Embed Size (px)
DESCRIPTION
...........
Citation preview

Incidence of Colorectal Cancer
Colorectal cancer affects about 5% of the population, with up to 150,000 new cases per year in the United States alone. Cancer of the large intestine accounts for 21% of all cancers in the US, ranking second only to lung cancer in mortality in both males and females. It is, however, one of the most potentially curable of gastrointestinal cancers. Colorectal cancer is detected through screening procedures or when the patient presents with symptoms. Screening is vital to prevention and should be a part of routine care for adults over the age of 50 who are at average risk. High-risk individuals (those with previous colon cancer, family history of colon cancer, inflammatory bowel disease, or history of colorectal polyps) require careful follow-up.
There is great variability in the worldwide incidence and mortality rates. Industrialized nations appear to have the greatest risk while most developing nations have lower rates. Unfortunately, this incidence is on the increase. North America, Western Europe, Australia and New Zealand have high rates for colorectal neoplasms (Figure 1).
Figure 1. Geographic distribution of sporadic colorectal cancer.
Typical Causes of Colorectal Cancer
The development of cancer of the colon and rectum is thought to be influenced by diet, genetic, and environmental factors. The incidence of colorectal cancer increases with age beginning at 40 but remains relatively low until the age of 50 and then rapidly accelerates. This prevalence appears to double with each successive decade until about age 80. Those with a personal history of adenomas or colorectal cancer are at increased risk. Individuals with a family history of colorectal cancer or adenomas, various genetic polyposis and nonpolyposis syndromes, other cancers, and inflammatory bowel disease are also at higher risk of developing colorectal cancer. It is important to note, however, that most patients have no identifiable genetic risk factors (Figure 2).

Figure 2. Incidence of types of colorectal cancer in the United States.
Where in the colon does colorectal cancer occur?
Colorectal adenomas have a potential to progress to malignancy. Malignancy may spread by direct extension into other organs in the abdominal cavity. Invasion of the lymph vessels leads to lymph node metastases and invasion through the blood stream (hematogenous) can result in metastasis to distant sites such as the liver. Figure 3 illustrates the distribution of colorectal tumors.

Figure 3. Frequency and location of colon and rectal cancers.
ANATOMY
The term colorectal cancer refers to cancer that arises in the lower gastrointestinal tract, which is divided into the cecum, the ascending (right) colon, the transverse colon, the descending (left) colon, the sigmoid colon, and the rectum. The large intestine (colorectum) begins at the cecum, which is a pouch of approximately two to three inches in length. Ileal contents empty into the cecum through the ileocecal valve. The appendix extends from the base of the cecum.
The ascending colon rises from the cecum along the right posterior wall of the abdomen, to the right upper quadrant and to the undersurface of the liver, where it turns toward the midline (hepatic flexure), becoming the transverse colon. The transverse colon crosses the abdominal cavity toward the spleen in the left upper quadrant; where it turns downward at the splenic flexure. Continuing along the left side of the abdomen, the descending colon turns medially and inferiorly to form the S-shaped sigmoid colon. The rectum makes up the last five to ten inches of the large intestine, beginning from the end of the sigmoid colon down to the anal canal.
The rectum is located within the pelvis and is not a true intra-abdominal structure. The diameter of the rectum is larger than that of the colon, and serves primarily as a storage reservoir.
The pelvic musculature, or levator ani muscles and the internal and external anal sphincter muscles, bind the most distal rectum and anus. The sphincter muscles maintain bowel continence.

Normal colorectal anatomy. A: anatomy of the colon; B: anatomy of the rectum.
The entire large intestine is approximately five to six feet in length, with a diameter that varies from one to two inches.
It is the site of salt and water absorption. Glands secrete large quantities of alkaline mucus that lubricates the intestinal contents and neutralizes acids formed by bacteria in the intestine. These bacteria aid in the decomposition of undigested food residue, unabsorbed carbohydrates, amino acids, cell debris, and dead bacteria through the process of segmentation and putrefaction. Short-chain fatty acids formed by bacteria from unabsorbed complex carbohydrates provide an energy source for the cells of the left colon. Maintenance of potassium balance is also performed by the colon, wherein the epithelium absorbs and secretes potassium and bicarbonate.
Next: From Polyp to Cancer
Almost all colorectal cancer starts in the mucosa the inntermost lining of the large intestine. The intestines are made of five layers. Starting from the inside of the intestine or lumen (lumen refers to the empty space or cavity), the first layer is the mucosa where nutrients, fats and proteins are absorbed from the foods we eat (this is also the layer that is biopsied during a colonoscopy). Next is the muscularis mucosa that forms a barrier between the mucosa and the third layer called the submucosa. The submucosa is rich in vessels that provide the intestines with their blood supply while carrying the digested nutrients away to other vital organs. The fourth layer is the muscularis propria, which acts to propel food through the intestines, and the outermost layer is the serosa.

Colorectal cancers usually begin as benign polyps that grow from the mucosa. Some individuals are more likely than others to develop polyps, especially those with a personal or family history of polyps and/or colorectal cancer, and those that carry specific genes for hereditary forms of colorectal cancer. New information has also indicated that individuals who have type 2 diabetes and those who are considered obese are also at greater risk for developing polyps and colorectal cancer.
Most polyps remain benign and are often termed hyperplastic polyps. The likelihood that hyperplastic polyps will become cancer is very low. Other benign polyps are sometimes referred to as pre-cancerous. These polyps are not malignant, themselves, but have a chance of becoming cancerous if not removed. Examples include adenomatous and hamartomatous polyps. Adenomatous polyps that have tubular or villous characteristics have a higher chance of becoming cancerous. Adenomatous and hamartomatous polyps are also the types of polyps that are usually associated with hereditary colorectal cancer syndromes. The only truly Òmalignant polypÓ is one that has been shown to contain invasive carcinoma. Sometimes the carcinoma is confined to the polyp, and other times it has invaded one or more layers of the intestine.
Adenomas usually grow on a stalk, resembling small mushrooms. They tend to grow slowly over a decade or more. The risk of an adenoma developing into cancer increases as the size of the adenoma increases and with the amount of time the have been growing in the colon. Adenomas that are malignant are called adenocarcinomas. In the very early stages, abnormal cells are contained inside the polyp and can be easily removed by colonscopy before the develop into invasive cancer. However, as cancer cells grow and divided within the polyp, they can eventually invade nearby colon tissue and grow into and beyond the wall of the colon or rectum. If the cancer becomes advanced, the tumors will grow though all of the tissue layers of the colon rectum, and may metastasize, shedding cells into the circulatory system, spreading the cancer to other organs such as the liver and lungs.
Progression from Polyp to Cancer
Fewer than 10% of all adenomas become cancerous, however, more than 95% of colorectal cancers develop from adenomas. Recent research has also shown that some polyps long considered to be benign may also become cancerous as well. For this reason, doctors will remove all polyps during a colonoscopy screening. Small polyps are easily and painlessly removed, as they are snared and severed with a retractable wire loop that is passed through the colonoscope. As well, very small polyps may be destroyed with an instrument that delivers heats the polyps, delivering a small burst of electrical current. Very large polyps may require surgery, whether they are benign or cancerous.
Abnormal cell growth and inflammation can be another precancerous condition of the colorectal tissue, and is known as dysplasia. The abnormal areas and inflammatory polyps will be biopsied and sent to a pathologist who will examine the tissue form malignant cells. If they are benign, as they often are, then no further treatment is necessary,
Cut away view of rectum and magnification of the various layers colonic tissue.

though your doctor will recommend a routine colonoscopy schedule to keep track of the area of your colon that appears abnormal.
The Discovery and Science of the Polyp to Cancer Progression
Scientists at Johns Hopkins were the first to describe the progression of a polyp to a colorectal cancer. Dr. Bert Vogelstein discovered that colorectal polyps and colorectal cancer develops as a result of genetic mutations or other chemical modifications, causing inactivation or promotion of specific genes known as tumor suppressor and tumor promoter genes. The ÒVogelgramÓ shown below, depicts the specific molecular events as a polyp transitions to a cancer. This genetic model of the pathway of colorectal cancer results from chromosomal instability, and details some of the most common point mutations that occur in colorectal cancer related tumor suppressor genes, such as APC, P53, as well K-ras, a common tumor promoter gene.
Vogelgram detailing the molecular alterations in multiple genes that cause Colorectal Cancer to develop in well-defined stages within an individual cell
As the Vogelgram depicts, the adenoma is considered to be the precursor lesion to CRC, occurring rarely in individuals under 49 (1.7-3.5%), but becoming more prevalent later in life. In the 6th, 7th, and 8th decades of life the prevalence of adenomas has been estimated to occur at a rate of 10%. The dwell time of an early adenoma to its maturation into an advanced adenoma has been projected to be approximately 2-5 years. Similarly, the dwell time of an advanced adenoma has been estimated at 2-5 years, before it matures into an early cancer.
Next: Diagnosis
Diagnostic tests are often performed when an individual exhibits signs and symptoms of colorectal cancer or laboratory studies suggest a cancer may be present. Often a doctor can make a preliminary diagnosis based on the results of a biopsy of a tumor polyp that was removed during colonoscopy. This is especially true if there is a single precancerous or benign polyp and no family history or personal history of cancer. If a polyp or cancer is found however, your doctor will often recommend a series of tests in order to fully consider all factors when making a diagnosis of colorectal cancer.
Diagnostic tests can help you and your medical team make a number of decisions. They can help to confirm the presence of cancer, or rule it out. In cases where cancer is discovered, the tests can help to determine three criteria
the grade of the cancer or how aggressive it may be
the extent of the cancers invasion into the intestinal wall (the stage)

