Transl. Med. Res 2016;21(3):201-206 DOI: 10.21614/jtmr-21-3-94
Received: 25.07.2016Accepted: 07.09.2016
ABSTRACT
Background: Rosacea is a chronic inflammatory dermatosis, frequently associated to variousgastrointestinal disorders. Recent studies suggest that intestinal alkaline phosphatase, anenzyme that guards intestinal homeostasis might be involved in the pathogenesis of rosacea. Objective: The objective of this study is to investigate serum intestinal alkaline phosphatase– (IAP) enzymatic activity levels in rosacea patients and correlate them with different clinicalforms. Methods: Twenty six rosacea patients and twenty three age - and sex-matched healthy controls were included in our study. The severity of rosacea was assessed according to theNational Rosacea Society classification system. The levels of serum IAP enzymatic activitywere measured in all individuals.Results: There was no statistically significant difference between IAP enzymatic activity levels in the patient and control group, but we demonstrated a significant difference(p<0.05) when comparing patients with papulopustular rosacea to healthy controls and alsowhen comparing patients younger than 40 years to matched controls younger than 40 years.Conclusion: Our results suggest that increasing IAP enzymatic activity especially in papulo-pustular rosacea by special diet or by IAP supplementation might be beneficial in controllingthis disease.Key words: rosacea, intestinal alkaline phosphatase, age, papulopustular, erythemato-telangiectatic
INTRODUCTION INTRODUCTION
Rosacea is a common chronic inflammatory facial dermatosis. Although ingeneral rosacea affects young adults in their thirties to fifties with phototype IIor III sun sensitive skin any person regardless of skintype or age can developflushing with diffuse erythema, telangiectasia anda papulopustular eruption,namely the clinical signs specific to rosacea. In the medical literature, rosacealesions have been reported even in children or in individuals of African descent.The prevalence of the disease in Europe is highly variable; in some countriesupto one person in five presents rosacea. It affects women more than men, butthe most severe cases appear in males (1). According to the grading system of
Corresponding author:Andreea Merticariu, MDSf. Pantelimon Clinical EmergencyHospital, Bucharest, RomaniaE-mail: [email protected]
Study of Serum Intestinal Alkaline Phosphatase in Rosacea
Andreea Merticariu1, Luminiţa Marinescu2, Călin Giurcăneanu3,4
1Sf. Pantelimon Clinical Emergency Hospital, Bucharest, Romania2CMI Marinescu Luminita, Bucharest, Romania3Elias Clinical EmergencyHospital, Bucharest, Romania4Carol Davila University of Medicine and Pharmacy, Bucharest, Romania

202 Journal of Translational Medicine and Research, 21 (3), 2016
Andreea Merticariu et al
rosacea, published by the National Rosacea Society inThe United States of America in 2002, rosacea has fourdistinct clinical forms: erythematotelangiectatic (RET),papulopustular (RPP), phymatous and ocular (2).Telangiectasia, diffuse erythema and local burningsensation prevail in RET; inflammation with oedema,papules and pinpoint pustules are the hallmark in PPR, while in phymatous rosacea hyperplasia andhypertrophy of sebaceous glands on the nose, chin orless often ears are noticeable. In ocular rosacea patientshave mainly ocular signs and symptoms, such as conjunctivitis, blepharitis, conjunctival telangiectasia,dryness or light irritation. Different types of lesions canbe present simultaneously in one patient, but the lesionthat clinically dominates is important for classifying thedisease. Usually, in the evolution of the disease some ofthe existing clinical features accentuate graduall yornew ones emerge. The latest clinical classificationsinclude uncommon variants of rosacea: granulomatousrosacea, neurogenic rosacea (3,4).
Despite the fact that so many people suffer fromrosacea, studies proving that the impact rosacea has onthe patient quality of life is similar to psoriasis (5), andthat ample research has been done in all aspects of rosacea, scientists still did not succeed to clearlyestablish the etiology of this condition. Severaletiopathogenic hypotheses regarding either local cuta-neous anomalies or various infectious microorganismshave been proposed. Presently, it is postulated that vasculature and neuroimmune local dysregulations,dermal matrix degeneration, excessive oxidative stressdue to high levels of reactive oxygen species, andabnormally high levels of antimicrobial peptides such ascathelicidins expressed in the skin all play central rolesin rosacea development (6). Various studies also provedthat pathogens such as Demodex mites, Bacillus oleronius or Helicobacter pylori might be important ininitializing the cascade of events that lead to cutaneousinflammation, the pathogenic basis of rosacea (7,8).
It appears that there is a strong link between theskin and the gut microbiota. Dysregulation of the bacterial population resident in the stomach or in thesmall intestine and certain infectious agents are respon-sible for gastrointestinal conditions that are describedas possible comorbidities for rosacea: chronic gastritis,ulcerative colitis or Crohn’s disease (some scientistsimply that a not yet identified infectious microorganismmight be the cause for these inflammatory bowel diseases) (9,10). In addition rosacea flare-ups can betriggered by certain types of food or beverages, some ofwhich also modulate the activity of intestinal alkalinephosphatase (IAP) (11). IAP is an enzyme localized in
the brush border of the intestine with several protec-tive functions. It has complex roles in maintaining gastrointestinal homeostasis and in blocking the inflam-matory response triggered by pathogenic bacteria. IAPis involved in detoxification of drugs, heavy metals orfoods, in regulating the intestinal surface pH and thepassage of vasoactive peptides released into the intestinal lumen, through the intestinal brush borderinto the blood stream (12). Hormones such as gastrin,vasoactive intestinal peptide (VIP) and secretin havepotent vasodilator properties and are known rosaceatriggers. In IAP functional disturbances, dilators havefree pathway into the blood and determine worseningof rosacea symptoms (11).
Recent studies showed that IAP might be the missing link to the influence some gastrointestinal conditions or dietary factors have on rosacea develop-ment and evolution (11). Therefore we conducted thepresent study to investigate this possible relationshipbetween rosacea and IAP by evaluating IAP enzymaticactivity in rosacea patients.
METHODESMETHODES
We recruited anumber of 49 human subjects forour experiment (26 rosacea patients and 23 healthymatched controls). Rosacea was diagnosed based onclinical signs and symptoms. We divided our patientgroup in 2 subgroups, in accordance with the form ofrosacea: erythematotelangiectatic rosacea (RET) subgroup (15 patients) and papulopustular rosacea(RPP) subgroup (11 patients). None of the individualshad any systemic treatment or gastrointestinal symptom for the last two months previous to samplecollection. Each included subject signed a writteninformed consent.
In order to evaluate IAP enzymatic activity, a 10ml fasting blood sample was collected from each person within our study population. Each samplewas immediately centrifuged at 1500 rpm, followedby electrophoresis and analysis of enzymatic activityin separate fractions. The results were expressed asµmol/sl and after ward converted in IU/L (commonlyused value), using the standard conversion factor.
The statistical methodology used F-test for differences in variances, t-test for differences in meansand histograms.
RESULTS RESULTS
Our patient group included 17 women with an agerange of 21-75 years (mean age 39.58) and 9 men with

Journal of Translational Medicine and Research, 21 (3), 2016 203
Study of Serum Intestinal Alkaline Phosphatase in Rosacea
an age range of 19-69 years (mean age 53.22). Sex ratiowas approximately 2:1. The two mean ages correlatewith patients’general behaviour: women seek medicalexamination at the onset of their disease while men askmedical advice in later, more severe stages. The controlgroup was comparable in terms of sex (17 women, 7men) and age (women age range 24-68 years, meanage 41.64; men age range 24-66 years, mean age 47.42)to the patient group.
All individuals had total alkaline phosphatasealkaline enzymatic activity within normal referencerange (30-120 IU/L). Values for intestinal alkalinephosphatase enzymatic activity did not exceed 15% of the total alkaline phosphatase value (as considered normal by the laboratory performing theanalysis) (13), except one higher value obtained inone control who was referred to gastroenterology.The above mentioned subject was excluded from ourstudy, therefore 48 individuals were observed forthis study.
In the rosacea group IAP activity values were normalin relation to total AP and varied from a minimum of0.00 IU/L to a maximum of 11.38 IU/L (mean value 2.1 IU/L). In the control group values varied from a minimum of 0.0 IU/L to a maximum of 14.97 IU/L(mean value 3.78 IU/L) (table 1, fig. 1).
After we rejected the hypothesis that the variancesof the two samples are equal (F-test, p = 0.03), we tested for differences in the means of the patient andcontrol samples. We found no statistically significantdifferences between IAP levels in the patient (M = 3.78;SD = 4.76) and control groups (M =2.1; SD = 3.26):
t(36) = 1.40, p = 0.085 for one-tail test. However, as thecombined histogram from fig. 2 shows, it appears thatlower values are more frequent in patients than in controls.
Table 1. Statistical characteristics of IAP values in rosacea groupand in control group
Rosacea patients Controls Total individuals 26 22Mean 2.10 IU/L 3.78 IU/LMedian 0.00 IU/L 2.99 IU/LStd. deviation 3.26 IU/L 4.76 IU/LMinimum 0.00 IU/L 0.00 IU/LMaximum 11.38 IU/L 14.97 IU/L
Figure 1 - Mean values of the Controls and Rosacea patients subsamples with one standard deviation bar
Figure 2 - Frequency of IAP values in patients versus matched controls

204 Journal of Translational Medicine and Research, 21 (3), 2016
Andreea Merticariu et al
The t-test methodology was repeated in the RET (15patients) and RPP (11 patients) subgroups. The difference was not statistically significant when the RETsubgroup was compared with the controls. In the caseof the RPP subgroup, we found evidence for differentmeans with the t-test t(31) = 2.05, p = 0.024. As confirmed by the histograms, the difference betweenIAP values from controls is less clear in RET patients,but in the case of the RPP subgroup we notice thatpatients more often have smaller IAP values (fig. 3).
IAP levels were not affected by gender in eitherpatient or control group. Then we investigated whetherthe age could play a significant role in the distributionof IAP values. The scatter plot of IAP levels against age(fig. 4) shows that there appear to be a positive correlation in the case of patients and a negative one inthe case of controls.
We detected a significant difference, t(13) = 1.85, p-value = 0.043 for one-tail t-test, assuming unequalvariances,between IAP levels in rosacea patientsyounger than 40 years versus matched controlsyounger than 40 years (fig. 5). In this patient group wenotice a higher distribution of 0.0 IU/L IAP activity value and of small values of IAP, IAP activity being significantly lower in rosacea patients. The 40 yearsthreshold was chosen because in scientific literature inmajority of patients this disease debuts after the age of30 and up to 50 years (14) and because in our studypopulation median age was close to 40 (43 years) l.Thus, the age of 40 could be a relevant threshold,because it assures that our study can find a reasonablesample size of patients while being as close as possibleto the age interval that is characteristic for rosacea, i.e.,after 30 years.
Figure 3 - Difference in IAP value distribution in erythematotelangiectatic (RET) and papulopustular rosacea (RPP) patients compared to control group

Journal of Translational Medicine and Research, 21 (3), 2016 205
Study of Serum Intestinal Alkaline Phosphatase in Rosacea
DISSCUSIONDISSCUSION
The results of our study reveal that overall there is aslight but no statistically significant difference betweenIAP activity value in patients versus healthy controls.We observed that we have fewer individuals with no detectable IAP in our control group: 10 healthy individuals compared to 14 patients (6 with RET and 7with RPP) had IAP enzymatic activity value 0.00 UI/L.We also noticed fewer matched controls with small IAPvalues. In addition the highest normal values were
distributed in the control group (13.17; 13.77; 14.97IU/L). The subsample test that separated the rosaceapatients according to their form of disease, indicated asignificant difference in IAP mean enzymatic activitylevels between patients diagnosed with papulopustularrosacea and the control group.
These findings suggest that IAP might have reducedactivity in patients with inflammatory papulopustularrosacea and might play a role in its pathogenesis.
On the other hand, IAP values are significantly lowerin those under 40 years of age, within the patient group
Figure 4 - Scatter plot of age versus IAP. Trend lines show that levels decrease with the age for controls and increase with the age for rosacea patients
Figure 5 - IAP according to age threshold value of40 years is statistically significantly lower in rosacea patients than matched controls

206 Journal of Translational Medicine and Research, 21 (3), 2016
Andreea Merticariu et al
compared to IAP values within the control group. Inthese patients IAP activity is lower and taking intoaccount the fact that in adult population IAP activitydoes not differ between age groups (15), it supports theidea that IAP is important in rosacea evolution inyoungadults. A possible explanation might be that young people nowadays have a more chaotic lifestyle with an irregular and unbalanced diet, based onhighlyprocessed foods and low in fresh vegetables, inducingan acidic pH in the intestine which inhibits IAP function.This coupled with a genetic predisposition to rosacea,which now we know it is real (16), might promoterosacea onset. Further studies on larger study groupsneed to be conducted in order to confirm our resultsand to assess if IAP is involved in late onset rosacea.
CONCLUSION CONCLUSION
It appears that IAP might have a certain degree ofinfluence in rosacea, especially in severe cases andinyoung adults in whom our study indicates that thisenzyme has low activity. There might be also impor-tance in studying if any therapeutically valuable resultwould be obtained in IAP supplementation in a subsetof rosacea patients. So far, IAP administered intra-venously has been successful in adjuvant therapy ofnecrotizing enterocolitis in neonates and sepsis inadults, by attenuation of the systemic inflammatoryresponse and administered orally in moderate to severeulcerative colitis, which led to short term improvementof the diseases (17-19). Patients with RPP could modifytheir diet, including more alkalizing foods in order tostimulate IAP enzyme function. A healthy IAP activitywill prevent intestinal hormones or peptides fromentering the bloodflow with its consequent increase inlocal cutaneous inflammation and vasodilation. Wecould debate that by mitigating inflammation in peopleaffected by rosacea, administered IAP would be benefi-cial for these patients, but this hypothesis needs to befurther evaluated. In addition larger study groups mightbe useful to definitely establish if IAP plays or not amain role in rosacea development, regardless of age.
REFERENCESREFERENCES
1. Chosidow O, Cribier B. Epidemiology of rosacea: updated data. AnnDermatol Venereol. 2011 Nov;138 Suppl 3:S179-83. doi: 10.1016/S0151-9638(11)70087-4.
2. Wilkin J, Dahl M, Detmar M, Drake L, Liang MH, Odom R, et al.National Rosacea Society Expert Committee. Standard grading systemfor rosacea: report of the National Rosacea Society Expert Committeeon the classification and staging of rosacea. J Am Acad Dermatol.2004 Jun;50(6):907-12.
3. Wilkin J, Dahl M, Detmar M, Drake L, Feinstein A, Odom R, et al.Standard classification of rosacea: Report of the National RosaceaSociety Expert Committee on the Classification and Staging ofRosacea. J Am Acad Dermatol. 2002 Apr;46(4):584-7.
4. Scharschmidt TC, Yost JM, Truong SV, Steinhoff M, Wang KC, BergerTG. Neurogenic rosacea: a distinct clinical subtype requiring a modi-fied approach to treatment. Arch Dermatol. 2011 Jan;147(1):123-6.doi: 10.1001/archdermatol.2010.413.
5. Cresce ND, Davis SA, Huang WW, Feldman SR. The quality of lifeimpact of acne and rosacea compared to other major medical condi-tions. J Drugs Dermatol. 2014 Jun;13(6):692-7.
6. Two AM, Wu W, Gallo RL, Hata TR. Rosacea: part I. Introduction, cat-egorization, histology, pathogenesis, and risk factors. J Am AcadDermatol. 2015 May;72(5):749-58; quiz 759-60. doi: 10.1016/j.jaad.2014.08.028.
7. Holmes AD. Potential role of microorganisms in the pathogenesis ofrosacea. J Am Acad Dermatol. 2013 Dec;69(6):1025-32. doi: 10.1016/j.jaad.2013.08.006. Epub 2013 Sep 5.
8. Lazaridou E, Giannopoulou C, Fotiadou C, Vakirlis E, Trigoni A,Ioannides D. The potential role of microorganisms in the developmentof rosacea. J Dtsch Dermatol Ges. 2011 Jan;9(1):21-5. doi: 10.1111/j.1610-0387.2010.07513.x. Epub 2010 Nov 8. English, German
9. De Hertogh G, Geboes K. Crohn's disease and infections: a complexrelationship. Med Gen Med. 2004 Aug 10;6(3):14.
10. Merticariu A, Marinescu L, Giurcăneanu C. Rosacea and its comorbidities J. Transl. Med. Res 2016;21(1):17-23. doi: 10.21614/jtmr-21-1-68.
11. Whitehead J. Intestinal alkaline phosphatase: the molecular link betweenrosacea and gastrointestinal disease? Med Hypotheses. 2009Dec;73(6):1019-22. doi: 10.1016/j.mehy.2009.02.049. Epub 2009 Jul 1.
12. Estaki M, DeCoffe D, Gibson DL. Interplay between intestinal alkalinephosphatase, diet, gut microbes and immunity. World J Gastroenterol.2014 Nov 14;20(42):15650-6. doi: 10.3748/ wjg.v20.i42.15650.
13. Laborator Synevo. Referinte specifice tehnologiei de lucru utilizate2010. Ref Type: Catalog.
14. Wolff K, Johnson R, Saavedra A. Fitzpatrick's Color Atlas andSynopsis of Clinical Dermatology, 7th Edition, part 1, section 1.McGraw-Hill Education/Medical; 2013. P. 9-13.
15. Van Hoof VO, Hoylaerts MF, Geryl H, Van Mullem M, Lepoutre LG, DeBroe ME. Age and sex distribution of alkaline phosphatase isoenzymesby agarose electrophoresis. Clin Chem. 1990 Jun;36(6):875-8.
16. Chang AL, Raber I, Xu J, Li R, Spitale R, Chen J, et al. Assessment ofthe genetic basis of rosacea by genome-wide association study. JInvest Dermatol. 2015 Jun;135(6):1548-55. doi: 10.1038/jid.2015.53.Epub 2015 Feb 19.
17. Riggle KM, Rentea RM, Welak SR, Pritchard KA, Oldham KT, GourlayDM. Intestinal alkaline phosphatase prevents the systemic inflamma-tory response associated with necrotizing enterocolitis. J Surg Res.2013 Mar;180(1):21-6. doi: 10.1016/j.jss.2012.10.042. Epub 2012Nov 8.
18. Pickkers P, Heemskerk S, Schouten J, Laterre PF, Vincent JL,Beishuizen A, Jorens et al. Alkaline phosphatase for treatment of sep-sis-induced acute kidney injury: a prospective randomized double-blind placebo-controlled trial. Crit Care. 2012 Jan 23;16(1):R14. doi:10.1186/cc11159.
19. Lukas M, Drastich P, Konecny M, Gionchetti P, Urban O, Cantoni F, etal. Exogenous alkaline phosphatase for the treatment of patients withmoderate to severe ulcerative colitis. Inflamm Bowel Dis. 2010Jul;16(7):1180-6. doi: 10.1002/ibd.21161.

