Embed Size (px)
Citation preview

Gonser et al, FHR artifacts and fetal Doppler blood flow 411
J. Perinat. Med.17(1989)411
Evaluation of fetal heart rate artifacts, hemodynamics and digoxintreatment in fetal tachyarrhythmia by Doppler measurement offetal blood flow — case report of a pre-excitation syndrome
Markus Gonser, Johannes Dietl, Karlheinz Pfeiffer, and Jean-Pierre Glees
Department of Obstetrics and Gynecology, University Hospital Tübingen, WestGermany
1 Introduction
A fetal cardiac arrthythmia may cause uninter-pretable or even misleading fetal heart rate(FHR) tracings with unreliable signs of fetaldistress [1]. Therefore evaluation of such artifactsand the haemodynamic relevance of a fetal ar-rhythmia by alternative methods [9] is necessaryfor management and therapy. Doppler measure-ment of fetal blood flow has been reported to beuseful for hemodynamic assessment of fetal car-diac arrythmias [9,10], for detection of imminentheart failure prior to fetal hydrops and for mon-itoring of therpaeutic effects of therapy [11].
2 Material and methods
External indirect FHR-monitoring during preg-nancy and internal direct FHR-monitoring fromthe fetal scalp during labor and delivery wasperformed with a comerical fetal monitoring sys-tem with autocorrelation technique (HP 8040Cardiotocograph, Hewlett-Packard, FRG). Forthe recording of a tachycardic FHR, Hewlett-Packard (Böblingen, FRG) supplied an espe-cially constructed HP 8041A Cardiotocographprototype.FHR records from both systems were checkedby cw (continuous wave)-Doppler blood flowmeasurements in umbilical artery (Doptek Spec-trum Analyser 9000 with built-in 4 MHz cw-Doppler, Foptek Ltd, GB).Blood flow in the fetal descending aorta wasmeasured with combined real-time and pulsedDoppler ultrasound (Kretz Combison 320-5:
Curriculum vitae
MARKUS J. GONSER,M.D., was born in 1953in Horb-Altheim, WestGermany. He studiedmathematics and physics,from 1973 to 1977, med-icine, from 1977 to 1984,and in 1984, he graduatedfrom the Faculty of Med-icine at the University of ' ^ *Tubingen. From 1984 to ^1985, he did industrial re-search fellowship in pharmacokinetics from the Boehrin-ger Ingelheim Fonds, Foundation for basic research inmedical sciences. Since 1985, he is specializing in ob-stetrics and gynecology at the University of Tübingen.
5 MHz Sector Ultrasound Scanner with built in2.2 MHz pulsed Doppler, Duplex system,KretzTechnik, Austria); with real-time display of"full" spectral Doppler sonogram (pulse repeti-tion frequency PRF: 6.25 MHz, wall motionfilter WMF: 125 Hz; adjustments fixed by M. G.)and off-line estimate of mean velocity (intensity-weighted spectral and temporal average). Fetalsize and vessel diameter were measured on frozenultrasound image from the same system.
3 Clinical information and results
A 28-year-old healthy woman was referred at 30weeks of gestation because of fetal tachycardia-bradycardia-arrthythmia. Apart from a hydropicplacenta, ultrasound examination showed nor-
1989 by Walter de Gruyter & Co. Berlin · New York

412 Gonser et al, FHR artifacts and fetal Doppler blood flow
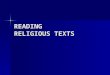
Figure 1. External FHR record in fetal arrhythmia with paroxysmal bigeminal and trigeminal pulse. Check ofthe questionable tracings with cw-Doppler blood flow measurement in umbilical artery (pseudobradycardia).