whether the cancer has spread (metastasized)
Biopsies & The definition of poorly, well and moderately differenitated
Polyps that are removed during a colonoscopy are sent to the pathology lab to be be examined and tested. Pathologists use a grading system to asses the severity of an individual cancer. This system is based on how closely the tumor cells resemble normal cells. As normal cells grow and develop they differentiate, which simply means that they become more specialized based on where they are in the body. Pathologists can view cells under the microscope and discern a difference between the different cells in the body, for example colon cells look distinctly different than liver cells, which look distinctly different than breast cells. Normal cells in different tissues of the body are considered to be fully differentiated, whereas cancer cells are not fully differentitated. If the cancer cells look very similar to normal cells and are grouped together in an organized fashion, they are called well differentiated.
Cancer cells fall into one of three categories:
Well Differentiated cancer cells which appear to be most similar to normal cells
Moderately Differentiated cancer cells which appear to be somewhat different than normal cells
Poorly Differentiated cancer cells which appear very different than normal cells
Click on each image below for enlarged versions of the different levels of differentiation:
poorly differentiated moderately differentiated well differentiated
Blood Tests
If colon cancer is diagnosed, your medical team will draw your blood to assess various factors which are used to assess the nature of the cancer.
CEA Colorectal cancer may produce high levels of a protein molecule known as carcinoembryonic antigen (CEA). While this test is not reliable for detecting early colorectal cancers, it is a useful tumor marker which can indicated the progress of your treatment. Levels of CEA are measured before treatment in order to provide your medical team with a baseline so that they can track your CEA throughout and following treatment. For surgery, CEA levels may be measured both before and after surgery to evaluate

both the success of the surgery. The CEA should decrease when treatment is successful, however in some cases chemotherapy and radiation therapy can cause a temporary rise in CEA due to the death of tumor cells and release of CEA into the blood stream. After surgery, with a curative resection of the cancer the CEA should return to normal in one to four months. Approximately 50% of patients with stage II and III cancers have elevated CEA levels.
Normal CEA Levels:
Nonsmokers: Less than 3 nanograms per milliliter (ng/mL) or 3 micrograms per liter (mcg/L).Smokers: Less than 5 ng/mL (or 5 mcg/L)
CBCA complete blood count (CBC) is a standard diagnostic test that determines the amount of red and white blood cells in your blood. This information can alert the doctor to whether you have an infection or anemia. Anemia can be a sign of cancer and is often times a side effect of chemotherapy. If you are receiving chemotherapy, your medical team will perform a CBC before each infusion in order to ensure you have an adequate number of white and red blood cells.
Imaging Tests
X-raysIf colon cancer is being diagnosed, your doctor may order a chest x-ray to see if cancer has spread to the lungs.
Intraoperative ultrasoundThe intrapoperative ultrasound is used during surgery to determine whether cancer has spread to the liver. The liver can be directly measured with a special probe that fits onto the end of the ultrasound device, giving doctors a much more accurate picture than one that is taken through the skin with a CT scan.

Intraoperative ultrasound with special probe fitted for imaging the liver directly
Magnetic resonance imaging (MRI)This imaging procedure uses radio waves and strong magnets to create images of the interior of the body. MRI scans are helpful in looking for colon cancer that has spread to other parts of the body, particularly, the liver, brain, and spinal cord. An MRI often takes longer than CT scans and you may have to be placed inside a narrow cylinder or tube for the test. An MRI machine makes a loud clicking and thumping noise, which your radiologist will help to ease by providing you headphones with music to block out the noise.
Computed Tomography (CT & Spiral CT Scans)CT imaging combines special x-ray equipment with sophisticated computers to produce multiple images or pictures of the inside of the body. These cross-sectional images of the area being studied can then be examined on a computer monitor or printed. CT scans of internal organs, bone, soft tissue and blood vessels provide greater clarity and reveal more details than regular x-ray exams. Using specialized equipment and expertise to create and interpret CT scans of the body, radiologists can more easily diagnose problems such as cancers, cardiovascular disease, infectious disease, trauma and musculoskeletal disorders. A CT scan may be used if colorectal cancer has metastasized to other organs. Spiral CT scans provide three-dimensional images at a lower dose of radiation than regular CT scans.

CT scan of the pelvis.
Positron emission tomography (PET)The PET scan is used along with CT scans to search for metastasized cancer. Before a PET scan, the radiologist will inject a radioactive sugar solution into your vein. Since cancer cells absorb sugar in higher amounts than do normal cells, cancer cells are easily visualized by the radiologist as they take up the sugar. A PET scan will appear mostly dark except for areas where the cancer is absorbing high amounts of the sugar, these areas will appear as Òhot spotsÓ to the radiologist (see images below). PET scans are often combined with a CT scan in a very accurate PET-CT scan, helping your medical team to more accurately visualize where the cancer cells are within your body.
Rectal cancer on FDG PET imaging showing intense glucose metabolism where the cancer is located. FDG is a glucose tracer that indicates tissue metabolic activity in terms of
Colorectal cancer showing metastatic disease to the liver on FDG PET imaging. The heart shows the most FDG uptake (normal). Just below and to the right are two foci of increased FDG uptake

regional glucose uptake. showing cancer in the liver.
Rectal cancer on PET/CT imaging showing intense glucose metabolism as well as a detailed anatomical view.
Next: Staging Colorectal Cancer
If a colon polyp or cancer has been discovered on a colonscopy, your medical team may perform many tests to classify the stage and grade of colorectal cancer. Staging and grading are universal systems to describe, evaluate and compare a particular cancer and its treatments, so that health professionals can communicate on the same level across the world.
As is displayed below, polyps have the potential to turn into cancer if they remain in the colon for a long period of time as shown below. This process is discussed in great detail in the section From Polyps to Cancer.
Adenomatous polyps and adenocarcinoma are epithelial tumors of the large intestine, and the most common and clinically significant of intestinal neoplasms. The potential for polyps or adenomas to develop into cancer increases with the age of the patient. Adenomas larger than one centimeter, with extensive villous patterns, have an increased risk of developing into carcinomas.
Progression from Polyp to Cancer

The vast majority of colorectal cancers are adenocarcinomas, tumors that arise from the mucosa cells of the colon. While most adenocarcinomas are well or moderately differentiated, approximately 15% are poorly or undifferentiated tumors. These tumors are associated with a poorer prognosis. Mucinous or colloid carcinomas, with moderate to prodigious mucin production, are also associated with less favorable five-year survival rates.
Staging of Colorectal Cancer
Staging of colorectal cancer refers to how far a cancer has spread on a scale from 0 to IV, with 0 meaning a cancer that has not begun to invade the colon wall and IV describing cancer that has spread beyoned the original site to other parts of the body. Tumors are staged or graded for severity, according to evidence of invasion into the intestinal wall, or evidence of spread. There is a close correlation between advancing stage and cancer mortality. Tumor size does not appear to be important in terms of outcome. The aggressiveness of colorectal cancer is based upon its ability to grow and invade the colonic wall, lymphatic system, and blood vessels.
Your doctor may not be able to determine the stage or grade of your cancer until after surgery, when the tumor has been examined by a pathologist.
The Staging System describes whether the cancer is:
in the inner linining of the colon only embedded in the colon wall penetrating through the colon wall involving lymph nodes metastatic (spread to other organs)
The prognosis for colorectal cancer patients depends on the extent of disease and the adequacy of the surgical procedure. Patients have a worse prognosis if the cancer has spread to the lymph nodes or distant organs, has invaded blood and lymphatic vessels, or is poorly differentiated. Colorectal cancer is called a metastatic disease when the cancer has spread from the colon or the rectum to another part of the body. Colorectal cancer most commonly spreads to the liver or the lungs.
Although staging of your cancer is is an important indication of the type of treatment you may receive, it is not the sole factor in defining your specific treatment. All treatment decisions at Johns Hopkins are determined on an individual basis, because no two cancers and no two people are identical. Several other factors are considered in your individual assesment, including your age, general health, family history of cancer, other medical conditions, and whether it is a new cancer or one that has recurred. Since each patients situation is unique, you should ask your doctor for a detailed explanation of the implications of the stage of your cancer.
Classification of Tumor Spread
Doctors use two staging systems to define the extent of invastion of colorectal cancer: the Dukes' classification and the TNM staging staging system. In both systems, carcinoma in situ (also referred to as high grade dysplasia) is defined as intramucosal carcinoma that does not penetrate the muscularis mucosae.

TNM Staging SystemThe TNM System, developed by the American Joint Committee on Cancer (AJCC) is the most widely used, and is considered the most precise and descriptive. T stands for tumor and the depth to which it has penetrated the colon wall, N stands for lymph node involvement, and Mrefers to metastases, or whether the cancer has spread to other body parts.
A comparision of TNM and Dukes' Classification
Key for TNM Staging
Primary Tumor (T)TX – primary tumor cannot be assessedT0 – no evidence of primary tumorTis – carcinoma in situ: intraepithelial or invasion of lamina propriaT1 – tumor invades submucosaT2 – tumor invades muscularis propriaT3 – tumor invades through muscularis propria into subserosa or into nonperitonealized pericolic or perirectal tissuesT4 – tumor directly invades other organs or structures and/or perforates visceral peritoneum
Regional Lymph Nodes (N)NX – regional lymph nodes cannot be assessedN0 – no regional lymph node metastasisN1 – metastasis in one to three regional lymph nodesN2 – metastasis in four or more regional lymph nodes
Distant Metastases (M)MX – distant metastasis cannot be assessedM0 – no distant metastasisM1 – distant metastasis