Journal of Translational Medicine and Research, 21 (3), 2016 207
CASE REPORT
Copyright © Celsius Publishing House
J. Transl. Med. Res 2016;21(3):207-209 DOI: 10.21614/jtmr-21-3-95
An Unusual Cause of Overt Upper GI Bleeding: RetrogradeJejunogastric Intussusception
Hilmi D. Elsiddig1, S.H. Suliman1, El.H. Salim Omer1, Elnour Mustafa2, Mohamed G. Alnedar1, Yousif Mohd Khair1, S.Z. Ibrahim1
Corresponding author:Hilmi Daoud Elsiddig, MDAssistant professorDepartment of SurgeryUniversity of KhartoumConsultant General SurgeonSoba University HospitalPostal address: P.O Box 8081Khartoum Al Amarat, SudanE-mail: [email protected]
ABSTRACT
Retrograde jejunogastric intussusception is a well-recognized, rare, but potentially life threatening long-term complication of gastrojejunostomy. Diagnosis of this condition is difficult in most cases. We report on such a patient who presented with overt upper gastro-intestinal bleeding. The complication developed thirty years after the primary surgery withouthistory of acute upper abdominal pain in spite of a long segment of gangrenous jejunuminside the stomach. Resection and refashioning of the gastrojujenostomy was performed. Key words: gastrojejunostomy, retrogradejejunogastric intussusception, bleeding, strangulation
INTRODUCTIONINTRODUCTION
Retrograde Jejunogastric Intussusception is an uncommon but potentiallylife threatening complication of gastrojejunostomy or partial gastrectomy.Around 200 cases have been reported in English literature till now (1). Thispatient presented 30 years after the primary surgery and interestingly he had noepigastric pain in spite of a long segment of gangrenous jejunum inside thestomach. Diagnosis was confirmed by computed tomography.
CASE REPORTCASE REPORT
A 60 years old man presented with three days history bilious vomiting. Onadmission, he vomited one liter of dark blood. There is no history of upperabdominal pain. He has undergone vagotomy and gastrojejunostomy for pepticulcer 30 years back and he was asymptomatic until his recent admission to theemergency department. Patient was dehydrated; with pulse rate 110/min andBP 100/60 mm of Hg. He has an upper midline scar. Epigastric region was
Received: 08.06.2016Accepted: 19.08.2016
1Department of Surgery; 2Department of RadiologySoba University Hospital and University of Khartoum, Sudan

208 Journal of Translational Medicine and Research, 21 (3), 2016
Hilmi D. Elsiddig et al
distended and there was a vague feeling of epigastricmass. Laboratory investigation showed haemoglobin10 gm%, White cell count 10,000 /cmm with 87% polymorph, Plain X-ray abdomen was within normallimit. After initial resuscitation, upper GIT endoscopywas performed which revealed a large clot obscuringthe distal stomach. CT abdomen with oral contrastshowed small bowel loops in the stomach (fig. 1).Emergency laparotomy was carried out immediately.Stomach was found hugely distended with an intra-luminal bowel loops. The presence of posterior gastro-jejunostomy was confirmed with intussusception ofefferent jejunal loop into the stomach. A gastrostomywas done which revealed intussuscepted gangrenousefferent jejunal loop. Then intussusception wasreduced, the gangrenous segment was resected withresection of the oedematous area of gastrojejuno-stomy. End to end jejunal anastomosis was performedand the big gastrostomy was partially closed (reduced).A new gastrojujenostomy was done in two layers. Thepatient had an uneventful postoperative course andwas discharged on day eight.
DISCUSSIONDISCUSSION
Retrograde jejunogastric intussusception was firstdescribed by Bozzi in apatient with gastroenterostomy(2). According to the type of intussuscepted loop, JGI isclassified into three types: type I, antegrade or afferentloop intussusception; type II, retrograde or efferentloop intussusception; and type III, combined form (3).Efferent loop JGI is seen in 80% of the cases as in the
Figure 1 - Emergency CT- Scan of the abdomen: Dilated stomachwith intragastric non-homogeneous mass compatible with bowel
loops
Figure 2 - Intra operative photograph showing small bowel loopsinside a dilated stomach
Figure 3 - Intra operative photograph showing a dialted afferentloop of a retro colic gastrojujenostomy
Figure 4 - Intra operative photograph showing gangrenous jeju-nalsegment after dismantling

Journal of Translational Medicine and Research, 21 (3), 2016 209
An Unusual Cause of Overt Upper GI Bleeding: Retrograde Jejunogastric Intussusception
present case. Two different forms of JGI have beendescribed according to its clinical presentation (4). Inthe acute form, incarceration and strangulation of theintussuscepted loop causing acute severe epigastricpain, vomiting, and subsequently, hematemesis generally occur, however, spontaneous reduction isusual in the chronic type (1). A palpable abdominalmass can be observed in almost half of the cases (5). Inmost of the case reports, severe epigastric pain is animportant early symptom of JGI (1,6) however in thiscase report there is no history of epigastric pain in spiteof a gangrenous jejunum and the reason is not wellknown.
The treatment for JGI is surgical intervention as soon as possible. Surgical options include reduction,resection (6,7) and revision of the anastomosis, and fixation of the jejunum to adjacent tissue like meso-colon depending on the conditions found during theoperation. In this case report, resection and revision ofthe anastomosis were done.
CONCLUSIONCONCLUSION
Retrograde JGI is a very serious life-threateningcomplication of gastric surgery. There is a wide
variation in the lapse time between the gastric surgeryand occurrence of JGI, as seen in the present case.When a patient who has had history of gastric opera-tion presents with epigastric pain, vomiting and haematemesis, the possibility of JGI should be considered along with more common diagnoses suchas a recurrent stomach ulcer. Because this condition islife-threatening, awareness of this rare complication isessential to save live.
REFERENCESREFERENCES
1. Kshirsagar AY, Shinde SL, Langade YB, Pujari SG, Jeur AS. Retrogradejejunogastric intussusception with strangulation after posterior gastrojejunostomy. Med J Armed Forces India. 2008 Jul;64(3):282-3.doi: 10.1016/S0377-1237(08)80121-9. Epub 2011 Jul 21.
2. Bozzi E. Annotation, Bull.Acad Med. 1914;122:3-4.3. Shackman R. Jejunogastric intussusception. Brit J Surg.1940;27:475-
80.4. Archimandritis AJ, Hatzopoulos N, Hatzinikolaou P, Sougioultzis S,
Kourtesas D, Papastratis G, et al. Jejunogastric intussusception presented with hematemesis: a case presentation and review of literature. BMC Gastroenterol. 2001;1:1. Epub 2001 Jan 4.
5. Waits JO, Beart RW Jr, Charboneau JW. Jejunogastric intussuscep-tion. Arch Surg. 1980 Dec;115(12):1449-52.
6. Pervin SS, Biswas SK. Retrograde Jejunogastric Intussusception: A Case Report. Faridpur Med. Coll. J. 2010;5(1):32-34
7. Samarasam I, Chandran B, Shanker U, George B, Chacko A, MathewG. Jejunogastric intussusception: an unusual cause of haematemesis.Can J Gastroenterol. 2005 Dec;19(12):735-6.

210 Journal of Translational Medicine and Research, 21 (3), 2016
CASE REPORT
Copyright © Celsius Publishing House
J. Transl. Med. Res 2016;21(3):210- DOI: 10.21614/jtmr-21-3-J. Transl. Med. Res 2016;21(3):210-J. Transl. Med. Res 2016;21(3):210-214 DOI: 10.21614/jtmr-21-3-96
Recurrent Giant Phyllodes Tumour in a Young Female: A Case Report
Mahim Koshariya1, Ashish Sharma1, Ajay Gehlot1, Surbhi Garg1, M.C. Songra1, Karan Peepre2
Corresponding author:Mahim Koshariya, MS, FMAS, FIASGODepartment of Surgery, Gandhi Medical College & AssociatedHamidia Hospital, Bhopal, IndiaE-mail: [email protected]
ABSTRACT
Phyllodes tumors (PTs) are uncommon neoplasms of the breast, constituting 0.3 to 0.9% ofall breast tumors in females comprised of both stromal and epithelial elements. The termcystosarcoma phyllode was coined by Johannes Muller, a misleading term as tumors arerarely cystic and the majority follow a benign clinical course. The term giant phyllodes isused when the tumor size exceeds 10 cm in diameter. WHO (World Health Organization)classification has identified three categories of phyllodes tumors of the breast (PT): benign,borderline and malignant. The mainstay of treatment of non-metastatic phyllodes tumors ofthe breast is complete surgical resection with wide resection margins. Local recurrence upto 50 % after surgery has been reported in Phyllodes tumors. We report a case of twoepisodes of recurrent phyllodes tumor in a young female.Key words: Phyllodes Tumors (PTs), recurrence, mastectomy
INTRODUCTIONINTRODUCTION
The Phyllodes tumors (PTs) tumors of the breast are fibroepithelial tumorswhich are rarely seen and have potential for recurrence. Less than 1 % of all thebreast tumors consist of Phyllodes tumors (1-2). The majority of PTs occur inwomen between the age of 35 and 55 (3), although there are reported cases inadolescents, as well as in elderly women (4).
Phyllodes tumors are usually not considered initially in clinical diagnosis,show slow or rapid growth pattern, and are usually diagnosed after biopsy. These infrequent tumors are typically seen as a firm, circular, mobile,well-defined and painless mass in the diameter of 5 centimeters or more. Theterm giant phyllodes is used when the tumor size exceeds 10 cm in maximumdiameter (4). PTs with diameters of 40 centimeters have also been reported inthe literature (5). These lesions are difficult, if not impossible, to distinguish fromfibroadenoma on physical examination or by radiologic studies except when
1Department of Surgery; 2Department of Nuclear Medicine; Gandhi Medical College & Associated Hamidia Hospital, Bhopal, India
Received: 15.05.2016Accepted: 04.07.2016

Journal of Translational Medicine and Research, 21 (3), 2016 211
Recurrent Giant Phyllodes Tumour in a Young Female: A Case Report
quite large. The tumors are characterized by a combina-tion of a hypercellular stroma and cleft like or cysticspaces lined by epithelium into which classically projects the stroma in a leaf-like fashion (6,7). PTs aredistinguished from FA histopathologically by their cellular pattern, having increased cellular atypicalchanges and excessive stromal growth. WHO (WorldHealth Organization) classification has identified threecategories of phyllodes tumors of the breast (PT):benign, borderline and malignant (8). Zurrida and hisco-authors (9) reported that 9%, 44% and 33% ofbenign, borderline and malignant PTs developed localrecurrence
CASE REPORTCASE REPORT
A 32 year old lady presented to our departmentwith chief complaint of lump in her right breast since 1year. Patient had history of similar lump in past, 3 yearsback for which she was operated upon, a wide localexcision was done and histopatjology report was consistent with phyllodes tumor, but it was followed byrecurrence. Patient was again taken for surgery 2 yearsback, this time biopsy was indicative of Pericanalicularfibroadenoma. Unfortunately patient met with secondtime recurrence and patient was referred to us.
Examination revealed a large mass in the rightbreast measuring 18 x 15 cms with lobulated surface.Few dilated veins were noticed on the skin surface. Thenipple was pushed down inferolaterally. Two scar marksof previous surgery were seen in inferomedial andouter upper quadrant (fig. 1 a, b). Contra lateral breast examination was normal, and there was no lymphadenopathy on bilateral axillary examination.
Mammography was done which showed recurrenceof phyllode like growth in right breast with increasedintralesional vascularity. USG breast showed large multilobulated mass lesion completely replacing rightbreast with very less fibrofatty glandular tissue, therewas no significant axillary lymphadenopathy noted.USG abdomen was found to be normal. SPECT CT-Thorax and abdomen (fig. 2 a, b) showed a masslesion of 15X 12 cm with increased tracer uptake, no evidence of axillary or pectoral lymph node enlarge-ment. There was no evidence of liver metastasis.
Bone scan (fig. 3) was found to be normal. FNACdone from the lump confirmed the diagnosis of phyllodes tumor.
The patient underwent surgical management. Asimple mastectomy was performed with primary closure of the skin, without any skin graft or flap recon-struction. She had an uneventful post- operative course
and was discharged on 8th postoperative day. Cut section of mastectomy specimen revealed oval greywhite tissue measuring 18 x 15 x 10 cms. Histologicalsections (fig. 6) revealed breast tissue showing slit likeducts with epithelial hyperplasia with cellular spindlestroma, no atypia mitosis or necrosis was seen in stroma, no sarcomatous areas seen, picture was suggestive of Benign Phyllodes tumor. Reconstructivebreast surgery was offered to the patient but thepatient refused surgery probably because there washistory of two times recurrence. Patient was kept in regular follow up and after 1 year of surgery there wasno evidence of local recurrence.
DISCUSSIONDISCUSSION
Tumors of mixed connective tissue and epitheliumconstitute an important group of unusual primarybreast tumors. Phyllodes tumors contain a biphasic proliferation of mammary epithelium and stroma, the
Figure 1 - (a) Gross appearance (anterior view) showing a largemass in right breast involving whole of the breast. The nipple waspushed down inferolaterally. Two scar marks of previous surgery
were seen in inferomedial and outer upper quadrant(b) Gross appearance (lateral view) showing large mass in
the right breast measuring 18 X 15 cms with lobulated surface.Few dilated veins were also noticed
a
b

212 Journal of Translational Medicine and Research, 21 (3), 2016
Mahim Koshariya et al
latter determines the malignancy. Initially called cystosarcoma phylloides, a misleading description astumors are rarely cystic and the majority follow abenign clinical course. With increasing cellularity, invasive margin and sarcomatous appearance, thesetumors may be classified as malignant phyllodes
Figure 4 - (a) Intra-op picture showing dissection of tumor from chest wall. (b). Intra-op picture showing separation
of tumor from chest wall
a
b
Figure 2 - (a) SPECT CT- (Transaxial view) showed a mass lesion of 15X 12 cm with increased tracer uptake, no evidence
of axillary or pectoral lymph node enlargement. There was no evidence of liver metastasis. (b) SPECT CT- (Coronal View)
a b
Figure 3 - Bone Scan- No abnormal uptake in skeleton reflectsnormal bone scan

Journal of Translational Medicine and Research, 21 (3), 2016 213
Recurrent Giant Phyllodes Tumour in a Young Female: A Case Report
tumors. Histologically, these tumors are similar tofibroadenomas, but the whorled stroma forms largerclefts lined by epithelium that resemble clusters of leaflike structures (10).
The majority of PTs occur in women between theage of 35 and 55 (3). Patients usually presents withcomplaints of a firm round macrolobulated mass whichis painless in nature. Large lesions may be associatedwith dilated veins visible over the skin, which may bestretched and attenuated. Rare findings which havebeen reported are Nipple retraction (4, 11), skin ulcera-tion invasion of the chest wall (4, 12, 13), and bloodynipple discharge (13). Axillary lymph nodes are usuallynot involved however reactionary inflammatory lymphnodes are seen in about 20% cases (14)
Surgery remains the mainstay of treatment howeverthe extent of surgical approach historically has beencontroversial, and continues to evolve. Complete surgical resection with wide resection margins (at least 1cm) should be performed, except for lesions larger than10 cm in which total mastectomy is recommended. Ifthe initial surgery fails to achieve a negative margin, it isrecommended that the patient should undergo re-excision to obtain a wider margin in order to preventlocal recurrence.
Mastectomy is advocated for large tumors for amicroscopic margin of one centimeter without signifi-cant deformation of the breast, or recurrent tumorsdespite adequate margins (16). Axillary dissection is notroutinely recommend as metastasis to the lymph nodesoccur in less than 5% of patients
Mastectomy was the preferred treatment of choicein our case as the tumor was two times recurrent having a very large size covering almost whole of thebreast. Mastectomy has been the most commonly performed surgery for borderline and malignant PTs
Figure 5 - Showing primary skin closure
Figure 6 - (a) Resected specimen (gross appearance) showing a large mass with nodular surface and dilated veins.
(b) Cut section showing multilobulated surface
a
b
Figure 7 - Histopathological picture showing slit like ducts with epithelial hyperplasia with cellular spindle stroma, no atypia mitosis or necrosis seen in stroma, suggestive
of benign phyllodes tumor

