Embed Size (px)
Citation preview
J Clin Pathol 1990;43:287-290
Histogenesis of ovarian malignant mixedmesodermal tumours
T J Clarke
AbstractThe histogenesis of ovarian malignantmixed mesodermal tumours, whichincludes the concept of metaplastic car-cinoma, is controversial. Four suchtumours were examined for evidence ofmetaplastic transition from carcinoma tosarcoma using morphology and reticulinstains. Consecutive sections were stainedimmunohistochemically using cyto-keratin and vimentin to determinewhether cells at the interface betweencarcinoma and sarcoma expressed bothcytokeratin and vimentin. There was noevidence ofmorphological, architectural,or immunohistochemical transitionsfrom carcinoma to sarcoma in the fourtumours studied. This suggests thatovarian malignant mixed mesodermaltumours are not metaplastic carcinomasbut are composed of histogenetically dif-ferent elements.
Department ofHistopathology,Derriford Hospital,PlymouthT J ClarkeCorrespondence to:Dr T J Clarke, AreaDepartment of Pathology,Royal Devon and ExeterHospital, Exeter EX2 5DY
Accepted for publication19 October 1989
Ovarian malignant mixed mesodermal tumoursare rare neoplasms that arise typically innulliparous, postmenopausal women.1Recently they have been referred to as "mixedMullerian tumours of high grade malignancy"or as "carcinosarcomas". The prognosis isbleak and most patients die within 12 months ofpresentation.235 Theories concerning the his-togenesis of malignant mixed mesodermaltumours of the female genital tract have beendescribed as "a matter of art rather than ofscience".6 The same theoretical problems con-
cerning histogenesis are encountered with"carcinosarcomas" at other sites such asbreast,' lung,89 colon,'0 and urinary bladder." 12
It has been suggested that ovarian malignantmixed mesodermal tumours are "metaplasticcarcinomas" in which the sarcomatous com-
ponent (homologous and heterologous) arisesdirectly from the carcinomatous component(usually glandular in type). The concept ofmetaplastic carcinomas differs from that ofcarcinosarcomas, which are regarded as
heterogeneous tumours of combination, com-
position, or collision in type.'3 This study was
undertaken to investigate whether there were
morphological, cytoarchitectural, andimmunohistochemiccal transitions from car-
cinoma to sarcoma in ovarian malignant mixedmesodermal tumours.
MethodsSections of formalin fixed, paraffin wax
287
embedded tumour tissue were cut at 4 im andstained with haematoxylin and eosin, periodicacid Schiff (PAS) before and after diastasetreatment, Caldwell and Rannie's reticulinstain, and phosphotungstic acid haematoxylin(PTAH). Sequential sections were stained bythe indirect immunoperoxidase techniqueusing monoclonal antibodies directed againstcytokeratin (PKK1 which reacts with lowmolecular weight cytokeratins of 44, 46, 52 and54 kilodaltons), vimentin, a-l-antitrypsin andmyoglobin. Appropriate positive and negativecontrols, with omission of specific antisera inthe latter, were performed. Haematoxylin andeosin stained sections were examined forsecondary fluorescence using a Leitz Dialux20ES microscope and mercury vapour lightsource epifluorescence.Four patients, aged 68, 71, 72 and 73 presen-
ted with abdominal distension and discomfortand were found to have an ovarian malignantmixed mesodermal tumour of at least FIGOstage III.'" Three of the women werenulliparous and the parity of the fourth was notknown. Three died within one year of opera-tion and one was alive and free from diseasenine years after surgery. None of the patientsreceived radiotherapy or chemotherapy aftersurgery. Necropsy was performed in onepatient who died eight days after operation.This case has been reported previously.'"