TNM classification of colorectal cancer stages.
Dukes’ Classification (Astler-Coller modification)
Stage A tumors invade through the muscularis mucosae into the submucosa but do not reach the muscularis propria
Stage B1 tumors invade into the muscularis propriaStage B2 tumors completely penetrate the smooth muscle layer into the serosa
Stage C tumors encompass any degree of invasion but are defined by regional lymph node involvement
Stage C1 tumors invade the muscularis propria with fewer than four positive nodes
Stage C2tumors completely penetrate the smooth muscle layer into the serosa with four or more involved nodes
Stage D lesions with distant metastases Carcinoma in situ
(may be referred to as high grade dysplasia) – intramucosal carcinoma that does not penetrate the muscularis mucosae
Previous: Diagnosing CRC Next: Symptoms
What are the common signs and symptoms of colorectal cancer?
Common signs and symptoms of colorectal cancer include:
bright red or very dark blood in the stool a change in the frequency of bowel movements constipation, or a feeling that the bowel doesn’t empty completely

stools that are narrower than usual general abdominal discomfort, such as frequent gas pains, bloating, and/or cramps weight loss with no known reason constant tiredness vomiting
Colorectal cancer does not usually produce symptoms early in the progress of the disease. Symptoms are dependent upon the site of the primary tumor. Cancers of the proximal colon tend to grow larger than those of the left colon and rectum before producing symptoms.
As the tumor expands in the intestinal lumen (the space in the interior of a tubular structure), such as the intestine, abnormal vasculature and trauma from the fecal stream may result in bleeding. Typically, blood is mixed in with the stool and may not be obvious to the patient (occult bleeding). Patients may develop iron deficiency anemia. Alternatively, tumors of the anus, sigmoid colon, and rectum may give rise to hematochezia, blood in the stool that is readily apparent.
As colon cancer grows, several symptoms may appear. Obstruction of the colonic lumen may produce symptoms of abdominal distension, pain, nausea, and vomiting. Obstruction of the gastrointestinal tract suggests a large tumor and a poorer prognosis.
Other symptoms of colorectal cancer may suggest an invasive process. Invasive tumors can penetrate the muscularis propria and invade adjacent tissue. This results in pain and may initiate symptoms specific to the site of invasion: tenesmus is produced by tumor invasion into the rectum; bladder penetration may produce urinary symptoms such as pneumaturia; pelvic invasion may produce perineal or sacral pain; and colonic perforation may result in an acute abdominal pain.
Some tumors produce a wasting syndrome, cancer cachexia, characterized by loss of appetite, weight and strength. The wasting occurs despite the fact that most patients with colorectal cancer do not have hypermetabolic (the physiological state of having a greatly increased rate of metabolic activity) energy expenditure. Cancer cachexia is common in patients with advanced gastrointestinal malignancies.
Next: Risk Factors
What are the Risk Factors associated with Colorectal Cancer?
The exact causes of colorectal cancer are still unknown, but certain risk factors are known to increase the chances of developing this disease. Individuals who have cancer, including women with uterine, ovarian, and breast cancers, are at increased risk of colorectal cancer. Individuals who have been previously treated for colorectal cancer are at risk for recurrence.
Known Risk Factors
Personal history of adenomatous polyps Personal and/or family history of colorectal cancer Inflammatory Bowel Disease Irritable Bowel Syndrome Ulcerative Colitis
Possible Risk Factors:
Environment Diet Tobacco Use Age - over 50 at increased risk

Physical inactivity
Colorectal cancer most commonly occurs inside of a polyp,which are usually benign growths that protrude from the mucous membrane forming in the colon and rectum. However, if polyps are left untreated they can become adenomatous polyps, which will eventually progress into cancer. As individuals age, their risk of developing polyps increases as does their risk for developing colorectal cancer. Proper screening for colorectal polyps is recommended to begin at 50 years old in the general population and sooner in individuals with a family history of colorectal cancer.
Location of the colon in the body, with the corresponding cut-away section of a colon segment with polyps.
Genetics
Those with family members who have had colon cancer are at increased risk. Several genes are known to cause colon cancer, and there may be others not yet identified. Doctors say that a family has hereditary colorectal cancer when the exact gene causing the disease in that family has been pinpointed.
Colorectal cancer, or a predisposition to this disease, may be inherited. In particular, familial adenomatous polyposis (FAP) is an autosomal dominant disorder in which affected patients have 100 percent risk of colorectal cancer development. A mutation of the APC gene (adenomatous polyposis coli (APC)) on chromosome 5 causes this disease. Gene testing is available to identify patients with this genetic mutation. Sporadic colorectal cancer is the term given to those patients who are affected with the disease, but have no family history of this condition.

Hereditary nonpolyposis colorectal cancer (Lynch syndrome or HNPCC), an autosomal dominant disorder, is a disease in families where multiple members have colorectal and other forms of cancer. The syndrome causes right-sided colon cancer and may produce primary cancers in other sites. Researchers have isolated five mutated genes associated with HNPCC: human MutS homolog 2 gene (hMSh2), MutL homolog 1 gene (hMLh1), human PMS homolog 1 gene (hPMS1), and human PMS homolog 2 gene (hPMS2) and MSH6 (MS homolog 6 gene). Hereditary nonpolyposis colorectal cancer is characterized in families with at least three members with colorectal cancer (one must be a first degree relative of the other two), at least two successive generations.
Diet
Diet is considered a determinant of increased risk in the development of colorectal cancer. Although it is difficult to ascertain which components of the diet are most important in conferring cancer risk, compelling evidence suggests a strong dose-related association between red meat and fat intake and colorectal cancer.
While consumption of animal fat is positively associated with colon cancer, consumption of fish and skinless chicken is associated with lower risk. Higher cholesterol values (a reflection of total dietary fat intake) correlate significantly with later tumor development. Obesity in middle age is also associated with increased risk of colon cancer in men; increased physical activity appears to eliminate this risk.
Dietary fiber demonstrates a protective effect in the pathophysiology of colorectal cancer. Diets rich in vegetables and high fiber grains demonstrated significant protection against fatal colorectal cancer, as revealed in a prospective study of more than 760,000 people. Fiber appears to have a number of mechanisms responsible for its protective effects. First, fiber decreases the fecal transit time by increasing stool bulk. Fiber also appears to dilute the concentration of other colonic constituents, which tend to minimize contact between carcinogens and colon epithelium. In addition, fiber is not digested or absorbed in the small intestine but undergoes fermentation in the presence of the colonic flora. This reduces fecal pH and generates short-chain fatty acids (certain short-chain fatty acids can protect isolated colonic epithelial cells).
Diet appears to play a significant role in determining the incidence of colorectal cancers in the general population. Although the international incidence of colorectal cancer varies widely, groups migrating from low-risk to high-risk regions experience an increase in the incidence of the disease. Diets high in fat and low in fiber have consistent associations with increased colorectal cancer risk. Suggestions for diet modification to reduce cancer risk include: reduced caloric intake, reduction of dietary fat to less than 35% of caloric consumption, increased consumption of fresh fruit and vegetables with at least 25 g of fiber (see Lifestyle) (link to hereditary colon cancer web site Lifestyle section). Those using aspirin have less colorectal cancer than the rest of the population. Though the mechanism by which aspirin and NSAIDs exert a protective effect against tumor formation is speculative, studies have revealed a significant reduction in relative risk of colon cancer death among users (aspirin use more than 16 times per month).
Ulcerative Colitis and Crohn's Disease
Individuals with ulcerative colitis and Crohn's disease, among other inflammatory bowel diseases, are at increased risk of developing colorectal cancer.Ulcerative colitis and Crohn's disease are inflammatory

conditions of the intestines; both are known risk factors for colorectal cancer. The risk of development of colorectal cancer is related to the severity and duration of the disease. Patients with ulcerative colitis and Crohn’s disease should undergo colonoscopic surveillance for epithelial dysplasia, a precursor to cancer, at routine intervals. Surveillance should be performed every 1–2 years in patients with 8-10 years duration of disease and annually in those with disease history of over 15 years.
Next: Screening & Prevention
Routine Screening Prevents Colon Cancer
Screening for the prevention and early detection of colon cancer is crucial to improve one's chances against colon cancer. Screening has led to a decline in the number of deaths from colon cancer over the last 20 years. Early detection is essential to ensure survival if cancer is found. When polyps or cancer in its early stages are found, the cure rate is close to 100%. Unfortunately fewer than half of Americans over the age of 50 have had any kind of colon-cancer screening test.
Regular screenings starting at age 50 for people at average risk have a very good chance of catching polyps on their way to becoming cancer. Colorectal cancer is typically slow gorwing, taking 5 to 10 years to develop. When benign or precancerous polyps are removed during coloncoscopy screenings, coon cancer may be prevented from developing at all. This represents more than just a means of detecting cancer early, IT PREVENTS COLORECTAL CANCER FROM STARTING IN THE FIRST PLACE.
Educational campaigns and screening strategies targeted at high-risk groups are urgently needed to increase the public's awareness of colorectal cancer screening for prevention and early detection.
Screening for hereditary colorectal cancer syndromes involves genetic testing.
The Johns Hopkins colorectal cancer health care team utilizes the lastest in diagnostic tests to screen for colorectal cancer:
Colonoscopy Flexible sigmoidoscopy Barium enema Virtual colonoscopy
Fecal occult blood test Stool DNA
Screening for Patients at Average Risk for Colorectal Cancer:

Screening for Patients at Increased Risk for Colorectal Cancer:
Note: The term surveillance refers to screening done after treatment to detect cancer recurrence or metastasis

TREATMENT
Treatment for colorectal cancer depends on the stage at which cancer was discovered. Early stage colorectal cancer is best treated with surgery. Approximately 95% of Stage I and 65-80% of Stage II colorectal cancers are curable with surgery. Rectal cancer however, may require additional radiation therapy to minimize the risk of recurrence. Advanced stage (Stage III and Stage IV) often consists of a combination of therapies, including: surgery, chemotherapy, and radiation.
Although staging of your cancer is an important indication of the type of treatment you may receive, it is not the sole factor in defining your specific treatment. All treatment decisions at Johns Hopkins are determined on an individual basis based on discussions with surgical medical and radiation oncologists, because no two cancers and no two people are identical. Several other factors are considered in your individual assesment, including your age, general health, family history of cancer, other medical conditions, and whether it is a new cancer or one that has recurred. Since each patients situation is unique, you should ask your doctor for a detailed explanation of the implications of the stage of your cancer.
At Johns Hopkins we provide each patient with a comprehensive approach guided by the top specialists in colorectal cancer care. This ensures that patients receive treatment specifically targeted to their disease.
Explore the various therapeutic options for colorectal cancer by choosing a disease stage below. If you are unsure what stage your cancer is, ask your doctor.
What is Stage I Colorectal
Cancer?
The cancer has grown through several layers of the colon, but has not spread outside the colon wall itself. Surgery to remove the cancer is the standard treatment. Additional therapy is not needed. Approximately 95% of patients with Stage I colorectal cancers are cured by surgery alone.
Explore Therapies for Stage I Colorectal Cancer
What is Stage II Colorectal
Cancer?
The cancer has grown through the wall of the colon and may extend into nearby tissue, but has not spread to the lymph nodes. Surgery is usually the only treatment needed for colon cancer but radiation therapy may be needed for rectal cancers. In some cases your doctor may recommend additional chemotherapy.
Explore Therapies for Stage II Colorectal Cancer
What is Stage III Colorectal
Cancer?
The cancer has spread to nearby lymph nodes, but has not spread to other parts of the body. Surgery is the first treatment, followed by chemotherapy. Radiation therapy may be used depending on the location & size of the tumor.
Explore Therapies for Stage III Colorectal Cancer
What is Stage IV Colorectal
Cancer?
The cancer has spread to distant organs and tissues, most commonly the liver. Depending on the extent of the tumor's spread, chemotherapy may be combined with with surgery and/or