mal fetal and cardiac anatomy, but with arrhyth-mia in fetal real-time and M-mode echocardio-graphy [7, 8]. The obtained FHR-record wasirregular, showing alternating periods of severebradycardia. Checking this questionable tracingby cw-Doppler assessment of umbilical arteryblood flow revealed periods of bigeminal andtrigeminal pulse with a numerically normal heartrate (figure 1). Obviously the fetal monitoringsystem was triggered by one of two or threepulsations respectively and thus demonstratedpseudobradycardia.During the next four hours, the FHR turned toregular tachycardia by ascultation, but conven-tional FHR-monitor concealed fetal tachycradiaand mimicked falsely normal FHR. A secondFHR-monitor prototype, designed especially forfetal tachycardia, recorded FHR correctly, witha mean hart rate of 240 bpm as demonstratedwith cw-Doppler (figure 2). Oral transplacentaldigitalization was started (beta-acetyldigoxin,3 χ 0.2 mg/d) [4] to prevent recurrent tachycardiaand worsening of fetal heart failure [7, 11 15].Transplacental cardioversion was not achieveddefinitively, however FHR was basically normalduring treatment.
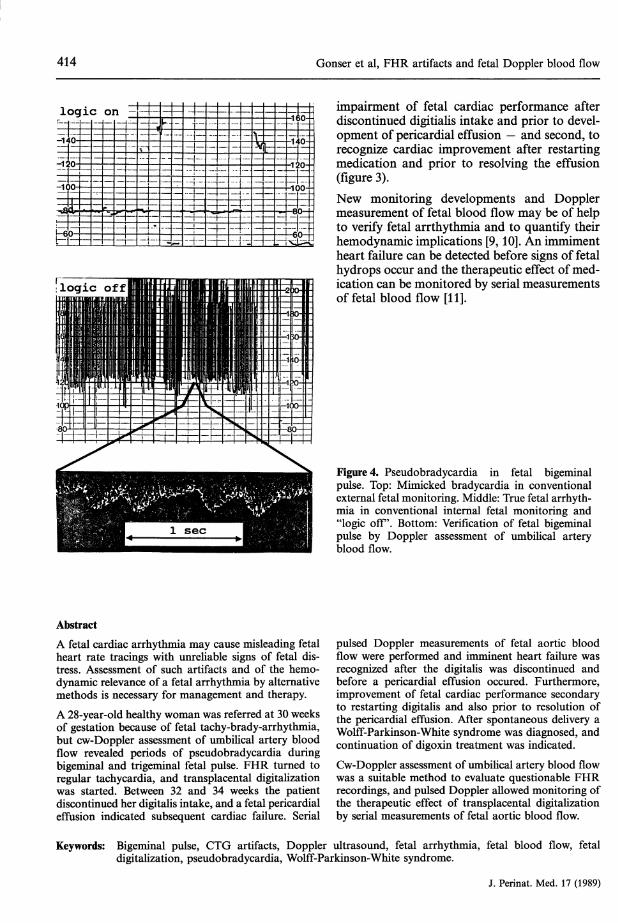
Between 32 and 34 gestational weeks, the patientdiscontinued digitalis intake against medical ad-vice, and a temporary pericardial effusion, be-tween 34 and 36 weeks, indicated subsequentworstening of fetal cardiac failure [2]. Serialpulsed Doppler measurements of fetal aorticblood flow [3, 9, 10] were performed at 30, 32,33, 35 and 36 weeks of gestation. Thus imminentfetal heart failure was recognized after discontin-ued medication and before pericardial effusionoccured. Furthermore, improvement of fetal car-diac performance secondary to restarting themedication and prior to resalution of pericardialeffusion was recognized also (figure 3).During spontaneous labor and delivery, at 37weeks of gestation, fetal arrhythmia with bige-minal pulse recurred, and again internal FHRmonitoring from the fetal scalp showed pseu-dobradycardia; however, the FHR recording wascorrect when "logic" was switched off (figure 4).The nonhydropic male infant weighed 4150 gand demonstrated minimal signs of neonatal dis-tress (Apgar score 5 and 1 at 1 and 5 min re-spectively) with delayed onset of respiration andbradycardia, although the pH of umbilical cordblood was normal (art: 7.32, ven: 7.39).