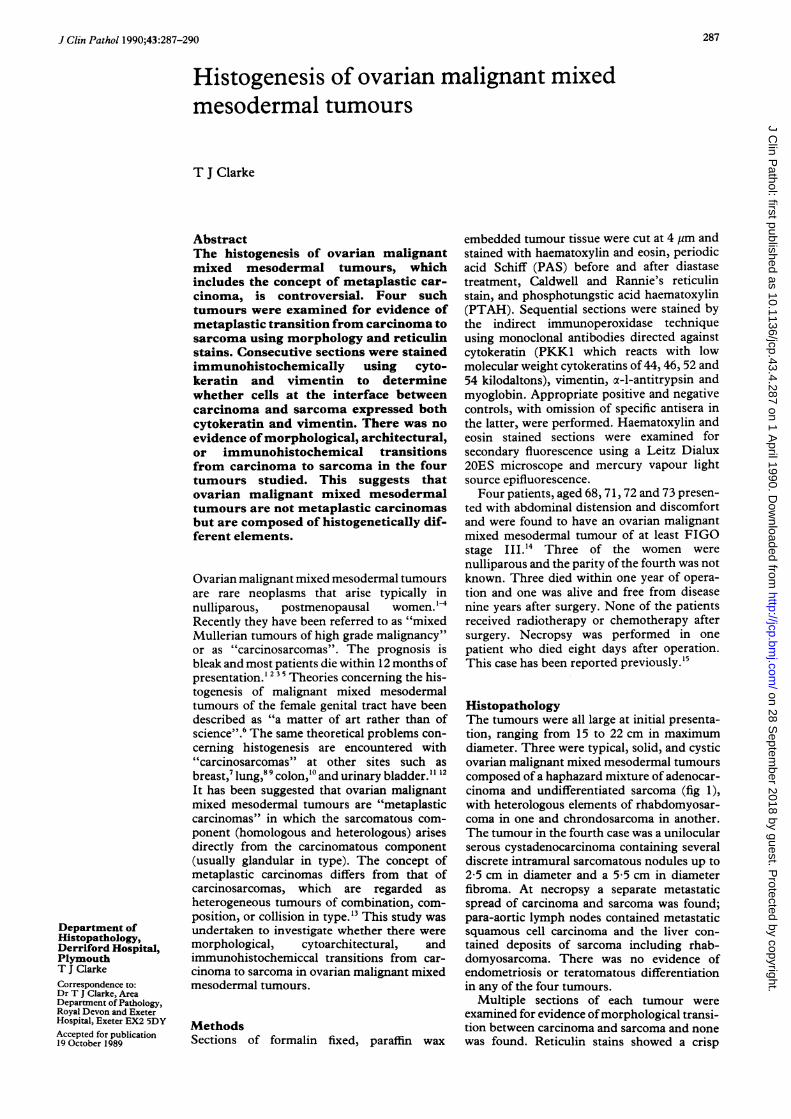
HistopathologyThe tumours were all large at initial presenta-tion, ranging from 15 to 22 cm in maximumdiameter. Three were typical, solid, and cysticovarian malignant mixed mesodermal tumourscomposed of a haphazard mixture of adenocar-cinoma and undifferentiated sarcoma (fig 1),with heterologous elements of rhabdomyosar-coma in one and chrondosarcoma in another.The tumour in the fourth case was a unilocularserous cystadenocarcinoma containing severaldiscrete intramural sarcomatous nodules up to2-5 cm in diameter and a 5 5 cm in diameterfibroma. At necropsy a separate metastaticspread of carcinoma and sarcoma was found;para-aortic lymph nodes contained metastaticsquamous cell carcinoma and the liver con-tained deposits of sarcoma including rhab-domyosarcoma. There was no evidence ofendometriosis or teratomatous differentiationin any of the four tumours.
Multiple sections of each tumour wereexamined for evidence ofmorphological transi-tion between carcinoma and sarcoma and nonewas found. Reticulin stains showed a crisp
on 28 Septem
ber 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.43.4.287 on 1 A
pril 1990. Dow
nloaded from
288
_i4
Figure I Ovarian malignant mixed mesodermal tumourcomposed of adenocarcinoma and sarcoma.(Haematoxylin and eosin.)