radiation.
Explore Therapies for Stage IV Colorectal Cancer
Welcome to the Johns Hopkins Hereditary Colorectal Cancer Website. This site is provided to educate and inform people about hereditary colorectal cancer. To begin, please review our overview of hereditary colorectal cancer to learn more about the involved in the various hereditary colorectal cancer syndromes.
Specific information on Familial Adenomatous Polyposis (FAP), Hereditary Nonpolyposis Colorectal Cancer (HNPCC), and a gene mutation called APC I1307K may be accessed on the menu below. We also offer information about the Hereditary Colorectal Cancer Registry as well as tailored material for children with a genetic risk for FAP.
HNPCC FAP APC I1307K Kid's FAP
General Information There are a number of different inherited conditions that have a significant risk of colon cancer. Research into these conditions and the knowledge that researchers have gained have led to the development of screening and management guidelines for both patients and their relatives. These guidelines can lead to prevention of cancer and other complications associated with these diseases.
Most colorectal cancers are sporadic, meaning that they have no prior family history of the disease. Individuals with a family history of colorectal cancer are described as having familial or hereditary colorectal cancer.
Figure 2. Distribution of colorectal cancers (flow chart).
What is Familial Colorectal Cancer?The occurrence of colorectal cancer in more than one family member may be due to chance alone. However, it could also mean the potential for developing colorectal cancer has been passed from one generation of the family to the next generation, but the exact gene causing the cancer has not been identified. Relatives of a person with colorectal cancer may be more likely to develop it themselves.

Figure 4. Basic family pedigree
It is estimated that 15–50% of colorectal cancers are familial. A single gene, a combination of genes, or a combination of genetic and environmental factors can cause familial colorectal cancer. Typically these families have one or two members with a history of colorectal cancer or precancerous polyps.
What is Hereditary Colorectal Cancer? We say that a family has hereditary colorectal cancer when the exact gene that causes the disease is known. Several genes that cause hereditary colorectal cancer have been identified. There may be other genes that have not yet been discovered.
If more than one person in a family has colorectal cancer, it could mean that the potential for developing this form of cancer has been passed from one generation of a family to the next generation (hereditary). In these families, relatives of people with colorectal cancer may be much more likely to develop it themselves.
Inherited colorectal cancers are associated with a genetic mutation in a cancer susceptibility gene. Everyone inherits one susceptibility gene from each of their parents, making a total of two working copies of each gene. If a mutation in one copy of a cancer susceptibility gene is passed from the parent to their child, the child is predisposed (or has the potential) to develop cancer.
The genetic causes of two hereditary colorectal cancer syndromes, familial adenomatous polyposis (FAP) and hereditary nonpolyposis colorectal cancer (HNPCC) have been identified.
What is FAP?Familial adenomatous polyposis (FAP) is a disorder that leads to hundreds, even thousands, of polyps in the colon and rectum at a young age, usually as a teenager or young adult. Other names for this condition are hereditary polyposis of the colorectum, familial polyposis, and Gardner’s syndrome. This condition is inherited and primarily affects the gastrointestinal tract, commonly the colon and less often the stomach and small intestine. More on FAP

What is HNPCC? Hereditary nonpolyposis colorectal cancer (HNPCC) is also known as Lynch syndrome or cancer family syndrome. It is a condition in which the tendency to develop colorectal cancer is inherited. People with HNPCC have a 50% chance of passing the HNPCC gene to each of their children. A mutation in the genes (hMLH1 and hMSH2), that when functioning normally would protect against colon cancer, is the cause of HNPCC. People affected with this type of colorectal cancer do not develop large numbers of polyps (only a small number may be present or none at all). In families with HNPCC, cancer usually occurs on the right side of the colon. It often occurs at a younger age than colon cancer that is not inherited. Other cancers can occur in these families, including cancer of the uterus, ovaries, stomach, urinary tract, small bowel and bile ducts. More on HNPCC
What is APC I1307K? About 6% of Jews whose ancestors came from Eastern Europe have an increased risk (18–30%) of developing colon cancer. This risk is much higher than the normal 5% risk. In 1997 a Johns Hopkins research team discovered an inherited gene mutation called APC I1307K. This gene increases the susceptibility for colorectal cancer. More on APC I1307K
Click here for our downoadable educational resources on hereditary colorectal cancer syndromes.
Visit the Johns Hopkins Hereditary Colorectal Cancer Registry to see how you can help researchers learn more about hereditary colorectal cancer syndromes.
What is Hereditary Nonpolyposis Colorectal Cancer?
HNPCC is also known as Lynch syndrome or cancer family syndrome. HNPCC is a condition in which the tendency to develop colorectal cancer is inherited. “Nonpolyposis” means that colorectal cancer can occur when only a small number of polyps are present (or polyps are not present at all). In families with HNPCC, cancer usually occurs on the right side of the colon. It often occurs at a younger age than colon cancer that is not inherited. Other cancers can occur in these families including cancer of the uterus, ovaries, stomach, urinary tract, small bowel, and bile ducts.
Hereditary nonpolyposis colorectal cancer (HNPCC) syndrome was first described over 100 years ago. It is the most common of the recognized inherited colorectal cancer syndromes. HNPCC is usually characterized by a predisposition to cancer in the third and fourth decades of life, although it is not infrequent to have earlier or later onset. It accounts for approximately 5% of all colon cancer cases. Tumors in patients with HNPCC begin as adenomas and frequently transform to carcinoma. Endometrial, ovarian, urinary tract, biliary tract, small intestine, and gastric cancer are also characteristic of this syndrome and are seen more often in these families with HNPCC than in the general population.
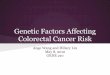
How is HNPCC Inherited?
HNPCC is an autosomal dominant condition. This means that people with HNPCC have a 50% chance of passing the HNPCC gene mutation (change) to each of their children. The gene mutation can be passed on even if the parent has had surgery to remove his or her own colon. Individuals who do not inherit the gene mutation cannot pass it to their own children. The vast majority of individuals with HNPCC develop cancer (Figure 1).

Some individuals with HNPCC do not have an affected parent. These individuals, who are the first in the family to have the condition, are referred to as having a new mutation (newly altered gene). They can, however, pass this HNPCC gene mutation to their children.
Fig. 1 HNPCC Family Pedigree
1. George has HNPCC. His wife, Susan, is unaffected. They have three children, George, Jr., Stephen, and Carol. All were at 50 percent risk of developing HNPCC. George, Jr., and Carol are affected.
2. George, Jr. and his wife, Connie, have two children. Both children have a 50 percent chance of inheriting HNPCC. Their daughter, Alice is affected.
3. Stephen and his wife, Gloria, have two children. Because Stephen is unaffected, there was no risk to his children of developing HNPCC.
4. Carol and Bill have three children. Each child had a 50 percent change of inheriting HNPCC and two are affected; son Billy is not.
How is HNPCC Diagnosed? Persons at risk for HNPCC usually have a family history of two successive generations of colorectal cancer or at least one generation with colorectal cancer and one generation with polyps. Men and women at risk for HNPCC need examinations of the entire colon. Women at risk should also have yearly endometrial and ovarian screening. Tests such as colonoscopy and barium enema with flexible sigmoidoscopy are available to tell whether polyps or cancer are present in the colon. For patients at risk for HNPCC, colonoscopy is the preferred method of screening.
Why is Early Diagnosis Important? Early diagnosis is important for early detection and prevention of cancer. Regular screening should start at the ages described in the exam guidelines below. When colorectal cancer is detected early, the chance of cure is much better.
Genetic Counseling and TestingGenetic counseling is available, and recommended, for individuals with HNPCC and their family members. Genetic counselors will explain the inheritance pattern of HNPCC, discuss which family members are at risk for developing the condition, and provide necessary information regarding genetic

testing. Counseling services are available through genetic and oncology departments in many hospitals. To make an appointment with a member of the Johns Hopkins professional medical team or to speak with someone at the Colorectal Cancer Risk Assessment Service, please call (410) 614-LIFE (5433). Also, it is recommended that HNPCC families contact registries for access to resources and for help with identification of family members at risk.
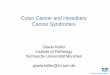
Mutations (alterations) of one of five genes are now known to be responsible for most cases of HNPCC. These genes are called hMSH2, hPMS1, MSH6 (all on chromosome 2), hMLH1 (chromosome 3), and hPMS2 (chromosome 7). Other genes, presently undiscovered, may also cause HNPCC. Gene tests for HNPCC are available for selected individuals from families who have HNPCC. A family member affected with colon cancer should be tested first, whenever possible.
Fig 2. Chromosomes 2, 3, and 7
Microsatellite Instability Testing Microsatellite instability (MSI) testing is used as a screening test to see how likely it is that a person’s cancer was caused by one of the genes associated with HNPCC. It is usually done on colon tumor tissue that is removed and stored as part of the normal process when a person has surgery for colon cancer.
If the tumor tissue tests MSI positive, it is considered more likely that the cancer is due to one of the HNPCC gene mutations. People who have a positive MSI test have the option to pursue the genetic blood test. If the tumor tissue tests MSI negative, however, it is highly unlikely that current genetic testing will be helpful for the affected person’s family. An MSI negative test result does not rule out the diagnosis of HNPCC.
Results and Screening Guidelines For Individuals Who Have Had HNPCC Gene Testing
The following four outcomes are possible results from your genetic testing:
1. Positive gene test—an HNPCC gene mutation was found in a person’s blood sample. Persons with a positive gene test should have a colonoscopy every year and follow the exam guidelines