214 Journal of Translational Medicine and Research, 21 (3), 2016
Mahim Koshariya et al
with local recurrence rates of 5% and 12%; respectively(15,16,17).
Local recurrence is usually seen within the first fewyears of surgery and histologically resembles the original tumor. Occasionally, recurrent tumors showincreased cellularity and more aggressive histologicalfeatures than the original lesion. In most patients, localrecurrence is isolated and is not associated with thedevelopment of distant metastasis (18). Important riskfactors predicting recurrence is positive margin, youngage at presentation, large tumor size, histological type.Other parameters such as stromal hypercellularity, stromal atypia, stromal overgrowth, and mitosis, weresignificantly associated with local recurrence (19). Themost important risk factor for recurrence is the resection done within 1-2 cm negative surgical margins(20). It is important that these factors be identified andappropriate surgical procedure be selected to ensureclear margins.
Radiotherapy has a role in reducing local recurrencein borderline and malignant phylloides but has noimpact on over all survival and disease free survival(21).
CONCLUSIONCONCLUSION
Phyllodes tumor are rare tumors of breast but arenotorious for local recurrence. Wide local excision is anacceptable method of treatment but for recurrent andlarge tumors (>10 cm) simple mastectomy is preferredfor complete tumor excision. Most important factor toprevent local recurrence is to keep a sufficient marginof healthy tissue. It is necessary that the patients bekept in follow up as there is a risk of local recurrenceand distant metastasis.
REFERENCESREFERENCES
1. Azzopardi JG. Sarcoma in the breast. In Benningron J (ed). Problemsin Breast Pathology. Major Problems in Pathology. Vol 11,Philadelphia: WB Saunders Co; 1979. p. 335-359.
2. Rowell MD, Perry RR, Hsiu JG, Barranco SC. Phlyllodes tumors. AmJ Surg. 1993 Mar;165(3):376-9.
3. Salvadori B, Cusumano F, Del-Bo R, Delledonne V, Grassi M, Rovini D,
et al. Surgical treatment of phyllodes tumors of the breast. Cancer.1989 Jun 15;63(12):2532-6.
4. Reinfuss M, Mituś J, Duda K, Stelmach A, Ryś J, Smolak K. The treatment and prognosis of patients with phyllodes tumour of thebreast: an analysis of 170 cases. Cancer. 1996 Mar 1;77(5):910-6.
5. Liang MI, Ramaswamy B, Patterson CC, McKelvey MT, Gordillo G,Nuovo GJ, et al. Giant breast tumors: Surgical man agement of phyllodes tumors, potential for reconstructive sur gery and a review ofliterature. World J Surg Oncol. 2008;11:117.
6. Pietrusuzka M, Barnes L. Cystosarcoma phyllodes: a clinico-pathologic analysis of 42 cases. Cancer. 1978 May;41(5):1974-83.
7. Moffat CJ, Pinder SE, Dixon AR, Elston CW, Blamey RW, Ellis IO.Phyllodes tumours of the breast: a clinicopathological review of thirty-two cases. Histopathology. 1995 Sep;27(3):205-18.
8. World Health Organization. Histological typing of breast tumors.Tumori. 1982 Jun 30;68(3):181-98.
9. Zurrida S, Bartoli C, Galimberti V, Squicciarini P, Delledonne V,Veronesi P. Which therapy for unexpected phyllode tumour of thebreast? Eur J Cancer. 1992;28(2-3):654-7.
10. Kelly K. Hunt, Marjorie C. Green, and Thomas A. Buchholz. Diseasesof the breast. In Sabiston textbook of surgery, Nineteenth ed USA:Elsevier-Saunders; 2012. p. 845.
11. Deodhar SD, Joshi S, Khubchandani S. Cystosarcoma phyllodes. JPostgrad Med. 1989 Apr;35(2):98-103.
12. Dyer NH, Bridger JE, Taylor RS. Cystosarcoma phylloides. Br J Surg.1966 May;53(5):450-5.
13. Chen WH, Cheng SP, Tzen CY, Yang TL, Jeng KS, Liu CL, et al. Surgicaltreatment of phyllodes tumors of the breast: retrospective review of172 cases. J Surg Oncol. 2005 Sep 1;91(3):185-94.
14. Rowell MD, Perry RR, Hsiu JG, Barranco SC. Phyllodes tumors. Am JSurg. 1993 Mar;165(3):376-9.
15. Treves N, Sunderland DA. Cystosarcoma phyllodes of the breast: amalignant and a benign tumor; a clinicopathological study of seventy-seven cases. Cancer. 1951 Nov;4(6):1286-1332.
16. Asoglu O, Mustafa M, Blanchard K, Grant CS, Reynolds C, Cha SC, etal. Risk factors for recurrence and death after primary surgical treatment of malignant phyllodes tumors. Ann Surg Oncol. 2004 Nov;11(11):1011-7.
17. Barth RJ Jr. Histologic features predict local recurrence after breastconserving therapy of phyllodes tumors. Breast Cancer Res Treat.1999 Oct;57(3):291-5.
18. Ahmad Z, Koshariya M, Shukla S, Vatti V, Diwan A. A rare case of recurrent malignant phyllodes tumor of the breast in a young nulliparous woman. Clin Cancer Investig J. 2014;3:173-5.
19. Wei J, Tan YT, Cai YC, Yuan ZY, Yang D, Wang SS, et al. Predictive factors for the local recurrence and distant metastasis of phyllodestumors of the breast: a retrospective analysis of 192 cases at a singlecenter. Chin J Cancer. 2014 Oct;33(10):492-500. doi: 10.5732/cjc.014.10048. Epub 2014 Aug 8.
20. Lenhard MS, Kahlert S, Himsl I, Ditsch N, Untch M, Bauerfeind I.Phyllodes tumour of the breast: clinical follow-up of 33 cases of thisrare disease. Eur J Obstet Gynecol Reprod Biol. 2008 Jun;138(2):217-21. Epub 2007 Sep 14.
21. Zeng S, Zhang X , Yang D , Wang X, Ren G. Effects of adjuvant radio-therapy on borderline and malignant phyllodes tumors: a systematicreview and meta analysis. Mol Clin Oncol. 2015 May;3(3):663-671.Epub 2015 Feb 6.

Journal of Translational Medicine and Research, 21 (3), 2016 215
ABSTRACTS
Copyright © Celsius Publishing House
J. Transl. Med. Res 2016;21(3):215-236 DOI: 10.21614/jtmr-21-3-97
ORAL PRESENTATIONS (OP)ORAL PRESENTATIONS (OP)
OP-01
LIVER TRANSPLANTATION (LT) USING DCD DONORS WITH 20 MINUTESNO TOUCH PERIOD: PRELIMINARY ITALIAN EXPERIENCE AT NIGUARDA CA GRANDA HOSPITAL
L. De Carlis1, A. De Gasperi2, E. Mazza2, R. De Carlis1, C. Pagan de Paganis2, F. Russo2, R. Limuti2, A. Corti2, A. Brunetti2, M. Zanierato3
1Transplant Surgery; 2Anesthesia CCM Niguarda, Niguarda Ca Granda H, Milan,Italy3Anesthesia, Policlinico S Matteo, Policlinico San Matteo, Pavia, Italy
Introduction: Donation after cardiac death (DCD), since long considered in EU and USA toexpand the donor pool, is possible also in Italy with the ALBA project since 2009 (1). Due tothe long “no touch period” (20 minutes) requested by the Italian law after cardiac arrest todeclare death(much longer if compared to 5 – 10 mins of France or Spain), liver transplan-tation (LT) has never been considered, major concerns being the long warm ischemia time(WIT) and the possible major liver injury. With strict entry criteria for donors (1), the constantuse of normothermic regional perfusion (NRP, regional ECMO),an option for hypothermicmachine perfusion (hMP) and very selected recipients, a LT program from DCD donors wasstarted at Niguarda Ca Granda H in September 2015 (2). Since then and up to now (August2016), eight LT procedures were performed at Niguarda Ca Granda H (Milan). Aim of thispreliminary report is the description of our results, (FU period 60- 320 dd). Methods: Between Sept 2015 and July 2016, eight (over eleven possible) controlled (2,cDCD) and uncontrolled (6, uDCD) DCD donors were considered fordonation aiming at LT.Median age was 49 yo(range 31-63), median WIT in uncontrolled donors was 126 minutes(including no touch and low flow periods), median NRP time 240 mins (before in situ coldperfusion of the liver graft). hMPwasused in 5 donors (3 uDCD, 2 cDCD) for a median time
Abstracts from the 23rd International Meeting of LICAGE,Bucharest, Romania, 8-9 September 2016

216 Journal of Translational Medicine and Research, 21 (3), 2016
ORAL PRESENTATIONS
of 170 minutes. The median cold ischemia time (CIT) in the eight donors used for LT was 340 mins (range 270 – 425 mins). Atthe end of NRP, median pH was 7.26 (range 7.38 – 7.18), lactates 8 mMol/L (range 6 – 12), AST 390 UI/ L (range 55 – 550). Asper protocol, after ad hoc informed consent, eight MELD < 20 (median 10)/CHILD A (median 5) candidates suffering for HCC wereconsidered for LT (males 7/8). Median recipients’ age was 55 yo (range 54-59). Results: The follow up period ranges from 60 to 340 dd: survival rate at POD 60 is 100%: at July 30 2016 all the 8 pts are alive,at home and fit. Incidence of primary graft non function (PGNF) and early allograft dysfunction (EAD)(3) were 0 and 12.5% respec-tively. Median length of surgery was 402 min (345 – 585 min), while median estimated blood loss was 1500 ml (500 – 5000 ml).Median intraoperative requirement of packed red cells was 2 U (0-8), median intraoperative fluids infusion was 4600 ml (crystal-loids, 4000; albumin 600 ml), with a median total diuresis of 2000 ml and a median CVP ranging from 8 to 11 mmHg in the various phases of LT. At the end of the procedure, median pH was 7.35, median lactate 5 Mmol, median Hb 10.5 gr/dL. From 12to 20 hours after the end of surgery 7/8 pts were extubated (median postop intubation time 15 hours). On POD 2, Lactates were1.2 Mmol, ALT 768 UI/L, Bilirubin 1.9 mg / dL, PT (INR) and aPTT(R) 1.35 and 1.39 respectively, pCreatinine 1.08 mg/ dL. As atAugust 20, no major surgical complications and ischemic cholangiopathy have been recorded. One pt had biliary stricture due totechnical reasons. Moderate and severe acute kidney injury were absent (median pCreatinine at discharge from H 1.1 mg / dL, range0.7 – 1.6) Two pts (25%) had major infections episodes (one intraabdominal, one pulmonary) and recovered completely. MedianICU and H LOS were 5 (range 3-7) and 23 (17 – 44) days respectively.Conclusions: In spite of a long “no touch period“ (20 mins), preliminary results of this first Italian LT series performed with DCDdonors (2) are at the moment favourable and at least comparable with the most recent EU experiences (4). Key points able to impacton this favourable outcome, might be (but should not be limited to…) (a) the constant use of NRP,able to reduce liver injury, possibly inducing, after circulatory arrest, a sort of ischemic preconditioning before the cold ischemia period (5,6). NRP shouldallow a much safer prolongation of the WIT; (b) quite a short CIT; (c) an extremely favourabledonor age. The role of hMP, indeedan interesting optin, has yet to be clarified, both in our series and in the literature. In conclusion, DCD donation for LT, with a mandatory and strict selection of both donors and recipients might become , also in Italy, a concrete option to expand the donorpool notwithstanding the long“no touch period”. Further studies and much larger experience are of course mandatory to make moresolid these preliminary results. References:
1. Geraci PM, Sepe V. Non-heart-beating organ donation in Italy. Minerva Anestesiol. 2011 Jun;77(6):613-23.2. De Carlis L, Lauterio A, De Carlis R, Ferla F, Di Sandro S. Donation After Cardiac Death Liver Transplantation After More Than 20 Minutes of Circulatory
Arrest and Normothermic Regional Perfusion. Transplantation. 2016 Apr;100(4):e21-2. doi: 10.1097/TP.0000000000001136.3. Olthoff KM, Kulik L, Samstein B, Kaminski M, Abecassis M, Emond J, et al. Validation of a current definition of early allograft dysfunction in liver
transplant recipients and analysis of risk factors. Liver Transpl. 2010 Aug;16(8):943-9. doi: 10.1002/lt.22091.4. Savier E, Dondero F, Vibert E, Eyraud D, Brisson H, Riou B, et al. First experience of liver transplantation with type 2 donation after cardiac death in France.
Liver Transpl. 2015 May;21(5):631-43. doi: 10.1002/lt.24107.5. Oniscu GC, Randle LV, Muiesan P, Butler AJ, Currie IS, Perera MT, et al. In situ normothermic regional perfusion for controlled donation after circulatory
death - the United Kingdom experience. Am J Transplant. 2014 Dec;14(12):2846-54. doi: 10.1111/ajt.12927. Epub 2014 Oct 3.6. Mathur AK, Heimbach J, Steffick DE, Sonnenday CJ, Goodrich NP, Merion RM. Donation after cardiac death liver transplantation: predictors of outcome.
Am J Transplant. 2010 Nov;10(11):2512-9. doi: 10.1111/j.1600-6143.2010.03293.x.
OP-02
Renal perfusion, function and oxygenation in the early postoperative periodafter liver transplantation
Jenny Skytte Larsson, Bengt Redfors and Sven-Erik Ricksten
Department of Anaesthesia and Intensive Care, Sahlgrenska University Hospital, Gothenburg, Sweden
Introduction: Acute kidney injury (AKI) after liver transplantation is a common complication with an incidence of approximately 50%[1], associated with high morbidity and mortality. Little is known about the early effects of liver transplantation on renal perfusion,filtration and oxygenation. This information is needed in order to increase the possibilities to prevent/treat AKI after liver transplan-tation.Objectives: The aim of this study was to gain insights into renal perfusion, filtration and oxygenation in the immediate post-operative period after liver transplantation and to compare these data to those obtained from a group of patients undergoing majorsurgery with no postoperative renal impairment. Methods: Informed consent was obtained preoperatively from twelve patients with normal renal function accepted for liver transplanta-tion. Glomerular filtration rate (GFR) was measured pre-operatively by plasma clearance of Cr-EDTA. The patients were studied after livertransplantation in the ICU in the immediate postoperative period, sedated and mechanically ventilated. Systemic haemodynamics andrenal variables where obtained during two 30-min periods. Renal blood flow (RBF) and GFR were measured by the renal vein retrograde

Journal of Translational Medicine and Research, 21 (3), 2016 217
Abstracts from the 23rd International Meeting of LICAGE, Bucharest, Romania, 8-9 September 2016
thermodilution technique and by renal extraction of Cr-EDTA (=filtration fraction, FF), respectively. Arterial (a) and renal vein(rv) blood samples were taken for measurements of arterial(CaO2) and renal vein (CrvO2) oxygen contents. Renal oxygenconsumption [RVO2 = RBF x (CaO2-CrvO2)], renal oxygen delivery (RDO2=RBF x CaO2) and renal oxygen extraction [RO2Ex= (CaO2-CrvO2)/ CaO2)] were calculated. Sixty-three patientsundergoing uneventful cardiac surgery with no postoperative renalimpairment served as controls.Results: Cardiac index (65%) and systemic oxygen delivery index(62%) were higher and systemic vascular resistance index waslower (-38%) in the liver transplant group compared to controls(p<0.001). RBF was 17% higher and renal vascular resistancewas 16% lower compared to controls (p<0.05). In the liver trans-planted group, GFR was 35% lower compared to the preoperativevalue (p<0.05, fig. 1), accompanied by a 41% increase in serumcreatinine (p<0.05). After surgery, when compared to controls,GFR and FF was 23% and 40% lower, respectively (p<0.05,p<0.01), and RVO2 and RO2Ex were 42% and 24% higher,respectively, in the liver transplanted patients (p<0.01, p<0.05).RVO2 was strongly correlated to both GFR (controls r2=0.724,liver transplants r2 = 0.603), and to sodium resorption (controlsr2 = 0.739, liver transplants r2 = 0.624) in both groups. RVO2 per mmol sodium reabsorbed and per ml sodium filtered, where higherin the liver transplanted group than in the control group, as shown by the higher regression slope intercepts in the liver transplanted groupthan in the control group (fig. 2a, 2b). Conclusions: Despite the hyperdynamic systemic circulation, GFR is considerably reduced immediately after liver transplantation,most likely caused by a post-glomerular renal vasodilation, decreasing upstream glomerular filtration pressure. Renal oxygenationis impaired to a greater extent after liver transplantation compared to after cardiac surgery, due to a higher RVO2, which is not metby a proportional increase in RDO2.Reference:
1. Hilmi IA, Damian D, Al-Khafaji A, Planinsic R, Boucek C, Sakai T, et al. Acute kidney injury following orthotopic liver transplantation: incidence, risk factors, and effects on patient and graft outcomes. Br J Anaesth. 2015 Jun;114(6):919-26. doi: 10.1093/bja/aeu556. Epub 2015 Feb 10.
Figure 1 - Glomerular filtration rate before and after liver transplantation
Figure 2a - Shows the individual data on the relationship between renal oxygen consumption and GFR.
x = liver transplanted group, o = control group
a
Figure 2b - Shows the individual data on the relationship betweenrenal oxygen consumption and renal sodium reabsorption.
x = liver transplanted group, o = control group
b