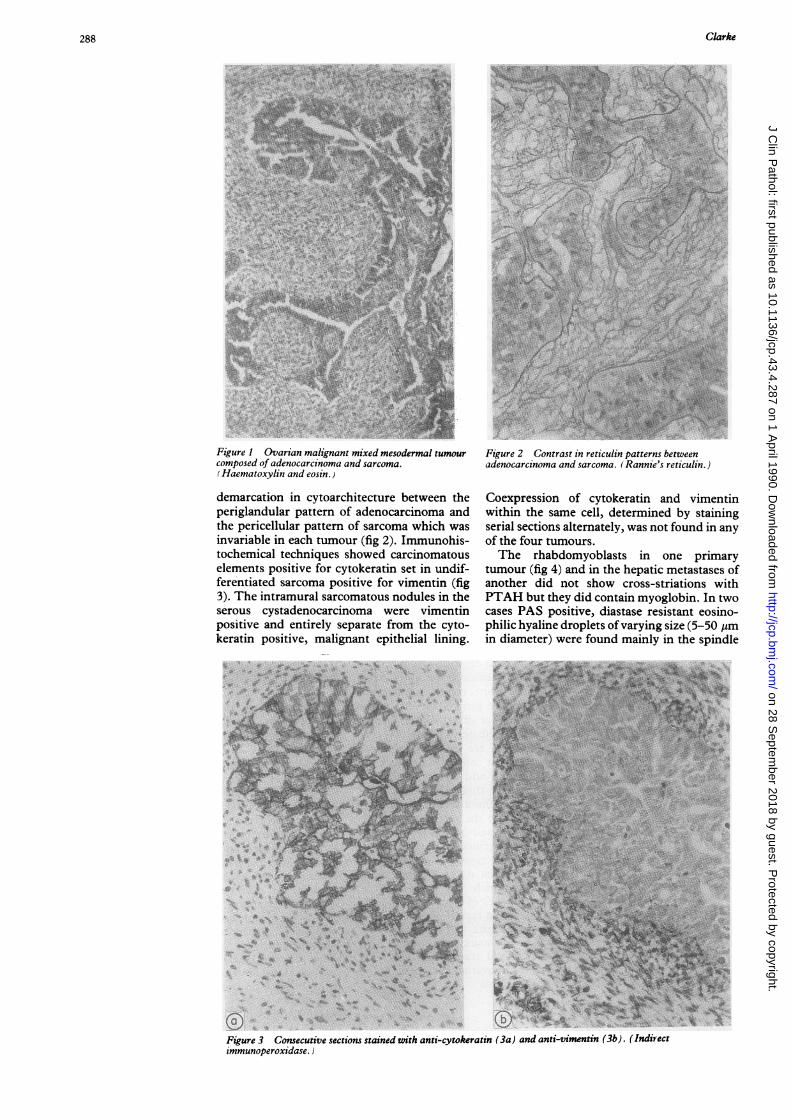
demarcation in cytoarchitecture between theperiglandular pattern of adenocarcinoma andthe pericellular pattern of sarcoma which wasinvariable in each tumour (fig 2). Immunohis-tochemical techniques showed carcinomatouselements positive for cytokeratin set in undif-ferentiated sarcoma positive for vimentin (fig3). The intramural sarcomatous nodules in theserous cystadenocarcinoma were vimentinpositive and entirely separate from the cyto-keratin positive, malignant epithelial lining.
}'So r¢EaCjT >
r4̂, + * sx
~N_
0 % .., t¶
-.'If;'a~~~~~~~~~~~~~~~~~A
40 J~~~~
Figure 2 Contrast in retzculin patterns betweenadenocarcinoma and sarcoma. (Rannie's reticulin.)
Coexpression of cytokeratin and vimentinwithin the same cell, determined by stainingserial sections alternately, was not found in anyof the four tumours.The rhabdomyoblasts in one primary
tumour (fig 4) and in the hepatic metastases ofanother did not show cross-striations withPTAH but they did contain myoglobin. In twocases PAS positive, diastase resistant eosino-philic hyaline droplets of varying size (5-50 pmin diameter) were found mainly in the spindle
tt~ & . ,X }rt..*....
Kr-' % *...............
WE~~~~~~~~~~~
-844291 *v>~~~~~~~~~~~~~~~~~~~~~~~~~~~.
W
N~~~~~~~~~~~~~~~~~~~
90 SVei
...
Figure 3 Consecutive sections stained with anti-cytokeratin (3a) and anti-vimentin (3b). (Indirectimmunoperoxidase.)
Clarke
4'i'
.3..Q
I'd
on 28 Septem
ber 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.43.4.287 on 1 A
pril 1990. Dow
nloaded from

Histogenesis of ovarian malignant mixed mesodermal tumours
Figure 4Rhabdomyoblasts stainedwith anti-myoglobin(Indirectimmunoperoxidase.)
cell sarcomatous component. They staineddeep blue with PTAH but did not showsecondary fluorescence in sections stained withhaematoxylin and eosin or contain ac-l-antitrypsin.