for people at risk listed below. In addition, other ways to prevent cancer, surgeries such as colectomy, hysterectomy, and oophorectomy, may be considered.
2. Negative gene test—No HNPCC gene mutation was found in a person’s blood sample and an affected family member has had a positive gene test. Persons with a negative gene test (an HNPCC gene mutation was not found), require careful evaluation by their doctor and a genetic counselor to determine the best screening guidelines to follow.
3. No mutation found—No HNPCC gene mutation was found in a person’s blood sample and no affected family member has had a positive gene test. Continue to follow screening guidelines for persons with a family history of colorectal cancer.
4. Variant of Unknown Significance - A mutation was detected in a person's blood, however the significance of the mutation is unclear. It is not possible at this time to determine the effects of a variant of unknown significance until a sufficiently large populatin with a similar variant is studied. Your genetic counselor will make screening recommendations based on your family history and the likelihood of your specific result being deleterious.
At this time, the available gene tests cannot detect all HNPCC-causing genes. Future advances in technology may provide more accurate diagnosis. A genetic counselor or physician will assist in finding a laboratory that provides the best testing
Screening Guidelines For Individuals at Risk Who Have Not Had HNPCC Gene Testing
1. Colonoscopy every 1–2* years starting by age 25 years or 5–10 years before the age of earliest colorectal cancer diagnosed in the family, whichever is younger. At age 40 begin annual colonoscopy.
2. Annual stool hemoccult tests, urinalysis, and blood tests for liver function starting when colonoscopy begins.
3. For women: yearly pelvic exam with Pap test and transvaginal ultrasound of the uterus and ovaries or Pipel biopsy starting at age 25 and continuing annually.
4. Consider annual upper endoscopy in families with gastric cancer.
*Colonoscopy is recommended every year for a person with a positive gene test. If colon polyps or cancer is found, follow the treatment guidelines.
What is FAP?
Familial adenomatous polyposis (FAP) is an inherited condition that primarily affects the gastrointestinal tract. This disorder leads to hundreds or thousands of polyps inside the colon and rectum (less often in the stomach and small intestine). Symptoms typically appear in teenagers or young adults. Other names for this condition include hereditary polyposis of the colorectum, familial polyposis, and Gardner’s syndrome.

Familial adenomatous polyposis is an inherited condition caused by a mutation on chromosome 5. FAP is characterized by hundreds to thousands of polyps in the gastrointestinal tract (primarily the colon and rectum). These polyps are at increased risk for malignancy. Polyps begin to appear during teen years and often become cancerous by age 40.
Fig 1. A: Appearance of FAP inside the colon; B: Endoscopic image of polyposis; C: Enlargement of polyps in the colon
Polyps (abnormal mushroom-like growths) may vary in size from less than one tenth of an inch to 1–2 inches. They may be large enough to block part of the intestine. If patients with FAP are left untreated, one or more of these polyps may develop into cancer. FAP may also be associated with benign tumors of the skin, soft connective tissue, and bones. It is caused by a mutation in a gene called APC. In some people FAP may be inherited, whereas in others it is not (sporadic).

Fig 2. Illustrative comparison of polyp size
Attenuated FAP
Some families are affected with attenuated FAP (AFAP). This is a mild (or attenuated) form of FAP in which affected individuals develop fewer polyps at a later age than those with typical FAP. Although people with AFAP tend to develop colon cancer at a later age than individuals with typical FAP, they still have a near 100% lifetime risk of colon cancer. If AFAP is suspected within a family, it is important that family members be screened with colonoscopy rather than flexible sigmoidoscopy because polyps are not evenly distributed throughout the colon. Because the number of polyps and age of onset can vary greatly from one family member to another in a family with AFAP, screening should begin at age 11.
Other Symptoms Associated with FAPIndividuals with FAP often develop polyps in organs other than the colon, such as stomach and small intestine. Although most polyps that develop in the stomach and small intestine are benign, cancer may develop in them. Desmoid tumors may also develop. Young children affected with FAP have a small increased risk for hepatoblastoma, a liver tumor. Tumors may also occur in the thyroid gland, adrenal gland, bile ducts, and pancreas. Affected individuals may also have some, or all, of the following: lumps or bumps on the bones of the legs, arms, skull and jaw; cysts of the skin; teeth that do not erupt when they should; and freckle-like spots on the inside lining of the eye. Thus, physicians recommend that patients continue with life-long follow-up examination for cancer prevention.
How is FAP Inherited?
People with FAP have a 50% chance of passing the condition to each of their children. The condition can be passed on even if the patient has had his or her own colon removed. Children who do not inherit the condition from their parent cannot pass it to their own children.
About one third of people with FAP do not have an affected parent. An individual who is the first in the family to have the condition has a new or spontaneous mutation. Individuals with new mutations can pass

FAP to their children
Figure 3. FAP family pedigree
1. George has FAP, his wife Susan is unaffected. They have 3 children, George, Jr., Stephen, and Carol. All were at 50% risk of developing FAP. George, Jr., and Carol are affected.
2. George, Jr. and his wife Connie have 2 children. Both children had a 50% chance of inheriting FAP. Their daughter Alice is affected.
3. Stephen and his wife Gloria have 2 children. Because Stephen is unaffected, there was no risk to his children of developing FAP.
4. Carol and Bill have 3 children. Each child had a 50% chance of inheriting FAP and two are affected; son Billy is not.
Genetic Testing and Counseling for FAP
Genetic counseling is available and recommended for individuals with FAP and for their family members. Genetic counselors will explain the inheritance pattern of FAP, discuss which family members are at risk for developing the condition, and provide necessary information regarding genetic testing. Counseling services are available through genetic and oncology departments in many hospitals. To make an appointment with a member of the Johns Hopkins professional medical team or to speak with someone at the Colorectal Cancer Risk Assessment Service, please call (410) 614-LIFE (5433). Also, it is recommended that FAP families contact registries for access to resources and for help with identification of family members at risk.
Genetic testing is available for Familial Adenomatous Polyposis (FAP), Hereditary Nonpolyposis Colorectal Cancer (HNPCC), and APC I1307K.
The altered gene that causes FAP in most patients is now known.

Fig 4. Chromosome 5 for FAP
A blood test can locate the change in the APC gene, which is causing the disease in about 80% of families with FAP. In these families, children can learn if they have inherited the changed APC gene from their parent with FAP. If a child does have the gene mutation, he or she will eventually develop FAP. The mutation in the APC gene cannot be detected in about 20% of families with FAP. Children in these families must continue to have regular colon screening according to the guidelines for families in which a gene mutation could not be found.
The test requires a small blood sample. The gene test results will influence the future management of individuals who are at risk for FAP. For example, if the test shows that a person does not have the APC gene mutation known in the family, he or she can avoid many unnecessary colon examinations. If the test shows that a person does have the gene mutation, then the physician will need to be alerted to schedule colon examinations at least yearly and to plan for future treatment when polyps develop.
Is insurance discrimination a risk for those seeking genetic testing?With any gene test, there is a risk of insurance (life or health) or employment discrimination. At this time, federal laws offer some protection against the discrimination against people who already have medical insurance through a group health plan. Some states have other laws to protect people, but the laws on insurance and employment discrimination vary from state-to-state. The Americans with Disabilities Act may protect people with a positive gene test result from discrimination in the work place. These issues will be carefully explained during the genetic counseling session.
This section is dedicated to kids and teenagers who have a genetic condition called FAP. FAP, or its full name, familial adenomatous polyposis, is a condition in which polyps (pronounced pol-ips) form in the digestive tract and are inherited. Polyps are abnormal, mushroom-like growths that form on the inside of the digestive tract.
What is FAP?

Familial adenomatous polyposis, is a condition in which polyps (pronounced pol'ips) form in the digestive tract and are inherited. Polyps are abnormal, mushroom-like growths that form on the inside of the digestive tract.
Figure 1. A: Appearance of FAP inside the colon; B: Endoscopic image of polyposis; C: Enlargement of polyps in the colon
The polyps occur most often in the colon or large intestine. The total length of the colon is approximately 5 feet in the adult and it is responsible for forming, storing, and expelling waste matter.

Figure 2. Anatomy of the large intestine
Polyp sizes can vary from the size of a pencil point to the size of a quarter.
Fig 3. Illustrative comparison of polyp size

Kids with FAP develop hundreds to thousands of polyps throughout the colon at a young age, usually as a teenager or young adult. The major concern about this condition is that the polyps will become cancerous. A person with polyps usually has no idea that the polyps are there.
The most important things to remember are that FAP can be treated and that most kids with FAP lead normal, healthy lives!
What causes FAP?
A gene mutation or change in a gene causes FAP. This gene change can be inherited or passed from a parent to a child. The mutation occurs on chromosome 5.
Fig 4. Chromosome 5 for FAP
What do kids do if their parent has FAP?
Kids can inherit FAP from a parent who has this condition. If one of your parents has FAP, you have a 50% chance of also having FAP. Normally kids would go for their first colorectal exam around age 11.
Sometimes genetic testing can be helpful in telling which kids have inherited FAP and which have not.
This family pedigree shows how the grandfather has passed the FAP gene to his daughter. His daughter then passed the FAP gene on to two of her three children.
What is the Treatment for Kids with FAP?

If polyps are found at examination the doctor will discuss options for treatment. People with FAP will need colorectal surgery after polyps begin to form. People who have their colons removed do live full lives with minor adjustments.
Stories from Kids, Teens and Parents with FAP
The following are stories sent to us from kids, teens, and young adults with FAP. Please feel free to send us a story at [email protected]
From Chris, Age 17 My name is Chris and I have been in an FAP study [information on study] for three years. I was 14 when I entered the study. At first I thought it would be neat to be in the study and that it would be a good thing for my future health. Now three years have passed and I am 17. Looking back, I'm not sure I want to be in the study because I am not sure I want to know about "the gene.”
I am a normal 17 year-old boy. I get up in the morning, I go to school, and then I go to football, do homework then I go to bed. I liked my life the way it was. It’s still the same BUT you have more weight holding you down. You get up sometimes and think," Did I grow a polyp, did it turn into cancer, am I going to die earlier than most people, am I going to have to go through this my whole life?"
There are some days that I am glad I am doing this. Every time I come out of the doctor’s office and he says he did not find anything, what a relief!!! But you need to know that the worry comes back.
If I had to do it all over again I don’t know what I would do. It is hard for me to advise other kids because everyone is different. I know that if the parents really care they will let their kids make the decision themselves or at least listen to their children’s decisions. It may not be the right one but that’s life. There is no way to know if the choice that you make is right, you just have to wait and see.
This part is for the parents of the kids. You can suggest it and list all the good things but you better list the bad things too. You can make the study sound like there is nothing wrong with it, but there is a bad side to everything. You know what they say: “Nothing is perfect.”
Back to the kids. I may make the study sound bad but it’s not that bad. The only thing that makes it worthwhile is the people who do it. They are the kindest people at the hospital. They do not make you do anything you don't want to. You get a lot of suckers and even some brownies. (Believe me I know.)
Well I suggest that you do go into the study if you want to BUT ONLY IF YOU WANT TO. It is your life not your parents’, your friends’, or anyone else’s. Here are your options, now make the right choice.
From Ashley, Age 12 Hi, my name is Ashley. I'll tell you about FAP. I don't like having FAP. I feel alone, left out. It's not fair. My life has changed since I found out I had it. I don't know why I have it, but it stinks! I have my own opinions. You might feel different though. You might be on a study program and take pills like me.
From Suzanna, Age 15 When I first found out that I had FAP, I was very upset. I did not want to take medicine and maybe later have colon cancer. After a few trips and quite a few months later, I got used to it all. The doctor and