218 Journal of Translational Medicine and Research, 21 (3), 2016
ORAL PRESENTATIONS
OP-03
AN INCIDENTAL FINING DURING PERIOPERATIVE USE OF TRANSOESOPHAGEAL ECOGRAPHY FOR ORTHOTOPIC LIVER TRANSPLANT
Edward Mathers, Rob Bromhead, Zoka MilanDepartment of Anesthetics, King's College, London, United Kingdom
A 62 year old female, blood group O, with alpha-1 antitrypsin deficiency presented to hospital for an orthotopic liver transplant(OLT). She had been pre-assessed 1 year previously by an anaesthetic consultant as part of the routine assessment process thatall patients undergo during consideration for transplantation. This pre-assessment identified her as being overweight (BMI 38). Herechocardiogram was unremarkable, with only trivial to mild aortic valve cusp thickening with good excursion. She underwent cardiopulmonary exercise (CPX) testing and achieved an anaerobic threshold of 7.4 mls/kg/min and peak VO2 of 14.8 mls/kg/min,with a maximum heart rate or 168 bpm and no ST-segment changes. Her ECG showed normal sinus rhythm 74 bpm, normal axis,nil else. Spirometry as within normal limits. She had minimal ascites and peripheral oedema to mid-thigh. Blood tests revealed aplatelet count of 64000, INR 1.44 and fibrinogen 0.8. At this time, she was caring for 4 foster children, living in a 2 storey house,and reported as being fully independent with an unlimited exercise tolerance. At the listing meeting, there were no objections fromany health professionals, other than advice that she should lose weight. She was subsequently placed on the waiting list for OLT,aware that as a blood group O she might have to wait for an extended period of time for a suitable organ to become available. Onthe day the patient attended for OLT, the attending anaesthetists were given a copy of the proforma that includes details of her previous anaesthetic assessment. Although the CPX results were particularly poor and her synthetic function markedly deranged,her unremarkable echocardiogram and spirometry, and functional status (reported as unlimited exercise tolerance) were reassuring. When the patient was collected for theatre, it became immediately obvious that her physical condition had changed significantly since her pre-assessment. She had gross pedal oedema up to her waist with chronic skin changes, and there was obvious large volume ascites. The patient was unable to transfer from bed to operating table, and when interrogated reported hermobility was now limited to metres and with the use of a zimmer frame. After an uneventful induction of anaesthesia, a trans-oesophageal probe was inserted to assess her cardiac function. She had a globally grossly enlarged heart, with a markedly enlargedleft atrium. Biventricular function was preserved. There appeared to be a at least mild mitral regurgitation, although this is difficult to assess accurately under general anaesthesia. The thickening of the aortic cusps was also seen, with good excursion aspreviously documented. It had the appearances of a heart that had compensated for chronic volume overload. Her underlying coagulopathy remained severe, and this became evident when inserting central venous and renal replacement catheters. She wasgiven cryoprecipitate prior to knife to skin. Her subsequent course was surprisingly uncomplicated. 9 litres of turbid ascitic fluid wasdrained. Her only period of hypotension was during reperfusion of the 3 hepatic vein piggy back DBD liver, but quickly correctedwith modest doses of vasopressor and calcium chloride. Total blood loss was in the region of 7 litres. Despite a thin initial thromboelastogram (TEG), her TEG at closure was near normal. This case highlighted not the difficulties in managing these patientsunder anaesthesia, but just how quickly and profoundly this cohort can decompensate. All patients need full anaesthetic assessment at the time of listing, but this case shows how follow-up assessment is essential for patients who wait a long time fora suitable organ, such as those with blood group O like this patient. Fortunately, despite her significant cardiac changes, surgerywas uneventful. However, a similar patient might not have such a smooth course, and prior knowledge of any changes to their physiology could help plan what might be a difficult anaesthetic.

Journal of Translational Medicine and Research, 21 (3), 2016 219
Abstracts from the 23rd International Meeting of LICAGE, Bucharest, Romania, 8-9 September 2016
OP-04
COAGULATION TESTS IN ACUTE LIVER FAILURE: THE ING AND YANG OF HEMOSTASIS. A CASE PRESENTATION
Mihai Popescu1,2, Simona Dima3, Dana R. Tomescu1,2
1Carol Davila University of Medicine and Pharmacy, Bucharest, Romania2Fundeni Clinical Institute, Anesthesia and Critical Care Dept. III, Bucharest, Romania3Fundeni Clinical Institute, Centre of Digestive Diseases and Liver Transplantation, Bucharest, Romania
Introduction: Acute liver failure (ALF) represents a life-threatening medical condition with limited chance of survival unless livertransplantation (LT) is rapidly performed. Most times, a severe coagulopathy is the hallmark of ALF. Methods: We present the case of a 9 year old child with no prior medical history admitted to hospital for acute liver failure, massive gastrointestinal bleeding, grade II encephalopathy and jaundice. Our local protocol for ALF diagnosis was applied immediately after ICU admission and the patient was listed for LT. Results: At the time of admission paraclinical results showed severe cholestasis (bilirubin = 516 umol/L) and coagulopathy(INR=5.25, PT=60.1 sec, Fibrinogen 123 mg/dl) and moderate thrombocytopenia (90000/uL). At the same time ROTEM assayshowed near normal values. Transfusion of PRBc was administered for correction of anemia (5.2 g/dL) but no other blood products were administered. An upper endoscopy was performed but no esophageal varices or portal-hypertensive gastropathywere found. A computer tomography of the abdomen and pelvis showed signs of portal hypertension - increased diameter of portal vein and superior mesenteric vein, parietal thickening of the small intestine and colon. On the 5th ICU day Wilson disease wasconfirmed and emergency living-related LT was performed. Postoperative outcome was excellent and the patient was dischargedfrom hospital 24 days later. Conclusion: We noted a severe discrepancy between standard coagulation tests and ROTEM findings. The use of ROTEM helpedus to lower unnecessary transfusion in a patient that otherwise presented with massive bleeding.
OP-05
PREDICTION OF INTRAOPERATIVE TRANSFUSION REQUIREMENTS DURING ORTHOTOPIC LIVER TRANSPLANTATION: THE VALUE OFROTEM
Antoni Sabate, Annabel Blasi, Joan Beltran, Marta Costa, Raquel Reyes, Ferran TorresDepartment of Anesthesiology, Hospital Universitari de Bellvitge, University of Barcelona Health Campus. Barcelona,Spain
Background: Although preoperative hemoglobin and MELD or one of its components may correlate with blood product usage, prediction of intraoperative blood product based on preoperatively available variables is unreliable. We hypothesized that basal(presurgery) data from Rotem may predict blood product requirements.Method: Data from a randomized, multicenter, hemoglobin-stratified, double-blind placebo-controlled trial of pre-emptive adminis-tration of concentrated fibrinogen has been analyzed. The transfusion threshold for platelets and fibrinogen were 50.000 /mm forplatelets and 1g/L of fibrinogen. For the aim of the study, data from all patients were taken together. The predicted values from amixed model for repeated measures including logistic regression and longitudinal values for preoperative data and ROTEM variables.Results: 92 patients were included; 48% received RBC’s, 17.5% platelets, 10.9% FFP, median of 2.74 g of fibrinogen were administered. 24% received tranexamic. RBC administration was related to basal: MELD Odds1.38 [1.19 - 1.60]; Hb 0.33 [0.21 -0.54]; Fibrinogen 0.35 [ 0.15 - 0.80]; Platelets 1.00 [1.00 - 1.00]; PTT 3.48 [1.25 - 9.68]; maxim amplitude-MA (0.94 [0.89 -1.00]; MA 10min 0.79 [ 0.67 - 0.95]; FibMax10 0.79 [0.66 - 0.93]. Any blood product usage was related to: MELD 1.24 [ 1.12 -1.37]; Hb 0.52 [ 0.40 - 0.69; Fibrinogen 0.27 [0.12 - 0.63] ; Platelets 1.00 [1.00 - 1.00]; MA 0.84 [0.77 -0.92]; MA 10 min 0.67[0.55 - 0.83]; FibMax10 0.71 [0.59 - 0.86]. In a multivariate analysis, only Maxim Amplitude showed prediction for RBC: Odds (per1 unit change) prereperfusion 0.92 [0.86 - 0.99], Odds (per 1 unit change) postreperfusion 0.88 [0.81 - 0.96]; ROC AUC :0.733.As well as for any blood product usage: MA Odds (per 1 unit change) prereperfusion 0.85 [0.78 - 0.93], Odds (per 1 unit change)postreperfusion 0.84 [0.76 - 0.92]; ROC AUC :0.788.Discussion and conclusions: MELD and basal Hb stratified patients at risk of blood product usage,however, basal maxim amplitude is the only predictive data in both prereperfusion and postreperfusion of the graft. Correction of Rotem parameters mayreduce blood product usage.

220 Journal of Translational Medicine and Research, 21 (3), 2016
ORAL PRESENTATIONS
OP-06
ENCEPHALOPATHY-ALWAYS TRIGGERED BY GRAFT DYSFUNCTION?
Fuat Saner, Andreas Paul, Laura MazilescuDepartment of General-, Visceral- and Transplant Surgery, Medical center Duisburg-Essen, Germany
Background: The incidence of neurological complications influences significantly the recovery of patients after liver transplantation.Neurological complications include encephalopathy, seizures, cerebral edema, central pontine and extrapontinemyelinolysis or pos-terior reversible encephalopathy syndrome. The incidence is reported up to 25%. Case report: We present the case of a 51-year-old female patient. The lady suffered from Budd-chiari syndrome. The diagnose wasmade more than one year before she presented to our center. As risk factors for thrombosis polycythemia vera and Factor V Leidenwere diagnosed. The lady was treated with coumarin together with 5-hydroxy urea and discharged from the hospital. On admissionto our hospital she was decompensated with jaundice, ascites and encephalopathy. We made a high-urgency request toEurotransplant, which was confirmed by the ELAC Audit. Within 72 hours a suitable organ was allocated and the patient was transplanted. Immunosuppression was calcineurin-inhibitor (CNI) (tacrolimus) based together with mycophenolate mofetil and corticosteroids. The trough-level of tacrolimus was 5.8ng/ml during her ICU stay. The liver function tests and synthesis parameterwere in normal range within one week. However, she developed dysarthria, dysphagia and inconstant myoclonus. The neurologicwork-up which included CCT, C-MRI was clear, but EEG indicated a drug-induced toxic effect. After switch from tacrolimus tocyclosporine A all symptoms resolved within eight days. The patient was referred to a peripheral ward on the twentieth postopera-tive day (POD) and discharged from the hospital on the thirty-six POD. Conclusions: Neurological complications after liver transplantation occur frequently, which is often associated with the CNI´s. Afterexclusion of pathological changes in CCT and C-MRI, the immunosuppression should be modulated.
OP-07
A RARE CASE OF GRAFT FAILURE
Fuat Saner, Andreas Paul, Laura MazilescuDepartment of General-, Visceral- and Transplant Surgery, Medical center Duisburg-Essen, Germany
Background: Liver transplantation was approved by the FDA as treatment of choice for end-stage liver disease (ESLD), whencyclosporine A (CSA) was launched in 1983 to avoid acute or chronic rejection. When CSA was used for immunosuppression one-year survival increased from 30% to 70-80% in different centers. Acute graft failure represents a life threatening condition. Mostpatients can only survive with emergency retransplantation. Case report: We herein report the case of a 42-year-old recipient suffering from primary biliary cirrhosis (PBC) who lost her graft sixdays after transplantation due to acute cellular rejection. The initial clinical course was uneventful. The patient could be extubated on thesecond postoperative day (POD). Immunosuppression was calcineurin-inhibitor (tacrolimus) based together with mycophenolate mofetiland corticosteroids. The trough-level of tacrolimus in the first days varied between 5-8 ng/ml. On the sixth POD the doppler ultrasoundindicated a nearly no-flow pattern of the portal vein. The patient was scheduled for an emergency relaparotomy with suspicion on portalvein thrombosis. The Fogarty maneuver did not show a thrombus formation. The reason for this no flow state was a significant edema-tous swollen and necrotic liver. The liver specimen indicated an acute cellular rejection. The transaminases increased to AST 10200U/Land ALT 3789U/L, the patient developed a dialysis dependent kidney failure, lactate went up from normal values to 10 mmol/l. We discussed this case in our transplant board and came to the conclusion that the liver would not recover. The patient was listed for emergency transplantation at Eurotransplant. After 24 hours a suitable organ was allocated. The patient received a second transplan-tation. Twelve days after the second transplantation transaminases and bilirubin were increasing again and a liver biopsy showedan acute cellular rejection. Patient received pulse dose cortisone and the tacrolimus trough-level was adjusted to 14 ng/ml. Fourdays later a second biopsy showed again signs of slight rejection, so the patient received again pulse dose cortisone. Afterwardsthere were no more signs for rejection. The recovery of the patient was prolonged due to dialyses dependent kidney failure, criticalillness neuropathy and right sided pneumonia.Conclusions: PBC is an immunologic disease,therefore these patients are more prone to cellular rejection compared to virus hepatitis patients. In the recent 20 years there has been tremendous improvement of immunosuppression, which reduced significant the number of severe life threatening rejections. However, when the flow pattern of the doppler ultrasound changes, oneshould also consider rejection as a possible diagnose, rather than technical failure, particular in patients with PBC.

Journal of Translational Medicine and Research, 21 (3), 2016 221
Abstracts from the 23rd International Meeting of LICAGE, Bucharest, Romania, 8-9 September 2016
OP-08
HEMOSTASIS DISORDERS IN A FULMINANT HEPATIC FAILURE PATIENT- A CASE REPORT
Ecaterina Scarlatescu1, Dana R. Tomescu1,2
1Department of Anaesthesia and Intensive Care III, Fundeni Clinical Institute, Bucharest, Romania2University of Medicine and Pharmacy “Carol Davila”, Bucharest, Romania
Background: Acute liver failure patients present a unique challenge in hemostasis assessment and management, especially in thecase of extracorporeal therapies or liver transplantation.Material and Methods: This is a case report of a young patient with fulminant hepatic failure due to acute HVB infection, admittedto the ICU with hepatic encephalopathy grade 4, important hepatic cytolysis, cholestasis and prolonged standard coagulation tests(SCTs). Progressive diffuse cerebral edema was diagnosed and managed with mild hypothermia, hypernatremia, hypocapnia andhigh-volume hemofiltration (CRRT) with UFH anticoagulation.The patient was not bleeding and thromboelastometry parameterswere in the normal range. In day 3 he underwent liver transplantation with minimal intraoperative bleeding, without the administra-tion of procoagulant therapies or blood products. Thromboprophylaxis was started on the first postoperative day. Complete neuro-logic recovery allowed extubation, but the postoperative evolution was complicated by the occurrence of deep venous thrombosisand low resistive index (RI) of the hepatic artery. Treatment included therapeutic anticoagulation, antiplatelet treatment, and prosta-cyclin. The evolution was favorable with complete remission of DVT and normalization of the RI of the hepatic artery.Results and Conclusions: This case illustrates the complex hemostasis disorders encountered in the perioperative management ofacute liver failure patients. In this patient, the profound alterations of standard coagulation tests were not correlated with the resultsof viscoelastic tests used, nor with bleeding in the preoperative and intraoperative period. The prothromboticstatus revealed afterliver transplant when the patient developed deep venous thrombosis and low resistive index of the hepatic artery. In conclusion, thiscase illustrates the fragile balance of procoagulant and anticoagulant factors in acute liver failure patients with prolonged SCTs butpreserved hemostatic capacity, making management and monitoring of anticoagulant therapy a difficult task.
OP-09
THROMBOCYTOPENIA IN CIRRHOSIS: AND THE CONTRIBUTION OF FIBRINOGEN TO BLEEDING RISK
S.V. Thakrar and S.V. MallettRoyal Free Perioperative Research Group. Department of Anaesthesia and Critical Care, Royal Free London, London UK
Introduction: A platelet count of <50 x 109/L is a trigger for platelet transfusion for bleeding prophylaxis in those requiring liver biopsy (1,2). However, this threshold may not be appropriate in cirrhotic liver disease. A “rebalancing” of haemostasis has beendescribed, with thrombocytopenia partially compensated for by increased Von Willebrand Factor and reduced ADAMTS-13. (3) Thecontribution of Fibrinogen to clot strength in severe thrombocytopenia in haematological conditions has also been previously shown(4). We investigated the relationship between baseline platelet count, clauss fibrinogen, maximum amplitude (MA) on thrombo-elastography (TEG), and blood loss in our Orthotopic liver transplant (OLT) population.Methods: We conducted a retrospective analysis of our OLT database (2006-2015). Baseline haematology and intraoperative bloodtransfusion, as a combination of cell salvage and estimation of 300 mls/unit of allogenic blood, was noted as a surrogate for intra-operative bleeding. 2 groups: Haemorrhage (>1200ml returned) and Non Haemorrhage (<1200 ml returned) were analysed.Statistical analysis was performed using SPSS.Results: Of 322 OLT patients, 77 were excluded due to fulminant disease; redo transplant or baseline haemoglobin (Hb) of <80g/L.114 (46.3%) were classified into the haemorrhage group,132 (53.7%) in the Non-Haemorrhage group.