DiscussionThree tumours corresponded with the typicaldescriptions of ovarian malignant mixedmesodermal tumours, being composed of adisorganised mixture of carcinoma and sar-
coma with a predominance of adenocarcinomaof serous type.2 In one case, however, thetumour was a "forme fruste" ovarian malig-nant mixed mesodermal tumour from whichthe separate metastatic spread ofcarcinoma andsarcoma nevertheless fulfilled the necessarydiagnostic criterion. The presence of rhab-domyosarcoma in metastases alone has beennoted before.2 Ovarian endometriosis hasoccasionally been described in association withovarian malignant mixed mesodermaltumours,''`20 but none was found in thisseries. The eosinophilic hyaline droplets were
tinctorially similar to those in previousreports2'2- but did not show secondary fluores-
23 21-23cence or contain c-l-antitrypsin.It has been suggested that ovarian malignant
mixed mesodermal tumours are metaplasticcarcinomas, and morphological transitionshave been described. 12 The intraperitoneal andlymphatic spread of ovarian malignant mixedmesodermal tumours is consistent with thismode of spread of a carcinoma,24 but themetastases are frequently sarcomatous.2Masuda grew a carcinoma cell line derivedfrom an ovarian malignant mixed mesodermaltumour in low cell density tissue culture andfound that there was a- loss of epithelial charac-teristics.25 This phenomenon has been des-cribed, however, in tissue culture using other
epithelial cell lines.26 It is due to decreased cellto cell contact27 and is, therefore, not proof ofmetaplasia. When examined by electronmicroscopy, two ovarian malignant mixedmesodermal tumours showed no evidence oftransitional cell forms or discontinuity in thebasal lamina separating carcinoma from sar-coma."8 Electron microscopy was not used inthis series but the difference in reticulin pat-terns between the two components supportsthe previously reported ultrastructural find-ings. The biphasic pattern of cytokeratin andvimentin expression has been describedbefore29 but immunohistochemical transitionsbetween the two elements were not inves-tigated.The light, electron microscopic, and
immunohistochemical findings suggest thatovarian malignant mixed mesodermal tumoursare not metaplastic carcinomas-that is,tumours in which the sarcomatous componentderives from the carcinomatous. Meyer clas-sified carcinosarcomas into collision, combina-tion, and composition types."3 There is noevidence to suggest that ovarian malignantmixed mesodermal tumours are collisiontumours formed following coalescence of twoseparate tumours; moreover, ovarian carcin-omas are common and sarcomas are rare."6 In acombination tumour the carcinosarcoma isthought to arise from a precursor stem cell(Ahnzelle) which differentiates along twodivergent pathways. There is evidence fromtissue culture experiments using cells frommalignant mixed mesodermal tumours to sup-port"' and refute3' this; but, again, extrapola-tion from tissue culture work is fraught withdifficulties. In a composition tumour there issynchronous malignant change in adjacentepithelium and stroma. This change wasevident in the forme fruste ovarian malignantmixed mesodermal tumour in this series. Theother three tumours may have been either ofcombination or composition in type.
In conclusion, examination of the generalmorphology, cytoarchitecture, and immuno-histochemistry of four ovarian malignantmixed mesodermal tumours produced noevidence to suggest that such neoplasms aremetaplastic carcinomas, and it is suggested thatcarcinosarcomas at other sites be reexamined inthe manner described in this study.
This paper is based on work presented at the Association ofClinical Pathologists' Junior Members Research Award inLondon on October 14, 1988.
I thank Mrs Carol Stoddard for technical assistance. Mrs GMarshall for typing the manuscript, and Professor P P Anthonyfor constructive criticism.
1 Dehner LP, Norris HJ, Taylor HB. Carcinosarcomas andmixed mesodermal tumors of the ovary. Cancer1971;27:207-16.
2 Fenn ME, Abell MR. Carcinosarcoma of the ovary. Am JObstet Gynecol 1971;1 10:1066-74.
3 Dictor M. Malignant mixed mesodermal tumor ofthe ovary:a report of 22 cases. Obstet Gynceol 1985;65:720-4.
4 Barwick KW, LiVolsi VA. Malignant mixed mesodermaltumors of the ovary: a clinico-pathologic assessment of 12cases. Am J Surg Pathol 1980;4:37-42.
5 Hanjani P, Petersen RO, Lipton SE, Nolte -SA. Malignantmixed mesodermal tumors and carcinosarcoma of theovary: report of eight cases and review of the literature.Obstet Gynecol Surv 1983;38:537-45.
289
on 28 Septem
ber 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.43.4.287 on 1 A
pril 1990. Dow
nloaded from

Clarke
6 Marshall RJ. Mixed Mullerian tumours of the gyn-aecological system other than endometrial tumours. In:Williams CJ, Kirkorian JG, Green MR, Raghavan D, eds.Textbook of uncommon cancer. Chichester: J Wiley,1988:65-75.
7 Oberman HA. Metaplastic carcinoma of the breast: aclinicopathologic study of 29 patients. Am J Surg Pathol1987;11:918-29.
8 Huszar M, Herczeg E, Lieberman Y, Geiger B. Distinctiveimmunofluorescennt labelling of epithelial and mesen-chymal elements of carcinosarcoma with antibodiesspecific for different intermediate filaments. Hum Pathol1984;15:532-8.