nurses were very nice to me. They made me feel like family and I felt important.
When my family found out that my younger sister had polyps, I was very sad. I wanted to be alone so that I could cry. I would rather had it been me, she’s too young. Only 13! I am happy that we went through all that we did. Although it was hard, I know that we have a future and hopefully can help many other people.
From a parent with a child with FAP Anyone with an ostomy who is willing to share any quick/easy tips they've learned or even show someone how they put their appliance on etc. [would make living with an ostomy] far more relaxing and acceptable. We all know our ostomies act differently at times from food and stress. So anything [anyone can do] to ease the situation or help someone through an embarrassing moment or to help prevent one is welcomed. Once you feel comfortable and your friend understands how you now work you can begin to joke and feel like you fit in.
For those with the section only [the rectum is still intact], I can't stress enough the importance of 3–6 month check-ups and being part of any studies on the subject to find a cure.
From an adult with FAP Being older when I found out I had FAP, my feelings were mixed, but I must say that the biggest feeling I have is THANKFULNESS... Of course, my original feeling was of SADNESS for my family that they might have to take care of me through the sickness. When I learned of the operation and the chances of recovery, I became THANKFUL that I could live to take care of them the way I had always hoped.
When I learned, through Johns Hopkins, that I could pass the gene to my children I became SAD again that I could do this to my children. I learned, again through Johns Hopkins, that there were medications to relieve or eliminate the disease and I agreed to be part of the study to help my children. This made me THANKFUL that I could do something to help them and other families to overcome FAP.
Truly, I am THANKFUL that Johns Hopkins has the doctors, especially Dr. Giardiello, nurses, especially Linda Hylind and the staff, especially Rahj and Kathy, who are willing to, day after day, perform the "Procedure," study the results…This makes me THANKFUL that my children and you, as you get older and marry, will be able to have children knowing FAP is being controlled.
I have had the operation and I am THANKFUL that it has not really changed my life, I don't live in pain, I am happy and I hope to live many more years so I can keep pestering Dr. Frank, Linda, and Kathy.
From Amy The other day I had a test, not the normal kind that I would study for. I was given a hospital gown to wear. I laid down on a bed, which was rather comfortable. A nurse put an IV into my arm and took me into a surgery room. I was given medicine to make me sleep. Before they started the procedure, which was very uncomfortable, the doctor took a long tube-shaped object and inserted it into my rectum. It had a light and camera in it. The doctor lasered about three or more polyps out of my colon. I am a little sore from time to time. Polyps are little growths that are in my colon. They can cause a serious disease like cancer. If I were to go untreated, I would get very sick, and could possibly die from colon cancer.
The procedure that deals with the lasering and camera is called endoscopy. If you want my option, it's rather nasty. I have to drink yucky medicine that makes me have loose bowels. Practically my whole family, on my mother's side, has had this disease and many other relatives, including my mom, have had numerous operations

What is APC I1307K?
Adenomatous polyposis coli is a tumor-suppressing gene that plays an important role in the carcinogenesis of colorectal cancer. If the APC gene is defective it fails to suppress colon cancer development. The mutation appears to make the gene unstable and prone to acquire mutations during normal cell division. The APC I1307K mutation is found in Ashkenazi Jews and has not been found in anyone who is not of Ashkenazi descent. This gene mutation causes a substantial increase in the risk of colorectal cancer (approximately 18–30% lifetime risk). Studies of APC I1307K are ongoing to better understand its role and implications.
In 1997, a Johns Hopkins research team found an inherited genetic mutation called APC I1307K. This mutation is found primarily in people of Ashkenazi Jewish heritage (Jews of Eastern European or Russian ancestry). Researchers believe that 6% of the Ashkenazi Jewish population carries this gene mutation, which gives them a significantly increased risk of developing colorectal cancer.
Both the APC I1307K mutation and mutations that cause FAP occur in the same gene, the APC (adenomatous polyposis coli) gene. The APC I1307K mutation is different from other APC mutations because the mutation itself does not cause colorectal cancer. Instead, this particular mutation creates an unstable spot in the gene that makes the gene more susceptible to additional genetic changes that may, in turn, lead to colorectal cancer.
How Is the APC I1307K Mutation Inherited?
People with the APC I1307K gene mutation have a 50% chance of passing the gene mutation to each of their children. Children who do not inherit the gene mutation cannot pass it to their own children.
Fig. 1 Example pedigree of APC I1307K Mutation
1. George has colon cancer and carries the APC I1307K gene mutation. His wife, Susan, does not have the gene mutation. They have three children, George, Jr., Stephen, and Carol. All were at 50 percent

risk of inheriting the APC I1307K gene mutation from George. In fact, both George, Jr., and Carol do carry the mutation and both have developed polyps.
2. George, Jr., and his wife, Connie, have two children. Both children had a 50 percent chance of inheriting the gene mutation. Their daughter, Alice, is affected.
3. Stephen and his wife, Gloria, have two children. Because Stephen does not have the gene mutation, his children had no risk of inheriting the gene mutation from him.
4. Carol and Bill have three children. Each child had a 50 percent chance of inheriting the gene mutation from Susan. Peter and Sally carry the gene mutation, but neither one has yet developed polyps or colon cancer.
*Children who do not inherit the gene mutation cannot poass it to their own children.
Why Is This Mutation Most Common in People of Ashkenazi Jewish Descent?
Recent scientific studies tell us that certain groups of people, including Ashkenazi Jews, have unique genetic mutations that increase their risk of certain cancers or diseases. In most cases, doctors who study genetics believe that the first time a gene change occurs in a group of people, it occurs by chance. When this group is small and separate from other groups, by geography or culture, for example, the gene change may become more frequent from one generation to the next. This is probably why the APC I1307K gene mutation is most commonly found in people of Ashkenazi Jewish descent.
Diagnosing APC I1307K - Genetic/DNA Testing
There is a gene test to look for this inherited gene mutation.
Fig 2. Chromosome 5 showing APC I1307K
Who Should Consider Testing for the APC I1307K Mutation?

Any person of Ashkenazi heritage who has a personal or family history of colorectal cancer or colorectal polyps may wish to consider testing. A family history means having at least one close family member with colorectal cancer or polyps. Ashkenazi Jews without a family history of colorectal cancer may still wish to obtain genetic counseling to learn the value of gene testing in their own unique circumstances.
Genetic counseling is available, and recommended, for individuals who may have the APC I1307K mutation, and their family members. Genetic counselors will explain the inheritance pattern of APC I1307K, discuss which family members are at risk for developing the condition and provide necessary information regarding genetic testing. Counseling services are available through genetic and oncology departments in many hospitals. To make an appointment with a member of the Johns Hopkins professional medical team or to speak with someone at the Colorectal Cancer Risk Assessment Service, please call (410) 614-LIFE (5433). Also, it is recommended that APC I1307K families contact registries for access to resources and for help with identification of at-risk family members.
What Should You Do if You Receive a Positive Gene Test Result?
It is important to detect colon polyps or cancer early. Routine screening is the best way to do this. At this time, experts recommend the following:
Persons with a positive test result, who do not already have colon cancer or polyps, should have a routine colonoscopy every 2 years beginning at age 35 OR 5–10 years before the earliest age at which colon cancer or polyps occurred in the family, whichever is younger.
Patients with a personal history of colon cancer or polyps should have a routine colonoscopy every 2 years, or more often at the recommendation of their doctor.
Relatives of people testing positive for this gene mutation should consider counseling and testing as well.
Genetic Testing and Insurance
With any gene test there is a risk of insurance (life or health) or employment discrimination. At this time there are federal laws that offer protection against discrimination of people who have medical insurance through a group health plan. Some states have laws to protect people, but the laws on insurance and employment discrimination vary from state to state. The Americans with Disabilities Act may protect people with a positive gene test from discrimination in the workplace. These issues can be discussed with a genetic counselor.
Symptoms
Many patients with colorectal cancer experience no symptoms in the early stage of their disease. In fact, many people have no symptoms until the disease is quite advanced. Therefore, routine colorectal screening and an appreciation of risk factors are extremely important.