J. Perinat. Med. 17 (1989)
Gonser et al, FHR artifacts and fetal Doppler blood flow 413
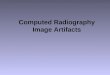
Figure 2. Fetal tachycardia with two-to-one block inconventional fetal monitor (CTG artifact). Top: Ex-ternal prototype FHR-monitor (*), showiing a correcttrace. Middle: External convention FHR-monitor withmisleading "normal" tracing, as a result of "halving"true FHR [5]. Bottom: Check of FHR with cw-Dopp-ler assessment of umbilical artery blood flow: 240 pbm.(*) Prototype supplied by Hewlett-Packard, Böblingen,FRG.
Postpartum echocardiography confirmed nor-mal heart anatomy and ECG showed pre-exita-tion with delta-waves [14], but no signs of digi-talis intoxication. Thus a Wolff-Parkinson-Whitesyndrome was diagnosed and continuation ofdigoxin treatment was indicated [6, 12]. At sixmonths of life, treatment was stopped and fur-ther examinations revealed normal developmentand normal sinus rhythm (Dept. of Pediatrics,Div. of Pediatric Cardiology, University Hospi-tal, Tübingen).
4 DiscussionIn fetal monitoring systems, preprocessing ofincoming signals according to certain preset lim-
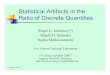
Volume flow: Q ( m l / m i n - k g )300
200
100
Mean velocity: v (cm/s)50
30
1028 32 36 40
ß-Acetyl - N==l 1=1 Cfdigoxin 3xo.2 mg/dPericardial effusion [ - [
Figure3. Blood flow in fetal descending aorta: Re-cognition of impairment and improvement of fetalcardiac performance prior to evolution and prior toresolution of pericardial effusion. This effusion ap-peared after discontinued digitalis intake. Sponta-neously delivery after 37 weeds of gestation, 4150 g,Apgar 5/7/9, pH A: 7.32; V: 7.39.(Nomogram after ERSKINE RLA and RITCHIE JWK[3]).
its, such as maximal FHR range or maximalFHR changes ("logic"), and autocorrelationtechnique allow indirect and automatical FHRdetection and recognition, in spite of minimalmaternal or fetal movements. These technicalapproaches can obscure FHR monitor andfalsely normal FHR is mimicked [5, 7, 8, 13]. Inthis case, pre-excitation with bi- or trigeminalpulse caused severe tachycardia, but on the fetalmonitor appeared a "normal" heart rate tracing(figure 2); or during the preceding and intrapar-tum periods of bi- and trigeminal pulse FHRwas numerically normal, but a severe bradycar-dia was recorded (figures 1, and 4).Cw-Doppler assessment of umbilical arteryblood flow was a suitable method to check ques-tionable FHR recordings quickly. With serialpulsed Doppler measurements of fetal aorticblood flow, it was possible, first to recognize
J. Perinat. Med. 17 (1989)
414 Gonser et al, FHR artifacts and fetal Doppler blood flow
logic on -I—I— 3=H-
H-
-8.0-+
Ffcaoi
impairment of fetal cardiac performance afterdiscontinued digitialis intake and prior to devel-opment of pericardial effusion — and second, torecognize cardiac improvement after restartingmedication and prior to resolving the effusion(figure 3).New monitoring developments and Dopplermeasurement of fetal blood flow may be of helpto verify fetal arrthythmia and to quantify theirhemodynamic implications [9,10]. An immimentheart failure can be detected before signs of fetalhydrops occur and the therapeutic effect of med-ication can be monitored by serial measurementsof fetal blood flow [11].