222 Journal of Translational Medicine and Research, 21 (3), 2016
ORAL PRESENTATIONS
Haemorrhage Non Total P ValueHB (g/L) Haemorrhage
Mean 101.90 109.71 106.09 0.000SD 16.89 15.379 16.53
Platelets (x109/L)
Mean 83.18 107.29 96.12 0.005SD 55.03 75.14 67.53Median 67 84.5 76.0IQR 42.5 77.5 61.25
Fibrinogen (g/L)
Mean 1.96 2.60 2.3 0.000SD 0.91 1.15 1.09
Hep MA (mm)
Mean 42.15 47.71 45.14 0.001SD 12.68 11.87 12.54
Total blood returned (ml)
Mean 3323 487 1802 0.000SD 2536 419 2251
Univariate logistic regression with a cut-off of platelets < 50 x 109/L as the predictor and Haemorrhage as the outcome showed anOdds Ratio (OR) of 1.393 (95% CI 0.758-2.563; P = 0.286).ROC curves for platelets, clauss fibrinogen and predicted probabilities from multivariate analysis with Haemorrhage as the outcomeare described:
AUC 95% CI P value
Platelet Count 0.64 0.534 – 0.674 0.05
Clauss Fibrinogen 0.678 0.612-0.744 0.000
Predicted probability from multivariate 0.749 0.689-0.812 0.000analysis: UKELD, HB, Plt, Fib, MA
Conclusions: A cut off value of 50 x 109/L for platelet count is not a good predictor of intraoperative bleeding in the cirrhotic population. ROC curves show a relationship between low baseline platelet count and haemorrhage, however baseline Clauss fibrinogen level is a better predictor (AUC 0.678, 95% CI 0.612-0.744; P=<0.001). Measurement of Clauss Fibrinogen before invasive procedures provides useful information and should be included in routine pre-procedure coagulation testing in cirrhoticpatients.References:
1. British Committee for Standards in Haematology, Blood Transfusion Task Force. Guidelines for the use of platelet transfusions. Br J Haematol. 2003Jul;122(1):10-23.
2. Patel IJ, Davidson JC, Nikolic B, Salazar GM, Schwartzberg MS, Walker TG, et al. Consensus guidelines for periprocedural management of coagulationstatus and hemostasis risk in percutaneous image-guided interventions. J Vasc Interv Radiol. 2012 Jun;23(6):727-36. doi: 10.1016/j.jvir.2012.02.012.Epub 2012 Apr 17.
3. Tripodi A, Mannucci PM. The coagulopathy of chronic liver disease. N Engl J Med. 2011 Jul 14;365(2):147-56. doi: 10.1056/NEJMra1011170.4. Lang T, Johanning K, Metzler H, Piepenbrock S, Solomon C, Rahe-Meyer N, et al. The effects of fibrinogen levels on thromboelastometric variables in
the presence of thrombocytopenia. Anesth Analg. 2009 Mar;108(3):751-8. doi: 10.1213/ane.0b013e3181966675.

Journal of Translational Medicine and Research, 21 (3), 2016 223
POSTERS (P)POSTERS (P)
P-01
CORRELATION OF CLAUSS FIBRINOGEN AND TEG FUNCTIONAL FIBRINOGEN IN ACUTE LIVER FAILURE
L. Abeysundara, S.V. Thakrar, O. Pietroni, S.V. MallettRoyal Free Perioperative Research Group, Royal Free London NHS Foundation Trust, London, UK
Background: Clauss fibrinogen (CF) is the gold-standard laboratory measure of plasma fibrinogen. Thromboelastograpic functional fibrinogen (FF-TEG) provides values for estimation of fibrinogen level (FLEV) and raw-TEG fibrinogen maximum amplitude (FF-MA). Thesepermit rapid assessment of fibrinogen using near-patient testing. Good correlation between FF-TEG and CF exists for baseline measurements during orthotopic liver transplantation (OLT). However, discrepancies between TEG-FF andCF in the post-reperfusionstages of OLT have been reported1. It is uncertain whether there is a reliable correlation between FF-TEG and CFin patients withacute liver failure (ALF). We aimed to assess whether baseline FLEV or FF-MA correlate with CF during OLT for ALF. We also soughtto evaluate the association of CF and FLEV/FF-MA with bleeding risk. Method: A retrospective database analysis of OLTs for all-cause ALF was conducted. All cases predating introduction of FF-TEGmeasurement were excluded. A threshold of 1200ml red cell transfusion was used as a marker of significant intraoperative bleeding. Spearman correlation coefficients and statistical data comparisons were calculated using SPSS. Results: 24 patients were included. A statistically significant correlation was found between FLEV and CF (Spearman’s rho 0.455;p=0.025) and FF-MA and CF (rho 0.48; p=0.018). A correlation is shown between FLEV and platelet count (rho: 0.599; p=0.002)and FF-MA and platelet count (rho: 0.595; p=0.002). There was no correlation between CF and platelet count (rho 0.09; p=0.675).An association between FLEV/FF-MA and significant bleeding was also demonstrated (Table 1).
Conclusion: FLEV and FF-MA are correlated with Clauss fibrinogen in patients undergoing OLT for ALF. Clauss fibrinogen was notfound to be associated with risk of clinically significant bleeding. FLEV and FF-MA, however, were associated with bleeding risk andthis may provide useful clinical information. Overall numbers in this analysis were small and further prospective evaluation isrequired to explore these trends. Reference:
1. Yang Lu S, Tanaka KA, Abuelkasem E, Planinsic RM, Sakai T. Clinical applicability of rapid thrombelastography and functional fibrinogen thrombelastography to adult liver transplantation. Liver Transpl. 2014 Sep;20(9):1097-105. doi: 10.1002/lt.23923. Epub 2014 Aug 8.
Table 1
Group1 (n = 5) Non-sign bleed <1200 Group 2 (n = 19) Sign bleed >1200 ml p-value
UKELD
Mean 57.8 57.2 p = 0.803SD 2.167 6.67Median 59.0 59.0
Range 5 24
Platelet count
Mean 150.6 84.5 p = 0.155SD 90.85 61.2Median 145.0 62
Range 233 235
Clauss Fibrinogen
Mean 2.02 1.62 p = 0.643SD 1.78 1.47Median 1.50 1.3Range 4.6 5.2
FLEV
Mean 5.24 2.99 p = 0.049SD 1.83 2.03Median 5.10 2.40Range 4.9 8.6
FF-MA
Mean 28.70 15.83 p = 0.042SD 10.0 11.41Median 28.1 13.30
Range 26.9 47.70

224 Journal of Translational Medicine and Research, 21 (3), 2016
POSTERS
P-02
COLONISATION/INFECTION IN PATIENTS AFTER LIVER TRANSPLANTATION-1 YEAR SURVEILLANCE AT A GERMAN UNIVERSITY HOSPITAL
K. Bangert1, D. Wichmann1, L. Fischer2, S. Eckard3, S. Kluge1
1Department of Intensive Care Medicine, University Hospital Hamburg, Germany2Department of Transplantation and Hepatobiliary surgery, University Hospital Hamburg, Germany3Department of Epidemiology, Bloomberg School of Medicine, John Hopkins University, Baltimore
Introduction: Post transplantation infections are a significant threat to patients and graft survival and affect morbidity and mortality. Despite recent improvements in surgical technique, antimicrobial and antifungal prophylaxis and immunosuppression, thenumber of infectious is still high, although regional and centre to centre differences are reported. Moreover, the number of patientscolonized with multidrug-resistant (MDR) bacteria on the waiting lists for OLT increases. Thus data from different countries and centres may help to improve prevention and treatment strategies in theses patients.Methods: From January 2013 to December 2013 we prospectively enrolled 58 patients undergoing liver transplantation in our centre. Data on immunosuppressive and antimicrobial medication, clinical outcome and microbiological surveillance were collected. Microbiological isolates were classified as colonization or infection according to the criteria of the Centre of DiseaseControl and Prevention. Results: Standard immunosuppression consisting of Prednisolon, Tacrolimus and Basiliximab was given in 42 patients, the remaining 16 patients received individual combinations including CyclosporinA, Everolimus or Mycofenolat. Based on individual riskassessment antimicrobial prophylaxis was given in 32 patients. In the 30 day period post transplantation 44 patients (75%) developed an infection. Urinary tract infections (n = 23), pneumonia (n = 11), surgical site infections (n = 18) were the most frequently diagnosed. Microbiological surveillance revealed 87 isolates, 53 gram positive bacteria including 51 Enterococci, 22gram negative bacteria and 15 yeasts. Fourteen patients were colonized with MDR bacteria, 5 of them pre transplantation, theremaining 11 patients acquired the MDR pathogen post transplantation. In 6 cases the MDR pathogen was associated with infections. In 18 cases intraoperative sampling from the biliary tract revealed 15 gram positive (predominantly Enterococci) and 9gram negative isolates. No association between intraoperative isolates and future infections could be seen. Six patients died, 4 dueto septic complications and 2 due to graft failure.Conclusion: In our cohort the number of positive microbiological specimens was high and infections occurred frequently.Enterococci and gram negative bacteria were the most relevant pathogens. The rate of patients colonized with MDR bacteria pretransplantation was low, but 24% of patients acquired an MDR-pathogen throughout the 30 day period post transplantation.Nevertheless no impact on mortality or infection rates was correlated with this. Results from intraoperative microbiological sampling could not predict the kind of pathogen or infectious complication. For post transplantation prophylaxis Enterococci shouldbe included. The small number of patients and the single centre setting may limit generalization of these results.
P-03
AGREEMENT BETWEEN FIBTEM AND FIBRINOGEN PLASMA VALUES IN LIVER TRANSPLANTATION
Annabel Blasi1, Antoni Sabate2, Joan Beltran3, Marta Costa2, Raquel Reyes2, Ferran Torres4
1Hospital Clínic de Barcelona, Dept of Anaesthesiology, Barcelona, Spain 2Hospital Universitari de Bellvitge, Dept of Anaesthesiology, Barcelona, Spain3Hospital Clínic, Dept of Anaesthesiology, Barcelona, Spain 4Universitat Autonoma de Barcelona, Statistics
Background: FIBTEM have been used as transfusion criteria of fibrinogen in liver transplant (LT). Despite that overall correlationbetween FIBTEM and fibrinogen has proven to be acceptable, the agreement (i.e. linear relationship between two variables underthe constraint where the intercept is zero and the slope is one) between both parameters have not been investigated until now. Weaim to assess the agreement between FIBTEM and fibrinogen plasma values across LT procedure. Methods: Data from a randomized, multicenter, hemoglobin-stratified, double-blind placebo-controlled trial of pre-emptive administrationof concentrated fibrinogen has been analyzed. The transfusion threshold for platelets and fibrinogen were 50.000 /mm and 1g/L, respec-

Journal of Translational Medicine and Research, 21 (3), 2016 225
Abstracts from the 23rd International Meeting of LICAGE, Bucharest, Romania, 8-9 September 2016
tively; which were monitored to ensure consistency and compliance across all the research centers. Fibrinogen plasma was determinedby Clauss method. For the aim of the study, data from all patients were taken together. The predicted values from a mixed model forrepeated measures including longitudinal values for ROTEM variables were compared to the actual fibrinogen values using the Lin’s concordance coefficient.Results: 92 patients were included; 51 to the fibrinogen group and 48 to the saline group. Patient’s characteristics no differ betweengroups. In the fibrinogen group a median of 400 ml preemptive fibrinogen (3.54 g) were administered. In the saline group a median of 300 ml of preemptive saline were administered. Maximum amplitude at 10 minutes (A10MA-FIBTEM) was t he FIBTEMparameter that best predicted fibrinogen values, in both preemptive group and control? Pearson correlation coefficient was R=0.5(0.8 and 0.3 pre / post reperfusion, respectively), all p<0.001. Lin´s concordance correlation coefficient was showed in table 1.Overall, A10MA-FIBTEM correlated with fibrinogen plasma levels; however, the agreement between both parameters was unacceptably low, especially in patients with advanced stage of liver disease after graft reperfusion.
Table 1 - Lin´s concordance correlation coefficient between fibrinogen predicted values from MMRM analysis of A10MA-FIBTEM and actual plasma fibrinogen values
Lin’s concordance coefficient (95% CI)
All values 0.333 [0.287 to 0.377]
Pre-Reperfusion 0.756 [0.710 to 0.796]
Post-Reperfusion 0.144 [0.083 to 0.204]
Baseline Meld ≤ 16 0.517 [0.451 to 0.579]
Baseline Meld > 16 0.082 [0.033 to 0.131]
A10MA-FIBTEM: maximum amplitude at 10 minutes. Median MELD=16
Discussion & Conclusions: Qualitative alterations in fibrinogen synthesis (disfibrinogenemia) and hemodilution respectively, couldpartially explain these results. Studies should be conducted in other to find which one is the best predictor of blood product trans-fusion in this context.
P-04
THE USE OF TRANEXAMIC ACID IN THE PERIOPERATIVE MANAGEMENT OF PATIENTSUNDERGOINGORTHOTOPIC LIVER TRANSPLANTATION
E. Chew, E. Christopher, L. Davidson, J. Fretwell, J. Kiang, A. Shearer, L. Tan, S. Train, M. KelleherUniversity of Edinburgh, Scotland
Introduction/Background: Orthotopic liver transplantation (OLT) is a common surgical procedure indicated in patients with liver failure. It involves a myriad of complications such as haemorrhage, transplant rejection, and adverse effects from immuno-suppressants. Haemorrhages in particular increase pre- and post-transplantation mortality rates, and arise from haemostatic disturbance. Activation of the fibrinolytic cascade significantly contributes to haemorrhaging, thus antifibrinolytics such as aprotininand tranexamic acid (TA) are administered to reduce blood loss and the need for transfusion. While aprotinin used to be the standard antifibrinolytic administered in OLT, its use has been associated with an increased mortality risk and has thus beenremoved from the pharmaceutical market. This review explores whether TA can be justified as a substitute in routine OLT.Materials and methods: Four databases – Medline, Embase, Scopus and Web of Science – were used to find relevant studies. Theinclusion criteria ensured that studies were full clinical trials comparing TA with placebo/other antifibrinolytics.Results: Seven studies met the inclusion criteria. Results were qualitatively categorised into the effects of TA on blood loss, transfusion requirements, coagulation, and adverse effects such as mortality.Discussion: TA significantly reduces blood loss and transfusion requirements and is better at coagulation compared to placebo.While its ability to reduce blood loss and transfusion requirements pales in comparison to aprotinin, it is better at achieving coagulation than aprotinin. None of the studies were sufficiently powered to measure safety and mortality.Conclusion: TA is a viable alternative in OLT that would be more beneficial than forgoing the administration of an antifibrinolytic.