9 Addis BJ, Corrin B. Pulmonary blastoma, carcinosarcomaand spindle-cell carcinoma: an immunohistochemicalstudy of keratin intermediate filaments. J Pathol1985;147:291-301.
10 Weidner N, Zekan P. Carcinosarcoma ofthe colon: report ofa unique case with light and immunohistochemicalstudies. Cancer 1986;58:1126-30.
11 Young RH. Carcinosarcoma of the urinary bladder. Cancer1987;59:1333-8.
12 Fromowitz FB, Bard RH, Koss LG. The epithelial origin ofa malignant mesodermal mixed tumor of the bladder:report of a case with long-term survival. J Urol1984;132:978-81.
13 Meyer R. Beitrag zur verstandigung uber die namengebungin der geschwulstlehre. Zentralblatt fur Allgemeine Path-ologie und Pathologische Anatomie (Jena) 1919;30:291-6.
14 Intemational Federation of Gynaecology and Obstetrics.Classification and staging of malignant tumors of thefemale pelvis. Acta Obstet Gynaecol Scand 1971;50:1-7.
15 Clarke TJ. Sarcoma-like mural nodules in cystic serousovarian tumours. J Clin Pathol 1987;40:1443-4
16 Azoury RS, WoodruffJD. Primary ovarian sarcomas: reportof 43 cases from the Emil Novak Ovarian TumourRegistry. Obstet Gynecol 1971;37:920-41.
17 Cooper P. Mixed mesodermal tumor and clear cell carcin-oma arising on ovarian endometriosis. Cancer1978;42:2827-3 1.
18 Saunders P, Price AB. Mixed mesodermal tumour of theovary arising in pelvic endometriosis. J Roy Soc Med1970;63: 1050-1.
19 Marchevsky AM, Kaneko M. Bilateral ovarian
endometriosis associated with carcinosarcoma of the rightovary and endometrioid carcinoma of the left ovary. Am JClin Pathol 1978;70:709-12.
20 Ricci M, Santini G, Mazzoleni G, Gelli MC, Bazzocchi F.Malignant mixed mesodermal tumours of the ovary: aclinico-pathological study of four new cases. Arch AnatCytol Pathol 1987;35:41-3.
21 Dictor M. Ovarian malignant mixed mesodermal tumor: theoccurrence of hyaline droplets containing s,-antitrypsin.Hum Pathol 1982;13:930-3.
22 Dictor M. Alpha-l-antitrypsin in a malignant mixedmesodermal tumor of the ovary. Am J Surg Pathol1981 ;5:543-50.
23 Dervan PA. Alpha-l-antitrypsin haematoxylin and eosinfluorescence: a rapid, useful screening technic. Am J ClinPathol 1984;82:188-90.
24 Czemobilsky B, LaBarre GC. Carcinosarcomas and mixedmesodermal tumor of the ovary: a clinicopathologicanalysis of 9 cases. Obstet Gynecol 1968;31:21-32.
25 Masuda A, Takeda A, Fukkami H, Yamada C, MatsuyamaM. Characteristics of cell lines established from a mixedmasodermal tumor of the human ovary. Cancer1987;60:2696-703.
26 Ben-Ze'ev A. Differential control of cytokeratin and vimen-tin synthesis by cell-cell contact and cell spreading incultured epithelial cells. J Cell Biol 1984;99: 1424-33.
27 Lane EB, Hogan BLM, Kurkinen M, Garrels JI. Co-expression of vimentin and cytokeratins in parietalendoderm cells of early mouse embryo. Nature1983;303:701-4.
28 Geisenger KR, Dabbs DJ, Marshall RB. Malignant mixedHullerian tumours: an ultrastructural and immunohisto-chemical analysis with histogenetic considerations. Cancer1987;59:1781-90.
29 del Poggetto CB, Virtanen I, Lehto V-P, Wahlstrom T,Saksela E. Expression of intermediate filaments in ovarianand uterine tumors. Int J Gynecol Pathol 1983;1:359-66.
30 Takeda A, Matsuyama W, Kuzuya K, Chihara T, Tsubou-chi S, Takeuchi S. Mixed mesodermal tumor of the ovarywith carcinoembryonic antigen and alkaline phosphataseproduction. Cancer 1984;53:103-12.
31 Centola GM. Long-term growth of a heterologous mixedMullerian tumor of the ovary. Invasion Metastasis1986;6: 123-32.
290
on 28 Septem
ber 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.43.4.287 on 1 A
pril 1990. Dow
nloaded from





