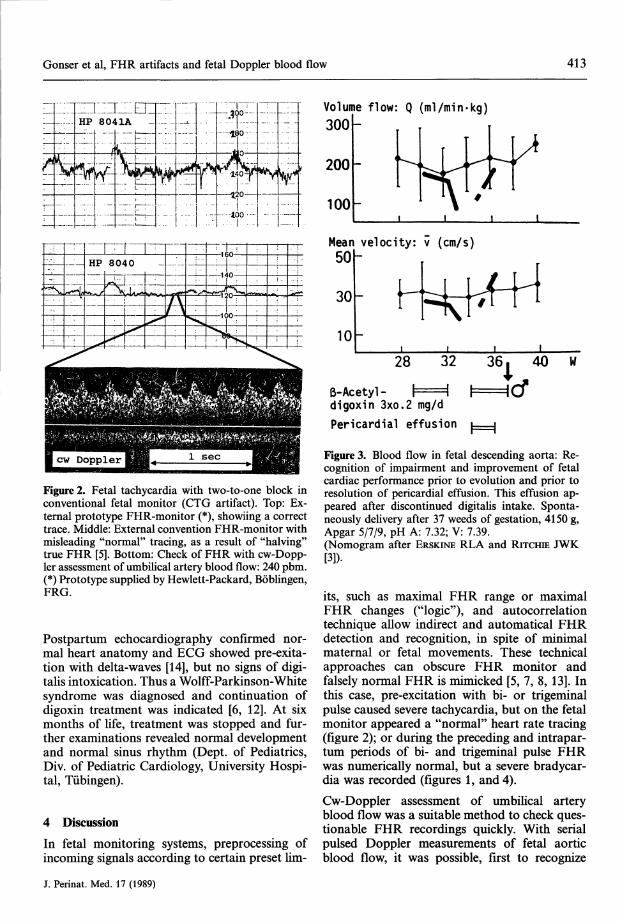
Figure 4. Pseudobradycardia in fetal bigeminalpulse. Top: Mimicked bradycardia in conventionalexternal fetal monitoring. Middle: True fetal arrhyth-mia in conventional internal fetal monitoring and"logic off". Bottom: Verification of fetal bigeminalpulse by Doppler assessment of umbilical arteryblood flow.
Abstract
A fetal cardiac arrhythmia may cause misleading fetalheart rate tracings with unreliable signs of fetal dis-tress. Assessment of such artifacts and of the hemo-dynamic relevance of a fetal arrhythmia by alternativemethods is necessary for management and therapy.A 28-year-old healthy woman was referred at 30 weeksof gestation because of fetal tachy-brady-arrhythmia,but cw-Doppler assessment of umbilical artery bloodflow revealed periods of pseudobradycardia duringbigeminal and trigeminal fetal pulse. FHR turned toregular tachycardia, and transplacental digitalizationwas started. Between 32 and 34 weeks the patientdiscontinued her digitalis intake, and a fetal pericardialeffusion indicated subsequent cardiac failure. Serial
pulsed Doppler measurements of fetal aortic bloodflow were performed and imminent heart failure wasrecognized after the digitalis was discontinued andbefore a pericardial effusion occured. Furthermore,improvement of fetal cardiac performance secondaryto restarting digitalis and also prior to resolution ofthe pericardial effusion. After spontaneous delivery aWolff-Parkinson-White syndrome was diagnosed, andcontinuation of digoxin treatment was indicated.Cw-Doppler assessment of umbilical artery blood flowwas a suitable method to evaluate questionable FHRrecordings, and pulsed Doppler allowed monitoring ofthe therapeutic effect of transplacental digitalizationby serial measurements of fetal aortic blood flow.
Keywords: Bigeminal pulse, CTG artifacts, Doppler ultrasound, fetal arrhythmia, fetal blood flow, fetaldigitalization, pseudobradycardia, Wolff-Parkinson-White syndrome.