226 Journal of Translational Medicine and Research, 21 (3), 2016
POSTERS
P-05
PREDICTION OF FLUID RESPONSIVENESS BY RESPIRATORY VARIATION IN INFERIOR VENA CAVA DIAMETER (ΔICV) IN LIVER TRANSPLANT PATIENTS
Mariana Cojocaru1, Fadi Risk1, Yves Heurtematte1, Gilles Dhonneur1, Eric Levesque1,2
1Department of Anaesthesia and Surgical Intensive Care - Liver ICU, AP-HP Henri Mondor Hospital, Creteil, France2INSERM, Unit U955, Creteil, France
Introduction: Dynamic parameters such as the respiratory variation in inferior vena cava (IVC) diameter are accurate indices of fluidresponsiveness in septic shock patients.In patients undergoing liver transplantation, anatomical changes related to the vena cavamay exist. Indeed, LT can be performed using the standard caval replacement or side to side cavo-caval techniques.The aim of thisstudy is to assess validity of respiratory variation of ICV to predict fluid responsiveness in liver transplant recipient. Patients and methods: Forty patients undergoing liver transplantation from November 2014 to November 2015 at Henri Mondor Hospitalwere included in this prospective study. Data were recovered from medical charts. Cardiac index (CI), inferior vena cava distensibility index [∆IVC= (Dmax – Dmin) / Dmin x100] were measured before and after a passive leg raising test (PLR) using transthoracic echo-cardiography. Patients were considered to be responders and non-responders when CI increased to either ≥ 10% or < 10% after PLR.Results: Twenty-seven recipients (67.2%) were male and the median age at liver transplantation was 58 [25-70] years. The causes of livertransplantation were end stage liver disease (n=17, 42%) and hepatocellular carcinoma (n=12, 30%). The mean MELD score was 19.42± 10.42. Thirty patients (75%) were considered to be responders. There were no statistically significant differences between fluid respon-ders and non-responders in relation to clinical parameters such as age, sex and MELD score. Before the PLR test, the responders displayeda Dmin IVC lower than the non-responders(18.6 ± 2.1 mmvs. 23.3 ± 2.1 mm, p=0.01). In addition, ΔIVCwas higher in responders (15 ± 11 % vs.3±7% p=0.009). The best cut-off value for ΔVCI as defined by the ROC curve analysis was 12.5% to predict fluid respon-siveness in liver transplant recipients, for which sensibility and specificity were 56% and 90%. Conclusion: Despite the complexity of IVC anatomical changes after liver transplantation, the respiratory variation of IVC seemsvaluable in predicting fluid responsiveness in liver transplants recipients.
P-06
QUALITY OF LIFE AND ANAEMIA IN PATIENTS UNDERGOING ASSESSMENT FOR LIVER TRANSPLANTATION
J. Gan1, B. Clevenger2, T. Richards1, S.V. Mallet2
1University College London, London, UK2Royal Free Perioperative Research Group, Royal Free Hospital, London, UK
Background: Liver transplantation is not only aimed to improve survival from liver disease, but also to improve quality of life (QoL)of recipients.(1) QoLcan be affected by many factors, including liver disease, malnutrition and anaemia. We implemented a qualityimprovement project to assess the QoL of patients undergoing assessment for addition to the transplant waiting list as a baselinemeasure for their long term QoL follow up. Methods: All patients presenting for clinical assessment for eligibility for addition to the liver transplant waiting list at the Royal FreeHospital, London between October 2013 and March 2015 were given the EQ-5D-5L and Multidimensional Fatigue Inventory (MFI)QoL questionnaires to complete as part of their routine admission paperwork and collected prior to discharge. Results: 89 patients (mean age 54 (SD 10.5)) returned completed questionnaires. Median MELD was 13 (IQR 10-18). Mean Hbwas 111.2 g/L (SD 19.1) and 63% of patients were anaemic (Hb<120 g/L). MELD and Hb were inversely correlated (R2=0.1p=0.003). In the UK population 68.2% have an EQ-5D Visual Analogue Scale (VAS)>80 (out of 100). (2) Only 34% of patients hada score >80 (mean 65.5 (SD 21.5)). EQ-VAS scores were not significantly related to MELD, however, this measure was significantly correlated to Hb (p=0.031). Measures of general and physical fatigue on the MFI were significantly related to MELDscore, but not Hb. A regression model adjusting for age, MELD and Hbdid not show a significant correlation to the QoL measures. Conclusion: These patients had a reduced QoL compared to the general population. The reasons for this are multifactorial, yet therewas a variable relationship between the severity of liver disease and QoL. Significant numbers of patients are anaemic and this wasrelated to QoL in one of instruments used. Interestingly fatigue scores were more strongly related to MELD than to Hb. QoL data aswell as other physiological data should be routinely collected prior to transplantation as an additional outcome variable. References:
1. Yang, L. et al, Liver transplantation: a systematic review of long-term quality of life, Liver Int. 2014: 34: 1298–1313 2. Devlin, N.et al. Valuing Health-Related Quality of Life: An EQ-5D-5L Value Set for England, https://www.ohe.org/publications/valuing-health-related-
quality-life-eq-5d-5l-value-set-england

Journal of Translational Medicine and Research, 21 (3), 2016 227
Abstracts from the 23rd International Meeting of LICAGE, Bucharest, Romania, 8-9 September 2016
P-07
AUDIT: A DECREASING FREQUENCY IN THE USE OF INTRACRANIAL BOLTS FOR THE MANAGEMENT OF ACUTE LIVER FAILURE
Simon Heaney, Janice Davidson, Kenneth Simpson, Euan ThomsonDepartment of Anaesthesia, Critical Care and Pain Medicine, Edinburgh Royal Infirmary, Edinburgh, Scotland
Background: The onset of hepatic encephalopathy in patients with Acute Liver Failure (ALF) is associated with an increased risk of cerebral oedema and brain herniation. A failing liver leads to the accumulation of cerebral ammonia which is converted intoosmotically active glutamine that drives cerebral oedema and a rise in intracranial pressure (ICP)(1). A high ICP (>25 mmHg) isan ominous sign and is linked to a higher mortality and neurological damage in ALF survivors with or without liver transplantation. Placement of an intracranial bolt is the most sensitive and specific method available to detect a high ICP. A bolt also enables thederivation of cerebral perfusion pressure, guides evaluation of ICP lowering therapies and aids anaesthetic practice during transplantation. Critics of ICP bolt monitoring in ALF highlight the risks associated with the procedure, in particular intracerebralhaemorrhage, and the failure to show a mortality benefit from invasive monitoring (2). We sought to better understand our own practice by establishing the proportion of our ALF patients that received a bolt and whether this had changed in recent years.Methods: Single centre, retrospective audit of all patients with ALF from 1993 to 2016.Results: 1278 ALF patients were identified, mean 55 per year (SD 9.5). In total 321 received an ICP bolt, mean = 25% per year(SD 9). For the last 4 years there has been a downward trend in the proportion of ALF patients receiving ICP bolts, 16, 8,10 and13%.Conclusion: The downward trend in bolt insertion observed is likely due to a greater emphasis placed on the risks of the procedurewithin our unit. In line with the most recent evidence only the most severe acetaminophen ALF patients receive bolts (3).References:
1. Singanayagam A, Bernal W. Update on acute liver failure. CurrOpinCrit Care. 2015;21(2):134-141.2. Karvellas CJ, Fix OK, Battenhouse H, et al. Outcomes and complications of intracranial pressure monitoring in acute liver failure: A retrospective cohort
study. Crit Care Med. 2014;42(5):1157-1167.3. Fortea JI, Banares R, Vaquero J. Intracranial pressure in acute liver failure: To bolt or not to bolt-that is the question. Crit Care Med. 2014;42(5):1304-
1305.
P-08
INTRAOPERATIVE OXYGEN ADMINISTRATION IN PATIENTS UNDERGOING LIVER TRANSPLANTATION AT THE ROYAL FREE HOSPITAL, LONDON
W.J. Liew1, C.M. Morkane1,2, R.C.J. de Jonge3, D.S. Martin1,2
1University College London, London,UK2Royal Free Hospital Perioperative Research Group, Royal Free Hospital, London, UK3Sophia Children’s Hospital, Department of Neonatology, Rotterdam, The Netherlands
Introduction: Supplemental oxygen is the most commonly administered drug during general anaesthesia. Hyperoxaemia(PaO2>13.3 kPa) is associated with adverse changes to the respiratory and cardiovascular systems (1,2). This has particular relevance during liver transplantation where ischaemia-reperfusion injury (IRI) post Pringle manoeuvre is potentiated by oxygen-induced production of reactive oxygen species and immune cell activation (3). Supra-physiological partial pressures of oxygen mayhence worsen postoperative outcome. This audit of practice assessed intraoperative oxygenation during liver transplantation.Methods: This retrospective audit looked at intraoperative data for sequential liver transplants performed over a period of 15 months(October 2014 to January 2016) at the Royal Free Hospital. Data were retrieved from anaesthetic charts, arterial blood gases (ABGs)and laboratory reports. We calculated the area under the curve (AUC) of PaO2 to determine cumulative intraoperative PaO2 per hour.We calculated the percentage of operative time during which each patient had a measured partial pressure of oxygen within 4 specified ranges (determined by taking the median and IQR of all PaO2 results, fig. 1).

228 Journal of Translational Medicine and Research, 21 (3), 2016
POSTERS
Results: 118 patients were included; 69.5% were male (n= 82). The median age of all patients was 50.5 years. The median number of intraoperative ABGs per patient was 9 (range 5 to 23). AUC analysis for each patient revealed that overall, patients spent4.9% of the operation with a measured PaO2 of <13.9 kPa. For 45.5% of the overall operative time patients had a PaO2 of 13.9–24.7kPa and 43% of the time the PaO2 was 24.8 – 35.5 kPa. The PaO2 was > 35.5kPa for 6.7% of the operation.
Conclusion: We have demonstrated the presence of intraoperative hyperoxaemia throughout liver transplantation surgery. Thereappears to be no adjustment of FiO2 in response to hyperoxaemia, despite the lack of evidence that hyperoxaemia is beneficial during major surgery. Further research is required to explore this observation in other transplant centres.References:
1. Milone SD, Newton GE, Parker JD. Hemodynamic and biochemical effects of 100% oxygen breathing in humans. Can J PhysiolPharmacol. 1999;77:124-130.
2. Farquhar H, Weatherall M, Wijesinghe M et al. Systematic review of studies of the effect of hyperoxia on coronary blood flow. Am Heart J. 2009;158:371-377.
3. Zangl Q, Martignoni A et al. Postoperative hyperoxia (60%) worsens hepatic injury in mice. Anaesthesiology. 2014; 121:1217-25
P-09
COMBINED LIVER TRANSPLANTATION AND GASTRIC SLEEVE RESECTION. A CASE REPORT
F. Lucci1, J.W. Freeman, M.B. Silvi1, G. Tisone2, M. Dauri1
1Department of Anesthesia and Intensive Care, University of Rome Tor Vergata, Italy2Department of Hepatobiliary and Liver Transplant, University of Rome Tor Vergata, Italy
Background: Obesity is common even in liver transplantation (LT) yet optimal mana-gement remains unclear. Hepatobiliary inter-
Figure 1 - Example of the intra-operative oxygenation
profile of an individual patient.AUC represents the cumulativeoxygen dose. Horizontal lines
allow the visualization of proportion of time patients areoxygenated within predefined
ranges (<13.9kPa, 13.9-24.7kPa,24.8-35.5kPa, >35.6kPa)
Table 1 - Oxygenation and haemoglobin values according to operative stage for all patients
Operative stage Median FiO2 Median PaO2 in kPa Median P:F ratio in kPa Median Haemoglobin(number of samples) (IQR) (IQR) (IQR) g/l (IQR)Stage 1: dissection (330) 0.48 (0.08) 24.70 (11.2) 54.05 (21.7) 94 (25)
Stage 2: anhepatic (186) 0.49 (0.09) 25.85 (8.8) 55.51 (19.4) 89 (20)
Stage 3: reperfusion (349) 0.46 (0.10) 23.50 (9.8) 53.60 (22.2) 83 (17)

Journal of Translational Medicine and Research, 21 (3), 2016 229
Abstracts from the 23rd International Meeting of LICAGE, Bucharest, Romania, 8-9 September 2016
ventions in morbidly obese patients are associated with increased risk of bleeding, postoperative complications and mortality andmorbid obesity is a relative contraindica-tion to liver transplantation (3–6). Long term impact of obesity on post-LT outcomes including recurrence of NASH and hepatitis C virus (HCV) is becoming evident (1-3). Obesity is associated with many causes ofmorbidity and mortality post-LT (4). A non invasive approach to weight reduction may not be successful especially for those withlong-standing obesity. Bariatric surgery may be suitable for patients with early-stage li-ver disease (5), but may be contraindicated(6). Post transplant bariatric surgery may be an option (7)Material and Methods: We present the case of a 45 years old woman, BMI 38, scheduled for li-ver transplant for Hepatitis C under-going combined liver transplant and Sleeve gastrectomy. We performed the liver transplant first, cognisant of the risk of massivebleeding and hemodynamic instability. She received 2 gr of fibrinogen, 2 units of RBC, 6 unit of FFP and 5lt of crystalloid during theprocedure. The post-operative period was uneventful and pa-tient was discharged home 6 days after the combined procedure.Results: Hepatobiliary complex interventions are with many postoperative com-plications and mortality. Morbid obesity is a relativecontraindication to liver transplantation for the same reason. Our patient is currently alive after 8 month from combined procedurewith significant weight loss (BMI = 28 Kg/m2).Conlusion: Combined liver transplant plus gastric sleeve resection can be performed safely. Careful follow up to avoid malnutritionand excessive weight loss is necessary.References:
1. Contos MJ, Cales W, Sterling RK, et al. Development of nonalcoholic fatty liverdisease after orthotopic liver transplantation for cryptogenic cirrhosis. LiverTranspl 2001; 7: 363–373.
2. Dureja P, Mellingerr J, Agni R, et al. NAFLD recurrence in liver transplant recipients. Transplantation 2011; 91: 684–668. 3. Gane EJ. Diabetes Mellitus following liver transplantation in patients with hepatitis C virus: Risks and consequences. Am J Transplant 2012; 12: 531–538. 4. Watt K, Pedersen RA, Kremers WK, Heimbach JK, Charlton MR. Evolution of causes and risk factors for mortality post liver transplant: Results of the
NIDDK long term follow-up study. Am J Transplant 2010; 10: 1–8. 5. Weingarten TN, Swain JM, Kendrick ML, et al. Nonalcoholic steatohepatitis (NASH) does not increase complications after laparoscopic bariatric surgery.
Obes Surg 2011; 21: 1714– 1720. 6. Mosko JD, Nguyen GC. Increased perioperative mortality following bariatric surgery among patients with cirrhosis. Clin Gastroenterol Hepatol 2011;9:
897–901. 7. D’Hondt M, Vanneste A, Pottel, et al. Laparoscopic sleeve gas- trectomy as a sin-gle-stage procedure for the treatment of morbid obesity and the
resulting quality of life, resolution of comorbidi- ties, food tolerance, and 6-year weight loss. SurgEn-dosc 2011; 25: 2498–2504.
P-10
TRANSIENT PACE INSERTION DUE TO ELECTROCARDIOGRAPHIC DISTURBANCE DURING LIVER TRANSPLANTATION
Sivrikoz Nükhet, Yavru Hacer Ayæen, Özden Ilgin, Sarıkaya Remzi, Durmaz Ugurcan Özlem, Telci LütfiIstanbul University Medical Faculty, Dept. of Anesthesiology, Istanbul-Turkey
Introduction: We report the second case in our hospital presenting ECG rhythm disturbances during hepatic graft reperfusion.Case report: A 17 year-old male was hospitalized with jaundice and abdominal swelling. His CHILD and MELD scores were 8 and25. His past history consisted of a living-related liver transplantation due to infantile cholestasis syndrome at 9 years-old andechocardiography showed hepatopulmonary shunting. With the diagnosis of secondary biliary cirrhosis, the patient underwent asecond living-related liver transplantation. Although total of 26 units of erythrocyte suspension (ES), 20 units of fresh frozen plasma (FFP), 5 units of solution apheresis platelets (SAP), crystalloids, colloids and inotropes such as dopamine (5-15 μg/kg/min), norepinephrine (0.05-0.3 μg/kg/min) and epinephrine (0.05-0.2 μg/kg/min) were infused to the patient until the 11th hour of the surgery (2 hours after reperfusion), his heart rate was still less than 45 beats/min. He was consulted with cardiology department and temporarypacemaker inserted into the right ventricle outflow tract. The patient received 45 units of ES, 45 units of FFP and 9 units of SAP during thesurgery. He was transferred to the intensive care unit (ICU) with an arterial blood gas values of pH: 7.48, PaCO2: 36 mm-Hg, PaO2: 202.7mm-Hg, Hemoglobin: 7.9 g/dL, hemotocrit: 22.4%, Lactate: 11.2 mmol/L, Na+: 146 mmol/L, K+2: 3.2 mmol/L, Cl-1: 100 mmol/L, IonizedCa+2: 1.15 mmol/L, and under inotropic agents, after a 28-hour surgery. No anesthesia- or surgery-related complication was occured. Onthe postoperative 5th day he was extubated, and 7th day his pacemaker was removed. After his 14 days of uneventful ICU follow-up, hewas sent to the gastroenterology service and discharged before long. His 2 years follow-up has been trouble-free with normal hepatic function test values. Conclusion: In the litherature there are rare case reports reporting that inserting pace makers in the early period ensure succesfullclinical results.

