-
8/12/2019 Jacques Ker
1/29
Guidelines on the early
management of head injury J Kerr
A&ERoyal Infirmary, Edinburgh
-
8/12/2019 Jacques Ker
2/29
Head Injury
10% of A/E workloadA/E Dept seeing 85,000 annual
attendances8,500 head injuries1,700 admissions35 head injuries
requiring resuscitation
20 require neurosurgery220 patients require CT scan5100 patients
can be discharged safely from A/E
Significant cost
Expeditious management reduces secondary braininjuryAssociated
injuries and secondary effectsHigh proportion of patients have a
subsequentdisability
-
8/12/2019 Jacques Ker
3/29
Guidelines
Guidelines for initial management after head injury in adults
-Suggestions from a group of neurosurgeons March 1984 Commission on
the Provision of Surgical Services. Report ofthe Working Party on
Head Injuries. London: RCS; 1986
European Brain Injury Consortium. Guidelines for themanagement
of severe head injury in adults 1997 British Neurological Surgeons
1998 Report of the Working Party on the Management of Patients
with Head Injuries - Prof Galasko; Royal College of Surgeonsof
England June 1999 SIGN August 2000Canadian CT Head Rules 2001
NICE June 2003
-
8/12/2019 Jacques Ker
4/29
SIGN
Scottish Intercollegiate Guidelines NetworkFormed in 1993
Development of SIGN Guidelines - series of70+ publications
No 46: Early Management of Patients with aHead Injury -
published August 2000
-
8/12/2019 Jacques Ker
5/29
-
8/12/2019 Jacques Ker
6/29
NICE
National Institute for Clinical ExcellenceEstablished as a
Special Health Authority inEngland and Wales, April 1st
1999Technology appraisals and clinical guidelinesHead Injury;
Triage, assessment, investigationand early management of head
injury ininfants, children and adults published June2003
-
8/12/2019 Jacques Ker
7/29
Guidance represents the view of the Institute, whichwas arrived
at after a careful consideration of the
available evidence. Health professionals are expected totake it
fully into account when exercising their clinical
judgement, it does not however override their
individualresponsibility to make appropriate decisions in the
circumstances of the individual patient, in consultationwith the
patient and/or guardian or carer.
-
8/12/2019 Jacques Ker
8/29
NICE SIGN
AGREE
-
8/12/2019 Jacques Ker
9/29
HISTORY
Mechanism of Injury (MOI)Fall
RTA AssaultBlunt or penetrating trauma
Associated injuries ALCOHOL
-
8/12/2019 Jacques Ker
10/29
Symptoms
LOCAmnesia
Nausea and/or vomitingEpistaxisVisual disturbance
HeadacheDizziness/drowsiness
-
8/12/2019 Jacques Ker
11/29
GLASGOW COMA SCALE
Eye opening 4 eyes open spontaneously3 open to speech2 open to
pain1 no opening
Motor response 6 obeys commands
5 localizes to pain4 flexion3 abnormal flexion2 extension1 no
movement
Verbal response 5 orientated4 confused3 inappropriate words2
incomprehensible sounds1 no speech
-
8/12/2019 Jacques Ker
12/29
Indications for referral tohospital
GCS < 15 at any time since the injuryAmnesia
Neurological symptomsClinical evidence of a skull
fractureSignificant extracranial injuriesMOI not trivialContinuing
uncertainty about diagnosisMedical co-morbidityAdverse social
factors
-
8/12/2019 Jacques Ker
13/29
Periorbital bruisingSubconjunctival
haemorrhageCSF rhino/otorrhoeaEpistaxisHaemotympanumBattles
sign
Base of skull fracture
-
8/12/2019 Jacques Ker
14/29
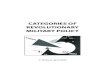
BASE OF SKULLFRACTURE
-
8/12/2019 Jacques Ker
15/29
Skull x-ray indications - SIGN
GCS < 15 orGCS 15, but:
MOI not trivial