J. Perinat. Med. 17 (1989)

Gonser et al, FHR artifacts and fetal Doppler blood flow 415
CTG-Artefakte, Hämodynamik und Digitalisierung beifetalen Tachyarrhythmien — dopplersonographischeÜberwachung am Beispiel eines PräexzitationssyndromsEine fetale cardiale Arrhythmie kann nicht interpre-tierbare oder irreführende Aufzeichnungen der fetalenHerzfrequenz (FRF) verursachen. Daher ist die Un-tersuchung solcher CTG-Artefakte [1] und der hämo-dynamischen Relevanz einer aktuellen fetalen Arrhyth-mie durch alternative Methoden [9] im Hinblick aufManagement und Therapie notwendig.Die externe CTG-Überwachung erfolgte mit einemherkömmlichen Autokorrelationscardiotokographen(HP 8040). Die FHF-Aufzeichnungen wurden durchdopplersonographische Strömungsmessungen in derUmbilikalarterie überprüft (Doptek Spectrum Analy-ser 9000 mit eingebautem 4 MHz cw-Doppler). DieDurchblutung in der absteigenden fetalen Aorta wurdemit kombinierter Real-Time und Pulsdoppler-Sono-graphie gemessen (Kretz Combison 320-5, Duplex-System).Uns wurde eine 28jährige gesunde Frau in der 30.Schwangerschaftswoche wegen fetaler Tachy-/Bra-dyarrhythmien überwiesen. Die FHF-Aufzeichnungenwaren irregulär, alternierend traten Phasen mit schwe-rer Bradykardie auf. Die zugehörigen Dopplersono-gramme der Umbilikalarterie zeigten jedoch Periodenmit Bigeminus und Trigeminus, wobei die Herzfre-quenz numerisch normal war (Abb. l u. 4). Offensicht-lich wurden im CTG nur eine von 2 oder 3 Pulsationenerkannt und es zeigte daher eine Pseudobradykardie.Während der nächsten Stunden wechselte die FHF zueiner regelmäßigen Tachykardie mit einer mittleren
Frequenz von 240 spm, und wir begannen mit eineroralen transplazentaren Digitalisierung [15]. Zwischen32 und 34 Wochen unterbrach die Patientin die Digi-taliseinnahme und zwischen 34 und 36 Wochen tratzeitweilig ein Perikarderguß als Hinweis auf eine ma-nifeste Herzinsuffizienz auf [2]. Die Durchblutungs-messungen in der fetalen Aorta ließen eine Verschlech-terung der Herzleistung nach Absetzen der Medikationund vor Auftreten des Perikardergusses erkennen. Imweiteren Verlauf war eine Verbesserung der Herzlei-stung nach Wiedereinsetzen der Medikation und vorRückbildung des Perikardergusses nachweisbar(Abb. 3).Nach 37 Schwangerschaftswochen kam es zur Spon-tangeburt eines Kindes ohne Hydrops. Man diagno-stizierte ein Wolff-Parkinson-White-Syndrome undsetzte die Digitalisbehandlung fort [6,12].Die Bearbeitung aufgenommener Signale gemäß ge-wisser vorgegebener Grenzen wie maximalen Bereichder FHF und maximale FHF-Änderungen ("Logik")ermöglicht eine automatische FHF-Anzeige und -Er-kennung. Jedoch können mit dieser Technik FHF-Aufzeichnungen bei fetalen Tachyarrhythmien unklarbleiben [1]. Doppleruntersuchungen der Nabelarterienerwiesen sich als geeignete Methode, um zweifelhafteFHF-Aufzeichnungen abzuklären. Mit dem gepulstenDoppler war es möglich, eine beginnende Herzinsuf-fizienz vor Auftreten von Hydropszeichen zu erkennenund den therapeutischen Effekt einer transplazentarenDigitalisierung durch Verlaufsmessungen der fetalenAortendurchblutung nachzuweisen [11].
Schlüsselwörter: Bigeminus, CTG-Artefakte, Dopplersonographie, fetale Arrhythmie, fetale Digitalisierung,fetaler Blutfluß, Pseudeobradykardie, Wolff-Parkinsln-White-Syndrom.