Since many of the symptoms of colorectal cancer are also symptoms of a variety of other colon diseases, it is important to see your physician so that the necessary tests can be run and a diagnosis made.
The following is a list of symptoms that may occur:
• Blood in the stool• Diarrhea that is not the result of diet or illness • A long period of constipation • Crampy pain in the abdomen • Change in bowel habits • Persistent decrease in the size or caliber of stool • Frequent feeling of distention in the abdomen or bowel region(gas pain, bloating, fullness, with or without cramping) • Weight loss with no known reason • Vomiting and continual lack of energy
In addition to polyps, abnormalities in other areas of the body may give early clues to the presence of FAP. These abnormalities may include bumps or lumps on the bones of the legs, arms, skull, and jaw; cysts of the skin; teeth that do not erupt when they should; and freckle-like spots on the inside lining of the eyes.
It should be emphasized that there is no safety in simply waiting for symptoms to develop. It is vital that parents and guardians make every effort to have examinations of their children starting at age 11 even if they do not have symptoms.
What Is Hyperplastic Polyposis?
Individuals are diagnosed with hyperplastic polyposis when they have multiple hyperplastic polyps, usually greater than 20 polyps. The number of polyps ranges anywhere from 6 to greater than 100, though most individuals with hyperplastic polyposis have between 40 and 100 polyps. A diagnosis of Hyperplastic polyposis may also made in individuals who present with fewer than 20 hyperplastic polyps, but whose polyps are larger, often greater than 2 centimeters. Individuals may also be diagnosed with multiple serrated adenomas or a mix of both serrated adenomas and hyperplastic polyps. Hyperplastic polyposis is usually diagnosed in individuals in their 40’s to 60’s, though it has been reported in individuals as young as 11 years old. Individuals with hyperplastic polyposis are at an increased risk for developing colorectal cancer, so routine screening is extremely important. Although the genetic basis for FAP, HNPCC, Peutz-Jeghers, MYH-Associated Polyposis, and juvenile polyposis has been identified, hyperplastic polyposis has not yet been explained. Hyperplastic polyposis is suspected to have a familial basis and reports have shown that is inheritable in 5% of cases, though the exact mechanism of inheritance has not been identified.
What are Hyperplastic and Sessile Serrated Polyps?
Hyperplastic polyps are not an uncommon polyp, and are often routinely found during colonoscopy screening. The importance of the hyperplastic polyp as a precursor for colorectal cancer has not been

well studied, though most evidence indicates that hyperplastic polyps are not generally associated with colorectal cancer. Hyperplastic polyps are generally thought to be truly benign growths, possessing no potential for progression to colorectal cancer. Contrast this with the adenoma, the colon polyp strongly associated with colorectal cancer, fewer than 10% of all adenomas become cancerous, however, more than 95% of colorectal cancers develop from adenomas.
Hyperplastic polyps share similar features to a related polyp known as a sessile serrated adenoma. Sessile serrated adenomas are related to hyperplastic polyps, but have dysplasia, this feature makes it more likely for a sessile serrated adenoma to progress to colorectal cancer than hyperplastic polyps. While hyperplastic polyps are similar to sessile serrated adenomas, and other adenomas the research shows that the adenoma is clearly considered a precancerous colon polyp, whereas the hyperplastic polyp is considered to be benign, rarely progressing to colorectal cancer. Click here to read more about the pathology of colon polyps.
You can help with hyperplastic polyposis research!
The Johns Hopkins Hereditary Colorectal Cancer Registry is currently studying hyperplastic polyposis with the hope of better understanding this new syndrome. If you have been diagnosed or are suspected of having hyperplastic polyposis or multiple hyperplastic polyps, please contact us for more information and to find out how you can help further our understanding of this syndrome. Please call us at 1-888-772-6566 or email us at [email protected] to find out more.
You can reduce your risk of colon cancer!
Numerous research studies are consistently showing that the choices we make each day can have an important impact on colon cancer risk. Whether we decide to eat a cookie instead of a carrot, ice cream instead of yogurt, or whether we choose to take the elevator rather than the stairs, or spend more time in front of the computer instead of taking the time to exercise or walk the dog. These choices add up over time and actually shift ones risk for colorectal cancer either towards the higher or lower end of the spectrum.
By simply managing the risk factors within your control, you can lower your risk of colorectal cancer. For example a person's risk can be significantly lowered by eating plenty of fruits and vegetables while at the same time reducing the intake of red meat, and high-fat and fried foods. With the addition of regular exercise, ones risk is even further decreased. The goal of our Integrative Health section is to highlight activities and choices of a healthy lifestyle that when practiced a little bit each day, can truly lower ones risk of developing colorectal cancer.
The general consensus from scientific literature is that 30-40 percent of all cancers could be prevented by getting regular physical activity, eating a healthy diet, and maintaining a healthy weight.
As you read the information in the follwing sections try to make mental notes of the small changes you can make each day to lower your risk of colorectal cancer.
Visit the Johns Hopkins Integrative Medicine and Digestive Center ;for more information on incorporating healthy lifestyle changes into your recovery plan.

Eating to Fight and Prevent Colorectal Cancer
Diet and proper nutrition are vital tools in the fight against colon cancer. Rapidly accumulating evidence supports eating a healthy diet for both prevention and treatment. In general, dietary recommendations include consuming less saturated fat and salt and eating a variety of colorful fruits, and vegetables rich in vitamins, minerals and antioxidants.
A healthy diet provides a multitude of benefits beyond preventing colon cancer By following the healthy guidelines below for preventing colorectal cancer you may experience a multitude of other positive healthy benefits including feeling more energetic and losing weight.
1. Eat plenty of brightly colored fruits and vegetables
2. Eat fresh fish 1-3 times per week
3. Limit consumption of red meat
4. Avoid excess salt and saturated fats
5. Maintain a healthy weight and keep physically active
6. Limit alcohol consumption
7. Avoid tobacco in any form
There are several foods well recognized as powerhouses of cancer fighting antioxidants and nutrients. These superfoods may already be part of your daily diet, view each of the foods below for more information:
Suggestions for lifestyle modifications include: maintaining a healthy body weight and exercising to reduce the risk of obesity. A reduction of dietary fat to less than 30% of caloric consumption and an increased intake of fresh fruit and vegetables, with at least 25 grams of fiber and protective omega-3 fats common in fatty fish, nuts and canola oil can be helpful.
Diet is considered a determinant of increased risk in the development of colorectal cancer. Although it is difficult to ascertain which components of diet are most important in increasing the risk of colorectal cancer, compelling evidence suggests a strong association between red meat and fat intake and colorectal cancer. While high consumption of animal fat is positively associated with colorectal cancer, consumption of fatty fish and low fat intake may lower risk. Higher cholesterol values (a reflection of total dietary fat intake) correlate significantly with later tumor development. Obesity and lack of physical activity are also associated with an increased risk of colorectal cancer. Green Pharmacy is a terrificwebsite highlighting the benefits of a healthy diet and is updated regularly by acclaimed

ethnobotanist Jim Duke PhD. Dr. Duke travelled the world seeking plants with high anticancer activity for the National Cancer Institute and is a wealth of knowledge on food pharmacy, or using food as medicine.
Weight LossFor patients with colorectal cancer, maintaining a healthy diet is important in order to withstand the rigors of treatment, and, to reduce the severity of side effects from treatment, whether surgical, chemotherapy, radiation therapy, or a combination of any of these. A healthy diet includes: fluids, to prevent dehydration; protein, to maintain muscle mass and repair body tissue; carbohydrates and fats, to produce the calories that supply fuel to the body for energy; and vitamins and minerals, to maintain normal body functioning.Nutritional status is measured by body weight. Side effects from colorectal cancer treatment that cause weight loss and an unhealthy nutritional status include: constipation, diarrhea, fatigue, gas and bloating, loss of appetite, nausea, sore mouth and throat, taste changes, and vomiting.A diagnosis of colorectal cancer can also cause anxiety, and the treatment can cause pain, both of which can also lead to weight loss.
Omega-3 fatty acids have been found to be beneficial for neuropathy and appetite in cancer patients. A current study at Johns Hopkins has experts looking at fish oils to stimulate appetite. Omega-3 fats have protective properties against cancer and all the other chronic diseases. Omega-3 fats are found in fatty fish (salmon, herring, and mackerel), flax seed and flax seed oil, walnuts, and canola oil. In terms of prevention, patients should take a standard multivitamin with one hundred percent of each vitamin and mineral needed for the day.
Dietary fiber has a protective effect on the pathophysiology of colorectal cancer. Diets rich in vegetables and high fiber grains demonstrated significant protection against fatal colorectal cancer, as revealed in a prospective study of more than 760,000 people.
Fiber appears to have a number of mechanisms responsible for its protective effects: it decreases fecal transit time by increasing stool bulk; it appears to dilute the concentration of other colonic constituents, which tends to minimize contact between carcinogens and colon epithelium; and it is not digested or absorbed in the small intestine but undergoes fermentation in the presence of the colonic flora, which reduces fecal pH and generates short-chain fatty acids. Certain short-chain fatty acids can protect isolated colonic epithelial cells.Diet appears to play a significant role in determining the incidence of colorectal cancers in the general population. Although the international incidence of colorectal cancer varies widely, groups migrating from low-risk to high-risk regions experience an increase in the incidence of the disease. Diets high in fat and low in fiber have consistent associations with increased colorectal cancer risk.
Dietary Modifications and the Side Effects of Treatment
Patients with colorectal cancer can manage many of the side effects of treatment. Knowing that surgery can lead to fluid and electrolyte loss, patients can supplement their diet with as many caffeine- and alcohol-free drinks as possible, and with sports drinks with electrolytes and liquid supplements, such as Ensure, Boost®, Carnation® Instant Breakfast®, etc. Surgery can also cause the mal-absorption of some vitamins; patients can add a regular multivitamin supplement to the diet.Because patients may be at risk for obstructions at the time of surgery, high residue foods, including nuts, popcorn, seeds, raw fruits and vegetables, and anything with a skin, should be avoided.During chemotherapy and radiation therapy, patients can become dehydrated as well as nauseous. Liquids and clear, bland food (baked chicken, buttered noodles, crackers, etc.) can alleviate these side effects.
Eating and drinking slowly and having meals at room temperature or a little colder can alleviate nausea. Patients should not lie down for two hours after a meal. If possible, patients should not eat in a room with cooking smells, and should have someone else prepare the meals.