230 Journal of Translational Medicine and Research, 21 (3), 2016
POSTERS
P-11
IMPACT OF INR ON TEG VELOCITY CURVES
L. Oostvogels, S.V. Thakrar, L. Abeysundara, F. Blake and S.V. MallettRoyal Free Perioperative Research Group, Royal Free London NHS Foundation Trust, London, UK
Introduction: In liver cirrhosis, a rebalancing of haemostasis has been described (1), with a reduction in both procoagulant and anti-coagulant factors. Standard tests of coagulation e.g. INR correlate poorly with bleeding (2). We investigated the relationship betweenINR and Thromboelastography (TEG), in particular Velocity Curves, in our Orthotopic liver transplantation (OLT) population.Methods: We performed a retrospective analysis of baseline TEG and INR data in 114 consecutive OLT patients from 2013-2015.We excluded those patients with fulminant hepatic failure or redo transplantation, and those with baseline haemoglobin of 80 g/L.Statistical analysis was performed using a statistics package (SPSS).Results: From a total of 63 data sets, 4 sets (6%) of data were incomplete. Table 1 shows descriptive statistics for Velocity curveand heparinase TEG parameters for INR values of <2, 2 to 2.5 and >2.5. MRTG: Maximum rate of thrombus generation (mm/min),TMRTG: time to maximum rate of thrombus generation (S), TG: Thrombus generated (mm/min).
INR <2.0 INR 2.0-2.5 INR >2.5 P valuen 50 4 5
Peak Height
Mean 4.62 2.00 1.75 0.10SD 2.76 2.0 1.71Median 4.00 4 1.50
MRTG Range 12.00 4.00Mean 3.29 1.82 1.26 0.23SD 1.87 1.94 0.96Median 2.79 3.29 1.61
TG Range 9.57 2.12Mean 447.51 388.7 316.15 0.93SD 437.04 268.9 258.89Median 577.65 392.3 368.93
Hep R Range 1800.69 681.1 608.39Mean 21.91 55.0 63.85 0.01SD 12.59 74.4 82.78Median 19.45 21.8 23.40
Hep K Range 73.40 169.1 167.40Mean 10.34 10.72 13.40 0.99SD 8.15 9.80 0.79Median 8.10 8.30 13.10
HepAng Range 52.4 1.50Mean 26.71 21.30 17.03 0.60SD 10.91 21.90 0.91Median 25.70 13.90 16.90Range 52.90 1.80
Hep MA
Mean 40.70SD 47.11 12.10 34.63 0.50Median 47.10 23.80 33.80Range 98.90 18.70
Conclusion: Trends of a decrease in peak height, MRTG and TG were apparent with increases in INR, although not statistically significant on ANOVA. R time (P= 0.01) and K time increased with a progressive increase in INR. Lower INR cut-off values (1.5)have previously been used to assess viscoelastic tests, but our results suggest that clot kinetics assessed at higher INR values mayprovide useful information. Further prospective investigation is required.References:
1. A Tripodi PM. The coagulopathy of Chronic Liver disease. N Engl J Med. 2011;365:147-56. 2. Massicotte L DA, Thibeault L, Hevesi Z, Nozza A, Roy A. Relationship between conventional coagulation tests and bleeding for 600 consecutive liver
transplantations. Transplantation. 2014;98(2):e12-3.

Journal of Translational Medicine and Research, 21 (3), 2016 231
Abstracts from the 23rd International Meeting of LICAGE, Bucharest, Romania, 8-9 September 2016
P-12
EFFECTS OF PLATELET COUNT ON ROTATIONAL THROMBOELASTOMETRY IN PATIENTS WITH END-STAGELIVER DISEASE
Mihai Popescu1,2, Dana R. Tomescu1,2
1Carol Davila University of Medicine and Pharmacy, Bucharest, Romania2Fundeni Clinical Institute, Anesthesia and Critical Care Department III, Bucharest, Romania
Introduction: The rebalanced approach in patients with End-Stage Liver Disease (ESLD) has lead to the search of new hemostatictests in such patients. Of these, ROTEM assay is used world-wide in guiding blood transfusion in the perioperative setting or in theICU. The aim of our study was to assess the impact of platelet count on ROTEM parameters in patients with ESLD. Methods: We included 162 consecutive patients with ESLD admitted to the ICU before liver transplantation. Exclusion criteria consisted of: presence of hepatocellular carcinoma, pro-hemostatic or anti-thrombotic therapy within the last 7 days, extrahepatichemostatic disorders. Recorded data included: demographic variables, standard coagulation tests, ROTEM parameters (standardparameters and derived parameters: thrombin potential index – TPI, maximum velocity of clot formation – MaxV, time to MaxV –MaxVt, area under the curve – AUC and maximum clot elasticity – MCE), liver functional tests and severity scores.Results: The mean age in our study group was 54±12.6 years and the mean MELD and MELD scores were 18.75±7.32 and19.46±7.39, respectively. The median platelet count was 73378 [12000-247000]. We found a direct linear correlation betweenplatelet count and ExTEM TPI (p=0.000, R2=0.466) and a non-linear, quadratic correlation between platelet count and ExTEM MCF(p=0.008, R2=0.451) and ExTEM MCE (p=0.000, R2=0.362). A cut-off of 70000 platelets was determined below which bothclot elasticity and firmness fall below the lower-normal limit. Conclusion: Platelet count has a significant impact on hemostasis in patients with ESLD and this can be determined using derivedROTEM parameters. Although we could determine a cut-off for platelet count below which coagulation becomes impaired, furtherdata are required in order to determine the lower safety value below which this becomes clinically significant.
P-13
PRELIMINARY RESULTS OF A PREHABILITATION PROGRAM IN LIVER TRANSPLANT CANDIDATES
R. Risco, A. Barberan, M. Ubre, A. Hervas, E. Gimeno, D. Capitan, F. Dana, G. Martinez-PalliAnesthesia Department Hospital Clinic Barcelona, Spain
Background: Postoperative complications have a strong negative impact on clinical outcomes of the liver transplantation (LT). There isevidence indicating that aerobic capacity is associated with better postoperative prognosis. Prehabilitation, defined asthe process of enhancing the functional capacity, appears as highly promising preventive intervention in candidates for LT who characteristicallyexhibit poor cardiorespiratory reserve and exercise capacity.Objective: to evaluate the feasibility and safety of a personalized physical trening program to improve aerobic capacity in LT candidates.Methods: Prospective pilot quasi-experimental study. Candidates for LT were invitedto participate in a 6 to 8-week outpatient fitness program (personalized and elapsed inthe community setting). Main outcome measures: training-induced enhancement ofaerobic capacity (endurance time [ET]) and health-related quality of life (time frame: before and after the exercise training program). Data werecompared to those from contemporaneous matched LT candidates that follow standard care.Results: Up to now, 22 patients (58±6 yr-old): 12 (preHAB-group) and 10 (control group) were included. No baseline differences in sex,age, MELD score, aerobic capacity (endurance time [ET]: 262±61 and 287±108 sec, respectively, p=0.70), physical activity (YALE index 45±8 and 43±4, respectively p=0.88), nor quality of live (CLDQ 4±0.7 and 5±1, respectively, p=0.59) werefound between groups. All patients in preHAB group followed the training program. PreHAB-group showed an increase in physical activity index (from 45±8 to 79±15, p=0.02) and CLDQ (from 4±0.8 to 5±0.5, p=0.04) and a trend to increase in aerobic capacity(ET from 262±61 to 764±383 sec, p=0.09) after the program. Control group remained unchanged after the same period.Conclusions: A personalized physical training program is feasible and may help toimprove the level of physical activity, quality oflife and probably aerobic capacity in LTcandidates. Its impact on postoperative outcome needs to be evaluated in a randomized trial.

232 Journal of Translational Medicine and Research, 21 (3), 2016
POSTERS
P-14
IMPACT ON FIBRINOGEN RICH PRODUCTS CONSUMPTION OF TWO DIFFERENT STRATEGIES FOR ANTIFIBRINOLYTIC ADMINISTRATION DURING LIVER TRANSPLANTATION
E. Rivas1, A. Blasi1, C. Fondevila2, G. Martínez-Pallí1, J. Balust1, J. Beltran1
1Anesthesia Department, 2Surgery Department, Hospital Clinic Barcelona, Spain
Background: ROTEM® helps to significantly reduce the administration of blood products during liver transplantation (LT).Additionally, ROTEM® gives the opportunity to monitor the appearance of fibrinolysis and to avoid the prophylactic use of anti-fibrinolytics. We aimed to compare the impact of two different strategies for antifibrinolytic administration during liver transplanta-tion surgery, universal prophylactic administration or administration guided by ROTEM® criteria.M&M: All LT performed during 2010 and 2015 were reviewed. Demographic, transfusion requirements and outcome data (earlygraft function, postoperative re-intervention for bleeding, thrombotic events within 6 months after LT, and long hospital stay) wererecorded. Until 2010, antifibinolytics were administered profilactically after anesthesia induction in all patients without contraindica-tion; thenceforth, antifibrinolytics were administered if fibrinolysis was detected on ROTEM®’ analysis. The rest of the transfusionpolicy was similarly according to our ROTEM® evaluation algorithm, (fig. 1).
Figure 1 - ROTEM algorithm forhaemostatic management during
liver transplantation used in Hospital Clinic of Barcelona

Journal of Translational Medicine and Research, 21 (3), 2016 233
Abstracts from the 23rd International Meeting of LICAGE, Bucharest, Romania, 8-9 September 2016
Results: 72 LT were performed during 2010, and 67 LT were performed during 2015 in our institution. Data from the overall population was: Age 56 (50-63) years, Sex 96 male/43 female, BMI 25 (22-29), MELD 16 (9-22), etiology of liver disease: 28%HCV, 26% HCC, 16% OH ,30% others, with no significant differences between both years. Antifibrinolytic (tranexamic acid) wasadministered to 59% of LT recipient in 2010, and in 29% of LT recipients in 2015 (p<0.01). Blood product requirements in 2010and 2015 are showed in table 1. The estimated increase in the global cost of the fibrinogen rich products was 20.268 euros. Therewere no differences in the outcome parameters.
Discussion & Conclusions: The administration of antifibrinolytics by ROTEM® criteria lead to a significant reduction in the anti-fibrinolyticadministration compared to the prophylactic policy. This change was accompanied by a significant increase in the fibrinogen rich productsconsumption and administration, without variations in red blood cells requirements, neither in the overall outcome. Given the cost-efficacyimplications, prophylactic vs therapeutic use of tranexamic acid deserves to be reviewed in this context.
P-15
COAGULOPATHY ASSESSMENT IN CIRRHOTIC PATIENTS WITH PORTAL VEIN THROMBOSIS OR REDUCEDPORTAL FLOW VELOCITY. A CASE CONTROL PILOT STUDY
Ecaterina Scarlatescu1, Alexandra Marcu1, Ana Maria Buruiana1, Gabriela Droc1,2, Dana R Tomescu1,2
1Department of Anaesthesia and Intensive Care, Fundeni Clinical Institute, Bucharest, Romania2University of Medicine and Pharmacy “Carol Davila”, Bucharest, Romania
Background: Portal vein thrombosis (PVT) in cirrhotic patients is usually associated with worsening outcomes. Local and/or systemic pro-thrombotic factors may play a role in the development of PVT, but risk factors associated with PVT in cirrhosis arestill under debate.The aim of this study was to assess coagulation disturbances in critically ill cirrhotic patients with recent PVT orreduced portal flow velocity and to compare the results tostable cirrhotic patients with preserved portal blood flow.Material and Methods: Cirrhotic patients with PVT or portal flow velocity less than 15 cm/s admitted in the ICU were included inthe study group (SG). Cirrhotic patients with preserved portal flow velocity were included in the control group (CG). Exclusion criteria: chronic kidney or hematologic diseases, bleeding, pregnancy, anticoagulant/antiplatelet therapy, blood derivates or procoagulantsin the last 7 days. The following tests were performed: SCTs,individual coagulation factors plasmatic levels(PLs) androtation thromboelastometry (ROTEM) with standard parameters and new parameters providing indirect measures of thrombin generation (Sorensen et al, 2003) calculated from the first derivative of the clot firmness curve: Maximum Velocity (MaxVel), Timeto MaxVel (t-MaxVel), Area under the curve (AUC). MCE (Maximum clot elasticity) was used to calculate δMCE, a parameter reflecting the platelet component of clot strength (Solomon et al, 2015).Results and Conclusions: 32 patients were included in the SG and 52 patients in the CG. SG patients had prolonged SCTs, but nosignificant differences were noted in standard ROTEM parameters or PLs. SG patients had higher t-MaxVel and AUC (p=0.017,p=0.016), MCE and δMCE( p=0.024, p=0.014) compared to CG, showing a delayed coagulation initiation, followed by increasedthrombus formation with higher platelet contribution to clot strength as compared to CG patients.These abnormalities were onlydetected by dynamic hemostasis measurements but not with SCTs. For firm conclusions, the completion of this pilot study isrequired.
Table 1 - Blood product requirements in 2010 and 2015
2010 (n=72) 2015 (n=67) pRCB, n 2 (0-4) 2 (0-3) 0,91
FFP, units 4 (0-6) 0 (0-0) 0,00
PLAT, yes / no (%) 31 / 69 15 / 85 0,023
FRP, yes / no 41 / 58 55 / 44 0,076FC, yes / no 17 / 83 47 / 52 0,000Cryoprecipitates, yes / no 26 / 74 16 / 83 0,111

234 Journal of Translational Medicine and Research, 21 (3), 2016
POSTERS
P-16
CLINICAL AUDIT PROMPTS A SOLUTION TO HANDOVER DIFFICULTIES IN ORTHOTOPIC LIVER TRANSPLANTATION (OLT)
Era Soukhin, David Cosgrave, Anand PuttappaSt Vincent's University Hospital Elm Park, Dublin, Republic of Ireland
Background: The decline in kidney function is common following orthotopic liver transplantation (OLT). Many perioperative factorsinfluence its incidence and severity. The extent of this influence in our transplant population and whether any improvement can bemade in their perioperative care are unknown. Material and Methods: Audit of perioperative events in all the OLT recipients operated on in 2015 at the SVUH (1) National LiverTransplant Centre. After accounting for preoperative variation, we assessed whether intraoperative concerns (e.g. haemodynamicfactors, surgical technique, graft quality) correlate with kidney function in the immediate post operative period.Results: Sixty-two patient files were reviewed. Due to the sample size and missing data points, no definitive conclusions could bemade regarding specific areas for service improvement. However, we discovered that salient intraoperative information was mostly hand written, in different locations within the patient file, making it difficult to form a snapshot of the intraoperative course.This posed a risk of important intraoperative information being over looked in the immediate postoperative period (2) and complicated the work of our ICU and Hepatology colleagues. Therefore we developed a single page (A4) handover template, using widely available Microsoft Office. The information can be entered via an Excel spreadsheet (presenting an opportunity for aprospective database to be maintained), automatically transferred into a Word document using Mail Merge function and then printed as the a tre-to-ICU handover.Conclusion: During our audit, we identified elements of suboptimal handover process, prompting development of an efficient solution both for handover documentation and an intraoperative event database. This solution would appeal to OLT services lacking Information Technology support and/or funding to facilitate succinct handover documentation.References:
1. St Vincent’s University Hospital, Elm Park, Dublin, Republic of Ireland2. Johnson JK, Arora VM. Improving clinical handovers: creating local solutions for a global problem. Quality and Safety in Health Care. 2009 Aug
1;18(4):244-5.
P-17
HIGH MELD SCORE AND EXTENDED OPERATING TIME PREDICT PROLONGED INITIAL ICU STAY AFTER LIVER TRANSPLANTATION AND INFLUENCE THE OUTCOME
Panagiota Stratigopoulou, Fuat H. Saner, Andreas Paul, Georgios C. SotiropoulosDepartment of General, Visceral and Transplantation Surgery University Hospital Essen, Essen, Germany
Background: Expectations for an immediate intensive care unit (ICU) stay after liver transplantation (LT) have changed remarkablyover the last decade. The present study aimed to determine the incidence of prolonged initial ICU stay after LT (>3 consecutivedays) and to identify recipient, donor, and surgical factors associated with it. Its influence on survival has also been investigated.Material and Methods: We retrospectively analyzed data of adult recipients who underwent deceased donor LT at the University Hospital Essen (11/2003 -07/2012). Exclusion criteria were death within 3 days after LT, retransplantation, multiple organtransplant and diagnosis of early allograft dysfunction after LT.Results: Of the 374 recipients finally included in our cohort, 225 (60.16%) had a prolonged ICU stay. On univariate analysis, lastdonor INR, high vasopressor doses, “rescue offer” grafts, being hospitalized at transplant, high urgency cases, labMELD at transplant, alcoholic cirrhosis, pre-LT renal replacement therapy and length of surgery were associated with prolonged ICU-stay.After multivariate analysis, only labMELD and length of surgery were independently correlated with an ICU-stay longer than 3 conscecutive days. Cut-off values for MELD and duration of LT were 19 and 293.5 min, respectively. A score was constructed indicating the probability of a recipient to stay in the ICU longer than 3 conscecutive days: 1/[1 + EXP (- (- 2.869 + 0.15 xLabMELD + 0.004 x Duration of operation (min)))](c-index = 0.72555). Moreover, prolonged intial ICU stay was also associatedwith longer total length of hospital stay (27.78±10.30 vs. 35.23±22.48, p<0.001) and impaired patient survival rates (81.7% vs.98% at 3 months, 75.7% vs. 91.6% at 1 year and 61.6% vs. 80.3% at 5 year, p<0.001).Conclusions: For recipients with optimal graft function, prediction of a prolonged initial ICU stay is feasible based on labMELD andduration of operation.

Journal of Translational Medicine and Research, 21 (3), 2016 235
Abstracts from the 23rd International Meeting of LICAGE, Bucharest, Romania, 8-9 September 2016
P-18
PREOPERATIVE CORONARY ARTERY CALCIUM SCORE AS A SCREENING TOOL FOR CORONARY ARTERYDISEASE AND PREDICTING CARDIAC EVENTS IN LIVER TRANSPLANT RECIPIENTS
Vijay Vohra, Vinayak Aggarwal, Sanjeev Rohtagi, Sanjeev Saigal, Nikunj Gupta, Annu Sarin Jolly, Seema Bhalotra, AS SoinMedanta, The Medicity, Gurgaon, India
Objective: The purpose of this study was to ascertain the role of coronary artery calcium score (CACS) as a modality of screeningthe asymptomatic patients for coronary artery disease (CAD) inpatients undergoing liver transplantation.Background: Marked haemodynamic changes are noticed in the perioperative period in the recipients of the liver transplantation andthis affects the outcome in patients with coronary artery disease. End stage liver disease is accompanied with low systemic vascular resistance thereby masking the effect of stress on the heart. Cardiovascular mortality of upto 50% and morbidity up to 80%has been reported in patients with coronary artery disease post liver transplant surgery. It is therefore important to identify thesepatients before transplant so that necessary intervention and management can be undertakenMaterial and Methods: Asymptomatic adult patients undergoing liver transplantation were screened with coronary artery calciumscore preoperatively as a modality of detecting coronary artery disease over three year period from 2013 to 2015. They were further investigated for coronary artery disease if they had other risk factors like dyslipidemia, diabetes mellitus, NASH, smoking orage more than 50 years. CT angiography or conventional angiography was performed as per protocol. The necessary interventionslike PTCA or CABG was undertaken with cardiology consultation.Results: 45 % of the asymptomatic patients undergoing liver transplantation had a CACS greater than zero, whereas 17% of patientshad CACS score > 100. Patients with CACS > 100 had significantly higher incidence of critical CAD (p=<0.05). Similarly adverse cardiovascular events were more (p=<0.05 ) in those with CACS > 100.Conclusions: CACS score of < 100 has a good negative predictive value for presence of CAD and predicts a low cardiac complication rate as well.