Resume
Evaluation des artefacts CTG, de Phemodynamique etdu traitement par digoxine dans les tachyarythmiesfetales a l'aide de la mesure Doppler du FLUX sanguinfoetal. A propos d'un cas de syndrome de preexitationUarythmie cardiaque foetale peut entrainer des enrigs-trements du rythme cardiaque foetal (RCF) ininterpre-tables ou meme trompeurs. C'est la raison pour la-quelle la mise en evidence de tels artefacts du RCF [1]et de Phemodynamique seconaires ä une arythmiefoetale en cours par des methodes alternatives [9] estnecessaire pour la prise en charge et la therapeutique.Le monitorage du RCF par voie externe a ete realiseä l'aide d'un Systeme du surveillance foetale ducommerce avec une technique d'auto-correlation (car-diotocographe HP 8040). Les enregistrements du RCFont ete completes par des mesures doppler au niveaude Tartere ombilicale (Doptek spectrum analyser 9000avec 4MHZ cw Doppler), et de Faorte descendantepar association d'echographie combinee en temps reel
et doppler pulse (Kretz Combison 320-5, Duplex sys-tem).Une patiente de 29 ans, en bonne sante a ete adresseeä 30 semaines de gestation en raison d'une tachy-brady-arythmie foetale. Le RCF etaie irregulier, avecalternance de periodes de bradycardies majeures, maisPexamen doppler de Fartere ombilicale a mis en evi-dence des periodes de bigeminisme et de trigeminismeavec un rythme cardiaque foetal numeriquement nor-mal (figures 1, 4). A Fevidence le monitorage foetal älui seur ne recommit qu'une des deux ou trois pulsa-tions respectives et met en evidence une pseudobra-dycardie.Au cours des heures suivantes, le RCF evolua vers unetachycardie reguliere, avec un rythme moyen de 240bpm, et une digitalisation transplacentaire par voieorale fut commencee [15]. Entre 32 et 34 semaines, lapatiente interrompit son traitement digitalique et unepanchement pericardique temporaire, entre 34 et 36
J. Perinat. Med. 17 (1989)
416 Gonser et al, FHR artifacts and fetal Doppler blood flow
semaines, fut le temoin d'une defaillance cardiaqueconsecutive [2]. On effectua des series de mesure dop-pler pulse du flux sanguin aortique foetal ce qui permitde reconnaitre une defaillance des performances car-diaques foetales apres arret de la therapeutique. Enoutre, l'amelioration des performances cardiaquesfoetales secondaires au redemarrage de la therapeutiqueet avant la disparition de 1'epanchement pericardiquefut mis en evidence (Figure 3).A 37 semaines de gestation naquit un enfant nonhy-dropique de fagon spontanee. On fit le daignostic desyndrome de Wolf-Parkinson White et la poursuite dutraitement digoxique fut indiquee [6,12].Le pretraitement des signaux d'entree selon certaines
limites preetablies, telles que Fetendue maximale duCRF et les variations maximales du RCF ("logiques"),permet la detection automatique du RCF et sä recon-naissance. Mais cette technique peut masquer Fenre-gistrement du RCF en cas de tachy-arythmie foetale[1]. L'etude doppler du flux sanguin dans Fartere om-bilicale est une methode appropriee pour faire le biland'enregistrement du rythme cardiaque foetal a pro-bleme. Par doppler pulse il est possible de reconnaitreune defaillance cardiaque imminente avant Fapparitiondes signes d'hydrops foetal, et de surveiller les effetstherapeutiques de la digitalisation transplacentaire pardetermination en serie du flux sanguin aortique foetal[11].
Mots-cles: Artefacts CIG, arythmie foetale, debit sanguin foetal, digitalisation foetale, echographie Doppler,pseudobradycradie, pulse bigemine, syndrome de Wolf-Parkinson-White.