With all types of colorectal cancer treatment, patients should eat small, frequent meals, usually consisting of foods high in calories and protein. Variations in the amounts of protein and calories may occur when patients address specific side effects. Patients should try not to skip a meal, no matter how bloated or nauseous they feel.Patients should not take any more than one hundred percent of the recommended dose of any vitamin or mineral. A regular Centrum® or One-A-Day® would be within the guidelines. Any amount over one hundred percent may affect the effectiveness of treatment. Patients are encouraged to eat a good variety of foods, including plenty of fruits and vegetables, in order to get all of the necessary nutrients from food rather than from supplements.
Patients should also discuss any side effects they experience with the Johns Hopkins colorectal cancer health care team. Medications may be necessary to lessen the severity of some side effects.
Different side effects require different dietary strategies to manage. The strategies found herein are generalized. Some may work for some patients, others may not. To alleviate constipation, patients should drink plenty of fluids, including prune juice and small amounts of caffeinated beverages, and eat high fiber foods, including bran cereal, oatmeal, and raw fruits and vegetables. If making a change in diet does not work for the patient, medications might be necessary.
To alleviate diarrhea, patients should drink clear liquids, eat low fiber, low fat foods, and avoid heavy, greasy foods, raw fruits and vegetables, strong spices, and caffeine.
To alleviate gas, patients should eat slowly, use a straw and drink out of a glass instead of a bottle, and try Beano®, if necessary. Patients should not eat cruciferous vegetables, including broccoli and cabbage, beans, eggs, garlic, onions, or foods with fructose or sorbitol added. Sometimes dairy products cause gas, so patients should try lactose-free items. Patients should not drink carbonated beverages.To alleviate sore mouth and throat, which patients may experience from treatment with chemotherapy, patients should eat soft, creamy foods; adding gravies, sauces, and dressings to anything to help soften the food. Patients should drink through a straw, and drink liquid supplements, such as meal replacement drinks.
Patients should avoid eating or drinking anything very hot or very cold, and should not eat crispy, crunchy, sour, acidic, or very salty foods or spices, such as pepper, curry, or peppermint. Alcohol and caffeine should also be avoided.
To alleviate taste changes, which patients may experience from treatment with chemotherapy, patients should eat anything that is tart and sour, such as lemonade, limeade, etc. Sourballs tend to help, as does adding spices, herbs, and marinades to food, to give it the strongest flavor possible.If patients experience a metallic taste, they should use plastic silverware and drink with a straw. They should eat and drink things that are cold, cool, or room temperature.
With any and all side effects, patients are encouraged to keep trying a food because taste continually changes. What tastes off today, might taste fine tomorrow. As a patient’s gastrointestinal tract adapts to colorectal cancer treatment, and repairs and replaces lost tissue, symptoms will resolve slowly. Patients are encouraged to add items in slowly, to add one new food or drink at a time to assess tolerance.
After Treatment
All of the nutritional recommendations for patients who have completed colorectal cancer treatment are the opposite of what is recommended for patients during treatment. During treatment, diet is dictated to a great extent by the side effects a patient experiences. After treatment, patients now need to follow eating patterns that will maintain good health and prevent cancer and other chronic diseases, such as heart disease, hypertension, and diabetes.Patients who have completed their treatment regimen and whose side effects have subsided should: eat fruits, vegetables, and whole grains; limit fats, and choose good fats versus bad fats; eat lean meats and poultry; and eat low-fat dairy products. These patients should

reduce or restrict alcohol intake.To prevent cancer, the recommended amount of fruits, vegetables, and whole grains is ten servings daily. A piece of fruit, one half cup of fruit juice, a cup of canned fruit, one half cup of chopped vegetables; each is one serving. In terms of fiber, the goal is to aim for 20 grams per day. These foods provide antioxidants and phytochemicals, which protect against cell damage and tumor growth.
Patients should reduce total fat intake. Excess fat causes more bile acids to come into the intestine to digest the fat. Excess bile acids could change the bacteria in the intestine, possibly leading to cell damage and tumor growth. Patients should eat lean meats, low-fat dairy products, and, the good fats, the omega-3 fats.
Both diet and exercise enhance the body's defense system, providing an adverse environment for cancer cells. Patients should engage in 30 minutes a day of moderate, physical intensity.
Diet and nutrition also play a part in complementary and alternative medicine. Besides monitoring diet, palliative care may also be useful to alleviate pain and discomfort comprise.
Staying Fit to Fight Colon Cancer
Several reports have shown that regular physical activity both improves the outcome of
patients with colorectal cancer as well as serve as a strong preventative tool protecting against its development.
See below for reviews of the research highlighting the benefits of exercise in colon cancer prevention and therapy.
Recent studies highlighting the benefits of exercise during colon cancer therapy.
According to two recently published studies, simply walking 30 minutes per day can significantly reduce the risk of recurrence in patients recently diagnosed with colon cancer. "Higher levels of physical activity contributed to a 50% reduced risk of recurrence and mortality when combined with standard therapies," says Jeffrey Meyerhardt from Dana-Farber Cancer Institute, the lead author of two recently published studies linking exercise to improved colorectal cancer survival.
In the first study, researchers found that patients diagnosed with stage III colon cancer who were physically active (walking 6 or more hours per week) at six months following therapy, had significantly lower rates (50%) of recurrences and death from the disease than inactive patients. In a subsequent study, the same researchers observed 573 women with stage I to III colorectal cancer and determined those patients who increased their physical activity experienced a 50% reduction in mortality. In an editorial which accompanied these studies, Wendy Denmark-Wahnefried from Duke University concluded that "These strong epidemiological studies give consistent data about the benefits of exercise for cancer survivors."
Check out the Active Surviors Network to see how you can recover through physical activity.
Impact of physical activity on cancer recurrence and survival in patients with stage III colon cancer: findings from CALGB 89803. Journal of Clinical Oncology. 2006 Aug 1;24(22):3535-41. Physical activity and survival after colorectal cancer diagnosis. Journal of Clinical Oncology. 2006 Aug 1;24(22):3527-34

Mind & Body Therapies
Mind/body therapy uses a variety of techniques designed to enhance the mind's capacity to
affect bodily function and symptoms. Some techniques that were considered complementary in the past have become part of conventional treatments, such as patient support groups and cognitive-behavioral therapy. Other mind/body techniques are still considered complementary, including meditation, prayer (both by the patient and intercessory), mental healing, aromatherapy, and therapies that use creative outlets such as art, music, or dance.
The mind/body techniques of meditation, deep breathing, yoga, or relaxation techniques are safe, inexpensive, and patient-controlled, an important factor in preventing cancer from psychologically controlling the patient at every moment.
Other mind/body practices also empower the patient. Hypnosis is relatively safe, and very good for conditioned responses, such as dealing with anticipatory nausea that a patient feels walking into the chemotherapy treatment room, or doctorÕs office.
Visual imagery via feedback has been proven beneficial to patients from spiritual and psychosocial perspectives. Mindfulness-based stress reduction is offered as a treatment modality at Johns Hopkins because it has been shown to lessen stress, decrease pain, and improve coping mechanisms for patients with cancer.
Manipulative and Body-based TherapiesManipulative and body-based practices are based on manipulation and/or movement of one or more parts of the body.
Acupressure and acupuncture have been documented to benefit patients with nausea, vomiting, acute pain, fatigue, dry mouth, swelling, and shortness of breath. The side effects are minimal, so these are deemed a safe modality of complementary treatment.
Acupressure and acupuncture are contraindicated, however, in patients with: unstable spines, clotting or bleeding disorders, very low white blood counts, a neutrophil count less than a thousand, and lymphodema.
Chiropractic treatments are relatively safe, since most patients experience only minor discomfort for a day or two, but, with manipulation of the cervical spine, there have been some adverse reactions, such as tinnitus. A patient must engage only a certified chiropractor.
Massage therapy has been documented beneficial for relaxation, pain control, and insomnia. Doctors are treating patients who have lymphodema, a swelling of their limbs due to surgery, with massage therapy called Òmanual, emphatic drainageÓ. The side effects are very minimal, and the benefit is high.
The contraindications of massage therapy are few. If a patient has open wounds, massage therapy is not recommended because of the oils used in the practice. If a patient has fractures, bone metastases, massage therapy is not recommended because it would put pressure on those areas. It is debatable whether massage therapy is safe to use over the internal bed of a tumor.

CLINICAL TRIAL
Mission
Clinical trials and research studies are a key component of the multidisciplinary approach of the Johns Hopkins Colon Cancer Health Care Team. Clinical trials test new treatments in people with cancer, such as: new drugs, newcombinations, new approaches to surgery or radiation therapy, or, new methods, such as gene therapy.research is to find better ways to treat cancer and help cancer patients.
Overview
Clinical trials and research studies are important tools in the discovery of new treatments against cancer. Clinical trials contributeknowledge and may lead to new breakthroughs in the treatment of cancer. If a new treatment proves effective in a study, it may become a new standard treatment that can help many patients. Most of today's most effective standard treatments are based on previous study results, such as those for breast, colon, rectal, and childhood cancers.
Patients who participate may be helped personally by the treatment(s) they receive. Trial participants get up-to-date care from cancer experts, and they receive either a new treatment being tested or the best available standard treatment for their cancer. Of course, there is no guarantee that a new treatment being tested or a standard treatment will produce good results. New treatments also may have unknown risks.
But, if a new treatment proves effective, or more effective, than standard treatment, study patients who receive it may be among the first to benefit. Many patients receiving standard treatment benefit from it. In the past, clinical trials were sometimes seen as a last resort for people who had no other treatment choices. Today, patients with common cancers often choose to receive their first treatment in a clinical trial.
The following Johns Hopkins trials currently being evaluated in order to improve the efficacy of colorectal cancer treatments areanyone meeting the eligibiligy criteria. For additional information please call our clinical trials specialist at (410) 614-3163
Ongoing Research
Stage I Colorectal Cancer

J0746: Biomarker blood test to detect the recurrence of colorectal cancer
Neoadjuvant chemoradiation therapy and local excision for rectal cancer.
Stage II Colorectal Cancer
E5202: FOLFOX vs. FOLFOX plus Avastin (bevacizumab) for patients who have undergone resection of stage II CRC
Randomized trial comparing preoperative radiation therapy and capcetabine with preoperative radiation therapy and continuous infusion of 5-FU for patients with operable carcinoma of the rectum
J0746: Biomarker blood test to detect the recurrence of colorectal cancer
Stage III Colorectal Cancer
Randomized trial comparing preoperative radiation therapy and capcetabine with preoperative radiation therapy and continuous infusion of 5-FU for patients with operable carcinoma of the rectum
J0746: Biomarker blood test to detect the recurrence of colorectal cancer
N0147: FOLFOX vs. FOLFOX plus Erbitux (Cetuximab) for patients who have undergone resection of Stage III CRC
Stage IV Colorectal Cancer
Rapid Medical Donation Program. One way that patients with terminal colorectal cancer can greatly benefit colorectal cancer research is

by agreeing to undergo an autopsy.
J04104: Sorafenib in combination with Irinotecan and Erbitux (Cetuximab) for patients who have had disease progression after 2 lines of chemotherapy
J0745: Vaccine plus Cytotaxan for patients who have had previously resected colorectal liver metastasis and chemotherapy
J0660: Therasphere for the Treatment of Liver Metastases from Primary Colorectal Cancer
J09110: ARRY, an oral MEK inhibitor for patients who have progressed through standard chemotherapy
Hereditary Colon Cancer
Curcumin for Treatment of Intestinal Adenomas in Familial Adenomatous Polyposis (FAP)
v