P-19
ACUTE FULMINANT HEPATIC FAILURE IN PREGNANCY; AN UNCOMMON PRESENTATION REQUIRINGTRANSPLANT
C. Thomas, K. RaoDepartment of anaesthesia, St James University Hospital, Leeds, UK
Background: Acute fatty liver of pregnancy (AFLP) is uncommon, occurring in around 1:20,000 deliveries. Caused by a deficiencyof fatty acid metabolism, it may be in a spectrum of disorders including intra-hepatic cholestasis of pregnancy and HELLP 1. Rarely,acute fulminant hepatic failure occurs.Patient details: A 22year old, 37/40 pregnant with twins presented to a district general hospital with abdominal pain, jaundice andencephalopathy. She was coagulopathic with a PT>320 and an APTT>240. Intra-uterine deaths were identified and a diagnosis ofAFLP was made. After transfer to St James University Hospital, coagulopathy was managed with vitamin K, Octaplas, platelets andfibrinogen. A caesarean section (CS) was performed 6 hours after arrival. After multi-disciplinary team and family discussion, super-urgent listing for transplant was made with a UKELD score of 66. Transplantation occurred 24 hours after CS; native thrombo-elastography is shown in fig. 1.
Discussion: The decision to list for transplant was difficult as hepatic function may resolve after delivery of the placenta 2 and trans-plantation for this aetiology is rare. The team at King’s Hospital, London were consulted for advice. Multi-disciplinary approach isessential and team working in this case was highly effective; the patient made a good recovery. The severity of hepatic failure was greater than expected following AFLP and the liver appeared steatotic and ischaemic at transplant. An additional pathology contributing to the marked hepatocellular necrosis seen in the explant histopathology was sought but not found.References:
1. Rajasri AG, Srestha R, Mitchell J. Acute fatty liver of pregnancy (AFLP) - an overview. J ObstetGynaecol. 2007; 27(3):237-40.2. Lee WM. Etiologies of liver disease. Semin Liver Dis. 2008; 28(2):142-152
236 Journal of Translational Medicine and Research, 21 (3), 2016
POSTERS
Figure 1

s
Journal of Translational Medicine and Research, 21 (3), 2016 237
A
Abeysundara L. ....................... 223, 230
Aggarwal Vinayak ................... 235
Ayșen Yavru Hacer ................. 229
B
Balust J. ................................... 231
Bangert K. ............................... 224
Barberan A. .............................231
Beltran Joan ............................219, 224,
232
Bhalotra Seema ...................... 235
Blake F. .................................... 230
Blasi Annabel .......................... 219, 224,
232
Bromhead Rob ....................... 218
Brunetti A. .............................. 215
Buruiana Ana Maria ............... 233
C
Capitan D. ............................... 231
Chew E. ................................... 225
Christopher E. ......................... 225
Clevenger B. ........................... 226
Cojocaru Mariana ...................226
Cosgrave David ....................... 234
Corti A. .................................... 215
Costa Marta ............................ 219, 224
D
Dana F. .................................... 231
Dauri M. .................................. 229
Davidson Janice ...................... 227
Davidson L. ............................. 225
De Carlis L. .............................. 215
De Carlis R. .............................. 215
De Gasperi A. .......................... 215
De Jonge RCJ .......................... 227
Dhonneur Gilles ...................... 226
Dima Simona .......................... 219
Droc Gabriela .......................... 233
E
Eckard S. .................................... 224
F
Fischer L. .................................... 224
Fondevila C. ............................... 232
Freeman J.W. ............................. 228
Fretwell J. .................................. 225
G
Gan J. ......................................... 226
Gimeno E. .................................. 231
Gupta Nikunj ............................. 235
H
Heaney Simon ........................... 227
Hervas A. ................................... 231
Heurtematte Yves ..................... 226
I
Ilgin Özden ................................. 229
J
Jolly Annu Sarin ......................... 235
K
Kelleher M. ................................ 225
Kiang J. ....................................... 225
Kluge S. ...................................... 224
L
Larsson Jenny Skytte ................. 216
Levesque Eric ............................ 226
Liew WJ ...................................... 227
Limuti R. ..................................... 215
Lucci F. ........................................ 228
Lütfi Telci ................................... 229
M
Mallet S.V. ............................... 221, 223,
226, 230
Marcu Alexandra .................... 233
Martin D.S. .............................. 227
Martinez-Palli G. ..................... 231, 232
Mathers Edward ..................... 218
Mazilescu Laura ...................... 220
Mazza E. .................................. 215
Milan Zoka .............................. 218
Morkane C.M. ......................... 227
N
Nükhet Sivrikoz ...................... 229
O
Oostvogels L. .......................... 230
Özlem Durmaz Ugurcan ........ 229
P
Pagan de Paganis C. ............... 215
Paul Andreas .......................... 220, 234
Pietroni O. .............................. 223
Popescu Mihai ....................... 219, 231
Puttappa Anand ..................... 234
R
Rao K. ...................................... 236
Raquel Reyes .......................... 219, 224
Redfors Bengt ......................... 216
Remzi Sarıkaya ........................ 229
Richards T. .............................. 226
Ricksten Sven-Erik .................. 216
Risco R. ................................... 231
Risk Fadi .................................. 226
Rivas E. .................................... 232
Rohtagi Sanjeev ...................... 235
Russo F. ................................... 215
ABSTRACTS - AUTHOR INDEX

238 Journal of Translational Medicine and Research, 21 (3), 2016
Abstracts - Author Index
S
Sabate Antoni .......................... 219, 224
Saigal Sanjeev ......................... 235
Saner Fuat H. .......................... 220, 234
Scarlatescu Ecaterina .............. 221, 233
Shearer A. ................................ 225
Silvi M.B. .................................. 228
Simpson Kenneth .................... 227
Soin A.S. ................................... 235
Sotiropoulos Georgios C. ........ 234
Soukhin Era ............................. 234
Stratigopoulou Panagiota ....... 234
T
Tan L. ....................................... 225
Thakrar S.V. .............................. 221, 223
230
Thomas C. ................................ 236
Thomson Euan ........................ 227
Tisone G. .................................. 228
Tomescu Dana R. ................... 219, 221
231, 233
Torres Ferran ........................... 219, 224
Train S. ..................................... 225
U
Ubre M. ................................... 231
V
Vohra Vijay .............................. 235
W
Wichmann D. .......................... 224
Z
Zanierato M. ........................... 215

INFORMATIONS FOR AUTHORS
SCOPESCOPE
The Journal of Translational Medicine and Research (JTMR) will consider for publication articles of clinical research in allmedical fields.
You can send original articles, new surgical techniques, clinical case presentations, letter to the editor, or comprehensivegeneral reports on surgical topics.
The journal este published quartely and articles are accepted for publication in English language.
ONLINE MANUSCRIPT SUBMISSIONONLINE MANUSCRIPT SUBMISSION
The Journal of Translational Medicine and Research (JTMR) only accepts electronic submission of manuscripts, directlyonto the journal’s Web site. Electronic submission saves time and allows the manuscript to be handled in electronic formthroughout the editorial process. To submit a manuscript electronically, please go to our website www.jtmr.ro / SubmitArticle.
Manuscripts must be submitted by one of the authors of the manuscript, and should not be submitted by anyone on theirbehalf.
During submission you will be asked to provide a cover letter – click on the terms and conditions.
OPEN ACCESSOPEN ACCESS
The Journal of Translational Medicine and Research (JTMR) provides free access to the full text of articles.
DUPLICATE PUBLICATIONDUPLICATE PUBLICATION
Manuscripts are reviewed for possible publication under the understanding that they are being submitted only to JTMRand have not been published, simultaneously submitted, or already accepted for publication elsewhere.
Copies of any possibly duplicate published material should be submitted with the manuscript under consideration, witha statement in the cover letter as to why the manuscript currently being submitted is not a duplicate publication.
CONFLICTS OF INTERESTCONFLICTS OF INTEREST
Authors must state all possible conflicts of interest in the manuscript, including financial, consultant, institutional andother relationships that might lead to bias or to a conflict of interest. If there is no conflict of interest, this should also beexplicitly stated as none declared. All sources of funding should be acknowledged in the manuscript. All relevant conflictsof interest and sources of funding should be included on the title page of the manuscript with the heading “Conflicts ofInterest and Source of Funding”.
ETHICAL POLICIESETHICAL POLICIES
When reporting experiments on human subjects, authors should indicate whether the procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Committee for Human Rights. If doubt exists whether or not the research was conductedin accordance with the Helsinki Declaration, the authors must explain the rationale for their approach and demonstratethat the institutional review body explicitly approved the doubtful aspects of the study. When reporting experiments onanimals, authors should indicate whether the institutional and national guide for the care and use of laboratory animalswas followed.
COPYRIGHT ASSIGNMENTCOPYRIGHT ASSIGNMENT
Papers are accepted for publication under the understanding that exclusive copyright in the paper is assigned to JTMR.Authors are asked to sign a copyright assignment form after the acceptance of their papers (www.jtmr.ro / For Authors /Copyright Agreement).
Signature of the copyright form is a condition of publication and papers will not be passed to the publisher unless a signedform has been received.
Please return the completed and signed Copyright Agreement to: [email protected]
PERMISSIONSPERMISSIONS
Authors must submit written permission from the copyright owner (usually the publisher) to use direct quotations, tables,or illustrations that have appeared in copyrighted or published form elsewhere, along with complete details about the
Journal of Translational Medicine and Research, 21 (3), 2016 239

source. Any permissions fees that might be required by the copyright owner are the responsibility of the authors requesting use of the borrowed material, not the responsibility of the journal JTMR.
AUTHORSHIPAUTHORSHIP
All persons listed as authors are assumed to have been actively involved in one or more key aspects of the reported study.All authors must confirm that they have met the criteria for authorship as established by the International Committee ofMedical Journal Editors (http://www.icmje.org). Full responsibility for the content of articles lies with the authors.
MANUSCRIPT PREPARATIONMANUSCRIPT PREPARATION
Articles submitted to the journal must be written in English language. The journal only accepts electronic submission ofmanuscripts in Word format. Do not send your manuscripts in PDF format. Manuscripts should be typed (font size 11),double spaced on A4 paper, including tables, figures and references.
Recommended dimension of the articles is: - 8-10 pages for an original article (clinical studies, surgical treatment); - 3-4pages for case-reports; - 1-2 pages for: book references, reviews of certain periodicals, reports concerning the work of different societies or scientific acts.
Title pageThe title page should include: - the title of the article; - full name of each author involved; - name of department(s) andinstitution(s) with which each author is affiliated; - the corresponding author’s full name, postal address, phone and faxnumber and e-mail address; - information regarding whether the authors consider the paper an Original Article, CaseReport etc.; - cite all sources of support for the work being reported, including grants, equipment etc.
AbstractThe articles must include abstract in English language. Structured Abstract (for Original Articles only) of no more than 200words, stating Background, Methods, Results, and Conclusions, or Standard abstract (for Case Reports, Reviews, SurgicalTechniques - short abstract); Key words - up to six.
IntroductionIntroduction - which explicitly shows why certain subject attracted the author’s attention (the reasons for accomplishingthe study) and presents a concise depiction of the actual stage of the matter at hand; in this section just a minimum number of bibliographic references should be quoted, without an exhaustive presentation of the literature.
Material and MethodMaterial and Method - should clearly describe the recruitment criteria of the patients in the study, the pursued clinicaldata, number of observations (for clinical studies) or entire description of the animal lots (for experimental studies). Thestatistic methods and special laboratory measurements should also be mentioned, with bibliographic references.
ResultsResults - should include the findings of the work, presented in a logical order of tables, images, pictures. The content ofthe tables or images should not be repeated as information in the text.
DiscussionsDiscussions - must include the comparison of personal results with similar data from the medical literature. New perspec-tives revealed by the study should be underlined and their implications, as well as the study limits must be commented.The data shown in the “Results” section should not be repeated. It is recommended to avoid assertions that cannot besupported by bibliographic references or by the study’s results.
ConclusionsConclusions - explains the significance of the work.
AcknowledgementsAcknowledgements - the persons that contributed to the study, but were not included as authors, should be mentionedjust in case.
ReferencesBibliographic references, Romanian or foreign, should be numbered in the order in which they appear in the text. The reference to the quoted text will be marked with Arabian numbers inside round brackets. It is mandatory for all sourcesincluded in the “References” section to be quoted in the text and references to works that do not appear in “References”
240 Journal of Translational Medicine and Research, 21 (3), 2016

should not occur. Journal titles should be abbreviated according to international style (see Index Medicus). Only referencesthat were consulted by the authors of the article should be quoted. See below eight examples of accurate citation:
journal article1. Halpern SD, Ubel PA, Caplan AL. Solid-organ transplantation in HIV-infected patients. N Engl J Med. 2002 Jul 25;347(4):284-7.
journal article with more than six authors2. Rose ME, Huerbin MB, Melick J, Marion DW, Palmer AM, Schiding JK, et al. Regulation of interstitial excitatory amino acid
concentrations after cortical contusion injury. Brain Res. 2002 May 10;935(1-2):40-6.
volume with supplement3. Geraud G, Spierings EL, Keywood C. Tolerability and safety of frovatriptan with short- and long-term use for treatment of migraine
and in comparison with sumatriptan. Headache. 2002;42 Suppl 2:S93-9.
article not in English4. Ellingsen AE, Wilhelmsen I. Sykdomsangst blant medisin - og jusstudenter. Tidsskr Nor Laegeforen. 2002;122(8):785-7. Norwegian
article published electronically ahead of the print version5. Yu WM, Hawley TS, Hawley RG, Qu CK. Immortalization of yolk sac-derived precursor cells. Blood. 2002 Nov 15;100(10):3828-31.
Epub 2002 Jul 5.
journal article on the Internet6. Abood S. Quality improvement initiative in nursing homes: the ANA acts in an advisory role. Am J Nurs (Internet). 2002 Jun (cited
2002 Aug 12);102(6):(about 1 p.). Available from: http://www.nursingworld.org/AJN/2002/june/Wawatch.htmArticle
monograph7. Murray PR, Rosenthal KS, Kobayashi GS, Pfaller MA. Medical microbiology. 4th ed. St. Louis: Mosby; 2002.
chapter in a book8. Meltzer PS, Kallioniemi A, Trent JM. Chromosome alterations in human solid tumors. In: Vogelstein B, Kinzler KW, editors. The
genetic basis of human cancer. New York: McGraw-Hill; 2002. p. 93-113.
TablesTables must be at the end of the manuscript. The citation should appear in the order of entry in the text. Each table, complete with title and footnotes, should be on a separate page, and should be constructed using the table function within a Word type document; do not insert the table as a picture.
IllustrationsIllustrations must be at the end of the manuscript. Illustrations should be numbered consecutively according to the orderin which they have been first cited in the text. The authors should point within the text the place where the illustrationsshould be located. All illustrations must have legends. The legends should allow the interpretation of the images withoutreference to the text. The format for electronic submission is TIFF or JPG. Images should be professionally drawn and photographed; freehand is unacceptable. Pictures must be at least 300 dpi to ensure quality. Do not use too large images.If photographs of persons are used, the subjects must not be identifiable, or their pictures must be accompanied by written permission to use the photograph. If an image has been previously published, acknowledge the original sourceand submit written permission from the copyright holder to reproduce the material.
Colour pictures: The Journal of Translational Medicine and Research (JTMR) accepts for publication colour images that willenhance an article. Authors who submit colour images will receive an estimate of the cost for colour reproduction. If theydecide not to pay for colour reproduction, they can request that the images be converted to black and white at no charge.
AbbreviationsIt is recommended that all measurements be converted to international units and in SI. Only internationally acceptedabbreviations should be used.
MANUSCRIPT SUBMISSION REQUIREMENTSMANUSCRIPT SUBMISSION REQUIREMENTS
Address questions about submissions to: [email protected]
AFTER ACCEPTANCEAFTER ACCEPTANCE
Page proofs and corrections: when a manuscript has been edited and is ready for printing, a copy of the proof will be sentto the author by e-mail as a PDF file. At this stage, authors may make minor corrections; significant changes to the manuscript are not accepted.
Proofs must be checked carefully and corrections sent in 48 hours beginning with the time of delivery.
Journal of Translational Medicine and Research, 21 (3), 2016 241