References
[1] BEALL MH, RH PAUL: Artifacts, blocks and ar-rythmias: confusing nonclassical heart rate trac-ings. Clin Obstet Gynecol 29 (1986) 83
[2] DEVORE GR, RL DONNERSTEIN, CS KLEINMAN,LD PLATT, JC HOBBINS: Fetal echocardiography.II. The diagnosis and significance of a pericardialeffusion in the fetus using real-time-directed M-mode ultrasound. Am J Obstet Gynecol 144(1982) 693
[3] ERSKINE RLA, JWK RITCHIE: Quantitative meas-urement of fetal blood flow using Doppler ultra-sound. Br J Obstet Gynaecol 92 (1985) 600
[4] GONSER M: Transplacental digitalisation of thefetus — Proposal of loading and maintenancedose calculations based on maternal weight andcreatinine clearance. Naunyn-Schmiedeberg'sArch Pharmacol 337 (1988) R4 (suppl), abstr
[5] HERTOGS K: Supraventricular tachycardia in uterowith two-to-one block in fetal monitor. Lancet i(1981) 1158
[6] JAMES TN: Cardiac conduction system: fetal andpostnatal development. Am J Cardiol 25 (1970)213
[7] KLEIN AM, IR HOLZMAN, EM AUSTIN: Fetaltachycardia prior to the development of hydrops— Attempted pharmacological cardioversion:Case report. Am J Obstet Gynecol 134 (1979) 347
[8] KLEINMAN CS, RL DONNERSTEIN, CC JAFFE, GRDEVORE, EM WEINSTEIN, DC LYNCH, NS TALNER,RL BERKOWITZ, JC HOBBINS: Fetal echocardio-graphy. A tool for evaluation of in utero cardiacarrhythmias and monitoring of in utero therapy:analysis of 71 patients. Am J Cardiol 51 (1983)237
[9] LINGMAN G, J-A DAHLSTRÖM, SH EIK-NES, KMARSAL, P OHLIN, S OHRLANDER: Haemodyn-amic assessment of fetal heart arrhythmias. Br JObstet Gynecol 91 (1984) 647
[10] MARSAL K, A LINDBLAD, G LINGMAN, SH EIKNES:Blood flow in the fetal descending aorta;intrinsic factors affecting fetal blood flow, i.e.fetal breathing movements and cardiac arrhyth-mias. Ultrasound in Med Biol 10 (1984) 339
[11] MARSAL K, A LINDBLAD, G LINGMAN, P SIND-BERG-ERIKSEN: Fetal circulatory changes associ-ated with cardiac arrhythmia, smoking and ex-perimental asphyxia. In: SHELDON CD, DHEVANS, JR SALVAGE (eds.): Obstetric and neonatalblood flow. Biological Engineering Society, Con-ference Proceedings, Vol 2, London, 1987, pp59-66
[12] MOENE RJ, JP Roos: Transient Wolff-Parkinson-White" syndrome and neonatal reciprocating tach-ycardia. Circulation 59 (1973) 443
[13] REES L, PR VLIES, J ADAMS: Hydrops fetalis, anunusual cause, presentation and method of diag-nosis. Case report. Br J Obstet Gynaecol 87 (1980)1169
[14] VIDAILLET HJ, JC PRESSLEY, E HENKE, FE HAR-RELL, LD GERMAN: Familial occurence of acces-sory atrioventricular pathways (preexcitation syn-drome). N Engl J Med 317 (1987) 65
[15] WLADIMIROFF JW, PA STEWART: Fetal therapy.Treatment of fetal cardiac arrhythmias. Br J HospMed 34 (1985) 134
Received March 20, 1989. Accepted October 16,1989.
Dr. Markus GonserUniversitäts-FrauenklinikSchleichstr. 4D-7400 TübingenWest Germany
J. Perinat. Med. 17 (1989)