LOCAmnesia or has vomitedFull thickness scalp laceration/boggy
haematomaInadequate history
-
8/12/2019 Jacques Ker
16/29
Skull x-ray indications - NICE
Skull x-rays have a role in the detection of non-accidental
injury in children
Skull x-rays in conjunction with high-quality in- patient
observation also have a role where CTscanning resources are
unavailable
-
8/12/2019 Jacques Ker
17/29
Skull X-ray
Advantages Quick
No need for radiologist
Low dose of radiation(0.14mSv)
Inexpensive
Disadvantages Increased workloadInconclusive
-
8/12/2019 Jacques Ker
18/29
CT Indications - SIGN
GCS 12/15 or lessDeteriorating GCS or progressive focal
neurologicalsigns
Confusion or drowsiness (GCS 13-14) followed byfailure to
improve within at most 4 hours of
clinicalobservationRadiological/clinical evidence of fracture
GCS 15, no fracture but:Severe/persistent headache, N+V,
irritability or altered
behaviour, seizure
-
8/12/2019 Jacques Ker
19/29
CT Indications - NICE
GCS less than 13 at any point since the injuryGCS 13 or 14 at 2
hours after the injurySuspected open or depressed skull fractureAny
sign of BOS fracture
Post-traumatic seizureFocal neurological deficit>1 episode of
vomitingAmnesia > 30 minutes before impact
In patients with some LOC or amnesia since the injury:
Age > 65CoagulopathyDangerous MOI
-
8/12/2019 Jacques Ker
20/29
CT Scan
AdvantagesHigh sensitivity/specificityDetection of
intracranial
haematomaDefinitive (except ultra
early)
Disadvantages
High dose of radiation(2.0mSv)Radiologist required
-
8/12/2019 Jacques Ker
21/29
-
8/12/2019 Jacques Ker
22/29
NICE vs SIGN
NICE based on Canadian CT head rules NICE lowers threshold for
CT scanning
Difficulty in obtaining out-of-hours CT scansMassive increase in
workload of radiologydepartmentsIncreased patient exposure to
radiationIncrease in cost
-
8/12/2019 Jacques Ker
23/29
Management
ABC (including C spine control)GCSO2, analgesia, tetanus,
?antibiotics, IVI
?bloodsImaging
Neuro obs: pupil size and reactivityRepeated GCS scoreGeneral
obs including p, BP, temp, BM, O2 sats, RRAlcometer
-
8/12/2019 Jacques Ker
24/29
Admission or Discharge?
GCS < 15GCS 15, but
Continuing amnesiaContinuing nausea/vomitingSevere headache
Any seizureFocal neurological signsSkull fracture
Abnormal CT
Significant medical problemsSocial problems/no supervision at
home
-
8/12/2019 Jacques Ker
25/29
Discharge from A/E
None of the above exclusion criteriaPatient must be given head
injury advice
Responsible adult to supervise the patientEasy access to a
telephoneReasonable access to a hospitalEasy access to
transport
-
8/12/2019 Jacques Ker
26/29
Transfer to Neurosurgery
Abnormal CT scanCT is indicated but cannot be done within an
appropriate
period Clinical features which warrant neurosurgical
assessment,monitoring or management:
Persisting coma (GCS 8/15)Persisting confusionDeteriorating
GCSProgressive focal neurologySeizure without full
recoveryDepressed skull fracturePenetrating injuryCSF leak/BOS
fracture
-
8/12/2019 Jacques Ker
27/29
Neurosurgical assessment andmonitoring
Experienced staff
Intensive, specific monitoringintracranial pressure
monitoringdedicated neuro-intensive carespecialised theatre
suites
Rapid access to theatre
-
8/12/2019 Jacques Ker
28/29
Head Injury Audit
Scottish Trauma Audit Group (STAG)98% coverage throughout
ScotlandAll head injuries attending A/E Departments in4 teaching
hospitalsAll head injuries admitted to Scottish hospitals
Pre-implementation November 1999Post-implementation May 2001
-
8/12/2019 Jacques Ker
29/29
QUESTIONS?